Embed Size (px)
Citation preview

THE EFFICACY OF YOGA WITH ADDICTIONS:
A SYSTEMATIC REVIEW OF EVIDENCE
By Alexander El Amanni
The Salvation Army – Addiction Caseworker
University of Auckland – Master of Health Practice
Matua Raki 9th National Addiction Research Symposium 2018
1

• Addiction effects 3.5 percent of the New Zealand population (Oakley Browne, Wells, & Scott, 2006)
• The combined total social and treatment financial costs of addiction in New Zealand are an estimated 1.8 billion dollars annually (McFadden Consultancy, 2016)
• Common tertiary addiction interventions include psychosocial rehabilitation and inpatient detox
• The relapse rates post psychosocial rehabilitation are 25-70% within 12-18 months (Vanderplasschen, et al., 2013)
• The relapse rates post inpatient detox could be as high as 95% (National Addiction Centre & Matua Raki, n.d.)
• Yoga has been suggested as a complementary therapy in addiction treatment to enhance recovery and prevent relapse (Harris, 2015; Khanna & Greeson, 2013; Posadzki, Choi, Soo Lee, & Ernst, 2014; Sarkar & Mohit, 2016)
2

• Traditional addiction treatments are no ‘cure’, neither is yoga with addictions pitched as a definitive ‘cure’
• Yoga with addictions is complementary therapy not a replacement
• Eastern World 2500 years; ‘Western’ World 50 years (Harris, 2015)
• Brain GABA levels increase after a session of yoga (Streeter, et al., 2007)
• Yoga helps with depression by lowering plasma-cortisol levels, and adrenocorticotropic ACTH hormones (Cramer, Lauche, Langhorst, & Dobos, 2013)
• Yoga reduces stress hormone levels (Vedamurthachar, et al., 2006)
• Recent theses have found interesting evidence (Next slide) (Harris, 2015; Holthaus, 2004; Griffiths, 2007)
3

• Mantra is chanting sounds and humming vibrations, and may include clenching/pulsing back molar teeth.
• The meridian palate:
• Tuning in to the Gurus,
Masters, and Teachers,
to channel energy.• “84 meridian points, located on the palate behind the teeth … contain
information about self-perception and include deeply rooted belief systems, automatic personality traits, and habits. When the tongue struck the meridians, this stimulates the endocrine system and the hypothalamus, pituitary, and pineal glands respond. By using this built-in technology, habits can be re-formulated by chanting mantra” (Harris, 2015, p. 41).
4

The objective was to perform a search on the EBSCO Host, ProQuest, and Google Scholar databases using the search strategy; "yoga AND addictions OR (substance use disorders)”.
Exclusion criteria is any articles published in 1996 or later, and/or not specifically related to yoga interventions used with a sample of substance use disorder subjects. Ten articles were selected for the sample.
Using the (n=10) representative articles, a systematic review has been produced which employs a mixed-methods approach to the methodology and is designed as a narrative-style, scoping search.
The PRISMA checklist was followed.
5

• (1) What are the outcomes of implementing yoga as an intervention tool with substance users in ten peer reviewed articles?
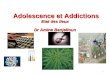
• (a) In which areas have substance users improved their health and life where yoga has been implemented as a complementary intervention tool, in the ten representative articles?
• (b) What types of yogic interventions have proven to be effective in the ten representative articles with the treatment of substance use disorders?
6

First author
(year)
Study design Type of
addiction (n)
Experimental
intervention
Control
intervention
Primary
outcome
measure
Main result (between
group differences or
otherwise)
Follow
up(s)
Author conclusions
Anand
(2013)
RCT* pilot with 2 par
llel groups
Drugs (n=20) SN* & YA*, 2 hrs per
day for 6 wks
Standard
Treatment
1. SCI*
2. OPAS*
1. Sig (P<0.001)
2. Sig (P<0.001)
None Yoga therapy is effective
in addi ction treatment.
Anju
(2015)
RCT with 2 parallel
groups
Opioids (n=84) SKY*, 12 hrs over 3
days, 30 mins a day
FU*
Standard
Treatment
1. WHO .
QOL*
1 Sig (P<0.05) phy
Sig (P<0.001) psy
Sig (P<0.001) env
Baseline, 3-
m & 6-m*
SKY can improve QOL at
6-m FU.
Chen
(2010)
Controlled clinical
trial pilot
Drugs &
Alcohol
(n=207)
Qigong Medit ation,
x10 per wk, for 4 wks
Standard
Treatment +
SMART*
1. TCR*
2. VAC*
3. SAS*
1. 92%sg 78%cg
2. N.s (P=0.69)
3. N.s (P=0.76)
Baseline, 1-
wk & 2-wk*
Mostly females will
benefit from Qigong.
Devi
(2016)
RCT with 2 parallel
groups
Drugs &
Alcohol (n=66)
M*
Yoga, 1 hr per day, 7x
a wk, for 4 wks
Waiting List 1. PSQI*
2. RSES*
3. BDI II*
1. Sig (P<0.001)
2. Sig (P=0.005)
3. Sig (P<0.001)
Baseline, &
4-wk*
Improvement to self-
esteem using yoga.
Hallgreen
(2014)
RCT pilot with 2 para
llel groups
Alcohol (n=14) Yoga, 10x 1.5 hour
sessions
Treatment As Usual 1. RAC*
2. HADS*
3. SDS*
1. N.s (P=0.17)
2. N.s (P=0.67)
3. N.s (P=0.79)
Baseline, &
6-m
Study was limited by
small sample size.
Khalsa
(2008)
Qualitative case
study pilot
Drugs &
Alcohol (n=8)
Kundalini Yoga, 3x per
day, x90 days
No Control Group 1. PSS*
2. BASIS*
3. QRI*
1. N.s (P=0.44)
2. Sig (P<0.05)
3. Sig (P<0.05)
Baseline,mi
d,end, 1-m
Yoga had a significant
impact on subjects.
Manju
(2017)
Cohort survey study Alcohol
(n=127)
Active Life Style
Factor Yoga, ongoing
No Control Group Null/alternate
(𝐻𝑎) h
ypothesis
Sig 𝐻𝑎 =(P<0.01)
(r =0.724)
N.m Correlation between
yoga and sobriety.
Marefat
(2011)
RCT with 2 parallel
groups
Drugs (n=24) Yoga, 60 mins, 3x per
wk, for 5x wks
Waiting List 1. BDI*
2. STAIT*
1. Sig (P=0.048)
2. Sig (P=0.023)
None Positive effect on
anxiety and depression.
Shaffer
(1997)
Crossover RCT with 2
groups
Drugs (n=61) HY* + MM*, 75min
per day for 22 wks
MM + Psycho-
therapy
1. SCL*
2. ASI*
3. GSI*
1. N.s
2. N.s
3. N.s
None HY+MM not more
effective than control.
Vedamurthachar
(2006)
RCT with 2 parallel
groups
Alcohol
(n=60)
SKY*+NY* 1hr per day
for 2 wks
No Intervention 1. BDI*
2. ACTH*
3.Cortisol
1. Sig (P<0.001)
2. Sig (P<0.001)
3. Sig (P<0.001)
None SKY has antidepressant
effects on alcoholics.7

First author
(year)
Study design Type of
addiction (n)
Experimental
intervention
Control
intervention
Primary
outcome
measure
Main result (between
group differences or
otherwise)
Follow
up(s)
Author conclusions
Anand
(2013)
RCT* pilot with 2 par
llel groups
Drugs (n=20) SN* & YA*, 2 hrs per
day for 6 wks
Standard
Treatment
1. SCI*
2. OPAS*
1. Sig (P<0.001)
2. Sig (P<0.001)
None Yoga therapy is effective
in addi ction treatment.
Anju
(2015)
RCT with 2 parallel
groups
Opioids (n=84) SKY*, 12 hrs over 3
days, 30 mins a day
FU*
Standard
Treatment
1. WHO .
QOL*
1 Sig (P<0.05) phy
Sig (P<0.001) psy Sig
(P<0.001) env
Baseline, 3-
m & 6-m*
SKY can improve QOL at
6-m FU.
Chen
(2010)
Controlled clinical
trial pilot
Drugs &
Alcohol
(n=207)
Qigong Medit ation,
x10 per wk, for 4 wks
Standard
Treatment +
SMART*
1. TCR*
2. VAC*
3. SAS*
1. 92%sg 78%cg
2. N.s (P=0.69)
3. N.s (P=0.76)
Baseline, 1-
wk & 2-wk*
Mostly females will
benefit from Qigong.
Devi
(2016)
RCT with 2 parallel
groups
Drugs &
Alcohol (n=66)
M*
Yoga, 1 hr per day, 7x
a wk, for 4 wks
Waiting List 1. PSQI*
2. RSES*
3. BDI II*
1. Sig (P<0.001)
2. Sig (P=0.005)
3. Sig (P<0.001)
Baseline, &
4-wk*
Improvement to self-
esteem using yoga.
Hallgreen
(2014)
RCT pilot with 2 para
llel groups
Alcohol (n=14) Yoga, 10x 1.5 hour
sessions
Treatment As Usual 1. RAC*
2. HADS*
3. SDS*
1. N.s (P=0.17)
2. N.s (P=0.67)
3. N.s (P=0.79)
Baseline, &
6-m
Study was limited by
small sample size.
Khalsa
(2008)
Qualitative case
study pilot
Drugs &
Alcohol (n=8)
Kundalini Yoga, 3x per
day, x90 days
No Control Group 1. PSS*
2. BASIS*
3. QRI*
1. N.s (P=0.44)
2. Sig (P<0.05)
3. Sig (P<0.05)
Baseline,mi
d,end, 1-m
Yoga had a significant
impact on subjects.
Manju
(2017)
Cohort survey study Alcohol
(n=127)
Active Life Style
Factor Yoga, ongoing
No Control Group Null/alternate
(𝐻𝑎) h
ypothesis
Sig 𝐻𝑎 =(P<0.01)
(r =0.724)
N.m Correlation between
yoga and sobriety.
Marefat
(2011)
RCT with 2 parallel
groups
Drugs (n=24) Yoga, 60 mins, 3x per
wk, for 5x wks
Waiting List 1. BDI*
2. STAIT*
1. Sig (P=0.048)
2. Sig (P=0.023)
None Positive effect on anxiety
and depression.
Shaffer
(1997)
Crossover RCT with 2
groups
Drugs (n=61) HY* + MM*, 75min
per day for 22 wks
MM + Psycho-
therapy
1. SCL*
2. ASI*
3. GSI*
1. N.s
2. N.s
3. N.s
None HY+MM not more
effective than control.
Vedamurthachar
(2006)
RCT with 2 parallel
groups
Alcohol
(n=60)
SKY*+NY* 1hr per day
for 2 wks
No Intervention 1. BDI*
2. ACTH*
3.Cortisol
1. Sig (P<0.001)
2. Sig (P<0.001)
3. Sig (P<0.001)
None SKY has antidepressant
effects on alcoholics.
1 SIG
2 SIG
3 SIG
4 SIG
5 SIG
6 SIG
7 SIG 8

0 1 2 3 4 5
QoL
Anxiety
Urges/Cravings
Depression
3
3
4
5
Number of Outcome Measures with Statistically Significant Results
Are
a o
f H
eal
th o
r Li
fe
Outcome Measure Themes
9
0 1 2 3 4 5
Self-Efficacy
Sleep
Stress
Withdrawal Symptoms
Social Functioning
2
2
2
2
2
Number of Outcome Measures with Statistically Significant Results
Are
a o
f H
eal
th o
r Li
fe
Outcome Measure Themes
10

Types of yoga Description Effectiveness
Active Life Style Factor Physical work out, emotional psychology, inhibits dopamine surge Low
Hatha yoga Yoga postures, breathing and deep relaxation techniques Low
Kundalini yoga Chanting, mindful meditation, kriya, mindful breathing Low
Qigong meditation Relaxation, breathing, guided imagery, inward attention,
mindfulness, and tranquil states
Low
Surdarshan Kriya Yoga (SKY) Breathing techniques and exercises High
Surya Namaskar & Yogic
Asanas
Asanas, kapal bhatti, pranayama and meditation Low
Yoga practice/exercise/
intervention
Not described Unknown
11

• One RCT evidenced that Hathya Yoga is equally as effective as GPT
• One RCT was limited by small sample size
• One cohort study was limited by not being randomised nor controlled
• One case study pilot used Kundalini yoga as the main intervention; it is was difficult to determine the cause of the benefits
• One study was a controlled clinical trial but was not randomised
• Only one type of yoga was rated as effective (SKY)
• Due to the nature of the intervention, there is no patient/subject blinding
• The heterogeneity of the data was compromised by too many different outcome measures; the differing study designs, and control interventions; creating too many confounding variables. 12

• Five RCTs were considered empirically sound, and provided strong evidence about the positive effects of yoga with addictions (p=<0.05).
• Yoga with addiction is most effective as a complementary intervention
• Yoga stimulates physiological and biochemical activity – no matter what the patients beliefs and values are about spirituality or yoga (Matus, 2013)
• Yoga helps with depression by lowering plasma-cortisol levels, and adrenocorticotropic ACTH hormones (Cramer, Lauche, Langhorst and Dobos, 2013)
• There is now a growing body of epistemological evidence detailing the benefits of yoga as a complementary therapy in the treatment of substance use disorders
13

• The evidence of the studies suggests that yogic interventions, such as SKY, are suitable to recommend to patients with a substance use disorder and co-existing depressive symptoms, as a complementary intervention.
• More longitudinal clinical trials are needed to measure the relapse prevention efficacy of yoga with addictions.
• Conclusions are limited by both a high risk of bias due to no patient blinding, and an excess of differing outcome measures which created too many confounding variables.
14

• Anand, M., Alagesan, J., & Prathap, S. (2013). Effect of yoga therapy in rehabilitation of drug addicts. Medical Science, 2(7), 153-154.
• Anju, D., Anita, C., Raka, J., Deepak, Y., & Vedamurthachar. (2015). Effectiveness of yogic breathing intervention on quality of life of opioid dependent users. International Journal of Yoga, 8, 144-146.
• Chen, K., Comerford, A., Shinnich, P., & Ziedonis, D. (2010). Introducing Qigong meditation into residential addiction treatment: A pilot study where gender makes a difference. The Journal of Alternative and Complementary Medicine, 16(8), 875-882.
• Cramer, H., Lauche, R., Langhorst, J., & Dobos, G. (2013). Yoga for depression: A systematic review and meta-analysis. Depression and Anxiety, 30(11), 1068-1083.
• Devi, N., & Singh, T. (2016). A randomised control trial of the effect of yoga on quality of sleep, self-esteem and depression in substance abusers. International Journal of Multidisciplinary Approach and Studies, 3(4), 9-11.
• Griffiths, M. (2007). Teaching yoga in addiction recovery: A social work perspective (Unpublished masters thesis). Melbourne, Australia: University of Melbourne.
• Hallgren, M., Romberg, K., Bakshi, A., & Andréasson, S. (2014). Yoga as an adjunct treatment for alcohol dependence: a pilot study. Complementary therapies in medicine, 22(3), 441-445.
• Harris, W. (2015). Beyond addiction: Kundalini yoga and mindfulness meditation for recovery from opioid dependence. (Unpublished doctoral thesis). LA, United States of America: California School of Professional Psychology.
• Holthaus, S. (2004). A phenomenological study: Yoga during recovery from drugs or alcohol (Unpublished doctoral thesis). Carpinteria, CA: Pacifica Graduate Institute.
• Khalsa, S. B., Khalsa, G. S., & Khalsa, M. K. (2008). Evaluation of a residential Kundalini yoga life style pilot programme for addiction in India. Substance, 7(1), 67-80.
• Khanna, S., & Greeson, J. (2013). A narrative review of yoga and mindfulness as complementary therapies for addiction. Complementary Therapies in Medicine, 21, 244-252.
15

• Manju, E., & Chandrasekav, K. (2017). A study on recovery from substance addiction by yoga with active life style factor. Asian Journal of Applied Science and Technology, 1(7), 95-97.
• Marefat, M., Peymanzad, H., & Alikhajeh, Y. (2011). The study of the effects of yoga exercises on addicts' depression and anxiety in rehabilitation period. Procedia - Social and Beahavioural Sciences, 30, 1494-1498.
• McFadden Consultancy. (2016). Research report: The New Zealand drug harm index 2016 (2nd ed.). Wellington, New Zealand: Ministry of Health.
• Shaffer, H., LaSalvia, T., & Stein, J. (1997). Comparing Hatha yoga with dynamic group psychotherapy for enhancing methadone maintenencetreatment: A randomised clinical trial. Alternative Therapies in Health and Medicine, 3(4), 57-66.
• National Addiction Centre & Matua Raki. (n.d.). Orientation to the addiction treatment field Aotearoa New Zealand. Retrieved from www.otago.ac.nz/nationaladdictioncentre/pdfs/orientation.pdf
• Oakley Browne, M. A., Wells, J. E., & Scott, K. M. (Eds.). (2006). Te rau hinengaro: The New Zealand mental health survey. Wellington, New Zealand: Ministry of Health.
• Posadzki, P., Choi, J., Soo Lee, M., & Ernst, E. (2014). Yoga for addictions: A systematic review of randomised clinical trails. Focus on Alternative and Complementary Therapies, 19(1), 1-8.
• Sarkar, S., & Mohit, V. (2016). Yoga and substance use disorders: A narrative review. Asian Journal of Psychiatry, 25, 191-196.
• Streeter, C., Jensen, E., Perlmutter, R., Cabral, H., Tian, H., Terhune, D., . . . Renshaw, P. (2007). Yoga asana sessions increase brain GABA levels: A pilot study. The Journal of Alternative and Complmentary Medicine, 13(4), 419-426.
• Vanderplasschen, W., Colpaert, K., Autrique, M., Rapp, R., Pearce, S., Broekaert, E., & Vanderveld, S. (2013). Therapeutic communities for addictions: A review of their effectiveness from a recovery-orientated perspective. (V. D. Shioiri, Ed.) Scientific World Journal, 2013(427817).
• Vedamurthachar, A., Janahiramaiah, N., Hegde, J., Shetty, T., Subbakrishna, D., Sureshbabu, S., & Gangadhar, B. (2006). Antidepressant efficacy and hormonal effects of Sudarshana Kriya Yoga (SKY) in alcohol dependent individuals. Journal of Affective Disorders, 94, 249-253. 16

Ka Kite Ano Au I A KoutouThank you all for listening
Any questions?
Presentation, speech notes, full paper, and research proposal, all made available via email.
17