Embed Size (px)
Citation preview

Kidney International, Vol. 31(1987), pp. 142—155
NEPHROLOGY FORUM
The hypercalcemia of malignancyPrincipal discussant: GREGORY R. MUNDY
The University of Texas Health Science Center, San Antonio, Texas
Case presentations
Patient I. A 54-year-old black man was admitted to the AudieMurphy Memorial Veterans Hospital in San Antonio 3 years ago with ahistory of pain in the left clavicular region and weakness and pain in theleft arm that had been present for approximately one month. He hadlost 40 pounds over the previous year and for 6 months had had a coughproductive of sputum, which recently had become blood streaked. Hehad smoked one pack of cigarettes per day for 40 years. Physicalexamination revealed a thin man weighing only 80 pounds with a hard,nontender mass in the left supraclavicular region. He had decreasedsensation over the lateral aspect of the left arm, and Homer's syndromewas present. No abnormal motor findings were present. Chest x-rayrevealed a mass in the left upper lobe of the lung consistent with aPancoast tumor. The lung mass measured 4 x 2 cm. Sputum cytologywas consistent with squamous cell carcinoma. Bronchoscopy showedno evidence of an endobronchial lesion, although the bronchoscopywashings were positive for squamous cell carcinoma. During thisadmission the serum calcium was 10.5 mg/dl and the serum albumin 3.6g/dl. A bone scan, CT scans of the abdomen and head, and an ab-dominal sonogram revealed no evidence of metastatic disease. Localradiation therapy produced relief of the bone pain. The patient received5400 rads to the left upper lobe and 4000 rads to the mediastinum andsupraclavicular area.
The patient was discharged but was readmitted to the hospital 2months later with marked confusion. His mental status had deterioratedrapidly over the week prior to admission. The findings were the same ason the first admission, except that now he was dehydrated, the bloodpressure was 80/40 mm Hg, and a new mass was present in the rightsupraclavicular region. The serum calcium was 16.0 mg/dl; albumin, 2.9g/dl; sodium, 130 mEq/liter; chloride, 100 mEq/liter; bicarbonate, 26mEq/liter; potassium, 4.2 mEq/liter; BUN, 38 mg/dl; and creatinine, 2.1
Presentation of the Forum is made possible by grants from Merck Sharp& Dohme, Pfizer Laboratories, and Sandoz, Incorporated.
© 1987 by the International Society of Nephrology
mg/dl. Plasma PTH (C-terminal) was 50 zEq/ml (normal, 20—120Eq/ml).
He was treated with salmon calcitonin, 200 MRC units intramuscu-larly each 12 hours, and hydrocortisone, 100 mg intravenously each 6hours, and vigorous infusion of normal saline. After 4 days, calcitoninwas withdrawn and he was given oral corticosteroids. The BUNgradually fell to 20 mgldl. Biopsy of the right supraclavicular massrevealed lymphoid tissue extensively infiltrated with squamous cellcarcinoma. Although the serum calcium level was controlled by medicaltherapy, the advancing malignancy caused a progressive deterioration.Chemotherapy was not considered advisable, and he died one monthafter the second admission.
Autopsy disclosed squamous cell carcinoma of the left upper lobe ofthe lung with widespread metastases in the liver, right lung, lymphnodes, brain, and bone marrow. There was no evidence of bonemetastases. The parathyroid glands were normal. Metastatic tumortissue obtained from the right supraclavicular lymph nodes was probedwith a cDNA probe for parathyroid hormone and a cDNA probe fortransforming growth factor (TGF)a using the Northern technique.Parathyroid hormone was not expressed, but TGFa mRNA was ex-pressed excessively.
Patient 2. A 43-year-old factory worker came to the Royal HobartHospital, Hobart, Tasmania, with severe low-back pain of 2 monthsduration, confusion, and dehydration. At the time of admission, he wasthin, lethargic, and disoriented; the pulse was 120 beats/mm and theblood pressure was 90/60 mm Hg. The serum calcium was 15 mgldl;serum albumin, 3.9 g/dl; blood urea, 80 mg/dl; and serum creatinine, 4mg/dl. A radiologic survey showed widespread osteolytic lesions in theskull and long bones, and osteopenia of the vetebral bodies withcollapse of T7 and T8. A bone marrow examination revealed increasedcellularity with marked rouleaux formation and increased backgroundstaining. Myeloma cells comprised 80% of all nucleated marrow ele-ments and included binuclear forms and syncytia. Plasma proteinelectrophoresis revealed an abnormal band in the gamma region, andplasma protein immunoelectrophoresis showed an IgG monoclonalprotein. Immunoglobulin assays revealed an IgA of 130 mg/dl (normal,167—410 mgldl); IgG, 3000 mg/dl (normal, 870—1520 mg/dl); and 1gM, 20mg/dl (normal 50-110 mg/dl). Bence Jones proteinuria was present. Thepatient was given 6 liters of normal saline during the first 24 hours afteradmission and was treated with corticosteroid therapy (100 mghydrocortisone intravenously every 6 hours), and the serum calcium fellto 10.5 mgldl over the ensuing 3 days. His lethargy and confusionimproved markedly, and he was able to give a clear history of disablingback pain, which had been progressive in the weeks prior to admission.
Symptomatic improvement followed treatment with cyclophospha-mide for myeloma, with relief of the bone pain. He was not able toreturn to work but was able to walk with the aid of crutches and toreturn home. During the remission, a small maintenance dose ofcorticosteroid (prednisone, 10 mg daily) was required to keep the serumcalcium within the normal range. When the bone pain recurred 5months later, cyclophosphamide was discontinued; melphalan and localradiation therapy to his back again relieved local symptoms. The serumcalcium remained in or near the normal range and corticosteroidtherapy was continued. He was readmitted one year after the initialadmission with fever and hypotension. Blood cultures revealed gram-negative bacteria. The serum calcium did not exceed 11 mg/dl. Despiteantibiotic therapy he died 48 hours after admission.
142
EditorsJORDAN J. COHENJOHN T. HARRINGTONJEROME P. KASSIRERNICOLAOS E. MADIAS
Managing EditorCHERYL J. ZUSMAN
University of Chicago Pritzker School of Medicineand
Tufts University School of Medicine
CORE Metadata, citation and similar papers at core.ac.uk
Provided by Elsevier - Publisher Connector

The hypercalcemia of malignancy 143
Discussion
DR. GREGORY R. MUNDY (Head, Division of Endocrinologyand Metabolism, and Professor of Medicine, The University ofTexas Health Science Center, San Antonio, Texas): These twocases illustrate the wide range of circumstances under whichpatients with malignancy develop hypercalcemia. The firstpatient had hypercalcemia in association with a solid tumor(squamous cell carcinoma of the lung) and without evidence ofbone metastasis. This syndrome is known as humoral hypercal-cemia of malignancy, and presumably is due to circulatingtumor products, which increase both bone resorption and renaltubular calcium reabsorption and lead to an increase in extra-cellular fluid calcium. Tumor tissue from this patient wasprobed for evidence of both PTH mRNA expression, and TGFcmRNA expression (by Dr. R. Derynck, of Genentech Inc.,South San Francisco). There was no evidence of PTH biosyn-thesis, but TGFa was clearly synthesized by this tumor and islikely to be responsible, at least in part, for the hypercalcemia.(This patient comprised one of the cases reported by Simpson etal [11.) The second patient, who made a lasting impression onme when I was a house officer, had extensive lytic bone de-struction in association with myeloma, and in addition hadhypercalcemia with fixed impairment of renal function. In thiscase, the hypercalcemia presumably was due to localized bonedestruction mediated by locally active myeloma cell products,in association with decreased renal calcium clearance due toimpaired glomerular filtration. The prognosis in both patientswas poor. The hypercalcemia was controlled satisfactorily withmedical therapy, but both patients expired from advancingmalignancy within twelve months. These 2 patients illustratethat the pathophysiologic mechanisms responsible for hypercal-cemia in patients with malignancy are heterogeneous fromtumor type to tumor type [21. As will become apparent duringthe following discussion, many individual tumors probablyproduce several products that work in concert to disruptcalcium homeostasis. This should not be surprising, becauseextracellular fluid calcium is normally under such tight regula-tion. Any disease process that causes a disturbance in thissuperb homeostatic mechanism must be not only powerful, butalso is likely to be complex. As studies on the pathophysiologyof hypercalcemia and malignancy proceed, knowledge probablywill accumulate not only on how individual tumor productsaffect target organs, but also on how these multiple effectsinteract to cause an increase in serum calcium.
Hypercalcemia, a relatively common clinical problem, hasbecome even more frequently recognized as autoanalyzer mea-surements of serum calcium have become routine on all serumsamples drawn for electrolyte determinations. After the patientis recognized as having hypercalcemia, a number of diagnosticpossibilities that might not have been considered previously areraised. Primary hyperparathyroidism is the most common causein the ambulant population, and patients with this disorder areoften asymptomatic [3, 4]. Current estimates are that primaryhyperparathyroidism may have the astonishing annual inci-dence rate of 250 new patients per million population per year[3, 4}. In hospitalized patients, such as the 2 presented here,malignant disease is the commonest cause of hypercalcemia. Inthe following discussion I will review the multiple pathophysi-
ologic mechanisms that have been linked with the presence ofhypercalcemia in patients with malignant disease.
Normal calcium homeostasisExtracellular fluid calcium is regulated primarily by the
effects of three systemic hormones, each of which in turn iscontrolled (either directly or indirectly) by serum ionized cal-cium, thus yielding three negative feedback loops. These threehormones are parathyroid hormone (PTH); 1,25 dihydroxyvi-tamin D (l,25D); and calcitonin. The relative importance ofeach of these hormonal systems on calcium homeostasis is notfully clear, nor is it certain that there are not additionalimportant mechanisms, possibly mediated at the tissue level ofthe target organs. However, at least as far as chronic control ofserum calcium is concerned, PTH and l,25D are clearly moreimportant than is calcitonin, which may have only acute ortransient effects. I say this because persistent alterations incalcium homeostasis do not occur either with absence of thethyroid gland or with tumors of the calcitonin-secreting cells(medullary thyroid carcinoma).
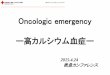
The maintenance of serum calcium depends on the transportof calcium across three organs: the gut, kidney, and bone (Fig.1). Several points about calcium transport across these organsand their relationship with the extracellular fluid should beemphasized, because they are important in the hypercalcemiaof malignancy. Bone is an enormous reservoir for calcium. Ofthe total calcium in the body, 99% is present in bone. In thenormal adult before middle life, bone resorption and boneformation are in balance, but the amount of calcium exchangedper day with the extracellular fluid is relatively small. Boneresorption and bone formation lead to a daily exchange ofapproximately 500 mg of calcium with the extracellular fluid.
1 g/day
Fig. 1. Estimates of calcium balance and amounts of calcium exchangebetween bone, gut, kidney, and soft tissue and the extracellular fluid ina normal adult in zero calcium balance.

144 Nephrology Forum
This amount is less than one-millionth of the total skeletalcalcium. Although bone is a potential major source of calcium,whether acute control of serum calcium is regulated by thebalance between resorption and formation is still unknown.
In contrast, the kidney filters large amounts of calcium, onlyto reclaim the great majority by tubular reabsorption: approxi-mately 10 g cross the glomerulus each day, 98% of which isreabsorbed by the renal tubules. Approximately 65% is reab-sorbed in the proximal tubule, 20% to 25% in the ascending limbof Henle's ioop, and approximately 10% in the distal tubule. Inthe normal individual, fine regulation of calcium reabsorptionoccurs at the level of the distal tubule, primarily under theinfluence of parathyroid hormone. In the proximal tubule,calcium reabsorption probably is not influenced by PTH, butrather is linked to sodium and volume reabsorption.
In the gastrointestinal tract, dietary calcium is absorbedunder the primary influence of 1,25 dihydroxyvitamin D (andindirectly by PTH, which stimulates production of 1,25 dihy-droxyvitamin D by the kidney). Little is known about theregulation of calcium excretion into the gut lumen via intestinaljuices. In normal individuals in calcium balance, net absorptionfrom the gut is equivalent to the amount of calcium excreted inthe urine, and usually is in the range of 150 to 250 mg/day.Calcium exchange also occurs between the extracellular fluidand the soft tissues. This exchange is of course relatively minorcompared with the fluxes that occur across kidney, bone, andgut. Whether the exchange between soft tissues and the extra-cellular fluid is hormonally regulated is not known.
Several aspects of this complex system are important to thepathophysiology of hypercalcemia in malignant disease. (I) Thesystem is highly integrated (even appearing redundant at firstglance) and contains many checks and balances against theoccurrence of hypercalcemia or hypocalcemia. (2) The kidneyhas a considerable, although finite, capacity to protect againstan increase in the entry of calcium into the extracellular fluidsufficient to cause hypercalcemia. The kidney can increasecalcium excretion by about fivefold to maintain normal extra-cellular fluid calcium. Maximal urinary calcium excretion ratesusually are not more than 600 mg/day; in many hypercalcemicpatients, despite a lack of PTH in the circulation, distal renaltubular calcium reabsorption almost certainly is occurring. (3)Bone, an enormous potential reservoir of calcium, could pro-vide an important source of calcium together with calciumabsorbed from the gut. The increased entry of calcium into theextracellular fluid has been termed "through-put" by Nordin,Peacock, and coworkers [5]. In the presence of a three- tofivefold increase in bone resorption rate, "through-put" in-creases, and the kidney's capacity to excrete calcium is over-whelmed.
Pathophysiology of hypercalcemia in primaryhyperparathyroidism
Primary hyperparathyroidism is the commonest cause ofhypercalcemia. Most cases are due to a benign, single parathy-roid gland adenoma that secretes excessive PTH. The serumcalcium is elevated because of both an increase in calciumabsorption from the gut and increased renal tubular calciumreabsorption. The role of bone is unclear. Bone turnover isclearly stimulated, with increases both in bone formation and
bone resorption. Whether net bone resorption occurs in anyindividual patient often is difficult to know. The changes incalcium transport across the gut, kidney, and bone are notcaused by PTH alone, but rather by the combined effects ofPTH and 1,25 dihydroxyvitamin D [6], which is synthesized inthe proximal tubules of the kidney in response to PTH.Hypercalcemia rarely occurs in secondary hyperparathyroid-ism in spite of PTH concentrations far above the normal range,because 1,25 dihydroxyvitamin D concentrations are low.Moreover, the effects of PTH on both bone and kidney arealmost certainly increased by, and in fact may be dependent on,1,25 dihydroxyvitamin D. There is evidence that 1,25 dihydroxy-vitamin D enhances the effects of PTH on calcium reabsorptionin the distal tubule [6], and that l,25D works in concert withPTH on bone [71. Thus hypercalcemia in primary hyper-parathyroidism results not from effects of PTH alone, but ratherfrom the combined effects of PTH and 1,25 dihydroxyvitamin Don kidney and bone and from the effect of 1,25 dihydroxyvita-mm D on the gut.
Pathophysiology of hypercalcemia in malignant diseaseNo type of non-parathyroid malignancy yet described mimics
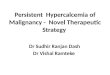
exactly the changes in calcium transport that occur in primaryhyperparathyroidism. In malignant disease, a number of dil-ferent but distinct patterns exist—and possibly more—that haveyet to be fully elucidated. These patterns are representeddiagrammatically in Figure 2. I will discuss three examples inwhich the pathophysiology is different: solid tumors withhypercalcemia, multiple myeloma, and T-cell lymphomas.
Solid tumors and hypercalcemia. The two commonest causesof hypercalcemia of malignancy are lung cancer and breastcancer [8]. The clinical circumstances under which hypercalce-mia occurs in these two conditions are often very different,however. Hypercalcemia can occur early or late in lung cancer,and it may or may not be associated with bone metastases. Incontrast, hypercalcemia in breast cancer usually occurs onlylate in the disease and in patients who have extensive bone andother metastases. The general pathophysiologic disturbance incalcium transport mechanisms may be similar in both types oftumors, but there are probably differences in the humoralmechanisms causing these disturbances.
In lung cancer and related solid tumors associated withhypercalcemia (neoplasms of the kidney, pancreas, ovary, andsquamous cell tumors of the head and neck), hypercalcemia isassociated with increased bone resorption, probably decreasedbone formation, and increased renal tubular calcium reabsorp-tion (for review, see Refs. 2 and 9). Gut absorption of calciumis decreased in those cases in which it has been measured. Therole of humoral and nonhumoral mechanisms in these distur-bances is fiercely debated. Several different tumor factors areinvolved, just as two different humoral factors are involved inthe pathophysiology of hypercalcemia in primary hyperpara-thyroidism. In comparison with normal individuals and patientswith primary hyperparathyroidism, a marked increase in boneresorption must exist in these cancer patients to provide suffi-cient input of calcium into the extracellular fluid (in the pres-ence of the decreased gut absorption of calcium) to cause anincrease in serum calcium. The urinary calcium excretion is inthe same range as that in patients with primary hyperpara-thyroidism, indicating that renal tubular calcium reabsorption is

The hypercalcemia of malignancy 145
Lymphomaci
Lung Cancer—SC +*a7
cAMP
£
Fig. 2. Patterns of abnormalities in calcium transport in patients withdifferent types of hypercalcemia of malignancy. The upper left panelrepresents the abnormalities in myeloma, where increased bone resorp-tion, decreased bone formation, decreased calcium absorption from thegut, and impaired glomerular filtration are associated with hypercal-cemia. The upper right panel indicates the situation in solid tumors,such as lung cancer, which may or may not be associated withmetastases. In this case there is increased bone resorption, decreasedbone formation, increased renal tubular calcium reabsorption anddecreased calcium absorption from the gut. These patients frequentlyhave increased nephrogenous cyclic AMP production. The lower rightpanel shows the situation in breast cancer, which is similar to that inlung cancer except that the patients almost always have bone metasta-ses and usually do not have increased nephrogenous cyclic AMP. Thelower left panel shows the unusual group of patients with variouslymphomas and malignancy who may have increased calcium absorp-tion from the gut because of an increased 1 ,25D concentration inassociation with increased bone resorption.
increased and that the relative increase in bone resorption overbone formation must be considerable to account for thehypercalcemia, given the decreased calcium absorption fromthe gut in this condition. In comparison, patients with primaryhyperparathyroidism have similar increases in the serum cal-cium, but calcium absorption from the gut is increased ratherthan decreased, as in most patients with hypercalcemia ofmalignancy. In malignancy, hypercalcemia usually is steadilyprogressive, unlike primary hyperparathyroidism, in which thelevel of serum calcium can remain constant for many years.Possibly in primary hyperparathyroidism there is still someform of negative feedback, by extracellular fluid calcium onparathyroid hormone synthesis and secretion, as well as possi-bly on the number of PTH-secreting cells, which establishes anew "set-point" for the relationship between serum calciumand PTH secretion different from the normal [10]. This might besimilar to the situation in many patients with pituitary tumors,
in which the secretion of the tumors is constrained by feedbackmechanisms. A good example is Cushing's syndrome due tosmall ACTH-secreting pituitary tumors. These pituitary tumorscan respond to pharmacologic concentrations of cortisol (thebasis of the high-dose dexamethasone suppression test), butwhen the adrenals are removed and only maintenance replace-ment doses of cortisone are given (less than the amounts ofcortisol produced by the abnormal glands prior to removal), thepituitary tumor can grow actively and cause Nelson's syn-drome.
Myeloma. Myeloma almost always is accompanied by in-creased osteoclastic bone resorption and often by hypercalce-mia [11]. The hypercalcemia is associated with increased boneresorption, decreased glomerular filtration, and decreased ab-sorption of calcium from the gastrointestinal tract. In theskeleton, rates of bone formation are usually decreased, and thex-rays show discrete punched-out osteolytic lesions or gener-alized osteopenia with little or no evidence of new boneformation. Reduced bone formation is confirmed by bonescans, which indicate little uptake of the labeled bisphosphon-ate by serum alkaline phosphatase mechanisms, a reliablemeasure of mature osteoblast activity. Impaired glomerularfiltration could be the consequence of a combination of disor-ders including Bence Jones proteinuria, uric acid nephropathy,pyelonephritis, and occasionally amyloidosis. Renal tubularcalcium reabsorption is not increased unless a reversible ele-ment of decreased glomerular filtration is superimposed due todecreased renal blood flow.
T-cell lymphomas. Hypercalcemia occurs much less com-monly in other forms of hematologic malignancy than it does inmyeloma. In one special type, however, it is present in almostall the patients. This disorder is the human T-cell lymphotropicvirus, type-i adult T-cell lymphoma, which is particularlycommon in the southeastern United States, the Caribbean, andJapan. Lymphoid cells carrying this virus produce most of theknown lymphokines [12], and increased bone resorption islikely due at least in part to one or more of the cytokines thatresorb bone. Moreover, we have found macromolecular bone-resorbing activity in cell culture supernatants [13]. An addi-tional mechanism also might be operative in this situation.Some of these patients, as well as some others with lympho-proliferative malignancies and hypercalcemia, have increasedserum concentrations of 1,25 dihydroxyvitamin D, and in-creased calcium absorption from the gut [14]. These findingscontrast with those in other patients with hypercalcemia ofmalignancy, in whom calcium absorption from the gut andserum 1 ,25D concentrations are almost invariably decreased.We have examined lymphoid cells infected with this virus andfound that they have the capacity to convert 25 hydroxyvitaminD to 1,25 dihydroxyvitamin D [15].
Increased bone resorption in hypercalcemia of malignancyBone resorption is increased in patients with hypercalcemia
associated with malignancy. This phenomenon is well docu-mented in histomorphometric studies of bone surfaces, whichshow evidence of increases in osteoclast activity, particularlyon trabecular surfaces [16, 17]. The morphologic changes inbone are different from those of primary hyperparathyroidism,however. In primary hyperparathyroidism, cortical resorp-tion—and particularly subperiosteal resorption—is prominent,
Breast Cancer

146 Nephrology Forum
whereas this form of osteoclastic bone resorption rarely if everis found in malignancy-associated hypercalcemia. Moreover, inmalignancy, rates of bone formation are decreased [161. Thisfinding again contrasts with that in primary hyperparathyroid-ism, in which bone turnover is increased and rates of boneformation are increased. A word of caution is still necessary toavoid overinterpreting the information on rates of bone forma-tion in hypercalcemia of malignancy. Studies on bone formationhave not been controlled by examination of nonhypercalcemiccancer patients; it is possible that the decreased rates offormation observed are due to other factors such as poornutrition, wasting, or immobilization, frequent sequelae inpatients with cancer.
Other clinical evidence indicates that rates of bone resorptionare increased in patients with the hypercalcemia of malignancy.Urinary hydroxyproline is increased, x-rays frequently showsigns of destructive bone lesions (particularly in patients withbreast cancer and with myeloma), and hypercalcemia is almostalways alleviated by drugs that specifically inhibit osteoclasticbone resorption, such as plicamycin (mithramycin) and thenewer bisphosphonates [18].
The notion that increased bone resorption plays a major rolein the pathophysiology of the hypercalcemia associated withmalignancy is confirmed by the demonstration from manystudies of in-vitro bone-resorbing activity in tumor extracts ofculture supernatants of tumor cell lines derived from patients oranimal models of the hypercalcemia of malignancy. The majorarea of controversy in this field is the nature of the humoralmediator or mediators produced by these tumors, and therelative importance of bone resorption compared with othermechanisms, such as increased renal tubular calcium reabsorp-tion, in the pathogenesis of the hypercalcemia. Six factors havebeen proposed as potential mediators of increased bone resorp-tion associated with hypercalcemia. These are the transforminggrowth factors, the parathyroid hormone-like factors, the pros-taglandins, the leukocyte cytokines, 1,25 dihydroxyvitamin D,and colony-stimulating factors. It appears likely that there alsowill be other factors, not yet fully identified, that will beresponsible for hypercalcemia in some tumor types [19].
Transforming growth factors. The tumor-derived transform-ing growth factors, polypeptide stimulators of cell replication,are produced by most, if not all, tumors. Two major classeshave been identified, TGFa and TGF/3. Although interest inTGF/3 and its effects on bone is intense, currently more isknown about the effects of TGFa on bone cell function. Manytumors produce TGFa, including the solid tumors commonlyassociated with hypercalcemia such as squamous cell carci-noma of the lung, head and neck, kidney, and breast. Suchpolypeptides obtained from the rat and human have beenpurified [20, 211 and that from the rat has been synthesizedchemically [22]. The rat and the human genes have been cloned[23, 24], and the human material has been engineered forexpression in E. coli [24]. A 5000dalton peptide, TGFa has asequence of 50 amino acids. However, larger forms also arefound in tumor cell culture supernatants and probably representunprocessed forms of the molecule [25]. The TGFa precursorhas a relatively unique structure without a leader sequence andwith an amino acid configuration, suggesting that it is atransmembrane protein. Release of the precursor from themembrane of the cell might involve a novel proteolytic mech-
Effects of TGFa and PTH on Bone in vitro,TGFa 0PTH
a,Ca
S20
T 60--0
40 //20
C-) b_b I io-io- ioConcentration (M)
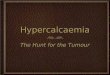
Fig. 3. Effects of recombinant human TGFa and parathyroid hormoneon parameters of bone resorption and bone formation in vitro. Recom-binant human TGFa was obtained from Dr. Rik Derynck fromGenentech, Incorporated [30]. PTH was bovine PTH (1—84). FRLBrepresents fetal rat long bones, in which bone resorption is assessed bythe release of previously incorporated 45Ca over 72 hours of organculture. NMC represents neonatal mouse calvaria that also have beenprelabeled with 45Ca and cultured in the presence of the bone-resorbingfactor for periods of 72 hours. Alkp'ase is alkaline phosphatase contentin cells with osteoblast characteristics assessed as the percentagedecrease in response to TGFa and PTH. Coil synth is the percentage ofinhibition of collagen synthesis measured as collagenase-digestibleprotein in fetal rat calvarial organ cultures.
anism, possibly directed by an oncogene [23]. Epidermalgrowth factor (EGF) receptor binds TGFa, and the peptideprobably mediates all its effects through this receptor [26, 27].TGFa causes all the known biologic effects of EGF, andevidence indicates that its binding site on the EGF receptor issimilar or even identical to that of EGF, in spite of an aminoacid homology with EGF that is not more than 40%; however,both molecules contain a similar conformation and threedisulfide bonds. The close overlap of the biologic effects ofTGFa with those of EGF was the rationale for our investigationof the role of TGFa in the bone destruction associated withmalignancy. Both the synthetic and recombinant forms havepowerful effects on bone cell metabolism [27—30]. They clearlystimulate osteoclastic bone resorption in both neonatal mousecalvaria and fetal rat long bones (Fig. 3). The effects on neonatalmouse calvaria are mediated by prostaglandins and can beinhibited by indomethacin, although osteoclastic bone resorp-tion in fetal rat long bones is not affected by indomethacin [28,301. Identical results are found in both of these systems withEGF. However, in our hands, osteoclastic bone resorptionoccurs at concentrations at least one order of magnitude lowerthan those of EGF [301. The effects of TGFa also are importantin in-vitro systems for bone formation. It is a powerful inhibitorof collagenase-digestible protein synthesis in fetal rat calvariaand inhibits the alkaline phosphatase content of rat osteosarco-ma cells with the osteoblast phenotype [30]. In fetal rat calvaria,TGFa stimulates DNA synthesis [30]. Its actions on osteoclas-tic bone resorption may be mediated by effects on osteoclastprogenitors; we found in our long-term marrow culture systemthat TGFa stimulates increased formation of cells withosteoclast characteristics by increasing proliferation of mono-nuclear cells [31]. The stimulatory action in this system occurs
60
40
3.0
2.0-IU- 1.0
10—10 I bo_8io io

The hypercalcemia of malignancy 147
in concentrations as low as 0.01 ng/ml, the lowest concentrationof TGFa yet known to produce a biologic effect in any system.
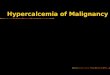
Strong evidence suggests that TGFa plays an important rolein the increased bone resorption associated with some tumors.The most thoroughly studied model has been the rat Leydig celltumor, which occurs in 50% of aged Fischer rats and can becarried in culture or transplanted subcutaneously [32]. The ratsbecome rapidly hypercalcemic over 3 weeks and have most ofthe characteristics of the humoral hypercalcemia of malignancyseen in patients with solid tumors. Leydig tumors produce bothbone-resorbing activity and TGFa activity, which co-elutesfrom gel filtration columns [33]. The Leydig tumor expressesTGFa mRNA excessively. In fact, it expresses TGFa incomparable amounts to the FeSV tumor from which TGFa waspurified and the gene cloned. Moreover, the bone-resorbingactivity present in Leydig tumor cell culture supernatants canbe blocked by neutralizing antibodies to the EGF receptor [34,35]. These antibodies, supplied by Dr. Graham Carpenter atVanderbilt University, are of two types, one that binds to theEGF binding site and blocks the biologic effects of EGF andTGFa, and another that is separate from the EGF binding siteand does not block the biologic effects of EGF or TGFa. Wehave found that the antibodies that bind to the EGF binding siteinhibit the bone-resorbing activity produced by the Leydigtumor, but that the antibodies that do not block the effects ofTGFa have no effect on the bone-resorbing activity (Fig. 4A,4B). We also have obtained similar results in several othertumors associated with hypercalcemia. A human squamous cellcarcinoma of the lung, which has been well characterized anddescribed by Kukreja, Abramson, and associates at the Univer-sity of Chicago, expresses TGFa excessively, and the bone-resorbing activity also is blocked by the antibody to the EGFreceptor [36]. We have examined two other tumors, the ratFeSV tumor and the human melanoma A532. These are thetumors, respectively, from which rat and human TGFa wereoriginally purified and, in the case of the FeSV tumor, fromwhich the gene for rat TGFa was cloned. We found that animalscarrying either of these tumors develop hypercalcemiá.
In most of these tumors, the major bone-resorbing factor islarger than the smallest form of TGFa. To my knowledge, allthe tumor systems producing TGFa produce larger-molecular-weight forms, which probably represent unprocessed largerforms of the TGFt molecule [24]. It is now well recognized,however, that other proteins in addition to EGF and TGFamight bind to the EGF receptor and mediate their effectsthrough the EGF receptor. The most recently characterized isthe vaccinia virus protein, which is similar in size to the largerforms of TGFa, but which has a similar conformation to TGFaand EGF and which seems to bind to, and mediate its effectsthrough, the EGF receptor [37].
Although different from those of TGFa, the effects of TGFI3on bone also are interesting. Transforming growth factor 13 is ahomodimer of 25,000 daltons and is secreted by most, it not all,rapidly replicating cells (for review, see Ref. 38). One of itsmost abundant sources in the human is the normal platelet, butTGF13 also has been found in bone, placenta, and kidney. Thereare two different forms found in bone, a major form and a minorform of smaller molecular weight [39, 40]. These proteins haveimportant effects not only on bone cell function but also oncartilage cells. They stimulate chondrocyte mitogenesis and
TCM TCM 1CM TCM TCM TCM TCMTCM TCM EGF EGF EGF+ + + + + + + +Ab Ab Ab Ab Ab Ab Ab Ab451 310 451 310 451 310 451 310
Experiment 1 Experiment 2 Experiment 3
Fig. 4. Effects of antisera to the EGF receptor on bone-resorbingactivity due to the Leydig cell tumor. A Antisera 451, which blocks EGFand TGFa biologic activity, inhibits the bone-resorbing activity pro-duced by the Leydig cell tumor. B Antisera 310, which does notinterfere with EGF binding or the biologic activity of EGF or TGFa,has no effect on the bone-resorbing activity produced by the Leydigtumor (From Ref. 35).
increase proteoglycan synthesis [41]. On osteoblasts they stim-ulate alkaline phosphatase content in osteoblast-like osteosar-coma cells and DNA synthesis in fetal rat calvaria. No effectshave yet been shown on osteoblast collagen synthesis. How-ever these prnteins stimulate fibroblast collagen synthesis andmight be important in wound healing [42]. They stimulate boneresorption in mouse calvaria by increasing prostaglandin syn-thesis [281, although homogenous purified preparations havenot yet been shown to stimulate osteoclastic bone resorption in
PTH PTH+
1/300
TCM 1CM+ +
1/1000 1/3000
Dilution of Ab 451
TCMI1CM
+1/300
A2.0
1.8
1.6
1.4
1.2
1.0
0.8
B2.0
1.8
1.6
1.4
1.2
1.0
0.8
a)
Cea)1)
00Ce
0C0
C)
CeCe
I-
a)
a)Ce
CeC)
00Ce
2C0
C)
Cea,I-
EGF EGF+
1/300

148 Nephrology Forum
fetal rat long bones. Thus, whether tumor-derived TGF/3 is animportant mediator of the effects of tumors on the skeleton hasyet to be shown,
Parathyroid hormone-like factors. Parathyroid hormone-likefactors are macromolecular proteins that are operationallydefined by their capacity to bind to PTH receptors in vitro.They have been assayed in two ways, either by their capacity tostimulate adenylate cyclase in target cells [43—45], or by theircapacity to stimulate G6PD content in renal tubular cells [46].Both of these effects can be inhibited by synthetic antagoniststo PTH. It is assumed that they bind to the PTH receptor, butit remains conceivable that these factors could affect thereceptor without binding to it. Parathyroid hormone-like factorsare produced by many tumors associated with the hypercal-cemia of malignancy and are produced by normal keratinocytes[47]. The increase in nephrogenous cyclic AMP found in manypatients with the humoral hypercalcemia of malignancy pre-sumably is due to these factors. Although some tumors thatproduce these factors also exhibit bone-resorbing activity, suchactivity does not appear to be mediated through the PTHreceptor, because it is not inhibited by synthetic chemicalantagonists to PTH [48]. This finding is not surprising in thecase of the Leydig tumor, because this tumor produces largeamounts of TGFa, and the bone-resorbing activity is blockedby antisera to the TGFa!EGF receptor [35]. Similar activity hasbeen found in tumors of patients with oncogenic osteomalacia[49]. The relationship among the PTH-like factors found intumors with oncogenic osteomalacia, in keratinocytes, and insolid tumors associated with hypercalcemia remains to beclarified. These factors have been partially purified, and therange of molecular weights is between 10,000 and 30,000daltons [44, 50]. These factors do affect the renal tubule as wellas isolated bone cells, and it is likely that they may work inconcert with other factors in the pathophysiology of thehypercalcemic syndrome. Some paradoxes remain, however.Tumors associated with production of these PTH-like factorsare not associated with the same abnormalities in calciumtransport across gut, kidney, and bone that are seen in primaryhyperparathyroidism. For example, in patients with solid tu-mors, gut absorption of calcium usually is decreased and 1 ,25Dsynthesis is decreased, in contrast with what occurs in primaryhyperparathyroidism. One possible explanation for this appar-ent discrepancy is that there are several classes of PTHreceptors [51, 521. Another possibility is that the other factorsproduced by tumors associated with the hypercalcemic syn-drome oppose some of the PTH-like effects on either bone orkidney. Clarification of these discrepancies will require furtherinvestigation.
Prostaglandins. Prostaglandins of the E series (PGEs) resorbbone in vitro, and infusions, albeit in large amounts, canincrease serum calcium [53, 541. These observations suggest arole for PGEs in the hypercalcemia of malignancy, and inspecial situations these mediators probably are important.Convincing evidence indicates that PGEs are important inseveral animal models, namely the HSDM mouse fibrosarcomaand the rabbit VX2 carcinosarcoma [55, 56]. In these animalmodels, cultured tumor cells produce PGEs and stimulatebone-resorbing activity; the PGE synthesis and the stimulatedbone-resorbing activity are inhibited by treatment with indo-methacin. Similarly, hypercalcemia in the animals is alleviated
by indomethacin therapy. In no similar human system has a rolefor prostaglandins been convincingly demonstrated. Most pa-tients with the hypercalcemia of malignancy do not respond toindomethacin or related drugs [18]. However, in special situa-tions in human malignancy, prostaglandins can mediate boneresorption. For example, in metastatic breast cancer, the serumcalcium level can increase acutely following treatment withestrogens or tamoxifen. When breast cancer cells with estrogenreceptors are incubated in vitro with estrogens or tamoxifen,the cells release bone-resorbing activity, which appears to bePGEs, as production of this activity is inhibited by indometh-acm administration [57]. Moreover, these agents cause thetumor cells to release PGE [57].
The effects of TGFa on human bone cells also might involveprostaglandin synthesis. In organ cultures of mouse calvaria,for example, TGFa-induced bone resorption is inhibited byindomethacin [28, 30]. But in fetal rat long bones, an alternativeorgan culture system, TGFa stimulates bone resorption inde-pendent of prostaglandin synthesis [27, 30]. Which of these twosystems is more applicable to human bone resorption is un-known, but indirect production of prostaglandins could beimportant. In 1975, Seyberth Ct al demonstrated that PGEmetabolites were excreted in increased amounts in some pa-tients with the humoral hypercalcemia of malignancy [581. Thesource of these prostaglandins, the mechanism for their produc-tion, and their effects on calcium homeostasis have still to bedetermined. They might be produced, for example, in targetcells in bone and kidney in response to agents such as thetransforming growth factors. However, whether they play arole in the pathogenesis of hypercalcemia remains to be dem-onstrated.
Cytokines. When peripheral blood leukocytes are activatedby an antigen or a mitogen such as phytohemagglutinin, bone-resorbing activity known as osteoclast activating factor (OAF)appears in the culture supernatants [59]. Similar bone-resorbingactivity is released by myeloma cells [60] and by malignantlymphoid cell lines [61]. These observations have suggestedthat the bone destruction in certain hematologic malignancies isthe consequence of OAF release by the malignant cells. Al-though many of the biologic effects of this activity on bone invitro were described throughout the 1970s, final identificationand isolation of its mediators remained difficult, as with all theother known lymphokines and monokines. The advent of thebiotechnology revolution in the 1980s and the interest of thebiotechnology companies in cytokines that have potential ther-apeutic applications have led to significant advances in theunderstanding of bone destruction. It is apparent now that anumber of cytokines resorb bone and thus are potential mem-bers of the OAF family. Several of these factors now haveclearly been documented, including interleukin-l (both alphaand beta molecules) [62—64], lymphotoxin, and tumor necrosisfactor [65]. In short-term phytohemagglutinin-activated leuko-cyte cultures, interleukin-l probably is the mediator; Dewhirstand colleagues found that the bone-resorbing factors in theseculture supernatants had a partial amino acid sequence identicalto the interleukin-l molecule of p1 7 [661. In our hands, lym-photoxin, tumor necrosis factor, and interleukin-l are equallypotent in the bone-resorption assay systems. The mediator ofOAF activity in any leukocyte culture supernatant may dependon the conditions of the leukocyte culture, such as cellular

The hypercalcemia of malignancy 149
composition of the leukocytes, duration of the culture, andmechanisms of stimulation. Cytokines are potential mediatorsof the bone destruction associated with malignant lymphoidcells. In fact, we recently found that human myeloma cellsfreshly isolated or in culture express both lymphotoxin andtumor necrosis factor mRNA, although only lymphotoxin issecreted [65]. All the bone-resorbing activity stimulated bythese cultured cells in vitro could be inhibited by specificmonoclonal antibodies to lymphotoxin. Lymphotoxin thus isthe mediator in these particular culture systems. Whetherlymphotoxin will prove to be the mediator of bone destructionin all patients with myeloma or in other types of hematologicmalignancy is unknown but probably is unlikely. It is possiblethat many hematologic malignancies involving monocytic cellsmay release interleukin-l or tumor necrosis factor as themediators of bone destruction.
1,25 Dihydroxyvitamin D. The metabolite 1,25 dihydroxyvi-tamin D is produced in the proximal tubule of the kidney inresponse to PTH or decreased ambient phosphate concentra-tion [671. A few cases of hypercalcemia associated withlymphoid malignancies in which circulating concentrations of1 ,25D are increased have been documented, yet neither in-creased PTH nor reduced phosphate levels are involved [14,68—70]. This finding contrasts with the vast majority of cases ofthe hypercalcemia of malignancy, in which 1 ,25D is decreasedin the plasma, and calcium absorption from the gut is similarlydecreased. The lymphoid malignancies associated with in-creased 1 ,25D concentrations include adult T-cell lymphomaand Hodgkin's disease. Some of the cases of adult T-celllymphoma have been associated with the HTLV-l type-Cretrovirus infection. We have examined cultured lymphoid cellsinfected with this virus; these cells act in every way like thelymphoma cells carrying the virus [71, 72]. Using co-elution ina number of chromatographic systems and definitive massspectrometry, we found that these cells in vitro can convertlabeled 25 hydroxyvitamin D to 1,25 dihydroxyvitamin D [73].In adults with T-cell lymphoma, 1 ,25D might be only part of themechanism for hypercalcemia. These cells also release a bat-tery of lymphokines that could be involved in the increase inbone resorption [74]. Moreover, serum 1 ,25D concentrationsusually are normal in hypercalcemic patients with HTLV type-imalignancies (Matsumoto T, personal communication).
In addition to this list of bone-resorbing lymphokines andmonokines released by normal and malignant immune cells,lymphoid cells also release factors that could inhibit boneresorption. Among these is gamma interferon, a powerfulinhibitor of osteoclastic bone resorption [75, 761. In our hands,gamma interferon is more effective in inhibiting bone resorptionstimulated by cytokines such as lymphotoxin, tumor necrosisfactor, and interleukin- 1 than it is in inhibiting bone resorptionstimulated by PTH. The effects of gamma interferon might bemediated via effects on cell differentiation rather than oncellular proliferation [77]. This finding might prove importantbecause if it can be confirmed in vivo, gamma interferon wouldbe a potentially useful agent in the treatment of hypercalcemiaor of increased bone resorption due to mediators such as thecytokines.
Colony-stimulating factors. A number of cases of the hyper-calcemia of malignancy that are associated with marked leuko-cytosis have been well documented [78, 80]. When tumors from
these patients have been innoculated in nude mice, the micedevelop hypercalcemia and leukocytosis. Moreover, the tumorextracts contain colony-stimulating factors of the granulocyte-macrophage type [81]. This colony-stimulating activity has notbeen fully characterized yet, although preliminary results sug-gest that it might be separate from the bone-resorbing activity[82]. These observations are of intense interest from severalpoints of view. First, CSF- 1 (the lineage-specific colony-stim-ulating factor for cells of the monocyte family) and CSF-GMboth stimulate proliferation of mononuclear cells in long-termmarrow cultures. These mononuclear cells are precursors of,and increase the formation of, these osteoclast-like cells [82].Second, Wiktor-Jedrzejczak and colleagues have shown that inthe opiop variant of mouse osteopetrosis, a deficiency exists inthe production of colony-stimulating activity by stromal mar-row fibroblasts [83]; this deficiency presumably is responsiblefor the decreased formation of osteoclasts. Third, in the meta-tarsal culture system developed by Burger and coworkers [84],osteoclast formation depends on the presence of a source ofcolony-stimulating activity. Fourth, since there is a large bodyof evidence, albeit controversial, that osteoclasts are derivedfrom cells of the monocyte-macrophage family, it is conceivablethat production of the colony-stimulating factors by tumor cellscould lead to both an increase in leukocyte colony formation aswell as to an increase in osteoclast formation. Neverthelesssome perplexing and unexplained issues remain. In all the casesof which I am aware, the leukocytosis is represented by agranulocytosis and not a monocytosis. Potential connectionsbetween granulocytes and osteoclasts are unclear. Also thisassociation of leukocytosis and hypercalcemia is relativelycommon in Japanese patients but is rare in the United States; tomy knowledge it has not been reported elsewhere in the world.The reasons for these apparent geographic or ethnic differencesare unknown. Studies of individual tumors associated withthese two presumably paraneoplastic syndromes, leukocytosisand hypercalcemia, might lead to insights into the control ofosteoclast formation and the relationships between osteoclast-opoiesis and hematopoiesis.
The mechanisms for increased bone resorption in malignantdisease are complex and likely to be heterogeneous. In manytumors it is likely that several factors act in concert on bone.For example, in some solid tumors the transforming growthfactors and PTH-like factors might work together synergisti-cally to affect bone resorption, as already has been demon-strated in vitro for PTH and EGF [85]. Moreover, these factorsmight be exerting their effects not just on bone but on other sitesthat control regulation of serum calcium, such as kidney andbone.
The role of the kidney in hypercalcemia of malignancyThe kidney has long been considered central in the patho-
physiology of hypercalcemia by European investigators, but ithas been relatively ignored until recently by Americans. Thekidney probably plays an extremely important role in thepathogenesis of hypercalcemia, producing its effects by changesin glomerular filtration or renal tubule calcium reabsorption.Decreased glomerular filtration in the presence of increasedbone resorption could lead to an increase in serum calcium bysimple impairment of the kidney's capacity to clear ultrafilter-able calcium. Glomerular filtration rate is decreased in many

150 Nephrology Forum
patients with hypercalcemia because of volume depletion (dueto emesis, poor intake, misuse of loop diuretics, etc.) as well asthe renal hemodynamic effects of hypercalcemia itself. In somepatients, particularly patients with myeloma, the impairment inglomerular filtration can be due to other causes such as BenceJones nephropathy, uric acid nephropathy, or pyelonephritis[86]. When prerenal azotemia is present, decreased glomerularfiltration in turn leads to increased proximal renal tubularsodium and calcium reabsorption. In myeloma, evidence sug-gests that the patients with the most extensive bone destructionhave the highest level of OAF production in vitro by themyeloma cells, but no positive correlation exists between OAFproduction and the serum calcium [871; other factors (such asdecreased glomerular filtration) thus probably are involved inthe pathogenesis of hypercalcemia.
There is additional mounting evidence pointing to an increasein renal tubule calcium reabsorption in many patients with solidtumors and hypercalcemia. The evidence comes from a numberof clinical studies, the first recorded by Peacock et al [881; theseinvestigations have confirmed that patients with solid tumorsand the hypercalcemia of malignancy have net tubular reab-sorption of calcium similar to that in primary hyperpara-thyroidism. This information is derived from observations onserum calcium and renal calcium excretion in patients withhypercalcemia. In normal individuals, there is a curvilinearrelationship between ultrafilterable calcium and renal calciumexcretion [88—90]. For any given ultrafilterable calcium, a levelof renal calcium excretion below the normal range indicates anincrease in net tubular calcium reabsorption, provided glomer-ular filtration is normal. Although there are several limitationsto these observations in hypercalcemic patients, neverthelessthe overall conclusions are probably correct. The limitations(reviewed in Ref. 90) are that (1) in most studies the total serumcalcium, rather than ultrafilterable calcium, has been measured(this limitation is not likely to alter significantly the conclusionsof most studies); (2) glomerular filtration is often impaired inthese patients (because of dehydration or hypercalcemia perse); and (3) saline infusions used in the management alter renaltubular calcium handling. In spite of these problems, theobservation that net renal tubular calcium reabsorption isincreased has been made so frequently that it seems almostcertain to be correct.
The mechanism for this putative increase in renal tubularcalcium reabsorption is controversial. Bijvoet and coworkersbelieve that it is predominantly due to sodium-linked calciumreabsorption in the proximal tubule that is associated withdecreases in glomerular filtration, although in their hands somepatients with carcinomas of the kidney or lung had an additionalspecific effect on the renal tubule (personal communication). Incontrast, other groups believe that a tumor factor promotesrenal tubule calcium reabsorption [9 1—96]. If tumor factorsincrease renal tubule calcium reabsorption, it will be interestingto determine which factors work in this way and what their sitesof action are. If the PTH-like factors mimic the effects of PTHon the kidney, as seems likely at least in some instances, thenwe would expect distal renal tubule calcium reabsorption to beincreased. However, as has been noted before, only some of theeffects of PTH on the kidney can be ascribed to PTH-likefactors. Some findings, such as the decreased 1 ,25D concentra-tions, are opposite to what is seen in primary hyperpara-
thyroidism. Also, the transforming growth factors could beaffecting the kidney, thereby promoting calcium reabsorption.Epidermal growth factor promotes sodium and hydrogen ionexchange [97]. Both EGF and TGFa could be anticipated to acton the proximal tubule of the kidney, causing sodium and waterreabsorption. Because calcium reabsorption in the proximaltubule is linked to sodium reabsorption, calcium reabsorptionprobably would be promoted by EGF, and because all theeffects of EGF mimic those of TGFa, it is possible that TGFacould be producing similar effects on the renal proximal tubule.Elucidation of the effects of tumor products on renal tubularcalcium handling will require in-vitro studies using the sophis-ticated techniques now available to renal physiologists. Thisinvestigative area appears to be potentially productive and evenmight lead to an improved understanding of the control ofnormal renal tubular calcium handling.
Granted that increased net renal tubule calcium reabsorptionis an important factor in some patients with hypercalcemia, asappears incontrovertible now from the available evidence, themajor question is its relative importance compared with otherfactors such as increased bone resorption. One group hasattemped to develop an algorithm for determining the relativeimportance of increased renal tubule calcium reabsorption,bone resorption, and decreased glomerular filtration [94]. Thisalgorithm is a thoughtful attempt to sort out these complicatedissues in a setting made complex because of the limitations ofthe measurements that can be made [91].
Role of the gutIn normal adults in calcium balance with a stable serum
calcium, net calcium absorption from the gut is balanced byurinary calcium excretion. In the great majority of patients withthe hypercalcemia of malignancy, absorption of calcium fromthe gut is decreased, as are circulating 1 ,25D levels [98]. In spiteof this decrease in entry of calcium into the extracellular fluid,in most patients the serum calcium rises progressively. Thisincrease clearly indicates that the relative increase in boneresorption and decrease in calcium clearance by the kidneysmust be substantial. For example, these changes must becomparatively much greater than the increase in bone resorp-tion and decreased clearance of calcium by the kidneys that arepresent in primary hyperparathyroidism, in which calciumabsorption from the gut is increased. Although most tumors areassociated with decreased calcium absorption from the gut,several exceptions have been well documented. One has al-ready been mentioned, namely the lymphoid malignanciesassociated with an increased circulating I ,25D concentration.Another is a variant of the VX2 carcinosarcoma in the rabbit, inwhich increased calcium absorption from the gut was clearlydemonstrated [99]. In fact, in most of the animal models of thehumoral hypercalcemia of malignancy, calcium absorption fromthe gut is not decreased as it is in humans, but increased [44,81]. This increase also occurs in some tumors in humans and innude mice. The same tumor in humans that causes decreases incalcium absorption and l,25D concentration may cause anincreased 1 ,25D concentration in the nude mouse. The reasonsfor these disparate results are not known. One possibility is thatin spite of the production of PTH-like factors and phosphatewasting, which would stimulate 1,25D synthesis in a normalindividual, other factors produced by the tumor might be

The hypercalcemia of malignancy 151
interfering with this response. The only explanation for differ-ences in behavior of the same tumor in the patient from whomit was derived and in an athymic rodent is that the effects of thetumor factors might be species-specific for some target organs,and thus might impair 1 ,25D concentration in humans but not inrodents. Whatever the explanation, in most circumstances thegut does not play an important role in the pathophysiology ofhypercalcemia of malignancy.
SummaryIn summary, the hypercalcemia of malignancy is mediated by
complex and heterogeneous mechanisms. Once thought of as asimple paraneoplastic syndrome mediated by the effects oftumor production of PTH [100], it is now clear that multiplemechanisms are involved and that these mechanisms involveabnormalities in calcium transport in bone, kidney, and gut.Calcium homeostasis in normal individuals is complex andtightly regulated. Although much has been learned over the last20 years about the effects of individual hormones on targetorgans, much remains to be understood about how thesehormonal systems interact to control extracellular fluid cal-cium. Future studies on disturbances in calcium homeostasis,such as that occurring in association with malignant disease,should do much to clarify how these complex hormonal mech-anisms function in the normal individual.
Questions and answersDR. JOHN T. HARRINGTON (Chief, Department of Medicine,
Newton-Wellesley Hospital, Newton, Massachusetts): Dr.Mundy, do we know the precise site of the increase in renaltubular calcium reabsorption? Also, what is the relative contri-bution of the kidney to the hypercalcemia of malignancy?
DR. MUNDY: We do not know where in the renal tubule theincreased calcium reabsorption occurs. It would be attractive topostulate that it occurs in the distal tubule in those cases inwhich PTH-like factors are involved. But so far no one hasstudied the tubular site of increased calcium reabsorption.Unfortunately, we do not know the relative importance of therenal effects. John Kanis and his colleagues in Sheffield havetried to develop an algorithm to assess the relative contributionsof bone resorption, impaired glomerular filtration, and in-creased renal tubular calcium reabsorption in hypercalcemicpatients with breast cancer [94]. Their estimates are that therenal tubules may be responsible for approximately 30% of theincrease in serum calcium in the hypercalcemia of breastcancer,
DR. JEROME P. KASSIRER (Associate Chairman, Departmentof Medicine, New England Medical Center Hospitals, Boston,Massachusetts): Does hypercalcemia result from the physicaldestruction of bone by direct tumor invasion, or is there alwaysan interpolated humoral mechanism?
DR. MUNDY: A number of years ago I thought that it waslikely that there was a direct cellular effect, and we showed thathuman breast cancer cells could resorb devitalized bone in vitroindependent of osteoclasts [101]. However, when we and Dr.Alan Boyde of University College, London, later examinedbone surfaces from patients with metastatic cancer using scan-ning electron microscopy, all we found was evidence ofosteoclastic resorption. There was no indication of non-osteo-clast-mediated resorption. I now suspect that the osteoclast is
the sole cellular mediator of bone resorption in metastaticmalignancy. If a direct tumor cell mechanism is involved, itprobably plays a minor part.
DR. MICHAEL KAPLAN (Endocrinology Division, New En-gland Medical Center Hospitals): In patients with myeloma,there is no coupling of increased bone formation with boneresorption. Do these studies explain that finding? Second, whataccounts for the difference between the rodent models and thehuman with solid tumors, as far as 1,25 dihydroxyvitamin Dproduction is concerned?
DR. MUNDY: You raise an extremely interesting and impor-tant issue. The abnormalities in bone remodeling that occur inmyeloma are different from those in other tumors. Myeloma ischaracterized by marked impairment of bone formation despitethe increase in bone resorption. In other words, the couplingmechanism that normally links bone formation to bone resorp-tion seems to be disrupted. We do not know why this uncou-pling occurs, but the cytokines released by myeloma cells thatresorb bone probably are unable to trigger the same sort ofremodeling sequence that occurs, for example, in states ofparathyroid hormone excess. As you said, there are differencesbetween the rodent models and humans with respect to 1,25dihydroxyvitamin D production. In the rodent models, 1,25dihydroxyvitamin D production is not suppressed, in contrastwith humans with solid tumors. We don't know why there aredifferences in the regulation of 1—hydroxylase activity in dif-ferent species. The situation is even more complex, becausenude mice carrying human tumors do not have suppressed 1,25dihydroxyvitamin D concentrations, whereas before surgicalexcision of the same tumors, the patients carrying these tumorshave had low serum 1,25 dihydroxyvitamin D concentrations.The regulatory mechanisms responsible for these differencesare not understood, however.
DR. NIcoLAos E. MADIAS (Chief, Division of Nephrology,New England Medical Center Hospitals): Recent experimentalevidence suggests that, under some circumstances, the level ofplasma calcium concentration is an important modulator of theplasma level of 1,25 dihydroxyvitamin D [1021; changes inplasma calcium produced changes in vitamin D3 in the oppositedirection, at times overriding opposing influences by plasmaphosphorus concentration and PTH. In your opinion, do thesedata provide any additional insight into the pathogenesis of thedepressed vitamin D3 level accompanying the hypercalcemia ofmalignancy?
DR. MUNDY: The observations made by Hulter et al dosuggest that long-term control of the 1,25 dihydroxyvitamin Dconcentration might be influenced by the level of plasmacalcium as well as by other factors such as parathyroid hormoneand serum phosphorus concentrations. It is conceivable that thesuppression of the 1,25 dihydroxyvitamin D concentration inthese tumors in humans could be related to the serum calciumconcentration, but that does not explain why the 1,25 dihy-droxyvitamin D concentration should not be suppressed in therodent models or why the 1,25 dihydroxyvitamin D concentra-tion is often increased in patients with primary hyperpara-thyroidism.
DR. HARRINCTON: Is there any potential therapeutic use ofmonoclonal antibodies directed either at transforming growthfactors or their receptors?
DR. MUNDY: Not at present, although such approaches might

152 Nephrology Forum
be possible in the future. No antibodies currently are availablethat can neutralize biologic activity due to TGFa. Antibodies tothe receptor have been useful in our in-vitro studies, but theseantibodies are not available for in-vivo studies either. If anappropriate antibody that could neutralize biologic activitywere available in sufficient amounts, it might be possible to useit in this way.
DR. MADIAS: Could you please summarize the principles oftreatment of the hypercalcemia of malignancy?
DR. MUNDY: The principles of treatment are first, control theunderlying disease ii possible, and second, lower the serumcalcium with the use of therapies that promote urinary calciumexcretion or inhibit bone resorption. The choice of agentsdepends on the severity of the hypercalcemia and whether thepatient is symptomatic.
For patients with severe hypercalcemia and with a correctedserum calcium concentration greater than 13 mg/dl, urgenttreatment is required. I prefer to use normal saline and thecombination of calcitonin and glucocorticoids in this situation.Normal saline promotes a sodium diuresis, and because renaltubular handling of calcium and sodium is linked, the sodiumdiuresis is accompanied by a calcium diuresis. Moreover, manypatients are dehydrated at the time of admission, so fluidreplacement is necessary for this reason alone. Calcitonin andglucocorticoids in combination are effective in up to 75% ofpatients with severe hypercalcemia. These nontoxic agentsinhibit bone resorption and are particularly useful in patientswith hematologic malignancies who have impaired renal func-tion. The other drugs that can be used for severe hypercalcemiaare loop diuretics, mithramycin, and intravenous phosphate.Loop diuretics such as furosemide will enhance urinary calciumexcretion but they must be used in very large doses (100 mgevery 1—2 hours) and their use may lead to other electrolyteproblems. They should not be used until rehydration is com-plete. I believe that the benefits they add over those of normalsaline alone are not sufficient to warrant their use, unlesspatients are overhydrated or have cardiac failure. Mithramycinacts less rapidly and is potentially dangerous in patients withimpaired renal function because it is nephrotoxic and dependson the kidney for its clearance. It usually is effective, and worksby inhibiting bone resorption. Intravenous phosphate is evenmore hazardous because of the danger of soft tissue calcifica-tion.
For less urgent therapy in the patient who is ambulant, thechoices are wider. Oral phosphate can be useful in patients whohave normal renal function and a serum phosphorus less than4.0 mg/dl. Some patients are unable to tolerate this therapybecause of diarrhea. Corticosteroids work in about 30% ofpatients and are most effective in patients with hematologicmalignancies. Either mithramycin or calcitonin and corticoste-roids in combination can be used in ambulant patients, but thesetherapies are inconvenient because they have to be givenparenterally. I predict that in the future the most widely usedagent will be one of the new bisphosphonates that currently arebeing developed. These agents are used extensively in Europeand have proved effective. None is available in the UnitedStates at present that is effective when given orally to patientswith the hypercalcemia of malignancy.
DR. MICHAEL P. MADAIO (Division of Nephrology, NewEngland Medical Center Hospitals): How do corticosteroids
reverse hypercalcemia? Specifically, could you comment ontheir effect on bone and tumor cells?
DR. MUNDY: Corticosteroids in pharmacologic doses inhibitbone resorption. This effect has been shown in organ culturestudies for many years. Steroids are particularly effective inlowering serum calcium in patients with hematologic malignan-cies, but are much less effective in hypercalcemia associatedwith parathyroid hormone excess. It appears likely thatcorticosteroids inhibit bone resorption by interfering with theformation of mature osteoclasts from precursor cells.
DR. KAPLAN: What about the long-term use of calcitonin withsteroids?
DR. MUNDY: Calcitonin and corticosteroids can be usedchronically. This combination is not very convenient for long-term therapy because calcitonin has to be given by injection.However, it can be a good form of therapy in specific situations.For example, in a patient with myeloma and fixed impairment ofrenal function, the choice of agents is limited if corticosteroidsalone are ineffective. In this situation, calcitonin can be usedeffectively with corticosteroids for a number of months [81.However, patients will still tend to relapse unless calcitonin iswithdrawn from time to time. One schedule we have foundconvenient is giving the patient corticosteroids daily but with-drawing calcitonin over the weekends [8].
DR. MADIAS: Are any of the factors you were discussingimportant for normal calcium homeostasis?
DR. MUNDY: It is hard to know whether any of the tumorproducts are important in normal calcium homeostasis. There isno evidence that any of them are controlled by the circulatingconcentration of calcium by a negative-feedback mechanism. Itis likely, however, that some of these tumor factors producedby their normal cellular counterparts are important for normalskeletal homeostasis and in the control of osteoclast activityduring normal bone remodeling.
DR. KASSIRER: How carefully has the "other side of thecoin" been studied? That is, what is the mechanism of calciumdeposition and occasional hypocalcemia in patients withosteoblastic metastases?
DR. MUNDY: This disorder is much less common than ishypercalcemia. Nevertheless, some tumors are associated withthe production of factors that stimulate osteoblast activity andnew bone formation, and occasionally these tumors are associ-ated with hypocalcemia. We have found that prostatic cancertissue sometimes produces a factor that stimulates osteoblastactivity in vitro [1031. Of course there is great interest inidentifying factors that stimulate bone formation, because thesesubstances might lead to therapies for patients with diseases ofbone loss.
Note added in proof
Since presentation of this Forum, two papers reporting laboratorystudies on the Leydig model of hypercalcemia of malignancy haveclearly documented the importance of renal tubular calcium reabsorp-tion [104, 105].
AcknowledgmentsThe author is grateful to a number of collaborators who have helped
in these studies including Donald Bertolini, Sharyn D'Souza, RikDerynck, James Dunn, Dianne Fetchick, Maxine Gowen, GloriaGutierrez, Kenneth Ibbotson, Michael Katz, David Lee, David Rood-man, George Todaro, Daniel Twardzik, Alex Valentin, and Toshiyuki

The hypercalcemia of malignancy 153
Yoneda. The work reported here was in part supported by NationalInstitutes of Health grants CA40035, AM28149, RR01346, andAM07464. The author is also grateful to Nancy Garrett for expertsecretarial assistance.
Reprint requests to Dr. G. Mundy, Professor and Head, Division ofEndocrinology and Metabolism, The University of Texas HealthScience Center at San Antonio, 7703 Floyd Curl Drive, San Antonio,Texas 78284, USA
References
1. Sii'so EL, MUNDY GR, D'SOUZA SM, IBBOTSON KJ, BOCK-MAN R, JACOBS JW: Absence of parathyroid hormone messengerRNA in nonparathyroid tumors associated with hypercalcemia. NEngi J Med 309:325—330, 1983
2. MUNDY GR, IBBOTSON KJ, D'SOUZA SM: Tumor products andthe hypercalcemia of malignancy. J Clin Invest 76:391—395, 1985
3. MUNDY GR, COVE DH, FISKEN R: Primary hyperparathyroidism:Changes in the pattern of clinical presentation. Lancet 1:317—1320,1980
4. HEATH H III, HODGSON SF, KENNEDY MA: Primary hyperpara-thyroidism: Incidence, morbidity, and potential economic impactin a community. N Engi J Med 302:189—193, 1980
5. PEACOCK M, ROBERTSON WG, NORDIN BEC: Relation betweenserum and urinary calcium with particular reference to parathy-roid hormone. Lancet 1:384—386, 1969
6. YAMAMOTO M, KAWANOBE Y, TAKAHASHI H, SHIMAZAWA E,KUMURA S, OGATA E: Vitamin D deficiency and renal calciumtransport in the rat. J Clin Invest 74:507—513, 1984
7. GARABEDIAN M, TANAKA Y, HOLICK MF, DELUCA HF: Re-sponse of intestinal calcium transport and bone calcium mobiliza-tion to 1,25 dihydroxyvitamin D3 in thyroparathyroidectomisedrats. Endocrinology 94:1022—1027, 1974
8. MUNDY GR, MARTIN TJ: Hypercalcemia of malignancy—Patho-genesis and treatment. Metabolism 31:1247—1277, 1982
9. MUNDY UR, IBBOT5ON KJ, D'SOUZA SM, SIMPSON EL, JACOBSJW, MARTIN TJ: The hypercalcemia of malignancy: Clinicalimplications and pathogenic mechanisms. N Engi J Med 310:1718—1727, 1984
10. BROWN EM: PTH secretion in vivo and in vitro. Regulation bycalcium and other secretagogues. Miner Electrolyte Metab 8:130--ISO, 1982
11. MUNDY GR, BERTOLINI DB: Pathogenesis of destructive bonelesions and hypercalcemia in plasma cell myeloma. Semin Oncol290—299, 1986
12. SALAHUDDIN SZ, MARKHAM PD, LINDNER SG, GOOTENBERG J,POPOVIC M, HEMMI H, SARIN PS, GALLO RC: Lymphokineproduction by cultured human T cells transformed by human Tcell leukemia-lymphoma virus-l. Science 223:703—707, 1984
13. BERTOLINI DR, NEDWIN GE, BRINGMAN TS, MUNDY GR: Stim-ulation of bone resorption and inhibition of bone formation in vitroby human tumor necrosis factors. Nature 319:516—518, 1986
14. BRESLAU NA, MCGUIRE JL, ZERWEKH JE, FRENKEL EP, PAKCYC: Hypercalcemia associated with increased serum calcitriollevels in three patients with lymphoma. Ann Intern Med 100:1—7,1984
15. FETCHICK DA, BERTOLINI DR, SARIN P, MUNDY GR, DUNN JF:Metabolism of 25—hydroxyvitamin D by human T cell lymphotro-phic virus-transformed cord blood lymphocytes. J Bone MinerRes 1:323, 1986
16. VALENTIN-OPRAN A, CHARHON SA, MEUNIER PJ, EDOUARDCM, ARLOT ME: Quantitative histology of myeloma induced bonechanges. Br J Haematology 52:601—610, 1982
17. STEWART AF, VIGNERY A, SILVERGATE A, RAVIN ND, LIVOLSIV, BROADUS AE, BARON R: Quantitative bone histomorphometryin humoral hypercalcemia of malignancy—uncoupling of bone cellactivity. J Clin Endocrinol Metab 55:219—227, 1982
18. MUNDY GR, WILKINSON R, HEATH DA: Comparative study ofavailable medical therapy for hypercalcemia of malignancy. Am JMed 74:421—432, 1983
19. BRINGHUR5T FR, BIERER BE, GODEAU F, NEYHARD N, VARNERV, SEGRE GV: Humoral hypercalcemia of malignancy. Release of
prostaglandin-stimulating bone-resorbing factor in vitro by humantransitional-cell carcinoma cells. J Clin Invest 77:456—464, 1986
20. MARQUARDT H, TODARO GJ: Human transforming growth factor:production by a melanoma cell line, purification, and initialcharacterization. J Biol Chem 257:5220—5225, 1982
21. MARQUARDT H, HUNKAPILLER MW, HOOD LE, TODARO GJ: Rattransforming growth factor type I: structure and relation toepidermal growth factor. Science 223:1079—1082, 1984
22. TAM JP, MARQUARDT H, ROSBERGER DF, WONG TW, TODAROGJ: Synthesis of biologically active rat transforming growth factorI. Nature 309:376, 1984
23. LEE DC, ROSETM, WEBB NR, TODARO GJ: Cloning and sequenceanalysis of a cDNA for rat transforming growth factor-a. Nature313:489-491, 1985
24. DERYNCK R, ROBERTS AB, WINKLER ME, CHEN EY, GOEDDELDV: Human transforming growth factor-a: Precursor structureand expression in E. coli. Cell 38:287—297, 1984
25. LINSLEY PS, HARGREAVES WR, TWARDZIK DR, TODARO GJ:Detection of larger polypeptides stucturally and functionally re-lated to Type I transforming growth factor. Proc Nat! Acad SciUSA 82:356—360, 1985
26. CARPENTER G, STOSCHECK CM, PRESTON YA, DELARCO JEAntibodies to the epidermal growth factor receptor block thebiological activities of sarcoma growth factor. Proc NatI Acad Sci
USA 80:5627—5630, 198327. IBBOTSON KJ, TWARDZIK DR, D'SouzA SM, HARGREAVES WR,
TODARO GJ, MUNDY GR: Stimulation of bone resorption in vitroby synthetic transforming growth factor-alpha. Science 228:1007—1009, 1985
28. TASHJIAN AH, VOELKEL EF, LAZZARO M, SINGER FR, ROBERTSAB, DERYNCK R, WINKLER ME, LEVINE L: Alpha and betatransforming growth factors stimulate prostaglandin productionand bone resorption in cultured mouse calvaria. Proc NatI AcadSci USA 82:4535—4538, 1985
29. STERN PH, KRIEGER NS, NI55ENS0N RA, WILLIAMS RD,WINKLER ME, DERYNCK R, STREWLER GJ: Human transforminggrowth factor-alpha stimulates bone resorption in vitro. J ClinInvest 76:2016—2020, 1985
30. IBBOT5ON KJ, HARROD J, GOWEN M, D'SouzA 5, WINKLER M,CARPENTER G, DERYNCK R, MUNDY GR: Effects of humantransforming growth factor (TGF) alpha on bone resorption andformation in vitro. Proc Nat! Acad Sci USA 83:2228—2232, 1986
31. HON J, MUNDY GR, DERYNCK R, ROODMAN GD: Recombinanthuman transforming growth factor (TGF-a) stimulates the forma-tion of osteoclast (OCL)-like cells in long term human marrowcultures. J Bone Miner Res 1:68, 1986
32. SICA DA, MARTODAM RR, ARONOW J, MUNDY GR: The hyper-calcemic rat Leydig cell tumor—a model of the humoral hypercal-cemia of malignancy. Calcif Tissue Ini 35:287—293, 1983
33. IBBOT5ON KJ, D'SOUZA SM, NG KW, OSBORNE CK, NIALL M,MARTIN TJ, MUNDY GR: Tumor-derived growth factor increasesbone resorption in a tumor associated with the humoral hypercal-cemia of malignancy. Science 221:1292—1294, 1983
34. D'SOUZA SM, IBBOTSON KJ, CARPENTER G, MUNDY GR: Mech-anisms of humoral hypercalcemia of malignancy (HHM): Use ofanti-EGF receptor antibodies and PTH antagonists (abstract).Ca!cf Tissue mt 36:480, 1984
35. IBBOTSON KJ, D'SouzA SM, SMITH DD, CARPENTERG, MUNDYGR: EGF receptor antiserum inhibits bone resorbing activityproduced by a rat Leydig cell tumor associated with the humoralhypercalcemia of malignancy. Endocrinology 116:469-471, 1985
36. MUNDY GR, IBBOTSON KJ, D'SOUZA SM, KUKREJA SC,ABRAMSON EC, KUKLA U, CARPENTER G, DERYNCK R: Evi-dence that transforming growth factor alpha production causesbone resorption and hypercalcemia in squamous cell carcinoma ofthe lung. Clin Res 33:573A, 1985
37. BROWN EM: Set-point for calcium: its role in normal and abnor-mal parathyroid secretion, in Hormonal Control of Calcium Me-tabolism, edited by COHN DV, TALMAGE RV, MATTHEWSJL,Amsterdam, Excerpta Medica, 1981, pp 35—43
38. SPORN MB, ROBERTS AB: Autocrine growth factors and cancer.Nature 3 13:745, 1985
39. SEYEDIN SM, THOMAS TC, THOMPSON AY, ROSEN DM, PIEz

154 Nephrology Forum
KA: Purification and characterization of two cartilage-inducingfactors from bovine demineralized bone. Proc Nat! Acad Sci USA82:2267—2271, 1985
40. SEYEDIN SM, THOMPSON AY, BENTZ H, ROSEN DM, MCPHER-SON JM, CONTI A, SIEGEL NR, GALLUPPI G, PIEz KA: Carti-lage-inducing factor-a. Apparent identity to transforming growthfactor /3. J Biol Chem 261:5693—5695, 1986
41. POSER J, PFEILSCHIFTER J, COPPINGER W, LUCAS D, MUNDY G:Evidence that TGF$ mediates some of the biologic activitiesascribed to BMP. J Bone Miner Res 1(Suppl 1):307, 1986
42. SPORN MB, ROBERTS AB, SHULL JH, SMITH JM, WARD JM:Polypeptide transforming growth factors isolated from bovinesources and used for wound healing in vivo. Science 219:1329—1331, 1983
43. STEWART AF, INSOGNA KL, GOLTZMAN D, BROADUS AE: Iden-tification of adenylate cyclase-stimulating activity and cytochemi-cal glucose-6—phosphate dehydrogenase-stimulating activity inextracts of tumors from patients with humoral hypercalcemia ofmalignancy. Proc Nail Acad Sci USA 53:941—947, 1981
44. STREWLER GJ, WILLIAMS RD, NISSENSON RA: Human renalcarcinoma cells produce hypercalcemia in the nude mouse and anovel protein recognized by parathyroid hormone receptors. JGun Invest 71:769—774, 1983
45. RODAN SB, INSOGNA KL, VIGNERY AMC, STEWART AF,BROADUS AE, D'SOUZA SM, BERTOLINI DR, MUNDY GR,RODAN GA: Factors associated with humoral hypercalcemia ofmalignancy stimulate adenylate cyclase in osteoblastic cells. JClin Invest 72:1511—1515, 1983
46. GOLTZMAN D, STEWART AF, BROADUS AE: Malignancy associ-ated hypercalcemia: Evaluation with a cytochemical bioassay forparathyroid hormone. J Clin Endocrinol Metab 53:899—904, 1981
47. MERENDINO JJ, INSOGNA KL, MILSTONE LM, BROADUS AE,STEWART AF: A parathyroid hormone-like protein from culturedhuman keratinocytes. Science 231:388—390, 1986
48. D'SOUZA SM, IBB0TS0N KJ, MUNDY GR: Failure of PTH antag-onists to inhibit in vitro bone resorbing activity produced by twoanimal models of the humoral hypercalcemia of malignancy. J ClinInvest 74:1104—1107, 1984
49. SESHADRI MS, CORNISH CJ, MASON RS, POSEN S: Parathyroidhormone-like bioactivity in tumours from patients with oncogenicosteomalacia. Gun Endocrinol 23:689—697, 1985
50. RABBANI SA, MITCHELL J, Roy DR, KREMER R, BENNETT HPJ,GOLTZMAN D: Purification of peptides with parathyroid hormone-like bioactivity from human and rat malignancies associated withhypercalcemia. Endocrinology 118:1200—1210, 1986
51. PANG PKT, YANG MCM, KEUTMANN HT, KENNY AD: Structureactivity relationship of parathyroid hormone: separation of thehypotensive and the hypercalcemic properties. Endocrinology112:284—289, 1983
52. LOWIK CWGM, VAN LEEUWEN JPTM, VAN DER MEER JM, VANZEELAND JK, SCHEVEN BAA, HERRMANN-ERLEE MPM: A two-receptor model for the action of parathyroid hormone onosteoblasts: a role for intracellular free calcium and cAMP. CellCalcium 6:311—326, 1985
53. KLEIN DC, RAI5z LG: Prostaglandins: Stimulation of bone re-sorption in tissue culture. Endocrinology 86:1436—1440, 1970
54. FRANKLIN RB, TASHJIAN AH: Intravenous infusion of prostaglan-din E2 raises plasma calcium concentration in the rat. Endocrinol-ogy 97:240—243, 1975
55. TASHJIAN AH, V0ELKEL EF, LEVINE L, GOLDHABER P: Evidencethat the bone resorption-stimulating factor produced by mousefibrosarcoma cells is prostaglandin E2: A new model for thehypercalcemia of cancer. J Exp Med 136:1329—1343, 1972
56. VOELKEL EF, TASHJIAN AH, FRANKLIN R, WASSERMAN E,LEVINE L: Hypercalcemia and tumor-prostaglandins: the VX2carcinoma model in the rabbit. Metabolism 24:973—986, 1975
57. VALENTIN A, EIL0N 0, SAEZ 5, MUNDY GR: Estrogens andanti-estrogens stimulate release of bone resorbing activity bycultured human breast cancer cells. J Clin Invest 75:726-731, 1985
58. SEYBERTH HW, SEGRE GV, MORGAN JL, SWEETMAN BJ, PorrsiT, OATES JA: Prostaglandins as mediators of hypercalcemiaassociated with certain types of cancer. N EngI J Med 293:1278—1283, 1975
59. HORTON JE, RAISZ LG, SIMMONS HA, OPPENHEIM JJ, MERGEN-HAGEN SE: Bone resorbing activity in supernatant fluid fromcultured human peripheral blood leukocytes, Science 177:793—795, 1972
60. MUNDY GR, RAISZ LG, COOPER RA, SCHECHTER GP, SALMONSE: Evidence for the secretion of an osteoclast stimulating factorin myeloma. N EngI J Med 291:1041—1046, 1974
61. MUNDY OR, LUBEN RA, RAISZ LG, OPPENHEIM JJ, BUEL DN:Bone-resorbing activity in supernatants from lymphoid cell lines.N EngI J Med 290:867—871, 1974
62. GOWEN M, WOOD OD, IH1UE EJ, MCGuIIt MK, RUSSELL RG:An interleukin I like factor stimulates bone resorption in vitro.Nature 306:378—380, 1983
63. HEATH JK, SAKLATVALA J, MEIKLE MC, ATKINSON SJ,REYNOLDS JJ: Pig interleukin 1 (catabolln) is a potent stimulator ofbone resorption in vitro. Calcif Tissue Int 37:95—97, 1985
64. GOWEN M, MUNDY GR: Actions of recombinant interleukin-l,interleukin 2 and interferon gamma on bone resorption in vitro. JImmunol 136:2478—2482, 1986
65. BERTOLINI DR, NEDWIN GE, BRINGMAN T, DURIE B, GILLESTIEA, MUNDY GR: Evidence that tumor necrosis factor /3 (lympho-toxin) is the bone resorbing factor produced by myeloma cells inculture. J Bone Miner Res, in press
66. DEWHIRST FE, STASHENKO PP, MOLE JE, TOURUMACHI T:Purification of partial sequences of human osteoclast activatingfactor: Identity with interleukin 1 beta. J Immunol 135:2562—2568,1985
67. HAUSSLER MR, MCCAIN TA: Basic and clinical concepts relatedto vitamin D metabolism and action. N EngI J Med 297:974—983,1977
68. ROSENTHAL N, INSOGNA KL, GODSALL JW, SMALDONE L,WALDRON JA, STEWART AF: Elevations in circulating 1,25 dihy-droxyvitamin D in three patients with lymphoma-associatedhypercalcemia. J Glin Endocrinol Metab 60:29—33, 1985
69. ZALOGA GP, EIL C, MEDBERY CA: Humoral hypercalcemia in
Hodgkin's disease. Arch Intern Med 145:155—157, 198570. DAVIES M, HAYES ME, MAWER EB, LUMB GA: Abnormal
vitamin D metabolism in Hodgkin's lymphoma. Lancet 1:1186—1188, 1985
71. POPOVIC M, SARIN PS, ROBERT-GURROFF M, KALYANARAMANVS, MANN D, MINOWADA J, GALLO RC: Isolation and transmis-sion of human retrovirus (human T-cell leukemia virus). Science219:856—859, 1983
72. REINHARDT TA, HORST RL, ORF JW, HOLLIS BW: A microassayfor 1,25—dihydroxyvitamin D not requiring high performanceliquid chromatography: Application to clinical studies. J CliiiEndocrinol Metab 58:91—98, 1984
73. FETCHICK DA, BERTOLINI DR. SARIN PS, WEINTRAUB SE,MUNDY OR, DUNN JR: Production of 1,25 dihydroxyvitamin D byhuman lymphotrophic virus-i transformed lymphocytes. J ClinInvest, in press
74. SALAHUDDIN SZ, MARKHAM PD, LINDNER SO, GOOTENBERG J,
POPOVIC M, HEMMI H, SARIN PS, GALLO RC: Lymphokineproduction by cultured human T cells transformed by human Tcell leukemia-lymphoma virus-I. Science 223:703—707, 1984
75. JILKA RL, HAMILTON JW: Inhibition of parathormone-stimulatedbone resorption by Type I interferon. Biochem Biophys ResGommun 120:553—558, 1984
76. GOWEN M, NEDWIN GE, MUNDY OR: Preferential inhibition of
cytokine-stimulated bone resorption by recombinant interferongamma (abstract). J Bone Miner Res l:#67, 1986
77. ROODMAN GD, TAKAHASHI N, MUNDY GR: Recombinant humaninterferon (y-IFN) inhibits formation of osteoclast (OCL)-like cellsby inhibiting the fusion of their precursors. Clin Res 34:522A, 1986
78. LEE MY, BAYLINK DJ: Hypercalcemia, excessive bone resorp-tion, and neutrophilia in mice bearing a mammary carcinoma.Proc Soc Exp Biol Med 172:424—429, 1983
79. KONDO Y, SATO K, OHKAWA H, UEYAMA Y, OKABE T, SATON,ASANO S, M0RI M, OHSAWA N, KOSAKA K: Association ofhypercaicemia with tumors producing colony-stimulating fac-
tor(s). Cancer Res 43:2368—2374, 198380. O5HAWA N, UEYAMA Y, MORITAK, KONDO Y: Heterotransplan-
tation of human functioning tumors to nude mice, in Proceedings

The hypercalcemia of malignancy 155
of the Second International Workshop on Nude Mice, edited byNOMURA T, OSHAWA N, TAMAOKA N, FUJIWARA F, Tokyo,University of Tokyo Press, 1977, pp 395—405
81. SATO K, MlMuIt H, HAN DC, KAKIUCHI T, UEYAMA Y,OHKAWA H, OKABE T, KONDO Y, OHSAWA N, TSUSHIMA T,SHIZUME K: Production of bone resorbing activity and colonystimulating activity in vivo and in vitro by a human squamous cellcarcinoma associated with hypercalcemia and leukocytosis. J ClinInvest, in press
82. MACDONALD BR, MUNDY GR, CLARK S, WANG EA, ROODMANGD: Recombinant human hemopoietic colony stimulating factorincreases the number of osteoclast-like cells in long-term marrowcultures. J Bone Miner Res 1:143, 1986
83. WIKTOR-JEDRZEJZCAK W, AHMED A, SZCZYLIK C, SKELLY RR:Hematological characterization of congenital osteopetrosis inop/op mouse. J Exp Med 156:1516—1527, 1982
84. BURGER EH, VAN DER MEER JWM, VAN DE GEVEL JS, GRIBNAUJC, THEsINGH CW, VAN FURTH R: In vitro formation ofosteoclasts from long term bone cultures of bone marrow mono-nuclear phagocytes. J Exp Med 156:1604-1614, 1982
85. LORENZ0 JA, QUINTON J: Epidermal growth factor enhances theresorptive response to parathyroid hormone. Calcif Tissue ml36:465, 1984
86. HEYBURN PJ, CHILD JA, PEACOCK M: Relative importance ofrenal failure and increased bone resorption in the hypercalcemia ofmyelomatosis. J Clin Pathol 34:54—57, 1981
87. DURIE BGM, SALMON SE, MUNDY GR: Relation of osteoclastactivating factor production to the extent of bone disease inmultiple myeloma. Br J Haematol 47:21—30, 1981
88. PEACOCK M, ROBERTSON WG, NORDIN BEC: Relation betweenserum and urine calcium with particular reference to parathyroidactivity. Lancet 1:384—386, 1969
89. NORDIN BEC: Calcium phosphate and magnesium metabolism.Clinical physiology and diagnostic procedures. Edinburgh,Churchill Livingstone, 1976
90. KLEEMAN CR, BERNSTEIN D, ROCKNEY R, DOWLING JT, MAX-WELL MH: Studies on the renal clearance of diffusible calcium andthe role of the parathyroid glands in its regulation. Yale JBiol Med34: 1—30, 1961
91. KANIS JA, CUNDY T, HEYNEN G, RUSSELL RGG: The pathophys-iology of hypercalcemia. Metab Bone Dis Relat Res 2: 15 1—159,1980
92. RALSTON SH, FOGELMAN I, GARDNER MD, BOYLE IT: Relativecontribution of humoral and metastatic factors to the pathogenesisof hypercalcemia in malignancy. Br Med J 288:1405—1408, 1984
93. RALS-ON SH, FOGELMAN I, GARDNER MD, DRYBURGH FJ,COWAN RA, BOYLE IT: Hypercalcemia of malignancy: evidencefor a non-parathyroid agent with an effect on renal tubularhandling of calcium. Clin Sci 66:187—191, 1984
94. PERCIVAL RC, YATES AJP, GRAY RES, GALLOWAY J, ROGERS K,NEAL FE, KANIS JA: Mechanisms of malignant hypercalcemia incarcinoma of the breast. Br Med J 291:776-779, 1985
95. PEACOCK M, SELBY PL, GIBBS CJ, AARON JE: Pathogenesis ofneoplastic hypercalcemia. Calcif Tissue ml (suppl) 38:S37, 1985
96. CAVERZASIO J, Rizzou R, FLEISCH H, BONJOUR J-P: PTH likechanges of renal calcium and phosphate (Pi) reabsorption inducedby Leydig cell tumor in thyroparathyroidectomized (TPTX)Fischer rats. Calcif Tissue ml (suppl) 36:S26, 1984
97. MOOLENAAR WH, TSIEN RY, VAN DER SAAG PT, DE LAAT SW:Na + /HT exchange and cytoplasmic pH in the action of growthfactors in human fibroblasts. Nature 304:645—648, 1983
98. STEWART AF, HORST R, DEFTOS U, CADMAN EC, LANG R,BROADUS AE: Biochemical evaluation of patients with cancer-associated hypercalcemia: evidence for humoral and nonhumoralgroups. NEnglJMed3O3:1377—1383, 1980
99. DOPPELT SH, SLOvIK DM, NEER RM, NOLAN J: Gut-mediatedhypercalcemia in rabbits bearing VX2—carcinoma—New mecha-nism for tumor-induced hypercalcemia. Proc Natl Acad Sci USA79:640—644, 1982
100. LAFFERTY FW: Pseudohyperparathyroidism. Medicine 45:247—260, 1966
101. EILON G, MUNDY GR: Direct resorption of bone by human breastcancer cells in vitro. Nature 276:726—728, 1978
102. HULTER HN, HALLORAN BP, ToTo RD, PETERSON JC Long-term control of plasma calcitrol concentration in dogs and hu-mans. Dominant role of plasma calcium concentration in experi-mental hyperparathyroidism. J Clin Invest 76:695—702, 1985
103. SIMPSON EL, HARROD J, EILON G, JACOBS JW, MUNDY GR:Identification of a mRNA fraction in human prostatic cancer cellscoding for a novel osteoblast-stimulating factor. Endocrinology117:1615—1620, 1985
104. HIRSCHEL-SCHOLZ 5, CAVERZASIO J, Rizzoi R, BONJOUR J-PNormalization of hypercalcemia associated with a decrease inrenal calcium reabsorption in Leydig cell tumor-bearing ratstreated with WR-2721. J Clin Invest 78:319—322, 1986
105. RIzzoLl R, CAVERZASIO J, FLEISCH H, BONJOUR J-P: Parathyroidhormone-like changes in renal calcium and phosphate reabsorp-tion induced by Leydig cell tumor in thyroparathyroidectomizedrats. Endocrinology 119:1004—1009, 1986