Embed Size (px)
Citation preview

3/28/2012
1
Dr Liesl Page-ShippClinician’s Course
East London16 March 2012
The importance of an integrated approach to TB and HIV management
Outline
1. Background2. Research
• Systematic review• TB/HIV integration at PHC
3. How do we do it?
1. BackgroundTB incidence and HIV Prevalence South Africa 1990-2008
WHO Global TB Report http://www.who.int/tb/publications/global_report/2009/en/index.html
HIV drives TB Increases� Lifetime risk from 10%/lifetime to
>10%/year� Promotes progression to active TB� TB recurrence�Mortality 5-8% vs 16-35%�Active TB increases risk of HIV - associated
mortality�During TB treatment�After successful TB treatment
Policy: 2004World HealthOrganization

3/28/2012
2
Research
A. Systematic ReviewB. TB/HIV integration at PHC
A. TB/HIV service integration: a systematic review
Helena Legido-QuigleyCatherine M. MontgomeryPalwasha KhanAde FakoyaHaileyesus GetahunAlison Grant
1st Global Symposium on Health Systems Research
Methods
�Systematic review� low- or middle-income countries� integrated HIV and tuberculosis services�health facility level
� Inclusion: Description of a change to increase TB/HIV integration �133 reports
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
ResultsNumber of reports of different models of integration, by year
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Results: “TB refers” and “HIV refers” Advantages• Easy• Minimal additional resources Disadvantages• Referral may fail esp.
• ineffective referral criteria• referral pathway complex
• Patient costs increased • Potential risks to patient if poor
communicationTB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Results: “ TB “tests & refers”
Advantages• Increases HIV testing• Reduces potential stigma • Reduces unnecessary referrals• Maximise access to ARTDisadvantages• Financial and human resources• Adequate space• Stock-outs of HIV test kits• Referral failure/ costs
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010

3/28/2012
3
Results: “HIV tests & refers”
Advantages• Increases TB case detection • Reduces unnecessary referrals• IPTDisadvantages• Staff training• Sputum collection • All disadvantages of referral-based systems
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Results: “ “Single facility”
• Tuberculosis clinic provides HIV treatment
• HIV clinic provides TB treatment
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Results: “ “Single facility”
Advantages• Cross-fertilisation of expertise & best practice• Rapid diagnosis & treatment of infectious TB
should reduce risk of transmission• Minimises lost referrals• Increase ART uptake among HIV+ TB patients• Lower transport costs• High HIV prevalence
• efficient for providers & patients• most TB patients have HIV, particular gains by
avoiding need for referral
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Results: “ “Single facility”
Disadvantages• Potential high risk of TB transmission if
infection control inadequate• Significant investment to implement
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Barriers to Integration
Service delivery
•Lack of access to care and support•Infection control•Private space for HIV counseling and testing•Data collection systems not designed for
integrated care•Ineffective referral systems
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Barriers to Integration
Human resources
• Lack of staff trained• High staff turnover• In models with additional activities, staff
already overburdened• Staff attitudes
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010

3/28/2012
4
Facilitators of integration
• Bringing staff from two services together e.g.through joint training
• Designated staff member with responsibilityfor integration
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Measurement of effective implementation
Outcome indicator Impact indicator
TB Service Entry% TB patients referred for HIV testing (10)% TB patients with an HIV test result (45)% HIV-positive TB patients starting CPT (17)% HIV-positive starting/continuing ART (25)HIV Service Entry% HIV-positive screened for TB (26)% HIV-positive starting/continuing CPT (11)% HIV-positive starting IPT (8) % HIV-positive diagnosed with TB (5)% referred to TB clinics (4)
TB treatment outcomes (16)Death (6)
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Gap and Gaps in Knowledge
• Measures of effectiveness• Very few direct comparisons between
different models of care• Few measure patient-relevant impacts• No randomised trials
• Cost effectiveness assessment required
• The perspectives of users are rarely reportedTB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
Conclusions
• Many recent reports, diverse models
• Where high HIV prevalence, integrated care likely to serve patients best
• Where lower HIV prevalence, costs vs. benefits of closer integration may differ
• HIV testing in TB services (and vice versa) seems advantageous at any HIV prevalence
TB/HIV service integration: A systematic review. Legido-Quigley H , Montgomery CM, Khan P, Fakoya A, Getahun H,Grant A.1st Global Symposium on Health Systems Research, 2010
2 B. Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa
Liesl Page-Shipp , Yara Voss de Lima, Jacques de Vos, Kate Clouse, Ian M. Sanne , Annelies van Rie
CROI 2010
Methods� Retrospective review� 2 months of activities (Aug to October 2009)� Review 2 months later
� Assess monitoring (documentation) implementation (coverage)
� All available relevant records � TB registers� Clinic files� Electronic HIV database
� 3 Primary Health Care Clinics , Johannesburg
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, de Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.

3/28/2012
5
TB suspects (n=602)
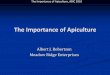
35%
11%7%
29%
18%
TB suspects HIV testing (n=602)
No record of HIVtestingHIV testing offered butrefusedHIV negative
Known HIV positivebefore suspect visitNewly diagnosed HIVinfection
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, de Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.
TB suspects (n=602)
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L, Voss de Lima Y, de Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.
TB patients (n=208)
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, Jde Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.
HCT (n=1104)• 306 (27.7%) HIV positive
• CD4 56.9%• Mean 336 cells/ mm3 (IQR 152, 502)
• TB Symptom screening not routinely recorded
• Only 2 of 306 HIV positive assessed by TB smear
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, Jde Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.
PLWH (n=6157)� 921 (15%) reported more than one
TB symptom
� 73 (7.9%) had diagnostic smear microscopy
� 13 (17.2 %) smear positive
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, De Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.
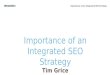
PLWH: Patients on ART (n=848)
59
16
12
8
5
0 10 20 30 40 50 60 70
Cough
Night sweats
Weight loss
Lymphadenopathy
Fever
Percentage of total TB symptoms reported
Figure 3: ART patients: TB symptoms reported (n=848)
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, Jde Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.

3/28/2012
6
Other collaborative activities
Very poorly documented/ not done
�Prevention messaging�CPT� IPT �ART
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, De Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.
Conclusion� TB/HIV documentation poor: > 30% of client
information missing for any indicator
� Coverage highest for HIV testing
� TB suspects (54%)
� TB patients (66%)
� Coverage lowest
� TB case finding among VCT clients (<1%)
� People receiving HIV care (8%)
� A vast number of missed opportunities for TB/HIV control were demonstrated
Successes and Missed Opportunities in TB/HIV collaborative activities at Primary Health Care Clinics in Johannesburg, South Africa. Page-Shipp L , Voss de Lima Y, De Vos J, Clouse K, Sanne I ,van Rie A. CROI 2010.
3. TB/HIV integration in South Africa
How, when , where?
OutlineA. Integration vs collaborationB. ObjectivesC. PrinciplesD. LogisticsE. Clinic flowF. Monitoring and evaluation
A. Integration vs collaboration
A practical guide for TB and HIV service integration at PHC facilities. SA DOH, 2011
B. Overall Objectives of TB/HIV integration� Decrease TB and HIV transmission� Decrease morbidity and morality� TB�HIV�Other HIV-related illnesses� Improve healthcare service efficiency� Patient centred approach� Efficient� Cost saving

3/28/2012
7
Specific objectives � Prevention� IPT� Infection control� PMTCT
� Intensified case finding� Smear negative/ EPTB�HIV ART
� Care� Cotrimoxazole
� Adherence support� Follow up
Specific objectives cont.
�Save time: Patient and HCW�Retrieving different files�Directing patients�Managing patient expectations�Dispense all meds at one time�Follow up
Principles
1. One-stop-shop �Including ANC/PMTCT
2. Quality service�HCW trained, competent, confident�On-site mentoring�“Demystify”
Road map to TB/ HIV service provision
A practical guide for TB and HIV service integration at PHC facilities. SA DOH, 2011
3. Task Shifting 4. Increased efficiency, decreased workload
� Decrease duplication�Administrative and clinical
� Decrease hospitalisation� Integrated data collection

3/28/2012
8
5.Community-based carePrimary Health Care reengineeringDECENTRALISE� Community Health Workers� BOTH TB and HIV� Prevention� Case-finding� Defaulter tracing� Mother and child health� NCD
6. Team approach� Roving ART team with a doctor� Site visits� Staff swop to share experience� Regional “specialist” days� Telephonic consultation� “on call” roster from local hospital
� Journal club/ in-service training
7. TB Infection Control�Commonly quoted as reason not to
integrate services
BUT
�Needed to practise infection control everywhere�Awareness is half the battle won!!
D. Logistics�Goal�All services in one consultation�TB infection control� Structure�Air flow rate and direction �Waiting areas
�Manage appointments!
E. Clinic flow� Cough screen at entry� Separate suspects and early TB treatment�Fast queue for sputum results� Pharmacy- outside window
� HIV testing and Pre-ART area� TB screening, IPT, CMX�Every clinic delivery area�PMTCT/ Infant PCR at ANC�TB area
Clinic flow cont.� TB/ART area�TB �Diagnosis�Drug dispensing�Records�HIV testing�ART� Initiation, management�Screening for TB�Records

3/28/2012
9
F. Monitoring and evaluation�Staple together the patient held cards�One clinic record�One data collection area�TB and ART next to each other�Sharing of records
Acknowledgements�Helena Legido-Quigley�Alison Grant�Kerrigan McCarthy�Annelies van Rie�Staff and patients at PHC
Questions? 1. TB/HIV collaboration
A. Is the ideal solution in high HIV prevalence situations
B. Implies Vertical TB and HIV programmesC. Does not include clear referral systemsD. Only occurs at PHC level
2. HIV increases theA. Length of TB treatment requiredB. Time to develop TBC. Risk of TB from 10% / lifetime to 10% every
10 yearsD. Mortality from TB in patients even after TB
has been treated
3. TB Infection controlA. Must be ideal before TB/HIV integration
activities can beginB. Relies on personal protective equipmentC. Patients must sit in a way that air is
directed away from them and towards the staff
D. Can be improved by simple activities in any facility

3/28/2012
10
4. Patients controlled on ARTA. Have the same risk of TB as HIV
negative patientsB. Do not need to be screened for TB
symptomsC. Should be seen by PHCNsD. No longer benefit from TB/HIV
integration activities
5. Barriers to TB/HIV integration includeA. Only nurses and doctors in the clinic can
influence TB/HIV integration activitiesB. Duplicate data collection systemsC. TB symptom screen must be done by a
nurse or doctorD. Only doctors can initiate IPT
Thank you