Embed Size (px)
Citation preview

J A C C : C A S E R E P O R T S VO L . 2 , N O . 3 , 2 0 2 0
ª 2 0 2 0 T H E A U T H O R S . P U B L I S H E D B Y E L S E V I E R O N B E H A L F O F T H E A M E R I C A N
C O L L E G E O F C A R D I O L O G Y F OU N D A T I O N . T H I S I S A N O P E N A C C E S S A R T I C L E U N D E R
T H E C C B Y - N C - N D L I C E N S E ( h t t p : / / c r e a t i v e c o mm o n s . o r g / l i c e n s e s / b y - n c - n d / 4 . 0 / ) .
MINI-FOCUS ISSUE ON CARDIOMYOPATHIES AND GENETIC COUNSELING
EDITORIAL COMMENT
The Ever-Expanding Landscapeof Cardiomyopathies
Babken Asatryan, MD, PHD,a Frank I. Marcus, MDbT he second half of the 20th century saw theemergence of a disease entity, referred to ascardiomyopathies: a group of myocardial dis-
eases associated with a risk of heart failure and sud-den death. The curiosity and dedication of manyminds to uncover this collection of conditions led tosignificant progress in the recognition of the clinicaland pathological features of cardiomyopathies.Initially, this was manifest as a predominantly post-mortem diagnosis. Subsequently, the clinical recogni-tion of the cardiomyopathies has evolved over time.In 1990, the first myopathic disease due to a pointmutation in the b-myosin heavy chain gene was iden-tified in a French-Canadian family with hypertrophiccardiomyopathy (HCM) (1,2). This finding initiated anew era of cardiomyopathy research, extending thecare from individual patients to entire families.
With the advent of next-generation geneticsequencing and multimodality cardiac imaging, thephenotype spectrum and genetic architecture of the 3main cardiomyopathies, dilated cardiomyopathy(DCM), HCM, and arrhythmogenic right ventricularcardiomyopathy (ARVC) (Figure 1), are increasinglyrecognized and clinically relevant genotype-phenotype-risk associations have become evident.Patients with DCM, characterized by idiopathic left
ISSN 2666-0849
From the aDepartment of Cardiology, Inselspital, Bern University
Hospital, University of Bern, Bern, Switzerland; and the bSarver Heart
Center, University of Arizona, Tucson, Arizona. The authors have re-
ported that they have no relationships relevant to the contents of this
paper to disclose.
The authors attest they are in compliance with human studies commit-
tees and animal welfare regulations of the authors’ institutions and Food
and Drug Administration guidelines, or patient consent where appro-
priate. For more information, visit the JACC: Case Reports author
instructions page.
ventricular or biventricular dysfunction and dilata-tion often present in the third to fifth decade of lifewith mild symptoms (3,4). Patients with DCMfrequently have ventricular arrhythmias and 30% diesuddenly (5). Although ventricular arrhythmias weretraditionally thought to occur at a later stage of thedisease in DCM with symptomatic heart failure,recent evidence has indicated that certain geneticforms are significantly arrhythmogenic even duringthe early course of the disease (6–8). Beyond thewidely recognized lamin A/C (LMNA), mutations ingenes encoding filamin C (FLNC), desmoplakin(DSP), phospholamban (PLN), and RNA bindingmotif protein 20 (RBM20) have been associated witha substantial risk of life-threatening ventricular ar-rhythmias despite only mild ventricular dysfunction(8–11). Mutations in the titin gene (TTN), the mostprevalent genetic substrate of DCM, are associatedwith a high incidence of ventricular arrhythmiasand particular susceptibility to environmentalstressors, such as viral infection, immune response,and toxic exposure (12). Genetic risk stratificationhelps in decision-making for the need of implant-able cardioverter-defibrillator therapy. However,present knowledge of the genetic background ex-plains only approximately 30% to 35% of DCMcases, hindering the precision care of many patientsand families (13).
HCM often has a silent course. Nevertheless, asizeable proportion of patients present with angina,dyspnea, palpitations, syncope, or sudden cardiacdeath (SCD). In hypertrophic obstructive cardiomy-opathy, nearly 70% of all deaths are sudden (14).Mutations in the b-myosin heavy chain gene, MYH7,result in an earlier and more severe phenotype thanother HCM forms (15). Patients with sarcomeric genemutations are diagnosed at a younger age and have a
https://doi.org/10.1016/j.jaccas.2020.02.006

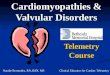
FIGURE 1 The Clinical and Genetic Characteristics of Hypertrophic, Dilated, and Arrhythmogenic Cardiomyopathies
*In the presence of family history of HCM, left ventricular wall thickness of $13 mm is diagnostic for HCM. CCB ¼ calcium channel blocker; CMR ¼ cardiac magnetic
resonance imaging; CRT-P/D ¼ cardiac resynchronization therapy pacemaker/ defibrillator; CT ¼ computed tomography; DHP ¼ dihydropyridine;
ECG ¼ electrocardiogram; EMB ¼ endomyocardial biopsy; FHx ¼ family history; HCM ¼ hypertrophic cardiomyopathy; HF ¼ heart failure; HOCM ¼ hypertrophic
obstructive cardiomyopathy; ICD ¼ implantable cardioverter-defibrillator; LGE ¼ late gadolinium enhancement; LV ¼ left ventricle; LVEF ¼ left ventricular ejection
fraction; LVH ¼ left ventricular hypertrophy; LVOTO ¼ left ventricular outflow tract obstruction; NSVT ¼ nonsustained ventricular tachycardia; PVC ¼ premature
ventricular contraction; RVEF ¼ right ventricular ejection fraction; SAECG ¼ single averaged electrocardiogram; SCA ¼ sudden cardiac arrest; SCD ¼ sudden cardiac
death; TWI ¼ T-wave inversion; VF ¼ ventricular fibrillation; VT ¼ ventricular tachycardia.
Asatryan and Marcus J A C C : C A S E R E P O R T S , V O L . 2 , N O . 3 , 2 0 2 0
The Expanding Landscape of Cardiomyopathies M A R C H 2 0 2 0 : 3 6 1 – 4
362

SEE PAGE 365, 372, 378, AND 384
J A C C : C A S E R E P O R T S , V O L . 2 , N O . 3 , 2 0 2 0 Asatryan and MarcusM A R C H 2 0 2 0 : 3 6 1 – 4 The Expanding Landscape of Cardiomyopathies
363
higher rate of familial SCD (16,17). The risk stratifica-tion in patients with HCM is based on a predictionmodel, which quantifies the risk of life-threateningarrhythmias during the following 5 years based onclinical variables (18). However, precision treatmentof patients with HCM is only in its early days. Drugsthat alter the myofilament calcium sensitivity andcalcium homeostasis such as blebbistatin, diltiazem,and ranolazine, modifiers of myocardial energeticsubstrates, inhibitors of mitogen-activated proteinkinase and mammalian target of rapamycin path-ways, as well as genome editing and gene transfertechnologies are currently under investigation andmay enable precision therapy for treatment of HCM inthe near future.
ARVC is genetic heart disease with a progressivecourse and a risk of SCD. In the advanced stages, it ischaracterized histopathologically by necrosis andfibrofatty replacement of the right ventricularmyocardium, which may lead to progressive heartfailure and increased susceptibility to SCD (19).However, ARVC may be manifest with life-threatening ventricular arrhythmias before thedevelopment of clinical structural heart disease (19).Due to its variable phenotype, there is no single goldstandard for the diagnosis of ARVC. Therefore, theTask Force diagnostic criteria were proposed in 1994,and then revised in 2010 to improve the sensitivitybut maintaining diagnostic specificity (19). During thepast decade, ARVC has been increasingly recognizedas a biventricular disease with involvement of the leftventricle to a lesser extent. Also, left-dominant formsof disease have been reported. These observationshave resulted in a broader term, arrhythmogeniccardiomyopathy, to reflect the spectrum of arrhyth-mogenic cardiomyopathies (20). Recently, a predic-tion model has been proposed to stratify the risk oflife-threatening arrhythmias in patients with ARVC,and tailor the therapy according to an individual pa-tient’s needs (21).
Most cardiomyopathies are not rare and are oftenseen by cardiologists, molecular geneticists, and pa-thologists. Because the phenotype in cardiomyopa-thies appears to be influenced by a variety of geneticand environmental factors, it is not uncommon to befaced with both a diagnostic and challenging thera-peutic situation in patients with cardiomyopathies.The ultimate need for improved care of patientsmandates the reporting of such rare experiences incase reports or case series to enable the transfer ofknowledge between clinical specialists.
For the purpose of promoting the understanding,recognition, and precision management ofpatients with cardiomyopathies, JACC: Case Reportslaunched this issue on inherited cardiomyopathies.Carreras-Mora et al. (22) describe a case of cardiogenicshock caused by right ventricular Takotsubo syn-drome. The authors emphasize the importance ofrecognizing this rare condition because patients withshock might benefit more from phosphodiesterase-3inhibitors than treatment with dobutamine, whichcan exacerbate the condition. Binder et al. (23)describe a new mutation in the FHL1 gene, whichsegregated with a phenotype of HCM, neuromusculardisease, and/or SCD, and underscore the implicationsof FHL1 screening in patients and families with HCM.Gi et al. (24) report a large atrial myxoma in a patientwith apical HCM. Concomitant occurrence of myxomaand HCM is characterized in LEOPARD syndrome, arare multiple congenital anomaly predominantly
affecting the skin, face, and heart. The authors haveexcluded LEOPARD syndrome because of the absenceof extracardiac manifestations. Based on this patientand the previous 6 reports of atrial myxoma in pa-tients with HCM, the authors raise the hypothesis thatthere may be a link between the 2 conditions,particularly based on the shared pathogenetic acti-vation of RAS/MASK pathway in LEOPARD syndromeand HCM, and the fact that RAS is the most commononcogene in humans. Ali et al. (25) describe a case of apatient with hypertrophic obstructive cardiomyopa-thy and accompanying aortic valve stenosis. In thispatient, percutaneous coronary intervention in theproximal left-anterior descending coronary artery,associated with occlusion of the first septal coronaryartery, resulted in substantial reduction in the leftventricular outflow tract gradient and improvementin the left ventricular function. These observationsillustrate the expanding spectrum of cardiomyopa-thies. The evolving knowledge of the genetics,mechanisms of disease, and determinants of pheno-type in cardiomyopathies will result in better riskstratification and improve the outcome in patientswith cardiomyopathy.
ADDRESS FOR CORRESPONDENCE: Dr. BabkenAsatryan, Department of Cardiology, Inselspital, BernUniversity Hospital, Freiburgstrasse 10, 3010 Bern,Switzerland. E-mail: [email protected].

Asatryan and Marcus J A C C : C A S E R E P O R T S , V O L . 2 , N O . 3 , 2 0 2 0
The Expanding Landscape of Cardiomyopathies M A R C H 2 0 2 0 : 3 6 1 – 4
364
RE F E RENCE S
1. Jarcho JA, McKenna W, Pare JA, et al. Mappinga gene for familial hypertrophic cardiomyopathyto chromosome 14q1. N Engl J Med 1989;321:1372–8.
2. Geisterfer-Lowrance AA, Kass S, Tanigawa G,et al. A molecular basis for familial hypertrophiccardiomyopathy: a beta cardiac myosin heavychain gene missense mutation. Cell 1990;62:999–1006.
3. Pinto YM, Elliott PM, Arbustini E, et al. Proposalfor a revised definition of dilated cardiomyopathy,hypokinetic non-dilated cardiomyopathy, and itsimplications for clinical practice: a position state-ment of the ESC working group on myocardial andpericardial diseases. Eur Heart J 2016;37:1850–8.
4. Bozkurt B, Colvin M, Cook J, et al. Currentdiagnostic and treatment strategies for specificdilated cardiomyopathies: a scientific statementfrom the American Heart Association. Circulation2016;134:e579–646.
5. Tamburro P, Wilber D. Sudden death in idio-pathic dilated cardiomyopathy. Am Heart J 1992;124:1035–45.
6. Meune C, Van Berlo JH, Anselme F, Bonne G,Pinto YM, Duboc D. Primary prevention of suddendeath in patients with lamin A/C gene mutations.N Engl J Med 2006;354:209–10.
7. Kumar S, Baldinger SH, Gandjbakhch E, et al.Long-term arrhythmic and nonarrhythmic out-comes of lamin A/C mutation carriers. J Am CollCardiol 2016;68:2299–307.
8. Gigli M, Merlo M, Graw SL, et al. Genetic risk ofarrhythmic phenotypes in patients with dilatedcardiomyopathy. J Am Coll Cardiol 2019;74:1480–90.
9. Ortiz-Genga MF, Cuenca S, Dal Ferro M,et al. Truncating FLNC mutations are associatedwith high-risk dilated and arrhythmogenic car-
diomyopathies. J Am Coll Cardiol 2016;68:2440–51.
10. Tobita T, Nomura S, Fujita T, et al. Geneticbasis of cardiomyopathy and the genotypesinvolved in prognosis and left ventricular reverseremodeling. Sci Rep 2018;8:1998.
11. Parikh VN, Caleshu C, Reuter C, et al. Regionalvariation in RBM20 causes a highly penetrantarrhythmogenic cardiomyopathy. Circ Heart Fail2019;12:e005371.
12. Verdonschot JAJ, Hazebroek MR, Derks KWJ,et al. Titin cardiomyopathy leads to altered mito-chondrial energetics, increased fibrosis and long-term life-threatening arrhythmias. Eur Heart J2018;39:864–73.
13. Sinagra G, Elliott PM, Merlo M. Dilated car-diomyopathy: so many cardiomyopathies! EurHeart J 2019 Dec 23 [E-pub ahead of print].
14. O’Mahony C, Elliott P, McKenna W. Suddencardiac death in hypertrophic cardiomyopathy.Circ Arrhythm Electrophysiol 2013;6:443–51.
15. Sedaghat-Hamedani F, Kayvanpour E,Tugrul OF, et al. Clinical outcomes associated withsarcomere mutations in hypertrophic cardiomy-opathy: a meta-analysis on 7675 individuals. ClinRes Cardiol 2018;107:30–41.
16. Olivotto I, Girolami F, Ackerman MJ, et al.Myofilament protein gene mutation screening andoutcome of patients with hypertrophic cardiomy-opathy. Mayo Clin Proc 2008;83:630–8.
17. Bos JM, Towbin JA, Ackerman MJ. Diagnostic,prognostic, and therapeutic implications of ge-netic testing for hypertrophic cardiomyopathy.J Am Coll Cardiol 2009;54:201–11.
18. Authors/Task Force members, Elliott PM,Anastasakis A, et al. 2014 ESC Guidelines ondiagnosis and management of hypertrophic car-diomyopathy: the Task Force for the Diagnosis and
Management of Hypertrophic Cardiomyopathy ofthe European Society of Cardiology (ESC). EurHeart J 2014;35:2733–79.
19. Marcus FI, McKenna WJ, Sherrill D, et al.Diagnosis of arrhythmogenic right ventricularcardiomyopathy/dysplasia: proposed modificationof the task force criteria. Circulation 2010;121:1533–41.
20. Towbin JA, McKenna WJ, Abrams DJ, et al.2019 HRS expert consensus statement on evalu-ation, risk stratification, and management ofarrhythmogenic cardiomyopathy. Heart Rhythm2019;16:e301–72.
21. Cadrin-Tourigny J, Bosman LP, Nozza A,et al. A new prediction model for ventriculararrhythmias in arrhythmogenic right ventricularcardiomyopathy. Eur Heart J 2019;40:1850–8.
22. Carreras-Mora J, Duran-Cambra A, Vilades-Medel D, et al. An exceptional cause of acute rightheart failure: isolated right ventricular Takotsubosyndrome. J Am Coll Cardiol Case Rep 2020;2:365–9.
23. Binder MS, Brown E, Aversano T, et al. NovelFHL-1 mutation associated with hypertrophic car-diomyopathy, sudden cardiac death, and myop-athy. J Am Coll Cardiol Case Rep 2020;2:372–7.
24. Gi W-T, Sedaghat-Hamedani F, ShirvaniSamani O, et al. Cardiac myxoma in a patient withhypertrophic cardiomyopathy. J Am Coll CardiolCase Rep 2020;2:378–83.
25. Ali RA, Katmeh L, Scheller B, Mahfoud F,Böhm M, Ewen S. Reduction of outflow tractobstruction after PCI to proximal LAD in a patientwith HOCM. J Am Coll Cardiol Case Rep 2020;2:384–8.
KEY WORDS arrhythmia, cardiomyopathy,genetics, precision medicine, sudden cardiac death