Embed Size (px)
Citation preview

Review
The future of traditional nonsteroidal
antiinflammatory drugs and cyclooxygenase-2
inhibitors in the treatment of inflammation and pain
Maria G. Sciulli, Marta L. Capone, Stefania Tacconelli, Paola Patrignani
Department of Medicine and Center of Excellence on Aging, “Gabriele d’Annunzio” University, School of
Medicine, and “Gabriele d’Annnunzio” University Foundation, Ce.S.I., Via dei Vestini 31, 66013 Chieti, Italy
Correspondence: Paola Patrignani, e-mail: [email protected]
Abstract:
Prostanoids act leading roles in a myriad of physiologic and pathologic processes because these autacoids participate in the
amplification of biological responses induced by innumerable stimuli. The formation of prostanoids is operated by two synthases
named cyclooxygenase(COX)-1 and COX-2. Traditional nonsteroidal antiinflammatory drugs (tNSAIDs) and COX-2 inhibitors
(coxibs) give rise to antipyretic, analgesic, and antiinflammatory actions, through their reversible clogging of the COX channel of
COX-2 – apart from aspirin which modifies irreversibly the catalytic activity of COX-2. tNSAIDs and COX-2 inhibitors resulted
clinically equivalent for the relief of acute pain and symptoms of arthropathies but they failed to modify disease progression. Clinical
evidence of the possible contribution of COX-1 in inflammation and pain in some occasion – as suggested by experimental and
pharmacology studies – is orphan because none efficacy trial with COX inhibitors was designed to establish it. COX-2 inhibitors
were developed with the aim to reduce the incidence of serious gastrointestinal (GI) adverse effects associated with the
administration of tNSAIDs ensued as a consequence of the inhibition of cytoprotective COX-1-derived prostanoids. However, the
reduced incidence of serious GI adverse effects compared to tNSAIDs demonstrated for 2 COX-2 inhibitors (e.g. rofecoxib and
lumiracoxib) has been countered by an increased incidence of myocardial infarction and stroke detected in 5 placebo controlled trials
involving the COX-2 inhibitors celecoxib, rofecoxib and valdecoxib. The future of COX-2 inhibitors will be an example of personalised
medicine as their use will be restricted to patients who do not respond to tNSAIDs or with increased risk of GI complications.
Key words:
cyclooxygenase, nonsteroidal antiinflammatory drugs, coxibs, prostacyclin, thromboxane
Abbreviations: AA – arachidonic acid, APC – Adenoma Pre-
vention with Celecoxib, APPROVe – Adenomatous Polyp
Prevention on Vioxx, Arg – arginine, bid – bis in die, CABG
– coronary artery bypass grafting, COX – cyclooxygenase,
CSF – cerebrospinal fluid, CVD – cardiovascular disease, DP
– PGD receptor, DKOs – double knockouts, EDGE – Etori-
coxib Diclofenac Gastrointestinal Evaluation, EMEA – Euro-
pean Medicines Agency, EP – PGE receptor, FAP – familial
adenomatous polyposis, FDA – Food and Drug Administra-
tion, FP – PGF receptor, GI – gastrointestinal, GSH – glu-
tathione, GST – glutathione-S-transferase, HOX – peroxi-
dase, IL – interleukin, im – intramuscular, Ile – isoleucine, IP
– PGI receptor, IPKOs – IP knockouts, iv – intravenous, LDL
– low-density lipoproteins, LPS – lipopolysaccharide, MAPEG
– membrane-associated proteins involved in eicosanoid and
GSH metabolism, tNSAIDs – traditional nonsteroidal antiin-
flammatory drugs, OA – osteoarthritis, ox-LDL – oxidised LDL,
PLs – phospholipases, PPAR – peroxisome proliferator-activated
receptor, PG – prostaglandin, PGDS – PGD synthase, PGES –
PGE synthase, PGI� – prostacyclin, POB – perforation, ob-
struction and bleeding, PUB – perforation, ulceration and
bleeding, RA – rheumatoid arthritis, TARGET – Therapeutic
Arthritis Research and Gastrointestinal Event Trial, tid – tris
in die, TP – TXA� receptor, TX – thromboxane, TXAS –
thromboxane synthase, Val – valine, VIGOR – Vioxx Gastro-
intestinal Outcomes Research
66 �������������� ���� �� ����� ��� ������ ���
�������������� ���� �
����� ��� ������ ���
��� ���������
��������� � ����
�� �������� � !�"�#"$�����
!����� %$"&�#� � �$���$��

Prostanoid biosynthesis
Prostanoids are ubiquitous lipid mediators that may
modulate a wide variety of physiologic and patho-
logic processes [24]. Under physiologic conditions,
prostanoids play an important role in the cytoprotec-
tion of the gastric mucosa, hemostasis and renal he-
modynamics. Their biosynthesis is induced in differ-
ent pathologic conditions, including inflammation,
cancer, pain and fever [12, 66, 78]. Prostanoids are
formed by arachidonic acid (AA) through the coordi-
nate activity of three consecutive enzymatic steps
(Fig. 1) [26, 77, 79, 94]: (i) the release of AA from
membrane phospholipids by phospholipase(PLs)s,
primarily cytosolic PLA2� (cPLA2�), (ii) the trans-
formation of AA to prostaglandin (PG) G2 and then to
the unstable endoperoxide PGH2 by prostaglandin H
synthases [popularly known as cyclooxyge-
nase(COX)s (Fig. 1)] and (iii) its metabolization to
prostanoids, i.e. PGE2, PGF2�, PGD2, prostacyclin
(PGI2) and thromboxane (TX) A2 by terminal cell-
and tissue-specific synthases (Fig. 1). Since the early
1990s, two isoforms of COX have been identified,
COX-1 and COX-2 which are both glycoproteins and
are associated with the membranes of the endoplas-
matic reticulum and the nucleus [77]. Although the
genes for COX-1 and COX-2 are clearly different, the
proteins share about 60% homology at the amino acid
level, have a similar molecular mass of about 70 kD
and are identical in length. Studies of the tertiary
structures of COX isozymes have demonstrated that
the amino acid conformation for the substrate binding
sites and catalytic regions are almost identical [29,
67]. However, there are important differences in these
regions, particularly the exchange of Isoleucine (Ile)
in COX-1 for Valine (Val) in COX-2 at positions 434
and 523, respectively, which gives access to a side-
�������������� ���� �� ����� ��� ������ ��� 67
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��
Different physical, chemical
and hormonal stimuli
Different physical, chemical
and hormonal stimuli
Fig. 1. Pathway of prostanoid biosynthesis. Arachidonic acid (AA) is released from membrane phospholipids by phospholipases and is me-tabolized into prostaglandin (PG) H
�by the cyclooxygenase and peroxidase activity of COX-1 and COX-2, then PGH
�is converted into
prostanoids by tissue- and cell-specific isomerases. Once formed, prostanoids bind to their specific membrane-associated receptors whichbelong to the G-protein-coupled rhodopsin-type family. COX – cycloooxygenase activity; HOX – peroxidase activity

pocket in COX-2 channel. These substitutions result
in a larger and more flexible substrate channel in
COX-2 than in COX-1 and in the inhibitor binding
site in COX-2, being 25% larger than that in COX-1
[29, 67].
COX-1 gene exhibits the features of a “housekeep-
ing gene” and is constitutively expressed in virtually
all tissues, while COX-2 is an immediate early gene
with many regulatory sites which is induced in re-
sponse to different proinflammatory stimuli [26].
However, this simplified paradigm of constitutive
COX-1 and inducible COX-2, has many exceptions:
COX-1 can be regulated during development [69, 78],
whereas COX-2 is constitutively expressed in differ-
ent tissues, i.e. brain [108], kidney [22, 32], pancreas
[82], malignant [93] and vascular endothelial cells
[92]. Since both COX-1 and COX-2 are found in
rheumatoid arthritis (RA) synovium [13, 72], induced
in response to interleukin (IL)-1� and inhibited by
dexamethasone, in synovial cells isolated from RA
patients [58], it has been claimed the possible contri-
bution of COX-1 to prostanoid biosynthesis at inflam-
matory sites, in some circumstances. The plausibility
of this mechanism is upheld by the finding that mice
deficient in COX-1, but not COX-2, exhibit a reduc-
tion in the inflammatory response to the dermal appli-
cation of AA [42]. Furthermore, McAdam et al. have
reported time-dependent expression of COX-1 in
monocytes after lipopolysaccharide (LPS) administra-
tion to humans [50].
Recently, it has been suggested that there is another
COX enzyme formed as a splice variant of COX-1,
named COX-3 [9]. COX-3 is made from the COX-1
gene but retains intron 1 in its mRNA; it was initially
reported to be expressed in canine cerebral cortex and
in lesser amounts in other analyzed tissues [9]. In hu-
mans, COX-3 mRNA was found to be expressed as an
5.2 kb transcript that was most abundant in cerebral
cortex and heart. The difference at the protein level
between COX-3 and COX-1 is the insertion of 30–34
aminoacids, depending on the mammalian species,
into the hydrophobic signal peptide. In COX-3 this
signal peptide is not cleaved; the protein is glycosy-
lated and displays COX activity [9]. Although canine
COX-3 expressed by transfected insect cells can be
inhibited by therapeutic concentrations of analge-
sic/antipyretic drugs such as acetaminophen, phena-
cetin, antipyrine, and dipyrone, recently, it has been
reported that this COX-1 variant is not expressed in
human, rat or mouse as the corresponding additional
intron 1 sequence in the mRNA transcript spans 94
(human) or 98 (rat and mouse) nucleotides, thus shift-
ing the coding sequence out of frame [15, 75].
After the metabolization of AA to PGH2 by COX
isoenzymes, PGH2 is transformed into prostanoids by
terminal cell- and tissue-specific synthases (Fig. 1) [94].
At least four glutathione (GSH)-dependent forms
of PGE synthases (PGES), have been recently identi-
fied [51]: two membrane-bound forms of PGES
(mPGES-1 and mPGES-2) and two cytosolic forms of
PGES [cPGES and glutathione-S-transferase (GST)
µ]. mPGES-1 is a member of the membrane-
associated proteins involved in eicosanoid and GSH
metabolism (MAPEG) superfamily which requires
GSH as an essential cofactor for its activity [37, 53].
mPGES-1 is up-regulated in response to various stim-
uli and acts downstream of COX-2 for PGE2 genera-
tion [12, 23, 25, 46, 66, 79]. Stimulation of various
cultured cells with proinflammatory stimuli leads to
a marked elevation of mPGES-1 expression with
a concomitant elevation of COX-2 expression and
PGE2 production [12, 23, 25, 46, 66, 79]. The coordi-
nate up-regulation of COX-2 and mPGES-1 and at-
tendant PGE2 generation are simultaneously reversed
by glucocorticoids up to basal levels [46, 53]. How-
ever, the kinetic induction of COX-2 and mPGES-1
often differs significantly [84], suggesting distinct
regulatory mechanisms for their expression.
mPGES-2 was originally purified from bovine
heart [89]. It is a 41 kD protein that contains an
N-terminal hydrophobic region, which is removed by
proteolytic processing, and a catalytic region homolo-
gous to glutaredoxin/thioredoxin. Overall structure of
mPGES-2 is rather distinct from mPGES-1. mPGES-2
is activated by various SH-reducing reagents and is
expressed constitutively in several tissues in which
mPGES-1 expression is relatively low. mPGES-2 can
be coupled with both COX-1 and COX-2 [52].
cPGES is a 23 kD cytosolic protein that is identical
to the heat shock protein 90 (Hsp90) [90], which has
been originally implicated as a cofactor for the mo-
lecular chaperone function of Hsp90 [90]. cPGES re-
quires GSH as an essential cofactor for its activity
[33, 104]. cPGES is expressed ubiquitously and con-
stitutively in the cytosol of a variety of tissues and
cells, with an exception in rat brain in which LPS
treatment increases its amount several-fold [90]. Co-
transfection and antisense experiments indicate that
cPGES is capable of converting COX-1-, but not
COX-2- derived PGH2 to PGE2 in cells, particularly
68 �������������� ���� �� ����� ��� ������ ���

during the immediate PGE2-biosynthetic response
elicited by Ca2+-evoked stimulus [90].
Recently, two cytosolic forms of PGES, i.e. GST-µ2
and -µ3, have been identified from the cortex of human
brain [1]. Both of them catalyze the conversion of PGH2
to PGE2, but which COX isoform is preferentially
linked with GST-µ2 and -µ3 remains to be determined.
PGD synthase (PGDS) exists in both lipocalin-type
and hematopoietic forms. The lipocalin type is a ma-
jor constituent of the human cerebrospinal fluid
(CSF), representing 3% of total CSF protein [107].
The hematopoietic form produces PGD2 in cells such
as mast cells, basophils, and Th2 cells. PGD2 is fur-
ther dehydrated to produce PGJ2, delta12-PGJ2, and
15-deoxy-delta(12,14)-PGJ2, the last of which is a ligand
for the nuclear receptor peroxisome proliferator-
activated receptor (PPAR)-� [95].
PGF2� is synthesized via three pathways from
PGE2, PGD2, or PGH2 by PGE 9-ketoreductase, PGD
11-ketoreductase, or PGH 9-11-endoperoxide reduc-
tase, respectively [102]. Although there are no reports
of PGF synthase being inducible, its levels in the
uterus may increase during pregnancy associated with
the peak of PGF2� production that accompanies partu-
rition [105].
PGI2 is produced from PGH2 by the action of PGI
synthase, a member of the P450 superfamily [31], and
there are some reports of this being inducible [40].
Thromboxane synthase (TXAS), which forms
TXA2 from PGH2, was originally identified in plate-
lets [55]. The important regulation of thromboxane
synthase gene transcription appears to be via NF-E2.
Other cis elements of the thromboxane synthase gene
may also play important regulatory roles [101].
Prostanoid receptors
Once formed, prostanoids bind to specific
membrane-associated receptors (Fig. 1 and Tab. 1).
The first prostanoid receptor to be isolated and cloned
was the TXA2 receptor (TP) [36, 96] a G-protein-
coupled receptor with seven transmembrane domains.
Homology screening of cDNA libraries resulted in the
isolation and identification of seven other prostanoid
receptors that had been predicted pharmacologically:
the PGD receptor (DP), four PGE receptors (EP1,
EP2, EP3, EP4), the PGF receptor (FP) and the PGI
receptor (IP). These receptors are highly conserved in
mammals, with several splice variants of the EP3, FP
and TP receptors occurring [54]. PGD2 actually acts
both through DP and the chemoattractant receptor
CRTH2, which is preferentially expressed in T helper
2 (Th2) cells, eosinophils and basophils in humans
�������������� ���� �� ����� ��� ������ ��� 69
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��
Tab. 1. Signal trasduction of prostanoid receptors
Prostanoid Prostanoid receptor Receptor subtype Receptor Isoforms Receptor coupled G-protein Receptor Signaling
PGE� EP
EP1 Gq Ca���
EP2 Gs cAMP�
EP4 Gs cAMP�
EP3 EP�� Gi cAMP�
EP�� Gs cAMP�
EP�� Gs �cAMP
EP�� Gi, Gs �cAMP �cAMP
Gq �IP3
PGD� DP, CRTH2 Gs, Gi �cAMP �cAMP
PGF�� FP FP�, FP� Gq �IP3
PGI� IP Gs, Gq �cAMP �IP3
TXB� TP TP� Gi, Gq �cAMP �IP3
TP� Gs, Gq �cAMP �IP3

[35]. Prostanoid receptors are expressed in many tis-
sues and cell types. Among the EP receptors, EP3 and
EP4 are the most widely distributed, whereas EP1 and
EP2 distribution is restricted to the kidney, stomach
and uterus, as well as to neuronal and non-neuronal
cells in the nervous system [85]. EP1, EP3 and EP4
mRNAs are expressed in primary sensory neurons, in
the dorsal root and trigeminal ganglia [57, 86], sug-
gesting involvement in PGE2-mediated peripheral
sensitization. Inflammatory signals affect the expres-
sion levels of many prostanoid receptor subtypes [91].
The function of the prostanoid receptors varies ac-
cording to cell type, ligand concentration and structure
[54]. Although the limited number of available specific
EP receptor agonists and antagonists, as well as the
complex tissue distribution pattern and cellular signal-
ing of the receptors, has restricted elucidation of their
function, transgenic mice deficient in each prostanoid
receptor are proving to be a very useful tool [54].
Pharmacological modulation of
prostanoid biosynthesis
Aspirin and related nonsteroidal anti-inflammatory
drugs – which are collectively named traditional
NSAIDs (tNSAIDs) – are an heterogeneous group of
compounds widely prescribed as analgesics and anti-
inflammatory agents due to the inhibition of
prostanoid biosynthesis [98]. Their mechanism of ac-
tion includes inhibition of both the COX-1 and
COX-2 isoenzymes [24, 25, 41, 44, 66, 87]; the inhi-
bition of COX-2 is thought to translate into their
therapeutic effects (i.e. antipyretic, analgesic, and an-
tiinflammatory actions) while that of COX-1 has been
assumed to cause the gastrointestinal (GI) adverse
events. Thus, COX-2 inhibitors – named coxibs –
were developed with the aim to reduce the incidence
of serious GI adverse effects [i.e. ulceration, bleeding,
perforation and obstruction (PUBs and POBs)], asso-
ciated with the administration of tNSAIDs on the as-
sumption that they ensued as a consequence of the in-
hibition of cytoprotective COX-1-dependent prostanoids
in gastric epithelium and disruption of hemostatic in-
tegrity by inhibition of platelet COX-1 derived TXA2
[24, 25, 66, 87, 99]. In fact, COX-1 is the major COX
isoform expressed in platelets and gastric mucosa of
normal humans.
Most tNSAIDs are acidic and inhibit prostanoid
biosynthesis by competing with AA for the binding to
the Arginine (Arg) at position 120 that is present in
both COX-isozymes [47, 64]. They, first, bind both
PGHS-isozymes near the solvent-accessible opening
of the hydrophobic channel; then, they translocate
along the length of this channel and associate with the
cyclooxygenase active site by a reversible interaction.
A third additional step is involved in selective COX-2
inhibition by coxibs, i.e. the formation of a tightly
bound enzyme-inhibitor complex, which involves the
optimisation of inhibitor and protein conformational
changes in the active site and the side-pocket [64,
100]. Differently, aspirin causes an irreversible inacti-
vation of COX-1 activity [61, 70], through a selective
acetylation of Ser529 of human COX-1 which pre-
vents the access of the substrate AA to the catalytic
active site of the COX channel [29]. The acetylation
of COX-2 at Ser516 by aspirin modifies irreversibly
the catalytic activity of the enzyme which acquires the
70 �������������� ���� �� ����� ��� ������ ���
0
50
100
150
200
250
300
350
400
450
500
0.5 0.6 0.7
18 19 29 3061
272
344
1 1.5 1.6 1.9 3.1
433
CO
X-1
IC5
0
CO
X-2
IC5
0
Ibu
pro
fen
S-K
eto
pro
fen
Nap
roxe
n
Flu
rbip
rofe
n
6-M
NA
Ace
tam
ino
ph
en
Ind
om
eth
acin
Pir
oxi
cam
Mel
oxi
cam
Nim
esu
lide
Dic
lofe
nac
Cel
eco
xib
Val
dec
oxi
b
Ro
feco
xib
Eto
rico
xib
Lu
mir
aco
xib
NonselectiveNSAIDs
COX-2 inhibitors
coxibs
COXCOX--22 selectivityselectivity
–500.5 0.6 0.7
18 19 29 3061
272
344
1 1.5 1.6 1.9 3.1
433
50
Ibu
pro
fen
S-K
eto
pro
fen
Nap
roxe
n
Flu
rbip
rofe
n
6-M
NA
Ace
tam
ino
ph
en
Ind
om
eth
acin
Pir
oxi
cam
Mel
oxi
cam
Nim
esu
lide
Dic
lofe
nac
Cel
eco
xib
Val
dec
oxi
b
Ro
feco
xib
Eto
rico
xib
Lu
mir
aco
xib
NonselectiveNSAIDs
COX-2 inhibitors
coxibs
Ibu
pro
fen
S-K
eto
pro
fen
Nap
roxe
n
Flu
rbip
rofe
n
6-M
NA
Ace
tam
ino
ph
en
Ind
om
eth
acin
Pir
oxi
cam
Mel
oxi
cam
Nim
esu
lide
Dic
lofe
nac
Cel
eco
xib
Val
dec
oxi
b
Ro
feco
xib
Eto
rico
xib
Lu
mir
aco
xib
NonselectiveNSAIDs
NonselectiveNSAIDs
COX-2 inhibitors
coxibs
COXCOX--22 selectivityselectivity
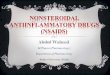
Fig. 2. The biochemical selectivity of cyclooxygenase inhibitors inwhole blood assays of COX-isozyme activity in vitro. The relative de-gree of isoform selectivity is expressed as COX-1/COX-2 IC
��ratios.
IC��
is the concentration of the drug required to inhibit the activity ofCOX-1 and COX-2 by 50%. The measurement of PGE
�production in
response to bacterial endotoxin (LPS) added to heparinised bloodsamples (for 24 h at 37�C) reflects the time-dependent induction ofCOX-2 in circulating monocytes, while the parallel measurement ofTXB
�production during whole blood clotting (for 1 h at 37�C) is used
as an index of platelet COX-1 activity. Nonselective COX inhibitors,profens and naproxen, exhibit COX-1/COX-2 IC
��ratios of 0.5–1.0.
COX-2 inhibitors, meloxicam, nimesulide, diclofenac, and the coxibscelecoxib, valdecoxib, rofecoxib, etoricoxib and lumiracoxib, showCOX-1/COX-2 IC
��ratios of 18–433

capacity to transform AA into 15R-hydroxyeicosatetra-
enoic acid but not PGG2 [43].
The assessment of COX-1/COX-2 selectivity in vi-
tro by the use of whole blood assays of the cellular ca-
pacity to produce prostanoids generated by one or
other enzyme [62] has evidenced that selectivity is
a continuous variable of COX inhibitors (Fig. 2) [66,
88]. However, they can be subdivided into two major
clusters: the nonselective NSAIDs which produce bal-
anced inhibition of both COX-1 and COX-2, as mir-
rored by profens – e.g. ibuprofen and flurbiprofen –
and naproxen, and COX-2 inhibitors which inhibit
more profoundly COX-2 vs. COX-1 and include me-
loxicam, nimesulide, diclofenac and coxibs (i.e. cele-
coxib, valdecoxib, rofecoxib, etoricoxib and lumira-
coxib) (Fig. 2). However, COX-1/COX-2 selectivity
assessed in vitro may fade in vivo in the light of de-
tectable intersubject variability in the inhibition of
COX-1 and COX-2 due to both pharmacokinetic (e.g.
polymorphisms of genes encoding metabolising en-
zymes) and/or pharmacodynamic variability (e.g. the
possible expression of variant isoforms of COX with
different sensitivity for inhibition by tNSAIDs and
coxibs) [66].
The first coxibs approved by Food and Drug Ad-
ministration (FDA) and European Medicines Agency
(EMEA) for the treatment of RA, osteoarthritis (OA)
and for relief of acute pain associated with dental sur-
gery and primary dysmenorrhea, rofecoxib and cele-
coxib, are diaryleterocyclic derivatives containing
a phenylsulphone and a phenylsulphonamide moiety
(Fig. 3), respectively, that interact with COX-2 side-
pocket, through slow, tight-binding kinetics [41, 66].
The two drugs display different COX-1/COX-2 IC50
ratios (IC50 is the concentration of the drug required
to inhibit the activity of COX-1 and COX-2 by 50%),
in the whole blood assays in vitro, i.e. 272 and 30, re-
spectively [87, 88]. The COX-1/COX-2 IC50 ratio of
rofecoxib detected in vitro translates into a specific in-
hibition of COX-2 when the drug is administered at
therapeutic doses and above [48]. Sparing of COX-1
is presumably involved in halving the incidence of GI
perforation, GI haemorrhage, or symptomatic peptic
ulcer in patients with RA treated with rofecoxib ver-
sus the nonselective NSAID naproxen in a large ran-
domized, double-blind GI outcomes study [the Vioxx
Gastrointestinal Outcomes Research (VIGOR) study]
[3]. In contrast, detectable inhibition of COX-1 by ce-
lecoxib at 800 mg/day [49] (i.e. 2-fold higher than the
maximal chronic dose recommended in RA) may
have contributed, at least in part, to its failure in re-
ducing the incidence of GI end-points versus diclofe-
nac or ibuprofen administered to OA patients, in the
Celecoxib Long-term Arthritis Safety Study (CLASS)
[76]. The fact that one comparator was the tNSAID
diclofenac, which shares pharmacodynamic traits
with celecoxib (Fig. 2), may have contributed in cele-
coxib failure. In fact, using the human whole blood
assays of COX isozyme activities in vitro the concen-
tration response-curves of diclofenac and celecoxib
are superimposable and have the same COX-1/COX-2
IC50 ratio values (i.e. 29 and 30, respectively) (Fig. 2).
Further evidences support the notion that diclofenac is
a celecoxib-like drug: i) diclofenac has no pharmaco-
dynamic interaction with aspirin similarly to the
COX-2 inhibitors rofecoxib and etoricoxib in healthy
subjects [8, 14] and no clinical interaction with aspi-
rin was detectable in the epidemiological study of
MacDonald and Wei [45]; ii) superimposition of the
gastrointestinal and cardiovascular events by diclofe-
nac and celecoxib was detected in the retrospective
look at CLASS in non-aspirin users [106].
Novel COX-2 inhibitors with improved biochemi-
cal selectivity over that of commercially available
coxibs, were developed, i.e. etoricoxib [5, 11], valde-
coxib [21], parecoxib (the prodrug of valdecoxib, it is
the only injectable COX-2 inhibitor) [10] and lumira-
coxib [16] (Fig. 3). They are characterized by differ-
ent pharmacodynamic and pharmacokinetics features
[87]. As reported by Tacconelli et al. [88], valdecoxib
inhibits platelet COX-1 and monocyte COX-2 activi-
ties with COX-1/COX-2 IC50 ratio of 60 which is
2-fold higher (p < 0.01) than that of celecoxib. Pare-
coxib, the water-soluble inactive prodrug of valde-
�������������� ���� �� ����� ��� ������ ��� 71
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��
H3C3C
Etoricoxib Lumiracoxib Valdecoxib
Rofecoxib Celecoxib
H3C3C
H3C3C
H3C3C
HO2
COOH
O
O
O
O
O
O
O
O
O
O
F
S
S
S S
N
NN
H3C
F3C
N
N N
H3C
NH
Cl
H2N
Fig. 3. Chemical structures of coxibs

coxib [10], is rapidly converted by hepatic enzymatic
hydrolysis to the active COX-2 inhibitor, valdecoxib,
thus sharing the same pharmacodynamic properties.
Etoricoxib (approved in Europe, Mexico, Brazil and
Peru while FDA has required additional safety and ef-
ficacy data) shows a COX-1/COX-2 IC50 ratio of 344
[88]. Finally, lumiracoxib (approved in UK but still
not approved by FDA) has peculiar pharmacody-
namic and pharmacokinetic features versus other
coxibs. In fact, it is characterized by the highest
COX-2 selectivity in vitro and the shortest half-life
(3–6 h). Using the whole blood assays, we have found
a COX-1/COX-2 IC50 ratio of 433 [59]. Unlikely
other coxibs, lumiracoxib is not a tricyclic compound,
its molecular phenyl acetic acid structure represents
an analogue of diclofenac (Fig. 3) [16].
Clinical efficacy
The results of several clinical trials demonstrate that
coxibs cause a similar clinical efficacy compared with
nonselective NSAIDs and that they are superior to
placebo in the treatment of OA, RA and acute pain
[i.e. primary dysmenorrhea and post-operative dental
pain [5, 10, 16, 21, 48, 60]. Differently from other
coxibs, etoricoxib has been approved also for the
treatment of chronic low-back pain and acute gouty
arthritis [2, 74]. Moreover, recent studies evidence the
efficacy of etoricoxib in patients with ankylosing
spondylitis [30, 97]. Finally, celecoxib is the only
coxib approved also for the treatment of familial ade-
nomatous polyposis (FAP) [83]. The main efficacy
studies of celecoxib, etoricoxib and lumiracoxib (i.e.
the commercially available coxibs) are listed in Ta-
bles 2–10.
Although the results of randomised clinical trials
have evidenced that coxibs have a similar efficacy
versus tNSAIDs, it has to be pointed out they were
designed to detect equivalence, not superiority, of ei-
ther. In fact, the low sensitivity of measurable efficacy
end-points would have required larger sample-size to
allow the detection of small differences in efficacy be-
tween coxibs and tNSAIDs which might reflect the
participation of COX-1-derived prostanoids in in-
flammation and pain [66]. Indeed, we have recently
evidenced that rofecoxib (50 mg daily) and diclofenac
(150 mg daily), administered for one week to patients
72 �������������� ���� �� ����� ��� ������ ���
placebo rofecoxib diclofenac–150
–100
–50
0
50
100
150
200
250
300
Syn
ovia
lfl
uid
PG
E2
%C
ha
ng
e
p = 0.010
placebo rofecoxib diclofenac–150
–100
–50
0
50
100
150
200
250
300
2000
4000
p < 0.001
Wh
ole
blo
od
LP
S-I
nd
uced
PG
E2
%C
ha
ng
e
p = 0.001
placebo rofecoxib diclofenac
–100
–50
0
50
100
150
–150
p = 0.005
p = 0.002
Seru
mT
XB
2
%C
ha
ng
e
n = 8 n = 8n = 9
A
B
C
Fig. 4. Effects of one-week oral dosing with placebo, rofecoxib ordiclofenac on synovial PGE
�levels and monocyte COX-2 and
platelet COX-1 activities ex vivo in RA patients. Patients with RA weregiven placebo, rofecoxib (50 mg/day) or diclofenac (50 mg tid) for 7consecutive days and blood was drawn 4 h after the last dose of thetwo drugs. (A) Synovial fluid samples, obtained 4 h after one weekoral dosing with the 3 treatments, were assessed for the levels ofPGE
�. (B) Heparinized whole blood samples, drawn 4 h after dosing
with placebo, rofecoxib or diclofenac, were incubated with LPS(10 µg/ml) for 24 h at 37�C and PGE
�levels were measured as an
index of monocyte COX-2 activity. (C) Whole blood samples, drawnwithout heparin 4 h after dosing with placebo, rofecoxib ordiclofenac, were immediately transferred into glass tubes, allowed toclot at 37�C for 60 min and serum was assayed for TXB
�as
a reflection of maximally stimulated cyclooxygenase activity ofplatelet COX-1 by endogenously formed thrombin. Results arereported as box and whiskers

with RA, at circulating concentrations causing a simi-
lar suppression of monocyte COX-2 activity ex vivo,
had a differential impact on synovial PGE2 levels (Pa-
trignani et al. unpublished results; Fig. 4 A, B). The
less consistent reduction of synovial PGE2 levels by
rofecoxib as compared to diclofenac may suggest the
contribution of COX-1 activity to PGE2 production in
chronic RA synovitis. In fact, differently from rofe-
coxib, diclofenac significantly inhibited platelet
COX-1 by 60% (Fig. 4C). The clinical relevance of
this observation should be verified in appropriate ran-
domised clinical trials.
Despite tNSAIDs and COX-2 inhibitors resulted
clinically efficacious for the relief of acute pain and
symptoms of arthropathies it has to be pointed out that
they failed to modify disease progression.
Safety and tolerability
GI safety profile
Three large-size clinical trials were performed to ver-
ify whether COX-1 sparing by celecoxib, rofecoxib
and lumiracoxib diminished the likelihood of serious
GI adverse effects versus tNSAIDs (i.e. ibuprofen and
naproxen, two balanced inhibitors of both COX-1 and
�������������� ���� �� ����� ��� ������ ��� 73
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��
Tab. 2. Clinical efficacy of celecoxib in AR and OA
Model ofacute pain
Primary end-points Treatments Results References
Rheumatoidarthritis
Improvement in signs andsymptoms of rheumatoidarthritis
Celecoxib 100, 200 or 400 mgbid, naproxen 500 mgbid for 12 weeks
All dosages of celecoxib and naproxensignificantly improved the signs andsymptoms of arthritis compared withplacebo
Simon LS et al.: JAMA,1999, 282, 1921–1928
Ostearthritisof knee or hip
WOMAC index, visual analoguepain scale, patient preferencebetween two treatments
Wash out, 6 weeks ofcelecoxib 200 mg/day,acetaminophen 1000 mg fourtimes a day, or placebo(study I); second “wash out”;crossover to 6 weeks ofsecond treatment (study II)
Celecoxib was more efficacious thanacetaminophen and placebo in bothperiods in both studies. Patientspreferred celecoxib to acetaminophen inboth studies
Pincus T et al.: AnnRheum Dis, 2004, 63,931–939
Patients were evaluated usingstandard measures of efficacyat baseline, 2–4 days afterdiscontinuing previous NSAIDor analgesic therapy, and after2, 6, and 12 weeks of treatment
Celecoxib 100, 200, or400 mg/day; naproxen1000 mg/day or placebo for12 weeks
All doses of celecoxib and naproxensignificantly improved the symptoms ofOA, at all time points compared withplacebo. This sustained treatment effectof celecoxib was dose dependent
Kivitz AJ et al.: J Int MedRes, 2001, 29, 467–479
WOMAC index (100-mm visualanalog scale [VAS])
Celecoxib 200 mg/day,rofecoxib 12.5 or 25 mg/day,or acetaminophen4000 mg/day for 6 weeks
Rofecoxib 25 mg, provided efficacyadvantages over acetaminophen,4000 mg, celecoxib 200 mg, androfecoxib 12.5 mg, for symptomaticknee OA
Geba GP et al.: JAMA,2002, 287, 64–71
Index joint pain by VAS,WOMAC index
Celecoxib 100 mg bid,diclofenac 50 mg tid orplacebo for 6 weeks
Primary efficacy measures indicatedstatistically significant improvementvs. placebo for both celecoxib anddiclofenac and no statisticallysignificant differences betweencelecoxib and diclofenac
McKenna F et al.: ScandJ Rheumatol, 2001, 30,11–18
Patients were evaluated withstandard measures of efficacy2 to 7 and after 2, 6, and
12 weeks of treatment withthe study drug
Celecoxib 50, 100, or 200 mgbid, naproxen 500 mg bid orplacebo for 12 weeks
All celecoxib doses were efficaciouscompared with placebo, although 50 mgwas minimally effective. Celecoxib(100 and 200 mg bid) were similarlyefficacious to naproxen
Bensen WG et al.: MayoClin Proc, 1999, 74,1095–1105

COX-2, and diclofenac, a drug that closely resembles
celecoxib in selectivity for COX-2; Fig. 2) [3, 73, 76].
Only for rofecoxib and lumiracoxib it was indeed
shown a lesser incidence of such serious GI adverse
effects compared to tNSAIDs [3, 73]. No such evi-
dence was provided for celecoxib [76]. Whether val-
decoxib is associated with reduced GI serious adverse
effects is unknown because its GI safety was extrapo-
lated from clinical efficacy trials [21]. Recently, re-
sults of a new large-size clinical study performed with
etoricoxib in patients with OA, known as the Etori-
coxib Diclofenac Gastrointestinal Evaluation (EDGE)
study, have been reported [17]. In this study, etori-
coxib significantly reduced the rate of discontinuation
by 50% due to gastrointestinal adverse events versus
diclofenac. However, there were essentially no differ-
ences between etoricoxib and diclofenac for GI perfo-
ration, ulceration or bleeding (PUBs), which are ex-
ploratory end points in this study. Failure of etori-
coxib to reduce the incidence of serious GI adverse
events versus diclofenac is plausibly related to the
fact that EDGE is an intra-class trial since both drugs
are COX-2 inhibitors. Despite etoricoxib has a higher
selectivity towards COX-2 in vitro than diclofenac,
74 �������������� ���� �� ����� ��� ������ ���
Tab. 3. Clinical efficacy of celecoxib in acute pain
Model ofacute pain
Primary end-points Treatments Results References
Post-operativedental pain
Totalpain relief score over 8 h(TOPAR8)
Celecoxib 200 or 400 mg,rofecoxib 50 mg, ibuprofen400 mg, or placebo
Rofecoxib 50 mg demonstratedsignificantly greater overall analgesicefficacy compared with celecoxib 400 mg.Time to onset of analgesic effect and peakanalgesic effect were similar for rofecoxib 50mg and celecoxib 400 mg
Malmstrom K et al.: Clin Ther,2002, 24, 1549–1560
TOPAR8 Single dose of celecoxib200 mg, rofecoxib 50 mg,ibuprofen 400 mg orplacebo
Compared with celecoxib, rofecoxib hadsuperior analgesic effects
Malmstrom K et al.: Clin Ther,1999, 21, 1653–1663
Orthopedicsurgery
Pain assessmentsconducted over thefollowing 8-h period
Celecoxib 200 mg,hydrocodone10 mg/acetaminophen 1000mg, or placebo within 24 hafter the end of anesthesia.Patients who had received <or =1 dose of rescuemedication during study Icontinued to take studymedication up to 3 times aday as needed
Patients with moderate to severe pain afterorthopedic surgery experiencedcomparable analgesia with single doses ofcelecoxib andhydrocodone/acetaminophen. Overa 5-day period, oral doses of celecoxib200 mg taken 3 times a day demonstrated
superior analgesia and tolerabilitycompared with hydrocodone10 mg/acetaminophen 1000 mg taken3 times a day
Gimbel JS et al.: Clin Ther,2001, 23, 228–241
Acuteshoulder pain
100-mm visual analogscale (VAS)
Celecoxib 400 mg/day vs.
naproxen 1 g/day for14 days
The difference in change from baseline atday 14 in maximum pain at rest was notstatistically significant
between the two treatment groups, but wasnumerically higher for celecoxib than fornaproxen
Bertin P et al.: J Int Med Res,2003, 31, 102–112
Acute shouldertendinitis/bursitis
Mean reduction inMaximum Pain Intensityat Rest, measured usinga 100 mm VAS, frombaseline to days7 and 14
Celecoxib 400 mg followedby 200 mg bid, naproxen500 mg bid, or placebo bid
for 14 days
Celecoxib showed comparable efficacy tonaproxen and superior to placebo inrelieving the pain of patients with acuteshoulder tendinitis and/or subacromialbursitis
Petri M et al.: J Rheumatol,2004, 31, 1614–1620

�������������� ���� �� ����� ��� ������ ��� 75
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��
Tab. 4. Clinical efficacy of parecoxib in postoperative acute pain
Model ofacute pain
Primary end-points Treatments Results References
Postoperativeinguinalhernia repair
Morphine consumption, pain atrest and while coughing, andpatient satisfaction throughoutthe first 12 h postoperatively
A single injection of 40 mgparecoxib or 2 injections of 2 gpropacetamol within the first12 h after surgery in patientsreceiving morphine
Patients in the parecoxib grouprated their pain management asgood or excellent (87% vs.
70% in the propacetamolgroup, p = 0.001). Within thefirst 12 h after inguinal herniarepair in adult patients, a singleinjection of parecoxib 40 mgcompares favorably with 2injections of propacetamol 2 g
Beaussier M et al.: AnesthAnalg, 2005, 100, 1309–1315
Postoperativegynecologiclaparotomysurgery
Total pain relief and patient’sglobal evaluation of studymedication and time to rescuemedication
A single dose of parecoxibsodium 40 mg im with singledoses of morphine 6 and12 mg im
Parecoxib sodium 40 mg im
demonstrated pain reliefstatistically similar to that withmorphine 12 mg im andsuperior to that with morphine6 mg im and a longer durationof action. Single-dose parecoxibsodium 40 mg providedsignificantly better painresponses to placebo ormorphine 4 mg and wascomparable to ketorolac 30 mg.Multiple-dose parecoxibsodium was comparable toketorolac, 4 times daily
Malan TP Jr et al: AnesthAnalg, 2005, 100, 454–460
Single-dose iv placebo,parecoxib sodium 20 mg or40 mg, ketorolac 30 mg, ormorphine 4 mg followed bymultiple-dose parecoxibsodium or ketorolac as needed
Bikhazi GB et al: Am J ObstetGynecol, 2004, 191,1183–1191
Postoperativehiparthroplasty
Cumulative morphine use Single iv dose of parecoxibsodium (20 or 40 mg) orplacebo together with iv
morphine 4 mg
Parecoxib sodium-treatedpatients used significantly lessmorphine over 24 and 6 h,compared to placebo
Malan TP Jr et al.:Anesthesiology, 2003, 98,950–956
Postoperativeorthopedicknee surgery
Pain relief Single iv dose of parecoxibsodium 20 and 40 mg,morphine 4 mg, and ketorolac30 mg
Parecoxib sodium 40 mg is aseffective as ketorolac 30 mgand is more effective thanmorphine 4 mg
Rasmussen GL et al.: AmJ Orthop, 2002, 31, 336–343
Oral surgery Pain intensity difference, timeto onset analgesia and time touse of rescue medication
Parecoxib sodium 20 mg im
20 mg iv, 40 mg im or 40 mg iv
vs. ketorolac tromethamine60 mg im or placebo
Parecoxib sodium 20 and40 mg im or iv and ketorolac60 mg im were significantlysuperior to placebo for allprimary end-points. The 40 mgdose was comparable toketorolac 60 mg on mostmeasures of analgesia but hada longer duration of action
Daniels SE et al.: Clin Ther,2001, 23, 1018–1031
Pain assessments at baselineand through 24 h postdose
Single im doses of parecoxib(1–20 mg) vs. ketorolactromethamine 30 mg im and vs.
placebo
Parecoxib 20 mg im is aneffective analgesic dose with anonset and magnitude
of analgesic effect approachingthat of ketorolac 30 mg im
Mehlisch DR et al.: J OralMaxillofac Surg, 2003, 61,1030–1037

76 �������������� ���� �� ����� ��� ������ ���
Tab. 5. Clinical efficacy of parecoxib in preoperative acute pain
Model of acute pain Primary end-points Treatments Results References
Preoperative laparoscopiccholecystectomy surgery
Length of stay in thepostanesthesia care unit,pain intensity, patientecovery after surgery andopioid-sparing efficacy
A single IV dose parecoxib 40 mgor placebo 30–45 min before theinduction of anesthesia. Six to12 h after the IV dose, theparecoxib group received a singleoral dose of valdecoxib 40 mg,followed by valdecoxib 40 mgonce daily on postoperative days1–4 and then 40 mg once daily asneeded on days 5–7
Patients in theparecoxib/valdecoxib groupwere significantly superiorto placebo for all primaryend-points
Gan TJ et al.: Anesth Analg,2004, 98, 1665–1673
Joshi GP et al.: Anesth Analg,2004, 98, 336–342
Preoperative orthopedicsurgery
Time to rescuemedication and painintensity
20-mg or 40-mg parecoxibsodium vs. placebo
Parecoxib sodium 20 and40 mg were superior toplacebo for all primaryend-points (significant for40-mg parecoxib sodiumvs. placebo)
Desjardins PJ et al.: J AmPediatr Med Assoc, 2004, 94,305–314
Preoperative oral surgery Time to rescuemedication, proportion ofpatients requiring rescuemedication, patientsglobal assessment andpain intensity
Single iv doses of parecoxibsodium (20, 40, and 80 mg)vs. placebo
For all primary end-points,all doses of parecoxibsodium were significantlysuperior to placebo. Therewere no significantdifferences between theparecoxib sodium 40 and80 mg groups
Desjardins PJ et al.: AnesthAnalg, 2001, 93, 721–727
Tab. 6. Clinical efficacy of etoricoxib in AR and OA
Model of acute pain Primary end-points Treatments Results References
Rheumatoid arthritis Patient global assessment ofdisease activity, investigatorglobal assessment of diseaseactivity, tender joint countand swollen joint count.
Etoricoxib 90 mg/day vs.
naproxen 500 mg bid vs.
placebo for 12-weeks
For all primary end-points,etoricoxib and naproxen werestatistically superior to placebo
In the second study, etoricoxibwas significantly superior tonaproxen and placebo
Collantes E et al.: BMC FamPract, 2002, 3, 10
Matsumoto AK et al.:J Rheumatol, 2002, 29,1623–1630
Ostearthritis of kneeor hip
WOMAC pain and physicalfunction subscales 100 mmVAS and patient’s globalassessment of disease status
Etoricoxib 30 mg/day vs.
ibuprofen 800 mg tid, andvs. placebo
Both etoricoxib and ibuprofenwere statistically superior toplacebo for all primary end-points
Wiesenhutter CW et al.:Mayo Clin Proc, 2005, 80,470–479
Etoricoxib 60 mg/day vs.
placebo or diclofenac 50 mgtid for 6-weeks
Etoricoxib was comparable inefficacy to diclofenac on all theparameters. The onset ofclinical benefit with etoricoxibon day one is more rapid thanthat of diclofenac
Zacher J et al.: Curr Med ResOpin, 2003, 19, 725–736
In Part 1 (6 weeks), patientsreceived
placebo, etoricoxib 5, 10, 30,60 or 90 mg/day. In Part 2(8 weeks), patients
received etoricoxib 30, 60 or90 mg/day or diclofenac50 mg tid
At 6 weeks, all the doses ofetoricoxib had
clinical efficacy superior toplacebo. Maximal efficacy wasseen with 60 mg. In Part 2,etoricoxib 30, 60 and 90 mgwere generally similar todiclofenac
Gottesdiener K et al.:Rheumatology, 2002, 41,1052–1061

the drug might cause detectable inhibition of COX-1
in vivo in some patients due to intersubject variability
in the inhibition of COX-isozymes [66].
Cardiovascular profile of COX-2 inhibitors and
tNSAIDs
An increased incidence of myocardial infarction and
stroke was detected in 5 placebo controlled trials in-
volving the COX-2 inhibitors celecoxib, rofecoxib
and valdecoxib [80, 106]. In the VIGOR trial, a study
of approximately 8000 patients with RA randomized
to receive the specific COX-2 inhibitor rofecoxib
(50 mg/day) or naproxen (500 mg bid) with a mean
duration of follow-up of 9 months, the rates of myo-
cardial infarction significantly exceeded by 5-fold in
rofecoxib-treated group [3]. This is only partly ex-
plained by a possible cardioprotective effect of
naproxen. In fact, Capone et al. [6] have found that
even within the context of a controlled and well moni-
tored study, the chronic administration of naproxen
500 mg bid gets into the functionally relevant range,
i.e. > 95% inhibition of platelet COX-1 activity ex
vivo at the end of the dosing interval, in some but not
all subjects studied. This is coherent with the hetero-
geneous results of several epidemiologic studies
which have been performed to establish the possible
antithrombotic effect of this drug [106]. Rofecoxib
has now been withdrawn from the market by Merck,
following premature cessation of the APPROVe
(Adenomatous Polyp Prevention on Vioxx ) study –
designed to seek an impact on benign sporadic colo-
nic adenomas – by its Data Safety and Monitoring
Board [4]. This action was taken because of a highly
significant 1.9 – fold increase in the incidence of
thromboembolic serious adverse events on rofecoxib
25 mg/day compared with placebo. Blood pressure
was elevated early in the rofecoxib group, but the in-
cidence of myocardial infarction and thrombotic
stroke began to diverge progressively between the
groups after a year of treatment [4]. The public an-
nouncement of the APPROVe results, which coin-
cided with Merck’s withdrawal of rofecoxib from the
market in September 2004, prompted scientists to re-
view the cardiovascular-safety results of a similar
trial, the Adenoma Prevention with Celecoxib (APC)
study [81]. At either 200 or 400 mg bid, celecoxib in
the APC trial was associated with a tripling of the risk
of cardiovascular events (relative risk, 2.8; 95% con-
fidence interval, 1.3 to 6.3) [81]. Finally, the results of
trials in patients undergoing coronary artery bypass
grafting (CABG) treated with aspirin, have shown an
increased risk of cardiovascular events in patients re-
ceiving valdecoxib or its intravenous formulation,
parecoxib [28, 56]. On April 7, 2005, the maker of
valdecoxib, Pfizer, announced that it has voluntarily
�������������� ���� �� ����� ��� ������ ��� 77
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��
Tab. 7. Clinical efficacy of etoricoxib in acute gouty arthritis and ankylosing spondylitis
Model of acute pain Primary end-points Treatments Results References
Acute gouty arthritis Patients’ assessment of painin the study joint (0–4-pointLikert scale) over days 2–5
Etoricoxib, 120 mg/day vs.
indomethacin, 50 mg tid for8 days
Both treatment groupsexperienced comparablepain relief over the entiretreatment period
Rubin BR et al.: ArthritisRheum, 2004, 50, 598–606
Schumacher HR Jr et al.:BMJ, 2002, 324, 1488–1492
Ankylosing spondylitis Patient’s assessment ofspinepain, patient’s globalassessment of diseaseactivity, and the BathAnkylosingSpondylitis FunctionalIndex
Etoricoxib 90 mg or120 mg/day vs. Naproxen500 mg bid vs. placebo for6 weeks (part I) and then vs.
naproxen 500 mg bid for other46 weeks
For all primary end-points,both doses of etoricoxibwere statistically superior toplacebo over 6 weeks.At the end of the 52-weektreatment period, bothetoricoxib dosesdemonstrated greatertreatment effects comparedwith naproxen, for allprimary end-points
van der Heijde et al.:Arthritis Rheum, 2005, 52,1205–1215
Time-weighted averagechange from baseline ofspine pain intensity
Etoricoxib 90 mg or120 mg/day vs. Naproxen500 mg bid vs. placebo for6 weeks
Etoricoxib and naproxenwere significantly superior toplacebo
Gossec L et al.: Ann RheumDis, 2005, (Epub ahead ofprint)

stopped the sales of the drug. This action was taken
after the FDA concluded that the risk of serious side
effects from taking valdecoxib outweigh the benefits
received from the treatment.
In the Therapeutic Arthritis Research and Gastroin-
testinal Event Trial (TARGET) study, comparing lu-
miracoxib (400 mg/day) with naproxen (500 mg bid)
and ibuprofen (400 mg tid) for one year in OA patients
mostly at low-risk of vascular events, the numbers of
events was small, but the relative risk in non-aspirin us-
ers was 1.47, although it did not attain significance [20].
Recently, the clinical study EDGE [17] has as-
sessed the cardiovascular safety of etoricoxib versus
diclofenac as secondary end-point. In the EDGE
study comparable rates of thrombotic cardiovascular
events were detected. Rates of discontinuation due to
hypertension-related adverse effects were higher on
etoricoxib than diclofenac.
An apparent increased incidence of myocardial in-
farction has been detected in users of tNSAIDs in
a recent observational study [34]. However, long-term
prospective, controlled clinical trials are required to
78 �������������� ���� �� ����� ��� ������ ���
Tab. 8. Clinical efficacy of etoricoxib in acute pain
Model of acutepain
Primary end-points Treatments Results References
Acute pain:post-operativedental pain
Total pain relief
over 6 h (TOPAR6)
Etoricoxib 120 mg, vs. oxycodone/acetaminophen 10 mg/650 mg vs.
codeine/ acetaminophen 60 mg/ 600mg and vs. placebo
Etoricoxib 120 mg vs. Oxycodone/acetaminophen 10/650 mg vs.
placebo
Etoricoxib demonstratedsignificantly greater overallanalgesic efficacy vs.
oxycodone/ acetaminophen andcodeine/acetaminophen Allactive treatments were superiorto placeboActive treatments werestatistically significantly superiorto placebo for all efficacymeasures. Total pain relief over 6h for etoricoxib was significantlymore than foroxycodone/acetaminophen
Malmstrom K et al.: Curr MedRes Opin, 2005, 21, 141–149
Chang DJ et al.: Anesth Analg,2004, 99, 807–815
Total pain relief over8 h (TOPAR8)
Etoricoxib 60, 120, 180, and 240 mgvs. placebo and vs. ibuprofen 400 mg
Etoricoxib 120 and 180 mg weresuperior to etoricoxib 60 mg andibuprofen
Etoricoxib 120 mg vs. placebo vs.
naproxen sodium 550 mg and vs.
Acetaminophen/codeine600/60 mg
Etoricoxib 120 mg wassignificantly superior to placeboand acetaminophen/codeine600/60 mg and similar tonaproxen sodium
Malmstrom K et al.: Clin Ther,2004, 26, 667–679
Malmstrom K et al.: Clin J Pain,2004, 20, 147–155
Acute pain:primarydysmenorrhea
TOPAR8 Etoricoxib 120 mg vs. placebo,naproxen sodium 550 mg vs. placeboover the course of 3 consecutivecycles
The TOPAR8 score for etoricoxiband naproxen were significantlygreater than that of placebo
Malmstrom K et al.: GynecolObstet Invest, 2003, 56, 65–69
Chronic lowback-pain
Assessment of lowback-pain intensityscale (0 to 100 mmVAS) over 4 weeksof treatmet
Etoricoxib 60 mg or 90 mg incomparison to placebo over12 weeks
Etoricoxib 60 or 90 mg/dayprovided clinical efficacysignificantly superior to placebo,which was observed as early asone week after initiatingtreatment, was maximal at4 weeks and was stablymaintained over 3 months
Pallay LM et al.: Scand J Rheumatol,2004, 33, 257–266
Birbara CA et al.: J Pain, 2003,4, 307–315

�������������� ���� �� ����� ��� ������ ��� 79
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��
Tab. 9. Clinical efficacy of lumiracoxib in AR and OA
Model of acute pain Primary end-points Treatments Results References
Rheumatoid arthritis American College ofrheumatology 20%improvement (ACR20%) atweek 13
Lumiracoxib 200 or400 mg/day vs. naproxen500 mg bid vs. placebo for26 weeks
Lumiracoxib was significantlysuperior to placebo
Geusens P et al.: Int J ClinPract, 2004, 58, 1033–1041
Ostearthritis of kneeor hip
WOMAC total score andpatient’s global assessmentof disease activity
Lumiracoxib 100 mg/day,lumiracoxib 100 mg/day witha loading dose of 200 mg/dayfor the first two weeks,celecoxib 200 mg/day, orplacebo for 13 weeks
All active treatments weresuperior to placebo for allco-primary variables. Nosignificant differences wereobserved between any activetreatments
Lehmann R et al.: Curr MedRes Opin, 2005, 21, 517–526
WOMAC total score, patient’sglobal assessment of diseaseactivity and pain intensity inthe target knee
Lumiracoxib 100 mg/day,lumiracoxib 100 mg/day witha loading dose of lumiracoxib200 mg/day for the first2 weeks, celecoxib 200 mg/day,or placebo for 13 weeks
Lumiracoxib was superior toplacebo and similar tocelecoxib on all primaryefficacy variables. Nosignificant differences wereseen between the lumiracoxibgroups at any time point.
Sheldon E et al.: Clin Ther,2005, 27, 64–77
Overall joint pain intensityand WOMAC score
Lumiracoxib 50, 100, or200 mg bid or 400 mg/day,Placebo or diclofenac 75 mgbid for 4 weeks
All lumiracoxib doses weresuperior to placebo andsimilar to diclofenac
Schnitzer TJ et al.: ArthritisRheum, 2004, 51, 549–557
Ostearthritis of hand Overall OA pain intensity(VAS mm) in the target hand
Lumiracoxib 200 or400 mg/day or placebo for4 weeks
Lumiracoxib doses weresuperior to placebo. Nosignificant differences wereseen between the lumiracoxibgroups
Grifka JK et al.: Clin ExpRheumatol, 2004, 22,589–596
Tab. 10. Clinical efficacy of lumiracoxib in acute pain
Model of acute pain Primary end-points Treatments Results References
Acute pain: primarydysmenorrhea
Summed pain intensitydifference from 0 to 8 hon day 1 (SPID-8)
Lumiracoxib 400 mg/day,rofecoxib 50 mg/day andplacebo (Study 1);lumiracoxib 400 mg/day,naproxen 500 mg bid andplacebo (Study 2)
All active treatments werestatistically superior toplacebo in each study;lumiracoxib was comparableto rofecoxib and naproxen
Bitner M et al.: Int J ClinPract, 2004, 58, 340–345
Acute pain:post-operativedental pain
Pain intensity difference over12 h
Single oral dose oflumiracoxib 100 or 400 mg,ibuprofen 400 mg andplacebo
Lumiracoxib 400 mg andibuprofen were superior toplacebo from 1 to 12 h postdose while lumiracoxib100 mg was superior from1.5 to 9 h.
Zelenakas K et al.: Int J ClinPract, 2004, 58, 251–256
Summed pain intensitydifference over the first 8 hpost dose (SPID-8)
Single oral doses oflumiracoxib 400 mg,rofecoxib 50 mg, celecoxib200 mg or placebo
Lumiracoxib demonstratedthe fastest onset of analgesiaand the longest time torescue medication use.Patient global evaluation oflumiracoxib was comparableto rofecoxib and superior tocelecoxib and placebo
Kellstein D et al.: Int J ClinPract, 2004, 58, 244–250

adequately assess the potential risk of serious adverse
cardiovascular events associated with tNSAIDs.
A plausible mechanism in cardiovascular
hazard by COX-2 inhibition
PGI2 and TXA2, the major products of AA metabo-
lism in endothelial cells and platelets, respectively, act
a leading role in cardiovascular homeostasis [24]. The
individual cardiovascular effects of PGI2 in vitro con-
trast with those of TXA2. An unbalanced biosynthesis
of these mediators seems to play a role in atherogene-
sis and thrombosis. However, it should be pointed out
that PGI2 may counteract any other agonist with simi-
lar biological effects to TXA2.
Platelet TXA2 causes the propagation of the initial
activation signal to adjacent platelets, by inducing
further platelet activation and TXA2 formation [63].
TXA2 is also a potent trigger of vascular smooth mus-
cle cell contraction and proliferation and it has been
recently shown to be a mediator of endothelial migra-
tion and angiogenesis. The importance of TXA2 is
highlighted by the efficacy of low-dose aspirin,
a platelet COX-1 inhibitor [6, 61], in prevention of
myocardial infarction and stroke [65].
Studies in vitro and in vivo in humans have shown
that COX-2 is the major COX isoform that contrib-
utes to endothelial PGI2 biosynthesis [7, 49, 92]. PGI2
potently inhibits aggregation of platelets induced by
all recognized agonists, vascular smooth muscle cell
proliferation and vascular tone in vitro and in vivo,
leukocyte-endothelial cell interactions and cholesteryl
ester hydrolase [25]. Recently, it has been reported an
antioxidant role for PGI2 through the induction of
hemoxygenase-1 [18]. For these manifold biological
effects, PGI2 mirrors the features of an atheroprotec-
tive mediator. The use of mice deficient in PGI2 re-
ceptor or TXA2 receptor has unravelled unambigu-
ously that TXA2 promotes and PGI2 prevents the ini-
tiation and progression of atherogenesis through
control of platelet activation and leukocyte-endothelial
cell interaction [19, 39].
Egan et al. [18] have recently found in mice that es-
trogen acts via its ERa receptor to upregulate COX-2-
dependent PGI2 formation. The vascular benefit of es-
trogen therapy in ovariectomized mice rendered prone
to atherogenesis was faded by IP receptor deletion.
This finding suggests that PGI2 inhibition by COX in-
hibitors might counteract the cardiovascular benefit of
endogenous and exogenous estrogens.
Recent findings suggest that COX-2 is involved in
the biosynthesis of renal vasodilatatory prostanoids.
In fact, COX-2 inhibitors or gene knockout dramati-
cally augment the pressor effect of angiotensin II [68].
Consistently, deletion of IP and EP2 – the receptors
for COX-2-derived prostanoids, PGI2 and PGE2 –
also results in elevation of blood pressure [38, 103].
Rudic et al. [71] have found that COX-2-derived
PGI2 also controls the changes that occur in the mus-
cular lining of blood vessels in response to pressure-
related changes in blood flow. Recently, Francois et
al. [27] have reported that mice lacking IP receptor [IP
knockouts (IPKOs)] develop salt-sensitive hyperten-
sion, cardiac hypertrophy, and severe cardiac fibrosis.
Coincidental deletion of TP receptor does not prevent
the development of hypertension, but cardiac hypertro-
phy is ameliorated and fibrosis is prevented in IPTP dou-
ble knockouts (DKOs). These results may suggest that
suppression of TXA2 with low-dose aspirin could reduce
the risk of heart disease if taking COX-2 inhibitors.
Overall these findings, in mice, suggest that during
prolonged dosing with COX-2 inhibitors, inhibition
of PGI2 may lead to several consequences – a rise in
blood pressure, initiation, and early development of
atherosclerosis, and the architectural and functional
response of blood vessels to such stress – which may
predispose individuals to an exaggerated thrombotic
response upon rupture of an atherosclerotic plaque.
Plaque rupture and subsequent thrombotic vascular
occlusion are the most deleterious sequelae of atheroscle-
rosis, underlying most fatal myocardial infarctions and
thromboembolic strokes. Recently, in Apobec-1/LDLR
DKO mice, it has been found that inhibition of systemic
PGI2 by a selective COX-2 inhibitor, in combination
with the TP antagonist S18886, was associated with the
induction of a vascular phenotype characteristic of an
unstable plaque, i.e. lost of vascular muscle smooth
cells in the fibrous cap of atherosclerotic lesion [19].
Conclusions
It is now unambiguously recognized that the in-
creased thrombotic risk associated with the admini-
stration of COX-2 inhibitors is a class effect. In fact,
80 �������������� ���� �� ����� ��� ������ ���

all these drugs inhibit PGI2 leaving unconstrained
TXA2 and any agonist with similar biological fea-
tures. The cardiovascular risk seems dose-dependent;
it is not simply associated with COX-2 selectivity, but
drug exposure (half-life and duration of dosing) plays
an important role. Furthermore, the hazard would be
expected to relate to clinical substrate (cardiovascular
risk). Finally, differences between individuals are
probably involved. Further studies should be per-
formed for the identification of characteristics of pa-
tients that are making them susceptible to cardiovascu-
lar adverse effects by selective COX-2 inhibitors. In
the meantime, the use of these drugs have to be under
scrutiny particularly in cardiovascular risk-population.
The EMEA has recommended a number of restric-
tions on use of all selective COX-2 inhibitors com-
mercially available (celecoxib, etoricoxib and pare-
coxib). They are now contra-indicated in patients with
established ischemic heart disease and/or cerebrovas-
cular disease (stroke), and also in patients with pe-
ripheral arterial disease and they should be prescribed
with caution in patients with risk factors for heart dis-
ease, such as hypertension, hyperlipidemia, diabetes
and smoking. They should be used in the lowest effec-
tive dose for the shortest possible period. Despite,
long-term controlled clinical trial data are not available
to adequately assess the potential risk of serious ad-
verse cardiovascular events associated with tNSAIDs,
FDA has extended the same restrictions to these drugs.
The future of coxibs may be an example of person-
alized medicine since the goal is to restrict their use in
people who really need them, i.e. who do not respond
to tNSAIDs or with increased risk of GI complica-
tions. Selective COX-2 inhibitors remain an appropri-
ate choice in patients at low cardiovascular risk but
with increased risk of GI complications.
Acknowledgments:
We wish to thank the collaboration of Drs Moreland LM, Chatham
WW, Punzi L, Todesco S, Riente L, Bombardieri S, Amin AR, Lee S,
Abramson S and Patrono C for the performance of the study on RA
patients treated with rofecoxib and diclofenac who was supported
by a grant from Merck & Co. The authors of the present review
article report no conflict of interest/relationship with any manufacturer
of COX-2 inhibitors or NSAIDs.
References:
1. Beuckmann CT, Fujimori K, Urade Y, Hayaishi O: Iden-
tification of mu-class glutathione transferases M2-2 and
M3-3 as cytosolic prostaglandin E synthases in the hu-
man brain. Neurochem Res, 2000, 25, 733–738.
2. Birbara CA, Puopolo AD, Munoz DR, Sheldon EA,
Mangione A, Bohidar NR, Geba GP: Etoricoxib Protocol
042 Study Group: Treatment of chronic low back pain
with etoricoxib, a new cyclo-oxygenase-2 selective in-
hibitor: improvement in pain and disability – a ran-
domized, placebo-controlled, 3-month trial. J Pain, 2003,
4, 307–315.
3. Bombardier C, Laine L, Reicin A, Shapiro D, Burgos-
Vargas R, Davis B, Day R et al., VIGOR Study Group:
Comparison of upper gastrointestinal toxicity of rofe-
coxib and naproxen in patients with rheumatoid arthritis.
VIGOR Study Group. N Engl J Med, 2000, 343, 1520–1528.
4. Bresalier RS, Sandler RS, Quan H, Bolognese JA, Oxen-
ius B, Horgan K, Lines C et al.: Adenomatous Polyp Pre-
vention on Vioxx (APPROVe) Trial Investigators. Car-
diovascular events associated with rofecoxib in a colo-
rectal adenoma chemoprevention trial. N Engl J Med,
2005, 352, 1092–1102.
5. Capone ML, Tacconelli S, Patrignani P: Clinical pharma-
cology of etoricoxib. Expert Opin Drug Metab Toxicol,
2005, 1, 269–282.
6. Capone ML, Tacconelli S, Sciulli MG, Grana M, Ricci-
otti E, Minuz P, Di Gregorio P et al.: Clinical pharmacol-
ogy of platelet, monocyte, and vascular cyclooxygenase
inhibition by naproxen and low-dose aspirin in healthy
subjects. Circulation, 2004, 109, 1468–1471.
7. Catella-Lawson F, McAdam B, Morrison BW, Kapoor S,
Kujubu D, Antes L, Lasseter KC et al.: Effects of spe-
cific inhibition of cyclooxygenase-2 on sodium balance,
hemodynamics, and vasoactive eicosanoids. J Pharmacol
Exp Ther, 1999, 289, 735–741.
8. Catella-Lawson F, Reilly MP, Kapoor SC, Cucchiara AJ,
DeMarco S, Tournier B, Vyas SN et al.: Cyclooxygenase
inhibitors and the antiplatelet effects of aspirin. N Engl
J Med, 2001, 345, 1809–1817.
9. Chandrasekharan NV, Dai H, Roos KL, Evanson NK,
Tomsik J, Elton TS, Simmons DL: COX-3, a cyclooxy-
genase-1 variant inhibited by acetaminophen and other
analgesic/antipyretic drugs: cloning, structure, and ex-
pression. Proc Natl Acad Sci USA, 2002, 99, 13926–13931.
10. Cheer SM, Goa KL: Parecoxib (parecoxib sodium).
Drugs, 2001, 61, 1133–1141; discussion 1142–1143.
11. Cochrane DJ, Jarvis B, Keating GM: Etoricoxib. Drugs,
2002, 62, 2637–2651; discussion 2652–2653.
12. Crofford LJ: COX-1 and COX-2 tissue expression: im-
plications and predictions. J Rheumatol, 1997, 49, 15–19.
13. Crofford LJ, Wilder RL, Ristimaki AP, Sano H,
Remmers EF, Epps HR, Hla T: Cyclooxygenase-1 and -2
expression in rheumatoid synovial tissues. Effects of
interleukin-1 beta, phorbol ester, and corticosteroids.
J Clin Invest, 1994, 93, 1095–1101.
14. Dallob A, Hawkey CJ, Greenberg H, Wight N, De Schep-
per P, Waldman S, Wong P et al.: Characterization of eto-
ricoxib, a novel, selective COX-2 inhibitor. J Clin Phar-
macol, 2003, 43, 573–585.
15. Dinchuk JE, Liu RQ, Trzaskos JM: COX-3: in the wrong
frame in mind. Immunol Lett, 2003, 86, 121.
�������������� ���� �� ����� ��� ������ ��� 81
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��

16. Doggrell SA: The safety of lumiracoxib when used in the
treatment of arthritis. Expert Opin Pharmacother, 2005,
6, 347–350.
17. EDGE trial; www.fda.gov/ohrms/dockets/ac/05/brief-
ing/2005-4090B2_01_Merck-Etoricoxib.pdf
18. Egan KM, Lawson JA, Fries S, Koller B, Rader DJ,
Smyth EM, FitzGerald GA: COX-2-derived prostacyclin
confers atheroprotection on female mice. Science, 2004,
306, 1954–1957.
19. Egan KM, Wang M, Fries S, Lucitt MB, Zukas AM,
Pure E, Lawson JA et al.: Cyclooxygenases, thrombox-
ane, and atherosclerosis: plaque destabilization by
cyclooxygenase-2 inhibition combined with thrombox-
ane receptor antagonism. Circulation, 2005, 111, 334–342.
20. Farkouh ME, Kirshner H, Harrington RA, Ruland S,
Verheugt FW, Schnitzer TJ, Burmester GR et al.,
TARGET Study Group: Comparison of lumiracoxib with
naproxen and ibuprofen in the Therapeutic Arthritis Re-
search and Gastrointestinal Event Trial (TARGET), car-
diovascular outcomes: randomised controlled trial. Lan-
cet, 2004, 364, 675–684.
21. Fenton C, Keating GM, Wagstaff AJ: Valdecoxib: a re-
view of its use in the management of osteoarthritis, rheu-
matoid arthritis, dysmenorrhoea and acute pain. Drugs,
2004, 64, 1231–1261.
22. Ferreri NR, An SJ, McGiff JC: Cyclooxygenase-2 ex-
pression and function in the medullary thick ascending
limb. Am J Physiol, 1999, 277, F360–F368.
23. Filion F, Bouchard N, Goff AK, Lussier JG, Sirois J:
Molecular cloning and induction of bovine prostaglandin
E synthase by gonadotropins in ovarian follicles prior to
ovulation in vivo. J Biol Chem, 2001, 276, 34323–34330.
24. FitzGerald GA: COX-2 and beyond: Approaches to pros-
taglandin inhibition in human disease. Nat Rev Drug
Discov, 2003, 2, 879–890.
25. FitzGerald GA, Patrono C: The coxibs, selective inhibi-
tors of cyclooxygenase-2. N Engl J Med, 2001, 345,
433–442.
26. Fitzpatrick FA, Soberman R: Regulated formation of ei-
cosanoids. J Clin Invest, 2001, 107, 1347–1351.
27. Francois H, Athirakul K, Howell D, Dash R, Mao L,
Kim HS, Rockman HA et al: Prostacyclin protects against
elevated blood pressure and cardiac fibrosis. Cell Metab,
2005, 2, in press.
28. Furberg CD, Psaty BM, FitzGerald GA: Parecoxib, val-
decoxib, and cardiovascular risk. Circulation, 2005, 111,
249.
29. Garavito RM, Mulichak AM: The structure of mammal-
ian cyclooxygenases. Annu Rev Biophys Biomol Struct,
2003, 32, 183–206.
30. Gossec L, van der Heijde D, Melian A, Krupa DA,
James MK, Cavanaugh Jr PF, Reicin AS et al.: The effi-
cacy of cyclooxygenase-2 inhibition by etoricoxib and
naproxen on the axial manifestations of ankylosing spon-
dylitis in the presence of peripheral arthritis. Ann Rheum
Dis, 2005, Epub ahead of print.
31. Hara S, Miyata A, Yokoyama C, Inoue H, Brugger R,
Lottspeich F, Ullrich V et al.: Isolation and molecular
cloning of prostacyclin synthase from bovine endothelial
cells. J Biol Chem, 1994, 269, 19897–19903.
32. Harris RC, Breyer MD: Physiological regulation of
cyclooxygenase-2 in the kidney: Am J Physiol Renal
Physiol, 2001, 281, F1–11.
33. Hernandez MP, Sullivan WP, Toft DO: The assembly and
intermolecular properties of the hsp70-Hop-hsp90 mo-
lecular chaperone complex. J Biol Chem, 2002, 277,
38294–38304.
34. Hippisley-Cox J, Coupland C: Risk of myocardial infarc-
tion in patients taking cyclo-oxygenase-2 inhibitors or
conventional non-steroidal anti-inflammatory drugs:
population based nested case-control analysis. BMJ,
2005, 330, 1366.
35. Hirai H, Tanaka K, Yoshie O, Ogawa K, Kenmotsu K,
Takamori Y, Ichimasa M et al.: Prostaglandin D2 selec-
tively induces chemotaxis in T helper type 2 cells, eosi-
nophils, and basophils via seven-transmembrane receptor
CRTH2. J Exp Med, 2001, 193, 255–261.
36. Hirata M, Hayashi Y, Ushikubi F, Yokota Y, Kageyama
R, Nakanishi S, Narumiya S: Cloning and expression of
cDNA for a human thromboxane A2 receptor. Nature,
1991, 349, 617–620.
37. Jakobsson PJ, Thoren S, Morgenstern R, Samuelsson B:
Identification of human prostaglandin E synthase: a mi-
crosomal, glutathione-dependent, inducible enzyme, con-
stituting a potential novel drug target. Proc Natl Acad Sci
USA, 1999, 96, 7220–7225.
38. Kennedy CR, Zhang Y, Brandon S, Guan Y, Coffee K,
Funk CD, Magnuson MA et al.: Salt-sensitive hyperten-
sion and reduced fertility in mice lacking the prostaglan-
din EP2 receptor. Nat Med, 1999, 5, 217–220.
39. Kobayashi T, Tahara Y, Matsumoto M, Iguchi M, Sano
H, Murayama T, Arai H et al.: Roles of thromboxane
A(2) and prostacyclin in the development of atheroscle-
rosis in apoE-deficient mice. J Clin Invest, 2004, 114,
784–794.
40. Korita D, Sagawa N, Itoh H, Yura S, Yoshida M, Kakui
K, Takemura M et al.: Cyclic mechanical stretch aug-
ments prostacyclin production in cultured human uterine
myometrial cells from pregnant women: possible in-
volvement of up-regulation of prostacyclin synthase ex-
pression. J Clin Endocrinol Metab, 2002, 87, 5209–5219.
41. Kurumbail RG, Stevens AM, Gierse JK, McDonald JJ,
Stegeman RA, Pak JY, Gildehaus D et al.: Structural ba-
sis for selective inhibition of cyclooxygenase-2 by anti-
inflammatory agents. Nature, 1996, 384, 644–648.
42. Langenbach R, Morham SG, Tiano HF, Loftin CD, Gha-
nayem BI, Chulada PC, Mahler JF et al.: Prostaglandin
synthase 1 gene disruption in mice reduces arachidonic
acid-induced inflammation and indomethacin-induced
gastric ulceration. Cell, 1995, 83, 483–492.
43. Lecomte M, Laneuville O, Ji C, DeWitt DL, Smith WL:
Acetylation of human prostaglandin endoperoxide
synthase-2 (cyclooxygenase-2) by aspirin. J Biol Chem,
1994, 269, 13207–13215.
44. Luong C, Miller A, Barnett J, Chow J, Ramesha C,
Browner MF: Flexibility of the NSAID binding site in
the structure of human cyclooxygenase-2. Nat Struct
Biol, 1996, 3, 927–933.
45. MacDonald TM, Wei L: Effect of ibuprofen on cardio-
protective effect of aspirin. Lancet, 2003, 361, 573–574.
82 �������������� ���� �� ����� ��� ������ ���

46. Mancini JA, Blood K, Guay J, Gordon R, Claveau D,
Chan CC, Riendeau D: Cloning, expression, and up-
regulation of inducible rat prostaglandin e synthase dur-
ing lipopolysaccharide-induced pyresis and adjuvant-
induced arthritis. J Biol Chem, 2001, 276, 4469–4475.
47. Mancini JA, Riendeau D, Falgueyret JP, Vickers PJ,
O’Neill GP: Arginine 120 of prostaglandin G/H
synthase-1 is required for the inhibition by nonsteroidal
anti-inflammatory drugs containing a carboxylic acid
moiety. J Biol Chem, 1995, 270, 29372–29377.
48. Matheson AJ, Figgitt DP: Rofecoxib: a review of its use
in the management of osteoarthritis, acute pain and rheu-
matoid arthritis. Drugs, 2001, 61, 833–865.
49. McAdam BF, Catella-Lawson F, Mardini IA, Kapoor S,
Lawson JA, FitzGerald GA: Systemic biosynthesis of
prostacyclin by cyclooxygenase (COX)-2: the human
pharmacology of a selective inhibitor of COX-2. Proc
Natl Acad Sci USA, 1999, 96, 272–277.
50. McAdam BF, Mardini IA, Habib A, Burke A, Lawson
JA, Kapoor S, FitzGerald GA: Effect of regulated ex-
pression of human cyclooxygenase isoforms on eicosa-
noid and isoeicosanoid production in inflammation.
J Clin Invest, 2000, 105, 1473–1482.
51. Murakami M, Kudo I: Recent advances in molecular
biology and physiology of the prostaglandin E2-biosynthetic
pathway. Prog Lipid Res, 2004, 43, 3–35.
52. Murakami M, Nakashima K, Kamei D, Masuda S, Ishi-
kawa Y, Ishii T, Ohmiya Y et al.: Cellular prostaglandin
E2 production by membrane-bound prostaglandin E
synthase-2 via both cyclooxygenases-1 and -2. J Biol
Chem, 2003, 278, 37937–37947.
53. Murakami M, Naraba H, Tanioka T, Semmyo N, Naka-
tani Y, Kojima F, Ikeda T et al.: Regulation of prosta-
glandin E2 biosynthesis by inducible membrane-
associated prostaglandin E2 synthase that acts in concert
with cyclooxygenase-2. J Biol Chem, 2000, 275,
32783–32792.
54. Narumiya S, FitzGerald GA: Genetic and pharmacologi-
cal analysis of prostanoid receptor function. J Clin Invest,
2001, 108, 25–30.
55. Nusing R, Ullrich V: Immunoquantitation of thrombox-
ane synthase in human tissues. Eicosanoids, 1990, 3,
175–180.
56. Nussmeier NA, Whelton AA, Brown MT, Langford RM,
Hoeft A, Parlow JL, Boyce SW et al.: Complications of
the COX-2 inhibitors parecoxib and valdecoxib after car-
diac surgery. N Engl J Med, 2005, 352, 1081–1091.
57. Oida H, Namba T, Sugimoto Y, Ushikubi F, Ohishi H,
Ichikawa A, Narumiya S: In situ hybridization studies of
prostacyclin receptor mRNA expression in various
mouse organs. Br J Pharmacol, 1995, 116, 2828–2837.
58. Onodera M, Horiuchi Y, Nakahama K, Muneta T, Mano
Y, Morita I: Induction of cyclooxygenase-1 in cultured
synovial cells isolated from rheumatoid arthritis patients.
Inflamm Res, 2004, 53, 217–222.
59. Patrignani P, Campestrini J, Branson J, Girani M, Hart-
mann S, Rordorf C, Patrono C: Lumiracoxib is a selec-
tive inhibitor of cyclooxygenase-2 in patients with os-
teoarthritis. Ann Rheum Dis, 2004, 63, 368.
60. Patrignani P, Capone ML, Tacconelli S: Clinical pharma-
cology of etoricoxib: a novel selective COX2 inhibitor.
Expert Opin Pharmacother, 2003, 4, 265–284.
61. Patrignani P, Filabozzi P, Patrono C: Selective cumula-
tive inhibition of platelet thromboxane production by
low-dose aspirin in healthy subjects. J Clin Invest, 1982,
69, 1366–1372.
62. Patrignani P, Panara MR, Greco A, Fusco O, Natoli C,
Iacobelli S, Cipollone F et al.: Biochemical and pharma-
cological characterization of the cyclooxygenase activity
of human blood prostaglandin endoperoxide synthases.
J Pharmacol Exp Ther, 1994, 271, 1705–1712.
63. Patrignani P, Sciulli MG: Amplification loops: throm-
boxane generation. In: Platelets in Thrombotic and Non-
thrombotic Disorders. Ed. Gresele P, Page C, Fuster V,
Vermylen J Cambrige University Press (UK), 2002,
369–380.
64. Patrignani P, Sciulli MG: Pharmaceutical exploitation:
cyclooxygenase and lipoxygenase inhibitors. In: The Ei-
cosanoids. Ed. Curtis-Prior P, Wiley Press, Cambridge
(UK), 2004, 599–612.
65. Patrono C, Coller B, FitzGerald GA, Hirsh J, Roth G:
Platelet-active drugs: the relationships among dose, ef-
fectiveness, and side effects: the Seventh ACCP Confer-
ence on Antithrombotic and Thrombolytic Therapy. Chest,
2004, 126, 234S–264S.
66. Patrono C, Patrignani P, Garcia Rodriguez LA:
Cyclooxygenase-selective inhibition of prostanoid for-
mation: transducing biochemical selectivity into clinical
read-outs. J Clin Invest, 2001, 108, 7–13.
67. Picot D, Loll PJ, Garavito RM: The X-ray crystal struc-
ture of the membrane protein prostaglandin H2 synthase-1.
Nature, 1994, 367, 243–249.
68. Qi Z, Hao CM, Langenbach RI, Breyer RM, Redha R,
Morrow JD, Breyer MD: Opposite effects of
cyclooxygenase-1 and -2 activity on the pressor response
to angiotensin II. J Clin Invest, 2002, 110, 61–69.
69. Rocca B, Spain LM, Pure E, Langenbach R, Patrono C,
FitzGerald GA: Distinct roles of prostaglandin H syn-
thases 1 and 2 in T-cell development. J Clin Invest, 1999,
103, 1469–1477.
70. Roth GJ, Stanford N, Majerus PW: Acetylation of pros-
taglandin synthase by aspirin. Proc Natl Acad Sci USA,
1975, 72, 3073–3076.
71. Rudic RD, Brinster D, Cheng Y, Fries S, Song WL, Aus-
tin S, Coffman TM et al.: COX-2-derived prostacyclin
modulates vascular remodeling. Circ Res, 2005, 96,
1240–1247.
72. Sano H, Hla T, Maier JA, Crofford LJ, Case JP, Maciag
T, Wilder RL: In vivo cyclooxygenase expression in
synovial tissues of patients with rheumatoid arthritis and
osteoarthritis and rats with adjuvant and streptococcal
cell wall arthritis. J Clin Invest, 1992, 89, 97–108.
73. Schnitzer TJ, Burmester GR, Mysler E, Hochberg MC,
Doherty M, Ehrsam E, Gitton X et al.; TARGET Study
Group: Comparison of lumiracoxib with naproxen and
ibuprofen in the Therapeutic Arthritis Research and Gas-
trointestinal Event Trial (TARGET), reduction in ulcer
omplications: randomised controlled trial. Lancet, 2004,
4, 665–674.
�������������� ���� �� ����� ��� ������ ��� 83
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��

74. Schumacher HR Jr, Boice JA, Daikh DI, Mukhopadhyay
S, Malmstrom K, Ng J, Tate GA et al.: Randomised dou-
ble blind trial of etoricoxib and indometacin in treatment
of acute gouty arthritis. BMJ, 2002, 324, 1488–1492.
75. Shaftel SS, Olschowka JA, Hurley SD, Moore AH,
O’Banion MK: COX-3: a splice variant of
cyclooxygenase-1 in mouse neural tissue and cells. Brain
Res Mol Brain Res, 2003, 119, 213–215.
76. Silverstein FE, Faich G, Goldstein JL, Simon LS, Pincus
T, Whelton A, Makuch R et al.: Gastrointestinal toxicity
with celecoxib vs. nonsteroidal anti-inflammatory drugs
for osteoarthritis and rheumatoid arthritis: the CLASS
study: A randomised controlled trial. Celecoxib Long-
term Arthritis Safety Study. JAMA, 2000, 284, 1247–1255.
77. Simmons DL, Botting RM, Hla T: Cyclooxygenase iso-
zymes: the biology of prostaglandin synthesis and inhibi-
tion. Pharmacol Rev, 2004, 56, 387–437.
78. Smith WL, Langenbach R: Why there are two cyclooxy-
genase isozymes. J Clin Invest, 2001, 107, 1491–1495.
79. Smith WL, Song I: The enzymology of prostaglandin en-
doperoxide H synthases-1 and -2. Prostaglandins Other
Lipid Mediat, 2002, 68–69, 115–128.
80. Solomon DH: Selective cyclooxygenase 2 inhibitors and
cardiovascular events. Arthritis Rheum, 2005, 52, 1968–1978.
81. Solomon SD, McMurray JJ, Pfeffer MA, Wittes J,
Fowler R, Finn P, Anderson WF et al.: Adenoma Preven-
tion with Celecoxib (APC) Study Investigators. Cardio-
vascular risk associated with celecoxib in a clinical trial
for colorectal adenoma prevention. N Engl J Med, 2005,
352, 1071–1080.
82. Sorli CH, Zhang HJ, Armstrong MB, Rajotte RV, Ma-
clouf J, Robertson RP: Basal expression of
cyclooxygenase-2 and nuclear factor-interleukin 6 are
dominant and coordinately regulated by interleukin 1 in
the pancreatic islet. Proc Natl Acad Sci USA, 1998, 95,
1788–1793.
83. Steinbach G, Lynch PM, Phillips RK, Wallace MH,
Hawk E, Gordon GB, Wakabayashi N et al.: The effect
of celecoxib, a cyclooxygenase-2 inhibitor, in familial
adenomatous polyposis. N Engl J Med, 2000, 342,
1946–1952.
84. Stichtenoth DO, Thoren S, Bian H, Peters-Golden M,
Jakobsson PJ, Crofford LJ: Microsomal prostaglandin E
synthase is regulated by proinflammatory cytokines and
glucocorticoids in primary rheumatoid synovial cells.
J Immunol, 2001, 167, 469–474.
85. Sugimoto Y, Narumiya S, Ichikawa A: Distribution and
function of prostanoid receptors: studies from knockout
mice. Prog Lipid Res, 2000, 39, 289–314.
86. Sugimoto Y, Shigemoto R, Namba T, Negishi M, Mi-
zuno N, Narumiya S, Ichikawa A: Distribution of the
messenger RNA for the prostaglandin E receptor subtype
EP3 in the mouse nervous system. Neuroscience, 1994,
62, 919–928.
87. Tacconelli S, Capone ML, Patrignani P: Clinical pharma-
cology of novel selective COX-2 inhibitors. Curr Pharm
Des, 2004, 10, 589–601.
88. Tacconelli S, Capone ML, Sciulli MG, Ricciotti E, Pa-
trignani P: The biochemical selectivity of novel COX-2
inhibitors in whole blood assays of COX-isozyme activ-
ity. Curr Med Res Opin, 2002, 18, 503–511.
89. Tanikawa N, Ohmiya Y, Ohkubo H, Hashimoto K, Kan-
gawa K, Kojima M, Ito S et al.: Identification and char-
acterization of a novel type of membrane-associated
prostaglandin E synthase. Biochem Biophys Res Com-
mun, 2002, 291, 884–889.
90. Tanioka T, Nakatani Y, Semmyo N, Murakami M, Kudo
I: Molecular identification of cytosolic prostaglandin E2
synthase that is functionally coupled with
cyclooxygenase-1 in immediate prostaglandin E2 bio-
synthesis. J Biol Chem, 2000, 275, 32775–32782.
91. Tilley SL, Coffman TM, Koller BH: Mixed messages:
modulation of inflammation and immune responses by
prostaglandins and thromboxanes. J Clin Invest, 2001,
108, 15–23.
92. Topper JN, Cai J, Falb D, Gimbrone MA Jr: Identifica-
tion of vascular endothelial genes differentially respon-
sive to fluid mechanical stimuli: cyclooxygenase-2, man-
ganese superoxide dismutase, and endothelial cell nitric
oxide synthase are selectively up-regulated by steady
laminar shear stress. Proc Natl Acad Sci USA, 1996, 93,
10417–10422.
93. Tsujii M, Kawano S, DuBois RN: Cyclooxygenase-2 ex-
pression in human colon cancer cells increases metastatic
potential. Proc Natl Acad Sci USA, 1997, 94, 3336–3340.
94. Ueno N, Murakami M, Tanioka T, Fujimori K, Tanabe T,
Urade Y, Kudo I: Coupling between cyclooxygenase, ter-
minal prostanoid synthase, and phospholipase A2. J Biol
Chem, 2001, 276, 34918–34927.
95. Urade Y, Eguchi N: Lipocalin-type and hematopoietic
prostaglandin D synthases as a novel example of func-
tional convergence. Prostaglandins Other Lipid Mediat,
2002, 68–69, 375–382.
96. Ushikubi F, Nakajima M, Hirata M, Okuma M, Fujiwara
M, Narumiya S: Purification of the thromboxane
A2/prostaglandin H2 receptor from human blood plate-
lets. J Biol Chem, 1989, 264, 16496–16501.
97. van der Heijde D, Baraf HS, Ramos-Remus C, Calin A,
Weaver AL, Schiff M, James M et al.: Evaluation of the
efficacy of etoricoxib in ankylosing spondylitis: results
of a fifty-two-week, randomized, controlled study. Ar-
thritis Rheum, 2005, 52, 1205–1215.
98. Vane JR: Inhibition of prostaglandin synthesis as a
mechanism of action for aspirin-like drugs. Nat New
Biol, 1971, 231, 232–235.
99. Vane JR: Towards a better aspirin. Nature, 1994, 367,
215–216.
100. Walker MC, Kurumbail RG, Kiefer JR, Moreland KT,
Koboldt CM, Isakson PC, Seibert K et al.: A three-step
kinetic mechanism for selective inhibition of cyclo-
oxygenase-2 by diarylheterocyclic inhibitors. Biochem J,
2001, 357, 709–718.
101. Wang LH, Kulmacz RJ: Thromboxane synthase: struc-
ture and function of protein and gene. Prostaglandins
Other Lipid Mediat, 2002, 68–69, 409–422.
102. Watanabe K: Prostaglandin F synthase. Prostaglandins
Other Lipid Mediat, 2002, 68–69, 401–407.
103. Watanabe H, Katoh T, Eiro M, Iwamoto M, Ushikubi F,
Narumiya S, Watanabe T: Effects of salt loading on
blood pressure in mice lacking the prostanoid receptor
gene. Circ J, 2005, 69, 124–126.
84 �������������� ���� �� ����� ��� ������ ���

104. Weaver AJ, Sullivan WP, Felts SJ, Owen BA, Toft DO:
Crystal structure and activity of human p23, a heat shock
protein 90 co-chaperone. J Biol Chem, 2000, 275,
23045–23052.
105. Winchester SK, Imamura T, Gross GA, Muglia LM, Vogt
SK, Wright J, Watanabe K et al.: Coordinate regulation
of prostaglandin metabolism for induction of parturition
in mice. Endocrinology, 2002, 143, 2593–2598.
106. Wong D, Wang M, Cheng Y, FitzGerald GA: Cardiovas-
cular hazard and non-steroidal anti-inflammatory drugs.
Curr Opin Pharmacol, 2005, 5, 204–210.
107. Xu S, Venge P: Lipocalins as biochemical markers of
disease. Biochim Biophys Acta, 2000, 1482, 298–307.
108. Yamagata K, Andreasson KI, Kaufmann WE, Barnes
CA, Worley PF: Expression of a mitogen-inducible cy-
clooxygenase in brain neurons: regulation by synaptic
activity and glucocorticoids. Neuron, 1993, 11, 371–386.
Received:
August 24, 2005.
�������������� ���� �� ����� ��� ������ ��� 85
The future of traditional NSAIDs and COX-2 inhibitors����� �� ���� �� ��