Embed Size (px)
Citation preview
The Global Obesity Pandemic
JHI Partners ForumOctober 2, 2012
Richard R. Rubin, PhD
Professor, Medicine and Pediatrics
The Johns Hopkins University School of Medicine
Obesity Pandemic Key Points
• Prevalence• Causes• Medical consequences• Financial consequences
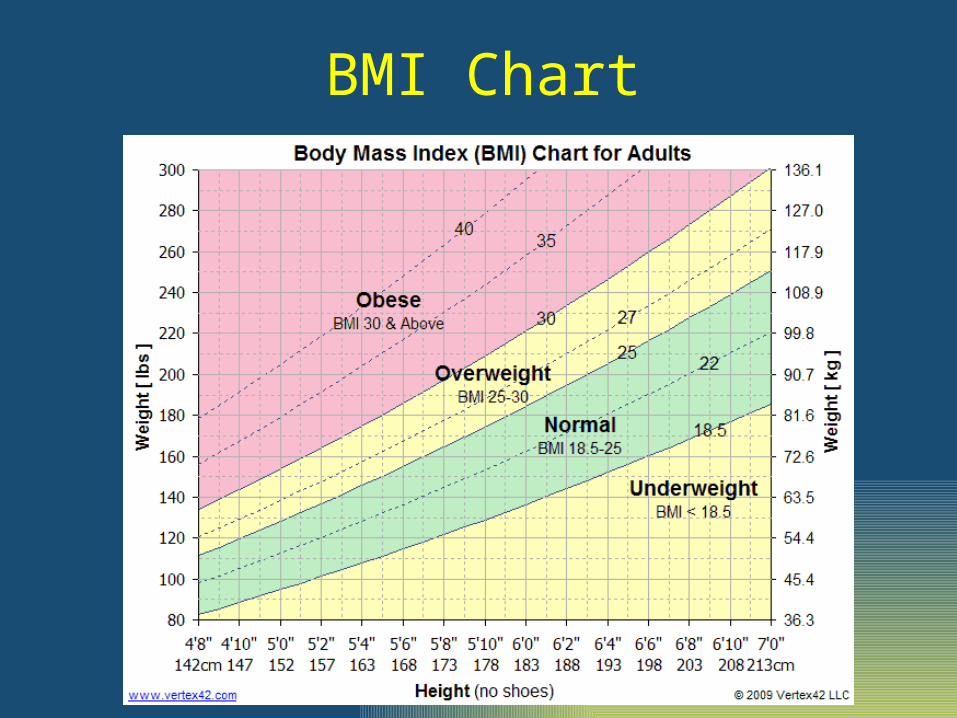
BMI Chart
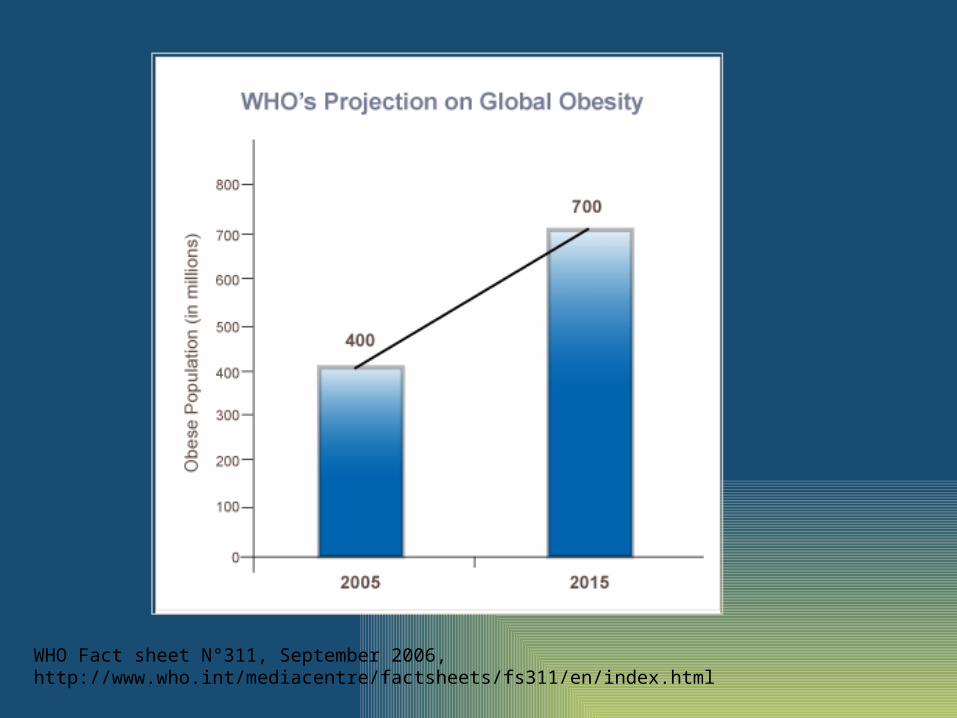
WHO Fact sheet N°311, September 2006, http://www.who.int/mediacentre/factsheets/fs311/en/index.html
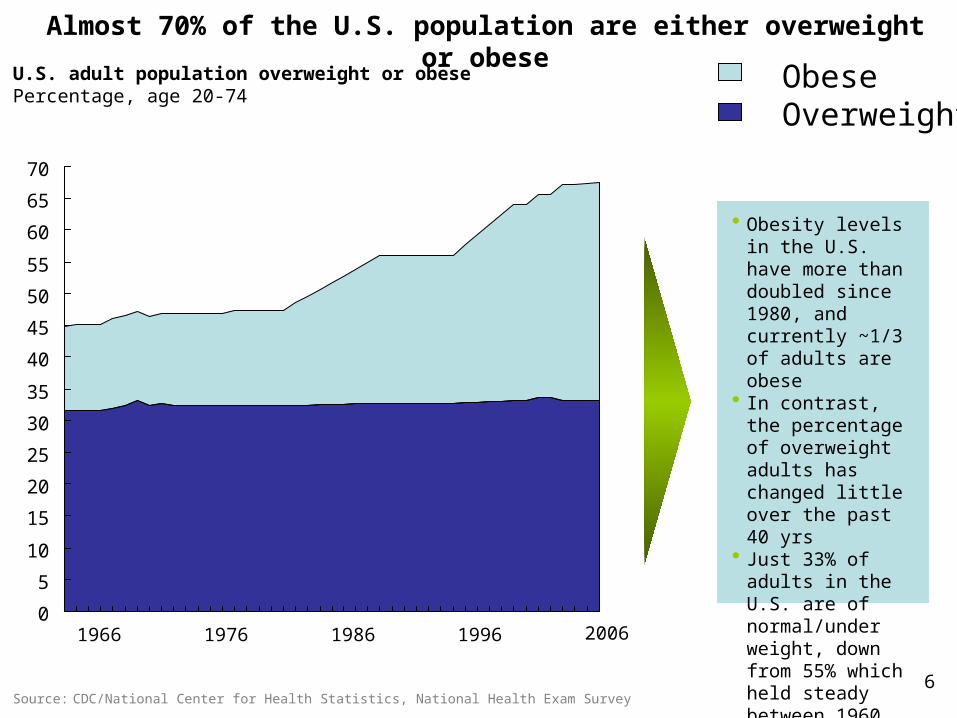
Almost 70% of the U.S. population are either overweight or obese
6Source: CDC/National Center for Health Statistics, National Health Exam Survey
U.S. adult population overweight or obesePercentage, age 20-74
• Obesity levels in the U.S. have more than doubled since 1980, and currently ~1/3 of adults are obese
• In contrast, the percentage of overweight adults has changed little over the past 40 yrs
• Just 33% of adults in the U.S. are of normal/under weight, down from 55% which held steady between 1960 and 1980
0
5
10
15
20
25
30
35
40
45
50
55
60
65
70
ObeseOverweight
1966 20061976 1986 1996

Portion Sizes 20 Years Ago to Today
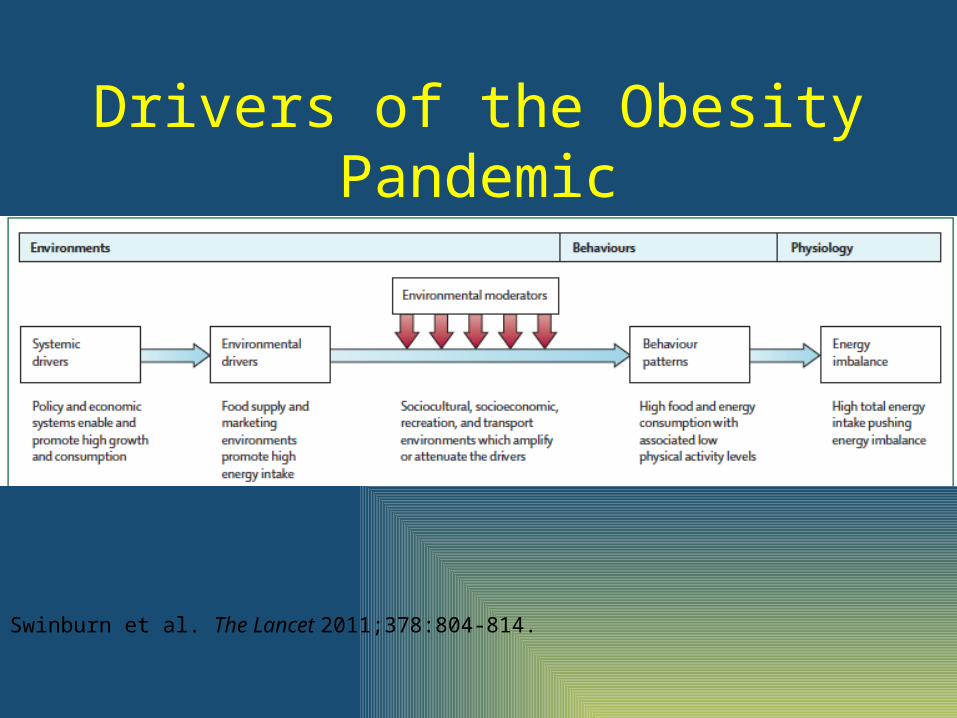
Drivers of the Obesity Pandemic
Swinburn et al. The Lancet 2011;378:804-814.
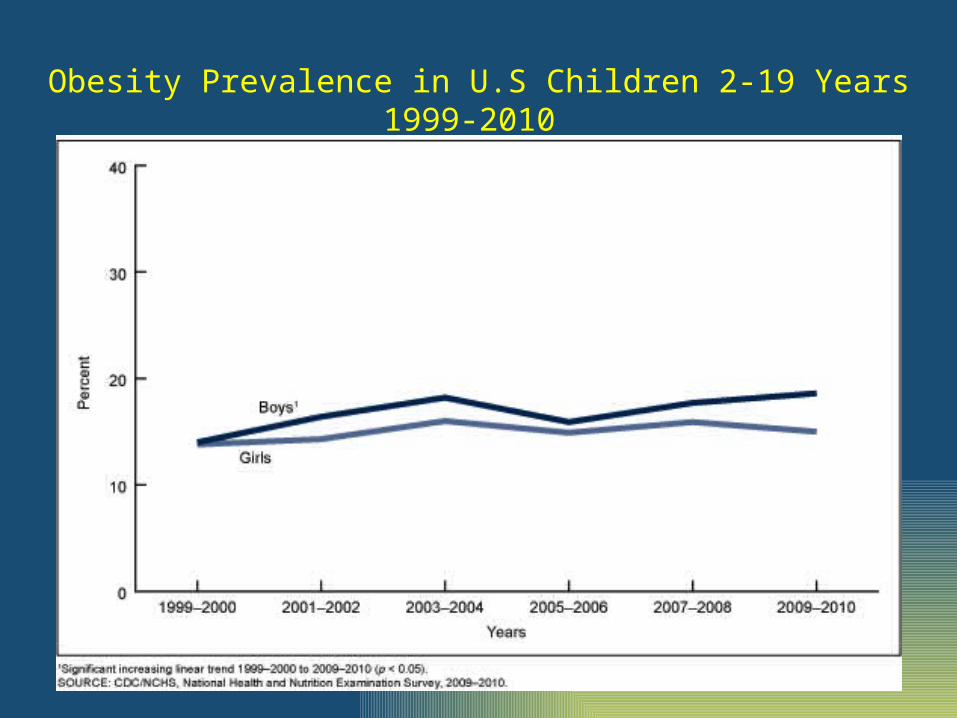
Obesity Prevalence in U.S Children 2-19 Years 1999-2010
93.2
0
25
50
75
100
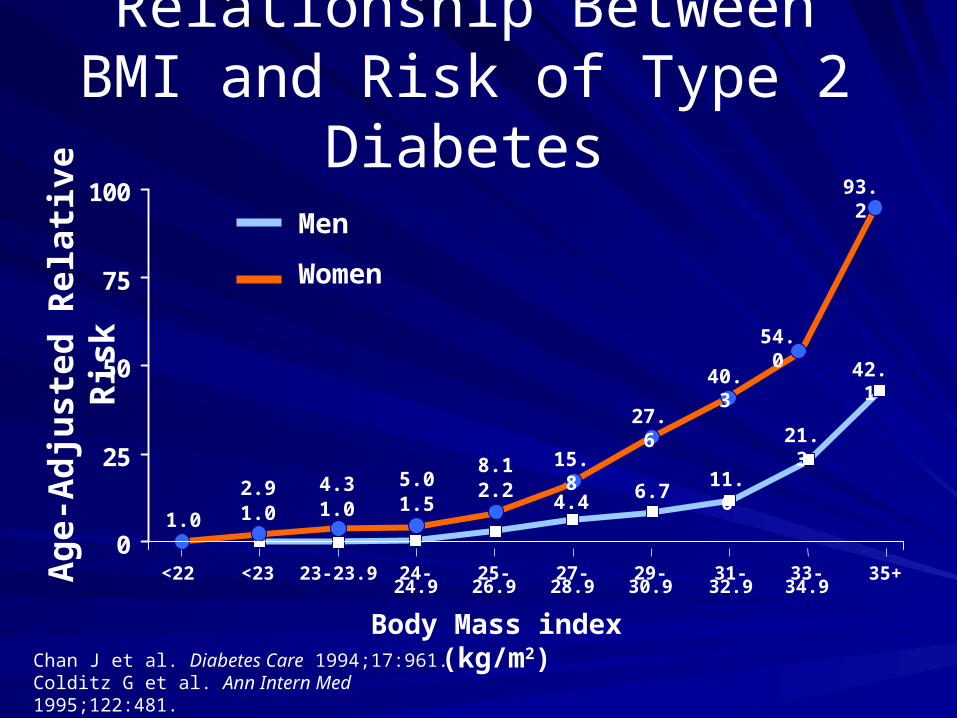
Relationship Between BMI and Risk of Type 2 Diabetes
Chan J et al. Diabetes Care 1994;17:961.Colditz G et al. Ann Intern Med 1995;122:481.
Ag
e-A
dju
ste
d R
ela
tiv
e R
isk
Body Mass index (kg/m2)
Men
Women
<22 <23 23-23.9 24-24.9 25-26.9 27-28.9 29-30.9 31-32.9 33-34.9 35+
1.0
2.91.0
4.31.0
5.01.5
8.12.2
15.8
4.4
27.6
40.3
54.0
6.711.6
21.3
42.1
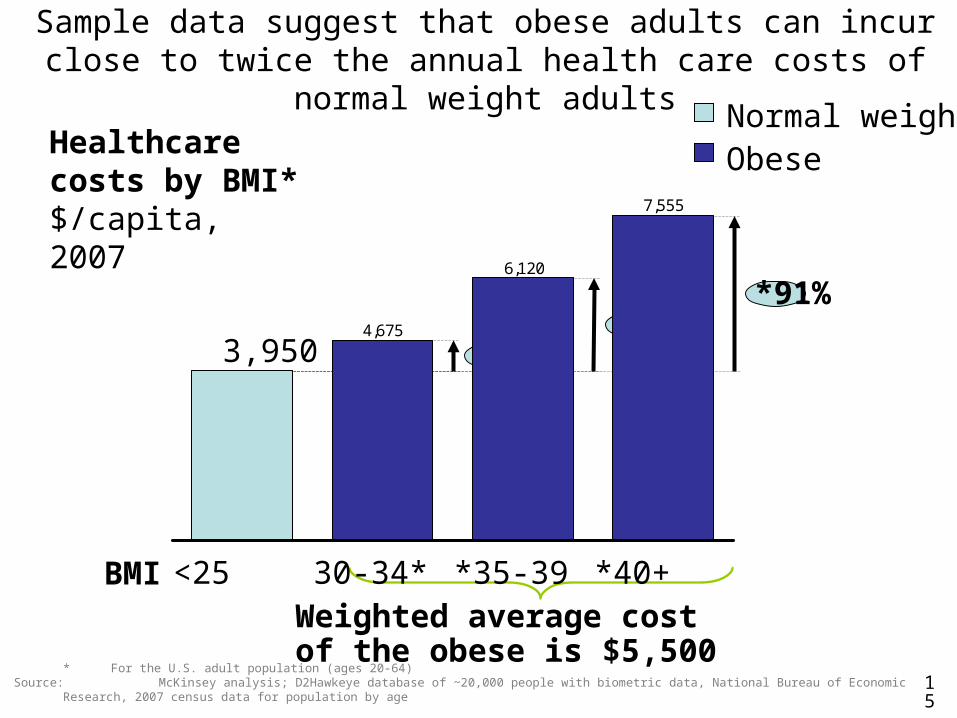
Sample data suggest that obese adults can incur close to twice the annual health care costs of normal weight adults
15
7,555
6,120
4,675
3,950
<25 30-34* *35-39 *40+
*18%
*91%*55%
Healthcare costs by BMI*$/capita, 2007
* For the U.S. adult population (ages 20-64) Source: McKinsey analysis; D2Hawkeye database of ~20,000 people with biometric data, National Bureau of Economic Research, 2007 census data
for population by age
BMIWeighted average cost of the obese is $5,500
Normal weightObese

Medical Management of Obesity
Kimberly Gudzune, MD, MPH
Assistant Professor of Medicine
Johns Hopkins Digestive Weight Loss Center
Johns Hopkins International Partners ForumOctober 2, 2012
Objectives
• Eligibility for obesity treatment• Description of medical management of
obesity• Review of new weight loss medications
coming on the market
Weight is more than about looking good…
• Heart disease• Diabetes• Cancer• Gall stones• Fatty liver
• Lung disease• Infertility• Arthritis• Incontinence• Disability
Decreased quality of life!Increased risk of early death!Shorter life span!

WHO IS ELIGIBLE FOR OBESITY TREATMENT?
Estimating Obesity• Measuring body fat requires specialized equipment
• Patients typically identified in the clinical setting using
body mass index (BMI)Weight (kg)
Height (m)2
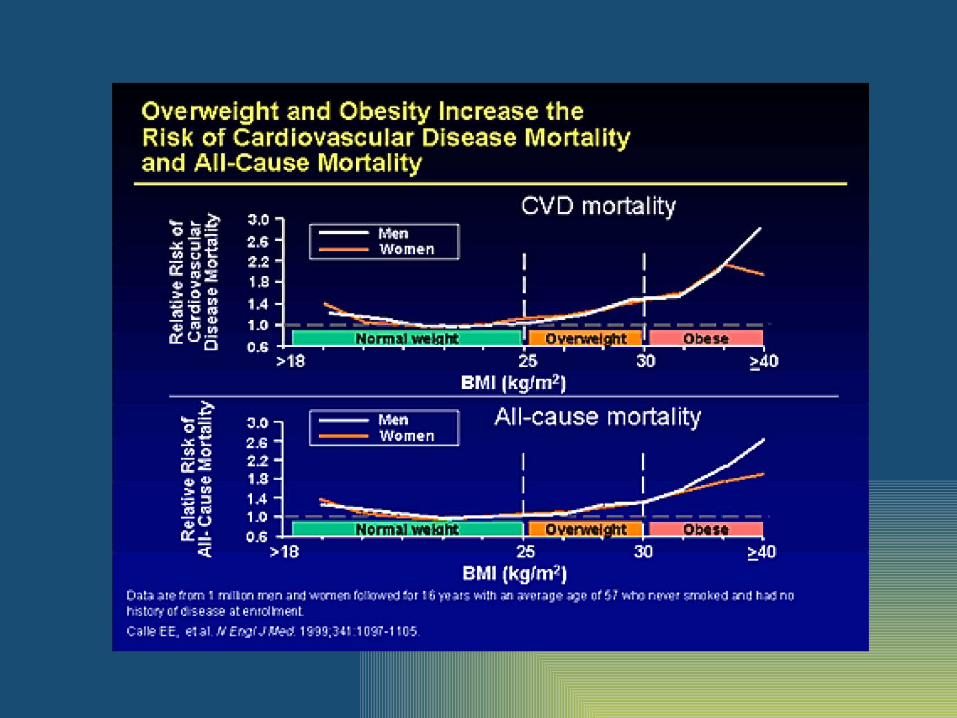
• NIH and WHO have categorized BMI based on
increased risk of cardiovascular (CVD) and other
diseases
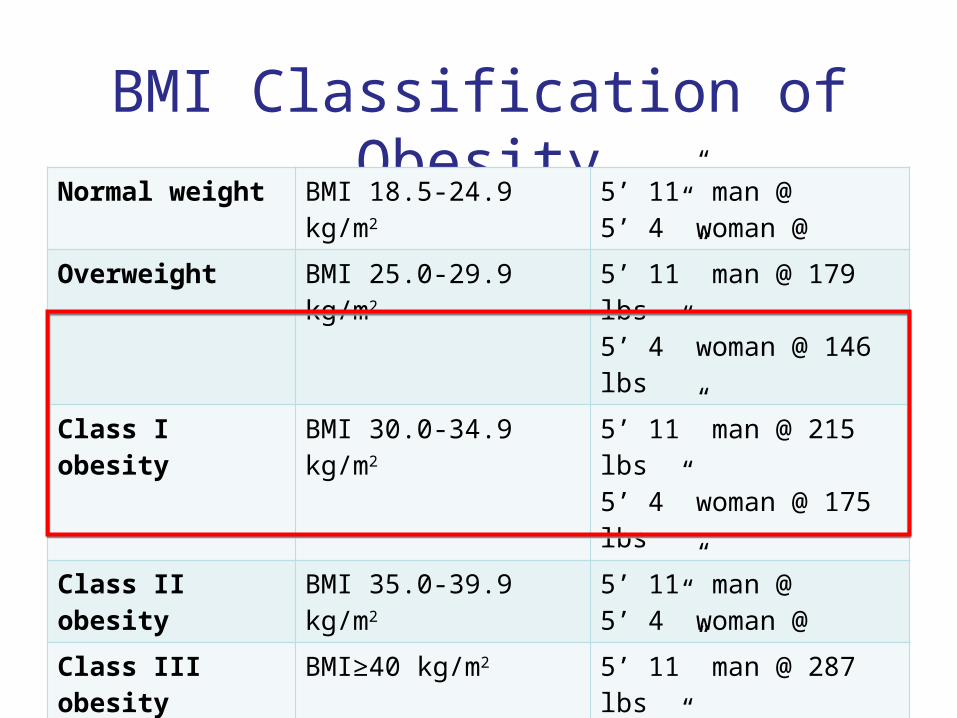
BMI Classification of ObesityNormal weight BMI 18.5-24.9 kg/m2 5’ 11” man @
5’ 4” woman @
Overweight BMI 25.0-29.9 kg/m2 5’ 11” man @ 179 lbs5’ 4” woman @ 146 lbs
Class I obesity BMI 30.0-34.9 kg/m2 5’ 11” man @ 215 lbs5’ 4” woman @ 175 lbs
Class II obesity BMI 35.0-39.9 kg/m2 5’ 11” man @ 5’ 4” woman @
Class III obesity BMI≥40 kg/m2 5’ 11” man @ 287 lbs5’ 4” woman @ 233 lbs
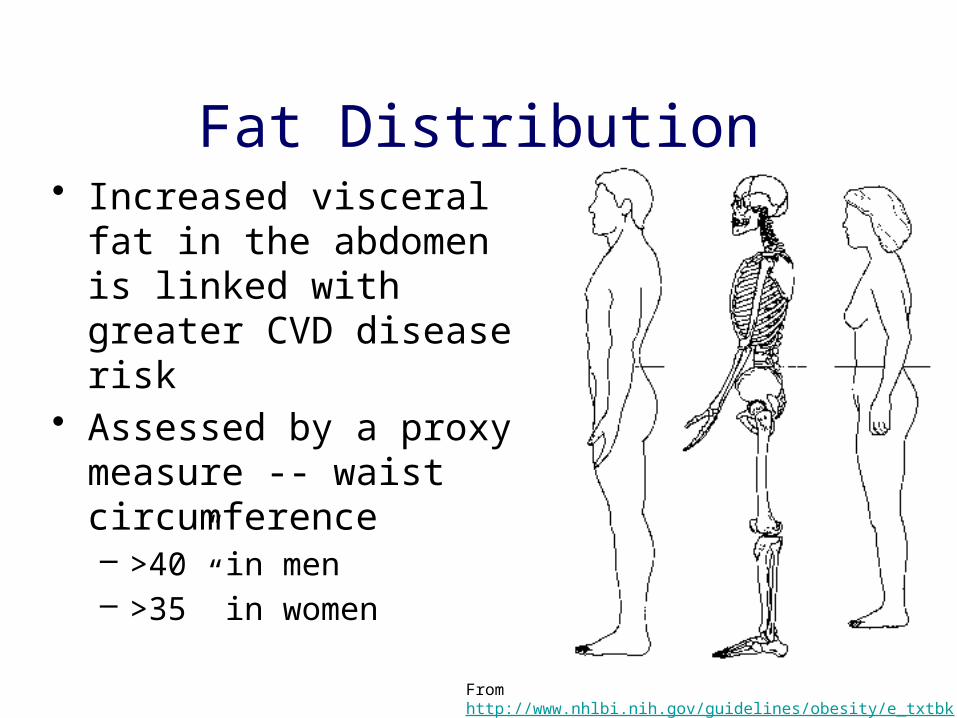
Fat Distribution• Increased visceral fat in
the abdomen is linked with greater CVD disease risk
• Assessed by a proxy measure -- waist circumference– >40” in men– >35” in women
From http://www.nhlbi.nih.gov/guidelines/obesity/e_txtbk/txgd/4142.htm
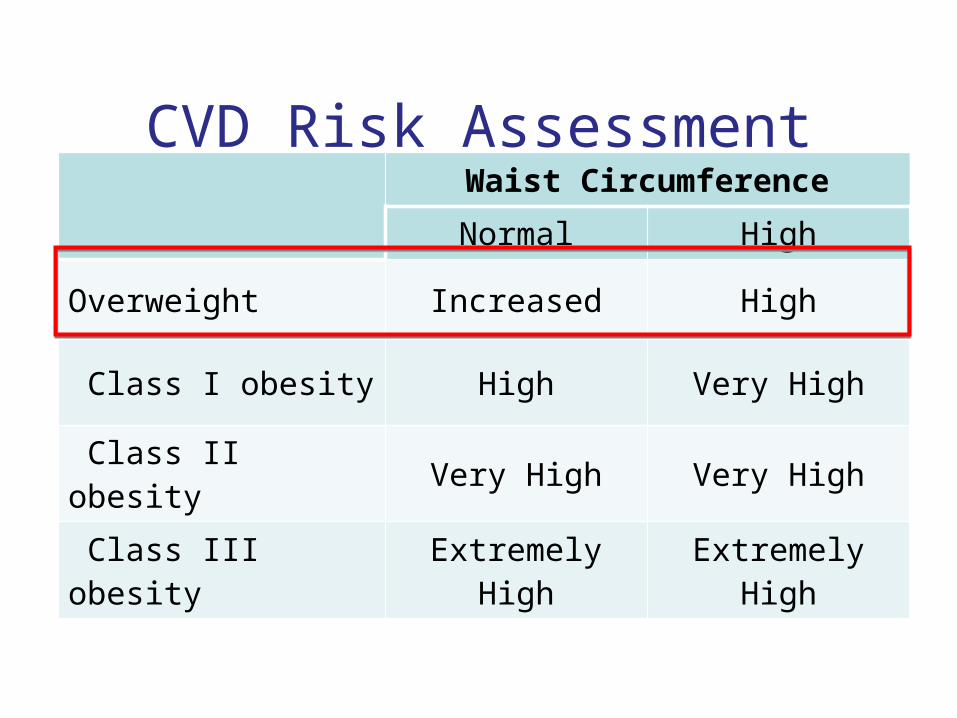
CVD Risk AssessmentWaist Circumference
Normal High
Overweight Increased High
Class I obesity High Very High
Class II obesity Very High Very High
Class III obesity Extremely High Extremely High
Obesity-related Comorbidities
• Hypertension• Heart disease• Dyslipidemia• Pre-diabetes• Diabetes mellitus• Gastroesophageal
reflux disease
• Fatty liver• Back pain• Arthritis• Polycystic ovarian
syndrome• Infertility• Incontience
WHAT SERVICES ENCOMPASS THE MEDICAL MANAGEMENT OF OBESITY?
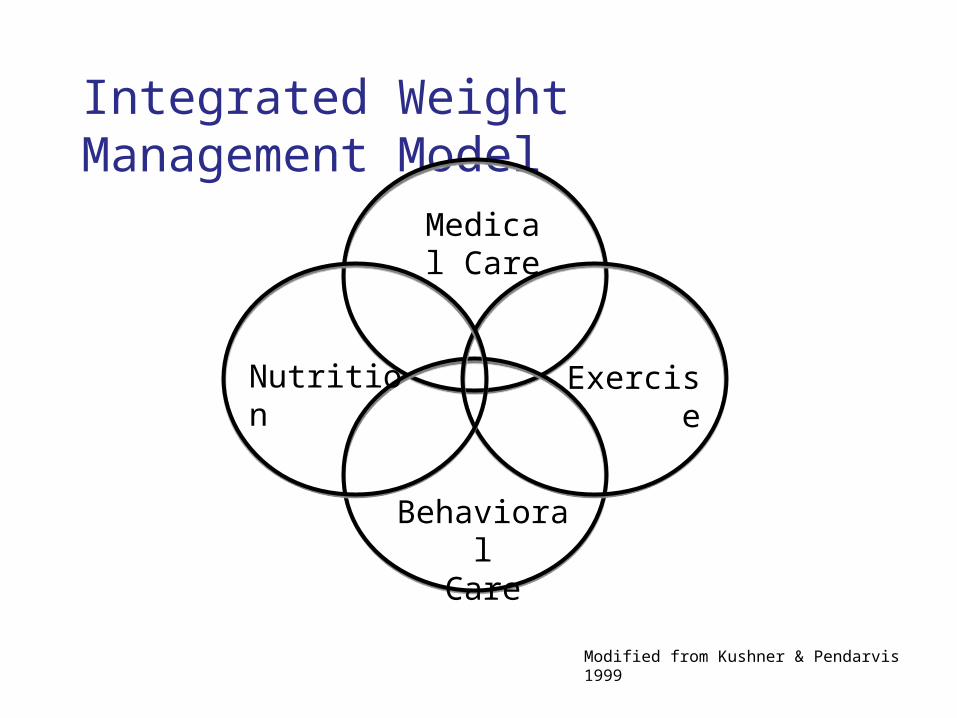
Integrated Weight Management Model
Modified from Kushner & Pendarvis 1999
Medical Care
BehavioralCare
ExerciseNutrition
Medical Care• Weight evaluation and
management performed by a physician– Primary care physician– Weight management
specialist
• Physician counseling can be more effective if the 5A’s or motivational interviewing used
Medical Care
• Role of the physician includes evaluation and management of:– Goal setting – Secondary causes of obesity– Co-morbidities associated with weight gain– Medications associated with weight gain– Candidacy for use of anti-obesity
medications
Goal Setting• Initial goal for weight loss is to achieve a
“healthier weight”– 5-10% loss of initial body weight
• Accomplishable for most people• Typically leads to improvement in blood
pressure, blood sugar, and other obesity-related diseases
– Goal rate of 1-2 lbs lost per week• Accomplishable for most people• Safe• Less risk of weight regain
Secondary Causes of Obesity
Common• Hypothyroidism• Polycystic ovarian
syndrome (PCOS)
Rare• Cushing syndrome• Hypothalamic obesity
syndromes • Melanocortin-4 mutations • Leptin deficiency
Co-morbid Conditions
Cardiovascular• Hypertension• Coronary heart disease
Pulmonary• Asthma• Obstructive Sleep Apnea
Metabolic• Diabetes mellitus• Dyslipidemia• Metabolic syndrome• Gout
Gastrointestinal• GERD• Gallbladder disease• Fatty liver
Co-morbid Conditions
Musculoskeletal• Osteoarthritis• Back pain
Cancer• Colorectal cancer• Prostate cancer• Endometrial cancer• Cervical cancer• Breast cancer• Ovarian cancer• Pancreatic cancer
Reproductive/GU• PCOS• Infertility• Incontinence
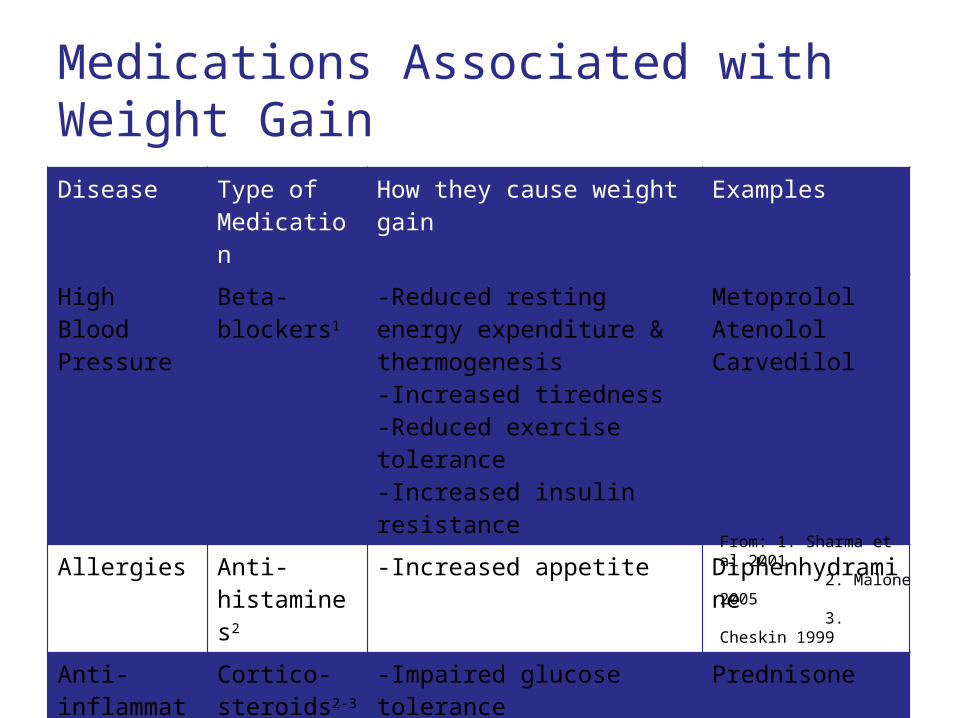
Medications Associated with Weight Gain
Disease Type of Medication
How they cause weight gain Examples
High Blood Pressure
Beta-blockers1
-Reduced resting energy expenditure & thermogenesis-Increased tiredness-Reduced exercise tolerance-Increased insulin resistance
MetoprololAtenololCarvedilol
Allergies Anti-histamines2
-Increased appetite Diphenhydramine
Anti-inflammatory
Cortico-steroids2-3
-Impaired glucose tolerance-Increased truncal fat
Prednisone
From: 1. Sharma et al 2001 2. Malone 2005 3. Cheskin 1999
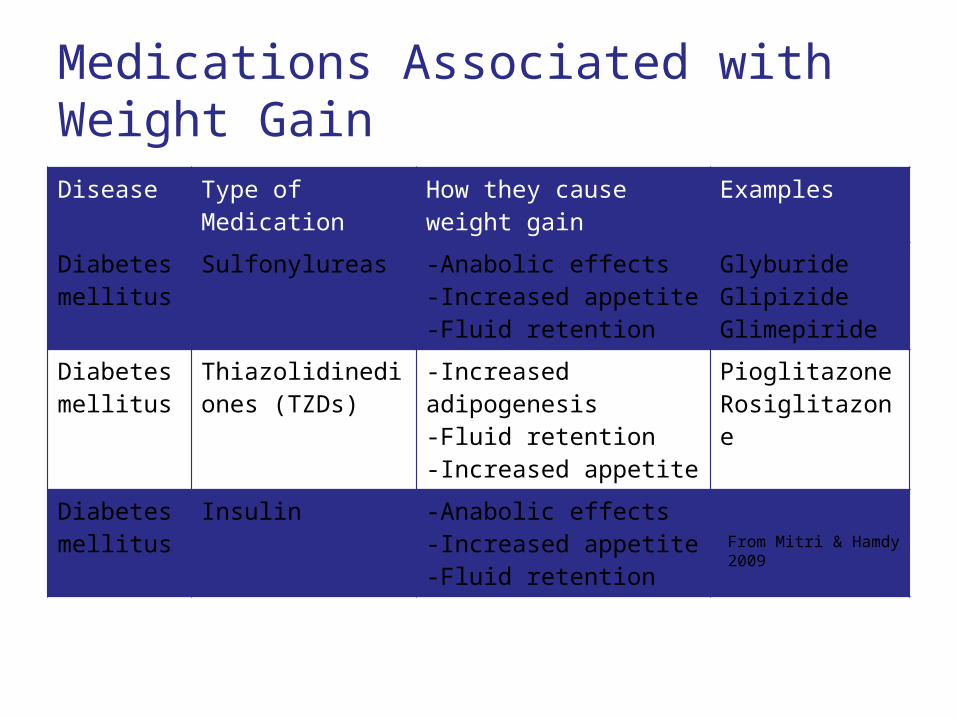
Medications Associated with Weight Gain
Disease Type of Medication How they cause weight gain
Examples
Diabetes mellitus
Sulfonylureas -Anabolic effects-Increased appetite-Fluid retention
GlyburideGlipizideGlimepiride
Diabetes mellitus
Thiazolidinediones (TZDs)
-Increased adipogenesis-Fluid retention-Increased appetite
PioglitazoneRosiglitazone
Diabetes mellitus
Insulin -Anabolic effects-Increased appetite-Fluid retention
From Mitri & Hamdy 2009
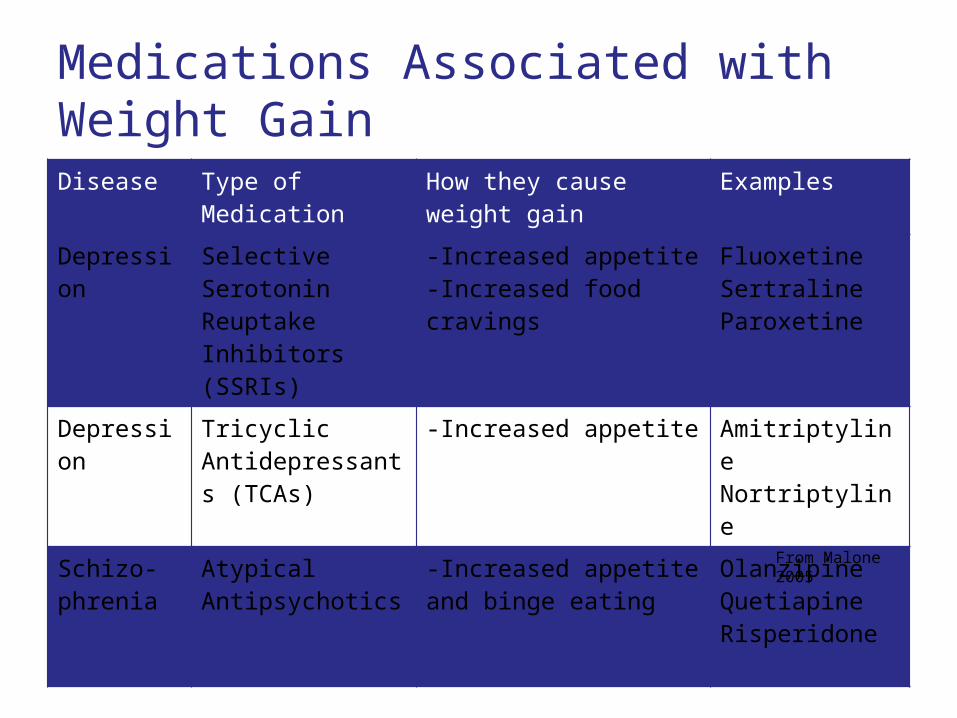
Medications Associated with Weight Gain
Disease Type of Medication How they cause weight gain
Examples
Depression Selective Serotonin Reuptake Inhibitors(SSRIs)
-Increased appetite-Increased food cravings
FluoxetineSertralineParoxetine
Depression Tricyclic Antidepressants (TCAs)
-Increased appetite AmitriptylineNortriptyline
Schizo-phrenia
Atypical Antipsychotics
-Increased appetite and binge eating
OlanzipineQuetiapineRisperidone
From Malone 2005

Nutrition
• Nutrition evaluation and diet plan– Trained physician– Registered dietician– Certified nutrition
specialist
Nutrition• Assessment of dietary habits• Tailor dietary recommendations to individual
patient needs• Work with physician to address diet and
medication changes as needed given co-morbid condition profile
• Address patient nutrition education and skill deficiencies
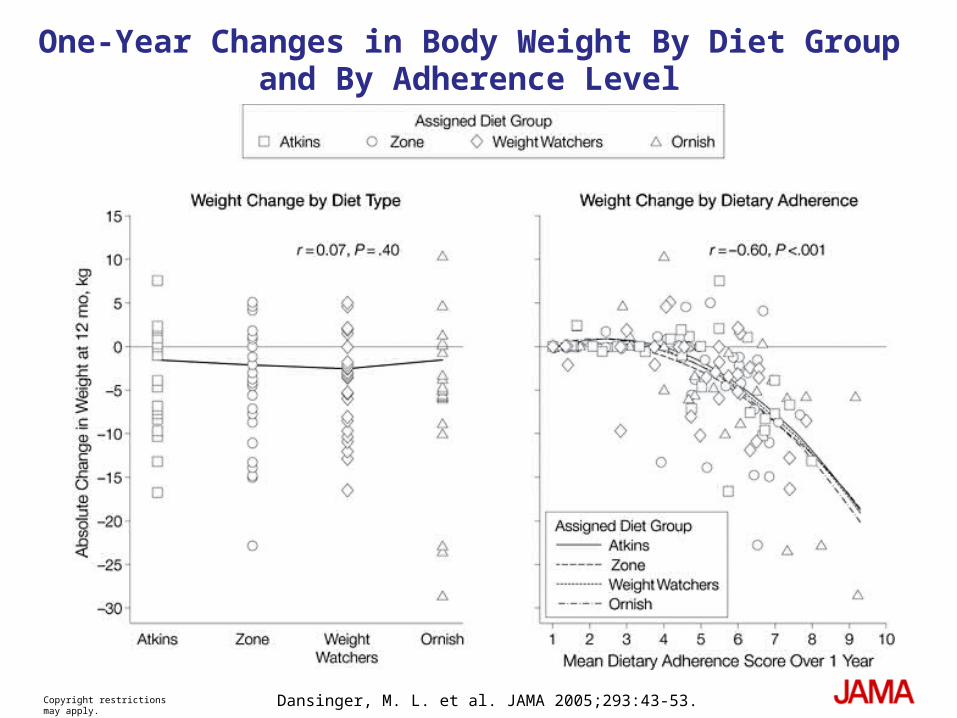
Copyright restrictions may apply. Dansinger, M. L. et al. JAMA 2005;293:43-53.
One-Year Changes in Body Weight By Diet Group and By Adherence Level
Exercise
• Physical activity evaluation performed by an exercise physiologist or personal trainer
Exercise
• Role of the exercise physiologist and/or personal trainer includes:– Assessment of exercise tolerance,
metabolic fitness, and cardiovascular risk– Create an individualized exercise
prescription
WHAT NEW WEIGHT LOSS MEDICATIONS WILL BE AVAILABLE?
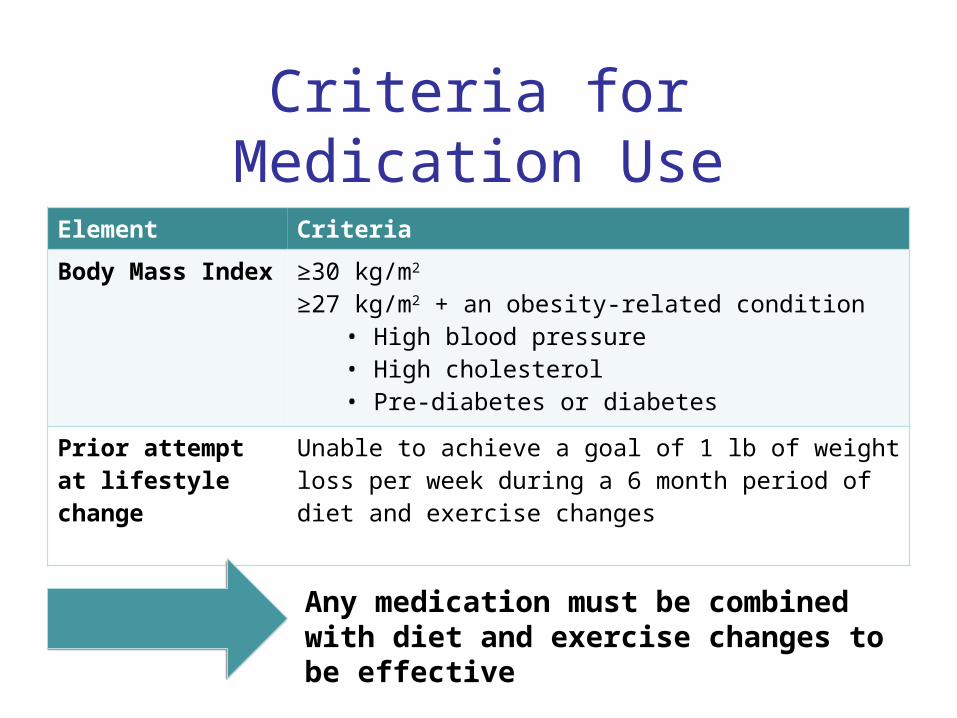
Criteria for Medication Use
Element Criteria
Body Mass Index ≥30 kg/m2 ≥27 kg/m2 + an obesity-related condition
• High blood pressure• High cholesterol• Pre-diabetes or diabetes
Prior attempt at lifestyle change
Unable to achieve a goal of 1 lb of weight loss per week during a 6 month period of diet and exercise changes
Any medication must be combined with diet and exercise changes to be effective
Patient Counseling• Expected weight loss • Potential side effects and risks• Interactions with other medications
Medication selected should be tailored to best suit each individual patient
QSYMIA
• Combination of phentermine and topiramate
• Works by suppressing the appetite
• Patients lost between 11-24 lbs at 12 months
QSYMIA
• Common side effects include tingling, dizziness, increased heart rate, and depressed mood.
• May not be a good choice if you have heart, liver or kidney disease
• Causes birth defects
BELVIQ
• New medication that targets a special Serotonin neurotransmitter receptor
• Works by suppressing the appetite
• Patients lost 10-12 lbs at 12 months
BELVIQ
• Common side effects include headache, dizziness, nausea, drowsiness
• May not be a good choice if you have heart, liver, or kidney disease
What current medication options do I have?
ALLI (orlistat)• Works by blocking
absorption of fat • Common side effects
include abdominal cramping, bloating, diarrhea
• May not be a good choice if you have gastrointestinal issues or liver disease
ADIPEX (phentermine)• Works by suppressing the
appetite• Common side effects
include headache, dizziness, nausea
• May not be a good choice if you have heart, liver, or kidney disease
Digestive Weight Loss Center
2360 W. Joppa Rd, Suite 200
Lutherville, MD 21093
410-583-LOSE
http://www.hopkinsmedicine.org/digestive_weight_loss_center/index.html

Janelle W. Coughlin, Ph.D.Johns Hopkins School of Medicine
Department of Psychiatry and Behavioral Sciences
Johns Hopkins Medicine International Partners ForumOctober 2, 2012
Behavioral Lifestyle Interventions for Obesity: The Foundation for Change

Objectives
To describe important components of behavioral lifestyle interventions for obesity
To summarize outcomes achieved with behavioral lifestyle interventions for obesity
To highlight recent innovative developments in behavioral lifestyle interventions for obesity

Surgery
Pharmacotherapy
Lifestyle Modification
Diet Physical Activity
BMI
Obesity Treatment Pyramid

Dietary Approaches to Lifestyle Modification
Calorie Deficit ~1200-2000 kcal/d
Dietary Approaches:Low-fatLow-carbohydrateMediterranean Low-glycemic loadPortion-controlled
diets

Increasing Physical Activity
> 180 m/wk MVPA for weight loss Must also include caloric restrictionAssociated with a number of health improvements,
independent of weight lossCritical for long-term weight loss maintenance
~ 60 m/d MVPACan be performed in short boutsIncreasing other lifestyle activities is also
effective > 2000 steps for weight loss; > 6000 to avoid
regain

Behavioral Strategies•Self-monitoring•Goal Setting•Stimulus control•Problem solving•Cognitive restructuring•Relapse Prevention
Increase self-efficacy and social support
Motivational Interviewing

Weight Loss MaintenancePatients gain ~
1/3 of their lost weight in the year following treatment
Nearly half of participants return to their original weight within 5 years
1:6 adults accomplish > 1 yr of maintaining > 10% of IBW
There is significant evidence that weight loss maintenance interventions can decrease the chance of weight regain
Regular ongoing contact following initial weight loss is perhaps the most successful method of preventing weight regain

Study DesignPhase IN=1685
Behavioral weight loss intervention
Weight loss ≥4 kg
Yes No
Phase II Randomization
N=1032
Self-directed control group
Personal Contact
Interactive Technology
No furthercontact
Phase I6 months
Phase II30 months
Data collection prior to Phase I, at randomization, then every 6 months

Change from initial weight
-10
-8
-6
-4
-2
0
-6 0 6 12 18 24 30
Months after Randomization
Wei
ght
chan
ge,
kg
Self-directed Interactive technology Personal Contact
-2.9 -3.3 -4.2
Svetkey et al., 2008

Remote/Telephone-delivered
Technology-Based
PCP-Enhanced or Promoted

Design
Control
Remote
In-Person
Randomization
= Measured weights and other outcomes
Baseline 6 Mo 12 Mo 24 Mo

InterventionsRemote In-Person
Mode of Delivery Telephone only Group meetingsIndividual meetings
Telephone
Coach Healthways Hopkins
Coach support Case management
Study website Educational modules Self-monitoring tools
Tailored emails
Physician Roles SupportiveReview weight progress reports

0 6 12 24-8
-6
-4
-2
0
2
Control Remote In-Person
Months after Randomization
We
igh
t ch
an
ge
, kg
-4.6*
-0.8
-4.3*
*P <0.001 (vs control)Appel et al, NEJM 2011;365:1959-68


Surgery
Pharmacotherapy
Lifestyle Modification
Diet Physical Activity
BMI
Does lifestyle modification enhance the effects of weight loss medications and surgery?

Thank You
Wadden et al., (March, 2012). Circulation




















![Dombrowski-Argument From Marginal Cases (JHI 45.1 [1984])](https://img.pdfslide.net/doc/110x75/577cd2a31a28ab9e7895b0f5/dombrowski-argument-from-marginal-cases-jhi-451-1984.jpg)


![Passmore-Treatment of Animals (JHI 36.2 [1975])](https://img.pdfslide.net/doc/110x75/577cc10f1a28aba711922032/passmore-treatment-of-animals-jhi-362-1975.jpg)






