Embed Size (px)
Citation preview


The human face
An account of the postnatal growth and
development of the craniofacial skeleton


The human face
An account of the postnatal
growth and development of
the craniofacial skeleton
Donald H. Enlow, Ph.D. Professor of Anatomy, University of Michigan, and Director, Craniofacial Program, University of Michigan Center
for Human Growth and Development, Ann Arbor
ILLUSTRATIONS BY W I L L I A M L. B R U D O N
Hoeber Medical Division Harper & Row, Publishers, New York, Evanston, and London

THE H U M A N FACE: AN ACCOUNT OF THE POSTNATAL
GROWTH AND DEVELOPMENT OF THE CRANIOFACIAL
SKELETON. Copyright © 1968 by Hoeber Medical Division, Harper & Row, Publishers, Incorporated. Printed in the United States of America. All rights reserved. For information address Hoeber Medical Division, Harper & Row, Publishers, 49 East 33rd Street, New York, N.Y. 10016.
LIBRARY OF CONGRESS CATALOG CARD NUMBER: 5 8 - 1 8 8 4 3

Contents
Preface xiii Acknowledgments xv
( I ) CARTILAGE AND BONE
(1 ) Cartilage 3
Structure and growth of cartilage 5 Cartilage—Two modes of growth 8 Age changes in cartilage structure 9 Cartilage and bone structure compared 9
(2) Bone 11
The composite nature of bone matrix 11 The evolution of bone and its components 12
TYPES OF BONE TISSUES 14
Cellular and noncellular bone 14 Vascular and nonvascular bone tissues 15 Lamellar and nonlamellar bone 15 Laminar bone 17 Primary vascular bone 17 Coarse cancellous bone 19

( v i )
Fine cancellous bone 21 The primary osteon 22 Plexiform bone 24 Periosteal and endosteal bone 25 The surface template 25 Compacted, coarse cancellous bone 27 Inner and outer circumferential bone 29 Haversian bone 31 Special varieties of bone 37 The structural nature of bone 37
THE GROWTH OF BONE 37
Centers of ossification 42 Intramembranous ossification 42 Endochondral (intracartilaginous) ossification 45 Adult distribution of endochondral and intramembranous
bone 52 Endochondral ossification in the skull 52 Growth sites 53 The functional role of the epiphyseal mechanism 54 Age changes in bone—Transitions between neonatal and
adult bone tissues 55
( 3 ) Skeletal morphogenesis 57
Remodeling 57
Bone surfaces and directions of growth 58 Area relocation 61 The V principle 65 Linear growth and remodeling 65 Cortical drift 69 Cortical layering 72 Cortical movement—Displacement versus growth 75 Differential growth 77 Wolff's law 79
( 4 ) The growth of soft tissue membranes associated with bone 83
The concept of the moving growth field 83
Contents

Contents
THE PERIODONTAL MEMBRANE 85
Composite movements of teeth and bone 85 Alveolar bone surfaces 87 The fibers of the periodontal membrane 89 The mechanism of periodontal drift 91 Secondary alveolar remodeling 94
SUTURES 94
The structure of the sutural membrane 94 Bone growth at sutures 95 Growth adjustments in the sutural membrane 95
THE PERIOSTEUM 99
Haversian remodeling 100 Periosteal-endosteal transitions 101
The perichondrium 101
( I I ) CRANIOFACIAL BONE GROWTH
( 5 ) Summary of growth principles 105
Generalized surface growth 105 Centers of growth 105 Generalized surface growth following cessation of
growth-center activity 105 Overall growth—Size increase and remodeling 107 Relocation 108 Surfaces facing directions of growth 108 Growth movements—Drift and displacement 108 The V principle 108
( 6 ) The mandible 109
The condylar mechanism J10 The condylar neck 110 The posterior margin of the ramus 112 The mandibular (sigmoid) notch 113 The coronoid process 115 The buccal side of the ramus 119 The lingual side of the ramus 121
( v i i )

( v i i i )
The antegonial region 123 The mandibular body 125 The sublingual fossa 127 The trihedral eminence 129 The mandibular arch 129 The chin 131 Muscle attachment on resorptive surfaces 131 Application of growth principles to the development
of the mandible 133 Generalized surface growth 133 Centers of growth 133 Generalized surface growth following cessation of
growth-center activity 134 Growth in conjunction with remodeling 135 Relocation 135 Surfaces facing directions of growth 135 Growth and displacement 136 The V principle 137
( 7 ) The nasomaxillary complex 138
Growth centers in the face 139 The maxilla 140 The maxillary tuberosity 141 The zygomatic process of the maxilla 143 The maxillary arch 144 The palatine processes of the maxilla 145 The premaxilla 148 The nasal region 151 The orbital floor 155 The maxillary sinus 157 Discussion 158 The zygomatic bone 159 The nasal bones 161 The palatine bone 163 The lacrimal bone 163
( 8 ) Comparative morphogenesis of the facial skeleton 168
FACIAL GROWTH AND REMODELING IN Macaca 171
The mandible 171
Contents

Contents
The nasomaxillary complex 175 General plan of facial growth 181
COMPARISON OF FACIAL GROWTH IN MAN AND THE
RHESUS MONKEY 182
T H E UPRIGHT NATURE OF THE HUMAN FACE 186
The facial pocket 186 Nasal and orbital orientation 188 Growth of the facial complex 189
( 9 ) Growth of the calvaria and the cranial base 194
THE SKULL ROOF 195
Growth fields 200
THE CRANIAL FLOOR 201
Basic plan of growth 201 Endocranial compartments 203 The occipital bone 207 The sphenoid bone 209 The pterygoid processes 217 The ethmoid 218 The vomer 219 The frontal bone 220 The temporal bone 221 The auditory ossicles 223 The malleus 223 The incus 225 The stapes 226
( 10 ) The composite nature of facial growth 227
GROWTH AND DISPLACEMENT 228
The standard cephalometric picture 228 Visualization of growth patterns without fixed
reference marks 230 Scheme of maxillary growth 233 Sutural and remodeling growth 236
THE MOSAIC PATTERN OF FACIAL GROWTH 239
The forehead 239
( i x )

(x )
The malar region 240 The nasal region 242 The maxillary arch 245 The anterior portion of the maxillary arch 246 The orbital region 247
FACIAL TOPOGRAPHY 250
(11) Glossary of reversals 253 The nasomaxillary reversal 257 The malar reversal 257 The zygomatic reversal 257 The intraorbital reversals 257 The circumnasal reversals 257 The pterygoid reversals 258 The circumcranial reversal 258 The petrosal reversal 258 The sphenoidal reversal 258 The circumspinal reversal 258 Medial mandibular reversals 259 The lateral mandibular reversal 259 Anterior reversal of the ramus 259 The antegonial reversal 259 The mental reversal 259 Other regional reversals 259
(12) Elementary principles of cephalometrics
W. Stuart Hunter 261
TECHNOLOGY 263
TOTAL ERROR AND ENLARGEMENT 264
THE USE OF CEPHALOGRAMS 265
Temporal bones 274 Sphenoid 274 Zygoma 274 Maxilla 274 Mandible 277
LANDMARKS 277
Nasion 277
Contents

Contents
Orbitale 279 Anterior nasal spine 279 Subspinale 279 Prosthion 279 Incision superius 279 Incision inferius 279 Infradentale 279 Supramentale 279 Pogonion 279 Gnathion 279 Menton 279 Basion 279 Posterior nasal spine 279 Sella 280 Articulare 280 Gonion 280 Pterygomaxillary fissure 280 Key ridge 280 Porion 280 Bolton point 280 Midline structures 280 Bilateral structures 280
CEPHALOMETRIC PLANES 280
Sella-nasion 280 Frankfort 281 Basion-nasion 281 Palatal 281 Occlusal 281 Mandibular 281 Ramal 281 Facial 28 J Incisors 281
CEPHALOMETRICS AND GROWTH STUDIES 281
Bibliography 287 Index 295
(x i )

Preface
This monograph deals with a selected, specialized body of information. It is not intended to be an encyclopedia of factual and historical data covering all facets of craniofacial biology. The objective is to describe and illustrate a particular, fundamental mode of approach to the study of craniofacial growth. The contents describe primarily the complex behavior of bone tissue during the growth of the skull. Basic principles and concepts are emphasized throughout. The general approach is that of a morphologist concerned with postnatal morphogenesis, and the particular points of view are based largely on the author's own investigations of bone remodeling and growth mechanisms in the human craniofacial skeleton.
By request, Dr. W. Stuart Hunter has prepared a special chapter on basic cephalometric techniques and procedures. It is felt that an introduction to the fundamentals will be useful to those lacking knowledge of this essential subject. It will also provide an introductory overview for individuals planning to specialize in this field.
Background training in the structure, growth, and remodeling of bone varies widely among the different workers in the field. The
introductory chapters in this monograph are provided for those who wish to expand the scope of their understanding. For those already knowledgeable in the subject these chapters will also serve as a review of relevant terms and concepts used in later sections. It has been the author's experience that bone descriptions in most elementary histology courses are generally inadequate for an advanced-level understanding of craniofacial bone growth. Such courses traditionally dwell on the structure of the Haversian system and the different zones in the epiphyseal cartilage. Beyond this, a comprehension of the truly dynamic qualities of bone and the many versatile mechanisms utilized in its growth and remodeling become difficult for the beginning student to appreciate and understand, particularly during rapid survey courses. The time given to the different basic sciences in current medical and dental curricula is continually being reduced, and additional effort has become required on the part of the individual to further his own knowledge of the fundamentals of craniofacial bone growth.
Because bone is hard, it represents a specialized kind of tissue. Because it is hard, bone has
xiii

( x i v )
features of structure that are specially adapted to it. Because bone has a hard calcified matrix, it has special processes of growth. These processes are clear cut and follow a well-defined, straightforward sequence. They are complex but can be readily traced if underlying principles, described in the first part of this monograph, are well understood. Part I is a consideration and an evaulation of bone from the standpoint of its behavior during skeletal morphogenesis. It is not intended as an elementary account. On the contrary, it is presumed that the reader already has a reasonable knowledge of this tissue and the vocabulary pertaining to it. The purpose is to go beyond standard textbook accounts in order to establish a special yet fundamental body of information prerequisite to dealing with the specialized topics discussed in Part II.
Part II deals with an analysis of growth in
Preface
the human craniofacial skeleton. It gives a detailed account of events involved in the maturation of each individual bone in the skull. No attempt has been made to include all viewpoints pertaining to facial growth since the objective is to provide a specialized reference book giving specific attention to this one facet. When the principles given in Part I and the application of these principles are considered together, the underlying nature of craniofacial bone growth can be visualized in more meaningful perspective. How these concepts are involved in the growth of bones in the human skull and what happens to the bones themselves as they grow are the particular subjects of this book.
Donald H. Enlow, P H . D .
Ann Arbor, Michigan

The primary organization and execution of the illustrations used in this monograph have been by Mr. William L. Brudon. Mr. Brudon has worked closely with me in translating the difficult concepts and events involved in craniofacial bone growth into meaningful, interpretive diagrams and illustrations. It is felt that he has succeeded in developing a series of descriptive figures that very effectively relate the moving, dynamic nature of growth in the human skull. Both Mr. Brudon and I are grateful for the assistance of Miss Janet Wyman, Miss Rosalind Price, and Mrs. Margot Hull for their skillful rendering of some of these illustrations.
Mrs. Hella Anderson, my chief technician, has helped with the preparation of many thousands of bone sections used throughout our long-term studies. I am indebted to Mr. Louis Martonyi for his skillful production of the
Acknowledgments
photomicrographs used in this book. Studies dealing with sutures and the process of sutural growth were carried out in collaboration with Dr. Leif Linge. I wish to acknowledge gratefully the tolerant manner in which Mrs. Antoinette Catron and Mrs. Pamela Gogulski have edited and typed the manuscript.
Permission has been granted by the C. V. Mosby Company, The Wistar Institute of Anatomy and Biology, and Charles C Thomas, Publisher, to reproduce figures from my previous works.
The original long-term research investigations that have led to the present monograph were supported in part by U.S.P.H.S. Grants DE 01903 and HD DE 02272.
Donald H. Enlow, P H . D .
Ann Arbor, Michigan

(I)
Cartilage
and bone

(1)
Cartilage
Cartilage is composed of cells and an intercellular matrix containing fibers and ground substance. The structure and function of cartilage, as in any connective tissue, are associated with the proportions in which these three components are combined. A moderate distribution of cells is present within a dense meshwork of fine collagenous fibers. The premium functional component of this tissue, however, is its distinctive ground substance. The matrix of young cartilage has a very high concentration of chondromucoprotein containing aggregates of sulphated polysaccharides. This substance, chondroitin sulfate (so named because of its characteristic presence in the matrix of cartilage), is associated with non-collagenous protein, a combination that has the special property of marked hydrophilia.
Because of the high water content within a viscous ground substance, cartilage is particu
larly firm and turgid, a feature that provides the structural basis for its several specialized functions. Cartilage is rigid, but unlike bone it is soft and flexible. Although this tissue can be readily cut with a fingernail, it provides primary support for a number of organs, including the trachea, nose, external ear, and larynx. Because cartilage is soft, however, support is flexible in character and permits a measure of distortion in the organ involved.
At the ends of most long bones, the soft, rigid, articular cartilage provides a specialized bearing surface for joint contacts. Cartilage is a tissue that is adapted to withstand direct compression, in contrast to bony tissues which generally have relatively low threshold sensitivity to pressure. Cartilage is able to tolerate great pressure without resorption, but at the same time it can provide a relatively friction-less surface in conjunction with synovial secre-
3


( 5 )
that are widely separated by ordinary intercellular ground substance containing a sparse scattering of immature fibrils. The entire area at this developmental stage is vascular in nature. The beginning of cartilage differentiation is marked by rapid proliferation of some of these cells. As the precartilage cells increase in number, they become enlarged in size, rounded in shape, and arranged in close proximity to one another. The intercellular matrix at this stage is negligible.
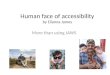
As a chondrogenic growth center begins its internal series of maturation steps, other mesenchymal cells located at the periphery of the same general area undergo a different sequence of cell and matrix changes. These particular cells become involved in the early formation of the perichondrium, a dense fibro-elastic sheath that very soon envelops the mass of developing and expanding cartilage. In Figure 1, note that proliferation of young chondrocytes and the subsequent increase in the cartilage mass proceed in such a way that existing blood vessels and nerves become positioned within the perichondrium but are excluded from the expanding cartilage matrix itself. As
Cartilage
tions. Because most articular-bearing surfaces lack a covering vascular membrane, the non-calcified matrix of cartilage provides a permeable medium for the passage of nutrients and metabolic wastes to and from distant vascular sources. Furthermore, cartilage is a tissue that is specially adapted to the rapidly growing fetal skeleton as well as to postnatal epiphyseal growth. The structural and physiologic basis for these various functions are outlined in the following paragraphs.
STRUCTURE AND GROWTH OF CARTILAGE.
Stages involved in the progressive differentiation of embryonal mesenchyme* into mature cartilage are illustrated in Figures 1 and 2. Prior to chondrogenesis, a region of future cartilage development is composed of a loosely organized aggregation of mesenchymal cells
* Succeeding generations of undifferentiated cells, comparable with mesenchyme, are maintained throughout the life of the individual. These cells provide a reserve that is available for continued growth, replacement, and repair. They are located in close proximity to capillaries and are termed undifferentiated perivascular cells. They become constandy utilized during the continued growth and maintenance of cartilage and bone.
The structure and growth of cartilage. In a center of chondrogenesis (a), the cells and matrix of undifferentiated vascular connective tissue (late mesenchyme) undergo a sequence of changes that leads first to a mass of precartilage (b). The cells enlarge and become closely packed (2). Other mesenchymal cells experience differentiation into cells of the young perichondrium ( I ) . Note that vessels are incorporated within this covering membrane but excluded from the matrix of the cartilage itself. As new chondrocytes are formed (4) directly from cells in the inner layer of the perichondrium, young existing chondrocytes simultaneously enlarge (3) and become more deeply enclosed within the growing
cartilage mass. These cells become rounded in shape. Ground substance is formed by the chondrocytes and deposited as a principal component of the matrix, which results in a characteristic hyalinization of the matrix. The fibers of the perichondrium can be seen to seemingly disappear as they enter the matrix of the cartilage. The rectangular inset shows the dense feltwork of fine matrix fibers as they would appear without superimposed ground substance. The continued formation of matrix progressively separates the cells within the cartilage. The deeper chondrocytes now undergo repeated cell divisions to form clusters of daughter cells (5).
Figure 1

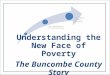
The nature of cartilage growth. The dual mechanism of cartilage growth is schematized in this succession of growth changes. It demonstrates the simultaneous oppositional and interstitial modes of enlargement. A chondrogenic cell in the perichondrium ( a ) is enveloped by new matrix and thereby becomes a young chondrocyte ( b ) . Wi th continued growth, this cell becomes successively more deeply enclosed as new cartilage is formed by the perichondrium (apposi
tional growth). The cell itself enlarges, thus contributing to cumulative interstitial growth ( c ) . It subsequently undergoes cell division ( d ) , and forms an isogenous group of daughter chondrocytes. Note that the scattered cartilage cells in general are becoming more distantly separated from each other as a result of continued matrix deposition. These latter three processes constitute interstitial growth.
Figure 2

Cartilage
the perichondrium undergoes continued differentiation, its former mesenchymal cells become elongated and fusiform, and young collagenous fibers are formed between them in a circumferential plane. These perichondrial cells resemble ordinary fibroblasts and have a similar function, but they retain an active chondrogenic potential.
The closely packed aggregation of young chondrocytes within the cartilage mass undergoes continued developmental and maturation changes. The intercellular matrix now begins to appear. A fine but dense feltwork of collagenous fibers, deposited by the chondrocytes themselves, is formed between cells. Simultaneously, chondrocytes produce and deposit ground substance which occupies interstices between the interlacing fibers. Because similar refractive indices exist between ground substance and fibers, the fibrous mesh becomes obscured. The intercellular matrix thus has become hyalinized* by the superimposition of ground substance over and around the fibrils. This results in a hyaline matrix that gives the tissue its name. In other varieties of cartilage, an increasing accumulation of either elastic or dense bundles of coarse collagenous fibers characterizes the interterritorial matrix between hyalinized islands of ordinary cartilage.
As the intercellular matrix (fibers and ground substance) accumulates between young chondrocytes, the cells are thereby pushed progressively farther from each other (Fig. lc) . Each chondrocyte undergoes repeated cell divisions and, sequentially, resulting daughter cells in turn become separated by their own production of intercellular matrix.
* Many tissues, such as bone, similarly become hyalinized during development. This term denotes a matrix that has been rendered glassy or homogeneous in appearance. If a tissue becomes hyalinized, this does not imply that it has become transformed into cartilage.
( 7 )
Simultaneous with these processes, which recur throughout the period of growth, the surrounding perichondrium itself is responsible for further growth increases of the cartilage mass. This membrane, as noted above, is composed of connective tissue that contains most or all of the neurovascular elements of the cartilage. Its matrix contains circumfer-entially oriented, densely arranged collagenous fibers with interspersed connective tissue cells (fibroblasts). The inner region is chondrogenic and contains elongate, fusiform cells that resemble ordinary fibroblasts but that have retained active growth potential. They undergo direct differentiation into young chondrocytes, a conversion process that involves essentially the elaboration of new matrix around each cell. Further maturation changes in both the matrix and the chondrocytes subsequently occur.
In Figure 2, it is seen that cells in the chondrogenic part of the perichondrium are elongate and spindle-shaped, in contrast to the more spheroid configuration of mature cells located deeper within the cartilage matrix. Note that a gradual transition in shape begins just deep to the perichondrium. Equalization of pressures in the deeper parts of the cartilage is believed responsible for this rounding of the cell's shape.
As the undifferentiated chondroblasts lay down a dense feltwork of young collagenous fibers around themselves, these fibers become directly continuous with the fibrous mesh of the underlying cartilage matrix and the coarser fibers in the enveloping outer part of the perichondrium. This process of linkage maintains uninterrupted fibrous connection from the outer covering membrane to the innermost part of the whole tissue mass. The fibers of the perichondrium, in turn, are continuous with the fibrous stroma of other contiguous organs.
As the fibrous mesh forms within new cartilage matrix, ground substance is simultane-

(8)
ously deposited by the cells, thereby hyaliniz-ing this formative matrix just deep to the perichondrium. The connective tissue cells formerly located in the chondrogenic part of the perichondrium have now become completely enclosed by their own matrix deposits, and they represent a new generation of young chondrocytes. Collagenous fibers entering the cartilage from the perichondrium may be traced for a short distance until they seemingly disappear within the hyaline matrix. The new, peripherally located chondrocytes retain their fusiform shape for a time but gradually become rounded as they are subsequently covered by still more formative cartilage laid down by the outward-moving perichondrium. The enclosing membrane itself keeps pace by continued proliferation of new connective tissue cells and collagenous fibers. As it does so, the entire perichondrium, including its vascular and nervous components, moves in a peripheral manner in advance of the enlarging cartilage mass. Cell division within the chondrogenic zone maintains the population of these undifferentiated cells as this layer continues to produce new cartilage beneath it.
The cells recently transformed from the chondrogenic layer of the perichondrium into young chondrocytes as a result of matrix deposition now undergo a continuation of the same basic sequence of growth changes. They (1 ) proliferate by cell division, and (2 ) become progressively separated from one another by continued matrix deposition. Thus, as new cartilage is formed externally by the perichondrium, the cartilage laid down by this membrane during former stages continues to undergo additional growth expansion.
CARTILAGE—Two MODES OF GROWTH. It
is apparent that the process of cartilage enlargement involves two separate, basic growth mechanisms which proceed independently but
Cartilage and bone
simultaneously. These are the appositional and the interstitial processes of growth.
The appositional growth of cartilage is brought about by deposition of entirely new layers of cells and intercellular matrix on existing outer surfaces of the cartilage through the activity of the perichondrium. When overall growth subsides, the chondrogenic zone of the perichondrium becomes dormant.
The interstitial growth of cartilage involves three changes. First, chondrocytes already present within the cartilage mass undergo division, thereby enlarging the total expanse of the tissue. Second, increase in the size of individual cells further contributes to overall tissue dimensions. Third, formation and continued accumulation of additional matrix adds to the total volume of cartilage. Appositional growth is a process of external addition. New cartilage is added onto the outer surface of the old. In contrast, interstitial growth is a process of internal expansion of already existing cartilage. Both growth processes occur in cartilage, and they proceed simultaneously.
Major variables in the relationships of cartilage with other tissues and organs, however, directly affect modes of growth. The versatility of the cartilage growth mechanism is such that one or the other, or both, of the processes described above may be utilized in differing circumstances. For example, the bearing surface of articular cartilage in long bones lacks a covering perichondrium. Thus, any increase or regeneration in this particular location must proceed solely by interstitial growth. Similarly, contact surfaces between cartilage and bone, as in the epiphyseal cartilage or the cartilage within a cranial synchondrosis, are without a perichondrium except for a small portion at their lateral margins. Cartilage growth must necessarily take place largely by interstitial expansion. Appositional growth here is subordinate and contributes primarily

Cartilage
to the lateral increase of the cartilage plate. In areas involving matrix calcification, however, interstitial growth cannot take place, and continued increases in overall size must proceed through appositional deposition by its enclosing perichondrium or by interstitial growth in adjacent noncalcified regions.
AGE CHANGES IN CARTILAGE STRUCTURE.
It is apparent that the older regions of a given cartilage mass occur within its deeper parts. Younger regions lie in proximity to the perichondrium. As a chondrocyte matures, its cytoplasm accumulates large quantities of glycogen and lipids, which add to the increasing size of individual cells as well as to the aggregate dimensions of the entire tissue. The chondrocytes become more remotely separated as a result of continued matrix formation. As growth begins to slow, however, the last-formed generation of daughter cells does not become subsequently separated as did previous generations. The cells remain in near contact and thereby form characteristic isogenous groups of cells (cell nests). Because ground substance production is a function of individual chondrocytes, a noticeable gradient of matrix basophilia occurs in a direction away from each cell and cell nest as a result of the decreasing content of chondroitin sulfate. This factor is responsible for the occurrence of the "capsule" as well as the territorial and inter-territorial matrices. With increasing age, this basophilia is typically lost in the interterritorial matrix so that the underlying eosinophilic fibrous matrix can be visualized. Accumulations of an albumoid further augment this interterritorial eosinophilia as the cartilage ages. Typical patterns of basophilia in some routine preparations may be lost as an artifact because of solubility of ground substance in the reagents used during tissue preparation and staining.
( 9 )
Young rapidly growing cartilage is characterized by smaller individual cells. These chondrocytes are positioned close together because they have not yet become widely separated by cumulative matrix increases. Cytoplasmic inclusions are minimal, and isogenous groups have not yet formed. The matrix is lightly basophilic, although gradients of staining reaction are not as apparent as in more mature cartilage. In a large mass of growing cartilage, the innermost central portions begin to show features associated with maturity; more peripheral areas appear less differentiated in general structure.
The intercellular matrix in old cartilage may become calcified. The usual staining response is a much deeper basophilia in comparison with ordinary noncalcified cartilage, in contrast to the characteristic eosinophilic nature of calcified bone matrix, a feature presumably caused by differences in ground substance. Calcification of ordinary cartilage is an aging change, and it is also a process that always precedes replacement by endochondral bone, as in some elements of the larynx. In the numerous "endochondral" bones of the young skeleton, however, such replacement is utilized as a routine developmental process (see Chapter 2) . Calcification is a step involved in sequential changes that can lead to cartilage resorption, regardless of age.
CARTILAGE AND BONE STRUCTURE COM
PARED. Both of these tissues represent specialized skeletal variations of ordinary connective tissue, and their respective features show a number of structural similarities. Both are composed of connective tissue cells with an intercellular matrix containing collagenous fibers and ground substance. They both have an enclosing vascular membrane, and this covering tissue is characterized by a marked growth potential. The matrices of cartilage and

( 1 0 )
bone are receptive to calcification, although cartilage shows much variability in this regard. The firm rigidity of both tissues is adapted to functions of support.
Varying functional and morphologic relationships, however, are associated with several major differences in their respective structure. Because cartilage for the most part is noncalci-fied, a system of canalicular connections between lacunae is not involved in the passage of extracellular materials. Furthermore, for the same reason a vascular canal system is lacking in cartilage, because direct diffusion through its soft matrix readily occurs. Because extrinsic pressures may be involved in the many functional relationships of cartilage, the lack of blood vessels within this tissue is an adaptation to the soft nature of its matrix. Bone, in contrast, has a calcified matrix housing a system of rigid-walled vascular canals with their continuing, elaborate network of canalicular channels.
As a direct consequence of the calcified nature of bone matrix, fundamental growth mechanisms in this tissue necessarily differ from those in cartilage. The latter utilizes both appositional and interstitial processes of growth. Bone, however, can enlarge only by an appositional mode of growth. (This basic consideration will be elaborated later.) Also, the calcified matrix of bone necessitates a complex, special process of structural remodeling
Cartilage and bone
during growth, a situation virtually lacking in ordinary cartilage. (Most tissues, hard or soft, undergo processes of internal reconstruction throughout life. The mechanism of remodeling in bone, however, represents an additional process concerned directly with morphogenetic changes associated with a mineralized tissue matrix.) For a variety of physiologic and mechanical reasons, bones ordinarily become hollowed in their interior. No division into a cortex and medulla occurs in cartilage, however, and internal membranes comparable to the endosteum are lacking. Cartilage, on the other hand, can function in normal circumstances in the absence of any covering membrane, a circumstance not found in bone because it requires a periosteum and an endosteum, or some other comparable tissue, in order to provide vascular supply. A process of resorption is a constant, normal feature during (as well as after) bone growth. Resorption in cartilage is ordinarily restricted to those parts associated with matrix calcification and bone replacement.
Bone is a most variable kind of tissue, and the structure and the arrangement of its components differ widely as a consequence of different growth circumstances. Some bone types, for example, are nonvascular and others are noncellular. The basis for these and many other structural variations will be discussed in later chapters.

(2)
Bone
Bone is a specialized tissue that provides the property of hardness in its calcified matrix. The specializations of structure and the peculiarities in growth are directly associated with this feature of hard rigidity, in comparison with cartilage and other connective tissues that have a soft matrix. Because bone is hard, the fundamental plan of tissue construction is adapted to its special relationships with other tissues and organs, to its distinctive manner of nerve and blood supply, and to its particular modes of repair, replacement, and reconstruction. Because of hardness in the bone matrix, the entire process of growth is unique, and it involves a specialized mechanism of progressive remodeling.
THE COMPOSITE NATURE OF BONE MATRIX.
Because bone represents a variety of connective tissue, it is composed basically of cells,
fibers, and ground substance. The intercellular matrix is characterized by two phases, the organic and the inorganic. The former consists of collagenous fibers and a mucopolysaccharide ground substance. The inorganic phase is composed of apatite and other mineral deposits.
If a whole bone specimen, such as the mandible, is decalcified using an acid or a chelator, the matrix is rendered soft. The bone's shape and volume, however, are not materially altered, and the bone can be bent or otherwise distorted without breaking. Conversely, if a whole bone specimen is calcined by intense heat or by chemical treatment so that only the mineral phase is retained, the bone still displays its original shape and volume. However, it is brittle, hard, and frangible. It is only when these two phases act in combination that they perform functions which neither can carry out separately. The merging of the or-
11

( 1 2 )
ganic and inorganic phases of bone makes possible the presence of rigid hardness and great tensile strength in the same tissue.
THE EVOLUTION OF BONE AND ITS COM
PONENTS. The first-known vertebrates (jaw-less fishes) in the lower Paleozoic already possessed both bone and cartilage.* Similarly, both membranous (dermal) and endochondral bone types were present in these ancient forms, and one did not precede or originate from the other in an ancestral manner. Endochondral bone, phylogenetically, represents a bone-replacement mechanism in provisional skeletal tissues (cartilage) located within the more interior regions of the developing body. Membrane bone, generally, represents a counterpart of the original, outer dermal armor of ancient (as well as some surviving) forms, and it develops within "membranous" connective tissue (the dermis) without intervention of a cartilage stage. Skeletal phylogeny, from the Paleozoic through the Cenozoic, has involved a complex series of adaptations, changes, combinations, consolidations, and losses of the many units within these generally inner and outer parts of the skeleton. Most of the original dermal elements have not been retained in modern "higher" groups. Those individual bones that have survived among most mammals are associated largely with the facial skeleton, the calvaria, and parts of the pectoral girdle. Many have become fused with each other as well as with some unrelated elements in the endochondral part of the skeleton.
Evolution is ordinarily associated with the phylogeny of organs and organ systems. In bone, as well as in other calcified structures,
* The old puzzle as to which of these two tissue types can be considered the more primitive is meaningless and irrelevant, since they represent two different kinds of tissues individually adapted to entirely different functions. One is not phylogenetically derived from the other.
Cartilage and bone
the historical development of a tissue can be visualized and traced in time because it survives in the fossil record. The preservation of histologic detail in the bone of ancient forms that are many millions of years old is often quite good, and thin-section preparations are usually comparable in general quality to sections of modern bone (Enlow and Brown, 1956, 1957, 1958).
Some of the oldest known bone tissues contained bone cells (their lacunae survive), canaliculi, a network of primary canals, and a calcified matrix. The collagenous nature of the intercellular matrix in a number of early fossil bone samples has been verified by histochemi-cal tests. A lamellar arrangement of the matrix can also be observed in some ancient fossil forms. Haversian systems, however, were not present in the bone of the earliest vertebrates. They are not, in fact, found in a great many vertebrate groups, either fossil or modern. The notion that Haversian systems represent a structural "unit" of bone is erroneous and has done much to confuse workers in interpretations of bone structure and growth. The Haversian system, further, is not a structural culmination of bone tissue evolution, presumably found only in higher but not in lower forms, as has sometimes been assumed. These structures are not present at all in many higher groups, but they are, on the other hand, found in some lower forms, fossil as well as recent.
A basic problem involved in attempts to interpret the evolution of bone is to properly equate ordinary phylogenic concepts to the tissue level. One is tempted, for example, to look for "intermediate" stages that form an evolutionary series, to attempt to recognize "straight-line" evolutionary progressions, or to apply the misleading concept of "primitive versus advanced" at the tissue level. The bone in any given vertebrate form, high or low in traditional classification and at any level in

Bone
geologic time, represents a tissue that is specially adapted to the size of the individual's body, its overall rate of enlargement, particular modes of skeletal growth, seasonal variations, duration of body growth, the morphology of the different bones, life span of the individual, and other related factors. As will be shown, all of these considerations bear directly on the structural nature of the bone tissue in any species.
A study of bone tissues in the fossil record shows that an orthogenetic series of straight-line, progressive, advancing changes from early vertebrates to those existing today has not taken place. Bone did not begin as a simplified, primitive kind of tissue that subsequently increased in complexity gradually through time in a succession of ancestral groups to finally reach an advanced status present in contemporary forms. There are no singular kinds of bone that can be identified specifically with all fish, amphibians, reptiles, birds, and mammals. One cannot identify in the bone of an ancient or modern amphibian unique ancestral characteristics that have led in an ascending manner to the bone in reptiles; nor does the bone of fossil or present-day reptiles have special characteristics that distinguish it as the intermediate, more primitive parent of modern mammalian bone. Intermediate stages or links in bone tissue structure also are not found in the morphologically intermediate species or groups among fish, amphibians, reptiles, and mammals. Marked similarities in structural pattern can occur between groups only remotely related. This is not a consequence of direct ancestry between them but rather a result of convergence caused by parallel factors involved in their growth and development.
It cannot be assumed, moreover, that the ontogeny of human (or other mammalian) bone recapitulates the phylogeny of all past evolutionary stages. Bone tissues in some early
( 1 3 )
fossil amphibians and reptiles, for example, can be much more "advanced," specialized, and complex in structure than the bone in many modern present-day mammals. The bone in the fetus is adapted primarily to the fetal circumstances of growth and not directly to ancestral heritage, except in the sense that it has become adopted into a genetic framework according to these same circumstances of growth.
What, then, is the basis for bone tissue evolution? The earliest known bone tissues were already in possession of the basic components of structure found in present-day bone tissue. The history of bone phylogeny has been one of recombining and rearranging these fundamental components according to factors involved in the characteristics of growth and physiology in each individual species or group. It is noteworthy that no major basic unit of structure has been added to this primitive (early) complement of structural components. However, some have become secondarily lost (phylogenic reduction) in certain groups. For example, some fishes have lost all adult bone cells. Some reptiles have lost most or all vascular canals in their bone. Parts of bones in many mammals, in fact, often have greater or lesser areas that are virtually nonvascular in structure.
If one examines the microscopic structure of bone from (1 ) different species, ( 2 ) different ages in the same individual, (3 ) different bones in the skeleton, and ( 4 ) different regions in the same bone, he will encounter a perplexing variety of structural designs. However, only about a dozen fundamental patterns of combination of the basic tissue components exist to account for most of these differences.
The essential consideration is that bone is a very labile and adaptable kind of tissue, both phylogenetically and ontogenetically, and that it is quite sensitive to the many factors of growth, physiology, life span, size, etc., that

( 1 4 )
characterize each species. The dozen or more basic kinds of bone tissue that exist are related to these particular factors, rather than a single phylogenetic plan that determines and establishes bone structure according to ancestry without regard to adaptive function and developmental circumstance.
Types of bone tissues
Differential growth rates, the length of life span, duration of body growth, and the overall size of the animal are basic factors associated with the occurrence and distribution of the different kinds of bone. For example, the fetal growth period of a laboratory white rat is measured in days; that in the human extends for months. The human newborn is much larger, however, than the adult size of the white rat. Bone growth in the postnatal human skeleton proceeds at a far more rapid rate than that in the much smaller growing rodent. Considerably more bone is deposited in shorter periods of time and over a much longer total span. Furthermore, the human will live for many decades, whereas the rat's life span is only a year or two.
Factors such as these bear directly on the marked differences in the microscopic structure of bone found in different animals. They are associated also with the many variations in structure found at succeeding age levels in any given species. Rate and extent of growth relate directly to the basic variety of structural patterns produced during bone deposition. Rapid growth is thus associated with certain kinds of bone tissue and, conversely, slower skeletal growth is associated with other quite different types.
A basic consideration is the contrasting rate of growth in various parts of a bone at the
Cartilage and hone
same time. Although some areas in a single bone undergo a fast pace of growth, other parts simultaneously follow much slower growth. Such variable growth rates may occur adjacent to each other and result in the formation of quite different patterns of structure in areas of close proximity. Most regions of a bone undergo periods of rapid increase followed in turn by increments of slower growth. This is a frequent occurrence and is associated with the progressive changes involved in the extensive remodeling processes that take place as a bone enlarges in overall size. Also, bone tissues laid down during the early postnatal periods of skeletal growth reflect the very rapid nature of general body growth. As maturity is approached and overall growth begins to slow, however, corresponding changes in the character of bone deposits occur. Thus, successive layers of contrasting bone tissue types accumulate in the cortex as a result of varying growth rates at different periods in each part of an individual bone.
CELLULAR AND NONCELLULAR BONE. Bone in the sizable, diverse family of teleost fishes is distinctive in structure because bone cells in the adult tissue can be lacking (Enlow and Brown, 1956, 1958). This example is of interest because it provides an opportunity for metabolic studies of the bone matrix in relation to its cellular physiology (Moss, 1963). However, the life of an osteocyte in any species is limited, and in long-lived forms such as the human bone cells ordinarily undergo necrosis with age (Frost, 1960a and 1960b; Enlow, 1962b). This is particularly true in those areas of bone tissue in which vascular distribution is sparse (Fig. 12) or where it has been interrupted by the plugging of canals with mineral deposits (Enlow, 1966d). In these situations, bone that was previously cellular may become noncellular because of progressive necrocytosis.

Bone
However, internal processes of reconstruction involving Haversian replacement can provide a mechanism for cellular repopulation. Details of this process are outlined in later paragraphs.
Osteocytes are generally positioned so that their broad side directly faces an adjacent vascular canal, thereby providing maximum cell and canalicular exposure to the vessel. Because of the characteristic elongate and flat configuration of bone cells, differing planes of section in tissue preparations can be determined by the orientation of osteocytes (or lacunae).
VASCULAR AND NONVASCULAR BONE TISSUES.
The calcified matrix of bone is essentially impermeable, but it contains an anastomosing network of vascular canals and interlacunar canaliculi that provides transport pathways. Dentin is comparable with bone in a number of respects, but it is ordinarily nonvascular (except in the specialized forms of "vasodentin" and "osteodentin" in some vertebrate groups). The presence of canals in bone provides a basis for extensive internal reconstruction within the depths of the tissue itself, a process that is negligible in deeper portions of the avascular matrix in dentin.
Young rapidly growing bone typically contains a rich, dense system of vascular canals (Fig. 3) . The more rapid the growth, the denser and closer together the individual canals tend to be arranged. As growth slows, the number of canals in newly deposited bone similarly decreases. Some areas of older, very slow-growing bone can have relatively few canals or may be virtually nonvascular in character. Because of differential growth rates in the various parts of a bone, some areas may show dense vascularization while others have only a few canals. Stratified layers of bone each containing different numbers of vascular canals are also common, and are a result of remodel-
( 1 5 )
ing processes associated with changing intermittent rates of local growth.
As a bone increases in overall size, areas of bone deposited during former growth periods become progressively enclosed by new layers involving more recent growth circumstances, thereby resulting in a layering of mixed bone tissue types. Continued bone enlargement results in the eventual resorptive removal of older layers which were laid down during previous, relatively fast growth periods. These older regions become superseded by more recent zones of slower growing bone. In the adult skeleton, only scattered remnants of bone produced during very rapid growth periods of early youth still remain.
Well-defined zones or layers of cortical bone in the older human skeleton (as well as in most other large, long-lived species) are often nonvascular. In some groups, such as the lizards and snakes, periosteal bone deposits characteristically occur that are nonvascular throughout the entire cortical thickness in all parts of the bone.
LAMELLAR AND NONLAMELLAR BONE. A
basic structural difference between these common types of tissue is the manner of fiber arrangement in the intercellular matrix. As new bone is laid down, extracellular fibrils deposited by the osteoblasts become enclosed within ground substance. This tissue is termed osteoid and normally becomes mineralized almost immediately. If these fibrils are laid down as a series of circumferential sheets each with a differing fibril orientation, the bone has a resulting plywood-like, alternate grained, lamellar structure. Individual lamellae are characterized by a varying content of collagen and mineral (Rouiller, 1956).
If fiber deposition proceeds in a manner that does not involve layering with successively different fibril orientation, the resulting bone

( 1 6 )
tissue is nonlamellar in structure. Two principle types exist. One is termed "parallel-fibered" bone and is characterized by a matrix composed of relatively fine fibers, similar to those in lamellar bone, but which are all arranged in the same general plane without stratification. They are typically aligned in a manner that conforms to the long axis of the blood vessels enclosed by them.
The osteocytes and their lacunae within
Cartilage and bone
both lamellar and parallel-fibered bone are generally positioned in uniform, regular rows. Because of this, it is sometimes difficult to distinguish them in ground sections or in ordinary decalcified preparations. Polarized light or special staining methods (Smith, 1961) may be required in order to demonstrate the underlying character of the fibrous matrix.
The second major type of nonlamellar bone is termed "woven-fibered" or "coarsely bun-
The vascular canals present in this transverse middiaphyseal section of the cortex represent one of the most common types encountered in young postnatal bone. They are primary vascular canals and are oriented in a predominantly longitudinal
manner. Note that typical Haversian systems are not present. The cortex in this section is entirely periosteal in origin. Rhesus monkey femur, X 60. (From Enlow, D. H.: Principles of Bone Remodeling, Thomas, 1963.)
Figure 3

Bone
died" bone tissue. In this widespread variety of bone, the fibers are arranged in a coarse, irregular, reticulate mesh without layering. As it is laid down during bone formation, the woven-appearing fibrous matrix encloses formative bone cells in an irregular random fashion that contrasts with the uniform lines of cells in lamellar and parallel-fibered bone, a feature that permits its recognition in routine preparations. The matrix usually shows a slight basophilia in comparison with the eosinophilia that typifies lamellar bone.
Nonlamellar bone tissue, in both its parallel and woven-fibered forms, is characteristically associated with fast-forming cortical and cancellous bone. It is the standard type of bone found in many parts of the fetal skeleton and in rapidly growing, young postnatal bones. Nonlamellar bone also represents the type utilized in callus formation and in exostoses. Nonlamellar bone often occurs in the form of fine cancellous tissue, as described below.
Lamellar and nonlamellar bone tissues frequently appear in mixed combinations throughout the young skeleton as result of differential growth rates in various parts of each bone. Thus, alternate layers or zones can be found as different regions of a bone undergo variable growth processes during remodeling changes involved in overall skeletal growth. The cortex in epiphyseal regions of long bones, for example, as well as certain parts of the diaphysis, may be composed of nonlamellar bone. In contrast, other slower-growing areas of the shaft can be made entirely of lamellar bone. As a consequence of cortical relocation, however, the circumstances of growth become constantly changed so that these various deposits in different parts of the bone subsequently become covered by other bone types, thereby producing stratification in the cortex. Similar patterns are found in all the irregular bones of the skull.
( 1 7 )
LAMINAR BONE. A number of poikilo-thermic forms, such as the turtle and the croco-dilians, undergo cyclic periods of body growth as a response to seasonal (climatic) and related metabolic changes. The compact bone of the cortex is marked by circumferential bands or laminae somewhat comparable with seasonal rings in woody dicots. During periods of active body growth, the cortex becomes enlarged by the periosteal additions of peripheral layers of new bone, usually of a rapidly growing type. In turn, during those seasonal periods involving a lesser rate of body growth, zones of slower growing bone are laid down. If hibernation or other intervals occur during which growth does not take place, an almost total lack of deposition results and a basophilic resting (cement) line is produced. The composite of these factors produces a distinctive cortex that is thus banded or laminated* in structure.
PRIMARY VASCULAR BONE. If a "standard" or a "typical" kind of bone tissue could be considered to exist, primary vascular bone would by far be the most representative (Fig. 3) . It is the most widely distributed and frequently encountered of all various types of bone tissue in the human skeleton as well as in most other species of all vertebrate classes. The well-known Haversian system has traditionally been singled out as the typical structural unit of bone. This is because of the customary use of aged human bone tissues in slide preparations for teaching purposes, or the use of bone from other species specially selected because they show a similar type of histologic structure. In such bone, Haversian systems are abundant.
* The term laminar hone has sometimes been misused to denote a special bone tissue type found characteristically in bovines and some other mammals. This should be avoided because of prior usage with a different meaning.

( 1 8 )
The early textbooks of histology emphasized the Haversian type of tissue structure, probably for similar reasons, and recent texts have followed suit. However, human bone at the younger age levels is composed largely of bone tissue types in which Haversian systems are much less prevalent. The osteon is not to be considered a principal or universal unit of bone tissue structure in the child's skeleton.
Two general classes of canals exist in bone —primary and secondary (compare Figure 12a with Figure 12b). The bone enclosing each of these canal types is correspondingly termed either primary or secondary bone tissue. A primary canal is one that becomes enclosed directly within newly formed bone during deposition beneath the periosteum (or endosteum). The periosteum is a vascular membrane arranged into an outer layer composed largely of dense, irregular connective tissue and an inner, predominantly cellular zone containing an innermost osteoblastic layer. As new bone is laid down, the inner vessels of the periosteum become gradually enclosed by the formative mineralizing matrix. This produces a progressively expanding, anastomosing network of vascular canals that ramifies throughout the enlarging cortex. The vessels are continuous with those still in the periosteum, as well as with the vessels of the medulla. The periosteum itself, with its blood vessels, is also growing and moving in advance of the enlarging bone. Note that blood vessels, with their enclosing primary canals, become directly incorporated into the forming bone as deposition progresses. They do not enter by a process of erosive, resorptive penetration into the existing cortex from the periosteum.
Enclosed vessels within primary canals thus represent inclusions that accompany the continued formation of surface bone. In contrast, a secondary canal is the product of an internal remodeling process within the cortex of the
Cartilage and bone
bone which secondarily alters the structure of already existing primary canals. The reconstruction process involves a resorptive change in the size and configuration of the canal lumen. This is followed by redeposition of replacement (secondary) lamellar bone within the resulting erosion space (see Haversian bone, below).
An ordinary primary vascular canal can be readily recognized by the absence of concentric rings of Haversian lamellae surrounding it (Figs. 3, 12a, 33, and 34a). These canals may be variously oriented in longitudinal, radial, or circumferential planes. The most commonly seen pattern in periosteal deposits, however, involves a course that is generally parallel to the long axis of the bone. This is a result of the predominantly longitudinal manner of blood vessel arrangement within the osteogenic portion of the periosteum. Radially oriented primary canals are frequently present in endosteal circumferential layers, presumably because of a lack of linear stresses within the endosteal soft tissues and component vessels associated with the deposition of new bone on medullary surfaces. Such perpendicularly oriented canals, often termed Volkmann's canals, are less frequently encountered on the periosteal side of the cortex. Periosteal vessels typically enter at a much more acute angle.
It is emphasized that primary vascular (non-Haversian) canals represent the most widely distributed kind of canal system in bone. They are found in all vertebrate forms except those having totally nonvascular bone tissues. The primary canal is by far the most representative type at age levels involving active growth. Furthermore, it represents virtually the only canal type, regardless of age level, in a large number of vertebrate forms. It is the standard canal in human hone throughout the years of postnatal growth. Only when skeletal maturity is approached does extensive replacement by

( 1 9 )
changes and cortical movements that are involved in growth and remodeling. Compact cortical bone can become altered to cancellous medullary bone tissue in two ways. First, the relatively small canals that characterize the compacta can become progressively enlarged toward the inner part of the cortex by a process of resorptive removal from the lining surface of their walls. In this manner, the porosity of the bone increases as the medulla is approached, and a transition zone between the two can be seen. The trabeculae thus are composed of remnants of periosteal bone originally deposited at an earlier growth stage by the periosteum but which became remodeled by the activity of the endosteum. The conversion process occurs as this part of the cortex becomes located toward the inner portion of the bone as a consequence of the continued outward drift of the entire cortical plate. Subsequent reconstruction of the resulting cancellous bone continues in association with the activity of the endosteum.
Cancellous bone also forms in medullary areas following a total, abrupt removal of periosteal bone on the endosteal side of the cortex with subsequent replacement by endosteal trabeculae. This is the more common mechanism of cancellous formation in most human bones. Continued remodeling produces the variety of characteristic trajectorial patterns found in the different parts of individual bones. Constant alterations maintain these patterns as the bone increases in size and as the cancellous trabeculae become adjusted to new locations as a result of changing dimensions in the whole bone.
Cancellous medullary bone also becomes converted into compact cortical bone during certain growth changes. This common, widespread occurrence is described in further detail under Compacted cancellous bone in a later section.
Bone
secondary canals become predominant in periosteal bone deposits, a progressive process which involves many years. Even in the aged human skeleton, primary canals are still to be found in some yet unchanged parts of the various bones. It has been noted that limited numbers of secondary (Haversian) canals are present in young, growing bone, but their distribution is restricted to certain specific and predictable locations. These will be outlined in a following section.
COARSE CANCELLOUS BONE. Most bones are composed of an outer cortex and an inner medulla. The cortex is made of bone which has a relatively compact texture, and it is thereby termed the compacta. The medulla, on the other hand, typically contains a much more porous kind of bone that encloses variable amounts of reticular connective tissue, hematopoietic elements, and adipose. These medullary soft tissues are laced with a supporting framework of cylindrical or platelike bony trabeculae which have marrow spaces of variable size and configuration. The dimensions of these anastomosing spaces increase progressively in a direction toward the middle of the bone. A similar pattern is found in flat bones, and the terms external and internal lamina and diploe are used to denote their cortical layers and enclosed spongy bone.
Because this type of bone is characterized by a coarsely porous texture, it is described as coarse cancellous, in contrast to the fine cancellous type described in the next section. It occurs primarily in the medulla and is formed bv the activity of the endosteal membrane. Progressive remodeling changes occurring in coarse cancellous bone are also brought about by the thin endosteal lining.
A direct conversion in bone structure from cortex to medulla, and conversely from medulla to cortex, takes place during the complex


( 2 1 )
rectly on the cortical surface as fine cancellous trabeculae, and it is typically nonlamellar in structure (Fig. 4a). In those areas involving endosteal bone formation on the inner sides of the cortex, the same kind of tissue can be deposited. Endochondral bone produced during epiphyseal growth is medullary in location and is also fine cancellous in character. Also, callus formation and exostoses are composed of fine cancellous bone tissue. In medullary regions where coarse cancellous bone is developing, a direct conversion from a fine to a coarse type structure occurs by a process of resorptive remodeling.
Fine cancellous bone, wherever present in the skeleton, is a characteristic product of rapid bone deposition, in contrast to the slower forming lamellar compact bone. It is a bone tissue type that provides a large amount of new bone in relatively short periods of time. Thus, during increments of very fast skeletal growth, as in the early postnatal phase, this particular kind of bone is regularly formed. At any subsequent period during growth, those regional parts of a bone that grow in a differentially rapid manner are characterized by fine cancellous bone deposits. Other bone types are found,
Bone
FINE CANCELLOUS BONE. There is another basic and extensively distributed variety of bone that in comparison has a less porous nature than the coarse cancellous tissue described above. It is relatively more spongy in density, however, than ordinary compact bone tissue. This type is intermediate in porosity between the two and is termed fine cancellous bone (Fig. 17d). Cortical bone in the fetal and early postnatal skeleton is characteristically composed of this bone tissue type. Compact bone is not extensively distributed in the prenatal cortex, and in most areas it is not present at all.
Reticular or young collagenous connective tissue typically occupies the relatively small cancelli rather than the red or yellow marrow found in coarse cancellous bone. Unlike coarse cancellous trabeculae, fine cancellous bone occurs in both the cortex and medulla, and it can be formed directly by either periosteal or endosteal deposition. Transitions between fine cancellous bone to and from compact bone commonly take place, and reciprocal conversions between cortex and medulla involving this tissue variety are frequent.
This common bone type is laid down di-
Figure 4a. A peripheral layer of fine cancellous bone has been laid down by subperiosteal deposition. This type of nonlamellar bone is widely distributed in the fetal and early postnatal skeleton and is typically found in those areas of the bone that involve rapid growth. Neonatal Rhesus monkey femur, X 75. (From Enlow, D. H.: Am. J. Anat., 1962a.)
Figure 4b. Following compaction of fine cancellous bone, primary (not secondary) osteons are formed, as in this section of cortical bone. The original fine cancellous trabeculae are located between the osteons. Subsequent growth processes
will involve the deposition of new inner and outer cortical zones composed of different tissue types. Neonatal Rhesus monkey, X 75. (From Enlow, D. H.: Am. ]. Anat., 1962a.)
Figure 4c. This section is composed entirely of endosteal bone tissues produced by coarse cancellous compaction and the deposition of inner circumferential lamellae. Periosteal surface A is resorptive, and endosteal side B is depository. Note the typically radial orientation of the primary vascular canals, in contrast to the predominantly longitudinal arrangement found in periosteal deposits. Human frontal bone, X 100.
Figure 4

( 2 2 )
however, in the slower growing areas of the same bone. When this bone tissue variety is encountered in microscopic preparations, it provides an indication of the past nature of growth in that particular region at the specific time of its formation, although the zone may since have become covered by other bone tissue types as changing growth circumstances followed in the same area.
THE PRIMARY OSTEON. The term osteon (or osteone) denotes an elongated cylinder of bone surrounding a central canal (see Enlow, 1963b, for an historic account). Two basic types of osteons are encountered, the primary and the secondary. Secondary osteons are familiarly known as Haversian systems, and the term osteon itself, unless designated as primary, ordinarily refers to this structure. Although extensively distributed in the young growing skeleton of most species, the primary osteon is not mentioned in most standard texts and has not been emphasized to beginning students. However, this structure represents an important and significant component of bone tissue well known to more advanced workers in the field.
The primary osteon is considered "primary" because it does not form as a secondary product of internal reconstruction involving resorptive remodeling. It forms instead by a process of bone deposition within the existing spaces of already formed, fine cancellous bone. This bone type is composed of nonlamellar (woven-fibered) trabeculae enclosing a variable, but often longitudinal, system of relatively small, cylindrical spaces (Fig. 4a). Bone deposition within these spaces results in a direct conversion from fine cancellous to compact bone, and it produces a series of anastomosing bony cylinders containing a central canal that approximates the dimensions of most other canal types in compact bone (Fig. 4b). The whole
Cartilage and hone
bony cylinders are necessarily small in comparison with typical Haversian systems, because they are formed within fine cancellous bone having original spaces of relatively narrow diameter. The osteon itself may be composed either of lamellar or parallel-fibered, non-lamellar bone. The original woven-fibered, fine cancellous trabeculae are retained between the individual osteons as interstitial bone. These two bone types are thus in close association and are easily distinguishable in routine sections (Fig. 5). In contrast to Haversian system formation, a prior stage of bone removal is not involved in the erosive enlargement of a resorptive space within which the osteon is formed. Reversal lines thus do not encircle the anastomosing cylinders of the primary osteons. If a lag in deposition occurs following the initial formation of fine cancellous bone, however, each osteon may be enclosed by a similar-appearing basophilic resting line.
As mentioned before, the fetal cortex is composed largely of fine cancellous bone tissue. Some time shortly before or after birth, many of these spaces become filled, thereby forming primary osteons. The original cancellous cortex thus becomes converted into a compacta. It has sometimes been erroneously assumed that these neonatal or early postnatal primary osteons become permanently established in the cortex and remain there to represent the Haversian systems found in adult bone. But this is not possible, of course, because the primary osteon is not the same actual structure as a secondary Haversian system. Furthermore, the bone of a young individual is not present in the adult skeleton, because it becomes removed as new deposits are laid down to bring about an increase in the size of each whole bone.
The primary osteon is a product of rapid growth, just as its components, woven-fibered and parallel-fibered bone, represent a response to relatively fast skeletal growth. Like all bone

Bone
types formed during such growth, the bone is densely vascular. Primary osteons are characteristically found in the very young skeleton during a period that represents rapid enlargement of the body as a whole. This kind of bone is not a feature of the mature, adult human skeleton, although it is abundant in the adult bones of fast-growing, short-lived forms such as the rabbit.
Primary osteons (and fine cancellous bone) thus provide relatively large amounts of new bone in short periods of time. An entire cortex may be composed of this tissue; or, because of intermittent growth spurts in different parts
( 2 3 )
of any individual bone as a consequence of remodeling processes, the cortex may become a layered accumulation of this bone type along with different kinds that enclose it. A single layer of primary osteons within other zones of lamellar bone is a common observation in the young skeleton (Fig. 5). In this situation, a subperiosteal band of fine cancellous trabeculae is laid down on the outer surface of a cortex composed of lamellar bone. This is related to a transient growth acceleration in this particular region of the bone. The row of fine cancellous spaces almost immediately receives deposits of parallel-fibered bone, thereby producing a cir-
A narrow zone of primary osteons is enclosed by other layers containing ordinary primary vascular canals. These osteons were formed within the trabeculae of original nonlamellar, fine can
cellous bone that subsequently underwent compaction. The nonlamellar (woven) bone can be seen surrounding each osteon. X 200.
Figure 5

( 24 )
cumferential zone of primary osteons. Subsequent deposition of a slower-growing bone type (lamellar bone) then covers this layer, which becomes progressively more deeply buried within the cortex.
PLEXIFORM BONE. Plexiform bone is a type of tissue that is a variation of compact bone structure similar in basic plan of construction to cortical tissue composed of primary osteons. It is formed by a process of lamellar
Cartilage and bone
compaction within the spaces of nonlamellar, fine cancellous bone. The primary osteon, as noted previously, is most commonly oriented in a predominantly longitudinal fashion. Plexiform bone, however, is laid down in such a manner that a three-dimensional plexus of radial, longitudinal, and circumferential canals is formed (Figs. 6 and 7). This canal system is characterized by its strikingly uniform, regular, and symmetrical arrangement, and it is readily recognizable wherever encountered in micro-
Plexiform bone. This bone tissue type is laid down in a manner comparable to the formation of primary osteons. It develops by the compaction
of uniformly arranged, fine cancellous trabeculae. Dog femur, X 75. (From Enlow, D. H.: Principles of Bone Remodeling, Thomas, 1963.)
Figure 6

Bone
scopic preparations. Plexiform bone, like the primary osteon, is a product of rapid skeletal growth, and it represents an adaptive response associated with massive bone formation. This bone type is commonly found in a number of species that have a large and thick-boned skeleton, such as the elephant (and some of the dinosaurs). Plexiform bone also characterizes the skeleton of many medium to large forms that have fast bone growth, including most artiodactyls (the deer, hog, sheep, bovine, etc.) and some carnivores, as in larger dogs. It is found in young human bone with enough frequency to warrant consideration, although not to the extent present in those species just mentioned. Plexiform bone develops more commonly by subperiosteal deposition, but it may also be formed by the endosteum.
PERIOSTEAL AND ENDOSTEAL BONE. Most parts of a bone are covered by a periosteum and lined with an endosteum. Except in regions of direct tendinous attachment, the periosteum is ordinarily a substantial, well-defined connective tissue membrane. Bone produced by its inner (osteogenic) layer is usually termed subperiosteal, or simply, periosteal bone. The endosteum is a much thinner membrane and may comprise little more than a single osteoblastic layer with a relatively small number of fine collagenous or reticular fibrils associated with it and with the blood vessels entering the inner surface of the cortex. Bone produced by this membrane is termed, in general, endosteal bone, and it develops on the endosteal (inner) side of the cortex as well as on the surfaces of cancellous trabeculae. Periosteal bone is formed only by intramembranous ossification, but endosteal bone can be produced by endochondral as well as by intramembranous formation. During inactive growth periods, an endosteal lining as such is often difficult to distinguish.
( 2 5 )
It is commonly, but mistakenly, assumed that most of the compact (cortical) bone tissue in the skeleton is largely of periosteal origin. It will be shown in following chapters that endosteal bone has an overall distribution that is quite extensive. It can, in fact, represent the predominant bone type in many skeletal elements and may exceed the total volume of periosteal bone present. In some parts of almost any bone, the entire thickness of the cortex can be composed of endosteal bone tissue. In many other parts, the cortex may contain one or more zones of endosteal origin.
THE SURFACE TEMPLATE. Because of the hard calcified nature of its matrix, bone is a tissue in which all new growth activity, involving both resorption and deposition, must necessarily proceed on existing, exposed surfaces. Except at the molecular level, interstitial growth changes deep to a surface are not possible in ordinary bone. As an existing surface becomes covered with additional bone deposits, a new surface is thereby formed. Any point in the compacta, however deep, at one time represented an actual exposed surface, either on the inner or outer side of the cortical plate (Fig. 15).
Two general classes of bone surfaces exist— periosteal and endosteal. The latter occurs on the inner side of the cortex as well as within vascular canals, resorption spaces, and cancelli. In addition, other surfaces are present within lacunae and canaliculi. It is apparent that new bone deposits must initially follow and conform to the contour and configuration of the particular surface upon which they are laid down. Because of this, the nature and disposition of this surface contribute directly to the character and the structure of the new bony layer. This was encountered previously in the formation of the primary osteon, for example, in which cylinders of new bone were formed


Bone
within the tubular spaces of fine cancellous bone. The role of the surface template in determining the structural pattern of bone deposits will also be seen in the following bone types.
COMPACTED, COARSE CANCELLOUS BONE.
During growth and remodeling, direct conversion of medullary, coarse cancellous bone tissue to compact, cortical bone frequently occurs as a result of the inward growth of the cortex (see Chapter 3). This conversion is brought about by the deposition of new lamellar bone within the large, irregular spaces of cancellous bone. Endosteal bone is laid down on the older surfaces of the trabeculae, and deposition continues until original cancellous spaces have each become reduced to a diameter approximating most other cortical canal types. The result is a direct change in tissue type from spongy to compact and, further, a change in relative location from medulla to cortex as the entire cortical plate grows and moves in an inward, endosteal direction. The outer, periosteal surface of the cortex is, correspondingly, resorptive in nature (Fig. 8) .
Compacted, coarse cancellous bone can be readily identified in microscopic sections (Figs. 9, 10, and 11). The contours of the old trabeculae are recognizable, and because the original configuration of these trabeculae follows an irregular, convoluted pattern, the compact bone produced by continued new deposits on their surfaces necessarily conforms to the same orientation. It is apparent that this
( 2 7 )
growth process follows the principle of the "surface template" described above. The compact bone produced by the process of cancellous compaction has a characteristic whorled, irregular appearance which corresponds directly to the template established by the original convolutions of the old cancellous bone. This type of tissue may be termed "convoluted" bone. It is primarily a product of endosteal formation since coarse cancellous bone is produced within the medulla by endosteal activity and is covered by the endosteal membrane. Convoluted bone is not formed by periosteal growth.
This variety of bone may eventually become partially or almost totally replaced by secondary Haversian systems in the more aged human skeleton. It is noted that the whorls and convolutions of the bone do not themselves represent osteons. Because convoluted bone is formed by a process of deposition within existing (but irregular) spaces, the sequence of formation is somewhat comparable with Haversian system formation. This factor has often led to the mistaken identification of such convoluted, compacted cancellous bone as typical Haversian tissue. This error is to be avoided because, as will be seen, proper recognition is basic to accurate reconstructions of past growth and remodeling changes. Wherever this bone type is encountered in tissue preparations, it provides reliable indication of a former endosteal growth stage that involved a direct, inward growth movement of the cortical plate.
These sections demonstrate the uniform symmetrical nature of the vascular network that characterizes plexiform bone tissue. Note the three-dimensional plexus of longitudinal, radial, and circumferential primary canals. A number of re
sorption spaces are also present, and the deposition of new replacement bone within these enlarged canals will produce a series of secondary osteons. Bos, X 100 (top) and X 50 (bottom').
Figure 7

Cartilage and bone ( 2 8 )
It is paradoxical that the cortex in some parts of a growing bone must move in an inward direction (A and B) in order that the bone as a whole can increase in size. As the cortical plate drifts in an endosteal manner by periosteal resorption and endosteal deposition, two basic kinds of bone tissue are produced. In some areas, inward growth proceeds into areas ( I ) already occupied by cancellous trabeculae, which results in a direct
conversion of medullary cancellous bone into cortical compact bone tissue (convoluted bone, indicated at Y) . In other regions the cortex moves inward into medullary regions ( 2 ) that did not contain spongy bone, which produces a layer of uninterrupted, endosteal circumferential bone ( X ) . (From Enlow, D. H. : Principles of Bone Remodeling, Thomas, 1963.)
Figure 8

Bone
Convoluted bone is quite extensively distributed in most bones. It can occupy two thirds or more of the total cortical volume in a whole bone. Convoluted bone tissue and the various types of primary vascular bone represent the predominant kinds of bone tissues in the young, growing, postnatal human skeleton. Curiously, neither of these basic types of bone are included in elementary text descriptions of bone tissue, even though they represent the
( 2 9 )
standard structure of human bone through early maturity. To advanced workers dealing with skeletal growth, positive recognition of both types, as well as an understanding of their modes of formation, is essential.
INNER AND OUTER CIRCUMFERENTIAL BONE.
If existing periosteal or endosteal surfaces of the cortex in any part of a bone are relatively smooth and evenly contoured, subsequently
The bone tissue that comprises this cortical plate is entirely of endosteal origin. It was formed during the inward movement of the cortex by endosteal deposition and periosteal resorption. Note the irregular convoluted character of the
bone, a pattern determined by the original trabecular template of the coarse cancellous bone prior to compaction. X 100. (From Enlow, D. H.: Principles of Bone Remodeling, Thomas, 1963.)
Figure 9

( 3 0 )
formed layers of lamellar bone follow this template and result in the formation of inner or outer zones of uninterrupted sheets of circumferential lamellae (Figs. 4c, 8, 11b, and 34). On the endosteal side of a cortical plate, directly continuous coarse cancellous trabeculae can be extensive, relatively sparse, or virtually absent, depending on the part of the bone involved. If endosteal deposition proceeds into
Cartilage and bone
medullary regions already occupied by trabeculae, the resulting compact bone is convoluted in nature. If the endosteal surface template is smooth and even, however, and contiguous trabeculae are lacking or are widely spaced (as in the middle of a long bone diaphy-sis), the resulting compact bone is in the form of a well-defined layer of inner circumferential lamellae.
This cortex is composed of convoluted endosteal bone tissue. The contours of the old cancellous trabeculae can be distinguished. The periosteal side of the cortex was resorptive and the endosteal surface was depository in nature. The entire cortex was drifting in an endosteal
direction. The process of cancellous compaction resulted in a direct conversion of medullary spongy bone into compact cortical bone tissue. X 80. (From Enlow, D. H.: Am. J. Anat., 1962a.)
Figure 10

Bone
HAVERSIAN BONE. The Haversian system
is secondary in nature. It is formed by a process of internal cortical reconstruction involving the removal of some pre-existing compact bone. This is followed by the addition of new, replacement bone tissue within the space thus formed. It is a secondarily superimposed structure that functions to replace some of the original primary bone or areas of previously formed secondary bone. For this reason, the Haversian system (secondary osteon) may also be termed, appropriately, a "replacement" osteon (Lacroix, 1960).
The initial step leading to the formation of a secondary osteon is the resorptive enlargement of a canal already present within the cortex. This results in a resorption space (Figs. 13& and 14). The original canal that undergoes this conversion process can be virtually any canal type, including the various primary canals, central canals located within primary osteons, canals in plexiform bone, canals within endosteal convoluted bone tissue, or old secondary Haversian canals that have previously undergone this reconstruction sequence and once again repeat the process to form second, third, or fourth generations of Haversian systems.
The final diameter of the resorption space determines the width of the osteon to be formed within it. Because a direct reversal occurs following the initial resorptive phase, the outermost layer of the formative Haversian cylinder is separated from the lining surface of the resorption space by a thin, basophilic reversal (cement) line. The progressive deposition of the concentric Haversian lamellae begins at the periphery of the enlarged tubular space and then proceeds, one lamella within another, toward the center. At completion, the resulting central canal has approximately the same diameter as the precursory canal prior to reconstruction (Figs. 12b and 14). During
( 3 1 )
the process, the resorption space itself is occupied by a loose, immature connective tissue containing two or three small vascular elements, a brief network of young collagenous and reticular fibrils, ground substance, and a scattering of various cell types, including undifferentiated perivascular cells. The cells lining the inner surface of the canal are osteoclasts during the resorptive phase (Fig. 132b) and osteoblasts during the depository phase. Both are derived from perivascular stem cells. The resorptive phase proceeds very quickly so that resorption canals encountered in routine preparations are usually of maximum diameter. They may remain at this stage for prolonged periods or may immediately become reduced to a Haversian canal by internal bone deposition. Note that Haversian deposition begins at the periphery of the resorption space and proceeds in a direction toward the center. An erroneous assumption sometimes held is that lamellar formation begins near the center to form the innermost layer adjacent to the central canal and then continues peripherally until final Haversian system diameter is reached. Another mistaken belief still encountered is that large, adult Haversian systems grow directly in size from small immature ones by a process of interstitial distention.
The process of secondary Haversian formation represents a mechanism of internal remodeling and reconstruction, and it takes place within existing cortical bone deep to the periosteal and endosteal surfaces. The gross morphology and the external contours of the whole bone with all of its parts, however, are not disturbed throughout this rebuilding process.
Secondary Haversian systems can be readily distinguished from primary osteons. The latter are relatively small structures whereas the secondary osteons are typically much larger, although their overall diameter is quite variable.


Bone
Interstitial regions between primary osteons are composed of woven-fibered bone; those between secondary osteons are usually composed of lamellar bone, particularly in the older skeleton. The interstitial bone associated with either of these osteon types can be of endosteal or periosteal origin. Secondary osteons are surrounded by a reversal line. The primary osteon lacks this structure, although an enclosing resting line may sometimes be present. The placement of the secondary osteon is such that it abruptly and noticeably interrupts the bone surrounding it, because it forms as a replacement structure within bone already present. In Figures 12b and 14, note the discontinuity between the Haversian cylinders and the interstitial remnants interposed between them.
The nature of the distribution of secondary osteons in cortical bone is characteristic and predictable (Enlow, 1962b), and two basic relationships exist. First, secondary osteons are a much more common structural feature in the older human skeleton. Haversian systems are present in young bone but are largely restricted to the circumstances described later. Only within the mature adult skeleton do secondary osteons show a generalized, widespread replacement of the original, younger bone laid down in the growing cortex. The process is progressive and cumulative (Amprino and Bairati, 1936). It is known that osteocytes
( 3 3 )
undergo death with increasing age (Frost, 1960a; Enlow, 1962b). Cell longevity in any part of a bone is associated with the relative extent of vascularity in that region (Enlow, 1966d). Nonvascular zones and areas that have only a sparse distribution of canals are the first to experience the normal process of cellular necrosis. This situation conforms to the "tissue cylinder" concept of Krogh, in which a central blood vessel is responsible for the sustenance of a functional cylinder of tissue surrounding it. In Figure 12a, note that a distinct cylinder of living osteocytes encircles the centrally placed canal. Beyond the limits of this cylinder, however, the cells have not survived. A critical cell-to-capillary distance is involved, and if this is exceeded during growth cells become increasingly susceptible to necrosis. Local regions in the cortex that have become deprived of vascular supply as a result of mineral occlusion in canals similarly undergo osteocytic death.
In all areas involving extensive necrocytosis, an orderly process of internal replacement occurs in which older, necrotic regions become partially removed through the formation of resorption canals. Subsequent deposition of bone within these erosion spaces thereby provides a new generation of living bone within a remnant framework of older, necrotic bone. The result is an anastomosing series of secondary Haversian systems. The cells in inter-
Figure 11a. The endosteal compact bone tissue in this section is of a convoluted type produced by cancellous compaction. The template was provided by the former trabeculae of the medullary spongy bone prior to conversion to compact cortical bone tissue, X 100.
Figure 11b. This pattern of cortical zoning was produced during reduction of metaphyseal diameter. The inner layer of circumferential
Figure 11
lamellae (A) was formed in the metaphyseal-diaphyseal area of junction that did not contain contiguous cancellous trabeculae. Note the presence of radial primary vascular (Volkmann's) canals. The outer zone of endosteal bone has a resorptive periosteal surface (B), and it contains superimposed secondary osteons. Rhesus monkey humerus, X 100. (From Enlow, D. H.: Am. ]. Anat., 1962b.)


Bone
stitial bone located between them remain largely necrotic. It is apparent that the Haversian system itself represents a "tissue cylinder." Its outer boundary marks the limit of support provided by the central blood vessel.
In the younger skeleton, the regular formation and destruction of bone on inner and outer cortical surfaces during generalized, continued skeletal growth provide this same basic function so that regions in which cell longevity becomes exceeded are removed during the normal course of growth. When such growth subsides, however, the internal mechanism of Haversian reconstruction then becomes the key process involved. Furthermore, bone produced in the young, rapidly growing skeleton characteristically contains a rich distribution of vascular canals. This is associated directly with a greater longevity of cells, because the cell-to-canal distance is a critical factor involved in cell survival. As growth becomes slowed in the older skeleton, the distribution of vascular canals is generally decreased. This in turn is associated with an acceleration of bone cell necrosis and coincides with the onset of more extensive Haversian reconstruction.
Haversian replacement in more aged bone tissue further simultaneously provides an effective system that contributes to mineral homeostasis (Amprino, 1965). By means of secondary reconstruction, turnover of inorganic
( 3 5 )
components can take place in a matrix that has become characteristically less responsive to surface molecular exchange than in younger bone. The role of the Haversian system in cell replacement within older bone may also be involved, since a direct relationship between mineral homeostasis and cell function may exist.
The second fundamental relationship associated with the occurrence and distribution of secondary osteons occurs in the young bone of the growing skeleton, and it is essentially independent of aging, necrosis, regeneration, and the other factors described above. In this relationship, Haversian systems are specifically located within the cortex just deep to areas of muscle and tendon attachment (Figs. 14a and b). As a bone enlarges in size, contiguous structures attached to the bone must necessarily become relocated in order to retain their relative positions. This process is complicated by the fact that the outer bone surfaces in such regions are frequently resorptive in character. The formation of resorption spaces and the deposition of new bone within these spaces function to provide fibrous continuity between the bone deep to the resorptive surface and the soft tissue structures attached to the bone, which are becoming repositioned (see pages 94 and 100). Because of these factors, such Haversian systems are characteristically found
Figure 12a. Compare the canals in this section of periosteal cortex with those in Figure 12b below. These are primary vascular canals. The canals are surrounded by living osteocytes (the darkly stained nuclei can be seen). Note that cellular necrosis has taken place, however, in the remote intervascular regions between the canals. The lacunae in these areas are empty. Each canal represents the axis of a physiologic
"tissue cylinder." Rhesus monkey femur, X 100. Figure 12b. In contrast to the primary type
of vascular canals seen in Figure 12a, most of the canals in this cortical section are typical Haversian canals. Each is surrounded by a cylinder of Haversian (replacement) lamellae, and the entire structure is a secondary osteon (see primary osteons in Figure 5), X 100.
Figure 12


Bone
(1 ) in endosteal zones of the cortex which have formed as a result of periosteal resorption combined with endosteal deposition, particularly in regions of muscle attachment (Fig. 34), and (2 ) in cortical areas composed of periosteal bone associated with the remodeling of tuberosities, crests, tubercles, etc., to which muscles or tendons are anchored (Fig. 14).
The Haversian system thus is a multifunctional structure formed in response to any one of several factors which involves the removal of existing bone to form internal resorption canals and the subsequent deposition of new bone within these enlarged spaces. The secondary osteon represents a variable "utility" structure produced in association with the different circumstances that involve the internal reconstruction of the cortex.
SPECIAL VARIETIES OF BONE. A number of specialized bone types exist that are adapted to specific locations or circumstances within a single bone. Others are adapted to the skeleton in certain individual vertebrate groups (Enlow and Brown, 1956, 1957, 1958). In some fishes, for example, a unique "fibriform" bone is found containing massive bundles of parallel fibers. In other fishes (the garpike, Lepidosteus, and the fresh-water dogfish, Amia), a curious type of "lepidosteoid" bone occurs which contains numerous dentin-like tubules. In most higher vertebrates, tooth-bearing bone is often characterized by the presence of prominent attachment fibers continuous with the perio-
( 37 )
dontal membrane. This well-known bone type is termed bundle bone (see page 87). A special type of "chondroid" bone sometimes occurs along alveolar crests, and also at the apex of some tuberosities in long bones. This kind of tissue represents another variety of fast-growing, nonlamellar bone. Its name is derived from the cartilage-like appearance of the large, spheroid cells scattered in random fashion (Or-ban, 1957; Enlow, 1962a).
THE STRUCTURAL NATURE OF BONE. A re
view of the multitude of different bone tissue types demonstrates that single, inclusive definitions of bone structure and growth cannot be applied. The Haversian system, for example, has traditionally but erroneously been regarded as the basic unit of bone structure. Similarly, bone cells, vascular canals, lamellae, etc., have been assumed to represent standard constants of structure. The variable presence or absence and variations in the distribution of these components, however, preclude simplified generalizations. These complex factors should instead emphasize the marked lability and the dynamic adaptability of bone as a tissue to the many different circumstances involved in skeletal growth and physiology.
The growth of bone
The enlargement of a bone involves two closely interrelated processes: actual size in-
Figure 13a. The external (periosteal) surface of this cortex is resorptive. The convoluted type of endosteal bone has been partially replaced by secondary osteons. Note the characteristically scalloped and pitted character of the resorptive surface. Rhesus monkey femur, X 200.
Figure 13b. On a predominantly resorptive
external surface, this small isolated region shows a "spot" deposit of periosteal bone (A), which contributes to the continuous attachment of mus-cles during the growth process. Note the enlarged resorption space containing vessels and osteoclasts (B). Rhesus monkey femur, X 200.
Figure 13


Bone
crease and remodeling. Bone growth in general proceeds either by an intramembranous or an endochondral means. These two modes of osteogenesis are reviewed briefly below. Remodeling is a companion process that accompanies bone growth and functions to adjust the bone's shape and dimensions as it simultaneously increases in size (this will be described in Chapter 3) .
A bone does not enlarge in the same manner that soft tissues grow. Because bone is hard, the circumstances associated with its growth are distinctive and necessarily involve a number of specialized adaptations. The processes of growth, differentiation, and development are variously defined, but if the term growth is restricted essentially to an increase in size, soft tissues may be seen to grow by several combined processes. First, many tissues, such as the epithelia, enlarge by cellular proliferation. The total population of cells steadily increases as long as growth continues, and following this they continue to divide in order to produce replacement cells. Second, some soft tissues, such as muscle and cartilage, increase in size by the continued enlargement of their cells. Third, some soft tissues can grow by an
( 3 9 )
increase in the material located between the cells (its matrix). All three kinds of growth are interstitial in nature because they involve expansive changes in tissue components already present.
It is apparent that a bone cannot enlarge by any of the three growth methods just outlined. Its cells cannot divide and proliferate because they are encased by a hard, calcified matrix. (The osteoblasts on the surface of a bone undergo mitotic cell divisions. This is interstitial growth, but it occurs in the soft tissue covering and not within the hard part of the bone itself.) They cannot increase in size for the same reason. Similarly, the intercellular bone matrix cannot increase in actual volume once it becomes mineralized. Bone thus is incapable of interstitial growth and expansion because of its hardness. Other basic growth mechanisms are therefore utilized in the enlargement process of bone.
The significance of the bone surface was previously mentioned. It was pointed out that surfaces represent the sites of active change, and that several surface types exist in a bone, including the periosteal (outer) and the endosteal (inner) surfaces. Growth activity must
Figure 14a. Tubercle drift. This bony prominence was undergoing growth movement in a direction toward the left. An accumulation of new lamellae on the surface facing this direction has occurred. The opposite (right) side of the tubercle was resorptive. Note the presence of secondary osteons in the cortex of the tubercle, a characteristic feature in areas of muscle attachment. These Haversian systems are formed by a process of reconstruction from original primary vascular canals (as seen in the lower portion of the section). The osteons develop progressively in the same direction toward which the tubercle
Figure 14
is drifting. Cercopithecus, X 75. (From Enlow, D. H.: Am. J. Anat., 1962b.)
Figure 14b. Secondary osteons are characteristically formed in areas of muscle attachment. As seen in this section, they develop by a process of resorptive enlargement of existing primary canals (A), followed by lamellar deposition within these resorption spaces (B). Prior to skeletal maturity, the distribution of Haversian systems is restricted largely to such areas of attachment, particularly those involving a resorptive periosteal surface. X 75. (From Enlow, D. H.: Am. J. Anat., 1962b.)

Cartilage and bone
necessarily take place on these surface exposures, because the underlying bone itself is not capable of expansion. New additions onto surfaces represent the essential mechanism for increasing bone size. This type of growth is termed appositional, in contrast to interstitial expansion (Fig. 15). All bone that is truly calcified grows in such a manner, regardless of the particular mode of enlargement in that part of that bone (i.e., intramembranous, endochondral, sutural, etc.). Appositional growth is a process of surface addition of new bone, and it occurs on inner as well as outer surfaces of the bone. How a bone can actually grow in size by additions on inside surfaces will be explained in a later discussion.
The deposition of bone on a surface exposure represents one phase in a two-part growth mechanism. The second phase is resorptive removal, a process that is as basic and essential to overall enlargement as is deposition. Bone growth by addition alone, without the companion process of resorption, does not ordinarily occur. The two processes must necessarily take place in combination, and as bone is added onto one surface, it becomes cor-
Figure 15
The appositional nature of bone growth. Bone can grow only by a process of surface appositional deposition. In the two growth stages schematized here, the star represents an arbitrary fixed reference point. As subperiosteal bone is laid down by the osteogenic layer of the periosteum, this enclosing membrane itself grows in a corresponding peripheral direction. Some surface osteoblasts (A) in stage a have become deeply buried as osteocytes (A) in stage b. The periosteal blood vessel (B) in stage a has become enclosed within a canal (B) in stage b. Every point in the cortex was at one time an actual exposed surface, as indicated by the positions of the arrows in stages a and b.
( 4 0 )

Bone ( 4 1 )
A bone does not increase in size by simply-enlarging all existing contours ( a ) following a process of uniform bone deposition on all external surfaces ( b ) . In the growth of the mandible and maxilla from infant to adult ( c ) , such a process
of uniform accretion on all outer surfaces (as in d) does not occur. Note that the bones would become progressively more disproportionate. Instead, a complex process of remodeling takes place during the continued growth of bones.
Figure 16

( 4 2 )
respondingly and simultaneously removed from some contralateral surface. This brings about a proportionate, balanced increase in the dimensions of the cortical plate. It also produces an actual growth movement of the cortex, as well as shifts in cancellous trabeculae, in the various directions associated with the growth of the bone. Resorption, like deposition, occurs on the various bone surfaces, including the periosteal as well as the different endosteal surfaces.
It is a common misconception of skeletal growth that a bone increases in size by uniform, generalized deposition on virtually all outer surfaces with corresponding generalized resorption from inside surfaces (Fig. 16). The whole bone presumably enlarges by a constant expansion of the existing surface contours. It cannot be emphasized too strongly that this notion is oversimplified and inaccurate and serves to obscure the real growth processes that actually take place. This particular point will be discussed in greater detail in the following chapter.
CENTERS OF OSSIFICATION. Bone ordinarily develops within connective tissue. This parent tissue provides the source of stem cells that subsequently differentiate into osteoblasts, which in turn bring about actual bone formation. The connective tissues also provide the blood vessels that later become established as a component part of the bone. Furthermore, connective tissue constitutes the enclosing membranes that represent the pathway into and from the bone for vessels, nerves, and lymphatics.
The onset of osteogenesis within connective tissue occurs in established locations termed ossification centers. A primary center of ossification is the first to appear, and this may be followed at a later time by one or more secondary centers. The appearance of the latter
Cartilage and bone
occurs in a regular sequence throughout the skeleton, usually after birth. In a typical long bone, the original primary center is responsible for the beginning formation of the shaft (dia-physis), and the secondary centers are associated with the epiphyses. The diaphysis and the epiphyses are typically separated by epiphyseal plates of cartilage during active skeletal growth (Fig. 18). The bone of most primary and secondary centers eventually coalesces and becomes merged into a single bony element. Similarly, primary centers of phylo-genetically separate bones can become fused to form a single composite bone, as in some components of the cranial base.
INTRAMEMBRANOUS OSSIFICATION. The
first visible change that marks the beginning of bone formation within a connective tissue membrane is a clustering of undifferentiated cells at the formative primary center (Fig. 17a). Between these cells, the initial appearance of bone matrix occurs in the form of osteoid (fibrils and ground substance), which subsequently becomes mineralized. The result is a slender spicule of bone covered on its surface by the same cells that just formed it. These cells represent the first osteoblasts. The process spreads throughout the region of the primary center and thereby brings about the formation of a three-dimensional mesh of delicate bony trabeculae. The spaces between the spicules are occupied by a young, vascular connective tissue. Continued activity by the covering sheet of osteoblasts results in a progressive enlargement of each of the bony trabeculae by appositional deposition on their surfaces. As osteoid matrix is laid down, it is almost immediately calcified. Some of the bone-producing cells become enclosed by their own deposits and are thereby established within bone as osteocytes. Very short cytoplasmic processes extend between adjacent osteoblasts, and

Bone
as cells separate to become fixed within the forming bone, these processes are drawn in length. Bone deposition around the cell processes results in the formation of canaliculi. An elaborate, delicate system of passageways is thereby included in the new bone matrix. The cytoplasmic processes may later become withdrawn, but the spaces that house them remain to provide extensive access channels from cell to cell and from blood vessel to cell. Each osteocyte thus becomes isolated in its own compartment, the lacuna, but intercommunication through the impermeable matrix is nevertheless maintained.
The mesh of bony trabeculae produced by this process is composed of nonlamellar bone. It is characteristically fine cancellous in character, both in cortical and medullary areas (Figs. 17c and d) . As bone formation continues, the enlarging primary center becomes regionally differentiated into the enclosing cortices and a middle zone that becomes progressively coarser (the diploe of flat membrane bones). This process involves continued resorp-tive enlargement of the original fine cancellous medullary spaces.
As these growth changes take place, the connective tissue surrounding the entire area undergoes differentiation to form an enclosing vascular periosteum. This membrane becomes arranged into an outer zone (the fibrous layer) composed largely of dense, coarse, collagenous fibers with scattered fibroblasts, vessels, and nerves. The inner zone develops into a much looser layer containing many cells interspersed between more slender collagenous fibrils and fibers. Vessels pass from this layer into and from the surface of the bone. The innermost part during active periods of growth is composed of a sheet of osteoblasts (or osteoclasts) that provides the osteogenic function of the periosteum. Continued bone growth by the periosteum proceeds in conjunction with other
( 4 3 )
growth activities occurring in different parts of the bone, as in the sutures and synchondroses.
The osteogenic layer of the periosteum becomes dormant during periods of growth quiescence, but it may differentiate into a functional, bone-producing zone during subsequent intervals of growth or remodeling activity, regardless of age.
Bone laid down by the periosteum is intra-membranous in nature, because it develops within a connective tissue membrane. If this process of subperiosteal bone formation takes place around an area involving cartilage, it is sometimes designated as perichondral bone. The sequence of its formation is the same.
As subperiosteal bone is formed, the surface-covering osteoblasts produce new, immature collagenous fibrils which are continuous with the fibers already embedded within the bone matrix. These new fibrils also become continuous with the older fibers of the periosteum as the periosteum itself grows and moves in an outward direction. Linkage is maintained so that the growing bone and the moving periosteum remain bridged by direct fibrous bonding (see page 99). As new fibers are formed by the osteogenic layer, ground substance is also produced and deposited between them. This matrix almost simultaneously undergoes mineralization. Some, but not all, of the cells within the osteogenic zone become fixed in the formative bone as osteocytes, and their lacunae are interconnected by canaliculi as bone is laid down around the lengthening cytoplasmic extensions of each cell.
The bone thus grows exclusively by apposi-tional surface deposition. In the fetus, as well as in many parts of the young growing postnatal skeleton, subperiosteal deposits are composed of fine cancellous trabeculae. In the cortex, postnatal fine cancellous bone becomes compacted soon after it is formed to produce

Cartilage and bone ( 4 4 )

Bone
primary osteons. Just as cells become enclosed within forming matrix, the vessels and their connective tissue sheaths are also incorporated into the enlarging cortex as the periosteum lays down new bone around them (Fig. 4a). These vessels become located within the forming spaces between fine cancellous trabeculae. In the somewhat older skeleton, primary vascular canals rather than fine cancelli are formed as vessels become enclosed in surface deposits (Fig. 15). Also, with increasing age bone is laid down in the form of lamellar sheets rather than as fine trabeculae, and the number of canals included in new bone deposits progressively decreases as growth slows.
All inner surfaces of a bone are lined by an endosteal membrane. Unlike the dense, substantial periosteum, this brief layer does not function in strong anchorage and attachment. It is composed essentially of an osteoblastic or osteoclastic layer and a very sparse amount of connective tissue associated largely with the vessels passing into the cortex. The surface covering of cells is prominent during active periods of growth. The osteogenic potential of
( 4 5 )
the endosteum is marked, and this thin membrane forms the dense collagenous matrix of new bone as readily as does the much thicker periosteum. Bone produced by the endosteum is termed endosteal bone tissue, and, in contrast to periosteal bone, it may be produced by either intramembranous or endochondral ossification because the endosteal membrane is also involved in bone deposition within the erosion spaces of cartilage.
ENDOCHONDRAL (INTRACARTDLAGINOUS ) OS
SIFICATION. The developmental sequence involved in the initial replacement of cartilage by bone, and the subsequent growth of the entire cartilage and bone complex, is reviewed in Figures 18, 19, and 20. The "bone" begins as a cartilaginous anlage surrounded by its perichondrium except at the ends. Compare this initial cartilage model, as in Figure 18a, with the later organ, as pictured in Figure 18c. Note that two remaining counterparts of the cartilage model are still represented: the articular cartilage and the epiphyseal plate. Prior to the appearance of a secondary center, the
Intramembranous bone formation. In a center of ossification (a), the cells and matrix of the undifferentiated connective tissue (late mesenchyme) undergo a series of changes that produce small spicules of bone. Some cells (1) remain relatively undifferentiated, but others (2) develop into osteoblasts that lay down the first fibrous bone matrix (osteoid), which subsequently becomes mineralized (as in stage 2b). Original blood vessels are retained in close proximity to the formative bony trabeculae (3). As bone deposition by osteoblasts continues, some of these cells are enclosed by their own deposits and thus become osteocytes (4). Some undifferentiated cells develop into new osteoblasts (6), and other remaining osteoblasts undergo cell division to ac-
Figure 17
commodate enlargement of the trabeculae. The outline of an early bone spicule (5) is shown in the enlarged trabeculae for reference. Blood vessels (3) have now become enclosed in the fine cancellous spaces. These spaces also contain a scattering of fibers, undifferentiated connective tissue cells, and osteoblasts. At lower magnification, the characteristic fine cancellous nature of the developing cortex is seen. This bone tissue type is widely distributed in the prenatal as well as young postnatal skeleton. It is a particularly fast-growing variety of bone tissue. Note that the periosteum (also formed from undifferentiated cells in the ossification center) has become arranged into inner (cellular) and outer (fibrous) layers.


Bone
terminal cap of the enlarged epiphysis is designated simply as an epiphyseal cartilage. It functions in both growth and articulation. Elsewhere in the bone, combinations of endochondral and intramembranous bone formation have brought about a conversion of the original cartilage prototype into the actual developing bone.
The first visible change in the primordial cartilage is hypertrophy of those chondrocytes located within the primary ossification center (Figs. 18 and 19). The matrix between these enlarged cells then becomes calcified, a step involved in the sequential process leading to cartilage removal. Small blood vessels from the perichondrium erode into this calcified area. As they do so, each vessel carries with it a sheath of undifferentiated connective tissue. A framework of the old calcified matrix remains as lacunar spaces of the cartilage are opened by resorption. Thus, (1 ) the calcified cartilage mass becomes extensively tunneled by vessels, and (2 ) these erosion spaces become simultaneously occupied by young vascular connective tissue, which is osteogenic. The
( 4 7 )
hypertrophied chondrocytes are released and either perish or undergo dedifferentiation into less specialized connective tissue cell types.
The perivascular connective tissue cells brought in by the vascular sprouts from the perichondrium now undergo differentiation into osteoblasts. They lie on the surfaces of the calcified cartilage remnants. These osteoblasts lay down osteoid matrix directly on the eroded cartilage spicules, and subsequent calcification results in the formation of a thin crust of bone (Figs. 19b and c). Endochondral bone tissue thus is formed within cartilage by a process of partial removal and replacement. The covering of new bone on the cartilage matrix spicules continues to increase in thickness by deposition on its growing surface. Some osteoblasts become incorporated in the forming bone as osteocytes. The lumina of the original resorption spaces in the calcified cartilage are progressively reduced as bone formation continues. The bone itself, like most other fetal bone tissues, is fine cancellous in structure. Endochondral bone can be easily recognized and distinguished from other bone types in micro-
Endochondral bone formation. In the cartilaginous anlage of a bone (a), the primary center of ossification has appeared (B). The remainder of the bone remains cartilaginous (A). The "bone" subsequently grows in two directions—longitudinally and circumferentially (arrows, stage b). The proximal and distal ends are covered by naked cartilage (C), and the underlying cartilaginous mass (D) continues to undergo rapid proliferation. As this cartilage grows in a linear course, it becomes successively replaced by endochondral bone (E). The former perichondrium now functions as a periosteum (F), and it lays down subperiosteal (intramembranous) bone that represents the bone collar
(formative shaft, G). With continued growth in both longitudinal and diametrical directions (stage c, arrows), secondary centers of ossification appear (J) that form the epiphyses. This subdivides the original epiphyseal cartilage (D in stage b) into a separate articular plate ( H ) and a growth (epiphyseal) cartilage (K). As the epiphyseal plate proliferates in a direction toward its own end of the bone, successive replacement by endochondral bone takes place (L). At the same time, cancellous bone previously occupying the medulla in the midshaft undergoes removal (P) . The periosteum (M) continues to lay down bone, so that the cortex of the shaft ( N ) increases in thickness as well as in length.
Figure 18

( 4 8 ) Cartilage and bone

Bone
scopic sections by the identifying cores of calcified cartilage matrix within the bony trabecul e (Fig. 19c).
It is apparent that formation of the endochondral bone tissue itself conforms to the same basic developmental process involved in intra-membranous ossification. The basic difference between the two is essentially the added step required in the removal of cartilage during endochondral bone formation. It is noted that endochondral bone is characteristically medullary in formation and location, and that it is associated primarily with the endosteal membrane.
At about the same time that initial cartilage replacement occurs deep within the cartilage mass, the cortex of the bone also begins formation and growth. The early cortex is a thin bony ring encircling the primary center of ossification. As endochondral bone replacement proceeds within the medullary area, the cortex (bone collar) forms around it by subperiosteal deposition. This collar is laid down by osteoblasts that have differentiated from primitive cells in the inner layer of the perichondrium (which is now a periosteum). The sequence followed in ordinary intramembranous bone formation takes place as fine cancellous, non-lamellar bone tissue is deposited.
Endochondral bone replacement in the
( 4 9 )
medullary region now proceeds in linear directions away from the primary center toward the ends of the bone, or toward the circumferential edges in flat types of endochondral bones. At the same time, the subperiosteal bone of the enclosing collar (cortex) extends for the same linear distance and also increases proportionately in thickness by continued subperiosteal accretion in a peripheral direction.
The proximal and distal sides of the growing cartilage in advance of the invading endochondral bone undergo the same series of changes that previously occurred in the original primary center (Fig. 20). This involves cell hypertrophy, matrix calcification, partial resorption by invading vascular sprouts, and the introduction of undifferentiated connective tissue into these erosion spaces. In this manner, a moving wave of tissue changes occurs within the cartilage which progresses toward each end of the bone. The entire process represents the epiphyseal growth mechanism. The successive series of changes brings about destruction of cartilage with subsequent replacement by bone. This longitudinally moving, epiphyseal "growth apparatus" is followed by endochondral bone deposition within the wake of re-sorbed spaces in the calcified cartilage.
Continued longitudinal growth of the cartilage itself is brought about by the rapid pro-
Endochondral ossification. In stage a the cartilaginous prototype of the bone (C) is undergoing initial tissue changes leading to bone formation. In the primary center of ossification (B), the chondrocytes hypertrophy and the intercellular matrix becomes calcified. This mass is then invaded by vessels from the perichondrium (A). In stage b, the calcified matrix (E) has become permeated by anastomosing erosion tunnels (D), each containing vessels from the perichondrium.
These vessels carry with them undifferentiated connective tissue cells ( H ) that subsequently develop into osteoblasts (G). In stage c, a crust of bone (J) has been deposited by osteoblasts (M) on the surface of the partially resorbed, calcified cartilage matrix (K). Endochondral bone, as a type, can be recognized in sections by the presence of these identifying spicules. Note that some of the osteoblasts have become incorporated into the bone as osteocytes (L).
Figure 19


Bone
liferation of chondrocytes near the proximal and distal ends of the elongating bone. Cell division produces isogenous groups of chondrocytes, but these cell nests are arranged in linear columns rather than in spheroidal clusters as found in ordinary hyaline cartilage. Because these cells proliferate in a linear direction, their repeated divisions bring about a progressive elongation of the developing bone (Figs. 18c and 20).
The growth site represented by the epiphyseal cartilage thus is composed of several distinct zones (summarized in Figure 20). It is apparent that each zone becomes transposed into the next, in succession, as the bone continues to elongate. The region of the proliferation zone, for example, changes directly into the zone of hypertrophy, and simultaneously a new zone of proliferation is formed as cartilage cells continue to divide. The zone of
( 5 1 )
calcification similarly becomes the new zone involving bone replacement as calcification advances in a longitudinal direction. This whole process repeats itself continuously throughout the period of growth. It results in the formation of medullary, fine cancellous, endochondral tissue, and the mechanism paces the longitudinal mode of the bone's growth. As these changes occur, the cortex simultaneously becomes lengthened in a linear direction by periosteal and endosteal activity. It also increases proportionately in thickness.
Within the epiphyseal cartilage, one or more secondary centers of ossification are formed in most bones. These develop for the most part after birth and make their appearance in a uniform sequence, a factor that can be utilized in the estimation of relative skeletal age. The development of a secondary center divides the original epiphyseal cartilage into a separate
Endochondral bone growth. In diagram a, the zones of the growth cartilage are schematized. Zone A, which is termed the reserve cartilage, feeds new cells into zone B, the zone of cell division. The cells in this latter zone undergo rapid division in a linear direction, thereby forming longitudinal columns of flattened chondrocytes (isogenous groups). This growth process is responsible for the elongation of the bone. In succession, the daughter cells undergo hypertrophy (zone C), the matrix calcifies (zone D), and this calcified matrix becomes partially resorbed and invaded by vessels (zone E). Undifferentiated cells carried in by vascular sprouts then provide osteoblasts, which in turn deposit a thin crust of bone on the remnants of the calcified cartilage matrix (zone F). This entire process is continuous and repetitive, so that one zone becomes transformed into the next in succession. Note that zone B becomes changed directly into zone C (arrow I ) , that zone D is transformed
Figure 20
into zone E (arrow 2), and that zone E becomes zone F (arrow 3) as the entire cartilage grows in a linear direction. By this means, the cartilage plate moves toward the top of the illustration as bone replacement follows.
In diagram b, the growth cartilage of a cranial synchondrosis is schematized. Note that proliferation and bone formation occurs on both sides of the plate, in contrast to the epiphyseal plate pictured in d.
Diagram c represents the growth cartilage of the mandibular condyle. A fibrous capsule (A) is present. A zone of chondrocyte proliferation (B) occurs just beneath this covering layer. Note that columns of chondrocytes resulting from repeated cell divisions are poorly represented (Duterloo, 1967).
A typical long bone epiphysis showing a secondary center, articular cartilage, epiphyseal (growth) plate, and medullary endochondral bone, is represented by diagram d.

( 5 2 )
articular cap and an epiphyseal plate (Figs. 18c and 20 d). The latter represents the actual growth cartilage and contains the graded series of zones involved in the replacement of cartilage by bone. The bone in the secondary center does not grow primarily through activity of the epiphyseal plate. Instead it increases cir-cumferentially by peripheral replacement of the growing cartilage surrounding it on all sides, including some contributions from the articular cartilage and the epiphyseal plate. The process itself, however, follows the same sequence of changes involving chondrocyte hypertrophy, matrix calcification, cartilage removal, and bone deposition. If a bone normally lacks a secondary center, the epiphyseal cartilage then functions as both a growth and an articular cartilage. This situation occurs in several human bones, and in nonmammalian forms it is common throughout the skeleton.
ADULT DISTRIBUTION OF ENDOCHONDRAL
AND INTRAMEMBRANOUS BONE. Bones are designated, familiarly, as either endochondral or membranous. Some bones, such as the mandible and clavicle, represent a fused composite involving originally separate ossification centers that produce both types in the same bone. Although a bone such as the sphenoid or the femur is classed as an "endochondral" element, it is understood that the cortical parts are actually of membranous origin. Also, endochondral medullary components become progressively removed by resorption during the normal progress of growth and remodeling and are replaced by cancellous bone of a membranous endosteal type. In the adult skeleton, only relatively few scattered remnants of original endochondral bone survive, and even these become progressively destroyed as postmatura-tion reconstruction changes occur. The adult femur thus is classed as an endochondral bone, but it is composed almost entirely of membrane
Cartilage and bone
bone. The femur of the growing child, on the other hand, contains both types; the cancellous bone of the medulla is composed partially of endochondral bone, particularly near the epiphyseal plate, and the cortices are made almost entirely of intramembranous bone (some spicules of endochondral tissue typically become incorporated into the compacta as a result of inward cortical drift).
ENDOCHONDRAL OSSIFICATION IN THE
SKULL. Some bones of the human cranial base, as in parts of the sphenoid and occipital, are classified as endochondral bones. They are composites, however, since mergers of separate endochondral and intramembranous units have occurred phylogenetically and ontogenetically. Those elements that develop in direct association with the chondrocranium have an endochondral origin but become fused with other, dermal bones that do not involve replacement of cartilage. The ossification sequence in the endochondral portions follows essentially the same steps involved in long bone growth. Unlike most synchondroses in long bones, however, those synchondroses in the cranial base are characterized by active bone replacement on both sides of the cartilage plate so that growth proceeds in opposite directions from the same growth center. This process is schematized in Figure 201?. Growth may occur at a different rate and to a different extent, however, on the opposite sides of the plate, as in the spheno-occipital synchondrosis (Chapter 9) .
The mandibular condyle represents a site that contributes to the endochondral growth of the mandibular ramus. The mechanism of endochondral bone formation itself apparently follows a developmental sequence similar to that in other bones. It is well known that the structure of the condyle, however, differs from long bone epiphyses in that a fibrous type of

Bone
cartilage occurs near the surface of the articular plate with a unique connective tissue covering (Fig. 20c). Koski and Ronning (1965) have found that the behavior and growth potential of condylar tissue differ from those in epiphyses. Duterloo (1967) has pointed out that the manner of chondrocyte proliferation in the condyle does not result in the typically elongated isogenous groups that characterize an ordinary epiphyseal plate, and that chondrocytes, once formed by parent cells in the inner part of the capsule, do not undergo subsequent repeated divisions.
GROWTH SITES. In the early development of any bone, "centers of ossification" occur that represent the initial appearance of bone tissue. In a typical long bone, a single primary center appears in the region of the mid-diaphysis, and from this bone then spreads to form the entire shaft. Secondary centers appear somewhat later than the original primary center, and these develop into the bony epiphyses. Several selected regions within an enlarging bone have been customarily designated as "growth centers," not to be confused with ossification centers, despite misleading terminology. The latter represent nuclei of beginning bone formation. The former are usually regarded as specific areas involving particularly active bone growth. Many workers prefer the term growth site to "center," because it does not suggest a limit to the extent of the growth area involved and does not necessarily imply direct regulatory control of growth activity.
The concept of the growth site is useful, because it serves to call attention to those parts of a growing bone that undergo key changes that are critical to overall growth. The epiphyseal plate in a long bone, for example, represents such a region. In the skull, a variety of different types of growth sites exist, includ-
( 5 3 )
ing the mandibular condyle, sutures, the periodontal membrane, the alveolar margin, and synchondroses. In the evaluation of the basic role of the various growth sites in the craniofacial skeleton, however, two limitations of a fundamental nature must be noted. It is sometimes mistakenly assumed that growth activity in a bone occurs almost exclusively within the major growth centers. It is implied that other remaining portions of a bone are virtually inactive, or at least provide growth contributions that are of lesser significance. All parts of a growing bone, including all of its internal and external surfaces, are directly involved in the total growth process. In the growing maxilla, for example, it is incorrect to assume that enlargement is produced solely by growth activity in the various sutures, the posterior maxillary tuberosity, and the alveolar margin. Although these localized parts of the bone make significant contributions to overall growth, virtually all other areas are also involved in active growth changes. This concept will be expanded in later sections.
Second, the concept of the growth center is sometimes extended to imply a direct regulatory control of growth processes in the other parts of the bone. This concept must be regarded with caution, because the nature of such control is difficult to evaluate, and the role of growth sites in this regard is not fully understood at present. Several basic factors must be considered. The generalized enlargement of a bone is necessarily a composite process that involves localized growth changes in all its regional areas. Although close coordination exists between these growing parts, it is an oversimplification to assume that a given "center" directly governs the course of activity in the many other areas of the bone. Growth activity in any given local region is separate and individual.
Graded levels of growth control exist, from

( 5 4 )
systemic to local. Systemic control, embodying the overall influence on skeletal growth by the hypophysis, the parathyroids, certain vitamins and nutrients, blood supply, etc., affects the generalized course of activity in all areas of the bone. The local control mechanism, however, is restricted to individual regions that undergo specific, differential growth processes. Its influence does not extend directly to adjacent regions which are simultaneously experiencing entirely different patterns of growth changes. For example, area A undergoes a process of periosteal bone deposition. Area B is a directly continuous surface adjacent to A, and both are covered by the same membrane, supplied by the same vessels and nerves, and are contiguous with the same nearby sutures, condyles, etc. Periosteal resorption, however, occurs in area B, and the nature of its growth activity and direction of cortical movement contrast sharply with area A. Furthermore, as a consequence of relocation (see page 61), area A will become sequentially relocated to occupy area B as growth continues in all parts of the whole bone. The regulatory factors controlling A will thus abruptly change as its relative location becomes moved. The local control process is a separate mechanism that is identified with each specific, changing regional area, and it does not function as such in adjacent regions. Although growth in each area takes place essentially as an independent process, the composite pattern of growth in all the different regions is an interrelated, mutually dependent, and closely coordinated total process.
The mandibular condyle is a growth site that contributes to the continued elongation of the upper ramus. Its specific growth function is the formation of endochondral bone within the medulla of the condyle and neck. It provides growth increases within a functional field involving pressure as well as articu-
Cartilage and bone
lation, and its endochondral mechanism is considered a localized adaptation to this growth circumstance. The overlying cortex, however, undergoes a separate series of growth changes involving complex inward and outward cortical movements. These are under the direct control of separate periosteal and endosteal "sites." The whole combination represents the total growth process in this area. Specific growth steps taken by any one part are separate and distinct from the others, yet all are coordinated with each other just as they proceed in concert with growth changes in all other parts of the mandible as well as with enclosing soft tissues.
It is noteworthy that neither (1 ) the local control mechanism nor (2 ) the controlling factors that function to coordinate the separate but mutually interrelated activities in different regional locations is presently understood. These considerations go beyond ordinary systemic types of control embodying hormones, nutrients, etc. A bone is sometimes erroneously visualized as an organ capable of "growing and remodeling itself." This is inaccurate in the sense that those soft tissues directly associated with the bone, rather than the actual hard part of the bone itself, represent the principal source of immediate control. This is an application of the "functional matrix" concept supported by Moss (1960).
THE FUNCTIONAL ROLE OF THE EPIPHYSEAL
MECHANISM. The cartilaginous portion of an epiphysis has two general functions: it provides an articular cap, and it represents a site contributing to the linear growth of the bone. During early growth periods prior to the appearance of a secondary center (or in epiphyses lacking secondary centers), the single mass of epiphyseal cartilage simultaneously provides both of these functions. With the formation of a secondary center, it becomes divided into a

Bone
growth region (the epiphyseal plate) and the separate covering articular cartilage.
Most epiphyses, including the mandibular condyle, conform to a design in which the articulating head is much larger than the adjacent neck. This provides an enlarged bearing surface that greatly increases mechanical efficiency in the joint. The cortex of the epiphysis is generally thin, but the underlying spongiosa is extensive. The converse is true in diaphyses. These factors make possible a large yet strong epiphyseal head composed of more or less the same bony mass as the narrow shaft. Medullary cancellous bone in the epiphysis and metaphysis is organized into complex, supporting trabecular patterns that are believed to be adapted to the corresponding patterns of external forces associated with the bone (Evans, 1957).
Contact surfaces between bones fall into two categories: those subject to tension during growth and those that bear direct pressure. Intervening soft tissues associated with the former are usually in the form of ordinary fibrous connective tissue, as in sutures. Articulating tissues associated with direct pressure, however, typically involve cartilage. Unlike bone, cartilage can withstand great pressure yet at the same time provide relatively friction-less movement on its bearing surfaces. It was previously pointed out also that cartilage represents a particular kind of tissue that is capable of continued growth in the presence of direct pressure. Cartilage within the epiphyseal apparatus provides growth by an interstitial process, a mechanism not possible in bone. Most articular surfaces lack a covering membrane, so that appositional growth here is not possible. Also, the absence of a covering vascular membrane on articular surfaces requires an underlying type of tissue that is necessarily nonvascular in nature. These structural, func-
( 5 5 )
tional, and growth relationships apply as well to synchondroses within the cranial base.
A G E CHANGES IN B O N E — T R A N S I T I O N S BE
T W E E N NEONATAL AND ADULT BONE TISSUES.
It was pointed out in the early part of this chapter that the microscopic structure of bone is directly related to various circumstances of growth. With increasing age, these circumstances change significantly in the skeleton as a whole, as well as in different parts of individual bones. The histologic structure of the bone shows corresponding changes. A primary factor related to these changes is the rate of skeletal growth and bone deposition. The actual amount or extent of deposition further influences the particular kind of bone laid down. Differences in location in the bone are necessarily involved since this governs localized rates and volume of bone deposited.
Cortical bone in the newborn skeleton is composed largely of fine cancellous, nonlamel-lar bone tissue. It may retain its cancellous texture, or it can become compacted by subsequent deposition of additional bone within the spaces to form primary osteons or plexiform bone (see previous descriptions). Because most parts of the fetal and neonatal skeleton undergo rapid increase in size, the distribution of these particular bone types is extensive. Growth is not uniformly rapid, however, because some portions of a bone characteristically enlarge faster than others in the same bone. Thus, as growth becomes regionally slowed in these parts, as in the mid-diaphysis of a long bone or in corresponding regions of the irregular bones in the skull (such as the mandibular body), other bone types begin to appear. These areas in the young postnatal skeleton, however, still demonstrate relatively fast growth, but resulting additions do not accumulate as rapidly by comparison as do cortical deposits in the other regions where growth is differen-

( 5 6 )
tially even more rapid, as in developing tuberosities, posterior surfaces of the maxillary body, the posterior margin of the mandibular ramus, alveolar processes, and other similar areas. An example of the somewhat less rapidly growing type of bone is lamellar or parallel-fibered bone tissue containing a dense network of primary vascular canals. Continued slowing of growth, both locally in any bone and throughout the skeleton as a whole, results in still other bone types. Lamellar bone containing a more sparse distribution of primary vascular canals then begins to appear. In general, the slower growth proceeds, the more widely spaced the canals become as the bone is deposited. Thus, a given bone begins to accumulate several different tissue types that reflect varying rates and amounts of growth in the various regions of the bone. These bone tissue types become stratified in successive layers, one over the other, as growth circumstances change in individual regions because of localized remodeling alterations (see Chapter 3) .
As skeletal growth continues through childhood, these conditions are repetitive throughout each bone. However, because bone growth involves resorptive removal on some surfaces as a companion process to new bone deposition in other areas, earlier zones are continually destroyed as the bone enlarges. Consequently, the record of bone growth, as demonstrated by layering of bone tissue types, can provide only a partial history of the bone's past growth ac-
Cartilage and bone
tivity since some former stages become removed.
The Haversian system is not a major structural feature of bone in the child. It may be present in some endosteal deposits and in regions of muscle and tendon attachment, but widespread replacement of original primary bone by secondary osteons throughout the cortex does not begin until skeletal maturity is approached. Even in older bone, cortical areas can be encountered in which Haversian systems are lacking.
The worker familiar with details of these complex growth factors can often estimate the approximate age of unknown bone samples with reasonable accuracy (Enlow, 1966c). One can further utilize certain differences in microscopic patterns to identify different species, although this is a hazardous procedure. It is not surprising that human bone lacks specific characteristics of structure that would make possible certain identification in unknown samples. Many mammalian forms have histologic patterns of bone structure compara-ble to human bone, although some specific vertebrate groups do have bone tissue features that permit positive group identifications. In attempting to determine whether or not a given bone sample is of human origin, it is usually possible to say only that it can be human, but that it might also belong to any one of several other mammalian groups.

(3)
Skeletal morphogenesis
It has heen emphasized that hone, because it is hard, is characterized by special features or histologic structure, and that it necessarily undergoes a specialized mechanism of growth. It was pointed out that the growth of bone involves two general processes—resorption and deposition—and that they occur only on the various inner and outer surfaces of the bone. The purpose of this chapter is to illustrate the manner in which these two basic processes are combined to bring about the overall enlargement of an entire bone.
Several misconceptions regarding skeletal growth exist, and workers dealing with craniofacial growth must be aware of them. One is the assumption that interstitial growth occurs in bone in a manner similar to that in soft tissues. Bone growth cannot proceed by internal expansion, however, because its matrix is calcified.
A widespread but inaccurate concept of bone growth is illustrated in Figure 16. A hone does not grow simply hy uniform, generalized accretion of new hone tissue on all of its periosteal surfaces, as pictured in the diagrams. The growth of a whole bone involves a series of much more complex events on its various internal and external surfaces. The factors that underlie these growth changes are outlined below.
REMODELING. Overall enlargement in the size of any bone involves two basic processes: growth and remodeling. Growth itself represents the sum of actual increases in size. Remodeling, on the other hand, provides those necessary changes within the bone that are a direct consequence of increasing size. Remodeling accompanies bone enlargement as a companion process. It is a mechanism of sequen-
57

( 5 8 )
tial, progressive adjustment that functions to maintain the shape and proportions of the bone throughout its growth period. Because growth additions in any area of a bone require corresponding changes in the configuration of other parts, the process of remodeling serves to continuously reshape and resize these parts as a result of their constantly changing locations and proportions.
BONE SURFACES AND DIRECTIONS OF
GROWTH. Surfaces that face the direction of actual growth are those that receive new bone deposits. Surfaces that face away from growth directions generally undergo resorption (Fig. 21). Depository and resorptive surfaces
Cartilage and hone
typically oppose each other on contralateral sides of a cortical plate. By the combined mechanism of bone addition on one side together with resorptive removal from the other, the entire cortex undergoes an actual movement in a specific direction according to the growth pattern in that region of the bone. The cortex becomes translocated by this process into progressively new positions, and this movement, together with proportionate increases in cortical thickness, represents growth itself.
The oversimplified notion that all periosteal surfaces categorically receive deposits and that endosteal surfaces necessarily undergo corresponding resorption leads the worker to an
Surfaces facing directions of growth. In some regions of an enlarging bone, the periosteal (outer) side faces the growth direction (X). Its opposite endosteal cortical surface (Y) faces away from this direction. In other areas the endosteal (inner) side faces the course of growth (B), and the contralateral surface of the
cortex faces away from this direction (A). Thus, surfaces X and B are depository ( + ) , and surfaces Y and A are resorptive (—). Note that the bone in area A enlarges in overall size even though its growth increases occur on the inner side of the cortex.
Figure 21

Area relocation. This growth principle represents the basis for most of the remodeling changes that take place during the enlargement of a bone. In a it is seen that area 2 of the younger bone (white) has become relocated into area H of the older bone (black'). Similarly, area 7 has become repositioned into area M. In each case, the circumstance of positional change has involved cortical remodeling that produced such regional
changes in size and shape. In b the young mandible experiences a comparable process of progressive relocation as it increases in overall size. Area 7 A, for example, has become repositioned into area 6B, and area 5J was relocated to 4K. Similarly, area 5N was moved in its relative position to area 3P. Structural remodeling accompanied all such growth changes.


Skeletal morphogenesis
inaccurate general concept of the growth mechanism; the converse of this pattern often occurs. In many parts of a bone, it is the endosteal side of the cortex that faces the actual direction of growth (Fig. 21); the contralateral periosteal side faces away from this direction. As a result, the inner surface is depository and the outer is resorptive. It seems paradoxic that a bone can actually grow in size by a process of removal from its outer side with additions on its inner surface. As will be seen, however, this situation is encountered repeatedly. Local growth processes in any region of a bone constantly change. A surface at any one time may be depository; this same surface can then become resorptive as a consequence of relocation to a new relative position (see below). Reversals thus occur as a result of sequential growth changes. Cortical bone produced by inward growth, usually with simultaneous periosteal resorption, is termed endosteal bone. Periosteal bone is formed by the converse process involved in outward growth. A reversal line characteristically occurs between endosteal and periosteal deposits, thereby separating them as distinct zones in the same cortex (Fig. 34).
These factors may be utilized in the interpretation of bone structure and the growth processes that lead to this structure. The differ-
( 6 1 )
ent combinations of periosteal and endosteal bone deposits and the distribution of resorptive and depository surfaces provide a record of past growth activities and a means by which growth movements in all parts of a bone can be analyzed. Bone markers, such as alizarin and the tetracyclines, are not needed for such interpretations since growth patterns may be readily identified without them, although quantitation is not possible.
In Figures 21 and 27, note that the different directions of growth and the orientation of the various inner and outer surfaces result in many different combinations of deposition and resorption. In all cases, cortical movement in the direction of growth is brought about by direct additions on surfaces facing this direction. The contralateral cortical surface is typically resorptive.
AREA RELOCATION. This principle is fundamental, and it underlies the basis for many of the extensive remodeling changes that occur during bone growth. When new bone is added onto an existing surface, the relative positions of all the old levels of the bone necessarily become shifted into new positions. This occurs down the line in virtually all parts of the entire bone. The process is termed relocation, and it represents a characteristic feature
Relocation. As growth stage a enlarges into b, the marker (indicated by arrow) becomes relocated from the inner to the outer side of the changing cortex as a result of an endosteal mode of growth. Note that both the shape and the size of a transverse section at the level of the dot changes markedly from a' to b' as a consequence of the relocation of this level.
In the growth of c to d the location of the dot in c no longer exists in stage d. The shape and
Figure 23
size of a section through this level have also become altered because of relocation.
As bone e grows to f, the point indicated by the dot has become translocated from the outer to the inner surface, in contrast to a and b above. Note the changes in shape and dimensions in a transverse section at the level of the marker. The diameter has increased (compare with a and b above).

( 6 2 )
of bone growth. It is a consequence of the appositional mode of growth in hard bone.
As relocation of a region into new positions takes place, localized shape, dimensions, and proportions of the old location in the bone must undergo remodeling into the different morphology that characterizes the new location. The basis for these events is illustrated in Figures 22, 23, and 24. Thus, as a bone grows, its various component parts, zones, regions, and levels necessarily undergo direct alterations in their size and shape as a consequence of changing relative positions. These changes are constant, sequential, and repetitive for the duration of skeletal growth, so
Cartilage and hone
that all individual areas of the whole bone experience a continued succession of structural adjustments as they become relocated sequentially from level to level. As one area becomes "moved" to the next, its place is taken in turn by the level behind it.
This process of relocation is the basis for bone remodeling. Because of the constant relocation of all parts in the growing bone, the whole bone represents a composite of differentially growing areas which are constantly becoming altered in structure. Thus, bone growth is not a process of simplified enlargement. The regional parts of a bone must become moved, in addition to increasing in size,
In a the movement of this model is indicated by the arrow (analogous growth movements are encountered in many areas of the cranial-facial skeleton). Point X has become relocated to point Y as the entire region shifts by a combination of bone addition (+) and resorption ( - ) . Note that old point X has now become repositioned as the new point Z, which involved a process of
cortical regression as the external surface experienced removal. In b the model is moving in an inferior direction (compare with the premaxillary region in the human face). Although the model itself is moving progressively to the left, note that the marker has shifted regressively (-) to the right from M to N. It has also been relocated from the bottom of the model to the top.
Figure 24

Skeletal morphogenesis ( 6 3 )
whole V structure moves in position in a course toward its own wide end (from p1 to p 2 ) . As it does so, however, former levels, such as X-X', become decreased in size, although the V itself has actually increased in dimensions (c and d ) .
The V principle. The entire V moves in the direction of the arrow ( a ) , by continued additions (+) on the inner surface of the V together with removal (-) from the outer side ( b ) . The V increases in overall size even though it grows by additions on its inner surface. Note that the

( 6 4 ) Cartilage and hone
The V principle as applied to long-bone growth. The schematic plan seen in Figure 25 applies to many parts of actual growing bones. In a simplified interpretation of long-bone growth, seen here, the endosteal side of the metaphyseal cortex faces the linear direction of increase. This funnel-shaped region has a V configuration in section. The V thus (1 ) moves
toward its own wide end by additions on the inner side with corresponding removal from the outer surface, ( 2 ) enlarges in overall size, and (3 ) becomes decreased in dimensions as former wide portions are relocated into new, more narrow positions. (From Enlow, D. H. : Principles of Bone Remodeling, Thomas, 1963.)
Figure 26

Skeletal morphogenesis
just to maintain their relative positions. Remodeling is a mechanism of resizing and reshaping that functions to adjust all parts of the bone to its own growth. It is an orderly process that serves to maintain constant shape and proportions of the bone as a whole. This principle will be applied repeatedly in later chapters dealing with the growth of specific craniofacial bones.
THE V PRINCIPLE. Most bones contain regions that have a V configuration. This situation is found frequently in the different parts of facial bones. In the growth of such a V-shaped region, the entire V increases in size, characteristically growing in a direction toward its wide end. The concept described earlier dealing with surfaces facing toward and away from directions of growth is relevant. In Figure
25, it is seen that the inner surface of the growing V faces the growth direction. This surface, therefore, receives new growth deposits. At the same time, the outer surface undergoes progressive resorption because it faces away from the course of growth.
These growth movements accomplish three results (Fig. 26). First, the entire V-shaped part of the bone enlarges in overall size (even though additions are made on the inside surfaces). Second, the entire V undergoes an actual movement as a consequence of its growth. This movement proceeds in a direction away from the narrow end. Third, growth and movement bring about a sequential relocation of the levels within the V. In Figure
26, note that as the V moves, former wide parts become located in new positions that are more narrow. This reduction is brought about by the same growth process that produces the movement. The progressive additions on the inner side with corresponding resorption from the outer side not only move the V, but they simultaneously serve to reduce regional dimen-
( 6 5 )
sions as the narrow parts come to occupy locations previously held by the wider levels (Fig. 27).
LINEAR GROWTH AND REMODELING. Many bones, particularly those that possess articular condyles such as the mandible, have a shape involving broad, expanded ends. The adjacent neck (metaphysis) is funnel-shaped, and it tapers into regions having a characteristically narrower configuration. Because the sequential steps involved in the longitudinal growth of typical long bones are relatively simple, they will be briefly outlined in order to demonstrate principles involved. These concepts will then be applied to the more complex but comparable growth processes in the irregular bones of the craniofacial skeleton.
A typical long bone is composed of a narrow shaft (diaphysis) between two broad epiphyses, thereby providing enlarged bearing surfaces for articulation. The bone grows in length by continued additions at its ends. Longitudinal growth is paced by the endochondral proliferation of bone behind the growing and moving epiphyseal plate. This leaves a wake of endochondral medullary bone in the elongating metaphyseal cone (comparable with the mandibular neck). The cortex simultaneously becomes lengthened in proportion by the activity of the periosteum and endosteum. As the bone elongates at its epiphyses, it grows in directions toward its own wide ends. The metaphyseal funnel has a V configuration and its growth sequence conforms to the V principle described in the previous section.
The following events occur sequentially and simultaneously. The wide end of the bone enlarges in diameter as it moves in a progressively linear direction producing a proportionate elongation of the whole bone (Fig. 27). Lengthening is not brought about by longi-

( 6 6 ) Cartilage and bone
Formation of cortical zones. Three successive growth stages are shown (black, stippled, and white areas). The manner in which a stratified cortex, composed of multiple superimposed zones, is produced during longitudinal and diametrical growth is schematized.
As stage 1 grows in length, the metaphysis is reduced in diameter so that I' becomes removed as the cortex moves in an inward direction by endosteal deposition and periosteal resorption. Because endosteal growth proceeds into medul
lary spongy bone, a convoluted irregular pattern of compacted cancellous bone is formed ( E ) . Inner circumferential lamellae, in the absence of cancellous bone, are laid down at surface A. Reversal in direction of growth has produced a zone of periosteal bone at surface B as the midshaft increases in diameter. With elongation of the bone, the projecting metaphysis at 2' becomes removed during its inward direction of growth, which results in continued formation of compacted cancellous bone ( E ) . Additional zones
Figure 27

Skeletal morphogenesis ( 6 7 )
of inner circumferential and periosteal bone are simultaneously deposited at C and D, respectively. Note that a middle layer of convoluted (compacted cancellous) bone has now become enclosed by endosteal and periosteal zones (arrow). As medullary areas previously containing cancellous bone become relocated toward the diaphysis as a result of continued elongation of
the whole bone, cancellous trabeculae are removed at G. Endosteal deposition in such regions, therefore, is in the form of evenly contoured circumferential layers. Cancellous bone formerly located in areas F no longer exist because of metaphyseal reduction in these regions. (From Enlow, D. H. : Principles of Bone Remodeling, Thomas, 1963.)
Figure 27, Continued

( 6 8 )
tudinal "expansion" of the shaft, but rather by additions only at the proximal and distal ends. The inner (endosteal) side of the metaphyseal cortex generally faces the direction of growth, and the outer, periosteal surface faces away from this direction. Following the concept of "surfaces and directions of growth" and the principle of the V, it is apparent that growth additions necessarily occur on the endosteal surface with corresponding and simultaneous resorption from the external surface. The inner side of the cortex does not actually face toward the center of the medulla, but obliquely toward the end of the bone, a direction that represents the course of linear growth. Note that the funnel of the bone enlarges even though new bone is laid down onto its inside surface and removed from its outer side.
Thus, in order to bring about an increase in overall size, some parts of the bone necessarily decrease in dimensions. The bulbous ends of the bone are wider than the shaft, and as these ends grow longitudinally the shaft correspondingly becomes elongated by continuous remodeling conversion. The old, wide metaphyseal regions are changed directly and sequentially into the lengthening, narrow dia-physis. This is an example of "relocation" with corresponding remodeling adjustments and changes that occur as a consequence of increases in length. The events and general sequence of these remodeling changes are outlined below. Although described, separately, they all take place simultaneously (see Figure 27).
1. The epiphyseal cartilage moves in a direction away from the existing shaft by interstitial growth combined with endochondral bone replacement on its diaphyseal side. This produces a core of medullary, fine cancellous, endochondral bone that becomes progressively extended in a linear manner as the cartilage
Cartilage and bone
plate grows and moves in a corresponding longitudinal direction.
2. Independent of the above process but closely coordinated with it, the cortex also becomes extended in a linear direction corresponding to the movement of the cartilage and the medullary core. Because the funnel-shaped metaphysis (neck) grows toward its own wide end, it follows the V principle. The endosteal side of the cortex faces this direction and is therefore the surface that receives new bone deposits. The contralateral, periosteal side undergoes resorptive removal at the same time. Because the medulla in this region of the bone is occupied by an elaborate system of cancellous trabeculae, the endosteal mode of cortical growth produces a convoluted type of bone tissue (Figs. 8 and 27; see also page 27). Local regions of the metaphysis usually involve tuberosities, tubercles, crests, and other irregularities of surface contour. In these areas, periosteal bone formation can occur as the region moves in a longtiudinal course. A reversal occurs, however, as these parts grade successively into the tapering funnel of the metaphysis (Fig. 32).
3. Formation of endosteal bone continues as the metaphysis decreases in size to become the more narrow diaphysis. As the diaphysis is approached, distribution of medullary cancellous trabeculae decreases, and inner circumferential lamellar layers are then formed rather than the convoluted bone produced by cancellous compaction (Fig. 8).
4. According to the V principle, these growth processes accomplish three results: The cortex of the metaphysis moves in a linear course behind the moving cartilage. At the same time, it becomes enlarged in overall size (even though its growth is endosteal in nature). As the metaphysis moves, former metaphyseal regions become remodeled into the narrow, elongating diaphysis. This involves a

Skeletal morphogenesis
direct decrease in diameter, and the endosteal nature of the inward growing cortex also accomplishes this related change.
These processes all occur in a sequential manner, and they are repeated successively as the bone lengthens. New metaphyses are formed, and as the old metaphysis in turn becomes remodeled into a new portion of the shaft, the whole bone is thereby lengthened.
5. The shaft increases proportionately in diameter as the bone elongates. The tapering metaphysis, as seen above, experiences a decrease in diameter as it grades into the shaft. The shaft, however, now undergoes an increase in width. At the point where these two regions of the bone join, an abrupt reversal takes place (Fig. 27). This point does not remain fixed but moves in a longitudinal direction with the moving metaphysis as the diaphysis correspondingly lengthens. On the diaphyseal side of the reversal, periosteal bone becomes formed and the endosteal surface becomes re-sorptive, in contrast to the basic pattern present in the metaphysis.
It is emphasized that these various growth movements all occur at the same time, and that the whole process is continuously repeated as each level of the bone becomes sequentially relocated into the next.
CORTICAL DRIFT. Constant remodeling adjustments in the cortex occur throughout the bone in response to successive changes in shape and dimensions brought about by relocation. These cortical adjustments are accomplished by a process of "drift" in which the entire cortical plate becomes moved in a variety of directions as the configuration of the area becomes altered. Cortical drift is a remodeling mechanism involving the same processes of deposition and resorption utilized in all other kinds of bone growth activity. It is concerned with growth changes that are essentially of a localized na-
( 6 9 )
ture and represents a direct response to the process of relocation (Figs. 28-31).
Cortical drift is brought about by the combination of deposition and resorption on opposite sides of the same cortical plate. The cortex can move in either an endosteal or a periosteal direction. In Figure 29, note the coordinated pattern of differential cortical drifting on all sides of the bone. The selective
Figure 28
Cortical drift. As a consequence of relocation (see Figures 22 and 23), the cortex in all local areas of a bone undergo a constant process of drift in order to bring about regional adjustments in size and shape. In this diagram, a lateral direction of drift is involved in aligning the axis of the bone relative to the bone's longitudinal curvature. This curvature is maintained and expanded as the whole bone elongates. The mid-diaphysis has shifted laterally from A to B by deposition ( + ) and resorption (—) on appropriate periosteal and endosteal surfaces.

Cortical drift. The sequence of remodeling changes that produced the cortical arrangement seen in photomicrograph A is schematized in B, C, and D. Prior to lateral drift, as seen in stage B, the cortex is composed of inner (endosteal) and outer (periosteal) zones. Simultaneously, new bone is added at surface I, removed from side 2,
Figure 29
added onto surface 3, and resorbed from side 4. The composite result is a drift movement of this entire region of the bone in the direction indicated by the arrows. The final stage D is comparable with photomicrograph A. X 5. (From Enlow, D. H. : Principles of Bone Remodeling, Thomas, 1963.)

Skeletal morphogenesis
occurrence of deposition and removal on the different inner and outer surfaces has brought about marked shift of the entire area in a lateral direction. In this particular region of the bone, drift has produced the characteristic curvature of the shaft. Tubercles, crests, and other similar bony processes become relocated as the bone grows by the same process of cortical drifting (Figs. 14, 30, and 31).
It was previously pointed out that all parts
( 7 1 )
of a bone are active during the overall processes of enlargement and remodeling. A growing bone is made up of a complex composite of many regional parts and areas. The cortex in each region undergoes its own local pattern of growth movement utilizing this process of cortical drift. Throughout the bone, the cortical plates in the various areas follow a number of differential remodeling changes, each of which is brought about by drift (as in Figures 58
Cortical drift. A number of craniofacial regions have a configuration comparable to the arrangement seen in this diagram. Their growth and remodeling patterns follow a similar procedure. Examples of such areas include the rim of the nasal aperture, the superior and inferior margins of the zygoma, the foramen magnum, the alveolar
Figure 30
crest, the sigmoid notch, the coronoid process, and many others. Both cortices drift in a common course (arrow) by an appropriate combination of deposition (+) and resorption (-) on contralateral periosteal and endosteal surfaces. The reversal occurs on the apical edge.

( 7 2 )
and 69). The process of drift may be defined, simply, as the actual movement of the cortex during growth and remodeling.
CORTICAL LAYERING. Remodeling, as de
scribed above, is a process of resizing and reshaping in response to the relocation of the bone's parts and regions during growth (Fig. 32). Because bone is a mineralized tissue, growth stages become fixed in the cortex and remain until that area of the cortex undergoes resorption or reconstruction in turn. The com-
Cartilage and bone
pact bone in the cortical plate is an accumulation of its own past growth stages, and each stage is represented by a layer or zone within the compacta. These zones are distinctive in appearance because they are typically produced during varying growth circumstances involving different kinds of bone tissue. Although a cortical plate may be made of a single layer, it is more frequently composed of a stratified series of superimposed zones, each containing a different kind of bone tissue.
Tubercle drift. As the long bone (a) increases in length (b), the protruding tubercle similarly moves in a corresponding direction. It becomes relocated in a progressive longitudinal course by deposition on the surfaces facing this direction ( + ) in conjunction with resorption from periosteal surfaces facing away from this same direction (—). The tubercle (or tuberosity, process,
crest, line, fossa, foramen, etc.) enlarges in size at the same time. A muscle attached to this surface will also become repositioned in a like direction (see Chapter 4). Note that a part of the muscle is inserted onto a depository surface, while other portions of the same muscle are attached (and successively reattached during drift) onto a resorptive external surface.

Skeletal morphogenesis
In Figure 33, two well-defined zones are present. The inner layer is composed of compacted cancellous, convoluted bone. It was produced during a former growth stage when it occupied a location in the metaphysis near the epiphyseal plate. This zone was formed
( 7 3 )
by endosteal deposition (together with periosteal resorption) as the cortex drifted in an inward direction. This level of the bone experienced successive relocation, and its relative position was shifted successively farther down the shaft as a result of continued growth
Relocation, drift, and cortical stratification. As the bone enlarges in size from J to 2, its levels (such as A, B, C) undergo sequential relocation. Reshaping and resizing at each successive level is produced by cortical drift (deposition and resorption on inner and outer surfaces). At level A, the greater part of the cortex is undergoing an inward mode of growth. The projecting tuberosity, however, shows periosteal deposition in this section. At level B, the entire cortex is experi
encing a direct decrease in diameter and is composed wholly of endosteal bone (stippled). A reversal occurs as the metaphysis grades into the shaft, and level C shows a zone of periosteal bone (shaded area) superimposed over the earlier-produced endosteal zone (stippled, area). This latter layer was formed during diameter decrease. The tuberosity in section A is at the level of outward-to-inward reversal and thus has overlapping deposition on both sides of the cortex.
Figure 32

( 7 4 )
at the end of the bone. Endosteal bone deposition occurred as the diameter became progressively reduced (compare with Figure 32). When the diaphysis was reached, a reversal took place and periosteal deposits were then formed. The endosteal surface became resorp-tive. This sequence of growth changes resulted in the formation of two distinct zones in the cortex—an initial endosteal and a subsequently
Cartilage and hone
produced periosteal zone. The developmental sequence involved in Figures 34a and b was similar but involved three layers. The middle zone of endosteal, convoluted bone with superimposed osteons was formed during metaphyseal reduction and represents the first layer produced. The inner zone of endosteal, circumferential lamellae was subsequently laid down as inward growth continued into a
The outer zone of this two-layered cortex is composed of subperiosteal bone containing numerous longitudinal, primary vascular canals. The inner zone is a layer of endosteal bone that had undergone resorption on its medullary surface as the entire cortex drifted in an outward direction.
This endosteal zone was originally laid down, however, during the inward movement of the cortical plate prior to reversal. Rhesus monkey mid-diaphysis, X 100. (From Enlow, D. H.: Principles of Bone Remodeling, Thomas, 1963.)
Figure 33

Skeletal morphogenesis
medullary area at the metaphyseal-diaphyseal junction where cancellous trabeculae were lacking. Following outward reversal, as this area became sequentially relocated as a part of the lengthening diaphysis, the periosteal zone of outer circumferential lamellae was then formed and represents the most recently produced layer. This three-layered pattern of cortical compact bone is usually pictured as "typical" in elementary textbooks, and the particular mode of formation just outlined represents a developmental sequence that leads to it. This structural arrangement is not as commonly encountered in the cortex, however, as are a number of other patterns such as those illustrated in Figures 3, 10, 11, 33, 50, 65, 67, 95, and 96.
It is apparent that the microscopic architecture of a bone is a cumulative product of its own sequential growth and remodeling processes. Random sections examined from different parts of the same bone typically show many different combinations of structural patterns. Because the cortex is composed of identifiable stages and landmarks produced as a consequence of its own formation, the history of a bone can be accurately reconstructed by interpretations of these recorded growth stages. It is noteworthy that the external contours and the gross morphology of a whole bone remain uniform and constant throughout the remodeling process, even though the underlying cortical bone itself undergoes extensive changes.
In summary, the basic function of remodeling during skeletal growth involves the constant adjustment of a bone's structure to the process of growth itself. Remodeling in bone is a special mechanism that is adapted to its hardness and appositional mode of enlargement. The progressive relocation of all areas in a bone represents the underlying factor that is the basis for these companion remodeling adjustments. The actual process of remodeling
( 7 5 )
involves reshaping and resizing each local area in all parts of the bone as they become successively relocated into new positions. This is brought about by a process of cortical drift in which the compacta moves in varying inward or outward directions in each area. New bone additions are deposited on those surfaces facing the growth direction, typically with corresponding resorption from contralateral surfaces.
CORTICAL MOVEMENT — DISPLACEMENT
VERSUS GROWTH. A bone becomes moved from one place to another during skeletal growth by two means. First, bones can be forcedly displaced by pushing or pulling of whole bones with respect to each other as they enlarge, producing direct changes in their actual positions. Second, a bone or part of a bone can grow from one place to the next by the process of cortical drift. Displacement by force represents movement that results from growth expansion producing a shove or a carrying of the entire bone to successive new positions. Movement by growth, on the other hand, is brought about by bone deposition and resorption on contralateral sides of a cortical plate. Various combinations of growth movement and movement by displacement are involved in patterns of composite movement in virtually all growing bones. These processes are outlined in Figures 35, 36, 37, and 38.
A bone such as the humerus becomes lengthened by growth extensions at its epiphyses in directions away from the existing ends. In so doing, it necessarily grows against other adjacent bones, which, at the same time, are also becoming lengthened. As a result, the different bones all become displaced away from one another as they actually grow toward each other. The proximal end of the humerus grows in a direction toward the scapula, and as a result the entire humerus becomes pushed away from the shoulder. All the other bones down


Skeletal morphogenesis
the line in the arm become similarly displaced relative to each other. Thus, growth movement proceeds in one direction, but displacement as a result of this growth produces complementary movement in an opposite direction. The total lengthening of the arm is represented by the combined displacement of all its separate component bones away from the scapula as each individual bone undergoes its own process of longitudinal growth.
A great many different combinations of such movements occur in the various bones of the skull. For example, the mandible grows in a general posterior course, but it becomes displaced in an opposite anterior manner. The maxilla grows in a number of different directions at the same time, but as it does so it simultaneously becomes displaced in forward and downward directions. The growth processes and the source of the force that bring about displacement may occur in the bone itself as well as in other nearby bones and soft tissues. The cartilage of the young nasal septum, for example, is believed to produce a forward movement of the maxillary complex while the
( 7 7 )
maxilla simultaneously undergoes its own separate but interrelated growth processes. Similarly, the bones of the calvaria become displaced in an outward course by the underlying, growing brain. The bones of the calvaria simultaneously experience a passive growth enlargement to keep pace with their displacement. Various combinations of growth and displacement are diagrammed in Figure 36.
DIFFERENTIAL GROWTH. Differences in the extent and rate of deposition and resorption between the various parts of an individual bone or between parts of two or more bones further contribute to the remodeling changes that occur during growth. For example, the maxillary tuberosity and the zygomatic process of the maxilla simultaneously grow in a posterior direction. The tuberosity, however, moves at a comparatively faster rate and to a greater extent than does the protruding malar region. This differential manner of growth movement serves to maintain the proportionate position of the zygomatic process relative to the entire lengthening maxillary arch.
Figure 34a. Two broad layers are present in this area of the cortex—an endosteal and a periosteal zone. The inner layer was originally formed during the endosteal direction of cortical growth in conjunction with the reduction of metaphyseal diameter. It contains superimposed secondary osteons, in contrast to the outer periosteal zone. The external layer was formed later, following outward reversal, and it contains abundant primary vascular canals. Rhesus monkey femur, X 100. (From Enlow, D. H.: Am. J. Anat., 1962b.)
Figure 34b. This is the traditional textbook example of bone structure. Three layers are present—outer and inner zones of circumferential lamellae and a middle Haversian zone. The mid
dle layer, formed first, was produced by endosteal cancellous compaction during the inward movement of the cortex as metaphyseal diameter became reduced. Secondary osteons typically develop in such areas in the young growing skeleton. As this region became relocated into the lengthening diaphysis, an inner zone of endosteal, circumferential lamellae was then added as inward growth continued in the absence of cancellous trabeculae. Following outward reversal, the periosteal zone of circumferential lamellae was subsequently laid down, and it represents the last-formed layer present. Rhesus monkey femur, X 100. (From Enlow, D. H.: Am. J. Anat, 1962a.)
Figure 34

( 7 8 ) Cartilage and bone

Skeletal morphogenesis
WOLFF'S LAW. Wolff's law of bone transformation has been well known since the latter part of the nineteenth century. It has become one of the most useful yet still controversial principles of our time. The concept states that the orientation and architecture of medullary trabeculae conform to certain trajectorial patterns adapted to the functional stresses placed on the bone, and that the trabeculae undergo remodeling processes which serve to constantly align them into such patterns as the bone grows or as stresses change in character (Evans, 1957). In general, Wolff's law as it is now applied maintains that the form and structure of a bone as a whole represent a direct product of function and the stresses placed on the bone.
This concept has been extended to the microscopic structure of compact bone as well. Osteons become arranged in the cortex, presumably, in a manner that is a response to external stresses. Evidence in support of this notion, however, is conflicting. It was pointed out in Chapter 2 that Haversian systems do not represent an actual unit of bone structure, and they are not extensively distributed in younger human bone. It is apparent that the young skeleton is subjected to essentially the same variety of stress forces as the adult. Fur-
( 7 9 )
thermore, osteons are entirely absent in many species. A number of recent studies have shown that such secondary (Haversian) bone actually lacks the degree of strength that characterizes the primary bone which it replaces (Currey, 1959). Also, the occurrence of the many large resorption spaces within the cortex necessary for osteon formation weakens the bone somewhat during extensive periods of Haversian reconstruction.
Bone as a tissue, however, is known to be sensitive to stresses, and it is quite responsive during and after growth to external pressures and tensions. A great deal of experimental and clinical evidence has verified these factors (Washburn, 1946, 1947; Avis, 1959). The problem remaining to be resolved is the nature of the mechanism by which extrinsic forces can become translated into direct bone changes. The actual qualitative and quantitative controlling factors involved at the tissue level are virtually unknown. This question is closely related to the problem of the local control mechanism discussed on page 54. These issues represent perhaps the most basic of our unresolved problems in bone biology.
It has been generally assumed that external tensions represent the primary factor respon-
Cortical drift and the process of displacement. A bone moves by either of two basic processes. In a the model has been positioned from P to P'. It may do this by direct cortical growth (drift) (k), or it may be carried by a process of displacement (c). These two processes frequently produce movement in divergent directions simultaneously. In d, for example, the model itself is growing to the right (arrow). The carrier, however, is moving to the left at the same time. In e, the model drifts (deposition in conjunction with resorption on contralateral surfaces) from
P to P' for a distance designated as d1. The carrier moves in an opposite course from X to 2 for the distance d2. In diagram g, the original relationship prior to these movements is indicated by X and G. The relative position of the model if drift alone occurred would be at H. The carrier, however, has moved from X to 2. If displacement alone occurred, the relative position of the model would be at E. The combination of both drift and displacement, however, results in the final positional relationship seen between 2 and F.
Figure 35

Growth and the process of displacement. As successive stages (a and b) grow in the direction of the arrow ( G ) , growth additions take place against contact surface X. This produces a displacement (DISP) of the entire growing bone in
the opposite direction (arrow, stage d). Stage c shows a growth increment as it would occur if the contact surface (heavy broken line) did not exist.
figure 37
Growth and the process of displacement. The heavy broken line represents a contact surface against which the schematic units are growing. In a an increment of growth (shaded segment) has taken place toward the "fixed" line, but the entire model necessarily becomes displaced in an opposite direction. Thus, the growth movement ( X ) represents an increase produced by thrust
as actual growth proceeds in the opposite direction.
In b the total movement (y) is the sum produced by displacement on one end and direct growth at the other. In c the position of surface Z remains constant, because growth and displacement on one side is offset by resorption on the other.

Skeletal morphogenesis
sible for determining the morphology of bones. It is held that these tensions, within threshold limits, serve to directly stimulate osteogenesis in the area of stress, and that this extrinsic force results in the formation of the various tuberosities, crests, and other bony protuberances to which the stress inducing soft tissues are attached. The bone's shape, in general, is presumed to be a result of these forces which function to augment the intrinsic genetic factors operating within the connective tissue membranes of the bone. However, it was pointed out in a previous section that many surface areas of a bone are resorptive in nature. About half or two thirds of a typical bone has an outer, periosteal surface that has experienced resorptive removal during growth (Figs. 9 and 10). The cortical bone itself was produced by endosteal deposition as it grew or drifted in a regressive, inward direction. It is a characteristic of bone that many of the more substantial areas of muscle attachment involve regions that are marked by such endosteal cortical growth (as in the metaphyses of a long bone). Many muscles thus are attached to bone surfaces that are actually resorptive in nature rather than depository, in contrast to the mistaken assumption that a muscle can only be attached to periosteal deposits of bone (Enlow, 1962b, 1965c; Enlow and Harris, 1964; Hoyte and Enlow, 1966). It is paradoxic that a muscle or tendon can be inserted onto a bone when the bone surface itself is undergoing resorptive removal. The actual mechanisms involved in this fundamental, widespread process are described in Chapter 4.
The fact that muscles or tendons are attached onto resorptive bone surfaces contradicts the belief that tension functions to shape bone by a singular process of stimulating periosteal bone deposition in the area of muscle insertion. Furthermore, a single muscle is often attached to a common hone surface in
( 8 1 )
which some portions are depository and other parts are resorptive. Thus, a periosteal surface associated with a given muscle can have separate areas that undergo entirely different remodeling changes at the same time.
It is generally accepted that muscle pull exerts some influence on bone development, and that it has a bearing on the course of normal skeletal growth. However, it is apparent that this influence can be associated with sur-
Figure 38
Growth and displacement. Each bone grows in length by additions at their proximal and distal ends. As they do so their contact ends (X) grow toward each other (b) The two bones thus become displaced away from one another at their articular junction (c).

( 8 2 )
face resorption and endosteal bone formation (cortical regression) as readily as with periosteal deposition. The assumption that muscle pull can only be associated with periosteal bone addition is thus not warranted, and the notion that the overall configuration of a bone is a product solely of bone additions caused by stress is an oversimplification.
The hard part of the bone itself is not directly responsive, since the connective tissue membrane of the bone is that part which
Cartilage and bone
brings about direct surface remodeling changes. Whether actual stress represents the primary stimulus that can trigger surface changes is not now known. A number of other factors, including vascular, nervous, hormonal, and enzymatic relationships, have not been investigated sufficiently in this regard, and such studies are encouraged. The physiologic and histochemical properties of the bone surface and its membrane associated with these remodeling changes are also poorly understood.

(4)
The growth of
soft tissue membranes
associated with bone
Studies on the structure and growth of hone have traditionally been concerned with the cortical and medullary portions of the bone and their contents. However, the bone proper represents a direct product of its own membrane activity, and virtually all changes that a bone undergoes during growth are brought about by the various soft tissues associated with the bone. The hard part of a bone, of course, is not capable of actually growing and remodeling itself. Changes take place primarily on surfaces, and they occur in association with the connective tissue membranes that cover these surfaces. The local control mechanism, previously mentioned, exerts its influence on the many different local parts of the bone directly through these membranes.
THE CONCEPT OF THE MOVING GROWTH
FIELD. The covering and lining soft tissue
membranes represent the actual sites involved in direct, local growth throughout the bone. Each individual area of the periosteum, endos-teum, suture, and periodontal membrane is a regional "center" that is concerned with bone growth activity in the specific area just deep to it. These widespread, continuous growth sites function essentially independently of each other, and the influence of each is restricted to its own regional growth field (directly comparable with the established principle of em-bryologic growth fields). Their composite activity, however, is closely interrelated and coordinated, and the changes produced at local levels in the bone proceed in concert with growth processes occurring in condyles, epiphyseal plates, and all other sites. The multiple, regional fields of growth in soft tissue membranes are in a state of constant change. Their activity is not fixed throughout growth but
83

( 8 4 )
becomes continuously revised in conjunction with remodeling changes. Fields of growth control become shifted in a sequential manner corresponding to successive cortical shifts produced during relocation.
The posterior edge of the mandibular ramus, for example, is an active growth site involving periosteal deposition (area A). Its surface is covered by periosteum which, in this specific area, constitutes a growth field associated with the posterior direction of growth movement. In contrast, a region of the ramus just anterior to this edge is characterized by surface resorption (area B). Its periosteal and endosteal fields are concerned with an endosteal mode of cortical growth. As area A moves posteriorly, the former location of the region then undergoes remodeling to become the "new" area B. The nature of the periosteal field overlying this area abruptly changes as the field associated with A moves posteriorly together with the backward moving margin of the ramus. Field A thus changes directly into field B, and its revised growth function is concerned with the remodeling conversion of one bony region sequentially into the next.
Periosteal fields of control exert a growth-regulatory influence that can involve different parts of two or more bones within the same field. In the cranial base and calvaria, for example, widespread areas of surface resorption and deposition occur in different characteristic regions. The boundaries of these areas, however, do not necessarily coincide with the margins of the separate bones involved. Thus, these growth fields overlap several different bones but do not follow the suture lines separating them. As the bones enlarge in size, the fields correspondingly expand in coverage, and they also become shifted in placement as a result of the successive relocation of the different parts in each bone.
Periosteal growth fields are comparable with
Cartilage and hone
fields of activity present in the periodontal membrane. This membrane, like the periosteum, is composed of localized growth regions each of which is governed by its own regional growth field. Under the influence of these fields, various combinations of deposition and resorption occur on lining alveolar bone surfaces. Similarly, sutural membranes also have a regional distribution of component growth fields. These different membrane types all exercise an immediate governing influence on the rate and amount of growth. Individual, localized fields within them carry out the composite of all the differential growth activities throughout the bone. As mentioned in an earlier chapter, the control of growth involves graded levels from systemic down to local. Regional field activity represents local control, and it is directly influenced in turn by the sum of all the extrinsic and intrinsic factors that contribute to the growth of the bone as a whole.
The composition of soft tissue membranes that cover or line the outer and inner surfaces of bones is often visualized as relatively stable or fixed in nature. The membrane has sometimes been regarded as a layer of more or less permanent connective tissue containing an inner, labile osteogenic zone. This osteoblastic layer produces new bone, and as it does so the remainder of the membrane draws ahead of the growing bone but otherwise remains essentially unchanged. The membrane at any one growth stage is thus presumed to represent essentially the same membrane composed of the same actual tissues found at later stages. This is not the case, however, because new membrane components are constantly being formed and subsequently reformed as the bone adjacent to it enlarges and undergoes extensive structural remodeling.
Just as the cortex experiences constant drift and movement during growth, the enclosing

Soft tissue membranes
membranes similarly undergo drifting. Drift in a connective tissue membrane represents its own internal mechanism for growth, movement, and adjustment. It is a special process that is adapted to this particular kind of soft tissue and its relationship to the changing bone which it encloses. The sequence by which a membrane undergoes drift is fundamentally different from that in the bone next to it. Membrane growth and drift involve the following factors:
1. The entire membrane enlarges in coverage as well as in proportionate thickness. It does this largely by interstitial proliferation of tissues already present within it, including the continued utilization of undifferentiated cells associated with blood vessels.
2. As the membrane grows, the contiguous bone also undergoes enlargement as a result of osteogenic activity by the growing membrane itself. If resorption rather than deposition is involved, the membrane undergoes a related growth process associated with the regressive bone surface. It grows toward, rather than away from, the receding bone surface. The membrane thus experiences direct drift movement in the same direction the bone surface moves. The drift process involves an internal mechanism of remodeling and reconstruction within the membrane itself. This process will be described in later paragraphs.
3. The remodeling activity within the membrane, in addition to producing drift, also provides the critical linkage adjustments between the growing and moving membrane and the growing and remodeling bone attached to it.
The growth activities of the various soft tissue membranes of bone, including the periosteum, sutures, and the periodontal membrane, are basically comparable, although several differences in internal structure and pat-
( 8 5 )
tern exist. These connective tissue membranes are considered separately in the following sections.
The periodontal membrane
The connective tissue lining the alveolar sockets in tooth-bearing bone is continuous with the surface periosteum and has a number of structural and functional similarities with it. The periodontal membrane provides firm attachment of individual roots to their surrounding bony walls by parallel bundles of collagenous fibers that bridge the span between them. These fibers are embedded in cementum on one side and alveolar bone on the other. In its more stable, adult form, the periodontal membrane is represented essentially by a single expanse of mature, coarse fibers. During active growth, however, a complex series of adjustments and changes is necessarily involved as the tooth-bearing bone grows in a variety of directions and as the teeth erupt and undergo their own series of movements (Fig. 39).
COMPOSITE MOVEMENTS OF TEETH AND
BONE. As the maxilla and mandible grow in size and as the teeth undergo constant positional movements, the bone adjacent to the root continuously undergoes change. These factors require an adjustment mechanism in the intervening soft tissue membrane between bone and tooth in order to maintain continuous, uninterrupted attachment.
The movements of teeth involve eruption as well as progressive drifting in either a distal or mesial direction, depending upon species or the particular tooth considered. This process serves to brace the dental arch by closing the teeth toward each other as their contact surfaces undergo attrition. During eruption and

This series of diagrams is an interpretation of adjustment mechanisms involved in the movements of the periodontal membrane during bone and tooth shifts. They illustrate successive and sequential changes that occur in the alveolar bone ( A ) , the outer periodontal zone ( B ) , intermediate periodontal zone ( C ) , inner periodontal zone ( D ) , and the cementum of the root ( E ) as both the bone and tooth drift to the right (arrows). The increment U designates an arbitrary distance moved during each growth stage. The drawings on the left (1, 2, 3) represent the series of drift changes on the depository (tension) side of the alveolar socket, and the drawings on the right ( 4 , 5 , 6 ) show changes on the resorptive (pressure) side. The points x and y are included as random position markers so that movements relative to a fixed point can be visualized.
On the tension side (1, 2, 3 ) , increments of new bundle bone are deposited on the alveolar surface, thereby progressively enclosing the fibers of the outer zone B. At the same time, the peripheral ends of the fibrils in the intermediate zone C are converted into the new fibers of the outer zone as the latter shifts to the right. The stable fibers of the inner zone D are pulled to the right and maintain constant linkage with the labile
fibrils of the intermediate zone C. These latter fibrils constantly elongate in a direction toward the right as they simultaneously become converted to outer zone fibers on the left.
On the pressure side (4 , 5, 6 ) , the stable fibers of the inner zone are moved to the right and similarly maintain constant linkage with the shortening inner ends of the fibrils in the intermediate zone. Some (not all) bone matrix fibers are uncovered from the resorbing surface of A. These, together with new fibers formed in conjunction with "spot deposits," become the fibers of the outer periodontal zone B. The inner ends of these same fibers are then converted successively into the elongating outer ends of the linkage fibrils in the intermediate zone. Direct fibrous continuity can be traced through each zone from A to E. Extensive bone reconstruction is seen deep to the resorptive alveolar surface, in contrast to the depository side, and resorption canals and secondary osteons are formed. This remodeling mechanism provides reattachment in some localized areas that previously involved total resorptive destruction of fibrous anchorage. Such alternating areas are shown along the contact between A and B. (From Kraw, A. G., and D. H. Enlow: Am. J. Anat., 1967.)

Soft tissue membranes
drift, teeth also experience tilting and rotating movements. In addition, however, another factor contributes to the basis for the drifting of teeth. The growth of the mandible and maxilla involves the continuous relocation of all their component areas and parts as each entire bone increases in overall size. As the various regions of the bone undergo consecutive repositioning, the teeth located within these areas necessarily experience corresponding and simultaneous shifts in positions in order to retain relative locations in the bone as a whole. The drifting movements of teeth contribute to this progressive and continuous process of relocation in relation to the growing and remodeling bone (Enlow, 1965b; Enlow and Bang, 1965).
ALVEOLAR BONE SURFACES. TWO general
kinds of bone surfaces line the alveolar cavity —depository and resorptive. Depository surfaces are characterized by an accumulation of successive layers composed either of lamellar or nonlamellar bone tissues. As new bone is laid down, coarse bundles of periodontal fibers are incorporated within the bone in a manner directly comparable with Sharpey's fibers as they become embedded in cortical areas underlying muscle attachment. The resulting bone type, termed bundle bone, is distinctive in structure (Fig. 40), and wherever present indicates original formation by a process of periodontal surface deposition. This kind of bone tissue may be termed simply periodontal bone. It is directly comparable to periosteal bone, in contrast to endosteal types of bone deposits. Periodontal bundle bone is the predominant tissue present on all depository lining surfaces in the alveolar cavity. However, scattered surfaces may be encountered where such fibrous inclusion during formation does not occur. In these areas, the only direct interconnection between bone and the periodontal membrane is by vascular bundles and cell processes.
(87)
Periodontal (surface-depository) bone is formed in those areas of the socket involving a movement of the tooth in a general direction away from the existing bone surface. Progressive deposition of new bone serves to maintain a constant tooth-to-bone relationship and distance as the tooth continues to move.
In contrast to the depository surface with its underlying periodontal (bundle) bone, resorptive alveolar surfaces are characterized by an eroded, scalloped, pocked margin (Fig. 41). During periods of active resorption, abundant osteoclasts are usually present on the irregular bone surface interspersed between the periodontal fibers. Resorptive alveolar surfaces are specifically located in areas of the socket involving progressive movements of the root in a direction toward the retreating bone surface. The combination of resorptive surface removal and progressive bone deposition on the contralateral sides of the same cortical plate serves to move this area of the alveolar wall in a direction corresponding to the movement of the advancing tooth. A constant tooth-to-bone relationship is thereby maintained.
If a thin, single cortical alveolar plate forms the entire partition between two adjacent sockets (Fig. 41b), it moves by periodontal surface deposition on one side together with surface resorption from the other. The plate is composed entirely of periodontal bone (in contrast to endosteal bone in the situation seen below), and as the cortex undergoes drift the bone tissue laid down on one side becomes continuously translocated over to the surface on the other side, which is resorptive. The bundles of anchoring fibers originally enclosed on the contralateral depository surface in the adjacent socket but now translocated to the resorptive side do not provide attachment for the root associated with this resorptive surface (as in Figure 41b). An entirely different mechanism is involved, as described in following paragraphs.

Cartilage and hone ( 88 )
On the depository ("tension") surface of the alveolar wall, the coarse fibers of the outer zone ( A ) pass directly into the bone. The mesh of fine fibrils of the intermediate zone ( B ) and the coarse fibers of the inner zone ( C ) adjacent to the root are apparent. Compare with resorptive
alveolar surfaces in Figures 41a and 41b This section was prepared using a differential polychrome stain for collagenous and precollagenous fibers. White rat, X 200. (From Kraw, A. G., and D. H. Enlow: Am. J. Anat., 1967.)
Figure 40

Soft tissue membranes
If the alveolar partition separating two sockets is relatively thick and is composed of two distinct cortical plates with an intervening cancellous medulla, the bone tissue underlying the resorptive side of the partition is of an endosteal type, in contrast to the situation described in the previous paragraph involving a thin, single-layered partition. As bone undergoes removal from the resorptive surface, the endosteal side adjacent to the medulla receives new bone deposits. Because this endosteal surface is continuous with cancellous trabeculae, a process of cancellous compaction takes place as spongy medullary bone becomes converted into the compact, convoluted bone of the alveolar cortex.
Fibrous continuity and attachment between bone and tooth ordinarily become severed as a consequence of the resorptive removal of alveolar bone at the surface. In all areas adjacent to advancing vascular elements of the membrane as they enter the bone within enlarged resorption spaces (Fig. 41), and in the immediate region just deep to individual osteoclasts, the bone surface is characteristically discontinuous with the fibrous matrix of the periodontal membrane. Direct attachment between the two is lacking except for cell processes and vessels. In such areas, the resorption of bone represents a total process involving complete destruction of the entire bony fibrous matrix. In some scattered, localized areas between Howship's lacunae, however, fibrous continuity does not necessarily become destroyed during the process of bone removal.* A trail of uninterrupted collagenous fibers can survive, and they are seen to emerge from the resorptive bone surface and enter the perio-
* Using historadiographic methods, Bohatirchuk (1966) has recently described a process of "calciolysis" in which resorption of the mineral phase of bone occurs without removal of some organic portions. He has distinguished this process from the old theory of "halisteresis."
( 8 9 )
dontal membrane (Fig. 41b). They may be traced directly into the general bone matrix deep to the resorptive surface. Prior to the removal of the bone around them, these fibers formerly served as a component part of the ordinary bone matrix. As they become uncovered and exposed at the receding bone surface, these surviving bone matrix fibers become incorporated into the drifting periodontal membrane and are converted into actual periodontal fibers. Because they were once actual bone fibers, these new periodontal components provide direct continuity with the fibrous bone matrix and the periodontal membrane in such restricted areas. The anchoring fibers in typical bundle bone on depository surfaces originate as periodontal elements and become incorporated into bone as inclusions. Conversely, the scattered fibers that survive resorption originate as bone fibers and subsequently become included as new components within the periodontal membrane. They are characteristically found in those areas of the resorptive bone surface where the general orientation of the underlying fibrous bone matrix coincides with the direction of tension placed on the periodontal membrane. In other resorptive regions in which the existing bone fibers do not align with the direction of stress, "spot" deposition of new bone and the establishment of new fibers are typically involved (see below).
THE FIBERS OF THE PERIODONTAL MEM
BRANE. Fibers of the actively drifting membrane are arranged into three component fibrous zones: (1 ) anchoring fibers attached to the cementum (inner zone), ( 2 ) anchoring fibers attached to the alveolar wall (border zone), and (3 ) linkage fibrils of the intermediate zone joining the inner and outer zones (Fig. 39). This pattern applies to membranes associated with both resorptive and depository alveolar surfaces. Such an arrangement is not


Soft tissue membranes
found, however, in the more stable periodontal membrane that is not associated with concurrent movement.
The inner zone, adjacent to the root, is characteristically composed of large, coarse bundles of mature collagenous fibers that insert directly into the cementum. The outer zone, adjacent to the bony alveolar wall, contains coarse, mature collagenous fibers that extend as parallel bundles into the alveolar bone. The inner zone is stable and undergoes relatively little turnover or reconstruction. The outer (border) zone is somewhat less stable, and extensive fibrous recombination occurs in this area. The middle, intermediate zone, however, is quite labile. Its linkage fibrils are of an immature, precollagenous type that undergo considerable recombination and reconstruction in the actively growing and drifting periodontal membrane. These fibrils are slender and delicate, and they serve to directly link the coarse, thick fibers of the inner and outer zones. A distinct overlap of these intermediate linkage
( 9 1 )
fibrils into both the inner and border zones occurs. This is caused by a direct merging of the various fibers and fibrils involved in the conversion processes described below. A scattering of mature, coarse fibers is usually seen in the intermediate zone. In the inactive membrane, however, the precollagenous fibrils progress to maturity, and the intermediate zone then loses its identity so that the entire membrane becomes composed of a single stable, mature collagenous zone.
The three-part zoning just described characterizes the active periodontal membrane adjacent to both resorptive and depository surfaces. Even though they are structurally similar, however, the internal sequence of changes taking place within the drifting membrane in response to these contrasting bone surface types is markedly different.
THE MECHANISM OF PERIODONTAL DRIFT.
The structural nature of the periodontal membrane provides an intrinsic mechanism en-
Figure 41 a. On this resorptive surface of the alveolar wall, the arrangement of the periodontal membrane is structurally comparable to that seen on depository surfaces (Fig. 40). Three zones are present—the outer (A), intermediate (B), and inner (C) . The sequence of changes in these zones involved in periodontal drift differs, however, from those that characterize the tension side (see text for descriptions). On the resorptive surface, small "spot" deposits are present (D and arrows) that function in transient membrane reattachment. Note that resorption spaces (E) and secondary Haversian systems (F) are formed deep to the receding, resorptive surface, which contribute to progressive maintenance of periodontal anchorage.
Figure 41b. The upper surface (A) of this thin alveolar cortex is depository, and the oppo
site side (B) is resorptive. Fibrous attachment in advance of vascular bundles has become severed (C) . In those areas where the ordinary fibers of the bone matrix coincide with the line of stress, some of these fibers undergo a direct conversion into the new fibers of the outer periodontal zone (D) as the bone experiences resorption. In other regions, scattered spot surface deposition can be seen (arrows), and these two processes in combination serve to continuously sustain anchorage between membrane and bone. In thicker areas of the alveolar wall, resorption spaces and secondary osteons are formed, a process that further contributes to periodontal reattachment. These sections were prepared using a differential polychrome stain for collagenous and precollagenous fibers. White rat, X 100. (From Kraw, A. G., and D. H. Enlow: Am. J. Anat., 1967.)
Figure 41

( 9 2 )
abling the membrane to continuously move in a manner corresponding to the variety of bone and tooth movements on either side of it. Just as teeth and alveolar bone drift together, the intervening membrane undergoes its own corresponding process of drift. At the same time, it permits differential vertical and rotating movements between the root and its surrounding bony wall while also maintaining continuous attachment between them. The complex growth movements of the periodontal membrane involve two basic and different mechanisms of drift. One is associated with resorptive alveolar surfaces, and the other is related to depository surfaces.
The processes of periodontal drift and the corresponding movements of the bony wall are schematized in Figure 39. Diagrams 1, 2, and 3 represent the sequential changes involving a depository surface, and diagrams 4, 5, and 6 show the processes associated with resorptive surfaces. In both cases, the three typical zones of the membrane are evident, including the inner and border zones with their coarse bundles of thick, mature collagenous fibers. The mesh of delicate precollagenous fibrils in the intermediate zone is present in both the resorptive and depository surface situations. A distinct overlap of these linkage fibrils is shown which extends well into the inner and particularly the border zones.
In 1, 2, and 3 of Figure 39, the tooth is drifting in a direction toward the right (away from the alveolar bone surface shown). This is the "tension" side. As new bone is added onto the alveolar surface, this surface moves to the right. The tooth shifts in a corresponding direction at the same time. The accumulating bone deposits progressively advance into areas previously occupied by the periodontal membrane as the latter also simultaneously drifts to the right. Fibers that were once a component part of the outer zone of this membrane be-
Cartilage and hone
come incorporated directly into the advancing bone as embedded Sharpey's fibers. An adjustment now occurs within the membrane because the coarse, mature fibers of the former outer (border) periodontal zone have become included as a part of the new bundle bone. A conversion process takes place in which a new bord er zone becomes formed from a former portion of the intermediate zone. Precollagenous linkage fibrils previously located in the intermediate zone now undergo maturation so that the former location of the intermediate zone at a previous growth stage becomes translocated into the newly formed border zone. At the same time, the continuously shifting and reforming intermediate zone grows in a direction to the right by an elongation of the precollagenous fibrils in a direction toward the tooth, while the opposite ends of these same fibrils (on the bone side) have in turn simultaneously undergone change into the mature fibers of the new border zone. As the root drifts to the right, the mature fibers of the inner zone, attached to the cementum, are carried in this direction by the moving tooth. The young fibrils of the continuously reforming intermediate zone become elongated behind the fibers of this stable inner zone and keep constant bond with them as they are pulled by the moving tooth. The overlap between these two zones represents the constantly drifting site of linkage between their component fibers. The entire periodontal membrane on this side of the tooth thereby keeps proportionate position and dimensions by first converting the precollagenous linkage fibrils of the middle zone into coarse, mature fibers of the border zone as the latter become involved in new alveolar bone formation. The former intermediate zone thus becomes changed directly into the new border zone as a generalized shift occurs. Second, the linkage fibrils elongate toward the drifting root thereby

Soft tissue membranes
forming a new intermediate zone between the outer and the stable inner zones. As these fibrils undergo conversion on one side, they are thus lengthened on the other to keep pace with the moving tooth and to maintain the status of the intermediate zone. The steps in this composite process all take place simultaneously, and they are continuous and repetitious as the tooth, bone, and periodontal membrane continue to drift together.
On the opposite "pressure" side of the root,* an equivalent but fundamentally different process is involved. As the root drifts to the right (diagrams 4, 5, and 6 in Figure 39), the bony alveolar wall simultaneously shifts in a corresponding direction. As the exposed (periodontal) surface of the socket undergoes progressive removal, the contralateral medullary side receives new deposits of endosteal bone. If the alveolar plate is very thin, as previously seen, the bone beneath the resorptive surface was originally deposited in the adjacent socket and then translocated as a result of cortical drift. These processes result in a shift of the entire alveolar partition in the direction of tooth movement. Proportionate thickness of the cortex is maintained.
As the root drifts to the right, the stable, coarse fibers of the inner zone adjacent to the cementum are carried in a similar direction. The inner ends of the linkage fibrils in the labile intermediate zone undergo a reduction as they continuously recombine with the fibers of the inner zone. At the same time, they become lengthened at their outer ends, thereby shifting the entire intermediate zone in the
* It is apparent that direct pressure from root to bone does not occur, and that the periodontal fibers between them are actually under tension. It is possible that the fluid-filled membrane, however, may transmit pressure from the moving tooth toward the bone surface. The role of pressure, if actually involved in a direct way in triggering resorption, is not understood.
( 9 3 )
direction of the tooth movement (to the right in Figure 39).
On resorptive surfaces of the alveolar wall, numerous Howship's lacunae are present. They appear as irregular, scalloped pits occupied by osteoclasts. Within brief, intermittent periods during which local bone removal does not occur, some of these small depressions become filled with a crust of periodontal (surface-depository) bone. The result is a scattering of minute, lenslike, spot deposits of new bone laid down on the predominantly resorptive surface (Fig. 41a and &b). As the resorption process continues, such spot deposits are subsequently removed. These irregularly distributed deposits function collectively to reestablish fibrous anchorage in areas where attachment had been severed. The coarse anchoring fibers that are embedded in them pass into the border zone of the periodontal membrane. As they grade into the labile intermediate zone, these same fibers then become shortened as the directly continuous linkage fibrils are simultaneously lengthened.
A few (not all) ordinary bone matrix fibers that coincide with the line of stress placed on the periodontal membrane are seen to survive the surface resorptive process in some areas between osteoclasts. As they are uncovered from the bone, they then become utilized as transient fibers in the moving border zone of the periodontal membrane. These exposed fibers retain their original attachment to the bone underlying the resorbing surface (which has now shifted to the right in Figure 39). As this occurs, the coarse fibers of the former outer (border) periodontal zone become proportionately shortened in turn as they pass into the intermediate zone. At the same time, the slender linkage fibrils of the intermediate zone become elongated in a direction toward the alveolar wall. Thus, as coarse bone fibers become uncovered, the border zone thereby

( 9 4 )
shifts behind the moving bone surface. The intermediate zone similarly moves to the right behind the shifting border zone by a direct conversion of the coarse outer fibers into the precollagenous linkage fibrils of the middle zone. Direct continuity between them is maintained. The molecular mechanism involved in this process of conversion, recombination, and dedifferentiation is not presently known.
Thus, it is seen that periodontal drift involves several contrasting adjustment mechanisms associated with basically different growth situations—that is, resorptive in contrast to depository bone surfaces. The membrane itself appears similar in each, but the nature and origin of fibers in the outer zone differ according to the course of periodontal drift. The labile linkage fibrils provide a differential growth-adjustment mechanism that accommodates these circumstances. Movements between the teeth and alveolar wall in both vertical and horizontal directions are also provided by the same adjustment processes. Direct, uninterrupted fibrous continuity and linkage are sustained throughout all three zones during these various simultaneously occurring conversion processes. Similarly, direct and continuous attachment is retained between the membrane, bone, and cementum.
SECONDARY ALVEOLAR REMODELING. A
collateral remodeling mechanism occurs during periodontal drift that accompanies the processes just described. This involves the continuous formation and reformation of secondary bone in advance of the resorptive, moving alveolar surfaces (Fig. 41). The process is somewhat comparable to spot deposition occurring on the surface of the alveolar wall. During resorptive removal from a bone surface, erosive penetration of enlarged resorption canals takes place which follows the course of vessels entering the bone from the periodontal membrane.
Cartilage and bone
It will be recalled that these areas involve a total disruption of fibrous attachment. New bone, however, is subsequently laid down within the resorption cavities to form secondary bone, which in turn reestablishes direct fibrous continuity in these particular localized areas. The entire fibrous matrix of the new secondary bone is continuous with the fibers of the drifting outer periodontal zone. As the resorptive front continues to advance, the recently deposited secondary bone undergoes removal in turn. New resorption spaces continue to develop in advance of entering periodontal vessels (Fig. 41), and secondary bone is formed within these spaces. This overall process provides a means by which successive fiber reattachment becomes established in regions associated with penetrating vascular bundles.
Sutures
Like the periodontal membrane, connective tissue within sutures contains varying combinations of collagenous and precollagenous fibers. The distribution of these fiber types is based on the nature of the movements that the sutural membrane undergoes. Just as the periodontal membrane experiences a process of drift in association with the movements of teeth and bone, sutures similarly undergo a process of movement and adjustment in conjunction with bone deposition and resorption. The basic mechanism involved is comparable.
THE STRUCTURE OF THE SUTURAL MEM
BRANE. In its adult stable form, a suture is composed essentially of a single zone of mature, coarse collagenous fibers that bridge two adjacent bone surfaces. During active periods of craniofacial growth, however, the internal structure of sutural connective tissue is adapted to complex adjustments that are related to the

Soft tissue membranes
bone's movement and to changes in its dimensions and configuration. In the growing suture, three or four distinct layers can be distinguished, and these have been variously named (Troitsky, 1932; Bernstein, 1933; Weinmann and Sicher, 1955; Moss, 1954; Scott, 1956; Pritchard et at., 1956). In general, a sutural membrane has a separating "capsular" layer with two "cambial" zones, one on either side of it adjacent to the two bone surfaces. The capsular layer may be regionally subdivided, however, into two component fibrous layers with a central, somewhat more loosely arranged zone (Pritchard et al, 1956).
The capsular zone is composed largely of coarse bundles of mature, thick collagenous fibers (Fig. 42). It is a dense, regular connective tissue layer which is directly continuous with the dense fibrous portion of the periosteum. When active growth and remodeling changes cease, the entire suture becomes essentially a single capsular zone.
The cambial layer (using Pritchard's terminology) is much looser in texture and more cellular. With differential staining methods (Kraw and Enlow, 1967), this zone is seen to be composed largely of immature, precollagenous fibrils. In structure and function, it is comparable with the intermediate zone of the periodontal membrane. The fibrils may be appropriately termed linkage fibrils. As these fibrils approach the sutural bone surface, they thicken to become mature, coarse collagenous fibers. They enter the bone in this form to serve as attachment fibers (Fig. 42). The sutural membrane thus is composed of (1 ) anchoring, coarse collagenous fibers that insert directly into the bone on one side (border zone) and on the other side grade into ( 2 ) the immature, precollagenous fibrils of the cambial (intermediate) zone, which in turn merge with (3 ) the coarse, mature fibers of the capsular (dense fibrous) layer.
( 9 5 )
BONE GROWTH AT SUTURES. Progressive growth in many of the bony elements in the face and calvaria involves new bone additions at sutural margins. These surfaces represent one of the "growth sites" in the various craniofacial bones. Sutural bone growth is considered to be a secondary response, however, to other expansive growth forces responsible for the actual displacement of the bones involved. Sutural bone additions are passive and do not in themselves produce the movement of the bony elements in directions away from each other. Instead, growth expansion within soft tissues associated with the bones, such as the brain, is believed to represent the primary source of the expansive force. The enlarging brain, for example, presumably produces a field of tension within the connective tissue of the suture, which in turn induces deposition of bone on the separating bony margins. As the bones become drawn from each other, progressive new bone additions occur on their contact edges, thereby maintaining proportionate relationships between the bones. If compression or a lack of tension is involved, as in parts of the cranial base or in the mandibular condyle by comparison, cartilage is ordinarily present, and a process of endochondral bone formation is typically involved.
GROWTH ADJUSTMENTS IN THE SUTURAL
MEMBRANE. The sequential events that occur within sutures during growth are outlined in Figure 43. As the two bones become separated from one another, bone is deposited on the sutural surfaces of each bone. Proportionate dimensions of the cortical thickness are maintained by additions on external periosteal surfaces and by varying combinations of deposition and resorption on endocranial periosteal (meningeal) surfaces.
Within the suture, the capsular layer is a direct continuation of the fibrous layer of the


Soft tissue membranes
periosteum. As previously noted, the middle part of this capsular layer may become differentiated into a more vascular, areolar zone, thereby dividing the capsule into three parts. The matrix of the capsular layer is composed largely of thick, mature collagenous fibers arranged in a mesh of coarse bundles (Fig. 43). Precollagenous fibrils are absent or scarce in this zone of the growing suture.
Fibers of attachment (Sharpey's fibers) are prominent beneath the sutural edge. They can be traced well into the bone but eventually become destroyed in the medulla due to the trabecular remodeling of the diploe. Although the sutural margin of the bone is perpendicular to the periosteal surface, bone deposited on the sutural surface does not necessarily follow this perpendicular plane. It can be laid down essentially parallel to the outer surface as a result of circumferential fiber arrangement within the connective tissue of the suture.
The attachment fibers embedded in the bone are mature collagenous fibers arranged in coarse, parallel bundles (Fig. 42). They extend into the sutural membrane and form a distinct zone adjacent to the bone surface. This layer is comparable to the outer zone of the periodontal membrane next to the alveolar wall. Between this border zone and the capsule, a distinct layer composed largely of delicate, slender, precollagenous fibrils occurs in the actively growing suture. A scattering of more coarse, mature fibers is usually present. This intermediate zone, composed primarily of linkage fibrils, is comparable to the intermediate
( 9 7 )
zone of the periodontal membrane. Its fibrils overlap into both the border zone and the capsule (dense fibrous zone), and are a bridge beween the two providing direct, uninterrupted fibrous continuity.
The sequence followed during sutural growth is similar to that seen in the periodontal membrane on the depository (tension) side of the alveolar socket. Bone is added onto the sutural surface to form a new layer of bone containing attachment fibers, the same fibers that previously constituted the border zone of the sutural membrane. As bone is laid down around them, a new border zone is continuously formed at the same time by direct conversion from a portion of the intermediate zone. In this process, the coarse fibers of the border zone become lengthened by maturation of the directly continuous precollagenous fibrils. The border zone of the membrane thus shifts progressively in the same direction in which the bone is growing. At the same time, the linkage fibrils become lengthened within the intermediate zone where they merge with the coarse fibers of the capsular layer. The fibers in this capsular zone are stable and undergo relatively little turnover and reconstruction.
The slender, precollagenous linkage fibrils are particularly abundant in that part of the sutural membrane near the junction of the suture with the periosteal surface of the bone. This site represents an active location of bone growth and, correspondingly, an active area involved in sutural adjustment.
These sections of the nasofrontal suture from a young rapidly growing kitten were prepared according to the differential polychrome procedure. All three zones in both Figs, a and b can be seen. The coarse fibers of the border zone
(A) and the delicate linkage fibrils of the intermediate zone (B) are indicated in photomicrograph b. The heavy, coarse fiber bundles of the capsular zone (C) are labelled in photomicrograph a. X 100.
Figure 42

( 9 8 ) Cartilage and bone
The sutural and periosteal membranes. In the upper diagram, the edges of two adjacent bones ( A ) are joined by the connective tissue of a suture. Note the position of marker X. The border zone (B) inserts directly into the surface of the bone. At its other end, each fiber of zone B continues into the labile linkage fibrils of the intermediate zone ( C ) . These fibrils are more delicate than the heavy coarse fibers of the border zone. The linkage fibrils then merge with the coarse fibers of the capsular zone ( D ) . This layer contains vessels (b) and may become regionally subdivided into a separate capsular zone for each side of the suture junction. The periosteum is similarly composed of a border zone ( B ) , an intermediate zone ( C ) , and a dense outer fibrous zone ( D ) .
In the lower diagram, an arbitrary increment of new bone has been added (+ arrows) to each sutural bone surface (A' ) - The old bones ( A )
have become displaced away from each other (DISPL arrows). Note the changed positions of the markers ( X ) . The fibers of the former zone B have now become embedded in the new bone ( A ' ) . A new border zone has formed from the old intermediate zone ( C ) as its fibrils lengthen in a direction away from bone surfaces. They undergo differentiation into coarse, mature collagenous fibers. The bone simultaneously increases in thickness by subperiosteal (and also endosteal) deposition (+ arrows). The coarse fibers of the border zone become embedded attachment fibers as the linkage fibrils of the continuous intermediate zone differentiate into the fibers of a new border zone. As the entire periosteum "drifts" in an outward course, the linkage fibrils lengthen in a direction toward zone D and increase in number to accommodate the expanded coverage.

Soft tissue membranes
Differential rates and extents of growth often occur between two adjacent bones. In this situation, the linkage fibrils of the intermediate zone provide the adjustments by which constant sutural connection between the differentially moving bones is maintained.
Various kinds of bone tissues characterize the deposits produced by sutural growth. These types are related to the same growth factors that determine the distribution of the different bone tissues in general (Chapter 2) . Rate and extent of formation are primary factors. The zygomaticotemporal suture, for example, shows particularly rapid growth, which results in a great deal of new bone formation relative to growth activity in some other less active facial sutures. Its bone tissue, which is nonlamellar and fine cancellous in young individuals, is a type associated with relatively fast growth. As sutural growth begins to slow with age, the type of bone deposits subsequently produced reflects both rate and amount according to the patterns previously described.
Different combinations of resorption and deposition occur in various sutures and parts of sutures, although depository surfaces are the most frequently encountered. If a sutural margin is resorptive, the sequence of connective tissue changes within the membrane is comparable to those in the periodontal membrane on the resorptive side of the alveolar socket.
The periosteum
Like the periodontal and sutural membranes, the periosteum is composed of several distinct structural and functional layers. The dense fibrous zone of the periosteum is similar to the capsular zone in the suture and is continuous with it (Fig. 43). A border zone of coarse, mature collagenous fibers is present in the periosteum adjacent to the bone surface. This
( 9 9 )
is continuous with a similar layer in the suture, and both are comparable with the outer zone of the periodontal membrane. Also, an intermediate zone is present in the periosteum which is comparable with the same layer in the other membrane types. It is composed of delicate, precollagenous, linkage fibrils with a scattering of coarser, mature fibers. The fibers and fibrils are continuous through these three zones. Sharpey's fibers extend directly from the border zone into the cortex as attachment fibers. They are arranged in coarse, parallel bundles and enter the bone at various angles depending upon the directions of periosteal tension at the time of bone deposition.
As in other kinds of connective tissue membranes associated with periosteal bone surfaces, bone deposits progressively enclose the coarse fibers of the border zone. The fibers of this zone become correspondingly lengthened, however, as they merge with the precollagenous linkage fibrils of the intermediate zone. This involves conversion from precollagenous to collagenous fibers. The linkage fibrils are then lengthened in turn within the intermediate zone as they grade into the mature, coarse fibers of the outer fibrous zone. Thus, the periosteum itself (1 ) grows and undergoes drift by a mechanism of internal expansion and reconstruction as it moves in conjunction with the outward growing bone, ( 2 ) increases proportionately in coverage and thickness, and (3 ) simultaneously maintains continuous attachment between bone and all layers within the membrane as well as with soft tissue organs to which the periosteum is attached.
Resorptive bone surfaces deep to the periosteum follow a sequence of changes comparable to those previously described for the periodontal membrane. In areas of direct muscle or tendon attachment, successive spot deposition of new periosteal bone serves to provide partial, transient membrane anchorage.

( 1 0 0 )
The attachment fibers embedded in these thin, irregular bone deposits merge with the fibrils of the intermediate zone in the periosteum, and one is changed to the other as the entire periosteum moves with the receding bone surface. These small patches undergo constant removal and others are formed in turn.
Some of the ordinary bone matrix fibers are apparently unaffected by the resorptive process, however, and they become uncovered and exposed at the bone surface. These surviving fibers form a distinct trail emerging from the bone and constitute a part of the new transient border zone of the periosteum. This conversion process characteristically occurs in those areas where general fiber arrangement in the existing bone matrix follows the same direction as the line of tension placed on the periosteum. As they join the fibrils of the intermediate periosteal zone, they undergo reduction. Here, conversion into precollagenous fibrils occurs as these linkage fibrils elongate in a direction toward the inward moving bone surface. The linkage fibrils are simultaneously shortened at their peripheral ends as they grade into the relatively stable, outer fibrous zone. Thus, the entire periosteum drifts in an inward direction behind the resorptive bone surface while sustaining continuous linkage and attachment between bone and the membrane itself.
On most resorptive surfaces that do not involve direct muscle or tendon insertion, periosteal attachment is fragile and appears to be restricted largely to entering cell processes and vascular bundles. A few very delicate precollagenous fibrils can be seen attached to the receding surface. It is not presently known, however, if they emanate directly from the resorbing bone (in the manner just described), or if they are merely apposed to the bone surface.
As a bone increases progressively in length, the muscles attached to it become correspond-
Cartilage and bone
ingly moved in a linear manner in order to maintain proportionate positions relative to the bone. This process of muscle shift is accomplished by the same fibrous relinkage mechanism described above in addition to Haversian reconstruction beneath the surface of the cortex.
HAVERSIAN REMODELING. It was pointed out in Chapter 2 that in the growing skeleton Haversian systems are characteristically located in cortical areas associated with periosteal surfaces of resorption, particularly in regions of muscle and tendon attachment. In young bone, such areas represent the principal location in which replacement (secondary) osteons can be extensively distributed. After skeletal maturity is reached, however, Haversian systems are then established elsewhere in the cortex in relationships that are independent of surface resorption or muscle attachment (see page 33).
In regions adjacent to vascular bundles in the periosteum, fibrous attachments between bone and the covering membrane become totally severed on resorptive surfaces. Enlarged, tubular resorption canals are formed that follow the course of the vessels into the bone. Subsequently, new bone is deposited within each resorption space, and a secondary osteon is thereby formed. The entire fibrous matrix of the resulting Haversian cylinder is continuous with the fibers of the periosteum. The Haversian system thereby provides a labile mechanism for fiber continuity in those local areas where periosteal attachment is destroyed in advance of blood vessels. The process is continuous and repetitive, and, as the resorptive periosteal surface follows an inward growth course, new generations of osteons are formed deep to the receding cortical surface.
In subsequent growth stages as the various portions of the bone as a whole receive reloca-

Soft tissue membranes
tion, reversals then occur. Areas formerly involving inward growth, with corresponding Haversian remodeling, now undergo an outward direction of cortical drift. Zones of Haversian bone previously formed during a former growth period subsequently become covered with new layers of non-Haversian bone (as in Figure 342?).
PERIOSTEAL-ENDOSTEAL TRANSITIONS. The
periosteum is ordinarily separated from the endosteum by a cortical plate of compact bone. In the very young, rapidly growing skeleton, however, another situation commonly exists. A type of tissue associated with rapid growth is frequently fine cancellous, nonlamellar bone. Because of its cancellous nature, the periosteal surface is characterized by numerous open passages that lead into the cancelli. In these openings, the periosteal membrane merges directly with endosteal connective tissue without an intervening layer of bone (Enlow, 1965a). This endosteal connective tissue contains, for the most part, relatively immature fibrils. As the cortex moves and drifts in outward
( 1 0 1 )
(periosteal) or inward (endosteal) directions, direct conversions take place as mature periosteal fibers grade directly into the precollagenous fibrils of the endosteal connective tissue. The sequence of changes is similar to the linkage process described in previous paragraphs.
THE PERICHONDRIUM. Ordinary surfaces of growing cartilage that do not involve direct attachments of muscles or tendons are covered by a perichondrial membrane composed of a single layer of mature collagenous fibers. A middle layer of precollagenous linkage fibrils is often lacking, although a brief intermediate zone can be present in areas involving abundant appositional growth. A thick, well-marked layer containing such linkage fibrils is not ordinarily involved in the perichondrium, however, because soft cartilage does not undergo extensive external remodeling changes, and differential movements between the un-calcified matrix of cartilage and surrounding tissues are not as pronounced as they are in bone.


(II)
Craniofacial
bone growth


(5)
Summary of
growth principles
The descriptions of facial and cranial growth presented in subsequent chapters are based largely on the various concepts of bone growth and remodeling explained in Section 1. A brief summary of these key principles is presented below.
GENERALIZED SURFACE GROWTH. The
growth of facial bones does not occur by a process of uniform, overall surface accretion that simply follows the surface contours already present. This common misconception is schematized in Figures 44a and 45. Note that it is impossible to derive an adult bone, such as the mandible or maxilla, from its neonatal form by such a growth process (Fig. 16c). Surface contours would become progressively more disproportionate, and the configuration of the bone would be lost.
CENTERS OF GROWTH. A given craniofacial bone usually has two or three major growth sites (sutures, condyles, synchondroses, etc.). However, it is a common misconception to assume that these "centers" are responsible for virtually all increases in the growing bone (Fig. 44b). The many other inner and outer surfaces of the bone are not passive, and virtually all parts in each individual bone are active during the growth period. The entire bone is directly involved in the complex remodeling changes that occur throughout its regional areas.
GENERALIZED SURFACE GROWTH FOLLOWING
CESSATION OF GROWTH-CENTER ACTIVITY.
The concept that generalized surface accretion of new bone occurs in a manner that simply conforms to existing contours is itself invalid,
105

( 1 0 6 ) Craniofacial bone growth
Summary of growth principles. The various bones of the craniofacial skeleton do not enlarge by a process of generalized surface accretion merely following existing contours, as schematized in a.
Facial growth is often regarded as a process occurring largely in facial sutures (1, 2, 3, 4 in diagram b), and by bone additions on the alveolar margin and maxillary tuberosity ( 5 ) . This over
simplification, however, does not take into account the extensive and fundamental process of remodeling growth that occurs in virtually all parts of all the bones.
A bone may move by two means. It can grow (cortical drift) by selective deposition and resorption ( c ) , or it can become displaced (d) from one position to another.
Relocation is shown by schematized segments
Figure 44

Growth principles
as mentioned above. However, this false notion is sometimes applied as an explanation for growth after sutures and other growth centers are presumed to become inactive. It is not possible for a bone to undergo any significant degree of surface accretion without corresponding additions at the various sutures. The sutural margin must also continue to grow proportionately as other bone surfaces receive continued deposits in order to maintain the proportionate configuration and dimensions of the whole bone and to retain its constant relative position. It is noted that all periosteal and endosteal bone surfaces represent a series of local "growth sites" equal in significance to sutures, condyles, etc.
OVERALL GROWTH—SIZE INCREASE AND RE
MODELING. Two distinct but closely coordinated growth processes contribute to increasing size. One is the addition of new bone at sutures, condyles, synchondroses, alveolar margins, and other major growth sites. These centers are responsible for continued growth pri-
(e). The black segment at left occupies the number one position. As longitudinal growth (addition of new segments) continues, however, the black segment becomes relocated in position to number two, three, four, etc. Although its relative position with respect to the other segments constantly changes, note that the black segment itself does not move. It becomes relocated because of growth taking place in other areas.
The process of relocation, as indicated in f, underlies most of the remodeling changes that take place during bone growth. In the mandible, for example, portions of the condyle become converted by remodeling into the neck. In these superimposed growth stages, sections of A and B show the local changes in size and shape that occur as the bone enlarges. Remodeling is a process of reshaping and resizing as a consequence of progressive, continuous relocation.
( 1 0 7 )
marily in the particular parts of the bone directly associated with them—i.e., medullary bone in the neck and head of the condyle adjacent to the condylar growth center. All other parts of the bone, however, simultaneously and continuously undergo extensive processes of remodeling growth, which contributes two basic functions. It provides sequential adjustments in structure necessary as a companion process to overall growth. This serves to maintain the constant configuration of the growing bone. It further provides proportionate increases in the size of these areas and parts. Essentially, remodeling is a process of regional reshaping and resizing, and it functions as a response to relocation.
Figure 45
Two superimposed growth stages of the human mandible are shown. The purpose of the next chapter will be to relate the complex sequence of remodeling changes that are involved during this growth. It would be appealing to suppose that the young stage (white area) simply grows into the older mandible (stippled area) by a process of direct bone deposition on all the various external (periosteal) surfaces as shown, together with resorption from all endosteal surfaces. However, such a process cannot occur, as will be seen. The superimposition shown in this diagram illustrates a manner of direct mandibular enlargement that does not take place. Compare with Figure 58.

( 1 0 8 )
RELOCATION. The successive, sequential relocation of all areas within a bone as a consequence of its own growth represents the key factor that is the basis for bone remodeling. This concept is schematized in Figures 44e and f. Note the changing relative positions of all the individual segments in this diagram when new segments are added. Because of this, each individual area of a growing bone must undergo constant remodeling alterations in shape and size to accommodate its successive new positions.
SURFACES FACING DIRECTIONS OF GROWTH.
The particular surface that faces the actual growth direction is the surface that receives new bone deposits. Contralateral surfaces facing away from this growth direction are usually resorptive. The result is a drift movement of the entire cortical plate which follows the course of growth. Cortical movement produced by direct drift is to be distinguished from movements produced by displacement.
GROWTH MOVEMENTS—DRIFT AND DIS
PLACEMENT. A cortical plate can become moved by two means. It may grow from one position to another by addition and resorption of bone on selected surfaces, a process termed cortical drift; or it may move by being pushed or drawn as a consequence of growth displacement (Figs. 44c and d) . Displacement is a result of two or more bones and contiguous soft tissues growing in relation to one another. In virtually all bones, various combinations of both kinds of movements occur at the same time, a factor which greatly complicates inter-
Craniofacial bone growth
pretations and analyses of the total growth process. The movements produced by displacement often appear to violate the principle stated above with regard to surfaces facing the direction of growth. For example, the pre-maxillary area faces the forward direction of overall enlargement. Yet this forward facing surface is actually regressive (resorptive) in nature. Facial growth, however, is a composite process involving actual growth in combination with displacement resulting from growth, so that a bone may undergo growth increases in one direction but become pushed or pulled in entirely different directions. Growth processes in each local area of a bone must be analyzed separately. The total growth of all the areas in each individual bone can then be visualized in an overall growth pattern. Finally, interrelated groups of bones may be viewed together in a composite picture that represents the cumulative sum of all these growth processes.
THE V PRINCIPLE. Many areas of the various craniofacial bones conform to a V configuration when viewed in section. These areas usually conform to a common growth plan which in most cases involves growth of the V toward its own wide end. Utilizing the principle stated above which deals with surfaces facing directions of growth, bone be
comes added to the inner side of the V and removed from the outer. This serves to move the V and to reduce diameter progressively as wide parts become relocated into more narrow parts. The entire V enlarges in size at the same time.

In the phylogenetic history of the mandible, the large number of individual bony elements that characterize the lower jaw of nonmam-malian forms has been reduced to a single element, the dentary. Among the primates this bone is fused at the midline symphysis. The result is a one piece mandible that has taken the form of an ordinary long bone but with a distinctive U configuration. The presence of a superimposed arch of thecodont-type teeth is accommodated by variations of the same remodeling processes already utilized during the growth of the bone.
In the changing face of a child, the mandible appears to grow essentially forward and downward. Because of the unique, U-shaped configuration, it would be reasonable to suppose that mandibular enlargement occurs by growth primarily at the forward end, which is the portion seen to move anteriorly as the
(6)
The mandible
bone grows. The vital staining experiments of Hunter (1771), Brash (1924), and others, however, and the recognition of condylar growth centers (Charles, 1925; Brodie, 1941b) have shown that the predominant course of growth is actually posteriorly, and that the forward projection of the jaw is a consequence of displacement that occurs during this backward direction of progressive growth. Mandibular elongation involves continued additions of bone at each condyle and along the posterior border of the ramus. This results in a linear mode of growth somewhat comparable to that found in typical long bones. The process of posterior enlargement, however, represents only one of many major movements associated with total growth. All the different parts and areas of the whole bone are involved in the growth process. The various areas throughout the bone, including virtually all
109

( 1 1 0 )
its inner and outer surfaces, represent localized growth sites. They function separately in their own regions just as the condylar center functions in the head of the ramus. The overall enlargement of the bone is accompanied by a complex series of major regional remodeling changes that serve to adapt each individual area to the total pattern of progressive growth. In the descriptions that follow, growth processes in each part of the mandible are considered separately. The interrelations of all these parts in the composite growth plan of the whole bone are then described.
THE CONDYLAR MECHANISM. The cartilaginous covering on the condyle serves a dual function: it represents an articular cartilage (although covered by a fibrous membrane), and it also functions as a growth cartilage. Interstitial and appositional growth in this plate produce a linear movement of the condyle in an obliquely upward and backward course toward the temporal bone. As it grows, the deeper portion of the proliferating cartilage becomes continuously replaced by endochondral bone, thereby producing medullary bone additions in the condyle and its neck. The cartilage plate moves by growth on one side and bone replacement on the other. Endochondral bone formation results in a medullary core of fine cancellous bone. It is not directly responsible for the formation of the outer cortical plate enclosing this core. The cortex is produced, instead, by the activity of the periosteum and endosteum independent of the growth cartilage but in conjunction with it. The condylar growth mechanism does not represent the primary center for the growth of the entire mandible and is not responsible for governing overall mandibular growth. Its primary role is the formation of the medullary core of bone in this particular region while, at the same time, providing articulation with the
Craniofacial bone growth
cranium. The condyle is a major site of growth involved in the upward and backward elongation of the ramus, in combination with coordinated growth activity by the periosteum and endosteum in cortical parts of the condyle, neck, and ramus. The condylar growth mechanism represents a means for providing direct linear growth in a field involving pressure, and it is a composite of articular endochondral (pressure adapted) growth and membranous (cortical) growth. This mutually interdependent process of enlargement produces a movement of the entire condyle that results in the elongation of the ramus. See pages 52, 54, 139 for further discussion.
As the condylar growth cartilage moves obliquely upward and backward, it leaves a tapering trail of medullary endochondral bone in the condylar head and neck. The entire head of the condyle moves in this same direction by forming a completely new condyle behind the moving cartilage. This process is continuous, and as the condyle moves by growth, former levels of the condyle become simultaneously converted into the elongating neck. The posteriorly and superiorly facing surfaces of the condyle are covered by cartilage. In other regions having a periosteal covering, however, a distinct cortex is present which is quite thin, a situation common to the epiphyses of most bones. The medullary area contains an elaborate system of cancellous trabeculae. The thin cortex and the underlying cancellous medulla together provide a stable condylar head having an enlarged articular bearing surface, although no significant increase in actual bony mass is present over the more narrow neck (metaphysis) with its thicker cortical plates.
THE CONDYLAR NECK. AS the relatively broad head of the condyle grades into its more narrow neck, a sequential series of remodeling

The mandible
changes occurs that produces a structural conversion from one to the other. It is apparent that the head, as it moves upward and backward, previously held actual positions occupied in sequence by the various levels of the neck and those parts of the ramus in line with the neck. Each level undergoes a direct process of transition as these successive changes in position occur. As the ramus elongates, former levels occupied by the head are remodeled into the upper neck. In sequence, the former upper parts of the neck undergo remodeling conversion into the new lower parts. In turn, the former lower portions receive direct remodeling changes (reshaping and resizing) into the ramus proper. This entire process is continuous and repetitive, and the changes involved all take place simultaneously. The successive growth movements involve the principle of area relocation, which represents the basic factor that underlies these remodeling processes (Fig. 44f). With each successive addition of new bone at the free end of the condyle, all the levels down the line in the neck and ramus necessarily receive relocation in their relative positions. Each local level, as it becomes repositioned, undergoes adjustments in shape and dimensions to convert it into the next level in sequence.
The condylar head is much broader than the neck beneath it. Because the neck is sequentially derived from the head by remodeling, a marked reduction in width takes place. This growth change is common to all bones having an enlarged articular head. In long bones, the remodeling process involved is termed metaphyseal reduction. The growth process in the mandibular condyle and its neck is comparable, and the changes follow the same sequence of steps. Reduction is brought about by surface resorption of bone on the outer (periosteal) side of the cortical plate together with continued, proportionate deposition of bone on
(111)
the inner (endosteal) surface. The entire cortex drifts in an endosteal direction as (1 ) the head moves progressively away from the existing neck, and ( 2 ) the neck becomes lengthened by this process of endosteal growth behind the moving head. The buccal and lingual cortical plates thus move in an inward, medullary direction toward each other as the transverse dimensions of the neck become reduced.
The growth and remodeling processes in the condylar neck follow the V principle. New bone is added to the inner side of the V-shaped neck while bone is removed from the outer (periosteal) surface at the same time (Fig. 46). The result is an actual growth movement of the entire V in a posterior and superior direction. It will be recalled that the V mechanism of remodeling provides three simultaneous growth functions. First, it moves the entire structure in a progressive course toward its free (wide) end, which brings about a continuous change in position of the condyle and neck to keep pace with the moving condylar growth cartilage. Second, it produces an overall enlargement of the whole V-shaped region proportionate to the increasing size of the mandible as a whole. Third, it results in a sequential reduction of the tapering wide part of the head and neck into more narrow areas as the latter becomes relocated into the former. This reduction is produced by cortical growth in an endosteal manner.
The growth principle dealing with surfaces facing toward and away from the direction of growth applies. Note that the endosteal side of the cortex in the funnel of the neck faces obliquely toward the head of the condyle rather than directly toward the center of the medulla. Conversely, the outer, periosteal surface faces away from this direction. To move the entire neck in an upward and backward direction, therefore, new bone deposits are

( 1 1 2 )
added on the surface facing this direction, which is the endosteal surface. Bone is correspondingly removed from the surface facing away from the growth direction, that is, the outer (periosteal) cortical surface (Fig. 46).
The endosteal manner of cortical growth involves a process of cancellous compaction which brings about a conversion of medullary spongy bone into compact cortical bone. The inward drifting cortex continuously moves into areas occupied by medullary cancellous bone, and deposition of endosteal bone in the irregular spaces reduces their lumen size to that of ordinary vascular canals. The result is a typical
Craniofacial bone growth
convoluted type of bone tissue that can be recognized by its irregular, whorled appearance (Fig. 51, left).
THE POSTERIOR MARGIN OF THE RAMUS.
As the condyle moves obliquely in a posterior and cephalic course, the posterior border of the ramus becomes lengthened vertically. At the same time, it receives proportionate additions of bone along its entire backward facing margin, thereby keeping pace with the posteriorly moving condyle. This process involves rapid deposition of relatively large amounts of new bone because it produces one of the dominant
The diameter of the narrow condylar neck as seen in d is progressively reduced from the wider dimensions of the posterior-moving condyle (a) . Inward growth of the buccal and lingual cortices (c) is accomplished by a combination process of
periosteal resorption (—) and endosteal deposition ( + ) . This is an example of the V principle (b). (Adapted from Enlow, D. H., and D. B. Harris: Am. J. Orthodont., 1964.)

The mandible
growth movements in the mandible. The type of bone laid down reflects this manner of deposition. During very active growth, it is typically in the form of fine cancellous, nonlamellar bone tissue. The thin cortex may subsequently receive compaction. In the young mandible, however, posterior cortical drift may be so rapid that the fine cancellous texture is retained during its relatively short existence since the moving cortex becomes constantly replaced by the medulla during growth movement.
The condylar neck, as described above, is composed largely of endosteal (inward-growing) bone. An outward, periosteal reversal occurs, however, as the base of the neck on its posterior side grades into the posterior margin of the ramus. Here, a superimposed zone of periosteal bone is formed over the older endosteal cortex that was produced earlier during the period of condylar reduction. Below this reversal junction at the base of the condylar neck, a cap of uninterrupted periosteal deposits continues down the length of the ramus (Figs. 47 and 51). This new bone brings about a vertical elongation of the ramus beneath the upward-moving condyle as well as direct posterior enlargement. Below the level of the neck, periosteal bone is laid down on the buccal in addition to the posterior surface as this part of the ramus now begins to shift its axis in a lateral direction (Figs. 47 and 51).
THE MANDIBULAR (SIGMOID) NOTCH.
Growth in this area is usually explained as an addition of bone on the posterior border of the coronoid process with removal from the anterior face of the neck (Fig. 52). This is an inaccurate interpretation, however, as will be seen below.
An outward periosteal reversal occurs on the anterolingual side of the neck (Fig. 47) so that a zone of periosteal bone extends downward from a level just below the condylar
( 1 1 3 )
head. This periosteal reversal on the anterior face of the neck takes place much higher than on the buccal side. Thus, the greater part of the sigmoid notch in this area, which forms a distinct ledge on its lingual side, is actually depository in nature rather than resorptive. This is in direct contrast to the oversimplified picture seen in Figure 52. (See also Fig. 57.)
Periosteal bone is added onto the lingual surface of the ramus in the region just below the sigmoid notch. These periosteal deposits continue down from the condylar head around the lingual side of the sigmoid notch and then extend up to the apex of the coronoid process. This occurs only on the lingual surface of the ramus. In Figure 50a, note that the recently deposited periosteal bone laid down on the lingual side becomes removed soon after its formation by periosteal resorption from the opposite buccal side on the thin edge of the sigmoid notch. This results in a shift of the anterior base of the neck in a lingual direction. Note that this surface faces lingually and cephalically, and continued deposition of periosteal bone produces a corresponding growth movement in both a lingual and a cephalic direction. The significance of the lingual drift will be explained in a later section. The height of the ramus becomes increased by the addition of new bone along the entire superior surface of the sigmoid notch. This occurs only on its lingual surface, however, which is the side that actually faces this upward direction. The surface that faces away from the growth direction, in the perimeter of the notch, is the buccal side. This side undergoes corresponding removal by periosteal resorption of the same bone that just recently was laid down on the opposite lingual side but transposed to the buccal as the whole cortical plate drifted in a cephalic and lingual manner.
The explanation that the sigmoid notch moves posteriorly by deposition on the posterior

( 1 1 4 )
margin of the coronoid process with resorption from the front of the condylar neck is thus an oversimplification of a process that does not, in fact, occur. Actual resorption is involved only on the buccal side, and this takes place around
Craniofacial bone growth
the entire perimeter of the notch along the coronoid process as well as on the neck. This resorptive process is concerned primarily with the upward growth of this region rather than with a posterior movement. It is apparent, also,
As the buccal and lingual sides of the condylar neck (b) are reduced in diameter (—), the margin of the mandibular notch receives periosteal deposits on its lingual side ( + ) as this surface grows in a cephalic direction. The opposite surface on the buccal side, which faces away from the direction of growth, undergoes corresponding re-
sorptive removal. The posterior margin of the neck receives periosteal deposits as this entire border of the ramus grows and moves in a buccal and posterior direction (c). The plane of section is indicated in a. (Adapted from Enlow, D. H., and D. B. Harris: Am. J. Orthodont, 1964.)
figure 47

The mandible
that growth activity is not confined to the various anterior and posterior edges of the sigmoid notch, condylar neck, and coronoid process.
In summary, the cephalic (upward) growth of the ramus in the region of the sigmoid notch is a result of bone deposition on the lingual side. This surface slopes medially in such a manner that its periosteal surface faces upward. The contralateral buccal side is oriented so that it faces away from the direction of growth. Its periosteal surface is resorptive and the endosteal side is depository. The cortex on the buccal surface is composed of endosteal bone, and the cortical plate on the lingual side is composed of periosteal bone. They join at the thin edge of the sigmoid notch to become a single cortex composed entirely of periosteal bone that is produced on the lingual side and resorbed from the buccal surface. The posterior (backward) movement of the sigmoid notch is produced by periosteal deposits on the entire lingual face of the coronoid process. This surface is oriented so that it is also directed posteriorly. At the same time, the elongating condylar neck is growing upward and backward behind the moving head. This serves to extend the sloping posterior margin of the sigmoid notch in an obliquely posterior direction while it simultaneously moves upward as a result of its periosteal bone deposits.
A minor variation can sometimes occur in which a thin crust of periosteal bone forms on the buccal side below the notch. Progressive growth in a cephalic direction is brought about by the much more extensive and rapid differential deposition of bone on the lingual face.
THE CORONOID PROCESS. TO produce a
backward movement of the ramus in toto, it is apparent that its anterior margin, including the coronoid process, must undergo progressive removal. This growth change, first recognized by John Hunter, was later verified by
( 1 1 5 )
Humphry (1864) in a clever experiment. He implanted small metal rings into the bone on both the anterior and posterior margins of the mandibular ramus in the growing pig. Humphry found that the rings inserted on the posterior side became more deeply embedded, but those secured on the resorptive anterior face became released from the bone as the ramus grew in a posterior course.
The growth movement of the coronoid process, as well as the entire ramus, does not represent a simple backward shift that follows a single plane in a straight posterior direction (Fig. 52a). Furthermore, the expanse of bone between the anterior and posterior borders (areas X, Y, Z in Fig. 52b) is not passive during the posterior growth process. Instead a number of complex remodeling changes occurs on all these surfaces during the growth and movements of the ramus and its projecting bony process. The cephalic apices of the paired coronoid processes move farther apart as they grow superiorly. They become shifted posteriorly as the entire ramus grows backward. The basal part of the process moves laterally, but the forward portion of each base shifts abruptly toward the midline as it joins the mandibular body. These complex, multidirectional growth movements all occur simultaneously.
In Figure 57, note that the forward-facing anterior border of each coronoid process is resorptive around to the temporal crest on the lingual side. The underlying cortical bone tissue is entirely endosteal in type. Note also that the greater portion of the lingual face of the process is depository, and that its cortex is composed of periosteal bone. The entire buccal surface, however, is resorptive in nature, and the inward-growing cortex on this side of the coronoid process is composed of endosteal bone.
The two coronoid processes are positioned in

( 1 1 6 )
such a manner that they form a vertically oriented V. The movement of this V in a direction toward its wider end involves new bone deposition on the inner side with bone removal from its outer surface. Thus, vertical growth and movement of the two coronoid processes are accomplished in a manner corresponding to the simplified V principle (Fig. 49). Bone deposition on the lingual surfaces of these two processes (the inner sides of the V) brings about growth in a cephalic direction and at the same time serves to move their apices farther apart, thus enlarging and widening the broad superior ends of the V. The contralateral buccal surface (outer side of the V) of each coronoid process is resorptive, and its cortical plate similarly moves in a cephalic direction by addition of bone on the endosteal surface of the cortex. As a second function performed by the V mechanism, the wider superior parts of the V become successively relocated into the more narrow, basal regions as the entire V enlarges in an upward manner. This progressive reduction in transverse dimension is accomplished by the same mechanism of bone addition on the lingual side with corresponding resorption from the outer buccal side.
These remodeling movements may also be explained by applying the principle dealing with selective bone addition and resorption on surfaces facing toward and away from directions of growth. The front edge of the coronoid process as well as the entire forward half on the lingual side faces anteriorly. This direction is oriented away from the general course of posterior growth. Thus, the forward-facing border and the lingual surface anterior to the temporal crest are both resportive, and their cortices are composed of endosteal compact bone. This growth pattern is associated with the backward mode of growth of the entire ramus. The remainder of each coronoid process
Craniofacial bone growth
is oriented so that its lingual surface faces three general directions: posteriorly, cephal-ically, and medially (Fig. 48). Correspondingly, the contralateral buccal surface faces away from these three directions. Thus, periosteal bone deposition on the greater portion of the lingual face of the coronoid process (with endosteal resorption), and periosteal resorption from the entire buccal surface (with endosteal deposition) serve in combination to move these processes in a superior direction and at the same time to shift them posteriorly. In brief, the composite of (1 ) a lingual deposition and (2 ) buccal resorption produces drift of the coronoid process in upward and backward directions, because the lingual side faces toward these directions and the buccal side faces away from them.
The fact that each coronoid process also faces medially and that bone is deposited on their lingual surfaces establishes another basic growth function. The apices of these processes move apart in lateral directions as they grow in a superior course. This brings about a progressive relocation of the base of the coronoid process, adjacent to its junction with the ramus, successively higher as it follows the upward moving apices. Levels formerly occupied by the correspondingly upward moving coronoid base become sequentially converted by remodeling into the ramus below it. Because the ramus is more medial in position than is the coronoid process, a medial direction of growth is involved. This is accomplished by the same deposition of bone on the lingual face of the coronoid process that also brings about its posterior and superior directions of growth movement (Fig. 49). This is an example of the "area relocation" principle in which the former coronoid process of a previous growth stage is relocated in a lingual manner in order to become a part of the new, enlarged ramus as it grows in height following the up-

The lingual surface of each coronoid process faces three general directions, and growth proceeds simultaneously in each direction. The coronoid process grows and moves cephalically, posteriorly, and lingually as pictured in these diagrams. Note in b that the medial direction of
movement at the base of the coronoid process carries the anterior part of the ramus in a lingual direction as it becomes relocated into line with the elongating mandibular body. (From Enlow, D. H., and D. B. Harris: Am. ]. Orthodont., 1964.)
Figure 48
( 1 1 7 ) The mandible

( 1 1 8 ) Craniofacial bone growth
A vertical section prepared through the coro-noid process and ramus ( a ) shows a characteristic growth pattern (b) that involves periosteal deposition (+) on the lingual surface of the coronoid process together with removal (—) from the buccal surface. The basal part of the ramus receives periosteal deposits on the buccal side with contralateral resorption from the lingual surface. In c the coronoid process moves from 1 to V. Note that the coronoid process of the younger (smaller) mandible occupies the same level as the lingual tuberosity in the older growth stage. The remodeling mechanism involved in this relocation is described below.
Diagram d illustrates the growth sequence of
the coronoid process by the V principle. Note that the two coronoid processes become larger and higher and that they grow farther apart at their apices ( 3 ) by additions on the lingual surface (4 ' ) with contralateral removal from the buccal side (4 ) . Note also that this same mechanism of lingual deposition brings their bases toward each other ( 5 ) . This combination of growth movements serves to move and enlarge the coronoid processes from 1 to 1' in c and to bring about simultaneously the lingual direction of movement seen at 2 in diagram c as the mandibular body becomes lengthened. (Adapted from Enlow, D. H., and D. B. Harris: Am. ]. Orthodont., 1964.)

The mandible
ward moving coronoid process. It is also an example of the V principle, as seen above, in which wider parts of the V are relocated and remodeled into more narrow levels as the entire V moves sequentially toward its wide upper end.
The entire anterior basal part of the ramus in turn continues this same lingual direction of shift until it reaches a line continuous with the axis of the mandibular body and dental arch. The body elongates in a posterior direction, and it comes to occupy locations previously held by the ramus. The latter is converted into the bone of the lengthening posterior body as a result of the lingual growth shift of the posteriorly moving ramus. Thus, the medial direction of drift of the coronoid process, together with the corresponding medial movement of the contiguous anterior part of the ramus, is produced by the characteristic mechanism of bone deposition on the lingual side. This also serves to bring about the cephalic and posterior movements of the coronoid process, as previously described.
The forward-facing anterior border of the ramus and coronoid process has a thin cortical plate composed of endosteal bone. It continues around to the temporal crest on the lingual side. Because the medullary regions here are occupied by extensive cancellous trabeculae, a process of progressive, inward-moving cancellous compaction is involved. This endosteal bone tissue is of a typical convoluted type.
In very young or small mandibular specimens, much of the coronoid process may be composed of a single plate of compact bone that forms the entire thickness from the buccal to the lingual surface. The lateral side of this cortex is made of bone previously formed on the opposite lingual surface but subsequently transposed to the buccal side as the plate drifts medially by lingual deposition and buccal resorption. An inner endosteal surface does not
( 1 1 9 )
exist on either the buccal or lingual side in this situation, because a middle medullary cavity is not present. Therefore, the bone deep to the resorptive buccal surface is not of an endosteal type, but rather is actually periosteal bone that was formed on the contralateral lingual side. In larger or older mandibular specimens, however, a narrow but distinct medullary space intervenes between the lingual and buccal cortices. The buccal cortex moves in its combined posterior, cephalic, and lingual directions by endosteal formation of bone on this medullary surface together with periosteal resorption.
THE BUCCAL SIDE OF THE RAMUS. In Figure 57, it is seen that the upper part of the mandibular ramus on its lateral side possesses a resorptive periosteal surface. Its endosteal cortex is a direct continuation of the inward growing bone that characterizes the condylar neck, the sigmoid notch, and the coronoid process on their lateral (buccal) sides. Thus, the resorptive outer surface continues down from the neck onto the upper part of the ramus, and the resorptive surface of the coronoid process similarly extends down well onto the ramus. An abrupt reversal occurs on a line marked by the prominent change in contour along the ridge that projects downward from the neck across the upper portion of the ramus. Below this line, the entire remainder of the ramus has an outer periosteal surface that is depository in character. This arrangement is based on the contrasting directions that these different areas of the ramus face during active growth. The factor of area relocation is directly involved.
Above this line of reversal (the lateral mandibular reversal, page 259), the buccal surface of the ramus faces generally away from the superior and posterior course of ramus growth. Its periosteal surface is therefore re-


The mandible
sorptive in nature and the cortex is composed of endosteal bone. Note that the posterior edge of the ramus, as it grades into the neck, is noticeably thicker than the region located anterior to it just below the sigmoid notch. Because the entire ramus is growing posteriorly, the thicker part is sequentially shifted backward by new periosteal deposits, and former such areas become repositioned to the new thinner regions beneath the sigmoid notch. This sequential relocation involves successive remodeling conversions. The endosteal mode of cortical growth brings about the change in dimensions, and it simultaneously provides the posterior direction of overall growth movement because its periosteal surface faces away from this direction.
In the transition zone below this line of reversal, which represents the approximate line along which the growing neck has passed during previous growth stages, the cortex is composed of two distinct layers. The inner layer is made of endosteal bone produced earlier during the cortical reduction of the neck. It is covered by a more recently deposited outer zone produced subsequent to reversal.
Below the reversal line, the contour on the
( 1 2 1 )
buccal side of the ramus is oriented so that its outer periosteal surface obliquely faces the backward direction of ramus growth. This surface is depository, and the inner endosteal side of the cortex is resorptive. Together with deposition of bone along the entire length of the posterior margin of the ramus, periosteal deposits on this large expanse of the buccal side of the ramus bring about continued posterior growth and relocation. In the anterior buccal part of the ramus, periosteal deposits continue directly onto the prominent trihedral eminence of the mandibular body.
A common variation may occur in which a vertical zone of surface-resorptive endosteal bone extends from the neck just in front of the posterior border of the ramus down to the gonial angle (Fig. 56). This is associated with a transient zone involved in reducing the thicker posterior margin during its relocation into the ramus proper as the whole ramus grows posteriorly.
THE LINGUAL SIDE OF THE RAMUS. AS seen previously, that part of the ramus on the lingual side located anteriorly and superiorly to the oblique ridge extending down from the
Figure 50a. This section was taken from the anterior crest of the condylar neck as it grades into the sigmoid notch. The lingual side is indicated by L. This surface (A) was depository. The opposite buccal surface (B) was undergoing corresponding surface removal of the same periosteal bone previously deposited on the lingual side. The entire cortex was drifting in a direction toward the right. X 12. (From Enlow, D. H., and D. B. Harris: Am. J. Orthodont., 1964.)
Figure 50b. Coronoid process. The lingual side (L) is characteristically depository, and the contralateral buccal surface (left) is resorptive. This
combination produces a movement of the coronoid process in a cephalic and posterior course, because the lingual surface faces these directions. X25 .
Figures 50c and d. In the area of the ante-gonial notch, the basal margin is composed entirely of endosteal bone, and its surface is characteristically resorptive (as in d). Just anterior to the notch, however, the periosteal bone on the buccal side begins to encircle the endosteal cortex base (as in c). This reversal divides the section into a periosteal portion (A) and an endosteal region (B). X 25.
Figure 50

( 1 2 2 )
neck onto the ramus is characteristically depository in nature (Fig. 57). The cortical bone above this line is periosteal in type, and progressive additions function to produce growth in a superior as well as a posterior direction. This depository type of periosteal surface continues obliquely across the ramus and grades into the lingual tuberosity of the mandibular body superior to the mylohyoid line.
As in other parts of the ramus, growth in this area conforms to the V principle, as well as the principle concerned with surfaces facing directions of growth. The right and left halves of the mandible in this region form a horizontal V configuration. This entire area moves progressively in a posterior direction and increases in overall size. The inner aspect of the V, which is the lingual side in this part of the ramus, faces this direction, and periosteal deposits serve to move it backward. This particular pattern of growth functions to progressively reduce the dimensions of the more narrow base of the V. The result is a shift of this part of the posteriorly growing ramus in a medial (lingual) direction as it merges with the more medially positioned mandibular body, which itself continues to elongate in a posterior direction. Since the backward-growing ramus becomes successively relocated into the newly lengthened body, a direct remodeling conversion from one to the other takes place. This is accomplished by a pronounced lingual shift of the ramus in this particular area. Periosteal deposits of bone on the lingual side move the area formerly located as the anterior basal part of the ramus into line with the more lingually situated axis of the body and dental arch.
Below the ridge of the mandibular neck and the mylohyoid line, the periosteal surface on the lingual side of the ramus is predominantly resorptive (Fig. 57). The characteristic medial mandibular reversal (page 259) follows this ridge, and it marks a prominent change in
Craniofacial bone growth
topographic contour. Its cortical bone is endosteal in type. In Figure 57 it is seen that the resorptive zone on the lingual side of the condylar neck descends in an obliquely forward direction and extends across the entire breadth of the ramus into the resorptive submandibular fossa of the body. In the neck, this surface-resorptive zone is concerned with condyle-to-neck remodeling and reduction in diameter. As the resorptive zone crosses the ramus, however, its functional basis changes. Note that the main portion of the ramus has a curvature following an anterior-posterior plane. The arc of this horizontal curvature is such that the posterior border is positioned more medially than the midportion of the ramus, which is curved in a lateral (buccal) direction. At the midpoint of the ramus, near the foramen, both the buccal and lingual surfaces are lateral to respective points on the posterior border. Recall that one function of cortical drift is to sequentially align the cortex along moving planes of curvature. Comparison of the buccal and lingual sides of the ramus shows an opposing pattern of depository and resorptive surfaces. In general, the upper part of the ramus, including the neck and coronoid process, is depository on the lingual side but resorptive on the buccal side. In the lower part of the ramus, the opposite combination occurs. The basis for this pattern of cortical drift in the various upper parts was outlined previously. The remodeling pattern characterizing the lower portion of the ramus brings about a progressive, continuous drift of the entire buccal and lingual cortical plates in a lateral (buccal) direction. This movement produces a constant shift of former areas occupied by the posterior border in a lateral manner in order to bring them into line with the horizontal curvature of the ramus. The posterior border, as it moves back, is thus progressively and sequentially remodeled into the remainder of the

The mandible
posteriorly growing ramus. Lateral cortical drift also widens and separates the lower portions of the two rami from each other, although this movement is not nearly as marked as their posterior manner of growth.
The entire length of the posterior edge of the ramus, as previously mentioned, is depository. This is associated with the predominantly backward course of ramus growth and movement. Together with the condylar head, this portion of the ramus represents one of the most active growth areas in the whole mandible in terms of distance covered and total amount of new bone deposited.
The depository posterior border forms a cap of periosteal bone that extends onto the lingual surface of the ramus for a short distance (Fig. 51, left). This is related to the inward (lingual) flare along the border. A resorptive reversal occurs on the lingual side, and as the posteriorly moving ramus becomes relocated in a backward course, the cortices are then shifted toward the buccal side. This cap of periosteal bone is seen to extend noticeably farther onto the lingual side of the ramus in the region of the enlarged and downward growing gonial angle, and it continues forward to a point just behind the antegonial notch.
Just as the ramus as a whole moves in a progressively posterior direction by different combinations of resorption and deposition on its various surfaces, the mandibular foramen becomes relocated in a corresponding direction and manner. The prominent lingula and the postlingular fossa drift posteriorly by continuous resorption in the fossa together with periosteal additions on the backward moving surface of the lingula. The cortex in the floor of the fossa is composed of endosteal bone. A periosteal reversal occurs on the crest of the lingula, and here the resorptive surface abruptly terminates. This moves the protruding lingula in a posterior direction into the area
( 1 2 3 )
previously occupied by the fossa, which has simultaneously drifted posteriorly. The periosteal reversal on the crest of the lingula is marked by thick periosteal deposits that con tinue forward across the anterior part of the ramus on its lingual side to the temporal crest and down onto the lingual tuberosity. These growth areas are concerned with the abrupt medial shift of the ramus in line with the elongating mandibular body.
THE ANTEGONIAL REGION. It was seen that a prominent zone of actively growing periosteal bone caps the posterior margin of the ramus. This continues around the angle and base of the ramus forward to the antegonial notch (incisure). At this point a reversal occurs, and the periosteal manner of growth is interrupted in the segment occupied by this incisure. On the inferior margin of the notch, periosteal resorption takes place on the surface of an endosteal cortex (Fig. 54a). The cortical plate drifts in a superior direction, thus producing a local elevation that is responsible for the formation of the antegonial notch.
It is apparent that as the gonial region moves posteriorly, areas formerly held by this area become successively relocated into the area of the antegonial notch. Because the base of this notch lies at a higher plane than the gonial angle, the remodeling process just described serves to elevate the basal cortex from the gonial level to that of the antegonial incisure.
The antegonial notch grades anteriorly into the body of the mandible. Areas formerly occupied by the backward-moving notch, in turn, become relocated into the posterior part of the lengthening body. A reversal occurs at this point. The elevating basal cortex in the notch now undergoes a change in which the resorptive surface becomes depository. This lowers the level of the basal plane to that of the mandibular body. At the reversal junction, a

Figure 51 (left). This transverse section prepared through the condylar neck is similar to that schematized in Figure 47b. Lingual surface A, which is the crest of the sigmoid notch, has received periosteal deposits. A reversal occurs, however, as this region grades into the medial side of the neck. This lingual surface (area B) is resorp-tive, and the cortex is composed of endosteal, compacted cancellous (convoluted) bone that was formed as condylar dimensions became reduced during backward relocation. Surface C, which is the posterior edge of the ramus, is characterized by a depository surface associated with the backward direction of ramus growth. An arrow indicates the endosteal-periosteal reversal between areas B and C. On the buccal side, the surface of area D is resorptive beyond the reversal indicated by the arrow, and the cortex is composed of endosteal bone formed during condylar reduction. Surface E is resorptive as the anterior portion of
the neck grows in a cephalic direction toward side A. X 10. (From Enlow, D. H., and D. B. Harris: Am. J. Orthodont., 1964.)
Figure 51 (right). This is a vertical section through the posterior part of the mandibular body similar to the area schematized in Figure 54a. On the buccal side periosteal bone deposits have produced the trihedral eminence in area A. A characteristic remnant of endosteal bone is seen at E, and periosteal deposits at D have brought about a cephalic direction of growth on the superior surface of the posterior mandibular body. The lingual tuberosity grows in a medial direction by continued bone additions on the periosteal surface in area C. Surface B is resorptive, and its underlying cortex is composed of endosteal bone. Reversals are indicated by arrows. X 6. (From Enlow, D. H., and D. B. Harris: Am. ]. Orthodont, 1964.)
Figure 51

The mandible
two-layered cortex is present. The inner endosteal zone is produced at the time the notch becomes raised by periosteal resorption and endosteal deposition. Following outward reversal as this area undergoes relocation, the outer periosteal zone is then deposited, thereby lowering the basal margin to a level in line with the bottom of the downward-growing body.
In some species other than the human, such as the rabbit and pig, a form of remodeling adjustment in this area occurs that differs from the one just described. Instead of producing elevation of the antegonial incisure by surface resorption, a mechanism of differential growth is involved. The surface of this notch is depository, but by differentially more rapid and extensive growth along the basal border of the gonial angle and posterior mandibular body, a similar end result is obtained.
( 1 2 5 )
THE MANDIBULAR BODY. It has been pointed out in descriptions of the ramus that a remodeling transition occurs at the junction between ramus and body. This is a key process because it involves conversion of one major portion of the mandible directly into another. Because the shape, disposition, and relationships differ markedly between the ramus and body, this remodeling conversion involves an extensive series of sequential changes.
In the superimposed mandibles pictured in Figure 49c, several contrasting relationships are seen between the two growth stages. The mandible has enlarged in all dimensions. The predominant course of growth movement, however, is posterior, and the right and left condyles have become only slightly separated. The body has increased proportionately in breadth, and both the body and the ramus have become significantly lengthened. Note particularly
It is generally assumed that the ramus and coronoid process grow in the manner schematized in a. However, this is an oversimplification and is inaccurate (see text). It is sometimes further assumed that the expanses of bone indicated by X, Y, and Z in diagram b are passive during
growth, and that remodeling activity occurs primarily at the margins, as shown in a. This is also inaccurate, because these entire surfaces are directly involved in cortical growth movements (compare with Figures 47, 48, and 49).

Craniofacial bone growth ( 1 2 6 )
As a result of the various growth movements pictured in Figures 48 and 49, the posterior part of the mandibular body becomes lengthened by deposits on the lingual surface of the ramus as it grades into the lingual tuberosity ( b ) . This tuberosity is at the same time being undercut by endosteal growth with periosteal resorption (white
arrows, c) as the body now grows in a buccal and cephalic direction. Periosteal deposits on the buccal cortex form the trihedral eminence and serve to enlarge the entire posterior mandibular body in an outward direction. (From Enlow, D. H., and D. B. Harris: Am. ]. Orthodont., 1964.)
Figure 53

The mandible
that the body elongates into regions previously held by the ramus, which in turn is moving in advance of the backward lengthening body. In this figure, the coronoid process and most of the ramus of the younger bone are within the area occupied by the body of the older bone.
The complex remodeling changes involved in the growth movements of the ramus, coronoid processes, lingual tuberosities, etc., are all interrelated in the various combinations of cortical movements that in the end provide a full mandibular arch which simultaneously has become displaced in a forward manner. It also becomes lowered to a position that accommodates the downward growth of the upper jaw.
The body of the mandible, it is emphasized, is growing continuously into successive areas previously occupied by the posteriorly moving ramus. This latter part of the mandible in turn becomes progressively relocated behind the backward moving condyles and posterior edge of the ramus. The posterior portion of the body becomes consecutively converted from the former ramus of an earlier growth stage by direct structural remodeling. This is a continuation of the V mechanism seen in different parts of the ramus. New bone deposits are added onto the inside (lingual) surface of the V-shaped, anterior portion of the ramus and posterior portion of the body as they both move posteriorly toward the wide end of the V.
Note that the entire mandibular body with its dental arch lies on an axis or line positioned well toward the midline from the ramus. The successive relocation of the old ramus into the elongating body requires a distinct shift in a lingual direction in order to carry the lengthening posterior body into a symmetrical line with the axis of the dental arch. By the progressive addition of new periosteal bone on the lingual surface, which faces the actual posterior (and cephalic) direction of ramus growth, the an-
( 1 2 7 )
terior part of the ramus thereby grows and moves in a lingual direction to accommodate alignment with the growing body. The lingual addition of bone thus serves to bring the basal part of the V toward the midline. This provides successive relocation of the ramus, during this conversion, into the more lingual position of the elongating body and dental arch. The anterior part of the ramus merges with the prominent lingual tuberosity of the body. This tuberosity grows and moves in both lingual and posterior directions as the body lengthens by massive periosteal additions on its medially facing surface (Figs. 53 and 54a).
The distinctive resorptive nature of the anterior edge of the ramus, as it merges with the dorsum of the body, is sometimes described as the means by which additional space for the third molar is provided. This is true, but the relationship is necessarily more complex, because a primary function of this resorptive anterior surface is its posterior movement in conjunction with the backward growth of the entire ramus and conversion from ramus to body during the relocation of one into the other. It is noted also that the inward projecting lingual tuberosity, housing the posterior molars, is particularly prominent in the human mandible, a factor apparently associated with wide condylar placement and a relatively narrow, short dental arch.
THE SUBLINGUAL FOSSA. In Figure 57, note that the broad resorptive band extending forward from the condylar neck obliquely down and across the lingual side of the ramus continues directly into the deep fossa located basally to the lingual tuberosity and mylohyoid line. The cortex in this fossa is composed entirely of inward growing endosteal bone, just as it is in the continuation of this resorptive zone in the ramus. A complex sequence of remodeling adjustments occurs in this region, as

( 1 2 8 )
seen in the series of transverse sections pic
tured in Figure 54. First, the l ingual tuberosity
above the fossa becomes shifted toward the
midline by massive deposits of periosteal bone.
T h e tuberosity itself is concerned with sup-
Craniofacial hone growth
porting the posterior molars and is aligned as
a medial projection to bring the posterior body
in line with the axis of the dental arch. T h e
fossa basal to the tuberosity, however, under
goes a different mode of growth. Its periosteal
A complex sequence of remodeling changes takes place during the growth of the mandibular body. The series schematized here corresponds to the photomicrographs in Figures 51 (right) and 55. A "buccal drift" of the posterior mandibular body is seen in a, b, and c as bone is added on the buccal side with corresponding resorption and endosteal bone formation on the lingual side. An area of periosteal bone deposition on the lingual surface has produced the lingual tuberosity. In d
only a thin zone of endosteal bone remains on the lingual side of the mandible as both the buccal and lingual cortices now increase in overall size by periosteal additions. In the area of the chin ( e ) the cortex on both sides grows in a generally lingual direction with some periosteal deposits being added at the apex of the chin itself. (Adapted from Enlow, D. H., and D. B. Harris: Am. J. Orthodont., 1964.)
Figure 54

The mandihle
surface is resorptive and the cortex is composed of endosteal bone. The resulting growth movement serves two functions. First, it moves the area in a buccal direction, opposite to that of the prominent overhanging tuberosity above it. This shifts the basal part of the posterior body laterally to keep pace with the rest of the mandibular body as it increases in overall dimensions in a buccal direction. It brings the basal margin into symmetrical line with the continuous contour of the enlarging mandibular body, trihedral eminence, and ramus. Second, the endosteal mode of growth in this fossa progressively undercuts the recently formed periosteal bone of the upward-growing lingual tuberosity located just above it. The combination brings about increases in the vertical dimensions of the body in this region. Thus, contrasting directions of cortical drift take place during the complex sequence of remodeling changes in the critical posterior portion of the elongating body. The superior portion on the lingual side drifts medially, and the inferior part drifts laterally. The entire cortex on the buccal side moves laterally.
THE TRIHEDRAL EMINENCE. The characteristic depository type of surface on the buccal side of the posterior mandibular body is a continuation of the broad depository zone extending across the ramus below the sigmoid notch and coronoid process. These periosteal deposits in the posterior portion of the body produce the bulbous trihedral eminence. On the inferior basal margin of the body in this region, the transition zone between the ante-gonial notch and the body occurs, so that gradual coverage by periosteal bone is found extending onto the basal margin from the buccal cortex as the antegonial notch grades into the body. Serial transverse sections prepared through this general area show the periosteal bone of the buccal side extending progressively
( 1 2 9 )
farther around the base until it completely caps it in the region of the last molar (Fig. 54).
The sloping cortical ledge located above the trihedral eminence just lateral to the molars shows a distinct reversal where the ramus merges with the body. Here, the resorptive surface on the anterior margin of the ramus changes to the depository periosteal cortex in this part of the body. The superiorly and laterally facing cortex of this ledge receives continued bone deposits that move it upward, with the moving teeth, and outward as the entire area becomes both lengthened and broadened.
THE MANDIBULAR ARCH. It has been seen that the several major components in the posterior portions of the mandible become progressively relocated in a general posterior course during growth. Thus, the condyle, coronoid process, ramus, gonial angle, lingula and its fossa, lingual tuberosity, posterior end of the body, trihedral eminence, and the antegonial notch all become successively moved backward (as well as in several other divergent directions). They are sequentially repositioned, one location to the next, as each area moves into the old position of the region just posterior to it. This pattern of consecutive movements represents the essential plan of continued growth, and it is the basis for the many remodeling processes associated with progressive mandibular structuring.
The various anterior-posterior levels within the mandibular body similarly undergo sequential shift in positions as the whole body becomes lengthened. The "molar" level at a very early growth stage, for example, is relocated to become the "premolar" area of a later stage, and in turn former premolar levels become sequentially positioned into the new cuspid region as a consequence of the elongation of the mandibular arch.
The bone tissue in any given area of the

( 1 3 0 )
mandibular arch should not be visualized as fixed or permanent in character, nor should the particular bone tissue in association with any tooth be viewed as stable in its relationship. As the mandibular bone grows and as area relocation proceeds, constant rebuilding of bone tissue occurs in relation to structural remodeling, and continuously changing relationships take place. The bone supporting any tooth and the level of the mandible occupied by that tooth do not represent the same actual bone tissue and level at succeeding growth stages. The remodeling adjustments associated with growth itself, which represent the sum of the various changes described in this chapter, are the factors underlying these complex growth processes. The drifting of teeth further contributes to the changing relationships that occur during these continuous remodeling adjustments as the whole bone grows (page 87).
The basic growth pattern present in the ramus-body transition continues directly into the posterior body and then forward to the anterior part of the mandibular arch. In this general region, however, several growth differences occur. The broad resorptive zone that begins on the lingual side of the neck just beneath the condyle extends obliquely downward and forward across the ramus and passes beneath the lingual tuberosity. It then continues forward to about the level of the canine or first premolar (Fig. 57). The differing functional relationships of this zone at each different level from the neck to the sublingual fossa have already been described. In the forward part of the mandibular arch, this resorptive zone narrows progressively until it terminates. Its functional role is comparable to that seen beneath the large lingual tuberosity. It provides (1 ) proportionate cortical drift in a buccal direction by the formation of endosteal bone, and (2 ) it undercuts the diminishing ledge found in this alveolar area. The result is
Craniofacial bone growth
a lateral movement of the lingual cortex associated with the widening of the mandibular arch and an elevation of its superior portion as the entire arch becomes heightened. This gradually narrowing resorptive zone terminates as it enters the genial region opposite the chin where contours and relationships abruptly change. The entire genial area is characterized by periosteal bone deposition on this lingual side of the mandibular arch.
On the buccal side, the whole mandibular arch is depository in nature except, characteristically, the mental region, which will be discussed in the next section. The entire basal portion of the arch is also depository. This enlarges the inferior border of the mandible in a downward direction in proportion to the increasing overall contours of the growing mandibular arch. The thickness of the basal cortical plate is increased at the same time. This downward growth of the mandibular body is less extensive in actual distance covered than the opposite upward manner of growth movement in the alveolar region (see Chapter 10).
Serial sections prepared through the arch of the mandible from the lingual tuberosity to the chin show a characteristic succession of changes (Fig. 54). In the posterior region of the body, the periosteal surface of the buccal cortex is primarily depository. Its superior surface, however, is resorptive in conjunction with the remodeling conversion from ramus to body. The lingual tuberosity is depository, but the fossa beneath it is resorptive. The inferior border is also resorptive in relation to remodeling changes in the antegonial notch. As serial sections are examined toward the chin, the resorptive zone on the lingual side gradually becomes narrowed as periosteal deposits continue around the basal margin progressively farther onto the lingual surface. The prominent ridge extending forward from the lingual tuberosity becomes correspondingly less promi-

The mandible
nent. In the genial region behind the mental protuberance, this resorptive zone ends, and the lingual cortex becomes entirely depository.
THE CHIN. The mental protuberance of the mandible, like the overhanging bony nose on the maxilla, is a unique anatomic feature of man. Because of this, the growth and remodeling processes associated with this region are basically different from those found in other species.
The diminutive chin of the young mandible becomes progressively more prominent with increasing age. The growth changes that bring this about involve a differential combination of surface resorption and deposition in the different parts of the mandibular arch in the general region forward of the bicuspids. This area is noticeably flattened in the human mandible and does not have the typically pointed configuration found in the muzzle of most other forms. The entire mandibular arch is "reduced" in conjunction with the correspondingly short and flattened maxilla. The chin appears to be a structural adaptation related to this overall reduction. The factors involved are discussed in Chapter 8.
Growth patterns in the area of the chin are quite variable (Fig. 56), more so than in most other parts of the mandible. Perhaps the most typical combination of remodeling changes is seen in Figure 54e. The protuberance itself is usually marked by massive deposits of periosteal bone. The cortex is thick, dense, and composed of typically slow-growing types of lamellar bone (Fig. 55d). These periosteal deposits encircle the base and continue onto the lingual side where they extend for the full height of the lingual cortex in the genial region. The maturation of the chin in shape and size proceeds slowly through the postnatal period of facial growth.
As the mental protuberance grades into the
( 1 3 1 )
alveolar region above it, a characteristic reversal occurs. Here, the cortex is composed of typical endosteal bone, and its external (periosteal) surface is resorptive. The positioning of the reversal line varies, however, a factor that appears to be associated with the marked variation in morphology and dimensions of this region among different individuals and differing bony adjustments involved in occlusion with the growing maxilla.
The combination of continued periosteal deposition around the base and apex of the chin, together with periosteal resorption and endosteal deposition in the alveolar region above it, serves to progressively enlarge the whole mental protuberance and change its contour. The alveolar region undergoes cortical regression and moves posteriorly while at the same time the protuberance continues to grow forward. This brings about an increasing projection of the chin and emphasizes its prominence. The resorptive, endosteal nature of the area superior to the chin is a primary remodeling factor that contributes to the flattened configuration characterizing the anterior part of the mandibular arch in comparison with other species having a more pointed lower jaw (see page 182).
MUSCLE ATTACHMENT ON RESORPTIVE SUR
FACES. It has been seen that resorptive periosteal surfaces are extensively distributed in different parts of the mandible (as well as in most other bones). It is apparent also that many of these outer resorptive surfaces are involved in muscle attachment. The connective tissue component of the muscle inserts directly into the regressive, inward-growing cortex. The resorptive anterior border of the coronoid process is an example of such an area. This relationship must be taken into account when analyzing the influence of muscle pull and stress on the morphology of a developing bone.


The mandible
In such areas, muscle function is associated with cortical recession rather than with periosteal deposition (see pages 81 and 100). This factor disagrees with the commonly held notion that muscle pull determines a bone's shape solely by inducing the apposition of new bone on surfaces just deep to the attachment of the muscle.
APPLICATION OF GROWTH PRINCIPLES TO
THE DEVELOPMENT OF THE MANDIBLE. The
basic principles of bone growth previously described in introductory chapters and briefly summarized on pages 105-108 provide a mor-phogenetic basis for interpretations of mandibular development. In order to relate their application to craniofacial growth in general, these various concepts are outlined below in conjunction with the growing mandible.
( 1 3 3 )
GENERALIZED SURFACE GROWTH. It is ap
parent that the mandible does not increase in size by a process of proportionate bone deposition on all its outer surfaces in a manner that simply follows the established contours of these surfaces. The nature of surface activity differs significantly throughout the various parts and regions of the whole mandible. Local surface contours constantly become changed during growth as a consequence of relocation and remodeling (Fig. 58).
CENTERS OF GROWTH. If overall enlargement is assumed to be primarily a result of activity in the two or three "growth centers" of a bone, increasing mandibular size would then be essentially a product of growth at the condyle, posterior and anterior borders of the ramus, and the alveolar ridges. This is not the
Figure 55a. The level of the vertical section through the mandibular body pictured here is represented by Figure 54b. The lingual side is represented by L. Surface A shows periosteal deposits that have formed the massive trihedral eminence. Periosteal deposition in area B extends farther around the basal margin than in Figure 51. A reversal occurs at the arrow, and the surface in area C is resorptive; its cortex grows in an endosteal direction. In area D periosteal deposits form the lingual tuberosity. X 5. (Photomicrographs on this plate are from Enlow, D. H., and D. B. Harris: Am. J. Orthodont., 1964).
Figure 55b. This section corresponds to the approximate level illustrated in Figure 54c. Areas D, C, and A follow the same growth patterns seen in corresponding regions of Figure 55a above. Note that periosteal deposits continue to extend farther around the basal margin. The periosteal-endosteal reversal occurs at the point marked by the arrow. Both the buccal and lingual cortices
undergo cortical drift in a lateral direction by periosteal deposition on surface A and endosteal deposition in area C. The lingual side is represented by L. X 5.
Figure 55c. The approximate level of the mandibular body corresponding to this section is indicated by d in Figure 54. Periosteal deposition on surfaces A and D serves to enlarge the dimensions of the body proportionately as the whole bone increases in overall size. Periosteal deposits have now completely encircled the base, and only a narrow zone of surface resorption remains in area C. The lingual side is indicated by L. X 4.
Figure 55d. The region of the chin seen here is characterized by a resorptive, regressive alveolar surface (A). The endosteal side is depository. A reversal occurs on the mental protuberance (arrow). (See also Figure 54e.) The entire contralateral lingual surface (c) is depository. The base is entirely depository in nature. The lingual side of the section is indicated by L.
Figure 55

( 1 3 4 )
case, however, because virtually all other parts of the entire bone contribute directly to multiple, interrelated growth changes in conjunction with the sites just mentioned. The mandible as a whole thus represents a multitude of active growth sites comprising all the regional
Craniofacial bone growth
periosteal and endosteal surfaces throughout the bone (Fig. 58).
GENERALIZED SURFACE GROWTH FOLLOWING
CESSATION OF GROWTH-CENTER ACTIVITY.
This misconception has been more often ap-
Common variations in endosteal-periosteal cortical patterns. Compare with Figure 57. Solid white lines indicate surfaces that grow by additions of periosteal deposits. Dotted lines represent surfaces that undergo resorptive removal during growth and remodeling. The incidence of occurrence in
the 25 mandibles studied is indicated for each variation: a, 6 specimens; b, 6 specimens; c, 4 specimens; d, 11 specimens; e, 4 specimens. X 4. (From Enlow, D. H., and D. B. Harris: Am. J. Orthodont., 1964.)

The mandible
plied to the maxilla, but it is also relevant to the mandible. For example, when growth activity of the condylar mechanism ceases, it should not be assumed that the entire mandible then continues to grow by simply adding new layers of bone onto all its periosteal surfaces. This false notion violates the other growth principles that are indeed involved in progressive growth (see also discussion of the nasomaxillary growth mechanism).
GROWTH IN CONJUNCTION WITH REMODEL
ING. It is apparent that successive growth additions at the condyle, posterior border of the ramus, etc., require corresponding remodeling adjustments throughout all parts of the mandible in order to adapt dimensions and regional shape to these increases. The changes involved occur simultaneously, and virtually all surfaces are active as these complex remodeling movements proceed in various directions during overall growth.
( 1 3 5 )
RELOCATION. The process of relocation is the key factor that underlies the basis for continued remodeling as the mandible increases in size. For example, as bone is added onto the various posterior surfaces of the ramus or the apex of the coronoid process, all other parts and levels down the line necessarily undergo shifts in relative position. Thus, a former portion of the ramus becomes changed into a part of the new body, and a former area of the coronoid process becomes remodeled into a segment of the enlarged ramus beneath it as all undergo increases in size. These changes are progressive and sequential, and they repeat themselves continuously until growth terminates.
SURFACES FACING DIRECTIONS OF GROWTH.
This principle applies to all parts of the growing mandible, including both the endosteal and periosteal sides of each cortical plate. It reflects the many divergent directions of
The distribution of resorptive and depository periosteal surfaces in the human mandible are mapped in these drawings. Periosteal surfaces that undergo progressive removal during growth are
indicated by dark stippling. Outer surfaces that are depository in nature are indicated by light stippling. See text for further descriptions.

( 1 3 6 )
growth movements that occur as the bone increases in size. It also provides a basis for understanding the complex patterns of distribution of resorptive and depository surfaces throughout the mandible in conjunction with the other basic growth principles (Fig. 58).
Craniofacial bone growth
GROWTH AND DISPLACEMENT. Growth and displacement are to be considered in greater detail later (Chapter 10) so that composite growth patterns in all areas of the face can be evaluated. It is evident, however, that in the mandible predominant directions of growth and
The composite of the various regional growth and remodeling movements that occur in the human mandible are summarized in this drawing.
See text for detailed descriptions of each area. (From Enlow, D. H., and D. B. Harris: Am. ]. Orthodont., 1964.)
Figure 58

The mandible
displacement directly oppose each other. Actual growth proceeds largely superiorly and posteriorly, but displacement involves an anterior and inferior manner of movement. This displacement is a consequence of mandibular growth itself together with growth activity in the maxilla, the cranial base, and facial soft tissues. Thus, the mandible becomes projected forward, but actual growth in the forward area at the chin itself is relatively slight. The marked lengthening process taking place at posterior ends represents the dominant mode of enlargement.
( 1 3 7 )
THE V PRINCIPLE. A number of prominent mandibular regions conform to the V growth mechanism, as previously seen, and they all follow a characteristic growth pattern in which successive deposits are laid down on the inner sides of a V-shaped structure. These surfaces face the actual direction of growth. The enlargement of the V involves (1 ) sequential relocation of wider parts into more narrow areas, (2 ) an actual movement in a direction away from the narrow end of the V, and (3 ) an increase in the size of the entire region.

( 7 )
The nasomaxillary
complex
The upper face is traditionally regarded as an area that grows "forward and downward." This concept is an oversimplification. The remodeling patterns found in the numerous individual bones that comprise the face are quite complex and involve regional growth movements that proceed in many divergent directions, all simultaneously. There is also the factor of displacement as the different bones grow in relation to one another and the cranial base in an interrelated composite of growth movements.
The maxilla does not, for the most part, simply grow forward and downward. Actual growth (not displacement) takes place in a variety of regional directions, many of which do not follow an anterior and inferior course. The growth of the maxilla has often been explained on the basis of three fundamental growth centers, including the sutures, the posterior maxillary tuberosity, and the alveolar
138
margins. It is sometimes implied that virtually all maxillary enlargement is a direct consequence of growth at these centers. Growth activity at the many other surfaces and regions in the bone is either not considered, or it is regarded as secondary. This belief, like the forward and downward concept, is misleading and inaccurate. A basic and equally significant process of remodeling growth also takes place in conjunction with growth at the other sites, and it involves virtually all endosteal and periosteal surfaces throughout the entire bone.
It has often been held that the maxilla grows primarily by "generalized surface deposition" subsequent to cessation of suture activity. This is also an inaccurate concept, as will be shown in following pages.
The growth of the nasomaxillary complex conforms to the same basic principles that were previously applied to the development of

The nasomaxillary complex
the mandible, as described in detail in the introductory chapters and briefly summarized on pages 105-108. Growth is not simply a uniform, proportionate expansion of the whole bone. It does not grow by adding new deposits in a manner that merely continues existing surface contours. Growth is instead a composite process involving bone additions at sutures, extensive surface deposition in certain other specific regions, and at the same time companion remodeling growth on all inside and outside surfaces. Remodeling growth functions to ( 1 ) increase the dimensions of the local parts and areas of each bone, and (2 ) reshape these local areas in order to maintain the constant configuration of the whole bone as it enlarges. The remodeling processes of resizing and reshaping are a direct consequence of relocation. As in the mandible, growth additions in the nasomaxillary complex produce a constant relocation of all its parts. Corresponding adjustments in size and shape take place throughout all areas of each component bone in a constant, sequential manner. Thus, the entire bone is active during growth, and the remodeling processes accompanying growth involve complex patterns of surface resorption and deposition in each regional area in response to overall increases in size.
In the present chapter, the specific processes that contribute to the composite growth mechanism are described and explained. Each individual area in the nasomaxillary complex is analyzed, and its role in the morphogenesis of the whole bone is discussed. The general picture of overall growth in all the facial bones in relation to each other will be evaluated in Chapter 10.
GROWTH CENTERS IN THE FACE. Unlike the mandible, long bones, and parts of the cranial base, the membranous bones of the middle face do not have an intrinsic endo-
( 1 3 9 )
chondral mechanism associated with linear growth. These dermal bones do, however, have a sutural growth process that contributes to elongation. Sutural and epiphyseal mechanisms, however, are basically dissimilar in character and are not directly comparable. They represent two different systems of growth, each adapted to different growth circumstances. The endochondral apparatus provides continued elongation in a field of pressure, and as the contiguous bones grow toward each other, resultant displacement in an opposite direction occurs. Thus, the mandibular condyle (like the epiphysis of the humerus) moves in a direction toward its articulation through new bone formation produced by the pressure-adapted endochondral growth mechanism. The growth of the functional matrix associated with the mandible, however, is believed to contribute to the process of displacement.
The sutural growth process does not ordinarily involve resultant separation of bones as a direct consequence of progressive bone additions on contact surfaces, which would be comparable with the pressure system of growth utilized in the epiphyseal mechanism. Instead, adjacent interlocking bones become separated by growth forces produced in other tissues. As this occurs, new bone becomes correspondingly added on sutural surfaces as a response, thereby keeping the bones in contact. Bone deposition is passive and secondary in nature. It is a consequence of bone displacement rather than a cause. Bone deposition on sutural surfaces ordinarily occurs in a field of tension, unlike endochondral proliferation, which occurs under direct compression.
In the calvaria, the expanding brain represents an underlying force that contributes to the displacement of its covering flat bones. Within the face, the soft tissue that is believed to pace sutural separation is the enlarging nasal

( 1 4 0 )
septum (Scott, 1953a). Because this structure is composed largely of cartilage during earlier growth stages, it is capable of growth and interstitial expansion in the presence of pressure involved in moving facial bones away from the cranial base. Future studies may show that the overall mechanism involves other contributing factors, but this vertically oriented cartilage plate appears to be a force associated with continued displacement of the facial bones. Thus, as these bones become moved ahead of the expanding septum, corresponding additions of bone at the various facial sutures passively function to maintain the bones in continuous sutural contact and to enlarge them in a linear manner.
The factor of sutural bone deposition requires extensive structural remodeling in the various other parts of the bone as a companion adjustment process. The progressive addition of new sutural bone results in direct relocation, down the line, of the successive levels behind the sutural surface. Consequent reshaping and resizing occur as each area becomes sequentially repositioned into the next. As in the mandible, relocation is the key factor that underlies continued remodeling changes. It provides, simultaneously, progressive increases in overall size in each regional area throughout the whole bone.
Certain sutures are oriented so that they face obliquely in several directions, such as anteriorly, inferiorly, and laterally. Growth additions, however, can produce enlargement in a selected direction. The zygomaticotemporal suture, for example, faces forward and downward, but its predominant course of bone growth follows ,a horizontal anterior-posterior direction (Gans and Sarnat, 1951). The fronto-maxillary suture faces a similar direction, but its bone growth proceeds in a largely vertical course. These two sutures, in combination, contribute to a composite forward and down-
Craniofacial bone growth
ward displacement. In a series of experiments using implants, Gans and Sarnat have demonstrated the nature of growth contributions in the individual facial sutures of different laboratory animals, including the Rhesus monkey. They have demonstrated the passive, secondary nature of sutural bone growth, and they have also provided experimental evidence that the nasal septum represents a primary source for this growth stimulus.
It is sometimes held that a facial bone can continue to grow by "generalized surface deposition" subsequent to sutural growth activity. As pointed out earlier, the generalized surface-deposition concept in any bone, including the maxilla, is inaccurate. Furthermore, it would not be possible for all other parts of a bone to increase significantly without corresponding increases at sutural margins. The suture is one of several basic surface types, and all surfaces are necessarily involved during proportionate growth. The bone surfaces in sutural junctions must be active throughout the generalized growth period so that the enlarging bone, as a whole, will maintain its symmetrical shape and dimensions. Although some sutures, such as the intermaxillary, show a lesser extent of growth activity, others must necessarily continue to function in bone deposition during the growth period so that the distance between two sutures can be extended to permit the enlargement of the intervening bone.
THE MAXILLA. In the interpretation of
overall nasomaxillary growth, the basic processes of actual growth must be distinguished from the process of displacement that is a consequence of growth. The interrelations between them will be considered in a subsequent chapter. It is necessary first to consider the growth pattern of the maxilla as a separate and independent bone. A predominant direction of

The nasomaxillary complex
growth in the maxilla, like the mandible, is posteriorly, with displacement occurring in an opposite anterior course (Figs. 60a and b). Another major direction of maxillary growth is superiorly, with corresponding inferior displacement. The many parts and areas of the whole maxillary bone, however, grow in a complex variety of other regional directions, and the entire bone becomes involved in these multidirectional growth movements.
THE MAXILLARY TUBEROSITY. AS the en
tire maxilla becomes displaced in an anterior direction, new bone deposits are progressively added onto the periosteal surfaces of the maxillary tuberosity (Fig. 59). This surface faces posteriorly, and continued bone deposition results in a direct posterior course of growth. The anterior-posterior dimensions of the growing maxilla are thereby increased, and the
( 1 4 1 )
dental arch is lengthened as the teeth increase in number or undergo replacement.
The posterior face of the tuberosity represents one of the most rapidly growing areas in the maxilla. Its cortex, during active periods of growth, is composed typically of fine cancellous, nonlamellar bone tissue, a type associated with rapid accretion. This bone tissue may subsequently undergo lamellar compaction. As growth slows, however, the composition of the cortical plate then becomes characterized by more slowly growing types of lamellar bone containing variable numbers of primary vascular canals.
As bone is progressively added onto posterior facing surfaces during the generalized posterior mode of maxillary growth, relocation of all the parts anterior to these surfaces occurs as a consequence. This factor is associated with a number of corresponding, extensive remodel-
The distribution of regional depository (light stippled areas) and resorptive (dark stippled areas) surfaces are mapped in this diagram. The white zones ( t) represent areas in which variation
normally occurs in placement of the reversal line between resorptive and depository surfaces. See text for further descriptions.
Figure 59

( 1 4 2 ) Craniofacial bone growth
Diagram a is an interpretation of posterior growth of the maxillary arch and the zygomatic processes. Bone growth proceeds along the entire inner (lingual) side of the arch as well as along its posterior margin (maxillary tuberosity) and the posterior face of the zygomatic process. Re-sorptive removal occurs from the outer cortex of the premaxillary area and from the anterior surface of the zygomatic process. Diagram b schematizes the apparent direction of growth which results from the anterior displacement of the maxillary body accompanying its actual growth in a posterior direction. Diagram c illustrates the mechanism of posterior and lateral movement of the combined zygomatic process of the maxilla
and the adjacent zygomatic bone. Bone deposition (+) proceeds in lateral and posterior directions (arrows'), together with complementary resorption (—) from anterior and medial surfaces. The generalized mode of maxillary growth and remodeling parallels that of the human mandible, shown here for comparison ( d ) . During posterior growth of the condyle and ramus, the coronoid process is continuously relocated in a posterior direction (arrows). Similarly, the zygomatic process of the maxilla also receives proportionate posterior relocation as the maxillary body grows in this direction. (From Enlow, D. H., and S. Bang: Am. ]. Orthodont., 1965.)

The nasomaxillary complex
ing changes that take place in other areas of the bone.
THE ZYGOMATIC PROCESS OF THE MAXILLA.
In Figure 60c, it is seen that the anterior and posterior sides of the protruding zygomatic process differ in their growth patterns. The forward-facing anterior side, comprising a portion of the cheekbone, has a periosteal surface that is resorptive. Its contralateral endosteal surface is depository. The backward-facing posterior side, however, is depository, and the opposite endosteal surface of its cortex is resorptive. This produces a posterior growth movement of this laterally projecting zygomatic process. The cortical plates of both the anterior and posterior sides drift backward together in conjunction with the posterior growth of the adjacent maxillary tuberosity.
As seen above, the posterior surface of the maxillary tuberosity faces the direction of posterior growth, and additions of periosteal bone bring about posterior elongation of the arch. These periosteal deposits continue directly onto the posterior face of the zygomatic process of the maxilla. The combined movements of the tuberosity and the zygomatic process are differential, however, so that the arch becomes lengthened to a greater degree than the backward shift of the zygomatic process. The basis for this differential extent of movement lies in the proportionate placement of the zygomatic process relative to the whole maxillary arch as it enlarges.
It is paradoxical that the forward-facing area of the cheek as well as some other facial surfaces are actually resorptive and regressive in character, since the whole face appears to grow directly forward. Two key factors are involved. One is concerned with the process of displacement; many parts of the face do not actually grow in a forward course but rather become displaced in this direction. Growth activities
( 1 4 3 )
occurring on the various forward-facing surfaces are essentially independent of this displacement process. The second factor associated with the resorptive nature of this anterior-facing part of the maxilla is its positional relationship during area relocation. If the cheek area were to actually move forward as the tuberosity grew posteriorly, the two would become disproportionately separated and the cheekbone would come to lie in a dissociated position far in front of its actual location. As new deposits of bone are added onto posterior surfaces of the tuberosity, the longitudinal dimensions of the whole maxillary arch become increased. However, constant relationships must be maintained between the various new and old parts of the entire bone. With successive additions on the posterior border, all areas down the line must necessarily be relocated into new positions because their old locations become shifted as a direct consequence of added growth. Thus, the resorptive anterior face of the zygomatic process, together with its depository posterior surface, serves to proportionately relocate the malar region in a continuous posterior direction as the whole maxilla becomes simultaneously lengthened by new growth on its posterior margin. This functions to constantly maintain malar position relative to the growing maxillary tuberosity, orbit, nose, cranial base, dental arch, and the premaxillary region.
An analogous growth pattern occurs in the mandible (Fig. 60d). It becomes lengthened in a posterior direction but becomes displaced in an opposite forward manner. It also grows superiorly with corresponding inferior displacement. As it grows posteriorly and superiorly, its parts and areas similarly undergo remodeling as a consequence of relocation in order to maintain proportionate positional relationships. The coronoid process of the ramus, like the zygomatic process of the maxilla, shifts back-

( 1 4 4 )
ward in conjunction with the posteriorly moving condyle, thereby keeping a constant but expanding relationship to it.
The cortex on the anterior side of the zygomatic process of the maxilla is composed of typical endosteal bone tissue. This bone is formed as the continuously moving, regressive cortical plate receives continued deposits on its endosteal surface. Because the medullary area in this region usually contains cancellous trabeculae, the resultant compact bone is of an irregular, convoluted type produced by cancellous compaction (Fig. 65k). In some regions, the trabeculae are more widely scattered, and inward growth produces layers of endosteal circumferential lamellae rather than convoluted bone. The endosteal cortex in the forward-facing zygomatic region of the maxilla continues directly into the anterior part of the maxillary arch as well as onto the front of the separate zygomatic bone, both of which are characterized by resorptive periosteal surfaces.
THE MAXILLARY ARCH. In Figure 59, note that a distinct line of reversal occurs along the ridge that extends down from the projecting zygomatic process onto the alveolar bone of the dental arch. The placement of this line is variable and may extend for greater or lesser distances forward into the premolar region. Posterior to the line, the cortical bone is of an outward growing, periosteal type associated with the posterior and slightly lateral growth of this region. Anterior to this line, the remainder of the external surface on the arch is resorptive in nature. A few scattered patches of periosteal bone may occur on outer alveolar surfaces in conjunction with eruptive remodeling, but these are localized situations that do not affect the basic endosteal growth pattern of the area as a whole. The characteristic resorptive surface is associated with a generalized process of cortical regression involving the for-
Craniofacial bone growth
mation of inward-growing, endosteal bone tissue. The basis for this growth pattern involves two remodeling factors.
First, the familiar V principle is applicable to the backward growth sequence of the whole maxillary arch. In Figure 60a, note the marked elongation at the free (distal) ends of the arch and, accompanying this, deposition of bone along the inner (lingual) side of the arch. Contralateral resorption occurs from the labial and buccal surfaces in the entire arch anterior to the malar region. The V-shaped maxillary arch thus increases in overall dimensions and at the same time becomes lengthened in a posterior direction toward its own wide end by a combination of deposition on the inner surface of the V with resorption from outer anterior surfaces. As in the growth and movement of any V-shaped structure, the narrower (anterior) portion becomes successively relocated into the wider parts, and the process of outer resorption and inner deposition serves to shift the cortex inwardly to accommodate this new position (Fig. 25). As a result, the superior portion of the arch (at an anterior-posterior level just below the nasal spine) becomes progressively shifted toward the midline as the entire arch expands laterally and posteriorly. Old, more narrow, areas of the enlarging V (the maxillary arch itself) come to lie in successive new locations that were formerly wider in their dimensions. The lingual direction of cortical growth functions to decrease this width in order to continuously maintain size proportions as the posterior ends and inferior margin of the maxillary arch both become lengthened.
The second consideration involves the complex contrasting nature of contours in different portions of the maxillary arch and the various directions their surfaces face during growth. Note the placement of the prominent reversal line that occurs along the vertical ridge extend-

The nasomaxillary complex
ing down from the zygomatic process onto the maxillary arch. This ridge separates the posterior portion of the arch from the anterior, and a basically different orientation of contours characterizes their respective surfaces.
Posterior to this reversal line, the periosteal surface is oriented so that it faces laterally, inferiorly, and posteriorly. Because this corresponds to the actual directions of growth in the particular region, continued periosteal deposition of bone results in the elongation and broadening of the posterior ends of the arch. Bone growth on the surface and along the free inferior margin of the alveolar cortex simultaneously increases vertical dimensions (Fig. 61a).
The extensive region anterior to this reversal line has a predominantly regressive cortex with a resorptive periosteal surface, in contrast to the depository nature of the surfaces posterior to the line. The periosteal surface in the anterior part of the arch in general forms a depression or a basin in the area below the orbit. The superior part of this basin is involved in the posterior movement that continuously repositions the entire malar region in a backward moving course in conjunction with posterior growth at the maxillary tuberosity. Note that the surface contour changes abruptly, however, as the cheek area grades into the region of the arch inferiorly and anteriorly to it. Here, growth circumstances change correspondingly. The cheek region faces anteriorly, away from its posterior direction of growth, and the outer surface is resorptive because the cortex grows essentially backward. That part of the arch in the premolar (bicuspid) area, however, has a predominant direction of growth that is essentially downward. Note that the outer periosteal surface in this region faces away from the direct inferior course of growth movement (Fig. 61b). The periosteal surface in the alveolar portion of the anterior maxillary arch
( 1 4 5 )
is therefore resorptive. Its cortex is composed of endosteal bone, and successive new bone deposits are added onto the medullary side of its cortical plate in conjunction with resorption from the periosteal surface. Thus, in general, outer surfaces in that portion of the maxilla located anteriorly and inferiorly to the orbit are characteristically resorptive in nature, and the formative basis for this pattern differs in the two major regions that comprise the area. The malar portion and the adjacent concave hollow just below the orbit are composed of endosteal bone because of their posterior mode of growth. On the other hand, the portion associated with the alveolar part of the arch is composed of a directly continuous cortex of endosteal bone that is concerned with a downward direction of growth movement. A distinct change in contour marks the separation between these two divergent growth areas. Even though the outer surface of the cortex in the anterior part of the arch is resorptive, the maxillary arch nevertheless increases in width. This is brought about in the manner illustrated in Figure 62b. Three planes of growth are thus involved simultaneously: anterior-posterior, vertical, and transverse.
The reversal line separating the posterior from the anterior portions of the maxillary arch becomes constantly shifted as a consequence of continued growth. Thus, the reversal line itself moves in a progressively posterior manner as the topographic contours that it separates become expanded during overall growth.
THE PALATINE PROCESSES OF THE MAXILLA.
As the posterior portion of the maxillary arch grows (1 ) backward by continued additions on the surface of each tuberosity, and (2 ) downward by deposition on buccal surfaces together with alveolar elongation, the right and left palatal shelves simultaneously undergo

( 1 4 6 ) Craniofacial bone growth
Marked differences are present in the surface contours of the maxillary arch anterior to the zygomatic process ( B ) and that part posterior to the zygomatic process ( A ) . Note that surface B is oriented so that its outer (periosteal) side faces away from the downward direction of growth. This outer surface is resorptive ( — ) . Surface A, in contrast, is oriented so that its outer side faces the direction of growth, which is downward as well as lateral; this surface is depository ( + ) The line of transition between A and B occurs along the ridge extending from the zygomatic process down onto the dental arch. As in area B,
the anterior face of the malar region is also resorptive, a condition associated with the posterior drift of the zygoma. The muzzle of the face grows downward by a combined process of periosteal resorption and endosteal deposition on the outer lamina of bone ( B ) . T h e nasal and oral sides of the palate move in a corresponding direction. Note that the arch simultaneously becomes widened by an elongation of the free (alveolar) margin. Thus, the arch becomes enlarged even though its outer surface is resorptive. This is an example of the V principle.

The nasomaxillary complex
complementary changes (Fig. 62). As previously seen, the maxillary arch itself forms a horizontally oriented V, and growth proceeds by deposition on its inner (lingual) sides with corresponding removal from some outer (labial) areas. The contiguous palatal arch, by comparison, represents a vertically oriented V.
( 1 4 7 )
Deposits are added onto the entire lingual surface of the palatal arch (the inner side of the V) . The roof of the oral cavity and the directly continuous maxillary arch on its lingual side are marked by periosteal types of bone tissue. The contralateral side of the palatal shelf is resorptive. This surface, which is
The oral palate (and floor of the nasal cavity) and the nasal spine move in a downward direction by bone deposition on the various inferior surfaces together with resorption from contralateral superior surfaces (a) . The premaxillary area simultaneously moves downward and somewhat posteriorly by an equivalent process. Following the principle of the V, the palate grows in an inferior
direction by subperiosteal bone deposition on its entire oral surface with corresponding resorptive removal from opposite surfaces (b) . The entire V-shaped structure thereby moves in a direction toward the wide end of the V and simultaneously increases in overall size. (From Enlow, D. H., and S. Bang: Am. J. Orthodont., 1965.)

( 1 4 8 )
the floor of the nasal chamber, moves downward in conjunction with the inferior movement of the labial surfaces on the maxillary arch. The combined result is a downward growth (drift) of the palate in conjunction with the downward movement of the remainder of the maxilla around it. As a result, the nasal cavity becomes greatly enlarged in vertical dimensions (page 242).
The maxilla as a whole thus has a configuration that involves two V-shaped arches—one vertically and the other horizontally placed. Directly continuous growth patterns bring about the expansion of each. In both cases, the inner (lingual) sides are depository, and the outer sides (labial cortex in the anterior part of the maxillary arch and the floor of the nasal cavity) are resorptive. By this growth process, each arch grows toward its own wide end producing a backward and, simultaneously, a downward shift of the whole maxillary arch. It becomes widened by this same growth process as the alveolar cortex becomes lengthened in an inferior direction.
The palatal shelves of the maxilla are quite thin in some regions of very young specimens, and the bony plate is composed of a single lamina of compact bone. New deposits are added onto the oral surface as bone is removed from the nasal side. The bone on the nasal side is actually of oral origin but has become translocated to the nasal side as a result of the downward drift of the entire cortical plate (Fig. 66c).
In most areas of the palate in older individuals, the bony shelves are relatively thick and are composed of two cortical plates separated by diploe. On the oral side, a substantial cortex of periosteal origin is characteristic; its endosteal surface is resorptive. The nasal cortex is composed of endosteal bone of a compacted, cancellous, convoluted type (Figs. 66d and 68b) because the cortical plate
Craniofacial bone growth
moves directly into the medullary diploe as it drifts in an inferior direction.
THE PREMAXILLA. In Figure 59, note the prominent reversal line that extends diagonally across the face. Its placement conforms to a change in surface contour that separates the nasal from malar and premaxillary areas. The periosteal surface inferior to this line is predominantly resorptive in nature, and the surface superior to it (the nose) is depository. A range of variation (t in Fig. 59) occurs in the position of this reversal line on either side of the infraorbital foramen.
It seems contradictory that the face as a whole grows forward, yet the forward-facing premaxilla itself is actually regressive in growth activity. As will be seen in Chapter 10, the anterior enlargement of the face is a composite cumulative result of a number of interrelated growth processes. In the human skull, however, premaxillary protrusion as a result of direct forward growth does not represent a dominant factor contributing to facial lengthening.
The premaxilla is composed of labial and lingual cortical plates separated by teeth or by interdental cancellous bone. The periosteal surface of the labial cortex is resorptive, as is the entire remainder of the maxillary arch anterior to the malar region. The endosteal side of the labial cortex is depository. The endosteal surface of the lingual cortex is resorptive, and the periosteal side of the lingual cortex is depository. Both cortical plates thus drift together in a lingual direction (Fig. 62a). These regressive movements are not, however, primarily concerned with a direct posterior mode of growth. Instead, cortical growth movements produce an essentially downward drift of the premaxillary arch in conjunction with palatal growth in a corresponding direction. Because the outer (labial) surfaces face away

The nasomaxillary complex
from these directions, they are resorptive in character. The lingual sides of both cortices are oriented downward, facing the growth direction, and they are therefore depository. Thus, the endosteal nature of premaxillary enlargement is a response to growth patterns that essentially involve an almost direct, downward manner of cortical movement.
Note that the inferior movement of the premaxillary region necessarily involves a process of continuous and sequential relocation. In Figure 62a, it is seen that the floor of the nasal cavity progressively comes to occupy regions previously held by the downward moving pre-
( 1 4 9 )
maxillary arch. The superior surface of the projecting nasal spine is resorptive, and its inferior surface is depository. This combination serves to move the spine downward and slightly forward, because it faces both of these directions. Because of the concave surface curvature of the premaxillary region, the inferior mode of growth results in a continuous relocation of the nasal spine down into former areas of the premaxillary depression. Similarly, the area of surface depression in the curvature moves progressively downward into regions previously occupied by the protruding alveolar margin. The resorptive nature of the periosteal
Diagram a illustrates the mode of downward premaxillary growth. The superior (buccal) surface is resorptive (—), and the inferior (lingual) surface is depository ( + ) . Between stages 1 and 7, the cortex moves downward and becomes slightly extended in an anterior direction because of alveolar elongation. Although direct posterior regression of the cortical plate as a whole does not occur, note that regional portions nevertheless undergo backward recession. Because of relocation, the point at A becomes repositioned in a
direct posterior manner. Note also that it is relocated from the bottom of plate 3 to the top of plate 4.
Diagram b illustrates the manner of remodeling in the sloping cortex of both the anterior surface of the bony nose and the orbital floor. In the course of movement from 1 to 7, continuous relocation is involved. Note that point A is raised to point B, and that it becomes repositioned from the middle of plate 4 to the top of plate 5.
Figure 63

( 1 5 0 ) Craniofacial bone growth
Diagram showing the nature of growth along the complex curvature at the contact between the malar area and the lateral wall of the nasal region. This contour becomes expanded as the nasal area (frontal process of the maxilla and adjacent nasal
bone) moves in progressive superior, lateral, and anterior directions (black arrow). Simultaneously, the malar area of the maxilla is receding in a posterior direction (white arrow). (From Enlow, D. H., and S. Bang: Am. J. Orthodont., 1965.)
Figure 64

The nasomaxillary complex
labial surface provides these successive remodeling shifts. It serves to move the cortical plates backward into new areas of the surface depression, thereby reducing the former alveolar projection when it held these positions, into the concave curvature forming the premaxillary depression. The alveolar projection simultaneously moves downward by the same basic combination of remodeling resorption and deposition. It also becomes lengthened by progressive bone deposition on its free margin.
The resorptive surface of the human premaxillary region thus is associated with the basic downward movement of growth, in contrast to a downward but also markedly forward growth in nonprimate forms. It provides, further, the basis for remodeling adjustments that occur as the levels of the concave arch become continuously relocated in a progressively inferior course (Fig. 63a).
The labial cortex in the premaxillary region is composed of typical endosteal bone types. In interdental areas involving a cancellous medulla, the bone tissue follows a convoluted pattern produced during endosteal cancellous compaction. In areas overlying teeth, the cortex is relatively thin and is usually composed of endosteal-produced, circumferential lamellar bone that has a resorptive periosteal surface (Fig. 65a). Periodontal fibers are often seen just deep to the external resorptive surface. They were originally formed within the alveolar socket but became translocated to the labial side of the cortex as a result of the inward manner of cortical drift.
Some scattered patches of periosteal bone may be found on the external surface of the premaxillary cortex (Fig. 59). These appear to be associated with the presence of unerupted teeth and to the various movements involved in eruption and drift. The presence of such transient patches of periosteal bone does not
( 1 5 1 )
interfere with the general direction of downward movement associated with a predominantly resorptive surface.
The lingual cortex in the premaxillary (incisor) region is composed entirely of periosteal bone with an endosteal resorptive surface. This periosteal cortical bone grades directly into the thick periosteal cortex of the palatal shelves as these two adjacent areas move together in an inferior manner.
THE NASAL REGION. The frontal processes of the maxilla comprise the greater part of the protruding bony walls enclosing the nasal chambers. A prominent reversal line occurs, however, as the nasal wall grades into the remainder of the maxilla below it. This reversal line begins at the approximate midpoint of the inferior orbital rim and extends in an oblique course inferiorly and medially to a point just above the junction of the nasal floor with the premaxilla. Note that the reversal line runs diagonally across the maxilla as an extension of the curved contour plane present in the floor of the nasal cavity near its anterior orifice. As pointed out previously, the placement of this reversal line shows a normal range of variation above and below the infraorbital foramen.
The orientation of the maxillary frontal process is such that its external surface faces laterally, anteriorly, and superiorly. This surface is characteristically depository in nature, and its cortex is composed entirely of periosteal bone. The contralateral inner (mucosal) side is resorptive, and this lining cortex is composed of endosteal bone tissue (Figs. 66b, 67b, and 67c). In some areas, particularly near the rim of the nasal opening, the bony plate may be quite thin and contain only a single cortical layer. Here, the wall is composed of a single layer of periosteal bone that has a resorptive mucosal surface.
Surface accretion on the outer side of the


The nasomaxillary complex
nasal wall (with contralateral resorption) brings about direct cortical drift in the multiple directions that it faces. It moves anteriorly, thereby lengthening the bony part of the nose in a forward manner. This growth movement, in conjunction with the essentially downward direction of growth in the premaxillary region, contributes to the protruding nose that characterizes the human face. The contrasting directions of growth in these two areas have produced a partial divergence of the snout and muzzle, in contrast to the face in other mammals (Chapter 8) .
Surface deposition on the cutaneous surface of the nasal wall also produces a distinct lateral movement of the entire cortical plate, because its periosteal surface also faces to the side. This results in a slight widening of the nasal bridge and a marked lateral expansion in the inferior portions of the nasal chamber. These lateral movements proceed in direct conjunction with the lateral relocation of the orbit and the malar region, as described later.
Because the nasal wall also faces superiorly, surface accretion further produces an elevation of its cortex. However, this process is associated primarily with a remodeling sequence that functions in response to relocation in the forward-growing nose. Because the bony nasal walls slope obliquely downward and forward, the anterior growth movement results in a constant relocation of the lower portions sequentially into positions situated more superiorly
( 1 5 3 )
along the slope (Fig. 63b). This is accomplished by the periosteal mode of new bone additions on this upward-facing surface. These deposits do not materially elevate the nasal wall, but serve to relocate the levels along the incline from one to the next, and to move the entire cortex forward and laterally at the same time. As anterior dimensions of the nasal cavity become lengthened, the vertical size is increased by the downward movement of the palate together with continued bone growth at the frontomaxillary suture (Chapter 10).
Continued deposition on the downward-facing rim of the nasal opening produces a downward extension of this free margin. The nasal tip thus becomes lowered during nasomaxillary growth.
As the forward edge of the nasal wall grades into the premaxillary region, a characteristic reversal occurs. Here, the forward-growing nose and the downward-growing maxillary arch abruptly undergo divergence in their respective growth patterns. The plane of contour extending across these two contrasting regions becomes progressively expanded with continued growth. The angulation of the anterior nasal margin also becomes markedly changed with age as the nasal area continues to grow forward in conjunction with the regressive manner of premaxillary movement below it.
Within the nasal cavity, the junctions between the maxilla and the conchae are marked by prominent bony ridges. These localized
Figure 65a. The external (periosteal) side of the premaxillary cortex is resorptive (A); the opposite alveolar surface is depository (B). The bone of the cortex was laid down on the endosteal side as the entire plate drifted in an inward direction. The bone tissue that forms the outer surface of the premaxilla thus was actually formed on the
internal side and subsequently transposed to the periosteal side of the moving cortical plate. X 75.
Figure 65b. The anterior lace of the malar is resorptive, as seen in this section, and the endosteal surface adjacent to the medullary cavity is depository. The cortex is composed of convoluted compacted cancellous bone tissue. X 60.
Figure 65


The nasomaxillary complex
regions represent islands of periosteal bone entirely surrounded by the resorptive surfaces that characterize the remainder of the bony nasal lining.
THE ORBITAL FLOOR. The bony orbit is composed of several separate bones that follow an interrelated sequence of remodeling changes. The different elements that comprise the whole orbit, including the maxillary, zygomatic, frontal, lacrimal, sphenoid, and ethmoid bones, will be considered separately in the following pages as each bone is described individually. The overall composite growth pattern of the entire orbit is discussed on page 247.
The maxillary bone forms the greater part of the orbital floor. This sloping surface faces three directions—laterally, superiorly, and slightly anteriorly—an orientation similar to that in the adjacent nasal wall. This orbital surface is composed of a single, thin plate of cortical bone that lacks a middle zone of diploe. The periosteal surface is depository in character, and the opposite endosteal surface overlying the maxillary sinus is characteristically resorptive (Fig. 67a). The bone is of a
( 1 5 5 )
lamellar type, and the very thin cortex contains only a scattering of vascular canals.
The lateral growth of the floor in each orbit moves them away from each other, thereby increasing the breadth of the nasal cavity. Because the orbital floor also faces somewhat anteriorly, a degree of forward movement also occurs, thus contributing to the composite manner of forward movement in the upper maxilla as a whole. This forward growth does not keep pace with the more rapid, anterior movement of the nasal wall, however, so that the two progressively draw apart as a result of their differential growth rates.
In addition, the orbital floor faces superiorly, and surface accretion thereby moves it in an upward direction. This serves two primary functions. First, as the orbital floor shifts laterally, all the parts along the sloping cortex become relocated. This is a sequential process in which portions formerly positioned in the lower lateral areas become elevated in succession into the more superior medial locations as the inclined floor drifts laterally (Fig. 63b). This is accomplished by the periosteal manner of its bone growth. The second function is a
Figure 66a. The lateral rim of the orbit is characteristically resorptive, as seen here, and it is composed of endosteal bone tissue. The inner surface is depository, and the entire cortex drifts in a posterior direction. (Photomicrographs on this plate are from Enlow, D. H., S. Bang, Am. J. Orthodont., 1965.) X 60.
Figure 66b. The lining surface of the nasal chamber is characteristically resorptive in nature. This area shows the frontal process of the maxilla as it grades into the suborbital region. The cortex is composed of typical convoluted bone produced by the process of cancellous compaction. The endosteal surface is depository.
Figure 66c. In this section of the palatine
process of the maxilla, a middle diploe is lacking, and the cortical plate is composed of a single bony layer deposited on the oral side (right of section). The contralateral nasal surface is resorptive.
Figure 66d. In thicker areas of the palatal shelf, a middle zone composed of cancellous trabeculae is present. The oral surface, seen here, has received deposits of lamellar bone. Note the embedded attachment fibers. As the entire bony palate descends by cortical drift, the spaces of the diploe follow by a process of progressive resorption into the moving oral cortex. The cortical plate on the contralateral nasal side is composed of compacted cancellous, convoluted bone tissue.
Figure 66

( 1 5 6 ) Craniofacial bone growth

The nasomaxillary complex
marked movement of the entire orbital floor in a progressively superior direction in response to sutural growth at the frontomaxillary junction. Sutural bone additions are associated with a downward displacement of the entire maxilla. The relative position of the orbital floor is maintained by simultaneously relocating it in a compensatory upward direction (Chapter 10).
Successive additions of new bone on the lining surfaces in the orbital cavity, including the orbital floor, would appear to reduce its internal dimensions. This is not the case, however, because growth at the various surfaces related to the orbit follows the standard V mechanism in which deposits are added onto the inner side of a funnel or V-shaped structure. The entire dimensions increase as the whole structure grows and moves toward its wide end, which in this case is the opening of the orbit. The factor of sutural growth between the different orbital bones is also involved, as mentioned above.
( 1 5 7 )
THE MAXILLARY SINUS. The human facial skeleton has a number of morphologic characteristics that distinguish it from most mammalian forms. Some of these features, also present in other higher primates, are associated with the development of massive maxillary sinuses. The human orbit has a broad, near-complete orbital floor, a partition that is not present in many nonprimate species. It separates each oribtal cavity from the adjacent infratemporal fossa, and it significantly extends the body of the maxilla posteriorly and superiorly into the infraorbital region. The orbital floor constitutes the roof of the maxillary sinus beneath it. In addition, the marked downward growth of the maxillary body further expands the internal volume in this suborbital region. The human orbits face distinctly forward, and the underlying, forward-facing malar area has a pronounced squared configuration with a marked lateral protrusion. These various factors in combination are associated with a suborbital region in the human
Figure 67a. The maxillary portion of the orbital floor is composed of a single, thin plate of periosteal bone. The surface to the right is depository, and the opposite side, which lines the maxillary sinus, is resorptive. (Photomicrographs in this plate are from Enlow, D. H., and S. Bang, Am. J. Orthodont., 1965.) X 60.
Figure 67b. This section illustrates the progressive advance of a medullary space into the periosteal cortex of the maxillary frontal process. The outer surface (right) is depository; its endosteal surface is resorptive; the opposite endosteal surface is depository, and the inner mucosal surface (left), which lines the nasal cavity, is resorptive. The combination of movements produces an outward drift of the entire cortex, as well as a similar shift of its enclosed cancellous spaces, by
bone additions on surfaces facing this direction together with corresponding resorption from contralateral surfaces.
Figure 67c. At the anterior rim of the nasal aperture, the depository external surface (right) abruptly becomes resorptive at the circumnasal reversal line. The mucosal surface (left) is resorptive.
Figure 67d. The outer premaxillary cortex is characteristically composed of endosteal bone tissue. This section was taken from the area where the resorptive floor of the nasal cavity passes directly onto the resorptive periosteal surface (left) of the premaxilla. The endosteal surface (right) is depository. The entire cortex drifts in an inward direction toward the right.
Figure 67

( 1 5 8 )
face that is quite extensive. The area is initially occupied by cancellous trabeculae, but it becomes progressively hollowed during continued facial growth.
The maxillary sinus essentially represents an adaptation of structure to the architectural arrangement associated with an expanded suborbital region, and it provides an outer bony cortical wall for this entire area of the enlarged maxillary body. The space occupies a region that is not otherwise utilized in the construction of the bone as a whole. Other suggested functions, such as voice resonance, are entirely secondary.
Most internal surfaces in the enlarging maxillary sinus are resorptive. By this means, internal sinus volume increases as the entire maxilla around it grows in size. The maxillary sinus expands into surrounding areas that are already occupied by spongy bone, and a slig ht compaction of the marginal cancellous spaces takes place, thereby forming a thin cortical wall within the body of the maxilla. The inner surface of this wall is resorptive, and it moves away from the enlarging sinus by continued cancellous compaction. Although most internal (lining) surfaces throughout the sinus are resorptive, the region adjacent to the nasal chamber has an opposite growth pattern, because this cavity similarly expands in internal volume. The nasal surface of the partition that separates them is resorptive, and the opposite (sinus) side is depository.
It has already been seen that the external cortical surface of the malar region below each orbit is resorptive in nature and regressive in growth pattern. Because the maxillary sinus within this cheek region is also resorptive, it is apparent that their respective cortices grow in directions toward each other. That they stop short is evident because breakthrough does not normally occur. The malar region enlarges significantly in a lateral direction, and
Craniofacial bone growth
the erosive advance of the sinus follows essentially in this lateral course, as well as in a posterior manner corresponding to the growth movement of the maxillary tuberosity and zygomatic process. The greatest extent of posterior drift by the zygomatic process occurs at its most lateral extremity, however, a region not occupied by the sinus.
DISCUSSION. It is apparent that the maxilla as a whole does not "grow" forward and downward as suggested by the traditional cephalo-metric picture. Instead, this complex bone, with its multiple contours and regional parts, grows in a wide variety of posterior, superior, inferior, and anterior directions (Fig. 69). Its various parts become drawn out in many different directions as the entire bone continues to grow. The nasal walls, for example, grow and move essentially forward and laterally. At the same time, the malar region of the maxilla recedes in a posterior direction. In Figure 64, note the expanding nature of the curvature that occurs between these two continuous regions as they follow their divergent courses of growth.
The descriptions in the previous pages deal with the processes of remodeling growth that take place in virtually all parts of the entire bone. Sutural growth represents another major growth process, and this is discussed in Chapter 10. The fundamental process of remodeling growth serves two primary functions. First, it brings about local increases in dimensions by appropriate, individual combinations of resorption and deposition on the different regional surfaces that constitute all parts of the whole bone. Second, this extensive process of remodeling growth functions to continuously adjust the shape and dimensions of these regional parts, because continued addition of new bone, whether on a sutural surface, alveolar margin, or maxillary tuberosity, results in

The nasomaxillary complex
the sequential relocation of all the other areas of the bone. The basic growth factors summarized on page 105 apply directly to these various remodeling processes, because they are concerned with growth itself rather than the composite of both growth and displacement.
It is noteworthy that basic patterns of growth in the maxilla closely parallel a number of growth movements seen in the mandible. As they enlarge, both bones undergo a process of displacement away from the cranial base. Both increase in overall anterior-posterior dimensions primarily by progressive growth at their posterior (distal) ends. This provides a lengthening of the dental arch in conjunction with the addition of new teeth or replacement by larger teeth. As both the mandible and maxilla grow progressively backward, all their various parts similarly undergo processes of relocation, and constant remodeling adjustments are correspondingly involved in each bone. The coronoid process of the mandible and the zygomatic process of the maxilla are examples of two comparable areas that experience extensive remodeling changes and movements in response to continued posterior growth of the whole bone. Both the maxilla and the mandible further represent a phylo-genetic consolidation of originally separate bones. In the human face, the upper and the lower jaws characteristically undergo a special remodeling process in which regressive growth occurs in the anterior portions of their arches. The upper and lower jaws both have an abbreviated, U-shaped configuration, in contrast to the projecting, pointed muzzle of other species. The maxilla possesses an elongate, vertical extension, the frontal process, that contributes to the positioning of the bone relative to the cranial floor. The mandible also has an elongate and vertical process, the ramus, which similarly functions in the placement of the bone relative to the cranial floor and the
( 1 5 9 )
maxilla. The human mandible possesses a characteristic mental protuberance with a concave surface in the adjacent incisor alveolar region. The human maxilla, with its protruding nasal spine, has a similar concavity in the incisor area. The arches in these two bones grow in directions toward each other. In general, the overall growth patterns in the mandible and maxilla form a mirror image, and growth processes in one complement those of the other.
THE ZYGOMATIC BONE. The separate zygomatic bone forms the middle segment of the zygomatic arch as well as a portion of the lateral orbital wall. Its growth movements proceed in direct conjunction with the enlargement of the zygomatic process of the maxilla, the zygomatic process of the temporal, and the adjacent sphenoid and frontal bones.
As in all other facial bones, the orientation of surfaces and the directions of regional growth are closely associated with the remodeling patterns found in this complex element. The anterior (malar) portion of the zygomatic bone moves progressively backward in conjunction with the posteriorly shifting zygomatic process of the maxilla. This forward-facing surface is resorptive, and its underlying cortex is composed of endosteal convoluted bone. The endosteal surface is depository in nature. The posterior manner of the growth movement is associated with the backward growth of the malar as it keeps proportionate pace with the elongating tuberosity and arch of the maxilla.
Although the anterior facing cortex of the malar region is regressive, it is interesting to note that the zygoma nevertheless represents a primary site associated with the marked anterior displacement of the entire maxilla. This occurs at the zygomatic sutures, in conjunction with various forward expanding soft tis-

( 1 6 0 )
sues that are believed to bring about this displacement. Thus, as the whole zygomatic arch elongates by sutural growth, the forward part of the malar region simultaneously undergoes posterior drift.
The cortex comprising the lateral surface of the zygoma is composed of periosteal bone, and the zygomatic arch thereby grows and moves in a lateral direction. Successive new bone additions result in a laterally drifting surface that broadens the right and left cheek areas as they grow away from one another. Note that a prominent, vertically oriented reversal line occurs along the lateral side of the zygomatic bone extending from its base to the tip of the frontal process. The surface anterior to this line is resorptive, and the surface posterior to it is depository. This remodeling combination contributes to the backward and, at the same time, lateral movements of the zygoma. The reversal line itself continuously moves in a posterior direction. The forward resorptive surface progressively overtakes the recently formed periosteal bone produced along the lateral side of the arch, which then becomes undercut and replaced by endosteal bone. The reversal is placed along a line that is marked by contour change as the anteriorly facing portion grades into the laterally facing surface.
The medial side of the zygomatic arch is characteristically resorptive. Its endosteal surface is depository, and the cortex is composed of typical convoluted bone. In conjunction with the depository nature of the lateral (cutaneous) side of the zygomatic arch, the combined pattern produces a lateral movement of the entire arch, including both the lateral and medial cortical plates (Fig. 60c).* The
* A variation is sometimes found in which the growth activity of these two sides becomes reversed. This would limit lateral growth and result in an essentially posterior course of zygomatic development.
Craniofacial bone growth
lateral movement of the zygoma, which also constitutes the lateral orbital wall, thus makes way for the lateral direction of growth in the orbital floor (orbital surface of the maxilla).
The posteriorly facing portion of the zygomatic bone within the temporal fossa is depository in nature. This surface grows posteriorly in conjunction with the resorptive and regressive anterior side of the malar region. Medially, the posterior depository surface crosses the zygomaticomaxillary suture and continues onto the posterior face of the zygomatic process of the maxilla, which undergoes a corresponding posterior shift. Laterally, a reversal line occurs as the posteriorly facing portion of the zygoma behind the malar area grades into the zygomatic arch proper. Here, the surface becomes resorptive as the whole arch drifts laterally.
The vertically placed frontal process of the zygomatic bone forms a portion of the lateral orbital wall. The anterior rim of this process is characteristically resorptive, and the posterior edge is depository. This produces a backward movement as the lateral orbital rim drifts posteriorly together with the malar region. Most of the lateral surface of the frontal process is depository. The reversal separating these two areas is continuous with the reversal line extending vertically across the body of the zygoma. The inner orbital face of the frontal process is resorptive. Together with complementary deposition on the lateral side, the entire frontal process thus moves laterally (as well as posteriorly) in conjunction with the malar and zygomatic arch. Note that the medial (resorptive) side of the frontal process faces away from these directions. The growth movements involved in these remodeling processes proceed in combination with movements in the numerous other elements that comprise the orbital complex (page 247).
The transverse shift of the lateral orbital wall and rim proceeds in advance of the en-

The nasomaxillary complex
larging orbital surface of the maxilla (the floor of the orbit) as the latter extends progressively into those areas previously occupied by the moving wall. The posterior drift of the lateral orbital rim serves to maintain its constant position relative to the posteriorly moving malar region.
The inferior edge of the zygomatic arch is characterized by a massive accumulation of periosteal bone deposits. This region shows a significant downward enlargement, particularly in the malar area (Fig. 108). The bone tissue involved is of a type associated with relatively rapid growth, in contrast to bone deposits found on the superior margin of the arch. The latter are also of a periosteal type, and they function primarily to reposition the upper edge in a superior direction as the entire arch is carried downward by sutural growth at the frontozygomatic junction and the various temporal sutures. This maintains the proportionate position of the superior level of the zygomatic arch in relation to the cranial base and orbit.
In general, the various growth and remodeling processes that characterize the zygomatic bone function to (1 ) enlarge its overall dimensions, (2 ) widen the right and left zygomatic arches, and (3 ) simultaneously move the anterior malar region and the lateral orbital rim posteriorly. The various zygomatic sutures function in the lengthening of the arch and the frontal process of the zygoma. These factors also are associated wth the anterior and inferior mode of maxillary displacement.
THE NASAL BONES. The diminutive, paired nasal bones comprise the upper portion of the abbreviated snout. The growth movements of the nasal bones and the maxillary part of the lateral nasal walls proceed in similar directions. A predominant growth direction characterizing both is anterior. The nasal bones also enlarge laterally, but to a lesser extent. The cutaneous
( 1 6 1 )
side of each nasal bone faces both anteriorly and laterally, and the periosteal surface is correspondingly depository in nature. The inner mucosal surfaces of the nasal bones are resorp-tive. This growth combination serves to move the roof of the nose forward, to expand it laterally, and to slightly widen the nasal bridge. The nasal bones thus do not grow forward by simply adding new bone on the anterior edge at the nasal tip. Instead, the entire flat periosteal surface is involved as the whole bone moves forward by a process of cortical drift.
The outer surface of each nasal bone also faces superiorly. The nose does not significantly rise in level, however, as continued deposition of bone occurs on this superior surface. The inclined downward sloping nature of the nasal bones requires a continuous relocation of the inferior parts (toward the tip) into the more elevated portions along the slope as the nose lengthens. This regional elevation is brought about by the upward mode of periosteal bone additions, as schematized in Figure 63b. As the nose elongates, its tip becomes slightly lowered as the downward facing anterior nasal rim receives new bone deposits.
The surfaces adjacent to the forward edge (free margin) of the nasal tip may show variable patches of surface resorption together with endosteal deposition. This produces small restricted areas in which the edge turns down slightly. Another variation is sometimes found in the proximal portion of each nasal bone. As much as two thirds may be composed of an inwardly growing, endosteal cortex. The opposite side, within the nasal cavity, has a depository surface. The inferior third of the nasal bones in this situation shows the usual pattern of external deposition with internal resorption. These combinations serve to depress the nasal bridge as the forward part of the nose continues to elongate and become broadened.


The nasomaxillary complex
THE PALATINE BONE. The separate palatine bone follows a developmental and remodeling course that parallels the growth pattern in the remainder of the palatal complex. This posterior portion of the shelf has an oral surface that is entirely depository. The contralateral nasal surface is characteristically resorp-tive. This combination brings about a marked downward movement of the entire, horizontally oriented palatal plate. The distribution of the various types of bone tissue involved in the growth movement is comparable to the maxillary segment of the palate (page 145). The vertically oriented, lateral portion of the palatine bone similarly conforms to the growth and remodeling pattern found in the contiguous part of the maxilla. The mucosal surface of the cortex on the nasal side is resorptive, and the contralateral surface lining the maxillary sinus is depository. This produces a lateral shift of the nasal wall thereby enlarging internal dimensions in this portion of the chamber. The maxillary sinus becomes correspondingly shifted in a lateral direction in conjunction with the lateral growth of the malar area. The contiguous nasal conchae similarly show a growth pattern that involves generalized lateral deposition and medial resorption, thereby shifting these bones laterally as the nasal wall undergoes a comparable movement.
That portion of the projecting pyramidal process of the palatine bone that abuts the pos-
( 1 6 3 )
teriorly facing surface of the maxillary tuberosity shows a characteristic reversal. The outer surface is resorptive, and its cortical bone is endosteal in type. This growth pattern provides a backward relocation of the pyramidal process as the maxillary arch becomes extended in this direction. The reversal occurs at that point where the last molars erupt through the cortex of the tuberosity.
The nature of sutural growth in the human palatine bone relative to the remodeling growth changes described above is not well known. Whether or not the extent of downward displacement associated with the various, complex superior palatine junctions is equivalent to that characterizing the maxilla has not been determined by experimental studies. If a difference exists, the separate palatine bone would necessarily require a differentially greater or lesser degree of cortical movement (drift) to keep pace with the maxillary portion of the palatal shelf and to maintain alignment between them. Further study on this question is needed.
THE LACRIMAL BONE. The lacrimal is a
small, very thin plate of bone situated in a general area of the skull that involves extensive remodeling changes. It is an isolated island of bone bounded on all contact edges by a sutural junction. The postnatal enlargement of this bone is slight when compared with the marked
Figure 68a. Lacrimal bone. Surface A is the external side of the cortex that forms a portion of the lining orbital wall. In the cephalic two thirds of the lacrimal, the surface is characteristically resorptive, as seen in this section. The contralateral side within the nasal chamber is depository (B). A similar pattern is seen within the lacrimal groove (C and D). X 60.
Figure 68
Figure 68b. This section of the palate overlies a tooth socket. Surface A is the nasal floor, and it is resorptive. Side B is depository. The entire bony shelf was drifting in an inferior course. Note the downward movement of medullary spaces by bone additions on superior lining surfaces and removal from their inferior surfaces. X 75.


The nasomaxillary complex
growth increases that occur on all sides of it. Although the lacrimal bone enlarges somewhat in vertical as well as anterior-posterior dimensions, the primary growth activity associated with this bone is a continuous process of remodeling that provides a means for adjustment and alignment between the various growing bones surrounding it.
The superior border of the lacrimal in the very young skull is positioned in line with the upper edge of the frontal process of the maxilla at the frontomaxillary suture. It maintains this positional relationship throughout subsequent development even though sutural growth between the frontal and maxillary bones is extensive. Both the maxilla and the lacrimal are displaced downward during bone growth on the frontal side of the frontomaxillary and frontolacrimal sutures. However, the frontal process of the maxilla becomes displaced much farther in conjunction with continued bone additions on the maxillary side of this suture. Its rate and extent of movement greatly exceed the growth of the adjacent lacrimal bone. Positional relationships between the two, in response to their differential modes of growth, are maintained by connective tissue adjustments within the maxillary-lacrimal suture. The frontal process of the maxilla, in effect, "slides" down its contact with the slower-growing lacrimal. This differential manner of movement is accomplished by fibrous relink-age, as described in the chapter dealing with the sutural growth mechanism (page 95). A similar but somewhat less marked adjustment process occurs within the other sutural contacts surrounding the lacrimal bone.
In Figure 70, it is seen that (1) the breadth
Figure 69
Summary diagram of maxillary growth and remodeling. See text for detailed descriptions.
( 1 6 5 )
of the nasal bridge enlarges slightly, but the extent of this transverse increase is relatively small in comparison to the expansion in other portions of the nasal complex; (2 ) the medial wall of the orbit and the floor of the orbital cavity enlarge significantly in a lateral direction. As these bony walls in each of the orbital cavities move laterally away from each other, they also shift distinctly upward and forward. The nearly perpendicular angle between the medial orbital wall and the floor in the very young skull becomes opened considerably as this area continues to expand. Thus, there occurs a differential extent of movement between the medial and inferior portions of the orbit on one side of the intervening lacrimal bone, and the nasal bridge on the other side. The lacrimal bone, bridging these differentially enlarging regions, represents a critical remodeling segment that serves to successively adjust the alignment between them as they grow at different rates and to different extents.
As the floor of the orbit moves progressively in a lateral and superior direction, the inferior half of the lacrimal bone similarly moves in a corresponding manner (Fig. 71). Periosteal bone is deposited on its orbital surface, and resorption occurs on the contralateral nasal side. Because of the differential extent of downward displacement between the floor of the orbit and the lacrimal in conjunction with the much greater degree of bone growth at the frontomaxillary suture, the upward movement of the maxillary portion of the orbital floor is correspondingly greater than that of the lacrimal. In both cases, however, upward growth serves to maintain the relative position of the whole orbit in response to downward sutural displacement. Periosteal bone deposits simultaneously function to move the floor laterally, because these surfaces also face this direction. Differential growth rates between the orbital and lacrimal parts of the orbital

In the infant skull (top), the floor and medial wall of the orbit are recessed in position (A, A')-In the older skull (bottom), however, this region, composed of portions of the separate ethmoid and maxillary bones, has become markedly expanded (B, B')- Note that the breadth of the nasal bridge (C and D) does not increase proportionately but remains relatively stable. The lacrimal bone func
tions as a critical pivot during these remodeling changes. Furthermore, as the frontal process of the maxilla increases significantly in vertical length, a differential movement between it and the lacrimal occurs. This adjustment is carried out in the sutural membrane that joins these two bones.

The nasomaxillary complex
floor are accommodated by the fibrous relink-age process within the suture separating them. The extent of periosteal bone deposition on the lower half or third of the lacrimal is variable and reflects the differing extent of adjustment provided by the lacrimal between the surrounding maxillary, ethmoid, and frontal bones.
The superior half or two thirds of the lacrimal bone, in contrast to its lower portion, has an orbital surface that is resorptive. As a variation, this entire side can be resorptive. In either case, the contralateral nasal side is depository. The posterior portion of the medial orbital wall is formed largely by the separate ethmoid bone, and this region expands significantly in a lateral manner during its growth (compare neonatal with mature skulls). The orbital surface of the ethmoid is entirely depository in nature, and its opposite nasal side is resorptive. The contrasting mode of growth between the ethmoid and the superior part of the lacrimal is an interrelated remodeling arrangement that provides a differentially greater lateral movement of the posterior part of the medial orbital wall relative to the anterior portion associated with the much more stable nasal bridge. The lacrimal represents the adjustment link between them. As the ethmoid bone shifts laterally, the lacrimal moves with it. At the same time, however, a gradient of resorptive cortical drift occurs over the orbital surface on the upper part of the lacrimal bone that serves to rotate it in a medial direction as the whole bone becomes displaced in an opposite lateral course. This serves to continuously maintain its alignment with the slower moving nasal bridge on one side and the ethmoid on the
( 1 6 7 )
other. Differential movements occurring at respective suture contacts are carried out by the fibrous relinkage process within the connective tissue of the suture.
The thin lacrimal bone is composed of a single lamina of nonvascular, lamellar cortical bone. Its surfaces are depository and resorptive on contralateral, medial, and lateral sides (Fig. 71), according to the characteristic distribution described above. In summary, the lacrimal has remained, phylogenetically, a separate bone, and it occupies a critical location at the junction between portions of the orbital and nasal regions. Despite its diminutive size, the lacrimal represents the key pivotal bone that maintains alignment between the several differentially growing and moving bones around it.
The lateral expansion of the orbital floor and medial orbital wall (ethmoidal portion) is accommodated by remodeling changes in the lacrimal, as schematized here. The inferior portion of this bone drifts laterally and superiorly, and the upper part moves medially.

(8)
Comparative
morphogenesis of
the facial skeleton
The human face is different. By ordinary mammalian standards, our facial features are unusual, specialized, and perhaps even grotesque. The long functional muzzle that marks the face of most other mammalian forms is all but lacking in man. The associated snout is reduced to a curious overhanging vestige. The face is flat, wide, and vertically disposed. Instead of a graceful facial contour sloping back to the skull roof, the human face possesses a unique, bulbous, upright forehead in front of an enormous braincase. The flattened face is diminutive in character relative to the remainder of an enlarged head. The eyes are close together and they face straight forward. The human dental arches are disproportionately small relative to the size of the whole body (Fig. 72).
Most mammals are able to rear back onto hind legs and briefly balance or move in an
168
upright position. The human body, however, is one of the few mammalian forms that has become adapted to a permanent bipedal stature. The front legs function as arms. All the bones in the entire human skeleton—from the podial phalanges to the bregma—are correspondingly modeled as adaptations to this unusual upright stance. The human feet stand by themselves, as it were, as a unique anatomic feature of Homo, a morphologic situation approached only by a relatively few other primates. Similarly, the pelvis, vertebral column, limb bones, hands, and shoulder girdle all reflect the standing nature of man's posture. The configuration of the human skull shows a number of direct structural relationships to the disposition of the skeleton beneath it.
The survival value of an elongated muzzle in man is reduced. Because of man's erect posture and the possession of free, agile arms

Comparative morphogenesis
with dexterous hands, the human jaws are much less critical in the procurement and manipulation of food and objects as compared with most other mammals. The defensive and offensive utility of man's jaws is similarly diminished.
The human brain functions in conjunction with the hand. The activity of one directly complements the other. Without the hand, the thinking mind would lack its primary tool and, conversely, the versatile hand without the mind would lack intelligent direction. The enormously expanded, heavy human brain occupies an enlarged cranium that has become balanced on an upright vertebral column. The positions of the sizable sternocleidomastoid muscles and the prominent mastoid processes at the skull base are adapted to the posture of the head. The foramen magnum is located directly beneath the skull, rather than at its posterior end as in most other forms. This factor, in conjunction with the marked forward growth of the prefrontal and temporal lobes of the cerebrum, contributes to the marked downward flexure of the human cranial floor.
The functional basis for the unusual construction of the human face is associated with several interrelated factors. In most mammals, the snout and the muzzle project forward in a combined manner. In the human and other primates, however, variable degrees of divergence have occurred between them so that the nose and the jaws are partially separated topographic structures. In fossil hominoids, the snout apparently led the process of regression, a situation also seen in living anthropoids. In terms of actual morphogenesis, the forward growth of the snout in these forms lags behind the forward protrusion of the upper and lower jaws. The result is a face characterized by a somewhat prognathic muzzle but with an overlying nasal region that is even more flattened. Even though the jaws protrude noticeably for-
( 1 6 9 )
ward, however, their proportions relative to the remainder of the skull are small and do not approach the dimensions of a typical mammalian muzzle.
In man marked nasal reduction is also featured, but the degree of jaw recession has come to bypass the reduced human nose so that a converse arrangement is present. The nasal area protrudes slightly but the muzzle has become even more flattened in comparison to the nose above it. It is important to realize that the term "reduction" implies a decreased relative extent of forward growth. The jaws and nose are reduced in the sense that they do not grow as far forward as they do in other species. As will be seen later, only in man does muzzle reduction involve an actual regressive growth movement.
Various vertebrate species have different emphasis placed on their basic senses. One or two of the senses are usually much more highly developed relative to the others. A deer, for example, has an acute sense of smell, but his visual perception is ordinary at best. With the wind direction in his favor, a deer may sense the presence of a human at great distances. However, he cannot distinguish a downwind, scarlet-clad hunter at close range from a tree stump if the hunter can manage to remain motionless until there is an opportunity to fire.
In comparison with a long-snouted deer, the flat-faced human has a much less perceptive sense of smell. Man's eyes, however, are notably keen, and they are placed in anatomic positions that give him the advantage of more effective binocular vision. With the placement of the orbits forward and close together, the region between the eyes has become greatly reduced. This transverse area in other species is ordinarily occupied by the base of the relatively wide, elongate snout. The massive forward expansion of the prefrontal and temporal lobes is developmentally associated with the


Comparative morphogenesis
corresponding forward positioning of the eyes (Fig. 84). Man's visual acuity in general represents a more critical sense than does his olfaction. The lack of a prominent obstructing snout provides the advantage of close-up binocular inspection of hand-held objects. The eyes, the mind, and the hands all form an interdependent complex of structural adaptations, the functions of which utilize less of a subordinated snout and muzzle in comparison with nonprimate forms. Other adaptive features have also resulted from this combination. The architectural design of the face and cranium is consistent with the balanced placement of the head on an upright body. It makes possible a wide variety of vertical and horizontal head movements with minimal mechanical disadvantage (Brues, 1966).
In order to establish the morphogenetic basis underlying the development of human facial features in comparison with the nonhuman face, the postnatal growth and differentiation of the monkey facial skeleton is described below. An evaluation of morphogenetic similarities and differences between the two species will then be presented.
( 1 7 1 )
Facial growth and remodeling in MACACA
The skulls of the Rhesus monkey and the human differ in the degrees of development of certain morphologic features. These differences provide the basis for a number of structural and developmental characteristics that are uniquely human in nature. The basic plan of growth and remodeling in the mandible, maxilla, and other facial bones is similar to that found in corresponding human bones, although several notable differences occur. The composite patterns of combined growth and displacement are comparable.
THE MANDIBLE. The predominant directions of elongation of the mandible are posterior and superior (Fig. 73). The basic processes of mandibular lengthening involve the remodeling factor of relocation. As the posterior ends of the bone move backward and become extended superiorly, each component area within the whole bone becomes sequentially relocated, a process that brings about the extensive remodeling changes that occur throughout the entire bone. Each level under-
Distinctive topographic features that characterize the human facial skeleton. (See text for detailed descriptions of the growth and remodeling processes that produce them.) A, vertically oriented face (note vertical alignment of the ramus, lateral orbital rim, orbits, forehead, nose, and jaws); B, protruding forehead; C, supraorbital margin that extends forward of the infraorbital rim; D, protruding, vertically oriented nose that projects slightly forward of the maxilla; E, concave premaxillary region that is resorptive in character; F, decreased prognathism; G, concave
supramental region that is resorptive; H, mental prominence; J, elongate, vertical ramus; K, protruding mastoid process; L, widened face; M, reduced interorbital area; N, nearly complete superior, inferior, posterior, and lateral orbital enclosure; O, fused mandible; P, forward-facing orbits; Q, prominent, squared, flat cheekbones; R, flattened face. Note that the orbit is positioned beneath the anterior cranial fossa, rather than anterior to it, and that the orbit lies above the posterior maxillary arch rather than behind it.
Figure 72

( 1 7 2 )
goes constant reshaping and resizing as its relative position becomes moved as a consequence of continued growth additions.
Growth at the mandibular condyle involves endochondral formation of bone responsible for the medullary core within the condyle and condylar neck. The condyle moves obliquely upward and backward during continued growth, and as it does so the condylar neck
Craniofacial bone growth
becomes reduced by the process of endosteal bone growth (inward cortical drift). The more narrow neck is sequentially remodeled from former levels of the widening, obliquely moving head. The remodeling process involved is comparable to "metaphyseal reduction." The endosteal surface of the cortical plate on both the buccal and lingual sides of the neck faces the actual direction of growth. Because the
A summary diagram of mandibular growth and remodeling in the Rhesus monkey. See text for
regional descriptions. (From Enlow, D. H.: Principles of Bone Remodeling, Thomas, 1963.)
Figure 73

Comparative morphogenesis
periosteal surface faces away from the growth direction, it is resorptive. The buccal and lingual cortices thus are composed of endosteal bone tissue, and they grow inward toward each other (Fig. 74a).
The posterior border of the ramus is actively depository, and this growing edge contributes to the posterior movement of the ramus in conjunction with the adjacent condyle. The entire anterior margin of the ramus is resorptive, and thereby the whole ramus is shifted backward as it simultaneously lengthens vertically. This posterior movement, however, directly involves all other internal and external surfaces of the ramus and the coronoid process. The expanse of bone between the posterior and anterior borders is not dormant, but rather contributes actively to the total movement process. Thus, the ramus does not become shifted posteriorly simply by the addition of bone on its posterior edge with removal from the anterior margin. Because most of the lingual side of the ramus actually faces the posterior course of growth, it is largely depository in nature. This follows the V principle in that the right and left rami form a growing V that enlarges and moves toward its wide end. Only special regions at the condylar neck and a local area associated with the inward-curving gonial flare are resorptive. On the buccal side, the resorptive nature of the periosteal surface in the neck continues inferiorly onto the main portion of the ramus. Because this surface faces away from _ its posterior growth direction it is resorptive. However, the periosteal surface on the buccal side of the ramus just in front of the posterior border is depository. Here, the margin of the ramus turns inward, and the buccal surface is oriented so that it faces the direction of growth, which is posteriorly.
The coronoid process is placed in such a manner that its lingual side faces medially, posteriorly, and superiorly. The periosteal sur-
( 1 7 3 )
face is depository, and progressive additions move the cortex in corresponding lingual, backward, and upward directions. The contralateral buccal side of the coronoid process is entirely resorptive, and its cortex is composed of endosteal bone. Both the lateral and medial cortical plates thus move together in these same directions (Fig. 74b). On the buccal side, an outward periosteal reversal occurs as the base of the coronoid process grades into the ramus. The ramus in turn slopes onto the trihedral eminence of the mandibular body. Because each area is relocated into the next in succession, the periosteal nature of bone deposits serves to reverse the endosteal mode of growth that occurred when this area was a part of the coronoid process. Former stages of the coronoid process become converted, as the coronoid process itself moves upward and backward, into the forward portion of the ramus and posterior portion of the body. Just anterior to the antegonial notch, on the inferior border of the body, an area of surface resorption with underlying endosteal bone occurs. This brings about a slight elevation of the lower margin as the anterior part of the gonial region becomes relocated into the lengthening body.
On the lingual side, the basal portion of the coronoid process becomes relocated into the ramus as each part grows and moves superiorly and posteriorly. Continued bone deposits on the lingual surface carry former levels of the coronoid process medially as they are sequentially converted into a part of the enlarging, more medially placed ramus. The moving ramus in turn becomes converted into the elongating mandibular body as the entire ramus drifts posteriorly. This sequential process in the monkey mandible directly parallels that found in the human. More detailed accounts of the remodeling changes involved are presented in Chapter 6.
In the mandibular body, the greater portion


Comparative morphogenesis
of the periosteal surfaces on both the lingual and labial sides are depository in character (Fig. 75). A localized resorptive reversal occurs just anterior to the trihedral eminence, a region occupied by a slight depression. Another area involving an endosteal, resorptive reversal is present just above and below the projecting genial tubercle. Except for the tubercle itself, the cortical bone in this region is characteristically endosteal, and the inward mode of growth undercuts the massive accumulation of periosteal deposits on the crest of the tubercle. The result is the formation of the characteristic simian shelf (Fig. 80).
THE NASOMAXILLARY COMPLEX. Like the mandible adjacent to it, the maxilla undergoes a progressive process of posterior growth. This brings about a backward elongation of the curved dental arch at its free (distal) ends. The posterior face of the bulbous maxillary tuberosity is depository, and its cortex is composed of relatively fast-growing types of periosteal bone. This region represents a major area of growth which, in conjunction with corresponding increase at the various zygomatic sutures, is responsible for the greater part of anteroposterior maxillary enlargement.
In the laterally projecting malar region of the maxilla, the periosteal surface is characteristically resorptive (Fig. 77). The underlying cortical bone is endosteal in nature, and was
( 1 7 5 )
produced by bone deposition on the medullary surface of the cortex. The combined result is a posterior movement of the protruding zygomatic process of the maxilla. This backward relocation functions to continuously reposition the malar area relative to the maxillary tuberosity, which is simultaneously moving posteriorly. Thus, as the entire maxillary arch lengthens, the regressive malar region becomes successively shifted in the same direction. As in the human skull, a range of variation is found in the placement of the reversal line separating the depository from adjacent resorptive areas in this region. Such variation appears to be related to slight individual differences in proportions and overall shape.
The growth and remodeling movements of the separate zygomatic bone proceed in conjunction with the changes occurring in the maxilla. The resorptive surface present on the lateral projection of the malar portion of the maxillary bone continues across the suture directly onto the anterior face of the curved zygomatic bone. As this region of the maxilla shifts backward, the contiguous anterior portion of the zygoma becomes correspondingly repositioned posteriorly, thereby maintaining proportionate positional relationships with the elongating maxillary arch. However, the lateral surface of the zygomatic arch is depository, and the medial side within the temporal fossa is resorptive. This combination moves the
Figure 74a. The cortices of the condylar neck on both the lingual and buccal sides are characteristically composed of endosteal compacted cancellous bone, as seen in this section. The periosteal surfaces are resorptive, and the cortical plates grow inward toward each other as the diameter of the condyle and neck undergo reduction. Rhesus monkey, X 75. (From Enlow, D. H.: Principles
Figure 74
of Bone Remodeling, Thomas, 1963.) Figure 74b. In the region where the coronoid
process grades into the ramus, the lingual surface (A) shows marked periosteal deposition. The contralateral buccal side (B), however, is characteristically resorptive and is composed of endosteal bone. Rhesus monkey, X 75. (From Enlow, D. H.: Principles of Bone Remodeling, Thomas, 1963.)


Comparative morphogenesis
zygoma progressively to the side as its forward part drifts posteriorly. The composite result is a widening of the right and left cheek areas and a horizontal expansion of surface contour among the malar, temporal, and nasal regions.
The lateral orbital rim faces essentially laterally as well as anteriorly (Fig. 77) Progressive bone additions on this surface move the rim in a lateral direction in conjunction with the lateral shift of the zygoma and the entire orbital cavity. The contralateral posterior side of the orbital rim, like the medial surface of the zygomatic arch, is resorptive. The cortex is composed of typical endosteal bone tissue.
As the maxillary arch undergoes continued posterior growth by deposition of bone on the posterior face of its tuberosity, it simultaneously enlarges in an inferior direction. This is a composite result of increase at the various frontal and zygomatic sutures, alveolar elongation, and downward nasal (palatal) growth. As in the human maxilla, the upper jaw of the monkey presents a V-shaped configuration that has a vertical as well as a horizontally disposed arch. The latter is involved essentially in the backward lengthening of the maxilla, and the former is associated with the downward mode of growth. Bone is added onto the entire periosteal cortical surface within the oral cavity. Deposition occurs on the inferior side of the palate and extends down onto the
( 1 7 7 )
lingual surface of the bony arch. The contralateral nasal side of the palate is generally resorptive, although several localized periosteal reversals are present that are associated with the complex surface topography of the nasal floor. The palate moves downward as the maxillary arch simultaneously extends posteriorly at its distal ends. The arch is widened by surface deposition on the labial side and by progressive elongation in the alveolar regions.
The enclosing walls in the anterior portion of the nasal chambers, including the paired nasal bones, the frontal processes of the maxilla, and the palatal shelf, grow and move in a manner that brings about enlargement of the nasal region in a combined anterior, lateral, and inferior direction. The outer (cutaneous) surfaces of the nasal wall face both laterally and anteriorly, and surface deposits of new bone move them in corresponding directions. Contralateral periosteal surfaces lining the inner (mucosal) side of the nasal chamber are characteristically resorptive. Thus, the nose enlarges anteriorly and laterally, and at the same time it increases vertically as the palate and the maxillary arch below the palate grow together in an inferior direction.
The protruding muzzle, composed of the separate premaxillary bones and the forward portion of the maxillary arch, is characterized
Figure 75a. The lateral side of the mandibular body has a depository surface, a characteristic that extends to the anterior point of the jaw, in contrast to the human mandible. Note the bundles of attachment fibers embedded in the cortex. Rhesus monkey, X 75. (From Enlow, D. H.: Principles of Bone Remodeling, 1963.)
Figure 75b. An endosteal surface-resorptive reversal occurs on the surface of the mandibular
body just anterior to the trihedral eminence. Forward of this area, the entire remainder of the buccal cortex is depository in character. In this section the outer zone of periosteal bone (A) was laid down over a remnant of the older endosteal cortex (B). The inner surface of the latter, following the reversal mentioned above, has become resorptive. Rhesus monkey, X 75. (From Enlow, D. H.: Principles of Bone Remodeling, 1963.)
Figure 75

( 1 7 8 ) Craniofacial bone growth
Rabbit mandible. Areas of surface resorption are indicated by dark stippled area. Regions of surface deposition are represented by light stippled area. The basic plan of growth in the rabbit mandible is similar to that for the human and monkey. A predominantly posterior course of growth takes place, and direct structural conversions are involved as parts of the condyle, neck, ramus, and body undergo successive relocation. Note that the buccal side of the ramus is resorp-tive, and that the lingual surface is largely depository. Differences in growth pattern between the rabbit and human mandibles are associated primarily with regional dissimilarities in gross morphology. The prominent coronoid process that characterizes the jaw of man is poorly represented in the rabbit. The complex remodeling changes associated with this area are thus all but lacking
in the rabbit. The protruding lingual tuberosity in the human mandible is inconspicuous in the rabbit, and the arrangement and extent of resorp-tive and depository zones in this area correspondingly differ. Further variations in growth are found in the mental region because the morphology in this region is dissimilar. The fused right and left halves of the mandible in man show a characteristic protuberance, and remodeling changes associated with this structure therefore do not occur in the rabbit. A restricted zone of periosteal resorption is found in the overlying alveolar region of each incisor in the rabbit and is related to the continuous depression of this area as the tooth erupts and moves in a curving, forward direction. (Adapted from Bang, S., and D. H. Enlow: Arch. Oral Biol, 1967.)
Figure 76

Comparative morphogenesis
by an external surface that is entirely depository in nature (Fig. 78). The opposite endosteal side of the outer lamina is resorptive. This periosteal cortical bone is typically thin in regions covering teeth and is usually composed of a single plate of relatively nonvascular,
( 1 7 9 )
lamellar bone tissue. In thicker areas of the cortex, it is often composed of a fine cancellous, nonlamellar type of bone in the young growing skull.
In conjunction with the descending growth movement of the palatal shelf, the entire maxil-
The distribution of resorptive and depository surfaces in the human and monkey skulls, indicating periosteal surfaces that undergo progressive resorption during growth (dark stippled area) and
outer surfaces that are depository in nature (light stippled area). See text for further descriptions. (From Enlow, D. H.: Am. J. Phys. Anthrop., 1966.)

( 1 8 0 )
lary arch moves downward as well as somewhat anteriorly (Fig. 79). The teeth located within this growing, moving bone become shifted in corresponding directions by drifting. Bone deposition along the entire free alveolar margin further contributes to the inferior and anterior enlargement of the arch and serves to lengthen the alveolar cortex. Although the predominant direction of maxillary elongation takes place in a posterior direction, the growth process in the maxillary region also contributes directly to overall lengthening of the upper
Craniofacial bone growth
jaw. This factor is associated with the prognathism that characterizes the muzzle.
In the region of the forehead, the entire external (cutaneous) surface of the frontal bone receives progressive periosteal bone deposits during active growth. The opposite (meningeal) periosteal surface lining the endocranial side of the frontal bone is largely depository in nature, although a number of localized patches of surface resorption with underlying endosteal bone are present. The frontal bone grows anteriorly and superiorly in
In contrast to the human premaxillary region, the external (periosteal) surface of this region in the monkey is characteristically depository. The
contralateral endosteal side is resorptive. Compare with Figure 65a. X 50. (From Enlow, D. H.: Am. ]. Phys. Anthrop., 1966.)
Figure 78

Comparative morphogenesis
conjunction with the expanding cerebrum. Progressive increase in cranial volume in this area is provided largely by sutural bone deposition, but the marked degree of forward growth in the prefrontal region results in an enlarged contour as the forehead grades into the anterior cranial fossa. The presence of endosteal bone
( 1 8 1 )
(with endocranial surface resorption) in some parts of the lamina interna lining the forehead provides an expansion of internal curvature overlying the large frontal lobes (see Chapter 9) . The placement of the various frontal sutures is such that sutural remodeling cannot produce this changed contour. It is brought about instead by the process of direct cortical drift.
GENERAL PLAN OF FACIAL GROWTH. The
overall enlargement of the face in the monkey is a cumulative, interrelated composite of several growth processes. Lengthening is provided by progressive additions on the posterior facing maxillary tuberosity and the posterior portions of the mandible, thereby increasing the anteroposterior dimensions of the entire face as teeth are added. Forward premaxillary and mental growth contribute to this lengthening, but to a lesser extent. Simultaneously, growth at the various posterior facing sutures and the mandibular condyle is associated with a direct forward displacement of the facial bones. As they grow essentially backward, these bones become translocated in an opposite forward course. Vertical increase is a result of the inferior enlargement of the entire nasal region and extension of the alveolar margin. At the same time, growth at the various downward facing sutures is associated with an inferior displacement
from the actual direction of growth. The opposite (lingual) surface of the cortex is depository. The vertical depth of the maxillary arch becomes lengthened by alveolar bone deposition on its free margin, which can result in a slight protrusion of the premaxillary region during growth. Remodeling differences between the human and monkey maxillary bones provide the morphogenetic basis for the decreased prognathism that is characteristic of the human skull. (From Enlow, D. H.: Am. J. Phys. Anthrop., 1966.)
The premaxillary area and the hard palate in both the monkey (top) and the human (bottom) grow in a downward direction. In the monkey the forward part of the maxillary arch also grows in an anterior course by new bone deposition on outer premaxillary surfaces (in addition to premaxillary sutural growth). The vertical depth of the maxillary arch simultaneously undergoes elongation by continued bone deposition along alveolar margins. The forward part of the human maxilla by comparison grows essentially in a straight downward course. The outer (labial) surface of the human muzzle is resorptive in character because this side of the bone faces away

( 1 8 2 )
of the maxilla, a movement that adds to the total process of downward growth. Corresponding downward movement occurs in the mandible as the ramus elongates behind the upward moving condyle. The depth of the mandibular body is increased by a vertical enlargement at its alveolar margin. Facial widening is brought about by lateral expansion of the zygoma and orbit on each side, by the enlargement of the nasal region, and by displacement at the zygomaticomaxillary suture. Alveolar elongation further contributes to the breadth of the maxillary arch.
In the various regional areas of the nasomaxillary complex and the mandible, virtually all cortical surfaces undergo a succession of localized growth movements that serve to enlarge each area and to maintain its regional shape and relative position. Thus, as new bone is added onto sutural surfaces, the posterior face of the maxillary tuberosity, the alveolar border, and the mandibular condyle, all other parts in each bone simultaneously undergo (1 ) remodeling changes as a consequence of their continued, progressive relocation, and (2 ) separate growth increases in each area in proportion to overall enlargement. These local growth movements follow a complex variety of divergent directions involving variable combinations of surface resorption and deposition as each part drifts in its own particular course.
Comparison of facial growth in man and the Rhesus monkey
It is apparent from the foregoing descriptions that the basic plan of facial growth in the Rhesus monkey parallels that found in man. Their respective patterns and directions of growth as well as displacement are comparable in most areas of the different facial bones. Several marked differences exist, however, in the
Craniofacial bone growth
sequence of remodeling changes that takes place in certain major areas (Fig. 77). They are associated with corresponding differences in the gross topography of the regions involved.
In the mandible, regional directions of growth and the local distribution of endosteal and periosteal bone deposits follow nearly identical patterns, area for area. In the mental region, however, a notable difference occurs on both the lingual and labial sides in the general area between the right and left cuspids. In the human mandible, a prominent chin marks this region, a feature that characterizes the face of modern man. This structure is lacking in Macaca, as well as the extinct species of the genus Homo. The mandible of the monkey, however, possesses a unique "simian shelf" on its lingual side, a structure not found in man but present in some anthropoids. These morphologic characteristics are produced by differing ontogenetic growth processes (Fig. 80).
In the pointed, chinless mandible of the monkey, the entire labial cortex is formed by periosteal deposits. The endosteal surface is resorptive. This growth combination produces cortical drift in a forward labial direction. Conversely, in the human mandible the upper (alveolar) portion of the arch located anterior to the mental foramina is characteristically resorptive. The portion occupied by the mental protuberance itself is typically (but variably) covered by periosteal bone. The differential combination of alveolar regression with progressive mental protrusion is responsible for the formation of the distinctive human chin (Fig. 80). This growth pattern does not occur in Macaca or in other mammalian forms. In the monkey, continued periosteal deposition on the entire labial side contributes to the elongate, angular, pointed nature of the mandible, in comparison with the short, rounded, and flattened forward mandibular arch in man.
On the lingual side opposite the mental

Because of remodeling differences involved in the growth of the monkey and human facial bones, corresponding anatomic differences are produced in several major areas. Compare the slope of the frontal bone, the relative positioning of the upper and lower orbital rims (B) , the angle of the lateral orbital rim ( A ) , the relationships between the tip of the nasal bone and the premaxilla ( C ) ,
the structure of the mental region of the mandible ( D ) , the presence of a simian shelf in the monkey mandible (E and F ) , and the differences in contour seen in the malar area (G and H ) . See text for more complete descriptions and discussion. (From Enlow, D. H. : Am. ). Phys. Anthrop., 1966.)
Figure 80

( 1 8 4 )
region, a contrasting growth pattern is found in these two species. In man the entire lingual side shows a marked accumulation of periosteal bone. In the monkey, however, this lingual surface is largely resorptive, and its endosteal mode of anterior growth complements the forward direction of growth on the opposing labial cortex. At the genial crest, however, a distinct reversal occurs, and periosteal deposits grow in a lingual direction below this line. The combination results in the formation of the prominent simian shelf (Fig. 80). The remodeling differences in the forward portion of the mandible, thus, produce a chin on one side and simian shelf on the other in man and the monkey, respectively. For an evaluation of the functional and phylogenetic nature of these structures, see Hooton (1946), and DuBrul and Sicher (1954).
The mandible of the monkey is noticeably more pointed and elongate in relative proportion than is the lower jaw of man. The arch of the human mandible has a much greater gross convexity, a characteristic associated with the unique regressive nature of the flattened incisor region together with the depository character of the opposite lingual side. Also, the prominent trihedral eminence in the human jaw adds to its overall rounded configuration. This eminence is somewhat more massive in the human than in the anthropoid mandible. It merges abruptly with the relatively short, U-shaped body, and continuous periosteal deposits grade from one to the other. In the monkey, however, a reversal occurs just anterior to the trihedral eminence in which the periosteal surface becomes resorptive on its buccal side. This continues forward to about the level of the second molar. This remodeling pattern brings about a distinct lingual shift of the mandibular body, which is derived sequentially from the posterior moving trihedral eminence, into line with the axis of the more
Craniofacial bone growth
medially positioned, angular body. The dental arch of the elongate, narrow mandible in a young adult Rhesus monkey is surprisingly as long as the rounded, flattened dental arch of the much larger adult human mandible.
The growth patterns found in the anterior portion of the maxillary arch in man and the monkey are basically dissimilar, and they result in contrasting modes of remodeling (Fig. 77). The arch of the maxilla anterior to the malar region is characteristically depository in the monkey. This differs from the typically resorptive nature of periosteal surfaces in the anterior part of the human maxilla. The external surface is convex in the monkey but uniquely concave in the human maxilla. In both species, a predominantly downward direction of growth occurs in this region. In the monkey, however, the forward portion of the maxillary arch, including its separate premaxil-lary bones, grows in a distinct forward course as well. This is produced by periosteal bone additions on the entire labial surface of the forward facing arch. In the concave human arch, the contrasting resorptive nature of corresponding forward-facing surfaces results in an endosteal mode of growth that is actually regressive in character. This produces an essentially downward course of growth in comparison with the downward and somewhat anterior growth movement that occurs in the monkey. These basically dissimilar remodeling patterns are schematized in Figure 79. The growth combination in the monkey produces a premaxillary region that protrudes noticeably forward of the nose. In the postnatal human face, loss of the premaxillary sutures, a lack of forward premaxillary cortical growth, and the reduced extent of anterior displacement associated with sutural growth at the various zygomatic and maxillary sutures result in a marked decrease in maxillary prognathism. The anterior mode of bony and cartilaginous growth

Comparative morphogenesis
in the overlying nasal region, although similarly reduced in extent, brings about the formation of the characteristic human nose which extends well forward of the short maxillary arch (Fig. 80).
In the human skull, it is seen that extensive anterior portions of the face have forward-oriented surfaces that are characterized by processes of regressive, endosteal growth. This occurs on both the mandible and maxilla in a complementary manner. They are functionally interrelated in the continued maintenance of normal occlusion throughout the growth period.
In both the monkey and man, the marked downward rather than primarily forward growth of the entire nasal area is also a critical factor associated with decreased prognathism. Reduced dentition in the monkey further contributes to a facial profile approaching that of man. In the human skull, dental reduction and the distinctively resorptive nature of the anterior maxillary and mandibular arches, together with the essentially vertical orientation of the face as a whole, are primarily responsible for the extreme lack of prognathism found in the human face.
The malar region in both species is characterized by a regressive growth movement in conjunction with the backward growth of the maxillary tuberosity. A significant difference in extent occurs, however, between these regions in the human and monkey skulls. This is related to the placement and differing configuration of the orbital cavities. In man, the cheekbone is noticeably squared. In the monkey, . the cheek area is much more rounded (Fig. 81). As a consequence, the lateral growth movement of the malar region in the monkey involves periosteal deposition that extends farther around onto the anterior-facing surface of the cheek, as illustrated in the accompanying diagrams.
The prefrontal area of the human forehead
( 1 8 5 )
is entirely resorptive on its endocranial, meningeal surface. A more limited and irregular distribution of endosteal bone occurs in corresponding regions of the monkey skull. This difference is related to the much more expansive forward movement of the bulbous human forehead and the extent of curvature involved in the frontal bone (Chapter 9) .
A basic difference exists in growth patterns
This diagram illustrates remodeling differences in the malar area of the monkey (a) and the human (b) face. Note that the anterior surfaces of both are resorptive (—) but that the squared configuration of the human zygomatic complex involves more extensive surface resorption, which extends around onto the lateral side of the zygoma. The rounded contour of the monkey zygomatic region, in contrast, involves a lateral depository surface (+) that extends farther onto the anterior face of the malar. (From Enlow, D. H.: Am. J. Phys. Anthrop., 1966.)

( 1 8 6 )
characterizing the lateral orbital area of the human and simian skulls. In Figure 80, note that this region in man is much more vertically disposed, a consequence of the upright forehead in the human face. The anterior border of the lateral orbital rim is entirely resorptive, and the opposite postorbital surface is depository. This serves to move the lateral rim in a posterior direction as the malar area beneath it grows in a corresponding course. The backward growth of the human malar region, together with the marked forward movement of the forehead, results in a lateral orbital rim (a structure that bridges these divergently moving regions) that is uniquely vertical in its placement. Conversely, in the monkey the forward facing surface of the lateral orbital rim is entirely depository with a resorptive postorbital side. In conjunction with a less marked forward expansion of the forehead, this growth pattern produces a lateral orbital margin that is correspondingly sloping. It grows essentially forward and laterally, rather than posteriorly and laterally as in the human face. In the much more upright face of man, the supraorbital rim is positioned well forward of the infraorbital margin (Fig. 80). However, the lower orbital rim in the monkey remains anterior to the upper margin. These contrasting features are a result of the much greater degree of differential forward frontal growth as well as backward malar movement in the human face as compared with the monkey.
The upright nature of the human face
The wide, flat, characteristically vertical face of man is a composite result produced by several morphogenetic circumstances. The interrelated factors involved are associated with an enlarged cranium and with upright body stance. The notable topographic features of the
Craniofacial bone growth
human face that are related to its vertical disposition include the greatly shortened snout and muzzle, the bulbous forehead, the placement of the eyes, and the configuration of the cheekbones.
THE FACIAL POCKET. In Figure 82, note the difference in configuration of the cranial base in the human and the nonprimate skulls. In the latter, the sloping spheno-occipital complex is relatively straight, and the backward-facing foramen magnum is located at the posterior aspect of the cranium. In man, the cranial floor is characterized by a distinctive downward bend with the foramen located on its ventral side. This is directly related to both upright body posture (Weidenreich, 1924) and the marked expansion of the anterior, middle, and posterior cranial fossae with their associated parts of the brain. Cerebral expansion produces a disproportionately enlarged cranial vault relative to the much lesser extent of growth in the cranial base. The bending of the spheno-occipital complex provides an adaptive adjustment between these two differentially growing regions of the cranium (see page 195). It also results in the placement of the foramen magnum in a ventral location compatible with vertical posture and the spheroidal configuration of the whole skull.
These factors are associated with the formation of a distinctive "pocket" located anterior to the bend of the cranial base beneath the overhanging prefrontal region of the cranium (Fig. 82). This pocket is occupied by the much changed facial complex. The human face, rather than comprising a projecting group of bones that extends essentially forward from a horizontally oriented cranium, is composed of a comparatively abbreviated composite of bony elements located in the space produced by the cranial flexure. The face in general grows downward to a somewhat greater extent than

Comparative morphogenesis
it moves forward, and this inferior manner of enlargement utilizes the region made available by the cranial flexure. In Figure 83 note that the posterior ends of the human maxillary arch retain a constant position relative to the
( 1 8 7 )
ethmoidal and presphenoidal regions of the cranial floor, but that they are brought into much closer approximation to the remainder of the cranial base as a consequence of the downward cranial bend.
The facial pocket. Compare the contrasting orientation of the foramen magnum (A and C) and the anterior cranial region (B and D) in the human (top) and a rodent (bottom, enlarged for comparison). The foramen magnum is placed ventrally in the human but posteriorly in the rodent. The anterior cranial floor and cribriform plate face directly downward in the protruding
frontal region of the human. The cribriform plate of the rodent, however, faces forward into an elongate snout. In the human, these relationships result in a marked flexure of the cranial base, which produces a "pocket" beneath the overhanging forehead. This recess houses the shortened, vertically oriented face. In the rodent note that the face is positioned anterior to the cranium.
Figure 82

( 1 8 8 )
NASAL AND ORBITAL ORIENTATION. Ex
tended cerebral expansion in the prefrontal area is associated with the unique, inferior-facing placement of the olfactory region and the bony cribriform plate. The configuration of the enlarged frontal and prefrontal portions of the human brain produces a displacement
Craniofacial bone growth
of the relatively small olfactory lobes into a ventral position that is oriented so that the olfactory filaments enter directly upward from the nasal cavity below it. Note that the vertical cribriform plate in nonprimate forms faces primarily forward (Fig. 82), and that filaments of each olfactory nerve enter from a projecting
In the human face (top), growth proceeds essentially in a backward and downward direction. Forward growth is abbreviated but produces a slight anterior extension of the nasal region. The human forehead, however, is greatly expanded in
a forward and superior direction. In the nonprimate (bottom), anterior facial elongation is produced by a composite of marked forward in addition to downward and backward growth.
Figure 83

Comparative morphogenesis
snout that is located anterior to the plate rather than inferior to it. In the human skull, the horizontal cribriform plate is oriented so that it faces inferiorly into a more vertically oriented nasal area. The downward nature of growth in the nasal region, without marked anterior extension associated with an elongated snout, is related to the enlarged cerebrum, the downward-facing displacement of the olfactory lobes, the vertical disposition of the olfactory nerves, and the horizontal placement of the cribriform plate. Note the comparatively small volume of the human olfactory fossae and the relatively reduced area for olfactory nerve distribution in the abbreviated snout.
The factor of frontal expansion, together with corresponding enlargement in the temporal lobes, is directly associated with the distinctive forward-facing positioning of the right and left orbital regions (Fig. 84). At the same time, however, this arrangement significantly reduces the extent of the nasal region located between the orbits.* It also contributes to the vertically disposed nature of the nasal region. Thus, effective binocular vision is provided, but at the expense of a reduced olfactory sense. The marked expansion of the cerebrum, in addition to providing a formative basis for the growth factors just outlined, results in the formation of the distinctive human forehead (see below). In Figures 72 and 83, note that the face is located beneath the overhanging floor of the anterior cranial fossa, and that the orbit is placed above rather than behind the posterior portion of the maxillary arch.
GROWTH OF THE FACIAL COMPLEX. The
muzzle region of the face in nonhuman forms follows a basic growth pattern involving (1)
* Scott (1958) has pointed out that the thermoregulatory function provided hy the large nasal cavities in nonprimate mammals has been taken over by the relatively hairless skin of man.
( 1 8 9 )
backward increase in the various posterior portions of the maxilla and corresponding maxillary and zygomatic sutures, (2 ) downward increase as a combined result of alveolar, nasal, and sutural growth, and (3 ) forward increase by direct anterior surface as well as sutural growth in the premaxillary region. The sum of these three growth processes determines the extent of forward projection of the muzzle (Fig. 83). It has long been realized that the jaws of anthropoids, as well as those in some nonprimate forms, are significantly reduced in their relative degrees of prognathism. This is associated with a corresponding reduction in dentition. Decreased prognathism is a combined result of a lesser extent of total forward displacement (in conjunction with posterior growth on the various backward-facing surfaces) together with decreased anterior growth on maxillary and premaxillary surfaces. It is noted that the anterior portions of the forward-facing premaxillary surfaces in both the maxilla and mandible, despite decreased prognathism, are nevertheless depository in character, and that they continue to produce growth movement in an anterior direction by progressive deposition of new bone on their external surfaces.
In the abbreviated muzzle and snout of man a basically different pattern of growth occurs. Maxillary growth proceeds essentially downward and posteriorly (Fig. 83). Forward movement of the growing face is largely restricted to the process of displacement produced by the backward mode of elongation. This results in a face, with its enclosed nasal chambers, that is more vertically than horizontally disposed. The downward enlargement of the middle face in the human skull, as in the monkey and other mammals, is the composite sum of descending nasal as well as maxillary arch growth movement.
In man, this downward manner of facial

( 1 9 0 )
growth is unique in that the concave forward-facing surfaces of both jaws are actually re-sorptive in nature. The "regressive" character of facial growth in the human skull actually involves a recessive growth pattern in some of
Craniofacial bone growth
its parts. In the maxillary arch, however, such cortical recession is concerned primarily with the inferior nature of nasomaxillary growth. A marked degree of posterior regression, as such, is not involved (see previous descriptions of
The marked forward and lateral expansion of the anterior and middle cranial fossae (A and B) have produced a "rotation" of the right and left orbits toward the midline. As a consequence, the orbital cavities are oriented in a more forward-
facing position (F) than in other mammals (as in the deer, G). This also results in a decrease in the breadth of the nasal bridge and interorbital region, as compared with other forms (D and E).

Comparative morphogenesis
maxillary growth and remodeling). The relative absence of prognathism in the human muzzle thus is not a direct consequence of extended endosteal (surface resorptive) growth of the labial premaxillary cortex in a posterior direction. It is apparent, however, that the resorptive nature of its growth pattern nevertheless precludes any significant forward elongation in the premaxillary region other than that produced by extension at the alveolar crest (Fig. 79).
Although nasal growth is essentially downward (and posteriorly as the whole maxilla grows in a corresponding backward direction), the lateral bony walls of the nose continue to grow in a slight forward course (Fig. 83). The topographic result is the protruding, overhanging nose of man, a distinctive facial feature. Reduction in the interorbital area, however, and the downward-facing orientation of the olfactory lobes combine to limit the forward extent of nasal projection (Fig. 84).
The marked downward growth of the combined nasomaxillary complex in the human skull and in other primates produces a corresponding lengthening of the mandibular ramus, thereby providing proper maxillary-mandibular occlusion. The nearly vertical orientation of the upright ramus is related to the positioning of the mandible and its dental arch more posteriorly than in other mammalian forms. This is a result of the placement of the flat, vertically disposed face within the facial pocket formed by the cranial base flexure (Fig. 82).
The resorptive, regressive character of the flattened alveolar region in the forward part of the mandible further contributes to the distinctive upright configuration of the face (Fig. 85). Vertical facial alignment is extended superiorly by the presence of the bulbous, massive human forehead. This is related to the enlarged cerebral cortex behind it, which in turn is associated with the numerous other
( 1 9 1 )
morphologic features of the vertical face and upright body posture. The characteristic regressive nature of the lateral orbital rims and the forward-facing placement of the orbits complete the vertical disposition of the human facial complex.
In Figure 80 it is seen that the anterior point of the nasal bone in the human face protrudes forward of the premaxillary alveolar margin below it, in contrast to the pattern in the anthropoid face. Similarly, the forward edge of the supraorbital rim in man is positioned noticeably forward of the lower orbital margin. The reverse situation is found in the nonhuman face. These relationships are associated with the relative extent of forward frontal growth and posterior malar growth in the different species.
The human facial complex is distinctly flattened in configuration. This feature is a result of several growth circumstances, including the regressive manner of cortical growth in the flattened incisor regions of the shortened, rounded maxillary and mandibular arches. In comparison, the jaws in most other forms are angular and pointed in nature. The squared cheekbones, the characteristic positioning of the orbits, the parallel zygomatic arches, the massive development of the mandibular trihedral eminences, and the expanded and forward-facing temporal regions all contribute to the flattened character of the human face. Note also that the solid lateral orbital wall faces forward in the human skull but laterally in the monkey (Fig. 77).
In most mammalian forms the elongate maxillary arch is positioned so that the greater part lies forward of the orbits. The last molar is at a level beneath the inferior orbital rim (Fig. 85). In the human craniofacial skeleton, more than half of the maxillary arch is positioned below rather than anterior to the orbital cavities. In nonprimate forms the presence of a muzzle that lies largely anterior to the orbits

( 1 9 2 )
is a result of the predominantly anterior mode of growth (and displacement) in conjunction with the more lateral and posterior location of the orbital cavities. The prefrontal cerebral lobes do not extend forward to the level of the inferior orbital margins (Fig. 85). In contrast, much of the facial area of man lies directly below the orbital region within the "pocket" produced by the cranial flexure. The prefrontal lobes extend forward to a level approximately even with the inferior orbital rim, and in doing so the supraorbital margins have become positioned anteriorly so that they protrude slightly
Craniofacial bone growth
forward of the inferior orbital rims. Thus, the upper portion of the facial complex moves superiorly and anteriorly, while the lower portion undergoes an inferior and a posterior direction of growth movement. This produces, in effect, a "rotation" of the human face by a process of differential growth movements, as schematized in Figure 85. The effect of these differential movements is augmented by the lack of forward growth on anterior premaxil-lary surfaces.
A consequence of the growth patterns just outlined is the inclusion of a large area of the
The upright human face. The facial orientation of the human and dog skulls are compared. In the latter, the distinctly forward and somewhat downward elongation of the snout and muzzle produce a long, sloping facial contour (D and E). In contrast, the abbreviated nose and jaws of man grow slightly forward, but predominantly downward
and backward (C and F). The forward expansion of the human forehead (A) and anterior and superior rotation of the orbits (B), together with the growth movements of the nose and jaws, produce a distinctively upright alignment of the face as a whole.
Figure 85

Comparative morphogenesis
maxilla located just inferior to each orbital cavity. This region is further increased by the extensive widening and squaring of the malar area in conjunction with orbital positioning. The suborbital region becomes hollowed to form the cavernous maxillary sinus. Sinuses in general are found in various sizes and locations in the skulls of many different mammalian species. In the deer, for example, a sizable maxillary sinus is present just superior to the maxillary dental arch. It provides a thick bony shell of supportive maxillary bone above the apices of the tooth roots. Medial to the right and left halves of the arch, the expansive surfaces of the nasal chambers form a greatly widened as well as elongate chamber. The paired, lateral sinuses are associated with a movement of the lateral tooth-bearing walls to each side in order to accommodate this marked internal nasal expansion. In general, the occurrence of cranial or facial sinuses serves to expand given areas of bone in conjunction with regional adaptations of morphologic structure. In man the presence of very large maxillary sinuses represents a response to the posi-
( 1 9 3 )
tioning of the maxillary arch in a location beneath each orbit. The forward and lateral expansion of the frontal and temporal cerebral lobes has, in effect, displaced the orbits from a typical mammalian position behind the maxilla to a location superior to the maxillary arch. This has resulted in the formation of a unique bony orbital floor, which serves also as an overlying roof for the sinus occupying the expanded region below each orbit.
In summary, the distinctive, upright face of man is a composite result of ( 1 ) the essentially downward elongation of the nasal cavities, without a marked degree of corresponding anterior projection, ( 2 ) a resorptive, flattened, downward-growing muzzle, (3 ) upright and regressive lateral orbital rims, ( 4 ) the vertically aligned superior and inferior orbital margins, ( 5 ) a regressive, flattened, and squared malar region, ( 6 ) a regressive, resorptive alveolar cortex together with a chin in the forward part of the mandible, (7 ) a greatly decreased extent of forward displacement of the snout, as well as of the muzzle, and (8 ) a greatly expanded forehead region.

In most vertebrates the general slope of the muzzle and snout is an extension of the contour formed by the skull roof. Thus, the flat, horizontally oriented forehead in nonprimate forms continues forward onto the elongate, projecting, horizontal face without an abrupt change in profile. In the anthropoid skull, the forward bulge of the cerebrum produces a more upright forehead, and its contour similarly continues down onto a near vertical face. In man this same situation is extended to an even greater vertical calvaria-facial relationship. The massive expansion of the cerebrum and the frontal region of the face is related to a displacement of the remainder of the facial complex into a much more inferior but less anterior position. The olfactory area of the brain is oriented almost directly downward into an upright face rather than forward toward an elongate snout, as in most nonprimate
194
(9)
Growth of
the calvaria and
the cranial base
forms. Thus, as the forehead grows upward and forward to a more vertical position, the remainder of the face similarly "rotates," in effect, downward and backward to a correspondingly vertical plane (see preceding chapter).
The cranial base in higher primates has a marked downward flexure. The angle produced by this bend results in a distinctive "facial pocket" beneath the overhanging base of the cranium, as described in Chapter 8. The developing facial complex is positioned largely within this pocket. It occurs ventral to the anterior cranial fossa and anterior to the clivus.
A significantly disproportionate mode of growth exists between the cerebral and cerebellar hemispheres and the ventral axis of the brain. A process of differential growth is involved in which the hemispheres, containing abundant cortical tissue, grow a great deal

Calvaria and cranial base
more rapidly and to a far greater extent. The ventral axis, composed largely of tracts, expands more slowly and involves a lesser amount of tissue (Fig. 91). The process of differential growth between these two general areas of the enlarging brain directly influences the modes of growth in the skull roof and the cranial base, respectively. It is a key factor involved in the structural relationships among the calvaria, the cranial base, and the face. The relatively stable nature of the cranial base during growth has been demonstrated by Moss and Greenburg (1955).
The characteristic flexure in the cranial base of the human and some other primate skulls has several fundamental morphologic relationships (Fig. 82). The prefrontal lobes produce a marked forward bulge that results in the formation of the forehead and further brings about a downward rotation of the anterior cranial floor, a factor contributing directly to the cranial base flexure. As seen earlier, this movement is also involved in the downward rotation, in effect, of the entire facial complex. The upright posture of man involves placement of the foramen magnum on the inferior side of the skull rather than at its posteriormost extremity. This location is produced by the downward bending of the spheno-occipital portion of the cranial base (the clivus). Relative to the frontal, temporal, and occipital parts of the brain, the foramen magnum occupies a midventral position providing proper head balance associated with a vertical, bipedal body stance.
If a strip of adhesive tape is firmly applied to one side of a rubber balloon and the balloon is then inflated, an expanded configuration is produced that shows lobation similar to that seen in the human brain and cranium. Prefrontal, parietal, and occipital "lobes" are produced around a restricted base. This analogy is based on the differential extent of en-
( 1 9 5 )
largement in the base as compared with the much greater and more rapid expansion of the bulging hemispheres around it. The taped portion of the balloon also shows a distinct flexure analogous to the bend in the ventral part of the brain and the cranial base (compare with Figure 90).
In summary, the flexure of the cranial base is directly associated with two interrelated growth factors. First, this bending is brought about by the formation of enlarged endocranial fossae, which in turn reflect the much greater degree of expansion of the hemispheres compared with the ventral axis of the brain. Second, the flexure provides a location for the foramen magnum that corresponds with upright body posture.
It was pointed out in Chapter 8 that vertical posture, bipedal stance, an enlarged cerebrum, mobile arms with dexterous hands, forward-facing eyes, a reduced snout and muzzle, and a ventrally positioned foramen magnum are human characteristics that are all closely interrelated and mutually interdependent. The basis for any one provides the basis for the others. The distinctive features of the human face, involving the eyes, nose, forehead, and muzzle, are thus a mutual result of many of the same factors associated with the characteristic configuration of the calvaria and the cranial base.
The skull roof
The growth of the bones in the skull cap is adapted to a "tension system" in which the pulling effect produced by the enlarging brain tends to separate the bones at their sutures and, presumably, thereby stimulate sutural bone growth. In addition, bone growth activity occurs on all periosteal and endosteal surfaces. Two periosteal surfaces are present: the outer

( 1 9 6 )
(cutaneous) and the inner (meningeal). Each cortical table (lamina) has a corresponding medullary, endosteal surface that is continuous with the trabeculae of the diploe.
In Figures 86 to 89 it is seen that the entire cutaneous side of the cranial vault is depository in nature. The cortical bone comprising the outer lamina is thus periosteal in type and
Craniofacial bone growth
is circumferentially oriented. The opposite, endosteal surface of this external cortical table is characteristically resorptive.
The meningeal surface of the inner, endo-cranial cortex is also largely depository in nature. This cortical plate is composed of periosteal bone (produced by the osteogenic component of the dura), and its endosteal
The distribution of resorptive (dark stippled area) and depository (light stippled area) periosteal surfaces, anterior view.

Calvaria and cranial base
surface is typically resorptive. The fact that the endocranial side of the calvaria actually grows inward although the bones themselves become displaced in an outward manner was puzzling to earlier workers (for historic accounts, see Baer, 1954; Moss, 1954).
Periosteal bone additions on both the external and the endocranial sides of the skull roof, with corresponding resorptive removal from their corresponding endosteal surfaces, serve to increase the thickness of the entire bony wall, to expand the diploe, and to thicken each cortical plate proportionately.
The actual outward movement of the cortical laminae that comprise the skull roof is produced by centrifugal displacement brought
( 1 9 7 )
about by the expanding brain. The bone itself is presumed to be essentially passive during this movement except for adjustments in proportionate thickness and curvature. As the various bones in the calvaria become separated, continuous contact at sutures is simultaneously maintained by horizontal, circumferential extension of the cortical plates at the sutural surfaces of each bone (see page 95). As deposits of new bone continue to be added at their margins, the internal volume of the entire cranial cavity is correspondingly increased (Figs. 97 and 98). It is noted that this process of enlargement does not involve a marked "drift" of each cortical plate produced by external deposition in combination with endo-
The distribution of resorptive (dark stippled area) and depository (light stippled area) perios
teal surfaces, dorsal view of cranial floor (left) and inner side of skull cap.

( 1 9 8 ) Craniofacial bone growth
The distribution of resorptive (dark stippled area) and depository (light stippled area) perios
teal surfaces, lateral external (top) and internal (bottom) views.

Calvaria and cranial base
cranial resorption. Instead, the enlargement of the cranial roof is largely a process of displacement with corresponding lateral elongation of the individual flat bones at their contact edges.
The growth process just described functions to progressively enlarge the calvaria in a manner that approximates the existing contour of the surface and its arc of curvature. The basic growth and remodeling factor of relocation thus is not as extensively involved in these bones as in other bones of the craniofacial
( 1 9 9 )
skeleton. A remodeling mechanism at the sutural margin can occur, however, that functions to adjust the curvature to conform with the surface configuration of the brain and to produce changes in contour (Massler and Schour, 1941; Baer, 1954; Moss, 1954; Wein-mann and Sicher, 1955; Hoyte, 1966). This is brought about by a process of endocranial resorption on the meningeal surface adjacent to the suture edge, together with deposition on the contralateral endosteal surface. The result-
The distribution of resorptive (dark stippled area) and depository (light stippled area) periosteal surfaces, ventral view. A, malar region; B,
Figure 89
pterygoid plate; C, petrous projection; D, jugular fossa.

( 2 0 0 )
ing. formation of endosteal bone in the inner table, in conjunction with surface bone formation on the periosteal side of the external table, moves both laminae in an ectocranial direction. This produces a generalized expansion of contour over the entire outer and inner cortical surfaces as the arc of curvature becomes decreased. In a series of human skulls with primary and mixed dentition studied by the author, this remodeling process was not found at all locations in the different sutural margins of the skull roof. However, it was observed in some scattered sutural areas and, where present, served to locally adjust surface contours and curvature. A consistent pattern of distribution of these local sites was not apparent in
Craniofacial bone growth
the particular skulls studied, which reflects the labile nature of the skull roof in response to varying skull configuration and size.
The skull roof is composed of the separate parietal bones and portions of the frontal and occipital bones. The latter two also contribute to the cranial floor. These are all dermal (intra-membranous) elements, and the growth processes described above characterize each one. However, those portions of the frontal and occipital bones that are located in the cranial floor follow a fundamentally different mechanism of growth.
GROWTH FIELDS. A well-defined, circumferential reversal line encircles the walls of the
The differential manner of expansion between the calvaria and the cranial base (and all related portions of the brain). The hemispheres and the
calvaria (B) grow to a much greater extent than the midventral part of the brain and the cranial base (A).

Calvaria and cranial base
calvaria on the meningeal side (Fig. 88). This key line separates the skull roof from the endocranial basin that forms the floor and a portion of the lateral walls of the cranium. Significant differences in the basic mode of growth occur above and below this line of reversal. Note the relatively complex surface topography that characterizes both the inner and the outer sides of the cranial base as compared with the calvaria. The comparatively simple growth pattern superior to the reversal line is in marked contrast to the complex regional combinations of growth and remodeling changes that occur in the more irregularly contoured cranial floor below the line. This is true for both the external and the endocranial sides of the skull wall.
In Figure 88, it is seen that this critical line of reversal, separating the contrasting types of growth fields above and below it, abruptly crosses the different bones without regard to the placement of suture junctions (see discussion of the field concept of growth, page 83). Thus, the entire surface of an individual bone does not function as a single, uniform growing unit. Instead, it is composed of separate growth fields, each following its own mode of growth activity. The circumcranial reversal line crosses the different bones in such a manner that it places a portion of each bone (frontal, parietal, occipital) superior to the line within the depository endocranial surface growth field. The remainder of each bone lies below the line in a predominantly resorptive surface growth field. Note that the reversal is aligned continuously, without interruption, as it extends from one bone to the next. It crosses, rather than follows, suture lines.
The cranial floor
In Figures 87 and 88, it is apparent that the greater portion of the bony surface lining the
( 2 0 1 )
cranial floor is resorptive. The underlying cortical bone is composed of typical endosteal types (Figs. 95b and 96). However, note that several well-marked regional, periosteal reversals occur, such as the petrous reversal in this protruding portion of the temporal bone. The fundamental pattern of growth and remodeling in the cranial floor differs significantly from that in the relatively even-contoured cranial roof.
BASIC PLAN OF GROWTH. Four basic considerations are involved in the growth of the cranial floor. First, the cranial floor conforms in its growth to the differential degrees of expansion of those particular portions of the brain that it encloses. Second, its growth pattern must provide positioning for the numerous passageways to and from the cranial cavity, through which the spinal cord, cranial nerves, and blood vessels pass. The cranial floor, in contrast to the vault, is the gateway for these structures. Third, it adjusts to the placement of the skull as a whole in relation to the vertebral column and the posture of the body. Fourth, its configuration directly influences the disposition of the contiguous facial complex.
A key factor involved in the basic mode of growth in the cranial floor, as compared with the calvaria, is the marked differential rate and extent of enlargement in the dorsal and lateral portions of the brain relative to its midventral region (Fig. 90). The brain as a whole does not expand uniformly in all directions. Instead the ventral axis (floor of the brain comprising the underside of the hypothalamus, the medulla, pons, etc.) is relatively stable. Its rate and extent of growth lag considerably, relative to the enormous enlargement of the cerebral hemispheres (Fig. 91). This longitudinally oriented ventral axis provides the relatively stable base around which the remainder of the brain expands in a disproportionate manner.

( 2 0 2 )
This factor is also associated with the distinct flexure of the cranial base, as noted previously.
Because of their differential modes of expansion, the calvaria and the cranial floor have correspondingly different mechanisms adapted to their growth. As seen in the previous section dealing with the cranial vault, sutural bone growth provides an enlargement of the superior portion of the cranial cavity in up-
Craniofacial bone growth
ward, lateral, anterior, and posterior directions. For the most part, major remodeling changes are negligible. Existing contours are maintained during continued postnatal growth with adjustments related primarily to expansions in curvature and proportionate increases in the thickness of the calvarial wall. Major changes in configuration produced by the process of relocation are minimal compared to most other
The much greater enlargement of the hemispheres relative to the midventral portion of the brain is illustrated (left; lateral view). In the overlying occipital bone (right; dorsal view), note that the outward growth of the supraoccipital
region greatly exceeds the slight backward growth movement of the foramen magnum. Contrasting mechanisms of growth bring about the differential manner of enlargement between the two parts of this single bone.
Figure 91

Calvaria and cranial base
bones. Adjustments concerned with the through passage of major nerves and vessels and the housing of appendages, such as the hypophysis and the auditory mechanism, are not involved.
Conversely, in the cranial base and floor a far more complex, interrelated series of growth and remodeling changes are necessarily involved in order to accommodate major regional differences in growth rate and also to maintain positional relationships between the bone and the major nerves and vessels passing directly through the bone. This complex pattern of growth involves combinations of (1 ) extensive cortical drift associated with the predominantly resorptive surface of the endocranial floor, (2 ) endochondral growth at synchondroses, and (3 ) a differential gradient of su-tural growth as the walls of the calvaria grade into the lateral parts of the cranial floor.
ENDOCRANIAL COMPARTMENTS. The floor of the cranium is characterized by the presence of several well-defined fossae, in contrast to the evenly contoured cranial vault. This com-partmentation follows the irregularly surfaced, ventral side of the brain, and the fossae contain the various lobes, hemispheres, and other parts of the brain as well as appendages such as the pituitary body and olfactory bulbs. The cranial floor thus is composed of a number of relatively confined, isolated culs-de-sac of varying sizes, and the configuration and placement of these compartments is such that sutures, where present, cannot solely produce proportionate expansion of curvature during growth.
Because of the factors just mentioned, the bony walls in the greater part of the cranial floor grow by a direct process of cortical drift in an ectocranial direction. The resorptive meningeal surface, together with a depository endosteal side, result in formation of an inner table that is characteristically composed of
( 203 )
endosteal bone. The outer table shows the opposite growth combination; its cutaneous side is depository with a resorptive, contralateral endosteal surface. The result is a composite outward movement of both cortices in conjunction with the outward expansion of the underlying parts of the brain. This growth process provides two basic growth functions. It serves to enlarge the internal volume of the cranium in the regional compartments, and it provides the remodeling basis for the expansion of curvature. In Figure 92, it is apparent that sutural growth in the endocranial fossae, such as those occupied by the prefrontal and the temporal lobes, cannot provide total expansion in the variety of divergent directions involved. Thus, expansion of internal cranial volume and major changes in contour are simultaneously brought about by the cortical drift mechanism of growth. This combined result could not be achieved by the sutural growth process alone, as in the cranial vault. The total absence of sutures in some endocranial pockets, and the placement of sutures where present in other fossae in a manner that cannot entirely produce curvature expansion, is thereby accommodated by the drift growth process (Figs. 97 and 98).
In portions of the lateral floor of the cranium and in the lateral walls, sutural bone growth contributes to cranial enlargement. A decreasing gradient of activity occurs as the axis of the cranial base is approached (Figs. 97 and 98). This is a response to the differentially decreased extent of growth in the base, and the correspondingly increasing gradient of growth by the drift mechanism, which in turn provides the remodeling changes associated with the cranial floor. This growth pattern provides the basis for maintaining stable relationships between the cranial floor and the passage of nerves, vessels, and the spinal cord, as will be described later.

( 2 0 4 )
The elongation of the cranial base by continued growth at the spheno-occipital synchondrosis (and a lesser contribution from the sphenoethmoidal junction) together with generalized cortical drifting in an anterior direction carry the middle face in a forward course. This movement correspondingly expands the sizable dimensions of the pharyngeal compartment just below the spheno-occipital complex. As this occurs, the anterior-posterior breadth of the mandibular ramus is proportionately increased, thereby bridging the progressively enlarging span between the temporal bone and the forward-moving placement of the maxillary arch. The downward enlargement of the middle face is similarly accompanied by a vertical lengthening of the ramus. A significant forward expansion of the anterior cranial fossa contributes to the marked enlargement of the "facial pocket" below it as the face simultaneously continues to elongate. This maintains proportionate position of the forehead region overlying the maxilla, although differential
Craniofacial bone growth
growth processes in some facial areas produce noticeable changes in topographic facial contours, as in the nose, glabella, premaxilla, malar region, and chin.
In summary, growth processes in the cranial vault and the cranial base involve the following factors (Figs. 93 and 94) :
1. The roof of the skull expands largely by sutural growth with corresponding, proportionate increases in cortical thickness on the periosteal surfaces of both the internal and external tables. Regional adjustments may occur in some localized sutural areas in response to changing contours.
2. The longitudinal base of the brain grows at a differentially limited rate and extent relative to the massive hemispheres. Differences in basic mechanisms of growth occur in corresponding portions of the skull.
3. The cranial floor is compartmented into numerous fossae, in contrast to the lateral walls and the roof.
In the culs-de-sac of the cranial floor, the process of sutural growth cannot accommodate the total extent of expansion, as seen in A. In addi
tion, cortical drift is directly involved (B), and in combination with sutural additions produces the enlargement of the various fossae.
Figure 92

Calvaria and cranial base ( 2 0 5 )
Schematic interpretation of growth in the cranial base and calvaria. In diagram 1 bones of the calvaria ( a ) are separated by sutures ( S ) . The bones of the cranial floor (b, c, y) are also separated by sutures ( S ) or by synchondroses. The circumcranial line of reversal is indicated by R. The endocranial fossae are represented by x. Posi
tion markers are shown in both the calvaria and the cranial base (black triangles and large dots).
In diagram 2, expansion of the calvaria by sutural bone growth is shown. Note the decreasing gradient of bone additions as the cranial floor is approached. Growth of the cranial base is not represented (see Figure 94) .

( 2 0 6 )
4. T h e cranial f loor is the pathway for
nerve, spinal cord, and blood vessel passage.
5. Growth in the cranial floor involves a
decreasing gradient of sutural activity as a re
sult of differential growth. Sutures in the
endocranial fossae are oriented so that they
Craniofacial bone growth
cannot provide the total extent of contour
expansion.
6. T h e elongation of some portions of the
cranial base is provided by synchondroses.
These produce an expansion of cranial volume
but require corresponding remodeling changes
The result of calvaria growth, as produced in Figure 93, is shown. Each component of the skull roof has also increased in cortical thickness.
The original position of the cranial floor (as in Figure 93) is indicated by broken lines. The lateral portions of the floor have now grown outward by direct cortical drift. The external surface is depository ( + ) , and the internal (l ining) surface is resorptive ( — ) . An increasing gradient of drift occurs as the lateral walls grade into the floor. Although the endocranial surface is predominantly resorptive, note that the elevated partitions (y in Figure 93) are depository. They increase in size in conjunction with fossa expansion. The
markers in the calvaria have become widely separated. The markers (large dots) in the cranial base, however, remain relatively less separated. This factor is involved in maintaining stable relationships with nerves and vessels as they pass through the cranial floor. It is apparent that the skull roof moves primarily by sutural bone growth. The slower-growing cranial floor, on the other hand, enlarges in dimensions by a decreasing gradient of sutural expansion together with direct cortical drift. The latter growth process is negligible or entirely absent in most portions of the calvaria (except in sutural remodeling).

Calvaria and cranial base
to sequentially position the different parts of the bones involved.
7. Outward expansion of the cranial floor as a whole is largely accomplished by the process of cortical drift in an ectocranial direction. An increasing gradient of drift occurs as the lateral walls grade into the floor, and growth by direct drift proceeds in combination with the limited contributions by ventral sutures and synchondroses.
8. In addition to providing outward growth, the process of drift also produces the remodeling expansion of contours in the various endo-cranial compartments.
9. Cortical drift in the floor and sutural growth in the vault provide the basis for their differing rate and extent of enlargement.
10. A key factor is that cortical drift provides a mechanism for local remodeling changes. Overall expansion of the entire irregularly contoured ventral part of the cranium is produced largely by drift, yet at the same time maintenance of constant relationships with the spinal cord, cranial nerves, hypophysis, auditory apparatus, etc., is provided. Just as sutural growth, as a sole mechanism, cannot accommodate expansion of curvatures in the endocranial fossae, neither could it sustain the constant positions of nerves and vessels passing through foramina in the cortex.
11. The mode of growth in the cranial floor provides a basis for structural relationships between the vertebral column, upright posture, and the vertically oriented facial complex. These factors involve a marked downward flexure of the cranial base, a circumstance also associated with the disproportionate nature of growth in the calvaria and the cranial base.
The role of each separate bony element of the cranial floor in this complex, composite pattern of growth is described in the following sections. An evaluation of the total growth
( 2 0 7 )
picture involving all the various individual components in relation to one another is also presented.
THE OCCIPITAL BONE. The originally separate units of the occipital complex, containing both dermal and endochondral elements, become fused into a single bony composite that forms, in addition to posterior parts of the cranial vault, a sizable portion of the cranial floor in the regions of the cerebellar and occipital fossae. The bone is penetrated by the foramen magnum, and this relationship involves a critical balance of growth processes in order to sustain relative positions during growth.
In Figure 88, note that the circumcranial line of reversal on the endocranial surface crosses the superior portion of the occipital bone (squamous portion including the interparietal). Above this line, the lining bony cortex is characteristically composed of inward-growing periosteal bone tissue. This continues down along the midline sagittal ridge to the posterior lip of the foramen magnum. The ridge becomes progressively more prominent as a result of its periosteal manner of growth together with the deepening of the posterior fossae by their endosteal modes of cortical drift. The extent of periosteal deposition on this ridge is variable.
Below the circumcranial reversal line, the remainder of the endocranial occipital surface is largely resorptive.* The underlying cortical bone is endosteal in nature and is composed principally of a convoluted type of bone tissue. The direction of growth produces a direct, outward drift of the cortex in this extensive area. In contrast, outward movement is produced primarily by displacement (associated with
* Using vital staining methods, Hoyte (1967) has recently demonstrated comparable resorptive surfaces in the cranial base of experimental animals.

( 2 0 8 )
sutural bone growth) in the superior parts of the occipital region. The entire external side of the occipital bone is depository in nature (Fig. 88).
It is seen in Figure 91 that backward enlargement of the posterior cranial fossa greatly exceeds a corresponding but very slight backward movement of the more stable foramen magnum. The foramen necessarily moves in this direction because its downward growth follows the backward-sloping brain stem as it grades into the spinal cord. This backward relocation is not marked, however, because of the nearly vertical alignment of the spinal cord relative to the cranial floor. A somewhat greater extent of posterior movement occurs in anthropoids because of the greater backward angle of the cord. In man the foramen shifts in an essentially downward direction. The very slightly backward but predominantly downward movement (drift) of the foramen magnum is brought about by the combination of endocranial resorption and ectocranial deposition. The fact that this area moves outward primarily by cortical drift permits selective degrees of posterior movement by the foramen in comparison to the adjacent cerebellar and occipital fossae. In Figures 91 and 97 note the decreasing gradient of sutural bone growth as the foramen is approached from the calvaria. The extent of cortical drift, however, follows a correspondingly increasing gradient as the foramen is neared. Thus, the foramen moves outward primarily by the process of cortical drift. The floor of the large occipital fossa, on the other hand, moves in an ectocranial direction by both sutural bone growth and drift in reciprocal combinations. As one decreases the other correspondingly increases in the two general regions of the bone. The end result is a marked downward and backward movement of the entire posterior base of the skull, but with a significantly lesser degree of foramen
Craniofacial bone growth
relocation in a posterior direction. A slight degree of postnatal enlargement in the diameter of the foramen magnum occurs, in conjunction with the enlarging cord, as resorption proceeds from the meningeal cortical surface with deposition on the external side.
The clivus of the cranial base is also lengthened by the growth movements just described. However, a significant degree of elongation is also produced by endochondral bone formation at the spheno-occipital synchondrosis. The greater part of this enlargement takes place on the occipital side of the cartilage junction (Fig. 97). This produces an obliquely downward and backward displacement of the basioccipi-tal. The entire occipital and sphenoidal complex also undergoes inferior displacement associated with sutural bone growth at the various temporal, parietal, and occipital sutures.
In Figure 97, note the slightly posterior but markedly inferior growth movement (drift) of the lateral exoccipital region in association with the foramen magnum. The contribution of sutural growth at the occipital sutures to downward movement in this area is negligible, although the temporoparietal suture is indirectly involved. In the region of the adjacent clivus, downward movement is a composite process including elongation of the basioccipital at the spheno-occipital synchondrosis and a degree of downward displacement produced by sutural growth at the temporoparietal junction. A constant process of remodeling in the sphenooccipital complex occurs in order to maintain alignment between the foramen magnum and the floor of the frontal fossa. This involves a downward growth movement of the cranial base in addition to its downward manner of displacement. The remodeling adjustment is carried out by a progressive, downward rotation of the cranial base from the relatively stable (but descending) anterior rim of the

Calvaria and cranial base
foramen magnum to the junction of the sphenoid with the floor of the frontal fossa. This growth process further contributes to the characteristic flexure present in the cranial base. The endocranial lining (meningeal) surface of the clivus is resorptive, and its cortical bone is endosteal in type. This combination produces a downward and forward rotation or tilt, in effect, of the basioccipital as it elongates at the synchondrosis and simultaneously drifts forward. The growth movement on the endocranial side is complemented by a corresponding movement of the external cortical plate involving the converse process of periosteal deposition and endosteal resorption. Note that the anterior-posterior position of the foramen magnum is relatively stable, although it moves significantly downward and slightly backward. Thus, the bones around it undergo different growth movements that differentially increase in extent in a direction away from the foramen. Unlike the various other synchondroses in the cranial base, the spheno-occipital synchondrosis is believed to remain active in growth throughout adolescence (Ford, 1958).
In summary, most of the meningeal surfaces of the occipital bone are resorptive. A periosteal reversal occurs in the squamous portion as the occipital grades into the cranial vault. Here, the primary mode of cranial expansion is represented by sutural bone growth. The midline bony ridge is also variably depository in nature. The entire cutaneous side of the occipital bone is depository. The basal posterior portion (cerebellar fossa) is characteristically resorptive. This provides a drift mechanism of growth that brings about a disproportionately extensive, backward expansion of the fossa relative to a much lesser posterior movement of the foramen magnum. The foramen moves downward in a nearly vertical plane with a very slight shift in a posterior direction as it follows the brain stem. This process lowers the
( 2 0 9 )
foramen in proportion to the inferior enlargement of the cerebellar fossa. The fossa represents one of several compartments that require a drift mechanism of contour expansion in addition to sutural growth. The endocranial surface of the basioccipital region of the clivus is resorptive, which produces a forward and downward rotation of this area in order to align the cranial base with the floor of the frontal fossa and at the same time maintain constant position relative to the more stable foramen magnum. The inferior direction of enlargement in this region of the cranial base is a result of elongation at the synchondrosis, by sutural growth in the lateral walls of the skull and by the remodeling drift process just mentioned. The relative positions of the various cranial nerves passing through the occipital bone do not become displaced by virtue of the differential drift mechanism of growth, for the same reason that the foramen magnum maintains its relative position even though the large fossae on all sides of it undergo extensive enlargement.
THE SPHENOID BONE. Like the occipital bone, the sphenoid represents a fused composite including a midline portion beneath the axis of the brain (the body of the sphenoid, a slower-growing region) and several flattened, laterally extended wings that form portions of the middle and anterior cranial fossae. These latter regions expand in dimensions at a differentially greater rate than the sphenoid body. A number of cranial nerves and major blood vessels pass through the sphenoid into and from the brain, and they maintain relatively constant positional relationships to each other as well as to the cranial base throughout the growth period.
As in other components of the cranial floor in general, the endocranial surface of the sphenoid bone is largely resorptive. The cortex


Calvaria and cranial base
underlying the dura is composed of typical endosteal, convoluted bone tissue (Fig. 951?). In Figure 87, note that a characteristic reversal occurs in relation to the sides of the endo-cranial prominence supporting the sella turcica. The cortex forming the walls of this elevation is depository. The entire projection occupies a large recess in the ventral region of the diencephalon. It provides a longitudinal, midline partition that separates the right and left middle cranial fossae. The sphenoidal area as a whole has a growth pattern involving a generalized downward direction of cortical drift in combination with an increasing gradient of sutural expansion in the lateral regions of the wings. This produces an enlargement of the cranial floor and serves to expand the concave contours of the lateral fossae. The large midline elevation produced by this periosteal reversal provides a bony protuberance that occupies the large recess at the floor of the brain, and it also functions to house the hypophysis.
In Figure 94, the formative basis for this growth pattern is schematized. As already seen, the floor of the cranium is composed of a number of regional pockets or fossae, and these compartments are separated from each other by several bony partitions, including the sella, the petrous portion of the temporal bone, the crista galli, and longitudinal midline ridges. As the contours of various fossae expand in
( 2 1 1 )
curvature and dimensions by a process of outward drift, these separating partitions become correspondingly enlarged, in proportion, by periosteal endocranial bone deposition. The characteristic reversal at the base of each partition provides differential directions of cortical movement—endosteal on one side of the line and periosteal on the other—which serves to increase the overall dimensions of both the fossae and their separating bony walls. In conjunction with these various growth and remodeling processes, the ectocranial side of the sphenoid is, for the most part, depository in nature (see later paragraphs). This serves to move its external cortical plates in an outward direction corresponding to the generalized growth of the endocranial portions. Extending from the sphenoidal wings toward the longitudinal midline axis of the sphenoid, a reciprocal gradient of growth occurs between sutural bone deposition and outward cortical drift, just as it did in the occipital bone. As the midline portion of the sphenoid is approached, sutural bone additions progressively decrease, and growth proceeds largely by an increasing degree of cortical drift. As in the occipital portion of the cranial floor, this is a direct adaptation to (1 ) the expansion of contours in the cranial fossae that cannot be accommodated solely by the sutures present; ( 2 ) the differential rates of growth between the calvaria and the cranial base; and (3 ) the
Figure 95a. This section was prepared through the base of the pterygoid (A) as it passes into the lateral plate (B). Surface A is depository (note attachment fibers), and the external face of the lateral plate (B) is resorptive. The bone deep to this surface was formed by endosteal deposition and is of a convoluted (compacted cancellous) type. X 75.
Figure 95b. This section of the sphenoid bone was taken from the middle temporal fossa. The periosteal surface formed a portion of the endocranial lining, and it is characteristically resorptive. The inner side adjacent to the medullary cavity is depository, and the cortex is entirely of endosteal origin. The bone tissue is of a convoluted, compacted cancellous type. X 75.
Figure 95

( 2 1 2 )
critical maintenance of positional relationships among the brain, cranial nerves, and vessels. This key relationship would become progressively disproportionate if sutural growth represented the dominant growth mechanism in the cranial floor.
In Figure 98, it is apparent that the sphenoidal complex becomes displaced in an inferior manner in association with sutural bone growth in the lateral walls of the calvaria. An elongation of the clivus, as already seen, is brought about by endochondral proliferation
Craniofacial bone growth
at the spheno-occipital synchondrosis. The greater part of this lengthening process occurs on the occipital side, and the junction remains active in bone formation into the adolescent period, although a range in closure time has been variously reported (Brodie, 1955; Powell and Brodie, 1963; Ford, 1958). Elongation in the different parts of the sphenoid at the anterior contacts with the frontal and ethmoid is considered to be of lesser significance and terminates at a much earlier age.
As the entire sphenoid becomes displaced
The endocranial periosteal surface of the frontal bone below the level of the circumcranial reversal line is resorptive (side A). The cortical bone is endosteal in origin and was laid down on surface B. The ectocranial side (C) is depository, and its contralateral, endosteal surface adjacent to
the diploe is resorptive. The external lamina is thin in this portion of the section, which was taken from a lateral area where the frontal bone grades into the floor of the anterior cranial fossa. X75 .
Figure 96

Calvaria and cranial base
downward, and as the clivus elongates at the synchondrosis (with some addition at the external lip of the foramen magnum), a key remodeling adjustment simultaneously occurs that functions to continuously reposition the moving sphenoid in relation to the remainder of the anterior cranial floor. The downward drift of the foramen magnum and the lowering of the frontal floor produce a progressively changing angulation between them. Because the anterior-posterior position of the foramen is relatively stable, its forward rim forms a pivot from which the cranial base moves forward and downward during continued growth in order to align with the floor of the anterior cranial fossa. The resorptive, endosteal growing endocranial surface of the spheno-occipital complex is characterized by an angular gradient of drift in this direction (Fig. 97). By this drift process, involving endosteal and periosteal growth on the inside and outside respectively, the cranial base undergoes a "rotation" from its axis at the anterior margin of the foramen magnum downward with the inferior moving cranial floor underlying the prefrontal cerebral lobes. This remodeling pattern contributes to the flexure of the cranial base.
As the midline bodies of the sphenoid and occipital undergo this growth movement, the laterally placed, horizontally oriented floors of the middle cranial fossae experience a corresponding downward drift, involving endocranial surface resorption, and they thereby expand in proportion to the enlarging temporal lobes occupying these depressions. The fossae are bounded by wings of the sphenoid and a portion of the temporal bone. They form a restricted compartment that increases in volume by a combination of drift and sutural growth. As in other cul-de-sac fossae in the cranial floor, contour expansion requires a drift process in addition to sutural bone deposition in order to enlarge the internal dimensions of
( 2 1 3 )
the pocket. Differential rates of growth, as previously noted, are also involved in this composite type of growth pattern, because the rate and extent of outward growth decrease as the midline is approached. Furthermore, cranial nerves and vessels are maintained in constant relative positions by this process.
In Figure 97, note that the downward movement of the occipital bone in the regions just lateral to the foramen magnum (exoccipital area) is accomplished primarily by direct cortical drift in an ectocranial direction, together with a lesser contribution by the temporoparietal suture. As this area grades into the lateral and posterior cranial walls, the outward mode of growth is produced by a changing combination of drift and sutural expansion. As one decreases, the other increases until sutural growth comes to represent the dominant type of increase. In the midline spheno-occipital region, by comparison, downward growth is a composite movement produced by elongation at the synchondrosis, displacement associated with sutural expansion in the lateral wall of the skull, and direct cortical drift. The sum of these various growth processes at the anterior rim of the foramen magnum balances the sum of the different processes that characterize the posterior side.
The floor of the sella shows a wider range of variation than other parts of the sphenoid. Its surface is typically resorptive in nature, a factor associated with the forward manner of relocation. Even though the cortical floor of the sella is composed of downward-growing, endosteal bone, the position relative to the remainder of the cranial floor can actually rise somewhat as a result of the differentially more extensive downward displacement and growth of the anterior and middle cranial fossae. However, various combinations of surface resorption and deposition may also be found in the cortex lining the bottom as well as anterior and


Calvaria and cranial base
posterior walls of the sella. Similarly, a wide range of corresponding variations is observed in gross morphology, including its overall configuration and dimensions. The most common variation is the presence of a floor that is entirely depository, which serves to produce an actual, rather than a relative, rise of the sella, a factor which may function in sustaining a constant relationship of the fossa to the hypophysis as the rest of the resorptive cranial floor descends during growth. It is apparent that the sella is not an actual "fixed" anatomic landmark, and that it undergoes processes of growth movement during the enlargement of the cranial base (see also Figure 109).
With increasing age, a variable extent of the cancellous region within the sphenoidal body becomes progressively replaced by an enlarging sinus. The endosteal bone surfaces enclosing this space are typically resorptive, thereby serving to hollow the area. The inner surfaces of the sphenoidal conchae are similarly resorptive, and their periosteal sides are depository. The sphenoidal surfaces in contact with the cavity of each concha are also resorptive in nature. The bulbous roof of that portion of the sinus just anterior to the sella (the tuberculum sellae) has a meningeal surface that is most commonly resorptive. The resorptive nature of the sinus deep to it, as in other
( 2 1 5 )
sinuses growing adjacent to an endosteal cortex, is such that sinus expansion ceases at a point where definitive cortical thickness is attained. A variation is seen, however, in which the meningeal surface of the tuberculum sellae, which lies beneath the optic chiasma, undergoes a reversal to become depository in nature. This results in an increasing volume of the area beneath it which in turn undergoes replacement by continued sinus expansion.
The wings of the sphenoid bone form most of the posterolateral wall of the bony orbit as well as the posterior portion of its roof. These plates of bone, and also the frontal bone in the anterior fossa, form the bony orbital lining on their external sides and the endocranial lining on the internal sides. The orbital surface of each cortical plate is characteristically depository in nature. The contralateral meningeal side is resorptive. This combination produces progressive cortical drift in an ectocranial direction. Note that the growth movement of the orbital wall proceeds in direct conjunction with the generalized process of resorptive endocranial growth in the cranial floor.
The process of periosteal bone deposition on most of the lining surfaces in the orbital cavity, together with resorption from most of the "outer" surfaces of the socket (the endocranial floor, the maxillary sinus, and the nasal cham-
An internal sagittal view of the skull (a) shows the cranial base and key sutures. The component bones have been separated in b. Sutural bone additions and bone deposits at the spheno-occipital synchondrosis are shown. The adjusted bones were then reassembled (c). The gradient of sutural deposits (1, light stippled area) and direct cortical drift in an outward direction (2, dark shaded area) are represented together as a coordinated growth composite. The clivus has become elon
gated by endochondral growth at the synchondrosis (3). The region surrounding the foramen magnum has moved inferiorly by direct cortical drift (0), and the cranial base has rotated anteriorly and inferiorly (0) by a similar process of cortical drift. Endocranial lining bone surfaces indicated by 2 and by 0 are all resorptive in nature. Note that cortical thickness in the cranial roof has also increased proportionately.
Figure 97

( 2 1 6 ) Craniofacial bone growth
The sum total of the growth changes in the cranial floor and roof ( a ) produces a generalized enlargement of these portions of the skull, as seen in b. Although the overlay in the lower diagram illustrates the overall, proportionate result of growth (as in Figure 45, showing mandibular
enlargement), it is emphasized that diagram b does not represent the actual picture of direct growth movements and increases in each part of the skull. It shows instead the end result of all the regional growth changes schematized in diagram a.

Calvaria and cranial base
ber), brings about an actual increase in orbital size during growth. This process follows the V principle. The orbital cavity has a conical, funnel-shaped configuration. Just as the metaphyseal funnel of a long bone and the conical neck of the mandibular condyle undergo enlargement by external resorption together with internal deposition, the V-shaped orbit similarly grows toward its own wide end. The growth course is anterior and lateral, and the surfaces facing this direction are represented by most of the various intraorbital surfaces of the cavity. On the posterolateral wall, the surface facing away from the direction of growth is the contralateral endocranial side, which is resorptive. Periosteal growth additions on the various cortical surfaces of the orbital lining, including its sphenoidal component, serve to move the orbit forward in conjunction with the forward movement of the brain behind it and to enlarge the internal dimensions of the entire orbital cavity by the forward expansion of its V.
A characteristic reversal occurs on the external side of the sphenoid near the lower margin of the posterolateral orbital wall adjacent to the inferior orbital fissure. The ectocranial surface in this region is resorptive in conjunction with an endosteal mode of bone formation. The entire remainder of the sphenoidal surface within the large pterygopalatine (sphenomaxillary) fossa is resorptive. This provides a lateral cortical movement in order to make way for the adjacent, laterally moving orbital floor and maxillary tuberosity. A similar situation exists in the zygomatic portion of the lateral wall. The total picture involved in orbital growth and remodeling, including the activities of its many other components, is evaluated in Chapter 10.
THE PTERYGOID PROCESSES. The medial
and lateral pterygoid processes form a downward-facing V-shaped trough. The entire basal
( 2 1 7 )
portion of the pterygoid near its junction with the sphenoid is depository on both the anterior and posterior sides. This produces a generalized forward, outward, and downward enlargement of the base. The major portion of the projecting processes, however, typically has resorptive periosteal surfaces on the medial and lateral external sides of the trough (Fig. 95a). The inner sides are correspondingly depository. This combination follows the V principle. The predominant course of growth is inferior, and the surface facing this direction is the inner side of the pterygoid fossa. The outer side, which is predominantly resorptive and is composed of endosteal bone tissue, faces away from this direction. The result is a progressive, downward growth movement together with a corresponding increase in the overall size of the fossa. The periosteal surface of the contiguous hamulus is entirely depository in character.
The resorptive endosteal mode of growth on the outer sides of the pterygoid plates serves another adaptive function. The pterygoid bone directly abuts the posterior face of the maxillary tuberosity. This surface represents a major growth site in the maxilla, and continued elongation of the maxillary arch occurs here. The actual position of this posterior surface relative to the cranial base, however, is comparatively constant because of the forward manner of maxillary displacement away from the cranial base. As the forward and downward growth of the pterygoid processes bring them into contact with the maxillary tuberosity, the forward direction of movement becomes reversed. This produces the reversal line on the outer sides of the processes, and subsequent growth then proceeds essentially in a downward course. The extremities of each process thus become resorptive on their superior-facing, anterior periosteal surfaces in order to produce this inferior direction of enlargement.

( 2 1 8 )
Both the medial and lateral ptergyoid processes are subject to a range of localized variations in resorption-deposition combinations on their different surfaces. This results in a corresponding range of structural variations in the disposition and slope of these processes. Perhaps the most common variation is the occurrence of a resorptive surface on the inside of the trough on some parts of either the medial or lateral process. This serves to produce a regional widening and expansion of the pterygoid fossa.
THE ETHMOID. This composite bone, composed of the horizontal cribriform plate with its crista, ethmoidal labyrinth, lamina papy-racea, and perpendicular plate, conforms generally to the remodeling and growth patterns found in the contiguous anterior cranial floor and the nasal chambers.
The endocranial surface of the cribriform plate is most commonly resorptive in nature. The opposite, nasal side is depository. In conjunction with the downward drift of the anterior cranial base, floor of the frontal fossa, and the nasal cavities, this diminutive plate (in the human skull) moves essentially in a directly inferior course. Its horizontal, downward-facing orientation is in contrast to a much more vertical, forward-facing placement in snouted animals (see Chapter 8) . Although typically resorptive, the endocranial side may show a less common depository meningeal surface. This apparently represents a secondary adjustment to a differentially lesser downward movement, relative to the descending frontal floor on either side, in order to maintain its level with respect to the olfactory lobes.
The projecting crista galli represents a partition separating the paired olfactory fossae. Its growth pattern, similar to other partitions in the cranial floor, usually involves progressive deposition of periosteal bone (Fig. 88). This
Craniofacial bone growth
produces an endocranial-projecting elevation that increases in size as the laterally placed olfactory fossae correspondingly enlarge. It follows the same growth pattern found in the continuing midline ridge of the frontal bone just anterior to the crista. The shape of the crista is often asymmetrical, and it may be skewered to one side or the other. This is associated with a range of variation in the growth pattern of its cortices. A variable extent of endosteal bone, with corresponding surface resorption, may be found at the base of the crista on either side.
The median perpendicular plate, extending inferiorly to join the vomer and the septal cartilage, is a thin lamina composed of a single sheet of cortical bone lacking diploe. It is sparsely vascularized. This plate shows a characteristic pattern of deposition on one side with resorption on the other. It is variable, however, in that either side may show a regional reversal in surface growth activity, and such a change in any area is usually accompanied by a corresponding reversal on the opposite side. These remodeling factors provide a formative basis for the variations seen in right or left deviations of the nasal septum as a whole, particularly in this cephaloposterior region.
The ethmoidal labyrinth has a basic growth pattern involving bone deposition on its numerous lateral and inferior surfaces with corresponding resorption from contralateral superior and medial surfaces. This enlarges the conchae and ethmoidal cells in an inferior, anterior, and lateral manner in conjunction with a similar mode of nasal expansion in general. The lateral side of the ethmoidal labyrinth (lamina papyracea) is characteristically depository in character. If a neonatal or very young postnatal skull is compared with a more mature specimen, this region is seen to undergo a marked lateral movement as a consequence of ethmoidal enlargement (Fig. 70).

Calvaria and cranial hase
The result is a significant expansion of the posterior nasal chamber and a noticeable superolateral shift of the medial orbital wall (see also pages 165-167).
THE VOMER. Like some other bones comprising the visceral portion of the cranium, such as the adjacent maxilla, the vomer shows a growth pattern involving an upward and backward direction of actual growth (Fig. 99). Displacement takes place in an opposite, forward, and downward direction. The enlarging vomer trails the expanding, forward-moving septal cartilage and, together with the perpendicular plate of the ethmoid (following its ossification as a separate mesethmoid center), provides a buttress contact for this thin cartilaginous plate. Although ossification of the vomer occurs in close association with the cartilaginous septum of the nasal capsule, the formation of this element is intramembranous in nature.
The broad trough of the vomer in contact with the sphenoid is characterized by a depository surface. Bone additions thus proceed superiorly and posteriorly in a direction toward the cranial base. As the entire vomer becomes translocated (displaced) in an anterior and inferior direction behind corresponding movements of the bony palate, it undergoes con-
( 2 1 9 )
tinued elongation toward its contact with the sphenoid, thereby maintaining a constant intermediary position between the palate and the cranial base. Bones at sutural contacts do not "push" themselves apart by continued bone growth but instead become separated by the expansion of an associated soft tissue with bone deposits added secondarily onto apposed surfaces in a field of tension rather than pressure. The vomer becomes drawn forward by the generalized process of anterior displacement, presumably under the influence of the expanding septal cartilage itself (Scott, 1953a). As it becomes moved, the bone simultaneously undergoes growth at its superior and posterior extremities in a manner similar to that in maxillary sutures.
In Figure 99, it is seen that the sphenoidal side of the broad vomerine trough, composed of two alar plates, is depository. The contralateral nasal surface is characteristically resorp-tive. This growth pattern follows the common V principle. The V-shaped trough grows and moves toward its own wide end and simultaneously enlarges in size by the process of cortical drift. The sphenoidal surface faces the direction of growth, and the resorptive naso-mucosal side is oriented away from this direction.
As the flared superior portion of the vomer
The vomer. Resorptive surfaces on the right (a) and left (b) sides are indicated by dark stippled area. Depository surfaces are indicated by
light stippled area. See text for a more detailed account of growth changes in this bone.

( 2 2 0 )
grades into the very thin plate that occupies a portion of the bony nasal septum, a distinct periosteal reversal occurs on one side of the bone, either right or left. This functions to reduce the broad, superior portion to the width of the thin inferior part, since a continuous process of sequential relocation of one into the other is involved as the whole bone increases in length. The perpendicular midline plate is composed of a single lamina of cortical bone that is periosteal in type. It continues downward for the remainder of the bone. The entire opposite side is resorptive. The perpendicular plate of the vomer thus shifts in a single lateral direction as the entire bone enlarges in an anteroposterior dimension. It does not increase in width on both sides of the thin cortex. The result is a slight deviation to either side corresponding to the declination of the thin ethmoidal plate above it.
THE FRONTAL BONE. With the fusion of the metopic suture, the paired frontal elements are joined into a single bone. The growth of this bone embodies a number of critical mor-phogenetic relationships. The frontal bone forms a significant portion of the skull roof as well as the cranial floor (the large anterior fossa). Because of this, differential rates of growth are involved between its superior and midventral parts, although not to the extent found in the sphenooccipital region. The enlargement of the frontal bone includes variable combinations of sutural growth and growth by cortical drift due to the differing circumstances between its calvarial and cranial floor portions. This bone constitutes the orbital roof, and it forms the forehead. A major paranasal sinus develops later in childhood.
The enlargement of the frontal bone involves contrasting modes of growth in its superior and inferior parts (Fig. 88). The entire cutaneous side is depository. In the skull roof,
Craniofacial bone growth
the endocranial surface is also depository, and growth proceeds by sutural bone additions in combination with proportionate increases in cortical thickness on both the ectocranial and endocranial sides. The prominent reversal line that encircles the entire inner aspect of the cranium bisects the endocranial surface of the forehead. Below this line, the entire remainder of the meningeal surface of the bone is characteristically resorptive. Its cortical bone is endosteal in composition (Fig. 96) and is largely of a convoluted type produced by cancellous compaction. In thinner areas, such as the orbital plate, it may be made of periosteal bone laid down on the orbital side but translocated to the resorptive cerebral surface as a consequence of outward cortical drift.
The formation of the bulbous forehead in the human skull results in a distinctive, forward-protruding anterior cranial fossa that overlies the orbital cavities. The floor of this fossa lies in a nearly horizontal position. These factors are related to the flexure of the cranial base and the disposition of the entire facial skeleton in a vertical, downward manner (see pages 186, 195).
The placement of the various sutures associated with the frontal bone is such that enlargement of the forehead region and the floor of the anterior cranial fossa involves a separate mechanism of outward cortical drift in addition to sutural expansion (Fig. 92). In order to bring about an enlargement of this frontal compartment, the cortical plates forming the orbital roof, forehead, and lateral walls of the anterior fossa up to the level of the circum-cranial reversal line must undergo a process of direct ectocranial surface deposition together with endocranial resorption. This increases the internal dimensions of the fossa and expands the overall surface contours of the area as a whole. The sagittal ridge is characterized by a periosteal reversal that produces a midline ele-

Calvaria and cranial base
vation on the cerebral side of the frontal bone in its anterior portion.
The fact that the floor of the anterior fossa is resorptive functions also to move the paired orbital cavities in a progressively anterior and inferior direction. The overhanging orbital ridges form the superior rim of the orbit. In Figure 89, note that the internal periosteal surface of the lateral half of the superior rim is resorptive. This lining orbital surface faces away from the anterior and lateral direction of orbital growth movement. As a consequence, it is resorptive in conjunction with the depository, external surface along the supraorbital margin. As new bone is added onto the supraorbital surface, it is removed from the opposite side (inner surface of the orbit). Thus, the lateral half of the orbital roof just beneath the overhanging orbital ridges progressively undercuts these ridges as they continue to enlarge anteriorly and laterally (see page 247 for a further evaluation of orbital remodeling).
In younger skulls, the frontal bone in the region of the glabella is characterized by a cortex composed of a flat lamina externa with underlying diploe. With increasing age, the cancellous trabeculae undergo resorption and the external lamina experiences a marked forward drift (outer deposition together with endosteal resorption). This produces the glabellar protrusion with an extensive frontal sinus within it. The region is particularly prominent in the Caucasian male.
THE TEMPORAL BONE. As in many other cranial bones, the temporal represents a composite produced by fusion of several separate elements. In Figures 87, 88, and 89, note that the entire external (cutaneous) side of the squamous portion is depository. The opposite endocranial surface lies below the circum-cranial line of reversal and is resorptive. The outward mode of growth in the squamous por-
( 2 2 1 )
tion of the temporal thus proceeds by cortical drift in combination with sutural growth at the temporal, parietal, and sphenoidal junctions. This pattern conforms to the general plan of growth in the ventral part of the cranium as a whole. It is concerned with differential rates of growth as the calvaria grades into the cranial floor and with contour expansion in the compartments (fossae) of the ventral cranium, as schematized in Figures 92 and 94. The process of ectocranial cortical drift serves to enlarge the middle fossa in relation to the more stable cranial base adjacent to it. This process could not be carried out by the temporal sutures alone because of the abrupt curvatures involved and the nature of sutural placement. The growth combination involves an inverse gradient between sutural growth and outward cortical drift from the calvaria to the cranial base.
The anteroposterior dimensions of the squamous portion of the temporal bone become enlarged primarily at the temporo-sphenoidal suture. This lengthening is such that the distance from the external auditory meatus to the anterior temporal margin increases to a much greater extent during postnatal growth than the distance from the meatus to the temporoparieto-occipital junction.
The zygomatic process of the temporal bone becomes correspondingly elongated as the squamous area enlarges. This occurs primarily at the zygomaticotemporal suture. The entire zygomatic arch becomes greatly lengthened during postnatal growth. It also undergoes a marked increase in depth by continued bone additions on its inferior margin. These increases occur largely on the separate zygomatic bone but also on the zygomatic process of the temporal. A lesser extent of periosteal deposition occurs along the superior border. The upper margin of the arch does not actually rise, however, because the entire zygomatic

( 2 2 2 )
complex becomes displaced in an inferior manner during sutural growth. The lateral surface of this forward-projecting process is entirely depository. The medial side within the temporal fossa, however, has a characteristic re-sorptive surface. This combination produces a continued lateral drift of the whole arch as it simultaneously grows downward by bone deposition along its inferior border. As the zygomatic process grades into the squamous part of the temporal bone, the resorptive surface undergoes a periosteal reversal, and surface deposition then characterizes the entire external side of the squamous area.
The ectocranial surfaces of the petrous, mastoid, and styloid portions of the temporal bone are largely depository in character, in keeping with the generalized growth pattern found on outer surfaces of the cranium. Differentially more rapid growth in the mastoid area produces a characteristic enlargement of this region in the human skull (see page 169). The anterior part of the pyramidal petrous part of the temporal often shows an ectocranial reversal involving a relatively small resorptive surface (Fig. 89). This serves to align the contour of its forward-growing conical tip with the adjacent posterior edge of the sphenoid at the base of the pterygoid processes. The jugular fossa also is usually resorptive and has a growth pattern that provides a progressive hollowing of this area as the ectocranial walls around it grow outward by continued periosteal additions (Fig. 89). The posterior wall of the auditory canal is characteristically depository, and the anterior wall is resorptive in nature. This combination produces a forward and downward drift of the entire canal.
On the endocranial side, the petrous part of the temporal shows a characteristic periosteal reversal. This meningeal surface receives bone additions, and it represents one of several such isolated depository regions within the predominantly resorptive cranial floor (Fig. 87). It
Craniofacial bone growth
covers most of the elevated portion of the petrous pyramid and continues posteriorly across the approximate superior half of the large sigmoid groove. At this point an endosteal reversal occurs, and the entire remainder of the posterior portion of the temporal (in its mastoid region) on the cerebral side is resorptive. This resorptive surface continues across the suture and extends onto the occipital surface. On the anterior side of the petrous part of the temporal bone, the resorptive surface terminates at a reversal line that occurs along the base of the pyramid where it grades into the floor of the middle cranial fossa. A zone of variation is found, however, in the region between the trigeminal impression and the thin tegmen tympani. This restricted surface area is often resorptive and is apparently concerned with positional adjustments of the bony cortex to the trigeminal ganglion on one side and the tympanic cavity on the other.
The distinctive nature of a depository type of periosteal (meningeal) bone growth on the petrous pyramid, in contrast to the much more widespread resorptive mode of cortical growth in most other regions of the cranial floor, provides the formative basis for the large bony housing of the middle ear apparatus and the membranous labyrinth of the inner ear. The elevation produced by this bony projection also forms the partition that separates the middle from the posterior cranial fossa. As seen in the schematic interpretation in Figure 94, the fossae expand largely by outward cortical drift. The elevated partitions (here the petrous pyramid) between these cranial compartments maintain proportionate size and position by a converse process of periosteal bone addition as the fossae enlarge through surface resorption. The thick, dense cortical bone deep to the depository surface of the petrous elevation is formed largely by a process of endosteal cancellous compaction beneath the outer layer of periosteal bone.

Calvaria and cranial base
As in the other components of the cranial floor, the growth pattern of the temporal bone, embodying combinations of sutural growth and particularly cortical drift, is an adaptation to differential growth, fossa expansion, and the critical maintenance of cranial nerve and vessel relationships.
THE AUDITORY OSSICLES. All three pairs of ossicles are fully formed in cartilage at about eight-and-one-half weeks of fetal age. No bone tissue is yet present, but the intra-membranous bone of the adjacent mandible has already begun to form. It develops around Meckel's cartilage, which still shows connection with the malleus at this stage. The otic capsule as yet is entirely cartilaginous, and the external acoustic meatus and auditory tube have approached the developing ossicles from contiguous auricular and pharyngeal areas. Ossification first occurs in the incus (16-week fetus) and soon follows in the malleus and otic capsule. Bone formation then begins in the stapes less than two weeks later.
The prenatal as well as postnatal growth and development of all three ossicles differ from other bones in one major respect: their linear dimensions are, for the most part, already established by the cartilaginous anlage that precede them. Very little elongation takes place during subsequent bone development. Thus, the many critical remodeling adjustments associated with the processes of elongation in a bone do not occur. Because these small bones do not lengthen appreciably, the factor of sequential relocation is thereby not involved. As a consequence, changes concerned with progressive reshaping and resizing are lacking. Because the bones do not appreciably move in position as a result of their own growth activity (although they become displaced because of movements of the temporal bone and other parts of the cranial base), processes of repositioning in response to their own
( 223 )
individual growth patterns are not involved. Because of these factors, the course of growth in the auditory ossicles is relatively direct and lacks the complexity of growth movements that characterize most other bones.
The resume of the prenatal growth processes in the three auditory ossicles presented below is based in part on the works of Anson and Bast, and Hanson and Anson (see Bibliography).
THE MALLEUS. This element is identifiable as a mesenchymal mass in the 10-mm embryo and has progressed to the cartilaginous stage in the 28-mm embryo. Adjacent to the cartilage, a projecting trabecula (the anterior process of the malleus) develops in the connective tissue membrane. This represents the only portion of the entire element not directly associated with cartilage.
As Meckel's cartilage begins to undergo degenerative changes anticipating conversion into ligamentous tissue, a single ossification center appears on the face of the manubrium at about fifteen weeks of age. The bone is "perichondral" in type and develops in the connective tissue membrane enclosing the cartilage. This bony center then begins to spread over the remainder of the malleus until the entire element becomes covered by a thin crust of perichondral cortex except at surfaces of articulation and points of ligament attachment. At this stage, the malleus is represented by a core of cartilage enclosed by a thin shell of bone. The cartilage cells undergo hypertrophy and the matrix calcifies.
Within the calcified cartilage core, invasion by vascular buds takes place, and endochondral bone replacement then occurs. One or more medullary spaces become formed by internal resorption. Endosteal lamellae are then laid down in these spaces on the inner margin of the perichondral bone cortex. In medullary areas not occupied by the spaces, compaction


Calvaria and cranial base
of the endochondral cancellous bone occurs. Within the medulla, combinations of convoluted bone, endochondral bone, and small islands of calcified cartilage matrix are thus found. At the tip of the manubrium, perichondral bone does not develop, but the cartilage undergoes partial endochondral bone replacement. A core of endochondral bone is formed which retains a covering of the original cartilage.
After birth, trabecular reconstruction takes place in the medulla and may continue until old age. Variable degrees of cancellous compaction occur within the secondary trabecular bone (Figs. 100a and b). Extensive Haversian replacement as such, however, does not take place. In contrast to the stapes, the malleus has a medullary area that is occupied by bone rather than by replacement, pharyngeal mucosal tissue (see below).
( 2 2 5 )
THE INCUS. Ossification begins in the four-month fetus in a primary center located on the long crus. A thin shell of perichondral (intramembranous) bone first appears, and chondrocyte hypertrophy and matrix calcification soon follow. As in the malleus, the developmental process involves ( 1 ) the formation of a cartilage prototype that approximates adult linear dimensions, (2 ) the formation of a perichondral bone cortex around this cartilage model, and (3) subsequent endochondral bone replacement within the cartilage core. Continued longitudinal growth and associated remodeling changes do not occur. As in the malleus, trabecular reconstruction takes place within medullary regions, and variable patterns of convoluted bone enclosing endochondral spicules result (Fig. 100a1). The latter changes, which may occur to some extent throughout life, are properly termed reconstruction rather than remodeling, because they are not involved
Figure 100a. Malleus, newborn. This section, from near the head, shows a thin periphery of cartilage enclosing the core of trabecular bone. The latter has completely replaced the endochondral bone which originally occupied the medulla. X 60.
Figure 100b. Malleus, newborn. Near the manubrium, a very thin crust of the original cartilage remains. The core of endochondral bone has been largely replaced by several irregular, Haversian-like structures that have been deposited within the medullary resorption spaces. Extensive Haversian reconstruction, however, does not occur. X60.
Figure 100c. Stapes, newborn. The obturator foramen in this section is bounded by two crura and the somewhat thicker base (at top). Each crus is composed of perichondral (intramembranous) bone. Although only a portion of the cortex is seen in section, the crura are hollowed along
their medial obturator face, and the cartilaginous core has become completely removed and replaced by mucosal tissue. Note that the external surface of the base retains a thin cartilaginous cover. The perichondral cortex adjacent to the obturator foramen has already been resorbed, and the original endochondral bone in this particular section has been replaced by irregular trabecular bone. X50.
Figure 100d. Incus, three-month infant. The bone is enclosed by a thin peripheral layer of perichondral (intramembranous) bone tissue. The original endochondral bone of the core has been largely replaced by irregular trabecular bone that has undergone compaction. A few Haversian-like structures were produced by deposition of lamellar bone within medullary spaces. Scattered calcified cartilage matrix spicules remain in the medulla. X60.
Figure 100

( 2 2 6 )
in major adjustments of the bone's shape and size in association with growth increases. As in the malleus, extensive Haversian reconstruction does not occur, although a few osteons are formed during medullary compaction.
THE STAPES. The growth sequence in this bone, in keeping with its ontogenetic and phylogenetic origins, differs somewhat in nature from that in the malleus and incus. At about fifteen weeks of fetal age, the unaltered cartilage tissue presents a configuration that is similar to that of the adult bone. A broad, platelike base is present with two projecting crura that enclose a central obturator foramen. The crura converge to form the head, which is in contact with the formative incus. At twenty weeks, changes within the cartilage anticipate the subsequent steps involved in bone formation. On the surface of the basal plate between the two crura, a primary center of ossification appears. Perichondral bone is formed within the connective tissue membrane and then spreads progressively over the surface to the crura and onto the base to form an enclosing cortical shell of intramembranous bone. Within the core of the base, the cartilage undergoes hypertrophy and calcification. It is invaded by vascular buds, and endochondral bone replacement soon follows. A similar center of endochondral bone formation occurs on the opposite side of the obturator foramen deep to the head. Adjacent to both endochondral centers, cartilage is retained on the contact surfaces of the head and the inferior side of the base.
Within the obturator foramen, the loose mesenchymal tissue that originally filled this space undergoes removal. An extensive process of surface bone resorption now takes place on the four sides that directly bound the foramen. The thin cortical crust of perichondral bone that covers the base, within the foramen, undergoes removal so that the underlying core of
Craniofacial bone growth
endochondral bone becomes exposed to the surface. This bone undergoes compaction to form an irregular, convoluted type of endosteal bone tissue containing scattered endochondral spicules. The basal plate becomes thinned as a consequence of this surface resorption. Similarly, the covering perichondral bone on the opposite pole of the obturator foramen (deep to the head) also undergoes surface resorption with the resulting uncovering and exposure of its endochondral core.
Resorption of the perichondral bone lining the obturator foramen is completed as the cortices of the two crura experience surface bone removal on the sides lining the foramen. Resorption progresses through the thin cortex and invades the cartilage core. Endochondral bone replacement in the two crura, unlike the head and base sides of the foramen, is negligible. Resorption now entirely removes the original unaltered cartilage medulla. The result is the formation of paired crura, which become hollowed on their obturator (medial) sides to form trough-shaped processes connecting the base with the head. The hollowed basin in each crus becomes lined by a mucosa of pharyngeal origin. At the points where the crura join the base, a thickening of exposed endochondral bone is retained. The crura themselves are composed only of a thin U-shaped cortex, composed of perichondral bone tissue. Original cartilage is retained on the articulating surfaces of the base and head. As in the other ossicles, however, the cartilaginous plates do not provide an epiphyseal growth mechanism, and linear increase does not occur. Corresponding remodeling changes associated with progressive elongation thus are not involved. Haversian replacement is negligible in the stapes. Unlike the malleus and incus, postnatal internal reconstruction involving trabecular changes is all but lacking. The histologic structure of the bone is essentially constant throughout postnatal age levels (Fig. 100c).

(10)
The composite nature
of facial growth
The neonatal human skull is characterized hy a large precocious cranium and a diminutive face. The slowing postnatal enlargement of the cranial base and calvaria, however, becomes bypassed by the differentially more rapid enlargement of the facial complex. The entire face undergoes progressive changes in which its configuration, proportions, and dimensions become markedly altered. As seen in previous chapters, the continued growth of the facial skeleton does not simply involve generalized sur-face bone deposition on all outer surfaces to produce an even symmetrical expansion. Instead all parts in each individual bone undergo an extensive, complex series of successive remodeling changes. It is incorrect to assume that facial enlargement is a result of activity only at sutures and other selected growth sites, such as the maxillary tuberosity and the alveolar margin. Remodeling growth represents
a basic and equally significant process that is also directly involved in facial enlargement and maturation. This process is concerned with the continuous maintenance of shape, proportions, and relationships in each part of an individual bone as the whole bone continues to enlarge in size. Remodeling serves to sequentially reposition all component areas in a growing bone. New bone additions in all the various regions of the bone result in successive relocation of its parts, and remodeling adjustments change the shape in each area as relative position becomes moved. Furthermore, remodeling growth functions to proportionately enlarge the size of each regional part relative to the increasing size of the bone as a whole. Remodeling serves as a companion process to sutural growth, condylar growth, growth at synchondroses, etc., and all proceed in direct coordination with each other.
227

( 2 2 8 )
Growth and displacement
In the growth of the human hand it is apparent that the fingers do not lengthen solely by adding new bone at the tip of each terminal phalanx. Elongation is a combined result of growth in all of the proximal, middle, and distal phalanges in addition to thrust produced by growth in the carpals and metacarpals. Total enlargement is a composite of growth in each bone in relation to the rest. As a result of their combined growth increases, a chain of displacement occurs in which the extent of movement of the distal phalanx represents the sum of growth movements in all the bones. Similarly, the enlargement of the facial complex is the cumulative sum of individual growth increases in all the separate bones of the face as well as those in the cranial base and calvaria.
A basic problem exists in interpretations of skeletal growth data. The dilemma presents itself when separate but contiguous bones are studied in relation to one another as a composite whole. The middle face is sometimes viewed as a single growing unit rather than as a mosaic of individual components. Cumulative interactions between its separately growing parts are difficult to evaluate because (1) the contact margins of many different bones cannot easily be distinguished in cephalograms, and (2 ) the actual extent of growth increases in each part of each bone is often difficult to determine in many elements of the human skull, as seen in serial cephalograms. As a result, misleading and sometimes unreal growth patterns can be inferred that give an oversimplified or inaccurate picture of actual growth processes.
It has been seen that bone can move from one position to another by two basic means: it may drift by actual direct cortical growth involving resorption and deposition on selected
Craniofacial bone growth
surfaces facing away and toward directions of local growth, or bone may move as a consequence of displacement. In the latter process, movement is produced by the bone's own growth (e.g., at the epiphyseal plate or a condyle), the growth of other contiguous bones, or it can be carried by expanding soft tissues, such as the brain or the cartilaginous nasal septum. Actual growth (cortical drift) and the additional factor of displacement (a consequence of growth) often follow divergent courses, which serves to complicate the evaluation of the overall growth process and is the basis for many of the interpretive difficulties encountered in cephalometric analyses.
In Figure 101, various possible combinations of growth and displacement are schematized. All are found in some part of the growing skeleton. Arbitrary landmarks have been inserted at various points to demonstrate that similar end results in total growth can be produced by several basically different combinations of growth activity. Evaluation of the relative contributions of the different growth processes (resorption, deposition, displacement) must be approached with caution because of the complexity of combinations involved.
THE STANDARD CEPHALOMETRIC PICTURE.
Growth increments are routinely visualized by superimposing cephalograms (or tracings prepared from these cephalograms) at successive age levels. The entire face is often considered as a growing unit because segregation of components is difficult. Regional growth increases at sutures and on many surfaces cannot be accurately distinguished and quantitated in ordinary serial cephalograms. Tracings are registered in such a way that prominent radiographic landmarks, such as the sella turcica, directly coincide. This provides a basis for evaluating growth changes relative to the par-

Composite facial growth ( 2 2 9 )
Various combinations of direct growth and the process of displacement resulting from this growth are schematized. Position markers are included to localize the extent of movements. In 1, the distance between the markers is indicated by the arrows. In 2, addition at the free surface of B moves the relative position of the marker, as shown. In 3, the same end result is obtained but is brought about by addition at the contact surface between A and B. In this instance the position marker has been displaced, in contrast to 2 above. In 4, addition at the contact surface together with resorption from the free end of B also produces a similar end result. By adding a growth increment
on A in 5, a different end result now occurs. Note the positions of the old and new position markers. In 6, additions on one contact surface (A) with resorption from the other ( B ) occur, while at the same time additions on free surface B take place. The end result ( 7 ) is analogous to 2, 3, and 4 above. In 8, a two-stage growth sequence is shown in which bone is first added to A and later to B. These diagrams emphasize the complexity of different growth combinations involved in craniofacial enlargement. Caution should therefore be exercised in all morphologic interpretations of growth data.

( 2 3 0 )
ticular registration point selected. These landmarks are sometimes assumed to be relatively stable in position, although it is generally realized that no bony point is actually fixed within the growing skull, a factor to be demonstrated in subsequent sections.
The tracing overlay in Figure 102 illustrates the picture of facial growth seen using the "fixed point" registration method. The cumulative composite changes of the facial mosaic, as seen in this diagram, are relative to the sella. The apparent growth of the whole facial complex in relation to the cranial base is thereby demonstrated. The face is seen to enlarge in the familiar forward and downward direction. This method is valid for its purpose because it shows those topographic changes that one actually sees grossly as the facial features he-come altered with increasing age. It is to be realized, however, that this picture represents (1 ) the sum of actual growth changes in addition to ( 2 ) the movements produced by displacement, and that the relative contributions of each cannot be distinguished. The overlay picture should not be assumed to demonstrate direct movements produced by cortical drift involving selective resorption and deposition in the different parts of each facial bone. As described earlier, the analogy dealing with the growth of the hand is applicable. Just as a finger does not lengthen solely by growth at its tip, it is similarly incorrect to assume that the face actually grows in a forward and downward direction, as suggested in the overlay, by a process of continued bone addition on all anterior and inferior surface exposures. In reality, many of these forward-facing surfaces are resorptive and regressive in their actual growth patterns.
The various basic principles and concepts of bone growth and remodeling are not applicable to the registration procedure seen in Figure 102, because it embodies primarily the
Craniofacial hone growth
results of displacement rather than of direct growth. For example, it was shown in previous chapters that a bone does not enlarge by a simple process of generalized surface apposition in a manner that expands already existing curvatures. In the superimposed tracings, however, such a simplified process appears to be occurring, but it is not. The fundamental principle of differential resorptive and depository activity on selected surfaces facing away and toward directions of growth is not demonstrated by this superimposition method. It is apparent that actual growth directions often do not coincide with the manner of facial displacement. Similarly, the basic factor of successive relocation cannot be visualized, since the process of growth itself is obscured by displacement of the bones involved. Furthermore, the whole process of remodeling cannot be interpreted using this method because the nature of regional changes occurring in the different parts of each individual bone is not identifiable.
VISUALIZATION OF GROWTH PATTERNS
WITHOUT FIXED REFERENCE MARKS. In Order
to accurately determine and interpret the actual growth (not displacement) of a closely interrelated complex of bones, it is necessary to segregate and consider each bone as an individually growing unit. When growth processes in separate bones are first determined, they may then be reassembled to visualize the composite pattern of total growth (including displacement). "Fixed" landmarks cannot be utilized because they have no relevance within a single growing bone and do not in fact exist. However, serial tracings of individual bones may be superimposed in such a manner that registration points are not required. A growing bone represents a complex of many regional surfaces that follow a number of divergent growth directions involving differential pat-

Composite facial growth ( 2 3 1 )
The standard cephalometric picture. By registering "fixed" reference points (such as the sella turcica), the "forward and downward" growth of the facial complex is demonstrated here. However, many parts of the various facial bones do not themselves grow in such an anterior and inferior direction. Growth actually proceeds in a complex variety of divergent regional directions. The face as a whole, regardless of localized growth movements, becomes progressively displaced in a forward and downward manner, thereby obscur
ing actual growth patterns. This particular method of superimposing tracings (stippled area) is of value because it enables the worker to visualize gross topographic changes that take place in the appearance of the growing face. Because the effect of displacement produces those visible morphologic relationships that are actually seen during continued enlargement of the child's face, methods utilizing such selected reference landmarks in the cranial base provide meaningful information.
Figure 102

( 2 3 2 )
terns of surface resorption and deposition.
Th i s factor is utilized. Instead of presenting
an obstacle to interpretations, the changing,
remodeling nature of the whole bone is thereby
Craniofacial bone growth
used to advantage because it has no fixed
points.
T w o growth stages of the mandible are pic
tured in Figure 103. T h e y have been registered
The growth stages in this diagram have been superimposed (stippled, area) according to regional directions of growth (see text). Fixed landmarks were not used. As the mandibular condyle moves in a cephaloposterior course by a process of endochondral bone formation, the posterior border of the ramus simultaneously grows in a corresponding direction by subperiosteal additions of bone along its entire posterior margin. Because the condyle moves obliquely in a superior as well as posterior manner, the overall distance traveled by the condyle exceeds that of the backward-moving ramus. The coronoid process drifts in a similar posterior direction, although its backward movement is less than the posterior border of the ramus. The result is a proportionate enlargement of the ramus in anteroposterior dimensions. As the condyle moves superiorly, the ramus becomes significantly increased in vertical dimension, thereby accommodating the marked downward enlargement of the nasomaxillary complex. The inferior margin of the mandibular body just anterior to the gonial angle (the antegonial notch) is characterized by resorptive surface remodeling. This notch successively occupies regions previously held by the posteriorly moving, protruding gonial angle. The superior border of the body along the alveolar
ridge grows in an upward direction. However, the extent of this superior growth movement in the mandible is noticeably less than the opposing inferior direction of movement in the whole maxilla, because the latter represents a composite of alveolar and nasal growth. As the dental arches of both the maxilla and mandible grow toward each other, their relative positions are continuously maintained by proportionate vertical lengthening of the ramus. Except for the antegonial notch, bone is laid down along the entire inferior border of the mandibular body, and massive accumulations of compact periosteal bone deposits provide increasingly stable support for the dental arch. Although these deposits produce a thick cortical plate, the distance moved in an inferior direction is less than the extent of superior alveolar growth movement taking place on the opposite border of the mandibular body. The mental protuberance typically receives thick deposits of periosteal bone, although growth patterns in this general region are quite variable. Note that the alveolar area just above the chin, however, is regressive (involving surface resorption). This combination of remodeling movements produces the protruding chin, a distinctive human facial characteristic.

Composite facial growth
in such a manner that the regional distribution of resorptive and depository patterns is expressed. The periosteal surfaces of resorption in the region above the chin, the antegonial notch, and the coronoid process are aligned so that their cortices demonstrate an endosteal (regressive) mode of movement. Similarly, all the regional areas characterized by surface deposition, such as the chin, sigmoid notch, etc., are positioned to show their outward manner of cortical movement. Using this procedure, only a relatively slight degree of latitude is possible in the arrangement of the tracings. Thus, the method is not based on an arbitrary system of superimposition even though reference landmarks are not used.
This procedure demonstrates gross morpho-genetic patterns of enlargement. They must be interpreted with caution, however, because the movements visualized represent approximations. It is necessary to utilize average known patterns of surface resorption and deposition as determined from other bone specimens. The individual variations of these patterns cannot be expressed. These factors do not preclude, however, a general evaluation of the growth process in any single bone, and the method can suggest differences in developmental patterns when applied to individual serial tracings.
All the individual bones in the facial complex may be similarly studied using registration according to the distribution of remodeling surface types. The maxilla or the zygoma, for example, may be superimposed in this manner. Because the nasal floor, the premaxillary area, and the anterior surface of the malar region are all resorptive in nature, an overlay of the maxillary bone conforms to the picture seen in Figure 109, which has been superimposed according to another (sutural) system of registration. Known surfaces of periosteal deposition are similarly expressed using this procedure.
( 2 3 3 )
Such a system for approximating growth and remodeling changes can only be applied to single, separate bones. If two or more bones are considered in relation to each other, the actual growth pattern becomes obscured by the process of displacement, and the basis for registration utilizing differential remodeling movements is thereby invalid. However, if the actual growth pattern is first considered for each bone separately and then reassembled into a composite, it becomes possible to evaluate the combined patterns of mosaic growth. The resulting picture coincides with the overlay seen in Figure 109, which utilizes a sutural registration system.
If the various basic concepts and principles of growth are applied to this system of registration without fixed registration points, it is seen that one does not violate the other, in contrast to methods employing fixed landmarks. This is true because the procedure is in fact based directly upon these principles, including the process of regional remodeling changes, cortical relocation, and differential surface activities.
SCHEME OF MAXILLARY GROWTH. The
composite movements that the maxilla experiences during growth are schematized in Figures 104 and 105. The purpose of this interpretive diagram is to illustrate the cumulative composite effects of (1) differential resorption and deposition on its various surfaces, and (2 ) the process of displacement as the bone simultaneously becomes moved downward and forward in association with sutural growth from above and behind. In the first figure of the series, the maxilla is pictured with its frontal and premaxillary projections. Several arbitrary points are included as reference marks to demonstrate the nature of movements relative to the different growth processes involved. The maxillary process of the frontal

Craniofacial bone growth ( 234 )
Diagram of maxillary growth. See text for descriptions. (Continued*)

Composite facial growth
bone (y ) and the maxillary process of the zygomatic bone (x) are also schematized. For simplicity of illustration the zygomatic projection from the maxillary body is omitted.
In the second diagram of the series (Fig. 104, bottom), the singular effect of displacement relative to sutural growth associated with x and y is illustrated. (This growth is interpreted as essentially passive in character. The force of displacement is considered to originate in other contiguous tissues, such as the nasal septum, the expanding soft tissues of the oral cavity, etc.) The frontal portion (y) moves in a forward direction (arrow) as a consequence of its own growth (cortical drift) as well as an
( 2 3 5 )
anterior movement produced by growth within the cranium. Similarly, the zygomatic portion (x) moves inferiorly (arrow) as a result of its own cortical growth and growth in the cranial base and calvaria. Both bony processes, however, become elongated during sutural bone growth, as shown by the shaded increments. Displacement of the maxilla associated with y results in a downward movement of the whole bone, and displacement at x is associated with a forward movement of the entire maxilla from position 1 to position 2. Note that the reference points (A, B, C, D) are carried in corresponding directions. Actual growth changes in the bone, although occurring simultane-
Diagram of maxillary growth. See text for descriptions. (Continued from Figure 104)

( 2 3 6 )
ously, are not shown in order to visualize the separate effect of displacement produced by growth in other bones.
In the third diagram (Fig. 105) growth changes occurring in the maxilla itself are schematized. Note the regional distribution of surface resorption (—) and deposition ( + ) that brings about cortical movements in a number of divergent directions. At the same time the whole bone becomes enlarged by this same remodeling process. Note also the relocation in relative positions of the various marker points. Point A no longer exists as such, because the bone comprising this point has undergone removal and its actual position is now located free in the nasal cavity. The resorptive surface shown represents the lining cortex of the nasal chamber. Point B has been relocated from the frontal process into the maxillary body (floor of the orbit). Point D has become released because of the regressive nature of the premaxillary cortex associated with its downward growth. Point C has become more deeply enclosed as a result of continued growth on all external sides of the maxillary tuberosity. The complexities encountered in attempting to localize and account for specific points in a growing, moving bone, such as the maxilla, are evident.
Position 3 marks the relative location of. the old outline of the maxilla, prior to its own size increase, within the greatly enlarged dimensions seen in final position 4. Note that the enlargement of the bone has contributed to further displacement of the maxilla. Displacement from I to 2 is associated with growth increases by the separate bones x and y. Displacement from position 2 to 3, however, is associated with the maxilla's own growth increases as illustrated in position 4.
In summary, the composite pattern of growth involves the following: downward movement in conjunction with the separate
Craniofacial hone growth
bone y; forward movement in conjunction with the separate bone x; combined forward and downward displacement in relation to maxillary growth itself; and regional increases in size with corresponding remodeling changes in local configuration by the process of cortical drift.
SUTURAL AND REMODELING GROWTH. As
seen above, the composite growth of the maxillary complex involves essentially (1 ) sutural bone additions, ( 2 ) extensive surface apposition on the posterior maxillary tuberosity, ( 3 ) alveolar elongation, and (4 ) remodeling growth in virtually all other parts and surfaces of the whole bone. The relative contributions of these different growth activities are difficult to visualize in ordinary cephalograms, because they merge directly with each other as a growth continuum. Although their individual roles can be visualized by tracing overlays utilizing differential surface activities (see previous section), the actual extent of each can only be approximated. Using the data derived from Bjork's metal implant studies, however, it is possible to segregate the relative contributions provided by sutural and remodeling growth, and to demonstrate the activity of one in relation to the other.
In Figures 106 and 110, composite profiles based on serial cephalograms of normal children at 6, 9, and 15 years of age are shown (Enlow and Hunter, 1966). The component facial bones, including the maxillary, frontal, and zygomatic, are then separated (Figs. 107, 108, 111). Utilizing Bjork's data, ratios of new bone additions at the various sutures were calculated for each age level, and these increments were then applied to the sutures, with half of the total increment to each side of the sutural line. Such equal additions on apposed sutural edges are necessarily arbitrary, since differentials in actual extents of growth can

Composite facial growth
occur. These differences, however, do not in themselves affect the total extent of displacement involved.
After sutural increments were added, the separated bones were then reassembled (Figs. 107, 108, 111). The resulting profiles, representing the facial configuration produced only by sutural bone growth, were then superimposed so that the 6-year-old face was registered over the 9-year-old and 15-year-old profiles. Sutural additions were applied to the 9-year-old face and then superimposed over the 15-year-old profile. In registering all profiles, the adjusted suture lines of the 6- and 9-year-old bones were aligned directly with corresponding suture lines of the older bones, respectively.
( 2 3 7 )
The resulting overlays demonstrate first the actual amounts of sutural increases and the extent of displacement associated with these increases. Second, they demonstrate the extent of remodeling growth that accompanies sutural increases. The differences between the surface contour lines of the younger and older profiles represent the directions of surface growth as well as actual distances moved as a consequence of cortical drift. Thus, the whole picture of remodeling movements with corresponding adjustments is seen in all areas of each bone considered, and the extent of regional resorption and deposition on the different periosteal surfaces can be visualized. The cumulative composite of these changes, includ-
Composite facial profiles at ages 6 (a), 9 (b), and 15 (c) years. Dimensions are based on an average of measurements taken from serial ceph-
alograms of 10 normal Caucasian children (5 boys and 5 girls). (From Enlow D. H., and W. S. Hunter: Am. J. Orthodont., 1966.)
Figure 106

( 2 3 8 )
ing the process of displacement, is responsible for the total extent of growth in the facial skeleton.
Developmental patterns visualized by this overlay procedure, unlike superimposition based on fixed registration landmarks in the cranial base, do not violate the fundamental principles of progressive bone growth. The procedure is based essentially on the growth increments themselves, rather than on the combination of growth and displacement seen when utilizing fixed landmarks in separate, unrelated bones. Thus, the principles of relocation, differential resorptive and depository
Craniofacial bone growth
activity on different surfaces according to directions of growth, and the other basic concepts dealing with actual bone growth are all directly applicable (see page 105). Furthermore, when the various separate bones are reassembled following additions of sutural growth increments, the factor of displacement is also demonstrated. If serial tracings of individual bones, such as the maxillary or the zygomatic, are superimposed according to known directions of endosteal and periosteal growth, as described in the previous section, the growth pattern conforms directly to overlays based on the present procedure.
Composite sutural and remodeling growth changes in profiles between the ages of 6 and 9 years. Tracings of individual component facial bones of the 6-year-old profile were separated and increments of bone were added to each side of the line at the frontozygomatic and frontomaxillary sutures. The parts were then reassembled and superimposed (stippled area) over the 9-year-old
profile. Downward displacement of the entire facial complex is associated with growth at these particular sutures. Remaining differences between the facial outlines at 6 and 9 years are produced by remodeling growth, which proceeds in conjunction with sutural growth. (From Enlow, D. H., and W. S. Hunter: Am. J. Orthodont., 1966.)

Composite facial growth
The mosaic pattern of facial growth
The modes of enlargement, the nature of successive remodeling changes, and the cumulative interrelations between the different growing bones are described below for the various major regions of the human face.
( 2 3 9 )
These descriptions are illustrated in Figures 107, 108, 109, and 111.
THE FOREHEAD. The massive expansion of the cerebrum results in a marked anterior and superior enlargement of the frontal bone. This portion of the cranium comes to overlie
Composite sutural and remodeling growth between the ages of 6 and 15 years. Tracings of individual bones of the 6-year-old facial complex show the addition of new bone increments on each side of the line at the frontozygomatic and fronto-maxillary sutures. The reassembled profile is then superimposed (stippled area) over the 15-year-old
face, with corresponding suture lines registered. The differences between the profile lines at the two ages indicate the regional directions and actual extent of remodeling growth. (From Enlow, D. H., and W. S. Hunter: Am. ]. Orthodont., 1966.)

( 2 4 0 )
the orbital cavities (compare with nonprimates, Figure 82). The floor of the anterior cranial fossa, formed by a part of the frontal bone, provides the roof for each orbit. The growth of the cerebral hemispheres is associated with a displacement of the right and left orbital cavities into a forward-facing position aligned with the flat, broad, vertical forehead above it. The breadth of the nasal bridge is simultaneously reduced in comparison with other forms (Fig. 84), and the cribriform plate becomes displaced to face downward toward a more vertical nasal chamber rather than forward as in species having an elongate snout.
The anterior and superior movements of the upper half of the forehead take place in conjunction with sutural expansion. In the lower half, however, the expansive movement is
Craniofacial bone growth
largely a result of direct cortical drift (see page 220). With increasing age, the frontal bone in the region just superior to the orbital rim is seen to drift forward, and its cortical thickness increases. The intervening diploe becomes progressively replaced by the frontal sinus. The dimensions of this space enlarge as the external cortical lamina continues to move anteriorly, thereby contributing to the formation of the glabella and the prominent supraorbital ridges. In Figure 108, note the diverging relationships between the forehead and the malar region as they continue to grow in anterior and posterior directions, respectively.
THE MALAR REGION. The malar complex undergoes growth movement in a progressive,
The 6- and 15-year-old profiles in this overlay were registered in a manner corresponding to that seen in Figure 108. In addition, the total extent of growth, remodeling, and displacement at the zygomaticotemporal suture is represented. The actual location of the sella relative to the 15-year-old profile is indicated (A). The original position
of the sella relative to the zygomatic process of the frontal bone in the 6-year-old stage (B and B') is indicated. Similarly, the original positions of the sella relative to the 6-year-old temporal bone (C and C) and the zygomatic bone (D and D') are shown.

Composite facial growth
posterior direction as the maxillary arch becomes lengthened at the posterior margin of its tuberosity (Fig. 108). This pattern functions to maintain a constant position of the malar region relative to the maxillary arch, the orbit, the temporal area, and the cranial base. Progressive resorption from the anterior face of the zygoma and the forward margin of the lateral orbital rim brings about the posterior manner of malar repositioning. The cortex in these areas is composed of endosteal bone.
The contrasting direction of growth that takes place in the malar region relative to the forehead produces a number of notable topographic characteristics in the face. The backward mode of malar movement and the forward movements of both the frontal and nasal regions serve to draw out overall anteroposterior dimensions and to expand the contours of the face. Because of their divergent growth directions, the positional relationships between the upper (frontal) and lower (malar) parts of the orbital rim undergo progressive change
( 2 4 1 )
with increasing age. In the younger profile pictured in Figure 106, the superior and inferior margins of the orbit lie in the same approximate vertical plane. The malar region of a neonatal skull actually lies anterior to the upper orbital margin. In the older profile, however, note that the supraorbital region has come to protrude noticeably forward of the cheekbone and the inferior orbital rim. The orbital ridges of the frontal bone extend beyond each eyeball in a mature face. The eyeball extends forward of the lower margin of the orbital cavity, however.
It is seen in Figure 108 that the entire zygomatic bone becomes displaced in an inferior manner in conjunction with continued bone growth at the frontozygomatic suture. In company with this movement, the zygomatic bone itself simultaneously undergoes a series of remodeling growth changes. The vertical dimensions of the arch increase significantly in depth, particularly in the anterior part near its junction with the maxilla. This increase is pri-
Frontal outlines at 6 (left) and 15 (right) years of age. (From Enlow, D. H., and W. S. Hunter: Am. ]. Orthodont., 1966.)

( 2 4 2 )
marily a result of massive bone deposition along the inferior margin of the zygoma. The superior border also receives new bone deposits but in lesser amounts. Note that the level of the superior margin remains in the same approximate positional relationship with the auditory meatus throughout these various growth changes. Even though the upper surface undergoes slight periosteal bone growth, the downward displacement of the whole zygoma obscures this cortical growth movement. The relationships between the lateral part of the orbital floor and the superior margin of the zygomatic arch undergo a positional change because of the resorptive nature of the zygomatic portion of the floor in the orbital cavity.
THE NASAL REGION. The nasal chambers become elongated in vertical axes in consequence of the downward displacement associated with continued bone deposition at the frontomaxillary suture. In this process, the lateral walls of the chambers comprising the frontal processes of the maxilla become significantly lengthened (Fig. 111). During the downward movement of the nasomaxillary region produced by displacement, its cortical components simultaneously undergo sequential remodeling growth changes. The periosteal surfaces of the lateral nasal wall are oriented in such a manner that surface bone deposits, together with contralateral resorption from the cortical surfaces lining the nasal cavity, produce cortical drift in a combined lateral, anterior, and superior direction. The forward direction of growth contributes to the progressively expanding contour between the nasal and receding zygomatic areas, and it projects the anterior margin of the nasal aperture in a continued forward direction. In Figure 106, the anteriormost point at the nasal tip in the younger profile lies somewhat behind the nasal spine beneath it, in contrast to the expanded
Craniofacial bone growth
positional relationships seen in the older profile. The characteristic protruding bony nose, a feature unique to the human face, is a result of these remodeling changes in combination with other related but contrasting growth movements taking place in the premaxillary region.
A characteristic reversal line occurs near the base of the nasal portion of the maxilla at a point where the nasal region grades into the premaxillary area. Below this reversal line, the bony nasal wall grows by cortical drift in an actual posterior direction. The periosteal surface is resorptive, and the cortex is composed of endosteal bone tissue, in contrast to the anterior direction of movement produced by periosteal deposition above the line. The regressive nature of cortical growth inferior to this key reversal is concerned with the downward movement of the premaxilla and the backward growth of the malar region. The resorptive character of the cortex in the lower portion of the nasal wall functions to adjust the changing relationships between the regressive premaxillary region and the forward-growing nasal wall above it. The anterior margin of this lateral wall becomes greatly lengthened as a consequence of the combination of anterior growth in the superior part with recession along the inferior portion. It also results in the markedly changing angulation of the anterior nasal rim, as seen in Figure 108.
The bony nasal walls also face laterally, and the pattern of cortical drift produces a corresponding distinct lateral enlargement of the nasal chamber, thereby significantly broadening its transverse internal dimensions. In Figure 111, note that the extent of lateral cortical movement is greater in the inferior part of the nasal cavity as it expands into suborbital maxillary regions.
Although periosteal bone is added onto the superiorly facing surface of the nasal walls, the

Composite facial growth
level of the upper nasal contour is not actually elevated during continued growth. The tips of the nasal bones do not rise but are seen to drop slightly in many individuals as a result of continued bone growth along the downward-facing anterior edge of the nasal aperture. The floor of the nasal chamber at the same time similarly descends but to a differentially greater extent. It was pointed out in Chapter 7 that forward growth of the sloping
( 2 4 3 )
nasal contour results in successive relocation of areas formerly located near the tip, which are lower in their level, into new regions placed farther up the elevated slope. The "upward" manner of growth thus functions primarily to bring about this sequential process of superior relocation in changing levels even though the entire nose itself does not move in an actual upward direction (Figs. 63 and 108).
Individual bones of the 6-year-old facial complex are separated in order to show increments of new growth on each side of the suture line at the frontomaxillary and frontozygomatic sutures. The reassembled, adjusted profile is superimposed over the 15-year-old face, with suture lines registered (c). Measurement of actual increases at the
zygomaticomaxillary suture cannot be accurately indicated in this plane because of its angle. The remodeling sequence of the upper orbit is illustrated in b and shows the lateral movement of the orbital roof. (See text for further descriptions.) (From Enlow, D. H., and W. S. Hunter: Am. J. Orthodont., 1966.)

( 2 4 4 )
The region of the nasal bridge represents an area in which normal variation in growth pattern occurs. Although the outer cortical surface in this area is typically depository in nature, it may demonstrate contrasting resorptive growth activity in some individuals. The process produces a downward cortical movement resulting in a slight depression of the nasal bridge (Fig. 112). In this situation the
Craniofacial bone growth
proximal half of the nasal bones is resorptive, but the approximate distal half remains depository. This brings about a marked change in the angulation and profile of the nose. A similar but less marked pattern can also apparently be produced in a nasal cortex that is entirely depository in character by differential growth rates in its proximal and distal parts.
The vertical dimensions of the nasal chambers become extensively enlarged during nasomaxillary growth. In Figures 108 and 111, note the marked descent of the nasal floor as the maxillary arch grows in an inferior direction. It was seen in Chapter 8 that the human nose, in comparison with the elongate snout of nonprimate forms, is oriented in a primarily vertical plane in association with the downward displaced olfactory lobes, the horizontally placed cribriform plate, and the vertically oriented olfactory nerves. These features are in contrast to the arrangement found in other species having a long, forward-projecting nose combined with a correspondingly elongate upper jaw. The decreased extent of anterior growth in the human nose reflects the reduced status of nasomaxillary elongation in general. In the human face, the predominant directions of nasal enlargement are downward and backward, a feature associated with the vertical alignment of the whole face. In snouted forms, a marked forward direction of growth occurs, although variable degrees of inferior and posterior expansion also take place.
The vertical elongation of the human nasal cavity is produced by the combination of (1 ) lengthening at the frontal process of the maxilla in a superior manner at the fronto-maxillary suture (associated directly with downward displacement), and (2 ) a significant inferior drop of the nasal floor. The latter is produced by the downward drift of the entire palate as bone is deposited on the oral side with resorption from the opposite nasal surface.
A remodeling variation in the region of the nasal bridge is schematized in a. It involves direct depression in the cephalic portion of the bony nose by a process of regressive cortical growth (solid line).
Diagrams b and c illustrate a spread of possible variation involved in the downward movement of the premaxillary cortex. In b note the "tilting" effect associated with normal premaxillary remodeling in which the upper part undergoes posterior regression while the lower portion becomes extended in an anterior direction. Note also that elongation at the alveolar margin produces a slight forward protrusion of the pre-maxilla even though the external surface of the premaxillary region as a whole is resorptive.

Composite facial growth
This resorptive surface continues directly onto the inner lateral walls where it contributes to the broadening of the nasal cavity in transverse dimensions.
THE MAXILLARY ARCH. Like all other portions of the maxilla, the maxillary arch undergoes varied movements that are produced by both displacement and growth. As the whole bone receives forward displacement, the arch becomes substantially lengthened by bone growth at its posterior free (distal) ends. As it experiences inferior displacement, the arch simultaneously undergoes a complementary process of downward remodeling growth. This inferior direction of cortical growth movement in turn embodies two major growth regions. The first is the alveolar ridge and the entire alveolar face, which become lengthened by continued bone deposition on the free margin and by appropriate combinations of resorption and deposition on periosteal and endosteal surfaces. The second growth area involves the palatal region, which undergoes a major inferior growth process. This adds significantly to the total distance of downward maxillary arch movement. The inferior manner of growth in the arch thus is a composite process involving displacement (in conjunction with bone additions at the frontomaxillary, zygomaticomaxillary, and frontozygomatic sutures), bone growth on the alveolar margin and the entire endosteal or periosteal alveolar surfaces, depending on the part of the arch involved, and downward growth associated with the palatal complex. The maxillary arch becomes widened by these same processes (Figs. 61 and 111).
Whereas the upward growth of the mandibular arch is produced by the single process of alveolar extension, the downward growth of the maxillary arch is the sum of these multiple contributing factors. Compare the dif-
( 2 4 5 )
ferential extent of upward mandibular arch movement (Fig. 103) with downward maxillary arch movement (Fig. 108). Note that the inferior margin of the maxilla moves a great deal farther because of the cumulative nature of its own growth in combination with the expansion of the vertically oriented nasal region. Similarly, maxillary teeth must also be carried in an inferior direction (by drifting in addition to the movements of eruption) much farther than the opposing mandibular teeth move in a superior direction during growth and eruption.
In response to the marked extent of downward, composite nasomaxillary growth, the ramus of the mandible in the human (and in some other primates) has become greatly lengthened in a vertical manner with a high-positioned condyle. This arrangement accommodates the relatively great degree of inferior nasomaxillary movement. The vertical disposition of the ramus also represents an adaptation for the closer positioning of the maxillary and mandibular arches to the cranial base as a consequence of the ventral cranial flexure.
In Figure 109 it is seen that the nasomaxillary complex undergoes processes of displacement in three primary planes. First, downward translocation of whole bony elements occurs with continued sutural bone growth at the frontomaxillary, zygomaticofrontal, and the zygomaticomaxillary sutures. A slight degree of forward thrust is also related to growth at the frontomaxillary suture. Lateral displacement in the malar region is associated primarily with growth activity at the zygomaticomaxillary suture. Forward displacement is related largely with continued bone growth at the zygomaticotemporal and, to a lesser extent, at the oblique, more transversely oriented, zygomaticomaxillary suture. In Figure 109, note the much greater degree of bone deposition at the zygomaticotemporal suture as com-

( 2 4 6 )
pared with the downward-facing sutures between the frontal, maxillary, and zygomatic bones.
In summary, the bones of the face undergo a process of displacement away from each other as they all enlarge in size. The process of displacement occurs largely at sutural contacts, although sutural bone growth itself is considered to be a secondary response to the force of displacement. As bone is added onto the sutural surface, as well as other surfaces throughout all the bones, the regional parts of each bone become involved in relocation. Remodeling alterations then function to reshape and resize each regional portion and to enlarge the entire element. It is interesting to note that in the movement of the maxillary complex, the downward process of displacement follows the same course as the downward-moving growth process in the arch. In the forward movement of the maxillary and mandibular arches, however, the anterior mode of displacement contrasts with the posterior manner of actual remodeling growth.
THE ANTERIOR PORTION OF THE MAXILLARY
ARCH. The outer surface of the cortical bone located anteriorly to the key malar reversal line is characteristically resorptive. Posterior to this line, the surface is depository in nature. The basis for this contrasting pattern of remodeling growth, as explained previously, lies in the directions these different regional surfaces face relative to the course of growth. In the forward portion of the arch the periosteal surface faces away from the actual inferior direction of growth movement. Its cortex thus moves by a process of endosteal bone formation together with surface resorption. Widening of the arch is accomplished at the same time by elongation of the alveolar plates at the crest. In the posterior half of the arch, surface orientation abruptly changes, and here the periosteal side
Craniofacial hone growth
faces the downward growth direction. Unlike the forward portion, the posterior part of the arch moves inferiorly by periosteal surface deposition as the alveolar region becomes lengthened and broadened.
As the entire maxillary arch grows inferiorly in advance of the downward-expanding nasal region, successive growth stages involve the formation and reformation of entirely new arches in a continuous manner. Each new arch in successive stages is composed of new bone tissue that is formed as the whole bone grows downward. Each advancing age level in Figures 107 and 108 is marked by a bony dental arch that not only becomes displaced inferiorly in relation to sutural growth but also becomes replaced by successively new generations of bone occupying new positions as a consequence of direct cortical growth movement. Thus, the alveolar bone that occurs in relation to the teeth at younger growth stages does not represent the actual bone tissue that encloses these same teeth in subsequent stages.
The profile overlays seen in Figures 107 and 108 demonstrate the nearly vertical downward growth of the premaxillary region. As mentioned above, this movement is accomplished by endosteal cortical growth in the outer lamina. The "regressive" nature of the human premaxilla, involving direct surface resorption, is thus concerned primarily with the marked inferior movement of the nasal floor and maxillary arch. Significant recession in a posterior direction, as such, is not involved. Because of the inclined concave orientation of the outer cortical plate, however, continuous relocation of parts along the vertical premaxillary curvature occurs, and the regressive nature of cortical drift functions to sequentially align the moving contour by localized backward growth movements (Fig. 63). In Figure 108, for example, note that the anteriormost tip of the premaxilla in the younger profile protrudes

Composite facial growth
forward of the level in the concave fossa occupying this same area at a later growth stage. This region thus undergoes continuous, direct, regional posterior growth movements as a consequence of the relocation of its areas produced by the downward enlargement of the whole bone.
Remodeling growth in the critical premaxil-lary area in general is subject to a range of individual variations. Its primary direction of movement is essentially straight downward. Although the periosteal surface of the outer cortical plate is resorptive, the tip of the pre-maxillary bone may protrude somewhat with increasing age as a result of elongation at the free edge of the alveolar margin. A "tilting" effect thus takes place in which the lower region elongates in an anterior direction while the upper part undergoes a slight regressive, posterior cortical drift. Normal variations in the differential extent of these divergent movements can produce the approximate range schematized in Figure 112. In the alveolar region just above the chin, the uniquely human characteristic of external surface resorption is associated with an adjustment process to the maxilla in stabilizing occlusion between the upper and lower jaws. It was pointed out previously that this particular region in the mandible is quite variable in structure and growth pattern. This variation appears to be an interrelated accommodation to the normal range of variation in the maxilla, as suggested in Figure 113.
THE ORBITAL REGION. The basic growth plan of the bony orbit represents one of the most complex remodeling patterns in the entire craniofacial skeleton. Its walls are composed of the separate frontal, maxillary, sphenoidal, ethmoidal, lacrimal, and zygomatic bones. The orbital roof is closely associated with growth changes occurring in the anterior
( 247 )
part of the cranial floor. Other portions of the orbit are directly related to growth processes taking place in the nasal region and parts of the middle face. The growth of the orbit is also related directly to the corresponding growth of its own soft tissue contents, including the eyeball, glands, adipose, vessels and nerves, and muscle tissue. The growth of the bony orbit, however, must necessarily proceed in conjunction with other orbital relationships including the brain from behind and above, the nasal chambers on the medial side, the dental arch below, and the muscles of mastication on lateral sides. The unique upright human posture, as seen in Chapter 8, is associated with the enlarged cerebrum, vertical face and forehead, broad and squared cheekbones, and re-
Figure 113
The range of normal remodeling variation (A, B, C) in the maxilla (X) and the mandible (Y) is apparently mutually interrelated as the growth pattern of one becomes directly adapted to the other. Exaggerated for clarity.

( 2 4 8 )
duced nasal breadth. These factors are all related to the distinctive placement and orientation of the paired orbital cavities in the human face.
In general, the orbits grow and move in a forward, descending, and slightly lateral direction. This is accomplished by the V principle of growth in which continued bone additions occur on the inner side of the conical cavity (inner surface of the V) . This moves the entire area forward and enlarges its dimensions at the same time. With the exceptions noted below, the lining of the orbit is characteristically depository in nature.
The medial wall of each orbit is depository except in a portion of the lacrimal bone, an element that functions as the critical remodeling link between the other differentially growing bones surrounding it (see page 163). Note that the part of the lateral wall on the inside of the orbit comprising the zygomatic bone is resorptive. This combination is the basis for the lateral shift of the orbits as they grow to the side away from each other. The movement of the lateral wall slightly exceeds that of the medial wall, thereby increasing the horizontal dimensions of the entire cavity. This lateral mode of growth takes place in conjunction with corresponding remodeling changes occurring in the glabellar region, the various superior parts of the maxilla, the nasal wall and separate nasal bones, and the ethmoidal portion of the nasal area. The latter region undergoes substantial lateral movement during postnatal growth (page 218). Remodeling movements in the lateral orbital area also proceed in conjunction with the changes occurring in the entire" zygomatic region. The zygomatic parts of the orbit, including the lateral rim and a portion of the lateral wall, undergo posterior regression. This part of the rim and the lining side of the wall have periosteal surfaces that are characteristically resorptive, thus
Craniofacial bone growth
producing a posterior as well as a lateral shift of the lateral orbital area as the whole zygoma drifts posteriorly. These resorptive surfaces face away from both growth directions.
As the entire lateral orbital rim recedes in a backward course, however, the superior rim grows in an opposite forward direction. This produces the changing relationships between them as the superior orbital margin comes to lie anteriorly to the inferior rim. This is a distinctive characteristic of the human face. A forward rotation, in effect, has taken place because of divergent directions of cortical growth in the upper, lateral, and lower margins that bound the orbital cavity.
The anterolateral part of the orbital roof beneath the overhanging supraorbital margin is characteristically resorptive. This provides two growth functions. First, it is associated with the transverse movement of the entire cavity. The resorptive nature of this portion of the domed roof brings about a lateral drift of its cortical lining, as seen in Figure 111. Second, because the inner resorptive surface faces away from the forward direction of growth at the external orbital ridges, it undercuts the supraorbital overhang, thereby moving the lining periosteal cortex anteriorly as the outer cortex drifts in a corresponding direction.
In conjunction with bone growth at the frontomaxillary suture (Fig. 111) the frontal process of the maxilla becomes lengthened, and the whole maxilla is simultaneously displaced downward in a direction away from the cranium. This process of displacement lowers the orbital floor continuously, but the floor itself receives periosteal bone deposits at the same time (Bjork, 1955b). This serves to raise it proportionately, thereby adjusting the level to that of the remainder of the orbit as the entire maxilla becomes displaced in an inferior course.
The orbital floor faces laterally, superiorly,

Composite facial growth
and slightly anteriorly, and continued bone deposits function to move it in all three directions. The lateral movement involves area relocation. The lateral portion of the sloping floor is lower in level than the more medial regions, and as the floor shifts to the side the medial part continuously comes to occupy regions that were lower in level. The depository nature of the orbital floor thus serves to sequentially elevate former lateral areas into the new, higher positioned medial regions. As the floor drifts laterally, the resorptiye lateral wall moves progressively to the side, thus making way for the lateral shift of the whole cavity. A portion of the orbital floor in the lateral part of the cavity is composed of the regressive zygomatic bone. The remodeling circumstances in these two parts of the floor differ markedly. Because the lateral, zygomatic portion is actually raised in conjunction with bone deposition at the zygomaticomaxillary suture (Fig. 111), the resorptive nature of its cortical surface serves to proportionately move it inferiorly to align the zygomatic surface with the differentially moving maxillary part of the orbital floor. Thus, the basic nature of cortical remodeling in the medial and more lateral portions of the orbital floor are in sharp contrast.
The inferior level of the lateral orbital rim drops somewhat with continued remodeling growth as the overall size of the orbit enlarges (Fig. 111). This drop is produced by the characteristically resorptive nature of surface growth activity in the zygomatic part of the lateral wall and floor.
In Figure 111, note the pattern of suture distribution between the bones that form the orbit. Growth and remodeling processes in the roof of the orbital cavity necessarily differ markedly from those in the floor because of suture placement. As the zygoma becomes displaced laterally, continued bone growth takes place at the zygomaticomaxillary suture. In
( 2 4 9 )
this same figure, note that a corresponding mechanism of sutural growth does not occur in the orbital roof. The lateral shift of the anterolateral part of the domed roof is produced solely by cortical drift associated with the characteristic resorptive surface that lines this region. In contrast, the shift to the side of the lateral part of the orbital floor is produced by a combined, complementary process of cortical drift and sutural bone growth. At the same time, the lateral (external) surfaces of the zygoma receive bone deposits in conjunction with the endosteal manner of bone growth on the opposite, lining side of the orbit, which contributes to the lateral remodeling movement in this part of the orbit. The process takes place in combination with bone growth at the zygomaticomaxillary suture.
In the lateral region of the roof beneath the overhanging supraorbital ridge, the resorptive nature of the cortical surface produces an actual elevation of this local area while the roof in general becomes lowered (Fig. 111). The basis for this change involves area relocation. As the vertex of the domed roof grows laterally (and anteriorly), it moves into lateral regions previously occupied by the downward-curving lateral wall. The area thus becomes successively raised to form the higher levels of the dome. This remodeling change is brought about by surface resorption with endosteal bone formation.
As a result of bone additions at the fronto-maxillary and zygomaticofrontal sutures, the relative height of the roof becomes increased. However, the lining surface of the orbital roof is depository (except for the restricted anterolateral zone of resorption mentioned above). This functions to proportionately lower the roof, as well as move it laterally and anteriorly in conjunction with the floor, as an adjustment to vertical lengthening at sutures. The same growth pattern serves to simultaneously lower

( 2 5 0 )
the floor of the anterior cranial fossa in relation to cerebral expansion.
Facial topography
The composite of all the morphogenetic and remodeling changes described in the preceding paragraphs represents the basis for changing topographic features that characterize the face from childhood through maturity (Fig. 114). These generalized changes are summarized below.
The forehead of the very young child is marked by its prominent, bulbous configuration. The remainder of the face is diminutive in general appearance. However, with the forward growth of the superior orbital margin, and the expansion of the frontal sinuses, the progressive enlargement of the supraorbital ridges, the protrusion of the glabella, and the elevation of the nasal bridge, the relative prominence in the appearance of the forehead becomes somewhat lessened. Its original bulbous character is altered to a more sloping contour (with ethnic and sex differences in extent).
The forward manner of remodeling growth in these various regions of the forehead is accompanied by forward movements in both the upper and lower jaws. The combined result is a progressive change in the overall angulation of the profile and the disposition of the face relative to the cranium.
The size of the nose increases significantly in a vertical plane. The maxillary arch of a young child actually occupies the area of the future nasal cavity in the adult. The nose also becomes more protruded as a result of continued bony as well as soft tissue growth in a forward manner. It expands further in breadth as the whole maxilla enlarges in transverse dimensions. The nasal bridge becomes progres-
Craniofacial bone growth
sively more prominent in most individuals, although it may become slightly depressed in some persons as a normal remodeling variation.
The eyes with their bony orbits move apart. The adjacent cheekbones also move laterally, away from each other, as the face broadens. The entire malar region becomes noticeably more massive and squared. It increases in depth because of extensive bone deposition along its inferior margin.
The mandible of the young child is characterized by its diminutive appearance. With increasing age, it also becomes more massive and squared in character. The forward contour of the lower jaw becomes flattened, as does the anterior portion of the maxillary arch. These factors, together with the growth pattern of the malar regions, produce a progressively more flattened appearance in the face as a whole.
The lateral growth of the mandibular trihedral eminences and gonial flares, the development of permanent dentition, and the expansion of the alveolar regions in both jaws produce a full external appearance in the entire masticatory region. These growth factors can partially obscure the marked extent of enlargement in the malar areas.
The chin is poorly developed in the neonatal mandible. With increasing age, the mental region becomes progressively more prominent and develops into a sizable bony protuberance.
Because of divergent growth directions in the nasal and malar portions of the maxilla, the contour that bridges these regions becomes noticeably expanded during postnatal maturation. Changing positional relationships between the forehead and the cheek are similarly observed as a consequence of their differing growth courses.
The vertical dimensions of the whole face become significantly lengthened. This is a composite result produced by growth of the

Figure 114
The growing face, at 8 months, 6 years, 8 years, and 20 years of age. (Courtesy of William L. Brudon.)

( 2 5 2 )
mandibular body with its dental arch, the mandibular ramus, and the marked downward growth of the nasal region and the maxillary arch in combination. The entire lower face is displaced inferiorly relative to the cranium. As a consequence, changing positional relationships occur between the various components of the face and independent cranial landmarks such as the sella and the auditory meatus.
The whole face becomes deeper in an anteroposterior plane. This is produced by the forward elongation of the nose, the anterior mode of maxillary and mandibular displacement, the posterior movement of the entire zygoma, the backward movement of the lateral orbital rim, and the overall posterior lengthening of the dental arches. Because these various facial growth movements proceed in differing directions, the whole face, in effect, becomes drawn out in several divergent planes.
In conclusion, a concept of growth equivalents is described. This involves direct interrelationships during growth between the cranial base, the nasomaxillary complex, and the mandible. These areas do not enlarge as separate, isolated units. Rather, they are bound by closely coordinated and mutually interdependent growth activities. Their various growth movements require complementary equivalents in functional and architectural design. Growth equivalents provide corresponding, adaptive adjustments that serve to consolidate overall processes of enlargement into a composite system of total growth. The anterior elongation of the spheno-occipital region, for example, necessarily produces a significant movement of the middle face in a forward direction. In the mandible, cranial base elongation and resultant anterior displacement of the maxilla are accommodated by corresponding increases in the breadth of the ramus, thereby moving the mandibular arch in a equivalent direction and to a proportionate extent. The ramus serves to bridge this elon-
Craniofacial bone growth
gating span between the temporal bone and the forward-moving maxillary arch. The growth of the anterior cranial fossa progressively expands the sizable "facial pocket" beneath it. This enlarges the prescribed area within which the face itself correspondingly continues to grow. Although characteristic differentials in timing and extent occur during such growth changes, the basic processes themselves are nevertheless directly related. The vertical elongation of the middle face is the sum of nasal, orbital, and maxillary alveolar lengthening. Compensatory positioning of the mandible relative to composite downward maxillary expansion is served by an equivalent, proportionate vertical elongation of the ramus. Maxillary placement in relation to the anterior cranial fossa is governed (indirectly) by the various sutures associated with the zygoma and by the maxillary frontal process. These sites "adjust" the maxilla in both a horizontal and a vertical plane. The overall growth of the mandibular ramus is, in effect, an equivalent to the growth in these particular sutures. The lengthening of the condylar neck may be equated to increases in the vertically oriented frontal processes of both the zygomatic and the maxillary bones together with downward palatal drift. Similarly, a distinct parallel occurs between the anteroposterior dimensions of the zygoma, the ramus, and the sphenooccipital portion of the cranial base. A proportionate but differential vertical relationship exists between the increasing height of the clivus, the middle face, and the ramus. In general, actual cause and effect relationships are operative as increases in any one anatomical part of the skull necessarily accompany corresponding increases in complementary mor-phogenetic segments of the other parts. Studies should now be made to identify and quantitate the principal "lead" segments in these and other similar relationships.

(11)
Glossary of
reversals
The 'placement and the orientation of reversal lines are a key factor related to the basic nature of remodeling patterns throughout the whole skull. The distribution of the major reversal lines determines the corresponding distribution of resorptive and depository surfaces and the occurrence and arrangement of endosteal and periosteal types of bone tissues. These factors are all involved in the regional modes of growth in the many localized areas and parts of each bone. They are concerned with directions of growth, sequential processes of relocation, differential growth activities on different surfaces according to directions faced, and the processes of reshaping and resizing. The positioning of any given reversal line is critical, because it is the factor that produces many of the regional differences in growth movements that characterize each individual bone.
As a bone enlarges in overall size, the re
versal line itself necessarily undergoes continuous relocation in order to maintain constant relative position on the surface of the growing bone. The line, thus, gradually moves across the bone surface in a given direction as this surface experiences progressive remodeling.
A normal range of variation occurs in the placement of most reversal lines. Within this range, differences contribute to a formative basis for variations in gross morphology and corresponding diversity in the topographic features of the face. Quantitative variations in the extent of differential growth activities further augment dissimilarities in the general appearance of the face.
The major reversal lines throughout the skull are listed below with a brief account of their functional significance. These various reversals are illustrated in Figures 115 through 117.
253

Craniofacial bone growth ( 2 5 4 )
Reversals, frontal views. A, malar; B, nasomaxillary; D, intraorbital (sphenoidal); E, intra
orbital (lacrimal); F, intranasal; G, intraorbital (lateral); L, lateral mandibular; M, mental.

Reversals ( 2 5 5 )
Reversals, internal lateral and dorsal views. F, intranasal; K, pterygoid; P, circumcranial; Q, petrosal.

( 2 5 6 ) Craniofacial bone growth
Reversals, external lateral views. A, malar; B, nasomaxillary; C, nasal spine; E, lacrimal (intraorbital); K, pterygoid; L, lateral mandibular; M,
mental; N, medial mandibular; O, anterior ramus; Z, zygomatic.

Reversals
THE NASOMAXILLARY REVERSAL. This line extends obliquely forward from the approximate midpoint of the inferior orbital margin to a point just superior to the junction of the lateral nasal wall with the premaxilla. It separates a broad, inferolateral zone of surface resorption (with endosteal cortical bone formation) from the external zone of surface deposition on the nasal wall. The nasomaxillary reversal line provides a pivot between the forward and laterally growing nasal region and the regressive malar and premaxillary areas. Surface resorption in the malar region is associated with its posterior manner of cortical drift, and surface resorption in the anterior part of the maxillary arch is related primarily to its downward course of growth movement.
THE MALAR REVERSAL. This long line extends vertically from the alveolar margin of the maxillary arch at about the second premolar or first molar along a ridge to the malar protuberance. It then crosses the zygomaticomaxillary suture and continues directly upward over the lateral surface of the zygomatic bone and extends vertically along the frontal process of the zygomatic bone. It terminates near the zygomaticofrontal suture on the lateral crest of the orbital margin. In the region of the maxillary arch, this reversal functions as the pivot between the downward-growing endosteal cortex in the anterior part of the arch, and the downward-growing periosteal cortex in the posterior portion. A marked change in contour and surface orientation occurs along the plane of this reversal. In the malar region, it is a pivotal line between the backward-moving anterior face of the cheekbone and the laterally drifting zygomatic arch. On the lateral orbital rim, the malar reversal line is concerned with the backward rotation of the vertical frontal process of the zygomatic bone. This maintains its position between the divergent movements
( 2 5 7 )
of the forward-growing forehead and the backward-growing malar region.
The malar reversal line thus crosses three essentially separate areas, each concerned with a different growth situation. The line itself, however, is continuous.
THE ZYGOMATIC REVERSAL. The entire
medial side of the zygomatic arch within the temporal fossa has a resorptive periosteal surface. The reversal line occurs along the margin of the superior, inferior, anterior, and posterior portions of the zygomatic bar, including both its temporal and zygomatic components. It functions in the lateral drift of the whole zygomatic arch.
THE INTRAORBITAL REVERSALS. Three separate reversal lines are present within the orbital cavity. The lateral intraorbital line extends vertically from the lateral floor of the orbit to the cortical lining of the lateral orbital wall and then into the fossa of the domed roof beneath the supraorbital ridge. It is concerned with the lateral and posterior movement of the anterolateral portion of the orbit and the forward growth of the region deep to the overhanging ridge. A posterior intraorbital reversal is present on the inferior aspect of the posterolateral wall of the sphenoid bone. It contributes to the lateral shift of this area to make way for the laterally moving orbital floor. The third intraorbital line—the lacrimal reversal—separates the approximate lower half of the small lacrimal bone from the upper half. It functions in adjustment changes associated with differential growth processes in the four major orbital areas surrounding it.
THE CIRCUMNASAL REVERSALS. With a few localized exceptions, the surface of the cortical lining in the entire nasal chamber is characteristically resorptive in nature. The re-

( 2 5 8 )
versal lines encircle the edge along the upper portion of the anterior nasal aperture and the margin of the entire posterior choana. Both the anterior and the posterior circumnasal reversal lines function in the outward expansion of the whole nasal cavity by a process of direct cortical drift.
THE PTERYGOID REVERSALS. The anterior
(external) face of the pterygoid trough shows variable reversal patterns. In general, they are concerned with the downward and lateral movements of the pterygoid laminae as well as positional adjustments during growth between the adjacent maxillary tuberosity and the anterior surfaces of the pterygoid bone.
THE CIRCUMCRANIAL REVERSAL. This prominent reversal line encircles the entire cranium on the meningeal side. Beginning at the posterior rim of the foramen magnum, it runs posteriorly along the base of the midline sagittal ridge of the occipital bone and then arcs obliquely across the cortical lining of the posterior cranial fossa. It crosses the occipitoparietal suture and continues forward on the endocranial surface of the parietal bone just superiorly to the junction with the squamous portion of the temporal bone. The line then intersects the frontoparietal suture and extends circumferentially around the inner side of the forehead. It curves sharply downward to run along the base of the midline sagittal ridge on the floor of the anterior cranial fossa. The line then continues onto the crista where it terminates at the posterior aspect of the ethmoid.
This reversal, which is the longest single, uninterrupted line in the skull, represents the key pivot between the fundamentally different growth mechanisms that occur in the skull roof and the cranial floor. Contrasting rates of growth, the factor of contour expansion in the confined endocranial fossae, and variable com-
Craniofacial bone growth
binations of sutural growth and cortical drift are all directly involved. The primary growth process superior to this reversal line is sutural expansion. The basic growth process below the line is direct cortical drift with a decreasing gradient of sutural growth as the cranial base is approached.
THE PETROSAL REVERSAL. Unlike the
greater part of the cranial floor in general, the protruding petrous portion of the temporal bone has a depository type of meningeal surface. The reversal line encircles its base and functions as the pivot among the outwardly drifting surfaces of the middle cerebral fossa, the posterior fossa, and the cranial base. It provides the periosteal reversal that produces the elevated endocranial housing for the auditory mechanism. The petrosal prominence occupies a large recess in this region of the brain, and it serves as a partition that separates the middle from the posterior cranial fossae.
THE SPHENOIDAL REVERSAL. A characteristic endocranial reversal occurs on the body of the sphenoid bone at its junction with the middle cranial fossa. The elevation produced by this periosteal reversal provides the bony prominence that occupies a recess in this region of the brain, and it contributes to the com-partmentation of the cranial floor. It also functions in the positioning of the sella in relation to the diencephalon and the hypophysis.
THE CIRCUMSPINAL REVERSAL. A perios
teal-endosteal reversal occurs at the rim of the foramen magnum. It is associated with the outward manner of drift that functions to enlarge this region of the cranium. Cortical drift is a selective growth mechanism that maintains the critical positioning of all the foramina in the cranial base relative to each other and to the brain during growth.

Reversals
MEDIAL MANDIBULAR REVERSALS. These reversal lines are associated with the broad, elongate zone of surface resorption and endosteal bone formation that begins on the lingual side of the condylar neck. It extends obliquely forward and downward across the ramus and continues directly onto the body just below the medially projecting lingual tuberosity. This resorptive zone then runs forward, decreasing in size, until it terminates just posterior to the genial region. Although the medial mandibular reversals produce a single continuous zone that extends nearly the entire length of the mandible on the lingual side, the relationships and basic growth functions successively change as the zone covers the regional parts of the neck, upper ramus, lower ramus, lingual fossa, and medial mandibular body. In general, this resorptive zone is concerned with the direct sequential remodeling conversion of each part into the next as continued posterior growth brings about a succession of regional relocations.
THE LATERAL MANDIBULAR REVERSAL.
This well-marked line extends from the posterior condylar neck obliquely downward across the buccal side of the ramus. It terminates at the junction of the ramus with the superior surface of the mandibular body. Note that this line coincides in approximate placement with the contralateral medial reversal line on the opposite, lingual side of the ramus. Contrasting patterns of resorption and deposition are present on these opposing sides. This is associated with the drifting of both the labial and lingual cortices together, as a unit, in their various regional directions. On the buccal side, the reversal is concerned with a growth pivot between the metaphyseal remodeling of the neck and the multidirectional growth movements of the sigmoid notch and the coronoid process. Below the line, generalized periosteal
( 2 5 9 )
depository growth occurs over the remainder of the buccal side of the ramus.
ANTERIOR REVERSAL OF THE RAMUS. A
vertical line of reversal extends from the superior crest of the coronoid process on the lingual side down the anterior face of the ramus to the body. It is concerned with the posterior drift of the entire ramus, and, where it merges with the mandibular body on the medial and lateral sides, it functions in the direct remodeling conversion of the upright ramus into the horizontal body.
THE ANTEGONIAL REVERSAL. This line delineates a restricted segment of endosteal bone just anterior to the gonial region. It is a direct extension from the medial resorptive area of the ramus onto the inferior border of the posterior body. This endosteal area functions in the remodeling conversion of the antegonial region into the lengthening body during relocation of the former into the latter.
THE MENTAL REVERSAL. The mental protuberance and the alveolar region just above it undergo contrasting directions of growth, and the mental line of reversal represents the pivot between them. The placement of this line is variable among different individuals.
OTHER REGIONAL REVERSALS. Throughout the remainder of the skull, a series of localized reversals occur that are concerned with relatively restricted remodeling changes. These are summarized below.
A reversal line is often present at the base of the projecting nasal spine on its inferior side. It is related to the downward drift of this small bony process.
Variable spot reversals may occur on ex-

( 2 6 0 )
terna] cortical surfaces in the premaxillary region. They appear to be associated with transient adjustments involved in local tooth movements.
Intranasal reversals are present at the attachments of the conchae within the nasal cavity. These thin plates have lateral depository and medial resorptive surfaces comparable to the lateral nasal wall itself. The reversal occurs at the basal line where the depository side of each plate joins the resorptive cortical lining of the nasal wall.
Small, variable external nasal reversals may occur at the tip of the separate, paired nasal bones. They produce a slight depression at the anterior edge of the bony nose. Other variable
Craniofacial hone growth
reversals can result in a depression of the nasal bridge.
A constant reversal is seen surrounding the sizable jugular fossa. Within the fossa, the surface of the cortex is typically endosteal. At its rim, the bone abruptly becomes periosteal in type on the external surface of the enclosing occipital and temporal bones. The resorptive nature of the surface within the fossa serves to circumferentially enlarge its dimensions.
The auditory reversal occurs within the auditory canal of the temporal bone and separates the resorptive anterior part of the cortical lining from the depository posterior portion. This remodeling pattern produces an anterior growth movement of the entire auditory canal.

W. Stuart Hunter*
(12)
Elementary principles
of cephalometrics
This chapter is an introduction to cephalometrics for those unfamiliar with the subject, and it has been included to complement the basically anatomic considerations of growth found in this volume. The purpose is to provide a brief description of the various applications of cephalometrics as basic procedures utilized in studies of craniofacial growth.
A cephalogram is a radiograph of the head in which the position of the head relative to the source of the x-rays and to the film has been standardized. The degree of standardization expected and obtained in lateral cephalo-grams is such that differences between landmarks on films taken for the same subject within a few days of one another will be less than one-half millimeter. The cephalogram
* Department of Orthodontics and Center for Human Growth and Development, University of Michigan, Ann Arbor.
therefore provides a precise method of studying growth using the same individual over a number of years. Its principal use has been for the study of human growth, although the technique is also adaptable to primate and small animal studies. The standardization is usually accomplished by positioning the subject in a head holder by means of rounded rods inserted partially into the external auditory meati (poria).
The equipment is designed so that the central ray of the source of x-rays coincides with the axis of the ear rods for the lateral projection. The midsagittal plane of the head is almost always 60 inches from this source. The distance of the film from the subject's mid-sagittal plane is frequently held constant at approximately 18 cm. Whether the face is tilted high or low makes no difference in the accuracy of the result in lateral cephalograms
261


Elementary cephalometrics
because the central ray and porion (ear rod) axis always coincide.
However, for the other three projections frequently used—i.e., the posteroanterior and the left and right oblique (or 45° views)—the cant of the head is of primary importance. The distortions created by slight departures from a standard position make the measurement of vertical distances most unreliable in posteroanterior radiographs (see Figure 118) and the measurement of any dimension hazardous in the oblique projection. On the other hand, width dimensions do not appear to be greatly affected by tipping of the head in the posteroanterior projection. Within a range of 10 degrees either way from Frankfort plane, the error in width measurements because of such tipping is less than one per cent of the distance measured. Since such problems do not arise in the lateral projection, its use has become increasingly popular since the inception of cephalometrics around 1920.
In all cases there is a basic enlargement of the projected structures because the x-rays diverge from a point source. Furthermore, the structures closest to the film are enlarged less than the structures farthest from the film. Although there is evidence that most facial bones are slightly larger on the right side (T . L. Woo, 1931), the amount of this excess is so small that symmetry may be assumed. Therefore, the midpoint between bilateral landmarks is used as the projection of both sides to the sagittal plane.
( 2 6 3 )
Technology
Technologically, two distinguishable methods exist for obtaining the previously mentioned standardization. The first embraces the Broadbent-Bolton technique, which utilizes two x-ray sources and two film holders (Broad-bent, 1931) so that the subject need not be moved to obtain both a lateral and a posteroanterior film. Because no movement of the subject occurs between exposures of the lateral and posteroanterior films, one may study them side by side in three dimensions with the help of a Wylie compensator as described by Woods (1950). This is clearly worthwhile. However, because two x-ray tubes are required, standard low-voltage equipment has usually been employed because of cost. The advantages of high-voltage x-ray tubes for cephalometrics are discussed below. The Broadbent-Bolton method also precludes obtaining oblique projections.
The second technique involves the use of one x-ray source and film holder and a head holder capable of rotation for at least the lateral and posteroanterior and, usually, the oblique projections. This equipment frequently utilizes a high-voltage rotating anode source resulting in good delineation of both hard and soft structures. The reasons why high-voltage equipment produces better x-rays are complex and beyond the scope of this presentation. The rotating anode permits the use of a smaller focal spot or source than does a fixed anode, resulting in less of a "penumbra" effect and there-
The top half of this figure shows the tilt of the head, which corresponds with the posteroanterior tracings shown in the bottom half of the figure.
Figure 118
Width dimensions are not significantly altered by such tilting, while height dimensions obviously are changed.

( 2 6 4 )
fore sharper shadows. Occasionally, a Potter-Bucky grid between subject and film is also used to produce sharper images. The grid resembles a Venetian blind which permits only rays coming from the source to pass through it. It thus absorbs radiation deflected by the bones, which is not traveling in straight lines from the point source. Such secondary rays tend to give the cephalogram a slightly fuzzy appearance. Moreover, the entire grid is moved mechanically during exposure, so that the image of its "leaves" is not left on the film.
However, the process of turning the subject 90 degrees, which is inherent in this second technique, tends to alter the position of the head in the head holder, thus limiting to some extent the three-dimensional interpretation. Attempts to combine the two approaches by fixing the head holder and chair together and rotating both have so far proved unproductive.
In both technologies, the use of intensifying screens has an impact on the quality of the ensuing film. They are used to reduce the exposure time significantly. Because growth studies involve human subjects, reduction of radiation exposure is very important. In essence, the screens glow when struck by x-rays, thus exposing the film by light. Because x-ray film is coated on both sides, two screens are used. However, the screens that glow the most (high speed) are coarse grained, as compared with "slower" screens, and thus result in a reduction of definition as compared with slower screens. A compromise is necessary, and a screen that results in standard exposure times of from one-fourth second to one second per film, depending upon subject age and size, has been found to be satisfactory. For a more complete discussion of these aspects of cephalometry see Krog-man and Sassouni (1957) and Salzmann (1961).
It should be noted that neither technologic approach has, until recently, involved a con-
Craniofacial bone growth
sistent effort to standardize the midsagittal plane to film distance for all subjects. This has tended to limit consideration of the relationships in the head to angular measures, thus avoiding the enlargement problem.
As a rule, in medical and dental radiography the radiograph is interpreted directly. In cephalometric radiography, on the other hand, it is usually a tracing of the radiograph that is interpreted. This procedure, apparently introduced by Broadbent in 1931, permits the super-imposition of the outlines of the bones at successive ages for a visual study of growth. Of course, it also introduces a source of error, which is usually evaluated and controlled by repeating the tracings or a sample of the tracings.
Landmarks used are discussed in detail below (page 277) and consist of two types: (1) anatomic landmarks such as nasion, which have been carried over from craniometry, and (2 ) derived landmarks such as sella, which are peculiar to the cephalogram.
Total error and enlargement
Total error of measurement may be evaluated by comparing measures from tracings of two successive films taken a day or so apart on the same subjects. To obtain an appropriate estimate of this error, the double films and measurements should be for a sample of approximately the same size as the size of the samples being compared in the main part of the study. However, because of the difficulty in obtaining double sets of films, the same films are usually traced and measured twice, and the average difference (and its variance), called the error of tracing, is accepted as accounting for most of the error involved.
Enlargement due to the divergence of the x-rays from the point source when the source

Elementary cephalometrics
to the sagittal plane is 60 inches and the sagittal plane to the film distance is about 18 cm, is about 10 per cent. When the sagittal plane to film distance is different for each subject, the analysis of dimensions must be preceded by correction for enlargement, because it will be different for each film. If the sagittal plane to film distance is constant, the correction may be done on averaged values. Thus, if an uncorrected group difference in mandibular length is 3.7 mm, the corrected difference would be 3.3 mm. Clinically, this 0.4 mm difference could be significant, and correction should always be made for the purpose of comparability with other studies.
The use of cephalograms
Two principle lines of endeavor have developed in the use of cephalograms. They are not related to the technology, but to craniometry and to orthodontic practice. The cranio-metric approach is typified by a wealth of studies in which almost everything that the investigator can measure is measured in the hope that some further understanding of craniofacial growth will ensue. Because the cephalo-metric technology permits precise measurement of the same subject through time, much useful growth data has resulted. Such studies are called serial or longitudinal studies. Thus, serial cephalograms consist of a series of radiographs taken on the same individual over a period of time, often at yearly intervals. An alternative method of studying growth is called cross sectional. In the cross-sectional method, different subjects are used at each age level, and the size differences between age groups are assumed to be the result of growth. If it is the average amount of growth for a given period that is of interest, either method is satisfactory. Indeed, the need for serial data for
( 2 6 5 )
such studies may be questioned. Moreover, it is very difficult to obtain data annually on large groups of the same children because of the geographic mobility of most populations today. On the other hand, studies of the rate of growth require serial data if the rate is not to be seriously underestimated because all children do not grow at the same rate at the same times. For example, the pubertal growth-rate increase occurs a year or so earlier in girls than in boys and earlier in some girls than in others. Thus, at a given age—for example, 11 years—the average rate of growth values for the early growers will be reduced by the lower growth-rate values of the late growers. A year or so later, the reverse situation will occur, and again the actual growth rate will be underestimated. Obviously, chronologic age is an unsatisfactory reference scale for growth-rate studies, and a satisfactory substitute remains to be established. Other types of craniometric studies include speech studies and genetic studies using twins, siblings, and families.
The second line of endeavor, typified by its relationship to clinical orthodontic practice, has had as its goal the establishment of a series of standard scores, such as one finds for a battery of psychologic tests. Carefully selected and/or large samples have been scored for these "tests" so that average values with their dispersions are available for various angles, measures, and proportions. The simplest example of this usage is that of the Tweed triangle (1954), in which a face is given three "tests." That is, three angles are measured and compared with the standard scores established by Tweed for the three angles. As in psychologic tests, the scores are frequently related in some fashion so that a low score (relative to the norm) on one measure may lead one to expect a high score on another related measure for the same individual.
The complex tables of values usually found

( 2 6 6 ) Craniofacial bone growth
Figure 119 Lateral cephalogram of a 9-year-old girl with
a severe malocclusion.

Elementary cephalometrics ( 2 6 7 )
Figure 120
Posteroanterior cephalogram of the same girl as shown in Figure 119.

( 2 6 8 )
in papers dealing with this aspect of cephalo-metrics are simply summaries of scores obtained for a bewildering variety of tests.
Among the most widely known battery of scores is that devised by W. B. Downs (1948) for clinical evaluation of lateral cephalograms. Downs selected twenty subjects from twelve to seventeen years of age with normal occlusion and good faces and computed their scores for nine angular and one metric measure.
The preponderance of angular values in such batteries of tests or analyses is a result of the fact that faces vary greatly in size and of course enlarge during growth, thereby making linear standards cumbersome for clinical use where simplicity is important.
Furthermore, because growing faces change in proportion as well as size, the effect of proportional change can be minimized by careful selection of angles used. Thus, several analyses utilize the angular relationship of the incisors to the facial plane or some variation of it. The population variance of this relationship far exceeds the change effected during growth so that, for practical purpose, a useful value can be established.
The utility for the orthodontist of such scores lies in the diagnostic and treatment areas. With respect to diagnosis, the divergence of a patient's score for a given measure from the norm indicates the severity of the problem. For treatment, those measures having to do with the teeth indicate in what direction and how far treatment might proceed. However, consideration of craniometric studies emphasizes human variability so that what is acceptable for one individual is seldom acceptable for another.
In order to use cephalograms the investigator must have some understanding of what can and cannot be seen in the cephalogram of a living subject. The following pages are an introduction to structure identification in the lateral and posteroanterior cephalograms. (A
Craniofacial bone growth
more detailed description of the bony structures will be found in Etter's Atlas of Roentgen Anatomy of the Skull and in Krogman and Sassouni's Syllabus in Roentgenographic Cephalometry.) Because posteroanterior cephalograms provide the width dimension of the three-dimensional structures of the face, each section includes both lateral and posteroanterior drawings. As the oblique projections have quite specialized uses, they are not included in subsequent discussions.
It is recommended that cephalograms be traced rather than marked directly. Frosted acetate .003-inch thick (obtainable at most drafting supply outlets) is quite satisfactory. It should be taped securely to the film. A 4H pencil is recommended, although many find this a trifle hard. If a softer pencil is used, it must be sharpened frequently because a line more than 0.2 mm. in width will increase the error factor. The film is traced on a backlighted glass or plastic surface. The light box or table should have a well-diffused light source (opal glass is far superior to frosted glass), the intensity of which can be altered if desired, and it should be used in a darkened room.
Without question, the tracing of a cephalogram is an art. It is a highly stylized art form, because only a few of the myriad of lines seen in the cephalogram are routinely traced. For example, in the posteroanterior cephalogram a diagonal line always crosses each orbit from its upper, outer curvature to the central region of the inferior rim. This is the outer surface of the greater wing of the sphenoid. Because these lines are always present and clearly seen, it is tempting to trace them, but until they can be shown to have some utility, there is no need to include them.
It should be noted that when tracing such structures as the lower border of the mandible, the line should be drawn over the black side of the junction between black and light gray,

Elementary cephalometrics
because it is this surface of the bone that is to be represented.
It should also be emphasized that success in tracing depends largely upon knowing what to look for and where to look. The tracing of the base of the skull from sella turcica to foramen magnum and then forward to the greater wings of the sphenoid is an example. Many times the anterior outline of the foramen magnum cannot be seen readily, but it is at the apex of the two sides of a backward-pointing triangle consisting of the sphenoid and occipital bones, which is one clue. Furthermore, the anterior tip of the foramen magnum is just posterior to the anterior outlines of the occipital condyles. These are readily seen until about age fourteen when the mastoid processes begin to obscure them. Lastly, the odontoid process of the axis frequently points toward the anterior rim of the foramen magnum and is usually no more
( 2 6 9 )
than 10 or 15 mm from it. Thus, by indirection, the anterior rim of the foramen magnum, called Basion, may almost always be established by knowing what to look for and where to look.
Because soft tissue structures occasionally overlie bony outlines, it is well to keep their existence in mind. They are ordinarily traced only when the investigator has a special purpose in so doing. Thus, for the orthodontist the soft tissue profile is important and, occasionally, the tongue and soft palate as well. For the speech pathologist the soft palate and nasal pharynx are significant, particularly when the cephalogram is made during the production of specific speech sounds.
Figures 119 and 120, which are lateral and posteroanterior cephalograms of a 10-year-old child, should be compared with their respective soft tissue drawings (Fig. 121). Because
Left, tracing of soft tissue structures seen in the lateral projection. A, cheek outlines; B, soft palate;
C, tongue; D, tonsil. Right, tracing of soft tissue structures seen in the posteroanterior projection.
Figure 121

( 2 7 0 ) Craniofacial hone growth
Figure 122
Lateral cephalogram of the skull of a child approximately 9 years of age.

Elementary cephalometrics ( 2 7 1 )
Figure 123
Posteroanterior cephalogram of the same skull shown in Figure 122.

( 2 7 2 )
the delineation of soft tissue depends greatly upon exposure factors, all the structures shown are not always seen. The investigator should be aware that the outlines of the cheeks frequently superimpose directly over the alveolar bone covering the maxillary incisors. The cheek outlines are convex while the bony outline at this point should be concave. The alar cartilages of the nose also should not be confused with the anterior nasal spine when these structures are superimposed.
Figures 122 and 123 are of a skull of a child approximately nine years of age, and it may be seen that none of the outlines in Figure 121 exist in these figures.
Craniofacial bone growth
Figure 124 represents standard tracings of the skull shown in the preceding figures. Because these are rather complex, each bone or pair of bones that contributes in a major way to the outlines seen will be dealt with separately with particular emphasis on visible sutures.
Figure 125 is a lateral cephalogram of the same skull with markers along the sagittal plane of the cranial base. Lead shot were placed at the suture sites. This figure also shows the method that was subsequently used to delineate each bone. All accessible surfaces of the zygomatic bones were covered with thin lead foil so that these bones stand out from the
Figure 124
Left, tracing of the lateral skull cephalogram shown in Figure 122. Right, tracing of the postero-anterior skull cephalogram shown in Figure 123.

Elementary cephalometrics ( 2 7 3 )
Figure 126
Tracing of the sagittal plane structures of the skull cephalogram shown in Figure 125. A, spheno-occipital synchondrosis; B, sphenoethmoid synchondrosis; C, cribriform plate; D, foramen caecum. The broken lines are not often seen radiographically.
Lateral cephalogram of a skull on which markers have been placed along the sagittal plane of the occipital, sphenoid, ethmoid, and frontal
bones (see also Figure 126). T h e accessible surfaces of the zygomatic bones were covered with thin lead foil.
Figure 125

( 2 7 4 )
rest of the face when radiographed. Left and right sides are superimposed but slightly offset. Because one is working only in two dimensions it is the convention to average outlines to the sagittal plane, it does not matter which is left or right.
Figure 126 is a tracing of Figure 125 with some additional outlines showing the approximate extent of the ethmoid bone and the nasal bone as seen in the lateral cephalogram. The ethmoid outlines are broken lines, because only the cribriform plate is routinely seen in the lateral projection.
TEMPORAL BONES. Figure 127 is included because of the contribution of the petrous part of the temporal to the posteroanterior cephalogram. In the posteroanterior projection the most superior outline of this bone is superimposed on the medial portion of the floor of the orbit (see Figure 130) and should not be confused with it.
SPHENOID. Figure 128 shows what is seen of the sphenoid. Note in the lateral view the asymmetry of the curvatures depicting the greater wings in this skull; this asymmetry is frequently less. The pterygoid plates are not always seen because they are covered by the rami of the mandible and superimpose on the soft palate outline. Therefore, they are indicated by broken lines. The posteroanterior tracing emphasizes the fact that the lesser wings of the sphenoid with their characteristic shape are usually seen in this projection, as is the floor of the hypophyseal fossa. Note also how the greater wings, which constitute the medial anterior portion of the floor of the middle cranial fossa, coincide with the inferior rim of the orbits when the Frankfort plane is perpendicular to the film. Because neither outline is at all clear in most posteroanterior cephalo-grams, this line is of doubtful utility.
Craniofacial bone growth
ZYGOMA. Figure 129 shows the bilateral zygomatic bones. Probably the most important structures here are the frontozygomatic sutures. In the lateral view they lie over the ethmoid air cells, which are glomerular in shape, whereas the sutures are jagged and extend only for the width of the processes. In the posteroanterior view these sutures are seen best under reduced or changing illumination.
MAXILLA. The maxillary structures are shown in Figure 130. Again, the frontomaxil-lary sutures are of great interest. In the lateral projection they generally lie in a plane somewhat inferior to the level of the zygomaticotemporal sutures and descend posteriorly from the frontonasal suture. They are jagged, dark lines usually found on a fairly uniform, light gray ground.
The anterior surfaces of the pterygomax-illary fissures—upside-down, teardrop-shaped areas of radiolucency—are taken as the posterior surfaces of the maxilla.
The teeth of left and right sides seldom superimpose exactly. Therefore, if specific dental landmarks are to be located, the teeth must be traced individually. If they are offset antero-posteriorly (Fig. 130) it is best to begin with the most posterior molar and work forward, accounting for each tooth on that side in turn. The use of a different colored pencil for the teeth of the opposite side is helpful. Identification of sides is not necessary because they will be averaged upon accounting for the same number of teeth on the opposite side. The same principles are followed when the teeth are offset vertically. Tracing the teeth is, without doubt, the most difficult of all tracing procedures and requires a good knowledge of dental morphology for accurate results. Numerous dental fillings may render the task almost impossible. As regards the incisors, the established convention is that only the most anteriorly

Elementary cephalometrics
placed incisor is traced. For evenly aligned incisors this is satisfactory, but when severe crowding is encountered the result is sometimes rather odd.
( 2 7 5 )
With respect to the posteroanterior projection, it may be observed that the anterior alveolar outline must usually be obtained by indirection, by assuming that it lies approximately
The temporal bone. Lateral (left) and posteroanterior (right) projections showing: A, petrous
portion; B, mastoid part. The squamous part is not shown because it is seldom seen clearly.
The sphenoid. Left, lateral projection showing: A, anterior clinoids (lesser wings); B, greater wings; C, pterygoid processes. Right, posteroanterior projection showing: A, lesser wings; B, greater wings; D, dorsum sella; E, floor of hy
pophyseal fossa; F, sphenooccipital synchondrosis. Note how the greater wing, which at G is the floor of the middle cranial fossa, coincides with the orbital outline.

( 2 7 6 )
at the cementoenamel junction of the incisors. Also, it should be remembered that in this projection the frontomaxillary sutures lie over the ethmoid air cells so that a jagged
Craniofacial bone growth
dark line is sought amidst a sort of bubbly mass. The teeth are as difficult to sort out in this projection as in the lateral projection, and the same principles should be applied
The zygoma. Left, lateral projection showing: A, zygomaticofrontal suture; B, zygomaticotemporal suture. Right, posteroanterior projection
showing: C, inferior surface of occipital; D, occipital condyles.
The maxilla. Left, lateral projection showing: A, frontomaxillary sutures; B, pterygomaxillary fissure. Right, posteroanterior projection showing:
A, frontomaxillary sutures; C, palatal surface; D, alveolar process.

Elementary cephalometrics
if arch asymmetries, for example, are to be studied.
MANDIBLE. The mandible, shown in Figure 131, requires little comment. The coronoid processes are not readily seen in either projection. In the lateral projection, tracing of the teeth is accomplished in identical fashion as has been described for the maxilla and only the most anterior incisor is traced. The root of the mandibular incisor is seldom seen, because at least three other tooth roots overlie the same location in the film. A stylized approach is therefore adopted, and the root is put where it should be, given the crown outline as it exists. Because the morphology of the mandibular incisors shows very little variation, this rather cavalier approach to a precise matter gives results within quite acceptable limits, as a rule.
Landmarks
The definitive work on landmarks, written by Krogman and Sassouni (1957), has been
( 2 7 7 )
published only in mimeographed binder form and is not widely available. Nevertheless, the interested reader is referred to it, because the following summary of the major landmarks is not meant to provide a comprehensive listing but rather a working beginning (see also Yen, 1960).
For convenience of discussion, landmarks may be divided into two categories: anatomic and derived. Anatomic landmarks are defined as those which have a real anatomic existence in or on the skull. For the purposes of this discussion, derived landmarks are defined as those peculiar to the cephalogram. The following are "anatomic" landmarks as seen in the lateral projection (see Figure 132a).
Nasion (Na). The junction of the frontonasal suture at the most posterior point on the curve at the bridge of the nose. The following are descriptions of several variations that are found cephalometrically:
1. The suture can be seen and is at the deepest part of the curve. Nasion appears as defined above.
The mandible. Left, lateral projection. Right, posteroanterior projection showing coronoid process (A).

( 278 ) Craniofacial bone growth
Landmarks and planes. A, anatomic landmarks; B, derived landmarks; C, posteroanterior land
marks; D, lines and planes. See text for explanation of letters.

Elementary cephalometrics
2. The suture can be seen but is above or below the deepest part of the curve. Nasion is at the suture-surface junction.
3. The suture can be seen but steps up just before joining the surface outline. Nasion is where the suture meets the surface outline.
4. The suture cannot be seen. In the absence of previous or succeeding films from which the point may be transferred, the most posterior point on the curve is taken as nasion.
Orbitale (Or). A bilateral landmark. When the outlines of the orbital rim can be visualized, the lowest point on the averaged rim outline is taken.
Anterior Nasal Spine (ANS). The most anterior point on the maxilla at the level of the palate. Although quite precise for vertical measures, this point should not be used for posteroanterior measurements because the point of convergence cannot, by its nature, be precise.
Subspinale (A point). The most posterior point on the curve between ANS and Pr (see below), usually determined by a tangent to this curve from Na. Remember the possibility of superimposition of the cheek contours. When a clear outline is not seen, this point should be located about 2 mm anterior to the apical portion of the incisor roots. Although reasonably precise for posteroanterior measures, A point should not be used for vertical measures because the angle of convergence of the tangent to the bony curve is acute, and therefore a discrete point does not result.
Prosthion (Pr). The most anterior, inferior point on the maxilla, usually at the cemento-enamel junction of the incisors.
Incision superius (Is). The incisal tip of the most anterior maxillary incisor.
Incision inferius (li). The incisal tip of the most anterior mandibular incisor.
Infradentale (Id). The most anterior, su-
( 2 7 9 )
perior point on the mandible at the cemento-enamel junction of the incisors.
Supramentale (B point). The point most posterior to a line from Id to Pog (see below) on the anterior surface of the symphyseal outline of the mandible. B point should lie over the apical third of the incisor roots. Frequently, it is determined by a tangent to this concave curve, from Na. When there is no curve, or the curve is convex, a point over the apical third of the roots is chosen with the help of preceding or succeeding films for the same subject, if available, because convexity is occasionally caused by erupting teeth.
Pogonion (Pog). The most anterior point on the contour of the chin, frequently determined by a tangent to the chin from Na. Strictly speaking, it should be located by a tangent perpendicular to the mandibular plane. When the curve is convex, this point must be estimated.
Gnathion (Gn). Best defined by Krogman and Sassouni (1957, p. 71) as the midpoint between Pog and Me on the contour of the chin determined by geometry or measurement.
Menton (Me). The lowest point on the symphyseal outline best determined by using mandibular plane as a tangent to this curve.
Basion (Ba). The most inferior, posterior point at the sagittal plane on the anterior rim of foramen magnum. See preceding discussion (page 269) for methods of locating this landmark.
Posterior Nasal Spine (PNS). The most posterior point at the sagittal plane on the bony hard palate. Because it must usually be taken as the confluence of the posteriorly converging, inferior and superior surfaces of the palate, it should not be used for anteroposterior measures. However, it is reasonably reliable for vertical measures.
The following are "derived" landmarks found in the lateral projection (see Figure 1 3 2 b :

( 2 8 0 )
Sella (S ) . The center of the hypophyseal fossa, determined by inspection. Because this point is located in space, it might well be termed a spacemark. It is helpful to sketch in a curve from anterior to posterior clinoids, giving an egg-shaped or round outline to the hypophyseal fossa, to assist in choosing the center.
The following landmarks are all bilateral. When both sides are visible, the distance between the two landmarks should be halved.
Articulare (Ar). The intersection of the inferior surface of cranial base and the posterior surfaces of the condyles of the mandible. It is best used as a measure of the anteroposterior position of the mandible relative to cranial base because it shifts with the mandible. However, because of the difficulty experienced in accurately tracing the head of the condyle, it is also used as an approximation of the location of the posterior surfaces of the condyles.
Gonion (Go). Strictly speaking, this is an anatomic landmark at the most posterior, inferior point on the body-ramus junction of the mandible. However, because it is most readily determined by bisecting the angle formed by the intersection of the tangents to the posterior surfaces of the rami and condyles, and mandibular plane, it seems sensible to use it as a spacemark at the junction of the ramal and mandibular planes.
Pterygomaxillary fissure (PTM). A bilateral, upside-down, teardrop-shaped area of radio-lucency, the anterior surfaces of which are taken as the posterior surfaces of the maxilla. The point itself is usually taken at the most anterior, inferior confluence of the curvatures.
Key Ridge (KR). Defined by Krogman and Sassouni (1957) as the lowest point on the outline of the zygoma, usually found in the vicinity of the apices of the maxillary first permanent molars.
Porion (Po). Usually defined as the top of
Craniofacial hone growth
the ear rods and, therefore, strictly a derived landmark.
Bolton point (Bo) Introduced by Broad-bent (1931), it is defined as the highest point on the curvature of the base of the skull, just posterior to the occipital condyles. On the dry skull there is no problem in locating this point, but in the lateral cephalogram the multiplicity of contours in this area makes it most difficult to locate reliably.
To complete the discussion, some of the landmarks seen in the posteroanterior projection are outlined briefly. (Letters in parentheses correspond to those in Figure 132c.)
Midline structures Crista galli. A vertically elongated diamond
shape, used by Harvold (1951) to help establish the sagittal plane (A) .
The floor of the hypophyseal fossa (B) . The septal structures of the nose ( C ) .
Bilateral structures Frontozygomatic sutures. Seen as dark lines
on a gray background ( D ) . Zygomatic processes. The lateral surfaces
may usually be seen ( E ) . Mastoid processes ( F ) . Gonial areas of the mandible ( G ) . Foramen rotunda. In the medial inferior por
tion of the orbital outlines ( H ) .
Cephalometric planes
Although Krogman and Sassouni suggest that a plane must have at least three points, many two-point planes continue to be used. The most frequently utilized lines and planes include the following (Letters in parentheses correspond to those in Figure 132d):
Sella-nasion. Simply from sella to nasion (A) .

( 2 8 2 )
combination of surface apposition (and resorption) and movement of each bone relative to its adjacent bones is, at least, complex.
The work of Bjork (1966) with metallic implants (which are seen radiographically) in the facial bones of growing children is thus of great importance. These tiny tantalum implants are placed in the bones under local analgesia in sufficient numbers so that by triangulation and measurement, movement of the pins within a bone during growth, relative to them-
Craniofacial hone growth
selves, can be ruled out. It then becomes possible to differentiate between the movement or displacement of the bone itself (relative to other bones) from movement of the surfaces of the bone as a result of remodeling. Thus, the amount and rate of bony apposition along the posterior borders of the mandible, for example, may be determined with great precision.
The implant method should prove to be a very productive refinement of the cephalo-
The growth of the face from 6 to 16 years as shown by superimposed tracings of lateral cephalo-
grams. The two tracings were superimposed on the line from sella to nasion and registered at sella.

Elementary cephalometrics
metric technique for the differentiation of ap-positional and sutural growth. The method has, of course, been used in various forms on experimental animals as well as on humans for many years, and the combination of cephalometry, implants, and vital staining in experimental animals can be very productive.
It is unlikely, however, that this added technical precision will greatly alter the general concepts regarding growth origins of bones of the face and their overall changing relationships as described in this volume. As observed in the lateral cephalogram, the chin "grows" downward and forward out of its "facial pocket" more or less along a line from sella to gnathion (Fig. 133). On the average, the mandible tends to grow a bit more forward than the maxilla and cranial base so that the angle between facial plane and Frankfort plane or sella-nasion increases during growth. Males tend to grow more than females and chronologically about a year later. The rate of facial growth is known to decrease steadily from birth to about age 11 and then to increase to about age 13 and decrease again until growth is essentially completed.
Given no change both in direction of growth and a constant rate, one could easily predict growth. However, the direction of growth of each bone can and frequently does change, and the rate varies considerably, as mentioned before. As a result of this, the great goal of growth research today is growth prediction. The outstanding work in the area has been done by Ricketts (1960) who recognized the complexity of the task and broke his evaluation down into about eighteen steps estimating the direction and amount of growth of the bones of the face over a period of one or two years. Of these eighteen estimates, about ten were based upon known growth rates. The remainder were sensible compromises and/or desirable goals for the position of the teeth upon completion of orthodontic treatment.
( 2 8 3 )
The procedure works because (1 ) it takes almost all important factors into consideration, ( 2 ) it is done usually for a period not exceeding two years, and (3 ) the position of the teeth is under the control of the orthodontist. Thus, although one may qualify the method as partially dependent upon treatment procedures, presumably the prediction of untreated facial growth could be handled in similarly small increments.
Such work is usually based in part upon the wealth of studies in the published literature of which the meticulous work of Meredith and his associates (for example, Jones and Meredith, 1966) is representative. The direction of growth is most frequently studied by the analysis of angles and their change through time. The rate of growth is best determined by the measurement of distances (usually in millimeters). Such values may also be converted to proportions, although the correct interpretation of a proportion is sometimes not simple.
Studies of facial growth are frequently cross sectional because it is very difficult to obtain records every year for ten or more years on a reasonably large sample (i.e., fifty or more subjects equally divided as to sex). Often, mixed longitudinal, cross-sectional data are employed satisfactorily, and with the coming of age of vast computer-data storage capacities it is likely that extensive sharing and pooling of longitudinal data will ensue. In a survey done by Moorrees (1967) for the International Society of Cranio-Facial Biology, at least twenty-four such studies were found to exist around the world in various stages of completion. Again, although it is unlikely that the added security of growth studies based upon large longitudinal samples will greatly alter existing general concepts of facial growth, the details are of unquestioned importance in a structure as finely coordinated and meshed as the human face.


Bibliography


Altmann, F. (1965): The finer structure of the auditory ossicles in otosclerosis. Arch. Otolaryng, 82: 569-574.
Amprino, R. (1947): La structure du tissu osseux envisagee comme expression de differences dans la vitesse de l'accroissement. Arch. Biol. LVIII(4): 315-330.
(1948): A contribution to the functional meaning of the substitution of primary by secondary bone tissue. Acta anat. 5(3):291-300.
(1951): Relations entre la structure et la physiologie de l'os. Ann. Soc. Roy. Sci. Med. Natur. Brux. 4(6):209-225.
(1952): Rapporti fra processi di ricostru-zione e distribuzione dei minerali nelle ossa. I. Richerche eseguite col metodo di studio dell'as-sorbimento dei raggi roentgen. Zschr. Zellforsch. 37:144-183.
(1965): "Bone structures and functions." In Aus der Werkstatt der Anatomen, ed. by W. Bargmann, Stuttgart, Thieme V, pp. 1—16.
Amprino, R., and A. Bairati (1936): Processi di ricostruzione e di riassorbimento nella sostanza compatta delle ossa delPuomo. Zschr. Zellforsch. 24:439-511.
Amprino, R., and G. Godina (1947): La struttura delle ossa nei vertebrati. Comment. Pont. Acad. Sci. 11 ( 9 ) : 329-467.
Anderson, C. E. (1962): The structure and function of cartilage. J. Bone Joint Surg. 44-A(4): 777-786.
Anson, B. J., and T. H. Bast (1946): The development of the auditory ossicles and associated structures in man. Ann. Otol. 55(3):467-494.
(1959a): Development of the incus of the human ear. Illustrated in Atlas Series. Quart. Bull. Northwest. Univ. Med. Sch. 33(2):110-119.
(1959b): Development of the stapes of the human ear. Illustrated in Atlas Series. Quart. Bull. Northwest. Univ. Med. Sch. 33:44-59.
Anson, B. J., T. H. Bast, and S. F. Richany (1955a): The fetal and early postnatal development of the tympanic ring and related structures in man. Ann. Otol. 64(3) : 802-824.
(1955b): The fetal development of the tympanic ring, and related structures in man. Quart. Bull. Northwest. Univ. Med. Sch. 29(1): 21-37.
Anson, B. J., D. G. Harper, and J. R. Hanson (1962): Vascular anatomy of the auditory ossicles
287
Bibliography

( 2 8 8 )
and petrous part of the temporal bone in man. Ann. Otol. 71 ( 3 ) : 622-631.
Anson, B. J., D. G. Harper, and T. R. Winch (1964): Intra-osseous blood supply of the auditory ossicles in man. Ann. Otol. 73(3) : 645-659.
Avis, V. (1959): The relation of the temporal muscle to the form of the coronoid process. Am. ). Phys. Anthrop. 17:99-104.
Baber, W. E., and H. V. Meredith (1965): Childhood change in depth and height of the upper face, with special reference to Downs' A point. Am. J. Orthodont. 51 (12) : 913-927.
Baer, M. J. (1954): Patterns of growth of the skull as revealed by vital staining. Hum. Biol. 26:80-126.
Bang, S., and D. H. Enlow (1967): Postnatal growth of the rabbit mandible. Arch. Oral Biol. 12:993-998.
Baume, L. J. (1961): Principles of cephalofacial development revealed by experimental biology. Am. J. Orthodont. 47(12):881-901.
Behatia, H. L., and R. F. Sognnaes (1963): Tetracycline discoloration and labelling of teeth and bone. A review. /. South. Calif. Dental Ass. 31: 215.
Bernstein, S. A. (1933): Ober den normalen histo-logischen Aufbau des Schadeldaches. Z. Anat. Entwicklungs. 101:652-678.
Bevelander, G., G. Rolle, and S. Cohlan (1961): The effect of administration of tetracycline on the development of teeth. J. Dent. Res. 40:1020.
Birkby, W. H. (1966): An evaluation of race and sex identification from cranial measurements. Am. J. Phys. Anthrop. 24( l ) :21-28 .
Bjork, A. (1947): The face in profile. Svensk Tandlak T. 40:56.
(1950): Some biological aspects of prognathism and occlusion of the teeth. Acta odont. scand. 9:1-40.
(1955a): Cranial base development. Am. J. Orthodont. 41:198-225.
(1955b): Facial growth in man, studied with the aid of metallic implants. Acta odont. scand. 13.:9-34.
(1963): Variations in the growth pattern of the human mandible: longitudinal radiographic study by the implant method. J. Dent. Res. 42: 400-411.
(1964): Sutural growth of the upper face studied by the implant method. Europ. Orthodont. Soc. Rep. Congr. 40:49-65.
Bibliography
(1966): Sutural growth of the upper face studied by the implant method. Acta odont. scand. 24:109-127.
Bohatirchuk, F. (1966): Calciolysis as the initial stage of bone resorption. A stain historadiographic study. Am. ]. Med. 47(5):836-846.
Brash, J. C. (1924): The Growth of the Jaws and Palate. London, Dental Board of the United Kingdom, pp. 23-66.
(1926): The growth of the alveolar bone and its relation to the movements of the teeth, including eruption. Dent. Rec. XLVI(12) :641-664.
(1927): The growth of the alveolar bone and its relation to the movements of the teeth, including eruption. Dent. Rec. XLVII(1): 1-26.
(1934): Some problems in the growth and developmental mechanics of bone. Edinh. Med. J. 41:305-318, 363-387.
Broadbent, B. H. (1931): A new x-ray technique and its application to orthodontia. Angle Orthodont. 2:45-66.
(1937): The face of the normal child. Angle Orthodont. 7:183-208.
Brodie, A. G. (1934): Present status of knowledge concerning movement of the tooth germ through the jaw. J. Am. Dent. Ass. 27:1830-1838.
(1941a): Behavior of normal and abnormal facial growth patterns. Am. J. Orthodont. & Oral Surg. 27:633-647.
(1941b): On the growth pattern of the human head. Am. J. Anat. 68:209-262.
(1946): Facial patterns: a theme on variation. Angle Orthodont. 76(3,4):75-87.
(1948): The growth of the jaws and the eruption of the teeth. Oral Surg. 7:334-341.
(1953): Late growth changes in the human face. Angle Orthodont. 23(3) : 146-157.
(1955): The behavior of the cranial base and its components as revealed by serial cephalo-metric roentgenograms. Angle Orthodont. 25(3) : 148-160.
(1966): The apical base: zone of interaction between the intestinal and skeletal systems. Angle Orthodont. 36(2) : 136-151.
Brues, A. M. (1966): "Probable mutation effect" and the evolution of hominid teeth and jaws. Am. J. Phys. Anthrop. 25(2) : 169-170.
Charles, S. W. (1925): The temporomandibular joint and its influence on the growth of the mandible. J. Brit. Dental Ass. 46:845-855.

Bibliography
Cohen, J., and W. H. Harris (1958): The three-dimensional anatomy of Haversian systems. J. Bone Joint Surg. 40-A(2): 419-434.
Conklin, J. C, D. H. Enlow, and S. Bang (1965): Methods for the demonstration of lipid applied to compact bone. Stain Techn. 40(4) : 183-191.
Costa, O. A., and W. P. Covell (1965): Variations in the enchondral bone of the otic capsule. Laryngoscope LXXV(9): 1462-1476.
Currey, J. D. (1959): Differences in the tensile strength of bone of different histological types. J. Anat. 9 ( l ) : 87 -95 .
(1960): Differences in the blood-supply of bone of different histological types. Quart. J. Micr. Sci. 202(3):35l-370.
Dass, R., and S. S. Makhni (1966): Ossification of ear ossicles. The stapes. Arch. Otolaryng. 84:88-94.
Davenport, C. B. (1940): Postnatal development of the head. Proc. Am. Phil. Soc. 83:1-26.
De Beer, G. R. (1937): The Development of the Vertebrate Skull. London, Oxford.
Delattre, A., and R. Fenart (1960): h'hominisation du crane. Paris, Editions du Centre National de la Recherche Scientifique.
Dempster, W. T., and D. H. Enlow (1959a): Osteone organization and the demonstration of vascular canals in the compacta of the human mandible. Anat. Rec. 133(2):268.
(1959b): Patterns of vascular channels in the cortex of the human mandible. Anat. Rec. 135(3):189-205.
Diamond, M. (1946): Posterior growth of maxilla. Am. J. Orthodont. 32:359-364.
Dixon, A. D. (1953): The early development of the maxilla. Dent. Pract. 3:331-336.
Downs, W. B. (1948): Variation in facial relationships: their significance in treatment and prognosis. Am. J. Orthodont. 34:812-840.
DuBrul, E. L., and H. Sicher (1954): The adaptive chin." Springfield, 111., Thomas.
Duterloo, H. S. (1967): In vivo implantation of the mandibular condyle of the rat. Doctoral dissertation, University of Nijmegen, Nijmegen, The Netherlands.
Eccles, J. D. (1959): Studies on the development of the peridontal membrane: the principal fibers of the molar teeth. Dent. Pract. 10:31-35.
Enlow, D. H. (1954): A plastic seal method for mounting sections of ground bone. Stain Techn. 29( l ) :21-22 .
( 2 8 9 )
(1957): Significant difference in bone histologic structure among vertebrate groups. Anat. Rec. 127(2):463-464.
(1961a): Decalcification and staining of ground thin-sections of bone. Stain Techn. 36(4) : 250-251.
(1961b): Sequence of microscopic structural changes involved in the gross remodeling of bone. Anat. Rec. 239(2):226.
(1962a): A study of the post-natal growth and remodeling of bone. Am. J. Anat. 110(2): 79-101.
(1962b): Functions of the Haversian system. Am. J. Anat. 110(3):269-306.
(1962c): The functional significance of the secondary osteone. Anat. Rec. 142(2): 230.
(1963a): Osteophytosis following experimentally induced cortical necrosis in the femora of white rats. Anat. Rec. 145(2): 138.
(1963b): Principles of Bone Remodeling. Springfield, 111., Thomas.
(1965a): Direct medullary-to-periosteal transition and the occurrence of subperiosteal haematopoietic islands. Arch. Oral Biol. 10:545-546.
(1965b): Mesial drift as a function of growth. Symp. on Growth, Univ. of West Indies. W. Indian Med. J. 14(2): 124-125.
(1965c): The problem of muscle tension and the stimulation of bone growth. Anat. Rec. 25I(3) :451.
(1966a): A comparative study of facial growth in Homo and Macaca. Am. J. Phys. An-throp. 24(3):293-308.
(1966b): A morphogenetic analysis of facial growth. Am. J. Orthodont. 52(4):283-299.
(1966c): "An evaluation of the use of bone histology in forensic medicine and anthropology." In Studies on the Anatomy Function of Bone and Joints, ed. by F. G. Evans, Heidelberg, Springer, pp. 93-112.
(1966d): Osteocyte necrosis in normal bone. J. Dent. Res. 45(1):213.
Enlow, D. H., and S. Bang (1965): Growth and remodeling of the human maxilla. Am. J. Orthodont. 51(6):446-464.
Enlow, D. H., and S. O. Brown (1956): A comparative histological study of fossil and recent bone tissues. Part I. Introduction, methods, fish and amphibian bone tissues, bibliography. Tex. J. Sci. VIII(4):405-443.

( 2 9 0 )
(1957): A comparative histological study of fossil and recent bone tissues. Part II. Reptilian and bird bone tissues. Tex. J. Sci. IX(2) :186-214.
(1958): A comparative histological study of fossil and recent bone tissues. Part III. Mammalian bone tissues, general discussion. Tex. J. Sci. X(2) : 187-230.
Enlow, D. H., and J. L. Conklin (1964): A study of lipid distribution in compact bone. Anat. Rec. 248(2):279.
Enlow, D. H., J. L. Conklin, and S. Bang (1965): "Observations on the occurrence and the distribution of lipids in compact bone." In Clinical Orthopaedics (No. 38), ed. by A. F. De Palma, Philadelphia, Lippincott, pp. 157-169.
Enlow, D. H., and D. B. Harris (1964): A study of the postnatal growth of the human mandible. Am. Orthodont. 50( l ) :25-50 .
Enlow, D. H., and W. S. Hunter (1966): A differential analysis of sutural and remodeling growth in the human face. Am. J. Orthodont. 52(11): 823-830.
Etter, L. E. (1955): Atlas of Roentgen Anatomy of the Skull. Springfield, 111., Thomas.
Evans, F. G. (1957): Stress and Strain in Bones. Springfield, 111., Thomas.
Fawcett, E. (1924): "The development of the bones around the mouth." Five lectures on The Growth of the Jaws, Normal and Abnormal in Health and Disease. London, Dental Board of the United Kingdom, pp. 1-21.
Felts, W. J. L. (1959): Transplantation studies in skeletal organogenesis. I. The subcutaneously implanted immature long-bone of the rat and mouse. Am. J. Phys. Anthrop. 27:201-215.
Foote, J. S. (1916): A contribution to the comparative histology of the femur. Smithsonian Contr. 35:3.
Ford, E. H. R. (1958): Growth of the human cranial base. Am. J. Orthodont. 44:498-506.
Frost, H. M. (1960a): In vivo osteocyte death. J. Bone Joint Surg. 42-A(l) : 138-143.
(1960b): Micropetrosis.J. Bone Joint Surg. 42-A(l) : 144-150.
(1960c): Observations on fibrous and lamellar bone. Henry Ford Hosp. Med. Bull. 8 (2 ) : 199-207.
Gans, B. J., and B. G. Sarnat (1951): Sutural facial growth of the Macaca rhesus monkey: a gross and serial roentgenographic study by means
Bibliography
of metallic implants. Am. J. Orthodont. 37(11): 827-841.
Gebhardt, W. (1905): Ueber funktionell wichtige Anordnungsweisen der groberen und feineren Bauelemente des Wirbeltierknochens. 2. Spezieller Teil. Roux Arch. Entwicklungs.-Mech. 20:187-322.
Godard, H. (1957: Les zones de croissance de la mandible. Assoc. Anat. Comptes Rendus 43:357-364.
Goldman, H. M. (1957): Histologic structure of the attachment apparatus. Alpha Omegan 25:102.
Goldstein, M. (1936): Changes in dimensions and form of the face and head with age. Am. J. Phys. Anthrop. 22:37-89.
Greenspan, J. S., and H. J. Blackwood (1966): Histochemical studies of chondrocyte function in the cartilage of the mandibular condyle of the rat. J. Anat. 100(3):615-626.
Gregg, J. M., and J. K. Avery (1964): Studies of alveolar bone growth and tooth eruption using tetracycline-induced fluorescence. J. Oral Ther. 2:268-281.
Gregory, W. K. (1929): Our face from fish to man. New York, Putnam.
(1931): Certain critical stages in the evolution of the vertebrate jaws. Int. J. Orthodont. 27.1138-1148.
Hanson, J. R., and B. J. Anson (1962): Development of the malleus of the human ear. Illustrated in Atlas Series. Quart. Bull., Northwestern Univ. Med. School, 36(2) : 119-137.
Hanson, J. R., B. J. Anson and T. H. Bast (1959): The early embryology of the auditory ossicles in man. Illustrated in Atlas Series. Quart. Bull. Northwest. Univ. Med. Sch. 33:358-379.
Harris, J. E. (1962): A cephalometric analysis of mandibular growth rate. Am. J. Orthodont. 48(3):161-174.
Harvold, E. P. (1951): The asymmetries of the upper facial skeleton and their morphological significance. Trans. Europ. Orthodont. Soc. pp. 6 3 -69.
Hellman, M. (1935): The face in its developmental career. Dent. Cos. 77:685-787.
Herovici, C. (1963): A polychrome stain for differentiating precollagen from collagen. Stain Techn. 38:204-205.
Hooten, E. A. (1946): Up from the Ape. New York, Macmillan.
Horowitz, S. L., and H. H. Shapiro (1951): Modi-

Bibliography
fications of mandibular architecture following removal of the temporalis muscle in rat. J. Dent. Res. 30:276-280.
Howells, W. (1949): Mankind So Far. Garden City, N.Y., Doubleday.
Hoyte, D. A. N. (1958): The relative contribution of sutural and ectocranial deposition of bone to cranial growth in rodents. J. Anat. 92:654.
(1961a): Resorption and skull expansion in rats. Anat. Rec. 139:307.
(1961b): The postnatal growth of the ear capsule in the rabbit. Am. J. Anat. 108:1-16.
(1964a): Facts and fallacies of alizarin staining: the exterior of the infant pig skull. J. Dent. Res. 43(No. 5 suppl.):814.
(1964b): Facts and fallacies of alizarin staining: the interior of the infant pig skull. Anat. Rec. 148:292-293.
(1965a): The role of the soft tissues in skull growth in rabbits. W. Indian Med. ]. J 4 (2 ) : 125.
(1965b): The sphenoidal complex in the first three months of its postnatal growth in rabbits: an alizarin study. Anat. Rec. 151:364.
(1966): Experimental investigations of skull morphology and growth. Internat. Rev. Gen. Exp. Zool. 2:345-407.
(1967): Some aspects of sphenoid bone growth in animals. Conf. on Craniofacial Growth. In press.
Hoyte, D. A. N., and D. H. Enlow (1966): Wolff's law and the problem of muscle attachment on resorptive surfaces of bone. Am. J. Phys. Anthrop. 24(2):205-214.
Humphry, G. (1864): On the growth of the jaws. Cambridge, Tr. Cambridge Phil. Soc.
Hunter, J. (1771): The Natural History of the Human Teeth, Explaining Their Structure, Use, Formation, Growth, and Disease. London, J. Johnson.
Isotupa, K., K. Koski, and L. Makinen (1965): Changing architecture of growing cranial bones at sutures as revealed by vital staining with alizarin red S in the rabbit. Am. J. Phys. Anthrop. 23(1) : 19-22.
Jones, B. H., and H. V. Meredith (1966): Vertical change in osseous and odontic portions of human face height between the ages of 5 and 15 years. Am. ]. Orthodont. 52:902-921.
Kerley, E. R. (1965): The microscopic determina-
( 2 9 1 )
tion of age in human bone. Am. J. Phys. Anthrop. 23(2):149-163.
Koski, K. (1965a): Growth potential of the mandibular condyle in the light of transplantation studies. Studieweek, pp. 35-45.
(1965b): Roentgen-cephalometry on anatomical basis. Studieweek, pp. 1-8.
Koski, K., and L. Makinen (1963): Growth potential of transplanted components of the mandibular ramus of the rat. 1. Suom. Hammaslaak. Toim. 59:296-308.
Koski, K., and K. E. Manson (1964): Growth potential of transplanted components of the mandibular ramus of the rat. II. Suom. Hammaslaak. Toim. 60:209-217.
Koski, K., and O. Ronning (1965): Growth potential of transplanted components of the mandibular ramus of the rat. III. Suom. Hammaslaak. Toim. 62(3):292-297.
Kraw, A. G, and D. H. Enlow (1967): Continuous attachment of the periodontal membrane. Am. J. Anat. I20( l ) :133-148.
Krogman, W. M. (1930): The problems of growth changes in the face and skull of anthropods and man. Dent. Cos. 72:624-630.
Krogman, W. M., and V. Sassouni (1957): A Syllabus in Roentgenographic Cephalometry. Philadelphia, Philadelphia Center for Research in Child Growth.
Lacroix, P. (1945): Remarques sur le mecanisme de l'allongement des os. Arch. Biol. 56:185-197.
(1960): "Ca45 autoradiography in the study of bone tissue." In Bone as a Tissue, ed. by K. Rodahl. New York, McGraw-Hill, pp. 262-279.
Latham, R. A., and W. R. Burston (1966): The postnatal pattern of growth at the sutures of the human skull. An histological survey. Dent. Pract. 17(2): 61-67.
Leblond, C. P., G. W. Wilkinson, L. F. Belanger, and J. Robichon (1950): Radio-autographic visualization of bone formation in the rat. Am. }. Anat. 86:289-341.
Manson, J. D. (1964): "Age changes in bone activity in the mandible." In Bone and Tooth. Proceedings of the First European Symposium, ed. by H. J. J. Blackwood. Oxford, Pergamon Press, pp. 343-349.
Massler, M., and I. Schour (1941): The growth pattern of the cranial vault in the albino rat as measured by vital staining with alizarine red S. Anat. Rec. 110:83-101.

( 2 9 2 )
Mednick, L. W., and S. L. Washburn (1956): The role of the sutures in the growth of the braincase of the infant pig. Am. J. Phys. Anthrop. 14(2): 175-192.
Moore, A. W. (1949): Head growth of the Macaque monkey. Am. J. Orthodont. 35:654-671.
Moorrees, C. F. A. (1967): Register of longitudinal studies of facial and dental development. Int. Soc. Cranio-Vacial Biol.
Moss, M. L. (1954): Growth of the calvaria in the rat. Am. ). Anat. 94:336-361.
(1960): Functional analysis of human mandibular growth. /. Prosth. Dent. 10(6):1149-1159.
(1961): The initial phylogenetic appearance of bone: an experimental hypothesis. Trans. N.Y. Acad. Sci. II., 23(6):495-500.
(1963): The biology of acellular teleost bone. Ann. N.Y. Acad. Sci. 109:337-350.
(1964): Differential mineralization of growing human and rat cranial bones. Am. J. Phys. Anthrop. 22(2) : 155-162.
Moss, M. L., and S. N. Greenburg (1955): Postnatal growth of the human skull base. Angle Orthodont. 25(2) : 77-84.
Moss, M. L., and R. W. Young (1960): A functional approach to craniology. Am. ]. Phys. Anthrop. 18:281-292.
Moyers, R. E. (1963): Handbook of Orthodontics, 2nd ed. Chicago, Year Book.
Murray, P. D. F. (1936): Bones. Cambridge, Cambridge Univ. Press.
Orban, B. J. (1957): Oral Histology and Embryology, 4th ed. St. Louis, Mosby.
Ortiz, M. H., and A. G. Brodie (1949): On the growth of the human head from birth to the third month of life. Anat. Rec. 103(3):311-334.
Perry, H. T. (1966): The temporomandibular joint. Am. J. Orthodont. 52(6) : 399-400.
Powell, T. V., and A. G. Brodie (1963): Closure of the spheno-occipital synchondrosis. Anat. Rec. I47( l ) :15 -23 .
Pratt, L. W. (1943): Experimental masseterectomy in the laboratory rat. J. Mammal. 24:204-210.
Pritchard, J. 'J. (1956): "General anatomy and histology of bone." In The Biochemistry and Physiology of Bone, ed. by G. H. Bourne. New York, Academic Press, pp. 1-25.
Pritchard, J. J., J. H. Scott, and F. G. Girgis (1956): The structure and development of cranial and facial sutures. J. Anat. 90:73-86.
Bibliography
Ricketts, R. M. (1960): Cephalometric synthesis. Am. ). Orthodont. 46:647-673.
Robinson, I. B., and B. G. Sarnat (1955): Growth pattern of the pig mandible. A serial roentgeno-graphic study using metallic implants. Am. J. Anat. 96( l ) :37-64 .
Roche, A. F., K. Manuel, and F. S. Seward (1965): Unusual patterns of growth in the frontal and parietal bones. Anat. Rec. 152(4):459-464.
Rouiller, C. (1956): "Collagen fibers of connective tissue." In The Biochemistry and Physiology of Bone, ed. by G. H. Bourne. New York, Academic Press, pp. 107-147.
Ruth, E. B. (1953): Bone studies. II. An experimental study of the Haversian-type vascular channels. Am. ). Anat. 93:429-456.
Salzmann, J. A. (1960): The research workshop on cephalometrics. Am. J. Orthodont. 46:834.
(ed.) (1961): Roentgenographic Cephalometrics. Proceedings of the second research workshop. Philadelphia, Lippincott.
Sarnat, B. G. (1963): Postnatal growth of the upper face: some experimental considerations. Angle Orthodont. 33(3) : 139-161.
(ed.) (1964): The Temporomandibular Joint, 2nd ed. Springfield, 111., Thomas.
Sarnat, B. G., and P. D. Shanedling (1965): Postnatal growth of the orbit and upper face in rabbits. Arch. Ophthal. 73:829-837.
Sarnat, B. G., and M. R. Wexler (1966): Growth of the face and jaws after resection of the septal cartilage in the rabbit. Am. J. Anat. 118(3):755-768.
Sassouni, V. (1960): The Face in Five Dimensions. Philadelphia, Philadelphia Center for Research in Child Growth.
Scott, J. H. (1953a): The cartilage of the nasal septum. Brit. Dent. ]. 95:37-43.
(1953b): The growth of the human face. Proc. Roy. Soc. Med. 47:91-100.
(1955): Craniofacial regions. A contribution to the study of facial growth. Dent. Pract. V(7):208-214.
(1956): Growth at facial sutures. Am. J. Orthodont. 42(5):381-387.
(1957): Muscle growth and function in relation to skeletal morphology. Am. J. Phys. Anthrop. 15:197-233.
(1958): The cranial base. Am. J. Phys. Anthrop. 16:319-349.
(1959): Further studies on the growth of

Bibliography
the human face. Proc. Roy. Soc. Med. 52(3) : 263-268.
Sicher, H. (1947): The growth of the mandible. Am. ). Orthodont. and Oral Surg. 33:30-35.
Sicher, H., and J. P. Weinmann (1944): Bone growth and physiologic tooth movement. Am. J. Orthodont. and Oral Surg. 30:109.
(1954): Principal fibers of the periodontal membrane. The Bur., 55:2-4.
Slavkin, H. C, M. R. Canter, and S. R. Canter (1966): An anatomic study of the pterygomaxil-lary region in the craniums of infants and children. Oral Surg. 21(2) : 225-235.
Smith, J. W. (1960): The arrangement of collagen fibers in human secondary osteones. /. Bone Joint Surg. 42-B(3):588-605.
(1961): Collagen fibre patterns in mammalian bone. /. Anat. 94(3).329-344.
Stallard, R. E. (1963): The utilization of H3-proline by the connective tissue elements of periodontium. Periodontics 1:185-188.
Stramrud, L. (1959): External and internal cranial base. A cross sectional study of growth and of association in form. Acta odont. scand. 17(2): 239-260.
Symons, N. B. B. (1951): Studies on the growth and form of the mandible. Dent. Rec. 71:41-53.
Takagi, Y. (1964): Human postnatal growth of vomer in relation to base of cranium. Ann. Otol. 73(l) :238-248.
Todd, T. W. (1932): Prognathism; a study in development of the face. J. Amer. Dent. Ass. 19: 2172-2184.
Tomelin, D. H., K. M. Henry, and S. K. Kon (1953): Autoradiographic study of growth and calcium metabolism in the long bones of the rat. Brit. J. Nutr. 7:235-251.
Troitsky, W. (1932): Zur Frage der Formbildung des Schadeldaches. Z. Morph. Anthrop. 30:504-532.
Tweed, C. H. (1954): The Frankfort-mandibular incisor angle (FMIA) in orthodontic diagnosis, treatment planning and prognosis. Angle Orthodont. 24:121-169.
( 2 9 3 )
Washburn, S. L. (1946a): The effect of facial paralysis on the growth of the skull of rat and rabbit. Anat. Rec. 94:163-168.
(1946b): The effect of removal of the zygomatic arch in the rat. J. Mammal. 27:169-172.
(1947): The relation of the temporal muscle to the form of the skull. Anat. Rec. 99:239-248.
Weidenreich, F. (1924): The special form of the human skull in adaptation to the upright gait. Z. Morph. Anthrop. XXIV (2):157-190.
(1941): The brain and its role in the phylogenetic transformation of the human skull. Trans. Amer. Phil. Soc. 31:321-442.
(1946): Apes, Giants, and Man. Chicago, Univ. Chicago Press.
Weinmann, J. P. (1954): The adaptation of the periodontal membrane to physiologic and pathologic changes. /. Oral Surg. 8:977.
Weinmann, J. P., and H. Sicher (1955): Bone and Bones, 2nd ed. St. Louis, Mosby.
Wexler, M. R., and B. G. Sarnat (1965): Rabbit snout growth after dislocation of nasal septum. Arch. Otolaryng. 81:68-71.
Woo, J. K. (1949): Ossification and growth of the human maxilla, premaxilla, and palate bones. Anat. Rec. 105:731-761.
Woo, T. L. (1931): On the asymmetry of the human skull. Biometrika 22:324-352.
Woods, G. A. (1950): Changes in width dimensions between certain teeth and facial points during human growth. Am. ]. Orthodont. 36:676-700.
Yen, P. K. J. (1960): Identification of landmarks in cephalometric radiographs. Angle Orthodont. 30: 35-41.
Yuodelis, R. A. (1966): The morphologenesis of the human temporomandibular joint and its associated structures. J. Dent. Res. 45(1): 182-191.
Zwarych, P. D., and M. B. Quigley (1965): The intermediate plexus of the periodontal ligament: history and further investigations. J. Dent. Res. 44:383-391.


Acoustic meatus, external, 223 Age, bone, estimation of, 56
changes in cartilage, 9 chronologic, 265
Alar cartilage, 272 Albumoid, 9 Alveolar bone, surfaces of, 87
margin, 53, 245 remodeling, secondary, 94
Amphibians, 13 Amprino, R., 33, 35 Animal, size of, 14 Anode source, high-voltage rotating, 263 Antegonial region, mandible, 123
reversal of, 259 Apatite, 11 Appositional growth, 6, 10, 40, 43 Arch, dental, 252
mandibular, 252 maxillary, 144, 204, 245, 246, 252 zygomatic, 221
Articulare, 280 Attachments, on resorptive bone surfaces, 89
muscle, 35, 39, 56, 81, 131 tendon, 35, 56
Auditory apparatus, 203, 207 meatus, 252 ossicles, 223 reversal, 260 tube, 223
Avis, V., 79
Baer, M. J., 197, 199 Bang, S., 87, 142, 147, 150, 155, 157, 178 Bairati, A., 33 Basion, 269, 279 Basion-naison plane, 281 Basophilia, matrix, 9 Bernstein, S. A., 95 Binocular vision, 169, 189 Birds, 13 Bjork, A., 236, 248, 282 Blood vessels, 5, 18 Bohatirchuk, F., 89 Bolton point, 280 Bone, adult, 55
age changes in, 55 estimation of, 56
alveolar surfaces, 87 bundle, 37, 87 cancellous, 55
course, 19 fine, 21, 45, 55
chondroid, 37 circumferential, 29 coarsely-bundled, 17 compacted, coarse cancellous, 27, 33, 73, 74 convoluted, 27, 33, 73, 74 cortical compact, typical pattern of, 75 elongation of, 51 endochondral, 12, 45, 52, 110, 139 endosteal, 25, 52, 61 evolution of, 12
295
Index

( 2 9 6 )
Bone (continued) fetal, 22 fibriform, 37 growth. See subjects as listed under Growth hardness in, 11, 57 Haversian, 31, 77
strength of, 79 See also Osteon
human, 56 intramembranous, 12, 52, 110 lamellar, 15, 45, 56 laminar, 17 lepidosteoid, 37 matrix, 11 membrane, 12 microscopic structure of, differences, 14 neonatal, 55 noncellular, 14 nonlamellar, 15, 21, 155 nonvascular, 15 parallel-fibered, 16, 22 perichondral, 223 periodontal, 87 periosteal, 25, 61 plexiform, 24, 27 primary vascular, 17 resorptive surfaces of, 89, 93 secondary. See Haversian bone specializations of structure, 11 spot deposits, 37, 89, 91, 93, 99 surfaces of, 25, 58, 108 vascular, 15 woven-fibered, 17, 22
Bones. See names of individual bones Brain, 201, 202, 203, 240
human, 169 olfactory, area of, 194 stem, 208
Brash, J. C, 109 Broadbent, B. K., 263, 264 Broadbent-Bolton technique, 263 Brodie, A. G., 109, 212 Brues, A. M., 171 Bundle bone, 37, 87
Calcification, matrix, 49 Calcioysis, 89 Calvaria, 84, 139, 194, 195, 206, 212, 228 Cambial zones, in sutures, 95 Canaliculi, 43
Index
Canals, non-Haversian, 18 primary vascular, 18, 45, 56 secondary, 18 Volkmann's, 18, 33
Cancellous bone, coarse, 19 compacted, 27 fine, 21, 45, 55
Capsular layer, in sutures, 95 Capsule, chondrocyte, 9 Cartilage, 12
age changes in, 9 alar, 272 articular, 3, 8 epiphyseal, 47, 68 Meckel's, 223 modes of growth, 8 resorption of, 10 structure and growth of, 5
Cartilage and bone structure compared, 9 Cell nests, chondrocyte, 9 Cells, perivascular, 5, 31
undifferentiated, 5, 31, 42 Cement line, 31 Cementoenamel junction, 276 Centers of growth, 53, 105 Cephalograms, error, 264
serial, 228 use of, 265
Cephalometrics, elementary principles of, 261 picture, 228, 231 planes, 280
Cerebrum, 194, 195 See also under Human
Charles, S. W., 109 Cheek outlines, 272 Cheekbone, 250
See also Zygoma Chin, 131, 184, 247,250
See also Mental region Chondroblasts, 7 Chondrocranium, 52 Chondrocytes, 7
hypertrophy of, 47 isogenous groups of, 9
Chondrogenic zone, 7, 8 Chondroid bone, 37 Chondroitin sulfate, 3, 9 Chondromucoprotein, 3 Chronologic age, 265 Circumcranial reversal line, 212, 220, 221, 258

Index
Circumferential, bone, 29 reversal line, 200
Circumspinal reversal, 258 Clinoid, anterior, 275 Clivus, 195, 208, 209, 213, 215, 252 Compact bone. See Cortex Comparative morphogenesis, 168 Compartments, endocranial, 203, 222 Conchae, 215 Condylar growth center, 109
mechanism, 110 Condyle, mandibular, 52, 54, 55, 139
neck, 110, 112, 252 occipital, 269, 276
Convoluted bone, 27, 33, 73, 74 Coronoid process, 115, 277
in Macaca, 173 Cortex, 10
compact bone, typical pattern of, 75 drift, 69, 70, 71, 75 movement-displacement, 75 stratification, 72, 73 zones, 66
Cranial base, 84, 201, 228, 252 compartments, 203, 222 flexure of, 169, 186, 195 fossae, 195
anterior, 213, 220, 240, 252 middle, 211, 213, 222,275 posterior, 208, 222
growth of, 194, 201 reversals of, 201, 212, 220, 258 spheno-occipital portion of, 195
Cribriform plate, 188, 218, 240, 244, 273 Cross-sectional growth studies, 265 Crura, of stapes, 226 Culs-de-sac, 203, 204, 213 Currey, J. D., 79
Deer, 169, 193 Dental arch, 252 Dentary bone, 109 Dentin, 15 Deposits, spot, 37, 89, 91, 93, 99 Diencephalon, 211 Differences in microscopic bone structure, 14 Differential growth, 77
rate, 99 in skull, 195
Displacement, 80, 81, 108, 136, 228, 237
( 2 9 7 )
Dorsum sella, 275 Downs, W. B., 268 Drift, 73, 108
cortical, 69, 70, 71, 75 of membrane, 85 periodental, 91, 92, 94 of teeth, 87 tubercle, 39, 72
DuBrul, E. L., 184 Duterloo, H. S., 53
Ear, membranous labyrinth, 222 middle, 222 See also Auditory apparatus
Endochondral bone, 12, 52 ossification, 45, 110, 139
in skull, 52 Endocranial compartments, 195, 203, 222 Endosteal bone, 25, 52, 61
transitions, 101 Endosteum, 25 Epiphyseal cartilage, 47, 68
functional role of, 54 in nonmammalian forms, 52 zones in, 51
Ethmoid, 166, 167, 212, 218, 248, 273, 274 sphenoethmoid junction, 204, 273
Etter, L. E., 268 Evans, F. G., 55, 79 Evolution of bone, 12 Exoccipital region, 208, 213 External nasal reversal, 260 Eye, 169, 195, 241
Face, human, characteristics of, 171 upright nature of, 186, 192
in Macaca, growth and remodeling, 171, 181 placement of, 189 rotation, 192, 194 upright, summary of features, 193
Facial growth, composite nature of, 227 directions of, 188 human, 189, 227 in Macaca, 171, 181 man and Rhesus monkey compared, 182 mosaic pattern of, 239 regressive, 185, 246 topographic changes, 230, 250
Facial pocket, 186, 187, 192, 194, 204, 252, 283 topography, 230, 250

( 2 9 8 )
Fetal bone, 22 Fibers, 3, 5
anchoring, 89 attachment, on resorptive bone surfaces, 89 bone, 11 of periodontal membrane, 89 Sharpey's, 87, 97, 177
Fibriform bone, 37 Fibroblasts, 7 Fish, 12, 13 Fixed landmarks, 230
line, 281 points, 281
Flexure, of cranial base, 169, 186, 195 Foramen caecum, 273 Foramen magnum, 169, 186, 195, 208, 209, 213,
269 Foramen rotunda, 280 Ford, E. H. R., 212 Forehead, 195, 239, 250
of Macaca, 180 See also Frontal bone
Fossa, anterior cranial, 213, 220, 240, 252 endocranial, 195 middle cranial, 211, 213, 222, 275 posterior cranial, 208, 222
hypophyseal, 275, 280 olfactory, 218 pterygopalatine (sphenomaxillary), 217 sublingual, 127
Fossil record, 12 of hominoids, 169
Frankfort plane, 263, 281, 283 Frontal bone, 21, 212, 220, 273
of Macaca, 180 process, 252 sinus, 240
Frost, H. M., 14, 33
Gans, B. J., 140, 236 Genetic factors, 81 Glabella, 221, 240, 248, 250 Glossary of reversals, 253 Glycogen, 9 Gnathion, 279; 283 Gonial area, 280
flare, 250 Gonion, 280 Greenburg, S. N., 195
Index
Growth, appositional, 6, 40, 43 of bone, 37 of calvaria, 194 centers, 53, 105 of cranial base, 194
basic plan, 201 directions of, 58 endochondral, 139 equivalents, 252 facial, comparison of man and Rhesus monkey,
182 composite nature of, 227 directions of, 188 human, 189 of Macaca, 171
general plan, 181 regressive, 185, 246 topographic changes, 230
fields, 83, 200 interrelationships during, 252 interstitial, 6, 39 intramembranous, 52, 110 linear, 65 maxillary, summary diagram of, 165
scheme of, 233 of membranes, 83, 85 movements, 108 patterns without fixed reference marks, visualiza
tion of, 230 of periodontal membrane, 85 of periosteum, 99 rates, differential, 14, 77, 99 remodeling, 138, 236, 237
in maxilla, 158 resorptive phase of, 40 skeletal, misconceptions of, 57 sites, 53 soft tissues, 39
See also Membranes stages, of mandible, 232 studies, cross-sectional, 265 surface, generalized, 105, 140
directions of, 135 of mandible, 133
sutural, 139, 140, 236 Ground substance, 3, 5, 11 Growth center, chondrogenic, 5
condylar, 109 in face, 139 of mandible, 133

Index
Halisteresis, 89 Hand, human, 169 Hardness of bone, adaptations to, 11, 57 Harris, D. B., 112, 114, 117, 118, 121, 124, 126,
128, 133, 134, 136 Harvold, E. P., 280 Haversian bone, 31, 77, 79 Haversian system, 12, 17, 27, 37, 56
as a multifunctional structure, 37 remodeling, below resorptive surface, 100 replacement, 15 See also Osteon
Head, movements of, 171 Head holder, 264 Hominoids, fossil, 169 Howship's lacunae, 89, 93 Hoyte, D. A. N., 81, 199 Human, bone, 56
brain, 169 face, 168
characteristics of, 171 comparison of growth with Rhesus monkey, 182 upright nature of, 186, 192 See also Growth
feet, 168 hand, 169 jaws, 169 orbital rim, 186 skull, configuration of, 168
neonatal, 227 Hunter, J., 109, 236 Hunter, W. S., 237, 238, 239, 241, 243 Hyalinization, matrix, 7 Hypertrophy of chondrocytes, 47 Hypophyseal fossa, 275, 280 Hypophysis, 203, 207,211
Incision, inferius, 279 superius, 279
Incus, 225 Infradentale, 279 Inorganic matrix, 11 Intercellular matrix, 3 Internal remodeling and reconstruction, 31 Interstitial growth, 6, 10, 39 Intramembranous ossification, 52, 110 Intranasal reversal, 260 Isogenous groups, of chondrocytes, 9
Jaw, human, 169
( 2 9 9 )
Jones, B. H., 283 Jugular reversal, 260
Key ridge, 280 Koski, K., 53 Kraw, A. G., 88, 91, 95 Krogh, tissue cylinder of, 33 Krogman, W. M., 264, 268, 277, 279, 280
Lacrimal bone, 163 Lacroix, P., 31 Lacunae, Howship's 89, 93
osteocyte, orientation of, 16 Lamellae, inner circumferential, 74, 77
outer circumferential, 74, 77 Lamellar bone, 15, 45, 56 Lamina, external and internal, 19 Laminar bone, 17 Landmarks, 230, 277
anatomic, 277 derived, 277
Lateral mandibular reversal, 119 Lepidosteoid bone, 37 Lingual tuberosity, 128 Linkage fibrils, 89, 95 Lipids, 9 Lobes, frontal, 188
olfactory, 244 prefrontal, 169, 188 temporal, 169
Local control mechanism, 54, 79, 83
Macaca, coronoid process, 173 facial growth, compared with man, 182
general plan of, 181 remodeling in, 171
forehead, 180 frontal bone, 180 malar region, 175, 185 mandible, 171, 172 maxilla, 175 nasomaxillary complex, 175 orbital rim, 177
margin, 186 palate, 179, 181 premaxilla, 180, 181 skull, 179 trihedral eminence, 175 zygomatic bone, 175

( 3 0 0 )
Malar, region of, 153,240 in Macaca, 175, 185
reversal, 257 See also Zygoma
Malleus, 223 Mammals, 13 Mandible, 250, 252, 277
antegonial region of, 123 arch, 129, 252 body, 125 comparison with maxilla, 159 condyle, 139
in Macaca, 172 growth, application of principles, 133
centers of, 133 stages of, 232 surface, generalized, 133
incisors, 277 of Macaca, 171 mental protuberance of, 131 phylogenetic history, 109 plane, 281 of rabbit, 178 reversal, lateral, 119, 259
medial, 122, 259 sigmoid notch of, 113 zygomatic process of, 143
Massler, M., 199 Mastoid process, 169, 269, 280 Matrix, basophilia, 9
in bone, 11 calcification of, 9, 49 organic and inorganic, 11 territorial and interterritorial, 9
Maxilla, 140, 274, 276 arch, 144, 204, 245, 252
anterior portion of, 246 comparison with mandible, 159 fissure, pterygomaxillary, 274 growth and remodeling of, 13,8, 158
scheme of, 233 summary diagram of, 165
in Macaca, 175
nasomaxillary complex, 245, 252 premaxillary, 148, 246 process of, frontal, 248
palatine, 145 sinus, 157
in deer, 193
Index
Maxilla (continued) sutures, frontomaxillary, 169, 242, 244, 245, 248,
249, 276 zygomaticomaxillary, 245, 249
tuberosity, 141 Medial mandibular reversal, 122 Medulla, 10 Membranes, 110
of bone, 12, 99 drift of, 85 growth of, 85 linkage fibrils, 89 periodontal, 53, 85 soft tissue, 83 sutural, 84 See also Periosteum
Mental region, 250 reversal of, 259 See also Chin
Menton, 279 Meredith, H. V., 283 Mesenchyme, 5 Metaphyseal reduction, 111 Misconceptions of skeletal growth, 57 Monkey. See Macaca Moorrees, C. F. A., 283 Morphogenesis, comparative facial, 168 Mosaic pattern of facial growth, 239 Moss, M. L., 14, 95, 195, 197, 199 Mucopolysaccharides, 11 Muscle, attachment of, 35, 39, 56, 81
on resorptive surfaces, 131
pull, 81 sternocleidomastoid, 169
Muzzle, 168, 194, 195 prognathic, 169, 191
Naison, 277 Nasal, bones, 161, 248, 274
bridge, 240, 244, 250 cavity, 250 orientation, 188 reduction, 169 region, 151, 155, 157, 242 reversals, circumnasal, 257
external, 260 internal, 260
septum, 77, 139 spine, anterior, 279
posterior, 279

Index
Nasomaxillary complex, 138, 245, 252 of Macaca, 175 reversal, 257
Necrosis, osteocyte, 14, 33 Neonatal human skull, 227 Nerves, 5, 188,203,207,244 Noncellular bone, 14 Nonlamellar bone, 15, 21, 55 Nonvascular bone tissue, 15 Nose, 195, 244, 250, 252
Occipital bone, 207, 273 condyle of, 276
Occlusal plane, 281 Olfactory area of brain, 194
bulbs, 203 fossae, 218 lobes, 244 nerve, 188, 244
Orbit, 215, 221, 247, 274 floor, 155, 157 lateral rim of, 155 margin, in Macaca, 186 orientation, 188 outline, 275 reversals of, 257 ridge of, 248, 249, 250 rim of, 252
human, 186 Macaca, 177
Orbitale, 279 Organic matrix, 11 Ossicles, auditory, 223 Ossification, centers of, primary, 42
secondary, 42 endochondral, 45, 52 intramembranous, 42
Osteoblasts, 31 Osteoclasts, 31 Osteocytes, 15 Osteodentin, 15 Osteoid, 15, 42 ,45 Osteon, 74
primary, 22, 23, 45 secondary, 22, 56, 77 See also Haversian system
Otic capsule, 223
Palatal plane, 281
( 3 0 1 )
Palate, 155, 276 of Macaca, 179, 181, 245 soft, 269
Palatine, bone, 163 process of maxilla, 145
Paleozoic, 12 Parallel-fibered bone, 16, 22 Pelvis, 168 Penumbra effect, 263 Perichondral bone, 223 Perichondrium, 5, 7, 101
chondrogenic layer of, 8 Periodontal, bone, 87
drift, 91, 92, 94 membrane, 53, 85, 89
Periosteal bone, 25, 61 "spot" deposits of, 37, 89, 91, 93, 99
Periosteum, 10, 18 formation, 43 structure and growth of, 99 transitions with endosteum, 101
Perivascular stem cells, 5, 31 Petrosal reversal, 258 Pharynx, 204 Phylogenetic concepts, 12 Pituitary. See Hypophysis Plexiform bone, 24, 27 Pocket, facial, 186, 187, 192, 194, 204, 252, 283 Pogonion, 279 Polarized light, use of, 16 Polysaccharides, 3 Porion, 280 Posture, upright, 168, 171, 195 Potter-Bucky grid, 264 Powell, T. V., 212 Premaxilla, 148, 153, 157, 180, 181, 246 Pressure, 79 Primary, center, 49
osteon, 22, 23, 45 vascular canals, 45, 56
Primary vascular bone, 17 Pritchard, J. J., 95 Prognathic muzzle, 169, 191 Prosthion, 279 Pterygoid, 211
processes of, 217, 275 reversals, 258
Pterygomaxillary fissure, 274, 276, 280 Pterygopalatine fossa, 217

( 3 0 2 )
Rabbit mandible, 178 Radiographs, 263 Ramus, 204, 252
anterior reversal of, 259 buccal side of, 119 lingual side of, 121 posterior margin of, 112
Reconstruction, internal, 10, 31 Regressive growth, in face, 185, 246 Relocation, 59, 61, 68, 73, 75, 108, 111, 135, 199 Remodeling, 39, 57, 75, 107, 135
alveolar, secondary, 94 growth, 138,236,237 Haversian, 100 internal, 31 linear, 65
Reptiles, 13 Reshaping and resizing, 65, 75, 107 Resorption, 57
in cartilage, 10 space, 31
Resorptive bone surfaces, fiber attachment on, 89, 93, 131
Reversals, 61, 66 antegonial, 259 anterior, of ramus, 259 auditory, 260 cement line, 31 circumcranial, 212, 220, 221, 258 circumnasal, 257 circumspinal, 258 external nasal, 260 intranasal, 260 intraorbital, 257 jugular, 260 lateral mandibular, 259 lines, 253 malar, 257 medial mandibular, 259 mental, 259 nasomaxillary, 257 petrosal, 258 pterygoid, 258 sphenoidal, 258 zygomatic, 257
Rhesus monkey. See Macaca Ricketts, R. M., 283 Ronning, O., 53 Rotation of face, 192, 194 Rouiller, S., 15
Index
Salzmann, J. A., 264 Sarnat, B. G., 140, 236 Sassouni, V., 264, 268, 276, 277, 280 Schour, I., 199 Scott, J. H., 95, 140, 189, 219 Sella, 211, 213, 215, 252, 264, 275, 280, 283 Sella-naison, 280 Senses, species differences, 169 Serial cephalograms, 228 Sharpey's fibers, 87, 97, 177 Sicher, H., 95, 184, 199 Simian shelf, 175, 183, 184 Sinus, frontal, 240 Skeleton, bone in newborn and child, 55 Skull, base. See Cranial base
differential extent of enlargement in, 195 endochondral ossification in, 52 human, configuration of, 168
neonatal, 227 of Macaca, 179 roof, 195
Smith, J. W., 16 Snout, 169, 194 Species, identification of, 56
differences, in senses, 169 Sphenoid, 211, 212, 273, 274, 275
reversal, 258 Sphenoethmoidal junction, 204, 273 Sphenomaxillary fossa, 217 Spheno-occipital portion of cranial base, 195, 252
synchondrosis, 204, 208, 209, 212, 273, 275 Spinal cord, 207, 208 "Spot" deposits, 37, 89, 91, 93, 99 Standard cephalometric picture, 228 Stapes, 226 Sternocleidomastoid muscle, 169 Stress, 79, 81 Subspinale, 279 Supramentale, 279 Supraorbital ridge, 248, 249, 250 Surface template, 25 Sutures, 55, 84, 195, 199, 205, 208, 212, 215, 220,
221, 252 frontolacrimal, 165 frontomaxillary, 165, 242, 244, 245, 248, 249,
276 rrontozygomatic, 241, 245, 280 growth of, 95, 139, 140, 236 structure of, 94 temporoparietal, 213

Index
Sutures (continued) temporosphenoidal, 221
Synchondrosis, 8, 52, 53, 205, 206 sphenoethmoid, 273 sphenooccipital, 204, 208, 209, 212, 273, 275
Teeth, movements of, 85, 87, 130 thecondont type, 109
Template, surface, 25 Temporal bone, 204, 211, 221, 252, 274, 275
portion of, mastoid, 222, 275 petrous, 222, 275 squamous, 275 styloid, 222, 275 zygomatic, 221
Tendon, attachments of, 35, 56 Tension, 79 Tissue, cylinder, 33, 35
growth of, 39 membranes, 8 3 profile, 269 reticular connective, 21 See also Bone; Cartilage
Tooth-bone changes, 85, 130 Topography, facial, 230, 250 Training techniques, 268 Transitions, periosteal-endosteal, 101 Trihedral eminence, 129, 250
in Macaca, 175 Troitsky, W., 95 Tubercle drift, 39, 72 Tuberosity, maxillary, 141 Undifferentiated cells, 5
See also Perivascular cells
( 3 0 3 )
Upright posture, 168, 171, 195
Vertebral column, 168 Vertical posture, 168, 171, 195 Vessels, 5, 18 Vision, binocular, 169, 189 Volkmann's canals, 18, 33 Vomer, 219 V-Principle, 63, 64, 65, 108, 137
Washburn, S. L., 79 Weidenreich, F., 186 Weinmann, J. P., 95, 199 Wolff's Law, 79 Woo, T. L., 263 Woods, G. A., 263 Wylie compensator, 263
Yen, P. K. J., 277
Zones, cortical, 66 of epiphyseal cartilage, 51
Zygoma, 249, 252, 274, 276 Zygomatic, arch, 221
bone, 159, 273 of Macaca, 175
process, 280 of maxilla, 143 reversal, 257 of temporal bone, 221
Zygomaticofrontal suture, 249, 276 Zygomaticomaxillary suture, 245, 249 Zygomaticotemporal suture, 99, 140, 221, 274, 276



![This Face Changes the Human Story. But How?€¦ · This Face Changes the Human Story. But How? 9/18/2015 7:27:50 AM] This Face Changes the Human](https://img.pdfslide.net/doc/110x75/5ec616d390a1e3175f25416d/this-face-changes-the-human-story-but-how-this-face-changes-the-human-story-but.jpg)