Embed Size (px)
Citation preview
THE EFFICACY OF THIOSINAMINUM 1X CREAM ON STRIAE.
By
Koketso Ramoupi
Student number: 820410563
A dissertation submitted to the Faculty of Health Sciences University of Johannesburg,
in partial fulfillment of the requirements for the Degree
Master of Technology: Homoeopathy
SUPERVISOR: ------------------------------ ------------------
Dr. R. Razlog Date
CO- SUPERVISOR: ------------------------------ ------------------
Dr. R. Moiloa Date
ii
DECLARATION
I declare that this thesis is my own unaided work. It is being submitted for the Degree of Master of
Technology in Homoeopathy at the University of Johannesburg. It has not been submitted before for
any degree or examination, at any other Technikon or University.
SIGNATURE OF CANDIDATE: ----------------------
Koketso Ramoupi
iii
ABSTRACT
Striae are linear scars in the dermis which arise from rapid stretching of the skin over weakened
connective tissue (de Angelis & Adatto, 2010).
Striae occur when collagen production cannot keep pace with a sudden growth of the underlying
tissues. Striae have no medical consequences but are frequently distressing to those afflicted. These
disfiguring marks are usually caused by excessive stretching of the skin that may occur with
pregnancy, adolescent growth spurts, obesity and weightlifting (Kang & Arbor, 1998).
Striae usually appear on the abdomen, thighs, buttocks, breasts and extremities. Patients’ quality of
life can be enhanced with the effective management of these unsightly marks. Modalities of
treatments that exist for the treatment of striae have been advocated with varying success and side
effects (Manuskiatti et al., 2010).
The aim of this study was to determine the efficacy of the topical application of a homoeopathic
preparation Thiosinaminum 1X on the appearance of striae.
The research was a double-blind placebo controlled study which took place at the Homoeopathy
Health Centre which is located at the University of Johannesburg(Doornfontein campus). Forty
female participants aged between eighteen and thirty-five were randomly selected to take place in
the study. The study was conducted over a period of twelve weeks. On recruitment, the participants
were required to read and sign the information sheet (Appendix A) and consent form (Appendix B)
assisted by the researcher. Participants were asked to complete a questionnaire (Appendix C) to
determine contributing factors e.g. duration of the stretch marks, the cause of the stretch marks and
any disease that may contribute to the formation of stretch marks. A pertinent case and vital signs
were taken at the initial consultation to eliminate any pathologies. All potential participants were
required to present with stretch marks on the thighs or buttocks present for at least 6 months prior to
the study. The stretch marks needed to have had a minimum length of 50mm and a maximum length
of a 100mm. The researcher was responsible for choosing the designated area that was treated. The
most distinct striae were selected by the researcher according to criteria for treatment. The
researcher took photographs of the treatment areas at the commencement of the study and this was
repeated at the end of the study (Appendix I). The length of the most prominent stretch mark
(according to criteria) below was also measured on the commencement of the study. To physically
iv
measure the most prominent stretch mark a string and a ruler was utilized. The same ruler and ball
of string was used each time to ensure validity of the results. A new piece of string was cut and tied
in a knot at the tip and placed on the stretch mark itself to mould to its shape and thereafter it was
placed on a ruler to determine the measurements in millimeters. To ensure that the same stretch
mark was measured every time, the researcher measured out the distance between the stretch mark
and a defined anatomical point for all the participants. The stretch mark was traced using plotting
paper.
The participants were required to apply the cream twice daily for the duration of the study.
Participants were able to rate their satisfaction on a monthly basis by completing a questionnaire.
The results of the study indicated that there was no improvement in the length of striae however
there was more improvement in satisfaction ratings throughout the study from the experimental
group.

v
DEDICATION
This dissertation is dedicated to my mother, Tsholofelo Ramoupi, my father Vincent Tlhoiwa, my
sister Lebogang Sedikwe and the rest of my family as well as everyone else who has supported me.
Most importantly it is dedicated to God. Thank you for always believing in me.
vi
ACKNOWLEDGEMENT
I would like to thank the following people for their valuable contributions:
My supervisor Dr. Razlog and co-Supervisor Dr. Moiloa for their guidance, supervision and
precious time.
Dr. Reshma Patel for her support, guidance and motivation.
My statician Juliana( Statkon) for her advice on statistical analysis.
vii
TABLE OF CONTENTS
TITLE PAGE i
DECLARATION ii
ABSTRACT iii
DEDICATION iv
ACKNOWLEDGEMENT v
1 INTRODUCTION 1
1.1 Purpose of the study 1
1.2 Problem statement 1
1.3 Hypothesis 1
1.4 Null Hypothesis 2
LITERATURE REVIEW 3
2.1 Introduction 3
2.2 Anatomy of the skin 4
2.2.1 Epidermis 4-5
2.2.2 Dermis 6
2.3 Types of striae 6
2.4 Structure and Role of collagen in the development of striae 7
2.5 Fitzpatrick skin types 8
2.6 Histopathology of striae 9
viii
2.7 Aetiology of striae 9
2.8 Clinical features 10
2.9 Pathophysiology of striae 11
2.9.1 Connective tissue disorders 11
2.9.2 Obesity 11
2.9.3 Pregnancy 12
2.9.4 Endocrine disorders 13
2.9.5 Adolescence growth spurt 14
2.10 Current treatment of striae 15
2.10.1 Tretinoin therapy 15
2.10.2 Chemical peels 15
2.10.3 Microdermabrasion 16-17
2.10.4 Laser therapy 17-18
2.10.5 Preventative measures 18-19
2.10.6 Lifestyle interventions 19-20
2.11. Homoeopathy 20
2.11.1 Law of Similars 20
2.11.2 Homoeopathic potencies 20-21
2.11.3 Homoeopathic prescription 21
2.12 Thiosinaminum 22
2.12.1 Origin of Mustard seed 22-23
ix
2.12.2 Homoeopathic uses 23
2.13 Indicated Homoeopathic Remedies 23-24
2.14 Homoeopathic dispensing 24-25
2.15 Related research 25
3 METHODOLOGY AND DATA COLLECTION 27
3.1 Research design 27
3.2 Research sample 27
3.2.1 Inclusion criteria 27
3.2.2 Exclusion criteria 27-28
3.3 Research procedure and design 28-29
3.4 Medication and administration 29
3.5 Data collection and analysis 29-30
3.6 Reliability and validity 30
4 Ethics 30
4 RESULTS 31
4.1 Introduction 31
4.2 Contents of the cream 31
4.3 Data Analysis 31-32
x
4.4 Participants’ mean weight and mean length of striae before and after treatment 32
4.5 Evaluation of photographs before and after treatment using the quartile
grading scale 32-33
4.6 Duration of time that participants have been afflicted by striae 34
4.7 Main causative factors involved in striae formation 34-35
4.8 Participants’ self-assessment of improvement in striae appearance over 36-39
time
5 DISCUSSION 40
5.1 Changes in weight observed in both groups 40
5.2 Changes in length in both groups 41-42
5.3 The quartile grading scale before and after treatment : Control 42-43
and Experimental groups
5.4 Duration of time : Control and Experimental groups 42-43
5.5 Patient monthly self-assessment of overall striae improvement 44-45
5.6 Overall patient assessment results 45-46
6 CONCLUSION 47
6.1 Conclusions 47
6.2 Recommendations 47-48
7 REFERENCES 49-54

xi
8 APPENDICES
A Participant Information sheet 55-56
B Consent form 57
C Questionnaire- Contributing Factors for striae development 58
D Questionnaire- Participant’s satisfaction scores 59
E Questionnaire- Physical appearance of striae 60-61
F Advertisement Poster 62
G Master Formula and Method Document 63
H Standard Operating Procedures: Research Photographs 64
I Research photographs 65-68
xii
LIST OF TABLES
Table 4.1 Effect of Thiosinaminum 1X treatment of striae on mean 32
weight and mean striae length of participants
Table 4.2 Results of the quartile grading scale 33
Table 4.3 Overall duration of time afflicted by striae 34
Table 4.4a Causative factors of striae development in the Control group 35
Table 4.4b Causative factors of striae development in the Experimental group 36
Table 4.5 Participant’s monthly self-assessment of improvement in striae 37
appearance

xiii
LIST OF FIGURES
Figure 4.4.3 (a) Participants’ assessment for improvement - Month 1 38
Figure 4.4.3 (b) Participants’ assessment for improvement – Month 2 38
Figure 4.4.3 (c) Participants’ assessment for improvement – Month 3 39
Figure 5.5 Patient monthly self-assessment of overall striae improvement 45
1. INTRODUCTION
1.1 Purpose of the study
The purpose of the study is to determine the efficacy of the topical application of a homoeopathic
preparation Thiosinaminum 1X on the appearance of striae.
1.2 Problem statement
Striae, commonly known as stretch marks, are an undesirable cutaneous disorder commonly found
on the abdomen, breasts, hips and thighs (Manuskiatti et al., 2010). Striae have no medical
consequences but are frequently distressing to those afflicted. These disfiguring marks are usually
caused by excessive stretching of the skin that may occur with pregnancy, adolescent growth spurts,
obesity and weightlifting (Kang & Arbor, 1998).
Due to the undesirable appearance of striae, some women (especially adolescents) may feel insecure
about their bodies and this can interfere with their social lives (Papadopoulos & Walker, 2003).
Many of these women are active and participate in activities that may expose their abdomen and
leave them feeling self-conscious about their appearance (Salter & Kimball, 2006).
Patients’ quality of life can be enhanced with the effective management of these unsightly
marks. Modalities of treatments that exist for the treatment of striae have been advocated
with varying success and side effects (Manuskiatti et al., 2010).
Thiosinaminum, prepared as a homoeopathic remedy, is indicated for the treatment of striae;
however no research exists on its efficacy. It is also used as a resolvent, externally and internally for
dissolving scar tissue, tumors, strictures and adhesions (Boericke, 2005)
1.3 Hypothesis
The topical application of a homoeopathic preparation Thiosinaminum 1X will improve the
appearance of striae in females.

2
1.4 Null hypothesis
The null hypothesis states there will be no significant difference between striae that have
been treated with topical application of Thiosinaminum 1X and striae that have been treated
with the placebo cream. The topical application of a homoeopathic preparation
Thiosinaminum 1X will thus be no more effective in improving the appearance of striae in
females than the placebo treatment.
3
2. LITERATURE REVIEW
2.1 Introduction
Striae are linear scars in the dermis which arise from rapid stretching of the skin over weakened
connective tissue (de Angelis & Adatto, 2010). Since ancient times, stretch marks have been a great
concern for women. This is more so evident in the writings of the ancient Egyptians who described
several formulations for the treatment of stretch marks. One of the most frequently referenced
therapies in frankincense was obtained from the Boswelia thurifera tree found in Somalia and
Ethiopia (Salter & Kimball, 2006).
Striae occur when collagen production cannot keep pace with a sudden growth of the underlying
tissues. Striae are bands of thin wrinkled skin, initially red but which become purple and white,
resulting from atrophy of the dermis and overextension of the skin (Piper, 2008).
While striae occur equally among races, they are more prevalent in women (de Angelis & Adatto,
2010). Clinically, striae appear as erythematous (striae rubra) or hypopigmented (striae alba) linear
bands of atrophic skin, usually involving the abdomen, thighs, buttocks, breasts and extremities
(Manuskiatti et al., 2010). Striae develop in a variety of circumstances including continuous
stretching of the skin, such as weight changes, adolescent growth spurts and pregnancy. The
appearance of striae on the body, depending on their location and severity can have a negative social
and psychological effect (Papadopoulos & Walker, 2003). Modalities of treatments available for
striae include; topical applications of tretinoin, microdermabrasion, 585nm-pulsed dye laser,
intensed pulsed light (IPL), and targeted phototherapy. All these treatments have been advocated
with variable successes and side effects (Manuskiatti et al., 2010).
The two major drawbacks of current treatments of striae are transient improvement which requires
maintenance treatments and an increased risk of post-treatment post-inflammatory
hyperpigmentation (PIH) in darker skinned individuals (de Angelis & Adatto, 2010).
Improving the appearance of striae, particularly striae alba has remained a challenge due to the
limited availability of effective and low-risk treatment options (Stotland et al., 2008). The main
desire of those affected with striae is to prevent or treat these lesions (Salter & Kimball, 2006).
4
Thiosinaminum, prepared as a homoeopathic remedy is used as a resolvent, externally and internally
to dissolve scar tissues, tumors, strictures and adhesions. It is also indicated for the treatment of
striae; however no research exists on its efficacy (Boericke, 2005).
2.2 Anatomy of the skin
Striae are visible though the skin, which is the largest organ in the human body. The skin has many
functions including regulating temperature, maintaining water and electrolyte balance and sensing
painful and pleasant stimuli. The most important fact about the skin is that it distinguishes people as
individuals because of the differences in skin colour, texture and folds (Beers et al., 2003).
The skin is composed of three layers namely; the epidermis, dermis and fat layer (Beers et al.,
2003).
2.2.1 Epidermis
The epidermis is the thin, tough top layer of the skin whose basic function is to prevent most
bacteria, viruses and other foreign substances from entering the body (Beers et al., 2003). The
epidermis is continually replacing itself and this is even more evident in cases where it has been
injured or diseased. Within the epidermis there are five less-distinct sub layers namely (see Figure
2.1); the stratum corneum, stratum lucidum, stratum granulosum, stratum spinosum (stratum
mucosum Mapighii) and stratum basale (stratum germinativum).
5
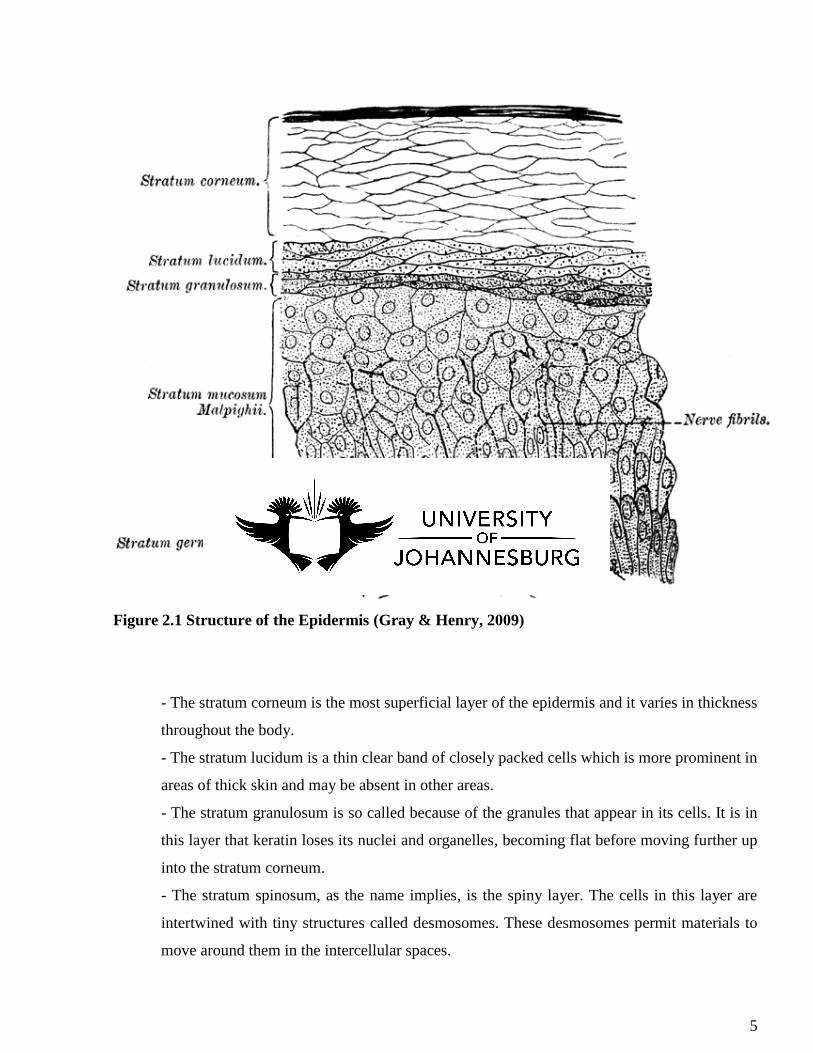
Figure 2.1 Structure of the Epidermis (Gray & Henry, 2009)
- The stratum corneum is the most superficial layer of the epidermis and it varies in thickness
throughout the body.
- The stratum lucidum is a thin clear band of closely packed cells which is more prominent in
areas of thick skin and may be absent in other areas.
- The stratum granulosum is so called because of the granules that appear in its cells. It is in
this layer that keratin loses its nuclei and organelles, becoming flat before moving further up
into the stratum corneum.
- The stratum spinosum, as the name implies, is the spiny layer. The cells in this layer are
intertwined with tiny structures called desmosomes. These desmosomes permit materials to
move around them in the intercellular spaces.
6
- The stratum basale is the ‘basement’ of the epidermis; it anchors the epidermis to the
dermis. All germinal cells, cells of regeneration for all the sublayers of the epidermis are
contained within this layer (Hill, 2006).
2.2.2 Dermis
The dermis which is the layer beneath the epidermis is a thick layer of fibrous and elastic tissue
(made mostly of proteins, collagen and fibrillin) that gives the skin its flexibility and strength. It
contains nerve endings, glands, hair follicles, and blood vessels. It is from this layer that stretch
marks originate (Beers et al., 2003). The dermis is crisscrossed with three types of fibres; reticular,
collagen and elastin which form a network that creates stability for the skin. The dermis is further
divided into the papillary and reticular layers based on differences in collagen texture.
The papillary dermis is the most superficial layer of the dermis and is the first layer of the skin to
contain capillary blood vessels, small nerves and lymphatic vessels. It is specifically responsible for
thermoregulation. The reticular dermis is located beneath the papillary dermis and rests on the thick
pad of fat known as subcutaneous tissue. Within the reticular dermis are structures called rete pegs,
which extend up into the epidermis to hold the dermis to the epidermis (Hill, 2007).
The fat layer helps insulate body from heat and cold, provides protective padding and serves as a
storage area (Beers et al., 2003).
Collagen and elastin fibres which are found in the dermis of the skin, are long-chain molecular
proteins that lie on top of the skin and bind water, preventing water loss. Collagen helps to prevent
wrinkling of the skin and the development of striae, thus keeping the skin smoother (Lees, 2007).
2.3 Types of striae
Striae can be classified according to the three different stages involved in their maturation. Initially
striae appear active with a pink to violaceous colour with notable surface depression. These striae
rubra represent the acute phase. The sub-acute stage is characterized by purpuric striae. Striae alba
represent the chronic stage and are characterized by white or hypopigmented, atrophied striae (de
Angelis & Adatto, 2010). Over time, the colour gradually fades, and the lesions exhibit a normal or
7
lighter-than-normal skin colour accompanied by fine wrinkles and surface depressions. These
characteristics are representatives of atrophic permanent striae (Kang & Arbor., 1998).
Histopathological analysis has shown striae alba to be similar to scars, demonstrating a thinned
epidermis with flattening of the rete pegs (Stotland et al., 2008).
Striae are referred to as striae gravidarum when they occur in pregnancy (Osman et al., 2007).
2.4 Structure and Role of collagen in the development of striae
Collagen is an insoluble protein found in connective tissues. It is a major constituent of connective
tissue and is the most abundant protein in the body. It is found in the skin, bones, ligaments and
cartilage. Collagen contributes to a range of structures from brain to cornea, thus its components
vary; there are at least 30 distinct types of collagen inhabiting the body (Hill, 2006). Collagen is not
flexible and this is what gives skin its firmness and inability to stretch (Lees, 2007).
It is due to the basis of the collagen structure that leads to its high strength and ability (Figure 2.2).
The smallest building blocks of collagen are called tropocollagen molecules and they are five to ten
times stronger than steel. Experiments have shown that collagen displays a design that consists of a
staggered assembly of tropocollagen molecules known as collagen fibrils with lengths of
approximately 300 nanometres (Buehler, 2006)
Type I Collagen runs throughout the dermis and it is responsible for the skin’s tensile strength and
for providing the skin with its youthful appearance of tightness, firmness, and fullness. The collagen
found in the papillary dermis is finely textured and contains projections called papillae that fit the
dermis to the epidermis (Hill, 2006). Skin distension leads to excessive mast cell degranulation with
subsequent damage of collagen and elastin fibres. This may then lead to the development of striae
(Samer, 2009).

8
Figure 2.2 Structure of a collagen molecule (Science Daily, 2006)
2.5 Fitzpatrick skin types
The Fitzpatrick classification system is based on how often a person burns and how well they tan
when exposed to the sun (Osman et al., 2007). This classification is used by dermatologists to
classify an individual’s skin by hereditary pigmentation, indicating their resistance to sun-related
damage and sunburn. The lower the number/type, the lighter the skin colour and the more the patient
is susceptible to sun-related damage or disease (Lees, 2007).
There are six different types of classification namely;
Type I – Always burns, very fair skin, red or blonde hair, blue eyes, likely freckled skin
Type II – Burns easily, tans minimally, fair skin; blue, green, hazel eyes; blonde or red hair
Type III – Sometimes burns, gradually tans, very common colouring; still fair, but with any
colour hair and eyes
Type IV – Rarely burns, always tans, typical Mediterranean Caucasian skin, medium to
heavy pigmentation
Type V – Very rarely burns, always tans, Middle-Eastern skin types, not sun sensitive
Type VI – Almost never burns, Black skin, generally never sun sensitive (Lees, 2007).

9
Skin types I-III have a lower risk for problems (e.g. skin discolouration, blotchiness,
hypopigmentation, hyperpigmentation) following cosmetic skin treatments, however skin types IV-
VI have a higher risk (Health Communities, 2007)
2.6 Histopathology of striae
Striae undergo a clinically recognizable evolution similar to that involved in scar formation or
wound healing (Kang & Arbor, 1998). Regardless of the aetiology all striae follow a natural
progression. In the early stages inflammatory changes predominate, oedema and perivascular
lymphocyte cuffing are present in the dermis. The later stage is characterized by the thinning of the
epidermis as well as the loss of the rete ridges. Elastic stains show breakage and retraction of the
elastic fibres in the reticular dermis. It is these broken elastic fibres that curl at the sides of the striae
to form a distinctive pattern. This arrangement is in contrast to normal skin which has thick, elastic
fibres with a regular distribution. The transmission electron microscopy shows the ultrastructure of
elastic and collagen fibers in striae is similar to that of normal healthy skin (Samer, 2009).
2.7 Aetiology of striae
The exact pathogenesis of striae has yet to be developed, but mechanical, hormonal, and genetic
factors may play a role. Compounding the problem is the fact that there is a paucity of research in
this area. Striae develop in a variety of circumstances, some of which involve a physical stretching
of the skin, such as large weight gain or adolescent growth spurts, and others that involve hormonal
changes, such as chronic steroid use or Cushing’s syndrome. What further confuses the picture is
that in several of these situations there is a physical component, stretching of the skin, as well as an
endocrinological change for instance, as is found during pregnancy. However, regardless of the
aetiology of the stretch marks, the effect of striae on the skin is the same (Yosipovitch et al., 2007)
Striae do not only affect females; males may also be affected though not as commonly. This may
partly be attributed to hormonal influences such as the presence of more oestrogen in women (Kang
& Arbor, 1998). It has been postulated that some hormones, like oestrogen, relaxin and
adrenocortical hormones decrease the adhesiveness between collagen fibres and increase ground
substance, which results in the formation of striae (Osman et al., 2007). Striae may also be found in

10
children who have had a growth spurt during puberty. Athletes and body builders can also develop
striae due to constant repetitive exercises (Kang & Arbor, 1998).
However it is clear that not all striae are equal. The severity and development of lesions appear to
depend more on the characteristics of the affected individual than on the circumstances involved,
suggesting a genetic component (Salter & Kimball, 2006). A study that was conducted to determine
the risk factors for the development of striae in pregnant women found that there was a strong
relationship between family history of striae and the risk of their development (Osman et al., 2007).
2.8 Clinical features
The location of striae depends in part on the circumstance under which they developed. Striae are
often symptomatic; causing burning, itching and emotional distress, but are mainly thought of as a
cosmetic nuisance and therefore, are often overlooked as not clinically significant (Salter &
Kimball, 2006).
When striae first appear they present as flattened, thinned skin with a pink hue that may be pruritic.
Gradually they increase in length and width and become violaceous in colour. The surface of striae
may be finely wrinkled. Mature striae are white, depressed and irregularly shaped bands with their
long axis parallel to the lines of skin tension. Striae are generally several centimetres long and may
be 1-10 mm wide. As striae mature over time they may fade and become inconspicuous (Samer,
2009).
Striae that occur as a result of prolonged steroid use are usually larger and wider than other types of
striae, and they also tend to involve widespread areas, occasionally including the face. Striae which
occur secondary to topical steroid use are usually due to the enhanced potency of the steroids when
using occlusive plastic wraps. These kinds of striae usually affect the flexures and may become less
visible if the offending treatment is stopped early enough (Samer, 2009).

11
2.9 Pathophysiology of striae
2.9.1 Connective tissue disorders
Marfan’s syndrome is an autosomal dominant connective tissue disorder which decreases extra
cellular microfibril formation normally required to maintain elastic fibres (Longmore et al., 2007).
People with Marfan’s syndrome are taller than expected for their age; their arm span is greater than
their height. They have long and thin fingers; most often their sternum is deformed and pushed
either outward or inward. Their joints may also be very flexible (Beers et al., 2003). Marfan’s
syndrome sufferers develop striae on their skin even without any weight change. These striae can
occur at any age and pose no health risks (Haines, 2005). In Marfan’s syndrome, some fibres and
other parts of connective tissue undergo changes that ultimately weaken the tissue. This weakened
tissue may stretch, distort and can even tear (Beers et al., 2003)
2.9.2 Obesity
Rapid weight gain resulting in tension on the skin parallel to the tensile direction may result in striae
(Novak, 2004). Obesity results from a chronic imbalance between food intake and energy
expenditure. The interaction between genetics and environmental factors is also important. Obesity
is related to a number of changes in skin physiology including effects on skin barrier function,
sebaceous glands and sebum production, collagen structure and function, wound healing,
microcirculation and macrocirculation and subcutaneous fat. In animal studies, obesity is also
associated with altered collagen structure and impaired healing. It was postulated that the decreased
mechanical strength of skin in obese mice resulted from failure of collagen deposition to match the
increase in skin surface area (Yosipovitch et al., 2007).
Striae were diagnosed in 40% of children with moderate to severe obesity and incidence was found
to be higher in those with a longer duration of obesity. Furthermore higher levels of
adrenocorticosteroids where found in obese patients with striae compared to obese patients without
striae. The clinical appearance of striae in obese patients where however found to be lighter,
narrower and less atrophic than in those with Cushing’s syndrome (Yosipovitch et al., 2007).
12
2.9.3 Pregnancy
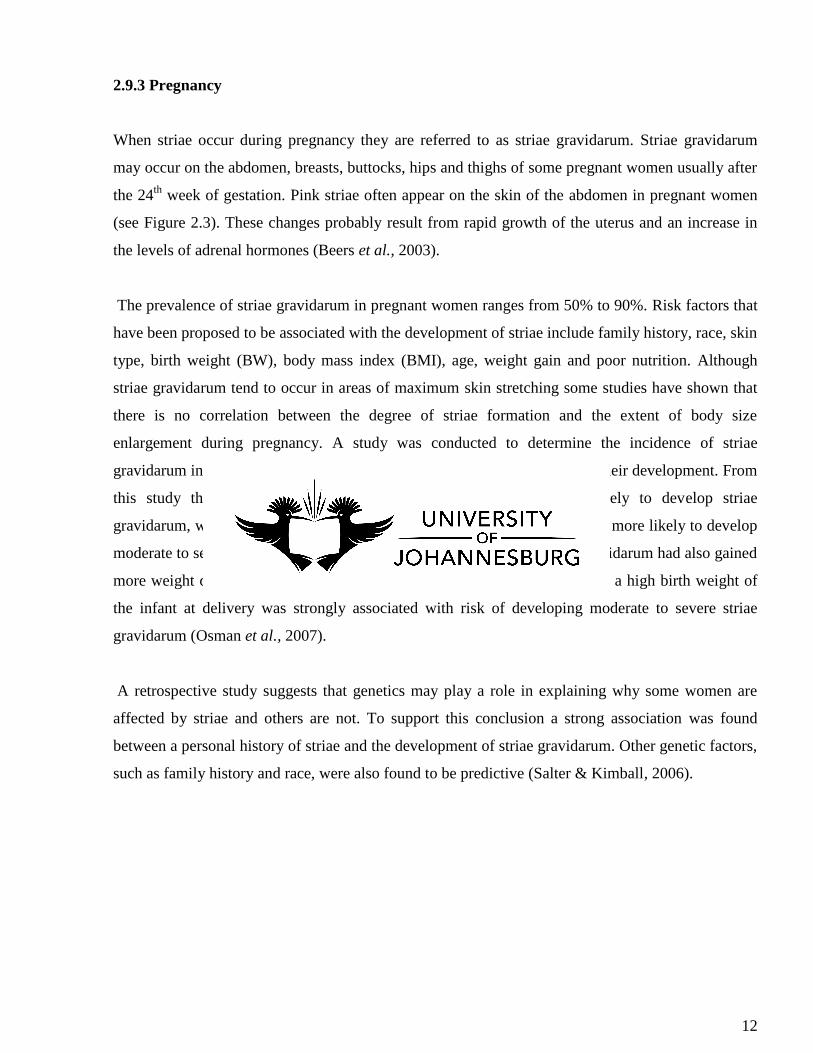
When striae occur during pregnancy they are referred to as striae gravidarum. Striae gravidarum
may occur on the abdomen, breasts, buttocks, hips and thighs of some pregnant women usually after
the 24th
week of gestation. Pink striae often appear on the skin of the abdomen in pregnant women
(see Figure 2.3). These changes probably result from rapid growth of the uterus and an increase in
the levels of adrenal hormones (Beers et al., 2003).
The prevalence of striae gravidarum in pregnant women ranges from 50% to 90%. Risk factors that
have been proposed to be associated with the development of striae include family history, race, skin
type, birth weight (BW), body mass index (BMI), age, weight gain and poor nutrition. Although
striae gravidarum tend to occur in areas of maximum skin stretching some studies have shown that
there is no correlation between the degree of striae formation and the extent of body size
enlargement during pregnancy. A study was conducted to determine the incidence of striae
gravidarum in primiparous women and identify risk factors associated with their development. From
this study the following were shown; younger women were more likely to develop striae
gravidarum, women with a positive family history of striae gravidarum were more likely to develop
moderate to severe striae gravidarum. Women who had developed striae gravidarum had also gained
more weight during pregnancy compared to those who did not. Furthermore a high birth weight of
the infant at delivery was strongly associated with risk of developing moderate to severe striae
gravidarum (Osman et al., 2007).
A retrospective study suggests that genetics may play a role in explaining why some women are
affected by striae and others are not. To support this conclusion a strong association was found
between a personal history of striae and the development of striae gravidarum. Other genetic factors,
such as family history and race, were also found to be predictive (Salter & Kimball, 2006).
13
Figure 2.3 Striae in pregnancy/ Striae gravidarum (Wala’a, 2007)
2.9.4 Endocrine disorders
Cushing’s syndrome
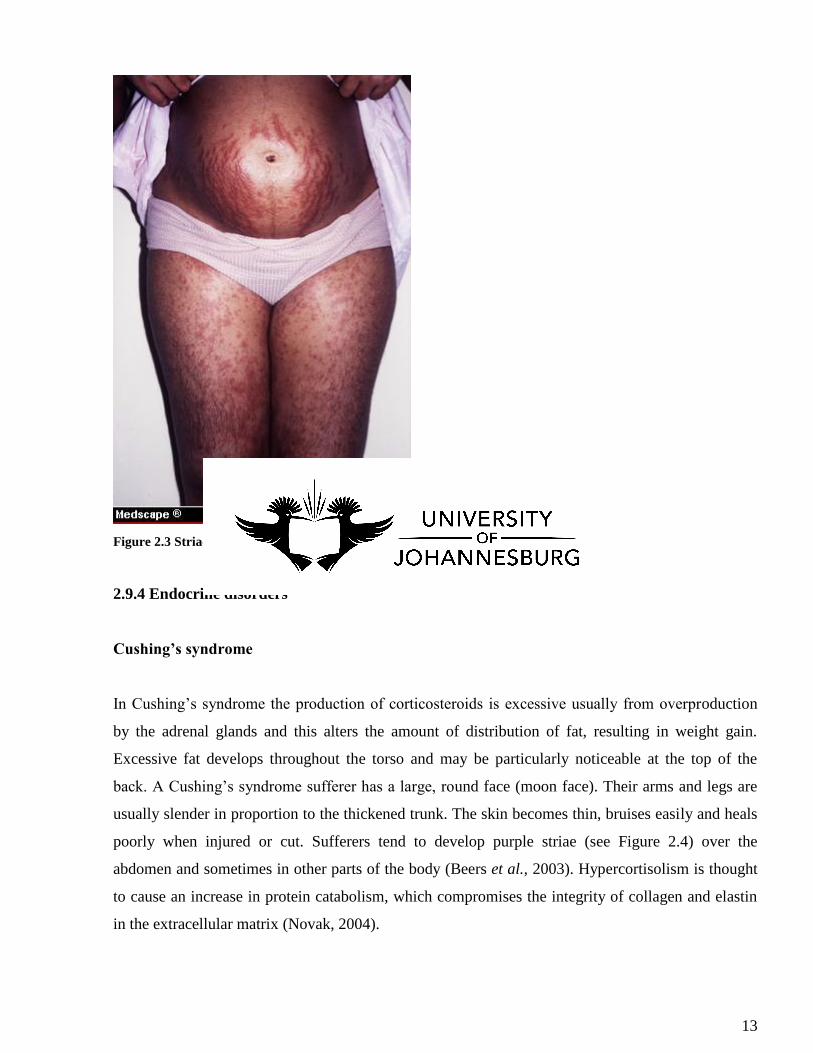
In Cushing’s syndrome the production of corticosteroids is excessive usually from overproduction
by the adrenal glands and this alters the amount of distribution of fat, resulting in weight gain.
Excessive fat develops throughout the torso and may be particularly noticeable at the top of the
back. A Cushing’s syndrome sufferer has a large, round face (moon face). Their arms and legs are
usually slender in proportion to the thickened trunk. The skin becomes thin, bruises easily and heals
poorly when injured or cut. Sufferers tend to develop purple striae (see Figure 2.4) over the
abdomen and sometimes in other parts of the body (Beers et al., 2003). Hypercortisolism is thought
to cause an increase in protein catabolism, which compromises the integrity of collagen and elastin
in the extracellular matrix (Novak, 2004).
14
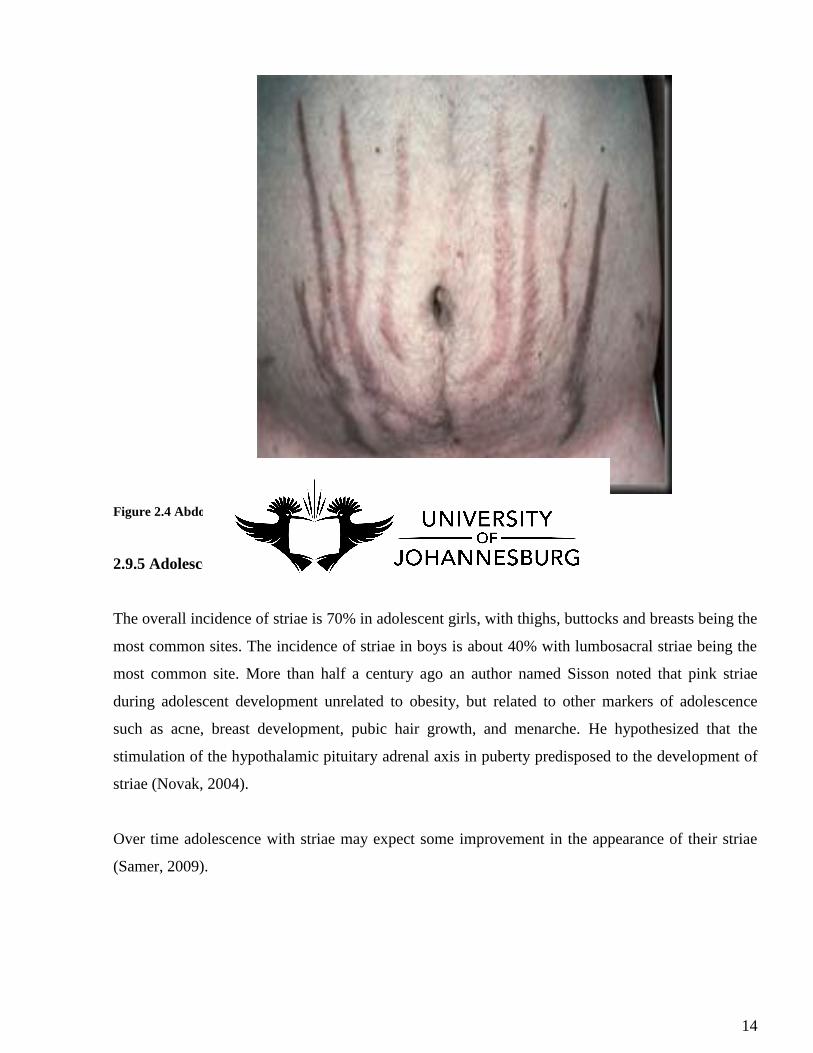
Figure 2.4 Abdominal striae in Cushing’s syndrome sufferer (Xydau, 2010)
2.9.5 Adolescence growth spurt
The overall incidence of striae is 70% in adolescent girls, with thighs, buttocks and breasts being the
most common sites. The incidence of striae in boys is about 40% with lumbosacral striae being the
most common site. More than half a century ago an author named Sisson noted that pink striae
during adolescent development unrelated to obesity, but related to other markers of adolescence
such as acne, breast development, pubic hair growth, and menarche. He hypothesized that the
stimulation of the hypothalamic pituitary adrenal axis in puberty predisposed to the development of
striae (Novak, 2004).
Over time adolescence with striae may expect some improvement in the appearance of their striae
(Samer, 2009).
15
2.10 Current treatment of striae
2.10.1 Tretinoin therapy
Tretinoin therapy has been established as a therapy for repair of dermal damage associated with
photoaged skin. Tretinoin belongs to the family of retinoids, which is Vitamin A. Retinoids act by
normalizing growth and differentiation in the keratinocytes. New studies have indicated that topical
tretinoin (0, 1%) is effective in the management of early striae to halt and potentially reverse their
progression (Hill, 2006).
Lower dose tretinoin 0,025% cream does not appear to be effective. Tretinoin is not recommended
in pregnant or breastfeeding females owing to a theoretical concern about its teratogenic effects
(Samer, 2009). In a double blind, randomized, placebo controlled trial there was a statistically
significant improvement in severity scores and decreases in length and width measurements on early
red active striae (striae rubra) on subjects who used topical tretinoin for 2 months. Comparison of
the elastin and collagen tissue stains between the tretinoin and control did not however show any
significant qualitative or quantitative differences (Stotland et al., 2008). All retinoids can be
potentially irritating, the redness, flakiness, and tender skin that present when the product is
overused make clients reluctant to carry on with the programme (Hill, 2006).
2.10.2 Chemical peels
Chemical peeling is an accelerated exfoliation induced by a chemical agent. Chemical peels are
intended to remove the outermost layers of the skin. In order to accomplish this task the chosen peel
solution induces a controlled partial-thickness injury to the skin. There are four levels of peeling;
very superficial, superficial, moderate and deep chemical peels. Each peel category is related to the
associated level of skin injury. For example, very superficial peels act only on the stratum corneum,
and moderate peels extend into the papillary dermis. The potential risks and the result of chemical
peels are directly related to the depth of the peel (Hill, 2006).
There are different types of peeling agents available, among the familiar agents are glycolic acid,
Jessner’s solution, salicylic acid, and phenol. Each peeling agent has a specific action on the skin
and therefore may be best indicated in certain conditions. Chemical peels have many benefits
16
including increasing the glycosaminoglycans (GAGs) in the ground substance of the skin,
thickening the epidermis, and increasing collage remodeling in the dermis. Best responses to
chemical peels are achieved when the patient’s objectives, the peel solution, skin indications and
clinician’s ability all coincide (Hill, 2006).
2.10.3 Microdermabrasion
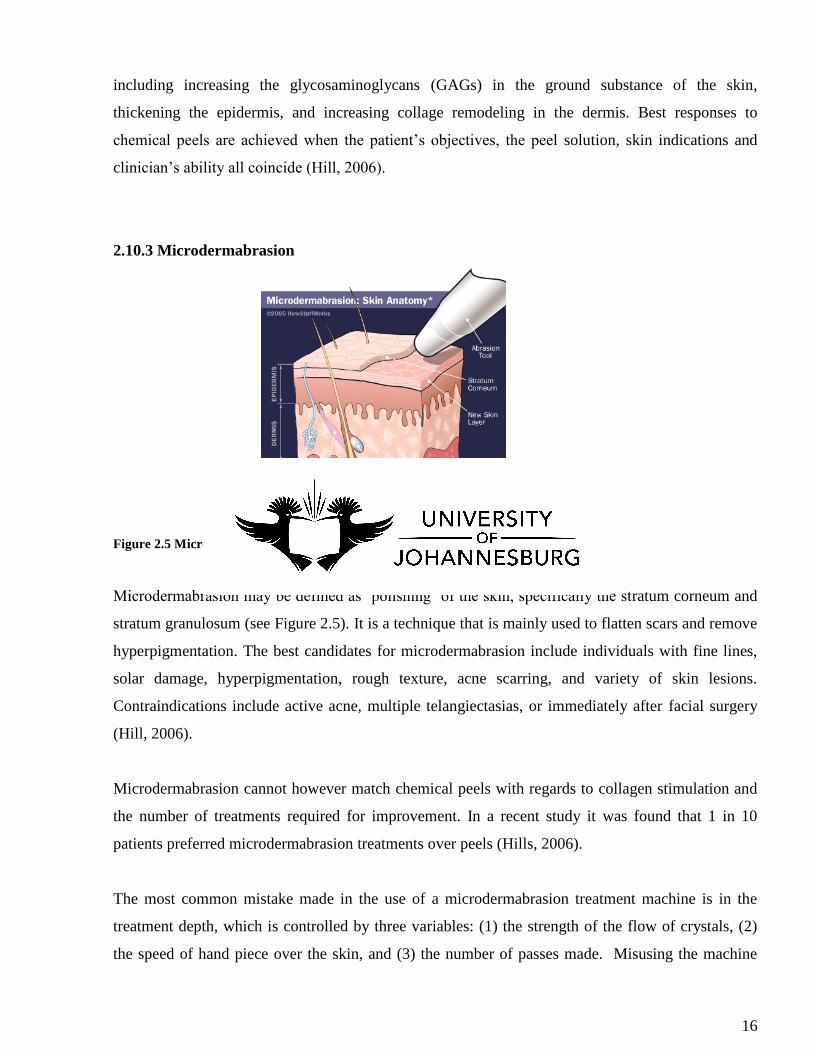
Figure 2.5 Microdermabrasion on the skin (Coustan, 2011)
Microdermabrasion may be defined as ‘polishing’ of the skin, specifically the stratum corneum and
stratum granulosum (see Figure 2.5). It is a technique that is mainly used to flatten scars and remove
hyperpigmentation. The best candidates for microdermabrasion include individuals with fine lines,
solar damage, hyperpigmentation, rough texture, acne scarring, and variety of skin lesions.
Contraindications include active acne, multiple telangiectasias, or immediately after facial surgery
(Hill, 2006).
Microdermabrasion cannot however match chemical peels with regards to collagen stimulation and
the number of treatments required for improvement. In a recent study it was found that 1 in 10
patients preferred microdermabrasion treatments over peels (Hills, 2006).
The most common mistake made in the use of a microdermabrasion treatment machine is in the
treatment depth, which is controlled by three variables: (1) the strength of the flow of crystals, (2)
the speed of hand piece over the skin, and (3) the number of passes made. Misusing the machine
17
could injure the client and the clinician. The hand piece is held at a 45-degree or 90-degree angle.
As the crystals move through the system, striking the skin, they exfoliate and then are returned to the
enclosed disposal canister (Hill, 2005)
The most common, expected and visible results after a microdermabrasion treatment is a deep
exfoliation that leaves the skin healthier and more refreshed. It appears this way because older, drier,
dead skin is removed at a pace that the natural sloughing process cannot match. However, not all
skin types or skin problems are appropriate for microdermabrasion. Complications associated with
microdermabrasion treatment include infections, abrasions and sunburns which occur after treatment
(Hill, 2005).
2.10.4 Laser therapy
Laser therapy has become a popular treatment for striae in recent years. Lasers that have been
studied in the treatment of striae include the intense pulsed light (IPL), ablative lasers, ablative
lasers and the 308-nm excimer laser. The use of ablative lasers has had limited use in the treatment
of striae due to post-treatment complications, including persistent erythema, prolonged wound
healing, infection, hyperpigmentation and hypopigmentation and permanent scarring (Stotland et
al.,2008).
Individuals with lighter skin tones are the best treatment candidates because little epidermal melanin
is present to serve as a chromophane for pulse dye laser absorption. Darker skins have increased
amounts of epidermal melanin which competes with haemoglobin as a chromophane for the laser.
This will result in post-inflammatory hyperpigmentation (PIH) of the skin (Salter & Kimball, 2006).
There have been a few studies reported about the effects of lasers in the treatment of stretch marks
on skin types 4-6. In a study that was conducted, four female patients with abdominal stretch marks,
present for a range of 8-19 years and skin types ranging from 4 to 6, were treated for stretch mark
long enough to be divided into three contiguous 2cm sections. Following the 585nm pulsed dye
laser treatment, at the 20-week follow-up, patients with type 4 skin showed no improvement, while
type 6 skins showed hyperpigmentation (Salter & Kimball, 2006).
Treatment of striae rubra and striae alba with a pulsed dye laser have yielded marginal success
(Yosipovitch et al., 2007) A study was conducted to evaluate the pulse dye laser in treating both
18
striae rubra and striae alba showed only a moderate improvement in the degree of erythema in striae
rubra with no clinical apparent change in striae alba (Stotland et al., 2008).
Laser therapy is an expensive alternative option and carries undesirable side effects especially for
darker skinned people (Alster & Handrick, 2000). Therefore, the use of the laser has restriction
when it comes to darker skinned people (Stotland et al., 2008). Other known adverse effects include
blister formation followed by secondary infection (Alster & Handrick, 2000).
2.10.5 Preventative measures
Vitamins are organic compounds that are required in small amounts in the diet and are involved in
many bodily functions. Most vitamins cannot be synthesized by the body or can only be synthesized
from certain dietary precursors (Webb, 2002). Inadequate supply of vitamins affect all types of skin,
making the skin dull and rough (Anne, 2011).
Vitamin A
Vitamin A is one of the essential vitamins for optimal skin care. It has a direct and profound
influence over the skin. Both inadequate supply and excess supply may cause harmful effects over
the skin. Synthetic vitamin A can be applied directly over inflamed skin areas caused by acne,
spotted pigmentation or skin wrinkling (Anne, 2011).
Vitamin C
Vitamin C is commonly known as ascorbic acid. It plays a significant role in healing damaged skin.
It is particularly beneficial in healing wounds. It functions by activating the oxidizing property of
the skin on which it is actually focused (Anne, 2011).
Vitamin E
Vitamin E or tocopherol functions as an antioxidant in the skin. It helps destroy free radicals and
provides sheath against skin damage. The skin damage caused by sun-burn can be alleviated
naturally with the help of vitamin E. It has been shown to penetrate the layers of the skin and reduce
19
formation of free radicals which interfere with healing. Vitamin E also influences the production of
collagen (Anne, 2011).
In one study vitamin E was used in the post-operatively after reconstructive surgery for burn
patients. One group of people applied vitamin E, while the other applied inert cream. After one year,
there was no statistically significant difference in scar thickness, size or overall appearance between
the two groups. Another study compared people who applied a cream to their scar with people who
applied the cream with vitamin E added. Both groups applied the cream twice a day for four weeks
starting soon after their surgery. Twelve weeks later, vitamin E had not improved the scar
appearance or worsened it in 90 percent of the people in the vitamin E group (Wong, 2007).
Zinc
Zinc is an essential trace element for all forms of life. The significance of zinc in human nutrition
and public health was recognized relatively recently. Zinc supplementation is a powerful theraupetic
tool in managing a list of illnesses. It is required for the metabolic activity of the body’s enzymes
and is considered essential for cell division and the synthesis of DNA and protein. In the skin, zinc
is necessary for tissue growth and wound healing. Zinc stimulates healing, proper connective tissue
formation, and increases the transport of Vitamin A from the liver to the skin, helping to protect
body tissue from damage and repair any damage present (Bhowmik et al., 2010)
In any striae treatment zinc is an essential supplement that should be taken to prevent striae. Zinc is
very important in the production of collagen, which aids in maintaining the skin’s vibrant tone. It is
important to supplement with zinc as it is not readily available in food (Admin, 2009).
2.10.6 Lifestyle interventions
Avoiding rapid weight loss or gain may help prevent the emergence of striae (Samer, 2009).
Keeping the skin adequately hydrated by drinking a lot of water will help to prevent striae (Hill,
2006).
There are other forms of alternative treatments that are available for skin problems due to connective
tissue damage. Many herbs are indicated for healing skin conditions by reducing scarring. Rose
20
water cleanses and tones the skin, smooths wrinkles and cools the skin by acting as an astringent. It
also aids in skin repair and reduces swelling. Chamomille’s antiseptic oils have a soothing effect and
they also help stimulate skin repair. Witch hazel has been used for centuries as a strong antiseptic
and for healing; its astringent tannins stop bleeding and lessened inflammation and scarring
(Cavanaugh, 2000).
2.11 Homoeopathy
Homoeopathy is a system for the treatment of an illness that is based on the recognition of patterns
within the symptoms of the illness and a wider consideration of how the individual is as a person.
The term homoeopathy is derived from two Greek words: homoios meaning similar, and pathos
meaning suffering (Ullman, 2007).
2.11.1 Law of Similars
Samuel Hahnemann was a German doctor who discovered the principle behind homoeopathy in the
late 18th
century (Worden, 2011). The basic principle of Homoeopathy is similia similibus curentur
or ‘let like be cured with like’ which states that any substance that makes a person ill can also cure
you: anything that can produce symptoms of disease in a healthy person can cure a sick person with
similar symptoms (Castro, 1993).
2.11.2 Homoeopathic potencies
Potentization is a process that involves a series of precise dilutions and succussions. A substance has
to undergo this process to be useful as a homoeopathic remedy. The repeated process of dilution and
succussion brings about an energetic change that gives the substance a deeper curative effect (Aziz,
2010). Higher potencies are stronger-acting than lower ones, even though they are more diluted. In
the case of acute illnesses, homoeopathic remedies are used in a frequency that is proportional to the
severity of the condition. In the case of chronic illnesses, remedies are used to effect a gradual deep
change in the person over many weeks and months (Nortman, 2011). Homoeopaths use extremely
small doses of medicinal substances that are highly individualized to a person, instead of using
conventional medicinal substances that have a broad-spectrum effect on a wide variety of people
with a similar disease (Ullman, 2007).
21
Doses are diluted to 1:10 (designated ‘X’) and 1:100 (designated ‘C’), and1:1000 (designated ‘M’).
Therefore a solution described as ‘1X’ is a 1:10 solution. Dilutions are made up to 2X (2C, 2M), 3X
(3C, 3M), etc., and even into infinitesimally weak solutions.
2.11.3 Homoeopathic prescription
The homoeopathic prescription consists of the homoeopathic remedy to be prescribed based on the
homoeopathic case analysis, and the dosage which consists of the potency and dose. Potency refers
to the strength and depth of a homoeopathic remedy (Nortman, 2011). It is expressed in terms of the
number of times the remedy has undergone the process of dilution and succussion (vigorous shaking
action).
Homoeopathic remedies are based upon the patient’s symptoms and personality which are obtained
through examination and interview. Different remedies may be used to try and find the closest
match to the patient’s symptoms. The smallest dose of medication is used and repetition of doses is
kept at a minimum. Homoeopathic remedies may also be used in combination with antimicrobial
agents and other conventional treatments. Homoeopathic remedies are not selected to treat isolated
symptoms or named diseases. In order to work correctly, they must be chosen to match the way an
individual’s system expresses its unique response to the current stress and illness. This means that
even with the same diagnosis, different people respond to different remedies (Aziz, 2010).
Classical homoeopathy is the practice of homoeopathy that is strictly based on Samuel
Hahnemann’s research and techniques. The main aim is to find “constitutional” remedies’ that
address the individual and the manifestation of a disease state, as opposed to finding a remedy based
merely on a few main symptoms. Clinical homoeopathy is different from classical homoeopathy
because it does not follow the principle that there is a single “constitutional” remedy which is totally
unique to the individual. Instead clinical homoeopathy is mainly focused targeting various systems
of the body and a wider concept of ‘symptoms’ (Evans, 2007). This study was based on a more
clinical approach as opposed to a classical one; determination of the selected cream, Thiosinaminum,
was solely based on clinical efficacy and anecdotal evidence in the treatment of dermatological
conditions.
22
2.12 Thiosinaminum
Thiosinaminum is a homoeopathic drug which is derived from mustard seed oil. It is used for a wide
variety of medical treatments, such as healing scar tissue, dissolving fibroids and treating tinnitus
(Dee, 2003).
Figure 2.8 Mustard seeds (Akpoghiran, 2011)
2.12.1 Origin of Mustard seed
The origin of the mustard seed is Canada and it is from there that it was brought to America. There
are several historical myths about the derivation of the mustard seed. Medical uses of mustard seed
for various diseases were in existence before the birth of Christ. In addition, it is supposed that
mustard seed has existence in countries like China and Africa long before the Christian era
(Wanjiru, 2011).
Mustard is a member of the Brassica family of plants which bears tiny round edible seeds as well as
tasty leaves. Its English name ‘mustard’ is derived from the Latin words ‘mustum ardens’ meaning
burning must (Fillipone, 2009). There are two types of mustard varieties seen in the mustard seed,
these varieties are Brassica hirta and Brassica juncea. Brassica hirta mainly generates the white and
yellow types of mustard seed, while the Brassica juncea produces brown and oriental mustard seeds.
The mustard seed like Brassica juncea are incorporated with ingredients that are non-volatile in
23
nature; these seeds acquire hot-blooded oil. Therefore this kind of oil gives warm, spicy and stinging
essence to the mustard seed (Wanjiru, 2011).
Historically mustard was considered a medicinal plant rather than a culinary one. In the sixth
century, the Greek scientist Pythagoras used mustard as a remedy for scorpion stings. A century
later, Hippocrates used mustard in a variety of medicines and poultices. Mustard plasters were
applied to ‘cure’ toothaches and a number of ailments (Fillipone, 2009).
2.12.2 Homoeopathic uses
Homoeopathically Thiosinaminum is used as a resolvent, externally and internally for dissolving
scar tissue, tumours, enlarged glands, lumps, strictures and adhesions (Boericke, 2005).
For healing scar tissue or other ailments that result in thickening of tissue it is considered best to use
Thiosinaminum prepared in a low potency tincture. Some people choose to inject a liquid solution
under the skin, while others prefer to consume capsules each day (Dee, 2003). Though no research
has been conducted to determine its efficacy on striae and scar tissue, Thiosinaminum is
recommended by numerous authors such as Vermeulen (2002) and Boericke (2005).
According to Dee (2003) Thiosinaminum can treat deafness caused by a thickened eardrum. In
addition, it may be helpful for people suffering from inflamed lymphatic glands. There have also
been claims that Thiosinaminum helps slow down aging. However, there has not been any scientific
studies proving these claims to be true, yet those who use it on a regular basis are convinced their
longevity is due to Thiosinaminum.
2.13 Indicated Homoeopathic Remedies for striae
Calcarea fluorica is a chemically white powder or cubic crystals which consist of 51% calcium and
49% fluorine. When used as a homoeopathic medicine, its main indications on the skin include
among others birth marks, vascular tumours, varicose veins, varicose ulcers, swelling and hard
nodes in ligaments and indurations of stony hardness (Vermeulen, 2002).
24
Silica is a non-metallic element in group 14 of the periodic element. It is the second most abundant
element on earth after oxygen. Homoeopathically it is indicated in cases where the healing reaction
of the connective tissue is insufficient. The skin also presents with eczema, never ripening boils with
hard margins, abscesses which do not break, but burrow under the skin, ulcers without healing
tendency with hard walls and secretion of pus (Vermeulen, 2002).
2.14 Homoeopathic dispensing
The homoeopathic remedy can be dispensed either in liquid form or in a tablet form. The liquid
form is based on a water or alcohol, and the tablet form may be made of sucrose or lactose suffused
with the homoeopathic remedy. The choice of format is based on personal patient considerations,
and sometimes on therapeutic considerations (Nortman, 2011). Homoeopaths use different vehicles
to prescribe their medicines. Vehicles are chemically neutral, therapeutically inert substances which
intend to carry the dynamic power of the drug safely to the interior of the organism, to fight against
the disease (Sahani, 2007).
The properties of an ideal vehicle include;
It should be chemically neutral.
It should be therapeutically inert.
It should not alter the medicinal property of the drug.
It must have the property of preservation of drugs and medicines.
The uses of vehicles are as follows;
For preparation of mother tincture, mother solution and mother substance.
For potentising the drug substance.
For dispensing medicines.
For preserving medicines.
For use in external applications.
25
The types of vehicles used to prescribe homoeopathic medicines are solid, liquid or semi-solid.
Solid vehicles include Saccharum lactis or sugar of milk (tablets, powders). Examples of liquid
vehicles are distilled water, alcohol, glycerin, olive oil, almond oil, sandalwood oil, lavender oil,
solvent ether, rosemary oil, simple syrup, sesame oil, hydrocarpus oil and chaumoogra oil. Semi-
solid vehicles include vaseline (yellow and white), waxes (bees wax, cetaceum, laolin, spermaceti),
Isin glass, Soap, Starch and prepared lard (Sahani, 2007).
2.15. Related research
Itamura (2007) conducted a study to determine the effect of homoeopathic treatments on 60
Japanese patients with chronic skin disease. The main objective of the study was to describe patient-
reported and clinically observed effects of individualized homoeopathic treatment of chronic skin
disease. The effectiveness of individualized homoeopathic treatment was measured using the
patient’s own assessments of seven elements (overall impression, improvement of skin condition,
reduction of itchiness, reduction of sleep disturbance, satisfaction in daily life, fulfilment at work
and satisfaction in human relations) using a nine-point scale. The chronic skin diseases that were
treated include in the study; atopic dermatitis (n=25), eczema (n=20), severe acne (n=6), chronic
urticaria (n=6), psoriasis vulgaris (n=2) and alopecia universalis (n=1). The duration of chronic skin
disease in these patients ranged from 2 to 41 years. These patients received individualized
homoeopathic treatments in addition to conventional dermatological treatment for a period of 3
months to 2 years 7 months (Itamura, 2007).
The effectiveness of the homoeopathic treatment was measured using patients’ self assessments and
assessments by physicians using a Visual Analogue Scale (VAS) of the improvement or
deterioration of the skin condition (Itamura, 2007).
The results were as follows; six patients reported a score of 4 (complete recovery), 23 patients a
score of 3 (75% improvement), 24 patients a core of 2 (50% improvement) and 7 patients a score of
1 (25% improvement). A total of 88,3% of patients reported over 50% improvement. Around one-
half of patients with atopic dermatitis and eczema reported greater satisfaction in daily life, greater
fulfilment at work and greater satisfaction in human relations (Itamura, 2007).

26
Smit (2001) conducted a research study on the effects of the application of a cream containing
Botulinum toxin expressed in potencies of D24, D30 or 200cH on vertical frown lines. It was a
double-blind study that involved four groups of fifteen participants each. These participants each
had a vertical frown line of at least half a centimetre long. The control group received a
placebo/unmedicated cream and the other three groups received medicated creams containing a
single potency of Botulinum toxin. The participants had to apply the cream twice daily as a
moisturizer in the morning and in the evening for a period of four months. The study resulted in a
statistical improvement and reduction of the vertical lines in all four treatment groups. Participants
in Group 2 and 3 using creams containing Botulinum toxins in potencies of 200CH and D24
respectively had the greatest and most significant improvement in frown line lengths (Smit, 2001).
27
3. METHODOLOGY
3.1 Research design
The research was a double-blind, placebo-controlled study that took place over a period of twelve
weeks at the Health Training Centre situated at the University of Johannesburg, Doornfontein
campus
3.2 Research sample
Posters and pamphlets (Appendix F) were distributed at the University of Johannesburg campuses,
homoeopathic and medical practices and health shops in Gauteng. Forty female participants aged
between eighteen and thirty-five years were selected to participate in the study. The study was
conducted over a period of twelve weeks.
3.2.1 Inclusion criteria
- Black female subjects, aged between eighteen and thirty-five years
- Individuals with stretch marks on the thighs or buttock area
- Individuals with striae that have a minimum length of 50mm and a maximum length of 100mm
- Individuals with stretch marks present for at least 6 months prior to the study.
3.2.2 Exclusion criteria
- Individuals who have been diagnosed or are diagnosed during the study with Cushing’s syndrome,
Marfan’s syndrome, any other connective tissue disorders, diabetes mellitus (type 2),
cardiomyopathies, neoplasms, HIV or any autoimmune disease
- People diagnosed with slow healing wounds or eczema
- Pregnant women or any who fall pregnant during the study
- Presence of red striae (recent stretch marks)
- Subjects that have a variation of their weight of more than 2kg in a period of four months prior to
the study or have excess weight gain of 2kg or more during the study
- Known allergy to mustard seed

28
- Use any other forms of treatments for stretch marks during the study.
3.3 Research procedure
On recruitment, the participants were required to read and sign the information sheet (Appendix A)
and consent form (Appendix B) assisted by the researcher. Participants were asked to complete a
questionnaire (Appendix C) to determine contributing factors e.g. duration of the stretch marks, the
cause of the stretch marks and any disease that may contribute to the formation of stretch marks. A
pertinent case and vital signs were taken at the initial consultation to eliminate any pathologies. All
potential participants were required to present with stretch marks on the thighs or buttocks present
for at least 6 months prior to the study. The stretch marks needed to have had a minimum length of
50mm and a maximum length of a 100mm.
The researcher was responsible for choosing the designated area that was treated. The most distinct
striae were selected by the researcher according to criteria for treatment. The researcher took
photographs of the treatment areas at the commencement of the study and this was repeated at the
end of the study (Appendix I). The length of the most prominent stretch mark (according to criteria)
below was also measured on the commencement of the study. To physically measure the most
prominent stretch mark a string and a ruler were utilized. The same ruler and ball of string was used
each time to ensure validity of the results. A new piece of string was cut and tied in a knot at the tip
and placed on the stretch mark itself to mould to its shape and thereafter it was placed on a ruler to
determine the measurements in millimetres. To ensure that the same stretch mark was measured
every time, the researcher measured out the distance between the stretch mark and a defined
anatomical point for all the participants. The stretch mark was traced using plotting paper.
Stretch marks may be aggravated by weight gain thus to ensure reliability the participant’s weight
was measured at the initial consultation and again at the follow up consultations. A weight gain of
2kg or more during the study would lead to exclusion from the study.
Follow up consultations were done at four, eight and twelve weeks. Physical measurements of the
stretch marks were done at these follow-up consultations. Clinical improvement in the appearance of
stretch marks shown in comparable, standardized, digital photographs, using a quartile grading scale
was determined, to assess improvement.
29
0 = < 25%
1 = 25-50%
2 = 51-75%
3 = > 75%
The quartile grading scale was used by the researcher at monthly intervals to represent the
percentages of any clinical improvements in the appearance of stretch marks. On the last follow-up
visit the participants were also asked to rate their overall satisfaction of the treatment received.
Satisfaction was rated using the following scale: I = not satisfied, II = slightly satisfied, III =
satisfied, IV = very satisfied, V = and extremely satisfied. (Appendix D)
3.4 Medication and administration
The creams were prepared by an independent Homoeopharmaceutics dispenser in the Homoeopathic
dispensary at the Health Training Centre. The creams were supplied to the participants in 100-gram
containers at monthly intervals. The medicating potency that was used to medicate the aqueous
cream was prepared in accordance with standard GMP procedures (Appendix G). The remedy and
the control creams were identical and the researcher and participants were blinded. The creams were
dispensed to the participants at the Homoeopathic Health Centre at the University, Doornfontein
campus. The participants were requested to apply the cream on the treatment area twice daily for a
period of 3 months. No other topical creams or treatment was to be used by the participants during
the study period.
3.5 Data collection and analysis
Records of all physical measurements of the stretch marks and photographs taken over the study
period were thoroughly documented. A comparison evaluation of the participants’ photographs of
the stretch marks at baseline and at the 3-month follow-up were evaluated by the researcher using
the quartile grading scale. Participants also rated their overall satisfaction of the treatment received
and these were represented on a scale (Appendix D). The physical measurements of the stretch
marks were accurately recorded in a note book at each interval. Data analysis was analysed by using

30
the Frequencies and Descriptives method. To test for normality the Shapiro Wilk and Kolmogorov-
Smirnov tests were utilised.
3.6 Reliability and validity
To establish reliability each stretch mark was measured three times on each occasion and the
average of these measurements taken. The physical measurements of the stretch marks were
performed by the same researcher to ensure reliability. Internal consistency was established by
measuring the same stretch mark on each participant using the same ruler and the same string
throughout the entire period of the study. To establish external consistency the sample group was
drawn out of the general population. The photographs were standardized using consistent patient
positioning, camera angling lighting and backdrop conditions (Appendix H)
The creams were prepared according to standard General Manufacture Procedures (Appendix G).
4. Ethics
Participation in this study was entirely voluntary. The participants were required to read and
complete the patient information sheet (Appendix A) and the consent form (Appendix B) which
fully explained the aim and requirements of the study. To ensure privacy, all records were kept in
the strictest confidentiality. Participants were free to withdraw from the study at any point in time.
There were no anticipated side effects from the topical treatment in this study and if participants
experienced any discomfort then they were required to immediately contact the researcher. The
results of the study were made available to the participants at the end of study.
31
4. RESULTS
4.1 Introduction
This was a double-blind, placebo-controlled study that took place at the Homoeopathy Health
Centre, located at the University of Johannesburg Doornfontein Campus, over a twelve week period.
The aim of this study was to determine the effect of Thiosinaminum 1X cream on the appearance of
striae.
The research sample group consisted of forty female participants between the ages of eighteen and
thirty-five years. All the volunteers participating in this study met the stipulated entry criteria. Of the
forty participants entering the study, thirty-three completed the study. After unblinding of the study
it was determined that twenty one participants were in the control group while nineteen participants
were in the remedy group. Three participants withdrew due to personal reasons and the other four
participants were excluded from the study as they no longer met the inclusion criteria and thus there
was missing data in the final analysis of these participants’ results. No participants were withdrawn
due to complications of the medication, adverse effects or poor adherence.
4.2 Contents of the creams
After completion of the double-blind study, the researcher was informed that the contents of the
cream where as follows:
Group 1: There were 21 participants in the control group, who received aqueous cream only.
Group 2: There were 19 participants in the experimental group, who received aqueous cream
medicated with Thiosinaminum 1X.
4.3 Data Analysis
The following tests were performed by Statkon (University of Johannesburg), to analyse the data
collected.
Parametric tests were performed. Frequencies and Descriptives methods were also utilized.
Shapiro-Wilk and Kolmogorov-Smirnov tests for Normality - to test for a normal distributed
population.
32
4.4 Participants’ mean weight and mean length of striae before and after treatment
According to the data provided in Table 4.1, the control group weighed 61.62 ± 10.414 kg and the
experimental group weighed 64.79 ± 14.077 kg on average at the beginning of the study. At the end
of the study the control and experimental groups weighed 60.95 ± 9.734 kg and 64.63kg ± 13.359 on
average, respectively. Overall there was negligible weight loss in the control and experimental
group.
The mean length of striae in the control group was 61.57mm ± 9.902 and the experimental group
was 69.16 mm ± 15.392. At the end of the study the control and experimental group’s striae
measured at 60.53 mm ± 9.410 and 69.44 mm ± 15.786 respectively.
Table 4.1 Effect of Thiosinaminum 1X treatment of striae on mean weight and mean striae
length of participants
Group Mean weight (kg) ±
SD
Mean striae length
(mm) ± SD
Control Group
(n=15)
Before = 61.62 ±
10.414 kg
After = 60.95 ±
9.734 kg
Before = 61.57 ±
9.902 kg
After = 60.53 ±
9.410 kg
Experimental Group
(n=18)
Before = 64.79
±14.077 kg
After = 64.63 ±
13.359 kg
Before = 69.16 ±
15.392 kg
After = 69.44
±15.786 kg n: Number of participants; SD: Standard deviation
4.5 Evaluation of photographs before and after treatment using the quartile grading scale
The quartile grading scale was used to evaluate the severity of participants’ striae before and after
the treatment. Participants’ photographs (Appendix I) showing areas affected by striae were
evaluated by the researcher who was blinded as to which group participant were in.
33
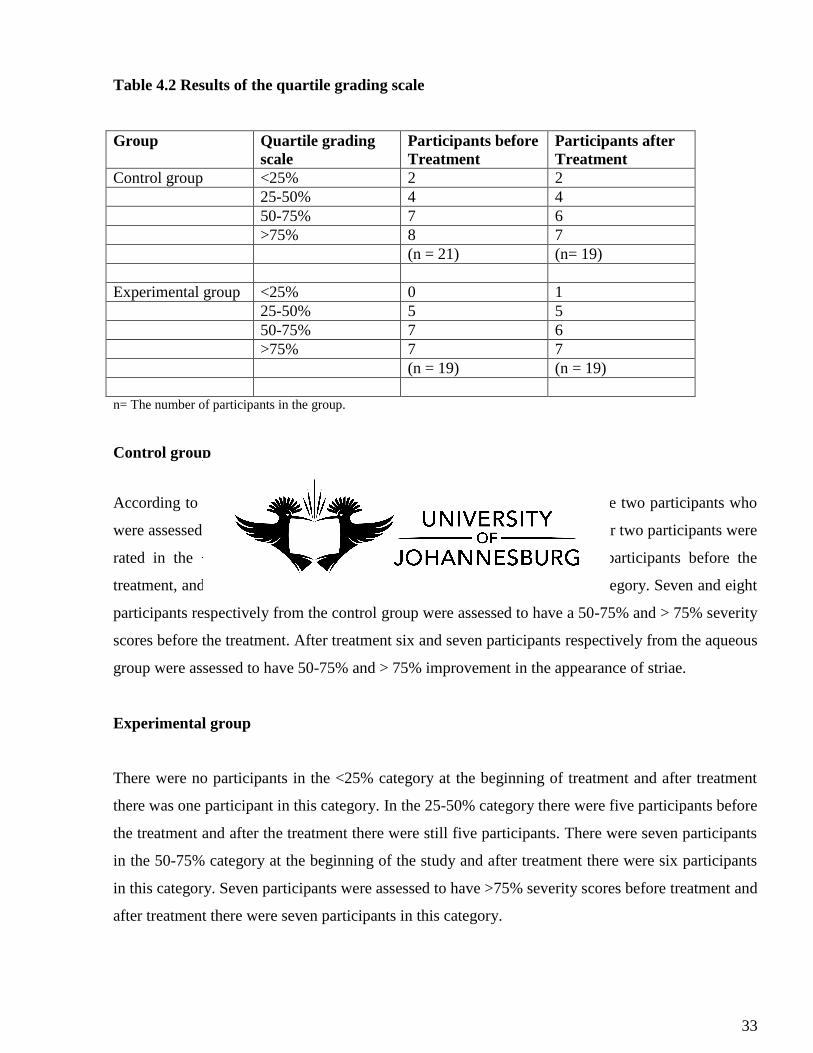
Table 4.2 Results of the quartile grading scale
Group Quartile grading
scale
Participants before
Treatment
Participants after
Treatment
Control group <25% 2 2
25-50% 4 4
50-75% 7 6
>75% 8 7
(n = 21) (n= 19)
Experimental group <25% 0 1
25-50% 5 5
50-75% 7 6
>75% 7 7
(n = 19) (n = 19)
n= The number of participants in the group.
Control group
According to the data presented in Table 4.2, before the treatment there were two participants who
were assessed to have a < 25% severity score and after the treatment a further two participants were
rated in the < 25% category. In the 25-50% category there were four participants before the
treatment, and after the treatment there were four participants in the same category. Seven and eight
participants respectively from the control group were assessed to have a 50-75% and > 75% severity
scores before the treatment. After treatment six and seven participants respectively from the aqueous
group were assessed to have 50-75% and > 75% improvement in the appearance of striae.
Experimental group
There were no participants in the <25% category at the beginning of treatment and after treatment
there was one participant in this category. In the 25-50% category there were five participants before
the treatment and after the treatment there were still five participants. There were seven participants
in the 50-75% category at the beginning of the study and after treatment there were six participants
in this category. Seven participants were assessed to have >75% severity scores before treatment and
after treatment there were seven participants in this category.
34
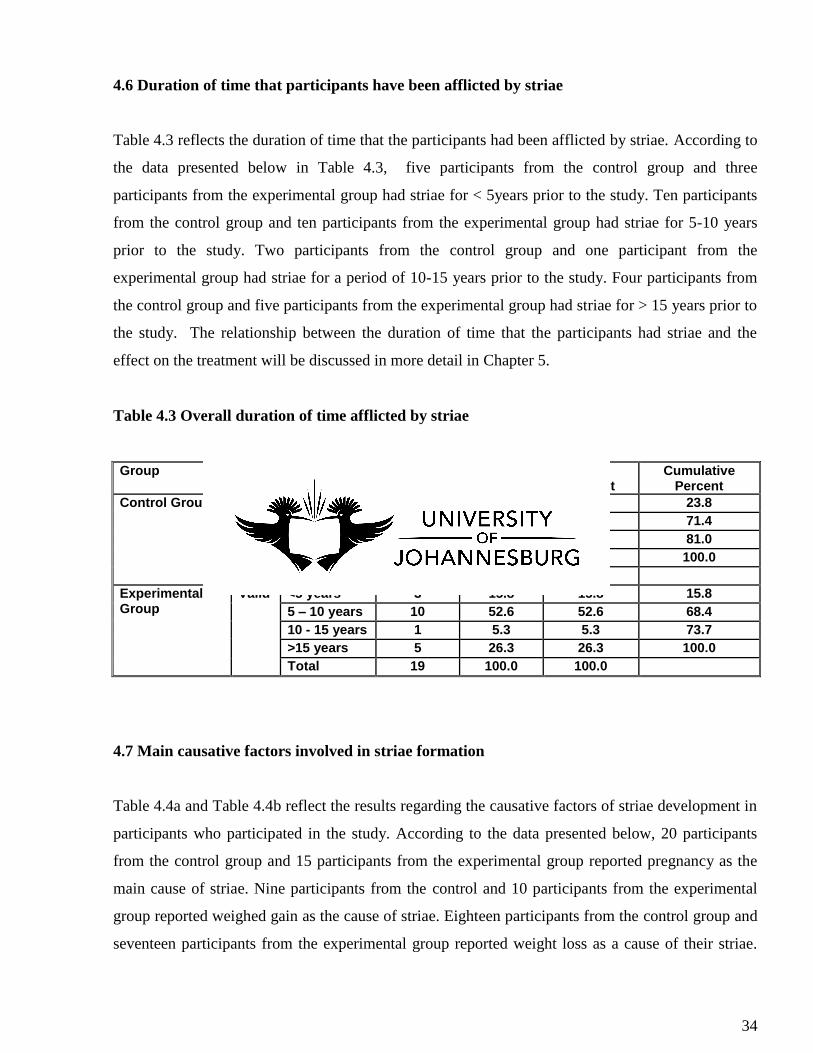
4.6 Duration of time that participants have been afflicted by striae
Table 4.3 reflects the duration of time that the participants had been afflicted by striae. According to
the data presented below in Table 4.3, five participants from the control group and three
participants from the experimental group had striae for < 5years prior to the study. Ten participants
from the control group and ten participants from the experimental group had striae for 5-10 years
prior to the study. Two participants from the control group and one participant from the
experimental group had striae for a period of 10-15 years prior to the study. Four participants from
the control group and five participants from the experimental group had striae for > 15 years prior to
the study. The relationship between the duration of time that the participants had striae and the
effect on the treatment will be discussed in more detail in Chapter 5.
Table 4.3 Overall duration of time afflicted by striae
Group Frequency Percent
Valid Percent
Cumulative Percent
Control Group Valid <5 years 5 23.8 23.8 23.8
5 – 10 years 10 47.6 47.6 71.4
10 - 15 years 2 9.5 9.5 81.0
>15 years 4 19.0 19.0 100.0
Total 21 100.0 100.0
Experimental Group
Valid <5 years 3 15.8 15.8 15.8
5 – 10 years 10 52.6 52.6 68.4
10 - 15 years 1 5.3 5.3 73.7
>15 years 5 26.3 26.3 100.0
Total 19 100.0 100.0
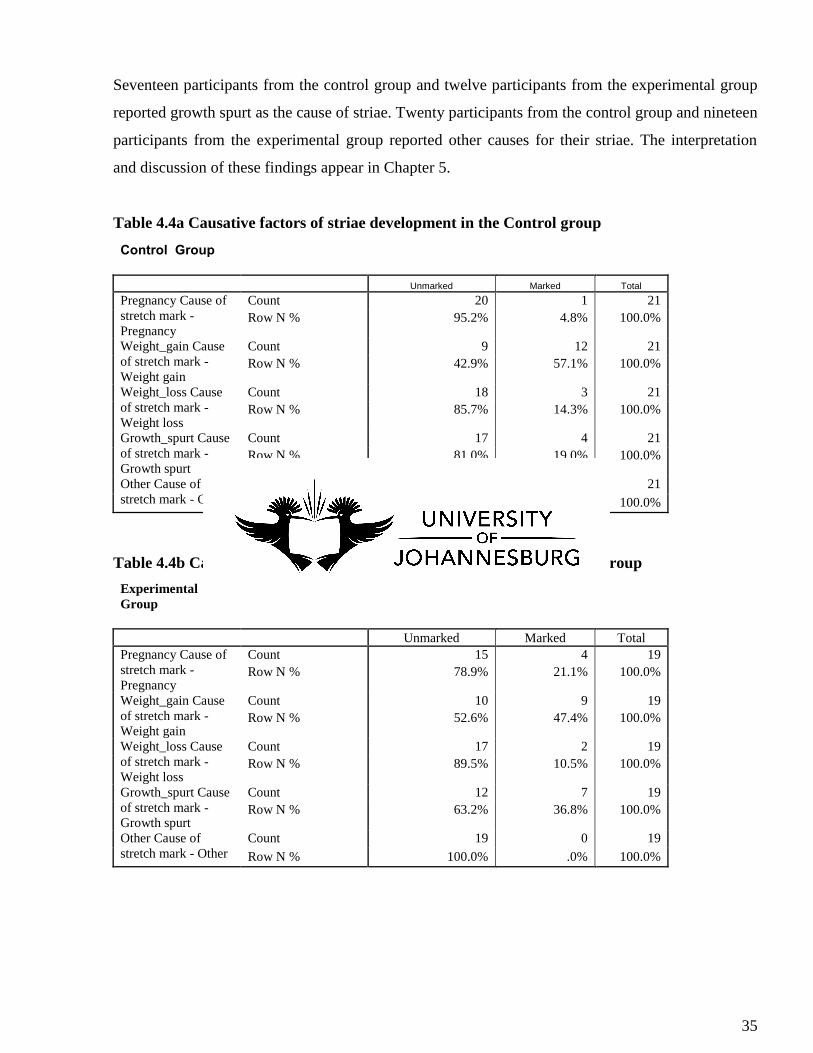
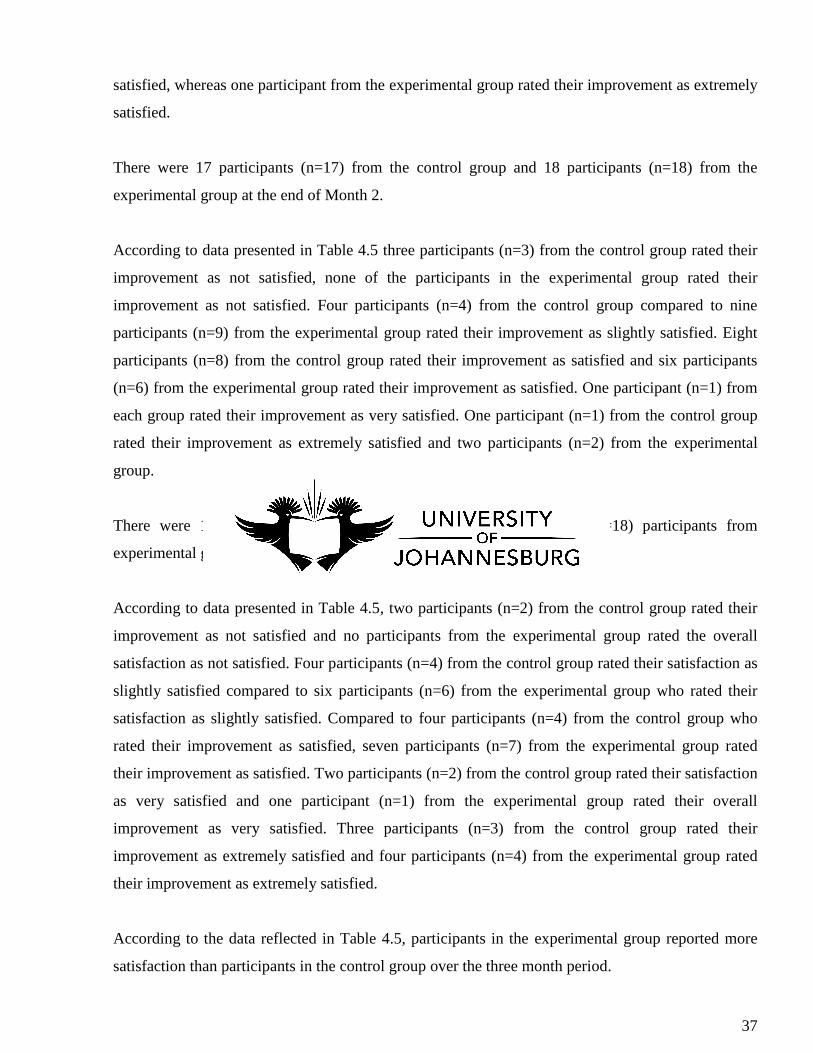
4.7 Main causative factors involved in striae formation
Table 4.4a and Table 4.4b reflect the results regarding the causative factors of striae development in
participants who participated in the study. According to the data presented below, 20 participants
from the control group and 15 participants from the experimental group reported pregnancy as the
main cause of striae. Nine participants from the control and 10 participants from the experimental
group reported weighed gain as the cause of striae. Eighteen participants from the control group and
seventeen participants from the experimental group reported weight loss as a cause of their striae.
35
Seventeen participants from the control group and twelve participants from the experimental group
reported growth spurt as the cause of striae. Twenty participants from the control group and nineteen
participants from the experimental group reported other causes for their striae. The interpretation
and discussion of these findings appear in Chapter 5.
Table 4.4a Causative factors of striae development in the Control group
Control Group
Unmarked Marked Total
Pregnancy Cause of
stretch mark -
Pregnancy
Count 20 1 21
Row N % 95.2% 4.8% 100.0%
Weight_gain Cause
of stretch mark -
Weight gain
Count 9 12 21
Row N % 42.9% 57.1% 100.0%
Weight_loss Cause
of stretch mark -
Weight loss
Count 18 3 21
Row N % 85.7% 14.3% 100.0%
Growth_spurt Cause
of stretch mark -
Growth spurt
Count 17 4 21
Row N % 81.0% 19.0% 100.0%
Other Cause of
stretch mark - Other
Count 20 1 21
Row N % 95.2% 4.8% 100.0%
Table 4.4b Causative factors of striae development in the Experimental group
Experimental
Group
Unmarked Marked Total
Pregnancy Cause of
stretch mark -
Pregnancy
Count 15 4 19
Row N % 78.9% 21.1% 100.0%
Weight_gain Cause
of stretch mark -
Weight gain
Count 10 9 19
Row N % 52.6% 47.4% 100.0%
Weight_loss Cause
of stretch mark -
Weight loss
Count 17 2 19
Row N % 89.5% 10.5% 100.0%
Growth_spurt Cause
of stretch mark -
Growth spurt
Count 12 7 19
Row N % 63.2% 36.8% 100.0%
Other Cause of
stretch mark - Other
Count 19 0 19
Row N % 100.0% .0% 100.0%
36
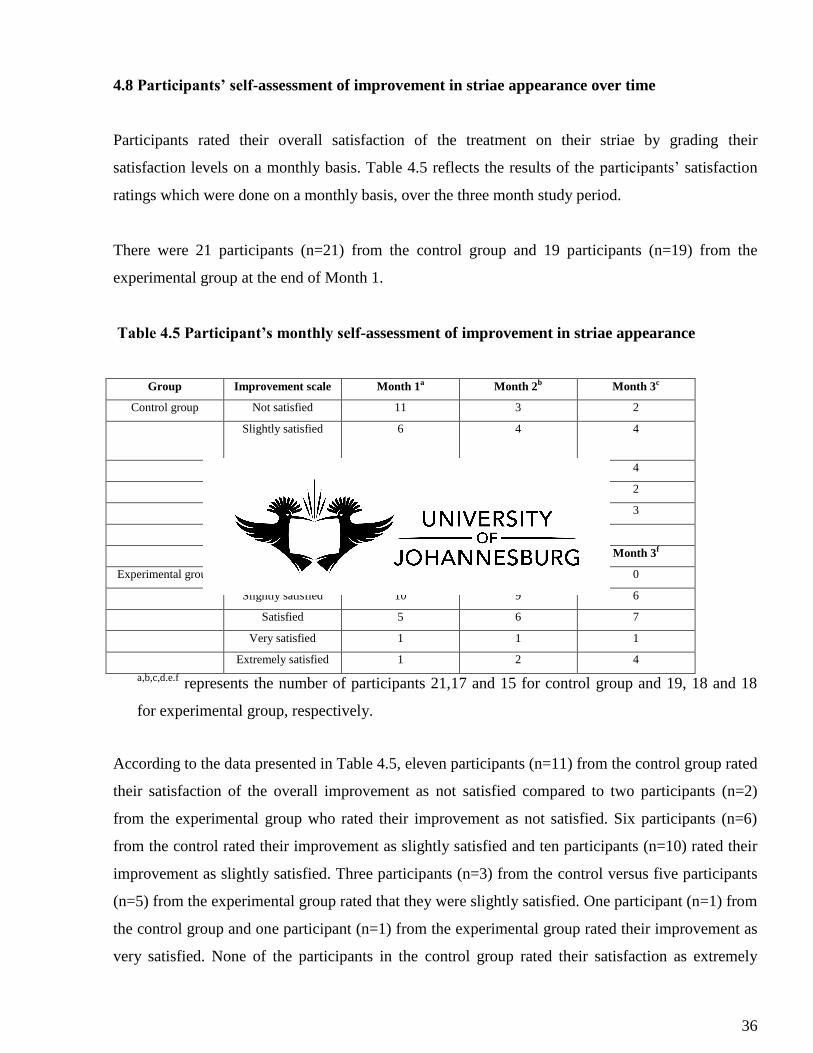
4.8 Participants’ self-assessment of improvement in striae appearance over time
Participants rated their overall satisfaction of the treatment on their striae by grading their
satisfaction levels on a monthly basis. Table 4.5 reflects the results of the participants’ satisfaction
ratings which were done on a monthly basis, over the three month study period.
There were 21 participants (n=21) from the control group and 19 participants (n=19) from the
experimental group at the end of Month 1.
Table 4.5 Participant’s monthly self-assessment of improvement in striae appearance
Group Improvement scale Month 1a Month 2b Month 3c
Control group Not satisfied 11 3 2
Slightly satisfied 6 4 4
Satisfied 3 8 4
Very satisfied 1 1 2
Extremely satisfied 0 1 3
Month 1d Month 2e Month 3f
Experimental group Not satisfied 2 0 0
Slightly satisfied 10 9 6
Satisfied 5 6 7
Very satisfied 1 1 1
Extremely satisfied 1 2 4
a,b,c,d.e.f represents the number of participants 21,17 and 15 for control group and 19, 18 and 18
for experimental group, respectively.
According to the data presented in Table 4.5, eleven participants (n=11) from the control group rated
their satisfaction of the overall improvement as not satisfied compared to two participants (n=2)
from the experimental group who rated their improvement as not satisfied. Six participants (n=6)
from the control rated their improvement as slightly satisfied and ten participants (n=10) rated their
improvement as slightly satisfied. Three participants (n=3) from the control versus five participants
(n=5) from the experimental group rated that they were slightly satisfied. One participant (n=1) from
the control group and one participant (n=1) from the experimental group rated their improvement as
very satisfied. None of the participants in the control group rated their satisfaction as extremely
37
satisfied, whereas one participant from the experimental group rated their improvement as extremely
satisfied.
There were 17 participants (n=17) from the control group and 18 participants (n=18) from the
experimental group at the end of Month 2.
According to data presented in Table 4.5 three participants (n=3) from the control group rated their
improvement as not satisfied, none of the participants in the experimental group rated their
improvement as not satisfied. Four participants (n=4) from the control group compared to nine
participants (n=9) from the experimental group rated their improvement as slightly satisfied. Eight
participants (n=8) from the control group rated their improvement as satisfied and six participants
(n=6) from the experimental group rated their improvement as satisfied. One participant (n=1) from
each group rated their improvement as very satisfied. One participant (n=1) from the control group
rated their improvement as extremely satisfied and two participants (n=2) from the experimental
group.
There were 15 participants (n=15) from the control group and 18 (n=18) participants from
experimental group at the end of Month 3.
According to data presented in Table 4.5, two participants (n=2) from the control group rated their
improvement as not satisfied and no participants from the experimental group rated the overall
satisfaction as not satisfied. Four participants (n=4) from the control group rated their satisfaction as
slightly satisfied compared to six participants (n=6) from the experimental group who rated their
satisfaction as slightly satisfied. Compared to four participants (n=4) from the control group who
rated their improvement as satisfied, seven participants (n=7) from the experimental group rated
their improvement as satisfied. Two participants (n=2) from the control group rated their satisfaction
as very satisfied and one participant (n=1) from the experimental group rated their overall
improvement as very satisfied. Three participants (n=3) from the control group rated their
improvement as extremely satisfied and four participants (n=4) from the experimental group rated
their improvement as extremely satisfied.
According to the data reflected in Table 4.5, participants in the experimental group reported more
satisfaction than participants in the control group over the three month period.
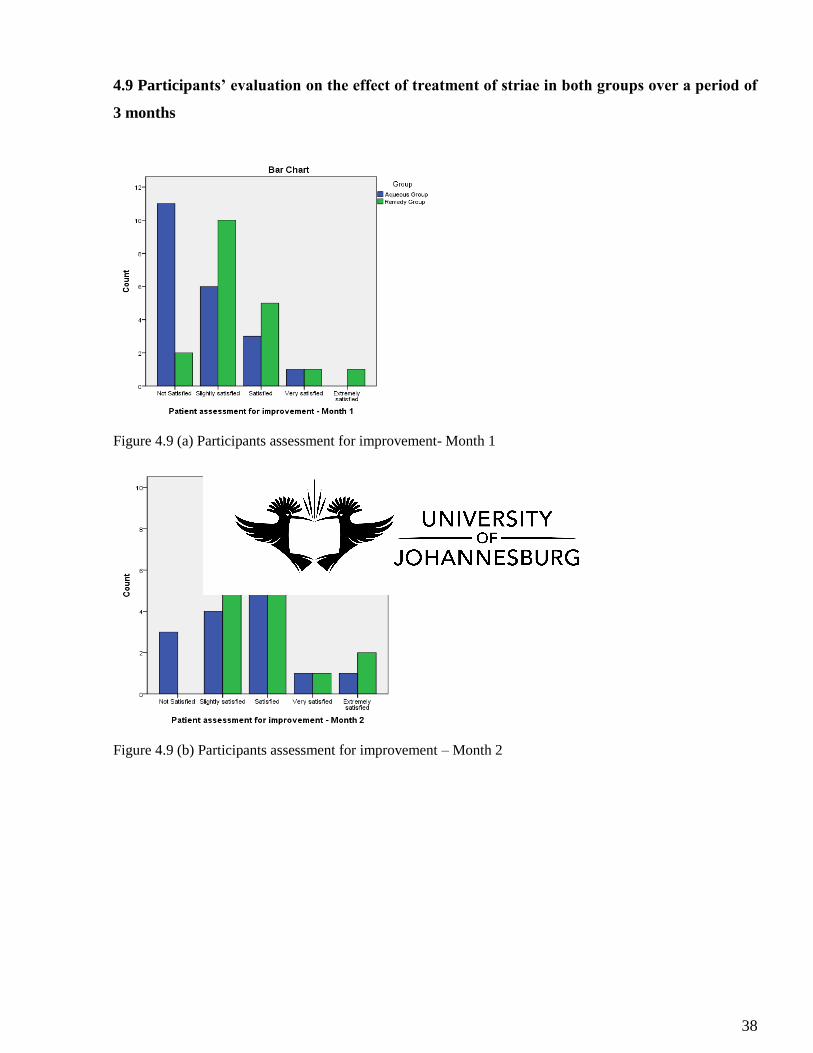
38
4.9 Participants’ evaluation on the effect of treatment of striae in both groups over a period of
3 months
Figure 4.9 (a) Participants assessment for improvement- Month 1
Figure 4.9 (b) Participants assessment for improvement – Month 2
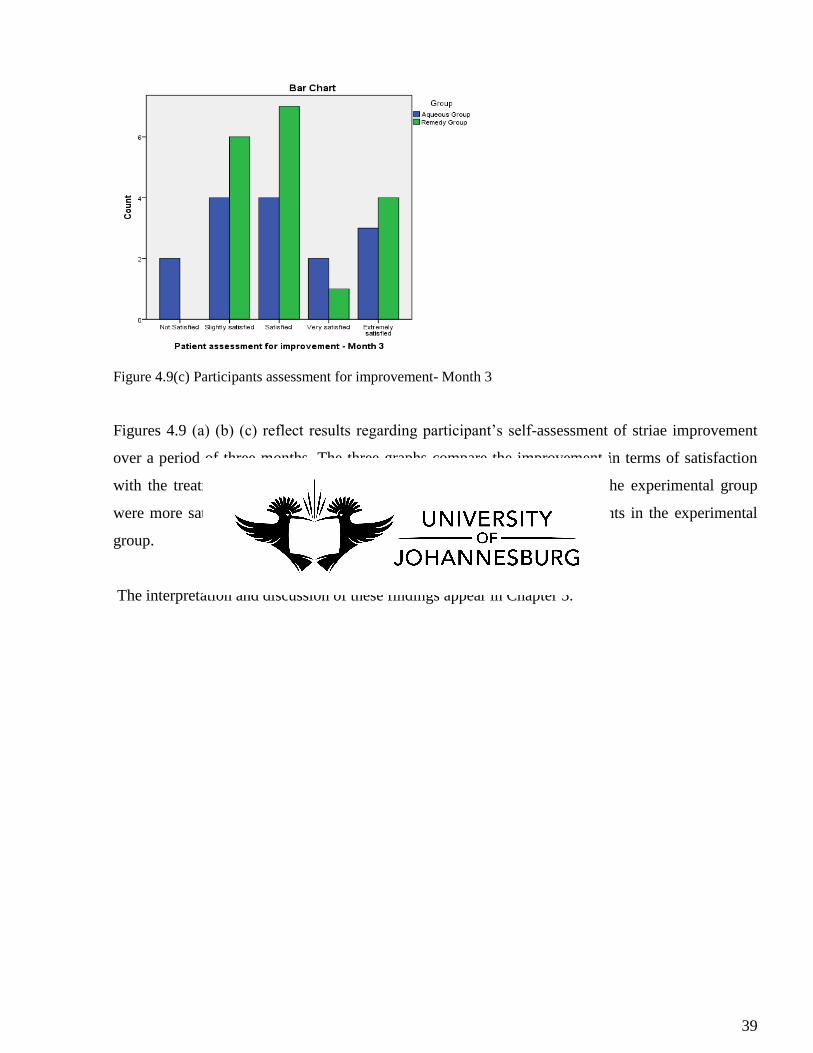
39
Figure 4.9(c) Participants assessment for improvement- Month 3
Figures 4.9 (a) (b) (c) reflect results regarding participant’s self-assessment of striae improvement
over a period of three months. The three graphs compare the improvement in terms of satisfaction
with the treatment. From these results it is evident that participants from the experimental group
were more satisfied about their overall improvement compared to participants in the experimental
group.
The interpretation and discussion of these findings appear in Chapter 5.
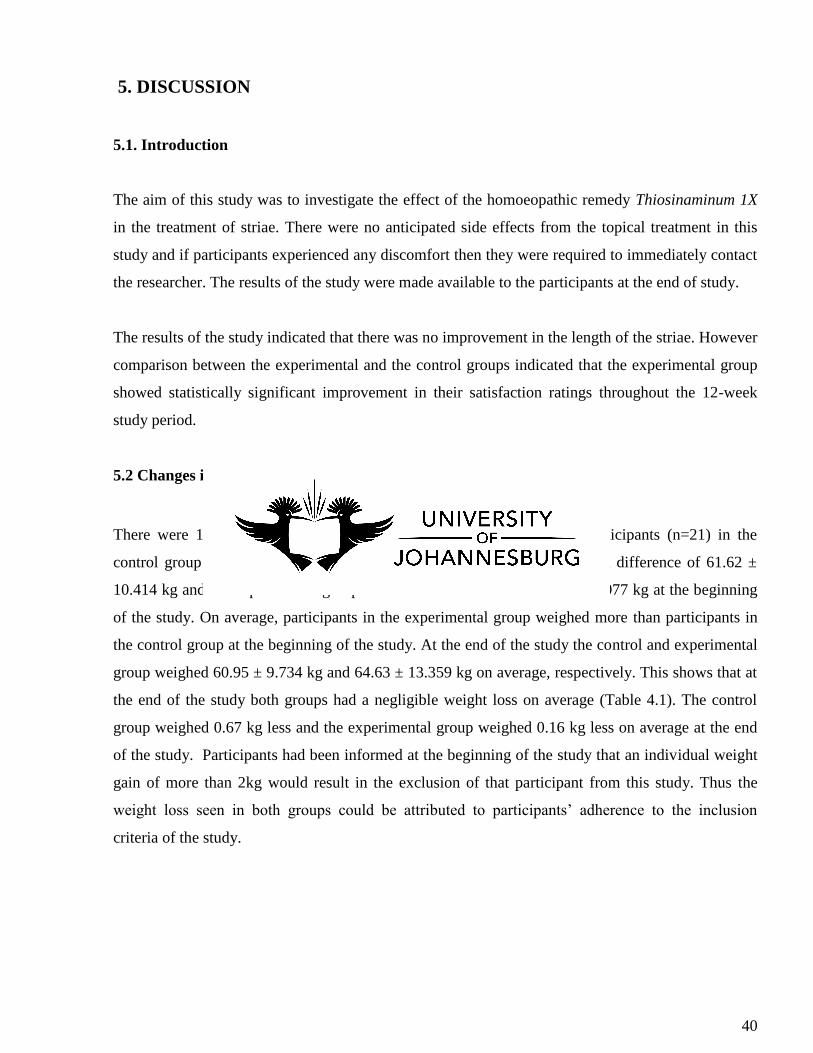
40
5. DISCUSSION
5.1. Introduction
The aim of this study was to investigate the effect of the homoeopathic remedy Thiosinaminum 1X
in the treatment of striae. There were no anticipated side effects from the topical treatment in this
study and if participants experienced any discomfort then they were required to immediately contact
the researcher. The results of the study were made available to the participants at the end of study.
The results of the study indicated that there was no improvement in the length of the striae. However
comparison between the experimental and the control groups indicated that the experimental group
showed statistically significant improvement in their satisfaction ratings throughout the 12-week
study period.
5.2 Changes in weight observed in both groups
There were 19 participants (n=19) in the experimental group and 21 participants (n=21) in the
control group at the beginning of the study. The control group had a mean difference of 61.62 ±
10.414 kg and the experimental group had a mean difference of 64.79 ± 14.077 kg at the beginning
of the study. On average, participants in the experimental group weighed more than participants in
the control group at the beginning of the study. At the end of the study the control and experimental
group weighed 60.95 ± 9.734 kg and 64.63 ± 13.359 kg on average, respectively. This shows that at
the end of the study both groups had a negligible weight loss on average (Table 4.1). The control
group weighed 0.67 kg less and the experimental group weighed 0.16 kg less on average at the end
of the study. Participants had been informed at the beginning of the study that an individual weight
gain of more than 2kg would result in the exclusion of that participant from this study. Thus the
weight loss seen in both groups could be attributed to participants’ adherence to the inclusion
criteria of the study.
41
5.2 Changes in length of striae in both groups
The average length of striae in the control group (61.57mm ± 9.902) was shorter than the average
length of striae in the experimental group (69.16mm ±15.392) at the beginning of the study. At the
end of the study the average length of the striae for participants in the control group (60.53mm ±
9.410) had decreased and the average length of striae for participants in the experimental group
(69.44mm ± 15.786) had increased. According to the data reflected in Table 4.1, the average length
of striae in the control group decreased by 1.04 mm and the average length of striae in the
experimental group increased by 0.28mm.
These changes could be ascribed to the following factors;
The control group had a shorter average length of striae compared to the experimental group
at the beginning of the study.
Standard deviation is a measure of how spread out the values are from the mean (Niles,
2011).Thus the standard deviation directly affects the mean. The experimental group had a
smaller standard deviation value (SD= ±15.392) at the beginning of the study compared to
the control group at the end of the study (SD=± 15.786). The higher the standard deviation,
the higher the mean; this may explain the increase in mean striae length in the experimental
group.
Thiosinaminum is indicated for the treatment of striae, however there are other well indicated
remedies that could be considered in future. Homoeopathic prescriptions are based on
individuality and treating the person as a whole rather than treating the symptoms on their
own. The remedy in this study was not prescribed according to homoeopathic principles
which states that ‘like cures like’; a whole-body-and-mind approach to treatment may have
yielded better results (Itamura, 2007).
The low potency of Thiosinaminum 1X could have had a negative effect in shortening the
striae length in the experimental group.
The experimental group had a mean weight of 64.79kg and the control group had a mean
weight of 61.62kg at the beginning of the study. The experimental group weighed more than
the control group and this could have affected the striae length of the experimental group
causing it to be slightly longer than the control groups’ striae length.
42
Aqueous cream has a moisturizing effect on the skin and this could explain the non-
significant yet shortening of the striae length in the control group.
The participants were required to apply the cream topically, twice a day; participants from
the experimental group may not have followed these instructions properly as compliance to
treatment was not monitored.
Homoeopathic medications often work well when they are prescribed orally (Dee, 2003). In
this study the participants were given the cream to apply topically, however randomization
of the participants was not based on skin types and because different skin types absorb
creams differently this could have had an effect on the results.
Participants from the control group had striae for a shorter period than participants from the
experimental group. Literature states that earlier striae are much easier to treat than more
established striae.
Participants were informed not to use any other form of striae treatment during the study
period; however compliance to these instructions was not monitored. Some participants from
the control group may have been using other products in conjunction with the
Thiosinaminum cream.
Participants’ striae were measured using a string which had a certain tensile strength, this
may have had an effect on the striae length. In future studies a more accurate and reliable
instrument should be used to measured striae.
5.3 The quartile grading scale before and after Treatment: Control and Experimental groups
Clinical improvement in the appearance of the striae shown in comparable, standardized digital
photographs, using a quartile grading scale, were analysed to assess improvement.
5.3.1 Control group
In the 50-75% category there were seven participants before the treatment and after the treatment
there were six participants. Eight participants were rated in the > 75% category before the treatment
and after the treatment there seven participants in this category. There was no improvement in the
other categories. This improvement could be explained by the fact that there were two participants
43
whose data was missing and this could have had an effect on the results of the final grading scale for
the aqueous group after the treatment.
This improvement in appearance was however not significant enough to influence the results.
5.3.2 Experimental group
In comparison to prior to treatment, there was improvement in the appearance of striae in the
remedy group. There were no participants from the experimental group in the < 25% before the
treatment and after the treatment there was one participant who was rated as having < 25%
improvement. This improvement in appearance was however not significant enough to influence
the results.
5.4 Duration of time: Control and Experimental groups
According to the data presented in Table 4.3 the longest time that the participants in both groups had
striae was for a period of 5-10 years. Five participants from the control group reported that they had
striae for < 5 years compared to three participants from the experimental group. There were ten
participants from both the control and experimental group who had striae for 5-10 years. Two
participants from the control group and 1 participant from the experimental group had striae for a
duration of 10- 15 years. Four participants from the control group and 5 participants from the
experimental group had striae for > 15 years.
On average participants from the group experimental had a longer duration of striae than
participants in the control group, thus giving the control group an advantage. Multiple treatment
have been used in varying degrees to treat early striae (striae rubra), however these treatments have
not proven helpful in treating striae alba which are mature striae, because they are more established
(Stotland et al., 2008). This can be further seen in the results and explain why participants who have
had striae for a longer period did not respond well to the remedy over the 12 week period.
It could therefore be suggested that a longer study period might be required in order to record more
favourable results.
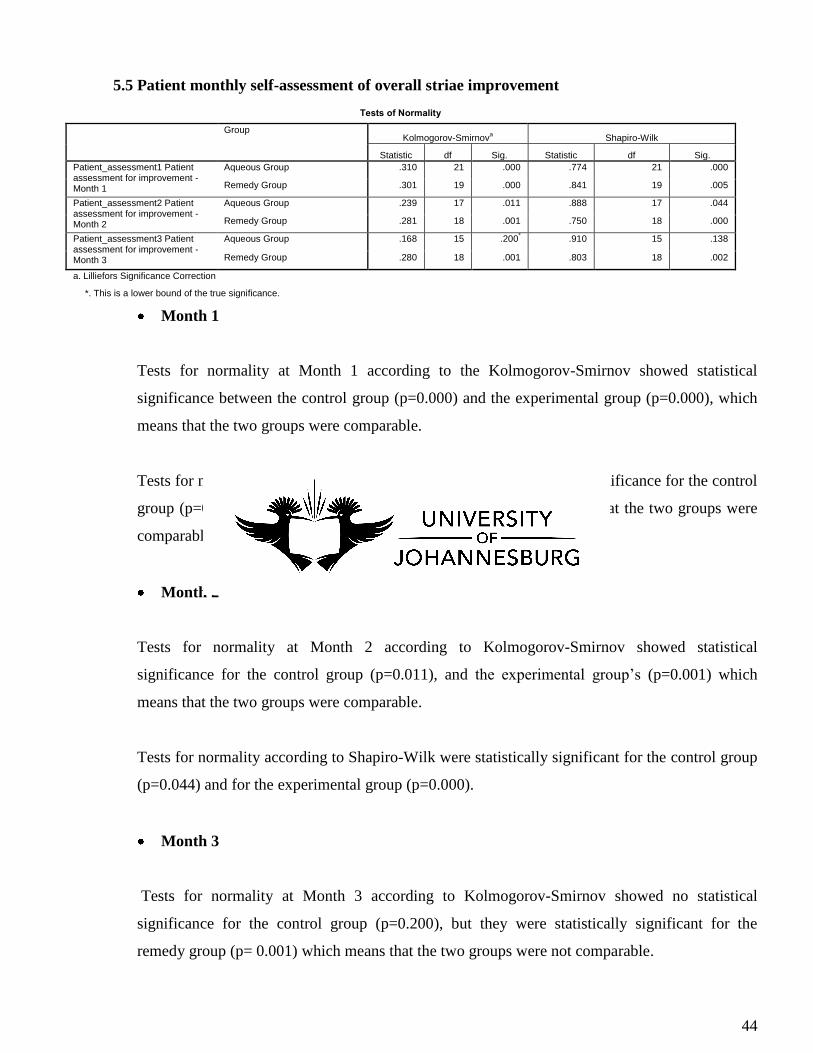
44
5.5 Patient monthly self-assessment of overall striae improvement
Tests of Normality
Group Kolmogorov-Smirnov
a Shapiro-Wilk
Statistic df Sig. Statistic df Sig.
Patient_assessment1 Patient assessment for improvement - Month 1
Aqueous Group .310 21 .000 .774 21 .000
Remedy Group .301 19 .000 .841 19 .005
Patient_assessment2 Patient assessment for improvement - Month 2
Aqueous Group .239 17 .011 .888 17 .044
Remedy Group .281 18 .001 .750 18 .000
Patient_assessment3 Patient assessment for improvement - Month 3
Aqueous Group .168 15 .200* .910 15 .138
Remedy Group .280 18 .001 .803 18 .002
a. Lilliefors Significance Correction
*. This is a lower bound of the true significance.
Month 1
Tests for normality at Month 1 according to the Kolmogorov-Smirnov showed statistical
significance between the control group (p=0.000) and the experimental group (p=0.000), which
means that the two groups were comparable.
Tests for normality according to Shapiro-Wilk test showed statistical significance for the control
group (p=0.000) and the experimental group (p= 0.005) which means that the two groups were
comparable.
Month 2
Tests for normality at Month 2 according to Kolmogorov-Smirnov showed statistical
significance for the control group (p=0.011), and the experimental group’s (p=0.001) which
means that the two groups were comparable.
Tests for normality according to Shapiro-Wilk were statistically significant for the control group
(p=0.044) and for the experimental group (p=0.000).
Month 3
Tests for normality at Month 3 according to Kolmogorov-Smirnov showed no statistical
significance for the control group (p=0.200), but they were statistically significant for the
remedy group (p= 0.001) which means that the two groups were not comparable.
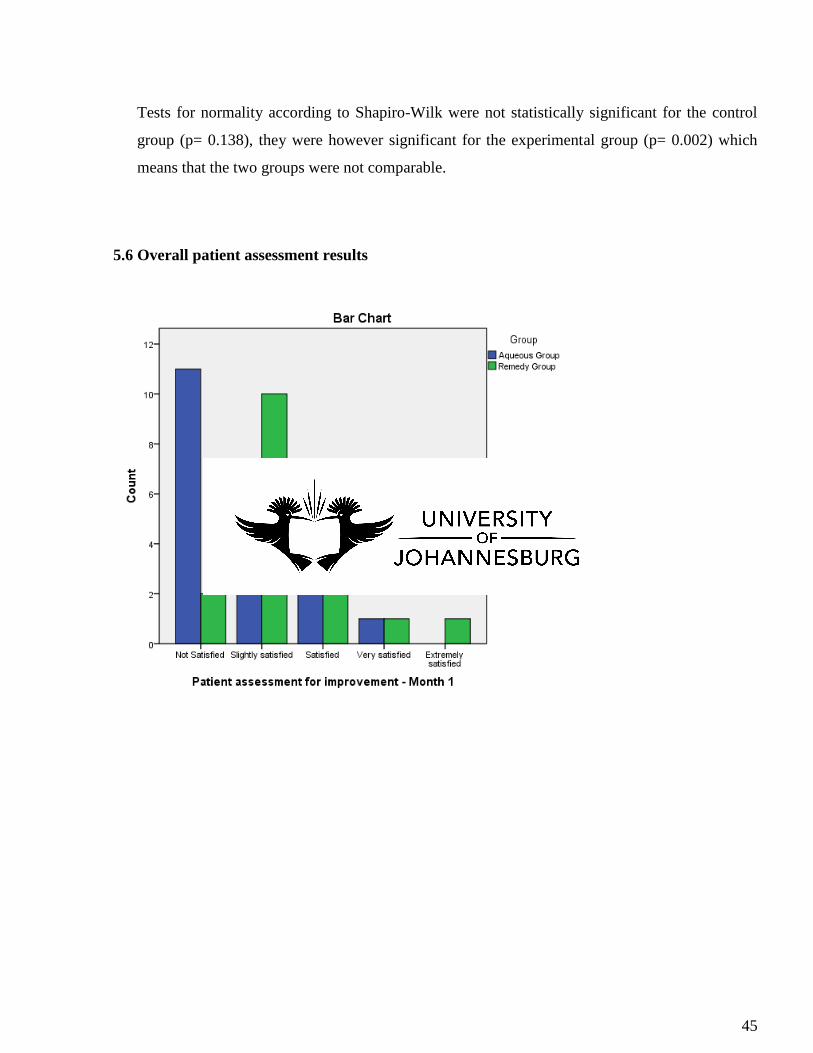
45
Tests for normality according to Shapiro-Wilk were not statistically significant for the control
group (p= 0.138), they were however significant for the experimental group (p= 0.002) which
means that the two groups were not comparable.
5.6 Overall patient assessment results
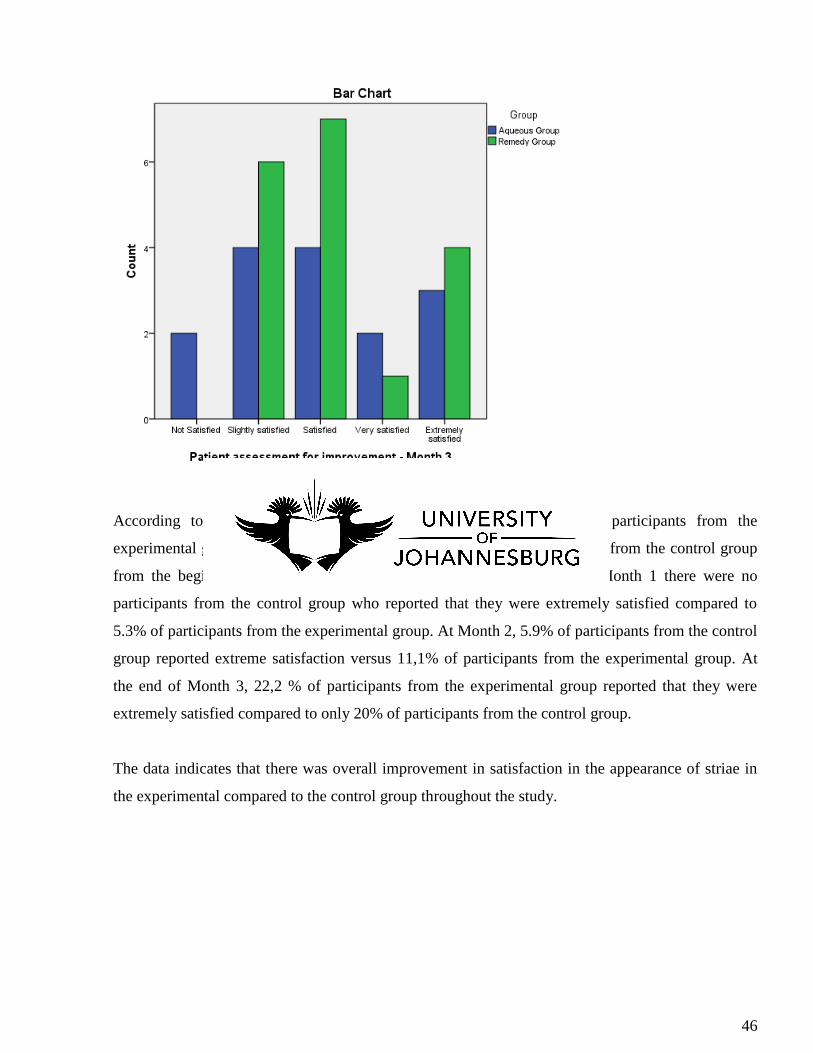
46
According to the participants’ subjective assessment, the majority of participants from the
experimental group were more satisfied with the treatment than participants from the control group
from the beginning of the treatment until the end of the treatment. At Month 1 there were no
participants from the control group who reported that they were extremely satisfied compared to
5.3% of participants from the experimental group. At Month 2, 5.9% of participants from the control
group reported extreme satisfaction versus 11,1% of participants from the experimental group. At
the end of Month 3, 22,2 % of participants from the experimental group reported that they were
extremely satisfied compared to only 20% of participants from the control group.
The data indicates that there was overall improvement in satisfaction in the appearance of striae in
the experimental compared to the control group throughout the study.
47
6 CONCLUSIONS AND RECOMMENDATIONS
6.1 Conclusions
Thiosinaminum 1X, a homoeopathic remedy, is indicated for the treatment of striae; however no
research exists on its efficacy. It is also used as a resolvent, externally and internally for dissolving
scar tissue, tumors, strictures and adhesions (Boericke, 2005)
This study aimed to determine the efficacy of the remedy Thiosinaminum 1X applied as a topical
application on the appearance of striae.
According to the results presented in Chapter 4, the treatment did not result in improvement in
appearance of striae; however, more participants from the experimental group reported that they
were more satisfied with the treatment. There was not enough evidence to support the hypothesis
that the topical application of Thiosinaminum 1X is an effective approach in treating striae.
6.2 Recommendations
In order to evaluate these findings in any future research on this topic, the following
recommendations should be taken into consideration.
Choosing a larger sample of participants (possibly 60 or more) as this could increase the
accuracy of statistical interpretations.
The study took place over a period of twelve weeks; in future studies it is recommended to
consider extending the research period perhaps from 12 weeks to 24 weeks in order to observe
more accurate changes in the appearance of striae.
Other forms of treatment such as oral administration of Thiosinaminum should also be
considered.
Experimenting with different potencies of the homoeopathic remedy Thiosinaminum.
Another suggestion for further research would be to test other indicated remedies for striae, for
example Calcarea Fluorica and Silica perhaps in combination with Thiosinaminum.

48
Participants were informed not to use any other treatments for striae during the course of the
study. Compliance should be carefully monitored.
Matching future studies in terms of skin types, age and duration of condition could possibly aid
in minimizing the placebo effect.
49
REFERENCES
Admin (2009). Stretch Mark Treatment- Zinc To Prevent Stretch Marks. Available from
http://www.bodystretchmarks.co./stretch-mark-treatment.html Accessed on 03-05-2011
Akpoghiran, P (2011). 16TH
Sunday in Ordinary Time (Year A). Available from
http://homilies4dsoul.blogspot.com/2011/07/16th-sunday-in-ordinary-time-year.html Accessed 09-
09-2011.
Alster, T., Handrick, C., (2000). Laser Treatment of Hypertrophic Scars, Keloids, and Striae.
Seminars in Cutaneous Medicine and Surgery, Vol 19, No 4 (Dec), 2000: Pg 287-292.
Anne, J (2011). Vitamins for Skin Care- Vitamins Which Protect your Skin. Available from
http://www.ehealthyone.com/Vitamins-Skin.html Accessed on 03-02-2011
Aziz, A (2010). The Law of Similars and Potentization. Available from
http://www.aliclinic.com/2010/11/the-law-of-similars-and-potentization/ Accessed on 19-05-2011
Beers, M.H., Fletcher, A.J., Jones, T.V., Porter, R., Berkwits, M.D., Kaplan, J.L. (2003). The Merck
Manual of Medical Information. Whitehouse Station: New Jersey. Pg.870, 1073-1074.
Bhowmik, D., Chiranjib, K., Kumar, S (2010). A potential medicinal importance of zinc in human
health and chronic disease. Int J Pharm Biomed Sci (2010), 1(1), 05-11. Available from
http://pharmainterscience.com/Docs/IJPBS-2010-01-02.pdf Accessed on 04-04-2011
Boericke, W. (2005). Pocket Manual of Homeopathic Materia Medica. Pg. 41, 150, 290, 312
Buehler, M (2006). Nature designs tough collagen: Explaining the nanostructure of collagen fibrils.
Available from http://web.mit.edu/mbuehler Accessed on 22 February 2011
Castro, M (1993). Homoeopathy for pregnancy, birth and your baby’s first year. St. Martin’s Press:
New York. Pg. 4,102,166
50
Cavanaugh, C (2000). Reader’s Digest: Curing everyday ailments the natural way . Heritage
Publishers: Newlands Pg 333
Coustan, D (2011). How Microdermabrasion Works. Available from
http://www.health.howstuffworks.com/skin-care/beauty/skin-treatmentys/microdermabrasion.htm
Accessed on 13-04-2011.
De Angelis, F., Adatto, M (2010). Fractional, Non-Ablative Laser Therapy for the Treatment of
Striae Distensae. Available from http://www.palomarmedical.com Accessed on 14-03-2011
Dee, S (2011). What is Thiosinaminum? Available from http://www.wisegeek.com/what-is-
thiosinaminum.htm Accesesed on 23-05-2011
Evans, R (2007).Homoeopathy: Classical, Clinical, and Complex. Available from
http://www.manteega.com/packlunch/articles/homeopathy.htm Accessed on 10-11-2011
Fillipone, P (2009). Mustard History- The History of Mustard as Food. Available from
http://homecooking.about.com/od/foodhistory/a/mustardhistory.htm Accessed on 19-04-2011
Gray & Henry (2009). Gray’s Anatomy: Descriptive and Applied. (Philadelphia : Lea &
Febiger,1913).Available from
http://images.search.yahoo.com/images/view?back=http%3A%2F%2Fsearch.yahoo.com%2Fsearch
%3Fei%3DUTF-
8%26p%3Depidermis&w=160&h=121&imgurl=www.bing.com%2Fimages%2Fsearch%3Fq%3De
pidermis%23focal%3D3bed27ee02330b550bb800d3db1db4e2%26furl%3Dhttp%253a%252f%252f
etc.usf.edu%252fclipart%252f54100%252f54137%252f54137_epidermis_lg.gif&size=&name=sear
ch&rcurl=http%3A%2F%2Fwww.bing.com%2Fimages%2Fsearch%3Fq%3Depidermis%23focal%
3D3bed27ee02330b550bb800d3db1db4e2%26furl%3Dhttp%253a%252f%252fetc.usf.edu%252fcli
part%252f54100%252f54137%252f54137_epidermis_lg.gif&rurl=http%3A%2F%2Fwww.bing.co
m%2Fimages%2Fsearch%3Fq%3Depidermis%23focal%3D3bed27ee02330b550bb800d3db1db4e2
%26furl%3Dhttp%253a%252f%252fetc.usf.edu%252fclipart%252f54100%252f54137%252f54137
_epidermis_lg.gif&p=epidermis&type=&no=3&tt=115&oid=http%3A%2F%2Fts2.mm.bing.net%2
51
Fimages%2Fthumbnail.aspx%3Fq%3D1146799599537%26id%3Daafadd43fa38219533dddb54437f
8b9f&tit=Section+of+the+Epidermis+Clipart&sigr=155dtp7o1&sigi=14ulp9q5p&sigb=11jrecjj1&f
r=yfp-t-423 Accessed on 12-08-2011
Haines, C. (2005). Stretchmarks. Available from http://www.medicinet.com/stretchmarks/
article.html Accessed on 03-09-2009.
Health Communities. (2007). Skin Types & Cosmetic Procedures. Available from
http://www.dermatologychannel.net/cosmetic/skin/skin-types.shtml Accessed on 13-06-2010
Hill, P. (2007). Permanent Makeup: Tips and Techniques. Thomson Delmar Learning: New York.
Pg. 25
Hill, P. (2006). Peels and Peeling Agents. Thomson Delmar Learning: New York. Pg. 2,108.
Hill, P. (2005). Microdermabrasion. Thomson Delmar Learning: New York Pg. 5, 77, 246.
Itamura, R. (2007) Effect of homoeopathic treatment of 60 Japanese patients with chronic skin
disease. Complementary Therapies in Medicine. (2007) 15, 115-120 Available from http://0-
www.sciencedirect.com.ujlink.uj.ac.za/science/article/pii/S0965229906000677 Accessed on 12-10-
2010
Kang, S., Arbor, A. (1998). Topical tretinoin therapy for management of early striae. Journal of the
American Academy. Vol. 39, Issue 2, Supplement 2, August 1998, Pg. S90-S92. Available from
http://0-www.sciencedirect.com.ujlink.uj.ac.za/science? Accessed on 06-02-2009.
Keegan, L (2001). Healing with complementary and alternative therapies. Available from
http://books.google.co.za/books?id=JF5STWO2qtQC&pg=PA135&lpg=PA135&dq=hOMOEOPA
THIC+DILUTIONS-
+KEEGAN+2001&source=bl&ots=5VZP5Idgx_&sig=10VHqI4mP5eifOVr4KbwTSJQl2Q&hl=en
#v=onepage&q&f=false Accessed on 08-10-2011
52
Lees, M (2007). Skin Care- Beyond Basics. Thomson Delmar Learning: New York. Pg.6, 77, 78 ,
136
Longmore, M., Wilkinson, I., Turmezei, T., Cheung, C.K. (2007). Oxford Handbook of Clinical
Medicine. Oxford University Press : New York. Pg. 698
Manuskiatti, W., Boonthaweyuwat, E., Varothai, S. (2010) Treatment of striae distensae with a
TriPolar radiofrequency device: A pilot study. Available from http://www.fisioestetica.com/art.
Accessed on 07-02-2010
Niles, R . Standard Deviation. Available from http://www.robertniles.com/stats/stdev.shtml Accesed
on 02-10-2011
Nortman, D (2011). Basics of Homoeopathic Prescription. Available from
http://www.homeopathyzone.com/blog/article/basics-of-the-homeopathic-prescription Accessed on
20-05-2011
Novak, M (2004). 50 Years ago in The Journal of Paediatrics. Colored striae in adolescent
children. Pg 645
Osman, H., Rubeiz, N., Tamin, H., Nassar (2007). Risk factors for the development of striae
gravidarum. American Journal of Obstetrics and Gynaecology (2007) 196: 62.e1-62.e5. Available
from http://www.ncbi.nlm.nlin.nih.gov/pubmed/17240237 Accessed on 03-04-2010
Papadoupoulos, L., Walker, C (2003). Understanding Skin Problems. Wiley: New Jersey. Pg.59
Piper, T (2008). Stedman’s Medical Dictionary for Health Professions and Nursing. (6th
edition).
Julie K. Stegman: United States of America. Pg. 1487
Quinn, D (2008). Homoeopathy and the Integration of Feelings. Available from
http://hpathy.com/homeopathy-papers/homoeopathy-and-the-integration-of-feelings/ Accessed on
22-04-2011
53
Sahani, M. (2007). Principles and Practice of Homoeopathic Pharmacy for Students. B. Jain
Publishers: New Delhi (India).Pgs.90-91.
Salter, S., Kimball, A (2006). Striae Gravidarum. Clinics in Dermatology (2006) 24, 97-100
Samer, A (2009). Striae distensae. Available from http://e-medicine.medscape.com/article/1074868
Accessed on 02-02-2010
Science Daily, (2006). Math Model Could Aid Study of Collagen Ailments. Available from
http://www.google.co.za/imgres?imgurl=http://images.sciencedaily.com/2006/11/061114190020.jpg
&imgrefurl=http://www.sciencedaily.com/release/2006/11/061114190020.htm&usg=_mNAjyGftZd
Vnso96A5R98o4kyE0=&h=300&sz=17&hl=en&start=24&zoom=1&itbs=1&tbnid=4I0 Accessed
on 24-08-2011
Smit, A. (2001). The effects of the application of a cream containing Botulinum toxin expressed in a
potency of D24, D30 or 200CH on vertical frown lines. Pg.10
Stotland, M., Chapas., M., Brightman, L., Sukal, S., Hale, E., Karen, J., Bernstein, L., Geronemus,
G. (2008). The safety and efficacy of fractional photothermolysis for the correction of striae
distensae. Journal of Drugs in Dermatology. Available from
http://www.accessmylibrary.com/com2/summary Accessed on 21-05-2009
Ullman, D (2007). The Homoeopathic Revolution. North Atlantic Books : California Pg 24
Vermeulen, F (2002). The Arcana of Materia Medica Illuminated. Similars and Parallels Between
Substance and Remedy. Emryss bv Publishers : The Netherlands. Pg. 314, 319, 1232, 1242.
Wala’a, E (2007). Polymorphic Eruption of Pregnancy. Available from
http://www.google.co.za/imgres?imgurl=http://www.medscape.com/content/1997/00/40/88/408878/
art-
wh3076.fig2.jpg&imgrefurl=http://www.medkaau.com/vb/showthread.php%3Ft%3D8709&h=450
&w=299&sz=22&tbnid=yw5AxLa-hn-
6CM:&tbnh=127&tbnw=84&prev=/search%3Fq%3Dabdominal%2Bstriae%2Bpregnancy%2Bpictu
54
res%26tbm%3Disch%26tbo%3Du&zoom=1&q=abdominal+striae+pregnancy+pictures&hl=en&us
g=__mQx6xtbkvGBwWHktDfjdh-
YSAqg=&sa=X&ei=g655TqipCMjE8QOCuu0Q&ved=0CBUQ9QEwAQ Accesesed on 22-05-
2010
Wanjiru, M (2011). History Of The Origins Of The Mustard Seed. Available from
http://www.streetdirectory.com/food_editorials/snacks/dips_and_sauces/history_of_th.. Accessed on
01-05-2011.
Webb, G (2002). Nutrition : A health promotion approach. Oxford University Press : New York.
Pg 277
Wong, C. (2007). Remedy for Scars and Scar removal. Available from
http://altmedicine.about.com/od/qalibrary/f/remedyscars.htm Accessed on 08-08-2011
Worden, J (2011). Homoeopathy. Available from http://www.netdoctor.co.uk/health
advice/facts/homoeopathy.htm Accessed on 20-05-2011
Xydau, (2010). Glucocorticoid Withdrawal Syndrome. Available from http://medipptx.
blogspot.com/2010/09/glucocorticoid-withdrawal-syndrome_3824.html Accessed on 10-08-2011.
Yosipovitch, G., Devore, A., Dwan, A. (2007). Obesity and the skin: Skin physiology and skin
manifestation of obesity. American Academy of Dermatology. Pg. 901 Available from
http://www.ncbi.nlm.nih.gov/pubmed/175047154
55
APPENDIX A
PARTICIPANT’S INFORMATION SHEET
Dear participant
A research study is to be undertaken by a student of homoeopathy, as partial requirement for the
completion of study to obtain a Master of Technology: Homoeopathy qualification. This course of
study is presented at the University of Johannesburg.
The researcher is Koketso Letitia Ramoupi, a student that has completed her fifth year.
Cellular phone number: 071 431 5114
Two qualified homoeopaths will be supervisors of this project:
Dr. R K Razlog. Telephone number: 011 406 2440
Dr. R. Moiloa Cellphone number: 082 858 4805
These professionals may be contacted.
A cream is to be applied to stretch marks on the abdomen, thighs or buttock area. The object of this
research project is to establish whether a specific homoeopathic remedy, Thiosanimium 1X
incorporated into this cream, will improve the appearance of stretch marks and make them less
invisible.
The forty participants will be divided into two groups. The one group will receive the medicated
cream and the other group known as the control group will be a placebo cream. This control group
will not be identified to the participant or researcher before, or during this period, therefore the
participants will not know whether the homoeopathic remedy has been incorporated into the cream
that they are using. A double blind study will thus be insured. The data gathered by the researcher
will not be biased.
The cream will have to be applied twice daily for a period of three months. Photographs and
physical measurements of the stretch marks will be done at the initial consultation and at monthly
intervals thereafter of three months. The remedy will be prepared homoeopathically and therefore no
physically measurable quantities of the toxin will be present. The creams will therefore not have the
56
same effects, as would an allopathic product. The homoeopathic remedy incorporated into the cream
will not result in any poisoning.
Participation in this study is voluntary and refusal to participate will involve no penalty or loss of
benefits to which the subject is otherwise entitled. The participant may discontinue at any time
without penalty or loss of benefits.
DIRECTIONS FOR USE OF THE CREAM
1. Participants will be advised not to apply any other creams/lotions/ointments on the treatment
areas, as this could affect the validity of the results.
2. Participants are to apply the cream on the demarcated treatment areas twice daily for a
minimum of three months.
3. Avoid over-exposure to the sun.
4. No other treatment for stretch marks is to be used during the research study.
5. Participants should immediately inform the researcher if any of the following is experienced:
- Any new unfavourable changes on the skin.
- Any discomfort attributed to the cream.
57
APPENDIX B
PARTICIPANT CONSENT FORM
I hereby consent to the following:
1. I will apply the cream as explained above.
2. Photographs of my face may be taken at the onset of and during the study for research
purposes.
3. My stretch marks may be physically measured and I give permission for photographs of the
treatment areas to be taken be and used for research purposes.
4. I am consenting to involvement in a research study and have no presumptions about the
results.
6. Records of my home address and telephone number may be kept for research purposes.
7. I am aware that my stretch marks may or may not show any improvement at the end of the
research study.
8. The possibility that none of the active substances may be administered exists, and the
researcher cannot reveal whether an active substance or a placebo is being administered.
9. I am free to withdraw from the trial at any time without prejudicing any treatment that is
required for existing or future medical conditions.
10. I am fully aware of the fact that participation in this study is voluntary and my refusal to
participate will involve no penalty or loss of benefits to which I am otherwise entitled.
Full Names: _______________________________
Surname :_______________________________ Initials :_________
Birth date: __________________ Age :_________
Physical address: __________________________________
___________________________________
Phone (Home):___________________
Cell number: _____________________
Signature of Participant: __________________________
Date: ______________________
58
APPENDIX C
QUESTIONNAIRE
1. Name: __________________________
2. Surname: ______________________
3. Age: _______________ 4. Date of birth: __________________
Please answer the following.
5. Do you have stretch marks? ________
6. What areas on your body are affected by stretch marks? _________________________________
7. Approximately, how many years have you had stretch marks? Tick the applicable answer.
Number of years that you have had stretch marks
< 5 years
Between 5 and 10 years
Between 10 and 15 years
More than 15 years
8. Cause of stretch marks. Tick the applicable answer.
Pregnancy
Weight gain
Weight loss
Unknown
9.Do you suffer from any of the following?
Cushing’s syndrome
Marfan’s syndrome
Slow healing wounds
Diabetes
Eczema
59
APPENDIX D
Patient assessment of improvement at the 3-month follow-up evaluation.
Name of participant:
Location of treatment area:
This assessment is to evaluate the level of improvement that you have observed during this
treatment. Please tick the appropriate answer.
I = NOT SATISFIED ………………
II = SLIGHTLY SATISFIED …………………
III = SATISFIED ………………..
IV = VERY SATISFIED ………………….
V = EXTREMELY SATISFIED ………………..
Comments about the study ……………………………………………………………
60
APPENDIX E
Name of participant:
Location of treatment area:
This assessment is to evaluate the appearance of your stretch marks as well as any psychological
effects that have been brought on by the stretch marks. Please tick the appropriate answer that may
apply to you.
PHYSICAL APPEARANCE OF STRETCH MARKS
1. I have noticed a change in the texture of my skin ever since I developed stretch marks.
Strongly Agree Agree Strongly
Disagree
Disagree
2. My stretch marks appear darker than my skin colour.
Strongly Agree Agree Strongly
Disagree
Disagree
3. My stretch marks appear lighter than my skin colour.
Strongly Agree Agree Strongly
Disagree
Disagree
4. My stretch marks are all symmetrical in size.
Strongly Agree Agree Strongly
Disagree
Disagree
5. The size (length and width) of my stretch marks has increased with time.
Strongly Agree Agree Strongly
Disagree
Disagree
PSYCHOLOGICAL QUESTIONS
1. I feel embarrassed about my stretch marks.
Strongly Agree Agree Strongly
Disagree
Disagree
61
2. My stretch marks make feel unattractive.
Strongly Agree Agree Strongly
Disagree
Disagree
3. I am ashamed to take my clothes off in front of people because of my stretch marks.
Strongly Agree Agree Strongly
Disagree
Disagree
4. I feel sad when I think about my stretch marks.
Strongly Agree Agree Strongly
Disagree
Disagree
5. I am irritated by my stretch marks.
Strongly Agree Agree Strongly
Disagree
Disagree
62
APPENDIX F
DO YOU SUFFER FROM STRETCH MARKS?
- Do you have stretch marks on your thighs or buttock area?
- Have you had stretch marks for 6 months or longer?
- Are you black female aged between 18 and 35 years of age?
IF you answered YES to all of the above, then you may qualify to participate in a research
study being conducted through the Department of Homoeopathy:
‘The efficacy of Thiosinaminum 1X in the treatment of striae gravidarum.’
Ethical clearance number:
This study is being conducted at the University of Johannesburg’s Homoeopathic Health
Centre.
Participation is voluntary and strictly confidential.
If you qualify to take part in this study consultations and treatment will be offered to you
FREE OF CHARGE.
Researcher’s name: Koketso Ramoupi
Contact details: 071 431 5114
63
APPENDIX G
MASTER FORMULA AND METHOD
100g Thiosinaminum CREAM
PRODUCT: 100g Thiosinaminum CREAM
DESCRIPTION OF PHYSICAL FORM AND STRENGTH: aqueous cream in a 100g plastic
container.
LIST OF STARTING MATERIALS:
Materials and manufacturing equipment Quantity
Thiosinaminum mother tincture 1ml
Unmedicated aqueous cream 99 g
100g plastic ointment jar container 1
Pastel and mortar 1
Label 1
TOTAL EXPECTED YIELD: 100 g of medicated aqueous cream
PROCESSING INSTRUCTIONS
1. Clean and flame equipment.
2. Measure 1ml of stock remedy.
3. Mass out 99 g of the aqueous cream. Pour it into the pastel.
4. Divide the required number of drops of medicating potency by 3 for triple impregnation using
a dropper bottle. Mix the aqueous cream with the remedy using the mortar.
5. Place the medicated aqueous cream into the 100g ointment jar.
64
APPENDIX H
Standard Operating Procedures (SOP): Research Photographs
1. The same camera (Samsung S700) was used to take pictures at the beginning of the study
and at the end of the study.
2. The settings (camera angling lightning) on the camera were always standard throughout the
trials.
3. The research photographs were taken in the same room for all participants at the beginning
of the study and at the end of the study.
4. The researcher was the one who took the research photographs at the required times during
the trials.
5. The back drop conditions in the room in which the photos were taken was standard during all
the photographic sessions.
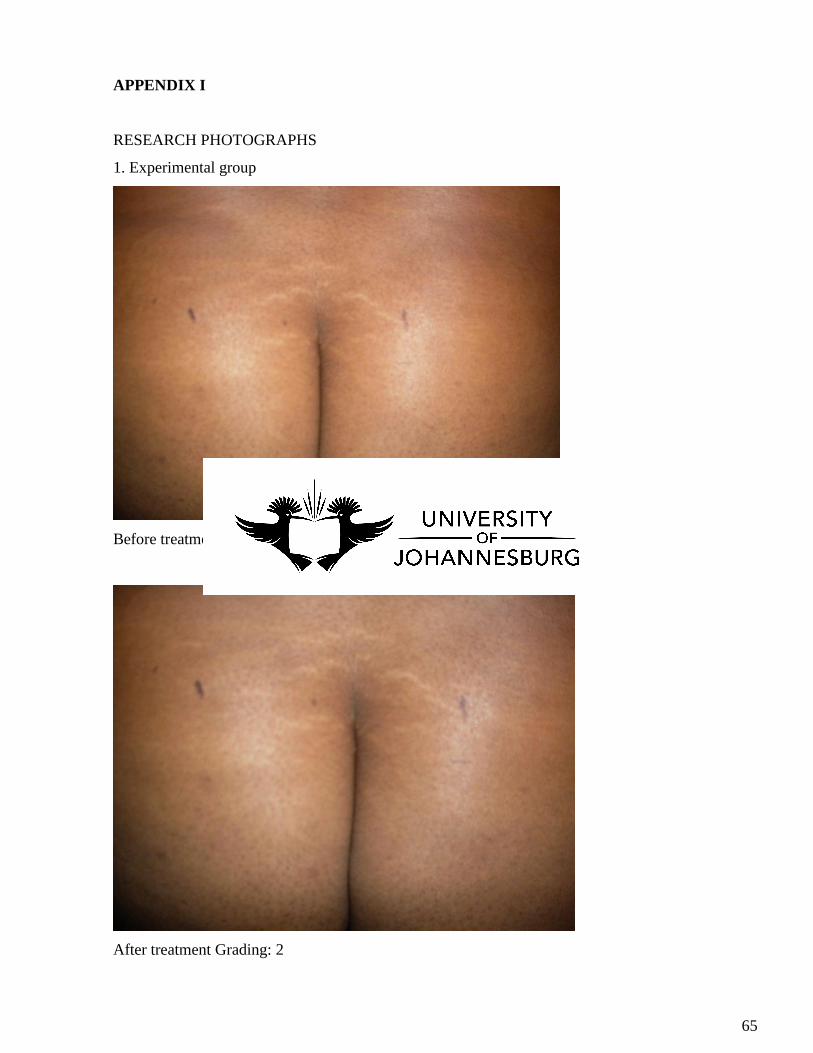
65
APPENDIX I
RESEARCH PHOTOGRAPHS
1. Experimental group
Before treatment Grading: 3
After treatment Grading: 2

66
Before treatment Grading: 4
After treatment Grading: 3
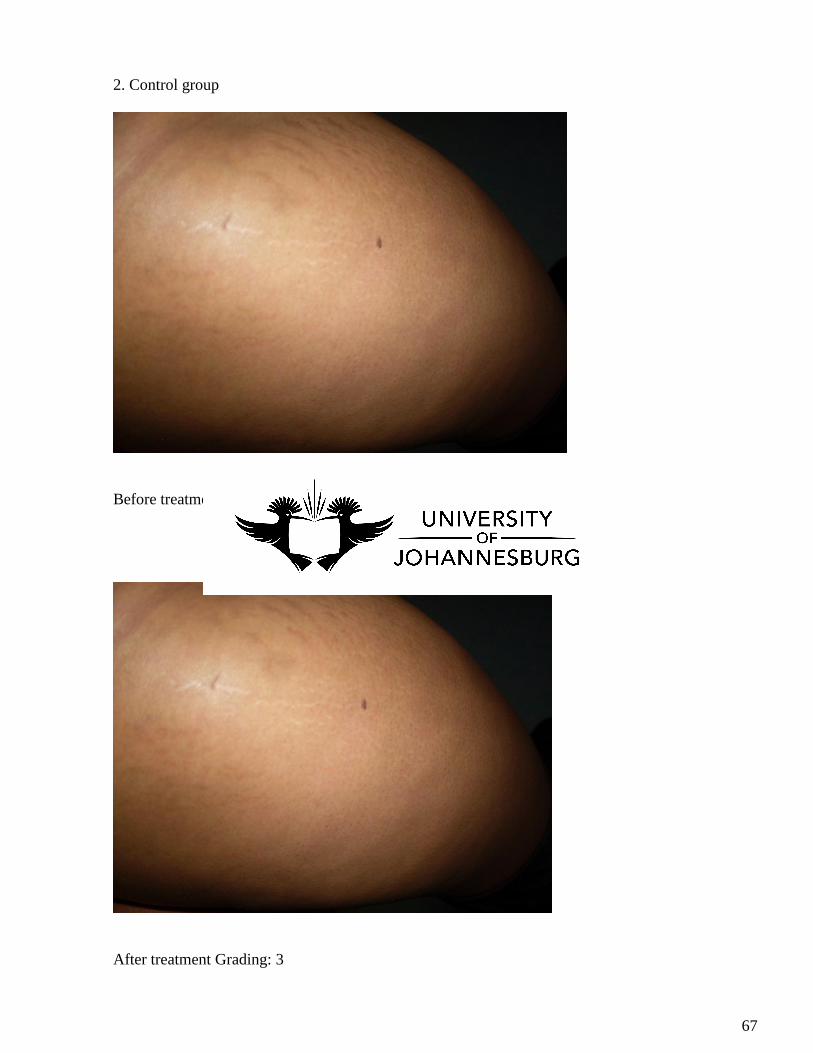
67
2. Control group
Before treatment Grading: 3
After treatment Grading: 3

68
Before treatment Grading: 3
After treatment Grading: 3

![TIE-25 Striae in optical glass 2006€¦ · The ISO 10110 part 4 [7] introduces 5 classes of striae grades for finished optical parts. In grades 1-4, only striae with intensities](https://img.pdfslide.net/doc/110x75/5b8a86117f8b9a9b7c8ca746/tie-25-striae-in-optical-glass-2006-the-iso-10110-part-4-7-introduces-5-classes.jpg)