Embed Size (px)
Citation preview

The impact of the implementation of
single exit pricing for
pharmaceuticals in South Africa
Daleen Pretorius
A research report submitted to the Faculty of Commerce, Law and
Management, University of the Witwatersrand, in partial fulfilment of the
requirements for the degree of Master of Business Administration
Johannesburg, 2011

ii
ABSTRACT
Pricing regulations have been implemented within the pharmaceutical industry
in South Africa to ensure improved access to healthcare.
The implementation of the Single Exit Price (SEP) effectively meant that the
private pharmaceutical sector had to adjust from a free to a regulated market,
where prices had to be cut and discounts discarded. The pricing structure
changed to a transparent structure. These price ceilings resulted into a
decrease in gross profit margins within independent, group and hospital
pharmacies in the private healthcare sector.
The aim of this research was to explore the impact of the implementation of
SEP for pharmaceuticals in the private sector in South Africa through
considering consistent pricing benefits to the patients as well as the changes in
the business environment for retail pharmacies.
A mixed methodology approach was pursued, using both quantitative and
qualitative data analysis. A specific and actual price was obtained for certain
medicines from 50 pharmacies to determine if consistent pricing benefits were
experienced by patients through the introduction of SEP. This construed the
quantitative data. In addition to this, 22 semi-structured interviews were
conducted with pharmacy managers from independent, group and hospital
pharmacies to determine the changes in the business environment following the
introduction of SEP. The qualitative data obtained was analysed from a
thematic perspective.
Key findings from the research were that consistent pricing benefits were not
realised to patients following the introduction of pricing regulations, and
specifically SEP. Changes in the business environment of private retail
pharmacies, following the introduction of SEP included: strategic changes,
survival tactics and day to day changes as well as restructuring.
Pricing regulation may initially seem to only have a positive impact on all
stakeholders involved. However upon closer investigation the true impact of
interference may be more harmful to all stakeholders in the long run.

iii
DECLARATION
I, Johanna Magdalena Pretorius, declare that this research report is my own
work except as indicated in the references and acknowledgements. It is
submitted in partial fulfilment of the requirements for the degree of Master of
Business Administration in the University of the Witwatersrand, Johannesburg.
It has not been submitted before for any degree or examination in this or any
other university.
-------------------------------------------------------------
Johanna Magdalena Pretorius
Signed at Centurion
On the …………………………….. day of ………………………… 2011

iv
DEDICATION
A dream sets out as an idea and becomes a reality through action. The
process and completion of the MBA degree proved to be a life changing event
for me. This was a confirmation that absolutely anything can be done through
setting the goal, creating a solid support system and daily deliberate action.
I would like to make this dedication with respect to some incredible individuals
who were instrumental to realising the goals in my life:
My incredible and supportive mother, who taught me that absolutely anything
can be done providing that you believe in yourself. I am eternally grateful for
your incredible love and support, Mom.
Sunél, for your continuous support and belief, even when the emotions ran high.
You are an amazing solid person. I am honoured to have you in my life.
Dr. Jeanette Lotter for the motivation, guidance, encouragement and support
regarding this research.
Prof. Bick for your direction, time and continuous support as supervisor and
lecturer.

v
ACKNOWLEDGEMENTS
MBA Class of 2008 / 2011 for showing me that the impossible can be done,
over and over again. You guys are amazing.
Sudier Ramparsad for the initial motivation to start with this degree. You will
always be a mentor and significant influence in my life.
Nevi Letcher for your continuous support as friend and mentor. I am blessed
with such an outstanding and talented friend.

vi
TABLE OF CONTENTS
ABSTRACT ..................................................................................... II
DECLARATION .............................................................................. III
DEDICATION ................................................................................ IV
ACKNOWLEDGEMENTS ............................................................... V
LIST OF TABLES ........................................................................... X
LIST OF FIGURES ...................................................................... XII
CHAPTER 1: INTRODUCTION ..................................................... 1
1.1 PURPOSE OF THE STUDY ............................................................................ 1
1.2 CONTEXT OF THE STUDY ............................................................................. 1
1.3 PROBLEM STATEMENT ................................................................................ 4
1.3.1 MAIN PROBLEM ...................................................................................................... 4
1.4 SIGNIFICANCE OF THE STUDY ...................................................................... 4
1.5 DELIMITATIONS OF THE STUDY..................................................................... 4
1.6 DEFINITION OF TERMS AND ABBREVIATIONS ................................................. 5
1.7 ASSUMPTIONS ........................................................................................... 6
CHAPTER 2: LITERATURE REVIEW ........................................ 7
2.1 INTRODUCTION .......................................................................................... 7
2.2 GENERAL PRICING METHODS ...................................................................... 7
MARKUP PRICING ............................................................................................................... 9 TARGET-RETURN PRICING ................................................................................................... 9 PERCEIVED-VALUE PRICING ................................................................................................ 9 VALUE PRICING .................................................................................................................. 9 GOING-RATE PRICING ...................................................................................................... 10 AUCTION-TYPE PRICING ................................................................................................... 10
2.3 PRICING IN THE PHARMACEUTICAL INDUSTRY .............................................. 10
2.4 THE IMPACT OF THE IMPLEMENTATION OF SINGLE EXIT PRICE (SEP) FOR PHARMACEUTICALS IN THE PRIVATE SECTOR IN SOUTH AFRICA .................... 13
2.4.1 PRICING REGULATION OR CONTROL IN DEVELOPED COUNTRIES ............................... 15 2.4.2 PRICING REGULATION / CONTROL IN DEVELOPING COUNTRIES ................................. 18 2.4.3 PRICING REGULATION / CONTROL IN SOUTH AFRICA ............................................... 23
2.5 CONCLUSION ........................................................................................... 25
2.6 RESEARCH QUESTIONS ............................................................................ 25
2.6.1 RESEARCH QUESTION 1 ....................................................................................... 25

vii
2.6.2 RESEARCH QUESTION 2 ....................................................................................... 25
CHAPTER 3: RESEARCH METHODOLOGY ............................. 26
3.1 RESEARCH METHODOLOGY /PARADIGM ...................................................... 26
3.2 RESEARCH DESIGN .................................................................................. 27
3.3 POPULATION AND SAMPLE......................................................................... 28
3.3.1 POPULATION ........................................................................................................ 28 3.3.2 SAMPLE AND SAMPLING METHOD ........................................................................... 28
3.4 THE RESEARCH INSTRUMENT .................................................................... 28
3.5 PROCEDURE FOR DATA COLLECTION .......................................................... 29
3.6 DATA ANALYSIS AND INTERPRETATION ....................................................... 29
3.7 LIMITATIONS OF THE STUDY ....................................................................... 30
3.8 VALIDITY AND RELIABILITY ......................................................................... 30
3.8.1 EXTERNAL VALIDITY .............................................................................................. 31 3.8.2 INTERNAL VALIDITY ............................................................................................... 31 3.8.3 RELIABILITY ......................................................................................................... 31
CHAPTER 4: PRESENTATION OF RESULTS ........................... 32
4.1 INTRODUCTION ........................................................................................ 32
4.2 DEMOGRAPHIC PROFILE OF RESPONDENTS ................................................ 32
4.3 RESULTS PERTAINING TO RESEARCH QUESTION 1 ...................................... 36 4.3.1 RESEARCH QUESTION 1 ...................................................................................... 36 4.3.2 RESULTS RESEARCH QUESTION 1 ....................................................................... 36 4.3.3 CONCLUSION – RESEARCH QUESTION 1 .................................................................. 40
4.4 RESULTS PERTAINING TO RESEARCH QUESTION 2 ...................................... 40
4.4.1 RESEARCH QUESTION 2 ...................................................................................... 40 4.4.2 RESULTS RESEARCH QUESTION 2 ....................................................................... 40 4.4.2.1 RESEARCH INSTRUMENT 2 – QUESTION B1 ....................................................... 43 4.4.2.2 RESEARCH INSTRUMENT 2 – QUESTION B2 ....................................................... 45 4.4.2.3 RESEARCH INSTRUMENT 2 – QUESTION B3 ....................................................... 49 4.4.2.4 RESEARCH INSTRUMENT 2 – QUESTION B4 ....................................................... 51 4.4.3 CONCLUSION RESEARCH QUESTION 2 ............................................................... 54
4.4 SUMMARY OF THE RESULTS ...................................................................... 54
CHAPTER 5: DISCUSSION OF THE RESULTS ......................... 55
5.1 INTRODUCTION ........................................................................................ 55
5.2 DEMOGRAPHIC PROFILE OF RESPONDENTS ................................................ 55
5.3 DISCUSSION PERTAINING TO RESEARCH QUESTION 1 ................................. 56
5.3.1 DISCUSSION PERTAINING TO RESEARCH QUESTION 1 ............................ 56 5.3.1.1 THE IMPACT OF THE IMPLEMENTATION OF SINGLE EXIT PRICE (SEP) FOR
PHARMACEUTICALS IN THE PRIVATE SECTOR IN SOUTH AFRICA ............................... 56

viii
5.3.2 CONCLUSION – RESEARCH QUESTION 1 ..................................................... 57
5.4 DISCUSSION PERTAINING TO RESEARCH QUESTION 2 ................................. 58 5.4.1 RESEARCH QUESTION 2................................................................................. 58 5.4.2 DISCUSSION PERTAINING TO RESEARCH QUESTION 2 ............................ 58 5.4.2.1 THE INFLUENCE OF THE INTRODUCTION OF SEP IN THE BUSINESS STRATEGY OF THE
PHARMACY .......................................................................................................... 59 5.4.2.2 THE CHANGES IMPLEMENTED IN ORDER TO SURVIVE AS A RESULT OF THE
INTRODUCTION OF SEP ........................................................................................ 60 5.4.2.3 THE DAY-TO-DAY CHANGES BROUGHT ABOUT WITH THE INTRODUCTION OF SEP ...... 61 5.4.2.4 RESTRUCTURING WITHIN THE PHARMACY AS A RESULT OF THE INTRODUCTION OF SEP
........................................................................................................................... 62 5.4.3 CONCLUSION - TO RESEARCH QUESTION 2 ................................................ 63
5.5 CONCLUSION ........................................................................................... 63
CHAPTER 6: CONCLUSIONS AND RECOMMENDATIONS ....... 65
6.1 INTRODUCTION ........................................................................................ 65
6.2 CONCLUSIONS OF THE STUDY ................................................................... 65 6.2.1 RESPONSE TO RESEARCH QUESTION 1 ................................................................. 66 6.2.2 RESPONSE TO RESEARCH QUESTION 2 ................................................................. 67
6.3 RECOMMENDATIONS ................................................................................ 68
6.4 SUGGESTIONS FOR FURTHER RESEARCH ................................................... 70
REFERENCES .............................................................................. 71
APPENDIX A QUANTITATIVE DATA (SCRIPT PRICING) ........... 77
INTERVIEWER ADMINISTERED QUESTIONNAIRE ...................................................... 78
APPENDIX B QUALITATIVE DATA ............................................. 79
SEMI-STRUCTURED INTERVIEW .................................................................. 80
APPENDIX C ADDITIONAL TABLES .......................................... 82
TABLE 12: THE INFLUENCE OF SEP ON THE BUSINESS STRATEGY OF INDEPENDENT
PHARMACIES .......................................................................................... 82
TABLE 13: THE INFLUENCE OF SEP ON THE BUSINESS STRATEGY OF GROUP PHARMACIES .......................................................................................... 83
TABLE 14: THE INFLUENCE OF SEP ON THE BUSINESS STRATEGY OF HOSPITAL
PHARMACIES .......................................................................................... 84
TABLE 15: SURVIVAL TACTICS FOLLOWING THE INTRODUCTION OF SEP FOR INDEPENDENT PHARMACIES ...................................................................... 85
TABLE 16: SURVIVAL TACTICS FOLLOWING THE INTRODUCTION OF SEP FOR GROUP PHARMACIES .......................................................................................... 86
TABLE 17: SURVIVAL TACTICS FOLLOWING THE INTRODUCTION OF SEP FOR HOSPITAL
PHARMACIES ........................................................................................... 87

ix
TABLE 18: THE INFLUENCE OF THE IMPLEMENTATION OF SEP REGARDING DAY TO DAY BUSINESS FOR INDEPENDENT PHARMACIES ............................................... 88
TABLE 19: THE INFLUENCE OF THE IMPLEMENTATION OF SEP REGARDING DAY TO DAY BUSINESS FOR GROUP PHARMACIES ......................................................... 88
TABLE 20: THE INFLUENCE OF THE IMPLEMENTATION OF SEP REGARDING DAY TO DAY
BUSINESS FOR HOSPITAL PHARMACIES ..................................................... 89
TABLE 21: THE INFLUENCE OF THE IMPLEMENTATION OF SEP ON THE RESTRUCTURING WITHIN INDEPENDENT PHARMACIES ........................................................... 90
TABLE 22: THE INFLUENCE OF THE IMPLEMENTATION OF SEP ON THE RESTRUCTURING WITHIN GROUP PHARMACIES .................................................................... 90
TABLE 23: THE INFLUENCE OF THE IMPLEMENTATION OF SEP ON THE RESTRUCTURING
WITHIN HOSPITAL PHARMACIES ................................................................. 91
TABLE 24: ACTUAL SCRIPTS PRICED AT FIFTY PHARMACIES (QUANTITATIVE DATA) . 92

x
LIST OF TABLES
Table1: Regulated Dispensing Fees for Pharmacies in the Private Health
Care Sector (Motsoaledi 2010).........................................................14
Table 2: Quantitative, Mixed and Qualitative Methods (Creswell 2009) .......26
Table 3: Demographic Data Including Functional Roles Reported by
Respondents ....................................................................................34
Table 4: Descriptive Statistics for Independent, Group and Hospital
Pharmacies.......................................................................................36
Table 5: ANOVA and Means...........................................................................37
Table 6: Kruskal-Wallis ANOVA......................................................................38
Table 7: Business Strategy Themes in Relation to SEP for Independent,
Group and Hospital Pharmacies.......................................................43
Table 8: Survival Tactics in Relation to SEP for Independent, Group and
Hospital Pharmacies.........................................................................48
Table 9: Day to Day Changes Implemented in Relation to SEP for
Independent, Group and Hospital Pharmacies.................................51
Table 10: Restructuring as a result of the Implementation of SEP for
Independent, Group and Hospital Pharmacies.................................53
Table 11: Comparison of the findings from the literature review and this study
regarding the impact of pricing regulations on the business
environment......................................................................................67
Table 12: The Influence of SEP on the Business Strategy of Independent
Pharmacies.......................................................................................83

xi
Table 13: The Influence of SEP on the Business Strategy of Group
Pharmacies.......................................................................................84
Table 14: The Influence of SEP on the Business Strategy of Hospital
Pharmacies.......................................................................................84
Table 15: Survival Tactics Following the Introduction of SEP for Independent
Pharmacies.......................................................................................85
Table 16: Survival Tactics Following the Introduction of SEP for Group
Pharmacies.......................................................................................86
Table 17: Survival Tactics Following the Introduction of SEP for Hospital
Pharmacies.......................................................................................87
Table 18: The Influence of the Implementation of SEP Regarding Day to Day
Business for Independent Pharmacies.............................................88
Table 19: The Influence of the Implementation of SEP Regarding Day to Day
Business for Group Pharmacies.......................................................88
Table 20: The Influence of the Implementation of SEP Regarding Day to Day
Business for Hospital Pharmacies....................................................89
Table 21: The Influence of the Implementation of SEP on the Restructuring
within Independent Pharmacies........................................................90
Table 22: The Influence of the Implementation of SEP on the Restructuring
within Hospital Pharmacies...............................................................90
Table 23: The Influence of the Implementation of SEP on the Restructuring
within Hospital Pharmacies...............................................................91
Table 24: Actual Scripts Priced at Fifty Pharmacies..........................................92

xii
LIST OF FIGURES
Figure 1: Price Regulations and Dynamics in the Pharmaceutical Industry in
South Africa (Economist Intelligence Unit 2005, 2009d; Gray 2009)
......................................................................................... ................14
Figure 2: Histogram of the Distribution of the Quantitative Data........................38
Figure 3: Box Plot of the Independent, Group and Hospital Pharmacy
Quantitative Data..............................................................................39
Figure 4: The Influence of SEP on the Business Strategy of the Independent
Pharmacy..........................................................................................41
Figure 5: The Influence of SEP on the Business Strategy of the Group
Pharmacy..........................................................................................41
Figure 6: The Influence of the SEP on the Business Strategy of the Hospital
Pharmacy..........................................................................................42
Figure 7: Survival Tactics Following the Introduction of SEP for Independent
Pharmacies ......................................................................................46
Figure 8: Survival Tactics Following the Introduction of SEP for Group
Pharmacies.......................................................................................46
Figure 9: Survival Tactics Following the Introduction of SEP for Hospital
Pharmacies.......................................................................................47
Figure 10: The Influence of the Implementation of SEP Regarding Day to Day
Business for Independent Pharmacies.............................................50
Figure 11: The Influence of the Implementation of SEP Regarding Day to Day
Business for Group Pharmacies.......................................................50
Figure 12: The Influence of the Implementation of SEP Regarding Day to Day
Business for Hospital Pharmacies....................................................50

xiii
Figure 13: The Influence of the Implementation of SEP on the Restructuring
within Independent Pharmacies........................................................52
Figure 14: The Influence of the Implementation of SEP on the Restructuring
within Group Pharmacies..................................................................52
Figure 15: The Influence of the Implementation of SEP on the Restructuring
within Hospital Pharmacies...............................................................53

1
CHAPTER 1: INTRODUCTION
1.1 Purpose of the study
The purpose of this research is to analyse the impact of the implementation of
the Single Exit Price (SEP) for pharmaceuticals (medicines and scheduled
substances) in South Africa. The research ascertains whether the
implementation of the legislated SEP results in a consistent cost saving benefit
for the general public in the private healthcare sector in South Africa. Further to
this the research established the perceived impact of SEP on retail pharmacies
in South Africa in terms of changes in the business environment.
1.2 Context of the study
The healthcare system in South Africa consists of a large public sector,
considered to include 82% of the population and a growing but smaller private
sector (Brand South Africa 2009). The private sector, with an estimated 18% of
the population is responsible for approximately 80% of the drug expenditure for
South Africa. The public sector however, servicing 82% of the population is
responsible for only 24% of the approximate R8.5 billion in total annual drug
expenditure (Department of Health 1996; Brand South Africa 2009). Public
sector facilities are used primarily by low income residents while high income
and medically insured residents make use of private doctors and healthcare
facilities (Gilson and McIntyre 2007). The per capita spending on drugs in the
private sector is estimated to be 10 times that of the public sector and therefore
diminishes chances of patients in the public sector to afford these costs and
receive improved treatment (Gray and Matsebula 2000).
Globally the economics of the pharmaceutical industry has been investigated for
more than 40 years (Scherer 2004; Gray 2009). The objective for further and
intensive investigation in post-apartheid South Africa, was to improve access to
healthcare services for previously disadvantaged citizens (Gray 2009). To
improve access to healthcare for these citizens in South Africa, a National Drug

2
Policy (NDP) was developed, approved by the Cabinet and published in 1996
(Department of Health 1996). Following the publication of this document, the
NDP was tasked to develop a pricing plan for medication used in South Africa,
for both the private and the public sector (Gray 2009). Following this, the
amended Medicines and Related Substances Act was introduced to legislate
the process with two inter-related sections – (Section 18A banning bonusing)
(preventing pharmaceutical manufacturers from offering discounts and/or
rebates to patients or healthcare providers) and Section 22G which created a
Pricing Committee (Gray 2009).
The SEP mechanism was then introduced for all medicines in the private
healthcare sector in South Africa, stipulating regulated maximum annual price
increases (Bodhania 2007). The implementation of SEP effectively meant that
the private sector had to adjust from a free market, to a regulated market where
prices had to be cut and all discounts discarded, ensuring transparent pricing
practices for the industry (Advanstar Communications 2009). The SEP became
a fixed maximum price at which manufacturer and importers had to sell
medicine, without an opportunity for offering discounts. This process resulted in
a decrease of gross profit margins within independent, group and hospital
pharmacies in the private healthcare sector. However, pharmaceutical
wholesalers and distributers were entitled to a logistics fee, included in the SEP,
for their service (Gilson and McIntyre 2007). The introduction of SEP in 2004,
lead to an immediate net pricing impact of 19% in that year and there were no
allowances for price increases within the private sector between 2003 – 2006
(Bodhania 2007). It appears that the introduction of SEP was beneficial to the
patient in terms of the drastically reduced costs of medication. However Calfee
(2001) notes that price controls for pharmaceuticals (like SEP in South Africa),
could tend towards complexity and the creation of vested interests, which could
become permanent and eventually lead to a negative impact on the patients.
Despite the implementation of SEP, medicine expenditure at a private
healthcare insurance level is still rising. According to Mediscor, an
administrator for certain medical insurance companies in South Africa, there is
still a marked increase in year on year medicine expenditure (Bester 2009).

3
Factors influencing the increase in medicine expenditure include an increase in
the utilisation of member benefits, changes in medicine mix used by the
population as well as more expensive therapies (Bester 2009). It could be
concluded that, despite the positive net impact of SEP, the rise of medicine
expenditure has a countering and negative impact on the cost of medicine in the
private sector for patients. However, the Council for Medical Schemes’ Annual
Report for 2008 – 2009 clearly shows that, although total medicines expenditure
is on the increase, the actual expenditure (“benefits paid”) per beneficiary per
month has remained near consistent since the introduction of SEP (Council for
Medical Schemes 2009). This clearly indicates that the increase in expenditure
per annum may well be due to an increase in the number of beneficiaries (i.e.
patients using the private medical insurance), rather than increased utilisation
(more medicines per patient), or increase in actual medicines costs (Lotter
2010a).
A more pertinent question is whether the benefits of the SEP effectively benefits
all private patients to an equal extent, i.e. whether the actual medicine prices
charged in the private sector are consistent across the broad range of
providers. In simple terms, the question has become whether the same
medicine would cost the same amount of money, irrespective of where it is
acquired in the private sector (from an independent, group owned pharmacy or
private hospital pharmacy) despite the Government’s strict medicine pricing
policies. Independent pharmacies refer to pharmacies owned either by an
individual or several partners, where the pharmacy does not form part of a
group owned pharmacy or a hospital pharmacy.
An analysis of the impact of the implementation of the SEP for medicines and
scheduled substances in South Africa aimed to establish the impact of the
implementation of the legislated SEP.

4
1.3 Problem statement
1.3.1 Main problem
Analyse the impact of the implementation of Single Exit Price (SEP) for
pharmaceuticals in the private sector in South Africa.
1.4 Significance of the study
The study investigates whether the cost benefits of SEP has in fact filtered
down in a consistent and predictable manner to a patient level in the private
healthcare sector in South Africa.
Various reports investigate the implementation of pharmaceutical price controls
as well as global pricing regulations for the pharmaceutical industry (Calfee
2001; Anon 2006; Pharmaceutical Executive 2006; Gilson and McIntyre 2007;
Gray 2009). However there is no current publication available to determine,
firstly, if the benefit of SEP is in fact consistently drawn by patients in the private
healthcare sector through consistency in price in South Africa and secondly
what the influence and changes were in the business environment of
pharmacies in the private healthcare sector in South Africa .
The study provided insight into the effectiveness of the drug pricing policy in
South Africa to both patients and pharmacies, and identified potential additional
areas for further legislation to be implemented, ultimately resulting in improved
regulation and benefits to the patient.
1.5 Delimitations of the study
This study only focuses on the private healthcare sector in South
Africa because SEP is only applicable to the private sector.

5
1.6 Definition of terms and Abbreviations
• Single Exit Price (SEP) – refers to a transparent pricing system
pertaining to all medicines and scheduled substances sold to any other
person except for the state in South Africa (Tshabalala-Msimang 2004).
SEP includes a logistics fee from pharmaceutical wholesalers and
distributors for their service (Gilson and McIntyre 2007). This price is
printed onto the container of the particular medicine or scheduled
substance and is deemed the fixed maximum selling price of medicine,
excluding the dispensing fee issued by a pharmacy (Tshabalala-
Msimang 2004).
• Market Access – the ability of a pharmaceutical manufacturer to sell its
medicines to patients often determined or restricted by procurement
policies (in South Africa; the tender system in the public sector and
medical scheme formularies in the private sector).
• Prescribed Minimum Benefit (PMB) – is a set of defined benefits to
ensure that all medical scheme members have access to certain
minimum health services, regardless of the benefit option they have
selected. The aim is to provide people with continuous care to improve
their health and well-being and to make healthcare more affordable
(Council for Medical Schemes 2010).
• Chronic Disease List (CDL) – specifies medication and treatment for the
25 chronic conditions that are covered in this section of the PMB’s
(Council for Medical Schemes 2010).
• National Drug Policy (NDP)
• Medicare Modernization Act (MMA)
• Drug Price Control Order (DPCO)
• Health Maintenance Organisations (HMO’s)
• Pharmacy Benefit Managers (PBM’s)

6
• Patented Medicines Prices Review Board (PMPRB)
• Preferred Provider Organisations (PPO’s)
• The National Health Service (NHS)
• Trade Related Aspects of Intellectual Property Rights (TRIPS)
1.7 Assumptions
The following assumptions have been made regarding the study:
a) Data were obtained from pharmacies in the private sector in South Africa
and the pharmacist had the correct information regarding the specific
price of the medication to be paid by the patient.
b) The pharmacist or pharmacist assistant was able to share information
regarding the price of the specific drug included in the study.
c) Pricing information was conveyed honestly and truthfully by the
respondents.

7
CHAPTER 2: LITERATURE REVIEW
Carnwell and Daly (2001) explain that the rationale behind a literature review is
to evaluate and combine or create a total picture of the currently available
information relating to the topic that is being researched.
Further to this, the purpose of the literature review is to identify gaps in the
available literature that will be addressed by new research. One of the most
important focal points of a review of high standard is to strategise well around
the literature search and selection of references (Carnwell and Daly 2001). The
literature review should assist in defining and perfecting the research question
and focus on designing future research.
2.1. Introduction
The focus point of the literature review for this research topic is on relevant
points to the study regarding the impact of the implementation of regulated
pricing within the pharmaceutical environment. The first section of the literature
review is focuses on pricing regulation or control in developed countries, while
the second section focuses on pricing regulation or control in developing
countries. Finally, pricing regulation or control in South Africa is investigated.
2.2. General Pricing Methods
The marketing mix comprises of product, price, promotion and place. The only
element of the marketing mix that produces profits is price (Marn and Rosiello
1992b, 1992a; Kotler and Keller 2006). Product, promotion and place all
produce costs. Price also communicates a company’s value positioning in
terms of a brand (Kotler and Keller 2006). Price might be the easiest
component to adjust in terms of the marketing mix.
One of the benefits of the introduction of price regulation through price caps is
the reduction in excess profits (Gilmore, Branston and Sweanor 2010). This
implies that consumers should benefit from this reduction in the event that the

8
full benefit is passed on to them. However, according to Philibert, (2009),
strict targets in terms of price caps and price floors may cause great economic
risk without a comparative advantage. The impact of pricing regulation may
entail risk and not necessarily result in an advantage for the consumer.
The available literature further explains that the existence of price caps
determine productivity trends (Lowry and Getachew 2009). Businesses would
seek to be more productive, particularly following the introduction of price caps.
Pricing regulation in the form of price caps leads to more efficient capital
replacement decisions (Biglaiser and Riordan 2000). The effect of pricing
regulations will therefore influence decision making within a business in terms of
more efficient management of funds.
Price regulation and specifically the introduction of price ceilings, may result in
perverse effects (Knittel and Stango 2003). Business may therefore resolve to
perverse actions in order to make up the lost profit, due to price regulation.
Reduction in overheads and overall business costs is a direct reaction to price
cap regulation. Price cap regulations create an incentive for businesses to
reduce service quality (Currier 2006).
Pricing methods are selected based on the following (Kotler and Keller 2006):
• costs as a setting for a floor price
• competitor and substitute prices as an orientation point
• customer assessments of the unique features as a price ceiling
A variety of pricing methods exist. The same pricing methods are not best
suited for all customers. It is therefore important to match the usage of a
pricing method to targeted consumer profiles to realise the most positive results
(Munnukka 2006). Various pricing methods are considered below e.g. mark-up
pricing, target-return pricing, perceived-value pricing, value pricing, going-rate
pricing and auction type pricing (Kotler and Keller 2006).

9
Mark-up Pricing
This is the most elementary method of pricing, where a standard cost as mark-
up is added to the product’s cost (Kotler and Keller 2006). For this reason a
firm does not have to forecast or predict the future (Naish 1990). However this
pricing method disregards current demand, perceived value and competition.
Lawyers and accountants utilise this pricing method (Kotler and Keller 2006).
Target-return Pricing
A price is determined by considering what is needed to yield the rate of return
on investment (Lavoie 1996). This method is dependent on a certain number of
unit sales to ensure arriving at a breakeven point. This method ignores price
elasticity and competitor pricing (Lavoie 1996; Kotler and Keller 2006). For
example, this method is used by i.e. General Motors and public utilities that
need to make a fair rate on return (Kotler and Keller 2006).
Perceived-Value Pricing
This pricing method is becoming increasingly popular among companies,
pricing products at the perceived value according to the customer, delivering the
value promised through the value proposition (Kortge and Okonkwo 1993;
Kotler and Keller 2006). Caterpillar utilizes this price method. Customers pay a
premium price, but collect more than the value of the premium price throughout
the year (Kotler and Keller 2006).
Value Pricing
Value pricing is a product of adjusting the supply chain to realise better value at
every point resulting in a lower price offering to consumers. Value pricing is
based on charging constant low prices with little or no promotion thus
rewarding loyal customers (Ailawadi, Lehmann and Neslin 2001). Company
operations are re-evaluated when utilising value pricing to ensure that they
become a low-cost producer without sacrificing quality, attracting many value

10
conscious customers (Kotler and Keller 2006). This pricing method is used by
IKEA, Wallmart and Southwest Airlnes.
Going-Rate Pricing
Prices are mostly based on competitor pricing by charging more, less or the
same as the competitor (Mochtar and Arditi 2000). In oligopolistic industries the
same price is normally charged in relation to the competitor considering
markets such as, the steel industry, paper industry or the fertilizer industry.
The leader companies are generally followed in terms of pricing. The method
is popular when competitor response is uncertain (Kotler and Keller 2006).
Auction-Type Pricing
The major purpose of auctions is to sell excess inventories or goods. This
pricing method has increased in popularity with the growth of the internet
(Kotler and Keller 2006; Design and Marketing Dictionary 2011).
This section explores the effect of pricing regulation as well as various pricing
methods, including examples of the industries or major corporations utilising
specific methods for pricing. The pharmaceutical market is unique in terms of
the industry dynamics. The following section explores pricing regulation within
the pharmaceutical industry.
2.3. Pricing in the pharmaceutical industry
“Medicines are priceless and therefore pharmaceutical companies should be left
to charge market prices” (Maitland 2002:451). This is quite a controversial
statement in light of the fact that the pharmaceutical industry is under
continuous pressure globally to decrease medicine prices. However, a closer
look at the principles of the pharmaceutical market is crucial for clear
understanding.

11
The majority of markets including food, appliances, clothing, homes and
electronics, function within the basic principle that a transaction is finalised,
once the seller agrees to sell an item for the amount offered by the buyer. The
pharmaceutical market does not function according to these principles and is a
unique market in the sense that patients / buyers do not select their medication;
which is rather prescribed by a physician. The consumer / patient in this case
does not have any knowledge regarding competitors in terms of effectiveness
and comparative pricing (Gray 2009). Pharmaceutical demand is relatively
inelastic (Docteur, Paris and Moise 2008a). Manufacturers of ethical, patented
medicine will have a monopoly in a specific market where they have a unique
product. The potential to take advantage of this monopoly was previously
recognised by global governments, leading to pricing regulations within the
pharmaceutical industry (Docteur et al. 2008a).
Various policy options exist for governments globally to regulate prices within
the pharmaceutical industry (Gray 2009). These include:
• Producer price control measures including direct price and profit controls,
reference pricing systems and therapeutic reference pricing, equity
pricing, international benchmark pricing and generic friendly policies
• Distribution chain cost controls including controls over mark-up, fixed
professional fees, removal or limits on tax
• Bulk purchase measures or tender and negotiation strategies and
regional activities
• International trade agreement relief measures including parallel importing
and compulsory licensing
• Demand side measures including measures to guarantee sensible
medicine use i.e. setting up formularies to utilise medicines and
medicinal budgets for doctors
The method of internal price referencing compares new product prices to prices
already paid by others for similar medication or medication of the same

12
therapeutic class. External price referencing involves a comparison for prices of
new medicines to prices already paid by other payers in other countries
(Docteur, Paris and Moïse 2008b).
Pharmaco-economic assessment has been incorporated in the pricing and
reimbursement practices of an evaluation method to determine the benefits of a
product relative to its costs (Docteur et al. 2008b). Pharmaco-economic
assessment ranges from information requests to pharmaceutical companies
regarding relative cost effectiveness in support of reimbursement applications to
conducting original assessments regarding the benefits that would be derived
from use of a product and expected costs to payers or society in general
(Docteur et al. 2008b).
Price regulation can affect cost and quality indirectly or directly.
The direct effect of price regulation would focus on affecting the prices and use
of existing medication. The indirect effect would amend or change the incentive
for pharmaceutical firms to engage in research and development (R & D) of new
drugs (Calfee 2001; Kessler 2004). Empirical research has found that price
regulation has adverse effects on the cost and quality of healthcare (Kessler
2004). It is evident in the literature that there is a stifling impact on investment,
regarding research and development for innovative lifesaving drugs with the
introduction of price regulation in the pharmaceutical industry (Oriola 2009).
Globally different countries implement various pricing regulation procedures.
There is no universal agreed practice for pricing regulations within the
pharmaceutical industry, therefore one needs to analyse each country situation
individually.
In order to view the various pricing regulation procedures, developed countries
and developing countries will be grouped together. From the literature it is
evident that South Africa is unique in terms of the pricing regulation procedures
and for this reason pricing regulations in South Africa will be viewed individually

13
2.4. The impact of the implementation of Single Exit Price
(SEP) for pharmaceuticals in the private sector in South
Africa
Various price control mechanisms have been introduced to regulate prices of
medicines in the South African pharmaceutical market for example price
ceilings or SEP, capped annual price increases as well as mandatory generic
substitution pertaining to medicines with expired patents. The combination of
the introduction of SEP and capped annual price increases lead to an overall
decrease of 22 % in medicine prices in South Africa in the first year after the
introduction of SEP (McIntyre and Thiede 2007; Lotter 2010b). This reduction
pertains to medicine selling prices for pharmacies in South Africa.
The SEP in South Africa is also considered as the selling price to wholesalers in
the South African pharmaceutical market as medicines are sold at this price to
wholesalers. Logistics fees paid by the various pharmaceutical companies are
included in this selling price and the process is not regulated. Previously
logistics fees were added on top of the wholesaler selling price.
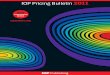
Medicines are sold into retail pharmacies in South Africa at the SEP. A
regulated dispensing fee is then added to the SEP to determine the selling price
to patients, as indicated in Figure 1. The dispensing fee regulation was
published on the 19th of November 2010 (Motsoaledi 2010). A maximum
percentage dispensing fee may be levied on top of the SEP based on a four
tiered regulation, set out in Table 1.

14
Figure 1: Price Regulations and Dynamics in the Pharmaceutical Industry
in South Africa (Economist Intelligence Unit 2005, 2009d; Gray 2009;
Lotter 2010b)
Table: 1 Regulated Dispensing Fees for Pharmacies in the Private Health
Care Sector (Motsoaledi 2010)
To fully understand the impact of existing pricing regulation in SA there is a
need to view this within the global context. A brief discussion of existing pricing
regulation / control in different countries (developed or developing) is provided
below.
Pharmaceutical Industry
Price Control for Medicines in the Private Sector in South Africa – Regulated by Department of Health
• SEP / Price Ceilings – 22 % Price Decrease
• Capped Annual Price Increases
• Mandatory Generic Substitution with Patent Expiry
Wholesaler
Logistics Fee Included in SEP – Not Caped at Specific % (not regulated)
Pharmacist
Sell at SEP + Dispensing Fee (Regulated since Nov 2011)
Patient / Consumer
Price of Scripted Medicine

15
2.4.1 Pricing regulation / control in developed countries
The pricing regulation / control mechanism varies from country to country.
Extensive research from the literature reveals the differences and similarities for
each country below.
Germany was the first country to roll out reference pricing (Docteur et al.
2008b). Reimbursement prices of pharmaceutical products are controlled
indirectly through limits on reimbursement within social insurance schemes and
doctors are allocated with drug budgets (Danzon 1999; Vernon 2002).
Substitution of generic branded equivalents is allowed in Germany and it is
believed that this executes further downward pressure on medicines prices
(Danzon 1999).
The United States of America (USA) is home to the world’s most competitive
pharmaceutical market (Oriola 2009). Prices of prescription medication are
largely unregulated in the USA due to the belief that price controls would
negatively impact on the investment in research and development for new
innovator medicines (Oriola 2009). Medicine prices in America are reported to
be 72 % higher than Canada and 102 % higher than in Mexico (Danzon 1999).
A strong argument exists that medicines prices are excessive in the USA and
that price controls would ensure affordable health care for all Americans. The
opposing argument creates fear regarding the incentive for pharmaceutical
companies to continuously invest in research and development of new
medicines (Vernon 2002). Although minimal price regulations exist in the USA,
Health Maintenance Organisations (HMO’s) and Pharmacy Benefit Managers
(PBM’s) create a list of preferred drugs to be used, known as formularies to
encourage physicians and patients to use these preferred drugs via price
incentives (Atella, Bhattacharya and Carbonari 2008). The purpose of the
introduction of the Medicare Modernization Act (MMA) in 2003, with a focus on
private health care plans, was to bridge divide between prescription medicine
for rich and poor recipients in America (Bakk 2009; Oriola 2009). The MMA
provided enhanced payments and financial incentives to health maintenance
organisations (HMO’s), established a network of preferred provider
organisations (PPO’s) as well as private fee-for-service plans (PFFS) (Bakk

16
2009). Generic medicines account for 46 % of prescriptions in the USA (Danzon
1999).
Price regulations for patented medicines in Canada aligned Canadian
pharmaceutical prices with European prices. Prices for off-patent and generic
pharmaceutical medicines are not regulated in Canada. Patented medicines
prices have been regulated since 1987 by the Patented Medicines Prices
Review Board (PMPRB), and price regulations are limited to the patent lifetime
only.
The proposed Canadian price for a newly registered medication is compared to
prices of existing medicines in Canada, or to prices in seven markets
designated in the regulations. These markets are: France, Germany, Italy,
Sweden, Switzerland, the United Kingdom and the United States (Paris and
Docteur 2009). All Canadians have access to medication provided in hospital
through a publically financed scheme, addressing hospital and physician
services at no cost. Medication dispensed outside of the hospital is not
considered under the insured benefits guaranteed by the Canadian Health Act.
For this reason, 66% of the Canadian population realises this coverage through
private health insurance, often accompanied by co-payments (Paris and
Docteur 2009).
Pharmaco-economic assessment has been incorporated in the pricing and
reimbursement practices in Canada (Docteur et al. 2008b). Substitution of
generic branded equivalents is allowed in Canada (Danzon 1999). The Federal
Government in Canada controls prices of new products and post launch prices
may not rise faster than the consumer price index (Danzon 1999).
Private health insurance accounted for 25 % of pharmaceutical expenditure in
2005. Approximately 61% of the pharmaceutical expenditure was derived from
the private sector (Docteur et al. 2008b). Private health insurance is the leading
source for of coverage for medicines and covers approximately 66 % of the
population (Docteur et al. 2008b; Paris and Docteur 2009).
Pharmaco-economic assessment is incorporated in the pricing and
reimbursement practices in Australia (Docteur et al. 2008b). The

17
Pharmaceutical Benefits Scheme (PBS) offers Australians government
subsidised prescription medicines at a cost that individuals in the community
can afford. This forms the central mechanism in Australia for supply of
prescription medication. Cost effective analysis, comparing existing products
and therapies to new products, determine PBS prices. Through this system, the
Australian government ensures strong market power to ensure relatively low
prescription medicine prices (Gray 2009). Generic prescription medicine prices
historically mimicked the prices of originator medicines as additional pressure
was evident on generic medicines due to extensions on patent expiry.
Patent extensions are believed to be one of the main reasons for the under-
penetration of generics in the Australian market. Generics cannot be produced
in Australia for export purposes whilst such a patent has not expired, therefore
global generic companies are selecting non-Australian facilities for
manufacturing purposes (Gray 2009).
The United Kingdom (UK) has utilised pharmaco-economic analysis or
economic evaluations to determine what the national healthcare system should
pay for therapeutic drug classes (Appasamy 2007).
The National Health Service (NHS) in the United Kingdom (UK), controls 95% of
the prescription drug market (Appasamy 2007). Indirect price controls feature in
the United Kingdom (UK). This is enforced by controlling profits (Danzon 1999;
Vernon 2002; Williams 2007). Companies with capital in the UK negotiate
around a reasonable rate of return on capital employed. Companies without
capital in the UK negotiate on the basis of reasonable rate of return on sales
(Williams 2007). Further downward pressure on medicines prices is established
by enforcing generic branded substitution at pharmacy level (Danzon 1999).
New Zealand utilises indirect price regulation through informal benchmarking
for medicines prices versus specifically identified countries, i.e. Austria, Canada
and the United Kingdom (Williams 2007; Docteur et al. 2008b). New Zealand
also incorporated pharmaco-economic assessments when deciding on
reimbursement applications.
The lowest generic prices are found in New Zealand (Docteur et al. 2008b).

18
In Belgium, pharmaceutical prices are regulated through controlling launch
prices of newly introduced medicines as well as the control of reimbursement
prices (Vernon 2002). External price benchmarking is utilised through a focus
on countries including, Austria, Finland, Greece, Hungary, Iceland, Netherlands,
Norway, Spain and the UK (Docteur et al. 2008b; Siva 2009). Pharmaco-
economic assessments are also utilized to evaluate reimbursement applications
for newly registered medicines, adding therapeutic value compared to existing
therapeutic alternatives (Docteur et al. 2008b).
Comparative European Union (EU) prices are considered in Belgium as
guideline for pricing (Mrazek 2002). Fixed pricing is utilized as a price
regulation mechanism in Belgium, i.e. a set price is allocated to a particular
medicine (Mrazek 2002).
Generic medicines have less than 10% volume and value share in Belgium
(Docteur et al. 2008b).
The following price controls are executed in the Netherlands (Mrazek 2002;
Vernon 2002; Atella et al. 2008; Siva 2009):
• Controlled launch prices (fixed pricing through price ceilings, the
Maximum Price Law introduction in 1996)
• Controlled Reimbursement prices (fixed pricing)
• Reference pricing (based on prices of a basket of countries including the
UK)
• Positive and negative listing
2.4.2 Pricing regulation / control in developing countries
Consumer access to essential medicines in developing countries is mainly
driven or blocked by price (Nóbrega, Marques, de Araújo, Karnikowski, de
Oliveira Silva Naves and Silver 2007). The pricing regulations and controls for
developing countries, excluding South Africa, where researched in the literature
and are stated below.

19
India is the country with the second largest population in the world, however
India only accounts for 1 % of global pharmaceutical sales (Bernstein Global
Wealth Management 2009b).
India is one of the countries with the lowest medicines prices and this is mainly
attributed to price controls introduced in 1970 with the drug price control order
(DPCO). Outpatient drug expenditure is practically not reimbursed (Bernstein
Global Wealth Management 2009b). The government in India set retail prices
for medicines through the DPCO as a profit control mechanism (Joshi 2003;
Gray 2009). A maximum allowable post manufacturing expense (MAPE) is set
by the DPCO (Joshi 2003). The DPCO regulates medicines prices in three tiers
(Bernstein Global Wealth Management 2009b):
• Bulk drugs
• Formulations
• Overall profitability
The DPCO is suggesting wider use of price controls through tighter monitoring
of non-DPCO products, obligatory controls on launch prices which are currently
not controlled as well as a reduction in purchase prices for the government.
The amount of medicines under price controls increased from 79, prior to the
introduction of the 2006 Pharmaceutical Policy to nearly 354 (Bernstein Global
Wealth Management 2009b).
The Brazilian economy poses a good example of a developing country intent
on to reforming its healthcare system through an increased focus on
preventative and primary care medicines as well as a drive behind increased
market penetration of generic medicines without driving increased costs
(Economist Intelligence Unit 2005). Brazil was reasonably free from price
regulations due to a high prevalence of cash paying customers prior to 2006.
The Brazilian government is likely to exercise pressure on pricing of medicines
because many wealthy patients are willing to pay cash for the latest specialized
medicines and are being unfairly charged by excessive drug prices and

20
unfortunately a strong influx of low cost generic and counterfeit medicines
entering Brazil from neighbouring countries (Bernstein Global Wealth
Management 2009a).
The pricing policy of Brazil is being implemented by the Cámara de Regulacão
do Mercado de Medicamentos (CMED), a non-transparent body. The
introduction of the outpatient reimbursement program in Brazil led to stretched
government healthcare budgets. Strict price control is used to control costs, i.e.
combined internal and external reference pricing focused on nine identified
markets, where a price could be higher than the lowest price. Extended
downward price pressure exist by utilizing the difference between the gross
domestic product (GDP) per capita between Brazil and the specific reference
country. The Brazilian government also regulates the annual medicines price
increase.
Higher prices have been established in the launch phase of new and improved
medicine formulations, although this is not common practice. Where competitor
products exist and another medicine is introduced within an existing therapeutic
class, the price is referenced to the class of existing products within the market.
The first generic entry within a therapeutic class is priced as being 35 % more
cost effective compared to the originator branded medicine, being an example
of a price ceiling. With the introduction of additional generics for a specific
therapeutic class, natural downward pressure drives prices down below the
initial ceiling price.
Sufficient availability of essential medicines, i.e. hypertension, infant asthma,
diabetes and some oral contraceptives are provided to the public through the
introduction of a program called, Farmácia Popular in 2006. Private registered
pharmacies provide these medicines at a discount of up to 90 % compared to
everyday retail prices (Bernstein Global Wealth Management 2009a).
Russia experienced a sharp increase in medicine prices in the past years as
the pharmaceutical market size grew from 3.6 Bil US$ in 2003 to10 bil US$ in
2008. This resulted in the introduction of pricing regulations focused on
essential medicines (Economist Intelligence Unit 2009c). The Russian

21
government is concerned about artificially inflated medicines retail prices and
the newly introduced law will tighten price control through limiting mark up on
medicines through wholesale and retail channels. The Russian government is
also increasing their focus on monitoring of pharmaceutical prices.
Egypt occupies the number one position in the Middle East and North Africa in
terms of pharmaceutical consumption and production. To provide medicines to
poor Egyptians, profit margins are controlled and set by the Egyptian
government and is kept between 8 – 10 %. Unfortunately this does not result in
sufficient availability of medicines to poor Egyptians and has a negative impact
on the profitability of pharmaceutical companies in Egypt (Economist
Intelligence Unit 2010). For this reason the Egyptian government introduced
reference pricing, targeting 22 comparator countries. Egypt has however not
introduced the World Trade Organisation’s Trade Related Aspects of Intellectual
Property Rights (TRIPS) agreement, focusing on increased protection of
intellectual property rights (Economist Intelligence Unit 2005). The main reason
for this is the direct implication of a rise in medicines prices in Egypt. The
Pharmaceutical Research and Manufacturers of America (PhRMA) complained
to the US administration in 2005, that the Egyptian government was directly
opposing the TRIPS agreement by granting licenses for hundreds of patented
medicines in Egypt. For this reason Egypt has been on the intellectual property
rights (IPRs) priority watch list since 2005 (Economist Intelligence Unit 2010).
The introduction of the TRIPS agreement is strongly opposed by the Egyptian
generic pharmaceutical industry, because this would directly constrain
manufacturing of generic medicines in the country. However, as the US is
home to a large number of manufacturers of originator (branded) medicines, the
US will not secure a free trade agreement with Egypt prior to the introduction of
the TRIPS agreement pressuring on the government of Egypt (Economist
Intelligence Unit 2010). Currently this dispute is unresolved.
Multinational pharmaceutical companies account for 30 % of local sales through
domestic manufacturing and 35 % through licensing agreements, the remainder
of the market is represented by local generic companies (Economist Intelligence
Unit 2005). To stimulate research and development of new innovative

22
medicines the Egyptian government suggested that prices for all
pharmaceuticals should be set based on benchmarking versus 22 countries.
This recommendation has strongly been opposed by pharmacists, claiming an
increase of 700 % on generic prices due to this suggested price regulation
(Economist Intelligence Unit 2010).
The healthcare system in Israel, is mainly insurance based, covering 95 % of
the population (Economist Intelligence Unit 2005). The Israeli government is
responsible for the finance and access to provision of medical care; however
four non-governmental, non-profit healthcare organisations provide the care by
collecting health care premiums through the National Insurance Institute (NII)
and managing these funds for the provision of a standardised healthcare
package. Competition is encouraged between the four insurers in Israel, by
providing switching options for members, once they have been with the insurer
for a period of a year (Economist Intelligence Unit 2009b). As the healthcare
funds are managed by the four healthcare organisations, doctors effectively
have certain budgets for the provision of healthcare and therefore Israel is
managing healthcare through demand side measures, providing budgets for
medicines and the delivery of healthcare services.
Medicine expenditure accounts for 10 % of total healthcare expenditure in Israel
and the bulk of the expenses is allocated to personnel; however an increase in
medicines expenditure is expected with the rise of the ageing population
(Economist Intelligence Unit 2005).
Due to the low per capita income, medicines prices in Mexico are considerably
lower comparative to the USA and European countries. It is documented that
the prices for medicines in Mexico are lower than most industrialised countries.
Medicine prices are regulated by the Mexican Government. Patent protection
for pharmaceuticals was only introduced in 1991 and medicines already in the
market were not affected by this law. Any newly introduced medication had to
compete with low cost imported generic medicines made as copies to non-
licensed medication. Prescription medicines are widely available in practice, in
Mexico without prescription. Anecdotal evidence suggests that retail

23
pharmacists compete by offering products at prices, below those set by
government (Danzon 1999).
Greece has the largest number of pharmacies per person ratio of any European
Union (EU) country (Economist Intelligence Unit 2009a). The improvement of
the healthcare systems is of major importance for the Greek government
(Economist Intelligence Unit 2009a). Pharmaceutical prices in Greece are
considered to be amongst the lowest in Europe (Economist Intelligence Unit
2009a).
All pharmaceutical prices are controlled through set retail prices this includes
fixed margins for wholesalers and retailers (Economist Intelligence Unit 2005,
2009a). International benchmarking was introduced as further price control
mechanism in 2005, by comparing the proposed price for a launch brand in
Greece to three of the lowest prices in Europe (Economist Intelligence Unit
2009a).
2.4.3 Pricing regulation / control in South Africa
The total healthcare expenditure for South Africa in 2002 totalled 7.3 % of GDP
(Economist Intelligence Unit 2005). The revenue in 2001 regarding
pharmaceuticals for the private sector was R6,9 billion. The wide differences in
income groups (with the largest part of the population being in the lower Living
Standards Measure (LSM) groups), means that the private healthcare sector
only provides service to 20 % of the population (Economist Intelligence Unit
2005). The market for generic medicines is growing in South Africa. The largest
generic manufacturer in South Africa is Aspen Phamacare.
The South African government introduced contentious pricing regulations in
2004, resulting in South Africa, being one of a few countries with price ceilings
for all prescription medicines in the private sector. The introduction of these
price ceilings resulted in an overall decrease in gross profit margins for
pharmacies in South Africa. A Single Exit Price (SEP) is set for all prescription
medicines by government (at ex-factory level) regardless of the channel of
purchase. The South African government has also introduced capped price

24
increases. These price increases were proposed on an annual basis.
However, since the introduction of the regulations in 2006, only one such
increase was realized and this effectively resulted in a price freeze within the
pharmaceutical market (Economist Intelligence Unit 2009d).
A policy for mandatory generic substitution has been implemented successfully
in the private sector. One of the greatest current pricing challenges for the
South African market is to realise a reasonable and enforceable dispensing fee
for pharmacists as these costs had not been regulated by law until November
2010 (Gray 2009; Motsoaledi 2010).
The above stated factors, render a unique situation for the South African
pharmaceutical market.
The interested reader can also refer to the following dissertations from the Wits
Business School Library for further information
• An Economic Assessment of Single Exit Pricing in The Pharmaceutical
Industry – L.M. Adams (1994)
• The Sensitivity in the Pharmaceutical Industry – S.T. Mthethwa (1996)
• Compatibility of Generic Medicine Policy and a Local Pharmaceutical
Industry – J.L. Carapinha (2005)
2.5. Conclusion
The literature clarifies that various pricing and control mechanisms are utilized
by governments globally to exert downward pressure on medicines and render
this essential commodity to more people. It is evident that developed countries
and developing countries utilise similar mechanisms for price controls, although
access to medicine is mainly driven by price in developing countries. The South
African pricing regulation environment ensures a unique situation within a
developing country with some contentious current issues, for example the
proposed National Health Insurance (NHI) scheme. The potential impact of NHI
in South Africa should be researched as a single focus area and will not be
covered within this research report.

25
2.6. Research Questions
2.6.1 Research Question 1
The following research questions emerge from the literature review.
What are the perceived pricing benefits for consumers through the
implementation of SEP in the private pharmaceutical market in South
Africa?
Significantly lower prices are realized through the implementation of price
regulations in the pharmaceutical market in developing countries compared to
markets such as the US with minimal regulations. However, over-regulation
could lead to a negative impact in terms of availability of medicines due to non-
viable business conditions for pharmaceutical companies, as seen in Egypt.
2.6.2 Research Question 2
What is the perceived impact of SEP on retail pharmacies in South Africa
in terms of changes in the business environment?
The introduction of the SEP as a price control mechanism in South Africa,
immediately cut prices of medicine by 19 % (which due to the influence of
normal market forces, became 22 % at the end of the first year) significantly
influencing the pharmaceutical industry (McIntyre and Thiede 2007; Lotter
2010b). Gross profit margins within the private sector including independent
pharmacies, group pharmacies and hospital pharmacies decreased as a result
of SEP. Profit margins were further impacted by the regulated dispensing fee
serving as a price ceiling in combination with the SEP in terms of scheduled
medicines in the private healthcare sector. These price control mechanisms
changed the dynamics within retail pharmacies as the profit on medicines is
now regulated.

26
CHAPTER 3: RESEARCH METHODOLOGY
This section introduces the plan and procedure followed to address the
research questions, including a literature review detailing the appropriate
research method and an explanation of the population and sampling for this
research. The final part of this section addresses the limitations and validity of
the research and data as well as the reliability of the results.
3.1 Research methodology /paradigm
The first part of this section looks at the specific design utilised to answer the
research questions. According to Creswell (2009), research designs can be
grouped into three major groups i.e. quantitative, mixed and qualitative
methods. These designs have specific characteristics listed in Table 2.
Table 2: Quantitative, Mixed and Qualitative Methods (Creswell 2009)
Quantitative Methods Mixed Methods Qualitative Methods
• Pre-determined
• Instrument based
• Performance data and
census data
• Statistical analysis
• Statistical interpretation
• Both pre-determined and
emerging methods
• Both open- and closed-
ended questions
• Multiple forms of data
drawing on all possibilities
• Statistical and text
analysis
• Across databases
interpretation
• Emerging methods
• Open-ended questions
• Interview data,
observation data,
document data and
audio-visual data
• Text and image analysis
• Themes, patterns
interpretation
The mixed approach method best suits this research as both qualitative and
quantitative data were collected. The mixed method approach was used to

27
gather comprehensive data for optimal understanding of the research questions
(Creswell 2009). The quantitative analysis was utilised to measure the
implementation of the pricing regulation on specific scheduled medicines in the
private pharmaceutical industry related to patient pricing benefit. The
Qualitative analysis explored the impact of the implementation of price
regulations on the business environment, strategy and survival of the retail
pharmacy in South Africa.
3.2 Research Design
A mixed method approach was followed as shown in Table 2. The mixed
method approach provided comprehensive understanding of the research
questions through diverse data collection as an advantage (Creswell 2009).
This approach resulted in an in depth understanding of the impact of the
introduction of the SEP in South Africa.
A potential disadvantage of this approach was that the researcher is
representing a pharmaceutical company that may introduce a bias to the
respondents and the researcher (Willig 2008).
The quantitative analysis research design used an interviewer administrated,
structured questionnaire, gathering numerical data for descriptive and inferential
statistics. Given that the sample of pharmacies can be considered
representative of the population of pharmacies in Gauteng, this analysis could
provide a general explanation of trends of a sample from which the researcher
could draw conclusions about a population (Creswell 2009). However, this
research cannot make this claim as a probability random sample was not
drawn. The reader is referred to section 3.3.2
The qualitative analysis research design involved data collection through semi-
structured interviews. The data were analysed through qualitative content
analysis. Content analysis played a supporting role in differentiating the levels
of the content into themes and main ideas resulting in a replicable and valid
method for making specific inferences from the interviews (Mayring 2000).

28
As almost half of the respondents formed part of both the qualitative and
quantitative data collection, the research design allowed for collaboration
between the qualitative and quantitative data. This resulted in further richness
in the interpretation of the research findings.
3.3 Population and sample
3.3.1 Population
The population for both the quantitative and qualitative analysis were all retail
pharmacies in the private sector in Gauteng, South Africa.
3.3.2 Sample and sampling method
The sample of pharmacies for the quantitative analysis was a non-probability
convenience sample, selected from a list of registered pharmacies in Gauteng.
The sample included pharmacies from all large pharmacy groups, i.e. Dischem,
Clicks, Link Group Pharmacies, Private Hospital Pharmacies, as well as
independent retail pharmacies. The sample size of 50 pharmacies is presented
in Table 24 in the appendix.
The sample for the qualitative analysis was a non-probability convenience
sample of pharmacy managers for the various pharmacy groups as well as
managers of independent retail pharmacies and hospital pharmacies. The
sample represented managers in retail pharmacies from all large pharmacy
groups, private hospital pharmacies as well as independent retail pharmacies
and the interviews were conducted in person to extract content, perceptions and
attitudes.
3.4 The research instrument
The research instrument utilised for the quantitative section was a questionnaire
(Appendix A). The quantitative questionnaire gathered data regarding the
selling price of selected prescribed ethical medicines.

29
The research instrument for the qualitative analysis was a semi-structured
interview schedule (Appendix B).
The interview proposed semi-structured questions to managers from the various
private pharmacy groups as well as independent retail pharmacies and hospital
pharmacies.
This instrument provided a tool for content analysis as an advantage relating to
the past and present impact of the introduction of SEP within the
pharmaceutical industry in South Africa.
3.5 Procedure for data collection
The researcher physically met with respondents and asked face-to-face
questions to either a pharmacist or pharmacy assistant to price a script and
determine a selling price for the quantitative data collection.
The qualitative content analysis was initiated telephonically or via e-mail
through invitations to set up semi-structured interviews. The interview location
was determined by the person being interviewed, provided that the location was
in Gauteng. The interviews were recorded through a process of active note
taking and the content was extracted for the interviewer to record the data.
The semi-structured interviews enabled the respondents to share their industry
perspectives by gather necessary data for content analysis, to address the
second research question.
3.6 Data analysis and interpretation
Both parametric and non-parametric data analysis techniques were applied to
the quantitative data of the questionnaire. Specifically, the variable analysed
was Rand value, measured on a ratio scale. The distribution of this variable
was graphed and assessed for Normality, using the Shapiro-Wilk Test as well
as the Kolmugorov-Smirnov and Lillifors tests. In addition the distributions of the

30
Rand values were plotted with Box plots, showing the medians, quartiles,
outliers and extreme values.
Both parametric and non-parametric analyses were computed as the data
displayed significant deviations from normality.
One-way Analysis of Variance (ANOVA) was used to compare the differences
in the mean Rand values of pharmacies in the 3 groups, with the Scheffe and
Tukey post hoc tests for pairwise comparisons in the case of a significant
difference. Furthermore the partial eta-squared was used to estimate the effect
size of the significant difference. The non-parametric equivalent, the KrusKal-
Wallis ANOVA was used on the ranked data in view of the non-normality of the
data (Creswell 2009).
Content analysis was used for the qualitative data to make inferences by
extracting themes from the research through objective and systematic
identification (Neuendorf 2002). The common themes derived from the
interviews were used to determine the perceived impact of the SEP on retail
pharmacies in South Africa in terms of changes in the business environment.
3.7 Limitations of the study
Only a small sample of individuals was used for both the qualitative and
quantitative research components of this dissertation. Secured responses from
the selected sample were imperative to reduce sampling bias.
The data was collected in Gauteng, posing a limitation from a geographical
point of view.
3.8 Validity and reliability
Reliability revolves around finding consistent results with repeated application of
specific research (Kalof, Dan and Diet 2008). Validity is concerned with
similarity or comparison within the details of the research, evidence and
conclusions (Kalof et al. 2008).

31
3.8.1 External validity
External validity enabled the researcher to generalize from a study or sample to
represent a population (Kalof et al. 2008).
Maximum external validity was assured for the questionnaire by selecting a
sample of pharmacies across pharmacy groups, independent pharmacies as
well as hospital pharmacies in Gauteng, no exclusion of a particular group.
A sample of pharmacy managers were selected for the interviews to ensure
representation of all pharmacy groups, independent pharmacies and hospital
pharmacies in Gauteng.
3.8.2 Internal validity
Internal validity refers to suitable conclusions being depicted by the data at
hand (Kalof et al. 2008). The questionnaires and interviews were consistent
and standardised throughout the process of data collection to maximize internal
validity.
3.8.3 Reliability
Consistent results with repeated application of specific research, defines
reliability (Kalof et al. 2008). The simple questionnaire and interview schedule
removed ambiguity in the response. Consistency was ensured by follow up
discussion with selected respondents after the data collection.

32
CHAPTER 4: PRESENTATION OF RESULTS
4.1 Introduction
A mixed methodology was followed in collecting the data for this report. Firstly
quantitative data was collected using a questionnaire developed to obtain
information regarding actual prices of specific medicines within independent
pharmacies, group pharmacies and hospital pharmacies. The actual script
prices were recorded and reported back using descriptive and inferential
statistics.
A second research instrument was designed, in the form of semi-structured
interviews to produce qualitative data by posing open ended questions to
respondents. The qualitative data were reported through content analysis and
through categorisation of the information into thematic groups as primary
themes. The secondary themes were utilised to examine the relation between
the quantitative data and these themes to provide a holistic interpretation of the
results. The qualitative data provided information regarding business strategy,
survival tactics and fundamental changes in day to day business as well as the
need for restructuring within each pharmacy. This information was considered
confidential and sensitive. For this reason transcripts of the actual interviews
have not been compiled. A number has been allocated to each respondent to
facilitate with the data reporting, see Table 3 below.
The population and sample for both the quantitative and qualitative data was
collected via non-probability convenience sampling as described in section 3.3
population and sample.
4.2 Demographic profile of respondents
The sample size for the quantitative data, in terms of actual prices for medicines
was set at fifty pharmacies within the private healthcare sector, including
independent, group and hospital pharmacies. This criterion was met and a total
of 50 scripts were priced at pharmacies in Gauteng. Scripts were obtained

33
from 12 independently owned pharmacies, 21 group pharmacies and 17
hospital pharmacies.
A sample size of between 20 and 30 respondents was initially set for the
qualitative semi-structured interviews in Gauteng. This criterion was met by
conducting 22 interviews among independent, group as well as hospital
pharmacies.
Table 3 below summarises the demographic data as well as the functional roles
reported by each pharmacy manager as per each individual semi-structured
interview.

34
Table 3: Demographic Data Including Functional Roles Reported by Respondents
Number Category (G, H, I) Rand Value
Years of Expe-rience
Number of personnel
Pharmacy Manager
Stock Control
Staff Manage-ment
Dispen-sary Service Roster
Locum Arrange-ments
Patient Consul-tation
Problem Solving Dispensing
Follow Unpaid Levies
Doctor Meetings
Accoun-tant
G1 Group R 1,193.47 7 45 � - � - - - � - - - �
G2 Group R 1,193.47 3.5 23 - � � � � - � � - - -
G3 Group R 1,419.10 20 6 - - � - � � � � - - -
G4 Group R 1,475.51 20 5 � � - - - � - � - - �
G5 Group R 1,193.46 17 8 - � � � � � � � - - -
G6 Group R 1,193.72 2 3 - � - � - � � � � - -
G7 Group R 1,295.55 3 4 - � � - - � - � - - -
G8 Group R 1,193.47 7 18 - � � � � � � � - - - Total Group Pharmacy 79.5 112 2 6 6 4 4 6 6 7 1 0 2
Group Pharmacy % N/A N/A 25% 75% 75% 50% 50% 75% 75% 88% 13% 0% 25%
Number Category (G, H, I) Rand Value
Years of Expe-rience
Number of personnel
Pharmacy Manager
Stock Control
Staff Manage-ment
Dispen-sary Service Roster
Locum Arrange-ments
Patient Consul-tation
Problem Solving Dispensing
Follow Unpaid Levies
Doctor Meetings
Accoun-tant
I1 Independent No Data 7 2 � � � - - � - � - - -
I2 Independent No Data 6.5 4 � � � - � � - � - - �
I3 Independent No Data 3 20 � � � - � � � � - - -
I4 Independent R 1,475.51 23 8 � � � - � � � � - - �
I5 Independent R 1,475.51 5.5 6 � � � - - � � � - - -
I6 Independent R 1,451.99 16 22 � � � � � � � � � - �
Total Independent Pharmacy 61 62 6 6 6 1 4 6 4 6 1 0 3
Independent Pharmacy % N/A N/A 100% 100% 100% 17% 67% 100% 67% 100% 17% 0% 50%

35
Number Category (G, H, I) Rand Value
Years of Expe-rience
Number of personnel
Pharmacy Manager
Stock Control
Staff Manage-ment
Dispen-sary Service Roster
Locum Arrange-ments
Patient Consul-tation
Problem Solving Dispensing
Follow Unpaid Levies
Doctor Meetings
Accoun-tant
H1 Hospital R 1,444.98 20 20 � � � � � � � � - - �
H2 Hospital R 1,475.75 8 40 � � � � � � � � - � �
H3 Hospital R 1,514.66 4 36 � � � � � � � - - � �
H4 Hospital No Data 12 17 � � � � � - � - - � -
H5 Hospital No Data 5 37 � � � � � � � � - � �
H6 Hospital No Data 10 56 � � � � � � � � - � �
H7 Hospital R 1,475.75 4 16 � � � � � � � � - � �
H8 Hospital R 1,329.44 14 25 � � � - � - � � - � �
Total Hospital Pharmacy 77 247 8 8 8 7 8 6 8 6 0 7 7
Hospital Pharmacy % N/A N/A 100% 100% 100% 88% 100% 75% 100% 75% 0% 88% 88%

36
4.3 Results pertaining to Research Question 1
4.3.1 Research Question 1
What are the perceived pricing benefits for consumers through the
implementation of SEP in the private pharmaceutical market in South
Africa?
4.3.2 Results – Research Question 1
The literature review in Chapter Two refers to Research Question One and the
reader is referred to the applicable paragraph in section 2.4.
The questionnaire in Appendix A, tests whether the introduction of SEP and
subsequent 22% overall medicines price reduction is experienced as a
consistent cost saving benefit by consumers in the private healthcare sector in
South Africa.
Table 4: Descriptive Statistics for Independent, Group and Hospital
Pharmacies
N Mean Median Minimum Maximum Std.Dev. Skewness
Group 21 R 1 255.02 R 1 193.72 R 1 191.23 R 1 494.09 R 109.94 1.50
Hospital 17 R 1 464.17 R 1 475.50 R 1 254.66 R 1 711.79 R 89.75 0.357059
Independent 12 R 1 405.55 R 1 462.44 R 1 183.46 R 1 612.37 R 135.13 -0.48281
Descriptive statistics are provided for the Rand values of each group in Table 4.
The mean pricing for group pharmacies was higher than the median (R1,255.02
and R1,193.72 respectively), in line with the positive skewness of 1.5. The
mean and median values for hospital pricing were similar at R1,464.17 and
R1,475.50, respectively, while for the independent pharmacies the mean Rand
value was substantially lower than the median at R1,405.55 and R1,462.44
respectively. The percentage within group price variation in the 3 groups was
25 % for group pharmacies, 36 % for hospital pharmacies and 36 % for
independent pharmacies respectively.

37
One way Analysis of Variance (ANOVA) was used to compare the differences in
the mean Rand values of group, independent and hospital pharmacies (referred
to as the 3 groups or levels of the independent variable, pharmacies), with the
assumption of ANOVA that the data are normally distributed. However,
according to the Shapiro-Wilk Test the data were significantly non-normally
distributed (W = 0.83, p < 0.001). In addition to the parametric ANOVA, the
non-parametric equivalent, the KrusKal-Wallis ANOVA was used on the ranked
data.
Both the parametric ANOVA and its non-parametric equivalent Kruskal-Wallis
ANOVA revealed consistent and significant differences between the means and
the ranks of the Rand values respectively.
The parametric ANOVA revealed an overall significant difference in the mean
prices of scripts within the 3 groups F (2,47) = 18.116, p< 0.001. Both the
Scheffe and the Tukey post-hoc test results revealed that independent and
hospital pharmacy mean prices are significantly higher than the mean price of
group pharmacies (p < 0.01 and p < 0.001 respectively). The mean price for
the independent pharmacies were R1,405.55, and the mean price for the
hospital pharmacies were R1,464.17, compared to the mean price for the group
pharmacies at R1,255.02. However, the difference between the independent
and hospital pharmacy prices was not significant as shown in Table 5 by the
Sheffe Test.
Table 5: ANOVA and Means
{1} - M=1255.0
{2} - M=1405.5
{3} - M=1464.2
Group {1} 0.001997 0.000003 Indepen-dent {2} 0.001997 0.377759
Hospital {3} 0.000003 0.377759
Scheffe Test; Variable: R Value (Data.sta) Marked differences are significant at p < .05000\

38
Table 6: Kruskal-Wallis ANOVA
Code Valid – N Sum of - Ranks
Group 101 21 319.5
Independent 103 12 349.5
Hospital 104 17 606
Kruskal-Wallis ANOVA by Ranks; R Value (Data.sta) Independent (grouping) variable:
Independent / Group / Hospital Kruskal-Wallis test: H ( 2, N= 50) =19.62171 p =.0001
Figure 2: Histogram of the Distribution of the Quantitative Data
Similarly, the Kruskal-Wallis ANOVA revealed significant differences between
the ranks (H (2) = 19.622, p < 0.001), with the sum of the ranks lowest for group
pharmacies followed by independent pharmacies and highest for hospital
pharmacies.
Furthermore when the Mann-Whitney U Test was applied to the ranked data to
examine pair wise differences, results consistent with the parametric post hoc
Sheffe Test were found with significant differences between the group and
hospital (Z = 4.24, p < 0.001) and the group and independent pharmacies (Z = -
Histogram: R Value
K-S d=.21757, p<.05 ; Li l liefors p<.01
Shapiro-Wilk W=.82954, p=.00000
1100 1200 1300 1400 1500 1600 1700 1800
X <= Category Boundary
0
5
10
15
20
25
30
No
. o
f o
bs.

39
2.724, p < 0.01). Once again, no significant difference was found between the
hospital and independent pharmacies (Z = 1.271, p > 0.05).
Partial eta-squared is the percentage of the total sum of squares or variation
accounted for by the main effect of pharmacy grouping as only 44 % of the
variation was accounted for by the pharmacy grouping, more than half of the
variation was not accounted for at all in the one way design. Thus there may be
other systematic variables, e.g. size of the pharmacy size of the pharmacy
group it, socio-economic location within the groups that could account for the
unexplained variation. The large variability within the data is evident in the Box
Plots of the 3 groups (see Figure 3). The clear lack of homogeneity of variance
of prices within the three groups once again supports the application of the
Kruskal-Wallis ANOVA nonparametric test.
Figure 3: Box Plot of the Independent, Group and Hospital Pharmacy
Quantitative Data
The retail price of the specified medicines incorporated in the questionnaire is
inconsistent across independent, group and hospital pharmacies. The minimum
price was R1,183.46 and the maximum was R1,711.79. A clear price difference
of R528.33 was therefore documented in the research.

40
4.3.3 Conclusion – Research Question 1
It can be concluded that consistent pricing benefits were not realised and
experienced by consumers in the private healthcare sector with the introduction
of SEP.
4.4 Results pertaining to Research Question 2
4.4.1 Research Question 2
What is the perceived impact of SEP on retail pharmacies in South Africa
in terms of changes in the business environment?
4.4.2 Results – Research Question 2
The reader is referred to section 2.4.3 of the literature review, Chapter 2, where
Research Question 2 originated.
In order to obtain data regarding this research question, the research instrument
in Appendix B was developed.
The questions in sections A and B of the research instrument were posed to the
respondents. Section A of the research instrument collected demographic data
and this information was included in Table 3.
The analysis of questions 1 – 4 from section B of the research instrument was
conducted from a thematic perspective. The responses to each question have
been listed in a response analysis, which was listed into common themes as
primary and secondary themes as the researcher aimed to examine the relation
between the quantitative data and these themes to provide a holistic
interpretation.
Figure 4, 5 and 6 below, reveal the responses of the participants regarding
question 1 of section B of the research instrument.

41
Figure 4: The Influence of SEP on the Business Strategy of the Independent Pharmacy
Figure 5: The Influence of SEP on the Business Strategy of the Group Pharmacy

42
Figure 6: The Influence of SEP on the Business Strategy of Hospital Pharmacies

43
The common themes were reported in a question by question format through
separate headings and follows below. Since the data was collected from
independent pharmacies, group pharmacies and hospital pharmacies, the
responses are reported in this structure.
4.4.2.1 Research instrument 2 – Question B1
Describe the influence of SEP on the business strategy of the pharmacy i.e.
additional products or services you are offering following the introduction of SEP
Question B1 focused on the changes that occurred in the pharmacy strategy
due to the decrease in gross profit with the implementation of the SEP.
Thematic analysis was conducted on the data obtained by the respondents. The
following themes were identified in relation to the influence of SEP on the
business strategy of the pharmacy. The reader is referred to Figure 4, 5 and 6
section 4.4.2.
The common business strategy themes in relation to SEP are reported in Table
7 Below.
Table 7: Business Strategy Themes in Relation to SEP for Independent,
Group and Hospital Pharmacies
Theme Independent Pharmacy (Refer to Figure 4)
Group Pharmacy (Refer to Figure 5)
Hospital Pharmacy (Refer to Figure 6)
Customer Retention Strategy
83% Crucial for survival
88 % Crucial for survival
25 % Extract majority of customer base from individuals in hospital or visitors of patients and therefore customer retention strategy is not a major focus point
Focus on alternative medicines for sales of non-scheduled medicines (not governed by SEP)
67% Gap identified as high profit opportunity
75 % Gap identified as high profit opportunity
75 % Gap identified as high profit opportunity
Increased focus on front shop sales
67 % Gap identified as high profit opportunity
75 % Gap identified as high profit opportunity
75 % Gap identified as high profit opportunity

44
Layout changes 0 % Often restricted in terms of space
38 % Naturally focused on layout from outset
25 % Not major focus
Focus on logistics and warehousing
0 % No buying power to drive this theme
75 % Buying power to negotiate increased logistics or warehousing cost to be absorbed by pharmacy group
63 % Buying power to negotiate increased logistics or warehousing cost to be absorbed by hospital pharmacy group
Joined a group pharmacy 0 % 38 % Utilised this opportunity to survive
0 %
Increasing profits by increasing volumes of sales on lower cost items
50 % Identified as a gap to realise increased profit
63 % Identified as a gap to realise increased profit
88 % Identified as a gap to realise increased profit
Increased focus on cash flow
50 % Due to general decrease in profit
50 % Due to general decrease in profit
63 % Due to general decrease in profit
Improved productivity 33 % Considered high standard prior to introduction of SEP
63 % To decrease costs indirectly
63 % To decrease costs indirectly
Improved service delivery 33 % Considered high standard prior to introduction of SEP
63 % To increase customer satisfaction
63 % To increase customer satisfaction
Additional service 33 % Added one additional service Constrained due to space restriction
38 % Added 3 additional services 25 % Added one or two additional services
38 % Added 2 additional services 13 % Added 1 additional service
Change in focus from profit to cost centre
0 % 0 % 100 % Only incorporated by Hospital Pharmacies – pharmacy is considered an additional service provided by the hospital

45
4.4.2.2 Research instrument 2 – Question B2
What changes occurred in the business of this pharmacy in order to survive the
implementation of SEP?
Question B2 determined the focus areas addressed for the pharmacy to survive
due to the decrease in gross profit margins with the implementation of SEP.
The evolving themes from this question is listed and discussed below.
Figure 7, 8 and 9 reveals the responses of the participants regarding question 2
of section B of the research instrument.
The survival tactics in relation to SEP are reported in Table 8 on page 49.

46
Figure 7: Survival Tactics Following the Introduction of SEP for Independent Pharmacies
Figure 8: Survival Tactics Following the Introduction of SEP for Group Pharmacies

47
Figure 9: Survival Tactics Following the Introduction of SEP for Hospital Pharmacies

48
Table 8: Survival Tactics in Relation to SEP for Independent, Group and
Hospital Pharmacies
Theme Independent Pharmacy (Refer to Figure 7)
Group Pharmacy (Refer to Figure 8)
Hospital Pharmacy (Refer to Figure 9)
Decrease general overheads
100 % 50 % Focus from smaller group pharmacies predominantly
Increase in working hours for pharmacy mangers / pharmacists
83 % Increased cost to employ locum pharmacists
38 % Only reported by smaller group pharmacies constrained by staff members
Increase Pharmacy Assistants
50 % In relation to the number of pharmacists to decrease expenses on salaries as salaries for pharmacy assistants are substantially less compared to salaries for pharmacists
75 % Most prevalent survival tactic for group pharmacies. This allowed for more scripts to be dispensed as pharmacists controlled the quality of dispensing by ensuring correct dispensing of medicines only prior to being received by the patients.
Increase Generic Substitution
33 % To offer lower cost medicines to patients to retain customers and increase unit sales
0 % Not reported as survival tactic
100 % Incorporated to show perceived cost advantage over other pharmacies and increase customer retention
Decrease Staff 0 % Could not function with less personnel
13 % Smaller group pharmacies – high need to cut overheads
Specialised Manager – Overheads Manage
0 % No additional manager employed to manage overheads as this would increase overall overheads
38 % Group pharmacies who did not have these managers in place from the outset and who were not constrained due to their size
Accurate Billing (Pertaining to each item
0 % This has been part
0 % Not reported as
88 % Decreased losses in

49
dispensed from the pharmacy)
of independent pharmacies prior to the introduction of SEP
survival tactic general
Calculate personnel to cut overheads
0 % 63 % To save costs
88 % Decreased overheads in general
Advertising 17 % Only in local papers – low cost
63 % Television advertising and newspaper advertising to increase customer base
13 % Pharmacy is an additional service offered by the hospital
Focus on per diem accounts (Approved daily allowance for Medical Aid expenses relating to a specific procedure)
0 % N/A
0 % N/A
88 % Manage daily expenses for these patients accurately whilst providing appropriate health care Overall cost saving realised
4.4.2.3 Research instrument 2 – Question B3
How did the implementation of SEP influence your day to day business?
The introduction of SEP with the accompanying changes in business strategy
and areas addressed for survival impacted on the day to day business of the
pharmacy was addressed through question B3. The thematic responses that
emerged through this question are listed and discussed below. The reader is
referred to Figure 10, 11 and 12. Table 9 reports the day to day changes
realised by all pharmacies as a result of the introduction of SEP.

50
Figure 10: The Influence of the Implementation of SEP Regarding Day to
Day Business for Independent Pharmacies
Figure 11: The Influence of the Implementation of SEP Regarding Day to
Day Business for Group Pharmacies
Figure 12: The Influence of the Implementation of SEP Regarding Day to
Day Business for Hospital Pharmacies

51
Table 9: Day to Day Changes Implemented in Relation to SEP for
Independent, Group and Hospital Pharmacies
Theme Independent Pharmacy (Refer to Figure 10)
Group Pharmacy (Refer to Figure 11)
Hospital Pharmacy (Refer to Figure 12)
Reduction in stock days 100 % Primary focus to reduce working capital
75 % Focus to reduce working capital
100 % Pharmacy operating as cost centre – all opportunities utilised to decrease general costs (less stock on shelves result less working capital tied up in the pharmacy)
Increased working hours 100 % Pharmacies operating with minimal personnel – increased involvement of pharmacy manager or pharmacist to reduce locum costs and further salary costs
63 % Attributed to some smaller group pharmacies (refer to Table 3, number of personnel)
63 % Mainly due to general working hours of the pharmacy increasing. To increase competitiveness towards other hospital pharmacies in the visitnity
Increased pressure to decrease overheads
0 % This was part of the survival strategy tactics for all independent pharmacies – therefore no additional focus on this as it was already implemented
0 % Not reported as daily change by any group pharmacy
63 % Due to hospital pharmacies operating as cost centres following the introduction of SEP
4.4.2.4 Research instrument 2 – Question B4
Was there any restructuring involved within this pharmacy following the
introduction of SEP and how did the restructuring affect your business?
Question B4 focused on direct and indirect restructuring and the effect of this on
the pharmacy as a result of the introduction of SEP. Direct restructuring refers
to actual restructuring and a decrease in personnel of the pharmacy. Indirect
restructuring refers to a lack of increase of personnel in the pharmacy with an

52
increase in workload / number of scripts dispensed or number of patients
admitted to the hospital as well as an increase in the hospital capacity.
Table 10 reports the day to day changes realised by all pharmacies as a result
of the introduction of SEP.
Figure 13: The Influence of the Implementation of SEP on Restructuring
within Independent Pharmacies
Figure 14: The Influence of the Implementation of SEP on Restructuring
within Group Pharmacies

53
Figure 15: The Influence of the Implementation of SEP on Restructuring
within Hospital Pharmacies
Table 10: Restructuring as a result of the Implementation of SEP for
Independent, Group and Hospital Pharmacies
Theme Independent Pharmacy (Refer to Figure 13)
Group Pharmacy (Refer to Figure 14)
Hospital Pharmacy (Refer to Figure 15)
Direct Restructuring 33 % Two of the independent pharmacies had to resolve to direct restructuring following the introduction of SEP One of these pharmacies had to close their doors due to the introduction of SEP and all employees lost their work
0 % N/A
0 % N/A
Indirect Restructuring (Positions not filled when employees resigned)
50 % 38 % 38 %

54
4.4.3 Conclusion – Research Question 2
The changes in the business environment, in particular business strategy and
survival, as well as changes in day-to-day business and ultimately business
restructuring were depicted in the preceding section. With this a description
was obtained showing the impact of SEP on retail pharmacy regarding changes
realised in the business environment.
It is evident from the research that the introduction of SEP in retail pharmacies
resulted in changes within the business environment. These changes were
mostly evident through a focus on improved service offering, optimisation of the
business environment, a drive to reduce overheads and focus on precision in
terms of stock management and billing.
4.5 Summary of the results
It is evident from the data obtained that consistent price benefits are not
realised by patients through the implementation of the SEP. The regulated
dispensing fee has also not been fully adhered to by all pharmacies investigated
in this research. The actual selling price of the medicines included in the
questionnaire was higher in selected cases than the maximum allowed price as
per the SEP and dispensing fees regulated by law.
Independent, group pharmacies as well as hospital pharmacies saw changes in
their business environment due to the impact of SEP. Pharmacies had to
incorporate additional services and adhere to stringent cost cutting or finding
alternative streams of income to survive as a result of the introduction of SEP.
Improved service offering and optimisation of the business environment through
a drive to be more productive also occurred following the introduction of SEP.

55
CHAPTER 5: DISCUSSION OF THE RESULTS
5.1 Introduction
The objective of this chapter is to focus on the discussion and explanation of the
results enclosed in Chapter 4. The structure reflects the composition of Chapter
4 four and the format was laid out in a comparable order.
5.2 Demographic profile of respondents
Retail pharmacies in the private healthcare sector were subdivided into three
groups independent, group and hospital pharmacies. The quantitative data or
actual script prices were obtained either from a pharmacist or pharmacy
assistant, as only these individuals could provide the correct information relating
to the prices of the actual medicines referred to in Research Instrument One in
the appendix. The reader is referred to section 4.2 in Chapter 4 for the
demographic profile of the respondents regarding the quantitative data.
Independent pharmacies represented 24 % of the quantitative data sample size,
whilst group pharmacies represented 42 % and hospital pharmacies 34 %.
The demographic profile of the respondents relating to the qualitative data was
reported in Table 3 on page 35. Differences exist in terms of the business
environment within these three groups. This is particularly evident in terms of
the number of personnel. Respondents from all three groups were interviewed
to ensure a holistic opinion for the analysis. Six respondents were included
from independent pharmacies, eight from group pharmacies and eight from
hospital pharmacies.
Only pharmacy / dispensary managers were interviewed as part of the research
to ensure accurate representation of all the information relating to pricing
regulation in the retail pharmacy following the introduction of SEP.
Regarding other demographic data the average number of years experience as
managers for the independent pharmacies was 10.1 years, 9.93 for group

56
pharmacies and 9.62 for hospital pharmacies. The independent pharmacies
employed 10.1 people on average, group pharmacies 14 employees on
average and the hospital pharmacies employed 30.8 people on average.
In terms of functional roles reported by the pharmacy managers, independent
pharmacies predominantly focused on stock control, staff management, patient
consultation and dispensing. The pharmacy managers from group pharmacies
focused mainly on dispensing, followed by problem solving, patient consultation,
staff management and stock control. The functional role focus of the hospital
pharmacy managers was centred on problem solving, arranging for locums,
staff management and stock control.
5.3 Discussion pertaining to Research Question 1
What are the perceived pricing benefits for consumers through the
implementation of SEP in the private pharmaceutical market in South Africa?
5.3.1 Discussion pertaining to Research Question 1
5.3.1.1 The impact of the implementation of Single Exit Price (SEP)
for pharmaceuticals in the private sector in South Africa
The introduction of SEP, coupled with capped annual price increases for
medicines in the private pharmaceutical industry resulted in an overall price
decrease of 22 % in medicine prices in South Africa, after the first year,
following introduction of the new legislation (McIntyre and Thiede 2007; Lotter
2010b). These results appear positive and due to the pricing regulation
consistent pricing benefits are therefore expected when considering medicine
prices for patients in the private healthcare sector in South Africa.
According to the literature, the introduction of price ceilings to medicines pricing
regulations in South Africa has led to an overall decrease in gross profit margins
for pharmacies in South Africa (Economist Intelligence Unit 2009d). It was
evident from the literature review that regulation of medicine prices can have a
negative effect on the availability of medicines, as experienced in Egypt

57
(Economist Intelligence Unit 2010). The research confirmed this argument as
stock control was confirmed as a functional role to all pharmacy managers from
the group and hospital pharmacies as well as 75 % of the independent
pharmacies interviewed.
According to additional empirical research price regulation has adverse effects
on the cost and quality of healthcare (Kessler 2004). This statement was
confirmed through the quantitative research, as it was evident from the
parametric ANOVA that a significant difference exists in the mean prices of
scripts within the three groups. The reader is referred to section 4.3.1 in
Chapter 4. The retail price of the combined medicines included in the
questionnaire (Appendix B), was not consistent across independent, group and
hospital pharmacies. In addition it was evident from the research questionnaire
results obtained that the recent introduction of the dispensing fee regulation in
2010 was not adhered to by all pharmacies included in this research as the
maximum price quoted for the medicines included in the questionnaire was
higher than the allowed regulated price. A total price difference of R528.33 was
documented in the research when the minimum and maximum prices were
considered.
5.3.2 Conclusion - Research Question 1
It is evident from the information discussed above, as well as actual prices of
medicines obtained through the research that consistent pricing benefits were
not realised by patients following the introduction of SEP in South Africa.

58
5.4 Discussion - Research Question 2
5.4.1 Research Question 2
What is the perceived impact of SEP on retail pharmacies in South Africa
in terms of changes in the business environment?
5.4.2 Discussion pertaining to Research Question 2
The second research instrument (Appendix B), was developed to obtain an
understanding for Research Question 2. The design of this research instrument
focused on demographic data in section A (as reported in Table 3 on page 34
and also referred to in Chapter 5, section 5.2). Section B of the semi structured
interview focused on eliciting a response to provide insight into Research
Question 2.
Changes in the business environment of retail pharmacies in South Africa, post
the introduction of SEP were evaluated using four questions. These four
questions addressed the following concepts through questions 1 - 4:
1. The influence of the introduction of SEP on the business strategy of the
pharmacy
2. The changes implemented in order to survive as a result of the
introduction of SEP
3. The day to day changes brought about with the introduction of SEP
4. Restructuring within the pharmacy as a result of the introduction of SEP
Common themes were derived from each of the four questions and the data
were tabulated (Appendix C, Table 12 – 23). A tick was assigned to a positive
response pertaining to a specific theme from the feedback obtained through the
question. The results were then visually displayed and the reader is referred to
Figure 4 – 15 in Chapter 4, section 4.4.2.

59
A discussion and an explanation follows as obtained from the field research
through the 22 semi-structured interviews.
5.4.2.1 The influence of the introduction of SEP in the
business strategy of the pharmacy
According to the literature, the introduction of price ceilings, through
SEP resulted a decrease in gross profit margins for pharmacies in
South Africa (Economist Intelligence Unit 2009d). This was reported
during the research as a driving factor to adapt or change the
business strategy. The reader is referred to Table 12 - 14 in
Appendix C. Various strategies were explored to offer additional
services or alternatively create income through ways previously
unexplored. Possible opportunities were identified to increase profit,
improve the overall productivity of the pharmacy, improve the cash
flow of the pharmacy improve service delivery and focus on customer
retention, resulting in a clear change in the business environment.
The reader is referred to Figures 4, 5 and 6. The main strategic
change reported for independent and group pharmacies was to focus
on customer retention, whilst the top strategic focus for hospital
pharmacies was to change their management focus from a profit
centre to a cost centre focus. According to all respondents from the
hospital pharmacies, the introduction of the SEP resulted in hospital
pharmacies to break even or operate at as loss. For this reason,
hospital pharmacies are managed as cost centres and no longer
profit centres.
A strategic drive to improve gross profit in retail pharmacies was
recorded through a prominent focus on the front shop. This was
reported by 73 % of all respondents. The only factors, preventing this
focus were space as well as personnel constraints, as was the case
for some independent pharmacies.

60
Prices of homeopathic medicines and vitamins are not regulated
through SEP. This gap was strategically identified by 73 % of all
respondents and an increased focus on the recommendation and
sales followed as a result.
The reader is referred to Figure 1, Chapter 2, section 2.4. The SEP
in South Africa is the selling price to wholesalers in the
pharmaceutical market. Medicines are sold at this price to
wholesalers and logistics fees paid by the various pharmaceutical
companies are included in this selling price. This process is not
regulated. As a direct result of this, 50 % of the interviewed
respondents focused on warehousing and generation of logistic fees,
following the introduction of SEP.
5.4.2.2 The changes implemented in order to survive as a
result of the introduction of SEP
All respondents from the independent pharmacies reported a focus
for survival based on reducing overheads. Secondary to this the
working hours for pharmacy managers increased due to the fact that
locums could not be afforded (see Figure 7, Chapter 4, section
4.4.2.2).
The main survival tactic of group pharmacies was to increase the
number of pharmacy assistants (Figure 8, Chapter 4, section 4.4.2).
The decreased gross profit generated in retail pharmacies due to the
introduction of SEP, led to a decrease in the supply or intake of
pharmacy students at tertiary institutions, training pharmacists in
South Africa. Currently a shortage of pharmacists, particularly newly
qualified pharmacists are experienced in South Africa. Due to the
increased demand for pharmacists, the salary expectancy increased
for private retail pharmacists. To increase the output of a pharmacy
or the number of scripts dispensed additional dispensers are
required. An increased number of pharmacy assistants are currently
appointed as salaries for these individuals are substantially less

61
compared to pharmacists. However, pharmacists need to conduct a
final quality check prior to handing over the dispensed scripts from
pharmacy assistants.
According to the literature review, a policy for mandatory generic
substitution has been implemented successfully in the private health
sector (Gray 2009). Hospital pharmacies utilised this policy to their
advantage as increased generic substitution was identified as
survival tactic by all respondents from hospital pharmacy
respondents in the research Figure 9, Chapter 4, section 4.4.2). This
implied that generic medicines could be offered at a lower price
compared to ethical or original medicines, drawing more patients to
hospital pharmacies from neighbouring communities effectively
driving customers into the hospital pharmacies as “one stop
pharmacies”. A secondary survival tactic evident from the research
for hospital pharmacies, now operating as cost centres, was to
ensure an optimal number of employees in relation to the pharmacy’s
needs as well as a focus to decrease overheads. These survival
tactics were identified by 88 % of the hospital pharmacy respondents.
The main survival tactic implemented by all respondents, across the
groups was, to decrease overheads. This is a logical survival tactic
due to the overall reduction in gross profit with the introduction of
SEP. The reader is referred to Table 17 in the Appendix C.
5.4.2.3 The day to day changes brought about with the
introduction of SEP
Three common themes were identified as a day to day change
following the introduction of SEP: reduced stock days on hand,
increased working hours for pharmacy managers and increased
pressure on pharmacy managers to reduce overheads. The reader
is referred to Table 20 in Appendix C (day – to - day).

62
Ninety one percent of the respondents reported a reduction in stock
days and 73 % reported increased working hours and therefore
increased pressure on pharmacy mangers.
All respondents from the independent pharmacies reported a
reduction in stock days and increased working hours for pharmacy
managers as part of the day to day activities following the
introduction of SEP. The reader is referred to Figure 10, Chapter 4,
section 4.4.2.3. The group pharmacies have an advantage in terms
of available capital to purchase stock and therefore not all
respondents reported on a daily focus to reduce stock days (Figure
11, Chapter 4, section 4.4.2.3).
It is also evident from the respondents in the research (Table 3,
Chapter 4, section 4.2) that the independent pharmacies employed
10 people on average in comparison to 14 employees working for
group pharmacies and 31 individuals employed by hospital
pharmacies. This might explain why 100 % of the respondents from
independent pharmacies and only 63 % of the respondents from the
group and hospital pharmacies reported increased working hours for
pharmacy managers as a result of the introduction of SEP.
Increased pressure to decrease overheads was reported by 63 % of
the hospital pharmacies and none of the other respondents. This
might be attributed to the focal change of hospital pharmacies being
managed as cost centres and not profit centres, following the
introduction of SEP as reported before. The reader is referred to
Figure 12, Chapter 4, section 4.4.2.3.
5.4.2.4 Restructuring within the pharmacy as a result of the
introduction of SEP
Two of the twenty one respondents reported direct restructuring as a
result of the introduction of SEP whilst seven reported indirect
restructuring Table 23 in Appendix C. Indirect restructuring is

63
referred to as not filling a position when an employee terminates their
service at a pharmacy or not increasing the number of employees
employed by a pharmacy whilst the need for more employees exist
due to growth experienced in the total size of the pharmacy. Direct
restructuring refers to termination of service of employment of an
individual due to the fact that the services of the individual can no
longer be afforded by the pharmacy.
Half of the independent pharmacies involved in the research reported
indirect restructuring, whilst 38 % of the group and hospital
pharmacies reported indirect restructuring as a result of the
introduction of SEP (Figure 13, 14 and 15, Chapter 4, section
4.4.2.4). Direct restructuring was only reported by 33 % of the
respondents of independent pharmacies. This might be due to the
fact that the utilisation of resources for independent pharmacies is
under more pressure compared to those of group and hospital
pharmacies, primarily due to the sheer size of the various groups.
5.4.3 Conclusion - Research Question 2
It is evident from the discussion above that strategic changes, survival tactics,
day to day changes as well as restructuring within retail pharmacies in South
Africa is a reality as a result of the introduction of SEP. The business
environment has therefore changed and the impact of the introduction of SEP is
evident.
5.5 Conclusion
The literature review in Chapter 2 highlighted that the introduction of SEP
immediately lead to a total price reduction of 22 % for medicines in South Africa.
The research report highlighted the fact that consistent pricing benefits were not
experienced by consumers in retail pharmacies in South Africa. The literature
warns that price controls for pharmaceuticals, like SEP in South Africa, could
lead towards complexity and the creation of vested interests, leading to an

64
ultimate negative effect on patients (Calfee 2001). The research indicated that
a consistent pricing benefit is not realised by the patients and that there is a
substantial difference in the price of medication pertaining to the maximum and
minimum price range as per the collected quantitative data.
It was also evident that the impact of pricing regulation in the form of SEP
resulted in changes in the business environment for retail pharmacies in the
private sector in South Africa. The research allowed the implementation of
pricing regulation to be studied and explained.
The literature as well as the research suggested that the introduction of price
ceilings such as SEP results in an overall reduction of gross profit margins for
pharmacies in South Africa.
The research found that the business environment for retail pharmacies in the
private sector in South Africa has changed as a result of the introduction of
SEP. The strategy of pharmacies was adapted, survival tactics were
implemented, day to day changes were realised and direct or indirect
restructuring in retail pharmacies was implemented.

65
CHAPTER 6: CONCLUSIONS AND
RECOMMENDATIONS
6.1 Introduction
This chapter concludes the thesis. Conclusions made in previous chapters
were combined to devise a shared conclusion to the research. In addition to
this, topics or concerns deemed relevant by the researcher are highlighted as
recommendations. The closing section to this chapter relates to propositions or
suggestions for future research.
6.2 Conclusions of the study
The research was introduced through Chapter 1 with particular focus on the
purpose, context, problem statement, significance, delimitations, definitions and
assumptions.
Improved access to healthcare services has been a focal point in South Africa
in the post-apartheid era. For this reason the NDP was developed and a pricing
plan for medicines followed for both the private and public sectors. A pricing
committee was created and SEP along with regulated price increases was
introduced in the private sector. Effectively the private sector had to adjust from
a free to a regulated market. A total pricing impact of 22 % was immediately
realised on medicine prices. It therefore appears that the introduction of SEP
lead to a direct pricing benefit to patients. However, the literature also states
that pricing controls for pharmaceuticals could lead to overall negative impact
on patients along with a creation of vested interest.
It was questioned if patients receive a consistent pricing benefit regarding the
cost of medicines in the private sector, following the introduction of SEP.
Subsequently the business environment within retail pharmacies in the private
sector in South Africa was adjusted through the introduction of price ceilings or

66
SEP. Further to this the changing business environment as a result of pricing
interference was evaluated.
6.2.1 Response to Research Question 1
What are the perceived pricing benefits for consumers through the
implementation of SEP in the private pharmaceutical market in South
Africa?
According to the literature review, one of the benefits of the introduction of price
regulation through price caps is the reduction in excess profits (Gilmore et al.
2010). A pricing benefit is therefore expected, provided that the full benefit of
the price cap is passed on to the patient or consumer.
The contentious pharmaceutical pricing regulations and in particular the
introduction of price caps by the South African government resulted in an
overall decrease in gross profit margins for pharmacies in South Africa.
Capped, regulated price increases along with regulated dispensing fees,
significantly changed the business environment where retail pharmacies
operate currently. A total reduction of 22 % of medicines prices was realised
through the introduction of SEP in South Africa.
According to Philibert, (2009), strict targets in terms of price caps and price
floors may cause great economic risk without a comparative advantage. Prices
beyond the regulated SEP and dispensing fees were reported throughout the
research. It can be inferred that the impact of pricing regulation may entail risk
and not necessarily result in an advantage for the patient or consumer. The
research confirmed that a consistent pricing benefit was not realised by
consumers, due to the significant and clear price difference documented
through the quantitative data in the research.
6.2.2 Response to Research Question 2
What is the perceived impact of SEP on retail pharmacies in South Africa
in terms of changes in the business environment?

67
The introduction of SEP is an uncontrollable macroeconomic factor that has
impacted businesses and needs to be taken into account in the way businesses
operate, to counter the impact.
The introduction of a price ceiling on medicines prices through SEP resulted in
clear changes in the business environment for retail pharmacies in South Africa.
Retail pharmacies had to implement strategic changes and survival tactics to
stay in business. This naturally resulted in changes in the way that pharmacies
were managed daily, i.e. reduced stock on hand and an increase in order
frequency of medicines, increased pressure on pharmacists to work longer
hours and a focus to decrease overheads in general.
With a reduction in overall gross profit generated by pharmacies, the pressure
in the business environment was evident.
The overall responses of all the pharmacists who were interviewed were
investigated in terms of the common themes identified. A particular theme was
reported in the table below as a finding from this study when it was reported by
more than 60 % of the interviewed pharmacists. The findings of the literature
were also reported in the table below.
Table 11: Comparison of the findings from the literature review and this
study regarding the impact of pricing regulations on the business
environment
Literature This Study
Price caps determine productivity trends (Lowry and Getachew 2009)
Due to the introduction of a price cap, through SEP, 55 % of the pharmacy managers who were interviewed confirmed a deliberate change in strategy to focus on improved productivity.
Increased working hours was reported by 73 % of the interviewed respondents and is aligned with the concept of improved productivity. New staff was not appointed, the current staff was working more productively.

68
Reduction in overheads and overall business costs is a direct reaction to price cap regulation (Currier 2006).
Seventy seven percent of the interviewed pharmacists in this study confirmed that part of the survival tactics following the introduction of SEP included an overall reduction in overheads.
Not reported in the literature review A shift in focus on identification of alternative opportunities where prices are not regulated through SEP was introduced by 73 % of the interviewed respondents
Not reported in the literature review Ninety one percent of the interviewed pharmacists reported a reduction in stock days and this therefore implies a reduction in working capital.
6.3 Recommendations
The benefits drawn from the implementation of the SEP appears clear at first
glance. An overall 22 % reduction in the price of medicines in the private sector
was realised.
The literature clearly highlights that the only element in the marketing mix that
produces profits, is price and of the four elements, price is the easiest to
influence. However, interference with price can lead to an overall negative
effect in terms of availability and overall quality of healthcare in the long run.
The following are recommendations made to the stakeholders that were
identified in Chapter 1, section 1.4.
The Pricing Committee within the Government:
A consistent pricing benefit to patients was not realised through the introduction
of SEP.
It is recommended that the enforcement of the new dispensing fee regulation is
closely monitored to ensure a consistent pricing benefit to all patients,
purchasing medicines from independent, group or hospital pharmacies.

69
The current demand for pharmacists in South Africa is outweighing the supply
and increasing the pressure on salaries for pharmacists. A recommendation is
to therefore increase the numbers of pharmacy students for intake at
universities and increase bursaries to assist in the filling of this need.
To view the introduction of pricing regulations in the private pharmaceutical
sector such as SEP as a learning curve for future introductions of new programs
such as the national health program. To think through the practical implication
and roll out of such a program along with the overall implication as part of
indirect influences due to such a new regulation.
The Retail Pharmacies:
Various strategic changes, survival tactics and day to day changes were
implemented across independent pharmacies, group pharmacies and hospital
pharmacies to adjust to the new business environment following the introduction
of SEP.
However, these concepts were not introduced into all pharmacies to improve
strive to improved overall profitability. It is recommended that pharmacists
specifically implement improved productivity, service delivery, accurate billing
and a drive to decrease overheads within pharmacies. The organisational
structure of the group pharmacies may have lent itself to best practice sharing
and improved implementation of these concepts already.
The Patients:
The introduction of the dispensing fee law as a sliding scale leads to continuous
pricing differences among pharmacies. Although strict enforcement of this
regulation should decrease the variance in prices from pharmacy to pharmacy,
price differences will still exist between various pharmacies. Patients should
prioritise their needs in terms of the services of their pharmacy, i.e. patient
consultation, price, service delivery, additional services such as free delivery.
Based on the offering of various pharmacies, a suitable pharmacy should be
selected, not only on the benefit it offers in terms of price. In this sense the

70
public would assist to rectify dignity within the pharmacy profession and we
might see an increase in the supply of pharmacists in South Africa.
6.4 Suggestions for further research
Suggestions for future research are as follows:
To conduct the same research on a national level in South Africa in order to
compare the findings of both these studies.
Researching the influence of pricing regulation across various industries in
South Africa and draw an overall conclusion of the benefits and negative
impacts of such regulations. This would assist in future decision making
regarding pricing regulation across industries.
Determine the influence of the pricing regulation, regulation against bonussing
and generic substitution on pharmaceutical companies in South Africa.
Establish the effect of further pricing regulation such as benchmarking on the
pharmaceutical industry in South Africa.
Develop and understanding of the true benefits to patients and concerns to
health care professionals, as well as the economy regarding the proposed
national health insurance in South Africa.

71
REFERENCES
Advanstar Communications (2009) Managing the market - distribution and logistics, Pharmaceutical Technology Europe, 21(5), pp. 47-48.
Ailawadi, K. L., Lehmann, D. R. and Neslin, S. A. (2001) Market Response to a Major Policy Change in the Marketing Mix: Learning from Procter & Gamble's Value Pricing Strategy, Journal of Marketing, 65(1), pp. 44-61.
Anon (2006) Cheaper Healthcare Insurance Could Trigger Ethical Market Boom, Pharmaceutical Executive, 26(3), pp. S8-S10.
Appasamy, T. (2007) The Microeconomics of the Price Policies in the Pharmaceutical Industry.
Atella, V., Bhattacharya, J. and Carbonari, L. (2008) Pharmaceutical Industry, Drug Quality and Regulation: Evidence from US and Italy, NBER Working Paper.
Bakk, L. (2009) Medicare Prescription Drug, Improvement, and Modernization Act of 2003: Implications for the Future of Health Care, Health & Social Work, 34(1), pp. 59-63.
Bernstein Global Wealth Management (2009a) Brazil, Black Book - Global Pharmaceuticals: Emerging Markets Should Infuse Badly Needed Revenues for Years to Come, pp. 19-28.
Bernstein Global Wealth Management (2009b) India, Black Book - Global Pharmaceuticals: Emerging Markets Should Infuse Badly Needed Revenues for Years to Come, pp. 41-51.
Bester, M. (2009) SEP legislation - Has it reduced the price of medicines?, Generic Medicines Congress - South Africa, Johannesburg.
Biglaiser, G. and Riordan, M. (2000) Dynamics of Price Regulation, RAND Journal of Economics, 31(4), pp. 744-767.
Bodhania, M. (2007) Pharmaceutical Sector Presentation for Private Health Sector Indaba, Private Health Sector Indaba p. 20, Pharmaceutical Industry, Johannesburg.

72
Brand South Africa (2009) Health Care in South Africa, (last accessed 27 Jan 2010), from http://www.southafrica.info/about/health/health.htm.
Calfee, J. E. (2001) Pharmaceutical Price Controls and Patient Welfare, Annals of Internal Medicine, 134(11), pp. 1060-1064.
Carnwell, R. and Daly, W. (2001) Strategies for the construction of a critical review of the literature, Nurse Education in Practice, 1(2), pp. 57-63.
Council for Medical Schemes (2009) Council for Medical Schemes Annual Report 2008-2009, Council For Medical Schemes.
Council for Medical Schemes (2010) Council for Medical Schemes, (last accessed 30 January, 2010), from http://www.medicalschemes.com/medical_schemes_pmb/index.htm.
Creswell, J. (2009) Research Design Qualitative, Quantitative and Mixed Methods Approaches, 3rd ed., Sage Publications California.
Currier, K. M. (2006) Quality-Adjusted Laspeyres Price Caps: A Graphical Analysis, Atlantic Economic Journal, 34(4), p. 481.
Danzon, P. (1999) Making sense of drug prices, REGULATION-WASHINGTON-, 23(1), pp. 56-63.
Department of Health (1996) National Drug Policy for South Africa, (last accessed 27 Jan 2010), from http://www.doh.gov.za/docs/policy/drugsjan1996.pdf.
Design and Marketing Dictionary (2011) Auction Type Pricing (last accessed 16 Jan 2011), from http://design-marketing-dictionary.blogspot.com/2010/07/auction-type-pricing.html.
Docteur, E., Paris, V. and Moise, P. (2008a) Pharmaceutical pricing policies in a global market, OECD.
Docteur, E., Paris, V. and Moïse, P. (2008b) Pharmaceutical Pricing Policies in a Global Market, Paris: OECD
Economist Intelligence Unit (2005) World, Industry Overview, EIU: Economist Intelligence Unit.

73
Economist Intelligence Unit (2009a) Greece: Healthcare report, Healthcare Industry Report: Greece, pp. 9-16.
Economist Intelligence Unit (2009b) Israel: Healthcare report, Healthcare Industry Report: Israel, pp. 9-21.
Economist Intelligence Unit (2009c) Russia: Healthcare report, Healthcare Industry Report: Russia, pp. 9-17.
Economist Intelligence Unit (2009d) South Africa: Healthcare report, Healthcare Industry Report: South Africa, pp. 8-18.
Economist Intelligence Unit (2010) Healthcare report, Healthcare Industry Report: Egypt, pp. 9-17.
Gilmore, A. B., Branston, J. R. and Sweanor, D. (2010) The case for smoke: how tobacco price regulation is needed to promote the health of markets, government revenue and the public, Tobacco Control, 19(5), pp. 423-430.
Gilson, L. and McIntyre, D. (2007) Post-apartheid challenges: household access and use of care, International Journal of Health Services 37(4), pp. 673-691.
Gray, A. and Matsebula, T. (2000) Drug Pricing, In: Health Systems Trust, Health Systems Trust, Durban
Gray, A. L. (2009) Medicine pricing interventions - the South African experience Southern Med Review, 2(2), p. 19.
Joshi, H. N. (2003) Analysis of the Indian Pharmaceutical Industry With Emphasis on Opportunities in 2005, Pharmaceutical Technology North America, 27(1), p. 74.
Kalof, L., Dan, A. and Diet, T. (2008) Essentials of Social Research, Open University Press, Maidenhead.
Kessler, D. (2004) The effects of pharmaceutical price controls on the cost and quality of medical care: a review of the empirical literature, draft paper submitted to the US International Trade Administration, p. 3.

74
Knittel, C. R. and Stango, V. (2003) Price Ceilings as Focal Points for Tacit Collusion: Evidence from Credit Cards, American Economic Review, 93(5), pp. 1703-1729.
Kortge, G. and Okonkwo, P. (1993) Perceived value approach to pricing, Industrial Marketing Management, 22(2), pp. 133-140.
Kotler, P. and Keller, K. (2006) Marketing Management, 12th ed., Pearson Prentice Hall, Upper Saddle River.
Lavoie, M. (1996) Unproductive outlays and capital accumulation with target-return pricing, Review of Social Economy, 54(3), pp. 303-321.
Lotter, J. (2010a) The essential role of medicines in the healthcare system - IIR Healthcare Summit 2010, Johannesburg South Africa.
Lotter, J. (2010b) Overall price reduction of medicines prices in South Africa, Health Projects Manager Innovative Medicines South Africa ed., Johannesburg.
Lowry, M. N. and Getachew, L. (2009) Price Control Regulation in North America: Role of Indexing and Benchmarking, Electricity Journal, 22(1), pp. 63-76.
Maitland, I. (2002) Priceless Goods: How Should Life-Saving Drugs Be Priced?, Business Ethics Quarterly, 12(4), pp. 451-480.
Marn, M. V. and Rosiello, R. L. (1992a) Managing Price, Gaining Profit, Harvard Business Review, 70(5), pp. 84-94.
Marn, M. V. and Rosiello, R. L. (1992b) Managing price, gaining profit, McKinsey Quarterly(4), pp. 18-37.
Mayring, P. (2000) 'Qualitative content analysis', Citeseer, pp. 2-00.
McIntyre, D. and Thiede, M. (2007) Healthcare Fincnacing and Expenditure, Health Systems Trust, Durban
Mochtar, K. and Arditi, D. (2000) Alternate pricing strategies in construction, Journal of Dimensi Teknik Sipil, 2(1), pp. 56–64.

75
Motsoaledi, A. (2010) 'Government Gazette', Medicines and Related Substances Act (101/1965): Regulations relating to a transparent pricing system for medicines and scheduled substances: Amendment (Dispensing Fee for Pharmacists), 19 November 2010, p. 8.
Mrazek, M. (2002) Comparative approaches to pharmaceutical price regulation in the European Union, Public Health 43(4), pp. 453-461.
Munnukka, J. (2006) Pricing method as a tool for improved price perception, Journal of Revenue & Pricing Management, 5(3), pp. 207-220.
Naish, H. F. (1990) The Near Optimality of Markup Pricing, Economic Inquiry, 28(3), p. 555.
Neuendorf, K. A. (2002) The content analysis guidebook, Sage Publications, Inc.
Nóbrega, O. d. T., Marques, A. R., de Araújo, A. C. G., Karnikowski, M. G. d. O., de Oliveira Silva Naves, J. and Silver, L. D. (2007) Retail prices of essential drugs in Brazil: an international comparison, Precios minoristas de medicamentos esenciales en Brasil: comparación internacional., 22(2), pp. 118-123.
Oriola, T. (2009) Strong Medicine: Patents, Market, and Policy Challenges for Managing Neglected Diseases and Affordable Prescription Drugs, Can. JL & Tech., 7, p. 57.
Paris, V. and Docteur, É. (2009) Pharmaceutical pricing and reimbursement policies in Canada.
Pharmaceutical Executive (2006) Cheaper Healthcare Insurance Could Trigger Ethical Market Boom, Pharmaceutical Executive, 26(3), pp. S8-S10.
Philibert, C. (2009) Assessing the value of price caps and floors, Climate Policy (Earthscan), 9(6), pp. 612-633.
Scherer, F. (2004) The Pharmaceutical Industry - Prices and Progress New England Journal of Medicine, 351(9), p. 927.
Siva, N. (2009) The drug price is right-or is it?, The Lancet, 373(9672), p. 1326.

76
Tshabalala-Msimang, M. (2004) Regulations on the Prices of Medicines, (last accessed 25 June, 2010), from http://www.doh.gov.za/docs/pr/2004/pr0115.html.
Vernon, J. (2002) Drug research and price controls, Regulation, 25(4), pp. 22–25.
Williams, K. (2007) Pharmaceutical price regulation, South African Journal on Human Rights, 23(1), p. 1.
Willig, C. (2008) Introducing Qualitative Research in Psychology: Adventures in Theory and Method, 2nd ed., McGraw Hill, Maidenhead.

77
APPENDIX A – QUANTITATIVE DATA (SCRIPT PRICING)
Letter to Respondents
Dear Respondent,
I am completing an MBA at Wits Business School, in Johannesburg. My MBA
dissertation is based on the following topic: The Impact of the implementation of
single exit pricing for pharmaceuticals in South Africa. The aim of the research
is to investigate the impact of SEP implementation on retail pharmacies as well
as patients in the private sector. I would be grateful if you could complete the
attached questionnaire for this purpose.
Confidentiality will be observed throughout the conveyance of the research and
the final report will be for academic purposes only. If you request that the
information you provide should not be attributed to you, this will be respected.
Should you wish to receive a copy of the final research, you may request it by
contacting me directly, as per my contact details below.
Your contribution to academia and agreement to arrange this interview is
greatly appreciated.
Yours sincerely,
Daleen Pretorius
Student No: 332082
WBS MBA Part Time April 2008 Intake
Email [email protected]
Cellphone 082 447 789 4
WBS Tel: 011 717 3600

78
Interviewer Administered Questionnaire
Cash sales price of the following medicines
Cipramil 20mg 28 pack R______________________
Lanzor 30mg 28 pack R______________________
Norvasc 10mg 30 pack R______________________
Augmentin 1g BD 5 days R______________________

79
APPENDIX B – QUALITATIVE DATA (SEMI-
STRUCTURED INTERVIEW)
Letter to Respondents
Dear Respondent,
I am completing an MBA at Wits Business School, in Johannesburg. My MBA
dissertation is based on the following topic: The Impact of the implementation of
single exit pricing for pharmaceuticals in South Africa. The aim of the research
is to investigate the impact of SEP implementation on retail pharmacies in the
private sector. I would be grateful if I could arrange an hour interview with you
to understand your perspective on the subject as a senior manager of a
pharmacy group / as an owner of a retail pharmacy / as a manager of a hospital
pharmacy.
Confidentiality will be observed throughout the conduction of the research and
the final report will be for academic purposes only. Notes of the discussion will
be made during the interview and this information will be utilised as part of the
research report. If you request that the information you provide should not be
attributed to you, this will be respected. Should you wish to receive a copy of
the final research, you may request it by contacting me directly, as per my
contact details below.
Your contribution to academia and agreement to arrange this interview is
greatly appreciated.
Yours sincerely,
Daleen Pretorius
Student No: 332082
WBS MBA Part Time April 2008 Intake
Email [email protected]

80
Cellphone 082 447 789 4
WBS Tel: 011 717 3600
Research Instrument: Interview Schedule
The Impact of the implementation of single exit price for pharmaceuticals in South Africa
Thank you for participating in this research as a pharmacy manager or owner.
Be assured that any information provided will be held in the strictest confidence.
The interview will be recorded with your permission and notes will be taken
throughout the interview. Should you request that the information provided by
you is not to be attributed to you, this will be respected. The data collected for
the purpose of research will not be used for any other purpose without obtaining
your permission for any alternative or additional use.
The following research focused on the impact of the implementation of
single exit price for pharmaceuticals in South Africa. The research
investigates the impact of the implementation of Single Exit Price (SEP) on
retail pharmacies in the private medical sector in South Africa.
For this purpose the following questionnaire is posed to you and will address
the impact of the implementation of pricing regulations within the private
pharmaceutical retail pharmacy setting in South Africa.
Virtually no research is available to analyse the impact of SEP on retail
pharmacies in the private sector. For this reason, your input is highly important
to advance the body of knowledge regarding the topic of price ceilings in the
private retail pharmacy setting in South Africa.
Thank you,
Daleen Pretorius

81
Section A : Demographic
1. Summarise your own background and experience in retail pharmacy
business and management by focusing on your current as well as
previous positions / experience. Please include the following:
a) Job description / title
b) Functional roles
c) Number of years experience as pharmacy manager / owner
d) Number of employees working in the pharmacy
2. Describe the type of your retail pharmacy that are affiliated with including
the amount of personally working at the pharmacy / group i.e.
a) Independent retail pharmacy
b) Pharmacy as part of a pharmacy group
c) Hospital pharmacy (independent / part of a pharmacy group)
Section B : The Impact of SEP
1. Describe the influence of SEP on the business strategy of the pharmacy
i.e. additional products or services you are offering following the
introduction of SEP
2. What changes occurred in the business of this pharmacy in order to
survive the implementation of SEP?
3. How did the implementation of SEP influence your day to day business?
4. Was there any restructuring involved within this pharmacy following the
introduction of SEP and how did the restructuring affect your business?
Thank You.
Daleen Pretorius

82
APPENDIX C
Table 12: The Influence of SEP on the Business Strategy of Independent Pharmacies
Pharmacy
Number
Front
Shop
Focus
Warehousing
and Logistics
Focus
Additional
Services
Focus on
Alternative
Medicines
Improved
Productivity
Cash
Flow
Focus
Improved
Service
Delivery
Joined a
Group
Pharmacy Layout
Customer
Retention
Strategy
Profit
to
Cost
Centre
Increase
Volume
Sales
Independent Pharmacies
I1 � - � � - � - - - � - -
I2 - - - - - - - - - � - �
I3 - - � - � - � - - - - �
I4 � - � � � - � - - � - �
I5 � - � � - � - - - � - -
I6 � - � � - � - - - � - -
Independent
Total 4 0 5 4 2 3 2 0 0 5 0 3
% Total
Independent 67% 0% 83% 67% 33% 50% 33% 0% 0% 83% 0% 50%

83
Table 13: The Influence of SEP on the Business Strategy of Group Pharmacies
Pharmacy
Number
Front
Shop
Focus
Warehousing
and Logistics
Focus
Additional
Services
Focus on
Alternative
Medicines
Improved
Productivity
Cash
Flow
Focus
Improved
Service
Delivery
Joined a
Group
Pharmacy Layout
Customer
Retention
Strategy
Profit
to
Cost
Centre
Increase
Volume
Sales
Group Pharmacies
G1 � � � � � � � - - � - �
G2 � � � � � � � - - � - �
G3 � � � - - - - � � - - -
G4 - � - � - � - � - � - -
G5 - � � - � - - � - � - �
G6 � - � � � � � - � � - �
G7 � - � � - - � - � � - -
G8 � � � � � - � - - � - �
Total Group 6 6 7 6 5 4 5 3 3 7 0 5
% Total
Group 75% 75% 88% 75% 63% 50% 63% 38% 38% 88% 0% 63%

84
Table 14: The Influence of SEP on the Business Strategy of Hospital Pharmacies
Pharmacy
Number
Front
Shop
Focus
Warehousing
and Logistics
Focus
Additional
Services
Focus on
Alternative
Medicines
Improved
Productivity
Cash
Flow
Focus
Improved
Service
Delivery
Joined a
Group
Pharmacy Layout
Customer
Retention
Strategy
Profit
to
Cost
Centre
Increase
Volume
Sales
Hospital Pharmacies
H1 � - - - - - - - � - � -
H2 � � � � - - - - - - � �
H3 � - - � � � � - - - � �
H4 - � - � - � - - - - � �
H5 � � � � � � � - � � � �
H6 � � � � � � � - - - � �
H7 � � � � � - � - - � � �
H8 - - - - � � � - - - � �
Hospital
Total 6 5 4 6 5 5 5 0 2 2 8 7
Total
Hospital
Pharmay 75% 63% 50% 75% 63% 63% 63% 0% 25% 25% 100% 88%
Total All
Pharmacies 16 11 16 16 12 12 12 3 5 14 8 15
Total % All
Pharmacies 73% 50% 73% 73% 55% 55% 55% 14% 23% 64% 36% 68%

85
Table 15: Survival Tactics Following the Introduction of SEP for Independent Pharmacies
Pharmacy
Number
Calculation
Personell -
Cut
Overheads
Specialised
Manager -
Manage
Overheads
Increase
Pharmacy
Assistants
Pharmacist
Working
Hours
Increase
Decrease
Overheads
Decreased
Staff Advertising
Increase
Generic
Substitution
Accurate
Billing
Per
Diem
Accounts
Independent Pharmacies
I1 - - - � � - - � - -
I2 - - - � � - - - - -
I3 - - � � � - - - - -
I4 - - � - � - - - - -
I5 - - - � � - � - - -
I6 - - � � � - - � - -
Independent
Total 0 0 3 5 6 0 1 2 0 0
% Total
Independent 0% 0% 50% 83% 100% 0% 17% 33% 0% 0%

86
Table 16: Survival Tactics Following the Introduction of SEP for Group Pharmacies
Pharmacy
Number
Calculation
Personnel -
Cut
Overheads
Specialised
Manager -
Manage
Overheads
Increase
Pharmacy
Assistants
Pharmacist
Working
Hours
Increase
Decrease
Overheads
Decreased
Staff Advertising
Increase
Generic
Substitution
Accurate
Billing
Per
Diem
Accounts
Group Pharmacies
G1 � � � - - - � - - -
G2 � � � - - - � - - -
G3 - - � � � - - - - -
G4 - - - - � - - - - -
G5 � - - � � � - - - -
G6 � - � - - - � - - -
G7 - - � � � - � - - -
G8 � � � - - - � - - -
Total
Group 5 3 6 3 4 1 5 0 0 0
% Total
Group 63% 38% 75% 38% 50% 13% 63% 0% 0% 0%

87
Table 17: Survival Tactics Following the Introduction of SEP for Hospital Pharmacies
Pharmacy
Number
Calculation
Personnel -
Cut
Overheads
Specialised
Manager -
Manage
Overheads
Increase
Pharmacy
Assistants
Pharmacist
Working
Hours
Increase
Decrease
Overheads
Decreased
Staff Advertising
Increase
Generic
Substitution
Accurate
Billing
Per
Diem
Accounts
Hospital Pharmacies
H1 - - � - � - - � � �
H2 � - - - � - - � � �
H3 � � � - - - � � � �
H4 � � - - � - - � � �
H5 � � � - � - - � � �
H6 � � - - � - - � � �
H7 � - - � � - - � - -
H8 � � � - � - - � � �
Hospital
Total 7 5 4 1 7 0 1 8 7 7
Total
Hospital
Pharmacies 88% 63% 50% 13% 88% 0% 13% 100% 88% 88%
Total All
Pharmacies 12 8 13 9 17 1 7 10 7 7
Total % All
Pharmacies 55% 36% 59% 41% 77% 5% 32% 45% 32% 32%

88
Table 18: The Influence of the Implementation of SEP Regarding Day to
Day Business for Independent Pharmacies
Pharmacy
Number
Reduction in
Stock Days
Increased
Working Hours
Increased Pressure to
Decrease Overheads
Independent Pharmacies
I1 � � -
I2 � � -
I3 � � -
I4 � � -
I5 � � -
I6 � � -
Independent
Total 6 6 0
% Total
Independent 100% 100% 0%
Table 19: The Influence of the Implementation of SEP Regarding Day to
Day Business for Group Pharmacies
Pharmacy
Number
Reduction in
Stock Days
Increased
Working Hours
Increased Pressure to
Decrease Overheads
Group Pharmacies
G1 - - -
G2 � - -
G3 - � -
G4 � - -
G5 � � -
G6 � � -
G7 � � -
G8 � � -
Total Group 6 5 0
% Total
Group 75% 63% 0%

89
Table 20: The Influence of the Implementation of SEP Regarding Day to
Day Business for Hospital Pharmacies
Pharmacy
Number
Reduction in
Stock Days
Increased
Working Hours
Increased Pressure to
Decrease Overheads
Hospital Pharmacies
H1 � � �
H2 � � �
H3 � - -
H4 � � �
H5 � - -
H6 � - -
H7 � � �
H8 � � �
Hospital
Total 8 5 5
Total
Hospital
Pharmay 100% 63% 63%
Total All
Pharmacies 20 16 5
Total % All
Pharmacies 91% 73% 23%

90
Table 21: The Influence of the Implementation of SEP on the Restructuring
within Independent Pharmacies
Pharmacy
Number
Direct
Restructuring Indirect Restructuring
Independent Pharmacies
I1 - �
I2 � -
I3 - �
I4 - -
I5 � -
I6 - �
Independent
Total 2 3
% Total
Independent 33% 50%
Table 22: The Influence of the Implementation of SEP on the Restructuring
within Group Pharmacies
Pharmacy
Number
Direct
Restructuring Indirect Restructuring
Group Pharmacies
G1 - -
G2 - -
G3 - �
G4 - -
G5 - �
G6 - �
G7 - -
G8 - -
Total Group 0 3
% Total
Group 0% 38%

91
Table 23: The Influence of the Implementation of SEP on the Restructuring
within Hospital Pharmacies
Pharmacy
Number
Direct
Restructuring Indirect Restructuring
Hospital Pharmacies
H1 - -
H2 - -
H3 - -
H4 - �
H5 - -
H6 - -
H7 - -
H8 - -
Hospital
Total 0 1
Total
Hospital
Pharmay 0% 13%
Total All
Pharmacies 2 7
Total % All
Pharmacies 9% 32%

92
Table 24: Actual Scripts Priced at Fifty Pharmacies (Quantitative Data)
Priced
Script
Number
Pharmacy
Number
Independent
/ Group /
Hospital R Value
1 IA Independent R 1,270.60
2 IB Independent R 1,475.51
3 IC Independent R 1,475.51
4 ID Independent R 1,516.04
5 IE Independent R 1,456.83
6 IF Independent R 1,451.99
7 IG Independent R 1,183.46
8 IH Independent R 1,475.50
9 II Independent R 1,468.04
10 IJ Independent R 1,226.28
11 IK Independent R 1,254.44
12 IL Independent R 1,612.37
13 GA Group R 1,494.09
14 GB Group R 1,295.55
15 GC Group R 1,193.72
16 GD Group R 1,193.72
17 GE Group R 1,193.72
18 GF Group R 1,295.81
19 GG Group R 1,193.72
20 GH Group R 1,193.46
21 GI Group R 1,419.10
22 GJ Group R 1,475.51
23 GK Group R 1,475.50
24 GL Group R 1,193.47
25 GM Group R 1,193.72
26 GN Grop R 1,193.72
27 GO Group R 1,193.47
28 GP Group R 1,193.72
29 GQ Group R 1,193.72
30 GR Group R 1,191.23
31 GS Group R 1,193.47
32 GT Group R 1,193.72
33 GU Group R 1,191.23
34 HA Hospital R 1,475.75
35 HB Hospital R 1,475.75
36 HC Hospital R1475.75
37 HD Hospital R 1,514.66
38 HE Hospital R 1,475.50

93
Priced
Script
Number
Pharmacy
Number
Independent
/ Group /
Hospital R Value
39 HF Hospital R 1,444.98
40 HG Hospital R 1,329.44
41 HH Hospital R 1,475.50
42 HI Hospital R 1,475.75
43 HJ Hospital R 1,475.50
44 HK Hospital R 1,711.79
45 HL Hospital R 1,444.98
46 HM Hospital R 1,475.50
47 HN Hospital R 1,254.66
48 HO Hospital R 1,475.75
49 HP Hospital R 1,475.75
50 HQ Hospital R 1,433.80