Embed Size (px)
Citation preview

The impact of depression and anxiety disorder symptoms on
the health-related quality of life of children and adolescents
with epilepsy*Dejan Stevanovic, yJasna Jancic, and yAneta Lakic
*Department of Psychiatry, General Hospital Sombor, Sombor, Serbia; and yClinic for Neurology and Psychiatry for Children and
Youth, Medical School University of Belgrade, Belgrade, Serbia
SUMMARY
This study evaluated the effects of depression and anxiety
disorder symptoms on the health-related quality of life
(HRQOL) of children and adolescents with epilepsy. Sixty
children and adolescents and their parents participated in
the study. Symptoms of anxiety disorders were identified
by the Screen for Child Anxiety Related Emotional Disor-
ders questionnaire (SCARED) and symptoms of depres-
sion by the Mood and Feeling Questionnaire (MFQ). The
Pediatric Quality of Life Inventory (PedsQL) was used for
HRQOL assessments. A series of simple and partial corre-
lations revealed that the levels of HRQOL significantly
decrease as symptoms of depression or anxiety disorders
increase and vice versa. Stepwise regression method of
children’s ratings resulted in a final model of school
achievement and symptoms of generalized anxiety and
separation anxiety disorder as predictors that explain
50.9% of the variation in HRQOL (F = 11.21, p < 0.000).
For parents’ ratings, the final model included symptoms
of depression and separation anxiety disorder as predic-
tors that explain 38.4% of the variation in HRQOL
(F = 10.82, p < 0.000). In summary, symptoms of depres-
sion and generalized and separation anxiety disorders
have the most significant impact on HRQOL.
KEY WORDS: Epilepsy, Children, Adolescents, Anxiety
disorders, Depression, Quality of life.
Depression and anxiety disorders have been recognizedas frequent mental health problems in pediatric epilepsy,with reported prevalence rates up to 33% for depression andup to 49% for anxiety disorders (Ekinci et al., 2009).Although it is well known that depression and anxiety disor-ders significantly affect the general outcome and prognosisof epilepsy, there are scarce data about their impact onhealth-related quality of life (HRQOL) in children and ado-lescents with epilepsy. It has been demonstrated that depres-sion affects only emotional well-being (Clary et al., 2010),whereas anxiety symptoms affect present worries and questfor normality as HRQOL aspects in pediatric epilepsy(Ronen et al., 2010). However, only one study found thatdepression and anxiety disorders are strong predictors ofHRQOL in adolescents with epilepsy (Adewuya & Oseni,2005).
This study was conducted to provide more data about theimpact of depression and anxiety symptoms on HRQOL inpediatric epilepsy. The study aimed (1) to determine the
independent effects of depression and different anxiety dis-order symptoms on self- and parent-rated HRQOL in chil-dren and adolescents and (2) to examine their impact onHRQOL with consideration of demographic and clinicalepilepsy variables as well.
Methods
ParticipantsSixty children and adolescents with their parents partici-
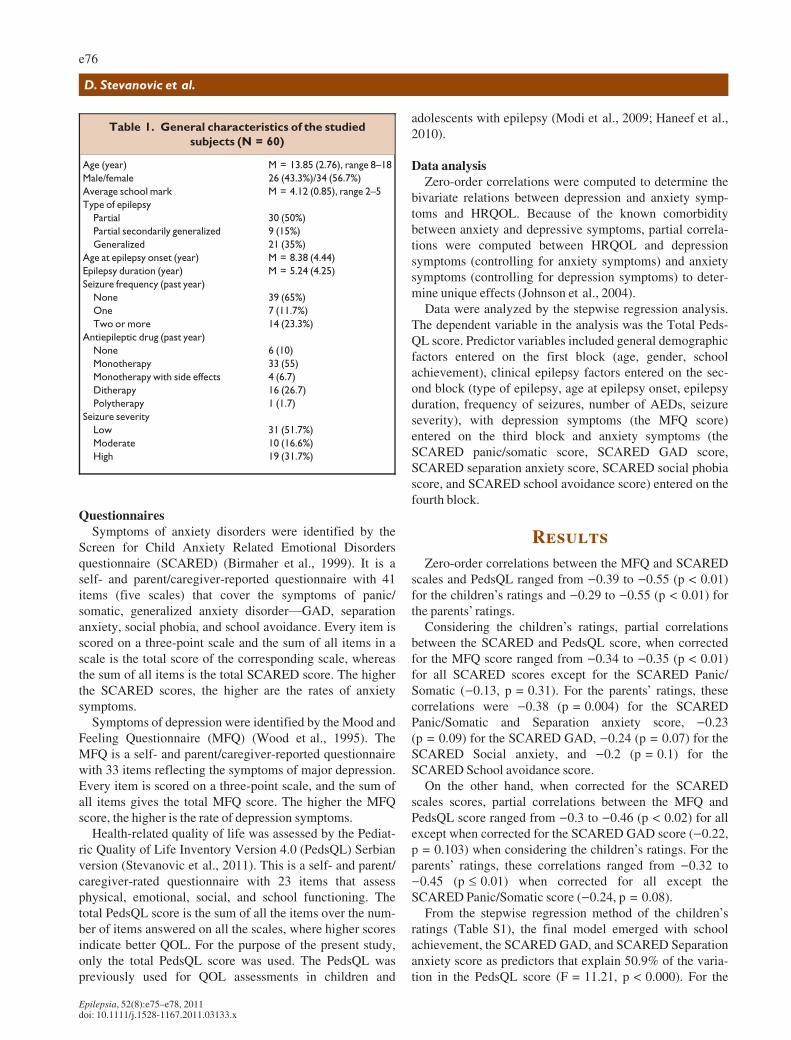
pated in the study (Table 1). The general study inclusion cri-teria were age 8–18 years, active epilepsy, regular schoolattendance, and reading and writing ability documentedfrom school reports. The subjects included had symptoms ofdepression or anxiety disorders as determined by the ques-tionnaires used (see below) and they did not have diagnos-able disorders. Children and adolescents diagnosed withsevere psychiatric disorders (e.g., psychosis, autism spec-trum disorder, and attention deficit/hyperactivity disorder),intellectual disability, severe neurologic impairments, or acomorbid chronic illness/condition were not included. Sei-zure severity was based on type and seizure frequency, andnumber of antiepileptic medications (Raty et al., 2004). TheEthics Committee of the Clinic for Neurology and Psychia-try for Children and Youth Belgrade approved the study.
Accepted April 21, 2011; Early View publication June 21, 2011.Address correspondence to Dejan Stevanovic, M.D., Department of Psy-
chiatry, General Hospital Sombor, Apatinski put 38, 25000 Sombor, Serbia.E-mail: [email protected]
Wiley Periodicals, Inc.ª 2011 International League Against Epilepsy
Epilepsia, 52(8):e75–e78, 2011doi: 10.1111/j.1528-1167.2011.03133.x
BRIEF COMMUNICATION
e75
QuestionnairesSymptoms of anxiety disorders were identified by the
Screen for Child Anxiety Related Emotional Disordersquestionnaire (SCARED) (Birmaher et al., 1999). It is aself- and parent/caregiver-reported questionnaire with 41items (five scales) that cover the symptoms of panic/somatic, generalized anxiety disorder—GAD, separationanxiety, social phobia, and school avoidance. Every item isscored on a three-point scale and the sum of all items in ascale is the total score of the corresponding scale, whereasthe sum of all items is the total SCARED score. The higherthe SCARED scores, the higher are the rates of anxietysymptoms.
Symptoms of depression were identified by the Mood andFeeling Questionnaire (MFQ) (Wood et al., 1995). TheMFQ is a self- and parent/caregiver-reported questionnairewith 33 items reflecting the symptoms of major depression.Every item is scored on a three-point scale, and the sum ofall items gives the total MFQ score. The higher the MFQscore, the higher is the rate of depression symptoms.
Health-related quality of life was assessed by the Pediat-ric Quality of Life Inventory Version 4.0 (PedsQL) Serbianversion (Stevanovic et al., 2011). This is a self- and parent/caregiver-rated questionnaire with 23 items that assessphysical, emotional, social, and school functioning. Thetotal PedsQL score is the sum of all the items over the num-ber of items answered on all the scales, where higher scoresindicate better QOL. For the purpose of the present study,only the total PedsQL score was used. The PedsQL waspreviously used for QOL assessments in children and
adolescents with epilepsy (Modi et al., 2009; Haneef et al.,2010).
Data analysisZero-order correlations were computed to determine the
bivariate relations between depression and anxiety symp-toms and HRQOL. Because of the known comorbiditybetween anxiety and depressive symptoms, partial correla-tions were computed between HRQOL and depressionsymptoms (controlling for anxiety symptoms) and anxietysymptoms (controlling for depression symptoms) to deter-mine unique effects (Johnson et al., 2004).
Data were analyzed by the stepwise regression analysis.The dependent variable in the analysis was the Total Peds-QL score. Predictor variables included general demographicfactors entered on the first block (age, gender, schoolachievement), clinical epilepsy factors entered on the sec-ond block (type of epilepsy, age at epilepsy onset, epilepsyduration, frequency of seizures, number of AEDs, seizureseverity), with depression symptoms (the MFQ score)entered on the third block and anxiety symptoms (theSCARED panic/somatic score, SCARED GAD score,SCARED separation anxiety score, SCARED social phobiascore, and SCARED school avoidance score) entered on thefourth block.
Results
Zero-order correlations between the MFQ and SCAREDscales and PedsQL ranged from )0.39 to )0.55 (p < 0.01)for the children’s ratings and )0.29 to )0.55 (p < 0.01) forthe parents’ ratings.
Considering the children’s ratings, partial correlationsbetween the SCARED and PedsQL score, when correctedfor the MFQ score ranged from )0.34 to )0.35 (p < 0.01)for all SCARED scores except for the SCARED Panic/Somatic ()0.13, p = 0.31). For the parents’ ratings, thesecorrelations were )0.38 (p = 0.004) for the SCAREDPanic/Somatic and Separation anxiety score, )0.23(p = 0.09) for the SCARED GAD, )0.24 (p = 0.07) for theSCARED Social anxiety, and )0.2 (p = 0.1) for theSCARED School avoidance score.
On the other hand, when corrected for the SCAREDscales scores, partial correlations between the MFQ andPedsQL score ranged from )0.3 to )0.46 (p < 0.02) for allexcept when corrected for the SCARED GAD score ()0.22,p = 0.103) when considering the children’s ratings. For theparents’ ratings, these correlations ranged from )0.32 to)0.45 (p £ 0.01) when corrected for all except theSCARED Panic/Somatic score ()0.24, p = 0.08).
From the stepwise regression method of the children’sratings (Table S1), the final model emerged with schoolachievement, the SCARED GAD, and SCARED Separationanxiety score as predictors that explain 50.9% of the varia-tion in the PedsQL score (F = 11.21, p < 0.000). For the
Table 1. General characteristics of the studied
subjects (N = 60)
Age (year) M = 13.85 (2.76), range 8–18
Male/female 26 (43.3%)/34 (56.7%)
Average school mark M = 4.12 (0.85), range 2–5
Type of epilepsy
Partial 30 (50%)
Partial secondarily generalized 9 (15%)
Generalized 21 (35%)
Age at epilepsy onset (year) M = 8.38 (4.44)
Epilepsy duration (year) M = 5.24 (4.25)
Seizure frequency (past year)
None 39 (65%)
One 7 (11.7%)
Two or more 14 (23.3%)
Antiepileptic drug (past year)
None 6 (10)
Monotherapy 33 (55)
Monotherapy with side effects 4 (6.7)
Ditherapy 16 (26.7)
Polytherapy 1 (1.7)
Seizure severity
Low 31 (51.7%)
Moderate 10 (16.6%)
High 19 (31.7%)
e76
D. Stevanovic et al.
Epilepsia, 52(8):e75–e78, 2011doi: 10.1111/j.1528-1167.2011.03133.x

parents’ ratings, the final model emerged with the MFQ andSCARED Separation anxiety score as predictors thatexplain 38.4% of the variation in the PedsQL score(F = 10.82, p < 0.000).
Discussion
A series of simple and partial correlations revealed thatthe levels of HRQOL in children and adolescents signifi-cantly decrease as symptoms of depression or anxiety dis-orders increase, and vice versa. When analyzed for thecomorbidity between the symptoms, the presence ofdepression and anxiety disorders have negative indepen-dent effects on HRQOL. Partial correlations demonstratedthat symptoms of anxiety disorders that correlate withHRQOL, when controlled for depression symptoms, dif-fered between children and parents. Symptoms of panic/somatic problems were not related to HRQOL as child-rated, whereas symptoms of generalized anxiety disorder,social anxiety, and school avoidance were not related toHRQOL as parent-rated. On the other hand, when con-trolled for symptoms of generalized anxiety disorder aschild-rated and panic/somatic problems as parent-rated,symptoms of depression were not significantly related toHRQOL. Therefore, these findings imply that symptoms ofdepression or anxiety disorders have strong effects onHRQOL, but the comorbidity between the symptoms deter-mines the independent effect of each.
The regression models showed that above 50% in thevariations in HRQOL in children and adolescents aschild-rated could be predicted by school achievement andsymptoms of generalized and separation anxiety disorders.Children and adolescents did not consider symptoms ofdepression and other anxiety symptoms or demographic andepilepsy variables as significant HRQOL predictors. On theother hand, the parents of children and adolescents reportedthat symptoms of depression and separation anxiety disor-ders were the only significant predictors of HRQOL. There-fore, when taken together, these findings suggest thatsymptoms of depression and generalized and separationanxiety disorders have the most significant impact onHRQOL compared to other anxiety symptom, demographic,and epilepsy variables.
It was demonstrated that epilepsy variables affectHRQOL to a significant degree (Yong et al., 2006; Ronenet al., 2010). In addition, the previous studies demonstratedthat depression disorder, frequency of seizure, anxiety dis-order, and side effects of AEDs together significantly influ-ence HRQOL in adolescents with epilepsy (Adewuya &Oseni, 2005), or at least emotional functioning as anHRQOL domain (Clary et al., 2010). However, the resultsof this study indicate that the explanatory power of epilepsyvariables is negligible when symptoms of depression andanxiety are considered. Moreover, symptoms of generalizedand separation anxiety disorders have more important
contributions than symptoms of depression in the regressionmodel.
Nevertheless, self-report questionnaires are not synony-mous with clinical diagnosis, and this is a significant limita-tion of the study as well as the using of generic pediatricHRQOL measure. Furthermore, more than one half of theparticipants had low overall seizure severity and childrenand adolescents were not separately evaluated, which couldbias the results and further limit the generalizability of thestudy.
In summary, this pilot study demonstrated that symptomsof depression and generalized and separation anxiety disor-ders have the most significant impact on HRQOL comparedto other anxiety symptom, demographic, and epilepsy vari-ables. Therefore, depression and anxiety symptoms arepowerful factors that need be considered in models ofHRQOL. However, different effects of depression and anxi-ety disorder symptoms on HRQOL based on parent andchild reports were observed, which agrees with the previousfindings about differences in parent and child reports ofmental problems, especially anxiety symptoms (Choudhuryet al., 2003), and it needs to be considered when determin-ing the source of rating.
Disclosure
None of the authors has any conflict of interest to disclose. We confirmthat we have read the Journal’s position on issues involved in ethical publi-cation and affirm that this report is consistent with those guidelines.
References
Adewuya AO, Oseni SB. (2005) Impact of psychiatric morbidity on parent-rated quality of life in Nigerian adolescents with epilepsy. EpilepsyBehav 7:497–501.
Birmaher B, Brent DA, Chiappetta L, Bridge J, Monga S, Baugher M.(1999) Psychometric properties of the Screen for Child Anxiety RelatedEmotional Disorders (SCARED): a replication study. J Am Acad ChildAdolesc Psychiatry 38:1230–1236.
Choudhury MS, Pimentel SS, Kendall PC. (2003) Childhood anxiety disor-ders: parent-child (dis)agreement using a structured interview for theDSM-IV. J Am Acad Child Adolesc Psychiatry 42:957–964.
Clary LE, Vander Wal JS, Titus JB. (2010) Examining health-related qual-ity of life, adaptive skills, and psychological functioning in children andadolescents with epilepsy presenting for a neuropsychological evalua-tion. Epilepsy Behav 19:487–493.
Ekinci O, Titus JB, Rodopman AA, Berkem M, Trevathan E. (2009)Depression and anxiety in children and adolescents with epilepsy: prev-alence, risk factors, and treatment. Epilepsy Behav 14:8–18.
Haneef Z, Grant ML, Valencia I, Hobdell EF, Kothare SV, Legido A, Khur-ana D. (2010) Correlation between child and parental perceptions ofhealth-related quality of life in epilepsy using the PedsQL V 4.0 mea-surement model. Epileptic Disord 12:275–282.
Johnson EK, Jones JE, Seidenberg M, Hermann BP. (2004) The relativeimpact of anxiety, depression, and clinical seizure features on health-related quality of life in epilepsy. Epilepsia 45:544–550.
Modi AC, King AS, Monahan SR, Koumoutsos JE, Morita DA, GlauserTA. (2009) Even a single seizure negatively impacts pediatric health-related quality of life. Epilepsia 50:2110–2116.
Raty LK, Soderfeldt BA, Larsson G, Wilde-Larsson BM. (2004) The rela-tionship between illness severity, sociodemographic factors, generalself-concept, and illness-specific attitude in Swedish adolescents withepilepsy. Seizure 13:375–382.
e77
Depression and Anxiety Affects HRQOL
Epilepsia, 52(8):e75–e78, 2011doi: 10.1111/j.1528-1167.2011.03133.x

Ronen GM, Streiner DL, Verhey LH, Lach L, Boyle MH, Cunningham CE,Rosenbaum PL; North American Pediatric Epilepsy QOL ResearchGroup. (2010) Disease characteristics and psychosocial factors:explaining the expression of quality of life in childhood epilepsy.Epilepsy Behav 18:88–93.
Stevanovic D, Lakic A, Damnjanovic M. (2011) Some psychometric prop-erties of the Pediatric Quality of Life InventoryTM Version 4.0 GenericCore Scales (PedsQLTM) in the general Serbian population. Qual LifeRes DOI 10.1007/s11136-010-9833-z.
Wood A, Kroll L, Moore A, Harrington R. (1995) Properties of the moodand feelings questionnaire in adolescent psychiatric outpatients: aresearch note. J Child Psychol Psychiatry 36:327–334.
Yong L, Chengye J, Jiong Q. (2006) Factors affecting the quality of life inchildhood epilepsy in China. Acta Neurol Scand 113:167–173.
Supporting Information
Additional Supporting information may be found in theonline version of this article.
Table S1. Results of multiple regression analyses.Please note: Wiley-Blackwell is not responsible for the
content of functionality of any supporting Information sup-plied by the authors. Any queries (other than missing mate-rial) should be directed to the corresponding author for thearticle.
e78
D. Stevanovic et al.
Epilepsia, 52(8):e75–e78, 2011doi: 10.1111/j.1528-1167.2011.03133.x