Embed Size (px)
Citation preview
The impact of WASH on maternal & newborn health:
What do we know?
Joanna Esteves MillsCEO SHARE Consortium
London School of Hygiene & Tropical Medicine
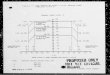
Is Sanitation correlated with Maternal Mortality? Yes.... Water is Too
Source: Gapminder.org
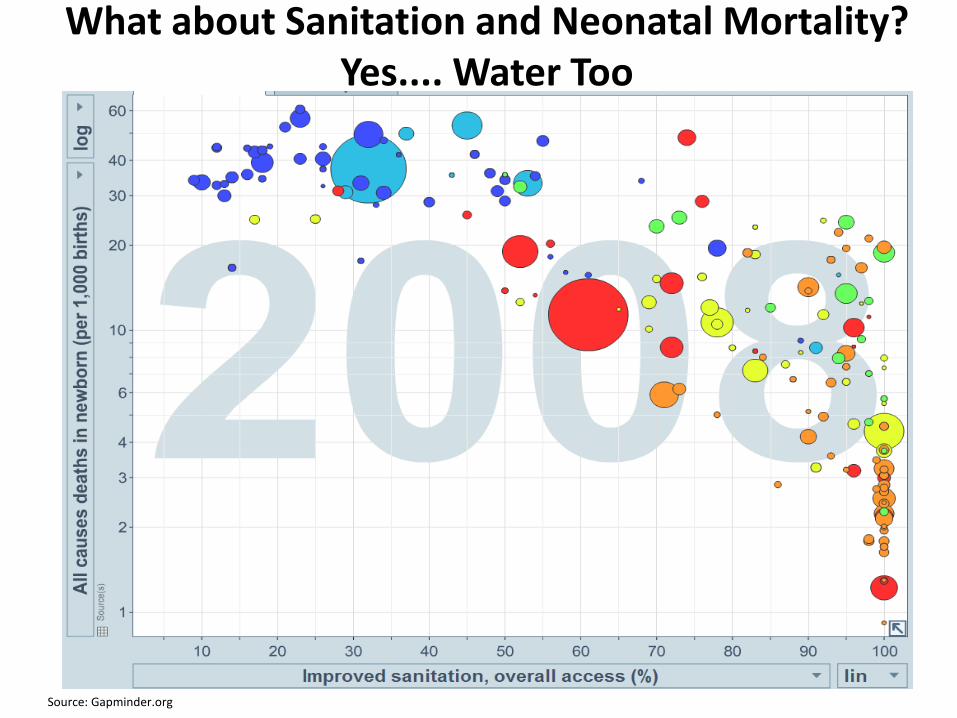
What about Sanitation and Neonatal Mortality? Yes.... Water Too
Source: Gapminder.org
Conceptual framework
Oona Campbell, Lenka Benova, Oliver Cumming, Giorgia Gon, Kaosar Afsana
Conceptual framework
Three lenses:
2. Gendered inequalities
1. WASH transmission
3. Life-course approach
1. In the water 2. Behaviour & location
Conceptual framework
Conceptual framework
WASH transmission
Water-borne Infections – via bacterial, parasitic and viral oral-faecal infections; Inorganic chemical compounds – natural contaminants
Water-washedInsufficient water for personal/domestic/institutional hygiene; Poor hygiene and faeces disposal
Water-relatedVia insects near water
Water-basedInfections - via aquatic vector
Conceptual framework
WASH transmission
Distance water sources or lack of water when needed Physical burden of carrying water, time and financial costs, drudgery
Perception of water and sanitation availability; stigma or feararound use of sanitation facilitiesReal or perceived availability of water or sanitation
Water/sanitation in risky or isolated locationsPests and perverts
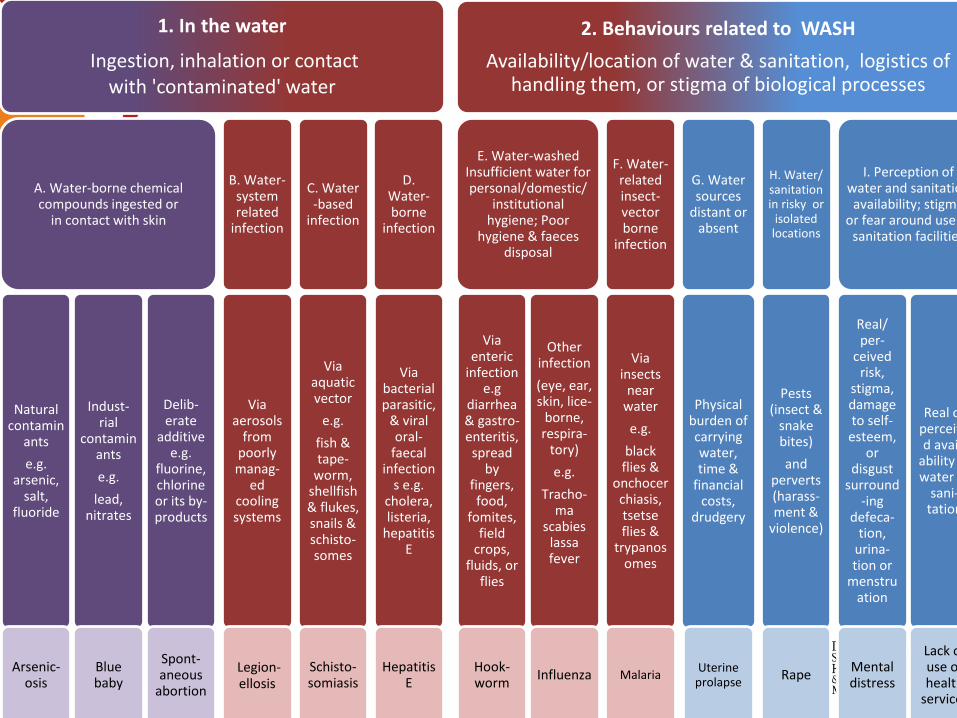
1. In the water
Ingestion, inhalation or contact with 'contaminated' water
A. Water-borne chemical compounds ingested or
in contact with skin
Natural contamin
ants
e.g. arsenic,
salt, fluoride
Arsenic-osis
Indust-rial
contaminants
e.g.
lead, nitrates
Blue baby
Delib-erate
additive e.g.
fluorine, chlorine or its by-products
Spont-aneous
abortion
B. Water-system related
infection
Via aerosols
from poorly manag-
edcooling systems
Legion-ellosis
C. Water -based
infection
Via aquatic vector
e.g.
fish & tape-
worm, shellfish & flukes, snails & schisto-somes
Schisto-somiasis
D. Water-borne
infection
Via bacterial parasitic,
& viral oral-
faecal infection
s e.g. cholera, listeria,
hepatitis E
Hepatitis E
2. Behaviours related to WASH
Availability/location of water & sanitation, logistics of handling them, or stigma of biological processes
E. Water-washed Insufficient water for personal/domestic/
institutional hygiene; Poor
hygiene & faeces disposal
Via enteric
infection e.g
diarrhea& gastro-enteritis, spread
by fingers, food,
fomites, field
crops, fluids, or
flies
Hook-worm
Other infection
(eye, ear, skin, lice-
borne, respira-
tory)
e.g.
Tracho-ma
scabieslassafever
Influenza
F. Water-related insect-vector borne
infection
Via insects
near water
e.g.
black flies &
onchocerchiasis, tsetse flies &
trypanosomes
Malaria
G. Water sources
distant or absent
Physical burden of carrying water, time &
financial costs,
drudgery
Uterine prolapse
H. Water/ sanitation in risky or
isolated locations
Pests (insect &
snake bites)
and perverts (harass-ment &
violence)
Rape
I. Perception of water and sanitation availability; stigma
or fear around use of sanitation facilities
Real/ per-
ceivedrisk,
stigma, damage to self-
esteem, or
disgust surround
-ingdefeca-
tion, urina-tion or
menstruation
Mental distress
Real or perceived avail-
ability of water or
sani-tation
Lack of use of health
services
Conceptual framework
Gender inequalities perspective
Diseases or conditions that are:
• unique to women or some subgroup of women
• more prevalent
• more serious
• for which the risk factors are different
• for which the interventions are different
(National Institutes of Health (1991))
For example: water-borne infectionsCholera versus Hepatitis E.
Infections: cord, skin & eye
Opportunity costs
Obstructed labour
Maternal DeathStunting
Cognitive impairment
School absenteeism/dropout
Prolapse
Spinal compression
Caloric expenditure
C-section
Spontaneous abortion
UTI
Repeated pregnancy
Unacceptable ANC, delivery & PNC services
Infections: enteric, parasitic, respiratory
Unacceptable child health services
Anaemia, rheumatic disease
Early marriage
Early childbearing
Pelvic inflammatory disease
InfertilityStigma
Low birth weightMorbidity
Poor mental health
Orphans
Harassment, rape
UTI
Unacceptable FP services
Stillbirth
AnaemiaCardiac disease
Unacceptable schools
Short adult
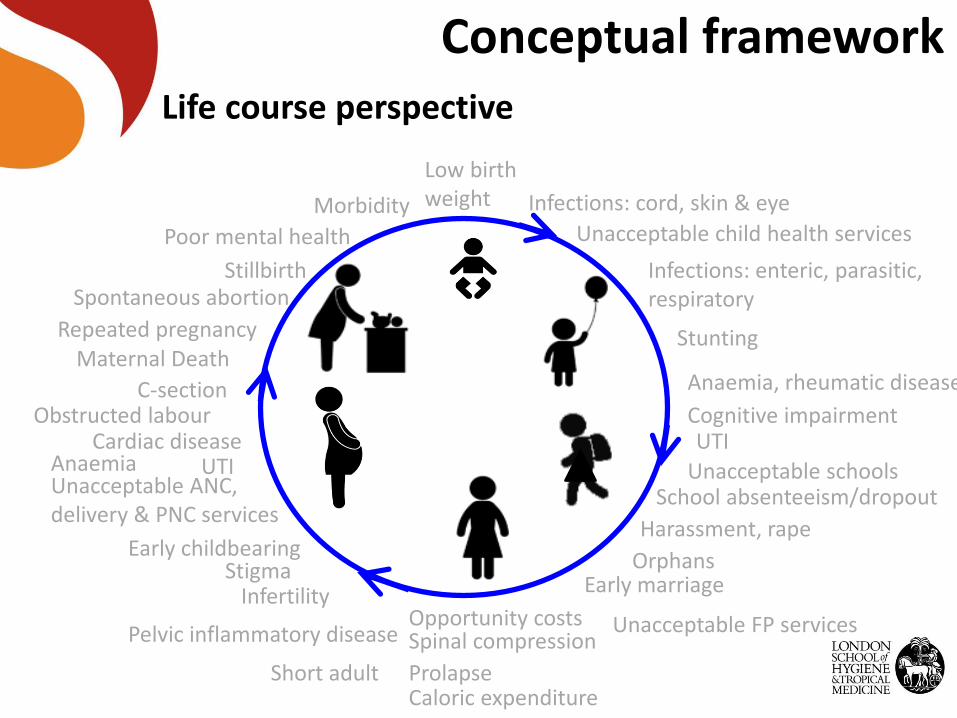
Conceptual frameworkLife course perspective
Infections: cord, skin & eye
Opportunity costs
Obstructed labour
Maternal DeathStunting
Cognitive impairment
School absenteeism/dropout
Prolapse
Spinal compression
Caloric expenditure
C-section
Spontaneous abortion
UTI
Repeated pregnancy
Unacceptable ANC, delivery & PNC services
Infections: enteric, parasitic, respiratory
Unacceptable child health services
Anaemia, rheumatic disease
Early marriage
Early childbearing
Pelvic inflammatory disease
InfertilityStigma
Low birth weightMorbidity
Poor mental health
Orphans
Harassment, rape
UTI
Unacceptable FP services
Stillbirth
AnaemiaCardiac disease
Unacceptable schools
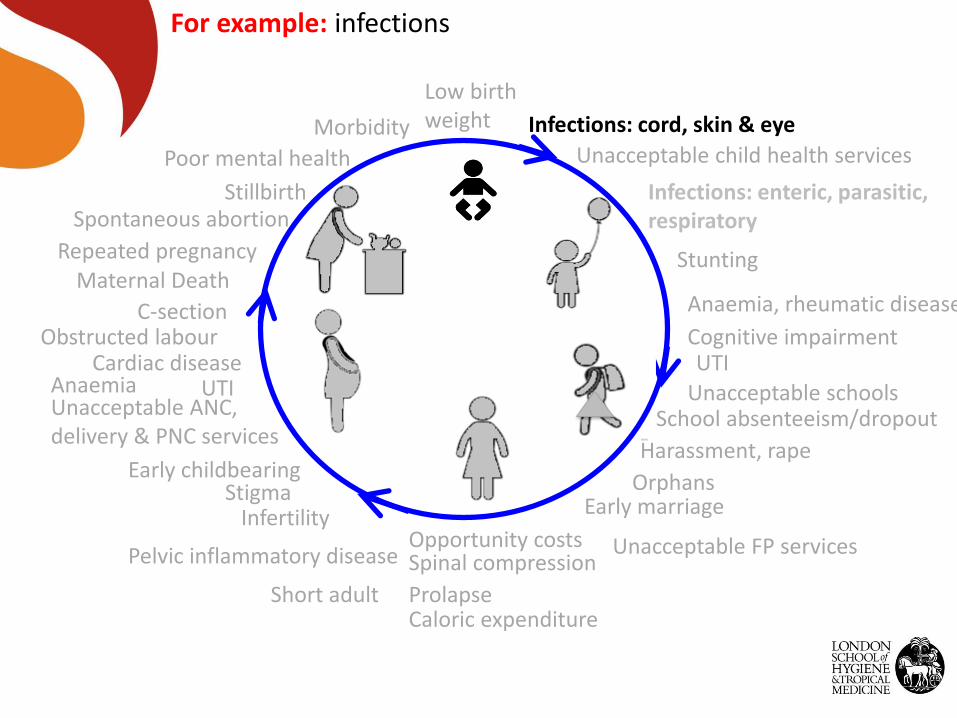
For example: infections
Short adult
Infections: cord, skin & eye
Opportunity costs
Obstructed labour
Maternal DeathStunting
Cognitive impairment
School absenteeism/dropout
Prolapse
Spinal compression
Caloric expenditure
C-section
Spontaneous abortion
UTI
Repeated pregnancy
Unacceptable ANC, delivery & PNC services
Infections: enteric, parasitic, respiratory
Unacceptable child health services
Anaemia, rheumatic disease
Early marriage
Early childbearing
Pelvic inflammatory disease
InfertilityStigma
Low birth weightMorbidity
Poor mental health
Orphans
Harassment, rape
UTI
Unacceptable FP services
Stillbirth
AnaemiaCardiac disease
Unacceptable schools
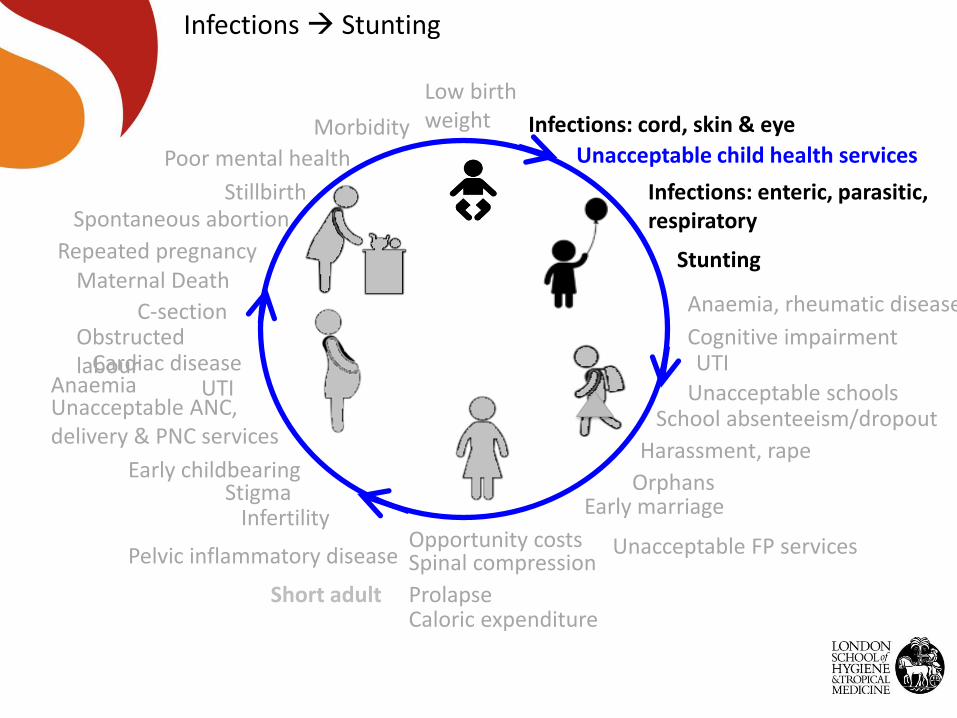
Infections Stunting
Short adult
Infections: cord, skin & eye
Opportunity costs
Obstructed labour
Maternal DeathStunting
Cognitive impairment
School absenteeism/dropout
Prolapse
Spinal compression
Caloric expenditure
C-section
Spontaneous abortion
UTI
Repeated pregnancy
Unacceptable ANC, delivery & PNC services
Infections: enteric, parasitic, respiratory
Unacceptable child health services
Anaemia, rheumatic disease
Early marriage
Early childbearing
Pelvic inflammatory disease
InfertilityStigma
Low birth weightMorbidity
Poor mental health
Orphans
Harassment, rape
UTI
Unacceptable FP services
Stillbirth
AnaemiaCardiac disease
Unacceptable schools
Short adult
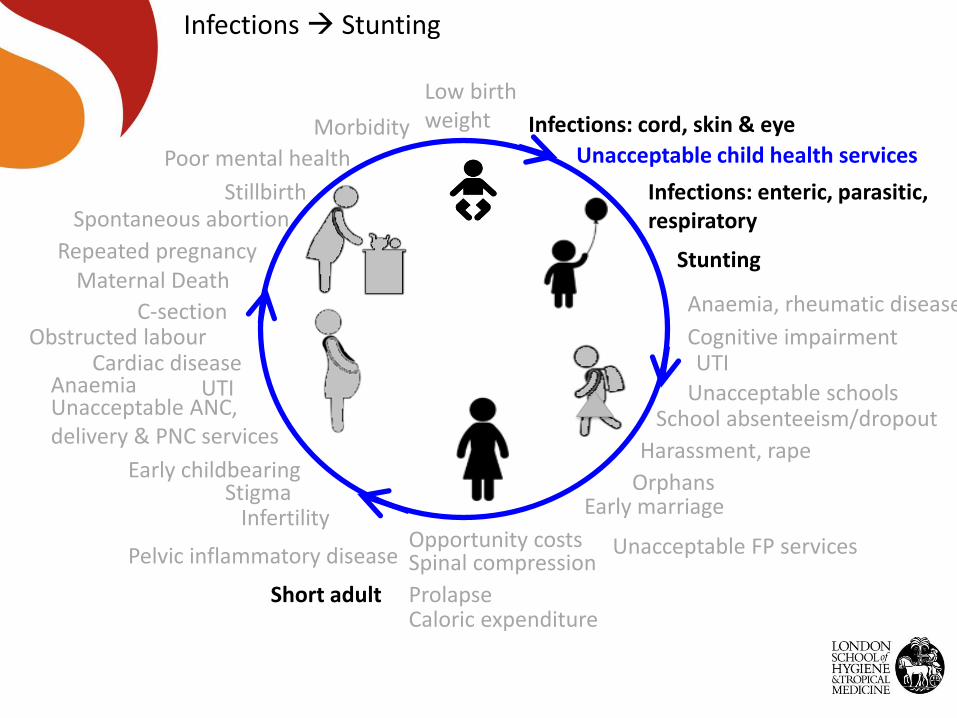
Infections Stunting
Infections: cord, skin & eye
Opportunity costs
Obstructed labour
Maternal DeathStunting
Cognitive impairment
School absenteeism/dropout
Prolapse
Spinal compression
Caloric expenditure
C-section
Spontaneous abortion
UTI
Repeated pregnancy
Unacceptable ANC, delivery & PNC services
Infections: enteric, parasitic, respiratory
Unacceptable child health services
Anaemia, rheumatic disease
Early marriage
Early childbearing
Pelvic inflammatory disease
InfertilityStigma
Low birth weightMorbidity
Poor mental health
Orphans
Harassment, rape
UTI
Unacceptable FP services
Stillbirth
AnaemiaCardiac disease
Unacceptable schools
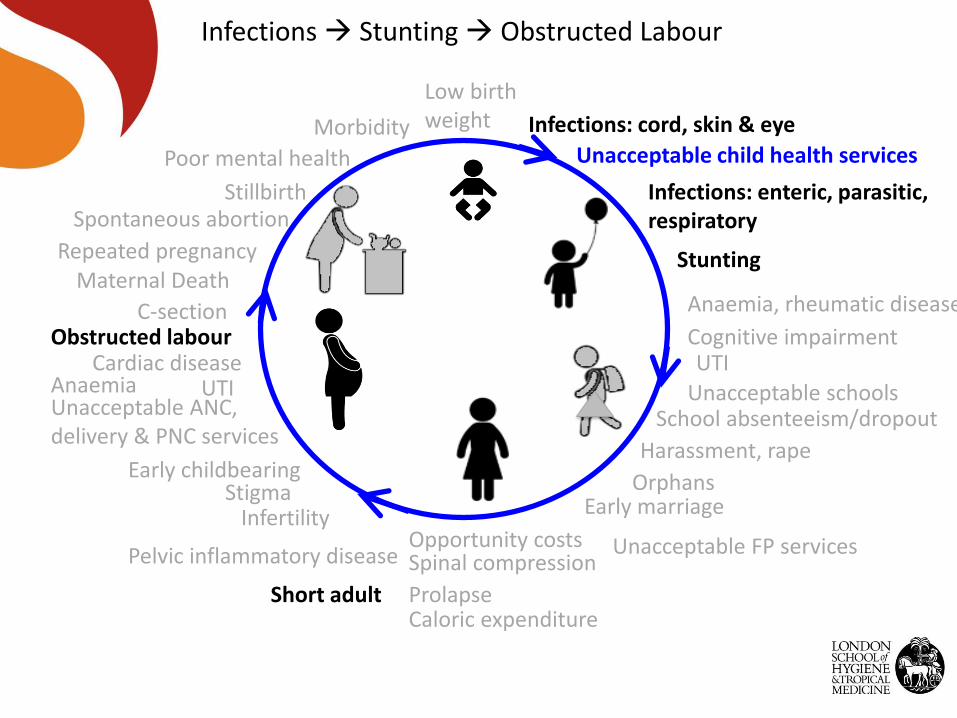
Infections Stunting Obstructed Labour
Short adult
Infections: cord, skin & eye
Opportunity costs
Obstructed labour
Maternal DeathStunting
Cognitive impairment
School absenteeism/dropout
Prolapse
Spinal compression
Caloric expenditure
C-section
Spontaneous abortion
UTI
Repeated pregnancy
Unacceptable ANC, delivery & PNC services
Infections: enteric, parasitic, respiratory
Unacceptable child health services
Anaemia, rheumatic disease
Early marriage
Early childbearing
Pelvic inflammatory disease
InfertilityStigma
Low birth weightMorbidity
Poor mental health
Orphans
Harassment, rape
UTI
Unacceptable FP services
Stillbirth
AnaemiaCardiac disease
Unacceptable schools
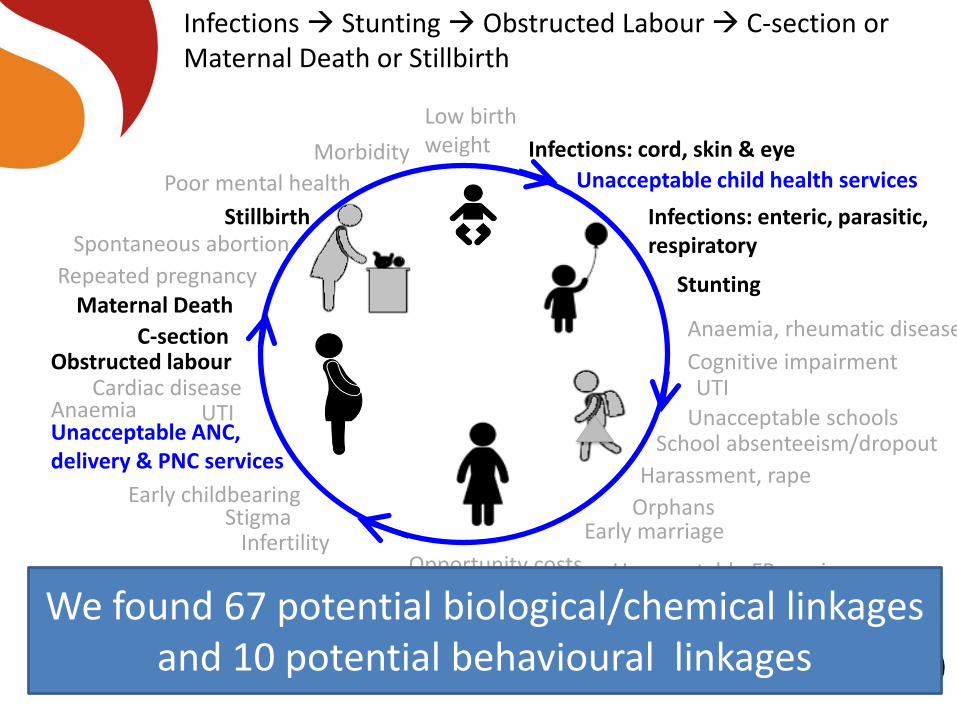
Infections Stunting Obstructed Labour C-section or Maternal Death or Stillbirth
Short adultWe found 67 potential biological/chemical linkages and 10 potential behavioural linkages
Insufficient evidence of impact
Insufficient evidence
Systematic reviews, secondary analyses & new data collection tools and analyses needed!
Supported by:
through the SHARE Research Consortium
The SHARE Research Consortium
generates new findings and
synthesis of existing knowledge on
sanitation and hygiene in order to
improved policy and practice.
shareresearch.org
Thank you
Clean birthing practices: a
mixed-methods observational
study in health care facilities in
Nigeria
Helen Buxton1; Erin Flynn1; Dr Olutunde Yinka2 Joanna EstevesMills1; Tess Shiras1; Stephen Sara2 Oliver Cumming1; Robert Dreibelbis1
1. London School of Hygiene and Tropical Medicine; 2. Maternal and Child Survival Program
Hygiene During Labor and Delivery
• Infection during labor
and delivery
• 10% of all maternal
deaths
• 15% of neonatal deaths
• Easily prevented
through improved
hygiene and infection
prevention and control
protocol
• Improvements proven
difficult
• Organizational barriers
• Environmental barriers
• Models based on
knowledge and
education
Understanding hygiene practices during labor
and delivery
• Childbirth is complex, • Multiple, embedded procedures
• Long duration with intermittent provider interaction
• Assessments tend to focus on binary relationships between hand hygiene practices and specific events• HWWS and glove use prior to vaginal examinations
• Need better methodologies that capture dynamic nature of risk
23
Background: Nigeria
Neonatal mortality rate:
• 34/1,0001
• SDG target: 12/1,000
Maternal mortality:
• 560/100,0002
• SDG target: 70/100,000
1. Liu (2015); 2. World Bank (2015)
Photo credit: Lucia Zoro Save the children
24
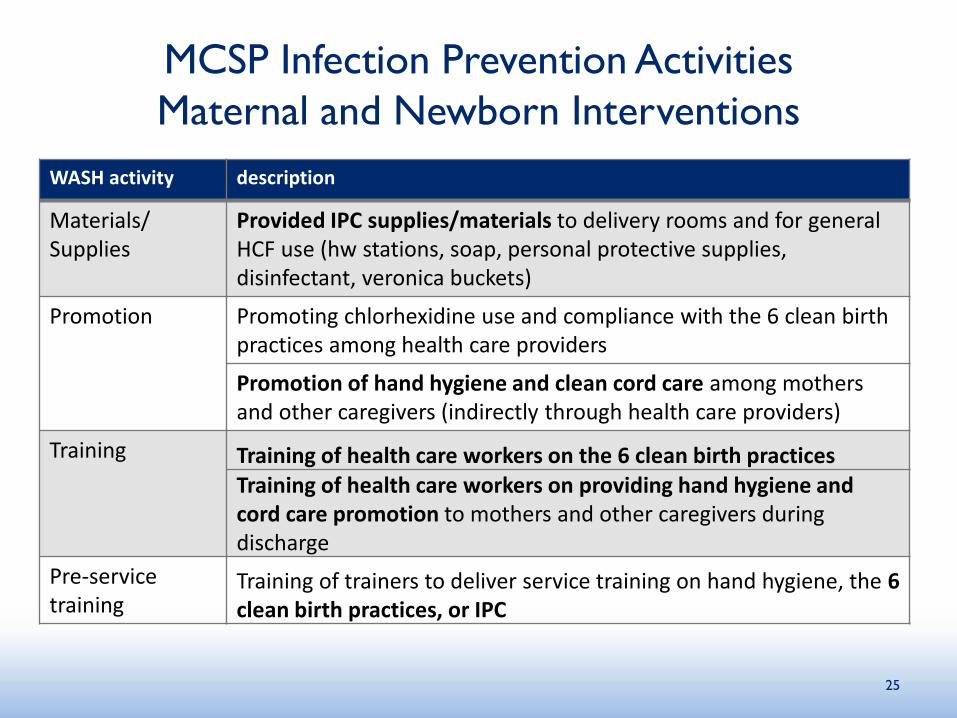
MCSP Infection Prevention Activities
Maternal and Newborn Interventions
WASH activity description
Materials/ Supplies
Provided IPC supplies/materials to delivery rooms and for general HCF use (hw stations, soap, personal protective supplies, disinfectant, veronica buckets)
Promotion Promoting chlorhexidine use and compliance with the 6 clean birth practices among health care providers
Promotion of hand hygiene and clean cord care among mothers and other caregivers (indirectly through health care providers)
Training Training of health care workers on the 6 clean birth practicesTraining of health care workers on providing hand hygiene and cord care promotion to mothers and other caregivers during discharge
Pre-service training
Training of trainers to deliver service training on hand hygiene, the 6 clean birth practices, or IPC
25
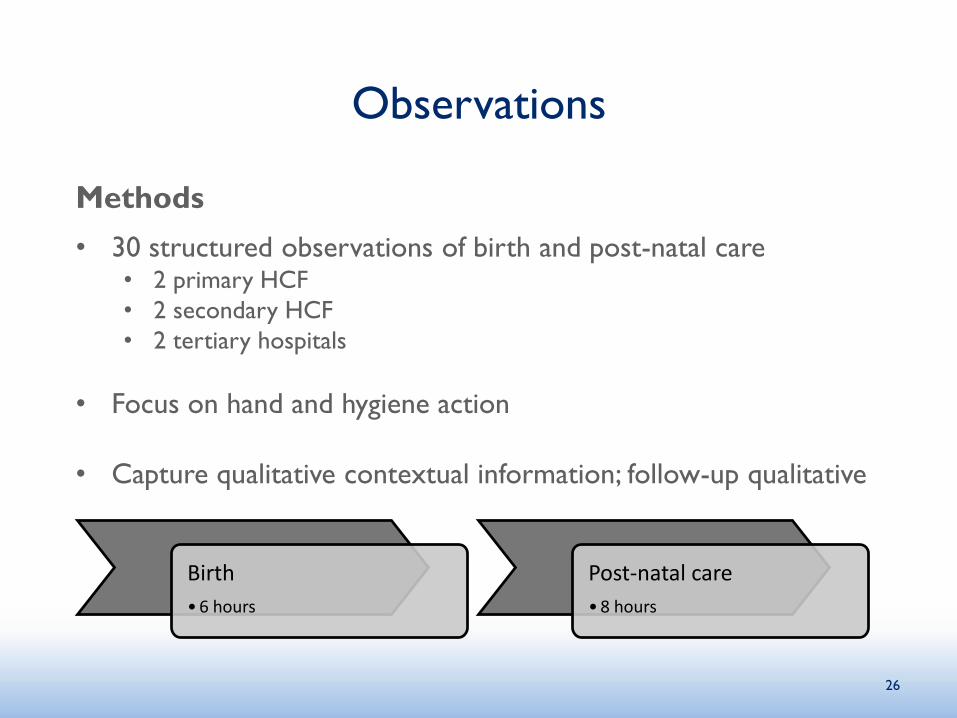
Observations
Methods
• 30 structured observations of birth and post-natal care• 2 primary HCF
• 2 secondary HCF
• 2 tertiary hospitals
• Focus on hand and hygiene action
• Capture qualitative contextual information; follow-up qualitative
26
Birth
•6 hours
Post-natal care
•8 hours
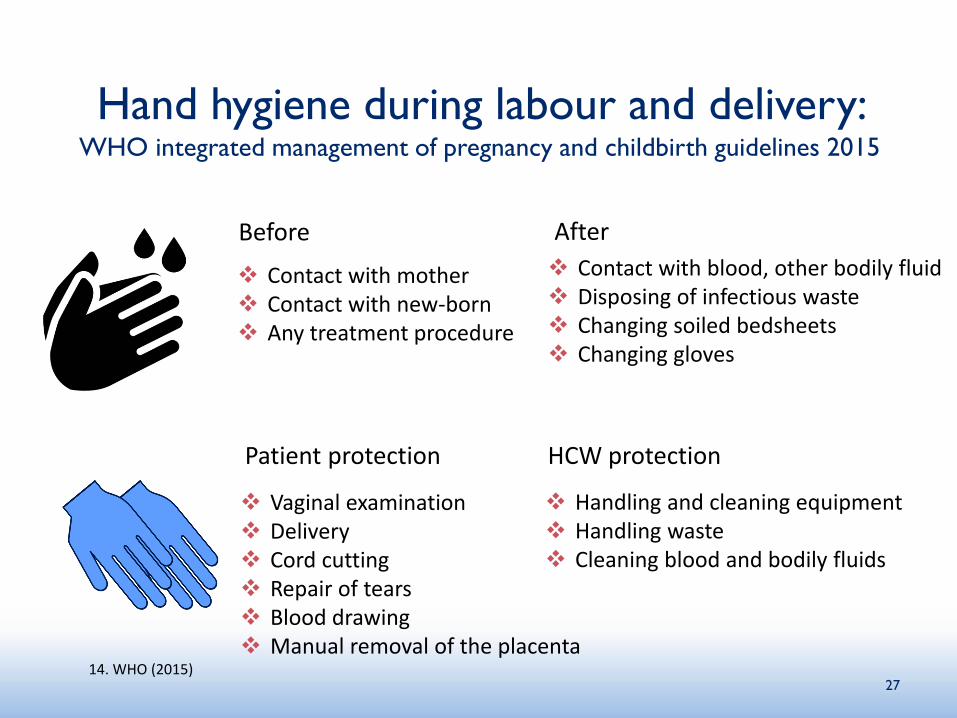
Hand hygiene during labour and delivery: WHO integrated management of pregnancy and childbirth guidelines 2015
Before
14. WHO (2015)
After
Contact with mother Contact with new-born Any treatment procedure
Contact with blood, other bodily fluid Disposing of infectious waste Changing soiled bedsheets Changing gloves
27
Patient protection HCW protection
Vaginal examination Delivery Cord cutting Repair of tears Blood drawing Manual removal of the placenta
Handling and cleaning equipment Handling waste Cleaning blood and bodily fluids
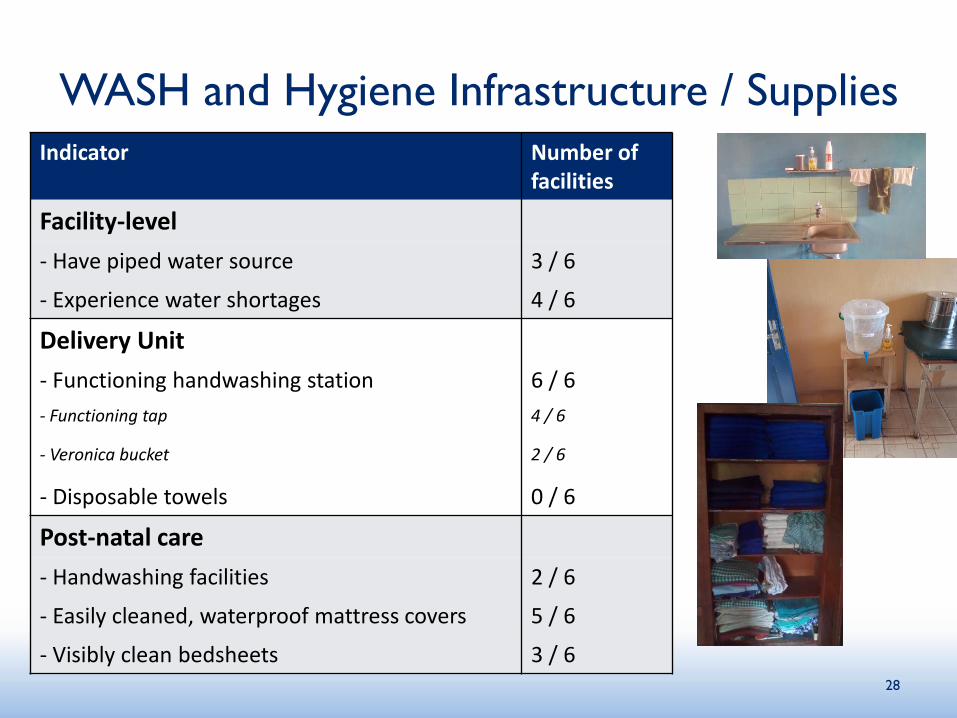
WASH and Hygiene Infrastructure / Supplies
Indicator Number of facilities
Facility-level
- Have piped water source 3 / 6
- Experience water shortages 4 / 6
Delivery Unit
- Functioning handwashing station 6 / 6
- Functioning tap 4 / 6
- Veronica bucket 2 / 6
- Disposable towels 0 / 6
Post-natal care
- Handwashing facilities 2 / 6
- Easily cleaned, waterproof mattress covers 5 / 6
- Visibly clean bedsheets 3 / 628
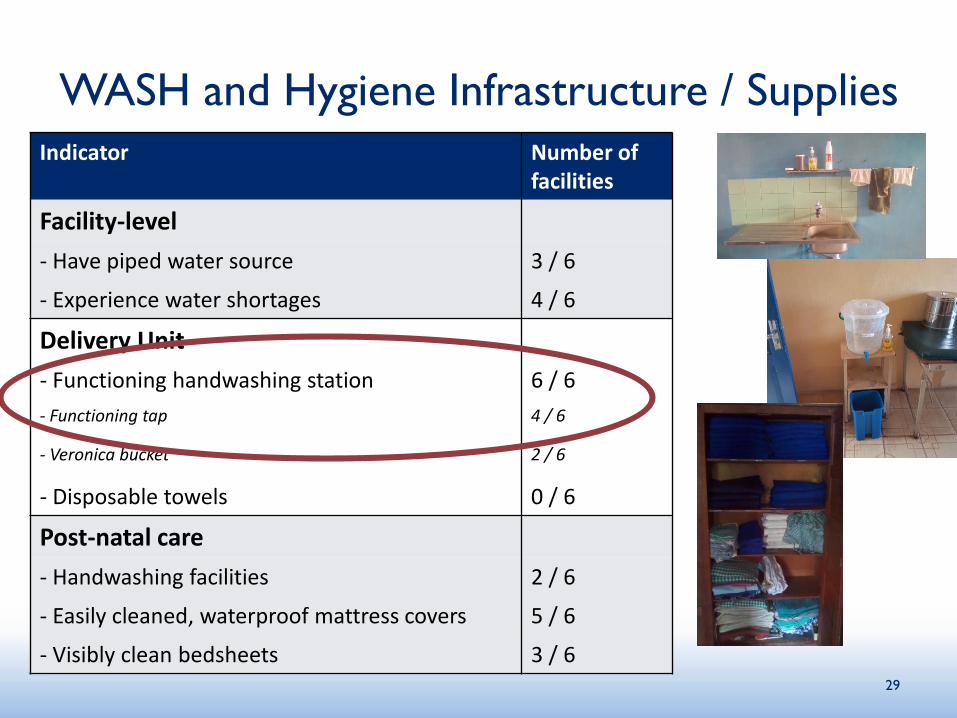
WASH and Hygiene Infrastructure / Supplies
Indicator Number of facilities
Facility-level
- Have piped water source 3 / 6
- Experience water shortages 4 / 6
Delivery Unit
- Functioning handwashing station 6 / 6
- Functioning tap 4 / 6
- Veronica bucket 2 / 6
- Disposable towels 0 / 6
Post-natal care
- Handwashing facilities 2 / 6
- Easily cleaned, waterproof mattress covers 5 / 6
- Visibly clean bedsheets 3 / 629
Hygiene Scoring for HCF Workers
Proper hygiene protocol: Hands washed with soap, gloves worn
Time
30
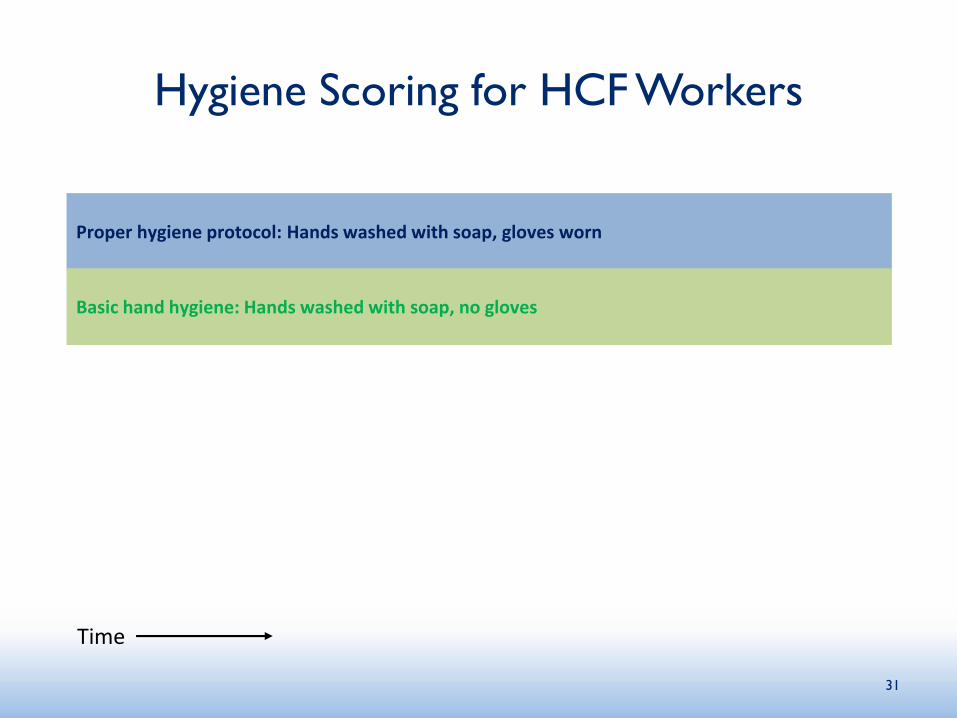
Hygiene Scoring for HCF Workers
Proper hygiene protocol: Hands washed with soap, gloves worn
Time
Basic hand hygiene: Hands washed with soap, no gloves
31
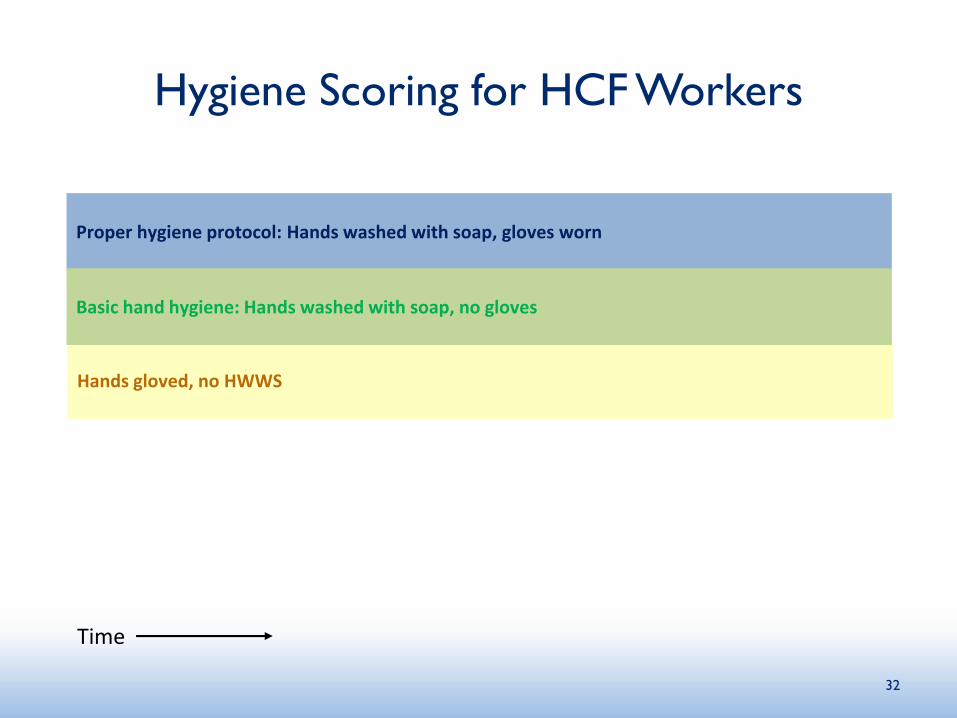
Hygiene Scoring for HCF Workers
Proper hygiene protocol: Hands washed with soap, gloves worn
Hands gloved, no HWWS
Time
Basic hand hygiene: Hands washed with soap, no gloves
32
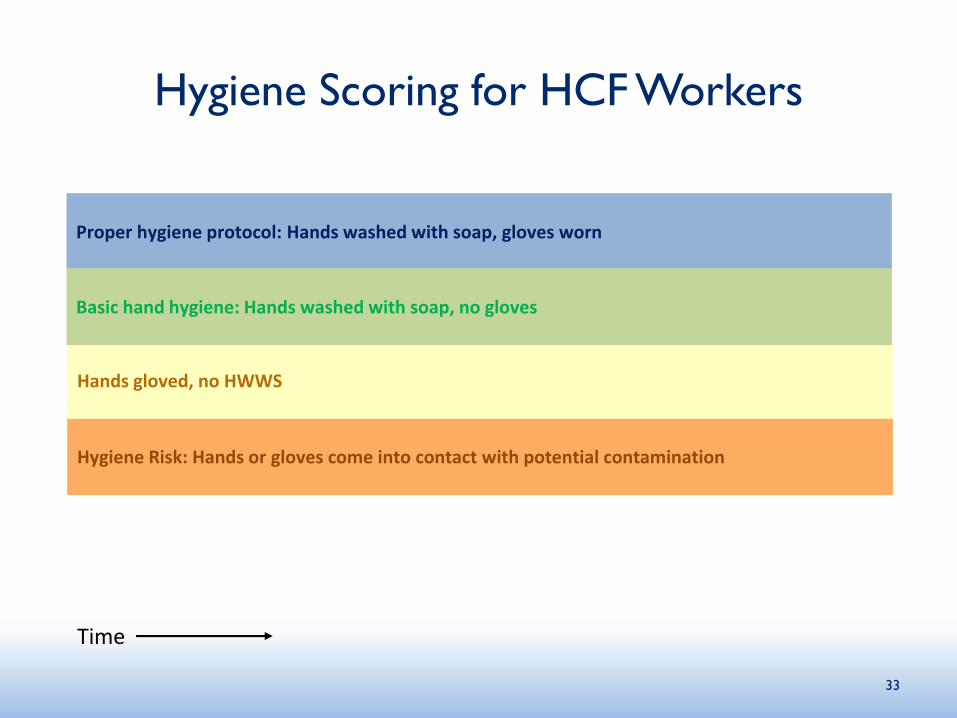
Hygiene Scoring for HCF Workers
Hygiene Risk: Hands or gloves come into contact with potential contamination
Proper hygiene protocol: Hands washed with soap, gloves worn
Hands gloved, no HWWS
Time
Basic hand hygiene: Hands washed with soap, no gloves
33
Hygiene Scoring for HCF Workers
Hygiene Risk: Hands or gloves come into contact with potential contamination
Proper hygiene protocol: Hands washed with soap, gloves worn
Hands gloved, no HWWS
Time
Basic hand hygiene: Hands washed with soap, no gloves
34
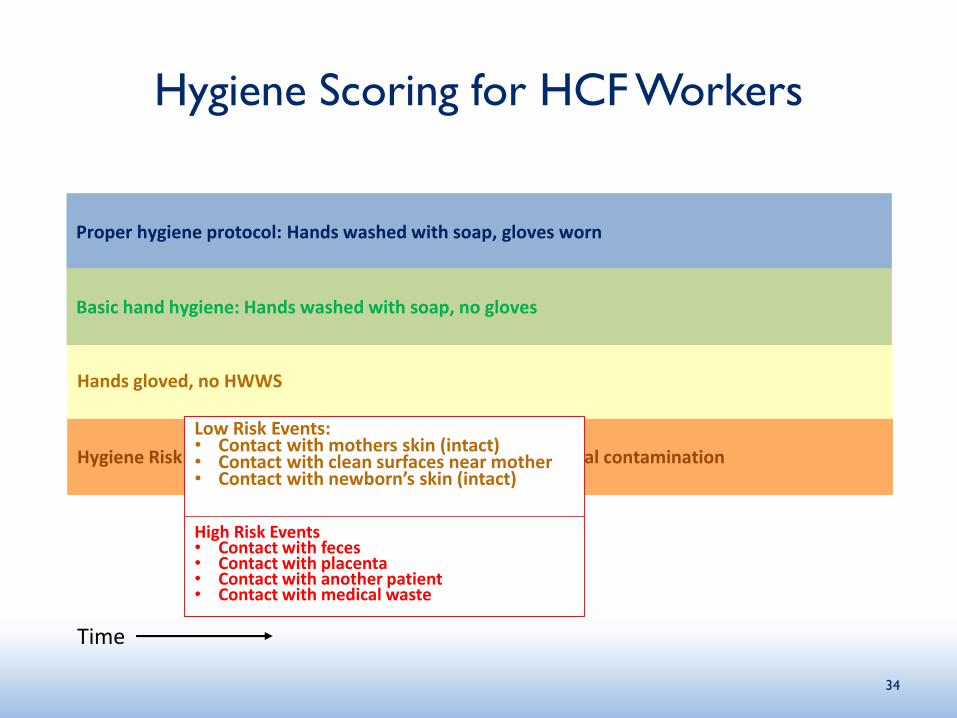
Low Risk Events:• Contact with mothers skin (intact)• Contact with clean surfaces near mother• Contact with newborn’s skin (intact)
High Risk Events• Contact with feces• Contact with placenta• Contact with another patient• Contact with medical waste
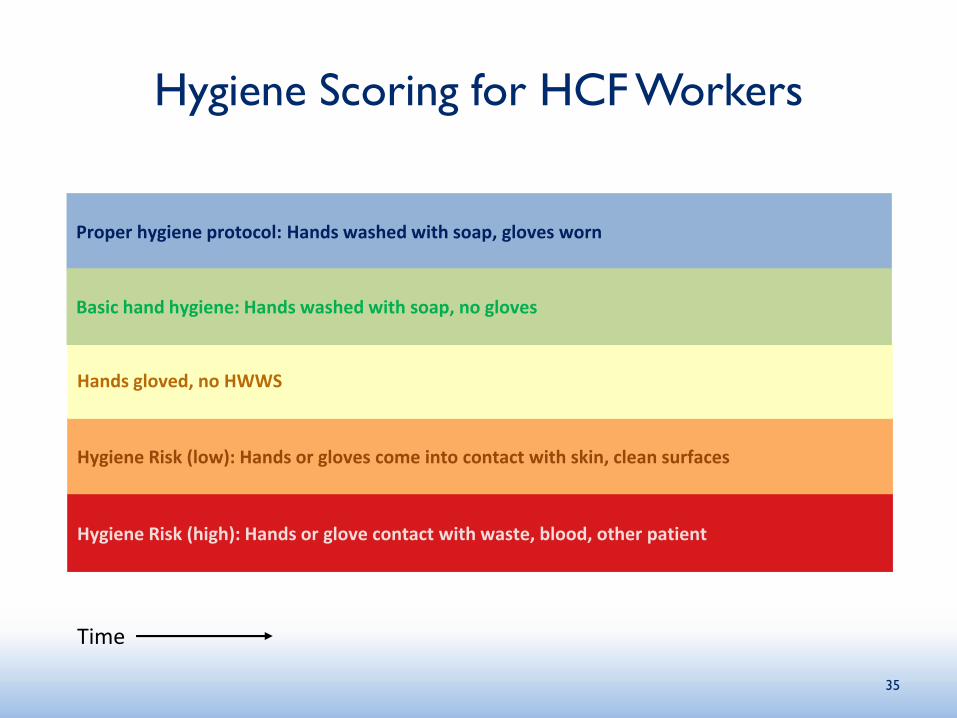
Hygiene Scoring for HCF Workers
Hygiene Risk (low): Hands or gloves come into contact with skin, clean surfaces
Proper hygiene protocol: Hands washed with soap, gloves worn
Hands gloved, no HWWS
Time
Hygiene Risk (high): Hands or glove contact with waste, blood, other patient
Basic hand hygiene: Hands washed with soap, no gloves
35
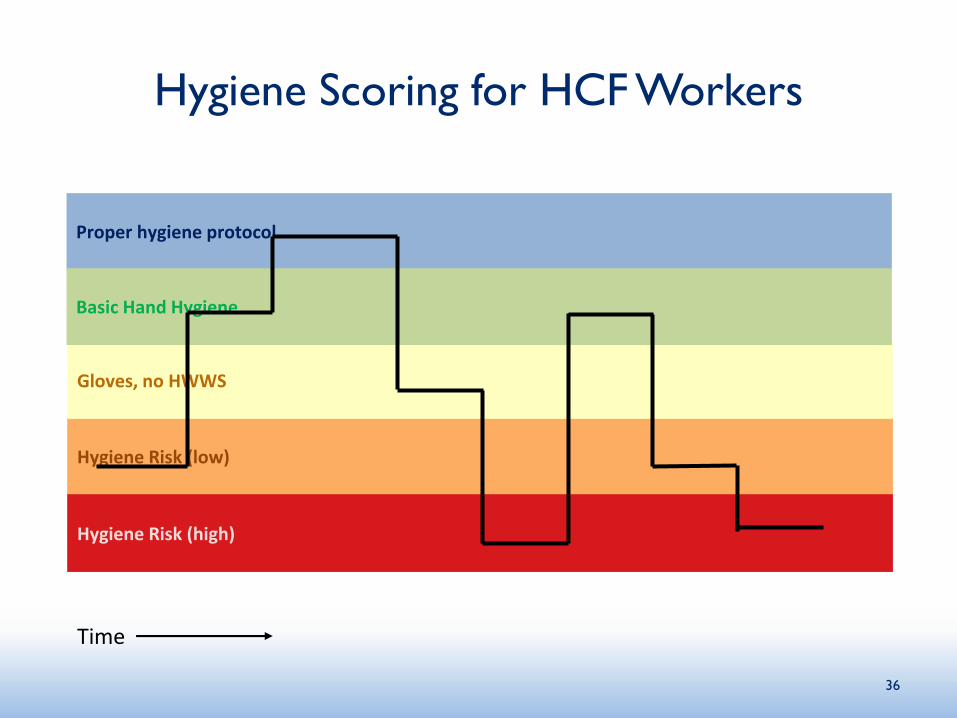
Hygiene Scoring for HCF Workers
Hygiene Risk (low)
Proper hygiene protocol
Gloves, no HWWS
Time
Hygiene Risk (high)
Basic Hand Hygiene
36
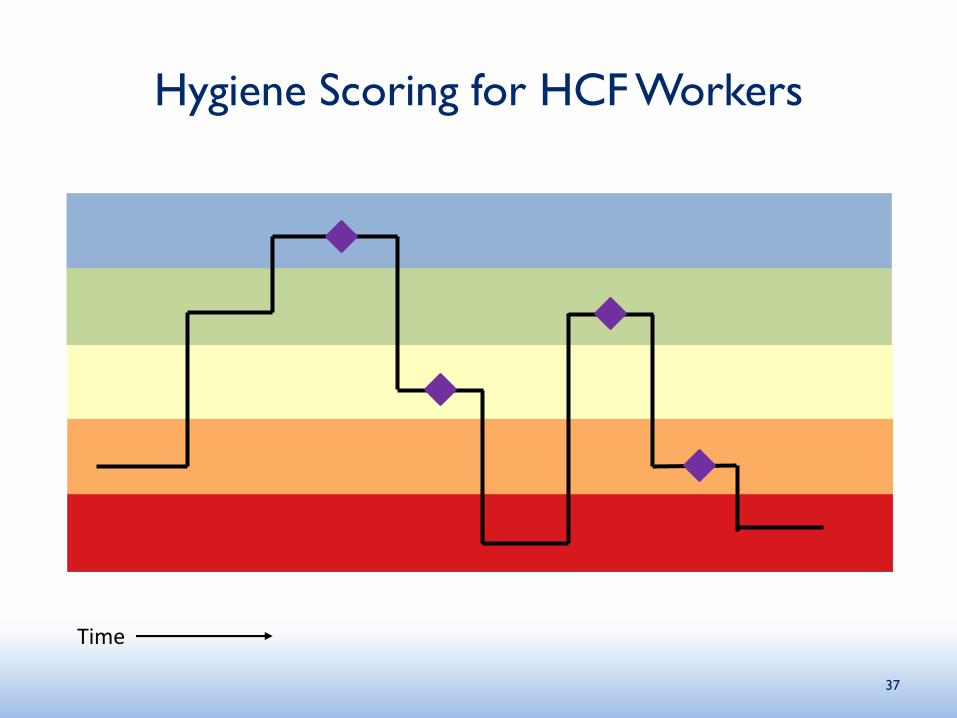
Hygiene Scoring for HCF Workers
Time
37
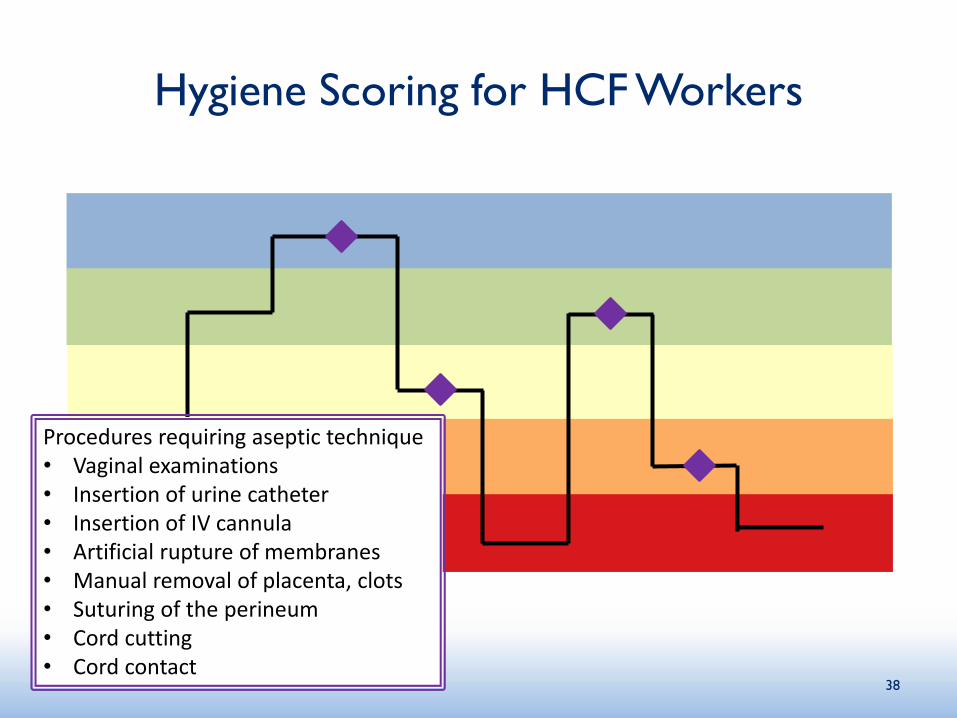
Hygiene Scoring for HCF Workers
Time
38
Procedures requiring aseptic technique• Vaginal examinations• Insertion of urine catheter• Insertion of IV cannula• Artificial rupture of membranes• Manual removal of placenta, clots• Suturing of the perineum• Cord cutting• Cord contact
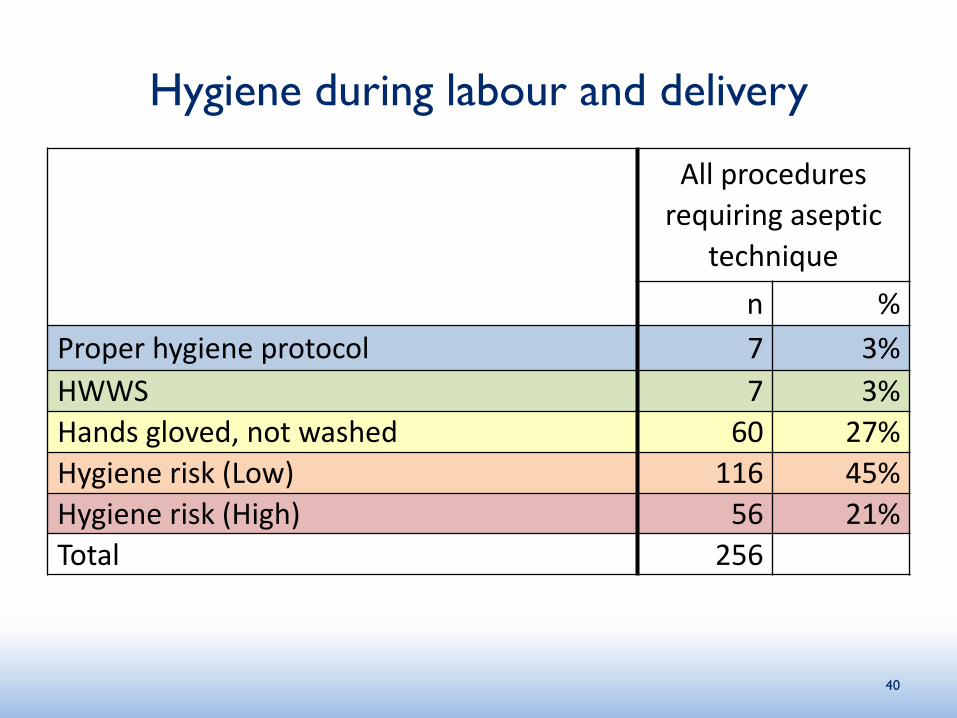
Hygiene during labour and delivery
40
All procedures
requiring aseptic
technique
n %
Proper hygiene protocol 7 3%
HWWS 7 3%
Hands gloved, not washed 60 27%
Hygiene risk (Low) 116 45%
Hygiene risk (High) 56 21%
Total 256
Key Findings
Conveniently placed handwashing infrastructure with both water and soap is necessary but not sufficient to ensure hand hygiene compliance
Glove use being used as a substitute for HWWS
Knowledge around hygiene protocols is high, training only reinforcing knowledge
• Accountability and supervision
• Motivation and ability, particularly during shifts with fewer staff
Visitors and auxiliary staff play a large role in maternal and newborn care
• Largely absent from most IPC training and interventions
• When included, focus on a small set of specific behaviours (ie: cleaning surfaces)
42
Next Steps
MCSP Nigeria developing new training
programs, focusing on supervisory support and
critical moments for handwashing
Integrate findings into larger literature review,
facility observations, and global key informants
43
For more information, please visit
www.mcsprogram.org
This presentation was made possible by the generous support of the American people through the
United States Agency for International Development (USAID), under the terms of the Cooperative
Agreement AID-OAA-A-14-00028. The contents are the responsibility of the authors and do not
necessarily reflect the views of USAID or the United States Government.
facebook.com/MCSPglobal twitter.com/MCSPglobal