Embed Size (px)
DESCRIPTION
The Impact of Diabetes Self-Management Education on Glucose Management in Ethnic Armenians. Zarmine Naccashian PhD, GNP, MN, RN , CDE Azusa Pacific University. Introduction. Diabetes: chronic and systemic disease Causes: not completely explicated - PowerPoint PPT Presentation
Citation preview

The Impact of Diabetes The Impact of Diabetes Self-Management Self-Management
Education on Glucose Education on Glucose Management in Ethnic Management in Ethnic
ArmeniansArmeniansZarmine NaccashianZarmine Naccashian
PhD, GNP, MN, RN, CDEPhD, GNP, MN, RN, CDE
Azusa Pacific UniversityAzusa Pacific University

IntroductionIntroduction
Diabetes: chronic and systemic Diabetes: chronic and systemic diseasedisease
Causes: not completely explicatedCauses: not completely explicatedPrevalence: Epidemic proportions, Prevalence: Epidemic proportions,
serious complicationsserious complicationsSelf-care is needed for effective Self-care is needed for effective
controlcontrolInvolvement of individuals in their careInvolvement of individuals in their careKnowledge, social and financial supportKnowledge, social and financial support

Significance of the StudySignificance of the Study
Results of DCCT & UKPDSResults of DCCT & UKPDS1%↓A1c, 35% reduction in complication1%↓A1c, 35% reduction in complicationA1c as diabetes mgmt. indexA1c as diabetes mgmt. index
DSME classes DSME classes Education thru empowermentEducation thru empowermentEngagement in self-care skillsEngagement in self-care skills
Medicaid does not cover DSMEMedicaid does not cover DSMEEthnic minorities on Medicaid or no Ethnic minorities on Medicaid or no
insuranceinsurance

Goal of NursingGoal of Nursing
Promote health maintenance, Promote health maintenance, Prevent disease exacerbation, Prevent disease exacerbation, Eliminate complications across all Eliminate complications across all
social ranks thru education, support, social ranks thru education, support, assuranceassurance
(AADE, position statement, (AADE, position statement, 2007)2007)

Orem’s Self-Care Orem’s Self-Care Conceptual FrameworkConceptual Framework
Holistic view of the personHolistic view of the personIndividual: unitary beingIndividual: unitary being
Reciprocal interaction world view Reciprocal interaction world view Individual and environmentIndividual and environmentPersistence and changePersistence and change

Self-CareSelf-Care
Self-directed, self-oriented, self-producedSelf-directed, self-oriented, self-producedVoluntary practice of actionVoluntary practice of actionDeliberate, learned over time, Deliberate, learned over time, Regulate one’s own functioning & Regulate one’s own functioning &
developmentdevelopmentContin. action system to care for one’s Contin. action system to care for one’s
selfselfAimed @ maintaining life,health,well-Aimed @ maintaining life,health,well-
beingbeing

CaringCaring
The most consistent theme in defining The most consistent theme in defining nursing (McCance et. Al, 1999)nursing (McCance et. Al, 1999)
People function and maintain life, People function and maintain life, health and well-being by caring for health and well-being by caring for themselvesthemselves
Most discussed and most usedMost discussed and most usedWide scope of application to any Wide scope of application to any
nursing practice situationnursing practice situation

Self-care deficit theory of Self-care deficit theory of nursingnursing(SCDTN)(SCDTN)
Theory of self-care
Theory of self-care deficit
Theory of Nursing Systems

Self Care Agency
Basic Conditioning Factors
AgeGender
Developmental stateSociocultural orientation
Health stateFamily system factors
Health care system factorsPatterns of Living
Environmental factorsResource availability and adequacy
Self-care requisites
Universal Developmental
Health Deviation
Self-Care Deficit
Nursing Agency
•Wholly compensatory•Partly compensatory•Supportive-educative
Theory of Self Care, Theory of Theory of Self Care, Theory of Self Care Deficit andSelf Care Deficit and
Theory of Nursing Systems Theory of Nursing Systems (Adapted from Orem, 1995)(Adapted from Orem, 1995)
Therapeutic Self-Care Demands
Self-Care

Self-Care Deficit Theory of Nursing (SCDTN)Self-Care Deficit Theory of Nursing (SCDTN)Application to Nursing ResearchApplication to Nursing Research
Empirical studies suggest that personal and Empirical studies suggest that personal and environmental factors affect one’s behaviors environmental factors affect one’s behaviors to achieve desirable health and well-being to achieve desirable health and well-being outcomes (Souza et al., 2005/06)outcomes (Souza et al., 2005/06)
Orem’s SCDTN was selected for this research Orem’s SCDTN was selected for this research study to ensure a framework for a practice study to ensure a framework for a practice issue such as diabetes self-management to issue such as diabetes self-management to provide understanding of outcomesprovide understanding of outcomes

Self-Care Deficit Theory of Nursing (SCDTN)Self-Care Deficit Theory of Nursing (SCDTN)Application to Current StudyApplication to Current Study
Health deviationHealth deviation Diagnosis: DiabetesDiagnosis: Diabetes
Self-care agencySelf-care agency Individual with DMIndividual with DM
Basic conditioning Basic conditioning factorfactor
Age, Gender, Age, Gender, Acculturation, Acculturation,
Years with DMYears with DM
Therapeutic self-care Therapeutic self-care demanddemand
Diet, BGM, Medication, Diet, BGM, Medication, ExerciseExercise
Nursing agency Nursing agency (educative-supportive)(educative-supportive)
Diabetes self-mgmt Diabetes self-mgmt class, reinforcement class, reinforcement by CDEby CDE
Self-careSelf-care Changes in HbA1c, Changes in HbA1c, EmpowermentEmpowerment

Self Care Agency
Individual diagnosed with
diabetes
Basic Conditioning FactorsAge, Gender
Developmental state Empowerment
Socio-cultural orientation Acculturation
Health stateYears with Type 2 DM
Self-care requisites
Health Deviation:Diagnosis of
diabetes
Nursing Agency
•Supportive-educative - DSME
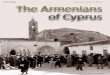
Self Care Deficit Theory of Self Care Deficit Theory of Nursing Nursing AppliedApplied
(Adapted from Orem, 1995)(Adapted from Orem, 1995)
Therapeutic Self-Care Demands
Diet , Medications, Exercise, Blood
Glucose Monitoring
Self-Care Deficit
Self-CareMeasured by A1c & DES

Literature ReviewLiterature ReviewPurposePurpose: Identify gaps in published : Identify gaps in published
research in relation to the impact of research in relation to the impact of diabetes education classes on diabetes education classes on diabetes self-care practices in first diabetes self-care practices in first generation immigrants of Armenian generation immigrants of Armenian descent.descent.
Will addressWill address: prevalence, types, : prevalence, types, burden of disease, minorities, burden of disease, minorities, Armenians, acculturation, Armenians, acculturation, empowerment.empowerment.

Literature Review (cont’d)Literature Review (cont’d)
PrevalencePrevalence : : PandemicPandemic40% of diabetic patients more than 65 40% of diabetic patients more than 65
yoyo66thth leading cause leading cause2050 to reach 48 million (1 in 3)2050 to reach 48 million (1 in 3)5.2 million undiagnosed and untreated5.2 million undiagnosed and untreated

Literature Review (cont’d)Literature Review (cont’d)
Financial BurdenFinancial Burden$132 billion (CDC, 2007) annual$132 billion (CDC, 2007) annual$3.8 billion hospitalization 2001 $3.8 billion hospitalization 2001
(AHCRQ)(AHCRQ)25% of total Medicare budget25% of total Medicare budget45.8 million Americans without 45.8 million Americans without
insuranceinsuranceHealth disparities among racial & ethnic Health disparities among racial & ethnic
minority groupsminority groups

Literature Review (cont’d)Literature Review (cont’d)
MinoritiesMinoritiesHigher in ethnic minoritiesHigher in ethnic minorities↑↑prevalence geriatric minority groups prevalence geriatric minority groups
(Calif. Medi-Cal Study, 2004)(Calif. Medi-Cal Study, 2004)40% patients age 64 40% patients age 64 ↑↑, , limited evidence to guide their limited evidence to guide their
management (Chin et al., 2000)management (Chin et al., 2000)Barriers: language, cultural beliefs, Barriers: language, cultural beliefs,
myths social support, attitudes, trust to myths social support, attitudes, trust to HCPHCP

Literature Review (cont’d)Literature Review (cont’d)
ArmeniansArmenians In America 1618-1619 (Mirak,1983)In America 1618-1619 (Mirak,1983) ““Hidden minority” (Rollins, 1981)Hidden minority” (Rollins, 1981) Half million in LAHalf million in LA Maintain high levels of Armenian identityMaintain high levels of Armenian identity American born Armenians: symbolic American born Armenians: symbolic
connotationconnotation No studies on diab self-mgment in ArmeniansNo studies on diab self-mgment in Armenians Other studies: perception of identity, impact Other studies: perception of identity, impact
of cultural attitudes on comm. ed., culturally of cultural attitudes on comm. ed., culturally sensitive educ to increase awarenesssensitive educ to increase awareness

Literature Review (cont’d)Literature Review (cont’d)
AcculturationAcculturation Process indiv adopts attitudes, beliefs, practices Process indiv adopts attitudes, beliefs, practices
and behaviors congruent with dominant culture and behaviors congruent with dominant culture (Berry, 1980)(Berry, 1980)
Acculturation: behavioral and psychologicalAcculturation: behavioral and psychological Four modes: Assimilation, Integration, Separation, Four modes: Assimilation, Integration, Separation,
MarginalizationMarginalization Three phase course:Contact, conflict, adaptationThree phase course:Contact, conflict, adaptation Adaptation:psychological(int.)psychosocial(ext)Adaptation:psychological(int.)psychosocial(ext) Evolution psychological adaptation varies in intra Evolution psychological adaptation varies in intra
groups, variation reflects outcome of progressgroups, variation reflects outcome of progress

EmpowermentEmpowerment
Gain mastery over their affairs Gain mastery over their affairs (Rappaport, 1987)(Rappaport, 1987)
Sense of control over their well-being Sense of control over their well-being (Nyatanga & Dunn, 2002)(Nyatanga & Dunn, 2002)
Psychosocial phenomenon, measured Psychosocial phenomenon, measured (Menon, 2002)(Menon, 2002)
Self-directed decision makers on their Self-directed decision makers on their care, active & responsible member of care, active & responsible member of the health care team (Anderson et al., the health care team (Anderson et al., 1991)1991)

Empowerment (cont’d)Empowerment (cont’d)
Patient in charge of their health, high Patient in charge of their health, high degree of psychosocial self-degree of psychosocial self-awareness to make educated awareness to make educated decisions in abiding in a self-care decisions in abiding in a self-care plan, realistic and applicable to their plan, realistic and applicable to their living situation (Anderson, 1995).living situation (Anderson, 1995).

Diabetes Self-Management Diabetes Self-Management Education Programs (DSME)Education Programs (DSME)
↑↑self-efficacy, predictor to self care self-efficacy, predictor to self care (meta analysis, Glasgow et al., 2001)(meta analysis, Glasgow et al., 2001)
Can be achieved: motivational Can be achieved: motivational interview, role play, behavior interview, role play, behavior modification (Peyrot et al., 2007)modification (Peyrot et al., 2007)
Research indicates: DSME improves Research indicates: DSME improves self-mgmtself-mgmt

MethodologyMethodology
Research design:Research design:Quasi-experimentalQuasi-experimentalBefore and after single groupBefore and after single group Impact of education on A1c & Impact of education on A1c &
empowermentempowerment

STUDY DESIGNSTUDY DESIGNPre-experimental one group pretest-posttest Pre-experimental one group pretest-posttest
designdesignBaselineBaseline Length of Length of
interventionintervention: :
6 week 6 week class class
1. 5 hours 1. 5 hours sessions sessions
eacheach
Last classLast class 3 months 3 months from from
baseline baseline datedate
EnrollmentEnrollment-DM Type 2 -DM Type 2 -Consent -Consent AssessmentAssessment--Demographics Demographics --Empowerment Empowerment -Acculturation-Acculturation
Obtain Obtain -HgbA1c from -HgbA1c from PCPPCP
DSME DSME interventionintervention
Assessment ofAssessment of-Empowerment-Empowerment
--Assessment Assessment of -HgbA1c of -HgbA1c from:from: -PCP -PCP -A1c Now -A1c Now kitkit
Sample selection criteria listed, assessment of HgbA1c within past six months of enrollment date obtained from PCPIV - DSMEMediator – Age, gender, acculturation and years with diabetesDV – Diabetes Self-Management measured by empowerment and HbA1c

Research QuestionsResearch Questions
Q 1: Patients diagnosed with Type 2 diabetes of Q 1: Patients diagnosed with Type 2 diabetes of
Armenian descent have higher scores on DES Armenian descent have higher scores on DES
after completing the DSME classes compared to after completing the DSME classes compared to
pre-class enrollment DES scores.pre-class enrollment DES scores.
Q 2: Patients of Armenian descent living in Los Q 2: Patients of Armenian descent living in Los
Angeles, diagnosed with Type 2 diabetes will Angeles, diagnosed with Type 2 diabetes will
have improved A1c levels after enrolling in DSME have improved A1c levels after enrolling in DSME
classes taught in Armenian compared to their classes taught in Armenian compared to their
A1c levels prior to the class enrollmentA1c levels prior to the class enrollment

Research QuestionsResearch Questions
Q 3: Is there a relationship between the characteristics Q 3: Is there a relationship between the characteristics
of the sample age, gender, acculturation, number of of the sample age, gender, acculturation, number of
years with diabetes and empowerment?years with diabetes and empowerment?
Q 4: Is there a relationship between the characteristics Q 4: Is there a relationship between the characteristics
of the sample age, gender, acculturation, type of of the sample age, gender, acculturation, type of
diabetes, number of years with diabetes and A1c diabetes, number of years with diabetes and A1c
levelslevels
The psychometric properties of the DES and AEOQ-R was The psychometric properties of the DES and AEOQ-R was
examined.examined.

DSME classes
AgeGender
AcculturationYrs with DM
Diabetes managementMeasured by
Empowerment scores and A1c levels
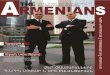
Statistical model with DSME classes as IVStatistical model with DSME classes as IVage, gender, acculturation, yrs with DM as age, gender, acculturation, yrs with DM as
mediator mediator and A1c and empowerment scores as DVand A1c and empowerment scores as DV
IV
DV
Mediating variable

SettingSetting
Daylight Adult Health Daycare Daylight Adult Health Daycare centerscenters

Target PopulationTarget Population
L A California: residence of L A California: residence of immigrants of diverse ethnic immigrants of diverse ethnic backgroundsbackgrounds
Glendale, California: residence of Glendale, California: residence of largest Armenian community outside largest Armenian community outside ArmeniaArmenia
Total city population: 200,000Total city population: 200,000Armenians in Glendale: 85,000Armenians in Glendale: 85,000

Target Population (cont’d)Target Population (cont’d)
Quota samplingQuota sampling Inclusion criteria: Inclusion criteria:
Medicare referral guidelinesMedicare referral guidelinesDM type 2DM type 2

Sample SizeSample Size
N= N= (SD¹ + SD²)(Z1-α + Z2-β)²(SD¹ + SD²)(Z1-α + Z2-β)² = =
Δ² (mean1-mean2)² Δ² (mean1-mean2)²
(1.7² +1.5²)(0.84+1.64) (1.7² +1.5²)(0.84+1.64) ==5.14+6.15 5.14+6.15 = =
7.3-7.6 0.3²7.3-7.6 0.3²
35/group (Neutens & Robinson, 35/group (Neutens & Robinson, 2002)2002)

Data Collection ProcedureData Collection Procedure
Flyers Flyers PostersPostersStudy will be explainedStudy will be explained9 hrs, 6 sessions (1 & ½ 9 hrs, 6 sessions (1 & ½
hours/session)hours/session)A1c will be retrieved from PCP office A1c will be retrieved from PCP office
at the time of study and 3 months at the time of study and 3 months after the study completionafter the study completion

ToolsTools
Demographics: gender, age, # yrs Demographics: gender, age, # yrs DMDM
HbA1cHbA1cDiabetes Empowerment Scale (DES)Diabetes Empowerment Scale (DES)Armenian Ethnic Orientation Armenian Ethnic Orientation
Questionnaire-Revised (AEOQ-R)Questionnaire-Revised (AEOQ-R)

Robert Anderson Ed.DRobert Anderson Ed.D

Data AnalysisData Analysis
Paired t-test, differences in scores Paired t-test, differences in scores empowerment and A1c (Q 1 & Q 2)empowerment and A1c (Q 1 & Q 2)
Two sets of multiple regression: age, Two sets of multiple regression: age, gender, acculturation, DM # of yrs on gender, acculturation, DM # of yrs on empowerment (Q 3) & on A1c (Q 4)empowerment (Q 3) & on A1c (Q 4)
Psychometric properties of DES & Psychometric properties of DES & AEOQ (factor analysis, alpha)AEOQ (factor analysis, alpha)

Results:Results:Demographic Data: genderDemographic Data: gender
NN %% Valid %Valid %
MaleMale 1616 21.321.3 21.321.3
FemaleFemale 5959 78.778.7 78.778.7
TotalTotal 7575 100100 100100

Results:Results:Demographic Data: age, yrs DMDemographic Data: age, yrs DM
NN MinMin MaxMax MeanMean SDSD
AgeAge 7575 6060 8989 75.3375.33 6.36.3
Yrs Yrs DMDM
7575 11 3535 10.6510.65 8.28.2

Results: paired t-testResults: paired t-testPre and post DES scorePre and post DES score
DESDES MeanMean NN SDSD SigSig
Pre-DESPre-DES 4.064.06 7575 0.550.55 0.010.01
Post-Post-DESDES
4.374.37 7575 0.520.52 0.010.01

Results: paired t-testResults: paired t-testPre and post A1cPre and post A1c
A1cA1c MeanMean NN SDSD SigSig
Pre-A1cPre-A1c 7.197.19 7171 1.251.25 0.000.00
Post-Post-A1cA1c
6.866.86 7171 1.031.03 0.000.00

Results: Inter-correlation of age, Results: Inter-correlation of age, gender, acculturation, # yrsgender, acculturation, # yrs
pre and post DESpre and post DES
11 22 33 44 55 66
1. Age1. Age -------- 0.32**0.32** 0.070.07 0.130.13 -0.10-0.10 0.200.20
2. gender2. gender 0.32*0.32***
-------- 0.740.74 -0.14-0.14 -0.18-0.18 -0.18-0.18
3. 3. acculturatiacculturati
0.070.07 0.740.74 -------- -0.10-0.10 0.110.11 0.130.13
4. # yrs4. # yrs -0.13-0.13 -0.14-0.14 -0.10-0.10 -------- -0.02-0.02 0.000.00
5. Pre-DES5. Pre-DES -0.10-0.10 -0.18-0.18 0.110.11 -0.02-0.02 -------- 0.20*0.20*
6. Post-DES6. Post-DES 0.200.20 -0.18-0.18 0.130.13 0.000.00 0.29*0.29* --------

Results: Inter-correlation of age, Results: Inter-correlation of age, gender, acculturation, # yrsgender, acculturation, # yrs
pre and post A1cpre and post A1c
11 22 33 44 55 66
1. Age1. Age -------- 0.27*0.27* 0.060.06 0.110.11 -0.08-0.08 -0.13-0.13
2. gender2. gender 0.27*0.27* -------- 0.080.08 -0.04-0.04 -0.05-0.05 -0.12-0.12
3. 3. acculturatiacculturati
0.060.06 0.080.08 -------- -0.09-0.09 -0.08-0.08 -0.07-0.07
4. # yrs4. # yrs 0.110.11 0.040.04 -0.09-0.09 -------- 0.140.14 0.140.14
5. Pre-DES5. Pre-DES -0.08-0.08 -0.05-0.05 -0.08-0.08 0.140.14 -------- 0.52**0.52**
6. Post-DES6. Post-DES -0.13-0.13 -0.12-0.12 -0.07-0.07 0.140.14 0.52**0.52** --------

DiscussionDiscussion
Reliability of tools used: DESReliability of tools used: DESDES-SF alpha 0.85 (original)DES-SF alpha 0.85 (original)DES-Chinese alpha 0.86DES-Chinese alpha 0.86DES-Swedish alpha 0.68-0.91DES-Swedish alpha 0.68-0.91Current study alpha 0.78 (pilot alpha Current study alpha 0.78 (pilot alpha
0.77)0.77)Correlation reliability Swedish 0.33-0.72Correlation reliability Swedish 0.33-0.72Current study correlation reliability 0.07-Current study correlation reliability 0.07-
0.58 0.58

DiscussionDiscussion
Reliability of tools used: AEOQ-RReliability of tools used: AEOQ-R15 item revised version alpha 0.7115 item revised version alpha 0.71Other study alpha 0.85 (Shirikian, 2006)Other study alpha 0.85 (Shirikian, 2006)This study 0.40This study 0.40Possible explanation: age groupPossible explanation: age group

The Impact of DSME The Impact of DSME on Empowermenton Empowerment
DES score increased from 4.05 to 4.36DES score increased from 4.05 to 4.36 Increase was 0.31 (sig. 0.01)Increase was 0.31 (sig. 0.01)Empowerment viewed by participants: Empowerment viewed by participants:
Conversation and contemplationConversation and contemplationNurse-patient dialogue, current status, Nurse-patient dialogue, current status,
backup plan in times of sicknessbackup plan in times of sicknessSpent time with the participantsSpent time with the participantsEducation by visual method (food plate)Education by visual method (food plate)

The Impact of DSME The Impact of DSME on A1con A1c
A1c reduced from 7.8% to 6.5% (sig A1c reduced from 7.8% to 6.5% (sig 0.00)0.00)
Community specific interventionsCommunity specific interventionsFamilyFamilyLanguageLanguage

Implications to PracticeImplications to Practice
Nurses have fundamental role in educating Nurses have fundamental role in educating patientspatients
Identify health behavior practices in Identify health behavior practices in particular ethnic groupparticular ethnic group
Be aware of similarities and differences Be aware of similarities and differences with other cultures with other cultures
Food preparation, food classification, Food preparation, food classification, portion sizing of existent ethnic dishes, portion sizing of existent ethnic dishes, family members’ understanding of food family members’ understanding of food choiceschoices

ConclusionConclusionBetter understanding of the Better understanding of the
self-care practices of ethnic self-care practices of ethnic ArmeniansArmeniansAppreciation towards Appreciation towards educationeducation
Trust in HCPTrust in HCPAdherence to health care Adherence to health care instructionsinstructions

The EndThe End
Thank you all for attendingThank you all for [email protected]
626-815-6000626-815-6000