Embed Size (px)
Citation preview

The European experience with protocol biopsies
Ian Roberts
Oxford, UK
Oxford Pathology
Should protocol biopsies be part of routine patient monitoring?
What is the evidence from the European experience of protocol biopsies?
How does this differ from the American, Asian and Australian experience?
How relevant is published data from elsewhere in the world to European practice?
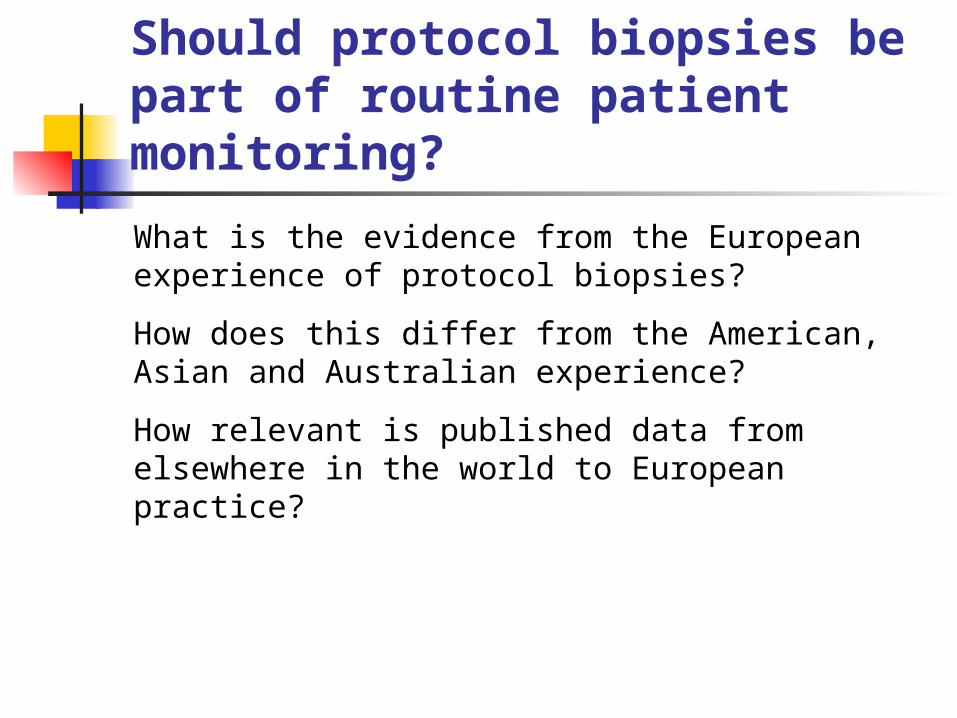
Should protocol biopsies be part of routine patient monitoring?
Protocol biopsies = allograft biopsies performed at pre-determined time points, irrespective of graft dysfunction.
Functions: graft selection, donor disease, baseline for post-transplant pathology, subclinical rejection, early diagnosis and quantification of chronic allograft nephropathy.
Risk
morbidity associated with allograft biopsy
Benefit
information that can be acted on to improve graft outcome
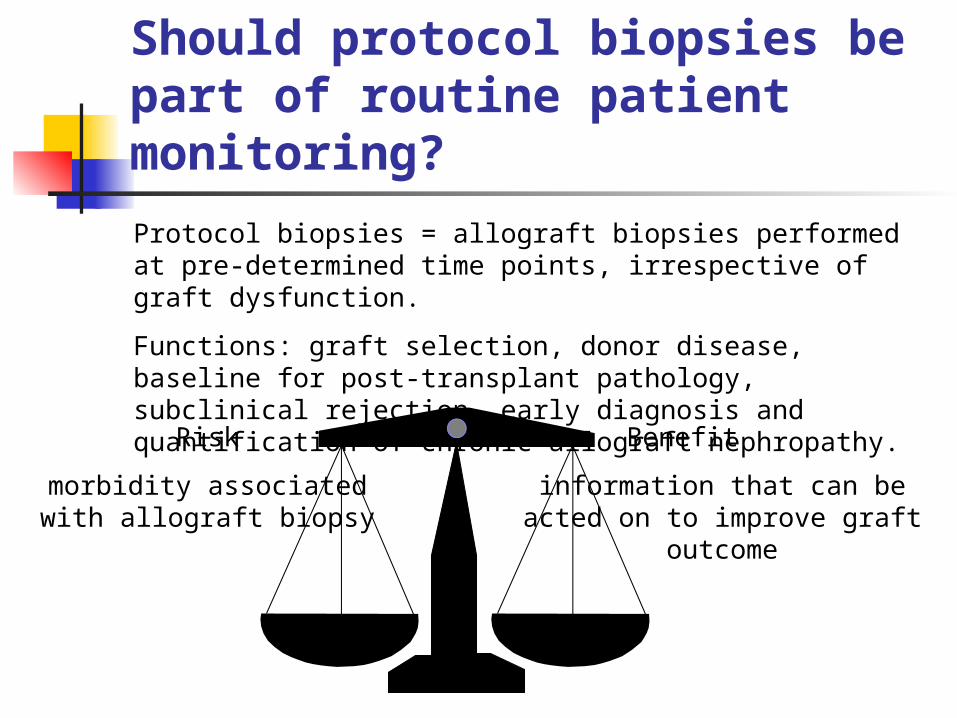
Impact of disease in the donor kidney: implantation biopsies
Biopsies of donor kidneys:
210 transplants, 129 no GS, 81 showed 1-60% GS
No GS >20% GS
GFR at 1 year 62 36
5 year graft survival 80% 35%
Escofet et al. Transplantation 2003;75:344-6
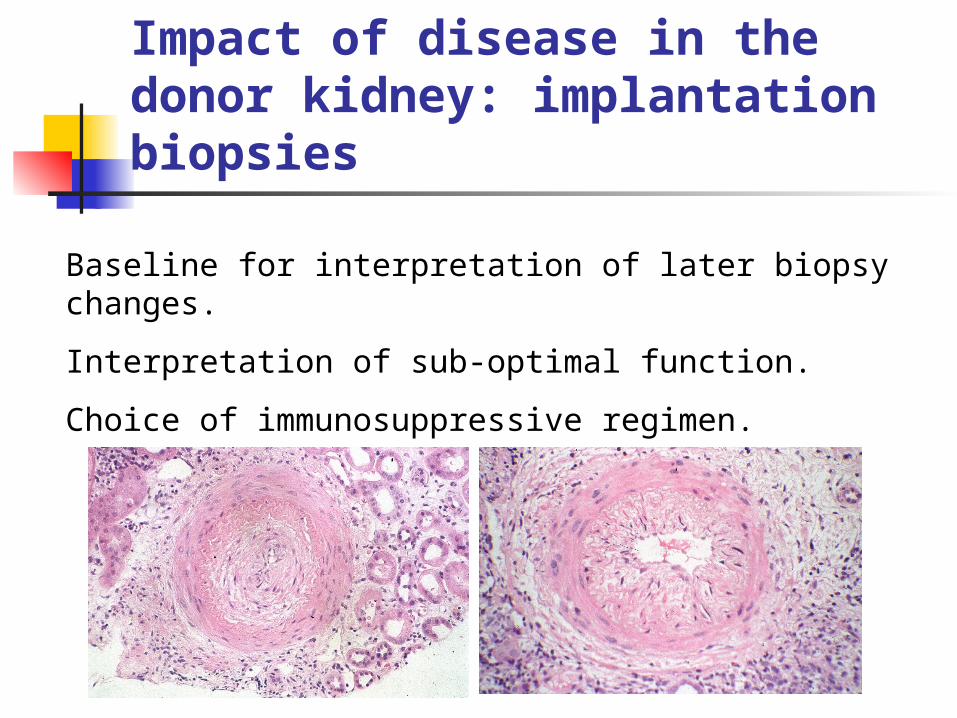
Baseline for interpretation of later biopsy changes.
Interpretation of sub-optimal function.
Choice of immunosuppressive regimen.
Impact of disease in the donor kidney: implantation biopsies

What level of risk is associated with protocol biopsies?
Retrospective audit of 2127 protocol biopsies audited for complications
No deaths
One graft loss
3 episodes of haemorrhage requiring intervention.
3 further patients requiring transfusion.
2 episodes of peritonitis
Furness et al. Transplantation 2003;76:969-73
What determines the potential benefit of protocol biopsies?
For protocol biopsies performed to diagnose subclinical rejection, the likelihood of benefit to an individual patient is a product of:
Frequency of subclinical rejection at the time of protocol biopsy in the patient population
X
The increased graft longevity to be gained from treating the subclinical rejection
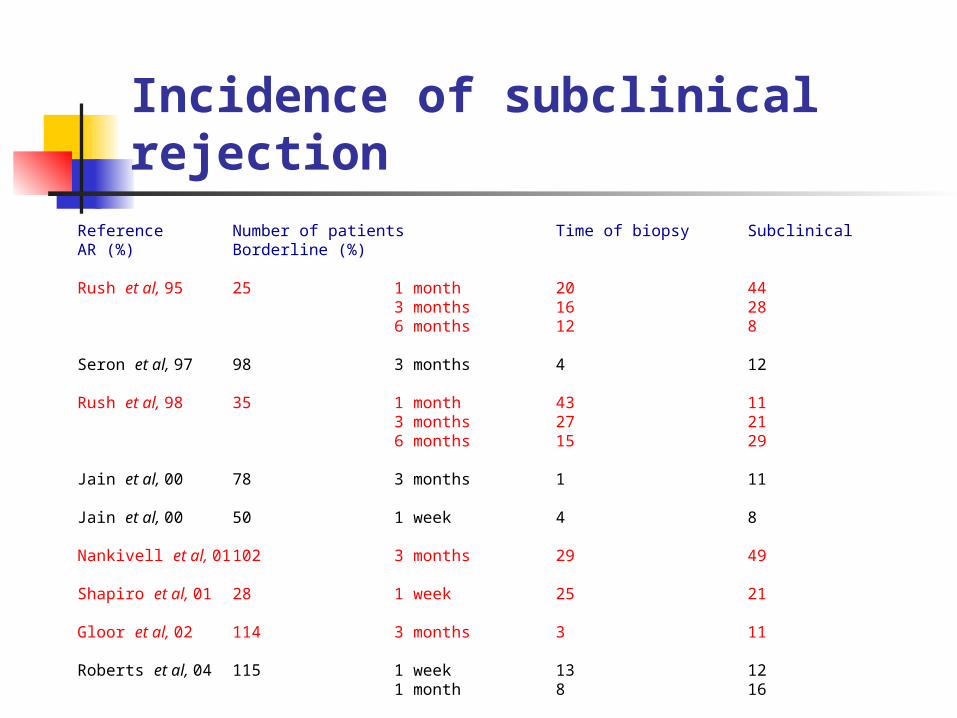
Incidence of subclinical rejectionReference Number of patients Time of biopsy Subclinical AR (%) Borderline (%)
Rush et al, 95 25 1 month 20 443 months 16 286 months 12 8
Seron et al, 97 98 3 months 4 12
Rush et al, 98 35 1 month 43 113 months 27 216 months 15 29
Jain et al, 00 78 3 months 1 11
Jain et al, 00 50 1 week 4 8
Nankivell et al, 01 102 3 months 29 49
Shapiro et al, 01 28 1 week 25 21
Gloor et al, 02 114 3 months 3 11
Roberts et al, 04 115 1 week 13 121 month 8 16
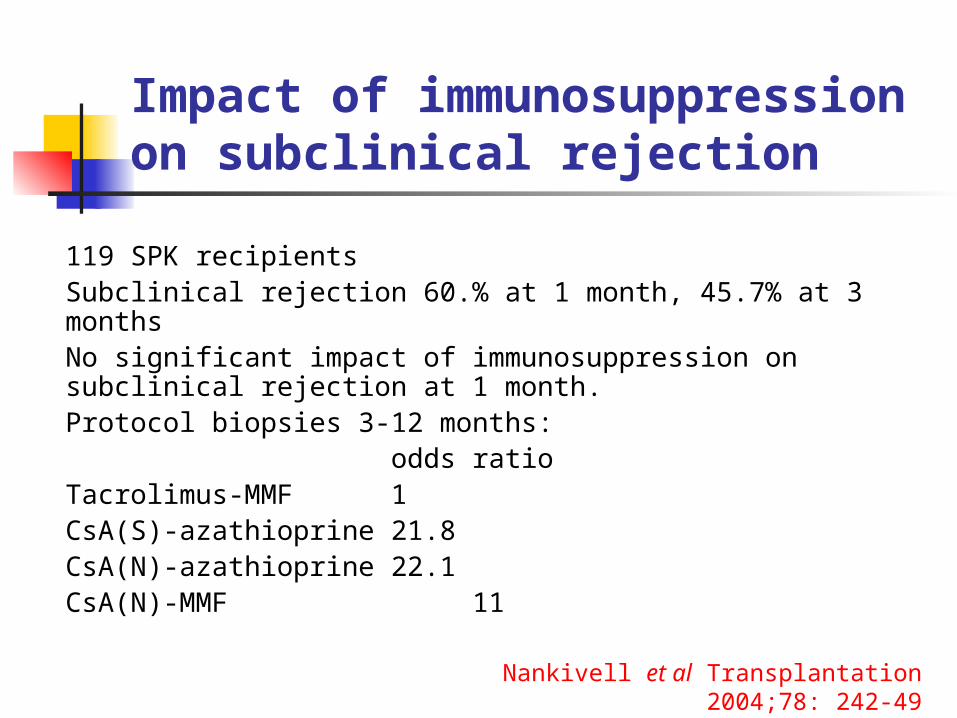
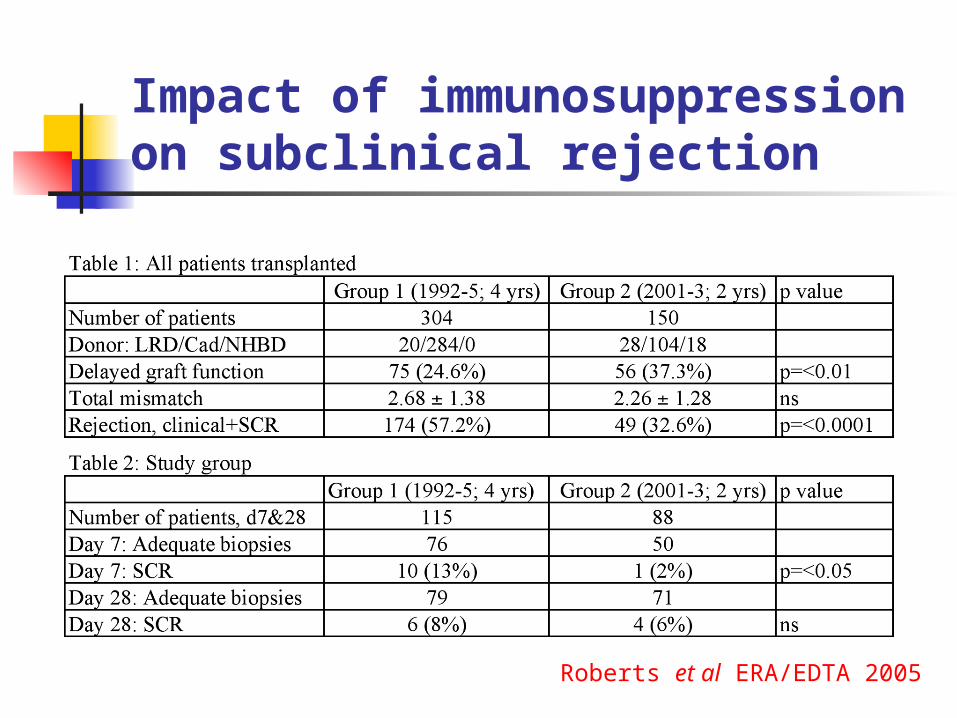
Impact of immunosuppression on subclinical rejection
119 SPK recipientsSubclinical rejection 60.% at 1 month, 45.7% at 3 monthsNo significant impact of immunosuppression on subclinical rejection at 1 month.Protocol biopsies 3-12 months:
odds ratioTacrolimus-MMF 1CsA(S)-azathioprine 21.8CsA(N)-azathioprine 22.1CsA(N)-MMF 11
Nankivell et al Transplantation 2004;78: 242-49

Impact of immunosuppression on subclinical rejection
Case-control study 98 patientsTacrolimus-MMF-prednisolone vs CsA-MMF-prednisolone4 months protocol biopsies scored using Banff 97:
Acute score Chronic scoreTacrolimus 0.61 ± 1.01 1.57 ± 1.97CsA 1.26 ± 1.45 1.51 ± 1.59
p=0.0115 p=ns
Relative risk of acute inflammation with Tacrolimus 0.3 (CI 0.11-0.84)
Moreso et al Transplantation 2004;78: 1064-8

Impact of immunosuppression on subclinical rejection
Roberts et al ERA/EDTA 2005
Comparison of subclinical rejection in two eras:
Group 1 (1992-5) received CsA, azathioprine and prednisolone
Group 2 (2001-3) stratified at transplantation according to immunological ris:
High risk: basiliximab induction, tacrolimus, MMF & pred
Medium risk: CsA, MMF & pred
Low risk: CsA, azathioprine & pred
Impact of immunosuppression on subclinical rejection
Roberts et al ERA/EDTA 2005
The incidence of early SCR is less than it appears
SCR = histological changes meeting recognised criteria for acute rejection in patients with good, stable graft function.
but this also applies to pre-clinical and post-clinical rejections.
True SCR = immune-mediated graft injury, not associated with acute graft dysfunction if untreated.
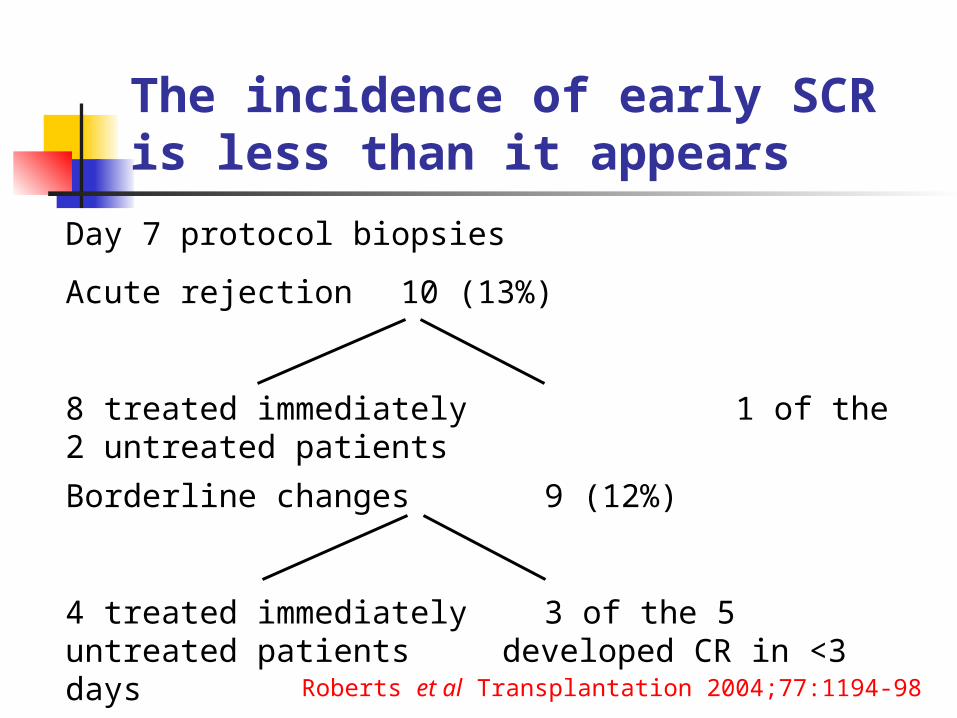
Day 7 protocol biopsies
Acute rejection 10 (13%)
8 treated immediately 1 of the 2 untreated patientsdeveloped CR in <3 days
Borderline changes 9 (12%)
4 treated immediately 3 of the 5 untreated patientsdeveloped CR in <3 days
Roberts et al Transplantation 2004;77:1194-98
The incidence of early SCR is less than it appears

Day 28 protocol biopsy
10/13 patients who had subclinical borderline changes had been treated for acute rejection in the previous 3 weeks
Roberts et al. Transplantation 2004;77:1194-98
Protocol biopsies 10 days after treatment of clinical acute rejection.
Over 25% of patients with full clinical response to anti-rejection therapy have persistent histological signs of rejection. Mazzucchi et al. Transplantation 1999;67:430-34
The incidence of early SCR is less than it appears
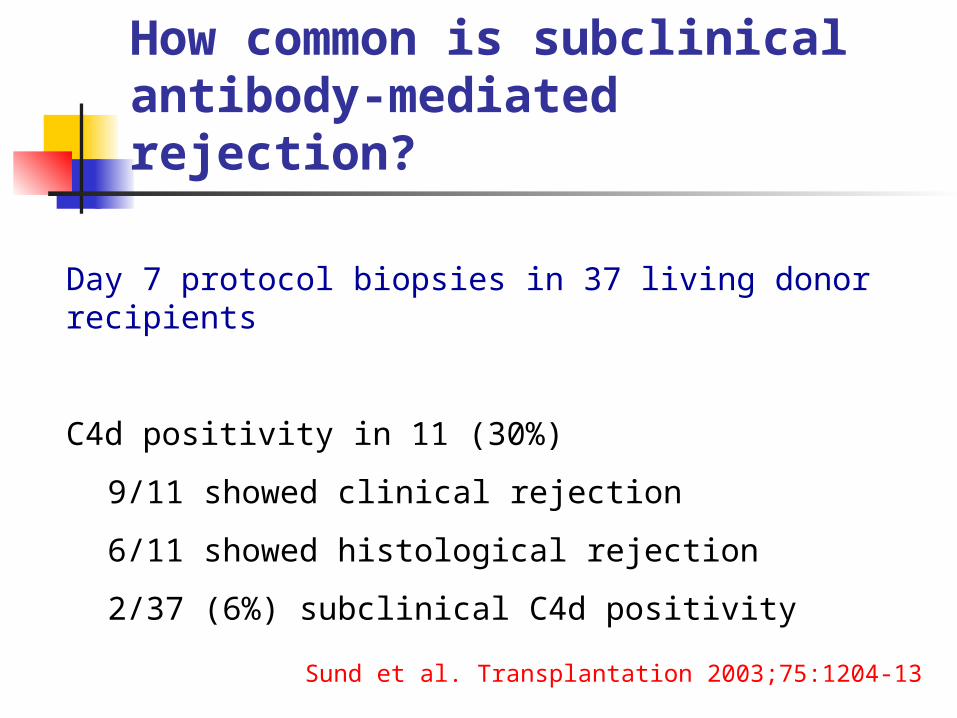
Day 7 protocol biopsies in 37 living donor recipients
C4d positivity in 11 (30%)
9/11 showed clinical rejection
6/11 showed histological rejection
2/37 (6%) subclinical C4d positivity
Sund et al. Transplantation 2003;75:1204-13
How common is subclinical antibody-mediated rejection?
Koo et al. Transplantation 2004;78:398-403
How common is subclinical antibody-mediated rejection?
48 day 7 protocol biopsies (Cad/LRD 41/7)
C4d positivity in 6 (13%)
5/6 showed clinical and histological rejection
all 5 with rejection had post-transplant DRA
One patient C4d positive, no histological rejection, no circulating alloantibodies, stable graft function (ie. doesn’t meet Banff criteria for humoral rejection) - never treated for rejection, sCr 104 micromol/L at 3 months
How common is subclinical antibody-mediated rejection?
Multicentre study, 551 protocol biopsies
Diffuse C4d positivity in 2%
Focal C4d positivity in 2.4%
Inter-centre variation reflecting variable numbers of pre-sensitised patients.
Subclinical C4d positivity had no significant impact on graft outcome.
Mengel et al. Am J Transplant 2005;5:1050-56

How common is subclinical antibody-mediated rejection?
Does subclinical C4d positivity equate to subclinical antibody-mediated rejection?
C4d positivity not due to antibody deposition (false positive).
Accommodation?
120 recipients of kidney-pancreas grafts
Protocol biopsies at 1 & 2 weeks, 1, 3, 6 & 12 months, annually thereafter. 70% of patients suffered clinical or SCR/borderline changes in first 3 months.
Patients with acute SCR in first 3 months showed higher grades of CAN in subsequent biopsies than did patients with no SCR (2.48 ±0.25 vs 0.32 ±0.09).
But: 3 month risk of SCR was increased by a previous episode of severe rejection (hazard ratio 2.46), no data on treatment of SCR.
Nankivell et al. N Engl J Med 2003;349:2326-33
Does early SCR contribute to chronic graft injury?

Day 28 protocol biopsies:
19 patients with subclinical rejection or borderline changes.
4 treated immediately, 3 for clinical rejection within one week.
12 never subsequently received treatment for rejection:
1 late graft failure at 6 years post-transplantation
2 patients died with functioning grafts (sCr 159 & 168)
9 had functioning grafts at 6 years
median sCr 119 umol/l (range 90-185)Roberts et al Transplantation 2004;77:1194-98
Does early SCR contribute to chronic graft injury?
72 patients randomised to protocol biopsies 1, 2, 3, 6 and 12 months vs 6 and 12 months only.
In the biopsy group, 80% of 1 month biopsies showed either acute rejection or borderline changes.
Sub-clinical rejection treated.
Early biopsy group had less chronic damage in 6 month biopsies and lower serum creatinine at 2 years than controls.
Rush et al. J Am Soc Nephrol 1998;9:2129-34
Does treatment of SCR improve graft outcome?
Protocol biopsies and the early diagnosis of CAN
Rationale: Renal scarring on histology is an earlier/more sensitive marker of chronic damage than is serum creatinine/GFR - by the time renal function deteriorates, it’s too late.
Assumptions:
1. Early histological evidence of chronic damage predicts chronic graft failure.
2. Intervention in patients with good renal function but CAN on biopsy can prevent/limit progression.
Problems:
1. Sampling error: subcapsular scar, vessel disease
2. Stable chronic damage
Protocol biopsies and the early diagnosis of CAN

How common is early CAN?
41 patients (10 HLA identical LRD, 31 cadaveric donor kidneys).
Protocol biopsies at 3 months and 2 years.
No CAN in recipients of HLA identical kidneys.
Cadaveric kidneys: 3 months 2 years
CAN 25% 50%
grade I 7 10
grade II 1 5
CAN correlates with donor age
Legendre et al. Transplantation 1998;65:1506-09
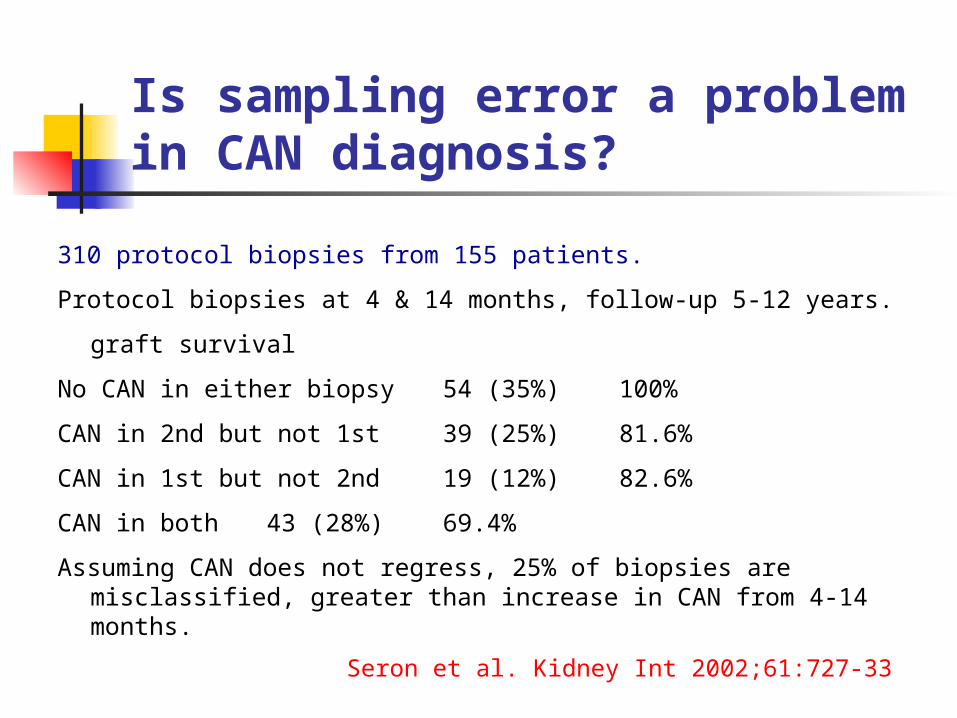
Is sampling error a problem in CAN diagnosis?
310 protocol biopsies from 155 patients.
Protocol biopsies at 4 & 14 months, follow-up 5-12 years.
graft survival
No CAN in either biopsy 54 (35%) 100%
CAN in 2nd but not 1st 39 (25%) 81.6%
CAN in 1st but not 2nd 19 (12%) 82.6%
CAN in both 43 (28%) 69.4%
Assuming CAN does not regress, 25% of biopsies are misclassified, greater than increase in CAN from 4-14 months.
Seron et al. Kidney Int 2002;61:727-33
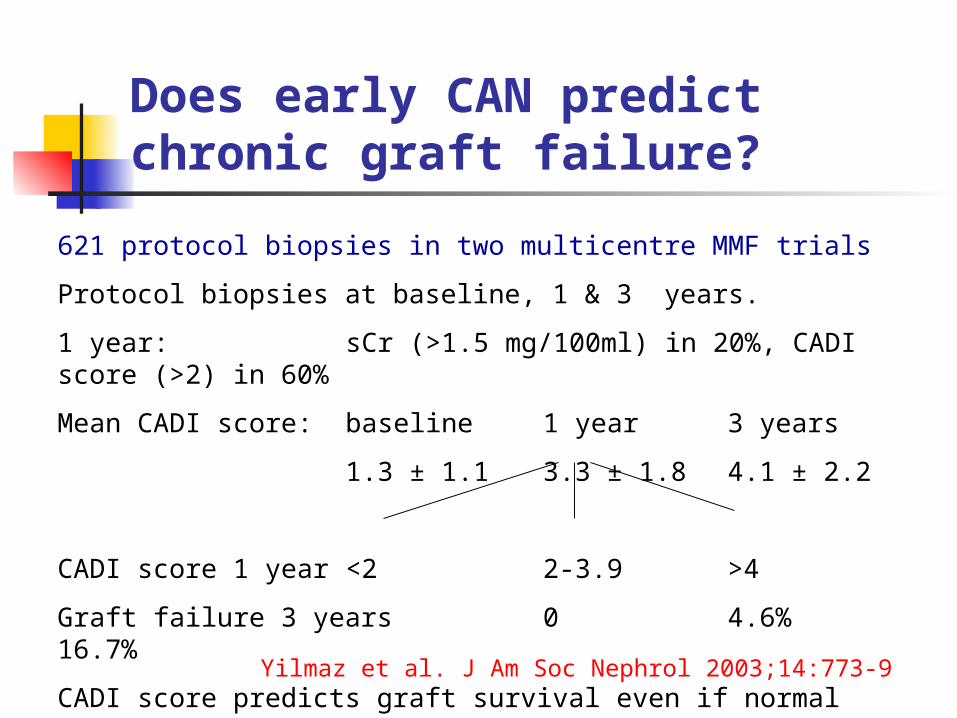
Does early CAN predict chronic graft failure?
621 protocol biopsies in two multicentre MMF trials
Protocol biopsies at baseline, 1 & 3 years.
1 year: sCr (>1.5 mg/100ml) in 20%, CADI score (>2) in 60%
Mean CADI score: baseline 1 year 3 years
1.3 ± 1.1 3.3 ± 1.8 4.1 ± 2.2
CADI score 1 year <2 2-3.9 >4
Graft failure 3 years 0 4.6% 16.7%
CADI score predicts graft survival even if normal renal functionYilmaz et al. J Am Soc Nephrol 2003;14:773-9
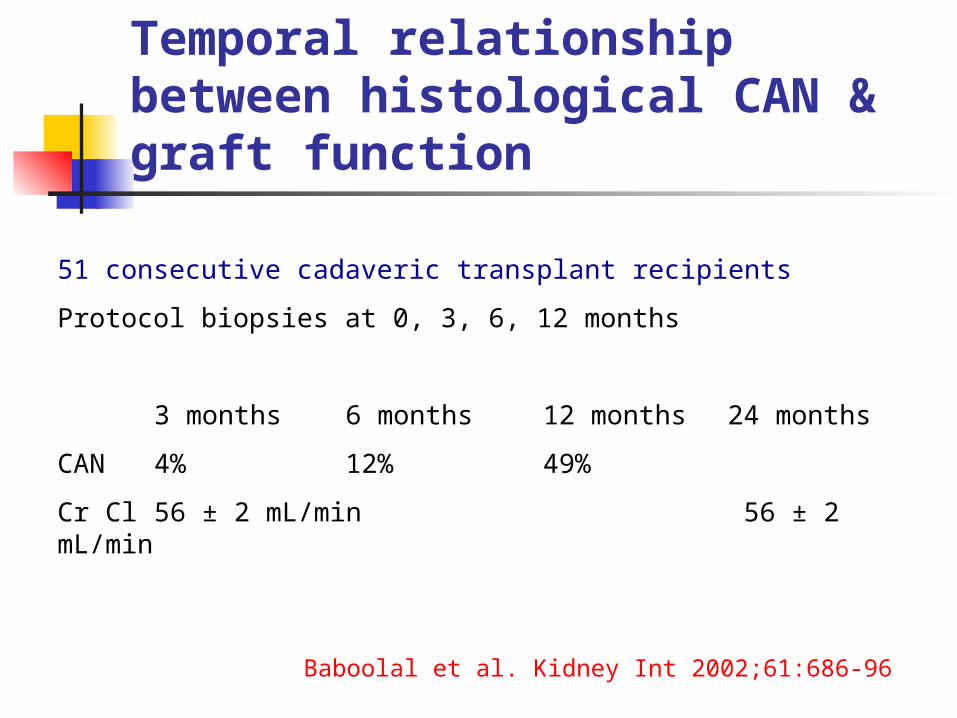
51 consecutive cadaveric transplant recipients
Protocol biopsies at 0, 3, 6, 12 months
3 months 6 months 12 months 24 months
CAN 4% 12% 49%
Cr Cl 56 ± 2 mL/min 56 ± 2 mL/min
Baboolal et al. Kidney Int 2002;61:686-96
Temporal relationship between histological CAN & graft function
Does early CAN predict chronic graft failure?
57 living donor transplants
Protocol biopsy at day 0 (n=57), 1 week (n=43) & 1 year (n=33)
Poor correlation between arteriosclerosis in day 0 and 1 week biopsies (sampling error).
Glomerulosclerosis, interstitial fibrosis and tubular atrophy, but not arteriosclerosis, increased from baseline to 1 year.
Extent of chronic tubulointerstitial damage in 1 year biopsies, but not baseline biopsies, correlated with sCr at 1 & 3 years.
Best predictor of renal function at 3 years was sCr at 1 year.
Sund et al. Nephrol Dial Transplant 1999;14:2445-54

258 patients
Protocol biopsies at 6, 12 and 26 weeks
In multivariate analysis, CAN in biopsy 3 (n=70) predicted by:CAN in biopsy 2Lower GFR at biopsy 2NephrocalcinosisAcute rejection
Renal functional decline preceded morphological changes of CAN
Schwarz et al 2005;67:341-48
Temporal relationship between histological CAN & graft function
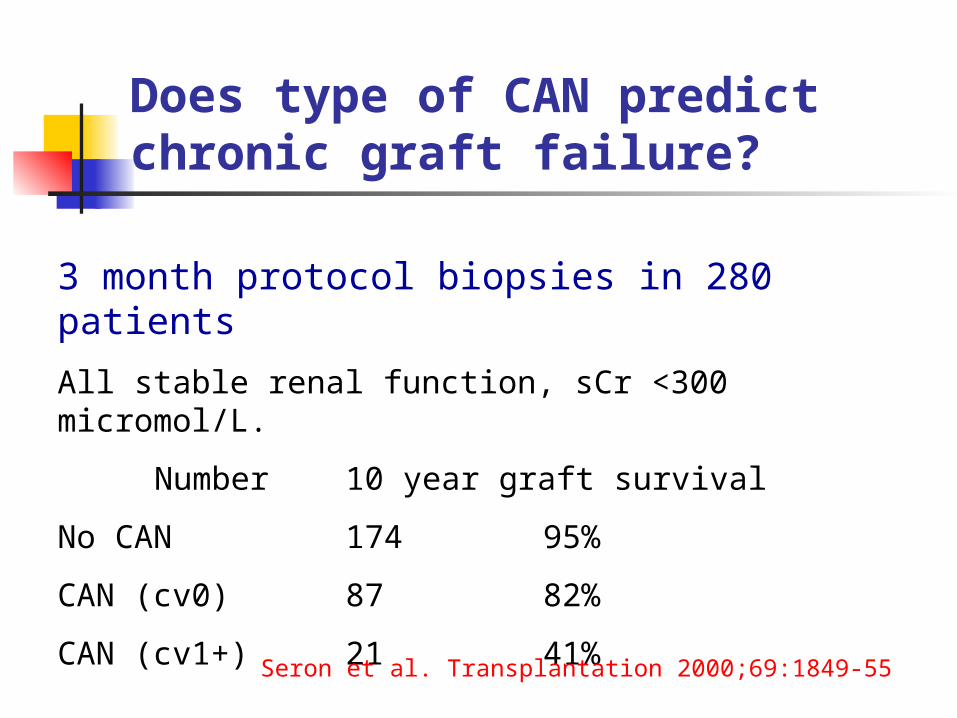
Does type of CAN predict chronic graft failure?
3 month protocol biopsies in 280 patients
All stable renal function, sCr <300 micromol/L.
Number 10 year graft survival
No CAN 174 95%
CAN (cv0) 87 82%
CAN (cv1+) 21 41%
Seron et al. Transplantation 2000;69:1849-55
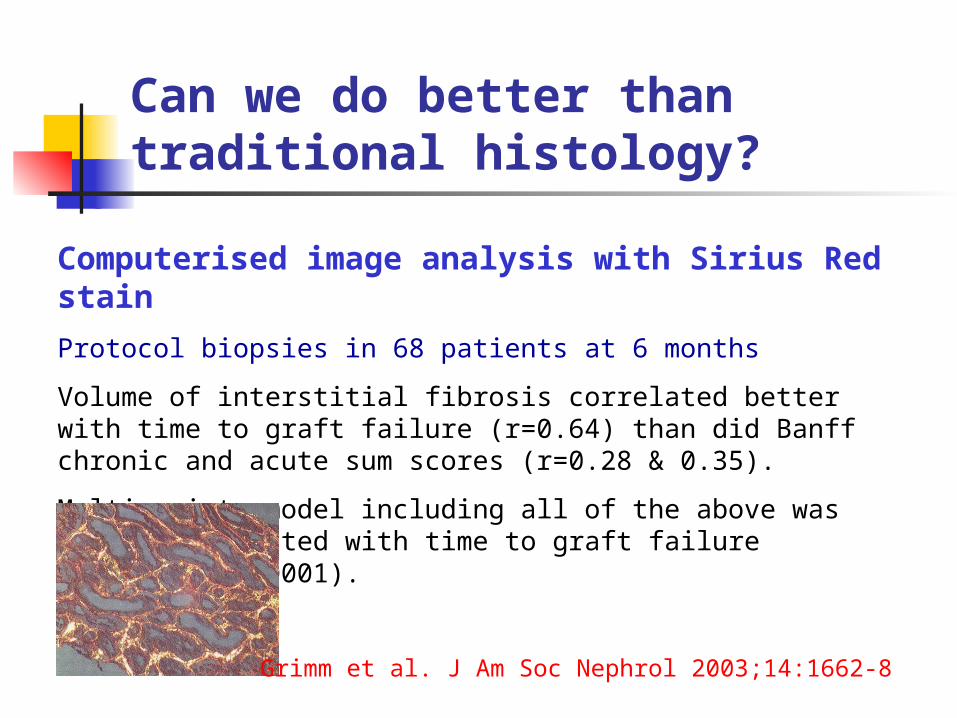
Can we do better than traditional histology?
Computerised image analysis with Sirius Red stain
Protocol biopsies in 68 patients at 6 months
Volume of interstitial fibrosis correlated better with time to graft failure (r=0.64) than did Banff chronic and acute sum scores (r=0.28 & 0.35).
Multivariate model including all of the above was highly correlated with time to graft failure (r=0.7, p=<0.0001).
Grimm et al. J Am Soc Nephrol 2003;14:1662-8
Can we do better than traditional histology?
TGF-beta
Protocol biopsies in 40 patients at day 0, 1 wk, 6 mnths
IF for active TGF-beta & semiquantitative scanning laser confocal microscopy.
active TGF-beta from day 0 to 1 wk to 6 mnths (p<0.0001)
DGF TGF-beta, but no association with acute rejection or IS drug (CsA vs Tac).
No correlation between TGF-beta expression at any timepoint and isotope GFR at 12 months.
Jain et al. Transplant Int 2002;15:630-4
Can we do better than traditional histology?
Other techniques with potential:
computerised morphometry combined with IH for:
type III collagen
tenascin
smooth muscle actin
Can we do better than traditional histology?
Sund et al. Nephrol Dial Transplant 2004;19:2838-45
Computerised image analysis (Sirius red) vs Banff scoring
Protocol biopsies in 33 patients at day 0, 1 year
Sirius red (Vint) correlates with Banff chronic score r=0.439, p=0.0003
1 year biopsies:
Banff chronic score correlated with 8-10 year sCr, p=0.01, and with late graft loss, p=0.0445
Sirius red (Vint) showed similar trend but did not reach statistical significance

Can we do better than traditional histology?
Other techniques with potential:
quantification of mast cells
Roberts et al. J Clin Pathol 2000;53:858-62

Can we do better than traditional histology?
Other techniques with potential:
quantification of mast cells
Biopsy diagnosis Mast cells/mm2 of cortexMedian (interquartile range)
p value (Mann-Whitney U)
Acute rejection, subsequentlyprogressing to chronic
3.0 (1.9-5.1)
Acute rejection, notprogressing to chronic
2.7 (1.0-5.3) acute vs chronic rejection<0.0001
Chronic rejection 27.1 (20.7-29.8)
Acute CsA toxicity 2.0 (1.3-2.5) acute vs chronic CsAtoxicity <0.0001
Chronic CsA toxicity 10.6 (7.2-21.3)
Roberts et al. J Clin Pathol 2000;53:858-62
CAN as a predictor of graft outcome
CAN alone is not a useful label.
What matters is:
1. Progression of CAN - need at least 2 biopsies
2. Type of CAN - cv lesions most significant
3. Severity of CAN - quantitative image analysis better than Banff scoring
4. Immune activity

Does intervention in subclinical CAN make a difference?
Assumption 2:
Intervention in patients with good, stable renal function but CAN on biopsy can prevent/limit progression.
Evidence?
Would you change immunosuppression in a patient with good stable graft function on the basis of some minor chronic changes in the biopsy?
Should protocol biopsies be part of routine patient management?
Baseline biopsies: yes - useful in the interpretation of subsequent pathology.
Post-transplantation: maybe, but must be clear on why they are being performed and have a protocol for acting on the results of the biopsies.
Subclinical rejection: overall benefit depends on the frequency of SCR in the unit. The benefit of treating SCR remains unproven.
Early CAN: a good early surrogate marker for graft survival in clinical trials. Relevance to management of individual patients unclear.