Embed Size (px)
Citation preview

Smallpox gone
Measles within
the next 10-15
years
The eradication of
measles infection
will increase child
mortality in
Africa
1Fra CDC public health images
Peter Aaby
Christine S Benn
Bandim

The eradication scenario• The ultimate dream in Public health: eradication
• Measles targetted within next 10-15 years
• Polio targetted within next 5-10 years
• Rubella may be targetted with measles
• To quote Gates: Smallpox gone; Polio 99% down; Measles deaths 98% down => Vaccines best buy in Global Health
2
Global Health
• Removing/reducing vaccinations and reduced outbreak control makes eradication efforts cost-effective
• This is clearly beneficial: Saving lives and money ................ .in the current paradigm where the only effect of vaccinations is to prevent against specific diseases
• What will happen if vaccines have other effects?

Measles eradication
• The immediate consequences:
1. WHO recommendations: The age of measles vaccination (MV) will be increased from 9 to 12 months – as in Latin America in 1996 when measles was eliminated.
2. It will become increasingly difficult to maintain
3
2. It will become increasingly difficult to maintain funding for MV activities
3. The supplementary immunisation activities (SIA) campaigns will be removed to save money
4. DTP/Penta/PCV is likely to be the last vaccinations to profile the immune system

Before-after measles vaccination (MV): Annual mortality rates in African community studies
6%
8%
10%
12%
14%Before
After
4
0%
2%
4%
6%
Bissau 6-35 mo Bandafassi 9-60 mo,
Senegal
Zaire 7-21 mo
Bissau: MV at 6 mo introduced 1979 – 3-fold reductionMeasles infection may have caused 10-20% of deaths!=> A beneficial effect unrelated to measles prevention

Reduction in mortality associated with MV and the
% deaths due to measles infection in unvaccinated children
405060708090
100
RCT
5
01020304050
Bss
au II
IB
issa
u IVSen
egal
Ban
glad
esh
Buru
ndiB
issa
u VB
issa
u VI
Bis
sau V
IIB
issa
u VII
IH
aiti
Ben
inSudan
+ Measles % Acute measles deaths
Not explained by prevention of acute (or delayed) measles infection!
Could it be selection bias?

Randomised/blind studies:
Measles vaccinated vs unvaccinated children
Design Control
group
Mortality (deaths/children) Mortality ratio
(MV+/MV-)Measles
Vaccinated
Not measles
vaccinated
Nigeria: Random, not
blind – 18 month
DTP 0%(0/26) 12%(3/27) 0.00 (0.0-2.5)
6
blind – 18 month
follow-up
0.00 (0.0-2.5)
Sudan: Random, not
blind – 5-9 months
Meningo-
coccal A+C
0.3%(1/340) 3.5%(6/170) 0.09 (0.0-0.7)
Bissau: Blind, not
random
2-years follow-up
Ineffective
measles
vaccine
5%(6/124) 13%(7/53) 0.32 (0.1-0.9)
Bissau: Random, not
blind – 3 months
during war
Inactivated
polio (IPV)
2%(4/211) 5%(11/222) 0.30 (0.1-0.9)

Surv
ival pro
babili
ty
EZ M
Control M
Control F
0.7
0.8
0.9
1.0
High-titre measles vaccine (HTMV), Bissau, 1986-90
7
Age (months)
Surv
ival pro
babili
ty
4 6 12 18 24 30 36 42 48 54
EZ F
0
0.6
0.7
Similar results in Senegal, Sudan and Haiti – HTMV withdrawn 1992
No explanation –but repeatable. How can an effective vaccine do this?

Introduction of DTP: Rural areas of Guinea-Bissau 1984-87
Surv
ival pro
babili
ty
0.96
0.98
1.00
DTP –
(N=868)
Children aged 2-8 moFollowed 6 mo
Unvaccinated: travelling; sick; days without vaccines
8
Follow-up (months)
Surv
ival pro
babili
ty
0 1 2 3 4 5 6
0.90
0.92
0.94 DTP +
DTP+ / DTP- 1.98 (1.03-3.8)
(N=967)
Diphtheria-Tetanus-Pertussis (DTP) effect strongest for girls

0
1
2
3
4
5
6
Cum
ula
ted M
ort
alit
y (
%)
0 1 2 3 4 5 6 7Age (months)
Early DTP
No early DTP
Females
0
1
2
3
4
5
6
Cu
mu
late
d M
ort
alit
y (
%)
0 1 2 3 4 5 6 7Age (months)
Early DTP
No early DTP
Males
Accumulated mortality curves for DTP-vaccinated vs no DTP at 2 months
9
355 356 353 304 11No early DTP (N=359)650 655 620 538 19Early DTP (N=668)
Number at risk
Age (months)
250 248 244 212 5No early DTP (N=256)524 531 498 418 14Early DTP (N=534)
Number at risk
Age (months)
DTP/noDTP MRR crude MRR adjusted
Girls 2.5 (0.9-6.5) 5.7 (2.1-16)
Boys 0.5 (0.2-1.2) 1.3 (0.5-3.1)
All 2.6 (1.4-5.1)

HTMV and DTP?
30
40
50
60
Nu
mb
er
of
de
ath
s
15
20
25
30
35
40
Nu
mb
er o
f d
eath
s
Girls
Boys
No DTP after HTMV DTP/IPV after HTMV
10
0
10
20
Senegal
HT
Senegal
routine
Bissau Gambia Sudan Congo
Nu
mb
er
of
de
ath
s
0
5
10
Senegal
HT
Senegal
Routine
Bissau Gambia Sudan
F/M ratio: 0.96 (0.7-1.3) F/M ratio: 1.93(1.3-2.8)
HTMV withdrawn for the wrong reason
Not RCT – but this ”proves” a causal biological process

Annual mortality in MV trials depending
on DTP status at enrolment
Study Girls Boys
No
DTP3
DTP3
< MV
MR No
DTP3
DTP3
< MV
MR
2-dose 7.5% 3.8% 1.97(1.0-3.7) 6.4% 6.0% 1.06(0.6-1.9)
11
2-dose
Bissau
7.5% 3.8% 1.97(1.0-3.7) 6.4% 6.0% 1.06(0.6-1.9)
Sudan 6.0% 2.8% 2.16(0.3-17.3) 1.4% 1.9% 0.71(0.1-7.9)
Congo 10.0% 2.8% 3.06(0.6-16.1) 10.6% 5.1% 2.06(0.5-9.22)
Total 2.10(1.2-3.7) 1.13(0.7-1.9)
DTP after measles vaccine associated with 2 fold higher mortality

40
60
80
10
0M
ort
alit
y r
ate
(p
er
10
00
ye
ars
)
Guinea-Bissau 1992-94
40
60
80
Mort
alit
y r
ate
(per
1000 y
ears
)
Gambia 1998-2002
What can be done to reduce the negative effect of DTP?
12
02
04
0M
ort
alit
y r
ate
(p
er
10
00
ye
ars
)
0 3 6 9 12 15 18 21 24 27 30 33 36Age (months)
Male Female
Bandwidth: 4 months0
20
Mort
alit
y r
ate
(per
1000 y
ears
)
0 3 6 9 12 15 18 21 24 27 30 33 36Age (months)
Male Female
Bandwidth 4 months
Increased female mortality in the age groups of DTP => Change the immunological profile with a live vaccine =>
RCT: Early Measles Vaccine at 4½ m

Testing non-specific effects of MV
Birth
BCGDTP/OPV
1 2 3 MV
36 mo9 mo6 10 14 weeks
Follow-upOPV
4½ mo
MV vs No vac
13
• Recruitment 2003-2007 – Follow-up to 2009
• 6,600 randomised to A) Edmonston-Zagreb (EZ) at 4½+9
mo, or B+C) no vaccine at 4½ mo and EZ MV or Schwarz
MV at 9 mo
• DTP3 four weeks before enrolment – to prevent the
problem of DTP after MV
• Study designed to test a 25% difference in mortality

RCT of two doses of Measles Vaccine
34
56
7accum
ula
ted m
ort
alit
y (
%)
Two-dose MV
One-dose MV
Children born before June 2004
34
56
7accum
ula
ted m
ort
alit
y (
%)
Two-dose MV
One-dose MV
Children born after June 2004
14
Two-dose standard MV at 4½ and 9 mo was fully protective and
reduced mortality with 50% - with 45% if measles was excluded
MRR=0.48 (0.26-0.87)
P-value=0.02
01
2accum
ula
ted m
ort
alit
y (
%)
750 660 594One-dose405 377 334Two-dose
Number at risk
0 1 2 3Age in Years
MRR=0.53 (0.28-1.00)
P-value=0.050
12accum
ula
ted m
ort
alit
y (
%)
1184 1062 940One-dose599 541 485Two-dose
Number at risk
0 1 2 3Age in Years
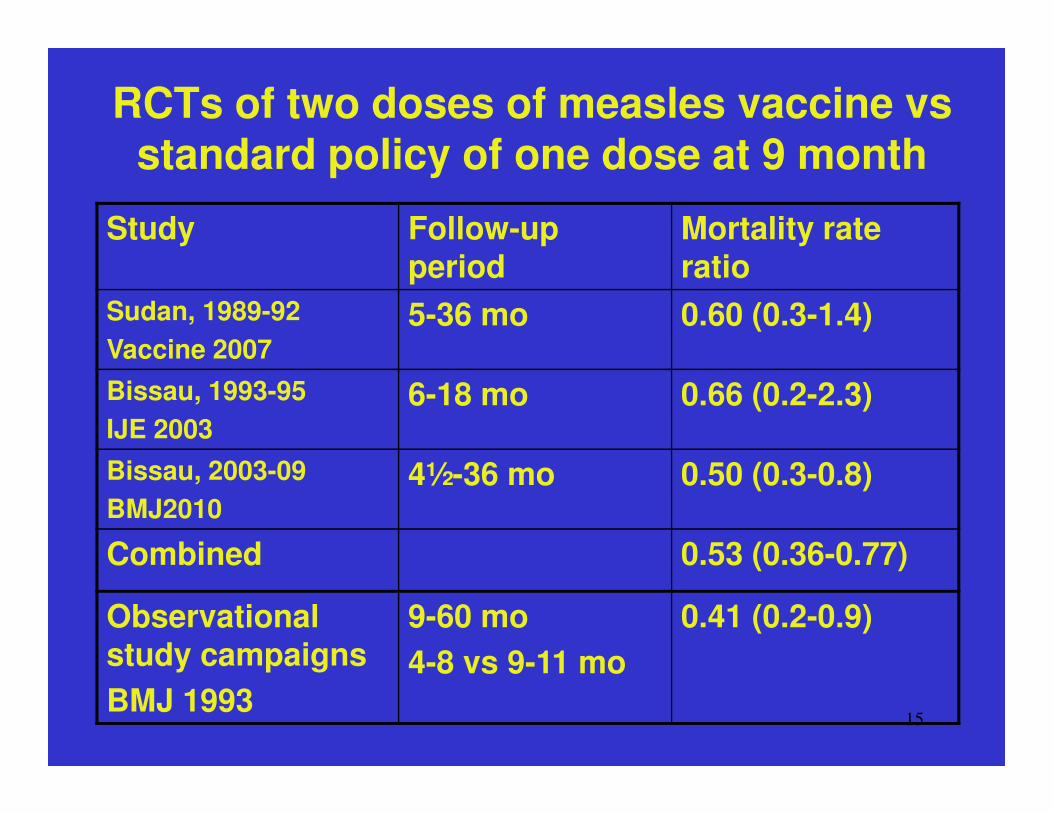
RCTs of two doses of measles vaccine vs standard policy of one dose at 9 month
Study Follow-up period
Mortality rate ratio
Sudan, 1989-92
Vaccine 2007
5-36 mo 0.60 (0.3-1.4)
Bissau, 1993-95 6-18 mo 0.66 (0.2-2.3)
15
IJE 2003
6-18 mo 0.66 (0.2-2.3)
Bissau, 2003-09
BMJ2010
4½-36 mo 0.50 (0.3-0.8)
Combined 0.53 (0.36-0.77)
Observational study campaigns
BMJ 1993
9-60 mo
4-8 vs 9-11 mo
0.41 (0.2-0.9)

Measles eradication I: age of MV from 9 to 12 months
and DTP becomes the last vaccination
0
1
2
3
4
5
6
Cu
mu
late
d M
ort
alit
y (
%)
Early DTP
No early DTP
Females
20
40
60
80
Mort
alit
y r
ate
(per
1000 y
ears
)
Gambia 1998-2002
16
0
355 356 353 304 11No early DTP (N=359)650 655 620 538 19Early DTP (N=668)
Number at risk
0 1 2 3 4 5 6 7Age (months)
0
0 3 6 9 12 15 18 21 24 27 30 33 36Age (months)
Male Female
Bandwidth 4 months
Instead of moving the age foreward as done in Bissau it will be
moved backwards => increased mortality, particularly for girls

Measles eradication II: Campaigns will be removed
200
250
300
350
400
Death
s p
er
1000 liv
e b
irth
sMV
MV MV
BCG
17
050
100
150
200
Death
s p
er
1000 liv
e b
irth
s
1980 1985 1990 1995 2000 20052007Year
Under-5 mortality in Bandim 1978-2007

Polio eradication
• The immediate consequences:
1. Change from OPV to IPV for fear of OPV related polio
cases and revision of OPV strains
2. Removal of OPV
Evidence:
18
1. OPV may have beneficial effects in natural experiments:
The hospital case fatality was 3-fold lower when DTP was
absent and only OPV given
Mortality lower among those who received OPV in campaign
2. OPV beneficial effects in RCT (ínterim results)
3. IPV associated with 52% (2-128%) higher female than
male mortality in RCT

Smallpox and vaccinia eradication
• The first example of eradication of a disease
(1977) and removal of a vaccine (1980)
• Due to the fear of what could happen when
measles was eradicated we started in 1998 to
examine what happened after the removal vaccinia
19
examine what happened after the removal vaccinia
1. In Bissau: we made scar surveys and
followed for mortality
2. In Copenhagen: We used school
health cards which had vaccination information
and could link to Danish health registers

Su
rviv
al p
rob
ab
ility
0.4
0.6
0.8
1.0
Live vaccines are good – what happens when removed? Vaccinia after smallpox eradication in Guinea-Bissau
Vaccinia+
20
Age (years)
Su
rviv
al p
rob
ab
ility
25 30 40 50 60 70 80 90 100
0.0
0.2
1
2
Mortality rate ratio for Scar/no scar: Study I (1998-2002) 0.60 (0.4-0.9); F 0.51(0.3-0.8); M 0.72(0.4-1.2)Study II (2003-5) 0.22 (0.1-0.6): F 0.19(0.1-0.6); M 0.40(0.0-3.7)
Protection against HIV for scar/no scar: Female: 46% (0-71%)
No vaccinia

Smallpox and BCG phased out between 1965-1976 in DenmarkWe used Copenhagen school health cards with information on vaccinations to link with Danish health registers
BCGBCG reduced lymphomas with 51%(7-74%)
Live vaccines are good – what happens when removed? Vaccinia after smallpox eradication in Denmark
21
BCG reduced lymphomas with 51%(7-74%) Vaccine 2009
Smallpox vaccineAsthma reduced with 45% (0-70%) – J Allergy Clin Imm 2003Hospitalisation for inf diseases reduced with 16% (2-28%) IJE 2011
BCG and smallpox vaccineReduced the risk of hospitalization for HIV-infection by 65% (12-86%)

1
1.5
2
2.5
3
3.5
Mo
rta
lity
Ra
tio
* ** *
**
* *
The eradication of measles will lead to DTP
being the last vaccination in childhood
22
0
0.5
BMJ 2000 Benin Bissau-war DTP
introduction
Hospital
fatality
Malawi
BCG DTP Measles V
Mo
rta
lity
Ra
tio
* Significant difference between DTP and BCG or between DTP and MV

MV at 4+9mo vs No vac(DTP3)+MV at 9mo
1
1.5
2
2.5
3
3.5
4
MV 4+9 mo
DTP3+MV 9 mo
0.33(0.1-0.9)
0.56(0.3-0.9)
0.50(0.3-0.8)
Mortality
rate
23
0
0.5
1
4-8 mo 9-36 mo 4-36 mo
Having DTP as last vaccinationThe only RCT suggests 3-fold higher mortality in infancy for DTP =>Globally this would mean 100,000s of children every year

The eradication scenario:What can be done?
• Global health’s eradication strategy is contradicted by all data
• INDEPTH sites are in best situation to resolve these contradictions: are there or are there not non-specific beneficial effects of vaccines
• Polio - OPV
– Test IPV vs OPV in RCT
– Document effect of OPV campaigns –
• Maybe have a phased implementation of a trial
– Gradual phasing out of OPV
24
– Gradual phasing out of OPV
• Measles vaccine
– Test 12 mo vs 9 mo in RCT
– Document effect of MV campaigns (SIA) of children aged 9-60 months
• Maybe phased implementation
• Comparison of effects above and below 9 months
– Gradual change in age of vaccination or phasing out
• Smallpox vaccine
– More surveys

Su
rviv
al p
rob
ab
ility
4 6 12 18 24 30 36 42 48 54
EZ M
EZ F
Control M
Control F
0
0.6
0.7
0.8
0.9
1.0
High-titre measles vaccine: 2-fold higher female mortality
Surv
ival pro
babili
ty
6 12 18 24 30 36 42 48 54 60
EZ M
EZ F
Con M
Con F
0
0.80
0.85
0.90
0.95
1.00
SENEGAL 1987-92, EZ-HTBISSAU 1986-90, EZ-HT
25
Age (months)
Lessons from high-titre measles vaccine (HTMV) trials:
• EZ HTMV was fully protective against measles => negative non-specific effect• Sex-differential effect
• Public health effects: 35% excess mortality from 4 to 60 months => at least ½ mill
annual deaths in Africa
WHO introduced HTMV 1989 and withdrew it in 1992 =>
Interpretation: Too much of a good thing => Major donors: Money for new vaccines!
=> We looked for important NSEs of other vaccines
Age (months)

MV at 4+9mo vs No vac(DTP3)+MV at 9mo by Vitamin A-at-birth status
0.8
1
1.2
1.4
1.6
1.8
2
MV 4+9 mo
DTP3+MV 9 mo
0.98(0.6-1.5) 0.34(0.2-0.7)Mortality
rate
26
0
0.2
0.4
0.6
0.8
Vitamin A Placebo
DTP3+MV 9 mo
P=0.012
Vitamin A may have a fundamental impact on the NSEs=> Only those who did not receive VAS-at-birth

Non-specific effects (NSE) of standard MV at 4½ and 9 months of age:
General reduction in childhood mortality
27
childhood mortality
• Vaccines stimulate the immune system affecting susceptibility
• The NSE are often more important than specific effects
• Vaccination programmes should take the NSE into consideration: age at vaccination,
number of vaccinations, sequence of vaccinations
• Reconsider assumptions –
•Focus: specific diseases or immune deviations
•Effects may differ for boys and girls
•Interventions interact
• INDEPTH in a unique position to pursue these problems
• => EU is (hopefully) going to fund a multicentre trial of early MV

Impact of preventing measles infection:
Reduction in mortality with or without measles
cases in the survival analysis
405060708090
100
%
28
010203040
BIS
SAU
III
BIS
SAU
IVSE
NE
GA
LB
AN
GL
AB
UR
UN
DI
BIS
SAU
VB
ISSA
U V
IB
ISSA
U V
IIB
ISSA
U V
III
SUD
AN
+ Measles - Measles
%
Hypothesis: Non-specific beneficial immunestimulation








![RRA - Who is at risk fo measles in the EU/EEA? May 2019 · measles eradication is biologically, technically and operationally feasible ’ [12, 13]. Eradication is defined as the](https://img.pdfslide.net/doc/110x75/5f38968f4ac9d57de80024bf/rra-who-is-at-risk-fo-measles-in-the-eueea-may-2019-measles-eradication-is-biologically.jpg)