Embed Size (px)
Citation preview
Corporate presentation - June, 2016
The HDL Company

Disclaimer
This document has been prepared by Cerenis Therapeutics (the "Company") and is for information purposes only.
The information and opinions contained in this document are provided as of the date of this document only and may be updated,supplemented, revised, verified or amended, and thus such information may be subject to significant changes. The Company is not underany obligation to update the information or opinions contained herein which are subject to change without prior notice.The information contained in this document has not been subject to independent verification. No representation, warranty orundertaking, express or implied, is made as to the accuracy, completeness or appropriateness of the information and opinions containedin this document. The Company, its subsidiaries, its advisors and representatives accept no responsibility for and shall not be held liablefor any loss or damage that may arise from the use of this document or the information or opinions contained herein.This document contains information on the Company’s markets and competitive position, and more specifically, on the size of its markets.This information has been drawn from various sources or from the Company’s own estimates. Investors should not base their investmentdecision on this information.This document contains certain forward-looking statements. These statements are not guarantees of the Company's future performance.These forward-looking statements relate to the Company's future prospects, developments and marketing strategy and are based onanalyses of earnings forecasts and estimates of amounts not yet determinable. Forward-looking statements are subject to a variety ofrisks and uncertainties as they relate to future events and are dependent on circumstances that may or may not materialize in the future.Forward-looking statements cannot, under any circumstance, be construed as a guarantee of the Company's future performance and theCompany’s actual financial position, results and cash flow, as well as the trends in the sector in which the Company operates, may differmaterially from those proposed or reflected in the forward-looking statements contained in this document. Even if the Company’sfinancial position, results, cash-flows and developments in the sector in which the Company operates were to conform to the forward-looking statements contained in this document, such results or developments cannot be construed as a reliable indication of theCompany's future results or developments. The Company does not undertake any obligation to update or to confirm projections orestimates made by analysts or to make public any correction to any prospective information in order to reflect an event or circumstancethat may occur after the date of this document.This document does not constitute an offer to sell or subscribe or a solicitation to purchase or subscribe for securities in France, theUnited States or any other jurisdiction. Securities may not be offered or sold in the United States absent registration under the USSecurities Act of 1933, as amended, or an exemption from registration thereunder. No public offering of securities may be conducted inFrance or abroad prior to the delivery by the French Autorité des marchés financiers (Financial Markets Authority) of a visa on aprospectus that complies with the provisions of Directive 2003/71/CE as amended. No offering of securities is contemplated in France orany jurisdiction outside France.
2Corporate Presentation| June 2016

Jean-Louis DASSEUX, PhD, MBA
Founder and CEO Over 25 years of experience in the pharmaceutical industry (Pfizer,
Esperion Therapeutics, Fournier Laboratories)
A leading world expert in lipid metabolism, atherosclerosis and cardiovascular diseases
Inventor of more than 60 patent families relating to HDL and the treatment of cardiovascular diseases
Cyrille TUPIN, CPA
CFO
Audit Director at Sygnatures, the largest private auditing and consulting company in Toulouse, France
More than 7 years at PWC working on high-profile business transactions
3
An experienced Management
Corporate Presentation| June 2016
Cardiovascular Disease: Still an unmet medical need after more than 30 years of existing therapy
4
ONLY ONE REAL SOLUTION: ELIMINATE CHOLESTEROL PLAQUE WITH CERENIS
1 out of 3 deaths worldwide (source: WHO)
The disease category with the greatest health expenditure:
– $107 bn in the United States, in 2010
– $110 bn in Europe, in 2009
Leading cause of death in the world
Only 1/3 of the cardiovascular risk is targeted by the best current treatments
A primary cause: atherosclerosis
Atherosclerosis: accumulation of cholesterol plaque in the arteries
Corporate Presentation| June 2016

How to eliminate the build-up of cholesterol plaque
5
HDL: THE SOLUTION FOR EFFICIENTLY REMOVING CHOLESTEROL
Food
Liver
Elimination
Artery
Badcholesterol: LDL 1
Goodcholesterol: HDL 2
Causes atherosclerosis Removes cholesterolfrom artery walls
1. LDL: Low Density Lipoprotein2. HDL: High Density Lipoprotein
Corporate Presentation| June 2016
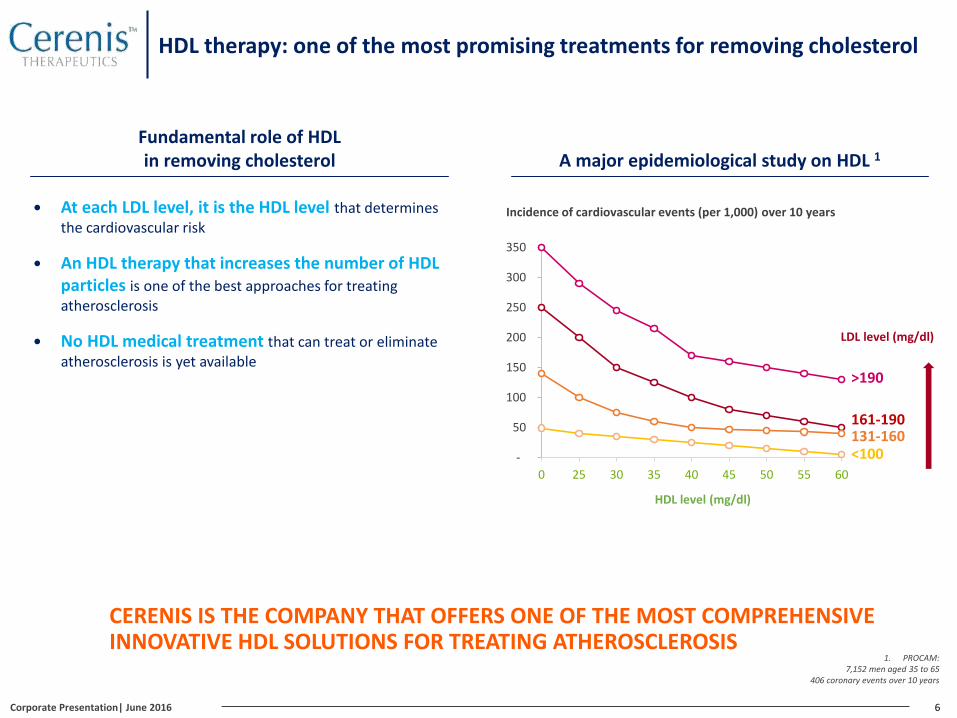
HDL therapy: one of the most promising treatments for removing cholesterol
6
Fundamental role of HDLin removing cholesterol
At each LDL level, it is the HDL level that determines the cardiovascular risk
An HDL therapy that increases the number of HDL particles is one of the best approaches for treating atherosclerosis
No HDL medical treatment that can treat or eliminate atherosclerosis is yet available
A major epidemiological study on HDL 1
Incidence of cardiovascular events (per 1,000) over 10 years
-
50
100
150
200
250
300
350
0 25 30 35 40 45 50 55 60
HDL level (mg/dl)
161-190131-160
>190
<100
LDL level (mg/dl)
CERENIS IS THE COMPANY THAT OFFERS ONE OF THE MOST COMPREHENSIVEINNOVATIVE HDL SOLUTIONS FOR TREATING ATHEROSCLEROSIS
1. PROCAM: 7,152 men aged 35 to 65
406 coronary events over 10 years
Corporate Presentation| June 2016

7
2005: creation of Cerenis 2015 2016 2017 2018
Product Indications
CER-001(HDLmimetic)
Post Acute Coronary Syndrome(ACS)
HDL genetic defects (FPHA 1)
CER-209(P2Y13 receptor agonist)
NAFLD/NASH/Atherosclerosis
Financing to date
Investors
Phase I
Phase II
Request for marketing approval
2nd Phase II
€25 m in 2005 €50 m in 2010€42 m in 2006
1st Phase II
Orphan disease designation
Preclinical development
POC 2
IPO:€53.4 m in 2015
POC 2
Preclinical development
Preclinical Clinical
Phase I Phase III
1. Familial Primary Hypoalphalipoproteinemia2. Proof of Concept
AMM
10 years of R&D to achieve one of the world’s most advanced HDL solutions
Preclinical development undergoing
POC 2 Clinical development plan to be defined
3 TARGETED INDICATIONS: ACS, FPHA AND NAFLD/NASH/ATHEROSCLEROSIS
Corporate Presentation| June 2016
Contents
Highlights since IPO
Potential for development in a large market
An HDL therapy with a validated manufacturing process
Compelling clinical results
1
2
3
4
8Corporate Presentation| June 2016

Part 1
Potential for development in a large market
10
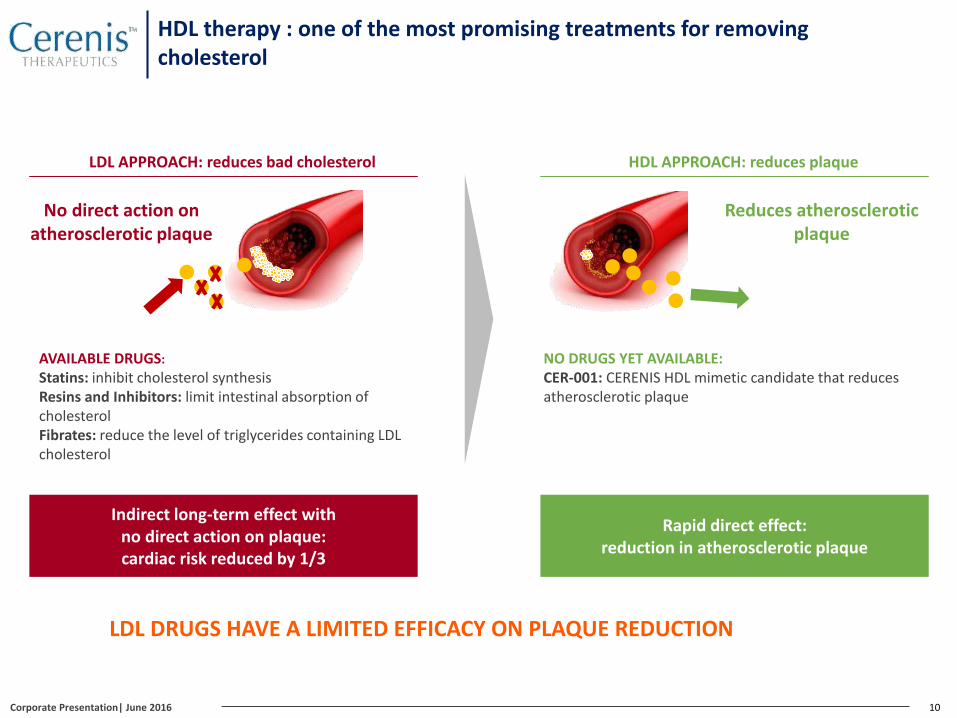
LDL DRUGS HAVE A LIMITED EFFICACY ON PLAQUE REDUCTION
Indirect long-term effect with no direct action on plaque:cardiac risk reduced by 1/3
LDL APPROACH: reduces bad cholesterol
Rapid direct effect: reduction in atherosclerotic plaque
HDL APPROACH: reduces plaque
Reduces atheroscleroticplaque
AVAILABLE DRUGS:
Statins: inhibit cholesterol synthesisResins and Inhibitors: limit intestinal absorption of cholesterolFibrates: reduce the level of triglycerides containing LDLcholesterol
No direct action on atherosclerotic plaque
NO DRUGS YET AVAILABLE:CER-001: CERENIS HDL mimetic candidate that reduces atherosclerotic plaque
HDL therapy : one of the most promising treatments for removing cholesterol
Corporate Presentation| June 2016
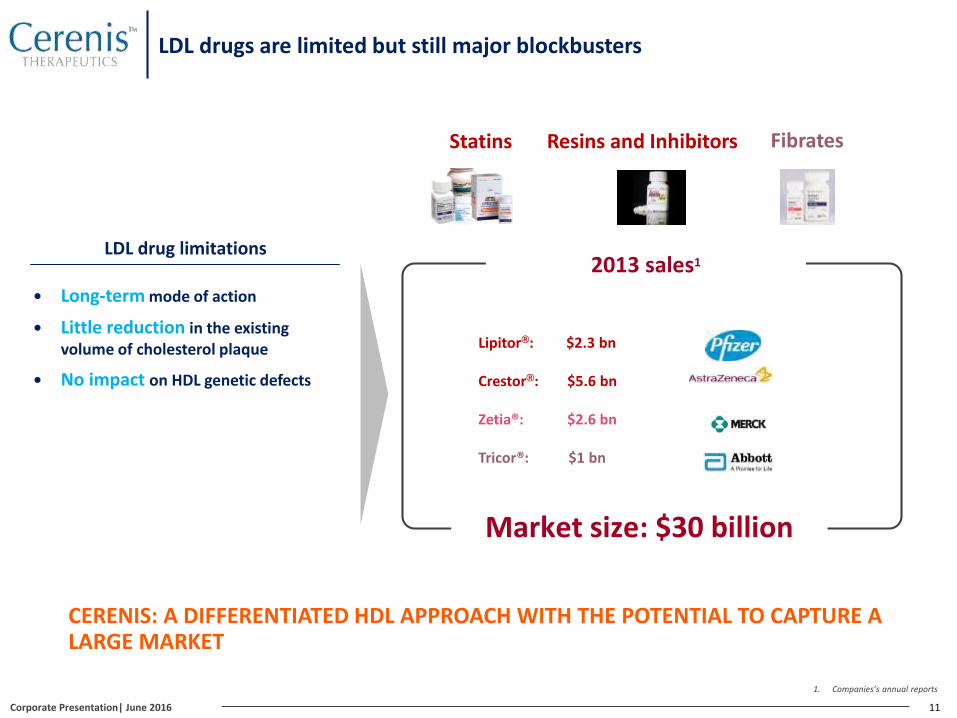
LDL drugs are limited but still major blockbusters
11
Lipitor®: $2.3 bn
Crestor®: $5.6 bn
Zetia®: $2.6 bn
Tricor®: $1 bn
Market size: $30 billion
2013 sales1
Statins Resins and Inhibitors Fibrates
LDL drug limitations
Long-term mode of action
Little reduction in the existing volume of cholesterol plaque
No impact on HDL genetic defects
CERENIS: A DIFFERENTIATED HDL APPROACH WITH THE POTENTIAL TO CAPTURE A LARGE MARKET
1. Companies’s annual reports
Corporate Presentation| June 2016
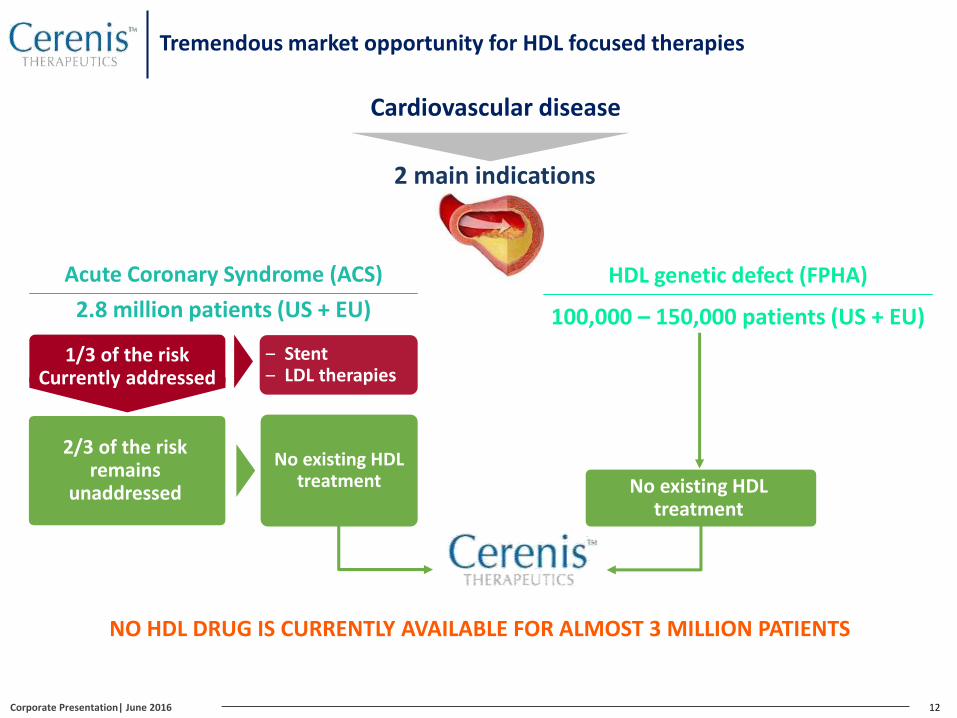
2 main indications
2.8 million patients (US + EU)
Acute Coronary Syndrome (ACS)
12
NO HDL DRUG IS CURRENTLY AVAILABLE FOR ALMOST 3 MILLION PATIENTS
Cardiovascular disease
100,000 – 150,000 patients (US + EU)
HDL genetic defect (FPHA)
No existing HDLtreatment
No existing HDLtreatment
‒ Stent‒ LDL therapies
2/3 of the risk remains
unaddressed
1/3 of the risk Currently addressed
Tremendous market opportunity for HDL focused therapies
Corporate Presentation| June 2016

13
12% 2 of patients relapse during the 12 months following an ACS, 2/3 of them during the first 2 months
19-26% 3 of patients over 45 years old die during the 12 months that follow a cardiovascular event
ACS hospitalization costs: $20,000 - $60,000 per patient per event
HDL THERAPY IS THE ONLY SOLUTION FOR THE CRITICAL 2-MONTH POST-ACS PERIOD
1. Vale N. et al Cochrane Database of Systematic Reviews 2014, Issue 9.2. PLATO clinical study, AstraZeneca
3. Source: AHS
Cardiovascular risk (relapse + mortality)
Critical period:the first 2 months
Rapid action Long-term action
1 year2 months
12%
HDL therapy:CERENIS LDL drugs (address 1/3 of the risk)
STATINS1, FIBRATES, RESINS
Value proposition: HDL therapy for ACS
Corporate Presentation| June 2016
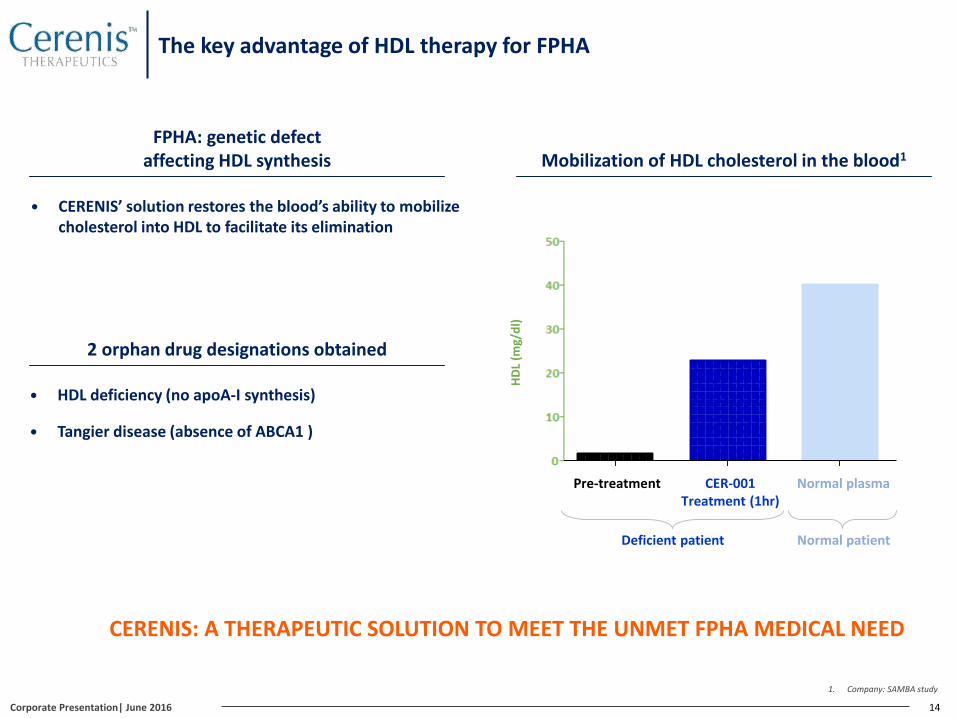
The key advantage of HDL therapy for FPHA
14
CERENIS: A THERAPEUTIC SOLUTION TO MEET THE UNMET FPHA MEDICAL NEED
HDL deficiency (no apoA-I synthesis)
Tangier disease (absence of ABCA1 )
FPHA: genetic defect affecting HDL synthesis
CERENIS’ solution restores the blood’s ability to mobilize cholesterol into HDL to facilitate its elimination
Mobilization of HDL cholesterol in the blood1
HD
L (m
g/d
l)
Pre-treatment CER-001 Treatment (1hr)
Normal plasma
Deficient patient Normal patient
2 orphan drug designations obtained
0
10
20
30
40
50
HD
L (
mg
/dl)
1. Company: SAMBA study
Corporate Presentation| June 2016
CER-209, a potential breakthrough treatmentfor Atherosclerosis and Nonalcoholic Steatohepatitis (NASH)
15
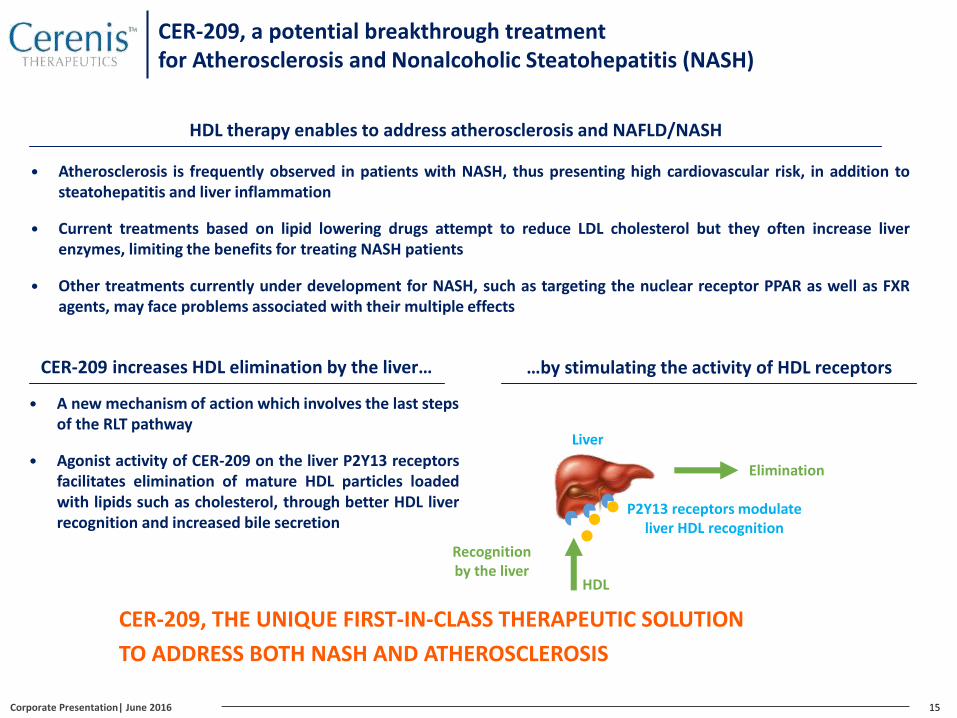
HDL therapy enables to address atherosclerosis and NAFLD/NASH
Atherosclerosis is frequently observed in patients with NASH, thus presenting high cardiovascular risk, in addition tosteatohepatitis and liver inflammation
Current treatments based on lipid lowering drugs attempt to reduce LDL cholesterol but they often increase liverenzymes, limiting the benefits for treating NASH patients
Other treatments currently under development for NASH, such as targeting the nuclear receptor PPAR as well as FXRagents, may face problems associated with their multiple effects
Liver
Elimination
P2Y13 receptors modulate liver HDL recognition
HDL
CER-209 increases HDL elimination by the liver…
A new mechanism of action which involves the last steps of the RLT pathway
Agonist activity of CER-209 on the liver P2Y13 receptorsfacilitates elimination of mature HDL particles loadedwith lipids such as cholesterol, through better HDL liverrecognition and increased bile secretion
CER-209, THE UNIQUE FIRST-IN-CLASS THERAPEUTIC SOLUTION
TO ADDRESS BOTH NASH AND ATHEROSCLEROSIS
…by stimulating the activity of HDL receptors
Recognition by the liver
Corporate Presentation| June 2016
NASH: a worldwide health issue
16
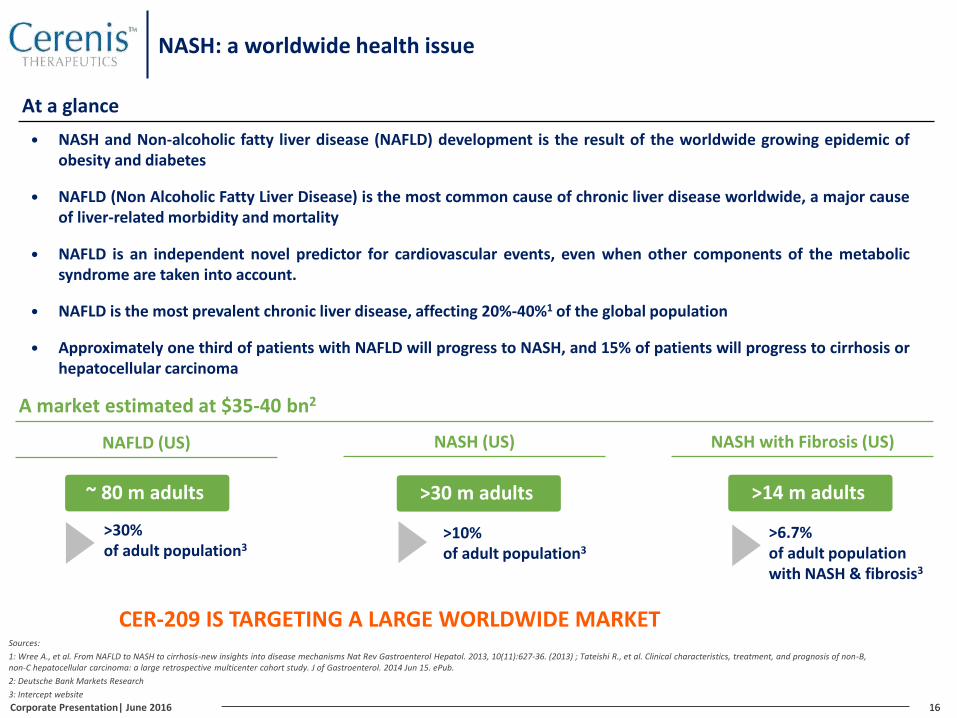
A market estimated at $35-40 bn2
NAFLD (US)
>30% of adult population3
NASH (US)
>10% of adult population3
NASH with Fibrosis (US)
>6.7% of adult populationwith NASH & fibrosis3
NASH and Non-alcoholic fatty liver disease (NAFLD) development is the result of the worldwide growing epidemic ofobesity and diabetes
NAFLD (Non Alcoholic Fatty Liver Disease) is the most common cause of chronic liver disease worldwide, a major causeof liver-related morbidity and mortality
NAFLD is an independent novel predictor for cardiovascular events, even when other components of the metabolicsyndrome are taken into account.
NAFLD is the most prevalent chronic liver disease, affecting 20%-40%1 of the global population
Approximately one third of patients with NAFLD will progress to NASH, and 15% of patients will progress to cirrhosis orhepatocellular carcinoma
~ 80 m adults >30 m adults >14 m adults
At a glance
Sources:
1: Wree A., et al. From NAFLD to NASH to cirrhosis-new insights into disease mechanisms Nat Rev Gastroenterol Hepatol. 2013, 10(11):627-36. (2013) ; Tateishi R., et al. Clinical characteristics, treatment, and prognosis of non-B, non-C hepatocellular carcinoma: a large retrospective multicenter cohort study. J of Gastroenterol. 2014 Jun 15. ePub.
2: Deutsche Bank Markets Research
3: Intercept website
CER-209 IS TARGETING A LARGE WORLDWIDE MARKET
Corporate Presentation| June 2016
Part 2
An HDL therapy with a validated manufacturing process
18
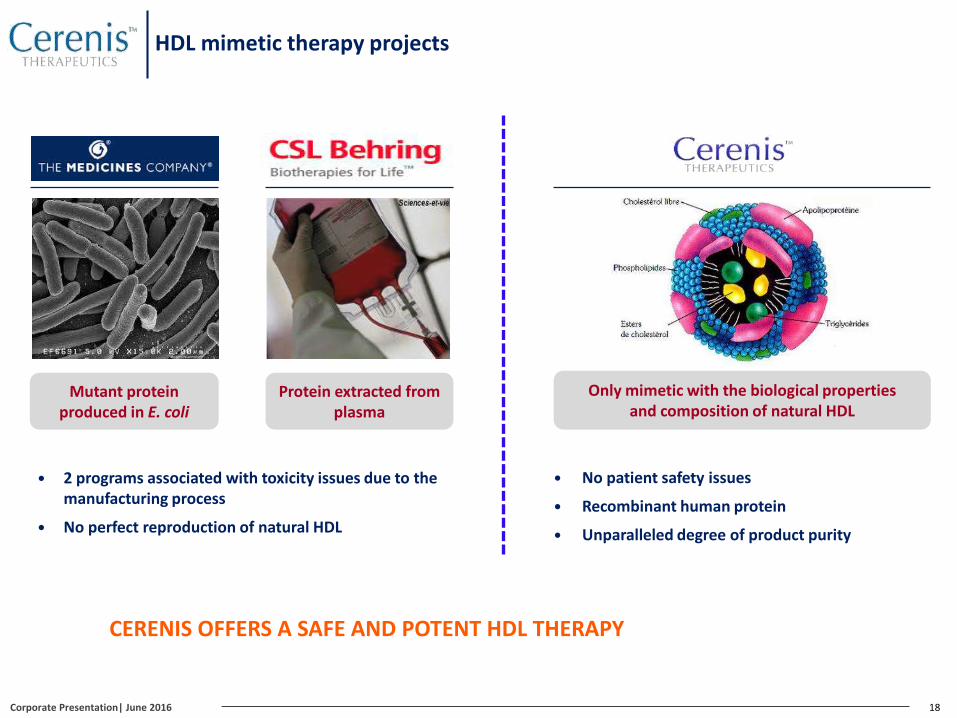
CERENIS OFFERS A SAFE AND POTENT HDL THERAPY
Mutant protein produced in E. coli
Protein extracted from plasma
Only mimetic with the biological properties and composition of natural HDL
2 programs associated with toxicity issues due to the manufacturing process
No perfect reproduction of natural HDL
No patient safety issues
Recombinant human protein
Unparalleled degree of product purity
HDL mimetic therapy projects
Corporate Presentation| June 2016
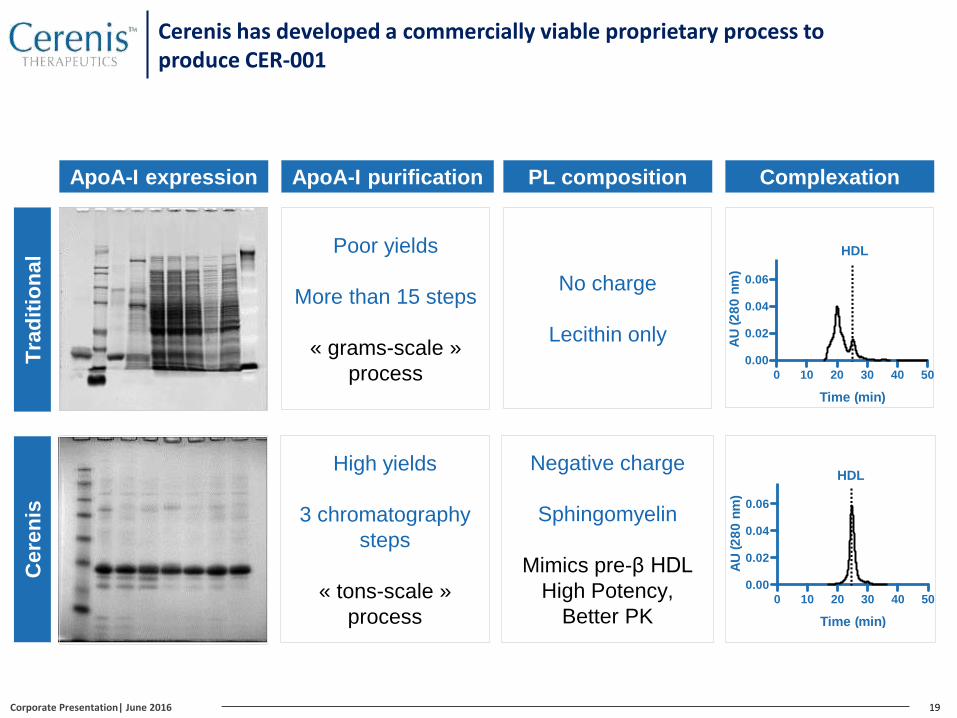
Cerenis has developed a commercially viable proprietary process to produce CER-001
19
Poor yields
More than 15 steps
« grams-scale »
process
High yields
3 chromatography
steps
« tons-scale »
process
Tra
dit
ion
al
Cere
nis
0 10 20 30 40 50
0.00
0.02
0.04
0.06
Time (min)
AU
(2
80
nm
)
0 10 20 30 40 50
0.00
0.02
0.04
0.06
Time (min)
AU
(2
80
nm
)
HDL
HDL
No charge
Lecithin only
Negative charge
Sphingomyelin
Mimics pre-β HDL
High Potency,
Better PK
ApoA-I purification ComplexationPL compositionApoA-I expression
Corporate Presentation| June 2016
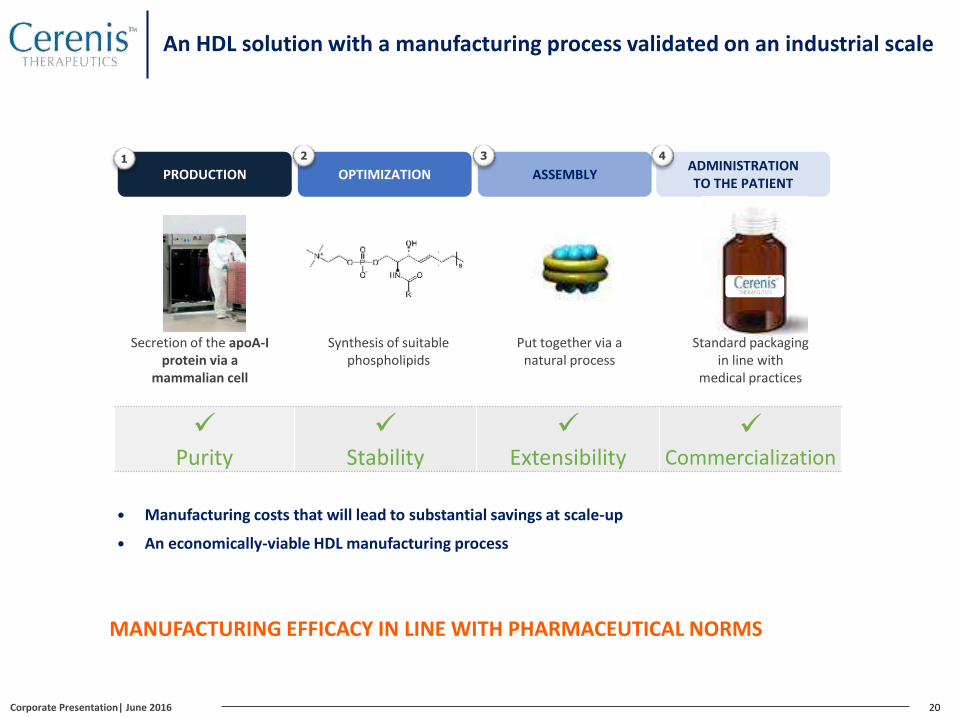
An HDL solution with a manufacturing process validated on an industrial scale
20
OPTIMIZATION
2
PRODUCTION ASSEMBLY
31
Purity
Stability
Extensibility
Commercialization
Secretion of the apoA-I protein via a
mammalian cell
Synthesis of suitable phospholipids
Put together via a natural process
ADMINISTRATION TO THE PATIENT
4
Manufacturing costs that will lead to substantial savings at scale-up
An economically-viable HDL manufacturing process
MANUFACTURING EFFICACY IN LINE WITH PHARMACEUTICAL NORMS
Standard packaging in line with
medical practices
Corporate Presentation| June 2016
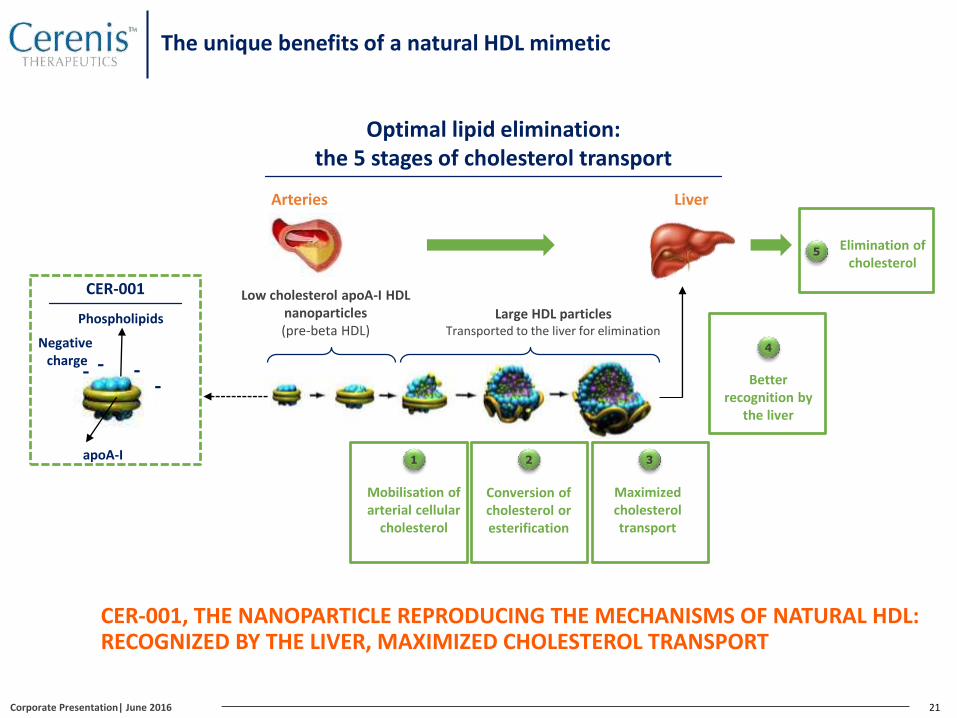
21
Optimal lipid elimination: the 5 stages of cholesterol transport
LiverArteries
Low cholesterol apoA-I HDL nanoparticles(pre-beta HDL)
1 2
Large HDL particlesTransported to the liver for elimination
3
Mobilisation of arterial cellular
cholesterol
Conversion of cholesterol or esterification
Maximized cholesterol transport
Better recognition by
the liver
4
Elimination of cholesterol
5
Phospholipids
apoA-I
CER-001
- --
-
Negative charge
CER-001, THE NANOPARTICLE REPRODUCING THE MECHANISMS OF NATURAL HDL: RECOGNIZED BY THE LIVER, MAXIMIZED CHOLESTEROL TRANSPORT
The unique benefits of a natural HDL mimetic
Corporate Presentation| June 2016
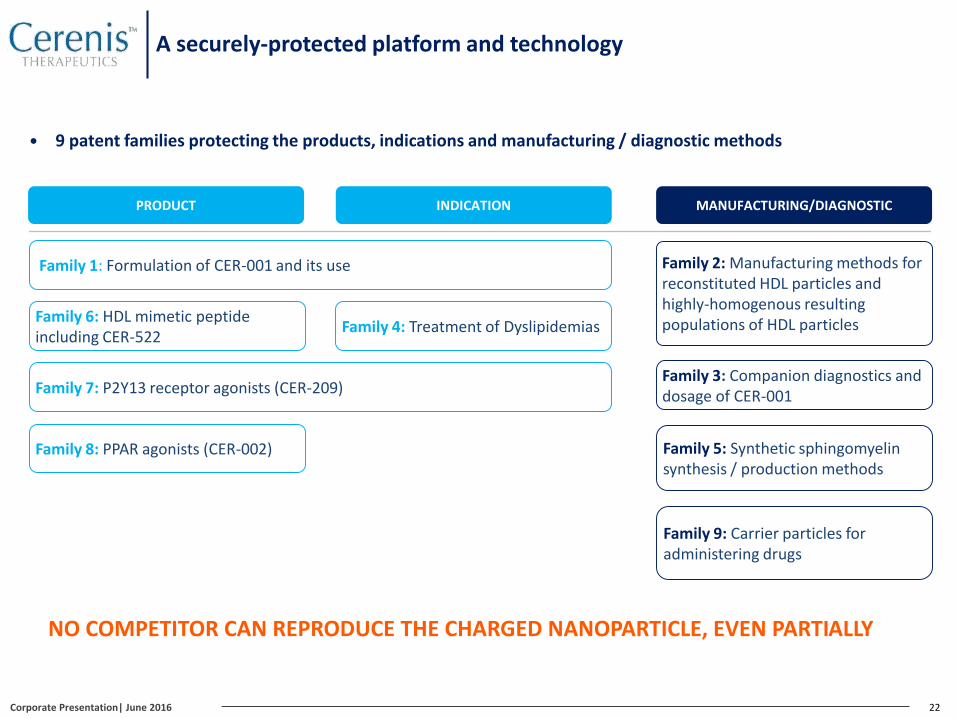
A securely-protected platform and technology
9 patent families protecting the products, indications and manufacturing / diagnostic methods
22
PRODUCT INDICATION MANUFACTURING/DIAGNOSTIC
Family 1: Formulation of CER-001 and its use Family 2: Manufacturing methods for reconstituted HDL particles and highly-homogenous resulting populations of HDL particles
Family 3: Companion diagnostics and dosage of CER-001
Family 4: Treatment of Dyslipidemias
Family 5: Synthetic sphingomyelinsynthesis / production methods
Family 6: HDL mimetic peptide including CER-522
Family 7: P2Y13 receptor agonists (CER-209)
Family 8: PPAR agonists (CER-002)
Family 9: Carrier particles for administering drugs
NO COMPETITOR CAN REPRODUCE THE CHARGED NANOPARTICLE, EVEN PARTIALLY
Corporate Presentation| June 2016

A safe and industrializable natural mimetic solution
CERENISThe Medicines
CompanyCSL
Product specificity
Only mimetic with the biological properties of natural HDL
Mutant protein produced in an E.colibacteria
Protein extracted from plasma
Composition of the nanoparticle
Natural HDL mimetic Mutant formMultiple forms of A-I apolipoprotein
Competitive advantage of CER-001
Purity Homogenous particle population
Mobilization of cholesterol / Efficacy Lower required dosage
Side effects/Toxicity No identified toxicity
Intellectual property Protection of the active principle blocking
any reproduction of the nanoparticle
Composition Only charged-complexnatural HDL mimetic
Manufacturing process Only 3 purification steps
23Corporate Presentation| June 2016

Part 3
Compelling clinical results
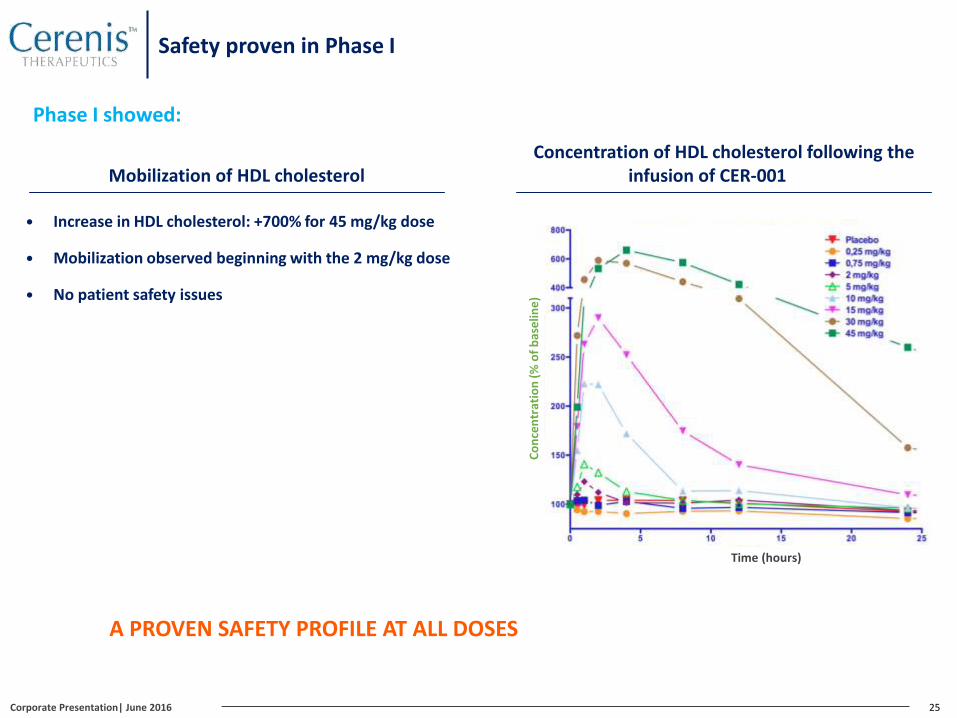
Safety proven in Phase I
25
A PROVEN SAFETY PROFILE AT ALL DOSES
Mobilization of HDL cholesterol
Increase in HDL cholesterol: +700% for 45 mg/kg dose
Mobilization observed beginning with the 2 mg/kg dose
No patient safety issues
Concentration of HDL cholesterol following the infusion of CER-001
Phase I showed:
Co
nce
ntr
atio
n (
% o
fb
ase
line
)
Time (hours)
Corporate Presentation| June 2016
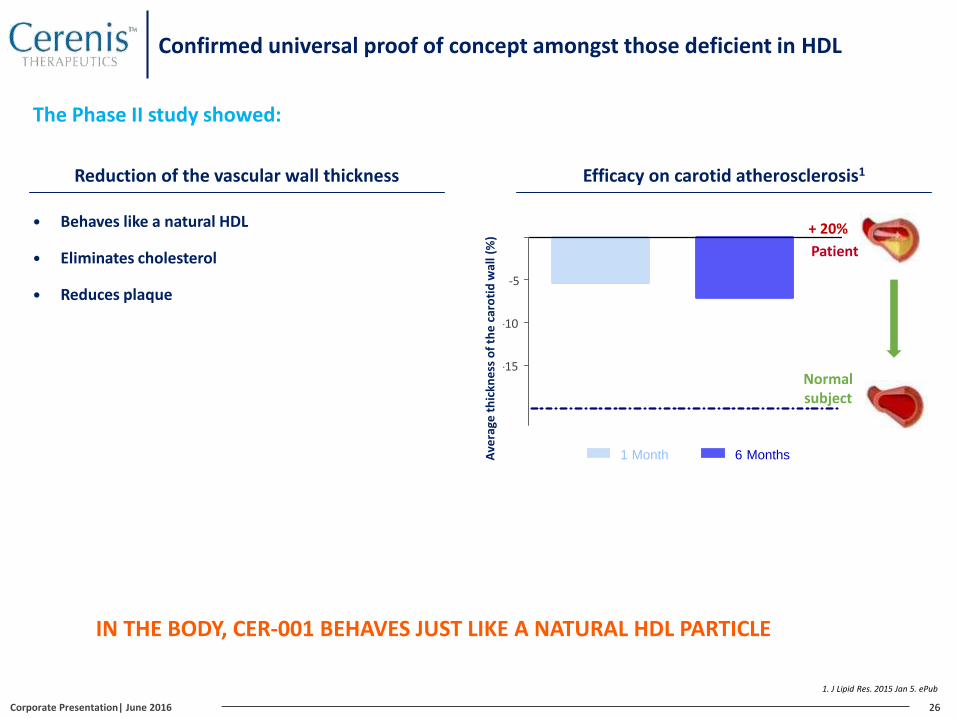
Confirmed universal proof of concept amongst those deficient in HDL
26
IN THE BODY, CER-001 BEHAVES JUST LIKE A NATURAL HDL PARTICLE
-15
-10
-5
1 Month 6 Months
+ 20%
Normal subject
Reduction of the vascular wall thickness
Behaves like a natural HDL
Eliminates cholesterol
Reduces plaque
The Phase II study showed:
Efficacy on carotid atherosclerosis1
Patient
Ave
rage
th
ickn
ess
of
the
car
oti
d w
all (
%)
1. J Lipid Res. 2015 Jan 5. ePub
Corporate Presentation| June 2016
27
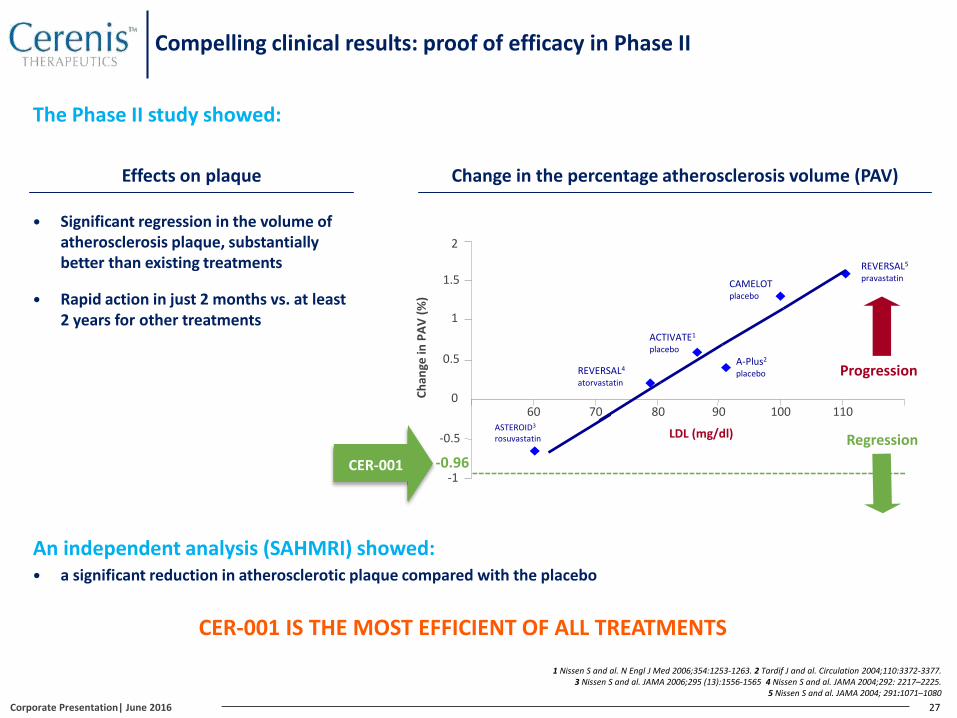
An independent analysis (SAHMRI) showed: a significant reduction in atherosclerotic plaque compared with the placebo
Change in the percentage atherosclerosis volume (PAV)
CAMELOT placebo
ACTIVATE1
placebo
REVERSAL4
atorvastatin
2
Ch
ange
in P
AV
(%)
-1
-0.5
0
0.5
1
1.5
60 70 80 90 100 110
A-Plus2
placebo
REVERSAL5
pravastatin
LDL (mg/dl)
Progression
ASTEROID3
rosuvastatin
CER-001
Regression
-0.96
CER-001 IS THE MOST EFFICIENT OF ALL TREATMENTS
Effects on plaque
Significant regression in the volume of atherosclerosis plaque, substantially better than existing treatments
Rapid action in just 2 months vs. at least 2 years for other treatments
The Phase II study showed:
1 Nissen S and al. N Engl J Med 2006;354:1253-1263. 2 Tardif J and al. Circulation 2004;110:3372-3377. 3 Nissen S and al. JAMA 2006;295 (13):1556-1565 4 Nissen S and al. JAMA 2004;292: 2217–2225.
5 Nissen S and al. JAMA 2004; 291:1071–1080
Compelling clinical results: proof of efficacy in Phase II
Corporate Presentation| June 2016
28
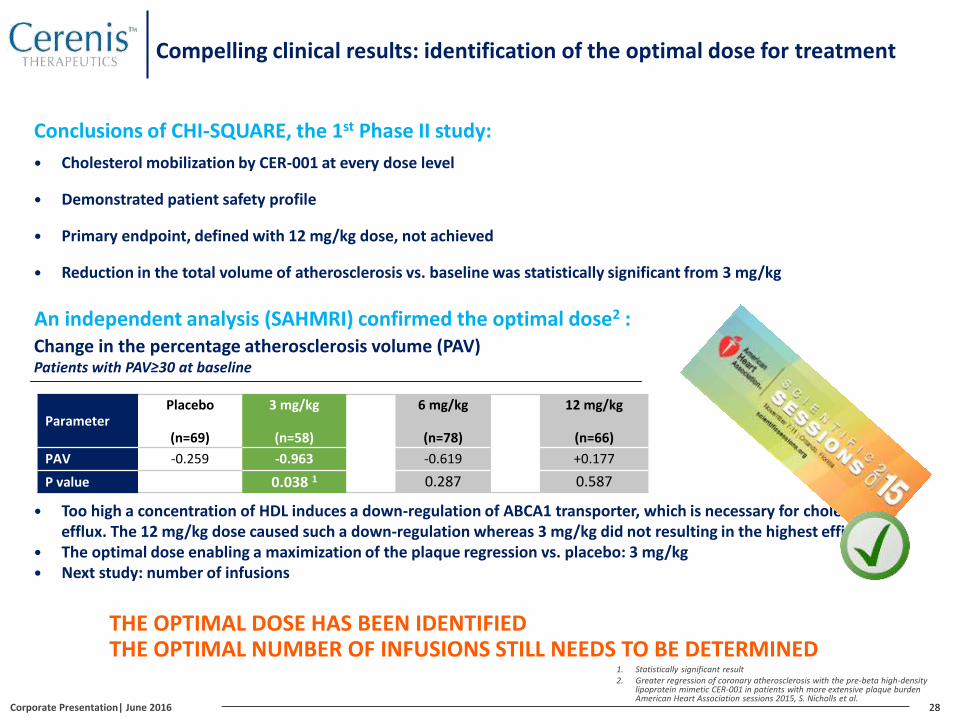
THE OPTIMAL DOSE HAS BEEN IDENTIFIED THE OPTIMAL NUMBER OF INFUSIONS STILL NEEDS TO BE DETERMINED
An independent analysis (SAHMRI) confirmed the optimal dose2 :
Conclusions of CHI-SQUARE, the 1st Phase II study:
Cholesterol mobilization by CER-001 at every dose level
Demonstrated patient safety profile
Primary endpoint, defined with 12 mg/kg dose, not achieved
Reduction in the total volume of atherosclerosis vs. baseline was statistically significant from 3 mg/kg
Too high a concentration of HDL induces a down-regulation of ABCA1 transporter, which is necessary for cholesterol efflux. The 12 mg/kg dose caused such a down-regulation whereas 3 mg/kg did not resulting in the highest efficacy
The optimal dose enabling a maximization of the plaque regression vs. placebo: 3 mg/kg Next study: number of infusions
Change in the percentage atherosclerosis volume (PAV)Patients with PAV≥30 at baseline
1. Statistically significant result2. Greater regression of coronary atherosclerosis with the pre-beta high-density
lipoprotein mimetic CER-001 in patients with more extensive plaque burden American Heart Association sessions 2015, S. Nicholls et al.
Compelling clinical results: identification of the optimal dose for treatment
ParameterPlacebo
(n=69)
3 mg/kg
(n=58)
6 mg/kg
(n=78)
12 mg/kg
(n=66)
PAV -0.259 -0.963 -0.619 +0.177
P value 0.038 1 0.287 0.587
Corporate Presentation| June 2016

29
CER-001 induced greater plaque regression in patients with baseline PAV≥ 30%
An inverse relationship was observed between CER-001 dose and effect on plaque burden
These findings identify patients who are most likely to benefit from CER-001 infusions and the most biologically active dose
Greater regression of coronary atherosclerosis with the pre-beta high-density lipoprotein mimetic CER-001 in patients with more extensive plaque burden
American Heart Association sessions 2015, S. Nicholls et al.
Corporate Presentation| June 2016
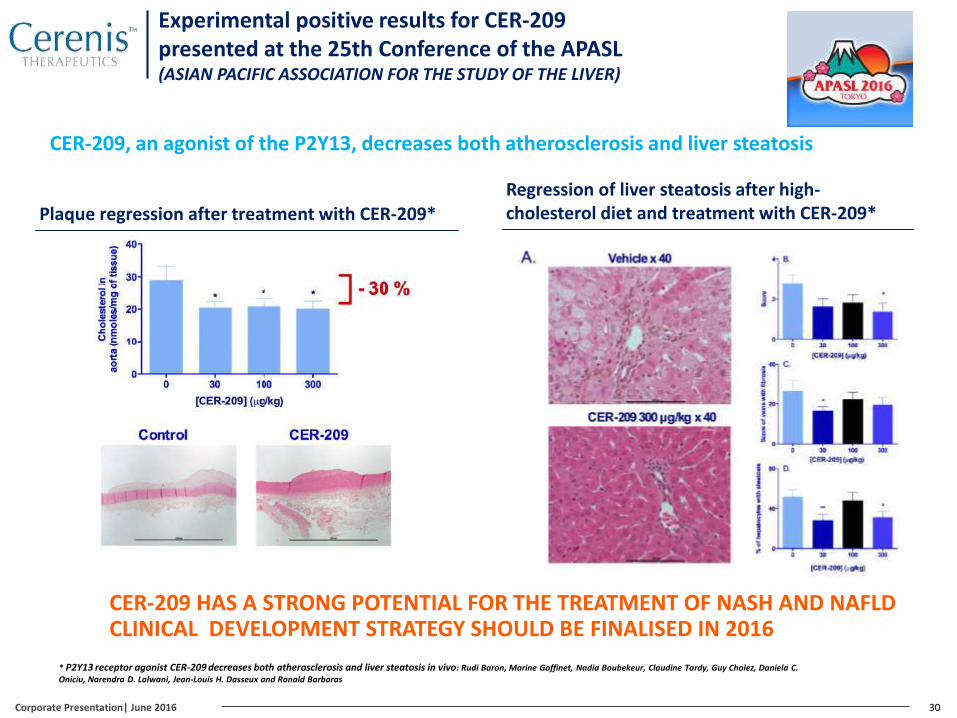
Experimental positive results for CER-209 presented at the 25th Conference of the APASL(ASIAN PACIFIC ASSOCIATION FOR THE STUDY OF THE LIVER)
CER-209, an agonist of the P2Y13, decreases both atherosclerosis and liver steatosis
30Corporate Presentation| June 2016
CER-209 HAS A STRONG POTENTIAL FOR THE TREATMENT OF NASH AND NAFLDCLINICAL DEVELOPMENT STRATEGY SHOULD BE FINALISED IN 2016
Plaque regression after treatment with CER-209*Regression of liver steatosis after high-cholesterol diet and treatment with CER-209*
* P2Y13 receptor agonist CER-209 decreases both atherosclerosis and liver steatosis in vivo: Rudi Baron, Marine Goffinet, Nadia Boubekeur, Claudine Tardy, Guy Cholez, Daniela C.
Oniciu, Narendra D. Lalwani, Jean-Louis H. Dasseux and Ronald Barbaras

Indications Preclinical Phase I Phase II Phase III
Products due to enter a new development phase
CER-001RecombinantHDL
Post-ACS
FPHA:Orphan diseaseApoA-I and ABCA1 deficiency
CER-209Stimulation of HDL receptors
Dyslipidemia with low HDL
Non-alcoholic steatohepatitis(NASH/NAFLD/Atherosclerosis)
Products in the portfolio
CER-522(back-up)
Peptide HDLMimetic
Aortic Valve Stenosis
CER-002Specific PPARdelta agonist
Dyslipidemia with low HDL
Non-alcoholic steatohepatitis (NASH)
Systemic Lupus Erythematosus (SLE)
Future growth drivers
31
A structured and diversified portfolio
Corporate Presentation| June 2016

Part 4
Highlights since IPO
A successful IPO success
33
GROSS PRODUCT• €53.4 m based on a price of €12.70 per share (top of the price range)
• 4,207,316 new shares issued
GLOBAL DEMAND
• Global placement: €120 m
• Open Price Offering (OPO): €35 m
• Offer oversubscribed: 3.8 times
REMINDER OF THE USE
OF PROCEEDS
• Finance all the costs of the Phase II study on the post-ACS prevention indication (CARAT), the results of whichshould be available during the first quarter of 2017, including the manufacturing costs of the tested product ;
• Finance all the Phase III study costs on the indication of the orphan disease PFHA (TANGO), including themanufacturing costs of the tested product. This Phase III study (TANGO) will support the market authorization forCER-001 by 2018 ;
• Finance the Company’s working capital.
SHARE INFORMATION
• 1st listing: March 30, 2015 on Euronext Paris (Compartiment B)
• Market price*: €8.40
• Market capitalization*: €149 m
• 3 months average daily volume*: 18 232
• Isin code: FR0012616852
• Mnemonic: CEREN
* Data as of 10/06/2016
MARCH 2015
Corporate Presentation| June 2016

Poster presentation at the 2015 ISA*(International Symposium on Atherosclerosis, Amsterdam)
34
CER-209, A POTENTIAL FIRST-IN-CLASS TREATMENTADDRESSING BOTH NAFLD/NASH AND ATHEROSCLEROSIS
Validation of a promising new mechanism of action focused on the treatment of both atherosclerosis and non-alcoholic steatohepatitis (NASH). CER-209 acts as a selective novel agonist of the P2Y13r, responsible for HDL recognition by liver receptors which leads to increased cholesterol and triglyceride elimination by the liver
A good preclinical safety profile
Significant decrease of liver steatosis content in the liver (NASH)
Observable decrease of atherosclerotic plaques in aorta
Preclinical models conclusion for CER-209 :
Decrease of steatohepatitis*
* Validated preclinical models: CER-209 administration following a cholesterol-intensive diet
Decrease of atherosclerotic plaques
MAY 2015
Corporate Presentation| June 2016

Appointment of two new Board Members
35
STRENGTHENING THE COMPANY’S ABILITY TO SUPERVISE ITS STRATEGY
Catherine Moukheibir, MA, MBA (Yale University)
Dr. Laura A. Coruzzi Esq., Ph.D. (University of Fordham, Mount Sinai School of Medicine)
20 years of experience in finance including 15 in the biotechnology industry
Executive board member at Innate Pharma
CFO of Movetis : leading both Euronext Brussels IPO and takeover by Shire
Director Capital Markets at ZETIA
Executive Director : Salomon Smith Barney, Morgan Stanley
Senior Vice President of Intellectual Property at REGENXBIO. Prior she was a partner in the Intellectual Property practice at Jones Day
Deeply involved in developing patent strategies related to HDL mimetics and Reverse Lipid Transport (RLT) modulating drugs
Has represented clients in biotechnology and pharmaceuticals for 30 years, participating in numerous landmark cases
Extensive experience in patent prosecution, litigation and appeals before the USPTO Board of Appeals, the Federal Circuit, and the U.S. Supreme Court
JUNE 2015
Corporate Presentation| June 2016
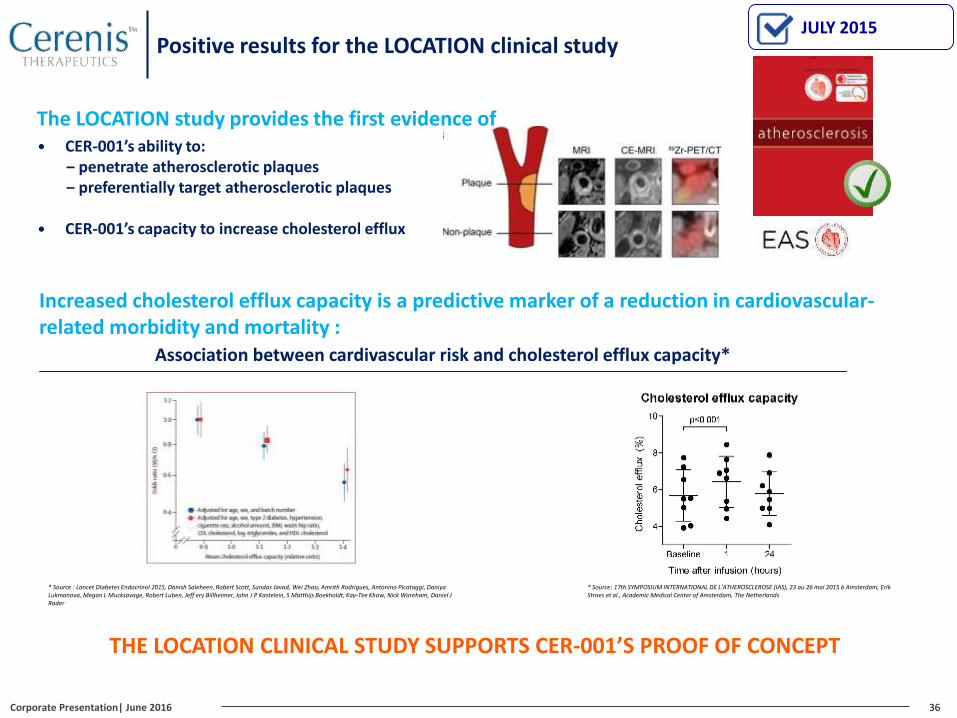
Positive results for the LOCATION clinical study
36
THE LOCATION CLINICAL STUDY SUPPORTS CER-001’S PROOF OF CONCEPT
The LOCATION study provides the first evidence of CER-001’s ability to:
‒ penetrate atherosclerotic plaques‒ preferentially target atherosclerotic plaques
CER-001’s capacity to increase cholesterol efflux
Increased cholesterol efflux capacity is a predictive marker of a reduction in cardiovascular-related morbidity and mortality :
Association between cardivascular risk and cholesterol efflux capacity*
* Source : Lancet Diabetes Endocrinol 2015, Danish Saleheen, Robert Scott, Sundas Javad, Wei Zhao, Amrith Rodrigues, Antonino Picataggi, DaniyaLukmanova, Megan L Mucksavage, Robert Luben, Jeff ery Billheimer, John J P Kastelein, S Matthijs Boekholdt, Kay-Tee Khaw, Nick Wareham, Daniel J Rader
JULY 2015
* Source: 17th SYMPOSIUM INTERNATIONAL DE L’ATHEROSCLEROSE (IAS), 23 au 26 mai 2015 a Amsterdam, Erik Stroes et al., Academic Medical Center of Amsterdam, The Netherlands
Corporate Presentation| June 2016
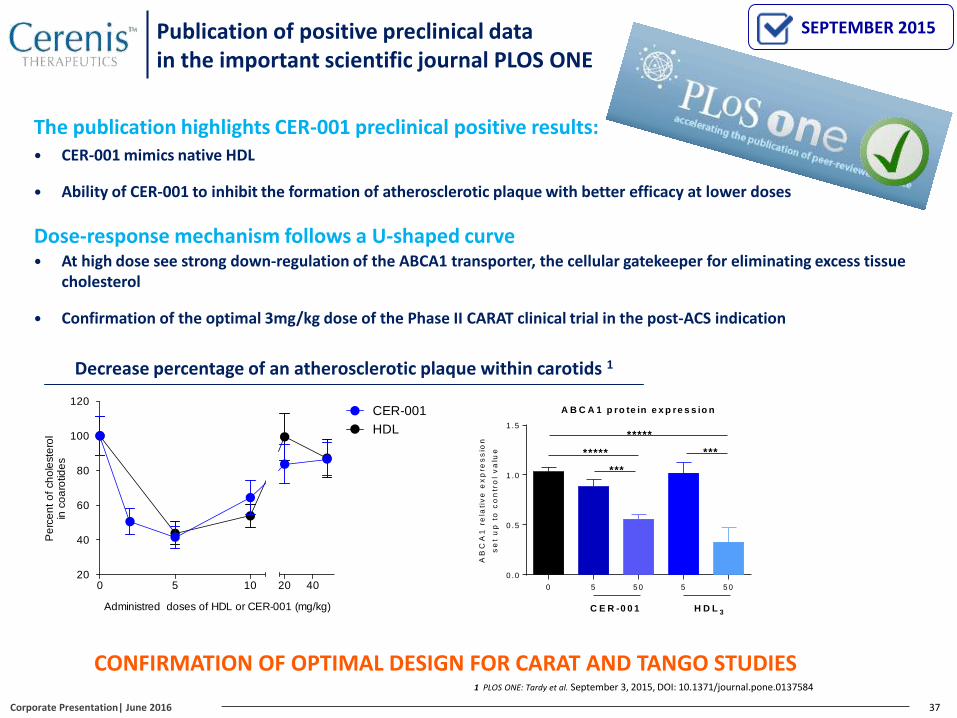
At high dose see strong down-regulation of the ABCA1 transporter, the cellular gatekeeper for eliminating excess tissue cholesterol
Confirmation of the optimal 3mg/kg dose of the Phase II CARAT clinical trial in the post-ACS indication
Dose-response mechanism follows a U-shaped curve
Publication of positive preclinical datain the important scientific journal PLOS ONE
37
CONFIRMATION OF OPTIMAL DESIGN FOR CARAT AND TANGO STUDIES
The publication highlights CER-001 preclinical positive results: CER-001 mimics native HDL
Ability of CER-001 to inhibit the formation of atherosclerotic plaque with better efficacy at lower doses
Decrease percentage of an atherosclerotic plaque within carotids 1
SEPTEMBER 2015
0 5 10 20 4020
40
60
80
100
120
Administred doses of HDL or CER-001 (mg/kg)
Pe
rce
nt
of
ch
ole
ste
rol
in c
oa
rotid
es
Percent of regression of atheroma plaques in carotides
CER-001
HDL
1 PLOS ONE: Tardy et al. September 3, 2015, DOI: 10.1371/journal.pone.0137584
A B C A 1 p ro te in e x p re s s io n
0 5 5 0 5 5 0
0 .0
0 .5
1 .0
1 .5
AB
CA
1 r
ela
tiv
e e
xp
res
sio
n
se
t u
p t
o c
on
tro
l v
alu
e *****
*****
C E R -0 0 1 H D L 3
***
***
Corporate Presentation| June 2016

CER-001: the future benchmark in HDL mimetic
Professor Stephen Nicholls“I’m particularly enthusiastic about collaborating with Cerenis
Therapeutics for the future Phase II CARAT clinical study of
CER-001. On the basis of our convincing analyses of the Phase
II CHI-SQUARE study highlighting the efficacy of the optimal
3mg/kg dose, I’m highly confident regarding the potential
success of this important clinical step to establish CER-001 as
the market benchmark in HDL mimetic.
38
Dr. John Kastelein
Dr. Béla Merkely
Dr. Stephen Nicholls, Principal Investigator
Dr. Steven Nissen
Dr. Kausik Ray
Dr. Gregory Schwartz
Dr. Stephen Worthley
A prestigious steering committee for the CARAT Study
Corporate Presentation| June 2016
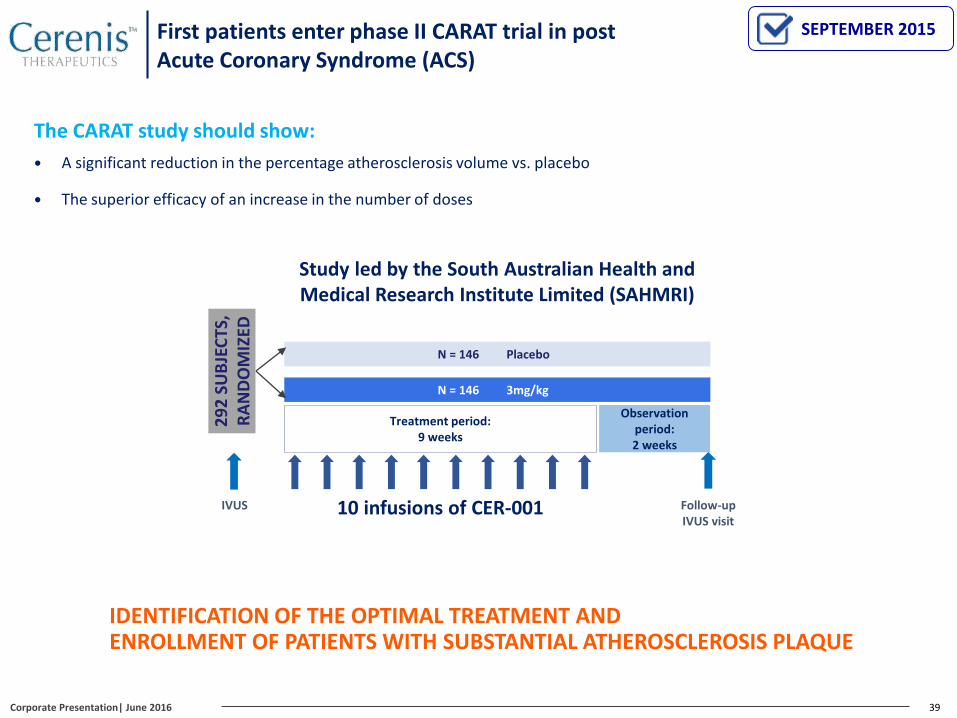
39
N = 146 Placebo
N = 146 3mg/kg
29
2 S
UB
JEC
TS,
RA
ND
OM
IZED
10 infusions of CER-001
Treatment period:9 weeks
Observation period:2 weeks
Follow-up IVUS visit
IDENTIFICATION OF THE OPTIMAL TREATMENT AND ENROLLMENT OF PATIENTS WITH SUBSTANTIAL ATHEROSCLEROSIS PLAQUE
The CARAT study should show:
A significant reduction in the percentage atherosclerosis volume vs. placebo
The superior efficacy of an increase in the number of doses
IVUS
Study led by the South Australian Health and Medical Research Institute Limited (SAHMRI)
First patients enter phase II CARAT trial in post Acute Coronary Syndrome (ACS)
SEPTEMBER 2015
Corporate Presentation| June 2016
40
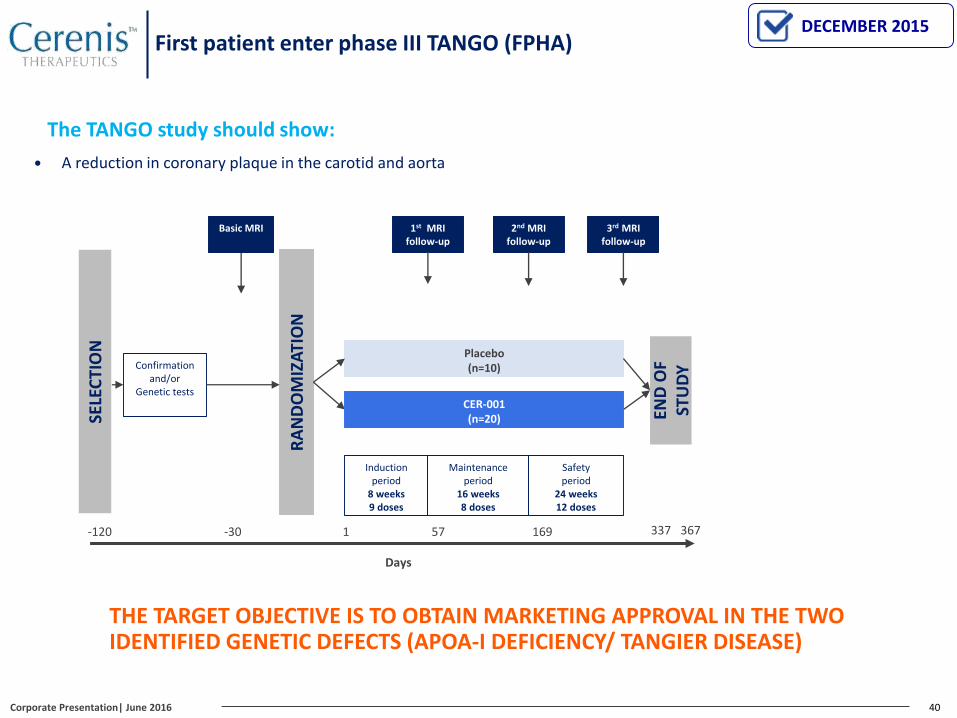
THE TARGET OBJECTIVE IS TO OBTAIN MARKETING APPROVAL IN THE TWO IDENTIFIED GENETIC DEFECTS (APOA-I DEFICIENCY/ TANGIER DISEASE)
SELE
CTI
ON
1st MRI follow-up
-120 1 57 337
Days
END
OF
STU
DY
169
Confirmation and/or
Genetic tests
RA
ND
OM
IZA
TIO
N
CER-001(n=20)
Placebo(n=10)
2nd MRI follow-up
3rd MRI follow-up
Induction period
8 weeks9 doses
Maintenance period
16 weeks8 doses
Safety period
24 weeks12 doses
367
Basic MRI
-30
The TANGO study should show:
A reduction in coronary plaque in the carotid and aorta
First patient enter phase III TANGO (FPHA)DECEMBER 2015
Corporate Presentation| June 2016

NAFLD/NASH/Atherosclerosis development
FPHA development, TANGO
Post-ACS development, CARAT
41
WEALTH CREATION PERSPECTIVE IN BOTH THE SHORT AND MEDIUM TERM
1st patient enrolled, FPHA study ✔
2015Q1
2015Q2
2015Q3
2015Q4
2016Q1
2016Q2
2016Q3
2016Q4
2017Q1
2017Q2
2017Q3
2017Q4
2018Q1
2018Q2
2018Q3
2018Q4
Last patient enrolled, FPHA study
Last visit for patients enrolled in the FPHA study
Application filed for orphan diseases
FPHA results
1st patient enrolled, CARAT study ✔
Q1CARAT results
Market approval
LOCATION study ✔
Board appointments ✔
Poster at the IAS ✔
PLOS ONE Publication✔
Done Upcoming
Solid short & medium-run newsflow
Published Newsflow
Timeline to be defined
Q3Last patient enrolled, CARAT
Q4Last IVUS visit CARAT
Corporate Presentation| June 2016
Two poster presentations on CER-209 at the APASL✔
Publication of the LOCATION clinical study results in Atherosclerosis journal ✔
42
A LISTED COMPANY WITH SUBSTANTIAL POTENTIAL IN HDL THERAPY
1. A therapy targeting 2/3 of the risk that is unmet with available medical treatments
2. Advanced and promising clinical developments
3. Compelling to big pharma (ex. of transactions, OMTHERA: $443 m, Esperion: $1.3 bn, KOS: $3.7 bn)1
4. A manufacturing process validated on an industrial level
CER-001: major potential in the treatment of patients post-ACS
In the short term: CER-001, a drug for treating orphan diseases
1. A potential of value creation in the short term
2. A major unmet medical need
3. Application for marketing approval before 2018
1. Press releases,OMTHERA: http://www.astrazeneca.com/Media/Press-releases/Article/20130528-omthera
Esperion: http://www.bloomberg.com/apps/news?pid=newsarchive&sid=apU2qcYCmkO4&refer=usKOS: http://www.bloomberg.com/apps/news?pid=newsarchive&sid=af_8tglk4fHE
Value proposition: why invest in CERENIS?
CER-209: major potential in the treatment of patients with atherosclerosis and NAFLD/NASH
1. A major unmet medical need
2. CER-209, a highly specific P2Y13 receptor agonist promoting lipid elimination
Corporate Presentation| June 2016

APPENDICES
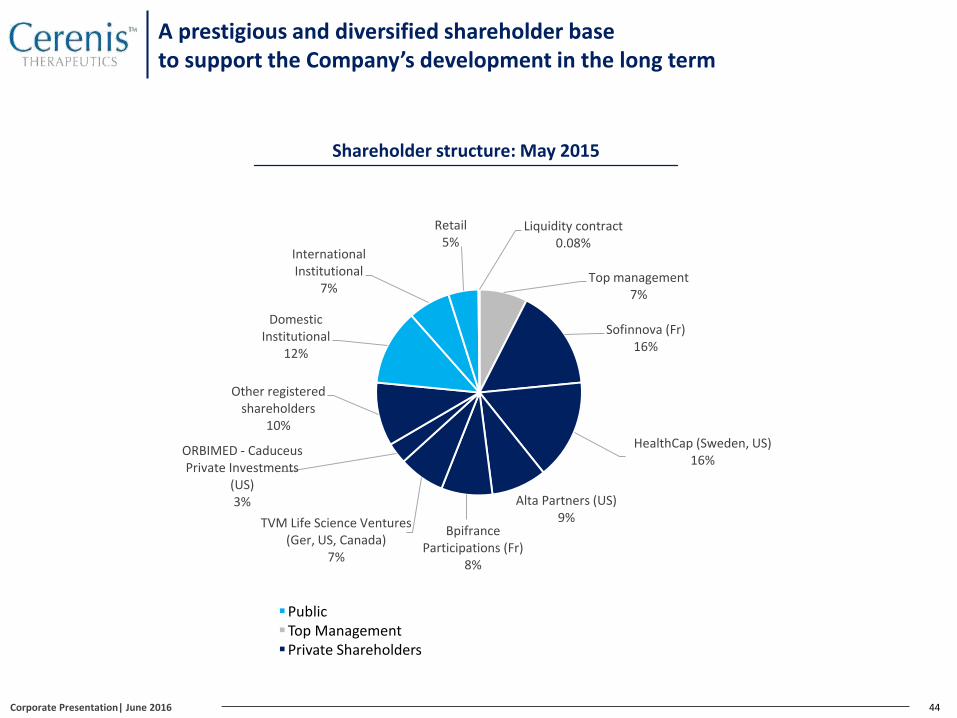
A prestigious and diversified shareholder base to support the Company’s development in the long term
44
Shareholder structure: May 2015
PublicTop ManagementPrivate Shareholders
Top management7%
Sofinnova (Fr)16%
HealthCap (Sweden, US)16%
Alta Partners (US)9%
Bpifrance Participations (Fr)
8%
TVM Life Science Ventures (Ger, US, Canada)
7%
ORBIMED - Caduceus Private Investments
(US)3%
Other registeredshareholders
10%
Domestic Institutional
12%
International Institutional
7%
Retail 5%
Liquidity contract0.08%
Corporate Presentation| June 2016
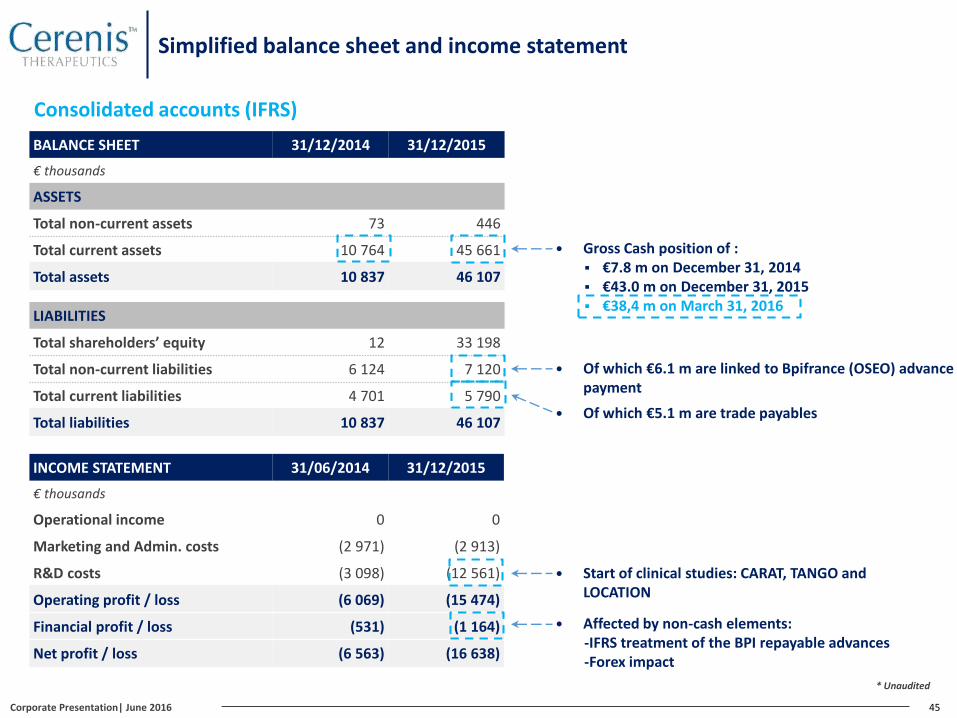
Simplified balance sheet and income statement
BALANCE SHEET 31/12/2014 31/12/2015
€ thousands
ASSETS
Total non-current assets 73 446
Total current assets 10 764 45 661
Total assets 10 837 46 107
LIABILITIES
Total shareholders’ equity 12 33 198
Total non-current liabilities 6 124 7 120
Total current liabilities 4 701 5 790
Total liabilities 10 837 46 107
INCOME STATEMENT 31/06/2014 31/12/2015
€ thousands
Operational income 0 0
Marketing and Admin. costs (2 971) (2 913)
R&D costs (3 098) (12 561)
Operating profit / loss (6 069) (15 474)
Financial profit / loss (531) (1 164)
Net profit / loss (6 563) (16 638)
Consolidated accounts (IFRS)
45
* Unaudited
Gross Cash position of : €7.8 m on December 31, 2014 €43.0 m on December 31, 2015 €38,4 m on March 31, 2016
Of which €6.1 m are linked to Bpifrance (OSEO) advancepayment
Affected by non-cash elements: -IFRS treatment of the BPI repayable advances-Forex impact
Start of clinical studies: CARAT, TANGO and LOCATION
Of which €5.1 m are trade payables
Corporate Presentation| June 2016
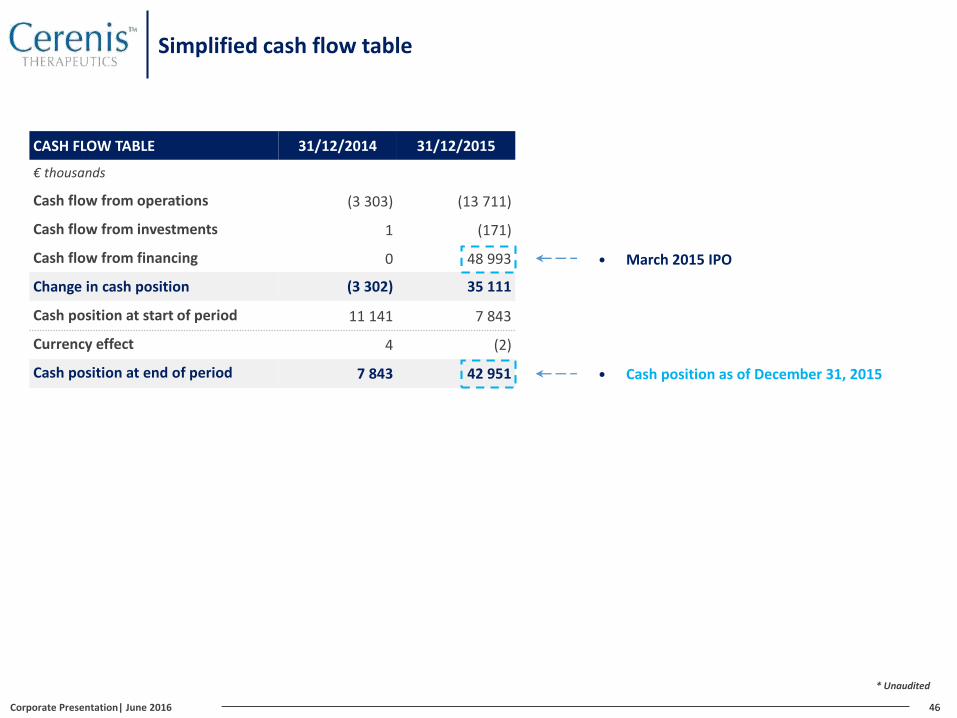
Simplified cash flow table
CASH FLOW TABLE 31/12/2014 31/12/2015
€ thousands
Cash flow from operations (3 303) (13 711)
Cash flow from investments 1 (171)
Cash flow from financing 0 48 993
Change in cash position (3 302) 35 111
Cash position at start of period 11 141 7 843
Currency effect 4 (2)
Cash position at end of period 7 843 42 951
46
* Unaudited
March 2015 IPO
Cash position as of December 31, 2015
Corporate Presentation| June 2016
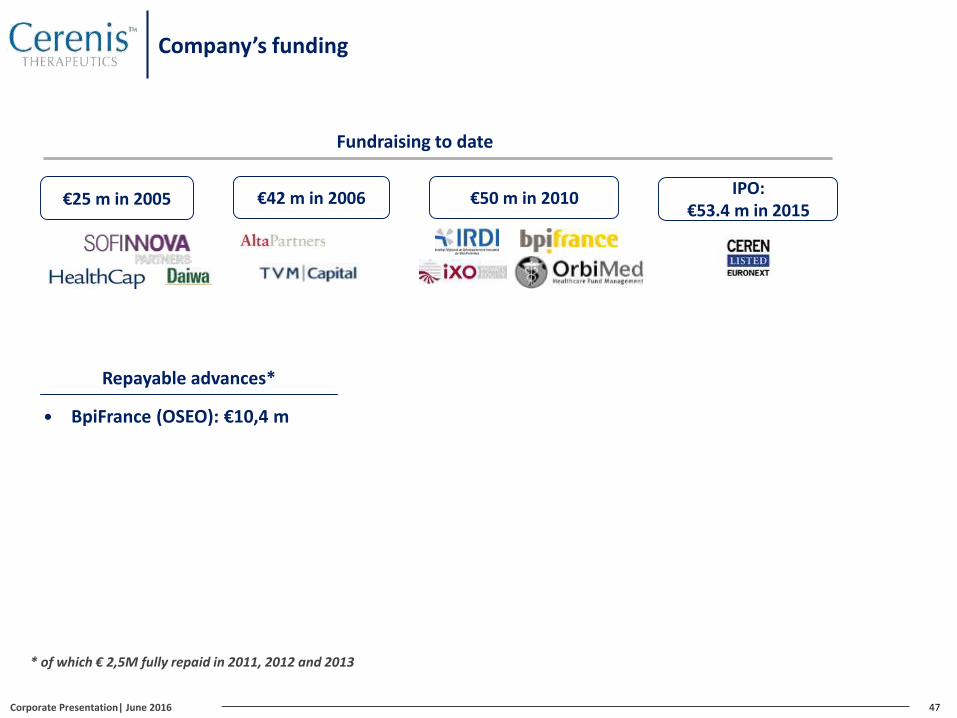
Company’s funding
47
Repayable advances*
BpiFrance (OSEO): €10,4 m
€25 m in 2005 €50 m in 2010€42 m in 2006
Fundraising to date
* of which € 2,5M fully repaid in 2011, 2012 and 2013
IPO: €53.4 m in 2015
Corporate Presentation| June 2016





























