Embed Size (px)
Citation preview

The impact of numeracy on reactions to different graphic risk presentation formats: An experimental analogue study
Article (Unspecified)
http://sro.sussex.ac.uk
Wright, Alison J., Whitwell, Sophia C. L., Takeichi, Chika, Hankins, Matthew and Marteau, Theresa M. (2009) The impact of numeracy on reactions to different graphic risk presentation formats: An experimental analogue study. British Journal of Health Psychology, 14 (1). pp. 107-125. ISSN 1359107X
This version is available from Sussex Research Online: http://sro.sussex.ac.uk/id/eprint/2229/
This document is made available in accordance with publisher policies and may differ from the published version or from the version of record. If you wish to cite this item you are advised to consult the publisher’s version. Please see the URL above for details on accessing the published version.
Copyright and reuse: Sussex Research Online is a digital repository of the research output of the University.
Copyright and all moral rights to the version of the paper presented here belong to the individual author(s) and/or other copyright owners. To the extent reasonable and practicable, the material made available in SRO has been checked for eligibility before being made available.
Copies of full text items generally can be reproduced, displayed or performed and given to third parties in any format or medium for personal research or study, educational, or not-for-profit purposes without prior permission or charge, provided that the authors, title and full bibliographic details are credited, a hyperlink and/or URL is given for the original metadata page and the content is not changed in any way.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
The impact of numeracy on reactions todifferent graphic risk presentation formats:An experimental analogue study
Alison J. Wright1*, Sophia C. L. Whitwell1, Chika Takeichi1,Matthew Hankins1,2 and Theresa M. Marteau1
1Health Psychology Section, Department of Psychology, King’s College London,London, UK
2Brighton and Sussex Medical School, Brighton, East Sussex, UK
Objectives. Numeracy, the ability to process basic mathematical concepts, may affectresponses to graphical displays of health risk information. Displays of probabilistic riskinformation using grouped dots are easier to understand than displays using disperseddots. However, dispersed dots may better convey the randomness with which healththreats occur, so increasing perceived susceptibility. We hypothesized that low numeracyparticipants would better understand risks presented using grouped dot displays, whilehigh numeracy participants would have good understanding, regardless of display type.Moreover, we predicted that dispersed dot displays, in contrast to grouped dot displays,would increase risk perceptions and worry only for highly numerate individuals.
Design and method. One hundred and forty smokers read vignettes asking themto imagine being at risk of Crohn’s disease, in a 2(display type: dispersed/groupeddots) £ 3(risk magnitude: 3%/6%/50%) £ 2(numeracy: high/low) design. They com-pleted measures of risk comprehension, perceived susceptibility and worry.
Results. More numerate participants had better objective risk comprehension, butthis effect was not moderated by display type. There was marginally significant supportfor the predicted numeracy £ display type interaction for worry about Crohn’sdisease, but not for perceived susceptibility to the condition.
Conclusions. Dispersed dot displays somewhat increase worry in highly numerateindividuals, but only numeracy influenced objective risk comprehension. The mosteffective display type for communicating risk information will depend on the numeracyof the population and the goal(s) of the communication.
Communicating probabilistic risk information is a key challenge for health
professionals. Effective risk communication strategies are needed, so that individuals
can make informed choices about their treatments and their health-related behaviours.
* Correspondence should be addressed to Dr Alison J. Wright, Health Psychology Section, Department of Psychology, King’sCollege London, London SE1 9RT, UK (e-mail: [email protected]).
TheBritishPsychologicalSociety
107
British Journal of Health Psychology (2009), 14, 107–125
q 2009 The British Psychological Society
www.bpsjournals.co.uk
DOI:10.1348/135910708X304432

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
The introduction of large population screening programmes in the UK and elsewhere,
such as that for bowel cancer (NHS bowel cancer screening programme, 2007) and
cardiovascular disease risk assessments ( Joint British Societies, 2005) means that many
more individuals will receive probabilistic risk information. Moreover, new
technologies, such as genetic testing for predisposition to common diseases, create
further demand for effective risk communication strategies.This study was conducted to inform the design of participant information in a trial
assessing the impact of genetic risk information on behaviour change (ISRCTN
21633644). Participants in the trial undergo risk assessments for Crohn’s disease.
Crohn’s disease runs in families, individuals with an affected first degree relative having
an elevated probability of developing the condition (Lewis et al., 2007). Smoking also
increases the likelihood that individuals at risk develop Crohn’s disease (Selby, 2003).
Learning that one is susceptible to Crohn’s disease, but that stopping smoking reduces
this risk, may motivate smokers to quit. However, the best way to communicatethe probabilities involved has yet to be determined. In previous trials assessing the
impact of genetic risk information on behaviour change, participants had difficulties
comprehending the risk information (Lipkus, McBride, Pollak, Lyna, & Bepler, 2004).
Graphic displays are thought to facilitate probabilistic risk communication
(Ancker, Senathirajah, Kukafka, & Starren, 2006). Graphic formats may make the
perception of risk information easier for individuals, so decreasing the cognitive
processing demands of the information. Reducing the cognitive effort required to
use information in decision-making can lead to its greater use (Hibbard & Peters, 2003),and reduce judgment errors (Feldman-Stewart, Kocovski, McConnell, Brundage,
& Mackillop, 2000).
Several studies have examined which graphic formats are most effective at
communicating probabilistic risk information. Based on a recent review of these
(Ancker et al., 2006), it was decided to use icon arrays to communicate risk
information. Icon arrays portray a risk using a group of individual icons such as dots,
oblongs, or human figures. Such arrays have several desirable properties for risk
communication. Firstly, individuals understand probabilities better when they arepresented at the discrete level, rather than as proportions or percentages (Berry,
2004). Secondly, icon arrays allow individuals to view two or more probabilities
expressed in terms of a common denominator. Comparing ‘4 in 1,000’ to ‘1 in 1,000’
is easier than comparing ‘1 in 250’ to ‘1 in 1,000’ (Cosmides & Tooby, 1996;
Gigerenzer & Hoffrage, 1995).
Icon displays can make part to whole relationships clearly visible. When icons are
arranged as a group, the ability to estimate what proportion object A fills of the larger
object B appears to be automatic (Stone et al., 2003). Alternatively, icons can bearranged so that those ‘affected’ appear randomly scattered throughout the array. Such
dispersed icon displays may help convey the randomness inherent in health risks, so
increasing perceived vulnerability to the health outcome, although there is an absence
of evidence to support or refute this (Baty et al., 1997; Schapira, Nattinger, & McHorney,
2001). However, dispersed icon displays make it difficult for viewers to estimate the
proportion affected as this can only be estimated by counting, rather than by judging the
proportion of the block area.
Several studies have compared the effects of different types of icon display.Participants who viewed grouped displays were more accurate at judging the larger of
two risks, at estimating the magnitude of the difference between two probabilities and
at judging the magnitude of a single probability (Feldman-Stewart et al., 2000). In a study
108 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
examining the ability of grouped displays, dispersed displays and bar graphs to convey
breast cancer risk information, participants perceived the magnitude of a 9% risk to
be higher when it was presented using a dispersed icon display than when it was
presented as either a grouped icon display or as a bar graph (Schapira, Nattinger, &
McAuliffe, 2006).
Evidence that individuals may prefer grouped displays to dispersed displays comesfrom a focus group study (Schapira et al., 2001), in which participants disliked dispersed
displays because the only way to understand the magnitude of the probability was to
count the affected icons. Therefore, while dispersed icon displays may increase
perceived susceptibility to a condition and so potentially promote risk-reducing
behaviour (Milne, Sheeran, & Orbell, 2000), participants’difficulties understanding such
displays could result in the risk information not being comprehended, and so failing to
motivate risk-reducing behaviour.
Numeracy and the communication of health risk informationOne individual difference likely to affect reactions to graphic displays of probabilistic
risk information is numeracy, ‘the ability to process basic probability and numerical
concepts’ (Peters et al., 2006b). There is considerable individual variation in numeracy.
Even within a highly educated sample, up to 20% of participants had difficultyanswering simple questions, such as choosing the option that represented the highest
risk from three different proportions or percentages (Lipkus, Samsa, & Rimer, 2001).
Numeracy may affect reactions to risk information for several reasons. People with high
numeracy are more fluent in converting percentages to frequencies and vice versa. They
may also experience more affect in response to numbers conveying probabilistic risk
information, and may use this affect more in guiding their decisions (Peters et al.,
2006b). Affect can influence decision-making by serving as information (Clore, Gasper,
& Garvin, 2001), individuals basing their decisions on how the alternatives make themfeel. Alternatively, the extent and valence of affect can alter how the information is
processed and thus influence decisions (Nabi, 1999; O’Keefe, 2002; Peters, Lipkus, &
Diefenbach, 2006a).
Evidence suggests that numeracy may moderate reactions to probabilistic risk
information and to graphic displays of such information. In a study of women’s ability
to apply information regarding the benefits of mammography to their estimated
lifetime risk of breast cancer, women with high numeracy were more accurate in
applying the risk reduction information, whereas less numerate participantsoverestimated the benefits of mammography to their lifetime cancer risk (Schwartz,
Woloshin, Black, & Welch, 1997). Another study found that participants perceived
risks of breast cancer as greater when presented with dispersed, compared to
grouped, displays, but that this effect was more pronounced for individuals with low
numeracy (Schapira et al., 2006).
In presenting risk information to motivate behaviour change, the communication has
two goals: to enable individuals to understand the size of the risk estimates provided;
and to alter participants’ perceived susceptibility to the condition in order to motivaterisk-reducing behaviour change. Compared to grouped displays, dispersed displays may
increase individuals’ appreciation of the role of chance in whether adverse health
outcomes occur and this may increase perceived susceptibility to these outcomes.
However, because dispersed displays are harder to comprehend, this effect may be
limited to numerate individuals.
Numeracy and risk communication 109

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
The present studyThe present study uses vignettes to investigate smokers’ reactions to risk information
about the likelihood of developing Crohn’s disease, and how these reactions differ
according to icon display type and participants’ numeracy. The likelihood of developing
Crohn’s disease conditional on continued smoking was varied systematically, to examine
the effects of display type at different levels of risk magnitude. We examine participants’subjective and objective understanding of the risk estimates contained in the vignette,
their perceived likelihood of, and their worry about, developing Crohn’s disease.
Individual’s appraisals of susceptibility to a health event are likely to be related to their
levels of worry as worry can be regarded as an affective perception of likelihood (Klein
& Stefanek, 2007). However, perceived likelihood and worry are only moderately
correlated (Lipkus et al., 2000), and both may make separate contributions to predicting
motivation for health behaviours. As numerate individuals may be more subject to
extracting affect from probabilistic risk information, they may experience more worryabout their risk of Crohn’s disease for a given risk magnitude than less numerate
individuals. This may be moderated by display type. Dispersed displays, which highlight
the role of chance in whether one develops Crohn’s disease, may produce more affect.
However, this effect may be restricted to more numerate participants, as it requires the
ability to extract meaning from the more complex, dispersed display.
Hypotheses
(1) Understanding of risk estimates† Grouped displays are easier to process than dispersed displays, leading to better
understanding of risk estimates, an effect that will be stronger for people with
low numeracy.
(2) Perceived susceptibility to Crohn’s disease† Higher magnitude risk estimates will lead to greater perceived susceptibility to
Crohn’s disease.† Dispersed displays will result in participants reporting greater perceived
susceptibility to Crohn’s disease than grouped displays, but this effect will be
weaker for people with low numeracy.(3) Worry about developing Crohn’s disease
† Higher magnitude risk estimates lead to greater worry about developing Crohn’s
disease.† Dispersed displays will result in participants reporting greater worry about
developing Crohn’s disease than grouped displays, but this effect will be weaker
for people with low numeracy.
Methods
DesignParticipants were randomly allocated to read one of six vignettes, asking them to
imagine being given information about their risk of Crohn’s disease, in a 2(display type:dispersed or grouped) £ 3(risk magnitude: 3, 6, or 50%) design. This study is part of a
broader study that also examined the effects of risk provenance (genetic test vs. family
history only). The results of the risk provenance manipulations are presented in a
separate paper (Wright, Takeichi, Whitwell, Hankins, & Marteau, 2008).
110 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
VignettesTo reflect potential clinical applications of genetic testing for Crohn’s disease, each
vignette asked participants to imagine that they had a sibling with Crohn’s disease,
and provided information about the condition’s symptoms. Participants imagined
undergoing a risk assessment, to ascertain their own risk of developing Crohn’s
disease. They were then presented with their hypothetical risk assessment results.To understand the probabilities involved, participants imagined 1,000 smokers with
the same result, who also had sibling with Crohn’s disease. Depending on the
magnitude condition, participants were told 30 (3% risk), 60 (6% risk), or 500 (50%
risk) of the 1,000 people were expected to develop Crohn’s disease. This was
illustrated in a 40 £ 25 array of dots. In the grouped display conditions, a triangular
section, starting at the bottom right-hand corner of the array, of the same number
of dots as people expected to develop Crohn’s disease, was coloured in. In the
dispersed display conditions, the same number of dots was coloured as in thegrouped display conditions, but the coloured dots were dispersed throughout
the entire display. In all conditions, participants were informed that stopping
smoking could halve their risk, and this was illustrated. Finally, participants learnt
that in the general population about one in 1,000 people are expected to develop
Crohn’s disease. The full vignettes are shown in the Appendix.
MeasuresObjective risk comprehension was assessed by asking participants: ‘Which of the three
sets of risk figures you were given was the biggest risk and which was the smallest risk?’
with the options ‘my chances of developing Crohn’s disease’, ‘my chances of developing
Crohn’s disease if I stopped smoking’, and ‘the general population chance of Crohn’s
disease’. In all conditions, the correct responses were that the general population
chance of Crohn’s disease was the smallest and the chance of developing Crohn’s
disease was the biggest.Subjective ease of understanding was assessed using a single item, ‘How easy did
you find it to understand the information we gave you about the chances of developing
Crohn’s disease?’ rated 1: ‘very difficult’ – 7: ‘very easy’.
Perceived susceptibility to Crohn’s disease was assessed using three items, reflecting
different aspects of perceived susceptibility (Weinstein, 1998). Susceptibility condi-
tional on continued smoking was assessed using ‘If you continue to smoke, how likely
do you think it is that you will develop Crohn’s disease?’ rated 1: ‘not at all’ – 7: ‘extremely
likely’. Susceptibility conditional on quitting smoking was assessed using ‘If you stopsmoking, how likely do you think it is that you will develop Crohn’s disease?’ rated 1:
‘not at all’ – 7: ‘extremely likely’. Susceptibility relative to other smokers was assessed
using ‘Compared to other smokers the same age as you, what do you think your chance
of developing Crohn’s disease is?’ rated: 1: ‘a lot more’, 2: ‘more’, 3: ‘average’, 4: ‘less’, 5:
‘a lot less’.
Worry about developing Crohn’s disease was assessed using 3 items (a ¼ :96)
(Cameron & Diefenbach, 2001): ‘To what extent are you worried about getting Crohn’s
disease?’, ‘To what extent are you concerned about getting Crohn’s disease?’, and ‘Towhat extent are you afraid of getting Crohn’s disease’, all rated 1: ‘not at all’ – 7:
‘extremely’.
Numeracy was assessed using eight items developed by Lipkus and his
colleagues (2001).
Numeracy and risk communication 111

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Demographic information and smoking behaviourParticipants were asked their age, gender, and educational qualifications. Nicotine
dependence was assessed using the Heaviness of Smoking Index (HSI; Heatherton,
Kozlowski, Frecker, Rickert, & Robinson, 1989).
ParticipantsThe Research Ethics Committee of a UK university approved the study. One hundred
and forty adult smokers, who did not have Crohn’s disease, were recruited from a
market research agency’s nationally representative internet panel. Panel members
complete surveys in return for ‘points’ that are exchangeable for consumer goods.Participants received 10 ‘points’ (approximate monetary value £1). This sample size is
sufficient to detect medium-sized (0.5 SD) main effects and interactions with a type I
error rate of 0.05 and a type II error rate of 0.8.
Sixty-one (43.6%) men and 79 (56.4%) women participated. Their mean (SD) age was
44.3 (13.5) years. Twelve (8.6%) had no formal educational qualifications, 30 (27.9%)
had qualifications usually completed at age 16 (GCSEs/O Levels), 34 (24.3%) had
qualifications usually completed at age 18 (A Levels or further education qualifications)
and 46 (32.9%) had a University degree. Nine participants had other qualifications. Theirmean (SD) HSI score was 2.6 (1.6), indicating a moderate level of nicotine dependence.
ProcedurePanel members were e-mailed a URL that linked to the survey. Participants first
completed the demographic and smoking behaviour items. Next, they read one of the
six vignettes, randomly allocated by the website software. Participants then completed
the main questionnaire, which began by assessing risk perceptions, then worry,perceived ease of understanding, objective understanding, and finished with the
numeracy items. While responding to the questionnaire, participants could choose to
view the risk information again, in a separate window.
Analyses overviewThe effects of display type and numeracy on subjective ease of understanding were
assessed using ANOVA. The effects of display type and numeracy on objective risk
comprehension were assessed using logistic regression ( Jaccard, 2001). The interaction
term’s ability to significantly contribute to the prediction of risk comprehension was
tested using a hierarchical regression strategy. For the perceived risk measures andworry, the effects of display type, risk magnitude, numeracy and their interactions were
examined using ANOVA. Significant interactions were probed using simple main effects
analysis, employing a Sidak adjustment for multiple comparisons. As dichotomizing
scales to create a two level factor may yield misleading results (MacCallum, Zhang,
Preacher, & Rucker, 2002), we did not dichotomize the numeracy scale using a median
split on the total scores. Instead, we subjected the items to psychometric analysis, and
then used the best discriminating item as a marker of numeracy.
Results
Numeracy levels in this sampleTable 1 shows the proportions of participants answering each numeracy item
correctly. The median score was seven, as it was in Lipkus et al.’s (2001) sample.
112 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
However, the participants performed differently on the items, being less likely to
correctly answer items 1–4, but more likely to correctly answer items 5–7 andsomewhat more likely to answer item eight correctly. Psychometric analysis1 of the scale
revealed that the first item had the highest variance (SD ¼ 0:49) and a good item-total
correlation (r ¼ :62). This item also had the second highest difficulty score (0.59)
(where difficulty is defined as the mean item score and thus, for a dichotomous item, the
proportion of participants getting it right), the highest discrimination value (0.83) (Allen
& Yen, 1979), indicating that it was the best item for discriminating between the top
third and bottom third of total scores on the numeracy measure, and a very good value
for Ferguson’s delta for discrimination (0.97) (Hankins, 2007). Therefore, participantswho answered this item correctly were treated as having higher numeracy, while those
who did not were considered to have lower numeracy.
Table 1. Proportion of correct responses to the numeracy scale made by the 140 participants,
in relation to the findings of Lipkus et al. (2001)
Item
Percentage (N)answering correctly
(N ¼ 140)
Percentage of participantsanswering correctly in
Lipkus et al.’s (2001) study
Which of the following numbersrepresents the biggest risk of gettinga disease: 1 in 100 risk of getting adisease/1 in 1,000 risk of getting adisease/1 in 10 risk of getting a disease
58.6 (82) 78.2
Which of the following numbers representsthe biggest risk of getting a disease:1% risk of getting a disease/10% riskof getting a disease/5% risk of getting a disease
76.4 (107) 83.6
If person A’s risk of getting a disease is1% in 10 years, and person B’s riskis double that of A’s, what is B’s risk?
85.7 (120) 90.5
If person A’s chance of getting a disease is1 in 100 in 10 years, and person B’srisk is double that of A’s, what is B’s risk?
77.1 (108) 86.6
If the chance of getting a disease is 10%,how many people would be expectedto get the disease out of 100?
88.6 (124) 80.8
If the chance of getting a disease is 10%,how many people would be expectedto get the disease out of 1,000?
87.9 (123) 77.5
If the chance of getting a disease is 20 outof 100, this would be the same ashaving a __% chance of getting the disease
76.4 (107) 70.4
The chance of getting a viral infection is .0005.Out of 10,000 people, about how manyof them are expected to get infected?
50.7 (71) 48.6
1 Full details of the psychometric analysis of the numeracy scale are available from the first author upon request.
Numeracy and risk communication 113

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
The high and low numeracy groups did not differ in terms of mean age, nicotine
dependence, the proportions of men and women they contained or in terms of
highest educational qualification. This latter finding echoes Lipkus et al.’s (2001)
observation that even individuals with university-level education may not be highly
numerate.
Effects of display type and numeracy on subjective ease of understandingMean subjective ease of understanding scores were high across all groups, ranging from
5.3 (SD ¼ 1:8) in the dispersed display, low numeracy condition to 5.7 (SD ¼ 1:4) in the
grouped display, high numeracy condition. Neither display type (Fð1; 136Þ ¼ 0:05,
p ¼ :82, partialh2 , :001), numeracy (Fð1; 136Þ ¼ 1:15, p ¼ :29, partialh2 ¼ :008) northeir interaction (Fð1; 136Þ ¼ 0:35, p ¼ :55, partialh2 ¼ :003) significantly influenced
subjective ease of understanding.
Effects of display type and numeracy on objective risk comprehensionTable 2 shows the results of the logistic regression predicting risk comprehension.
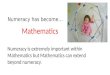
The percentages of participants responding correctly are shown in Table 3 and
illustrated in Figure 1. Adding the display type £ numeracy interaction term tothe model predicting correct comprehension did not improve its fit at a
statistically significant level, x2ð1Þ ¼ 1:55, p ¼ :21. Display type did not significantly
influence the odds of participants having correct objective risk comprehension.
The coefficient for numeracy in Table 2 means that the odds of having good objective
understanding for high numeracy individuals are nearly four times the odds of
having good comprehension for low numeracy individuals. This effect is conditioned
on the moderator variable (display) being equal to zero, and so applies only to
participants who viewed a grouped display. If the display variable is recoded, withzero corresponding to the dispersed display condition, then the odds ratio for
numeracy is 10.2. This indicates that when individuals saw a dispersed display,
the odds of participants with high numeracy responding correctly were 10 times the
odds of participants with low numeracy responding correctly. The coefficient for
the interaction term reflects the ratio of these two odds ratios. That the interaction
coefficient is not significant indicates that this ratio of ratios does not differ
significantly from one. In summary, while numeracy influences objective risk
comprehension, display type does not moderate its impact.
Table 2. Logistic regression predicting objective risk comprehension
95% C.I. for odds ratio
Odds ratio Lower Upper p
Display type 0.442 0.152 1.284 .134Numeracy 3.830 1.301 11.280 .015Display type £ numeracy 2.663 0.567 12.517 .215Constant 1.077 .847
Note. Dummy variable coding was as follows: Display type: grouped ¼ 0, dispersed ¼ 1; Numeracy:low numeracy ¼ 0, high numeracy ¼ 1.
114 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
The effects of display type, risk magnitude and numeracy on risk perceptionsand worryTable 4 shows mean scores by experimental group for perceived susceptibility and
worry. Table 5 details the ANOVA results for these variables.
For perceived risk conditional on continued smoking, the predicted main effect of
risk magnitude was not significant. Instead, a significant risk magnitude £ numeracyinteraction was observed. When numeracy was low, risk magnitude did not
affect risk perceptions (simple main effect (SME) of magnitude at low numeracy,
Fð2; 128Þ ¼ 1:267, p ¼ :285, partialh2 ¼ :019). However, when numeracy was
higher, risk magnitude influenced perceived risk more strongly, although the SME
was only marginally significant (Fð2; 128Þ ¼ 2:369, p ¼ :098, partialh2 ¼ :036).
Sidak-adjusted pairwise comparisons showed that, among individuals with high
numeracy, those in the 50% risk condition perceived greater susceptibility than those
in the 3% risk condition.For risk relative to other smokers, there was a marginally significant main effect of
numeracy: participants with high numeracy perceived themselves as more at risk of
Table 3. Proportions of participants correctly responding to the risk comprehension item, by
numeracy and display type
Response
Numeracy Display type Correct Incorrect
Lower Dispersed N 10 21% 32.3 67.7
Grouped N 14 13% 51.9 48.1
Higher Dispersed N 34 7% 82.9 17.1
Grouped N 33 8% 80.5 19.5
Figure 1. Proportions of participants providing a correct response to the objective risk
comprehension item, according to numeracy and display type.
Numeracy and risk communication 115

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Crohn’s disease relative to other smokers (mean ¼ 2:53, where low scores indicate
greater perceived risk) than did participants with low numeracy (mean ¼ 2:80).
There was also a significant risk magnitude £ display type interaction. SMEs analysis
showed that display type did not significantly influence relative risk perceptions forparticipants in the 3% group (mean relative risk ¼ 2:77 for dispersed display, 2.47 for
grouped display, SME of display Fð1; 128Þ ¼ 1:09, p ¼ :30, partialh2 ¼ :008) or those in
the 50% group (mean relative risk ¼ 2:76 for dispersed display, 2.75 for grouped display,
Fð1; 128Þ , 0:001, p ¼ :984, partialh2 , :001). However, participants who received a
6% risk estimate, and saw a dispersed display had significantly stronger relative risk
perceptions (mean ¼ 2:17, where low scores indicate greater perceived risk) than those
viewed the same risk magnitude illustrated by a grouped display (mean ¼ 3:07, SME of
display Fð1; 128Þ ¼ 11:03, p ¼ :001, partialh2 ¼ :079).Perceived susceptibility conditional on quitting was not significantly predicted by
any of the factors in the model, or their interactions.
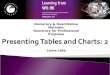
For worry about developing Crohn’s disease, the interaction between display type
and numeracy attained marginal statistical significance and is illustrated in Figure 2.
Inspection of means suggested that, in line with predictions, dispersed displays caused
more worry for highly numerate participants than for less numerate participants, while the
difference between more and less numerate participants viewing a grouped display was
smaller, and in the other direction. However, neither of the SMEs was statistically significant(SME of numeracy for dispersed displays: Fð1; 128Þ ¼ 2:47, p ¼ :118, partialh2 ¼ :019;
SME of numeracy for grouped displays: Fð1; 128Þ ¼ 0:814, p ¼ :369, partialh2 ¼ :006).
Discussion
This study examined the effects of numeracy and display type on reactions to risk
information about Crohn’s disease. The first hypothesis was that grouped displays would be
Table 4. Perceived susceptibility and worry (mean (SD)), according to display type, risk magnitude,
and numeracy level
Variable Numeracy Display 3% 6% 50%
Risk conditional on continued Lower Dispersed 4.00 (1.70) 3.75 (1.76) 3.89 (1.27)smoking (1–7) Grouped 5.00 (1.26) 4.11(1.76) 3.67 (0.89)
Higher Dispersed 3.64 (1.15) 4.42(1.16) 4.53 (1.36)Grouped 3.67 (1.33) 3.69 (1.44) 4.40 (1.35)
Risk conditional on quitting Lower Dispersed 2.80 (1.23) 2.67 (1.23) 2.33 (1.00)smoking (1–7) Grouped 3.33 (0.82) 2.56 (1.13) 2.58 (1.62)
Higher Dispersed 2.71 (0.91) 2.75 (0.75) 2.87 (1.30)Grouped 2.56 (1.20) 2.54 (0.88) 2.60 (1.07)
Risk relative to other smokers Lower Dispersed 2.90 (1.10) 2.42 (0.79) 3.11 (0.33)(rated 1: a lot more Grouped 2.17 (0.98) 3.22 (1.20) 3.00 (0.74)– 5: a lot less) Higher Dispersed 2.64 (0.50) 1.92 (0.79) 2.40 (1.06)
Grouped 2.78 (1.17) 2.92 (0.86) 2.50 (0.97)Worry (1–7) Lower Dispersed 2.93 (2.14) 3.22 (1.52) 3.59 (2.32)
Grouped 4.06 (2.34) 3.67 (1.31) 3.75 (1.22)Higher Dispersed 3.57 (1.79) 3.75 (1.63) 4.40 (1.69)
Grouped 3.31 (1.77) 3.74 (1.60) 3.20 (1.79)
116 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
easier to understand than dispersed displays, an effect that would be particularly
pronounced for individuals with low numeracy. The results for subjective understanding
did not support this hypothesis. Responses to the subjective understanding measure
may be affected by social desirability bias, participants being unwilling to admit
to comprehension difficulties. Also, the item asked about understanding of the risk
information in general terms, rather than specifically about understanding of the
probabilities. Even participants who had difficulty understanding the numerical riskestimates may have felt that, overall, they understood the vignette well, and responded
accordingly. Future studies should frame subjective ease of understanding questions to
be more specific regarding the part(s) of the risk information about which participants
should rate their subjective comprehension.
The results for objective risk comprehension also failed to support the hypothesis.
Less numerate participants were less likely to correctly answer the objective risk
comprehension item, but this effect was not modified by display type. Neither display
type enabled less numerate participants to understand the risk information as well as didmore numerate participants. The ability of other display types to facilitate probabilistic
Table 5. Results of risk magnitude £ display type £ numeracy ANOVAs on risk perceptions
and worry
Variable Effect df a F p Partial h2
Risk conditional on Magnitude 2 0.102 .903 .002continued smoking Display type 1 0.044 .834 , .001
Numeracy 1 0.002 .964 , .001Magnitude £ display type 2 0.877 .418 .014Magnitude £ numeracy 2 3.331 .039 .049Display type £ numeracy 1 1.842 .177 .014Magnitude £ display type £ numeracy 2 0.608 .546 .009
Risk conditional Magnitude 2 0.625 .537 .010on quitting Display type 1 0.001 .977 , .001
Numeracy 1 0.043 .837 , .001Magnitude £ display type 2 0.251 .778 .004Magnitude £ numeracy 2 1.049 .353 .016Display type £ numeracy 1 1.194 .277 .009Magnitude £ display type £ numeracy 2 0.194 .824 .003
Risk relative to Magnitude 2 0.304 .738 .005other smokers Display type 1 1.554 .215 .012
Numeracy 1 2.948 .088 .023Magnitude £ display type 2 5.132 .007 .074Magnitude £ numeracy 2 2.059 .132 .031Display type £ numeracy 1 1.761 .187 .014Magnitude £ display type £ numeracy 2 0.457 .634 .007
Worry about Magnitude 2 0.248 .781 .004Crohn’s disease Display type 1 0.020 .887 , .001
Numeracy 1 0.170 .681 .001Magnitude £ display type 2 0.886 .415 .014Magnitude £ numeracy 2 0.109 .897 .002Display type £ numeracy 1 3.002 .086 .023Magnitude £ display type £ numeracy 2 0.254 .776 .004
a df error ¼ 128 for all analyses.
Numeracy and risk communication 117

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
risk comprehension in individuals with low numeracy requires investigating. The
discrepancy in the effect of numeracy between subjective and objective risk
comprehension echoes previous findings that participants’ subjective levels of
confidence in their ability to use medical statistics were only weakly correlated withtheir objective understanding (Woloshin, Schwartz, & Welch, 2005).
For perceptions of susceptibility to Crohn’s disease, two effects were predicted.
The first was an interaction between display type and numeracy, dispersed displays
resulting in greater perceived susceptibility than grouped displays, but this effect being
weaker for less numerate participants. However, this interaction was not significant
for any of the perceived susceptibility variables. It appears that when grouped
and dispersed icon displays are presented alongside written descriptions of the
probabilities, neither type of display influences risk perceptions. There was limitedevidence that numeracy alone influenced perceived susceptibility. More numerate
participants reported greater risk relative to other smokers than did less numerate
participants. However, this difference was only marginally statistically significant.
More numerate participants may have been more able to use the probabilities presented
in the vignettes to guide their responses to the susceptibility items than were less
numerate participants. Given that all participants were told that their risks were greater
than that of the general population, perceiving higher susceptibility relative to others
seems a rational response by numerate participants to the vignette probabilities.The predicted main effect of risk magnitude on perceived susceptibility was not
significant for any of the susceptibility items. However, there was a significant
interaction between risk magnitude and numeracy on perceived susceptibility
conditional on continued smoking, the type of susceptibility perception probably
most likely to be affected by the risk information presented. More numerate participants
appeared to be influenced by the risk magnitudes presented in the vignettes, while less
numerate participants were not. Therefore, the lack of significant main effects of risk
magnitude may be due to there being considerable variance in the extent to which moreand less numerate participants’ susceptibility perceptions were influenced by the
vignette probabilities, with this variance then resulting in the main effect of risk
magnitude not being statistically significant.
There was also a significant interaction between risk magnitude and display on
susceptibility relative to other smokers, display type only making a difference to relative
Figure 2. Mean worry scores, according to numeracy and display type.
118 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
risk individuals in the 6% group. From a psychological standpoint, it is unclear as to why
display type only influenced relative risk for this particular risk magnitude. Further work
should explore the effects of display types at different levels of risk magnitude.
Finally, for worry about Crohn’s disease, two effects were predicted. The first was an
interaction between display type and numeracy, dispersed displays resulting in greater
worry than grouped displays, but this effect being weaker for less numerateparticipants. This interaction was marginally significant. As predicted, the dispersed
displays were associated with greater worry in more numerate participants than in less
numerate participants. However, contrary to prediction, grouped displays were
associated with greater worry in less numerate participants, although the absolute
magnitude of this difference between the two numeracy groups was not as pronounced
as that for dispersed displays. Given that the interaction between numeracy and display
type was only marginally significant, it requires replication. However, we might consider
these findings reason to build tentatively on Peters et al.’s (2006b) suggestion that highlynumerate individuals are more sensitive to the affective meaning of probabilistic risk
information, to also suggest that highly and less numerate individuals’ ability to extract
affective meaning from probabilistic risk information may vary according to how that
information is presented.
The predicted significant main effect of risk magnitude on worry was not observed.
Although there was a linear increase in mean worry scores across the three levels of risk
magnitude, the differences were small. Emotional responses to vignettes may be less
strong than those to real-world health risk information. Future studies should investigatewhether the effects of display type, risk magnitude and numeracy on worry are stronger
in clinical contexts.
Strengths and limitations of the current study and recommendations for furtherresearchThis is one of the first studies to examine whether numeracy moderates cognitive andemotional responses to risk estimates presented using different graphical formats. The
study benefits from using a sample with a wider range of educational backgrounds than
has hitherto been the case (Lipkus et al., 2001) and so the results may better generalize to
patient populations. While the smoking behaviour of participants in this study was very
similar to that of British smokers in general (Goddard, 2006), the internet-based
recruitment strategy may have disproportionately excluded socially deprived individuals.
Future research should attempt to examine the relationship between numeracy
and reactions to graphical displays of probabilistic risk information in such populations.Using vignettes allowed participants to be allocated to different risk magnitudes,
regardless of their smoking behaviour, so removing one potential confound in studies of
reactions to health risk information (Croyle, Sun, & Hart, 1997). However, vignettes are
obviously only representations of real-life situations, albeit representations intended to
focus attention on the experimental constructs of interest. The extent to which these
results generalize to individuals receiving probabilistic risk information in clinical
contexts remains to be seen.
There are several issues with the measures employed in this study. Items assessingworry were not conditional on continued smoking. Although worry is often assessed in
this manner (Cameron & Diefenbach, 2001), measurement error may have been
inadvertently introduced into the worry measure, some participants reporting lower
levels of worry about Crohn’s disease because they planned to quit smoking in the near
Numeracy and risk communication 119

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
future, but others reporting worry about developing Crohn’s disease contingent on
continued smoking. We operationalised numeracy using the item that best
discriminated individuals with high and low total numeracy scores in our sample.
This introduces a small additional degree of measurement error into the analyses, which
may be partly responsible for the lack of significant effects of numeracy. However, many
of the effect sizes associated with numeracy were small, and unlikely to attain statisticalsignificance in this sample, even if numeracy was measured more precisely. A further
limitation was that, to reduce response burden, many constructs were assessed using
single items. Further studies should use multiple items to assess both risk perceptions
and risk comprehension. Finally, we operationalised perceived susceptibility in several
different ways and performed ANOVAs on each item, potentially inflating the family wise
type I error rate. Therefore, some of the significant effects observed may be due to type I
error. However, if future studies replicate these findings, we would be more confident in
our conclusions.
How should probabilistic risk information be displayed?Dispersed displays did not consistently increase perceptions of susceptibility to Crohn’sdisease. There was only marginally significant evidence that they caused greater worry
than grouped displays in more numerate participants. Therefore, any benefit of display
type for motivating behaviour change may be limited to numerate individuals. Display
type also failed to facilitate risk comprehension. Given these findings, further research is
required before we can confidently recommend a particular display type for
communicating probabilistic risk information. In particular, the triangular grouping of
icons in this study differs from the linear grouping of icons used in other studies (Feldman-
Stewart et al., 2000). Pilot work suggested that individuals preferred this triangulargrouping, but further research should compare these two types of grouped displays.
Finally, the current study focused on a situation where the goal was to increase
perceptions of susceptibility. The optimal display to employ when probabilistic risk
communications are intended either to promote informed choices between treatment
options, or to reduce over-exaggerated perceptions of susceptibility, remains an
empirical question. Health professionals wishing to communicate probabilistic risk
information to their patients need to consider the target population and the goal(s) of
the communication when deciding which graphical display to employ.
Acknowledgements
This study was conducted as part of a programme of research funded by the Medical Research
Council (‘Risk communication in preventative medicine: Optimizing the impact of DNA risk
information’, MRC ref. G0500274). The first author is funded by a Wellcome Trust Research
Training Fellowship in Health Service Research (ref. 062183/Z/00/Z).
References
Allen, M. J., & Yen, W. M. (1979). Introduction to measurement theory. Monterey, CA: Brooks-
Cole.
Ancker, J. S., Senathirajah, Y., Kukafka, R., & Starren, J. B. (2006). Design features of graphs in
health risk communication: A systematic review. Journal of the American Medical
Informatics Association, 13, 608–618.
120 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Baty, B. J., Venne, V., McDonald, J., Croyle, R. T., Halls, C., Nash, J., et al. (1997). BRCA1 testing:
Genetic counseling protocol development and counseling issues. Journal of Genetic
Counseling, 6, 223–244.
Berry, D. (2004). Risk, communication and health psychology. Maidenhead, UK: Open University
Press.
Cameron, L. D., & Diefenbach, M. A. (2001). Responses to information about psychosocial
consequences of genetic testing for breast cancer susceptibility: Influences of cancer worry
and risk perceptions. Journal of Health Psychology, 6, 47–59.
Clore, G. L., Gasper, K., & Garvin, E. (2001). Affect as information. In J. P. Forgas (Ed.), Handbook
of affect and social cognition (pp. 121–144). Hillsdale, NJ: Erlbaum.
Cosmides, L., & Tooby, J. (1996). Are humans good intuitive statisticians after all? Rethinking some
conclusions from the literature on judgment under uncertainty. Cognition, 58, 1–73.
Croyle, R. T., Sun, Y. C., & Hart, M. (1997). Processing risk factor information: Defensive biases in
health-related judgments and memory. In K. J. Petrie & J. A. Weinman (Eds.), Perceptions of
health and illness: Current research and applications (pp. 267–290). Amsterdam: Harwood
Academic Publishers.
Feldman-Stewart, D., Kocovski, N., McConnell, B. A., Brundage, M. D., & Mackillop, W. J. (2000).
Perception of quantitative information for treatment decisions. Medical Decision Making, 20,
228–238.
Gigerenzer, G., & Hoffrage, U. (1995). How to improve Bayesian reasoning without instruction –
frequency formats. Psychological Review, 102, 684–704.
Goddard, E. (2006). General Household Survey, 2005: Smoking and drinking among adults.
London: Office for National Statistics.
Hankins, M. (2007). Questionnaire discrimination: (Re)-introducing coefficient delta. BMC
Medical Research Methodology, 7, 19.
Heatherton, T. F., Kozlowski, L. T., Frecker, R. C., Rickert, W., & Robinson, J. (1989). Measuring the
heaviness of smoking: Using self-reported time to the first cigarette of the day and number of
cigarettes smoked per day. British Journal of Addiction, 84, 791–799.
Hibbard, J. H., & Peters, E. (2003). Supporting informed consumer health care decisions: Data
presentation approaches that facilitate the use of information in choice. Annual Review of
Public Health, 24, 413–433.
Jaccard, J. (2001). Interaction effects in logistic regression. Thousand Oaks, CA: Sage.
Joint British Societies (2005). JBS2: Joint British Societies’ guidelines on prevention of
cardiovascular disease in clinical practice. Heart, 91(Suppl. V), v1–v52.
Klein, W. M. P., & Stefanek, M. E. (2007). Cancer risk elicitation and communication: Lessons from
the psychology of risk perception. CA – A Cancer Journal for Clinicians, 57, 147–167.
Lewis, C., Whitwell, S. C. L., Forbes, A., Sanderson, J., Mathew, C. G., & Marteau, T. M. (2007).
Estimating risks for common complex diseases across genetic and environmental factors:
The example of Crohn’s disease. Journal of Medical Genetics, 44, 689–694.
Lipkus, I. M., Kuchibhatla, M., McBride, C. M., Bosworth, H. B., Pollak, K. I., Siegler, I. C., et al.
(2000). Relationships among breast cancer perceived absolute risk, comparative risk, and
worries. Cancer Epidemiology Biomarkers and Prevention, 9, 973–975.
Lipkus, I. M., McBride, C. M., Pollak, K. I., Lyna, P., & Bepler, G. (2004). Interpretation of genetic
risk feedback among African American smokers with low socioeconomic status. Health
Psychology, 23, 178–188.
Lipkus, I. M., Samsa, G., & Rimer, B. K. (2001). General performance on a numeracy scale among
highly educated samples. Medical Decision Making, 21, 37–44.
MacCallum, R. C., Zhang, S., Preacher, K. J., & Rucker, D. D. (2002). On the practice of
dichotomization of quantitative variables. Psychological Methods, 7, 19–40.
Milne, S., Sheeran, P., & Orbell, S. (2000). Prediction and intervention in health-related behavior:
A meta-analytic review of protection motivation theory. Journal of Applied Social Psychology,
30, 106–143.
Numeracy and risk communication 121

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Nabi, R. L. (1999). A cognitive-functional model for the effects of discrete negative emotions on
information processing, attitude change, and recall. Communication Theory, 9, 292–320.
NHS bowel cancer screening programme (2007). Retrieved 15 July 2007, from www.cancer-
screening.nhs.uk/bowel/index.html
O’Keefe, D. J. (2002). Persuasion: Theory and research (2nd ed.). Thousand Oaks, CA: Sage
Publications.
Peters, E., Lipkus, I., & Diefenbach, M. A. (2006a). The functions of affect in health
communications and in the construction of health preferences. Journal of Communication,
56, S140–S162.
Peters, E., Vastfjall, D., Slovic, P., Mertz, C. K., Mazzocco, K., & Dickert, S. (2006b). Numeracy and
decision making. Psychological Science, 17, 407–413.
Schapira, M. M., Nattinger, A. B., & McAuliffe, T. L. (2006). The influence of graphic format on
breast cancer risk communication. Journal of Health Communication, 11, 569–582.
Schapira, M. M., Nattinger, A. B., & McHorney, C. A. (2001). Frequency or probability? A qualitative
study of risk communication formats used in health care. Medical Decision Making, 21,
459–467.
Schwartz, L. M., Woloshin, S., Black, W. C., & Welch, H. G. (1997). The role of numeracy in
understanding the benefit of screening mammography. Annals of Internal Medicine, 127,
966–972.
Selby, W. S. (2003). Current issues in Crohn’s disease – finding the cause, making the diagnosis and
optimising therapy. Medical Journal of Australia, 178, 532–533.
Stone, E. R., Sieck, W. R., Bull, B. E., Yates, J. F., Parks, S. C., & Rush, C. J. (2003). Foreground:
Background salience: Explaining the effects of graphical displays on risk avoidance.
Organizational Behavior and Human Decision Processes, 90, 19–36.
Weinstein, N. D. (1998). Accuracy of smokers’ risk perceptions. Annals of Behavioral Medicine,
20, 135–140.
Woloshin, S., Schwartz, L. M., & Welch, H. G. (2005). Patients and medical statistics – interest,
confidence, and ability. Journal of General Internal Medicine, 20, 996–1000.
Wright, A. J., Takeichi, C., Whitwell, S. C. L., Hankins, M., & Marteau, T. M. (2008). Impact of
genetic testing, risk magnitude and graphical format on motivation to stop smoking: An
experimental analogue study. Clinical Genetics, 73, 306–314.
Received 6 June 2007; revised version received 11 March 2008
122 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Appendix.
The
vign
ette
suse
din
the
study G
ene
posi
tive
Gen
eneg
ativ
eFa
mily
his
tory
Intr
oduct
ion
Pic
ture
yours
elfin
the
situ
atio
ndes
crib
edbel
ow
.Tr
yto
imag
ine
ascl
earl
yas
poss
ible
how
you
would
thin
kan
dfe
elif
you
wer
eac
tual
lyin
the
situ
atio
nIm
agin
eth
atyo
uhav
ea
sist
eror
bro
ther
who
has
Cro
hn’s
dis
ease
Dis
ease
info
rmat
ion
†C
rohn’s
dis
ease
affe
cts
the
gut
†It
tends
toru
nin
fam
ilies
and
ism
ore
com
mon
insm
oke
rs†
Sym
pto
ms
incl
ude
abdom
inal
pai
n,dia
rrhoea
,fe
ver,
loss
ofap
pet
ite,
and
wei
ght
loss
.T
her
eis
no
cure
for
the
dis
ease
.T
he
sym
pto
ms
can
be
trea
ted
by
med
icat
ion
but
most
pat
ients
will
intim
enee
dsu
rger
y†
The
sym
pto
ms
are
sose
rious
that
som
epeo
ple
with
Cro
hn’s
dis
ease
cannot
work
or
goout
Scen
ario
Your
doct
or
offer
syo
ua
risk
asse
ssm
ent,
usi
ng
age
net
icte
stto
find
out
your
risk
sofdev
el-
opin
gC
rohn’s
dis
ease
You
agre
eto
hav
eth
isge
net
icte
st
(iden
tica
lto
that
use
din
gene
posi
tive
conditio
n)
Your
doct
or
offer
syo
ua
risk
asse
ssm
ent,
usi
ng
the
info
r-m
atio
nab
out
your
fam
ilyhis
tory
tofind
out
your
risk
sofdev
e-lo
pin
gC
rohn’s
dis
ease
Test
resu
ltYo
ur
doct
or
tells
you
that
the
resu
ltofyo
ur
genet
icte
stsh
ow
sth
atyo
uhav
ea
vers
ion
ofa
gene
that
incr
ease
syo
ur
risk
of
dev
elopin
gC
rohn’s
dis
ease
Your
doct
or
tells
you
that
the
resu
ltofyo
ur
genet
icte
stsh
ow
sth
atyo
udo
not
hav
ea
vers
ion
of
age
ne
that
incr
ease
syo
ur
risk
of
dev
elopin
gC
rohn’s
dis
ease
Your
doct
or
tells
you
your
risk
of
dev
elopin
gC
rohn’s
dis
ease
from
your
risk
asse
ssm
ent
bas
edon
your
fam
ilyhis
tory
Ris
kes
tim
ate*
3%
6%
50%
3%
6%
50%
3%
6%
50%
*The
det
ails
ofth
isel
emen
tofth
evi
gnet
tear
esh
ow
nin
the
nex
tta
ble
.
Numeracy and risk communication 123

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
124 Alison J. Wright et al.

Copyright © The British Psychological SocietyReproduction in any form (including the internet) is prohibited without prior permission from the Society
Numeracy and risk communication 125