Embed Size (px)
Citation preview
1

2
The Hippocratic Oath (Original Version)
“ I swear by Apollo the Physician and Asclepius and Hygieia and Panaceiaand all the gods, and goddesses, making them my witnesses, that I will fulfillaccording to my ability and judgment this oath and this covenant:
To hold him who has taught me this art as equal to my parents and to live my lifein partnership with him, and if he is in need of money to give him a share of mine, andto regard his offspring as equal to my brothers in male lineage and to teach them thisart–if they desire to learn it–without fee and covenant; to give a share of precepts andoral instruction and all the other learning to my sons and to the sons of him who hasinstructed me and to pupils who have signed the covenant and have taken the oathaccording to medical law, but to no one else.
I will follow that system of regimen which, according tomy ability and judgment,I consider for the benefit of my patients, and abstain from whatever is deleterious andmischievous. I will give no deadly medicine to any one if asked, nor suggest andy suchcounsel; and in like manner I will not give a woman a pessary to produce abortion.
With purity and with holiness I will pass my life and practice my Art. I will not cutpersons labouring under the stone, but will leave this to be done by men who arepractitioners of this work. Into what ever houses I enter, I will go into them for thebenefit of the sick, and will abstain from every voluntary act of mischief and corruption;and, further from the seduction of femals or males, of freemen and slaves.
WHATEVER, IN CONNECTION with my professional practice or not, in connectionwith it, I see or hear, in the life of men, which ought not to be spoken of abroad, I willnot divulge, as reckoning that all such should be kept secret.
WHILE I CONTINUE to keep this Oath unviolated, may it be granted to me to enjoylife and the practice of the art, respected by all men, in all times ! But should I trespassand violate this Oath, may the reverse be my lot !
3
“DHANVANTARI” – The Hindu God of Medicine“DHANVANTARI” is regarded as the original exponent of Indian Medicine.
DHANVANTARI has many myths and legends woven around him. He emergedwith the pot of ambrosia (symbolic of medicine) in his hand from the ocean when itis churned by the contesting gods and demons. He is viewed as the very incarnationof God VISHNU.
Legends make him reappear as “DIVODASA”, the prince of Benaras (Kasiraja),in the family of Ayus, Dhanvantari, Divodasa and Kasiraja are names of same personwho is “ the first God and who freed the other Gds from old age, disease and death”and who in his Himalaya retreat taught surgery to Susruta and other sages.DHANVANTARI appeared on earth in Benaras in the princely family of Bahuja andbecame known as DIvodasa: he wandered about as a mendicant even during his earlyyears.
DHANVANTARI is regarded as the patron-God of all branches of medicine.While DHANVANTARI is not credited with any medical treatise of his own, in theearly accounts, there is voluminous glossary and materia medica in nine sections knownas Dhanvantari Nighantu: it is a compilation which is probably contemporaneouswith the famous Amara –Kosha (A.D. 100).
4
INDEX
President, IMA MS DR . BAKULESH S. MEHTA (022) 26832359/9820131926 [email protected]. Past President, IMA MS DR. ARUN B. PAWADE (07157) 223750 / 9373240703 [email protected]. State Secretary, IMA MS Dr. HOZIE D. KAPADIA (022) 23711051 / 9322593005 [email protected]. Treasurer, IMA MS DR. SHIVKUMAR S. UTTURE (022) 24305373 / 9820089321 [email protected]. Vice President, IMA MS DR. M. S. PATWARDHAN (0233)2232104 / 9423036173Vice President, IMA MS DR. T. C. RATHOD (07232) 245186 / 9422168300 [email protected] President, IMA MS DR. RAVINDRA D. JAGTAP (02166) 222998 / 9921992168 [email protected] President, IMA MS DR. ANIL SUCHAK (022) 2889148 /9820080151Hon. Jt. Secretary, IMA MS DR. ANIL LADDHAD (0712) 2765287 / 9822565225Hon. Jt. Secretary, IMA MS Dr. SANJEEV SHARANGPANI (02355) 256565 / 260665 / [email protected]
9422429224 [email protected]. Jt. Secretary, IMA MS DR. JAYESH M. LELE (022) 28823408 / 981981296 [email protected], IMA MS SSS DR. ANIL J. TALATHI (02143) 252261 / 9422594236 [email protected]. Secretary, IMA MS SSS DR. SHRIKANT H. KOTHARI (022) 25171198 /25001269/ [email protected]
9821012970Hon. Treasurer, IMA MS SSS DR. SHAILENDRA C. MEHTALIA (022) 25132114 / 9820377174 [email protected] of Studies DR. AKIL CONTRACTOR (022) 26127481 / 9892084360 [email protected] MS CGP FacultyHon. Secretary, DR. DILIP G. DEODHAR Tel. (020) 24334136 / 9371005036IMA MS CGP FacultyHon. Jt. Secretary, DR. VIVEK BILLAMPELLY Tel. (020) 26832658 / 9822894963 [email protected] MS CGP FacultyChairman, IMA AMS Chapter DR. RAVI S. WANKHEDKAR Tel. (02562) 246695 /94222 96495 [email protected]. Secretary, DR. MAYA TULPULE Tel. (020) 25440530 / 9923709210IMA AMS Chapter
IMA MAHARASHTRA STATE OFFICE BEARERS 2009-10
EDITORIAL ...................................................................... 5
PRESIDENT’S MESSAGE .................................................. 7
HON STATE SECRETARY’S MESSAGE ............................... 9
TIME TABLE FOR ELECTION .......................................... 10
MCI NOTIFICATION ...................................................... 11
BRSM MEMORANDUM ................................................ 13
WHEN IS INTERVENTION NOT REQUIRED? .................. 17
COMPLICATIONS OF INTERVENTIONS ......................... 17
SSS NEWS ..................................................................... 18
A VISIONARY WITH A MISSION .................................... 19
GALLERY ....................................................................... 31
LIFESTYLE MODIFICATIONS .......................................... 33
TITBITS ......................................................................... 35
BRANCH REPORTS. ....................................................... 37
REPORT OF THE ADVISORY COMMITTEE, BRMS ......... 39
DISCLAIMER : Opinions expressed in the various articles are those of the authors and do not reflect the views of IndianMedical Association. The appearance of advertisement in this news letter is not a guarantee or endorsement of theproduct or the claims made for product by the manufacturer.
EDITORIAL BOARDChairman : Dr. DEEPAK K. JUMANIEx.- Editor : Dr. ANIL SUCHAKEx.- Editor : Dr. P.N. RAOEx.- Editor : Dr. AJOY K. SAHA
MembersDr. RAJESH SUBHEDAR Dr. JAYESH LELEDr. BALKRISHNA INAMDAR Dr. Y. S. DESHPANDEDr. SUBRAMANIUM JAYARAM Dr. GOPINATHAN INDUMATIDr. NIRANJAN VAIDYA Dr. AVINASH BHONDWEDr. VYANKATESH METAN Dr. RAJENDRA GANDHIDr. SANJAY DESHPANDE Dr. KRISHNESHKARDr. RAVI PATEL Dr. GURUDATT BHATDr. AJAY TILWE Dr. GOVIND DHAWALE
Published by : IMA MAHARASHTRA STATEContact for write-ups, articles, interviews andadvertisements : Editor : Dr. Deepak Jumani
E-mail : [email protected]
IMA Bldg, 2nd Floor, J.R.Mhatre Marg, J.V.P.D. Scheme,Juhu, Mumbai - 400 049. Office : 2623 2965 / 6521 5756
E-mail : [email protected] : www.imamaharashtrastate.org
Advertisement Cheques must be drawnin favour of IMA MAHARASHTRA STATE
5
1 Action Committee & Dr. Pt. RelationshipChairman Dr. DEVENDRA K. SHIROLEConvener Dr. VIJAY GHATE
MembersDr. KISHORE GANGURDE Dr. SALIM SACCHANIDr. ARSHAD G. MOHAMAD Dr. PRATAP JADHAV
2 Press PublicityChairman Dr. BAKUL S. MEHTAConvener Dr. HOZIE DARA KAPAIDAMembers Dr. ANIL LADDHAD
3 Professional Protection SchemeChairman Dr. ANAND KATEConvener Dr. KRISHNA PARATE
4 Medico Legal CommitteeChairman Dr. MILIND M. NAIKConvener Dr. NISAR SHAIKH GULABMembers Dr. DILIP PATILDr. RAJENDRA ABHYANKAR Dr. SUBHASH TIWARI
5 Mahima Editorial BoardChairman Dr. DEEPAK K. JUMANIEx.- Editor Dr. ANIL SUCHAKEx.- Editor Dr. P.N. RAOEx.- Editor Dr. AJOY K. SAHA
MemberDr. RAJESH SUBHEDAR Dr. JAYESH LELEDr. BALKRISHNA INAMDAR Dr. Y. S. DESHPANDEDr. SUBRAMANIUM JAYARAM Dr. GOPINATHAN INDUMATIDr. NIRANJAN VAIDYA Dr. AVINASH BHONDWEDr. VYANKATESH METAN Dr. RAJENDRA GANDHIDr. SANJAY DESHPANDE Dr. KRISHNESHKARDr. RAVI PATEL Dr. GURUDATT BHATDr. AJAY TILWE Dr. GOVIND DHAWALE
6 Resource & Finance CommitteeChairman Dr. ANIL PANCHNEKARConvener Dr. ANIL SUCHAKMembers Dr. SANJAY S. JOSHI
Dr. AKIL CONTRACTOR7 Membership Promotion committee
Chairman Dr. SUHAS PINGLEConvener Dr. JAYANT MAKARANDE
MemberDr. DEEPAK KHALANI Dr. ANIL D. KABRADr. SHRIDHAR G. SHANBAUG Dr. KIRAN V. NABARDr. BALIGA PRADEEP Dr. CHANDAK UMAKANTDR. GANGADHAR V. MAHESHWARIDr. YUVRAJ GEHLOT (Not Member) Dr. PATEL RAMESH
8 Rural Health CommitteeChairman Dr RAVI WANKHEDKARConvener Dr SAVITA S. NAIK
MembersDr. NARAYAN K. PURANIK Dr. BHARAT VALVIDr. SEHEJWAL Dr. YASH LOKHANDWALADr. NAPHADE NINAD EKNATH Dr. RAJKUMAR SACHDEV
9 Medical Education Committee & Medical Ethics CommitteeChairman Dr. TATYARAO. P. LAHANEConvener Dr. KISHOR TAORIMembers Dr. GIRISH THAKREDr. YASH LOKHANDWALAL Dr. SUDHAKAR TAMBE
10 Occupational Health / Service Doctors CommitteeESIS/ LIC Sub Committee
Chairman Dr. YOGESH SHAHConvener Dr. MANGALA GOMARE
Dr. SANTOSH KADAMMembers Dr. RAJESH VASAVEDr. SAJAY SHINDE Dr. SUBHASH SHAH
11 Group Health & Insurance SchemeChairman Dr. DILIP DEODHARConvener Dr. DEVENDRA K. SHIROLE
12 Women Doctors WingChairman Dr. MAYA TULPULEConvener Dr. VIJAYA MALIMembers Dr. SUNITA KSHIRSAGARDr. VIDYUT SHAH Dr. SHRADDHA WALVEKAR
13 Constitution committeeChairman Dr. SHAILENDRA C. MEHTALIAConvener Dr. JAYESH LELEMembers Dr. NIRANJAN R. VAIDYADr. BHALCHANDRA WAGH Dr. DILIP SARDADr. PARTHIV SANGHVI Dr. PRASHANT NIKHADE
14 New Premises / Building CommitteeChairman Dr. ANIL PANCHNEKARConvener Dr. AJAY KATEMembers Dr. KAILASH GINDODIA
16 DASS CommitteeChairman Dr. Y. S. DESHPANDEConvener Dr. BAL INAMDARMember Dr. VANDANA GANDHI Dr. VILAS BHOLE
18 Award CommitteeChairman Dr BAKULESH MEHTAConvener Dr ARUN PAWADEMembers Dr R. D. JAGTAP
19 Projects committeeChairman Dr. PRAKASH DEOMember Dr. AKIL CONTRACTORDr. SUHAS PINGLE Dr. RAVI WANKHEDKAR
20 Co-ord. State H.Q. CommitteeChairman Dr. NIRANJAN VAIDYAConvener Dr. ANAND KATE
21 Anti Quackery cellChairman Dr. GHANSHAYAM UMREConvener Dr. BALDWA MAHESH
MembersDr. SANJAY DEORE Dr. SHRADDHA WALVEKARDr. SANDIP PHADKE Dr. PANKAJ GUPTADr. NITIN TURASKAR Dr. RAM SHIVEKDr. PRASAD MAGAR Dr. POLKAT
22 Information & CommunicationChairman Dr. JAYESH LELEConvener Dr. SATHAYE CHANDRASHEKHAR B,.Members Dr. JAYA DIGHE
23 Geriatric Cell CommitteeChairman Dr. DILIP DEODHARConvener Dr. PRAKASH J. KHALAPMembers Dr. RAMESH SHAH
25 Sports CommitteeChairman Dr. MANGESH GULWADEConvener Dr. SURESH GOKHALEMembers Dr. SACHIN PAWDE
Dr. CHARUHAS S. JAGTAP Dr. KISHOR GANDECHADr. ASHUTOSH KELKAR Dr. AMIT DEWAIKARDr. SANJAY DEOTALE Dr. UDAY PHUTEDr. RAJESH PATIL Dr. DILIP SHIRSHIKAR
26 BMW & Nursing HomeChairman Dr. SANJEEV SHARANGPANIConvener Dr. BAL INAMDAR
MembersDr. SANJAY DAMKE Dr. RAJENDRA JADHAVDr. VIPIN CHECKER Dr. AJAY TILWE
27 Advisory CommitteeDr. VIJAY PUNJABI Dr. VASANT PAWARDr. R. G. JIMULIA Dr. RAM ARANKARDr. ASHOK ADHAO
28 Legal Advisory CommitteeChariman Dr. JAYANT NAVRANGEConvenor Dr. SUBHASH TIWARIMember Dr. ANIL LADDHAD
Dr. BHUJANG PANDURANG Dr. NIKHIL DATAR
SUB COMMITTEE

6
ranaam to all my respected teachers,guiding guides and all the members ofIndian Medical Association all acrossmy state of Maharashtra.
Our bodies are our gardens to whichour wills are gardeners. The root of allhealth is in the brain, The trunk of it is inemotion, The branches and leaves are thebody, The flower of health blooms whenall parts work together. Natural forceswithin us are the true healers of disease.Let your food be our medicine and notmedicine our food. There are someremedies worse than the disease. An ounceof prevention is worth a pound of cure.Hence in this inaugural issue of Mahima weare fortunate to have Dr Pratiksha, adynamic first preventive womencardiologist of our country, as our GuestEditor. Her crusade to support actively anon-invasive cardiac treatment as EECP{Enhanced External Counter pulsation},which is safe, long lasting, affordable, non-medicated, out-patient & US FDA approvedevidence based treatment for coronaryartery disease, is commendable beyondtime & space.
If you want to live, you must walk, ifyou want to live long , you must run. This isbeautifully taught by the Rehabilitationteam of Institute of Preventive CardiologyHeart Care Centre as a package in theirtreatment for coronary artery disease.Over the years, medical science hasidentified all the primary systems of thehuman body, the circulatory, nervous,respiratory, gastrointestinal, urinary,endocrine immune system etc. but two
EDITORIAL
other systems which arecentral to the properfunctioning of a humanbeing need to beemphasized. These are The healing systemand the belief system. The two worktogether. To get the body in tone get themind in tune and at IPC Heart Care Centrethere is a awesome Yoga programcustomised to heal the mind, body andsouls of the critically ill cardiac patients.
I am convinced beyond an iota ofdoubt that we have a splendid pharmacyinside us that is absolutely exquisite. Itmakes the right medicine , for the precisetime, for the right target organ- with no sideeffects. Poor health is not caused bysomething you don’t have, its caused bydisturbing something that you alreadyhave. Healthy is not something that youneed to get it, its something you havealready if you don’t disturb it. SoPrevention and Wellness should beimplored upon by every physician and IPCHeart Care Centre excels in positivelypromoting the same. The world is in aconstant conspiracy against the brave. It’sthe age old struggle. There is a roar ofcrowd on one side and the voice of yourconscience on the other said Dr Pratikshawho rose to every occasion to listening toher conscience to build IPC Heart CareCentre to such a magnitude whichmatchlessly makes her a daring Ladyentrepreneur. So truly today life is either adaring adventure or nothing. After all oneisn’t necessarily born with courage genes,but one is born with potential and Courage
P
faces fear and thereby masters it. It’s thisunique moral quality of Dr Pratiksha whichmakes her irresistible to fly as high as tokiss the sky.
I have read and understood Dr DeanOrnish, who hails in Western World andhas successfully proved reversal of theheart diseases with all his non invasivetechniques and life style modifying science.In India we have our Dr Pratiksha who trainsand treats all her patients with similar infact better scientific instruments and hasbeen splendidly successful in curing over5000 patients in her passionate journey toheal without a needle or scalpel. One whohas health has hope and one who has hopehas everything . Every ailing heart’s hopeis Dr Pratiksha.
The reason why birds can fly and wecan’t is simply that they have perfect faith,for to have faith is to have wings. The airunder our wings are the teachings of ourteachers. One such teacher who is our bestteacher who still continues to teach withundying zeal and passion is Dr O P Kapoor.This year Dr O P Kapoor’s lectures shallbegin at Birla Matushri Auditorium fromJune onwards every Sunday morning. I feelthat there are two types of teachers on thisplanet, One is Dr O P Kapoor and secondare all the others. This should settle thedebate if any, on who is the greatestteacher of all time. Some are born with asilver spoon but my best teacher Dr O PKapoor is born with teaching in his soul.
It is easier to produce ten volumesof philosophical writings than to put oneprinciple into practice believes Dr BakuleshMehta, our dearest, dynamic president,who has vowed to turn every stone upturnto lift up, built and strengthen not only thepillars of IMA MS and make State office aself reliant and evergreen for ever. The one
thing which I assure our IMAites is thatunder the tenure of Dr Bakuleshbhai asPilot of our State Office all the branches ofour state shall flourish boundlessly.
In matters of style, swim with thecurrent, but in matters of principle standlike a rock explained our versatile anddynamic Hon State Secretary Dr HozieKapadia whose innate qualities of integrity,commitment and consistency makes all ofus feel really proud of him.
In this issue we have tried toemphasize the importance of non invasivetreatments for coronary artery disease,available for our patients and leadinginterventional cardiologists tell us woes ofinterventions. This leaves us with a coldchoice between two alternatives. Ourcreator has given us five senses to help ussurvive the threats from the external world,and a sixth sense to survive the internalthreats. Its how you spend your choice isall that matters.
Words fai l me to express mywholehearted thanks to Dr Jayesh Lele , DrAkil Contractor, Dr Suhas Pingle, Dr S K Joshi,Dr Ajoy Saha, Dr Prabhakaran Rao, Dr AnilSuchak, , Dr Niranjan Vaidya & our dearestPresident, Dr Bakulesh Mehta, for theirunconditional support and dependablecommitment to every little thing in makingof this issue of MAHIMA, as they all believethat no one is useless in this world wholightens the burden of anyone else. Afterall those who wish to sing always find asong.
With loads of love and light,
Dr. Deepak K. Jumani

8
With profound gratitude & great humbleness, Iwholeheartedly thank you for your recognition, love,respect & affections, in making me the president ofour esteemed Indian Medical AssociationMaharashtra State branch. Thank you all foreverything. Thank you for this wonderful moment. Iam expressing my views, my dreams & my ambitionsfor IMA Maharashtra State to all the members.
Before this 2010, my life was like any ordinaryperson, but now it has turned into an extraordinary experience. I admit, the air beneath mywings is you all friends, the intent of every actionof mine as usual have always been for the benefitof every member & uplifting the image, strength& spirit of our organization.
“Half the world is composed of people whohave something to say but can’t & the other halfwho have nothing to say but keep on saying it.”
During my campaign, I visited over 90branches in Maharashtra & I was welcomed everywhere with open arms, I learnt a lot, I felt a lotneeds to be done & lot can be done.
I have certain innate moral responsibilities& I am sure I shall fulfill these during my tenure. Ihave a solid battalion of strong, right thinkingheads, which shall always unconditionally be mymagic wand to bring about the good & bestneeded to be done. My friend Dr. Hozie Kapadia,Dr. Jayesh Lele, Dr. Shivkumar Utture, Dr. AnilPachnekar, Dr. Prabhakar Rao, Dr. Niranjan Vaidya,Dr. Ajoy Saha…. All of them are known for theirtimeless commitment are my real energies.
To name some of them which are our dire needs are:-1. Increase our Life member Membership strength.2. To initiate concrete steps in improving Doctor
- Doctor & Doctor – Patient relationships, asin this changing times, we have seen that mostof the untoward incidents of ransacking ofnursing homes, hospitals, bashing up ofdoctors etc, could have been avoided. Wemust also understand our own socialresponsibility, as we today see the mediablows up to glory what ever little wrongunintentionally any of our brethren does.
3. How to achieve this, Iwant suggestions fromyou. Our mouth piece ofthe IMA, MAHIMA shallbe published at leastthrice in a year and sentto as many members as possible. This will helpus to keep all the members involved & shall beable to pass on the information of activities ofIMA regularly.
4. To make website popular among all branches& members, the new & fast technique toconvey information / communication. I requestall the branches to develop E-Mail facility & tohave as many members connected by thisemails regularly.
5. Forum for senior citizens, to deal with theirproblems & to start activity and take careabout their health and social well being.
These challenges can’t be met by any oneleader or any one branch. Hence ouradministration has to work to establish a new eraof engagement in which all branches must takeresponsibility for the world we love to see.
I must put on record that whenever I havebeen called as Guest /Guest of honor / Chief Guesthas received excellent response, welcome. Allbranch members are very cordial & receptive,eager to know working of IMA. They want toparticipate & take active role. All the memberswant more news & information. We are planningto have 3 to 4 regional meeting. I will try to visit asmany branches as I can cover. We will continue tosend E-news letter on regular basis. Please formhabit to open e-mail on regularly & provide yourfriends e-mail addresses to Dr. Jayesh Lele who hasinitiated this ‘IMA MS eNews letter’
I also like to compliment all the branchesvisited by me. They have been carrying outexcellent activities & take part in commonlywelfare projects. As an individual we do lot ofsocial work in general & in particular for ourpatient, but unfortunately we do not report &make proper document. We should inform to IMAMS State office, so we can publish & send
President’s Message
9
information to our members, friends. Pleasedevote time to you self & family & to IMA.
President’s DiaryA) Visit 29/11/2009 at Alibag 1st ever IMA
scientific conference which was well attended/planned & excellent hospitality & verypractical / informative scientific topic.
B) Visit Nagpur Branch NIMICONC) Visit Raigad Medical Association Scientific
ConferenceD) Meeting with Health Minister Shri Suresh
ShettyE) Attended New Year eve programme at
Mumbai (Haji Ali) Branch.
All branches which I visited carry out at manygood activities for members & community. Eachbranch has unique way of functioning. We need tobring on record of their activity with documentation.
1. Pune – Special mentality.This branch is in front for doing exemplarilywork. I must put it on record & appreciate itfollowing work by Pune.a. Launch ‘Suryanamaskar Abhiyan’, about
400 city young doctors participated & havetake oath to do everyday 13suryanamaskar & for one year & end ofone year finding rescue will be IMA Pune.
b. Take lead with FOGSI & local NGO ‘RugnaHakka Samiti’ is formed.
c. ‘Patient – doctor’ relation & ‘doctor –doctor’ relationship programme, Patient’srights in Maharashtra in private clinic /hospitals is being formed. The detailedcharter was published in journal on 09/02/2010. This detail will be circulated to all,once we approved in 1st Executive meetingon 7th March, IMA MS will propagate andrecommend to all branches to adopt &circulate to all member. We will alsoforward to HQ.
2. IMA Ahmednagar – Small vibrant branch &enthusiastic branch. The branch members arevery active & wish to become active at State /centre. The branch is launch to get ½ acre land& Bhoomipujan was done on 14/02/2010 &proposed to have new building, where will bemultiutility center. I congratulate the membersof Ahmednagar.
3. IMA Mumbai west Branch along with CGPfaculty and IMA Maharashtra State branch CGPfaculty held ‘GERICON 2010’ on 20 and 21st Feb2010. This was a unique conference dedicatedto Geriatrics. IMA national Hony Financesecretary Dr D R Rai inaugurated the conference.
By the time MAHIMA was in press, IMA Jalgaonbranch arranged ‘Sports Mela’ which I attendedwith some office bearers. It was a great event.
BRMS COURSEShort term Media course for rural area is
proposed by MCI / Government.IMA central council passed a resolution
against this course, the same is being circulated.Meeting was called on 15/02/2010. Every memberpresent suggested few alternative proposals &suggested National President to pass it on togovernment & the support the proposal.
MCI NOTIFICATIONRegarding acceptance of personal gift &
sponsorship: The notification is published in thismagazine, please go through.
In conclusion I request all branches toincrease your branch membership to strengthenour IMA activity.
I am at this platform vouch of my unwaveringcommitment to strive hard as the Commander inChief of IMA State Branch to assure every Doctorof the security, that you wont have to live in fearof violence, I shall try & see that we resolveconflicts peacefully & not to let general publicconfront in ruthless & adverse way which not onlythreatens our image but our lives too.
My friends I believe that,
Work is worship I is motto of mineI can & I will work all the time
To produce for IMA something very fineAnd leave my print on the fading time.
With all my heart I wish all a great & wiser 2010.
Warm regards,
Dr. Bakulesh MehtaPresident IMA MS
10
Thanks very much for electing me to theaugust office of Hon. State Secretary of IMA,MS. I hope and wish that I fulfill all yourexpectations.
We heartily congratulate all the NationalIMA, HQ award winners at MEDICON 2009 atHyderabad. (Detailed list is given elsewherein this issue).
We are actively trying to have our ownpremises and in this I would like all thehonourable members to help us in this nobleproject.
We congratulate IMA Jalgaon branch forcarrying out THE ANNUAL SPORTS EVENT2010 very enthusiastically and successfully
MEMBERSHIP PROMOTION DRIVEPlease hurry up to enroll as many
members as possible at the old existing rates,as from April 1, 2010 IMA, HQ is going toincrease the HFC rates by around 25%.
We genuinely feel that we mustinvigorate our I.M.A. Maharashtra StateBranch by increasing our membership. Hence my personal request to all membersof IMA to increase the strength of LifeMembers as fast as possible, by March 2010.We should focus all our energies for this vitalproject. In a democracy, strength matters.
The Maharashtra Medical Counci lRegister shows about 80,000 doctors on itsrolls, but I.M.A. Maharashtra Statemembership is barely 23,000. Taking intoconsideration that some doctors may haveexpired or migrated abroad or practicing inother States, still we have to enroll about30,000 eligible doctors in Maharashtra State.
“The Assault on Doctors’ Ordinance”was due to our grit, determination and unity. I appeal to each and every member toconsider as his/her solemn and moral duty
towards our associationto enroll at least onemember each this month(more are welcome). Bythis we hope to doubleour strength. I have asincere feeling that you will all rise to theoccasion to fulfill your social obligation, spendsome more of your valuable time and energyin roping in as many members as possible.
Members are also requested to enrollfor the IMA, MS and IMA, HQ Social SecuritySchemes & Professional Indemnity Schemes.
DRH COURSEBRMS is to be now “Diploma in Rural Health”
A meeting of State IMA leaders was heldat New Delhi on 15th February 2010 tofinalize the Rural Health Care model for India.It was decided that the New Rural HealthCourse should be a Health Sciencesqualification and not a Medical Sciencequalification. It will be a Diploma with threeletters only.
1. Diploma in Rural Health – DRH2. Institution will be named as: Rural Medical
School – Rural Health School3. Title shall be Rural Health Provider (RHP)4. Registration not in State Medical Councils
& MCI under Schedule I5. Separate Register as a State Rural Health
Register6. Posting will be in villages of birth – PHC,
CHC, subcenters7. Only in Govt. service for 5 years8. Re-register every year for 5 years9. Selection Criteria, Infrastructure, Faculties
& Curriculum all to be defined by the MCI10.They will be given exposure to work in
Rural areas during the Course / Internship
Hon. State Secretary’s Message
11
11.Their Competencies – Dos & Dont’s willbe clearly stipulated by MCI.
The above were unanimously agreed by themembers present.
MCI NOTIFICATION REGULATION 2009The MCI with the previous sanction of
the Central Government has amended theIndian Medical Council (Professional ConductEtiquette and Ethics) Regulation 2002. Amedical practitioner shall not receive anygifts, shall not accept any travel facility, anyhospitality like hotel accommodation, cash ormonetary grants from any pharmaceuticaland allied health care industries. He has tomaintain professional autonomy in dealingwith pharmaceutical and allied health care
industry and maintain high ethical standards. He cannot endorse any drug or product of theindustry publicly.
We have carried out successfully severalSwine Flu projects and RNTPC projects invarious parts of the State.
Let us all serve the suffering communitywith ethics and compassion particularly, thepoor and downtrodden.
For any IMA work please feel free tocontact me or the office bearers of IMA, MS;
DR. HOZIE D. KAPADIAHon. State Secretary, IMA-MS
INDIAN MEDICAL ASSOCIATION, MAHARASHTRA STATETIME TABLE FOR ELECTION OF PRESIDENT & VICE PRESIDENTS
FOR THE YEAR 2010 - 2011SR. NO. ON / BEFORE DAY DISCRIPTION
1 20.06.2010 SUNDAY 1st Notice Of Election & information to be sent to allLocal Branches about HFC Status & MembershipStrength (Branches may inform if there is anydiscrepency in HFC status, latest by 04.07.2010
2 09.07.2010 FRIDAY Receipt of Nominations up to 5.00pm.3 11.07.2010 SUNDAY Scrutiny of Nomination Papers by Election Commission
(HFC to be paid up fully)4 12.07.2010 MONDAY To inform individual candidates about valid list of
Nominations alongwith withdrawal forms5 31.07.2010 SATURDAY Withdrawal of Nominations up to 5.00 pm.6 02.08.2010 MONDAY Effective Strength of membership & HFC Status of all
Branches to be informed to Contesting Candidates7 04.08.2010 WEDNESDAY To send Election papers / Ballot Papers to all branches8 10.09.2010 FRIDAY Last date of receipt of Ballot Papers up to 5.00 pm.9 19.09.2010 SUNDAY Counting of votes from 10.00 am. Onwards &
Declaration of result.
DR. N. N. MURKEY DR. C. M. GUPTA DR. SUHAS H. PINGLEChairman Member Member
9422918853 9422826117 9322250830
INDIAN MEDICAL ASSOCIATION MAHARASHTRA STATEELELCTION COMMISSION

12
MEDICAL COUNCIL OF INDIANOTIFICATION
New Delhi, the 10th December, 2009
No.MCI-211(1)/2009(Ethics)/55667 - In exercise of the powers conferred by Section33 of the Indian Medical Council Act, 1956 (102 of 1956), the Medical Council of India withthe previous sanction of the Central Government, hereby makes the following Regulationsto amend the “Indian Medical Council (Professional Conduct, Etiquette and Ethics)Regulations, 2002 : -
1. (i) These Regulations may be called the “Indian Medical Council (Professional Conduct,Etiquette and Ethics) (Amendment) Regulations, 2009 - Part-I”.
(ii) They shall come into force from the date of their publication in the Official Gazette.
2. In the “Indian Medical Council (Professional Conduct, Etiquette and Ethics) Regulations,2002”, the following additions/modifications/deletions/ substitutions, shall be, asindicated therein: -
3 The following clause shall be added after clause 6.7:-“6.8 Code of conduct for doctors and professional association of doctors in theirrelationship with pharmaceutical and allied health sector industry.
6.8.1 In dealing with Pharmaceutical and allied health sector industry, a medicalpractitioner shall follow and adhere to the stipulations given below:-
a) Gifts: A medical practitioner shall not receive any gift from any pharmaceutical orallied health care industry and their sales people or representatives.
b) Travel facilities: A medical practitioner shall not accept any travel facility inside thecountry or outside, including rail, air, ship , cruise tickets, paid vacations etc. from anypharmaceutical or allied healthcare industry or their representatives for self and familymembers for vacation or for attending conferences, seminars, workshops, CMEprogramme etc as a delegate.
c) Hospitality: A medical practitioner shall not accept individually any hospitality likehotel accommodation for self and family members under any pretext.
d) Cash or monetary grants: A medical practitioner shall not receive any cash or monetarygrants from any pharmaceutical and allied healthcare industry for individual purposein individual capacity under any pretext. Funding for medical research, study etc. canonly be received through approved institutions by modalities laid down by law / rules/ guidelines adopted by such approved institutions, in a transparent manner. It shallalways be fully disclosed.
e) Medical Research: A medical practitioner may carry out, participate in, work in researchprojects funded by pharmaceutical and allied healthcare industries. A medicalpractitioner is obliged to know that the fulfillment of the following items (i) to (vii)will be an imperative for undertaking any research assignment / project funded byindustry – for being proper and ethical. Thus, in accepting such a position a medicalpractitioner shall:-
13
(i) Ensure that the particular research proposal(s) has the due permission from thecompetent concerned authorities.
(ii) Ensure that such a research project(s) has the clearance of national/ state /institutional ethics committees / bodies.
(iii) Ensure that it fulfils all the legal requirements prescribed for medical research.
(iv) Ensure that the source and amount of funding is publicly disclosed at the beginningitself.
(v) Ensure that proper care and facilities are provided to human volunteers, if theyare necessary for the research project(s).
(vi) Ensure that undue animal experimentations are not done and when these arenecessary they are done in a scientific and a humane way.
(vii) Ensure that while accepting such an assignment a medical practitioner shall havethe freedom to publish the results of the research in the greater interest of thesociety by inserting such a clause in the MoU or any other document / agreementfor any such assignment.
f) Maintaining Professional Autonomy: In dealing with pharmaceutical and alliedhealthcare industry a medical practitioner shall always ensure that there shallnever be any compromise either with his / her own professional autonomy and /or with the autonomy and freedom of the medical institution.
g) Affiliation: A medical practitioner may work for pharmaceutical and alliedhealthcare industries in advisory capacities, as consultants, as researchers, astreating doctors or in any other professional capacity. In doing so, a medicalpractitioner shall always:
(i) Ensure that his professional integrity and freedom are maintained.
(ii) Ensure that patients interest are not compromised in any way.
(iii) Ensure that such affiliations are within the law.
(iv) Ensure that such affiliations / employments are fully transparent and disclosed.
h) Endorsement: A medical practitioner shall not endorse any drug or product ofthe industry publically. Any study conducted on the efficacy or otherwise of suchproducts shall be presented to and / or through appropriate scientific bodies orpublished in appropriate scientific journals in a proper way”.
(Lt. Col. (Retd.)
Dr. A.R.N. Setalvad)Secretary
Medical Council of India
FOOT NOTE : The Principal Regulations namely, “Indian Medical Council (ProfessionalConduct, Etiquette and Ethics) Regulations, 2002” were published in Part – III, Section (4) ofthe Gazette of India on the 6th April, 2002, and amended vide MCI notification dated 22/02/2003 & 26/05/2004.
14
15
16
17
ADVT
18
When is intervention not required?Intervention is required for relief of ischemia, therefore subjective or objective
evidence of ischemia is required to perform intervention. If there are no symptomsand no evidence of ischemia on stress imaging then the patient is unlikely to benefiteven if there is a lesion. Sometimes, on angiography, it is difficult to judge if thelesion needs to be treated. In this case a technique of coronary flow measurementusing a flow wire with maximum vasodilatation with intra coronary adenosine isperformed. There is a clear diagnostic cut off point on the basis of which decisionto intervene or not is made. If patient is symptomatic and has non critical lesions in two vessels, thistechnique helps to decide if only one or both lesions need to be stented.
Intervention should also not be performed if there is no viable muscle. PET scan and MRI testingare the most valuable tools for detecting viability. Even if the lesion is severe but patient has no anginaand no viability is demonstrated, intervention is not indicated. This situation is most commonly seen inpost infarction cases. However neither of these two modalities are 100% sensitive or specific and allclinical parameters need to be taken into account.
A plaque need not be severe to result in rupture and precipitation of an acute MI. Howeveraggressive treatment with antiplatelets and statins to stabilize the plaque is the more appropriate toprevent an MI and intervention can be reserved till evidence of ischemia develops
If patient has severe co morbid conditions which are more likely to result in early death or hassevere cerebrovascular or pulmonary pathology that would significantly increase the risk or morbidityof the coronary intervention, it would be wiser to treat medically.
Eventually the decision to intervene takes into account all factors, the age, clinical findingsassociated disorders and investigatory results. An informed decision is then taken by the patient, hisrelatives and the doctor.
Dr. Jamshed J. DalalDirector-Cardiac SciencesKokilaben Hosp.
Complications of InterventionsIn 1988, coronary intervention was done for first time in India and the
first organized workshop for multivessel diseases treated with coronaryinterventions was done at Jaslok Hospital and Research Centre in 1989.Although it is an attractive opinion to bypass surgery, it has its ownshortcomings and it is not completely free from complications,
Recurrence rate with balloon angioplasty was close to around 30%. Withinvention of stents, it came down to 15% but with drug eluting stents this rate dropped to 8%.
Acute stent thrombosis observed in 1% of the patients is a very serious complication andcan cause either death or Myocardial Infraction in as many as 45% of the cases. Apart from this,edge dissections, groin complications following arterial access, perforations and blood loss arealso known complications, although they are rare.
Recently stent thrombosis occurring even after one year is also described. This is called latestent thrombosis and can be observed even after 3 or 4 years. Its rate is estimated to be 0.6% per year.
New generation stents are likely to overcome this problem and in future it may significantlyreduce stent related complications.
Dr. Ashwin MehtaDirector-CardialogyJaslok Hospital & Medical Research Centre
19
IMA MS SOCIAL SECURITY SCHEME HON. SECRETARY’S REPORTDate : 01/02/2010.
- The Scheme was launched on 1st October 1990.- The Effective membership as on 01st Feb. 2010 - 5250 +
Total No. of death since 1990 – 124 (Barring 1 member, nominees of all are paid the deathbenefit) In the year 2009-2010 No. of deaths 12. & the nominees of each of 12 expired membersis paid Rs. 3,38,190/- within few days of getting information of the death.
This year(1) Member from Mumbai West Branch joined the scheme in May 2008 & expired in October 2008. Even though the
death was within 365 days of joining the scheme because it was accidental death (Crushed while crossing railwaytracks). The nominee was paid Rs. 3,08,930/- within a fortnight. The member had paid Rs. 6200/- while joining.
(2) A member from Parbhani Branch joined the scheme in December 2007 & expired in the car accident inOctober 2008. His nominee was paid Rs. 3,08,930/- inspite of not completing 365 days in the scheme – Ayoung man of age of 34 years. He had paid Rs. 2200/- while joining the scheme.
Young members, do not over look the security of family, thinking we are too young to die.Mishaps & deaths can occur any time unpredictably.
The younger – you join the less you pay – the more you accrue benefit for your members.
Request to members of the scheme :-- Please keep the IMA MS SSS certificate in secured place with all FFC receipts.- Please keep your nominee informed of your membership of the scheme & how to act in case of unfortunate
death to get the death claim amount.- Please note –The notices for FFC – 2010 will be dispatched latest by 15th April 2010 to all members, if one does
not get the notice by 10th May 2010 he has to inquire with the office. Without late fee the FFC must reach tothe office latest on 31st May 2010. No excuse of notice not received will be entertained.
Request to the President / Hon. Secretary of each Local Branch. :-1) Please incorporate the above matters in your news bulletins / correspondence to members.2) On death of any member inform & inquire with IMA MS Office, whether he / she was member of IMA MS SSS,
if yes, please help in expediting the process of sending death claim benefit to the nominee.3) Advise members to send proper amount as mentioned above along with filled in form with Xerox of age proof
& IMA Life Membership certificate in case of new membership.4) IMA MS SSS recognizes the Best Working of Local Branches for propagation of the SSS. Please enroll larger no.
& receive award for your Branch.5) The branch may collect FFC 2010 from their members & send collectively, so as to reach before 31st May
2010, without late fee.6) Please note change of payment schedules.
From 1st April 2009Age Group Admission Fee Advance FFC Annual Subs. 2 yrs. TotalUp to 30 years Complete Rs. 1000/- Rs. 1000/- Rs. 200/- Rs. 2200/-30 yrs. Complete to 40 yrs. Rs. 2000/- Rs. 1000/- Rs. 200/- Rs. 3200/-40 yrs. Complete to 50 yrs. Rs. 3000/- Rs. 1000/- Rs. 200/- Rs. 4200/-50 yrs. Complete to 55 yrs. Rs. 4000/- Rs. 1000/- Rs. 200/- Rs. 5200/-55 yrs. Complete to 60 yrs. Rs. 5000/- Rs 1000/- Rs. 200/- Rs. 6200/-
Please Note : 1. The AGM 2009 has deferred the amendment of changing the advance FFC from Rs. 1000 to2000., hence no change in our charges.2. Dr. Shrikant H. Kotahri was declared elected unanimously as the Hon. Secretary – IMAMS SSS for the period14th November 2009 to – November 2012. As Dr.Arun Bhagwat, (Akola) had sent his resignation ,the officebearers had nominated Umesh J. Rewanwar (Pusad) as the m,anaging committee member. Dr. Dilip V. Gokhale(Nashi), Dr. M. S. Patwardhan (Miraj) & Dr. Rajgopal N. Kalani (Parbhani) were re-elected unanimously for theterm of 14th November 2009 to – November 2012
Dr. Shrikant H. KothariHon. Secretary, IMA MS Social Security Scheme.

20
Dr. Pratiksha, a multi-.faceted youngPreventive Cardiologist of Mumbai, isvariously described as a missionary inpreventive heart care, EECP Therapist and anactivist supporting the movement for non-invasive cardiac treatment. After completingher MBBS from G. S. Medical College. KEMHospital, Mumbai, she pursued with a M.D.degree from Mumbai University.
She is a Gold medalist in Pubic Healthfrom the college of Physicians and Surgeons,also stood first with distinction in Diplomain Hospital Administration.
EECP Enhanced External CounterPulsation Therapy was first introduced inMaharashtra by her and now IPC is havingmaximum EECP machines in India from VasoMeditech, New York, USA where she isformally trained as EECP Therapist. She is theFounder and Chairperson of IPC Heart CareCenter, which has got various branches. Toaddress growing concern of the si lentepidemic, which is afflicting millions, she hasstarted an NGO ‘Institute of PreventiveCardiology Foundation’ which has launcheda National program to prevent and reverseheart disease.
She has also met India’s Hon. Ex.President Shri. A.P. J. Kalam in the year 2006for initiating this campaign at national levelthrough support of government.
Impressed with her pioneering work inPreventive Cardiology Superstar AkshayKumar supported in her mission of IPC ofcreating ‘Good Heart Ambassador’ in everyhome by creating campaign for Star Gold TV.
For her outstanding originalcontribution work in the field of PreventiveCardiology and Non – invasive cardiactreatments, she was felicitated as ‘Best
A VISIONARY WITH A MISSION…… Dr. Pratiksha
Woman Entrepreneur of theyear 2005-06’ by Hon.Finance Minister Mr. P.Chidambaram.
An excellent orator, she has been aninvitee speaker at a number of Seminars andsymposiums of medical practitionersworldwide. She was a Chairperson inPreventive Cardiology session in the WorldCongress on Interventional Cardiology, heldin Mumbai. She has been invited by variouscorporate and social organizations to conductpreventive cardiology programs throughwhich she has educated over fifty thousandindividuals.
She has given her expert honest medicalopinion to over 15000 cardiac cases duringpast ten years all over India through her 8branches. Through her team she hasmanaged over 5000 cardiac cases successfullywithout Bypass Surgery / Angioplasty withsuccess rate over 90%. She is also FounderMember of EECP Registry in India along withDr. Sanjay Mittal, Apollo & Dr. CherrianFrontier Lifeline.
Dr. Pratiksha has written a book inMarathi called ‘Bypassla Paryay’ published byRajhansa Publication. Also received ‘KarmavirBhaurao Patil’ award by State Government forthis book on 18th Jan 2009.
She is popular through her various TVprograms & over three hundred publicationsin the various leading newspapers andmagazines where her message has reachedover millions of people. Her mission is toreach each and every home and create a GoodHeart Ambassador in every home who willensure heart disease is prevented so thatWHO statistics of every fourth Indiansuccumbing to heart disease by the year 2010will be just statistics and not a reality.
21
WHAT IS EECP-EECP or Enhanced External Counter
Pulsation , is a Non-Invasive treatment for patientswho are refractory to or inappropriate for otherinterventions in cases of angina and heart failure.
History and evaluation of EECPWhile EECP is a newer medical innovation,
the technology has existed for more than fiftyyears. In early 1950s, an internal counterpulsationdevice called the intraaortic balloon pump(IABP)was developed .IABP consisted of a catheter witha small balloon tip which is inserted through groinartery(femoral) and threaded into the mainartery(aorta). The IABP supports circulation incritically ill cardiac patients by inflating duringdiastole, the heart’s resting phase, to helpincrease oxygen and blood flow to the heartmuscle through coronary arteries. The balloonrapidly deflates just before the next heart beat,decreasing the heart’s workload. EECP works viaexactly the same mechanism. Only difference isthat IABP works internally, while EECP worksexternal to body.
While the American medical establishmentturned its attention in the 1970s to high techsurgical procedures , EECP was far from forgotten.Tremendous interest in the treatment wasgrowing in China, where physicians werecaptivated by its non –invasiveness and cost –effectiveness. EECP is consistent with Easternphilosophy , which teaches that medicaltreatments should help the body heal itself,enhancing and aiding its natural tendencies ratherthan interfering with them. Cardiologists in USAbegan to show renewed interest in EECP upon thepublication of a scientific paper in 1992 by StonyBrook from New York state university ininoperable patients where EECP treatmentimproved them.
FDA gives its stamp of approvalIn the ensuing years, numerous studies were
published and all reinforced EECP,s safety andeffectiveness. In response, the U.S.FDA approvedEECP in 1995 as a treatment for chronic stableangina and cardiogenic shock, as well as for useduring a heart attack. These are the same FDA-
WHAT IS EECPapproved indications for the IABP. In fact, EECP wasslightly more successful in increasing bloodpressure in collateral vessels and improving thestrength of the heart’s contraction. In June 2002,FDA expanded the list of EECP approved uses toinclude the treatment of congestive heart failure.
Treatment RegimenEECP involves 35 days of treatment. Each
treatment session is for one hour and the patientsare asked to come 6 days a week for 6 weeks. It isimportant that the patient adhere to the one hourtime schedule fixed by the hospital or medicalcentre and the patient is expected to continue thetreatment without break.
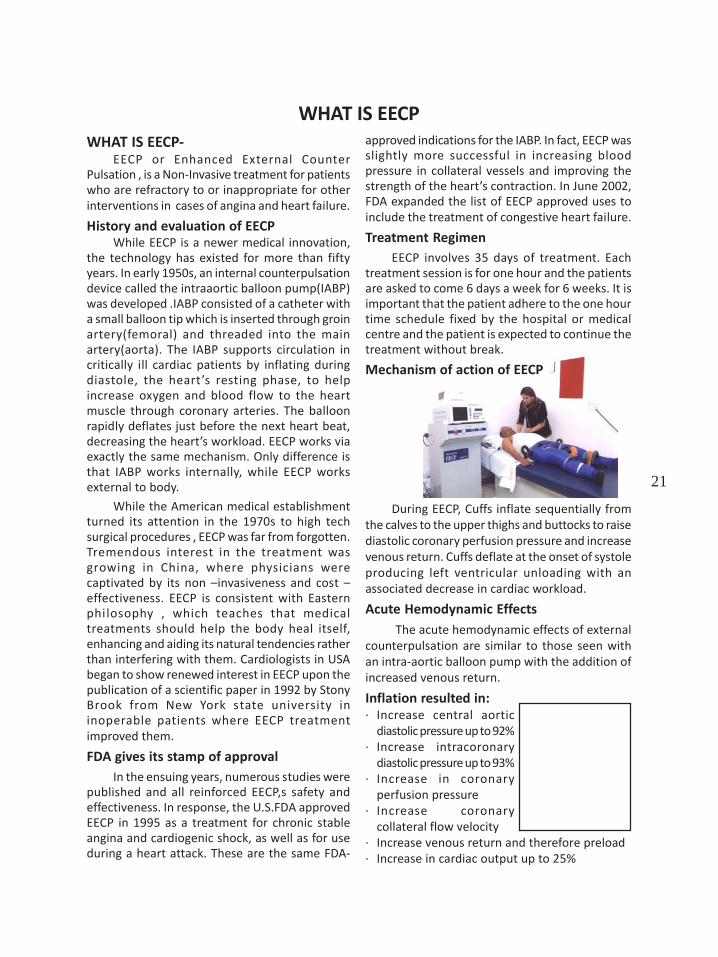
Mechanism of action of EECP
During EECP, Cuffs inflate sequentially fromthe calves to the upper thighs and buttocks to raisediastolic coronary perfusion pressure and increasevenous return. Cuffs deflate at the onset of systoleproducing left ventricular unloading with anassociated decrease in cardiac workload.
Acute Hemodynamic EffectsThe acute hemodynamic effects of external
counterpulsation are similar to those seen withan intra-aortic balloon pump with the addition ofincreased venous return.
Inflation resulted in:· Increase central aortic
diastolic pressure up to 92%· Increase intracoronary
diastolic pressure up to 93%· Increase in coronary
perfusion pressure· Increase coronary
collateral flow velocity· Increase venous return and therefore preload· Increase in cardiac output up to 25%
22
Microvascular AnginaCardiac syndrome X
Acute Coronary SyndromeUnstable AnginaAcute MICardiogenic shock
Contraindications Check ListSignificant ARDVT/active thrombophlibitiesCongenital Heart DiseaseGross CHFUncontrolled arrhythmia AF, VT, FrequentVPC’sExtreme Hypertension (BP>180/110mmHg)Extreme Tachycardia (HR>120 BPM)Cardiac Cath in Prior 1-2 weeksPregnancyBleeding Diathesis
PrecautionsIn some patients with a history of
congestive heart failure (CHF) or low ejectionfraction, left ventricular function may beinsufficient to compensate for increased venousreturn during EECP. These patients should havetheir fluid balance closely monitored. Cuffpressure and deflation timing should beoptimized for achieving maximum after loadreduction and reducing the possibi l ity ofpulmonary congestion.
EECP should be withheld if there isexacerbation of heart failure symptoms and maybe resumed once the patient has beenstabilized. In patient with manageable edemawith LVEF>35% continuous monitoring ofoxygen saturation should be initiated.
Severe peripheral vascular diseaseincluding significant i leofemoral arterialobstruction may limit the effectiveness of EECPtreatment due to decreased blood flow.
Patient suspected of having an abdominalaortic aneurysm should be evaluated for itsclinical significance prior to treatment with EECP.
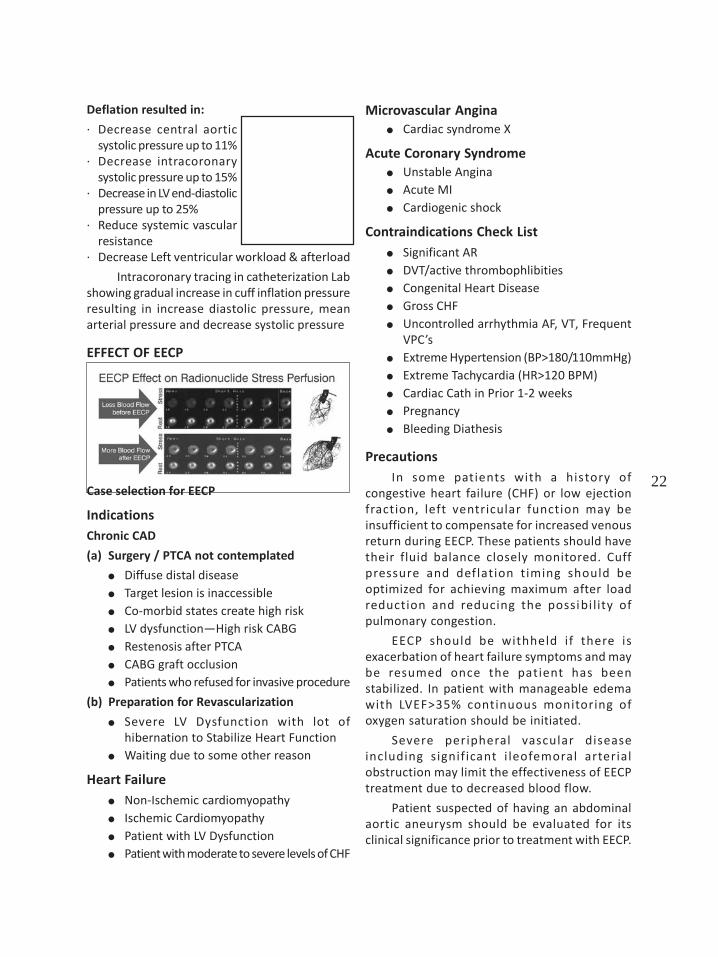
Deflation resulted in:
· Decrease central aorticsystolic pressure up to 11%
· Decrease intracoronarysystolic pressure up to 15%
· Decrease in LV end-diastolicpressure up to 25%
· Reduce systemic vascularresistance
· Decrease Left ventricular workload & afterload
Intracoronary tracing in catheterization Labshowing gradual increase in cuff inflation pressureresulting in increase diastolic pressure, meanarterial pressure and decrease systolic pressure
EFFECT OF EECP
Case selection for EECP
IndicationsChronic CAD
(a) Surgery / PTCA not contemplated
Diffuse distal diseaseTarget lesion is inaccessibleCo-morbid states create high riskLV dysfunction—High risk CABGRestenosis after PTCACABG graft occlusionPatients who refused for invasive procedure
(b) Preparation for Revascularization
Severe LV Dysfunction with lot ofhibernation to Stabilize Heart FunctionWaiting due to some other reason
Heart FailureNon-Ischemic cardiomyopathyIschemic CardiomyopathyPatient with LV DysfunctionPatient with moderate to severe levels of CHF
23
IPC journey with EECP
IPC introduced 1st EECP in Maharashtra, 2004IPC is India’s Largest EECP treatment provider(5 units installed)in technical collaborationwith Vaso Meditech,USA. These units areconnected to a unique software to controland monitor parameters online to providequality treatment.
EECP THERAPY POSITION STATEMENT
EECP external counterpulsation therapy is anon-invasive treatment for patients withmyocardial ischemia and is indicated for use instable and unstable angina pectoris, congestiveheart failure, acute myocardial infarction, andcardiogenic shock. The U.S. Food and drugAdministration (FDA) cleared vasomedical EECPtherapy systems in February 1995 for patientswith stable and unstable angina. In June 2002,FDA cleared EECP therapy for congestive heartfailure (CHF) other indications for use of EECPtherapy include acute myocardial infarct (MI)and cardiogenic shock. EECP therapy is a non-invasive treatment for patients who arerefractory to or inappropriate for otherinterventions.
Dr Pratiksha ,Chairperson IPC , is the foundermember ofIPER Registry.IPER is anOrganizationto supportE E C Pp r o v i d e r sw i t hadvanced Clinical Support
Dr Pratiksha represents India as one of themember IPER Expert Committee.
IPER Expert Committee
Unites States of America
Dr. John Hui Dr. William E. LawsonPh.D M.D.
Director and senior Professor of MedicineVP Vasomedical Inc Director interventionalAsst Professor in Cardiology Director,Department of Surgery Preventive CardiologyState University of Stony Brook
INDIADr Pratiksha MD Dr. Pradeep G. NayarInstitute of Preventive MD DNB (Cardiology)Cardiology, Mumbai Chettinad Health City
Dr. Sanjay Mittal Dr. Suresh KrishamurthyM.D. DM (Cardiology) MD MRCP, FACCIndraprastha Apollo Hosp. Medical Director of
Krishna Cardiac care Center
Dr Ashok Punjabi MD, DMMedical Director of KrishnaCardiac Care Center
· Dr Pratiksha as a Guest Speaker in F irstInternational ECP symposium held inGuangzhou, China on 13th and 14th of May 2006.
• Dr Pratiksha Invited as a Guest speaker on ‘Roleof EECP in treatment of heart patients’ in theNational Conference on Indian EECP Registry heldat Chennai on 21st Presented clinical researchpaper in First International EECP meet held in 2006at China, where more than 400 EECP Therapistfrom all over the World had participated.
• July 2007 and also in the Expert Committeewho will frame the guidelines to the cardiologistcommunity to use the EECP treatmenteffectively to the needy patients.
24
• Invited for lecture at Annual conference of IMAMaharashtra, MASTACON 2009 .Her topic ofdiscussion was Hope for Hopeless-Cardiactreatments in 21 st century.
• Invited for lecture at IMA Pune in January 2010• Invited for lecture at IMA South Mumbai in
January 2010• Presented lecture at Bandra –Khar Medical
Association in July 2009
• Presented lecture at Dahisar MedicalAssociation in August 2010
Long Term benefits of EECP
EECP is Clinical proven, evidence-basedtherapeutic systems documenting the effectivenessand safety of EECP in the treatment of patients withcoronary heart disease. There are various clinicalstudies demonstrating the long term effects withbenefits upto five year follow-up. Few selectedscientific studies are given as follows:
Must – EECP Trial Study
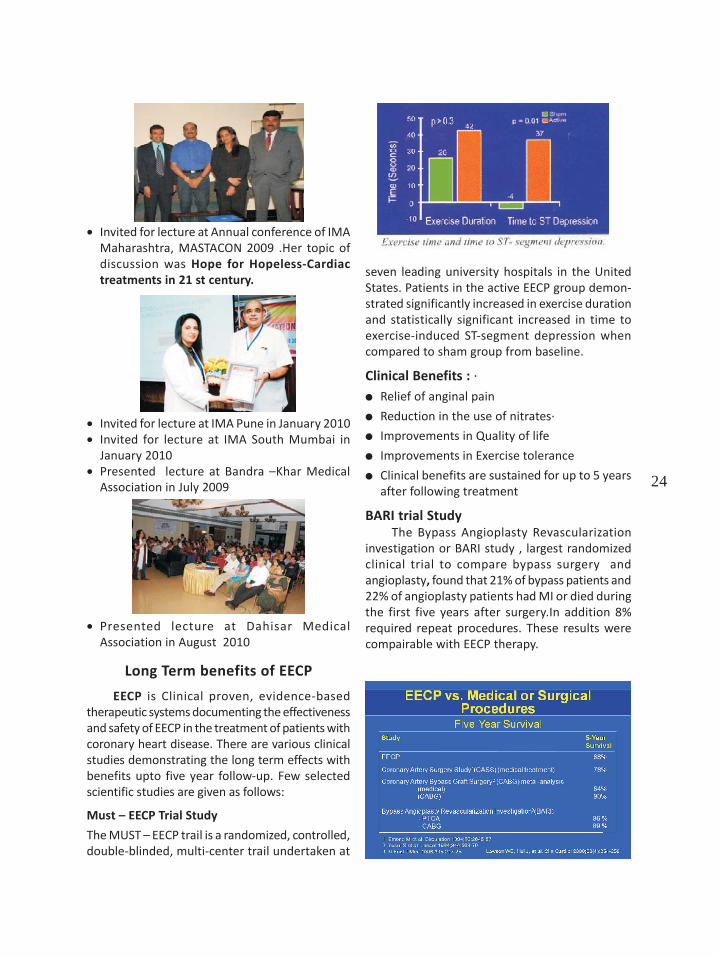
The MUST – EECP trail is a randomized, controlled,double-blinded, multi-center trail undertaken at
seven leading university hospitals in the UnitedStates. Patients in the active EECP group demon-strated significantly increased in exercise durationand statistically significant increased in time toexercise-induced ST-segment depression whencompared to sham group from baseline.
Clinical Benefits : ·Relief of anginal pain
Reduction in the use of nitrates·
Improvements in Quality of life
Improvements in Exercise tolerance
Clinical benefits are sustained for up to 5 yearsafter following treatment
BARI trial StudyThe Bypass Angioplasty Revascularization
investigation or BARI study , largest randomizedclinical trial to compare bypass surgery andangioplasty, found that 21% of bypass patients and22% of angioplasty patients had MI or died duringthe first five years after surgery.In addition 8%required repeat procedures. These results werecompairable with EECP therapy.
25
LATEST SCIENTIFIC STUDIES ON EECP
26
Frequently asked questions (FAQ)Q: What are the advantages of EECP?
Unlike bypass surgery, balloon angioplasty,and stenting procedures, EECP is non-invasive,carries no risk, is comfortable, and is administeredin outpatient sessions.EECP increases blood flow: * To heart by 20-42% * To brain by 22-26% * To kidneys by 19%
EECP also increases heart’s output (stroke volume)by 12% by reducing after load. This improves LVEF.Q: Are there any risks or side effects of EECP?
EECP is safe. Occasionally, some patientsexperience mild skin irritation under the areas ofthe blood pressure cuffs. Experienced EECPtherapists address this irritation by using extrapadding where needed to make the patientcomfortable. Some patients experience a bit morefatigue at the beginning of their course oftreatment, but it usually subsides after the firstfew sessions. In fact, patients typically feelenergized by EECP
Q: When can I expect to start feeling better fromEECP?
Most patients begin to experience beneficialresults from EECP between their 15th and 25thtreatments. These benefits include increasedstamina, improved sleeping patterns, decreasedangina, and less reliance on nitroglycerin and othermedications. There is variation, certainly, andsome patients start to feel better as soon as theirfirst week of treatment!
Q: Do the benefits of EECP last?Yes. In patients followed for three to five years
after treatment, the benefits of EECP, including lessangina, less nitroglycerin usage, and improvedblood flow patterns documented on stress tests,had lastedQ: How does EECP compare to angioplasty orbypass surgery?
The five-year outcomes for EECP patients arevirtually the same as for angioplasty and bypasssurgery patientsQ: Is EECP FDA-approved ?What kind of research has been done on it?
EECP was approved by the USA-FDA in 1995as a treatment for coronary artery disease andangina, cardiogenic shock, and for use during aheart attack. In 2002, the FDA approved EECP as atreatment for congestive heart failure. It hasundergone rigorous clinical trials at leading
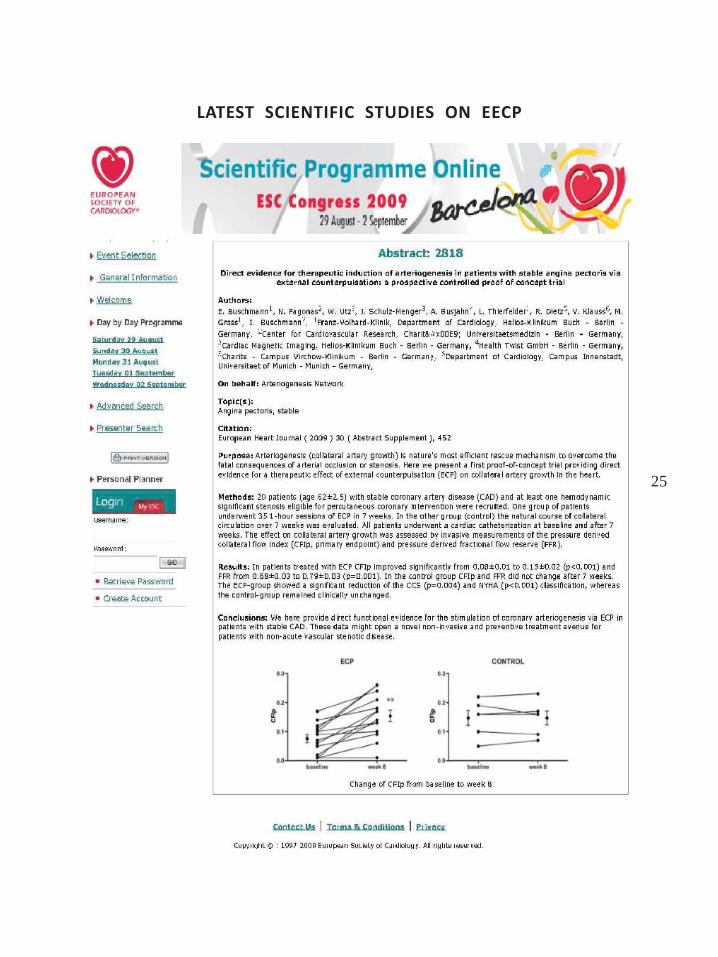
Published in European Journal of Clinical Investigation 2009This study provided direct functional evidence for the stimulation of coronary arteriogenis
via EECP.23 patients of stable coronary artery disease underwent cardiac catheterization at
baseline and after 7 weeks of EECP treatment.Measurements of pressure derived Collateral Flow Index (CFI) and Fractional Flow Result
(FFR) were done.CFI & FFR were significantly improved in patients who completed EECP therapy as
compared to controlled group.

27
universities around the country and EECP hasbeen the subject of more than 100 scientificstudies published in leading medical journalsthroughout the world.Q: I have already had bypass surgery/angioplasty/stents. Can I still have EECP?
Yes! Most of our patients have already hadone (or many) of these procedures. They comefor EECP treatment because they still have angina.Q: Can EECP dislodge plaque and cause a strokeor heart attack?
No. Our bodies obey the laws of physics, andone principle law is that fluid will follow the pathof least resistance. Atherosclerotic plaques arecalcified and hard, and they create an obstructionthat detours the blood through alternate routes.During EECP, when your blood is flowing to yourheart, it will naturally bypass arteries with plaqueand enter healthy, non-diseased blood vessels togo around the blockages. Going around theblockages is a longer trip, but it is a much easierone. In time, these new pathways are reinforcedand become lasting routes for blood to reach yourheart beyond the blockages. Every EECP patienthas had multiple, serious blockages. No one hasever had a heart attack or a stroke as a result ofthe treatment.
Q: Does EECP aggravate high blood pressure(hypertension)?
No. If you have hypertension that is properlymanaged, you may undergo EECP withoutdifficulty. Oftentimes, patients with hypertensionfind that their blood pressure improves as theyproceed with EECP. If your hypertension isuncontrolled, you must seek medical care to getyour blood pressure under control with propermedications before proceeding with EECP.Q: If EECP works so well, why haven’t I heardabout it before?
For a few reasons First of all, as mentionedbefore the USA-FDA only approved the procedureas an accepted medical treatment two years ago.Since then we are working hard to let every heartpatient know that there is an alternative tosurgical interventions in the treatment of heartdisease. Because EECP provides patients anopportunity to stay away from invasive surgery, itis precisely the reason you should not expect tohear too much about this safe and effective
alternative from your regular cardiologist.However, many cardiologists are beginning torealize that their patients know about thisalternative anyway, and are recommending EECPas a non-invasive natural bypass procedure, inpatients that are high risk for surgery or have noother alternatives.
Q: High pressure created during EECP will burstmy arteries?
No, this pressure is optimized and given inscientific way by monitoring your ECG duringdiastolic phase/relaxation phase of your vascularsystem. It will not burst your arteries.
CASE STUDIES1) Case One:
‘Mr.Patil , you have to sign this High RiskConsent with DOT(death on table) if we plan breastcarcinoma surgery for your wife’ These words weresaid to Mr.Patil by his wife,s oncology surgeon. Mr.Patil became speechless and with tears in his eyeshe left the cabin of surgeon .He felt helpless asher wife’s heart pumping capacity of 15% -20%for past 4 years was the reason for doctors askingfor DOT. He didn’t know what to do as if shedoesn’t get operated for carcinoma, the diseaseitself was progressing and if go ahead with surgeryrisk was too much. There was no treatmentavailable to increase the pumping as well. Mr.Patil,cousin who just completed his treatment at IPCsuccessfully for IHD, suggested them to consultat IPC. On her first day of visit to IPC, Mrs Patilwas diagnosed as a case of DilatedCardiomyopathy (catheter angio. Normal) She wasin NYHA class II-III with EF of 15% with moderatePH on 2-D Echo. She had bigeminy / trigeminy onECG . Team of doctors at IPC revised hermedications and in consultation with experts atUSA as well as team of oncologists decision to giveEECP was taken. Mrs. Patil completed her EECPwith intermittent follow ups with oncologists tokeep a close watch on progress of carcinoma. PostEECP her angina class improved to NYHA I , ECGbecame regular and LVEF improved to 25% withmild PH. She was given fitness to get operated.She got operated and discharged with in a weekfrom hospital.

28
This case explains the need of therapy forheart disease especially for cases who are eitherinoperable or where revascularization is not useful.
2) Case Two :Mrs. Swati Kambli
clerical staff at a Banksuffered from Heartattack in 1997 at the ageof 32 yrs. Sheunderwent CoronaryAngiography in thesame year which showed blockage in one majorvessel & Baloon Angioplasty for that. But this wasnot the end of her suffering as her Femoral arteryfrom where the probe was passed duringangioplasty was blocked with a large blood clot& she started getting unbearable pain in the leg.Doctors performed emergency operation toremove that clot & it was for around 7-8 hrs. Shewas bedridden for 3-4 months as a result of that.She suffered a lot financially & Psychologically asshe couldn’t resume the duties during that period.
The patient was maintaining on medicationstill in 2007 she again started getting the Anginalpain. She underwent Angiography which showed90% blockages in two major vessels. Now that shewas advised CABG which was beyond herimagination as she was very young , had nomoney, taking leave from office was difficult & nosupport from Family. Altough she bravely decidedthat she will maintain on medicines only but herincreasing symptoms were troubling her .
AT IPC she got the hope for life . Dt. Pratikshaevaluated her case & advised for EECP. She startedwith EECP in Nov’07 & by the time she completedthe treatment in Jan’08 she was quite normal. Herstress test was Negative, 2 D Echo showedimprovement in pumping capacity from 35% to 40%.
3) Case Three:Mr. Vishwanathan 68 yrs old gentleman was
a chronic case of Diabetes. He underwent surgeryfor liver abscess in 1980 & subsequently AorticValve replacement in 1983.
Lateron He started C/O chest heaviness,fatigue in 1998. Doctors advised for Angiographywhich showed LM-Normal, LAD-40% beforeD1,75%(ostium),LCX-75% ,RCA-90% .Then he
underwent Bypass Surgery in 1998 and at the sametime, Doctors found that his Prosthetic Aortic valvestarted getting damaged which was then replacedby metallic valve.
He was better after 1998 surgery, but againstarted with weakness, fatigue & pain in lt. handon exertion, palpitation in Oct. 2007 . Doctors didAngiography which showed LM-Normal, LAD-90%(prox), 79-80%(mid),80%(distal), LCX-99%(mid),RCA-total occlusion of the graft . henceunderwent Angioplasty immediately.
He was not better after angioplasty. He wasstill C/O weakness , chest pain, Doctors told himthat it is because of Keloids due to Bypass operation.
Then finally in Sept 2008 he did theDobutamine Stress Echo which was positive. Doctors advised him to undergo Preventivetreatment & EECP as he was not fit for any surgerythen.. They started with Skin treatment forKeloids. He started EECP at IPC .
His heart beats were irregular which wasunder control then & EECP worked Effectively.
He completed EECP successfully with thestress test improved & he traveled to USA at hisson’s place that was a greatest achievement forhim. EECP is a hope for the hopeless.
4) Case Four:Mr. Nooruddin Shaikh, 42yrs old gentleman, a tailorby profession came with acomplaint ofbreathlessness after 1-2min walking even after theangioplasty which wasdone only 6 months back.After angioplasty he was hardly better for 1 monthand again he started getting breathlessness afterlittle exertion. After 6 months of his angioplastyhe was advised to undergo 2nd angiography andbypass. He couldn’t even repay the loan which hetook for his angioplasty and the another bigproblem was in front of him in the form of 2nd
angiography and bypass surgery with which he wasreally frustrated.
In May’08 he came to IPC with keeping rayof hope in his mind that he can avoid 2nd CAG &bypass surgery. He immediately advised

29
hospitalization to correct the excessive fluidaccumulated in his body & after 15 days he startedwith EECP, noninvasive treatment to improveheart’s blood supply.
After 35 sessions of EECP over his 2 D echowas repeated and there was marked improvementin his LV systolic function (EF-35%) which was only(25-30%).Even after 1 yr of completing EECP heis able to carry out all his routine activities withoutany discomfort with daily walk of 20-25 min. Hedidn’t even require a single admission in this last1 yr, for cardiac complaint.
5) Case Five:Mr. Vijay Salvi ,a young businessman , a
Typical Type A Personality person . In these typeof people their Hurry, Worry & Curry are the fuelin the fire.
He got heart problem in the year 2000, atthe age of 47 yrs. His Left sided major arteryshowed 99% blockage which had severelyaffected his heart, dropping the Pumping capacityto 35%. He underwent Angioplasty at that timebut as he continued the same lifestyle the resultwas that he required2nd Angioplasty in thesame artery in 2001 i.e.merely in a year time .He developed the blocklower to the previousAngioplasty site.
He didn’t learnanything out of it as theBusiness was the major factor for him & hisproblem was solved by getting Angioplasty done.The concept of prevention & control was not yetin his mind ti ll he started getting Anginalsymptoms again in 2008. He read about Dr.Pratiksha & IPC in Newspaper & the concept ofEECP & Cardiac rehabilitation programme forprevention wad convincing for him.
He started with the treatment at IPC but hewas not ready to understand the importance of Cardiac Rehabilitation programme ( Diet, yoga ,Meditation , Exercise ) as it is too time consuming.It was the hard work & dedication of ourprofessionals that he realized the importance of
it & to our surprise he started religiously followingeverything.
As a result his Pumping capacity of heartimproved significantly to 60% & stress test wasNegative.
In his feedback form he wrote that thecombination of Cardiac Rehabilitation Programmewith the treatments is really needed for the goodresults & maintaining. He felt that he wasted histime all these years , if he would have got thetreatment earlier his Heart condition would havebeen controlled. He specially thanked Dr. Pratikshafor the Yoga meditation.
It shows that getting repeated angioplasty isnot the only solution. It may temporarily benefitbut we need to remove the root cause
6) Case Six:Mr.Annasaheb Vasagdekar ,65 yrs old
gentleman, a criminal lawyer by profession wasadvised to undergo a second bypass surgery 8 yrsof his first bypass and he was really against of it.
He is having history of dyslipidaemia since 20yrs for which he was taking regular medicines andthere was lot of mentalstress because of hisprofession.
In 1996 first time heexperienced chest painwhile traveling to court,as the pain was increasinghe rushed to a nearbyhospital. there his ECG was taken and it was a heartattack(IWMI) for which he was immediatelyhospitalized and treated. after MI he was well fornext 2 yrs. he was taking regular medicines. In1998 he started Ext.angina. he was advised CAGwhich revealed sever TVD and immediately hisbypass surgery was done.Till year 2005 he wascomfortable but since Dec’06again he startedgetting ext.angina. He had episode of unstableangina for which he was hospitalized and hisangiography was done. after his secondangiography he was advised to undergo secondCABG immedietly as his all the 4 grafts were totallyoccluded. Pt. was really against of taking anotherpainful experience of bypass surgery and he came
30
in IPC to consult Dr.Pratiksha .after the evaluationof his cardiac status he was advised to undergoECP .He completed 35 days course of EECPtreatment in Dec’06 and he felt remarkableimprovement in his chest pain & dyspnea on exertion.
After EECP he again started his law practiceand all his routine without any cardiac complaint.Even after 3 yrs of completion of EECP he is livinga healthy life without any cardiac events and noteven single hospitalization required for cardiaccomplaint. In July’09 he underwent a majorsurgery of Lumbar spine tumor without anycardiac complications.
7) Case Seven:Mr. Ashok Savtale,70 yrs old gentleman,
having his own business was advised to undergoa second bypass surgery but because of his lowpumping of heart it was a high risk surgery forwhich pt. was not ready.
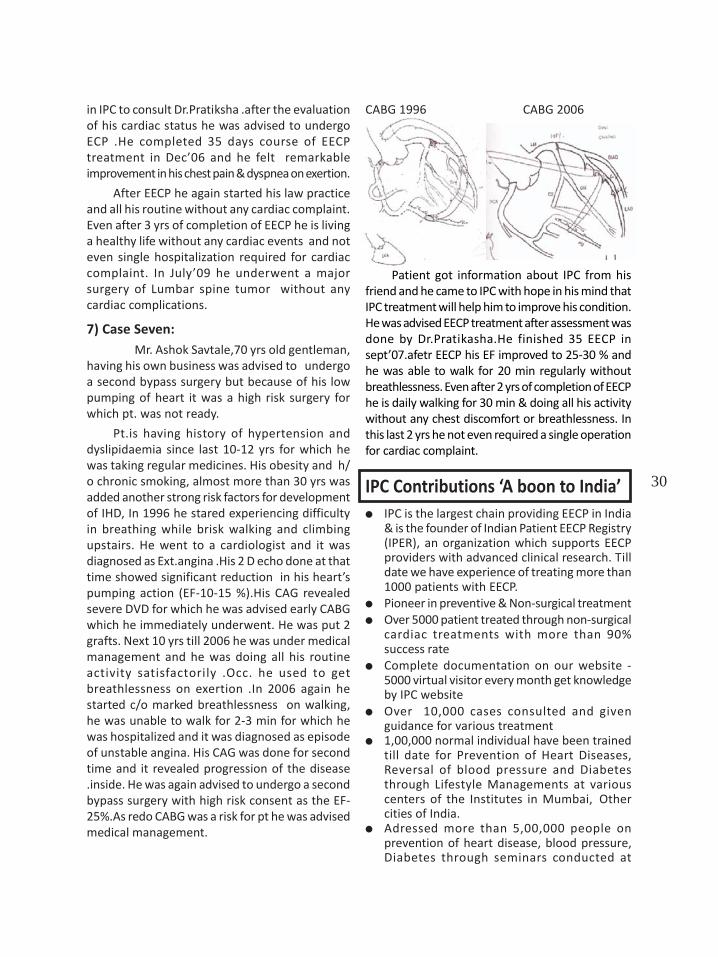
Pt.is having history of hypertension anddyslipidaemia since last 10-12 yrs for which hewas taking regular medicines. His obesity and h/o chronic smoking, almost more than 30 yrs wasadded another strong risk factors for developmentof IHD, In 1996 he stared experiencing difficultyin breathing while brisk walking and climbingupstairs. He went to a cardiologist and it wasdiagnosed as Ext.angina .His 2 D echo done at thattime showed significant reduction in his heart’spumping action (EF-10-15 %).His CAG revealedsevere DVD for which he was advised early CABGwhich he immediately underwent. He was put 2grafts. Next 10 yrs till 2006 he was under medicalmanagement and he was doing all his routineactivity satisfactorily .Occ. he used to getbreathlessness on exertion .In 2006 again hestarted c/o marked breathlessness on walking,he was unable to walk for 2-3 min for which hewas hospitalized and it was diagnosed as episodeof unstable angina. His CAG was done for secondtime and it revealed progression of the disease.inside. He was again advised to undergo a secondbypass surgery with high risk consent as the EF-25%.As redo CABG was a risk for pt he was advisedmedical management.
CABG 1996 CABG 2006
Patient got information about IPC from hisfriend and he came to IPC with hope in his mind thatIPC treatment will help him to improve his condition.He was advised EECP treatment after assessment wasdone by Dr.Pratikasha.He finished 35 EECP insept’07.afetr EECP his EF improved to 25-30 % andhe was able to walk for 20 min regularly withoutbreathlessness. Even after 2 yrs of completion of EECPhe is daily walking for 30 min & doing all his activitywithout any chest discomfort or breathlessness. Inthis last 2 yrs he not even required a single operationfor cardiac complaint.
IPC Contributions ‘A boon to India’IPC is the largest chain providing EECP in India& is the founder of Indian Patient EECP Registry(IPER), an organization which supports EECPproviders with advanced clinical research. Tilldate we have experience of treating more than1000 patients with EECP.Pioneer in preventive & Non-surgical treatmentOver 5000 patient treated through non-surgicalcardiac treatments with more than 90%success rateComplete documentation on our website -5000 virtual visitor every month get knowledgeby IPC websiteOver 10,000 cases consulted and givenguidance for various treatment1,00,000 normal individual have been trainedtill date for Prevention of Heart Diseases,Reversal of blood pressure and Diabetesthrough Lifestyle Managements at variouscenters of the Institutes in Mumbai, Othercities of India.Adressed more than 5,00,000 people onprevention of heart disease, blood pressure,Diabetes through seminars conducted at
31
various Corporates, Non Profit Organisations,NGOs & some prestigious Associations &Societies of India.Conducted Seminars and Workshops since 10yr and more then 50,000 people were coveredthrough seminar and public talk to spread themessage of preventionMessage reached to people through electronicmedia, Newspaper, TV channel and RadioGives Honest opinion to each and every caseand select cases which will be benefited byEECP treatmentIndia’s largest EECP provider and only centerin world with complete holistic approachunder one roofDedicated team of doctors in each and everybranch providing utmost patient satisfaction.
Other programmes at IPCIPC is the most cost effective centre in the
country that provides non-surgical Holistic &Integrated treatments for Heart diseases and forthose people who want to prevent themselvesfrom this silent killer. IPC has over 90% successratio in reducing blockages, improving blood flowto the heart thus vastly reducing the possibilitiesof heart attack and premature deaths.
At IPC we try to reach the root cause ofdisease we focus on lifestyle modifications throughour various programmes with the help of our teammembers. IPC’s Preventive programs, diabetes,blood pressure, and cholesterol programs are forall where modern medical management iscombined with alternative medicines and therapiesof Yoga, diet management, meditation and stressmanagement to reduce the risk factor causing“Heart Disease and Heart Attack” and to improvethe blood flow to heart and bring about reversalof Coronary Heart Disease.
CARDIAC REHABILITATION PROGRAMMERehabilitation programm is a customized
program of exercise and education. The goals ofcardiac rehabilitation are to help you regainstrength, to prevent your condition from worseningand to reduce your risk of future heart problems.And this will lead to a better quality of life.Cardiac Rehabilitation team comprises of
MD physician CardiologistCardiac rehabilitation therapistStress Counselor NutritionistYoga Instructor
Rehabilitation has two main components:
Medical evaluation: A thorough evaluation byMD doctor including TMT, 2D Echo helps us toassess your physical abilities, medicallimitations and other conditions you may have.Your team explores what risk factors you mayhave for cardiovascular diseases. All of thesefindings help your team tailor a cardiacrehabilitation program to your individualcondition, making sure it’s safe and effective.Physical activity: On the basis of medicalassessment, an exercise protocol is designedby the rehabilitation therapist. You will be riskstratified first and then (THR) target heart rateis set which is at optimum intensity as well assafe. Your cardiovascular fitness is improvedthrough walking, cycling and other enduranceactivities. You may also do strength training toincrease your muscular fitness. Don’t worry ifyou’ve never exercised before. Your cardiacrehabilitation team will make sure the programmoves at a pace you’re comfortable with.
Who is eligible to join Cardiac Rehabilitation?
Heart Attack AngioplastyBypass Surgery Heart FailureAngiography showing blockagesHeart Valve ReplacementStable Angina Pacemaker
YOGAYoga Therapy is a part of this Treatment. Yoga
therapy has play very important role in thistreatment. Nowadays, everybody has done yogain his/her life sometime or the other. There areclasses, camps, crash courses and TV showsteaching you ‘Yoga’. At IPC we have over 5000cases who have practiced the yogasanas in thisbook and have shown successful results in theirphysical and mental health. But now, as you re inIPC for reason, it is most important to make freshlook at your yoga practice in spite of your pastknowledge. Please remember that every Asanamay not be suitable for your heart condition. ATtimes, it my even do more harm than good. Hence,it is strongly recommended that you do only thoseAsanas which are taught to you by IPC Yoga Teamand do them in the same prescribed way.

32
Since ages, yoga is being practiced by millionsof people worldwide. The efficacy of the samehas been researched and documented by Medicalscience in India as well as western countries. Yogais science and way of life completely based onwonderful scientific truths.
Hence one should understand that ‘Yoga’ isnot limited to particular sect, cult of religion. It isalso not merely an exercise. It is unidirectionalway of life lading to state of pure health. It is alsonot for only heart patients or ailing people. Eventhe healthy people must practice it.
AS there is not only one Asana , Pranayamor Relaxation to control the disease so one shoulddo the yoga practices for the Heart Disease asadvised by IPC Yoga Team
HEARTY DIETCreating awareness among patients, their
family member, friends & relatives regarding rightchoice of food is aim of Diet Department & iscarried out by Dieticians in IPC. Dieticianemphasizes role of food in providing adequatenutrition for healthy heart.
Faulty food habits can cause hypertension,Atherosclerosis, Dyslipidemia, Obesity, Heart
attack, Early Ageing & several other metabolicdisorders. Keeping in mind key principles ofDietetics & Nutrition, Dietician assist in preventive& curative role.Special
Healthy Diets are givenTo maintain Ideal body WeightControlling HypertensionPreventing & reducing Heart Blockages.Increasing Good CholesterolIncreasing Blood CirculationPreventing damage caused due to Obesity,Diabetes Arthrities.Slowing down Ageing process (Free RadicalDamages )
In IPC Dietician gives one to one basis DietConsultation, group meeting, Discussion, Cookingworkshop in order to facilitate healthy lifestyle
IPC HONEST MEDICAL OPINIONBeing a pioneer in non-surgical cardiactreatments our constant Endeavour is to guideour patients honestly whether the treatmentsoffered by us how much will be the benefitand if required urgently we propose surgicalrevascularization as first line of treatment.

33
Dr. Rajendra R Chawhan, Past President IMABoisar branch in last five years, have collectedmore than 1000 bags of blood every yearthrough camps and donated it to State BloodTransfusion Council (Government hospital).Dr Rajendra Chawhan has been awardedtwice by Dy. Chief. Minister for this social workin 2007 & 2008. This year he has a recordcollection of 2028 bottles of blood and henceis our
Great Samaritan of Maharashtra.
Dr. Bakulesh Mehta At the 3rd Sports Melaorganised by IMA MS (Medisport 2010) atJalgaon.
Inauguration of Mastacon 2009Dr.Bakulesh Mehta, Dr. Arun Pawade,Dr. Anil Award, Dr. Jayesh Lele
Dr.Bakulesh Mehta addressing during hisacceptance as President Elect IMA MS.
Chief Guest & Finance Secretary of IMA HQSDr. D. Rai inaugurating Gericon 2010

34
Coronary heart disease (CHD) is one of themost prominent health problems at a global level.By 2020, it is expected that CHD will be the largestcause of disease burden worldwide.1 In thedeveloping world, demographic and lifestylechanges are resulting in an “epidemiologicaltransition” from infectious diseases to non-communicable diseases such as CHD. 1
Risk factors for CHD can be divided intobiological parameters such as lipoprotein levels,blood pressure, body fatness, cardiopulmonaryfitness, etc and lifestyle parameters such asexercise, daily physical activity, diet, obesity,smoking and tobacco consumption.2 There is nowa large body of evidence showing that the risk ofCHD events can be significantly reduced throughmodification of these risk factors.2 Recentguidelines have also clearly defined theimportance of changing the lifestyle andtreatment with prophylactic drugs. 2,3
In the West, the identification of risk factorsfor CHD has led to preventive efforts with somemeasure of success.1 In contrast, exposure to thesame risk factors appears to be increasing in Asiancountries like India via a “globalization” of dietaryhabits, and urbanization. 1,2 Unfortunately,systematically documented data on both CHDprevalence and incidence in countries like Indiaare scarce. Despite this paucity of data, there issufficient information to suggest an impendingepidemic and preventive measures to controlvarious lifestyle risk factors for CHD need to beactively pursued by physicians in developingcountries like India.1
Lifestyle Risk FactorsThe primary lifestyle risk factors for CHD
which can be actively modified or monitored bythe physician include:
· Exercise and daily physical activity· Smoking · Diet · Obesity
Lifestyle Modifications –How do they impact coronary heart disease?
Shantanu DeshpandeGopi Krishna Panicker
Yash Lokhandwala
Exercise and daily physical activityThe relationship between physical activity
and chronic disease morbidity and mortality hasbeen the focus of much scientific research. Resultsfrom these studies have generally been mixed. 4
One potential explanation for the inconclusivefindings is that activity levels were often estimatedfrom participants’ job descriptions with noindividual measures obtained.2,4 This couldincrease the risk of misclassification since differentpersons with the same job title may have a largevariability in physical activity. Other potentialexplanations include the types of activitiesperformed on the job (i.e., isometric vs. isotonic),limited variability in activity at work, and the factthat physical activity outside of work was notconsidered. 2,4 Studies of leisure time physicalactivity have been more consistent in finding aprotective effect of increased activity on a numberof disease endpoints including both fatal and non-fatal coronary heart disease (CHD)
Few studies have investigated the jointeffects of occupational and leisure time physicalactivity. Individuals with sedentary jobs likelyperform the bulk their activity during leisure time,whereas, those in physically demandingoccupations may be more active during work thanleisure. For women, particularly those who do notwork outside the home, typical leisure timeactivity questions may not appropriatelycharacterize overall activity levels. Studies that donot consider work and leisure time activity mayfail to appropriately characterize activity levels. Inthis context, the Buffalo Health study reported astrong significant interaction between physicalactivity and Body Mass Index (BMI) in regards tomortality. This study showed that beyond a certainBMI threshold, the benefits of activity on mortalitycannot override the harmful effects of excessweight.
35
This lack of a positive association in heavymen was attributed to the strong anaerobiccomponent (i.e., lifting 25 pounds or more,shoveling, etc.) in their daily activities. 2,4 Thisshowed that anaerobic activities did not influencemortality risks in the same manner aspredominantly aerobic activities usually performedduring leisure time in the form of exercise. This wasalso attributed to the observation that obese mentend to report significantly higher activity levelsleading to a measurement error. A potentialexception could be that obese men were less likelythan lighter men to adopt a physically activelifestyle after retirement.
These findings from this study suggestedthat an incremental increase of 1 kcal/kg/hr wouldrepresent a doubling of energy expenditure andcould be achieved in various ways. 2,4 An individualwho sleeps seven hours on average and iscompletely sedentary during the remainder of theday could achieve such an increase by spending:
· all waking hours in light activity and eighthours at a level slightly above rest or
· two hours in very vigorous activity andremaining quite sedentary throughout therest of the day
Smoking : Cigarette smoking is a major cause ofcardiovascular diseases and is responsible forapproximately 140,000 premature deaths fromcardiovascular diseases each year.5 Smokers have a 2.5-fold increase in the incidence of coronary heart diseasecompared with non-smokers.6 Accordingly, the relativerisk of myocardial infarction is 2–3 times higher in menwho smoke, and 1.5–3 times more common in womenwho smoke than those who do not. 6 Cigarette smokingalso influences levels of other cardiovascular risk factors,most notably serum lipid levels, but the effect ofsmoking on disease risks is independent of its effectson other risk factors. The risk attributable to smokingpersists even when adjustments are made fordifferences between smokers and nonsmokers in levelsof these other risk factors.
Data from the Framingham Study suggestthat smoking cessation can reduce the risk forcoronary heart disease up to 64%, and that thereis a 10-fold higher risk for sudden coronary deathin smokers and 4.5 times higher in women whosmoke. 6 This study also demonstrated that filteredcigarettes are not protective. 6
Considering the overwhelming evidenceagainst smoking, the cardiologists must
necessarily intervene by always asking about thesmoking status of their patients and it is their dutyto firmly and clearly indicate to stop smoking.5 Thisconduct must be reinforced in successive visits ortelephone calls.
The different methods to reach smokingcessation are:· sudden suppression (the most common),· gradual suppression,· use of cigarettes with low nicotine & tar content· Nicotine patches - active patch subjects were
more than twice as likely to quit smoking asindividuals wearing a placebo patch. 5 Nicotinereplacement is an effective smoking cessationaid and has the potential to improve publichealth significantly and should form the basisfor treating moderate to heavy smokers. 5
Obesity : Obesity was identified as a risk factorfor early mortality before being linked to CHD riskfactors. During the last half-century, people ofmany countries including India have experiencedan epidemic of obesity. So pervasive and persistentis this condition that it can be referred to as apandemic with the proportion of adults andchildren who store excessive amounts of energyas fat, and who thereby become more likely thannormal-weight persons to develop cardiovascularand other complications, having risen dramatically.Of the three actual cause-of-death categories—cardiovascular disease, cancer, or all othercauses—risk of death from cardiovascular diseasewas most predictable from the overweight. 7
Consequently, in 1998, the American HeartAssociation reclassified obesity as ‘‘a major,modifiable risk factor for coronary heart disease’’. 7
In a recent study, among 201,622 deaths, thehighest mortality rates were among the heaviestsubjects who had no history of chronic disease andwho had never smoked: the heaviest men had arelative risk of death of 2.68, and the heaviestwomen had a relative risk of 1.89. 7 However, thisfinding is not unexpected because smoking andchronic disease promotes leanness, and a largeproportion of these subjects died with lower-than-normal BMIs.
An important lifestyle factor which alsocontributes to obesity are the weight-related eatingmeasures such as eating while watching televisionor doing homework, eating when not hungry,sneaking food, eating fast food, and so forth.

36
Diet : Recently, several intervention trials havedemonstrated that dietary therapy with nuts,plant sterols, fiber, and soy protein is as effectiveas the first generation of statin drugs in loweringlow-density lipoprotein cholesterol and C-reactiveprotein levels (approximately 30% reduction inboth parameters for diet and drug treatment).3,8
There is now adequate evidence that typesof fat are more important than the total amountof fat in determining the risk of diabetes and CHD.Substituting unsaturated fat for saturated fat hasbeen shown to decrease low density lipoproteincholesterol and improve insulin sensitivity inintervention studies. 3,8 Higher intake of vegetablefat or polyunsaturated fat (from plant-based oils,nuts, and fish) is inversely associated with CHDrisk in large prospective cohort studies. 3,8
Secondary prevention trials have demonstratedthat substituting polyunsaturated fat for saturatedfat was effective in lowering serum cholesteroland reducing cardiovascular mortality in patientswith existing CHD.
The total percentage of carbohydrates in thediet has generally not been found to predict CHDrisk. However, several epidemiologic studies havefound that diets rich in cereal fiber may protectagainst the development of CVD. Thus, metabolicconsequences of carbohydrate intake depend notonly on their quantity but also on their quality.
Available evidence also suggests that a plant-basedeating pattern rich in fruits, vegetables, whole grains,and nuts is effective in reducing risk of CHD. 3,8
Epidemiologic and clinical trial evidencesupports the view that dietary and lifestyle factorsplay predominant roles in the development ofmajor chronic diseases. Whereas cigarette smoking,obesity, and physical inactivity have long beenestablished as major causes of chronic disease, therole of specific dietary factors had not been clearlydefined until more recently. Evidence is increasingthat the quality of fat and carbohydrate plays amore important role than the quantity, and thushealth strategies should emphasize replacingsaturated and trans-fats with unsaturated fats andreplacing refined grain products and sugar withminimally processed grains. 3,8
CONCLUSION : Lifestyle and dietary modificationhave much more impact in preventing myocardialinfarction and prolonging life than medications,interventions or bypass surgery. Many patientsdo not receive adequate lifestyle advice even aftera cardiac event. Despite evidence that such actionsreduce the further risk of morbidity and mortality;these preventive managements goals are not oftenachieved. Patient education must be formalisedand acknowledged as an official part of the healthcare system.
Titbits3 Ws to keep your Heart Healthy.Walking, walnuts and wine can boost your HDL.Walnuts : These are unsaturated fats which are known to raise HDL.Walking : Aerobics, walking have shown to increase HDL, Walking 2 miles is better than running
1 mile.Wine : 60-80 ml of Red wine is known to raise HDL.
3 causes of Raised ESR beyond 100.Extra pulmonary Tuberculosis, Malignancy, Connective tissue disorders.
3 drugs a must for all Type2 DM besides OHA/Insulin.Statins, Ace Inhibitors or ARBs and Aspirin.
3 Hathiyaars without which a physician should’nt practice besides a stethoscope andBP app. are Ophthalmoscope, Pulse Oximeter and a ECG machine.
3 ways a Primary Care Physician can touch skies.Examine each patient from top to bottom, Listen to your patient completely & Attend Dr O PKapoor’s lectures
37
ADVT
38
November 2009CME on ‘Pain in Abdomen in Paediatrics by.
Dr. Modak Raza spoke and Dr. Vivek RegePulse Polio vaccination, CME on “Liver and
Pancreatic disorders” at Raheja Hospital, by Dr.D. R. Kulkarni.
CME on ‘Nephrology’ was organized atBombay hospital.
A seminar on ‘HIV AIDS’ was organized at S.L. Raheja Hospital by Dr. D. G. Saple, consultingdermatologist.
Office bearers had a meeting with ChiefSecretary, legal department of MaharashtraGovernment to discuss extension of the ordinanceto prevent assault on doctors. The ordinance wasextended in November 2009 for a period of 6 month.
Aao Gaon Chalen sub committee membersvisited Deewanmal Pada and examined 41 patients.
December 2009Web Site of IMA Mumbai Branch www.ima-
mumbai.com was inaugurated by our PresidentDr. Ramesh C. Shah.
World AIDS Day. We have organized CMEon HIV AIDS and Malaria, the speakers were Dr. S.Jayram and Dr. H. Pardawalla.
District workshop on swine flu (IMA HQ) wasorganized, the speakers were Dr. Anil Pachnekarand Dr. Om Shrivastav.
Blood Donation Camp was organized onDadar (W.R.) bridge in association with WesternRailway Employees Union and Red Cross Society.About 60 bottles of blood were collected.
CME on Management of Backache, CME onUpdates on Piles Fissures and Fistula at S. L.Raheja Hospital.
CME on Profile and Imaging was held atBombay Hospital.
IMACON 2009 and Central Council meetingwere held at Hyderabad. About 14 membersrepresented IMA Mumbai Branch. I am pleasedto inform you that IMA CGP Mumbai sub-facultyhas received IMA Dr. C.L. Jagga Award for BestFaculty of IMA CGP for the year 2009 at the IMA
REPORT OF ACTIVITIES OF IMA MUMBAI BRANCH - MAHIMA(November 2009 to February 2010)
National level. This year we have also receivedSikchi Award for best IMA CGP at State Level. Dr.Rajendra H. Trivedi has received IMA PresidentAppreciation Award for best Adjudged Secretaryof local branch for the year 2009 and Dr. HozieKapadia was honoured with IMA News BulletinAward (Editor, MAHIMA) from Dr. Ashok Adhao,our National President.
January 2010 :New year social get-to-gether was organized.
At 7.00 p.m. “Ya Katarveli” drama written by Dr.Prakash Kawli, Directed by Dr. Kishor Khusale andperformed by IMA Members was organized.
Written letter to Commissioner of Mumbaiconcerning Menace of Quacks and requested ameeting for discussing ways and means to tacklethis problem.
A meeting with police inspector KalpanaGadekar from Varsova Police Station regardingMunirkhan and Quack Doctors. She gave thedetails and progress about the case and asked forour co-operation.
Office bearers of our branch were invited byPolice commissioner,Shri D. Sivanand on theoccasion of redevelopment of Police hospital andother police welfare schemes. Police personnelcheckup scheme in association Lintas India Pvt.Ltd., was also inaugurated. IMA members will beon panel of Police panel to prepare detailed dataof Mumbai Police health hazards.
24 senior IMA Members took part in seniorcitizen run of 4.3 km in Standard CharteredMumbai Marathon 2010. We had taken partunder the banner of IMA Mumbai Branch and wespread the message of “Save the girl child”.
Super Sixes Cricket Tournament for the“Electrobin Trophy” was held at IMA lawns. Sixteams participated.
CME Programme on “ENT” was organized atBombay Hospital in association with GPA GB andBombay Hospital. Free medical check up camp anddistribution of free Jaipur foot was organized.
Flag Hoisting ceremony at the hands of ourPresident Dr. Ramesh C. Shah was held at IMA

39
Lawns at 9.00 a.m. About 40 members werepresent for the function.
A CME on Recent Trends in Detection andManagement of Psychiatric Disorder was held atRaheja Hospital Dr. Hemangi Dhavale delivered atalk on “Depression – Current Scenario”
February 201039th Annual Conference of IMA Mumbai
Branch was held that Ravindra Natya Mandir,Prabhadevi. The theme of the conference was“Save Lives – With Safe & Skilled Drives”. Theconference was inaugurated by the Chief GuestDr. Dharam Prakash, Hon. Secretary General, IMAHQ. Shri. Eknathraoji Gaikwad, Member ofParliament – Mumbai and Dr. Vijay C. PanjabiNational Vice President IMA HQ. were Guests ofHonour. We felicitated Dr. Bakulesh MehtaPresident IMA MS, Dr. Hozie Kapadia, StateSecretary IMA MS and Dr. Shivkumar Utture, Hon.Treasurer IMA MS and MMC Member. About 500delegates enjoyed the scientific sessions.Telephone Directory of members of our branchwas inaugurated.
CME on “Hematology” at K. J. SomaiyaHospital was organized.
CME on “Trends & Advances in Treatment ofBreast Cancer” at S. L. Raheja Hospital.
For the 1st time IMA Mumbai Branch hasarranged an International Tour to Bangkok &Pattaya for members and their families.
CME on “Chest Diseases” at Bombay Hospital.We have received substantial donation for
renovation of the Family Welfare Centre in IMAHouse to increase the facilities for Child WelfareClinic, Elderly Welfare Guidance Centre and FamilyWelfare Centre.
REPORT of IMA Mumbai West FOR THEMONTH OF JANUARY & FEBRUARY - 2010
Cultural programme of HALDI KUM KUM &TILGUL SAMAROH was organized on THURSDAY,21ST JANUARY 2010 at our branch premises andwas well attended and appreciated.
An Orientation Workshop on “ REPRODUC-TIVE & CHILD Health” joint programme withMCGM was held on Thursday, 11th February 2010
Cooking Demonstration “Steal a RestaurantSecret” was held on Friday 13th February 2010.In this we learned different starter like Bruchetta,Volvonus, paneer Manchurian & paneer tikka etc.
Organize the programmes of decision onMedical Legal Issue held on Friday 19th February 2010.
GERICON – 2010 was organizes on Saturday& Sunday 20th & 21st February 2010. This confer-ence dedicated to Geriactrics.
Holi Pooja & Hasya Kavi Sammelan was held onSunday, 28th February 2010 on the occasion of Holi.
ACTIVITIES OF MULUND BRANCH OF IMA
November 2009Special CME on “Sex and Marriage from G.P.’s
Perspective by Dr. Rajan B. Bhonsle, Hon. Professorand Head of the Department of Sexual Medicine atSeth G. S. Medical College & K.E.M.Hospital, Mumbai
CME on “Cardiology – Clinical & Beyond” byDr.Manjeet Juneja, Interventional Cardiologist
January 2010One-Day Conference of Mulund IMA covering
major Specialties of Medicine.
40
A meeting of the Advisory Committee, constituted by the National President, IMA Dr.G. Samaram to look into the short term medical course (BRMS) was held at 12 Noon on 15th
February, 2010 at IMA House, New Delhi.
Dr. G. Samaram, National President, IMA informed the members about the ill-healthof Dr. Dharam Prakash, Hony. Secretary General, IMA and requested Dr. D.R.Rai, Hony. FinanceSecretary, IMA to be present on behalf of Hony. Secretary General.
Dr. G. Samaram, National President, IMA welcomed all the members present andinformed them about the Resolution which was passed in the Central Council Meeting of IMAheld at Hyderabad. He informed the members that as decided by the Central Council of IMA,he has made a Drafting Committee consisting of 5-members along with National President andHony. Secretary General, IMA. This Committee met on 17th January, 2010 and prepared aMemorandum in this regard which was submitted to Hon’ble Prime Minister, Hon’ble HealthMinister, Health Secretary, Govt. of India, all Central Council Members, Working CommitteeMembers, State Presidents & Secretaries, Local Branch Presidents & Secretaries, IMA StandingCommittee for Action, IMA Standing Committee for Medical Education, IMA Standing Committeefor Anti Quackery, all Speciality Organisations and all Principals and Deans of Medical Colleges,MCI & all its members.
He also informed the members that a delegation of IMA also met the President, MCIon 28th January, 2010 to discuss the view point of Indian Medical Association.
He again informed the members about the Workshop on Alternative Model forUndergraduate Medical Education, organized by Medical Council of India, on 4th & 5th February,2010 at New Delhi which was attended by National President and the Hony. Secretary General,IMA. During this Workshop, they also had an opportunity to meet the Hon’ble Health Ministerof India along with Health Secretary, Govt. of India.
In a brief meeting that lasted for more than 45 minutes, each and every aspect of theMemorandum was discussed with them in detail. The Health Minister was of the opinionthat if IMA can take the responsibility of providing doctors to run primary health centersand sub centers in all the districts of the country, he can think of dropping this innovativeshort term course which is the need of the hour today.
Afterwards, National President then requested Dr. Ketan Desai President MCI andPresident-Elect WMA to present his view point.
Dr. Ketan Desai, in detail, briefed the members about the genesis of this short termmedical course from the year 1999 when a study group under the Chairmanship of Dr. G.P.Dutta, Past Editor, JIMA presented the alternative Rural Health Model to MCI. He also briefedthe members the need of strengthening the rural health structure of the country.
He also detailed the members regarding the discussions/decisions taken in the MCImeeting held on 4th & 5th Feb. 2010 with educationists from the entire country including theDeans/Principals of all medical colleges, Vice Chancellors of medical universities, Director,Medical Education and State Health Secretaries, Govt of India officials, and MCI memberswhere IMA National President and Hony. Secretary General were also invited and participated.(A copy of the PP Presentation is attached)
Report of the Advisory Committee, BRMSheld on 15th February, 2010 at IMA House, I.P. Marg, New Delhi.
41
He also informed the members regarding the Short Term Medical Course started byChattisgarh, Bengal and Assam Govts.
Thereafter members deliberated in detail regarding the decision of Central Council,IMA, the Proposal made by MCI and Govt. of India and various other related issues. Afterdetailed discussions, it was decided unanimously that following changes be recommendedto MCI & Govt. of India for acceptance in their proposed model of “Bachelor of RuralHealthcare” :
1. The proposed nomenclature of “Bachelor of Rural Health Care” by MCI be changed as“Diploma in Rural Healthcare”.
2. The term “Medical College” be changed to “Rural Health schools”.
3. A separate mechanism should be provided for registering diploma holders from thisCourse other than the State Medical Register.
4. Since IMA Kerala State Branch is a Party in a PIL filed against BRMS in Delhi High Court, theyshould be provided all administrative help and related documents required for the case.
The National President was requested to form an Action Committee, under hisChairmanship, consisting of 7 members representing one from each zone including HSG asthe Convenor to take necessary steps to persuade the Govt. for its proper implementation.
The IMA HQs. shall forward the recommendations of this meeting to all the StateBranches to take up IMA’s view point with their respective State Govts. for its implementation.
The meeting ended with vote of thanks to the Chair.
(Dr. G. Samaram) (Dr. D. R. Rai)National President, IMA Hony. Finance Secretary
Congratulations and Kudo’s to your dynamic self forbeing rightly elected as the President of World MedicalAssociation.
Seasons may come, Seasons may go, Everything fadeswith time, this all of us know,
But one thing which freshly blossoms as fresh as dew,Is LOVE, RESPECT and AFFECTIONS for you.
We at IMA MS and the whole medical fraternity feelproud of you. India is proud of you.
May Lord shower upon you the essence of everychoicest things you dream in life.
CongratulationCongratulationCongratulationCongratulationCongratulation



![“Jîn” bi Kurdî u Inglîzî · S¸nda Hipokratik [Hippocratic Oath] yan S¸nda Lezanye [Lasagna Oath]. B¸k u zava li mehrª ji ber¸ Xwidª u xªzan u hevala s¸ndª dixwin](https://img.pdfslide.net/doc/110x75/5e6a97d289f6500e5a61ab6d/aoejna-bi-kurd-u-inglz-snda-hipokratik-hippocratic-oath-yan-snda.jpg)

























