Embed Size (px)
Citation preview

Taiwan Medical and Health Information Management Association
Saturday, July 28, 2012
Nelly Leon-Chisen, RHIA, Director Coding and Classification
American Hospital Association
Lee H. Hilborne, MD, MPH,
The Impact of ICD-10-CM and
ICD-10-PCS on Medical
Documentation, Patient Safety
And Quality Initiatives
Medical Director, Care
Coordination
UCLA Health System
Health Services Researcher
RAND Corporation
Medical Director
Quest Diagnostics

2
Public Reporting Of Data Is A Driving
Force
• Transparency is a property of a high reliability organization
• Many initiatives are emerging to evaluate and report quality
of care and patient safety
• Reported data serve four common interconnected purposes
– Quality Improvement
– Public Reporting
– Pay-For-Performance
– Research
Copyright (c) 2012 by American Hospital Association. All rights reserved.

3
Where Does The Pressure Originate?
• Employers
– Reducing costs
– Improving clinical quality
– Comparative performance data available in the public domain (e.g. Leapfrog Group, National Business Coalition on Health)
• Health plans
– Data to describe providers’ and enrollee’s actions, costs, and health outcomes
– Analysis of comparative performance data and pricing
• Consumer concerns
– Medical errors
– Increased cost
– Lack of coverage
– Access to comparative performance
Copyright (c) 2012 by American Hospital Association. All rights reserved.

4 Copyright (c) 2012 by American Hospital Association. All rights reserved.
Pay For Performance Is On Everybody’s Mind
• Also called value based purchasing
• Differential payment to hospitals
and physicians based on
performance on a set of specified
measures
– Quality
– Efficiency
– Patient experiences
– Structural reforms (e.g.,
information technology)
• Aligns financial incentives with
delivery of high quality care
• Rapidly expanding programs
0
50
100
150
200
P4P Programs
2003 2004 2005
2006 2008

5
Private Sector Initiates Most Pay for
Performance Programs
• Most link relatively small bonus payments to better performance on specific process measures with outcome correlation
• Focus on costly and relatively common conditions
• Hospital “pay for performance” (P4P) experiments are run either by commercial plans or by employer-payer coalitions
• Most include process and structure measures
– Some include condition specific clinical outcome measures
– But process measures are easiest to identify because what was actually done gets coded
• Wide range of incremental revenue from successful performance—from less than 1% to 15%
Copyright (c) 2012 by American Hospital Association. All rights reserved.

6
Pay For Performance Is A Centers for
Medicare & Medicaid Priority
• Shift in payment considerations
– Payment traditionally based on the process of care (what was
done)
– P4P: Outcome influences payment (treatment impact); better
outcomes paid more
– Value-based purchasing
• Goal
– Right care for every patient every time
– Conforms to Institute of Medicine (IOM) quality domains
• Safe
• Effective
• Centered on the patient’s needs
• Timely
• Efficient
• Equitable
Copyright (c) 2012 by American Hospital Association. All rights reserved.

7
Medicare Programs Target Multiple Settings
• Various initiatives to encourage improved quality
of care in all health care settings:
– Hospitals
– Physicians’ offices
– Ambulatory care facilities
– Nursing homes
– Home health care agencies
– Dialysis facilities
Copyright (c) 2012 by American Hospital Association. All rights reserved.

8
Quality Reporting Programs Working With CMS Are
Dramatically Impacting Hospital Care
• The Hospital Quality Alliance (HQA)
– Created in 2002 as the USA’s first multi-stakeholder
private/public organization dedicated to developing, reporting
and updating information about hospital quality performance,
and encouraging efforts to improve hospital quality.
– Transferred the quality measure review processes to the
Measures Application Partnership (MAP) in 2012.
– Catalyzed adoption of the Hospital Consumer Assessment of
Healthcare Providers and Systems (HCAHPS), the nation’s first
standardized survey for measuring patients’ perceptions of their
hospital care.
– Introduced the nation’s first measures of surgical site infections.
– Virtually all of the 10 core measures that the HQA first put
forward now are above 95 percent compliance.
– Advised CMS on the creation of Hospital Compare
Copyright (c) 2012 by American Hospital Association. All rights reserved.

9
Quality Reporting Programs Working With CMS Are
Dramatically Impacting Hospital Care (cont.)
• Hospital Compare www.hospitalcompare.hhs.gov
– The nation’s broadest compendium of publicly available,
internet accessible and comparable national hospital
quality measures.
– Currently reports on more than 50 performance
measures for inpatient and outpatient care and allows
the public and health care providers to compare the
performance of more than 4,500 hospitals across the
nation.
Copyright (c) 2012 by American Hospital Association. All rights reserved.

10
Addressing Quality Creates Data Challenges
• Retrospective chart abstraction
– Burdensome
– Time-consuming
– Mostly manual process
– Able to collect more specific clinical measures
• Administrative claims data
– More efficient
– Quality reporting as a by-product of the administrative
process
– Codes do not provide level of detail necessary
– Concerns over accuracy of coded data
Copyright (c) 2012 by American Hospital Association. All rights reserved.

12
We Agreed Safety Is Not New And Surely Not
Unique to the USA
“Grant me the courage to realize my daily mistakes so
that tomorrow I shall be able to see and understand in a
better light what I could not comprehend in the dim light
of yesterday” Maimonides (1135-1204)
“I would give great praise to the physician whose
mistakes are small for perfect accuracy is seldom to be
seen” Hippocrates
“…even admitting to the full extent the great value of the
hospital improvements in recent years, a vast deal of
the suffering, and some at least of the mortality, in these
establishments is avoidable.” Florence Nightingale, 1863

15
We Discussed Changing The Culture In Which
We Practice
• Vague/slippery concept
– “How we get things done around here”
– Unofficial organizing principles; the way problems are solved; organizational glue
– We know it when we see it
– It eats strategy for lunch
• But there are some themes
– Corporate self-esteem
– Organizational structures that are important
– How the organization views itself/outside world
– Degrees of autonomy/collaboration, expectations,
hierarchies of decision making

16
The Heart Of Culture Change In Medical Care
• The idea that medical errors are caused by bad systems is a transforming concept
• Complex systems have latent errors
– Design of work
– Conditions of work
– Training
– Design and maintenance of equipment
• Must have clear responsibility to make the changes needed
• Safety must trump personal preferences
• Safety is everyone’s responsibility

17
We Have Made Progress, But Are Reminded
We All Have Much More Work To Do…
• Several high profile quality and patient safety issues have
happened recently
– In the United States
– In Taiwan
• These high profile issues highlight
– The messages regarding safety and quality remain valid
– We have to keep focusing the light on the issues
– It’s not about our good intentions – it’s about what we do
• Better data can help inform decisions and prevent errors

18
So Can Better Data Help Improve Safety
and Quality?
Clinical Concern Care Variation
Health Services Research
Evidence Based Guidelines
Prioritize the Concern
Decision to Monitor Practice
Select/Define Indicators
Measurement Protocols
Performance Measurement
Identify Best Performers
Evaluate for Best Practices
Disseminate Recs/Findings

19
ICD-10-CM/PCS Potential
• ICD-10-CM/PCS codes have the potential to reveal much
more about quality of care, which will help clinicians better
understand complications, better designing of clinically
robust algorithms, and better tracking of the outcomes of
care.
• The ability to more finely differentiate diseases may help
analysts spot unusual patterns that would otherwise be lost
in the broader categories.
Copyright (c) 2012 by American Hospital Association. All rights reserved.

20
Impact of ICD-10 on Quality Measures
• Quality measures will need to be translated
• Issues related to translation
• Clinical intent of the measure
– The specificity of ICD-10 codes may alter the definition
of a quality measure
– ICD-10 coding conventions and guidelines can affect
the patient populations included or excluded from a
measure
– Can the patient population be better identified using
ICD-10?
• Impact on existing trend data
Copyright (c) 2012 by American Hospital Association. All rights reserved.

21
What If You Already Have Data In ICD-9-
CM?
• Data conversion issues
• Does change reflect a true picture or an artifact of
data conversion?
• What about mapping?
Copyright (c) 2012 by American Hospital Association. All rights reserved.

22
Hospital Value-based Purchasing
Program
• Quality measures
– Heart attack care
– Heart failure care
– Pneumonia
– Surgical care
– Patient safety
– Hospital acquired conditions
• Centers for Medicare & Medicaid (CMS) will evaluate
hospitals both on their achievement on each measure
during the “performance period” and the improvement in
their performance from a “baseline period” to the
performance period.
• CMS will translate each hospital’s total performance score
into an incentive payment.
Performance measure
populations are defined
using ICD-9-CM. Will need
to be re-specified with the
more specific ICD-10 codes
Copyright (c) 2012 by American Hospital Association. All rights reserved.

23
Hospital Value-based Purchasing
Program
• The Accountable Care Act (ACA)
requires CMS to make publicly
available hospital-specific
performance information on
individual measures, conditions or
procedures, and overall scores.
• CMS will publish on the Hospital
Compare website hospital-specific
information with respect to
individual measure scores,
condition-specific scores, domain-
specific scores and total
performance scores.
Performance measure
populations are
defined using ICD-9-
CM. Will need to be re-
specified with the
more specific ICD-10
codes
Copyright (c) 2012 by American Hospital Association. All rights reserved.

24
Quality Reporting Measures are Defined
Using Clinical Codes
• Joint Commission core
measures
• National Quality Forum
endorsed measures
• Physician Consortium for
Performance Improvement
(PCPI) measures
• CMS demonstration projects
• CMS Hospital Acquired
Conditions (HAC) Diagnosis
Related Groups (DRG) impact
• State data reporting
Performance measure
populations are
defined using
ICD-9-CM.
Will need to be re-
specified with the
more specific
ICD-10 codes
Copyright (c) 2012 by American Hospital Association. All rights reserved.

25
Accountable Care Organizations
• Shared savings
– Encourages groups of providers to
form accountable care organizations
(ACOs) to improve the quality and
efficient delivery of patient care and
to share in the cost savings they
achieve with the Medicare program.
• Quality measures
– 65 quality measures, the majority of
the measures do not overlap with the
56 quality measures (45 inpatient
and 11 outpatient) that hospitals
currently report and require data
collection from medical records or
surveys.
Performance
measure populations
are defined using
ICD-9-CM. Will need
to be re-specified
with the more
specific ICD-10
codes
The more specific ICD-10
codes will help you
better understand the
clinical picture of the
patients you treat and the
treatment you provide.
Copyright (c) 2012 by American Hospital Association. All rights reserved.

26
ICD-9-CM and ICD-10-CM/PCS Mapping
• To facilitate the transition from ICD-9-CM to ICD-10-CM/PCS,
mapping between the two coding systems has been
developed.
• The General Equivalence Mappings (GEMs) are used to
facilitate linking between the diagnosis codes in ICD-9-CM
and the new ICD-10-CM/PCS code sets.
• The GEMs as well as the documentation and user’s guide are
available online at:
http://www.cms.gov/Medicare/Coding/ICD10/index.html
Copyright (c) 2012 by American Hospital Association. All rights reserved.

27
General Equivalence Mappings (GEMs)
• The GEMs are a comprehensive
translation dictionary that can be used
to accurately and effectively translate
any ICD-9-CM-based data, including
data for:
– Tracking quality;
– Recording morbidity/mortality;
– Calculating reimbursement; or
– Converting any ICD-9-CM-based
application to ICD-10-CM/PCS.
• The GEMs can be useful for projects to
convert large data sets.
• They are not a substitute for learning
how to use ICD-10-CM or for selecting
ICD-10-CM codes.
GEMs should be
used with care and
require
understanding of
ICD-9-CM as well as
ICD-10, as well as
the intent of the
application or data
being converted.
Copyright (c) 2012 by American Hospital Association. All rights reserved.

28 Copyright (c) 2012 by American Hospital Association. All rights reserved.
ICD-9-CM and ICD-10-PCS Mapping
• Documentation and user’s guide available online
– Information on structure and relationships contained in
the mappings to facilitate correct usage
– Glossary of terms and conventions used in the mapping
along with their accompanying definitions

29
General Equivalence Mappings (GEMs)
• They are not a substitute for learning how to use ICD-
10-CM or for selecting ICD-10-CM codes.
• The GEMs as well as the documentation and user’s guide
are available online at:
http://www.cms.gov/Medicare/Coding/ICD10/index.html
Copyright (c) 2012 by American Hospital Association. All rights reserved.

30
Example of GEMs Translations: Single Code
• Only one alternative in a GEM (“one-to-one” translation)
– Are the codes identical?
Copyright (c) 2012 by American Hospital Association. All rights reserved

31
Example of GEMs Translations: Multiple
Code Alternatives
• There may be multiple translation alternatives all of which are
equally plausible depending on circumstances (e.g. burns).
Copyright (c) 2012 by American Hospital Association. All rights reserved.

32
Example of GEMs Translations: ICD-9
Code Clusters
• More than one ICD-9 code is required to equal a complete
translation of one ICD-10 code
Copyright (c) 2012 by American Hospital Association. All rights reserved.

33
Example of GEMs Translations: ICD-10
Code Clusters
Copyright (c) 2012 by American Hospital Association. All rights reserved.
• More than one I-10 code is required to equal a complete
translation of one I-9 code

34 Copyright (c) 2012 by American Hospital Association. All rights reserved.
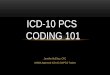
Number of ICD-9 and ICD-10 Codes for Diagnoses and
Procedures
68,000
72,600
3,000
13,000
0
40,000
80,000
Diagnosis codes Procedure codes
ICD-9
ICD-10
What does the additional detail provide for
quality reporting?

35
NQF Seriously reportable events in healthcare: Patient death or
serious disability associated with the use or function of a device
in patient care in which the device is used or functions other than
as intended.
ICD-9-CM
996.1 Mechanical
complication of
other vascular
device, implant,
and graft
ICD-10-CM
9 codes differentiating aortic graft, carotid arterial
graft, femoral graft from catheters.
Examples:
T82.49xA Other complication of vascular dialysis
catheter, initial encounter
T82.591A Other mechanical complication of surgically
created arteriovenous shunt, initial encounter
T82.593A Other mechanical complication of balloon
(counterpulsation) device, initial encounter
T82.595A Other mechanical complication of umbrella
device, initial encounter
ICD-10-CM Code Examples
Copyright (c) 2012 by American Hospital Association. All rights reserved.

36
NQF Seriously reportable events in healthcare: Patient death or
serious disability associated with intravascular air embolism that
occurs while being cared for in a healthcare facility
ICD-9-CM
999.1 Complications of medical
care, not elsewhere classified,
air embolism
(includes air embolism to any
site following infusion,
perfusion, or transfusion)
or
996.74 Other complications, due
to vascular device, implant, and
graft
(includes embolism, fibrosis,
hemorrhage, pain, stenosis)
ICD-10-CM
T80.0xxA Air embolism
following infusion,
transfusion and therapeutic
injection, initial encounter
T82.818A Embolism of vascular
prosthetic devices, implants
and grafts, initial encounter
ICD-10-CM Code Examples
Copyright (c) 2012 by American Hospital Association. All rights reserved.

37
ICD-10-CM Code Examples
ICD-9-CM
998.2 Accidental puncture or
laceration during a
procedure
ICD-10-CM
21 codes indicating accidental puncture
and laceration specifying organ or
body system and type of procedure
Examples:
D78.11 Accidental puncture and
laceration of spleen during a
procedure on the spleen
D78.12 Accidental puncture and
laceration of spleen during other
procedure
National Quality Forum Endorsed Quality Measure: Accidental
Puncture or Laceration
Copyright (c) 2012 by American Hospital Association. All rights reserved.

38
ICD-9-CM
998.4 Foreign body
accidentally left
during a
procedure
• Includes
adhesions,
obstruction or
perforation due to
foreign body left
accidentally during
surgery
ICD-10-CM
T81.525D Obstruction due to foreign body
accidentally left in body following heart
catheterization, subsequent encounter
T81.532A Perforation due to foreign body
accidentally left in body following kidney
dialysis, initial encounter
Plus 48 more unique codes specifying
complications due to foreign body (splitting
out obstruction, adhesions, perforations,
and other complications) and some
common procedures like surgical
operation, endoscopic procedures, removal
of catheter and infusion.
ACO quality measure, MS-DRG hospital acquired condition, Hospital Value
Based Purchasing Program measure: Foreign Body left after procedure
ICD-10-CM Code Examples
Copyright (c) 2012 by American Hospital Association. All rights reserved.

39
Local Coverage Determination: Hyperbaric oxygen therapy
includes indication of diabetic ulcer. ACO At-risk population
measure, Diabetes mellitus foot exam
ICD-9-CM
250.8x Diabetes with other
specified manifestations
+
707.x Chronic ulcer of skin
ICD-10-CM
E10.62x or E11.62x Type 1 or type 2
diabetes mellitus with foot ulcer or
other skin ulcer
Indication is captured in a single code
instead of requiring the combination of
2 codes
ICD-10-CM Code Examples
Copyright (c) 2012 by American Hospital Association. All rights reserved.

40
Local Coverage Determination: Percutaneous transluminal
angioplasty includes indication of vascular graft stenosis
ICD-9-CM
996.74 Other
complications due to
other vascular device,
implant, and graft
• Includes embolism,
thrombosis, fibrosis,
hemorrhage, pain, and
stenosis
ICD-10-CM
T82.858 Stenosis of vascular prosthetic
devices, implants, and grafts
ICD-10-CM Code Examples
Copyright (c) 2012 by American Hospital Association. All rights reserved.

41
Underdosing by (inadvertently) (deliberately) taking less substance
than prescribed or instructed.
Information may be useful to identify reasons for readmissions and
prevent readmissions
ICD-9-CM
Concept does not exist
Code to condition
ICD-10-CM
• T38.3X6 A Underdosing of insulin and oral
hypoglycemic [antidiabetic] drugs, initial
encounter
• T44.7X6A Underdosing of beta-
adrenoreceptor antagonists
ICD-10-CM Code Examples
Copyright (c) 2012 by American Hospital Association. All rights reserved.

42
ICD-10-CM Code Examples
ICD-9-CM
V15.81
Noncompliance
with medical
treatment
ICD-10-CM
Z91.11 Patient's noncompliance with dietary regimen
Z91.120 Patient's intentional underdosing of medication regimen due to financial hardship
Z91.128 Patient's intentional underdosing of medication regimen for other reason
Z91.130 Patient's unintentional underdosing of medication regimen due to age-related debility
Z91.138 Patient's unintentional underdosing of medication regimen for other reason
Z91.14 Patient's other noncompliance with medication regimen
Z91.15 Patient's noncompliance with renal dialysis
Z91.19 Patient's noncompliance with other medical treatment and regimen
Patient noncompliance: Information may be useful to identify
reasons for readmissions and prevent readmissions
Copyright (c) 2012 by American Hospital Association. All rights reserved.

43
ICD-10-CM Code Examples
ICD-9-CM
518.5 Pulmonary
insufficiency following
trauma and surgery
ICD-10-CM
J95.82 Postprocedural respiratory failure
AHRQ Patient Safety Indicators, Value Based Purchasing
Complication/patient safety indicators: Postoperative respiratory
failure
Copyright (c) 2012 by American Hospital Association. All rights reserved.

44
Greater Specificity – Laterality Example
ICD-10-CM
• L89.312 Pressure ulcer of
right buttock, stage II
• L89.324 Pressure ulcer of left
buttock, stage IV
• OR
• L89.322 Pressure ulcer of left
buttock, stage II
• L89.314 Pressure ulcer of
right buttock, stage IV
ICD-9-CM
• 707.05 Pressure ulcer buttock
• 707.22 Pressure ulcer stage II
• 707.24 Pressure ulcer stage
IV
• How many ulcers are there?
CMS, Hospital Acquired Condition: Pressure ulcer
Copyright (c) 2012 by American Hospital Association. All rights reserved.

45 Copyright (c) 2012 by American Hospital Association. All rights reserved.
ICD-9-CM vs. ICD-10-CM Sample Codes
ICD-10-CM
I97.410 Intraoperative hemorrhage and
hematoma of a circulatory system organ or
structure complicating a cardiac catheterization
I97.611 Postprocedural hemorrhage and
hematoma of a circulatory system organ or
structure following cardiac bypass
D78.01 Intraoperative hemorrhage and hematoma
of spleen complicating a procedure on the
spleen
D78.02 Intraoperative hemorrhage and hematoma
of spleen complicating other procedure
ICD-9-CM
998.11 Hemorrhage
complicating a
procedure
998.12 Hematoma
complicating a
procedure
Tracking complications, what really happened,
when?

46
ICD-10-CM Code Examples
ICD-9-CM
996.57 Mechanical
complication due to
insulin pump
ICD-10-CM
T85.614 Breakdown (mechanical) of insulin pump, or
T85.624 Displacement of insulin pump, or
T85.633 Leakage of insulin pump, or
T85.694 Other mechanical complication of insulin
pump
Plus
T38.3x6- Underdosing of insulin and oral
hypoglycemic [antidiabetic] drugs
or
T38.3x1- Poisoning by insulin and oral
hypoglycemic [antidiabetic] drugs, accidental
(unintentional)
National Quality Forum seriously reportable events in healthcare: Patient
death or serious disability associated with hypoglycemia, the onset of
which occurs while the patient is being cared for in a healthcare facility
Copyright (c) 2012 by American Hospital Association. All rights reserved.

47
ICD-9-CM vs. ICD-10-PCS Comparison
ICD-9-CM
• 39.31 Suture of artery
ICD-10-PCS
• 02QP0ZZ Repair pulmonary
trunk, open approach
• Plus 195 other codes based on
– Approach
• Open
• Open Endoscopic
• Percutaneous
• Percutaneous
Endoscopic
– Body part
• 67 different arteries
Copyright (c) 2012 by American Hospital Association. All rights reserved.
Tracking procedures, what was done?

48
National Quality Forum endorsed quality measure: Number of
admissions for lower-extremity amputation among patients with
diabetes.
ICD-9-CM
84.14 Amputation of
ankle through malleoli
of tibia and fibula
84.15 Other amputation
below knee
84.17 Amputation above
knee
ICD-10-PCS
Distinguishes between
• Right and left foot
• Complete foot only
• Lower leg (low, mid or high)
• Upper leg (low, mid or high)
Examples:
0Y6M0Z0 Detachment at Right Foot,
Complete, Open Approach
0Y6C0Z2 Detachment at Right Upper
Leg, Mid, Open Approach
0Y6J0Z3 Detachment at Left Lower
Leg, Low, Open Approach
ICD-9-CM vs. ICD-10-PCS Comparison
Copyright (c) 2012 by American Hospital Association. All rights reserved.

49 Copyright (c) 2012 by American Hospital Association. All rights reserved.
Number of ICD-9 and ICD-10 Codes for Diagnoses and
Procedures
68,000
72,600
3,000
13,000
0
40,000
80,000
Diagnosis codes Procedure codes
ICD-9
ICD-10
How does it affect documentation needs?

50
Documentation Issues
• ICD-10 requires more detailed documentation to specify
aspects of diagnoses and procedures required for more
detailed codes
• Assess current documentation specificity
• Physician education – not necessarily to obtain a more
specific code, but for
• Quality improvement
• Clinical purposes
• Patient safety
Copyright (c) 2012 by American Hospital Association. All rights reserved.

51
Documentation Improvement Program
• Work with your medical staff
• Audit- what is the quality of your documentation today?
• Are diagnoses and procedures documented in in sufficient detail
for coding?
• Are all significant secondary diagnoses properly documented?
• Refine any existing Clinical Documentation Improvement
programs to include ICD-10-CM/PCS requirements
• Will need support from administration
Copyright (c) 2012 by American Hospital Association. All rights reserved.

52
Assess Current Workflow
• Assess choices for provider
documentation
– Problem list
– Pick list – templates
– Free text
– Dictation/speech recognition
– Templates
– Combination?
Copyright (c) 2012 by American Hospital Association. All rights reserved.

53
Case of the Missing Documentation
• Paper vs. electronic
• Hybrid
• Documentation in multiple
locations
– Difficult to find
– Coders may need to
log into multiple
systems or paper
– Easy to miss important
information
– Coders are too
valuable to spend time
playing detectives
• Centralized records
– Scanning
– Electronic health
records
• Technology can be a
coder’s best friend (if done
right)
• Enable remote chart
reviews and audits
• Dealing with shortage of
qualified coders
Copyright (c) 2012 by American Hospital Association. All rights reserved

54
Does Your Organization Code Minor
Procedures?
• Review/revise coding policies on what to code
• Consider alternatives for obtaining required information
required for minor procedures and where should the coding
happen?
Copyright (c) 2012 by American Hospital Association. All rights reserved.

55
Focus Coding and Documentation Gap
Analysis
• Sample records
• Top MS-DRGs
• Most common surgical procedures
• Most active members of the medical staff (high
volume admission/surgeries)
Copyright (c) 2012 by American Hospital Association. All rights reserved.

56
Consider Solutions and Develop Plan
• Technical solutions
• People solutions
• Identify physician and executive champions
• Consider existing venues for disseminating information
• What’s in it for the physicians?
• It’s not only about getting a code number for the hospital or
the claim
Copyright (c) 2012 by American Hospital Association. All rights reserved.

57
Query Forms
• Will need to redesign physician queries.
• Coders and documentation specialists most
likely already know where the gaps in
documentation are
– Engage them to watch for gaps and work
on closing those gaps now!
• Review query form inventory
Copyright (c) 2012 by American Hospital Association. All rights reserved.

58
Dictation/Transcription
• Much more difficult (if not impossible in some instances) to
code without an operative report
• Do you want your coders to wait for the dictation and/or
transcription of the report?
• Filing (if working with paper)
• Address any workflow deficiencies upfront
Copyright (c) 2012 by American Hospital Association. All rights reserved.

59 Copyright (c) 2012 by American Hospital Association. All rights reserved.
Questions?