Embed Size (px)
Citation preview

The Florida BRITE Project: BRief Intervention and Treatment for Elders
Lawrence Schonfeld, PhDDepartment of Aging & Mental Health
Florida Mental Health InstituteUniversity of South Florida

History of Florida DCF’s Efforts on Substance Abuse among Older Adults
Legislative budget requests 2002 SAMHSA Grant proposal
Screening, Brief Intervention, Referral and Treatment (SBIRT)
Older Adult Workgroup on Substance Abuse
SBIRT concept funded by DCF in 2004 – later renamed as the Florida BRITE Project

Categories of Substance Misuse among Older Adults
Alcohol Abuse – the primary concern for substance abuse
Other substances: Medication Misuse – usually
unintentional misuse; related to patient errors, difficulties with regimen, & prescribing practices
Over-the-Counter (OTCs) medications
Illicit Drugs – an increasing trend?

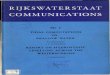
This 2001 report suggests that illicit drug use, binge drinking and heavy drinking among adults ages 55 and older is higher than previously thought.

15
.9
56
.8
37
.8
12
.8
7.8
58
.3
30
.3
7.6
4.9
53
.0
21
.1
5.3
1.0
37
.5
9.4
2.3
0
10
20
30
40
50
60
70
Any IllicitDrug Use
Any AlcoholUse
"Binge"Alcohol use
HeavyAlcohol Use
18 to 25
26 to 34
35 to 54
55 or Older
Percentage of Adults Aged 18 or Older Reporting Past Month Use of Any Illicit Drug or Alcohol by Age Group: 2000. (source NHSDA, 2001)
Per
cen
t R
epo
rtin
g U
se i
n P
ast
Mo
nth
12% of 55+ age group are either binge or heavy alcohol users


Admissions Age 55 or Older by Primary Substance at Admission: 1994-1999
(DASIS Report December 2001)
Primary substances in 1999:
76.1% Alcohol
12.6% Opiates
4.5% Cocaine
1.3% Marijuana
0.7% Sedatives/Tranquilizers
0.6% Stimulants
4.1% Other
Source: 1999 Treatment Episode Data System (TEDS)

Expert panel recommendations for screening and treating the older adult:
SAMHSA/CSAT Treatment Improvement Protocol (TIP) #26

TIP#26 Expert Panel Recommendations
1. Age-specific, group treatment that is supportive, not confrontive.
2. Attend to depression, loneliness; address losses.3. Teach skills to rebuild social support network4. Employ staff experienced in working with elders5. Link with aging, medical, institutional settings6. Content should be age-appropriate and offered at a
slower pace.7. Create a “culture of respect” for older clients8. Broad, holistic approach recognizing age-specific
psychological, social & health aspects.9. Adapt treatment as needed to address gender
issues

Florida’s Elder Population
Total population - about 17 million 22% are age 60 or older Among the adult population ages 18
and older, elders ages 60+ represent 28.5%
However, in 2000, among adults in Florida’s treatment for substance abuse problems, only 2% were ages 60+

The FMHI Model: Relapse prevention, group treatment using cognitive-behavioral interventions and self-management skills
• Gerontology Alcohol Project (1979-1981)• Substance Abuse Program for Elderly (1986-1994)• Replications:
• Chelsea Arbor Older Adult Recovery Center in Ann Arbor, Michigan (1990’s)
• GET SMART Program (West Los Angeles VA Hospital; 2000)
• Older Adult Substance Abuse Treatment Program – Tennessee (2005 - present)
• Zablocki VA Medical Center (Milwaukee, 2006 - present)

The alternative: Brief Intervention
Project GOAL (“Guiding Older Adult Lifestyles”) Fleming et al. (1999) focused on at-risk drinkers age 65+ in community-based primary care received 2 15 minute sessions of brief physician advice.
Health Profiles Project (Blow, Barry, et al.) – the largest randomized trial of brief alcohol advice to at-risk drinkers 60+ (N=454). Provided in-home brief intervention.
Later Used with aging services’ providers: Staying Healthy Project (Cullinane, Blow, Barry, et al.)- Screened 4,300+ older adults in California- 166 people entered randomized trials - 39% decrease in Experimental & 28% in Control
groups’ drinking

The Florida BRITE Projectfunded by the Florida Dept. of Children and Families
BRief Intervention and Treatment for Elders

Broward County Elderly & Veterans Services
Gulf Coast Community
Care
Coastal Behavioral HealthCare
The Florida BRITE ProjectBRief Intervention & Treatment for Elders
Center for Drug Free
Living – added in 2005
Orlando

The Florida BRITE Project - Goals
Implement screening, brief intervention, referral and treatment (SBIRT) relying on CSAT’s Treatment Improvement Protocols (TIP): Substance Abuse & Older Adults TIP #26 Brief Intervention & Brief Therapies TIP #34 CSAT manual: Relapse Prevention for
Older Substance Abusers (Dupree & Schonfeld)
Develop referral networks, screening and services appropriate for older adults in order to reach greater numbers of elders.

The Florida BRITE Project - Goals
Reach more older Floridians than previously served Screen older adults (ages 60+) considered:
At risk for substance misuse, or Demonstrating problems with substances
Reach elders unlikely to be served by “traditional” types of services: Low-income elders Minorities Isolated, withdrawn
Florida BRITE Project must remain flexible! Modified based on formative evaluation, system
changes and needs.

BRITE differs from usual services
• “Non-traditional” substance abuse referral sources to identify hidden abusers
• Screen where elders are more likely to be found or interviewed:• In their own homes• Elder-specific living, centers
• Exemption from Florida’s standard admission and assessment protocols
• Brief Interventions in home or on-site• Brief Treatment if needed (CBT/Self-Mgt.)

The Florida BRITE Project BRITE identifies older adults who misuse or are at
risk for misusing: Alcohol Prescription medications Over-the-counter (OTC) medications Illicit drugs
Depression and suicide risk are also being screened by BRITE providers since: Depression is the most frequent antecedent to
substance abuse in elders Few older adults participate in behavioral health
services Older adults have the highest rate of suicides
among all age-groups.

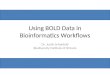
No
Yes
Pre-Screening by Nontraditional and other referral sources
Screening by BRITE Pilot Program
Client screens positive and agrees to be served.
End ScreeningRe-contact at
later date
Admit person for services appropriate to service plan
BriefIntervention
BriefTreatment
Refer to external services as
indicated in plan
Re-screen client prior to discharge
Completion of every six B.T. sessions,
discharge, 30 & 90 days
Re-Assess at Discharge, 30 and 90 days
post discharge
Enter Data & upload to KIT
Enter ScreeningData on Tablet PC &
upload to KIT Solutions
Enter data into ETIPS & upload

Pre-Screening for BRITE
• Prescreening through “traditional” referral sources for substance abuse services may not be appropriate for elders.
• Link with agencies that more likely to serve older adults with problems:
• Aging Services (AAA, County Aging)• Protective services• Visiting Nurses• Geriatric physicians• Assisted living facilities• Mental health centers• Health clinics

Pre-Screening for BRITE
• To date, much of the referral efforts have involved outreach efforts by BRITE providers through:• Presentations at senior housing, health
fairs, other group settings• The more efficient method we are trying to
establish is to build a community agency referral network in which BRITE providers • Identify local aging, social, & healthcare
services who frequently serve elders• Educate these services about BRITE• Develop schedule of regular contact

Screening
BRITE Screening Tool consists of scales that separately address the required domains of alcohol, medications, drugs, depression, suicide risk
Alcohol, Depression screens already valid
All screens in the public domain (no copyright infringement, free to use)
Easy to administer and comprehend
Translated into Spanish for BRITE Project
Includes interviewer’s impressions
Includes questions on substance use history and treatment

Short - Michigan Alcoholism Screening Test - Geriatric Version (SMAST-G)
A 10 item screen Includes risk factors appropriate to
elders YES/NO response format Scoring: 2 or more "YES" responses
are indicative of an alcohol problem.
Source: Frederic C. Blow, Ph.D., University of Michigan Alcohol Research Center, Ann Arbor, MI

S-MAST-G 1. When talking with others, do you ever underestimate how
much you actually drink? 2. After a few drinks, have you sometimes not eaten or been
able to skip a meal because you didn't feel hungry? 3. Does having a few drinks help decrease your shakiness or
tremors? 4. Does alcohol sometimes make it hard for you to remember
parts of the day or night? 5. Do you usually take a drink to relax or calm your nerves? 6. Do you drink to take your mind off your problems? 7. Have you ever increased your drinking after experiencing a
loss in your life? 8. Has a doctor or nurse ever said they were worried or
concerned about your drinking? 9. Have you ever made rules to manage your drinking?10. When you feel lonely, does having a drink help?

Interviewer's impressions of the personafter completing the "Brown Bag Review" ofprescriptions:
1. Does not correctly recall the purpose of one or more medications
2. Reports the wrong dose/amount of one or more medications
3. Takes one or more medications for the wrong reasons or symptoms
4. Needs education and/or assistance on proper medication use
Begin with a “Brown Bag” Review

Medication Misuse High Risk Behaviors?
• Takes more than one type of prescribed medication• Difficulty remembering how many meds to take• Prescriptions from two or more doctors• Felt worse soon after taking meds• Taking meds to help sleep• Uses up meds too fast• Takes meds for nervousness or anxiety• Doctor/nurse expressed concern about use of meds• Take pain relieving meds• Take pills to deal with loneliness, sadness• Saving old medications for future use• Chooses between cost of meds and other necessities• A family member reminds them to take pills• Uses dispenser or other method to help remind• Fails to take meds supposed to• Borrow someone else's meds• Feel groggy after taking certain medications

OTC Medication Use and Misuse - Risks
1. Do you frequently take aspirin, Tylenol, Advil, or other non-prescription pills for pain?
2. Do you ever tell your physician about the type of non-prescription pills you buy?
3. Do you use herbal pills such as Ginkgo, Saw Palmetto, St. John's Wort?
4. Do you take non-prescription pills or remedies for improving your memory?
5. Have you ever felt worse soon after taking over-the counter remedies?
6. Are you taking medications to help you sleep?
7. Do any of the non-prescription pills you take make you feel groggy?
8. Do you use plants or herbs to make your own remedies such as garlic, or aloe?

Drug Use
Use of any of the following in past year:
1. Marijuana?
2. Cocaine?
3. Crack?
4. Heroin?
5. Hallucinogens (such as LSD, PCP)?
6. Substances - sniffed or inhaled?
Recorded by interviewer - YES/NO format. Any YES responses results in a Flag for further assessment.

Short - Geriatric Depression Scale
1. Are you basically satisfied with your life? 2. Have you dropped many of your activities
and interests? 3. Do you feel that your life is empty? 4. Do you often get bored? 5. Are you in good spirits most of the time? 6. Are you afraid that something bad is going to happen to you? 7. Do you feel happy most of the time? 8. Do you often feel helpless? 9. Do you prefer to stay at home, rather than going out and doing new things?10. Do you feel you have more problems with memory than most?11. Do you think it is wonderful to be alive now?12. Do you feel pretty worthless the way you are now?13. Do you feel full of energy?14. Do you feel that your situation is hopeless?15. Do you think that most people are better off than you are?
Scoring:
5-9 = mild to moderate depression
10+ = serious levels of depression

Suicide Risk Items *
1. Has anyone in your family ever committed suicide?
2. If yes, who in your family committed suicide?
3. Have you ever thought about taking your life?
4. How recently have you thought about killing yourself?
5. Do you have a plan for doing this? (response selected from list of plans provided)
6. Have you ever been in the care of psychiatrist, psychologist, or other professional because of severe depression or mental problems?
7. Do you keep firearms in the house?
8. If yes, ask how many guns are in the house?* Adapted from Brown & Bongar (2004) Assessing risk for completed suicide in
elderly patients: Psychologists' views of critical risk factors. Professional Psychology: Research and Practice.

Following Screening
Older adults who screen positive for substance abuse can be offered one of two types of services Brief Intervention
1 to 5 sessions of brief advice, education about substance use
Health Promotion Workbook
Brief Treatment Up to 16 sessions using the Relapse
Prevention Curriculum (CSAT, 2005)

Brief Interventions can be delivered where older adults can be found
In the elder’s home Senior center, congregate meal sites Home Health Care Physician’s office ER’s or Hospital rooms Workplace

Florida BRITE
Health Promotion Workbook
Barry, Oslin, & Blow (1999)
and CSAT TIP #26 (1998)
(modified to include drugs, medications, OTCs, depression and suicide risk)

Resource for Pilot Program
Participants:
Health Promotion Workbook
Workbook Topics: Identify future goals for physical
and emotional health, activities, finances.
Summarize health habits: Exercise, tobacco, alcohol,
nutrition Alcohol use
What is a standard drink Types of older drinkers Consequences of drinking Reasons to quit or cut down Drinking agreement Drinking diary card Handling risky situations Visit summary

Resource for Pilot Program
Participants:
Health Promotion Workbook
Workbook Topics (continued): Medication misuse
Reasons for taking wrong dose
Things to tell your doctor Do’s and Don’ts for taking
medications Potential problems with OTC
Medications
Visit summary

Alternative to Brief Intervention is “Brief Treatment”
BRITE providers have the option to use the 16 session Relapse Prevention curriculum if: The client’s problem requires more
intensity The client requires more sessions The client does not succeed during
Brief Intervention

A Three Stage CBT/Self-Management Treatment Approach
(Dupree & Schonfeld, SAMHSA/CSAT manual, 2005)
1. For each person begin by identifying his/her antecedents and consequences for substance use to create an individualized “substance use behavior chain” using the Substance Abuse Profile for the Elderly
2. Teach the person how to identify the components of that chain so that he or she can understand the high risk situations for alcohol or drug use.
3. Teach specific skills to address these high risk situations to prevent relapse.

Relapse Prevention Curriculum
Each topic is presented as a module, with specific instructions to the leader regarding the theme of the lecture, materials needed, and exercises.
Instructions to the group leader to: prompt discussion among clients use diagrams or visual aids lead rehearsals/role plays provide homework/assignments

Teaching Relapse Prevention Skills
Each topic is presented as a module, with specific instructions to the leader regarding the theme of the lecture, materials needed, and exercises.
Instructions to the group leader to: prompt discussion among clients use diagrams or visual aids lead rehearsals/role plays provide homework/assignments

The Result:A 16-session curriculum manual for conducting brief treatment
(Dupree & Schonfeld, CSAT, 2005)

BRITE – Screenings fromMarch 2004 – October 17th 2006
• 2,945 screened by 4 agencies:• Broward Co. Elderly & Veterans Serv = 1,844• Gulfcoast Community Care (Pinellas) = 512• Coastal Behav. Health Care (Sarasota) = 319• Ctr. for Drug Free living (Orange)* = 270
* began in August 2005
• Most (67%) are identified through BRITE outreach, presentations to the public, visits to senior centers, etc.

Demographics
Living arrangements: 54% alone 20% with spouse 8% in group setting (e.g., ALF)
70% were women Median age = 75 Race
75% Caucasian 18% African American 6% multiracial
Hispanic 15%

Florida BRITE Project Screening:Alcohol Problems
8.4% of those referred to BRITE were for potential alcohol problems
75% of all 2,945 screened were drinkers 17% of drinkers consumed 3 or more
drinks on a drinking day 81% of referrals for alcohol problems and
14% of those referred for other reasons scored 2 or more on the S-MAST-G.
483 clients provided services – mostly brief intervention. Many of these showed other symptoms.

Florida BRITE Project Screening:Prescription Medications
25% were referred for prescription misuse Of this group:
9% reported wrong amount for one or more medication
13% could not recall purpose of one or more medications
20% need education and/or assistance on proper medication use
7% took prescription medications for wrong reasons or symptoms

Florida BRITE Project Screening:
Over-the-Counter Medications
• 8% referred for potential OTC misuse
Illicit Drug Use
< 1% referred to BRITE for illicit drug use

Florida BRITE Project Screening: Depression
67% of all 2,945 were referred for depression
Screening these with the Short-GDS: 24% of those referred had moderate
depression Another 9.6% with serious depression Similar proportions for those not referred
specifically for depression

Florida BRITE Project Screening:Suicide Risk
Only 0.6% referred for suicide risk Yet, 14% of all referrals indicated that
they contemplated suicide at some time 23% of these within the past year

Services Provided based on the limited data entered:
Preliminary Outcomes: Significant improvement in Geriatric
Depression Scores (S-GDS) for 270 of the 273 people screened (p<.001)
Significant improvement in S-MAST-G (alcohol screening) at discharge for 116 people receiving re-screening (p<.001)

The new SBIRT Grant
Screening, Brief Intervention,
Referral and Treatment
(funded by SAMHSA’s Center for Substance Abuse Treatment)

SAMHSA SBIRT Grant Florida was recently awarded a $14 million SBIRT
grant (Oct. 2006- Sept. 2011) Most of the funding goes to direct services
The new funding added to current funding will increase BRITE to a total of 12 sites Additional counties include: Charlotte, Duval,
Hillsborough, Miami-Dade, Palm Beach, and Pasco.
An RFP process will be used for selecting and awarding contracts to providers
The new grant will involve both “generalist” providers (e.g., physicians; aging services) and “specialist” providers (substance abuse treatment agencies).

Conclusions
Best or promising practices and curricula are available, yet few elder-specific programs exist.
Identifying older adults with substance abuse, misuse, or “at-risk” behavior remains a difficult task. Especially true for medication misuse
Depression is often associated with use and misuse among older adults, yet remains a challenge for substance abuse providers.
The new SBIRT Grant received by Florida aims to address many of these issues.