Embed Size (px)
Citation preview
Is it at all possible to separate function from esthet-ics? These days the trend seems to be to presentoral rehabilitations that are highly complex and
supported by various implants or that exhibit esthet-ics that would turn even Mother Nature green withenvy. In this article, I would like to remind the readerof what we originally set out to do—to provide re-placements for missing or damaged teeth. Ulti-mately, we fabricate our dental restorations—toothreplacements—to allow dentists to properly treattheir patients. This article will present a number oftopics related to the functional-esthetic complex.The question of tooth shade will not be discussedhere, as it is too prone to subjective perception.
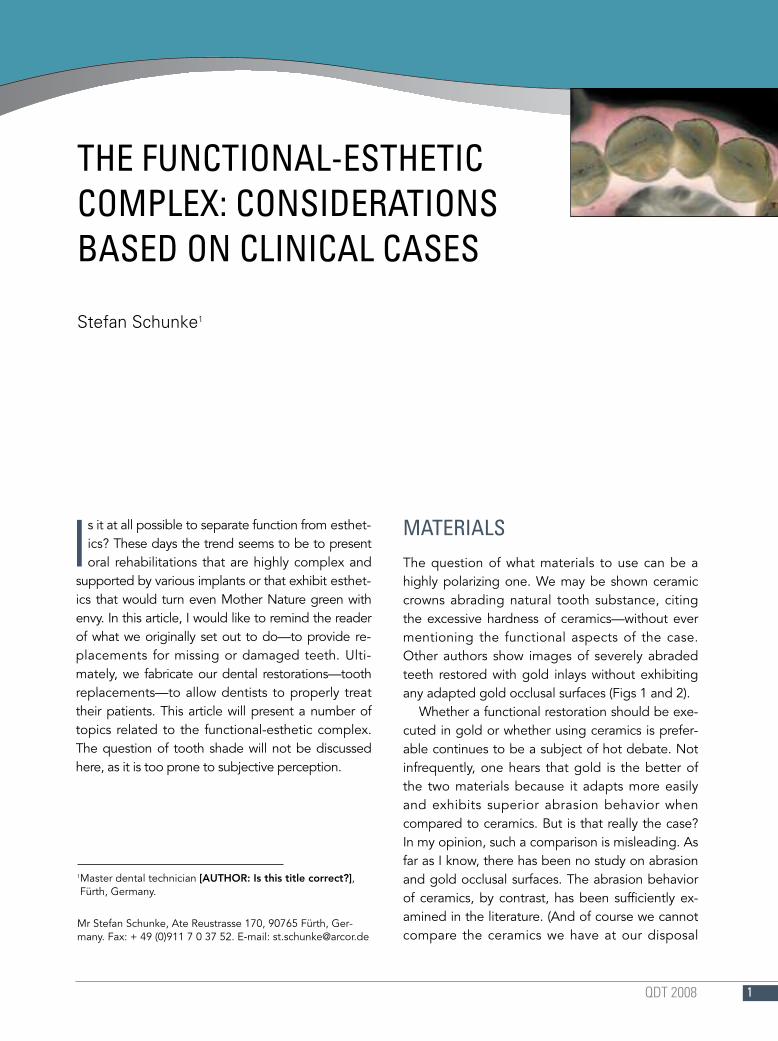
MATERIALSThe question of what materials to use can be ahighly polarizing one. We may be shown ceramiccrowns abrading natural tooth substance, citingthe excessive hardness of ceramics—without evermentioning the functional aspects of the case.Other authors show images of severely abradedteeth restored with gold inlays without exhibitingany adapted gold occlusal surfaces (Figs 1 and 2).
Whether a functional restoration should be exe-cuted in gold or whether using ceramics is prefer-able continues to be a subject of hot debate. Notinfrequently, one hears that gold is the better ofthe two materials because it adapts more easilyand exhibits superior abrasion behavior whencompared to ceramics. But is that really the case?In my opinion, such a comparison is misleading. Asfar as I know, there has been no study on abrasionand gold occlusal surfaces. The abrasion behaviorof ceramics, by contrast, has been sufficiently ex-amined in the literature. (And of course we cannotcompare the ceramics we have at our disposal
1Master dental technician [AUTHOR: Is this title correct?],Fürth, Germany.
Mr Stefan Schunke, Ate Reustrasse 170, 90765 Fürth, Ger-many. Fax: + 49 (0)911 7 0 37 52. E-mail: [email protected]
QDT 2008 1
THE FUNCTIONAL-ESTHETICCOMPLEX: CONSIDERATIONSBASED ON CLINICAL CASES
Stefan Schunke1
today with the materials we worked with in the1960s and 1970s.)
So if gold, as has been claimed, is abrasive, itshould exhibit a rough surface, but, contrarily,functional anomalies manifest themselves intrao-rally as areas of high luster. Metals only exhibithigh luster if they have been highly compressed,as in polishing, so high-luster areas simply consistof what would have to be considered cold-formedmetal. That in turn means that a lot of tension willhave built in the metal, tension that will be relievedin the form of natural enamel cracks or chipping,depending on the shape of the crown. This is oneof the reasons why onlays were promoted in thefirst place.
Preparation shapes, on the other hand, becameever more daring as dentists increasingly strove torespond to patients’ demands for better esthetics.
The advent of adhesive techniques helped allevi-ate the ensuing problems (Fig 3).
Consider a natural mandibular first molar with aparafunction at the distolingual cusp. Now let usassume that this parafunction is very pronounced,causing the cusp to fracture. Let us further assumethat we restore the tooth with a ceramic crownwithout changing the situation itself. What we getthen is, of course, exactly the same situation as be-fore, only in ceramics, and the ceramic cusp is ulti-mately bound to fracture as well. Assuming wehad restored the same situation with a gold crown,while there will be no fracture of that gold crown,the parafunction will persist but manifest itselfelsewhere—in the periodontal tissues, the bone,the orofacial muscles, the temporomandibularjoint, or even more remote parts of the body. Nota good prospect, either.
QDT 20082
SCHUNKE
Figs 1 and 2 When comparing ce-ramics and gold, it is not just thematerial and its technology thatcounts. Functional aspects, espe-cially of the more recent materials,also play a role.
1 2
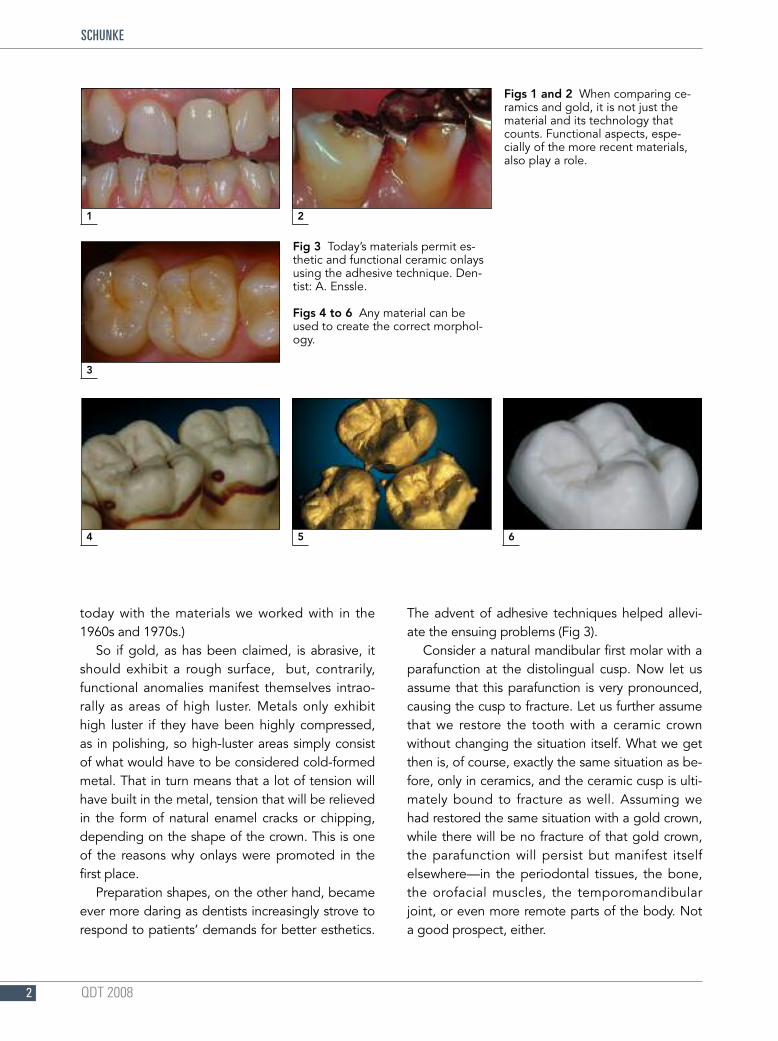
Fig 3 Today’s materials permit es-thetic and functional ceramic onlaysusing the adhesive technique. Den-tist: A. Enssle.
Figs 4 to 6 Any material can beused to create the correct morphol-ogy.
3
4 5 6
QDT 2008 3
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
It is therefore imperative for us to have inti-mate knowledge of the esthetic as well as func-tional aspects of the anatomic and morphologicstructures and to be able to imitate them. This isnot only true of metal occlusal surfaces, but also,and especially, of ceramic occlusal surfaces (Figs4 to 6).
The question of what kind of ceramics is alsoanswered in the literature, which likes to favorglass ceramics in this situation.i–3 Glass ceramics ex-hibits the most favorable abrasion behavior. Butdue to the (in my opinion) esthetic disadvantagesof pure glass ceramics, I currently prefer Inspiration(Heimerle + Meule, Pforzheim, Germany), a state-of-the-art two-phase leucite glass-ceramic mate-rial, for metal-ceramic restorations. The leucite isimportant for obtaining a beautiful esthetic result
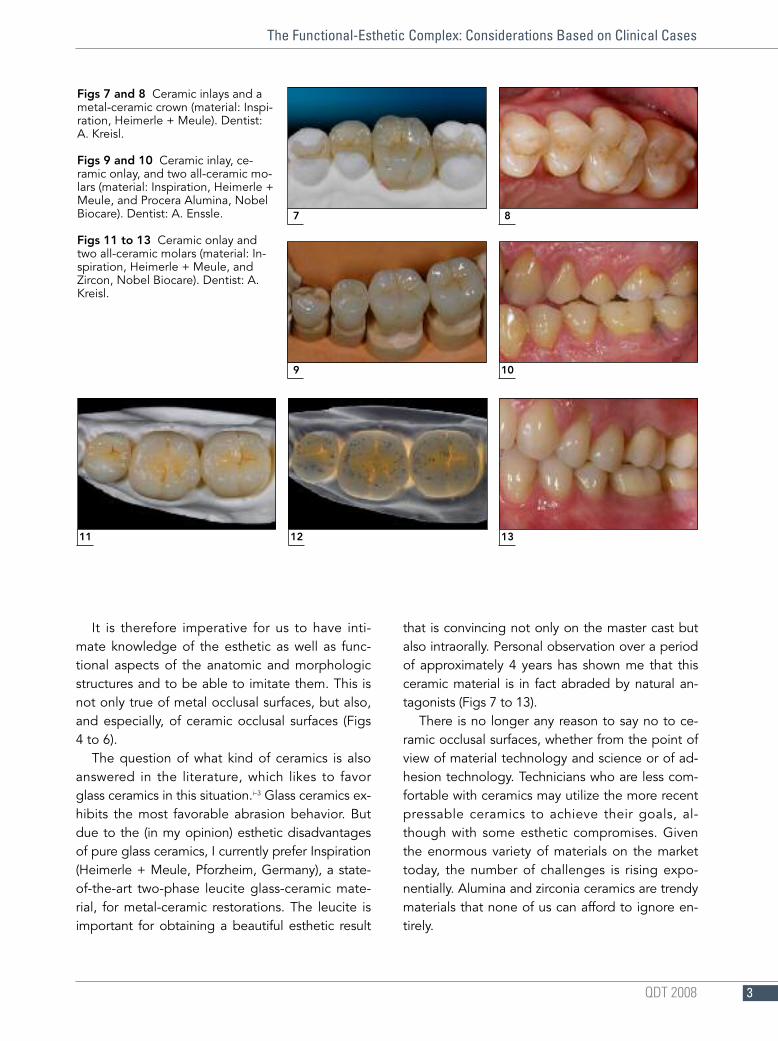
that is convincing not only on the master cast butalso intraorally. Personal observation over a periodof approximately 4 years has shown me that thisceramic material is in fact abraded by natural an-tagonists (Figs 7 to 13).
There is no longer any reason to say no to ce-ramic occlusal surfaces, whether from the point ofview of material technology and science or of ad-hesion technology. Technicians who are less com-fortable with ceramics may utilize the more recentpressable ceramics to achieve their goals, al-though with some esthetic compromises. Giventhe enormous variety of materials on the markettoday, the number of challenges is rising expo-nentially. Alumina and zirconia ceramics are trendymaterials that none of us can afford to ignore en-tirely.
Figs 7 and 8 Ceramic inlays and ametal-ceramic crown (material: Inspi-ration, Heimerle + Meule). Dentist:A. Kreisl.
Figs 9 and 10 Ceramic inlay, ce-ramic onlay, and two all-ceramic mo-lars (material: Inspiration, Heimerle +Meule, and Procera Alumina, NobelBiocare). Dentist: A. Enssle.
Figs 11 to 13 Ceramic onlay andtwo all-ceramic molars (material: In-spiration, Heimerle + Meule, andZircon, Nobel Biocare). Dentist: A.Kreisl.
7 8
9 10
11 12 13
QDT 20084
SCHUNKE
ANTERIOR/CANINE GUIDANCEMany dental technicians, when discussing esthet-ics, will talk about beautiful anterior teeth, morebeautiful than almost anything we ever see in na-ture. But while a beautiful appearance is one thing,function is another. Length-to-width ratios, gingivalscalloping, and emergence profiles are the focusof attention, while the functional aspects of the an-terior teeth are sometimes neglected. Let us there-fore take a look at the definition and the effects ofanterior/canine guidance.
In an Angle Class I situation, lateral movementsare characterized as follows: The distal slope of themandibular canine moves along the mesial slope
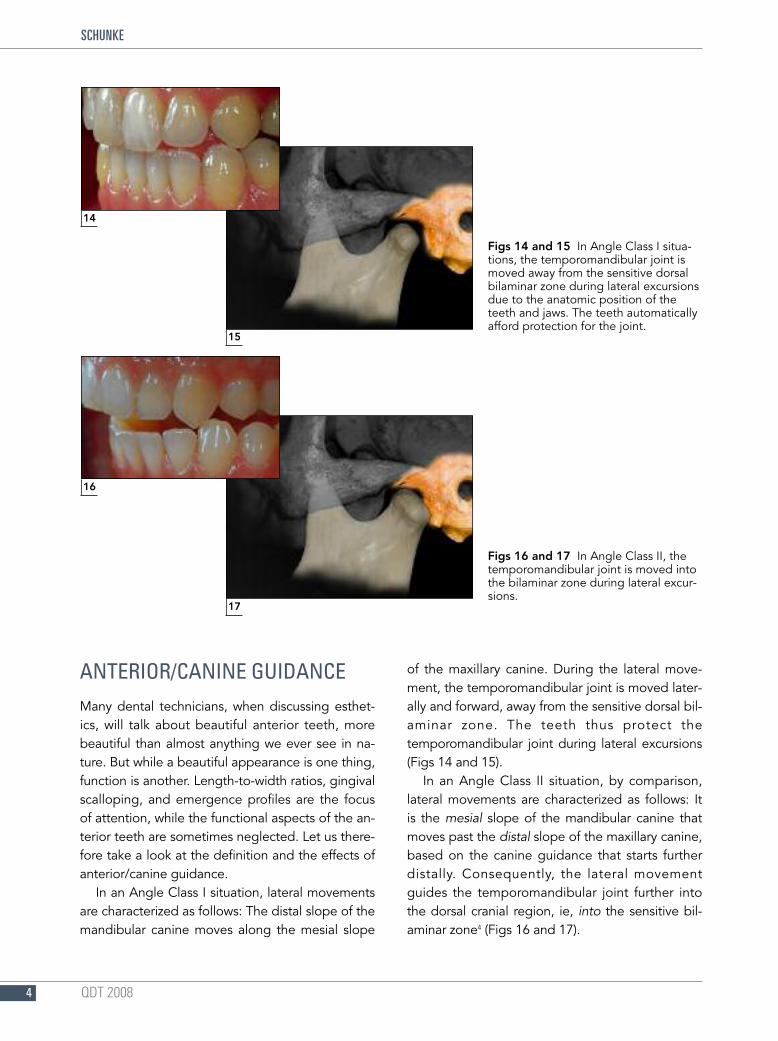
of the maxillary canine. During the lateral move-ment, the temporomandibular joint is moved later-ally and forward, away from the sensitive dorsal bil-aminar zone. The teeth thus protect thetemporomandibular joint during lateral excursions(Figs 14 and 15).
In an Angle Class II situation, by comparison,lateral movements are characterized as follows: Itis the mesial slope of the mandibular canine thatmoves past the distal slope of the maxillary canine,based on the canine guidance that starts furtherdistally. Consequently, the lateral movementguides the temporomandibular joint further intothe dorsal cranial region, ie, into the sensitive bil-aminar zone4 (Figs 16 and 17).
Figs 14 and 15 In Angle Class I situa-tions, the temporomandibular joint ismoved away from the sensitive dorsalbilaminar zone during lateral excursionsdue to the anatomic position of theteeth and jaws. The teeth automaticallyafford protection for the joint.
Figs 16 and 17 In Angle Class II, thetemporomandibular joint is moved intothe bilaminar zone during lateral excur-sions.
15
14
17
16
QDT 2008 5
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
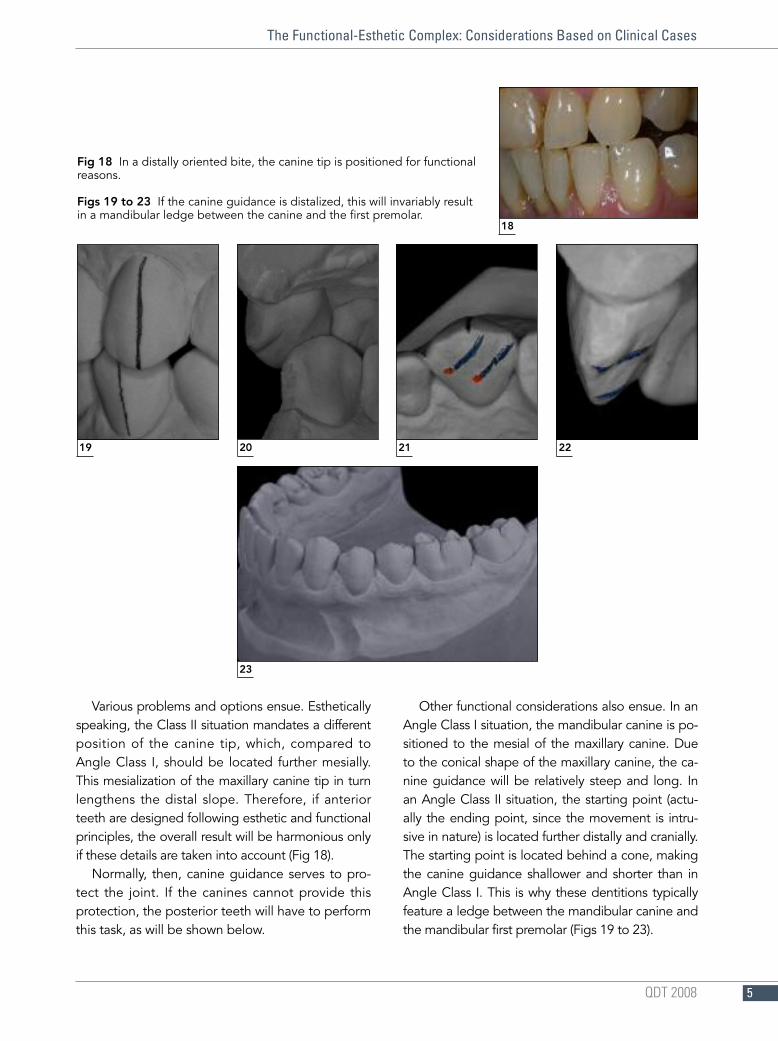
Various problems and options ensue. Estheticallyspeaking, the Class II situation mandates a differentposition of the canine tip, which, compared toAngle Class I, should be located further mesially.This mesialization of the maxillary canine tip in turnlengthens the distal slope. Therefore, if anteriorteeth are designed following esthetic and functionalprinciples, the overall result will be harmonious onlyif these details are taken into account (Fig 18).
Normally, then, canine guidance serves to pro-tect the joint. If the canines cannot provide thisprotection, the posterior teeth will have to performthis task, as will be shown below.
Other functional considerations also ensue. In anAngle Class I situation, the mandibular canine is po-sitioned to the mesial of the maxillary canine. Dueto the conical shape of the maxillary canine, the ca-nine guidance will be relatively steep and long. Inan Angle Class II situation, the starting point (actu-ally the ending point, since the movement is intru-sive in nature) is located further distally and cranially.The starting point is located behind a cone, makingthe canine guidance shallower and shorter than inAngle Class I. This is why these dentitions typicallyfeature a ledge between the mandibular canine andthe mandibular first premolar (Figs 19 to 23).
Fig 18 In a distally oriented bite, the canine tip is positioned for functionalreasons.
Figs 19 to 23 If the canine guidance is distalized, this will invariably resultin a mandibular ledge between the canine and the first premolar.
23
19 20 21 22
18
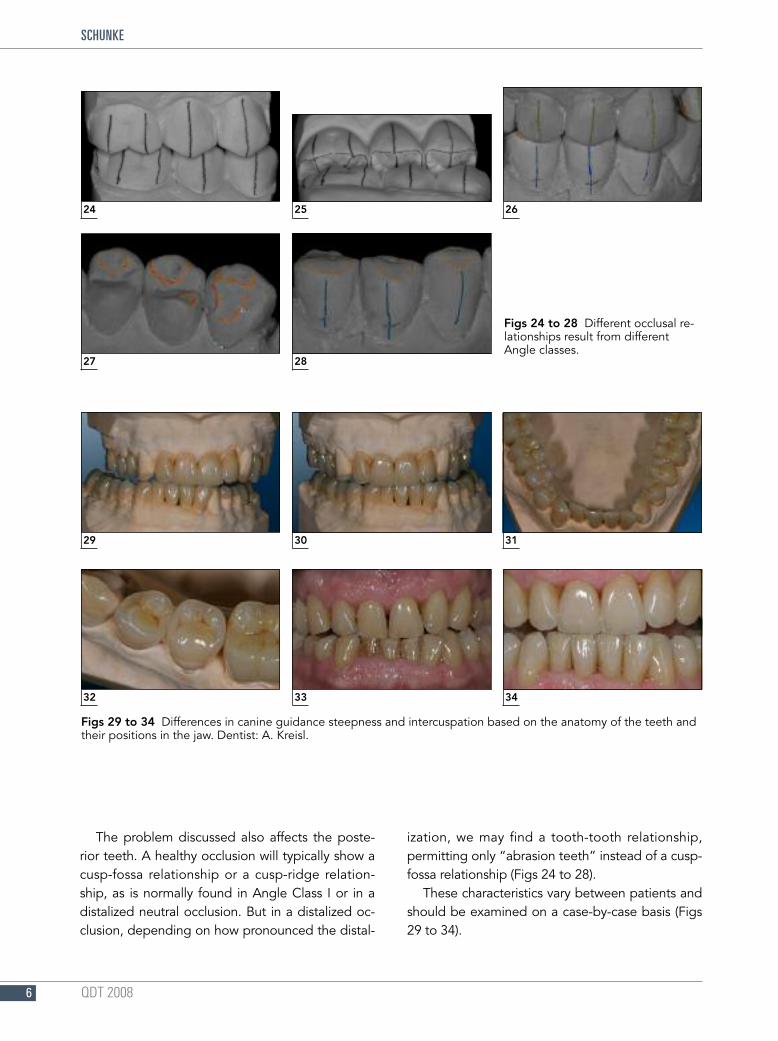
The problem discussed also affects the poste-rior teeth. A healthy occlusion will typically show acusp-fossa relationship or a cusp-ridge relation-ship, as is normally found in Angle Class I or in adistalized neutral occlusion. But in a distalized oc-clusion, depending on how pronounced the distal-
ization, we may find a tooth-tooth relationship,permitting only “abrasion teeth” instead of a cusp-fossa relationship (Figs 24 to 28).
These characteristics vary between patients andshould be examined on a case-by-case basis (Figs29 to 34).
QDT 20086
SCHUNKE
24 25 26
29 30 31
32 33 34
Figs 24 to 28 Different occlusal re-lationships result from differentAngle classes.
27 28
Figs 29 to 34 Differences in canine guidance steepness and intercuspation based on the anatomy of the teeth andtheir positions in the jaw. Dentist: A. Kreisl.

THE BIOMECHANICAL CONCEPTACCORDING TO POLZ
Many and very different concepts of function arebeing propagated today. Dentists have the luxuryof being able to concentrate on a single system toguide all their treatment efforts. Dental technicians,on the other hand, are faced with having to dealwith different dentists favoring different concepts—or no concept. In any case, dentists expect the fin-ished restoration to create no problems, whether atthe time of insertion or later. This is where thebiomechanical concept according to Master DentalTechnician M. H. Polz comes into play.
A frequently discussed aspect is the number ofcontacts to provide. The literature clearly indicatesan average of 3.9 contacts per tooth.5,6 Too manyocclusal stops restrict movement, especially in themolar region, which is strongly influenced by thetemporomandibular joint. This is demonstratedbelow on the basis of two directed movements.
One of these movements is the immediate sideshift (ISS). The question has been raised whetherthis movement exists at all, but it has beendemonstrated in various publications.7–10Whether itis physiological or pathological in nature is a ques-tion that must be answered by scientific research.The following two options exist in clinical practice:either the dentist believes that this movementshould be disregarded because it does not exist orthe dentist believes it to be pathological, takingthe requisite precautions to avoid this movement.
But not infrequently the dental technician will sim-ply be confronted with the task and will have to re-solve it somehow, without any additional informa-tion. The movement as such is defined as thetemporomandibular joint first moving medially (in-ward) on the mediotrusive (nonworking) side dur-ing lateral excursions before performing the re-mainder of the usual mediotrusive movement.Imagining this movement and its effect on thetemporomandibular joint and the molars in thefrontal view illustrates the problem.
If the joint really performs this type of move-ment, the classical gnathological waxup schemewill soon reach its limits. Even the early gnatholo-gists knew about this problem, and since theycould not compensate for it in their waxup con-cept, they accommodated it with an elaborate ar-ticulation technique.11,12
So what do we do if we do not have the requi-site information? M. H. Polz, being a keen ob-server of nature, was the first one to describe themorphologic structures as resembling “back-packs.”13–15 Occlusal stops would be placed onthese backpacks, creating space for the respectivemovements. For the ISS, this would mean that themandibular first molar has a prepended occlusalelement (the backpack) on its middle (distobuccal)cusp. And it is just this backpack that is contactedby the mesiopalatal cusp of the maxillary firstmolar. This provides the necessary space for theexcursion in the occlusal vicinity (Figs 35 to 37).
Another very important direction of movement iscalled laterotrusion. This term implies that the jaw
QDT 2008 7
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
35 36 37
Figs 35 to 37 The immediate side shift requires sufficient space by provid-ing “backpacks” in the correctly designed occlusal morphology.
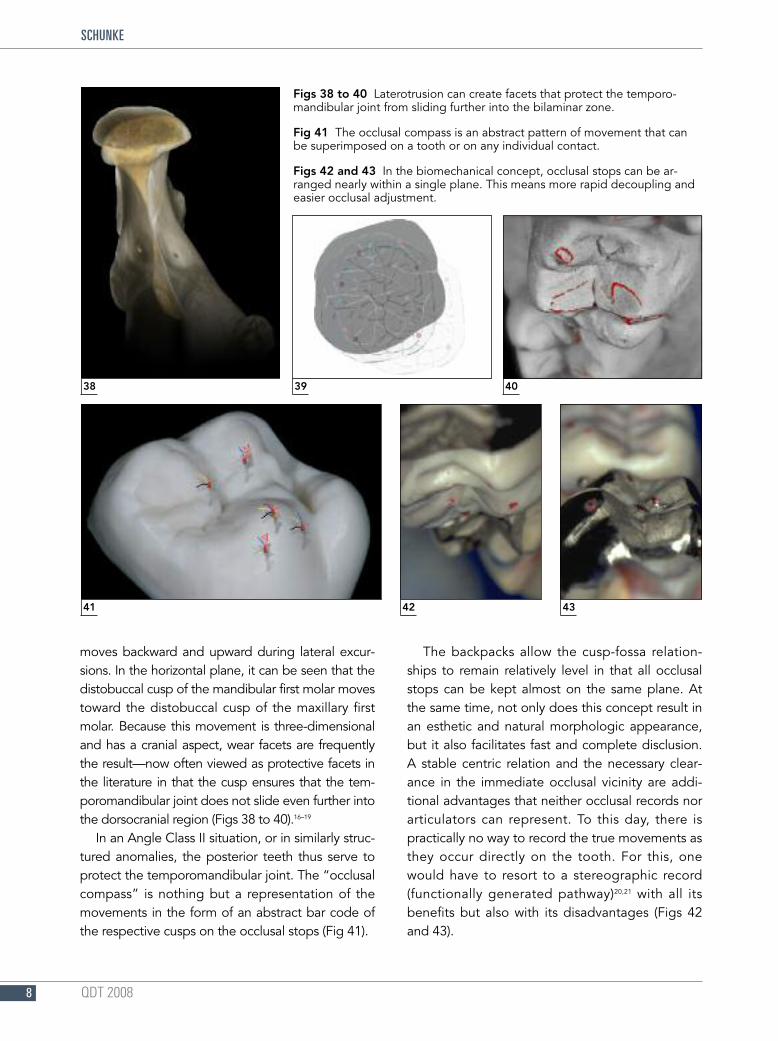
moves backward and upward during lateral excur-sions. In the horizontal plane, it can be seen that thedistobuccal cusp of the mandibular first molar movestoward the distobuccal cusp of the maxillary firstmolar. Because this movement is three-dimensionaland has a cranial aspect, wear facets are frequentlythe result—now often viewed as protective facets inthe literature in that the cusp ensures that the tem-poromandibular joint does not slide even further intothe dorsocranial region (Figs 38 to 40).16–19
In an Angle Class II situation, or in similarly struc-tured anomalies, the posterior teeth thus serve toprotect the temporomandibular joint. The “occlusalcompass” is nothing but a representation of themovements in the form of an abstract bar code ofthe respective cusps on the occlusal stops (Fig 41).
The backpacks allow the cusp-fossa relation-ships to remain relatively level in that all occlusalstops can be kept almost on the same plane. Atthe same time, not only does this concept result inan esthetic and natural morphologic appearance,but it also facilitates fast and complete disclusion.A stable centric relation and the necessary clear-ance in the immediate occlusal vicinity are addi-tional advantages that neither occlusal records norarticulators can represent. To this day, there ispractically no way to record the true movements asthey occur directly on the tooth. For this, onewould have to resort to a stereographic record(functionally generated pathway)20,21 with all itsbenefits but also with its disadvantages (Figs 42and 43).
QDT 20088
SCHUNKE
38 39 40
Figs 38 to 40 Laterotrusion can create facets that protect the temporo-mandibular joint from sliding further into the bilaminar zone.
Fig 41 The occlusal compass is an abstract pattern of movement that canbe superimposed on a tooth or on any individual contact.
Figs 42 and 43 In the biomechanical concept, occlusal stops can be ar-ranged nearly within a single plane. This means more rapid decoupling andeasier occlusal adjustment.
41 42 43

PLANESAnother aspect that is unfortunately frequently ne-glected is related to the various planes, of whichthe most important ones are defined as follows:
• Occlusal plane: A plane supported by themandibular central incisors and the distobuccalcusps of the mandibular second molars.
• Occlusal line: The sagittal curvature of the denti-tion relative to the masticatory plane, ie, theanatomical curve formed by the teeth, called thecurve of Spee (named after Ferdinand Spee, whodescribed this curve in 1890). Behind themandibular canine tip, this curve drops downslightly, turning to horizontal in the region of thefirst molars and ascending in their region of thesecond molars.22,23
• Esthetic plane24 (“glass-plate plane”): If we visual-ize the occlusal plane as a glass plate on whichwe place the maxilla, ideally the teeth will be incontact as follows: central incisors, yes; lateral in-cisors, no (lateroprotrusion); canines, yes; firstpremolars, yes (buccally); second premolars, yes(buccally and palatal); first molars, yes(mesiopalatally); second molars, no.
The occlusal plane and the so-called occlusalline are important because they are responsible forcorrect disclusion and for the correct transfer offorces to the entire cranium and the body as awhole.25
How can we ensure that the occlusal plane canbe checked immediately and integrated directlyinto our procedures? Probably the simplestmethod is the use of the Candulor bite fork (Can-dulor AG, Rielasingen/Worblingen, Germany)When fitted to the patient, as shown for the max-illa in Fig 44, it serves to check the so-called es-thetic plane, which must be in harmony with theocclusal plane. The esthetic plane should run par-allel to the bipupillary line. As Fig 44 clearly shows,this is not the case for the patient depicted. Theissue is whether this is an anatomic problem or achallenge that needs to be resolved prosthodonti-cally. Looking at the patient’s smile, additional seri-ous visual deficiencies become apparent. They arebest resolved by using provisional therapeuticrestorations, allowing the patient to become ac-customed to her new appearance, phonetics, andfunction. The definitive restoration would then sim-ply implement the result in ceramics and add thefinal touches (Figs 45 to 49).
QDT 2008 9
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
Fig 44 The Candulor can be used to check the relation-ship between the occlusal planes and the cranium in arelatively quick and simple manner.
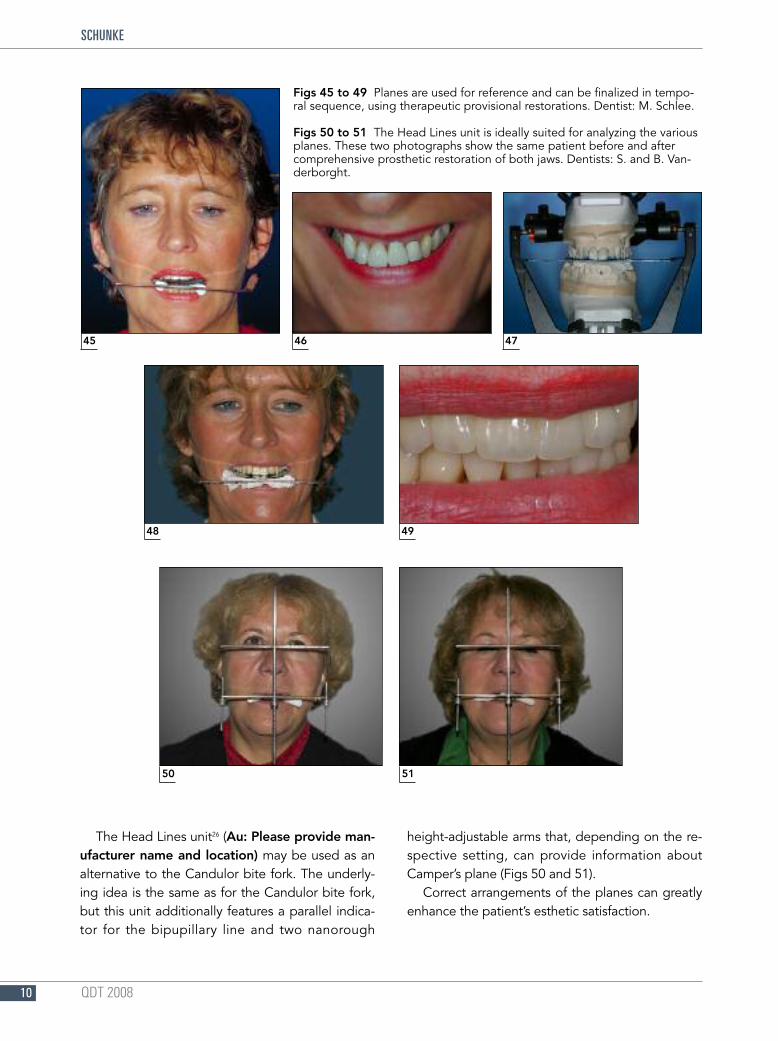
The Head Lines unit26 (Au: Please provide man-ufacturer name and location) may be used as analternative to the Candulor bite fork. The underly-ing idea is the same as for the Candulor bite fork,but this unit additionally features a parallel indica-tor for the bipupillary line and two nanorough
height-adjustable arms that, depending on the re-spective setting, can provide information aboutCamper’s plane (Figs 50 and 51).
Correct arrangements of the planes can greatlyenhance the patient’s esthetic satisfaction.
QDT 200810
SCHUNKE
45 46 47
Figs 45 to 49 Planes are used for reference and can be finalized in tempo-ral sequence, using therapeutic provisional restorations. Dentist: M. Schlee.
Figs 50 to 51 The Head Lines unit is ideally suited for analyzing the variousplanes. These two photographs show the same patient before and aftercomprehensive prosthetic restoration of both jaws. Dentists: S. and B. Van-derborght.
48 49
50 51
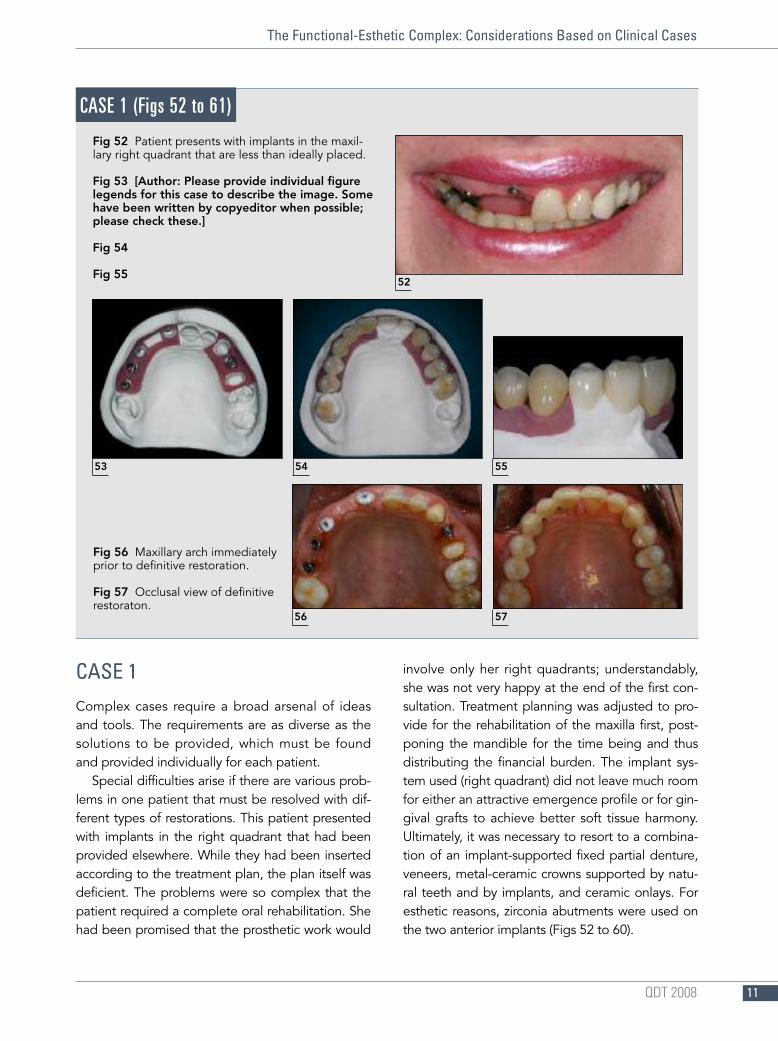
CASE 1Complex cases require a broad arsenal of ideasand tools. The requirements are as diverse as thesolutions to be provided, which must be foundand provided individually for each patient.
Special difficulties arise if there are various prob-lems in one patient that must be resolved with dif-ferent types of restorations. This patient presentedwith implants in the right quadrant that had beenprovided elsewhere. While they had been insertedaccording to the treatment plan, the plan itself wasdeficient. The problems were so complex that thepatient required a complete oral rehabilitation. Shehad been promised that the prosthetic work would
involve only her right quadrants; understandably,she was not very happy at the end of the first con-sultation. Treatment planning was adjusted to pro-vide for the rehabilitation of the maxilla first, post-poning the mandible for the time being and thusdistributing the financial burden. The implant sys-tem used (right quadrant) did not leave much roomfor either an attractive emergence profile or for gin-gival grafts to achieve better soft tissue harmony.Ultimately, it was necessary to resort to a combina-tion of an implant-supported fixed partial denture,veneers, metal-ceramic crowns supported by natu-ral teeth and by implants, and ceramic onlays. Foresthetic reasons, zirconia abutments were used onthe two anterior implants (Figs 52 to 60).
QDT 2008 11
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
52
Fig 52 Patient presents with implants in the maxil-lary right quadrant that are less than ideally placed.
Fig 53 [Author: Please provide individual figurelegends for this case to describe the image. Somehave been written by copyeditor when possible;please check these.]
Fig 54
Fig 55
Fig 56 Maxillary arch immediatelyprior to definitive restoration.
Fig 57 Occlusal view of definitiverestoraton.
CASE 1 (Figs 52 to 61)
53 5554
56 57
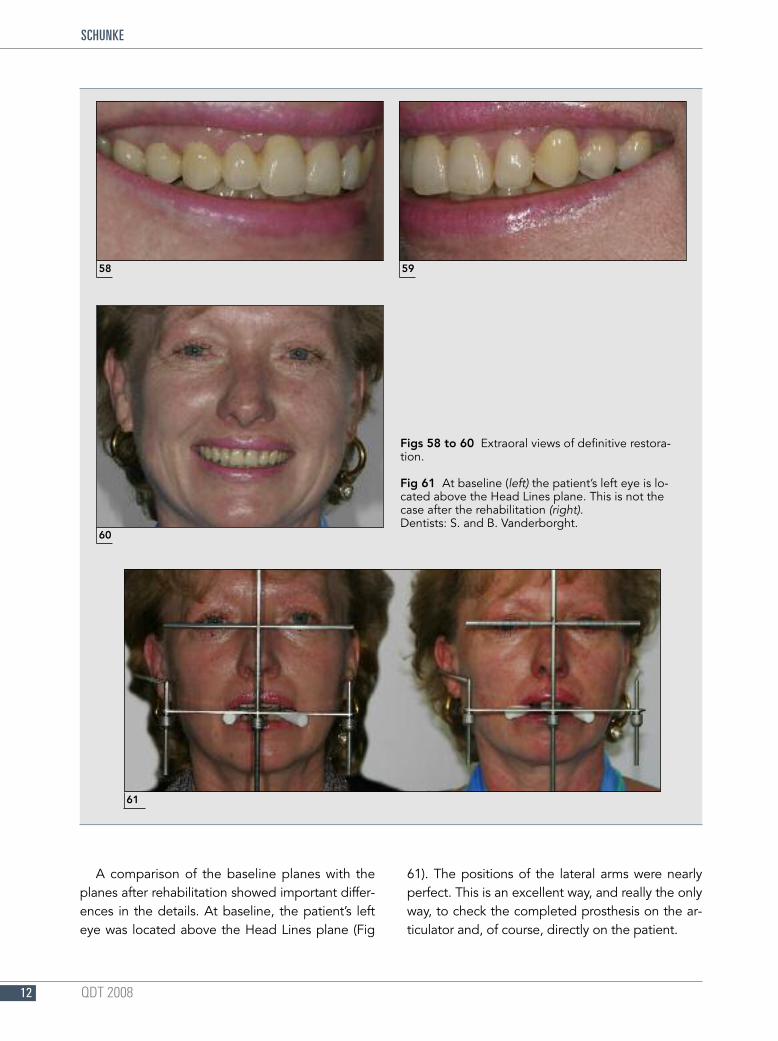
A comparison of the baseline planes with theplanes after rehabilitation showed important differ-ences in the details. At baseline, the patient’s lefteye was located above the Head Lines plane (Fig
61). The positions of the lateral arms were nearlyperfect. This is an excellent way, and really the onlyway, to check the completed prosthesis on the ar-ticulator and, of course, directly on the patient.
QDT 200812
SCHUNKE
58 59
Figs 58 to 60 Extraoral views of definitive restora-tion.
Fig 61 At baseline (left) the patient’s left eye is lo-cated above the Head Lines plane. This is not thecase after the rehabilitation (right).Dentists: S. and B. Vanderborght.
60
61
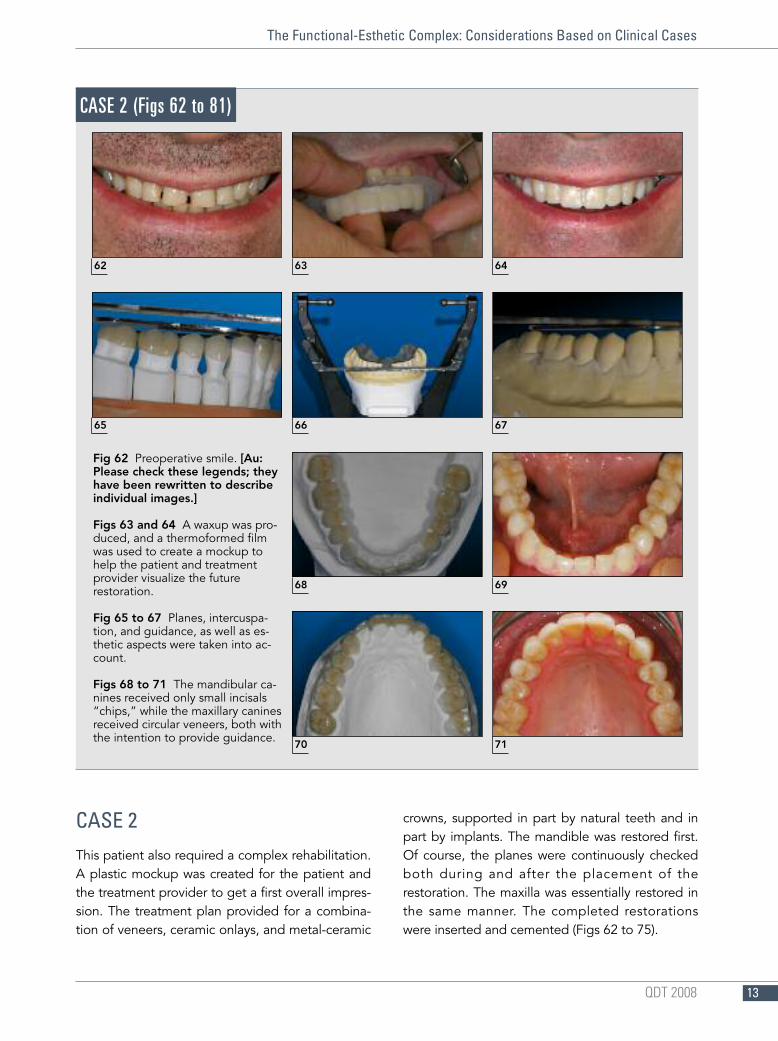
CASE 2This patient also required a complex rehabilitation.A plastic mockup was created for the patient andthe treatment provider to get a first overall impres-sion. The treatment plan provided for a combina-tion of veneers, ceramic onlays, and metal-ceramic
crowns, supported in part by natural teeth and inpart by implants. The mandible was restored first.Of course, the planes were continuously checkedboth during and after the placement of therestoration. The maxilla was essentially restored inthe same manner. The completed restorationswere inserted and cemented (Figs 62 to 75).
QDT 2008 13
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
Fig 62 Preoperative smile. [Au:Please check these legends; theyhave been rewritten to describeindividual images.]
Figs 63 and 64 A waxup was pro-duced, and a thermoformed filmwas used to create a mockup tohelp the patient and treatmentprovider visualize the futurerestoration.
Fig 65 to 67 Planes, intercuspa-tion, and guidance, as well as es-thetic aspects were taken into ac-count.
Figs 68 to 71 The mandibular ca-nines received only small incisals“chips,” while the maxillary caninesreceived circular veneers, both withthe intention to provide guidance.
CASE 2 (Figs 62 to 81)
62 63 64
65 66 67
68 69
70 71
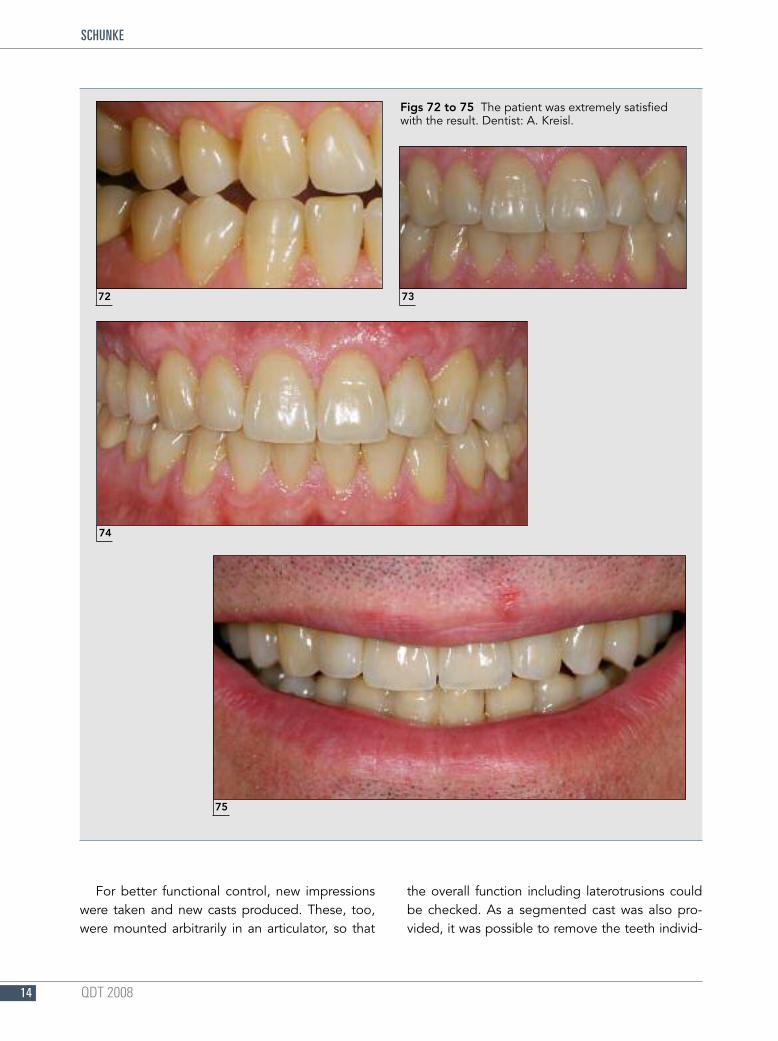
For better functional control, new impressionswere taken and new casts produced. These, too,were mounted arbitrarily in an articulator, so that
the overall function including laterotrusions couldbe checked. As a segmented cast was also pro-vided, it was possible to remove the teeth individ-
QDT 200814
SCHUNKE
72 73
74
75
Figs 72 to 75 The patient was extremely satisfiedwith the result. Dentist: A. Kreisl.
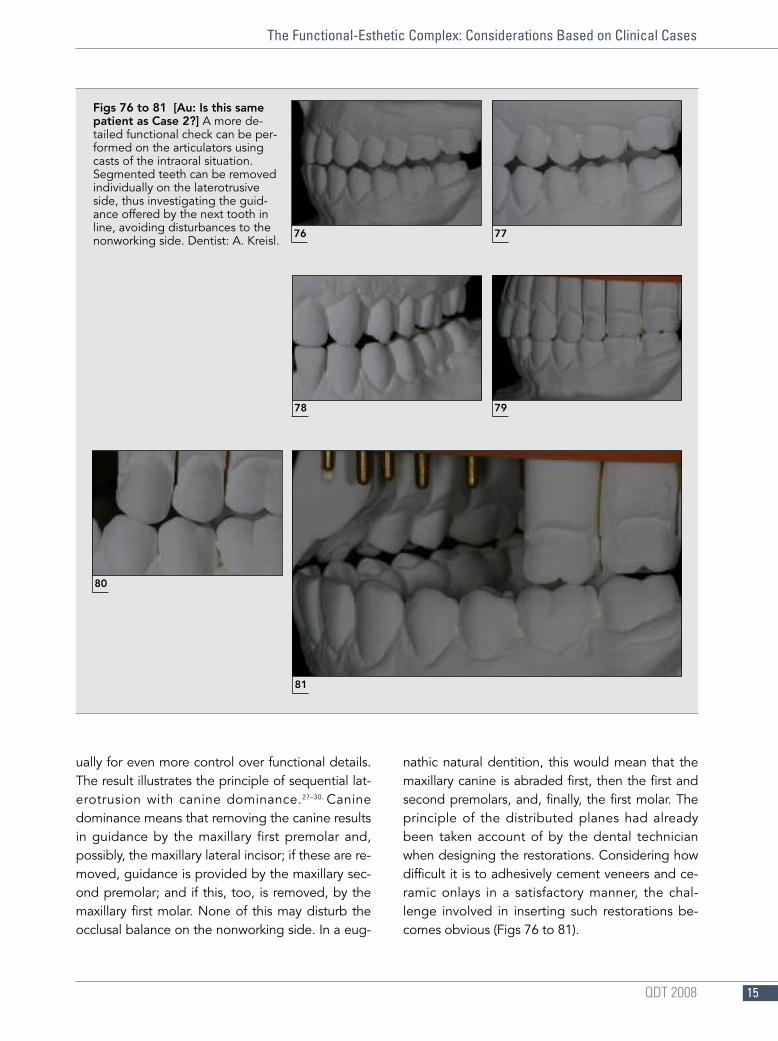
ually for even more control over functional details.The result illustrates the principle of sequential lat-erotrusion with canine dominance.27–30. Caninedominance means that removing the canine resultsin guidance by the maxillary first premolar and,possibly, the maxillary lateral incisor; if these are re-moved, guidance is provided by the maxillary sec-ond premolar; and if this, too, is removed, by themaxillary first molar. None of this may disturb theocclusal balance on the nonworking side. In a eug-
nathic natural dentition, this would mean that themaxillary canine is abraded first, then the first andsecond premolars, and, finally, the first molar. Theprinciple of the distributed planes had alreadybeen taken account of by the dental technicianwhen designing the restorations. Considering howdifficult it is to adhesively cement veneers and ce-ramic onlays in a satisfactory manner, the chal-lenge involved in inserting such restorations be-comes obvious (Figs 76 to 81).
QDT 2008 15
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
Figs 76 to 81 [Au: Is this samepatient as Case 2?] A more de-tailed functional check can be per-formed on the articulators usingcasts of the intraoral situation.Segmented teeth can be removedindividually on the laterotrusiveside, thus investigating the guid-ance offered by the next tooth inline, avoiding disturbances to thenonworking side. Dentist: A. Kreisl.
76 77
78 79
80
81
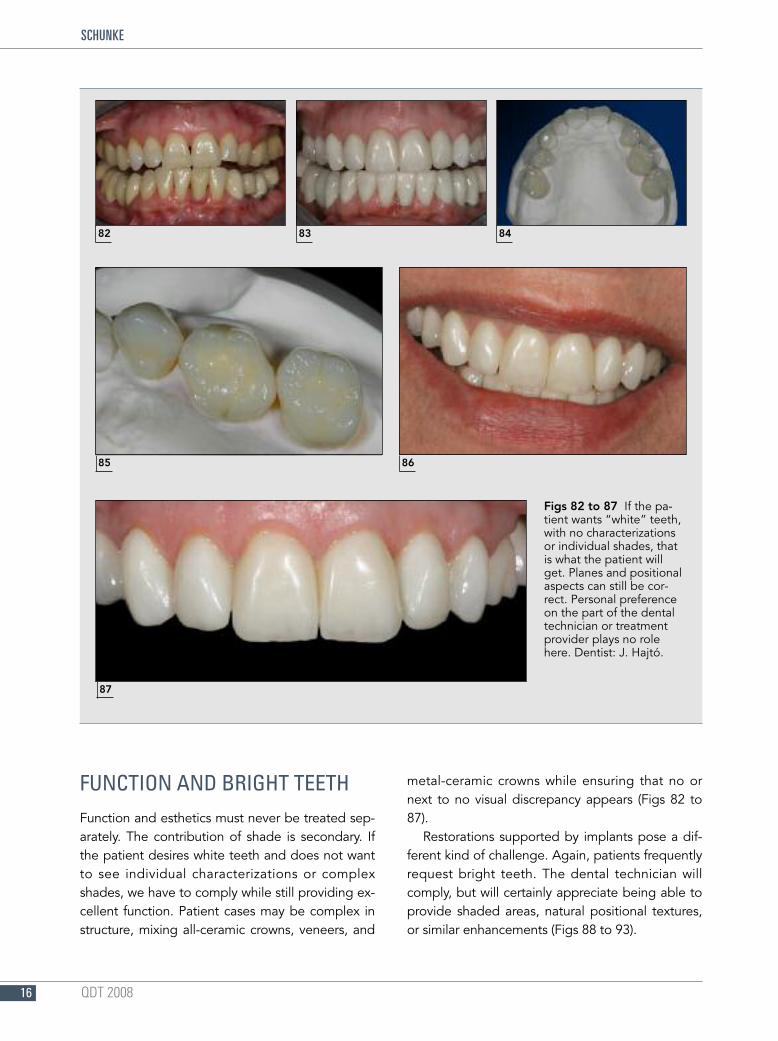
FUNCTION AND BRIGHT TEETHFunction and esthetics must never be treated sep-arately. The contribution of shade is secondary. Ifthe patient desires white teeth and does not wantto see individual characterizations or complexshades, we have to comply while still providing ex-cellent function. Patient cases may be complex instructure, mixing all-ceramic crowns, veneers, and
metal-ceramic crowns while ensuring that no ornext to no visual discrepancy appears (Figs 82 to87).
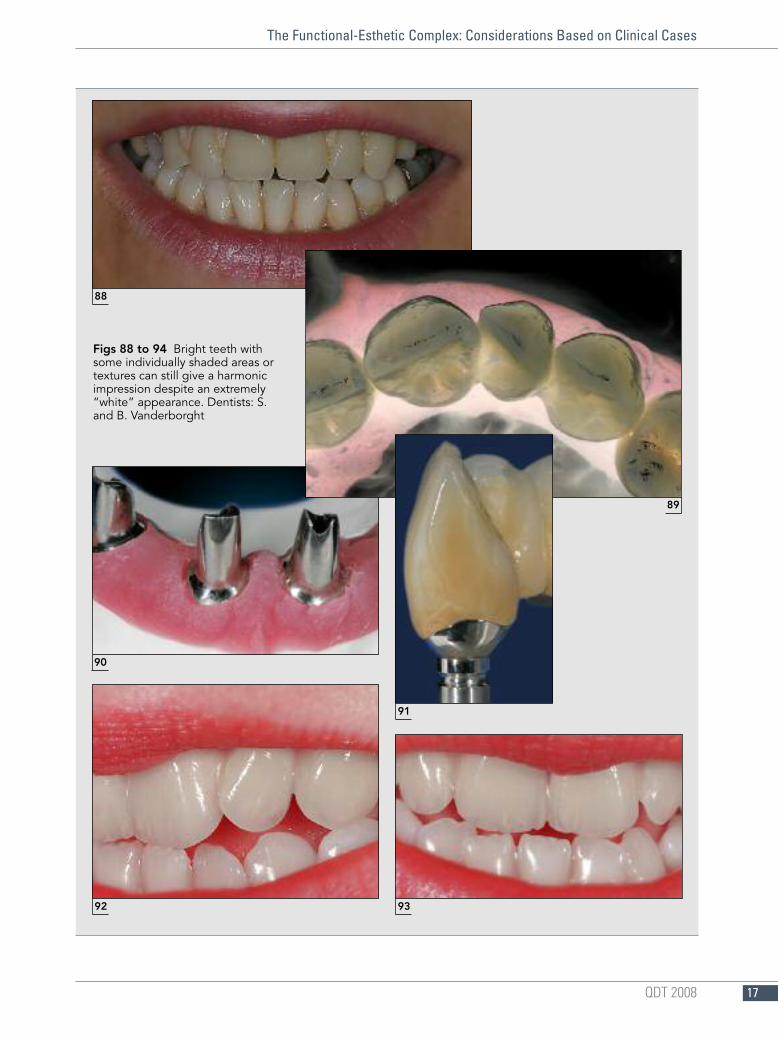
Restorations supported by implants pose a dif-ferent kind of challenge. Again, patients frequentlyrequest bright teeth. The dental technician willcomply, but will certainly appreciate being able toprovide shaded areas, natural positional textures,or similar enhancements (Figs 88 to 93).
QDT 200816
SCHUNKE
82 83 84
85 86
87
Figs 82 to 87 If the pa-tient wants “white” teeth,with no characterizationsor individual shades, thatis what the patient willget. Planes and positionalaspects can still be cor-rect. Personal preferenceon the part of the dentaltechnician or treatmentprovider plays no rolehere. Dentist: J. Hajtó.
QDT 2008 17
The Functional-Esthetic Complex: Considerations Based on Clinical Cases
Figs 88 to 94 Bright teeth withsome individually shaded areas ortextures can still give a harmonicimpression despite an extremely“white” appearance. Dentists: S.and B. Vanderborght
88
92 93
89
90
91

REFERENCES1. Schäffer H. Keramikinlays, Materialkundliche und klinische
Aspekte—experimentelle Untersuchungen [Thesis].Berlin: Quintessenz, 1993.
2. Hahn R. Vollkeramische Einzelzahnrestauration [Thesis].Berlin: Quintessenz, 1997.
3. Hohmann W. Dentalkeramik auf der Basis hydrothermalerGläser. Berlin: Quintessenz, 1993.
4. Bumann A, Lotzmann U. Funktionsdiagnostik undTherapieprinzipien. Stuttgart: Thieme, 2000.
5. Buth K. Zur funktionellen Gestaltung desKauflächenkomplexes bei festsitzendem Zahnersatz mithilfe der FGP—Technik und unter Anwendung vonKugelsegmentfertigteilen. Jahrestagung derArbeitsgemeinschaft Dentale Technologie, May 1989.
6. End E. Die physiologische Okklusion des menschlichenGebisses. München: Verlag Neuer Merkur, 2005.
7. Lundeen H, Gibbs C. Mandibular movement and istclinical significance [in German]. Phillip J RestaurZahnmed 1987;4(2):87–97.
8. Lundeen H, Gibbs Ch. The Function of Teeth. US: L and GPublishers, 2005.
9. Staehle H. Effect of the articulator joint on shaping themasticatory surface [in German]. Dtsch Zahnarztl Z1984;39:356–359.
10. Lückerath W. Das transversale und vertikaleBewegungsspiel des Unterkiefers im Bereich derKauflächen und der Kiefergelenke [Thesis], 1991.
11. McCollum BB, Stuart CE. A research report, published byStuart, P.O. Box 1298, Ventura. CA 93001, 1955.
12. Stuart CE, Golden IB. Gnathological instruments. In: TheHistory of Gnathology. Ventura, CA: Stuart CE, 1984.
13. Polz MH. Biomechanical basis of occlusal mastictorysurface design [in German]. Zahntechnik (Zur)1981(2);39:126–134.
14. Polz MH. Die biomechanische Aufwachstechnik bei Inlay-und Onlay-Restaurationen. In: in Caesar HH. Inlay- undOnlay-Techniken. München: Verlag Neuer Merkur, 1987.
15. Polz MH. Die biomechanische Kaufläche und derenAnwendung in allen okkluslalen Beziehungen.Jahrestagung der Arbeitsgemeinschaft DentaleTechnologie, May 1989.
16. Hugger A. Gelenknahe elektronissche Erfassung derUnterkieferfunktion und ihr Umsetzung in den Artikulator[Thesis]. Berlin: Quintessenz, 2000.
17. Lotzmann U. Studien zum Einfluss der okklusalen Prä-Therapie auf die zentrische Kieferrelation [Thesis]. Berlin:Quintessenz, 1999.
18. Koeck B. Experimentelle Untersuchungen zur Dynamikdes Unterkiefers während des Nachtschlafes [Thesis].Berlin: Quintessenz, 1982.
19. Schmierer A. Kiefergelenksfuntkionen—die retrusiveSurtrusion des Laterotrusionskondylus. Zahnarzt Magazin1991;4:24–35.
20. Dawson P. Grundzüge der Okklusion. München: VerlagZahnärztliches Schrifttum, 1978.
21. Lex Ch. FGP-Technik, praktischer Arbeitskurs bei BSI.Fürth, Germany, 1989.
22. Gysi A. Das Aufstellen der Zähne für Vollprothesen.Zürich: Schweizerische Zahntechniker Vereinigung, 1948.
23. Hajto J. Anteriors [in German]. Fuchstal, Germany:Teamwork Media, 2006:180.
24. Gysi A. The Gysi Method [in German]. DeTrey, 1932.25. Rossaint A, Lechner J, van Assche S. Das Cranio-sacrale
System. Heidelberg: Hüthig, 1996:59.26. Schöttl R, Bertram U, Karg R, Losert-Bruggner B. Präzision
der Modellposition im Artikulator bei der Übertragungmit mittellwertigen Gesichtsbögen. ICCMO Kompendium2004. Erlangen: International College of Cranio-Mandibular Orthopedics, 2004:109–120.
27. Slavicek R. Die funktionellen Determinanten desKauorgans [Thesis]. Wien, 1984.
28. Slavicek R, Mack H. Die funktionelle Morphologie derOkklusion. Dent Labor 1980;28:1307–1318.
29. Slavicek R. Das Kauorgan. Klosterneuburg: Gamma Med.-Wis, 2000.
30. Reusch D, Lenze PG, Fischer H. Rekonstruktion vonKauflächen undn Frontzähnen. Westerburg, Germany:Westerburger Kontakte, 1990.
QDT 200818
SCHUNKE





























