-
1
Department of Pharmaceutics School of Pharmacy University of
Washington Seattle, WA
http://sop.washington.edu/department-of-pharmaceutics/faculty-members/
Jashvant (Jash) D. Unadkat, Ph.D.
NEDMDG
The Importance of Concept of Fraction of Drug Transported (ft)
in Understanding and
Predicting Drug Disposition and DDI
-
NEDMDG 2
Tissue/Membrane Localization of Drug Transporters
?
Unadkat JD, Enzyme-and Transporter-Based Drug-Drug Interactions:
2010.
?
OATP1B1
OATP1B3
MATE1
NTCPOCT1
UrinePEPT
1,2 OAT4
MATE1,2
OCTN1,2
OAT1,3
OATP4C1 OCT2
Kidney
BBB
Brain Interstitial Space
Blood
P-gp BCRP
Cerebrospinal Fluid
BCSFB
Fetal blood
MRP 1,2,4,5BCRPP-gp
MRP 1,4
MRP 1,3,4,5,6
P-gpBCRP
MRP2MRP2,4
BCRPP-gp
P-gpBCRPMRP2
MRP2Liver BCRP BSEPP-gp
OATP2B1
OATP1A2
OATP3A1
OAT3
MRP1,3,5
MRP1,3,5,6
Bile
2B1
/2B1
-
NEDMDG 3
When a significant fraction of the drug dose is absorbed,
distributed into an eliminating or non-eliminating tissue, or
cleared from the body via transporters (i.e. ft is large)
Modulation of the transporter(s) by DDI or SNPs will NOT affect
exposure of the tissue to the drug (i.e. AUC) if the drug is
cleared primarily through that organ/tissue. However the Cmax and
Cmin in the tissue will be affected. NOT significantly affect the
systemic CL of the drug If the fraction of the dose distributing
into a tissue via a transporter is small But, will have a profound
impact on the tissue concentration and therefore potentially the
toxicity and efficacy of the drug – disconnect between the plasma
and tissue conc.
ft will determine the impact of transporter DDI or SNPs on
systemic or tissue conc. of drugs
When are Transporters Relevant to ADME?
-
NEDMDG 4
When a new molecular entity is found to be a substrate of a
transporter, consider the following : Is the transporter(s) present
in the tissue of interest? If so, what is its contribution relative
to CLdiffusion and CLother transporters? In vitro transport ≠ in
vivo relevance because transfected cell lines (or X. oocytes) often
exaggerate ft due to high expression of the transporter A substrate
can be a potent inhibitor of a transporter without being a
substrate Even if the affinity of the substrate for the transporter
is low and the expression of the transporter in the tissue of
interest is low, that transporter could still be important in
determining the clearance and/or tissue conc. of the drug if ft via
that transporter is large. ft is king!
Some Principles
-
NEDMDG 5
I.V. or S.C.
Oral Dose
Brain
Blood
Proximal Tubule
Renal Artery
Blood
Maternal Blood
Syncytiotrophoblast
Urinary Excretion
Liver
Gut Wall
Gut Lumen
Fecal Excretion
Bile Duct
Portal Vein
Endres et al., Eur J. Pharm. Sci., 2005
Illustration of these Principles Via a Magic School Bus Tour
Through the Body
-
Intestinal Transport
NEDMDG 6
?
OATP1B1
OATP1B3
MATE1
NTCPOCT1
UrinePEPT
1,2 OAT4
MATE1,2
OCTN1,2
OAT1,3
OATP4C1 OCT2
Kidney
BBB
Brain Interstitial Space
Blood
P-gp BCRP
Cerebrospinal Fluid
BCSFB
Fetal blood
MRP 1,2,4,5BCRPP-gp
MRP 1,4
MRP 1,3,4,5,6
P-gpBCRP
MRP2MRP2,4
BCRPP-gp
P-gpBCRPMRP2
MRP2Liver BCRP BSEPP-gp
OATP2B1
OATP1A2
OATP3A1
OAT3
MRP1,3,5
MRP1,3,5,6
Bile
2B1
/2B1
Unadkat JD, Enzyme-and Transporter-Based Drug-Drug Interactions:
2010.
-
NEDMDG 7 PCEUT527
Absorption : Transport can be Rate-limiting Step(s) in
Bioavailability of Drugs
fraction absorbed (fa) via transporters >> fraction
absorbed (fa) via passive diffusion (BDDCS class 3 & 4)
Benet, J Pharm Sci, 2012
[D]
Intestinal Lumen BloodEnterocyte
[D]
[D]
[D]
[D]
[D]
X
[D] [D]X[D]
[M]
[M]
[M]
dual rate-limiting steps for class 3 & 4 drugs – apical and
basal membrane
-
NEDMDG 8
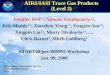
Concentrative Nucleoside Transporter 2 Limits the Intestinal
Absorption of Ribavirin (ft=~0.8)
Moss et al., Mol. Pharm. 2012
Na+
-Na+
Vectorial Transport
Ribavirin CNT2
ENT1
-
NEDMDG 9
Ribavirin Concentration in Intestinal Tissue of mEnt1(-/-) and
Wild Type Mice
20 uM 200 uM 5 mM
Rib
av
irin
Co
nc
en
tra
tio
n (µ
M)
Do
se N
orm
aliz
ed
to
20
µM
0.000.050.100.150.200.250.300.35
1.00
2.00
3.00
4.00
5.00
6.00
Wild Type mEnt1(-/-)
**
***
*** **
***
Equilibrative Nucleoside Transporter 1 (ENT1) Limits the Egress
of Ribavirin from the Intestine to the Blood
Moss et al., Mol. Pharm. 2012
-
Green Tea-Nadolol DDI – OATP1A2?
NEDMDG 10
AUC 85%
Misaka Clin Pharmacol Ther. 2014 Apr;95(4):432-8.
OATP1A2?
[D]
Intestinal Lumen Blood Enterocyte
[D] [D]
-
NEDMDG 11
Nadolol is transported by OATP1A2 but not by OATP2B1
OATP1A2 HEK293 cells
-
NEDMDG 12
Drozdzik et al., Mol Pharm. 2014 Oct 6;11(10):3547-55
But, OATP1A2 mRNA or protein was not detected in human
intestinal tissue! This DDI must be due to some other
mechanism(s)
For IVIVE and mechanism of DDI, important to ask if the
transporter is PRESENT in the tissue of interest
-
NEDMDG 13
When a drug is found, in vitro, to be a substrate of a
transporter, ask: Is the transporter present in the tissue of
interest? What is the contribution of this transporter relative to
diffusion or other transporters, i.e. what is ft for each
transporter? In specialized cells (e.g. enterocytes), transporters
can pose dual rate-limiting steps (apical and basal) in
bioavailability or clearance of drugs Inhibition of efflux
transporters (e.g. at the basal membrane) can profoundly increase
the local tissue conc. and therefore potential toxicity of the
drug
Summary
-
NEDMDG 14
Tissue/Membrane Localization of Drug Transporters
?
Unadkat JD, Enzyme-and Transporter-Based Drug-Drug Interactions:
2010.
?
OATP1B1
OATP1B3
MATE1
NTCPOCT1
UrinePEPT
1,2 OAT4
MATE1,2
OCTN1,2
OAT1,3
OATP4C1 OCT2
Kidney
BBB
Brain Interstitial Space
Blood
P-gp BCRP
Cerebrospinal Fluid
BCSFB
Fetal blood
MRP 1,2,4,5BCRPP-gp
MRP 1,4
MRP 1,3,4,5,6
P-gpBCRP
MRP2MRP2,4
BCRPP-gp
P-gpBCRPMRP2
MRP2Liver BCRP BSEPP-gp
OATP2B1
OATP1A2
OATP3A1
OAT3
MRP1,3,5
MRP1,3,5,6
Bile
2B1
/2B1
-
• Parallel Routes of Elimination • Metabolic (CLint)
• Canalicular Efflux (CLcef)
• Bi-Directional Hepatic Distribution • Sinusoidal Influx
(CLsin)
• Sinusoidal Efflux (CLsef)
• Diffusion
Bile MATE1
OATP 1B1
OATP 1B3/2B1
NTCP OCT1
Blood
MRP 1,3,4,5,6
MRP2
Liver
BCRP BSEP
P-gp
CYP
Parent Metabolite CLint
CLcef
CLsin/ef
Revisit and Modify Hepatic Clearance Concepts to Include
Transporters
NEDMDG 15
-
Key Assumptions Ignore Transporters or Permeability Limitations
: •The transfer from perfusate to the liver is instantaneous and
not limited by permeability • Unbound drug concentration in the
plasma and the liver are the same
Hepatic Well-Stirred Model
Perrier, D. and Gibaldi, M. ,J. Pharmacol. Exp. Ther., 191
(1974) Wilkinson, G.R and Shand, D.G. Clin Pharmacol Ther. 18
(1975)
int
int
L u
L u
Q f CLCLQ f CL
×=
+QL, Cin
Clint
VR
VL
Reservior
Liver
QL, Cout
NEDMDG 16
-
QL, Cin
Clint
VR
VL
Reservior
Liver
QL, Cout
NEDMDG 17
Modification of the Well Stirred Model to Include
Transporters
Endres et al., Mol Pharm. 2009 6:1756-65
-
( ) ( ) ( )( )( ) ( )( )sefcefLcefsinu
cef
sinu
sef
cefOtherL
cefOther
sinu
CLCLCLQCLCLCLfCLCLCLfCLCLCLCLQCLCLCLCLf
++++
++++++
intint
intintint
When CLother = 0 ( )( ) ( )( )sefcefLcefsinu
cef
sinLu
CLCLCLQCLCLCLfCLCLCLQf
++++
+
intint
int
and when CLsef ≈ 0 or
-
Clsin
Clsef
Dependence of Systemic Clearance on Sinusoidal Permeability of
the Drug
0.1 1 10 100
0.1
1
10
100
When CLsin is low or
-
(In)Dependence of Systemic Clearance (CL) on CLint and CLcef
Clearances
0.1 1 10 100 Clsin
Clsef 0.1
1
10
100
NEDMDG 20
Assumptions: CLother = 0 QL=1 (arbitrary vol/time units); Fp/FL
= 1
When sinusoidal distributional CL is 100-fold QL (=1), then
Clsys is limited by QL . When CLsin is
-
As CLsin ↑, systemic CL ↑, AUC reservoir ↓
BUT AUC liver ↔
As CLint ↑, systemic CL↔,
AUC reservoir ↔, BUT AUC liver ↓
When CLsin is
-
Changes in ALL clearance pathways WILL affect systemic AND
liver
AUC
22
CLother = 0.4; CLint =0.3, Clcef =0
When Clsef is not 0
( )( ) ( )( ) othersefcefLcefsinu
cef
sinLu
sys CLCLCLCLQCLCLCLfCLCLCLQf
CL +++++
+=
intint
int
-
NEDMDG 23 23
Hepatic OATPs limit Systemic CL of Atorvastatin: Rifmapin
DDI
7-fold ↑
2.7-fold ↑
Bile Blood [D] [D]
Met
CYP
Lau et al., 81, 2007
X
-
11C-Rosuvastatin – Rifampin DDI in the Rat
Blood
24
11C-Rosuvastatin blood conc. –time profile
NEDMDG
Bile Blood
[D]
[D]
[M]
Hepatocyte
OATPs
He et al., Mol Pharm. 2014
-
Hepatic Uptake and Biliary Excretion of 11C-Rosuvastatin in the
Rat
Coronal 2 min SUV images of 11C-Rosuvastatin
Mol Pharm., ‘14
Bile Blood
ROS
Hepatocyte
OATPs BCRP/MRP2
-RIF +RIF
25 He et al., Mol Pharm. 2014
NEDMDG
-
26
NEDMDG
-
Blood
+RIF
-RIF
27
11C-Rosuvastatin blood conc. –time profile
AUCR0-15min (AUCRIF/AUCcontrol) ↑ 230%
Liver
11C-Rosuvastatin hepatic conc. –time profile
AUCR0-15min 5% ↑
NEDMDG
11C-Rosuvastatin – Rifampin DDI in the Rat
He et al., Mol Pharm. 2014 OATPs
Bile Blood
ROS
Hepatocyte
BCRP/MRP2
-
NEDMDG 28
Hepatic transporter(s): What is the contribution of the
transporter relative to diffusion or other transporters, i.e. what
is ft for each transporter? If the uptake transport is a
concentrative, it may be the rate-limiting step. Modulation of this
transport (e.g. DDI, SNPs) may profoundly affect the systemic conc.
of the drug. But, the impact on hepatic conc. is likely to be much
smaller because:
• dX/dthepatic uptake = CLuptake remainder x Cp,u and Cp,u is ↑
• If the drug is mostly cleared by hepatic CL, it will eventually
be eliminated by passage through the liver
Inhibition of efflux transporters (e.g. MRP2) can profoundly
increase the hepatic conc. and therefore potential
toxicity/efficacy of the drug
Summary
-
NEDMDG 29
Tissue/Membrane Localization of Drug Transporters
?
Unadkat JD, Enzyme-and Transporter-Based Drug-Drug Interactions:
2010.
?
OATP1B1
OATP1B3
MATE1
NTCPOCT1
UrinePEPT
1,2 OAT4
MATE1,2
OCTN1,2
OAT1,3
OATP4C1 OCT2
Kidney
BBB
Brain Interstitial Space
Blood
P-gp BCRP
Cerebrospinal Fluid
BCSFB
Fetal blood
MRP 1,2,4,5BCRPP-gp
MRP 1,4
MRP 1,3,4,5,6
P-gpBCRP
MRP2MRP2,4
BCRPP-gp
P-gpBCRPMRP2
MRP2Liver BCRP BSEPP-gp
OATP2B1
OATP1A2
OATP3A1
OAT3
MRP1,3,5
MRP1,3,5,6
Bile
2B1
/2B1
-
NEDMDG 30 30
Sasongko et al (2005) Clin Pharmacol Ther. 77:503-514. Muzi et
al J Nucl Med, 2009 Eyal et al., Clin Pharmacol Ther. 2010
P-gp Transport of 11C-verapamil at the Human BBB and Inhibition
by Cyclosporine A (CsA)
11C-verapamil
CsA infusion (2.5 mg/kg/hr) for 60 min
Time
~45 min
15O-water
11C-CO
~45 min 12 min 15 min 15 min
11C-verapamil 15O-water
Continue CsA infusion for ~45 min
-
31
Plasma and Brain 11C-verapamil radioactivity concentration-time
profiles in the absence and
presence of CsA
Time (min)
0 10 20 30 40 50
Plas
ma
11C
-rad
ioac
tivity
/ D
ose
(L-1
)
0.01
0.1
Plasma
- CsA + CsA
Sasongko et al (2005) Clin Pharmacol Ther. 77:503-514.
Time (min)
0 10 20 30 40 50
Bra
in 1
1 C-r
adio
activ
ity /
Dos
e (L
-1)
0.01+ CsA - CsA
Brain
↑~2-fold
NEDMDG
Effect of CsA different than that in rodents: 87% vs. 1000%
-
NEDMDG 32
What is the ft of verapamil? Can the effect of maximal
inhibition of P-gp be discerned from our data?
Cb, cerebellum FC, frontal cortex OC, occipital cortex Pu,
putamen PI, pituitary T, thalamus V, lateral ventricle
A
B C
D E F
T
FC FC FC
OC OC OC
V V
C C
C
Pu Pu
T T CP CP CP
Pi Pi Pi
Cb Cb Cb
V
V V V
B C FC FC FC
C Pu
-CsA +CsA Eyal et al., Clin Pharmacol Ther. 2010
-
NEDMDG 33
Regional 0-10 min brain distribution of [11C]-radioactivity
0.00
0.05
0.10
0.15
0.20
Whi
te m
atte
r
Gre
y m
atte
r
Thal
amus
LT c
orte
x
Fron
tal c
orte
x
Cer
ebel
lum
Occ
ipita
l cor
tex
Par
ieta
l cor
tex
Put
amen
Cau
date
Before cyclosporineDuring cyclosporine
0.0
0.1
0.2
0.3
0.4
0.5
Late
ral t
empo
ral
corte
xLa
tera
l tem
pora
l co
rtex
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
0.00
0.05
0.10
0.15
0.20
Whi
te m
atte
r
Gre
y m
atte
r
Thal
amus
LT c
orte
x
Fron
tal c
orte
x
Cer
ebel
lum
Occ
ipita
l cor
tex
Par
ieta
l cor
tex
Put
amen
Cau
date
Before cyclosporineDuring cyclosporine
0.0
0.1
0.2
0.3
0.4
0.5
Late
ral t
empo
ral
corte
xLa
tera
l tem
pora
l co
rtex
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
Late
ral t
empo
ral
corte
xLa
tera
l tem
pora
l co
rtex
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
K1
of 11
C-r
adio
activ
ity (m
L/m
in/g
)
a
Cho
roid
ple
xus
Pitu
itary
b
b
b
b
a
Eyal et al., Clin Pharmacol Ther. 2010
ATP
ADP + Pi
Brain
Blood
-
NEDMDG 34
ft of [11C]-Verapamil radioactivity is ~0.8 in humans and
macaques
•Based on these data, the MAXIMUM increase (on complete
inhibition of P-gp) in verapamil distribution into the human brain
is predicted to be ~4-5 fold • confirmed by studies in nonhuman
primates, the macaque
Eyal et al., Clin Pharmacol Ther. 2010
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0.0
0.1
0.2
0.3
0.4
0.5
Whi
te m
atte
r
Gre
y m
atte
r
Thal
amus
LT c
orte
x
Fron
tal c
orte
x
Cer
ebel
lum
Occ
ipita
l cor
tex
Par
ieta
l cor
tex
Put
amen
Cau
date
Before cyclosporineDuring cyclosporine
Ext
ract
ion
ratio
Pitu
itary
Cho
roid
ple
xus
Late
ral t
empo
ral
corte
x
a
bb
bb
a
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0.0
0.1
0.2
0.3
0.4
0.5
Whi
te m
atte
r
Gre
y m
atte
r
Thal
amus
LT c
orte
x
Fron
tal c
orte
x
Cer
ebel
lum
Occ
ipita
l cor
tex
Par
ieta
l cor
tex
Put
amen
Cau
date
Before cyclosporineDuring cyclosporine
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
0.0
0.1
0.2
0.3
0.4
0.5
Whi
te m
atte
r
Gre
y m
atte
r
Thal
amus
LT c
orte
x
Fron
tal c
orte
x
Cer
ebel
lum
Occ
ipita
l cor
tex
Par
ieta
l cor
tex
Put
amen
Cau
date
Before cyclosporineDuring cyclosporine
Ext
ract
ion
ratio
Pitu
itary
Cho
roid
ple
xus
Late
ral t
empo
ral
corte
x
a
bb
bb
a
Ext
ract
ion
ratio
Pitu
itary
Cho
roid
ple
xus
Late
ral t
empo
ral
corte
x
a
bb
bb
a
Human
Ke et al., J Nucl. Med. 2013
CsA concentration (µM)
0 5 10 15 20 25 30
Per
cent
incr
ease
in E
R
0
100
200
300
400
500
600Macaque
-
NEDMDG 35
Substrates Brain to Blood Ratio mdr1(-/)/mdr1(+/+) ft(P-gp)
Nelfinavir 40 Very High (~ 0.975)
Verapamil 9.5 High
(~ 0.9)
Cetirizine (Zyrtec®) 2.3 Intermediate
(~ 0.6)
ft and P-gp DDI at the Mouse BBB
-
NEDMDG 36
Magnitude of P-gp based DDI at the
Human BBB Depends on f t(P-gp)
of the P-gp substrate
Hsiao et al., Mol. Pharm. 2014
-
NEDMDG 37
ft and apparent P-gp/BCRP synergism
Blood
Brain Interstitial Fluid
Brain Endothelial Cell P-gp BCRP
CLpgp CLbcrp CLdif
Diffusion
All values are for unbound drug and are arbitrary
ft = 0.95 due to efflux by P-gp and BCRP ftP-gp = 0.475, ftBCRP
= 0.475 ftdif= 0.05
• Cssb/Cssp= CLdif/CLefflux = 0.05 • when CLPgp=0, Cssb/Cssp=
0.095 • when CLBCRP=0, Cssb/Cssp = 0.095 ~ 2-fold ↑ when
CLPgp+CLBCRP=0, Cssb/Cssp = 1 (~20-fold ↑)
-
NEDMDG 38
BBB transporter(s): For high ft drugs (>0.9, via P-gp, BCRP
or both), there is
potential for inadvertent DDI at the human BBB to be clinically
significant if these drugs have a narrow therapeutic window
• Dual inhibition of both P-gp and BCRP could result in a
profound increase in brain conc. – but its not synergism, its just
ft!
• To estimate the maximum liability for P-gp-based drug
interactions that a NME will produce (perpetrator), I propose that
rodent studies be conducted with nelfinavir as the substrate and
the NME as the inhibitor.
• To estimate the maximum liability for P-gp based drug
interactions that a NME will be subjected to (i.e. victim), I
propose that the ft(P-gp) of the NME be determined in rodents.
Then, the maximum DDI be computed.
Summary
-
NEDMDG 39
When a significant fraction of the drug dose is absorbed,
distributed into an eliminating or non-eliminating tissue, or
cleared from the body via transporters (i.e. ft is large) If the
fraction of the dose distributing into a tissue via a transporter
is small, modulation (e.g. DDI) of this transporter by DDI or SNPs
will NOT significantly affect the systemic CL of the drug BUT, if
the drug is cleared primarily through that organ/tissue, the AUC in
the tissue will not be affected, but the Cmax will be if the drug
is NOT cleared primarily through that organ, it will have a
profound impact on the tissue concentration and therefore
potentially the toxicity and efficacy of the drug – disconnect
between the plasma and tissue conc.
ft will determine the impact of transporter DDI or SNPs on
systemic or tissue conc. of drugs
Transporters can serve dual rate-limiting step in the absorption
or clearance of drugs
.
Overall Summary: When are Transporters Relevant to ADME?
-
NEDMDG 40
Use primary cells and selective inhibitors But primary cells are
not available for many organs (e.g. BBB or intestine) Alternative
approach is to use quantitative proteomics and transfected cell
lines .
How Does One Determine ft?
ATP ADP + Pi
• Goal is to quantify the expression of transporters (and
interindividual variability) in various human tissues using
LC/MS/MS
• Funded by a consortium: Merck & Co, Genentech, Biogen Idec
(and Astra Zeneca)
•
http://sop.washington.edu/department-of-pharmaceutics/research-affiliate-program-on-transporters-uwrapt/
University of Washington Research Affiliate Program on
Transporters
-
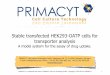
ATP ADP + Pi
Relative Transporter Abundance Pie Chart
41 Li et al. DMD 2015 NEDMDG
-
ATP ADP + Pi
Transporter Expression in Human Intestines
ABCB18% ABCC2 10%
ABCC3 7%ABCG2 4%
ASBT 6%OCT1
8%
OCT31%
OATP2B16%
PEPT1 50%
ABCB15%
ABCC2 25%
ABCC3 36%ABCG2 3%
OCT1 12%
OCT3 2%OATP2B1
12%
PEPT15%
small intestine colon
Relative contribution
42
OATP1A2 could not be detected in the small intestine
N=6, 5 males, 1 female;
NEDMDG
-
Bhagwat Prasad Anand Deo
43
YuYang Jiake He
Major Contributors
Vineet Kumar Gabriela Patilea Chris Endres and Aaron Moss
Li Wang
NEDMDG
-
44
Peng Hsiao Huixia Zhang Anita
Mathias Li Liu
Brain Kirby Alice Ke
Aaron Moss Dale Whittington
Mary Blonski Andrew Bostrom
Christina Shadle
Eun Woo Lee Raj
Govindarajan Francisco Chung
Joseph Zolnerciks
VaishaliDixit Amal Kaddoumi
Anshul Gupta Yurong
Lai
Sara Eyal Suresh Naraharisett
Xiaohui Wu Alexandra Vulpanovici
Andrei Mikheev
Alexander Odinecs
Lucy Sasongko
Unadkat Team
Chris Endres NEDMDG
Jiake He, Bhagwat Prasad, Vineet Kumar, Gabriela Patelia
44
-
NEDMDG 45
Other Collaborators Dept. of Radiology: Jeanne Link, David
Mankoff, Todd Richards, Janet Eary, Satoshi Minoshima, Ken
Maravilla, Mark Muzi, Steve Shoner and the PET suite team Dept. of
Medicine: Ann Collier and her team Dept. of Psychiatry: Soo Borson
& Mary Lessig Dept. of Anesthesiology: Karen Domino
Acknowledgement: NIH MH63641, P50 HD44404, RR 00166, HD47892,
AG031485, RC1NS068904
-
Univ. of WA Health Sciences
NEDMDG 46
Slide Number 1Tissue/Membrane Localization of Drug
TransportersSlide Number 3Slide Number 4Slide Number 5 Intestinal
TransportAbsorption : Transport can be Rate-limiting Step(s) in
Bioavailability of DrugsSlide Number 8Slide Number 9Green
Tea-Nadolol DDI – OATP1A2?Slide Number 11Slide Number 12Slide
Number 13Tissue/Membrane Localization of Drug TransportersRevisit
and Modify Hepatic Clearance Concepts to Include
TransportersHepatic Well-Stirred Model�Modification of the Well
Stirred Model to Include TransportersModified Clearance Concepts
Slide Number 19Slide Number 20�As CLsin ↑, systemic CL ↑, AUC
reservoir ↓ BUT�AUC liver ↔��As CLint ↑, systemic CL↔, �AUC
reservoir ↔, BUT AUC liver ↓Changes in ALL clearance pathways WILL
affect systemic AND liver AUCHepatic OATPs limit Systemic CL of
Atorvastatin: Rifmapin DDI �Slide Number 24Hepatic Uptake and
Biliary Excretion of 11C-Rosuvastatin in the RatSlide Number
26Slide Number 27Slide Number 28Tissue/Membrane Localization of
Drug TransportersSlide Number 30Slide Number 31Slide Number 32Slide
Number 33Slide Number 34Slide Number 35Slide Number 36ft and
apparent P-gp/BCRP synergismSlide Number 38Slide Number 39Slide
Number 40Relative Transporter Abundance Pie ChartSlide Number
42Slide Number 43Slide Number 44Slide Number 45Univ. of WA Health
Sciences