Embed Size (px)
Citation preview
The International Pharmaceutical Aerosol Consortium (IPAC) is an associa-
tion of companies which manufacture products for treating respiratory dis-
eases, including metered dose inhalers (MDIs). One of IPAC’s purposes is to
ensure that the vital role of the MDI is fully appreciated and accounted for in the imple-
mentation of the Montreal Protocol on Substances that Deplete the Ozone Layer and the
United Nations Framework Convention on Climate Change. The members of IPAC that
sponsored this Paper are AstraZeneca; Boehringer Ingelheim Pharmaceuticals, Inc.; Chiesi
Farmaceutici; Glaxo Wellcome; Norton Healthcare Ltd.; Rhône-Poulenc Rorer Inc.; and
3M Pharmaceuticals.
In October 1995, I PAC established an Ad v i s o ry Panel on HFC MDIs. The Panel was
charged with the pre p a ra t i on of a document that would explain the vital role of the HFC
M D I . The first edition of this Pa p e r, published in Ap ril 1997, was the result of the
Pa n e l’s effort . The Chairmen of the Panel were Dr. Wi lliam Gore and Dr. Ian Ta n s ey.
Dr. G o re is the Director of An a lyt i cal Sciences at Boehringer Ingelheim Ph a rm a c e u t i ca l s ,
I n c . Dr. Ta n s ey, n ow re t i re d , was Senior Te ch n i cal Manager at 3M Health Care Ltd.
Other members of the Ad v i s o ry Panel were Dr. Joel Se q u e i ra , Senior Associate Dire c t o r,
S ch e ri n g - Plough Research Institute; Dr. A a ron Ta u b, C on s u l t a n t , R h ô n e - Poulenc Rore r
I n c . ; and Mr. An t h ony Tayl o r, Senior Project Team Le a d e r, I n h a l a t i on Pro d u c t
D eve l o pm e n t , G l a xo We ll c om e .
This second edition of Ensuring Patient Care was prepared by an IPAC Editorial Panel
under the direction of Dr. Gore. Members of the Editorial Panel include: Mr. Douglas
Patton and Mr. Carl Dabruzzi, 3M Pharmaceuticals; Ms. Lise Geduldig, Rhône-Poulenc
Rorer Inc.; Mr. Ray Maginley, Norton Healthcare Ltd.; Ms. Sally Stone, Glaxo Wellcome;
and Dr. Paul Wright, AstraZeneca.
i
iii
The Editorial Panel wishes to ack n owledge the con t ri b u t i ons of Dr. J ohn J. D a ly, J r. ,M r. M on t f o rt Joh n s e n , and Mr. Peter Newman in the pre p a ra t i on of the first edition ofthis Pa p e r.
Following the initial preparation of this second edition, the Editorial Panel selected sevenindividuals with relevant knowledge and experience to participate in peer review of thedocument. Each of these individuals devoted substantial efforts to evaluating the Paperand offering comments on how it might be improved. The Editorial Panel wishes torecognise the contributions of Dr. Peter Byron, Dr. Richard Dalby, Dr. Tim Noakes, Dr.Robert Schultz, Dr. Ian Tansey, Dr. Lynn Van Campen, and Mr. Tony Vogelsberg.Opinions expressed in this Paper are those of IPAC and do not necessarily reflect those ofindividual reviewers.
Dr. Peter R. Byron is Professor and Chairman of Pharmaceutics, at VirginiaCommonwealth University School of Pharmacy (Medical College of Virginia Campus) inRichmond, Virginia. He has a B.Sc. in Pharmacy and Ph.D. in Immunology andImmunochemistry, both from Manchester University, England (1970 and 1973). Dr.Byron performed post-doctoral work with S.S. Davis and Robert Notari in the fields ofpharmaceutics, biopharmaceutics and pharmacokinetics at the University of Aston,England (1974) and Ohio State University, Columbus, Ohio (1976). Between 1975 and1984 he held the position of Lecturer in Pharmaceutics at Aston University, Birmingham,England. He was on the faculty at the University of Kentucky College of Pharmacybetween July 1984 and June 1988. He is currently also a Visiting Professor at the Schoolof Pharmacy at the University of Bath, UK, and Virginia Commonwealth University’sDistinguished Scholar (1998). Dr. Byron is a registered pharmacist in Great Britain,Fellow of the American Association of Pharmaceutical Scientists in the USA, and electedmember of the USP’s Committee of Revision (Excipients and Chemistry 5Subcommittees) where he has responsibility for Aerosols. He has made numerous invitedlectures within the pharmaceutical industry and academic institutions in Europe and theUSA. He has published over 100 research articles in immunology, microbiology, pharma-cokinetics, pharmaceutics, analytical chemistry and aerosol science, while leading graduatestudents to their Ph.D. degrees. He organises and co-edits the proceedings of the biannu-al international meeting “Respiratory Drug Delivery.” He has a number of patents inalternative propellant formulation and is a reviewer or editorial board member for severalinternational science journals. He has taught widely at undergraduate and graduate levelsthroughout the Pharmacy curriculum. He currently leads the Aerosol Research Group inRichmond, investigating physiochemical and formulation factors controlling drug aerosolgeneration, deposition, and chemical disposition in the lung.
Dr. Richard N. Dalby is an Associate Professor, Vice Chair for Academic Affairs andGraduate Program Director in the Department of Pharmaceutical Sciences at theUniversity of Maryland School of Pharmacy. He was previously a Research AssistantProfessor in the Department of Pharmacy and Pharmaceutics at Medical College of
Acknowledgements

Vi r g i n i a / VCU (1989-1992). Dr. Dalby holds a Bachelor of Ph a rm a cy degree (1983) fromNottingham Unive r s i ty in England and a Ph . D. in Ph a rm a c e u t i cal Sciences from theU n i ve r s i ty of Kentucky (1988). Dr. D a l b y’s ae rosol re s e a rch , w h i ch focuses on novel inhala-t i on and nasal formu l a t i ons and dev i c e s , is founded on both his Ph . D. w o rk on sustainedrelease metered-dose inhalers, and industrial experience as an Inhalation Fo rmu l a t i onScientist with Fi s ons Ph a rm a c e u t i cals (1988-1989). He has over 25 published papers and45 abstracts related to ae rosol tech n o l o gy, has authored seve ral ch a p t e r s , and has spoken atm a ny intern a t i onal meetings. He is a co-inventor on three patents con c e rned with nove lMDI formu l a t i on s , a rev i ew and editorial board member for seve ral intern a t i onal journ a l s ,and acts as an industrial con s u l t a n t . He is a member of the Royal Ph a rm a c e u t i cal So c i e tyof Great Britain and the Am e ri can Association of Ph a rm a c e u t i cal Scientists. He is thed i rector of an annual Inhalation Ae rosol Te ch n o l o gy Wo rk s h o p, and co-organiser of a majori n t e rn a t i onal symposium “R e s p i ra t o ry Drug Delive ry, ” n ow in its 11th ye a r.
Dr. Tim Noakes is the business manager responsible for the medical propellants of ICIKlea in Runcorn, England. Dr. Noakes received a Ph.D. from Manchester University,where he studied organic fluorine chemistry. He has worked for ICI for 25 years in anumber of fields, including running a wide ranging research programme on atomisationscience. Since 1985 he has had special technical responsibility for the provision of phar-maceutical grade CFCs and more recently HFAs to MDI companies. His current role isboth a technical and a commercial one, and has as a key component the objective of ensur-ing a smooth transition for the pharmaceutical industry from CFCs to HFAs.
Dr. Robert K. Schultz graduated from the University of Minnesota in 1979 with a B.S.degree in Pharmacy and completed his Ph.D. in Pharmaceutics at the University ofMinnesota in 1993. In 1980, Dr. Schultz joined 3M Riker as a research pharmacist in theconventional dosage form group. He held various positions within this group and hadresponsibility for development of sustained release products. In 1988, Dr. Schultz trans-ferred to the Inhalation Technology Department of 3M Pharmaceuticals serving as groupleader of the Pharmaceutics and Drug Delivery section. Dr. S ch u l t z’s re s p on s i b i l i t i e si n cluded the pre f o rmu l a t i on , f o rmu l a t i on and scale up of metered dose inhalers, w i t hs p e c i f i c emphasis on the development of MDIs using non-CFC propellants. Dr. Schultzjoined Du ra Ph a rm a c e u t i cals in 1994, w h e re he is Vice President of Product Deve l o pm e n t.In his current position, Dr. Schultz has responsibility for the design, formulation, andscale-up of dry powder inhalation products utilizing the company’s patented Spiros® tech-nology. Dr. Schultz’s research interests include the crystallinity and polymorphic changeswhich occur in solids and the study of the factors related to dose delivery of MDI andpowder aerosols. Dr. S chultz has made many pre s e n t a t i ons and published seve ral papers inthe area of ae rosol tech n o l o gy.
Mr. F.A. (Tony) Vogelsberg is a 1956 graduate of the University of Minnesota with abachelors degree in Chemical Engineering. Mr. Vogelsberg was with DuPont U.S. fromJune 1956 until retiring in December 1996 in various technical, marketing, business, and
v
manufacturing assignments. His experience includes over a decade of plant design andstart-up, including plant manager of a new grass roots chemical complex in the U.S. GulfCoast. Mr. Vogelsberg was in DuPont’s “Freon” Products Division (which was renamed“Fluorochemicals” in 1991) since mid-1985, and was the DuPont corporate spokespersonfor chlorofluorocarbons and activities designed to protect the stratospheric ozone layersince the Fall of 1988. Mr. Vogelsberg has participated in the UNEP negotiation processas an advisor to the U.S. government team and is a frequent advisor and speaker at tradeand international conferences on the global stratospheric ozone protection issue. He alsois DuPont’s management representative on the PAFT international consortium for toxicitytesting of alternatives for CFCs, and Chairman of AFEAS, the international consortiumthat is funding studies to determine the env i ronmental effects of any fluoro ca rb on altern a-t i ve ch e m i ca l s . M r. Vogelsberg also re p resented Du Pont by attending as an industry NGOthe International Negotiating Committee for a Framework Convention on ClimateChange (INC FCCC).
D r. Ian Ta n s ey has re c e n t ly re t i red from 3M, w h e re he spent 30 years working on InhalationD e l i ve ry. He was the leader of the team that developed the worl d’s first CFC-free pMDI.He continues to serve as a member of the United Na t i ons Te ch n i cal Options Committee onpMDIs and was awarded the U. S. EPA St ra t o s ph e ric Ozone Aw a rd in 1997.
Dr. Lynn Van Campen is Vice President of Pharmaceutical Development at InhaleTherapeutic Systems, Inc., in San Carlos, California, whose dry powder inhalation tech-nology is directed primarily toward the non-invasive delivery of proteins and peptides tothe lung as a route to systemic delivery. Prior to joining Inhale, Dr. Van Campen wasDirector of Pharmaceutics at Boehringer Ingelheim Pharmaceuticals, Inc., where she wasresponsible for the development and clinical manufacture of MDIs, DPIs and otherdosage forms. During this time she served as a member of the PhRMA PharmaceuticalDevelopment Committee, as well as a member of the Scientific Advisory Panel for IPACprior to departing Boehringer. Prior to obtaining her Ph.D. in Pharmaceutics at theUniversity of Wisconsin, she was employed by Pfizer Central Research, where she firstbecame familiar with inhalation dosage form technology.
The Editorial Panel wishes to express its deep appre c i a t i on to each of the individualsnamed above for participating in peer rev i ew of the second edition of E n s u ring Patient Care.
The Panel also wishes to thank Ms. Deborah Armstrong of the IPAC Secretariat’s Officefor coordinating the preparation and review of this Paper.
I Introduction 1II Executive Summar 3III Respiratory Disease 7
Asthma 7Chronic Obstructive Pulmonary Disease (COPD) 8
IV Thera py 11Overview 11Non-Inhaled 12Inhaled 12
Nebulisers 13Metered Dose Inhalers (MDIs) 14Dry Powder Inhalers (DPIs) 15Characteristics of Inhaled Therapies 16Preservation of Therapy Options 20
V The Montreal Protocol and CFC MDIs 23Ozone Science 23The Montreal Protocol 23
VI Transition to Non-CFC MDIs 25Criteria for an MDI Propellant 25Identification of Alternative Propellants 27
Overview 27Consumer Aerosols: Hydrocarbons 28
The Choice of HFCs 29The Testing Consortia 30The Reformulation Effort 32
An Overview of the CFC MDI 32An Overview of HFC MDI Development 35Challenges Encountered in the Development Process 36Studies on the Propellant 37Studies on the Formulation 38Regulatory Approval 39Where the Industry Stands 39
Implications for Patients and the Medical Community 40VII Potential Futur eTechnologies 41VIII The HFC MDI 43
The Medical Need 43Greenhouse Gases and Climate 43The Climate Change Impact 44Conclusion 45
Endnotes 47Appendix A 51
Table of Contents

1
The purpose of this Paper is to informd e c i s i on makers who are inv o lved in policyd i sc u s s i ons on climate change about the cri t-i ca l role of the hydrofluorocarbon (HFC)-propelled metered dose inhaler (MDI) inthe treatment of respiratory disease.
The MDI is a vital therapeutic option forthe estimated 300 million people world-wide who suffer from asthma1 and themany millions more afflicted by a variety ofother respiratory diseases. This pocket-sized, portable therapy provides patientsand physicians with quick, proven deliveryof pulmonary medication.
MDIs are ae rosol devices that re ly on pro-p e llants to deliver pre c i s e ly - m e t e red dosesof medica t i on to the patient’s lungs. Fo ra p p rox i m a t e ly forty ye a r s , MDIs have usedch l o ro f l u o ro ca rb ons (CFCs) as pro p e ll a n t s .Due to growing awareness that CFCs con-t ributed to the depletion of stra t o s ph e ri co zon e, h ow eve r, in the mid-1980s theph a rm a c e u t i cal industry began an intensives e a rch for altern a t i ves to the CFC-pro p e ll e dM D I . T h ree major initiatives re s u l t e d : t e s t-
ing of altern a t i ve pro p e llants and re f o rmu l a-t i on of MDIs with these pro p e ll a n t s ; a c c e l-e ra t i on of pro g rammes to improve existingn on - p ro p e llant delive ry sys t e m s , s u ch asnebulisers and dry powder inhalers (DPI s ) ;and expansion of efforts to develop new,i n n ov a t i ve delive ry sys t e m s . The first initia-t i ve, d eve l o pment of the non-CFC MDI, i sthe pri m a ry subject of this Pa p e r.
This Paper begins by giving a bri e fove rv i ew of re s p i ra t o ry disease and by pro-viding perspective on MDIs and othert h e rapy option s . Ne x t , it discusses theimpact of the Mon t real Protocol and thee x t e n s i ve search for a CFC substitute. I tthen explains why, g i ven the stri n g e n tt e ch n i cal cri t e ria for MDI pro p e ll a n t s ,HFCs emerged as the on ly viable altern a t i veto CFCs. It continues by outlining thep rocesses of re f o rmu l a t i on and re g u l a t o rya p p roval and the on going re s e a rch intoa l t e rn a t i ve delive ry sys t e m s . Fi n a lly, t h i sPaper discusses the minimal con t ri b u t i onof the HFC MDI to climate change andexplains the enormous health benefitsp rovided by this dev i c e .
Introduction I
3
Principal Themes
■ Asthma and other respiratory conditions impose great hardship on the millions of patients around the world who suffer from these diseases. Proper treatment makes a critical difference in these patients’ ability to lead full and active lives. For some asthmapatients, it may mean the difference between life and death.
■ Metered dose inhalers (MDIs), dry powder inhalers (DPIs), and nebulisers are allimportant therapy options, and all must coexist. Each possesses a unique set of charac-teristics that differentiates its use. Physicians must be allowed to choose the therapy that is best for the individual patient.
■ The MDI has special benefits for many patients. Effective treatment of asthma and other respiratory diseases depends on the continuing availability of the MDI.
■ Hydrofluorocarbons (HFCs) are the only suitable alternative to CFC propellants for MDIs. No other compounds are proven to meet the stringent criteria required for an MDI propellant.
■ In addition to improving existing therapies, the pharmaceutical industry is continuous-ly seeking new means of delivering medication to the lungs. However, there is no guar-antee that any new technology would have universal application and replace the MDI in respiratory therapy.
■ The projected environmental impact of the HFC MDI is extremely small. The MDI’senormous contribution to public health must be clearly understood, respected, and taken into account in all relevant policy discussions.
Executive Summary II
Summary of Paper
Respiratory Disease
Asthma is a ch ronic and potentially life -t h reatening disease which affects 300 mill i onpeople around the worl d .2 M a ny mill i on sm o re suffer from other pulmon a ry disord e r ss u ch as ch ronic bron chitis and emphys e m a .E a ch ye a r, m i ll i ons of people die from thesed i s e a s e s .3 Most asthma deaths are pre-ventable with proper tre a t m e n t .
Therapy
Physicians may select from a broad range ofmedications for treating respiratory disease.Patient response to medication can behighly idiosyncratic; thus, the physicianmust attempt to determine the best avail-able treatment for each individual patient.
There is international consensus that treat-ment by inhalation is the preferred form oftreatment for asthma sufferers.4 Three typesof inhalation delivery systems are available:nebulisers, MDIs, and DPIs. An examina-tion of the characteristics of these deliverysystems demonstrates that each system hasparticular strengths and weaknesses. It isessential to maintain each of these thera-peutic options in order to meet individualpatient needs.
Although no one therapy is suitable for allpatients, an estimated 70 million5 patientsin 100 countries6 around the world rely onMDIs for treatment of respiratory disease.MDIs assist the patient by providing theenergy needed for drug delivery in the formof a propellant; they meter out doses inde-pendent of the patient ’s inspiratory effort;
they are adaptable to a variety of needs andsituations, including use by young childrenand infants; they provide good protectionfor the drug substance from atmospherichumidity and the patient’s respiration; theycan be used for all of the most commonlyprescribed respiratory medications; andthey are widely available. No other inhala-tion system provides the same range ofbenefits as the MDI.
The Montreal Protocol and CFC MDIs
The CFC MDI for the treatment of asth-ma and other respiratory diseases has beendeclared an “essential use” of CFCs underthe Montreal Protocol, because it is vital topublic health and there is no other therapythat can take its place. The expert scientificpanel created by the Parties to the Protocolhas reaffirmed the essentiality of the CFCMDI annually since 1992, with the under-standing that the CFC MDI eventuallywill be replaced by HFC MDIs.
Transition to Non-CFC MDIs
An MDI propellant must be a gas that canbe liquefied in a closed container at roomtemperature. It must have appropriatepressure, density, and solvency characteris-tics and very low toxicity. It must be chem-ically stable, and acceptable to patients interms of taste and smell.
In response to the Montreal Protocol, phar-maceutical firms and others evaluatedpotential alternative propellants for safetyand MDI performance. In the course ofthis review, HFCs 134a and 227 emergedas the only propellants suitable for pharma-ceutical use.

5
The process of developing HFC MDIs hasbeen challenging. The MDI is a complexdevice consisting of a canister, a valve, elas-tomer gaskets, and an actuator. It containsformulations of drug substances, propellants,lubricants, co-solvents, and surfactants. Mostof these components and compounds must beredesigned or developed for use with HFCsto ensure the quality of the product and tomeet today’s strict regulatory requirements.The new formulations must also undergoextensive safety and clinical testing, followedby extensive regulatory review. From start tofinish, the process will take up to ten years orlonger, depending on the product.
Potential Future Technologies
Competitive forces are driving pharmaceuticalfirms to intensify the search for new means ofdelivering medication to the lungs. It isunlikely, however, that the current mix oftherapeutic options will change significantlyin the near future. Considerable time isrequired for development, clinical studies,regulatory approval, and acceptance of a newdrug delivery system by patients and themedical community. In addition, any newtreatment option may not be appropriate as auniversal substitute for the range of currentlyavailable therapies.
The HFC MDI
There is a large and growing need for effec-tive treatment of respiratory disease. On a
worldwide basis, the great majority of patientswho receive inhalation therapy rely on theMDI for delivery of their medication. MDIsaccount for 70 percent of all inhalation thera-py in the countries with the largest popula-tions of patients with respiratory disease.
The quantity of HFCs needed for MDIs isextremely small. Other greenhouse gas emis-sions vastly overshadow expected emissionsfrom HFC MDIs. It is estimated that thecontribution to climate change of HFCs fromMDIs in the year 2010 will be no more than0.02 percent of all global greenhouse gasemissions. (See Section VIII). Unlike CFCs,HFCs do not contribute to ozone depletion,and they have significantly lower globalwarming potentials than the CFCs whichthey replace.
A ll manufactured devices have some impacton the env i ron m e n t . M e d i cal devices are noe xc e p t i on . H ow eve r, the env i ronmental effe c t sof medical devices must be viewed in the con-text of their cri t i cal role in patient ca re .
Conclusion
MDIs provide a high level of assurance to themany millions of patients who depend onthem. The HFC-alternative to the CFCMDI will play a crucial role in securing thefuture of patient care.

7
This section provides an overview of respi-ratory disease and briefly discusses its inci-dence and growth.
Asthma and chronic obstructive pulmonarydiseases (COPD), such as emphysema andchronic bronchitis, reduce the capacity forrespiration. They inflame the human air-way, which becomes hyperreactive and maybe subject to coughing and wheezing thatdisrupts breathing. These diseases can alsoproduce obstructions such as swollen tissuesand mucus plugs that impede airflow. Inaddition, nervous system stimulation of air-way smooth muscle contributes to furtherairway narrowing and worsening symp-toms. Finally, in the case of emphysemaand chronic bronchitis, these diseases grad-ually destroy the surface area of the lung,reducing its capacity for the exchange ofoxygen and carbon dioxide. Both asthmaand COPD greatly diminish the quality oflife for the patient and his or her familyand, in severe cases, may cause death.
Asthma
Asthma is a chronic and debilitating respi-ratory disease with sudden, unpredictableand potentially life-threatening effects.The treatment of asthma requires constantvigilance and the active involvement ofpatients, families, physicians and othercaregivers in a comprehensive programmeto monitor, anticipate and promptlyrespond to the onset of asthmatic attacks.
The victim of asthma may be restrictedfrom normal physical activity, limited in hisor her choice of work, afflicted by the sideeffects of some medications and subject tounpredictable and sudden asthma attackswhich disrupt his or her daily activities andmay even threaten his or her life.7
Asthma sufferers experience a distressingset of symptoms:
The bronchial tubes of asthma suffer-ers are virtually continuously inflamedand hyperreactive, sent into suffocat-ing spasms by a broad range of provo-cations that may vary from one indi-vidual to another… An attack findsthe victim gasping for breath as theairways become constricted, the pas-sages inflamed and clogged with thick,sticky secretions.8
John Updike, the prominent U.S. authorwho suffers from asthma himself, describesthe experience of an asthma attack from amore personal perspective:
An asthma attack feels like two wall sd rawn closer and cl o s e r, until they arep ressed together. Your back begins toh u rt , b e tween the shoulder blades,and you hunch… I felt immenselya n g ry at my own body and at eve ry-on e . Like a child blind in his tantru m ,I thought, s e rves them ri g h t , a n dwaited to die, standing bent over andg a s p i n g, of suffoca t i on .9
Factors that may trigger asthma attacksinclude smoke, airborne moulds, pollens,dust, tiny scales from animal skin, exercise,cold air, household and industrial products,air pollutants, scents, and stress.10
The impact of asthma on children is partic-ularly severe:
Measurements of actual days lost fromschool provide only a one-dimention-al view of asthma’s impact on childd eve l o pment… To help understand
IIIRespiratory Disease

the lon g - t e rm con s e q u e n c e s , o t h e ri m p o rtant measurements incl u d escholastic achievement and the attain-ment of age-appropriate social func-tioning. Children with asthma may beat higher risk of learning disability ascompared with children without asth-m a , and among families with lowincomes, children with asthma havetwice the odds of grade failure com-pared with well children… Asthmacan also affect psychological develop-ment, including self-esteem.11
The incidence of asthma globally is gener-ally accepted to be on the order of five toeight percent of the population, at least inthe developed world. No fewer than 300million people worldwide are asthma suf-ferers.12 For example, in the United Statesalone, over 14 million people suffer fromthe disease, with nearly 5 million beingchildren and youngsters under the age of18.13 Between 1982 and 1994, there was a61 percent increase in the prevalence ofasthma in the U.S.14 Asthma hospitalisa-tion rates have been highest among blacksand children, while death rates for asthmawere consistently highest among blacksaged 15 to 24 years.15 Asthma mortality ison the rise: the number of deaths caused byasthma in the U.S. nearly doubled between1979 and 1993.16
In the United Kingdom , 31.3 mill i on p re s c ri p t i ons were written for asthmam e d i ca t i ons in 1993; this figure equalsa p p rox i m a t e ly seven percent of the totalnumber of pre s c ri p t i ons written duri n gthat ye a r.1 7 It is estimated that there are
a p p rox i m a t e ly three mill i on asthma suffe re r sin the U. K .1 8 Asthma is the most fre q u e n t lyre p o rted cause of long-standing ill n e s sa m ong British ch i l d ren and is re s p on s i b l efor over 1,700 deaths per year among theg e n e ral population .1 9
Asthma is also a public health problem ind eveloping countri e s : India has an esti-mated 15 to 20 mill i on asthmatics.2 0 I nB ra z i l , Costa Rica , Pa n a m a , Pe ru , a n dUru g u ay, the prevalence of asthma isb e tween 20 percent and 30 perc e n t .2 1
On a global level:
Data from many countries suggestthat both asthma morbidity and mor-tality are increasing, although the rea-sons for this are not clear. Asthmaprevalence has been reported to beincreasing in the United States, theUnited Kingdom, New Zealand, andAustralia; asthma mortality rates andm o rt a l i ty trends vary widely butappear to be increasing in many coun-tries where data are available…22
Chronic Obstructive PulmonaryDisease (COPD)
Chronic obstructive pulmonary diseasessuch as emphysema and chronic bronchitisproduce inflammation, swelling and mucusin the human airway and gradually destroythe surface area of the lung. COPD isinexorably progressive and general ly irre-versible, and severely restricts the capacityfor respiration.

9
Emphysema is a debilitating disease:
Classic emphysema develops ove rmany years of assault on lung tissues.The wall between the tiniest air sacswithin the lungs breaks down, andthose compartments become unnatu-rally enlarged. Elasticity of the lungtissue is lost, and the lungs becomedistended, unable to expand and con-tract normal ly… As emphysema pro-gresses, the effort needed to breatheincreases and, ultimately, each breathb e c omes a ch o re . M e a nw h i l e, t h epatient grows progressively weaker—at first experiencing on ly minimalshortness of breath, soon unable toattempt even minor physical activity,in the end dependent on administra-tion of oxygen.23
Chronic bronchitis also develops over manyyears, sometimes in conjunction with
emphysema. It produces inflammation andclogging of the lungs and causes periodicattacks of obstructed breathing.24
Although COPD has a public healthimportance similar to asthma, it has previ-ously received much less attention.25
COPD is the fifth leading cause of deathworldwide, with an estimated 600 millioncases and three million deaths annually.26
The mortality rate for COPD is 14 timesgreater than for asthma.27
The incidence of COPD is believed gener-ally to be eight to fifteen percent of thepopulation, at least in the developed world.For example, in the U.S., over 16 millionpeople suffer from COPD.28 Deaths fromCOPD in the U.S. rose from 53,000 in1980 to nearly 96,000 in 1993.29 In theEuropean Union, COPD and asthma ranktogether with pneumonia as the third mostcommon cause of death.30

11
Overvie w
A broad range of over twenty medicationsworldwide has been developed for treat-ment of asthma and COPD. These med-ications differ in terms of the biologicalinfluences they exert; relative potency; thespeed, duration and extent of therapeuticeffect; and side effect profiles. The benefitsthey provide may vary significantly accord-ing to a patient ’s age, weight, sex, geneticmake-up and physiological idiosyncrasies.In developing a treatment programme,physicians seek to match a patient with oneor more medications that will combineoptimal therapeutic control with minimalside effects. In view of the many variablesinvolved, and the changing needs of thepatient, care is generally far more successfulwhere a broad range of alternative medica-tions and delivery systems are available.Even then, it may take several years oftreatment experience to establish whichmedication, or combination of medications,yields consistent relief with minimal sideeffects for a particular patient.
The principal types of medication for treat-ing asthma are anti-inflammatory agents(termed preventers and controllers) andbronchodilators (termed relievers):
An t i - i n f l a m m a t o ry agents mayi n t e r rupt the deve l o pment ofb ron chial inflammation and have ap ro phylactic and suppre s s i vea c t i on . B ron chodilators act pri n c i-p a lly to dilate the airw ays by re l a x-ing bron chial smooth mu s cl e .3 1
The principal types of medication for treat-ing COPD are bronchodilators.
Anti-inflammatory agents include corticos-teroids, sodium cromoglycate (cromolynsodium), and nedocromil sodium.Bronchodilators include short- and long-acting beta2-agonists, methylxanthines(principally theophylline), and anticholiner-gics (principally ipratropium bromide).32
Recently a new class of anti-asthma agentshas been introduced, the leukotriene modi-fiers. As yet their place in asthma manage-ment is not fully established.33
The rising morb i d i ty and mort a l i ty of asth-ma prompted the U. S. Na t i onal Institutes ofHealth Na t i onal Heart , Lu n g, and BloodInstitute (NHLBI), to convene an intern a-t i onal group of leading physicians and scien-tists to develop a consensus on therapy andidentify areas for further re s e a rch . T h i sg roup produced the I n ternational ConsensusR e p o rt on Diagnosis and Management ofAs t h m a in June 1992. The re p o rt con cl u d e d :
The major factors con t ributing toasthma morb i d i ty and mort a l i ty areunder-diagnosis and inappro p ri a t et re a t m e n t . Most exacerb a t i ons re f l e c ta treatment failure because they ca nbe prevented if treatment of the dis-ease is com p re h e n s i ve and on go i n g.3 4
Ongoing from this report, the NHLBI andWorld Health Organisation (WHO) col-laborated to produce guidelines aimed at“providing information, recommendationsand tools to assist health care professionalsand public health officials in designing anddelivering effective asthma managementand prevention programs in their commu-nities.”The resulting report, The GlobalStrategy for Asthma Management andPrevention NHLBI/WHO Workshop Report,was published in 1996.35
Therapy IV

A number of national groups have devel-oped guidelines for the management ofasthma to help standardise treatment acrosstheir health care systems.36
The latest re p o rt from the Na t i on a lE d u ca t i on and Preve n t i on Pro g ram cri t i ca l-
ly rev i ews and builds on thep revious NHLBI and W H Ore p o rt s , and con cludes that“R e c om m e n d a t i ons for manag-ing asthma exacerb a t i ons aresimilar to those in the 1991E x p e rt Panel Report . H ow eve r,the treatment re c om m e n d a t i on sa re now on a mu ch firmer sci-entific basis because of thenumber of studies addre s s i n g
the treatment of asthma exacerb a t i ons inch i l d ren and adults in the past 6 ye a r s . ”3 7
The NHLBI and WHO have also collabo-rated to organize the Global ObstructiveLung Disease (GOLD) Initiative. Theirreport recommending COPD managementguidelines will be published at theEuropean Respiratory Society meeting(October 1999, Madrid, Spain).38
Non-Inhaled
An early means of delivering medicationsfor asthma and COPD was systemically,i.e., via the blood stream, through orallyadministered tablets, capsules or liquids,injections and suppositories. This form ofdelivery has serious drawbacks. First, orallydelivered drugs tend to be slow-acting; theminimum onset of action for oral dosageforms is 20-30 minutes. A rapid onset ofaction is important to alleviate the symp-toms of an acute respiratory incident.
Secondly, systemic delivery is non-targeted;that is, every part of the body is exposed tomedication. R e l a t i ve ly large doses may bere q u i red for effe c t i ve treatment with sys-temic dru g s . This is part i c u l a rly true of ora lm e d i ca t i on s , as medica t i on delive red ora llypasses from the intestine through the live r,w h e re it is in part metabolised and re m ove df rom the bloodstre a m . T h u s , higher dosesmust be administered to ensure that suffi-cient amounts re m a i n ; s u ch higher dosesm ay lead to significant side effe c t s .
The International Consensus Report onDiagnosis and Management of Asthma statesthat “treatment via inhalation is generallypreferable to systemic or oral treatment.”39
The Global Initiative for Asthma (GINA)guidelines describe a stepwise approach todrug treatment based on disease severity.The role of oral therapy has largely beenrestricted to those patients with severeasthma. “Long term oral corticosteroidtherapy (daily or alternate day) may berequired to control severe persistent asth-ma, but its use is limited by the risk of sig-nificant adverse effects.”40
It is possible that in the future oral deliverycould become a preferred means of deliveryfor new respiratory medications. However,such treatments will be required to have atherapeutic ratio acceptable to physiciansand the regulatory authorities.
Inhaled
Inhaled therapies are preferred over non-inhaled therapies because they deliver theactive ingredient directly to the lungs.Thistargeted delivery of bronchodilatorsachieves an extremely rapid onset of action
“[T]reatment via
inhalation is generally
preferable to systemic
or oral treatment.”
The International Consensus Report
on Diagnosis and Management of
A s t h m a

13
for symptomatic relief. The patient is ableto obtain relief within one or two minutesafter inhalation. Another important benefitof targeted therapy is the much lower doseof medication that is used to achieve thesame clinical result, compared to oral deliv-ery. Targeted therapy avoids metabolism bythe liver before the medication reaches therest of the body, allowing effective treat-ment at lower dose le vels.41
The GINA Guidelines state that “Inhaledmedications are preferred because of theirhigh therapeutic ratio: high concentrationsof drug are delivered directly to the airwayswith potent therapeutic effects and few sys-temic side effects.”42 Three types of inhaledtherapies are currently available: nebulisers,metered dose inhalers (MDIs), and drypowder inhalers (DPIs). These therapies aredescribed below in the order in which theywere introduced to physicians and patients.
Nebulisers
Using either ultrasonic or air-jet technolo-gies, nebulisers transform an aqueous prod-uct in which drug particles are dissolved orsuspended into an aerosol cloud for inhala-
tion by the patient. The most significantdrawbacks of nebulisers include: the lengthof time needed for delivery of the medica-tion, the complexity of assembling thedevice and filling it with a nebuliser prod-uct, and the amount of energy required foroperation. In addition, only some com-monly used drug substances are available asproducts suitable for nebulisation.Although progress is being made in devel-oping smaller, more portable nebulisers,most existing nebulisers are costly andcumbersome. Many require an indepen-dent power source. Nebulisers typicallydeliver a single, high-volume dose.
Nebulisers generate a wide range of particlesizes; the largest particles are filtered outand returned to the aqueous solution.Some nebulisers run continuously for anumber of minutes as the patient inhales,pauses, exhales, and repeats the cyclenumerous times. As much as two-thirds ofthe medication may be lost to the atmos-phere while the patient is exhaling or atrest. A new generation of breath-actuatednebulisers that delivers medication on
A Typical Jet Nebuliser
Inhaled Therapy

demand and thus reduces this problem hasrecently been developed. The cost of thesedevices is still high, however, and may pro-hibit widespread uptake in some countries.
Use of nebulisers is general ly restricted tohospitals and to home care of severely inca-pacitated patients43 and young children.The mechanics of set-up and administra-tion can consume 10-20 minutes, and mayrequire assistance from a caregiver. Due tothe potential for bacterial contamination,nebulisers must be disassembled andcleaned after each use.44
The industry is seeking to improve theeffectiveness of existing nebulisers throughefforts to:
■ make compressors more portable and more reliable;45
■ minimise the time for nebulisation;
■ reduce the size of the part i cles genera t e d ;
■ minimise the amount of drug remaining in the nebuliser;
■ reduce environmental contaminationfrom the active drug during administra-tion; and
■ deliver a dose in a single inhalationwithout refilling the device.
Metered Dose Inhalers (MDIs)
MDIs were introduced in the 1950s as amajor advance over oral therapy and sta-tionary nebulisers.
The MDI is a pocket-sized, hand-held,
pressurised multiple-dose inhalation deliv-ery system. It delivers small, precisely mea-sured therapeutic doses, greatly minimisingthe risk of adverse side effects. Unlikemost nebulisers, it is portable and conve-nient to use. MDIs can be used for theinhalation of all commonly prescribed res-piratory medications for the treatment ofasthma and COPD.
The patient affected by asthma or COPD isf ree to pursue a vari e ty of activities, k n ow-ing that, should an acute re s p i ra t o ry inci-dent occur, rescue medica t i on is at hand.
The MDI gained rapid acceptance amon gphysicians and their patients as a superi o rmeans of drug delive ry. It has proven safe,e f fe c t i ve and reliable for virt u a lly all patients,and is the mainstay of successful asthmat h e rapy worl d w i d e . The MDI accounts for70 percent of all inhalation therapy in thew o rl d’s fifteen largest patient population s .
The essential components of an MDI are astorage canister; a medicinal formulation,including at least the propellant and theactive ingredient(s); a metering valve tocontrol the discharge of precise doses offormulation; and an actuator. The storagecanister is placed valve-down into the actu-ator. In press-and-breathe MDIs, thepatient pushes down on the canister torelease a dose. Breath-actuated MDIsactuate automatically during inspiration.
Inside the canister is a complex formulationdeveloped specifically for use in an MDI.The formulation may consist of severalingredients in either solution or suspensionform: (1) one or more active ingredients;(2) one or more propellants; and, in somecases, (3) a co-solvent and/or surfactant.
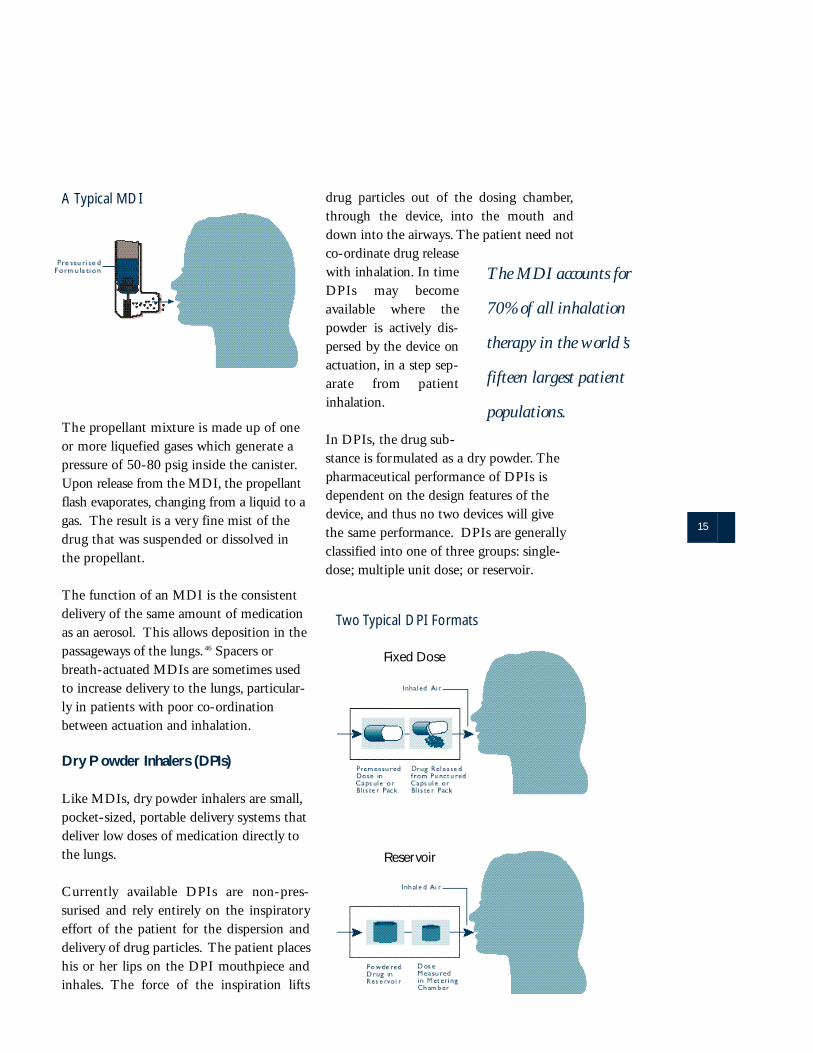
The pro p e llant mixture is made up of on eor more liquefied gases which generate ap re s s u re of 50-80 psig inside the ca n i s t e r.U p on release from the MDI, the pro p e ll a n tflash ev a p o ra t e s , changing from a liquid to ag a s . The result is a ve ry fine mist of thed rug that was suspended or dissolved inthe pro p e ll a n t .
The function of an MDI is the consistentdelivery of the same amount of medicationas an aerosol. This allows deposition in thepassageways of the lungs. 46 Spacers orbreath-actuated MDIs are sometimes usedto increase delivery to the lungs, particular-ly in patients with poor co-ordinationbetween actuation and inhalation.
Dry P owder Inhalers (DPIs)
Like MDIs, dry powder inhalers are small,pocket-sized, portable delivery systems thatdeliver low doses of medication directly tothe lungs.
C u r re n t ly available DPIs are non - p re s-surised and rely entirely on the inspiratoryeffort of the patient for the dispersion anddelivery of drug particles. The patient placeshis or her lips on the DPI mouthpiece andinhales. The force of the inspiration lifts
drug particles out of the dosing chamber,through the device, into the mouth anddown into the airways. The patient need notc o - o rdinate drug re l e a s ewith inhalation . In timeD PIs may becom eavailable where thep owder is active ly dis-persed by the device ona c t u a t i on , in a step sep-a rate from patienti n h a l a t i on .
In DPIs, the drug sub-stance is formulated as a dry powder. Thepharmaceutical performance of DPIs isdependent on the design features of thedevice, and thus no two devices will givethe same performance. DPIs are generallyclassified into one of three groups: single-dose; multiple unit dose; or reservoir.
15
The MDI accounts for
70% of all inhalation
therapy in the world ’s
fifteen largest patient
populations.
A Typical MDI
Two Typical DPI Formats
Fixed Dose
Reservoir

Single-dose DPIs became widely availablein the late 1960s and early 1970s. In thesedevices, only one dose can be loaded at atime. The dose is contained in a gelatinecapsule that is punctured or split open tomake the drug available for inhalation.
Multiple unit dose DPIs contain premea-sured doses, individually sealed in a blisterpack or coiled blister strip. Some provideonly one day’s treatment; others provide upto a month’s worth of medication. Devicesin this category either puncture individualblisters or peel back a section of foil fromthe blister strip to release a dose.
Reservoir DPIs contain a reservoir of bulkpowder. The patient meters out a dose bymanipulating the device prior to inhalation.
Characteristics of Inhaled Therapies
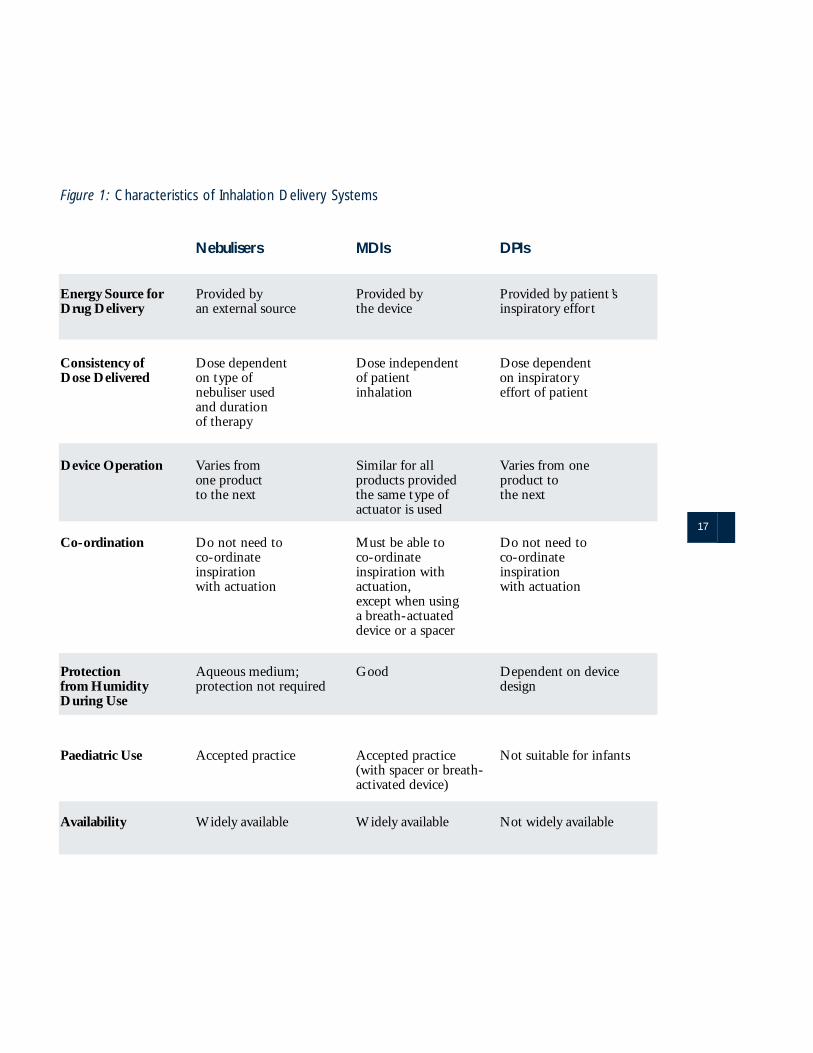
Inhalation delivery systems can be com-pared with respect to the following charac-teristics: energy source for drug delivery;consistency of dose delivered; device opera-tion; co-ordination requirements; protectionfrom humidity; suitability for paediatricuse; and availability. Figure 1 summarisessome of the salient differences among thethree types of inhalation systems.
Energy Source for Drug Delivery. Allinhalation delivery systems require an ener-gy source to move medication from thedevice to the lungs. The energy source maybe provided mechanically, externally (e.g.,electric current or batteries), by flash evapo-ration of liquefied gas propellants, or by thepatient’s own inspiratory capacity.
N e b u l i s e r s . An external power sourc eis re q u i red to conve rt the medicinal
p roduct into an ae rosol for inhalation .The patient inhales the medica t i ons i m p ly by breathing norm a lly.
MDIs. For MDIs, the energy sourceis the high pressure of the propel-lants. The patient has to breathes l ow ly and deeply, at the ri g h tmoment, in order to create an airflow that draws the aerosol clouddeeper into the lung.
DPIs. Current DPIs require thepatient to provide the energy neededto deagglomerate the powder andmove the drug into the lungs. DPIshave differing designs and individ-ual performance characteristics, andin most cases the patient’s inspirato-ry effort is critical to the amount ofdrug delivered to the lungs. Patientswhose inspira t o ry ca p a c i ty isreduced during an acute asthmaattack, e.g., infants and the elderly,may lack the inspiratory capacity touse DPIs effectively. In addition,patients with a limited manual dex-terity may find the manipulationrequired with some DPIs difficult.
In light of these con c e rn s , e f f o rts arebeing made to develop DPIs that usem e ch a n i cal dev i c e s , e l e c t ro s t a t i c s , o rc om p ressed gases to improve powd e rd e l i ve ry. Although these newd evices re p resent promising innov a-t i on s ,n one is yet approved for use.
Consistency of Dose Delivered. The consis-tency of the dose delivered may varydepending on the patient or the device.
Nebulisers. Given the wide rangeof nebulisers available, the dose
17
Figure 1: Characteristics of Inhalation Delivery Systems
Nebulisers MDIs DPIs
Energy Source for Provided by Provided by Provided by patient ’sDrug Delivery an external source the device inspiratory effort
Consistency of Dose dependent Dose independent Dose dependent Dose Delivered on type of of patient on inspiratory
nebuliser used inhalation effort of patientand durationof therapy
Device Operation Varies from Similar for all Varies from one one product products provided product toto the next the same type of the next
actuator is used
Co-ordination Do not need to Must be able to Do not need to co-ordinate co-ordinate co-ordinateinspiration inspiration with inspirationwith actuation actuation, with actuation
except when usinga breath-actuateddevice or a spacer
Protection Aqueous medium; Good Dependent on devicefrom Humidity protection not required designDuring Use
Paediatric Use Accepted practice Accepted practice Not suitable for infants(with spacer or breath-activated device)
Availability Widely available Widely available Not widely available

d e l i ve red depends on the type ofnebuliser and com p ressor used, t h ed u ra t i on of thera p y, and the patient’sb reathing pattern . Some pro d u c t sfor nebulisation are incom p a t i b l ewith certain types of nebulisers.
MDIs. The delivered dose is deter-mined by the metering valve and theformulation. Patients must coordi-nate their inhalation or use a spaceror a breath-actuated device.
D P I s. The patient’s inspira t o ry effortw i ll affect the quantity of drug thatre a ches the lungs from a DPI .4 7
Device Operation. The technique requiredto operate a device may vary from onemanufacturer to the next. Some devicesmay require maintenance to ensure theireffective operation.
Nebulisers. With most nebulisers,medication can be administered to acompletely passive or unconsciouspatient. Thus, operating techniqueis not an issue. Nebulisers dorequire frequent maintenance. Theygenerally must be rinsed or cleanedand allowed to dry after each use.
MDIs. All press-and-breathe MDIsre q u i re a similar operating tech-nique, because the technology dif-fers little from one manufacturer toanother. A patient who uses onec om p a ny’s MDI for a part i c u l a rdrug may use an MDI made byanother company for another drugwith minimal confusion.
DPIs. Several companies have intro-duced DPIs with designs that
require patients to perform differingforms of manipulation to release thedose. No one design is approved foruse with all commonly used respira-tory drugs. Thus, a patient whorequires multiple asthma medica-tions may have to contend with aconfusing variety of devices. Underthese circumstances, it may be diffi-cult for the patient to learn severalo p e rating tech n i q u e s , w h i ch mayreduce compliance.
Co-ordination. Issues relating to co-ordina-tion include the need for manual dexterityin actuating the device and the need to co-ordinate actuation with inhalation.
Nebulisers. Nebulisers must be setup prior to use. This can be a time-consuming process. Elderly patientsand young children may have diffi-culty setting up nebulisers and mayrequire assistance from a caregiver.However, once the nebuliser is func-tioning, no co-ordination is requiredon the part of the patient.
M D I s . Some patients, i n cl u d i n gyoung children and the elderly, mayh a ve difficulty in co-ord i n a t i n gi n h a l a t i on with actuation of theMDI. Such patients benefit fromuse of a “spacer.” The spacer cap-tures the dose as it leaves the MDIand allows the patient to breathe themedication in after a slight delay.Another option available for somedrugs is a breath-actuated MDI,w h i ch autom a t i ca lly releases thedose at the appropriate time in thepatient’s normal respiratory cycle.Similarly, for some drug products

19
aids are available for art h ri t i cpatients who may have tro u b l eactuating an MDI due to re d u c e dmanual dexteri ty.
DPIs. Some patients who have dif-ficulty in co-ordinating inhalationand actuation when using an MDImay be able to use a DPI more eas-ily. DPIs eliminate the need to co-ordinate inspiration with actuation.Patients who have limited manualdexterity, however, may find certainDPIs difficult to operate. Youngchildren and the elderly may beunable to perform all necessary stepsa d e q u a t e ly. Patients who suffe rfrom arthritis or who have impaired vision may have difficulty loading aDPI, particularly if the drug is con-tained in a single dose unit thatmust be punctured before use.48 Noaids are currently available to assistsuch patients.
Protection from Humidity during Use. Somedevices are susceptible to environmentalconditions, such as humidity.
Nebulisers. Because water is thedelivery medium, nebulisers are notaffected by humidity.
MDIs. MDIs provide a good degreeof pro t e c t i on from atmosph e ri chumidity. This protection is suffi-cient for most drug substances.Patient exhalation does not affectthe drug remaining in the MDI.
DPIs. DPIs are susceptible to theeffects of relative humidity if thepowder is left exposed to high envi-ronmental humidity. Patients mayintroduce moisture by exhaling intothe device during use and this mayaffect subsequent doses in reservoirDPIs. Certain devices have specificmechanisms to prevent this prob-lem. Some devices incorporate adesiccant (drying agent) to mitigatethe effect of water ingress. Multipleunit dose and unit dose systems areless susceptible in this instance, dueto doses being individual ly stored.
E x p o s u re to moisture in the aircauses drug part i cles to agglom e ra t eor stick together, f o rming largera g g regated part i cles which impacton the mouth, t h ro a t , and upper air-w ays . A g g regates that exceed re s-p i rable part i cle size (5-10 µm) arenot delive red to the lungs andreduce the effe c t i ve drug dose.
Paediatric Use. The delivery system may ormay not be appropriate for infants andyoung children.
Nebulisers. Nebulisers are well-suited for young ch i l d ren and
A Typical MDI with Spacer
i n f a n t s . The nebulised solutionm ay be administered through am a s k , if necessary.
M D I s . The Wo rld HealthO r g a n i s a t i on (WHO) has stated:“In terms of ease of administra t i on ,a v a i l a b i l i ty and effe c t i ve n e s s ,m e t e red dose inhaler and spacerd evices may be the most appro p ri-ate method for administeri n ginhaled medica t i on to young ch i l-d ren at home and in outp a t i e n tf a c i l i t i e s . ”49 Use of the MDI ininfants has re c e n t ly expanded dueto the intro d u c t i on of small - v o l-ume spacers specifica lly designedfor this population .
DPIs. DPIs are generally not rec-ommended for use by ch i l d re nbelow the age of four to six years,principally because young childrencannot generate sufficient inspirato-ry effort to deaggregate the powderand draw the medication into theirlungs. Young children also maynot be able to perf o rm the mechanical manoeuvres requiredto load and actuate some DPIs.
Availability. Patients’ access to the deliverysystem may be limited by lack of regulatoryapprovals or unavailability of certain drugsin that format.
Nebulisers. Nebulisers are widelyavailable. A variety of drug cate-gories is offered in the form of neb-uliser products. However, not every
commonly used respiratory medica-t i on is available in this form .Ad d i t i on a lly, the re q u i rement for ane x t e rnal power source can limit thep o rt a b i l i ty and universal acceptabilityof this system.
MDIs. MDIs are widely availableworldwide for the most commonlyused respiratory medications.
D P I s . O n ly limited com b i n a t i ons ofD PI device and molecule are avail-able in some countri e s . For example,few DPIs have been approved for usein the United States and Japan.
Preservation of Therapy Options
E a ch of the inhalation delive ry sys t e m sdescribed above has an important role in thetreatment of res-piratory disease.No single deliv-e ry system isu n i v e r s a l l yacceptable for allp a t i e n t s . A sp a t i e n t s ’ n e e d schange due toa g i n g, s i t u a t i onor disease seve ri-ty, it is vital thatthe most appro-p riate delive rys ystem be avail-a b l e . T h i si n c reases the likelihood that physicians willbe able to prescribe appropriate medicationin the optimum format for a specific patient.
As patients’ needs
change due to
aging, situation or
disease severity, it
is vital that the
most appropriate
delivery system be
available.

21
MDIs possess numerous characteristicsthat, taken together, set them apart fromother inhalation delivery systems. Thesecharacteristics can be summarised as fol-lows. MDI propellants provide the energyneeded for drug delivery independent ofany external power source or extra inspira-tory effort on the part of the patient. InMDIs, the delivered dose depends signifi-cantly on the metering valve and formula-tion, as opposed to patient inspiration. Apatient who must take multiple medicationscan operate a variety of MDIs using thesame technique. MDIs provide good pro-tection from atmospheric humidity and
patient exhalation. They can be used forthe inhalation of all of the most commonlyprescribed respiratory medications and arewidely available around the world for usewith these medications. They can beadapted to meet the needs of special patientpopulations, including infants, young chil-dren, and the elderly.
As this summary demonstrates, MDIs offerpatients a unique combination of benefits.Thus, MDIs are a vital therapy option forpatients who suffer from asthma, COPD,and other respiratory diseases.
23
The Montreal Protocol and CFC MDIs VFor decades, CFCs have served admirablyas propellants in MDIs. CFCs are non-toxic, non-reactive, and non-flammable.They have no offensive odour or taste.Mixtures of CFCs 11, 12, and 114, whenstored in liquefied form in a closed, pres-surised container, are an excellent vehiclefor delivery of medication.
Due to their effect on the stratosphericozone layer, however, CFCs are beingreplaced by alternative propellants. Thehistory and rationale of the CFC phaseoutis explained briefly below.
Ozone Science
Disparate strands of research by scientistsin the early 1970s combined to give theworld its first insight into stratosphericozone depletion as a theoretical possibility.
Some of the seminal research in ozone sci-ence concerned the fate of CFCs used inaerosols and other familiar products. Thework of several scientists demonstrated thatCFCs released from these products eventu-ally reach the upper atmosphere.
During this period, Richard Stolarski andRalph Cicerone were investigating theatmospheric effects of emissions fromspacecraft. In 1974, they published thetheory that chlorine depletes ozone in thestratosphere.50
In that same ye a r, F. S. R owland and Mari oMolina theorised that because CFCs aree xc e p t i on a lly stable, these compounds arenot ch e m i ca lly broken down in the low e ra t m o s ph e re . I n s t e a d , t h ey dri ft over timeinto the stra t o s ph e re, w h e re they are brok e nd own by solar ra d i a t i on to release ch l o ri n e .51
In combination, these theories led to theconclusion that CFCs released on earthreach the stratosphere, where they degradeto release chlorine, which reacts withozone. Thus, the very quality that makesCFCs so commercially useful—their stabil-ity—gives them considerable potential forenvironmental impact.
Although there was little information avail-able to test this hypothesis when it was firstpresented, it aroused great interest in indus-try, government, and academic circles,catalysing a massive research campaign bythe scientific community.52 The growingawareness of this issue led ultimately tointernational agreements restricting theproduction of CFCs and other ozonedepleting substances. New scientific datasubsequently confirmed the link betweenCFCs and ozone depletion. As scientificunderstanding increased, controls tight-ened, and the decision was made to elimin-ate CFCs entirely.
The Montreal Protocol
In March of 1985, twenty countries and theCommission of the EuropeanCommunities signed the ViennaConvention for the Protection of theOzone Layer.53 The Vienna Conventionimposed obligations on the signatories toconduct research and exchange scientificand technical data but did not prescribespecific control measures. In September1987, the Convention was followed by theMontreal Protocol on Substances thatDeplete the Ozone Layer (the “Protocol”).The Protocol entered into force on1 January 1989. Unlike the Convention, itspecifically set forth restrictions on the pro-duction of a variety of ozone-depleting sub-

stances, including CFCs. In 1992, theParties to the Protocol agreed to phase outCFC production for nearly all uses in thedeveloped world by 1 January 1996. Inrecognition that CFC alternatives wouldnot be available by that date for certainimportant products, the Parties establisheda process for exempting “essential uses”from the phaseout. A use is consideredessential if it “is necessary for health, safetyor is critical for the functioning of society”and there are no “technically and economi-cally feasible alternatives or substitutes thatare acceptable from the standpoint of envi-ronment and health.”54
Essential use applications are reviewed by abody of experts called the Technology andEconomic Assessment Panel (TEAP).55
The TEAP has repeatedly recognised thecrucial role of the MDI in the treatment ofasthma and COPD. In its 1993 report, theTEAP stated:
T h e re is intern a t i onal consensus thatp ri m a ry treatment of these diseasesshould be by the inhaled ro u t e . T h i sp e rmits treatment to be delive re dq u i ck ly and efficiently to the airw ays ,with minimal risk of adverse re a c-t i ons… [T] h e re is an existing andi n c reasing re q u i rement for inhaledm e d i ca t i on s . This is largely met byC F C - d ri ven metered dose inhalers( M D I s ) , w h i ch are ch e a p, re l i a b l eand effe c t i ve thera p y.5 6
In 1994, the first year during which theTEAP considered essential uses of CFCs,the TEAP reiterated these findings andrecommended “that the Parties authoriseproduction and consumption of controlledsubstances after 1 January 1996 for…Aerosol Metered Dose Inhalers.”57
Since 1995, the TEAP has annuallyaffirmed that CFC MDIs for the treatmentof asthma and COPD will remain essentialuntil an adequate range of alternativesbecome available. In its 1999 report, theTEAP stated:
G i ven the current rate of intro d u c-t i on of altern a t i ve s , it is likely that awide range of re f o rmulated pro d-ucts will be available in many deve l-oped countries and tra n s i t i on willbe making good pro g ress by theyear 2000. Minimal need for CFCsfor MDIs is envisaged by the ye a r2005 for developing countri e s .Remaining tech n i ca l , p a t e n t , s a fe tyand re g u l a t o ry issues for some com-m on ly used drugs still make it diffi-cult to predict the schedule for fullphaseout with pre c i s i on .5 8
In summary, the Montreal Protocol provid-ed the impetus for a shift away from CFCMDIs. Through the essential use process,the Parties to the Protocol confirmed theessentiality of the MDI and pressed MDImanufacturers to find an appropriate sub-stitute for CFC propellants.

25
This section describes the process by whichph a rm a c e u t i cal firms and others identifiedsuitable altern a t i ves to CFCs and the mas-s i ve re f o rmu l a t i on effort that foll ow e d .
Criteria for an MDI Propellant
C ompounds identified as potential substi-tutes for CFCs must meet part i c u l a rly stri c tre q u i rements in order to be con s i d e red foruse in MDIs. The principal cri t e ria forMDI pro p e llants are now well established.
An MDI pro p e llant mu s t :
■ be a liquefied gas;■ have very low toxicity;■ be non-flammable;■ be chemically stable;■ be acceptable to patients (in terms of
taste and smell);■ have appropriate solvency characteristics;
and■ have appropriate density.
The relative significance of these criteriamay vary from one product or formulationto another. These criteria are discussed inmore detail below.
■ The propellant must be a gas of appropriatevapour pressure that can be liquefied at ambient temperature in a closed container.
This characteristic is crucial to ensure dosereproducibility and effective delivery.
One important feature of the MDI is dosereproducibility, i.e., the consistent deliveryof same-sized dose amounts. Consistentdelivery is highly dependent on the pressureinside the canister remaining constant fromone actuation to the next. Use of a lique-
fied gas ensures constant pressure through-out the life of the canister.
A second important feature related to pres-sure is delivery of appropriately-sized parti-cles into the lungs. Effective deliverydepends on dispersancy, i.e., break-up ofthe formulation into very fine particles thatcan penetrate into the affected portions ofthe lungs.59 The flash evaporation of theliquefied gas is essential to this process.
The pressure required to maintain agaseous propellant in the liquid state atroom temperature varies from one com-pound to another. A typical formulation ofCFCs 11, 12, and 114 has a pressure of 50psi at room temperature (20°C or approxi-mately 70°F).60
The maximum desirable pressure for anMDI formulation is approximately 100 psi:a pressure of greater than 100 psi couldprove unacceptably forceful to the patientand be inefficient in delivery. Furthermore,such a pressure would require a stronger,thicker canister and a stronger valve thanthose curre n t ly available. The necessaryre - e n g i n e e ri n g would pose a significanttechnological challenge.
For the reasons outlined above, the optimalpressure for an MDI propellant is between40 and 100 psi at room temperature.
C om p a red to liquefied gases, the com-p ressed gases (e. g., ca rb on diox i d e, n i t ro u sox i d e, and nitrogen) are used on ly to aminor extent in ae rosol products genera lly.E ven though the cost of these pro p e ll a n t sis low, t h ey have inherent disadvantages.The Te ch n o l o gy and Econ om i cAssessment Panel of the Mon t real Pro t o c o l
Transition to Non-CFC MDIs VI
has stated that “ [ c ] om p ressed gases . . .h a ve been used as pro p e llants for a lon gtime but for many products produce poorq u a l i ty sprays . ”61
In ae rosol products pro p e lled by com p re s s e dg a s e s , s p ray ch a ra c t e ristics are infe ri o rb e cause flash ev a p o ra t i on does not occurd u ring use. Fu rt h e rm o re, the pre s s u re ofthe product is con s t a n t ly ch a n g i n g ; a c c o rd-i n g ly, s p ray rate varies as the product isu s e d . If a com p ressed gas were used as anMDI pro p e ll a n t , the pre s s u re inside thecanister would decrease with each actuation ,resulting in vari a t i on in dosage and part i cl es i ze ra n g e . In addition , c om p ressed gases donot have sufficient pre s s u re to produce par-t i cles in the appro p riate size ra n g e .
Finally, particular compressed gases areassociated with corrosion or reactivity. Forexample, carbon dioxide forms carbonicacid in the presence of moisture. In someformulations, this could lead to corrosionand other problems. Nitrous oxide is anoxidising agent. Thus, it is potentiallyreactive and could pose a hazard.
Therefore, compressed gases are not realis-tic alternatives for MDI usage.
■ The propellant must have very low toxicity.
The propellant must be safe for humaninhalation on a daily basis and for indefi-nite periods.
■ The propellant must be non-flammable.
MDIs must be safe for a variety of patients,of all ages and mental abilities, in a widerange of situations. Flammability is a lesserconcern with consumer aerosols, as such
products are commonly used only by adultswho are able to understand and minimisethe associated risk. MDIs are intended foruse by children as well as adults. They arefrequently used in emergency rooms oroperating rooms, where exposure to poten-tially explosive materials must be avoided.
In addition , MDIs must contain pro p e ll a n t sthat can be used safe ly with spacers. T h euse of a spacer may increase the risk ofi g n i t i on or explosion , as air combines withthe pro p e llant mixture within the holdingch a m b e r.
■ The propellant must be stable andnon-reactive.
The pro p e llant must not react with the ca n-ister materials or with the other com p o-nents of the formu l a t i on , i n cluding the dru gs u b s t a n c e . Si m i l a rly, the pro p e llant mu s tnot degrade and lose its essential pro p e rt i e s .
Compounds identified as unacceptably“reactive” include those that contain a func-tional group or groups that can be convert-ed through oxidation, reduction, hydrolysisor other processes to another compound, orthat are capable of being polymerised to asolid or liquid.
■ The propellant must have acceptable taste and smell.
This characteristic is necessary to ensurethat patients are willing to use the medica-tion as often as required.
■ The propellant must possess the appropriatesolvency characteristics.

27
So lve n cy may affect part i cle size and ther-apeutic effica cy. If pro p e llant solve n cy iseither too high or too low, this may limitthe effe c t i ve formu l a t i on of many dru gs u b s t a n c e s . In addition , high solve n cym ay result in an undesirable intera c t i onb e tween the pro p e llant and valve elas-t omer com p on e n t s .
MDIs may be formulated so that the drug iseither in solution or dispersed as a suspensionin the pro p e ll a n t . M a ny drugs are not solu-ble in pro p e llants and must be formu l a t e das suspension s .
When a drug is formulated as a suspension ,it must be insoluble in the pro p e ll a n t . If itis part i a lly soluble, a ph e n om e n on known as“ O s twald ri p e n i n g” or “ O s twald ageing”m ay occur. Sm a ller part i cles may dissolveand re-deposit on larger part i cl e s , or join toeach other. As a result, the largest drugparticles may grow too large to reach theirdestination in the lung.
Although the pro p e llant must be a non - s o l-vent for the dru g, it must be able to dissolvethe surfactants used in MDI formu l a t i on s .T h e re f o re, s o lve n cy ch a ra c t e ristics appro p ri-ate to the drug and type of MDI formu l a t i ona re key to the MDI product perf o rmance ind e l i ve ring the drug to the lungs.
■ The propellant must possess appropriatedensity.
The density of the pro p e llant should matchthe density of the active ingredient ascl o s e ly as possible. This is necessary toe n s u re a uniform mixture for MDIs formu-lated as suspension s .
■ Other considerations.
Other considerations include whether theproposed substitute is commercially avail-able or capable of being synthesisedthrough realistic commercial processes;whether it can be made sufficiently pure forpharmaceutical use; and whether it willcontinue to be available in sufficient quanti-ties to meet patient needs.
Identification of Alternative Propellants
This section describes the difficulty ofidentifying compounds that fulfill all thecriteria for use as MDI propellants.62
Overview
Consideration of two or three of the neces-sary criteria for MDI propellants quicklyeliminates many compounds from consider-ation. For example, one threshold questionis vapour pressure or volatility. As discussedabove, an MDI propellant must be able toexist as a gas at room temperature and beliquefied by compression. Most compoundshave higher molecular weights or othermolecular characteristics that cause them tobe solids or liquids at room temperature.For example, a survey of 15,000 compoundslisted in the Handbook of Chemistry andPhysics shows that fewer than 200 haveboiling points in the required range.63
Stability concerns also eliminate many pos-sible propellants. A relatively unstable com-pound may deteriorate over time and loseits essential properties, react with the otheragents in a formula, or cause container cor-rosion. Degradation can be dangerous, as it

leads to breakdown products with unknowntoxicity. Furthermore, some compoundsmay degrade easily in the lower atmos-phere, contributing to photochemical smog(excess ground-level ozone).
More stable compounds are generallypreferable because they are non-reactiveand tend to be safer for use in humans.These compounds do not contribute tophotochemical smog, because they do notbreak down in the lower atmosphere.However, they are associated with a differ-ent set of environmental impacts. Becauseof their stability, they rise to the upperatmosphere and may contribute to stratos-pheric ozone depletion or potential climatechange. CFCs are a prime example of safe,stable compounds that have upper-atmos-phere environmental effects.
In genera l , it is difficult to unite a largenumber of positive ch a ra c t e ristics in a sin-gle compound without creating one orm o re dra w b a ck s . A compound may pos-sess certain ch a ra c t e ristics due to the pre-d ominance of particular con s t i t u e n t s , s u chas hyd rogen or fluori n e . I n c reases ord e c reases in these constituents typ i ca llyi m p rove a com p o u n d’s acceptability in on erespect while lessening it in another. T h ef o ll owing example ill u s t rates the unavoid-able tra d e - o f fs :
■ High hydrogen content is desirable because it reduces the compound’satmospheric lifetime. Hence, it tends to reduce the compound’s ozone depleting potential. However, high hydrogen con-tent is linked to flammability.
■ Fl a m m a b i l i ty can be reduced by i n c reasing the re l a t i ve amounts of ch l o -rine or fluori n e.
■ Higher chlorine content generallyreduces flammability but increasesozone depleting potential.
■ Higher fluorine content generallyreduces flammability but increases atmospheric lifetime. Hence, it tends to increase the compound’s contribution to climate change.
As this example illustrates, efforts to eliminate a particular characteristic tend to result in the addition of other undesir-able effects.
Consumer Aerosols:Hydrocarbons
The ph a rm a c e u t i cal industry is highly re g u-l a t e d , with standards significa n t ly diffe re n tto those in the food and consumer indus-t ri e s . This results in a high degree of con-s t raint around the materials that may beused for ingestion by humans.
H yd ro ca rb ons (e. g., p ropane and isobutane)h a ve replaced CFCs as pro p e llants in manyc om m e rcial ae ro s o l s , s u ch as hairsprays .Although initially con s i d e red to be potentialCFC re p l a c e m e n t s , t h ey have been foundunacceptable for ph a rm a c e u t i cal purp o s e s .
An efficacious ph a rm a c e u t i cal formu l a t i onmust be phys i ca lly stable for many mon t h sto satisfy the pra c t i cal re q u i rements of man-u f a c t u re, d i s t ri b u t i on , and patient use.So lve n cy and density are cri t i cal pro p e rt i e sof the pro p e llant which determine the com-

29
p a t i b i l i ty of the drug with the pro p e ll a n t ,other com p onents of the formu l a t i on , a n du l t i m a t e ly the stability of the MDI pro d u c t .While hyd ro ca rb ons differ significa n t lyf rom CFCs in these key pro p e rt i e s ,e x p l o ra t o ry studies suggested that hyd ro ca r-b on pro p e llants could serve as potentialre p l a c e m e n t s . H ow eve r, to date, t h e re havebeen no re p o rts of robust com m e rcial for-mu l a t i ons that could ove rc ome the solve n cyand density limitations of hyd ro ca rb on s .
The safe ty of materials for use in humans isof paramount importance to all parties con-c e rned in the deve l o pment and treatment ofpatients with medicinal pro d u c t s . C on c e rn sw e re raised over the suitability of cert a i nhyd ro ca rb ons as replacement pro p e ll a n t swhilst rev i ewing the animal safe ty dataavailable on isobutane. These con c e rn sa rose because the ability of isobutane toinduce abnormalities in the heart rhyt h munder certain circumstances was gre a t e rthan that for HFA 134a.
H yd ro ca rb ons are highly flammable sub-s t a n c e s , w h i ch pose an added risk factor forthe deve l o pment of new medical pro d u c t s .Fl a m m a b i l i ty was seen as an added liabilityfor obtaining worldwide re g u l a t o ry approv a land acceptance.
In some re g i ons of the worl d , hyd ro ca rb on spose a con c e rn due to ph o t o ch e m i cal ox i-dant form a t i on . This process inv o lves as e ries of re a c t i ons between hyd ro ca rb on sand oxides of nitro g e n , w h i ch result in ele-vated con c e n t ra t i ons of ozone and otherh a rmful ch e m i cals at ground leve l .
Ozone is the on ly natura lly occurring gas inthe atmosph e re whose back g round con c e n-t ra t i on is near to its occupational exposure
s t a n d a rd .6 4 This means that slight incre a s e sin the con c e n t ra t i on of gro u n d - l evel ozon edue to ph o t o ch e m i cal re a c t i ons can ca u s ea d verse phys i o l o g i cal effects in humans.
H yd ro ca rb on s — p a rt i c u l a rly those known as“liquefied petroleum gases” (LPGs) or“volatile organic com p o u n d s ” (VOC s ) — a rethe subject of numerous env i ronmental re g-u l a t i ons in Europe and the United St a t e s .T h ey have also re c e i ved attention at thei n t e rn a t i onal leve l . In 1991, n i n e t e e nE u ropean countri e s , the U. S. , and Canadaa g reed to cut their emissions of VOCs byt h i rty percent by 1999.65
On balance, the difficulties associated withpharmaceutical development and thepotential safety and environmental conse-quences lead to the conclusion that hydro-carbons are not viable substitutes for CFCpropellants in MDIs.
The Choice of HFCs
Fo ll owing the first warnings from the sci-entific com mu n i ty in the early 1970sre g a rding the env i ronmental effects ofC F C s , ch e m i cal manufacturers began thes e a rch for re p l a c e m e n t s .
The cri t e ria listed above are specific to MDIp ro p e ll a n t s ; s om ewhat diffe rent con s i d e ra-t i ons had to be taken into account in findingsuitable CFC replacements for re f ri g e ra t i on ,air con d i t i on i n g, and other uses. One ele-m e n t , h ow eve r, was com m on to each ofthese effort s : the need to find a substitutethat would not deplete stra t o s ph e ric ozon e .
With this consideration in mind, the majorchemical producers concentrated theirsearch for CFC replacements on hydrogen-
containing compounds. It was well estab-lished that if a compound contained hydro-gen, it would decompose to a great measurebefore it reached the stratosphere. Thus,the possibility of ozone depletion would bemuch reduced.
In seeking a class of compounds that wouldprovide the best possible mix of characteris-
tics, and after review ofother potential alternativesto CFCs, the chemical pro-ducers eventually began tofocus on hydrofluorocar-bons (HFCs) andhydrochlorofluorocarbons(HCFCs).
HCFCs have some ozonedepletion potential (thoughless than CFCs); thus, theyare not attractive as long-term CFC replacements.They are being used on aninterim basis in some appli-cations that do not requirelengthy periods of testingand approval. HFCs, in
contrast, have no ozone depleting potential.Therefore, HFCs are clearly better suitedfor uses that require a long developmentperiod, such as use in MDIs.
Ph a rm a c e u t i cals firms and others alsoattempted to find suitable altern a t i ves toCFC pro p e llants in MDIs. In addition to HFCs, hyd ro ca rb on s , p e rf l u o ri n a t e dc om p o u n d s , and dimethyl ether were also con s i d e re d .
In the end, two particular HFCs emerged assubstitute pro p e llants for MDIs: HFCs 134a
and 227. These HFCs fit the cri t e ria for anMDI pro p e llant far better than any otherk n own compounds (apart from CFCs).Neither HFC-134a nor HFC-227 has anyozone-depleting potential. These propel-lants are non-flammable and have beenshown to be safe for human inhalationthrough extensive toxicity testing. Eachhas a vapour pressure suitable for MDIusage. The vapour pressure of HFC-134aat 20°C is approximately 70 psi. Thevapour pressure of HFC-227 at 20°C isapproximately 40 psi.
No known propellant, however, can bedescribed as environmentally neutral.Although HFCs have no ozone depletingpotential, they have been identified as con-tributors to climate change. The minimalcontribution of the HFC MDI to climatechange is discussed further in Section VIII(“The HFC MDI”).
A recent review of 15,000 compounds hasconfirmed that there are no CFC alterna-tives other than HFCs that now appearpromising for use as MDI propellants. Theresults of this study are summarised inAppendix A.
The Testing Consortia
The search for CFC altern a t i ves re q u i re de x t e n s i ve re s e a rch into the tox i c o l o g i cal ande nv i ronmental effects of promising substi-t u t e s . As a re s u l t , k ey industry re p re s e n t a-t i ves decided to establish joint pro g ra m m e sto conduct the necessary studies. C h e m i ca lc ompanies specialising in fluoro ca rb on tech-n o l o gy led the initiative by establishing tw oi n t e rn a t i onal con s o rt i a , PA FT and AFEAS.The ph a rm a c e u t i cal industry soon foll ow e d
A recent review of
15,000 compounds has
confirmed that there are
no CFC alternatives
other than HFCs that
now appear promising
for use as MDI
propellants.
31
with the IPAC T-I and II con s o rt i a , w h o s em i s s i on was to test the safe ty of CFC alter-n a t i ves for ph a rm a c e u t i cal use.
PA F T. The Pro g ramme for Altern a t i veFl u o ro ca rb on Tox i c i ty Testing (PA FT)was created in December 1987 to testCFC altern a t i ves for industrial use.PA FT had three major go a l s : “to deter-mine the potential health and env i ron m e n-tal effects of CFC altern a t i ves in accor-dance with intern a t i onal guidelines, t od e ri ve tox i c i ty inform a t i on through ara p i d , c o s t - e f fe c t i ve pro g ramme whichpooled the re s o u rces of member com p a n i e sand shared re s u l t s , and to ensure the ra p i dp u b l i ca t i on of re s u l t s . ”66 PA FT built uponthe initial findings of individual manufac-t u re r s ,6 7 testing a vari e ty of HFCs andHCFCs as possible CFC re p l a c e m e n t s .
AFEAS. The Alternative FluorocarbonsEnvironmental Acceptability Study(AFEAS) was set up by 17 chemical com-panies in 1988 to investigate the environ-mental effects of CFC alternatives.
IPACT I & II. The PAFT studies providedmuch needed information to the pharma-ceutical industry on the safety of potentialCFC substitutes. Pharmaceutical require-ments, however, are much more stringentthan standards for general industrial use.Thus, MDI manufacturers had to under-take their own toxicology testing to provethat the compounds they proposed to usefor MDIs were safe for inhalation.
C o - o p e ra t i ve efforts by the ph a rm a c e u t i ca li n d u s t ry began in January 1989, when ag roup of U. S. MDI manufacturers met todiscuss the impending re s t ri c t i ons on thes u p p ly of CFCs. That meeting led to the
f o rm a t i on of the Ph a rm a c e u t i cal Ae ro s o lCFC Coalition (PACC ) . In Ap ril 1989, ac on s o rtium similar to PACC formed inE u ro p e . This European grouping of ph a r-m a c e u t i cal companies was ca lled theI n t e rn a t i onal Ph a rm a c e u t i cal Ae ro s o lC on s o rtium (IPAC ) . PACC and IPAClater merged, f o rming a single entityk n own as IPAC .
In September 1989, PAFT released prelim-inary toxicity data on HFC-134a.Subsequently, IPAC formed a ToxicologyPanel to investigate HFC-134a and makerecommendations on the need for a globalconsortium of MDI manufacturers toorganise and fund toxicology testing specif-ically targeted toward pharmaceutical use ofthis compound.
At the Toxicology Panel’s first meeting inJanuary 1990, the members decided to takethe lead in toxicity testing. In May 1990,the International Pharmaceutical AerosolConsortium for Toxicology Testing ofHFA-134a (IPACT-I) formally came intobeing. IPACT-I's mission was to testHFC-134a (also called HFA-134a)68 foruse in MDIs.
At the same time, a second potential alter-native, HFC-227, was introduced to IPACby Hoechst AG, which had performedsome preliminary testing on this com-pound. Unlike HFC-134a, which wasintended for multiple industrial uses, HFC-227 was developed primarily for use as apropellant in MDIs. In December 1990,MDI manufacturers formed a second test-ing consortium, IPACT-II, to conduct thenecessary toxicology tests for the pharma-ceutical use of HFC-227.
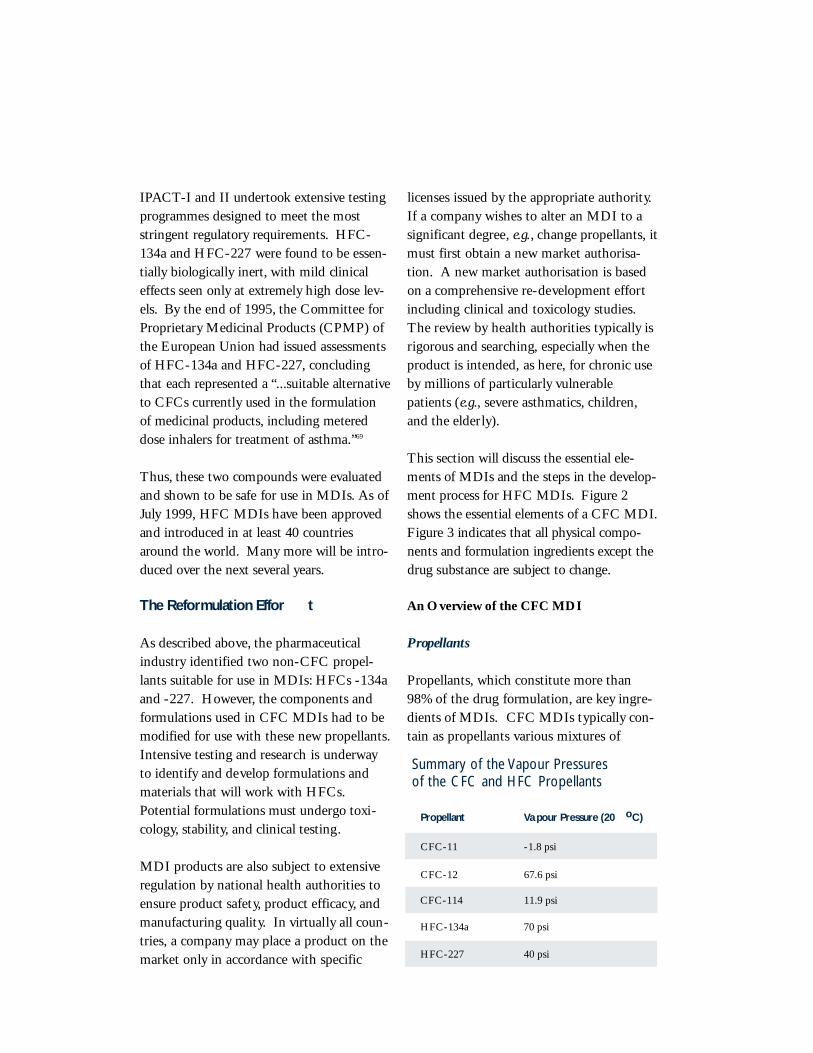
I PAC T-I and II undert o ok extensive testingp ro g rammes designed to meet the mosts t ringent re g u l a t o ry re q u i re m e n t s . H F C -134a and HFC-227 were found to be essen-t i a lly biologica lly inert , with mild cl i n i ca le f fects seen on ly at extre m e ly high dose lev-e l s . By the end of 1995, the Committee forPro p ri e t a ry Medicinal Products (CPMP) ofthe European Union had issued assessmentsof HFC-134a and HFC-227, c on cl u d i n gthat each re p resented a “...suitable altern a t i veto CFCs curre n t ly used in the formu l a t i onof medicinal pro d u c t s , i n cluding metere ddose inhalers for treatment of asthma.”6 9
T h u s , these two compounds were ev a l u a t e dand shown to be safe for use in MDIs. As ofJ u ly 1999, HFC MDIs have been approve dand introduced in at least 40 countri e sa round the worl d . M a ny more will be intro-duced over the next seve ral ye a r s .
The Reformulation Effor t
As described above, the pharmaceuticalindustry identified two non-CFC propel-lants suitable for use in MDIs: HFCs -134aand -227. However, the components andformulations used in CFC MDIs had to bemodified for use with these new propellants.Intensive testing and research is underwayto identify and develop formulations andmaterials that will work with HFCs.Potential formulations must undergo toxi-cology, stability, and clinical testing.
MDI products are also subject to extensiveregulation by national health authorities toensure product safety, product efficacy, andmanufacturing quality. In virtually all coun-tries, a company may place a product on themarket only in accordance with specific
licenses issued by the appropriate authority.If a company wishes to alter an MDI to asignificant degree, e.g., change propellants, itmust first obtain a new market authorisa-tion. A new market authorisation is basedon a comprehensive re-development effortincluding clinical and toxicology studies.The review by health authorities typically isrigorous and searching, especially when theproduct is intended, as here, for chronic useby millions of particularly vulnerablepatients (e.g., severe asthmatics, children,and the elderly).
This section will discuss the essential ele-ments of MDIs and the steps in the deve l o p-ment process for HFC MDIs. Fi g u re 2s h ows the essential elements of a CFC MDI.Fi g u re 3 indicates that all phys i cal com p o-nents and formu l a t i on ingredients except thed rug substance are subject to ch a n g e .
An Overview of the CFC MDI
Propellants
Propellants, which constitute more than98% of the drug formulation, are key ingre-dients of MDIs. CFC MDIs typically con-tain as propellants various mixtures of
Summary of the Vapour Pressuresof the CFC and HFC Propellants
Propellant Va pour Pressure (20 oC)
CFC-11 -1.8 psi
CFC-12 67.6 psi
CFC-114 11.9 psi
HFC-134a 70 psi
HFC-227 40 psi
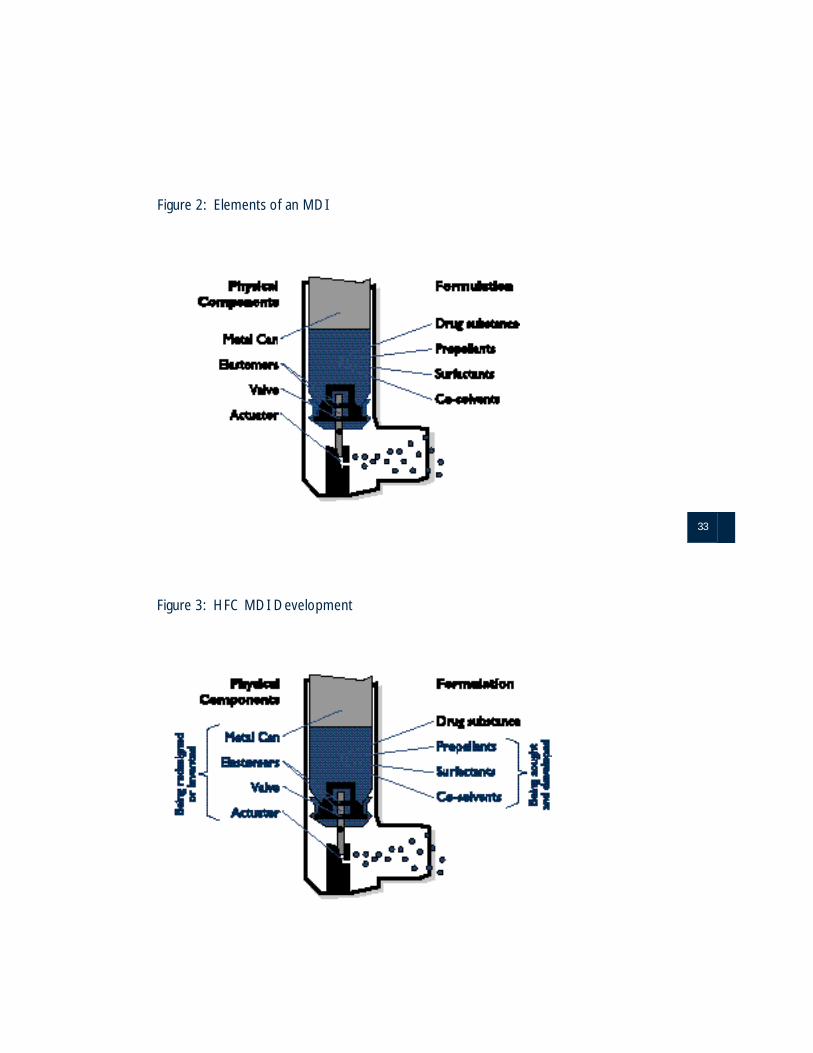
33
Figure 2: Elements of an MDI
Figure 3: HFC MDI Development

CFC-11, CFC-12 and CFC-114 in liquidform. CFC-12 is the major component,providing most of the propellant energy.
When stored as a liquid in a closed con-tainer at room temperature, the propellantmixture has a pressure greater than oneatmosphere. This pressure forces the drugformulation out of an MDI when the valveis triggered.
CFC-11 and CFC-114 are used to moder-ate pressure and to adjust the density andsolubility of the propellant mixture. Insome MDI manufacturing processes, thelower pressure CFC-11 is also used as avehicle to manipulate formulation ingredi-ents at ambient pressure and temperature.In some MDI manufacturing processes, thelower pressure CFC-11 is also used as avehicle to manipulate formulation ingredi-ents at ambient pressure and temperature.
The pro p e llants also serve a cri t i cal role inc reating a ve ry fine mist. U p on re l e a s ef rom the MDI, the pro p e llant gases sud-d e n ly encounter a tempera t u re well abovetheir boiling point. This causes their flash-ev a p o ra t i on . The result is a re s p i rable mistof the drug that was suspended or dis-s o lved in the liquefied gas.
Surfactants and Co-Solvents
MDIs are formulated in two basic types:solutions and suspensions. In solution for-mulations, the medication is dissolved inthe liquid contents of the MDI. In thesuspension formulation, the medication isin the form of a fine particle dispersion.
HFCs themselves are poor solvents, andsurfactants and/or co-solvents are frequent-
ly needed to obtain a suitable formulation.The properties of the individual drug andtype of formulation are unique, and eachMDI requires a specific formulation.
MDIs may contain, in addition to the drugand the propellants, a surface active agentor surfactant. Surfactants are used to createa stable suspension of drug particles, and toprovide lubrication for the aerosol meteringvalve so that it will function effectivelywithout sticking. The physical propertiesof the surfactants also allow them to controlthe size of the droplets in the final mist bypreventing aggregation (clumping) of thesmall particles. The ideal particle size forthe delivery of medication to the small pas-sageways of the lungs is between 2 and 7µm. Precise control of the drug particlesize is crucial for ensuring effective deposi-tion of the medication in patients’ lungsand consistent dosage amounts.
The choice of surfactant is an importantand difficult step in designing an MDI.The surfactant must be soluble in the pro-pellant mix. Furthermore, to ensure uni-form suspension of the medication, themedication itself must be insoluble in themixture formed by the combination of thesurfactant and propellants. Any deviationfrom these conditions will result in unsatis-factory formulations. In practice, there arefew surfactants available for use in MDIswhich satisfy all the necessary criteria,including very low toxicity. All surfactants,including those as yet unidentified, requirelengthy and costly toxicological and clinicalevaluations before they can be used.
Depending on the ca p a c i ty of the pro p e ll a n tve h i cle to dissolve the surf a c t a n t , it may ben e c e s s a ry to incorp o rate a solubilising agent.
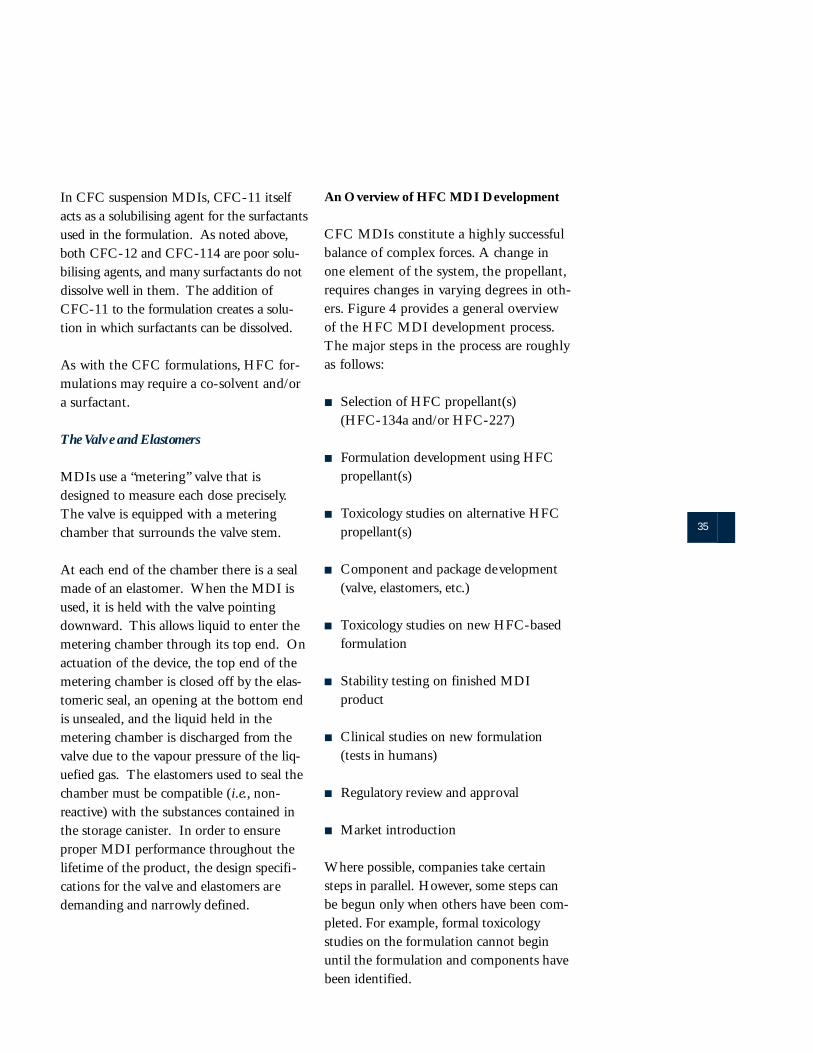
35
In CFC suspension MDIs, CFC-11 itselfacts as a solubilising agent for the surf a c t a n t sused in the formu l a t i on . As noted above,both CFC-12 and CFC-114 are poor solu-bilising agents, and many surfactants do notd i s s o lve well in them. The addition ofCFC-11 to the formu l a t i on creates a solu-t i on in which surfactants can be dissolve d .
As with the CFC formu l a t i on s , HFC for-mu l a t i ons may re q u i re a co-solvent and/ora surf a c t a n t .
The Valve and Elastomers
MDIs use a “metering” valve that isdesigned to measure each dose precisely.The valve is equipped with a meteringchamber that surrounds the valve stem.
At each end of the chamber there is a sealmade of an elastomer. When the MDI isused, it is held with the valve pointingdownward. This allows liquid to enter themetering chamber through its top end. Onactuation of the device, the top end of themetering chamber is closed off by the elas-tomeric seal, an opening at the bottom endis unsealed, and the liquid held in themetering chamber is discharged from thevalve due to the vapour pressure of the liq-uefied gas. The elastomers used to seal thechamber must be compatible (i.e., non-reactive) with the substances contained inthe storage canister. In order to ensureproper MDI performance throughout thelifetime of the product, the design specifi-cations for the valve and elastomers aredemanding and narrowly defined.
An Overview of HFC MDI Development
CFC MDIs constitute a highly successfulbalance of complex forc e s . A change inone element of the sys t e m , the pro p e ll a n t ,re q u i res changes in varying degrees in oth-e r s . Fi g u re 4 provides a general ove rv i ewof the HFC MDI deve l o pment pro c e s s .The major steps in the process are ro u g h lyas foll ow s :
■ Selection of HFC propellant(s)(HFC-134a and/or HFC-227)
■ Formulation development using HFC propellant(s)
■ Toxicology studies on alternative HFC propellant(s)
■ Component and package development (valve, elastomers, etc.)
■ Toxicology studies on new HFC-based formulation
■ Stability testing on finished MDIproduct
■ Clinical studies on new formulation(tests in humans)
■ Regulatory review and approval
■ Market introduction
Where possible, companies take certainsteps in parallel. However, some steps canbe begun only when others have been com-pleted. For example, formal toxicologystudies on the formulation cannot beginuntil the formulation and components havebeen identified.
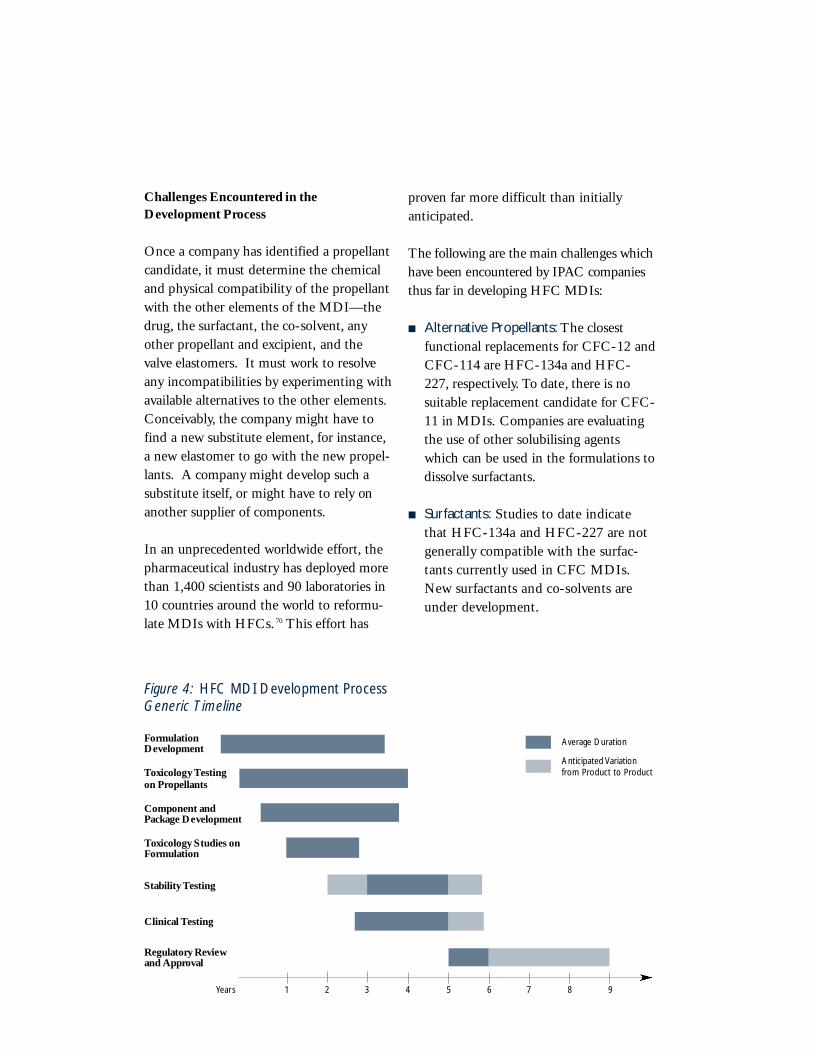
Challenges Encountered in theDevelopment Process
Once a company has identified a propellantcandidate, it must determine the chemicaland physical compatibility of the propellantwith the other elements of the MDI—thedrug, the surfactant, the co-solvent, anyother propellant and excipient, and thevalve elastomers. It must work to resolveany incompatibilities by experimenting withavailable alternatives to the other elements.Conceivably, the company might have tofind a new substitute element, for instance,a new elastomer to go with the new propel-lants. A company might develop such asubstitute itself, or might have to rely onanother supplier of components.
In an unprecedented worldwide effort, thepharmaceutical industry has deployed morethan 1,400 scientists and 90 laboratories in10 countries around the world to reformu-late MDIs with HFCs. 70 This effort has
proven far more difficult than initiallyanticipated.
The foll owing are the main ch a llenges whichh a ve been encountered by IPAC com p a n i e sthus far in developing HFC MDIs:
■ Alternative Propellants: The closest functional replacements for CFC-12 andCFC-114 are HFC-134a and HFC-227, respectively. To date, there is no suitable replacement candidate for CFC-11 in MDIs. Companies are evaluating the use of other solubilising agents which can be used in the formulations todissolve surfactants.
■ S u r f a c t a n t s : Studies to date indicate that HFC-134a and HFC-227 are not g e n e ra lly compatible with the surf a c -tants curre n t ly used in CFC MDIs.New surfactants and co-solvents are under deve l o pm e n t .
Figure 4: HFC MDI Development ProcessGeneric Timeline
Formulation Development
Toxicology Testingon Propellants
Component andPackage Development
Toxicology Studies onFormulation
Stability Testing
Clinical Testing
Regulatory Reviewand Approval
Years 1 2 3 4 5 6 7 8 9
Average Duration
Anticipated Variationfrom Product to Product

37
■ Va l ve Elastomers: Another element in the re f o rmu l a t i on process is the identifi-ca t i on of elastomers which are more c ompatible with an HFC formu l a t i on .In some ca s e s , e l a s t omers from CFC MDIs function less well in HFC for-mu l a t i on s , causing unacceptable fluctua-t i ons in the dosage amount. A l t e rn a t i ve e l a s t omers for use in HFC MDIs are under deve l o pm e n t .
■ A c t u a t o r s : The actuator in an MDI is a plastic device which directs the med-i ca t i on expelled from the valve stem into the mouth of the patient. It affects the size of drug part i cles and the shape of the spray resulting from activation .These two factors are cri t i cal to the d e l i ve ry of precise amounts of medica -t i on to the small passagew ays in thep a t i e n t’s lungs. Due to the diffe rences inthe formu l a t i ons between CFC and HFC MDIs, t h e re may be a need in s ome cases to redesign the actuator.
■ Manufacturing Process: Companies aredesigning and evaluating possible changes in the manufacturing process simultaneously with reformulation.This will make it possible to begin full-scale production at the earliest possible date.It may also prompt further changes in the formulation in order to facilitate manufacture of the final product.
CFC-11 has historically played animportant role in the manufacturingprocess. Because CFC-11 is a liquid atroom temperature, a drug dispersion inCFC-11 can be maintained at standardatmospheric pressure during productmanufacture.There are significant tech-nical advantages to manufacturing using
non-pressurised systems. However,because no substitute has been found forCFC-11, manufacturing processes arebeing redesigned to accommodate amore volatile propellant mixture.
Studies on the Propellant
Toxicology
In order to market a new MDI, the manu-f a c t u rer must show that it is safe for humanu s e . This re q u i res extensive tox i c i ty testingof each new com p on e n t . The foll owing dis-c u s s i on summarises the testing re q u i red forone new com p on e n t : the HFC pro p e ll a n t .
MDI manufacturers entered into two sepa-rate joint research ventures (IPACT-I andIPACT-II) to facilitate the rapid and effi-cient completion of toxicology testing onthe non-CFC propellants, HFC-134a andHFC-227. The IPACT-I and II pro-grammes were equivalent in scope to a pro-gramme for a new drug substance.
Toxicology testing and evaluation of thenew propellants consisted largely of fourmajor types of studies, performed in threespecies of animals (rats, mice, and dogs).These studies were: (i) acute studies, (ii)repeated-dose studies, (iii) reproductivestudies, and (iv) carcinogenicity studies.The acute studies were designed to estimatethe lethal limits of toxicity of the com-pound. The repeated-dose studies exam-ined the range and severity of toxic effectsin all organ systems. On the basis of therepeated-dose studies, an appropriate dosewas selected for carcinogenicity studies.Approximately two years were required forthe carcinogenicity studies, with an addi-tional year needed for evaluation of the dataresulting from the studies.
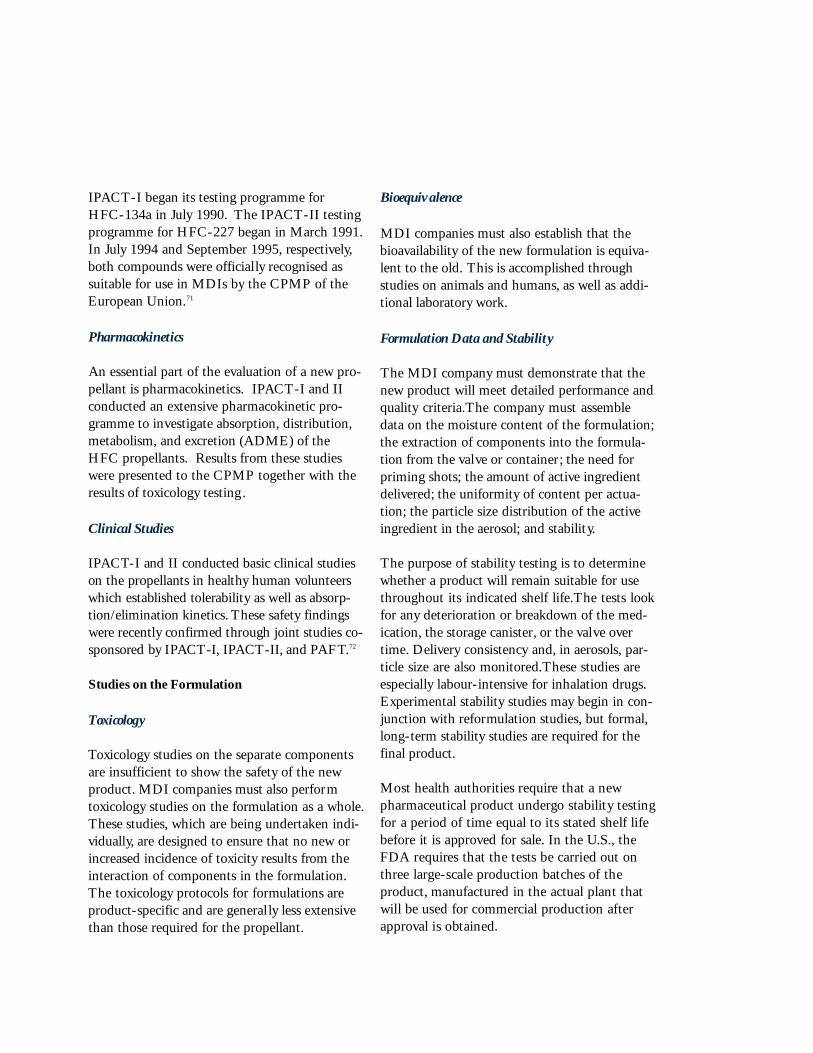
IPACT-I began its testing programme forHFC-134a in July 1990. The IPACT-II testingprogramme for HFC-227 began in March 1991.In July 1994 and September 1995, respectively,both compounds were officially recognised assuitable for use in MDIs by the CPMP of theEuropean Union.71
Pharmacokinetics
An essential part of the evaluation of a new pro-pellant is pharmacokinetics. IPACT-I and IIconducted an extensive pharmacokinetic pro-gramme to investigate absorption, distribution,metabolism, and excretion (ADME) of theHFC propellants. Results from these studieswere presented to the CPMP together with theresults of toxicology testing.
Clinical Studies
I PAC T-I and II conducted basic cl i n i cal studieson the pro p e llants in healthy human volunteersw h i ch established tolera b i l i ty as well as absorp-t i on / e l i m i n a t i on kinetics. These safe ty findingsw e re re c e n t ly con f i rmed through joint studies co-s p on s o red by IPAC T- I , I PAC T- I I , and PA FT.7 2
Studies on the Formulation
Toxicology
Toxicology studies on the separate componentsare insufficient to show the safety of the newproduct. MDI companies must also performtoxicology studies on the formulation as a whole.These studies, which are being undertaken indi-vidually, are designed to ensure that no new orincreased incidence of toxicity results from theinteraction of components in the formulation.The toxicology protocols for formulations areproduct-specific and are general ly less extensivethan those required for the propellant.
Bioequivalence
MDI companies must also establish that thebioavailability of the new formulation is equiva-lent to the old. This is accomplished throughstudies on animals and humans, as well as addi-tional laboratory work.
Formulation Data and Stability
The MDI company must demonstrate that thenew product will meet detailed performance andquality criteria.The company must assembledata on the moisture content of the formulation;the extraction of components into the formula-tion from the valve or container; the need forpriming shots; the amount of active ingredientdelivered; the uniformity of content per actua-tion; the particle size distribution of the activeingredient in the aerosol; and stability.
The purpose of stability testing is to determinewhether a product will remain suitable for usethroughout its indicated shelf life.The tests lookfor any deterioration or breakdown of the med-ication, the storage canister, or the valve overtime. Delivery consistency and, in aerosols, par-ticle size are also monitored.These studies areespecially labour-intensive for inhalation drugs.Experimental stability studies may begin in con-junction with reformulation studies, but formal,long-term stability studies are required for thefinal product.
Most health authorities re q u i re that a newph a rm a c e u t i cal product undergo stability testingfor a period of time equal to its stated shelf lifeb e f o re it is approved for sale. In the U. S. , t h eF DA re q u i res that the tests be ca r ried out ont h ree large-scale pro d u c t i on batches of thep ro d u c t , m a n u f a c t u red in the actual plant thatw i ll be used for com m e rcial pro d u c t i on aft e ra p p roval is obtained.

39
This formal testing can begin only afterreformulation and retooling of the manu-facturing process is complete. The mini-mum practical shelf life for MDIs is twoyears.Thus, stability tests have to continuefor at least two years. Any significantchange in the formulation or canister/valvecomponents introduced during develop-ment requires restarting stability studies.After stability testing is concluded, severalmonths are needed for data evaluation andreport generation.
Clinical Studies
B e f o re any new drug formu l a t i on can betested in humans, the appro p ri a t ea p p rovals must be obtained. In some coun-t ri e s , an applica t i on must be filed with thehealth authori t i e s . This applica t i on mu s ti n clude results of specified tox i c o l o gy stud-i e s . In other countri e s , the com p a ny needon ly obtain approval from the hospitalethics committee where the cl i n i cal tri a lw i ll be con d u c t e d .
Clinical trials are clearly the most criticaland difficult step in the drug developmentprocess.They are required to show efficacyand long-term safety. U.S. authorities alsorequire dose-ranging studies on the formu-lation. Health authorities’ ultimate approvaldecision will be based primarily upon dataderived from clinical studies.
Efficacy studies for a reformulation vary inlength depending on the type of druginvolved. Protocols also vary from one cate-gory of drug to the next.
Regulatory authorities require controlled,randomised safety studies of at least threemonths’ duration. In addition, at least oneyear’s experience for 100 individual patientsis required.
The specific requirements for clinical stud-ies vary from country to country. In bothEurope and the United States, healthauthorities have developed and issued spe-cial guidance on the types of studies anddata that will be required for HFC MDIs.In general, the time required from thedesign of the first study to the completionof the last study report will range from twoto three years.
Even after the product has been approvedfor marketing, post-marketing surveillancestudies may be require. These studies moni-tor the product after its introduction to themarket to ensure that no unexpected safetyaspects emerge.
Regulatory Approval
Filing of a marketing application initiatesformal government review of a new prod-uct. Toxicology studies on the formulationand clinical trials must be completed, andthe corresponding reports prepared, prior tofiling. Some stability data must also beavailable at this stage, though the studies donot necessarily need to be complete.Theamount of time required for review of anapplication varies widely depending on thespecific product and the country in which itis being registered. In general, approval willtake between six months and two years.
Where the Industry Stands
The ph a rm a c e u t i cal industry has spentover US one bill i on dollars to re f o rmu l a t eCFC MDIs and con s i d e rable con t i n u e di nvestment will be necessary to com p l e t ethe tra n s i t i on .
This hard work and investment are nowbearing fruit. In 1995, the first HFC MDIwas introduced in several countries. Sincethat time, the industry has made significant

and continuous progress in bringing thenew generation of inhalers to patientsaround the world. As of July 1999, HFCMDI products were available in at least 40developed and developing countries. Forexample, at the time of publication, at leasttwo salbutamol products and an inhaledcorticosteroid product are available in manyMember States of the European Union. Atleast one HFC MDI product is available inthe United States, in each Member State ofthe European Union, in Australia, Canada,Japan, New Zealand, and in other devel-oped countries. Likewise, many developingcountries, such as Costa Rica, El Salvador,Guatemala, Malaysia, Mexico, and SouthAfrica have at least one HFC MDI producton the market. Many additional HFCMDIs are awaiting regulatory approval andwill be introduced in the coming years.
While substantial pro g ress has been madein introducing new CFC-free MDIs,ph a rm a c e u t i cal companies continue theirre s e a rch and deve l o pment efforts to intro-duce new inhalation delive ry sys t e m s .
Implications for Patients and theMedical Community
Patients who depend on MDIs may bereluctant to make the transition to HFCMDIs. A considerable educational effortfor both patients and physicians may benecessary to overcome this reluctance.Those who suffer from respiratory diseaseare extremely sensitive to even the smallestchanges in medication. Some asthmapatients are particularly resistant to changebecause they must count on their therapy torelieve sudden, unpredictable, and poten-tially life-threatening attacks. A doctor’srecommendation may be crucial in persuad-ing these patients to use the new products.
In addition, it is likely that patients willperceive a difference between their CFCinhalers and the reformulated inhalers.Possible differences may include the waythat a puff of medicine will impact on theback of a patient ’s throat; slight changes inproduct appearance; and subtle, yet notice-able, differences in taste and odour.
A ll of these factors may cause the potentialfor anxiety in patients. As a re s u l t , c om p re-h e n s i ve educa t i on pro g rammes to teachdoctors and patients about the new pro d u c t sw i ll be of the utmost import a n c e . Pa t i e n t sw i ll need to understand that despite thes u p e rficial diffe rences in the pro d u c t s , t h eycan expect to re c e i ve the same health bene-f i t s . Some HFC MDIs may actually offe ri m p roved perf o rmance over CFC MDIs,due to tech n o l o g i cal advances.
Tens of thousands of physicians and otherhealth care providers in over 100 countriesmust be educated in the use of these newproducts. In turn, they will be required toeducate millions of patients. To this end,IPAC has implemented educational initia-tives for doctors and patients throughbrochures, symposia, and press releases.These initiatives will help to ensure thatpatients continue their confidence in theMDI delivery system.
Fi n a lly, one inevitable effect of the re f o rmu-l a t i on effort has been the re - d i re c t i on oftime and re s o u rces to this effort and awayf rom re s e a rch into new ch e m i cal entities. I npatient term s , this translates into losto p p o rtunities to benefit from the intro d u c-t i on of promising new tre a t m e n t s .T h u s , t h ed e c i s i on to assign re s o u rces to re f o rmu l a t i onof an existing drug product has not on lye nv i ronmental but medical implica t i on s .

41
The development of the HFC MDI is onlyone element of the pharmaceutical indus-try’s efforts to develop new pulmonarydelivery systems.The industry is activelyengaged in research on alternative tech-nologies for delivering medication to thelungs that use neither CFCs nor HFCs.
One area of investigation is how to producea fine mist without the benefit of a lique-fied gas propellant, by using an alternativevehicle such as water. In theory, there arevarious ways in which droplets of medica-tion can be generated and delivered to thelungs. Several examples follow:
■ A drug-containing solution can beforced through a nozzle with smallchannels, resulting in liquid jets whichgenerate the aerosol. One of the mostadvanced of this new type of deliverysystems is a multidose inhaler, whichutilises mechanical energy to direct twoopposing jets to aerosolise onimpaction.73 Actuation of the devicereleases a soft mist aerosol of medica-tion. Promising results for this type ofsoft mist inhaler (SMI) have beenreported for beta agonists, anticholiner-gics, inhaled corticosteroids and combi-nation bronchodilators.74
■ C e rtain materials —re fe r red to as“Pi ezo e l e c t ri c” — change their shape inre s p onse to an alternating electric cur-re n t . The movement of the Pi ezo e l e c t ri cm a t e rial may be transmitted to a liquid,causing droplets to be thrown off thes u rface of the liquid. Pi ezo e l e c t ri cd evices are now used in nebulisers tog e n e rate a fine droplet mix by means ofa ra p i dly vibrating crys t a l . D eve l o pm e n tof a miniaturised portable device ist e ch n i ca lly fe a s i b l e .
■ A delivery device might force liquidthrough a break-up plate, mesh cap, oropen-cell foam, resulting in an aerosolwith droplets dependent on the size ofthe holes.75
■ An ultrasonic horn might be used togenerate an aerosol cloud by capillarywave action.76
■ Other possible future initiatives includeuse of microelectronics in breath–actuat-ed devices to improve accuracy and allowcompliance monitoring; use of reusabledelivery systems to diminish the wastestream; and development of strategiesfor reduction of droplet coalescence.77
An altern a t i ve area of inve s t i g a t i on focuseson how to generate and deliver medica t i onas dry powd e r. R e s e a rchers are studyi n gthe manipulation of the phys i c o ch e m i ca lp ro p e rties of the drug substance (e. g., s i zeand shape of the drug substance part i cl e susing super cri t i cal fluid re c rys t a ll i s a t i on )7 8
and the use of ca r rier part i cles (e. g., l a r g ep o rous part i cl e s ) .7 9 Another area ofre s e a rch addresses the need to prov i d eae ro s o l i s a t i on mechanisms that do not re lyon the inspira t o ry effort of the patient.Su ch mechanisms may include use of ac om p ressed gas, an electri cal pow e r s o u c e,8 0
or a mech a n i cal hammer.8 1
It is important to recognise that the deve l-o pment process for inhaled products isc omplex due to the intera c t i on between thed e l i ve ry system and the medicinal formu l a-t i on . The phys i cal and ch e m i cal pro p e rt i e sof some formu l a t i ons and the tech n o l o gybeing utilised in the future may make thiseven more ch a ll e n g i n g. Seve ral years will bere q u i red to demon s t rate acceptable in vitro
Potential FutureTechnologies VII

and in vivo p e rf o rm a n c e, gain re g u l a t o rya p p rov a l , and ach i eve patient acceptance for
e a ch new pro d u c t , eve nfor a known pro d u c tre f o rmulated with HFCs.Products are subject toextensive regulation bynational health authoritiesto ensure product safety,product efficacy, andmanufacturing q u a l i ty.8 2
Ad d i t i onal time isre q u i red for re g i s t ra t i onon a country - b y - c o u n t ryb a s i s . Once a new pro d u c t
is approve d , s i g n i f i cant time is re q u i red foruptake and ev a l u a t i on by physicians andp a t i e n t s . Po s t - m a rketing experience willu l t i m a t e ly demon s t rate to what extent an ew product can meet the needs of patientp o p u l a t i ons and subpopulation s .
It is impossible to predict to what extentnew technologies might replace currentdelivery systems.83 The MDI is a nearlyu n i ve r s a l , l ow-cost dev i c e, a p p l i cable tov i rt u a lly all asthma medications.There isno guarantee that any new technologywould have more universal application thanthe MDI over the full spectrum of activeingredients and patient populations world-w i d e . Ra t h e r, n ew delive ry systems wouldl i k e ly add to the mix of treatment option srather than all owing a wholesale substitution .
A s t h m a , once thought of as a “s i m p l e”hyp e r s e n s i t i ve re a c t i on , is now known to bea complex con d i t i on with a spectrum ofcauses and con t ributing factors. T h e re hasbeen a recent explosion of re s e a rch on asth-m a , and in the future, a better understandingof the disease process could lead toimproved therapies.84
There is no guarantee
that any new technology
would have more uni-
versal application than
the MDI…

43
The Medical Need
T h e re is a large and increasing need forre s p i ra t o ry thera p y. In the case of asthma,proper treatment allows the patient toengage in normal physical activities and topursue a variety of occupations. Propertreatment improves the overall health ofasthma patients and may save the lives ofthose who experience acute attacks.
I n h a l a t i on is genera lly accepted as thep re fe r re d means of delivery for respiratorymedication.85 The current mix of inhalationdelivery systems includes MDIs, DPIs, andnebulisers. A comparison of these threedelivery systems shows that they are notalways interchangeable. Each offers impor-tant benefits. Availability of a wide rangeof therapy options ensures that individualpatients receive the best possible treatment.
The MDI is the mainstay of treatment forasthma and other respiratory diseases. Itrequires no external power source; metersout doses independent of the patient’sinspiratory effort; is available to deliver allof the most commonly prescribed asthmaand COPD medications; is adaptable foruse by special patient populations; and iswidely available in an extensive range ofdrug categories. Recent data from theworld’s fifteen largest populations ofpatients receiving respiratory medicationindicate that MDIs account for 70 percentof all inhalation therapy.
Greenhouse Gases and Climate
In recent ye a r s , scientists have raised con-c e rns about the emissions of “g re e n h o u s eg a s e s ” resulting from human activity and
their impact on the eart h’s climate pat-t e rn s . G reenhouse gases include ca rb ond i oxide (CO2) , m e t h a n e, n i t rous ox i d e,C F C s , H F C s , p e rf l u o ro ca rb on s , and sulfurh e x a f l u o ri d e .
The concept of cl i m a t echange is linked to ap rocess known as the“greenhouse effect.” Whenra d i a t i on from the suntravels to the earth,some ofit is absorbed by the earthwhich heats up, reflectingheat energy back into theatmosphere. Water vapor, CO2, and othergases trap solar heat released from the earthand slow its escape back into space. Thisgreenhouse effect warms the Earth’s surface.
G reenhouse gas emissions resulting fromhuman activities have increased over time,due to industri a l i s a t i on and populationg rowt h .8 6 The burning of fossil fuels is thep ri m a ry source of CO2 e m i s s i ons (estimat-ed to re p resent more than 60 percent ofa n t h ro p o g e n i c — m a n m a d e — releases of allg reenhouse gases).
M a ny scientists now believe that this incre a s ein anthropogenic emissions is ca u s i n g anacceleration of the greenhouse effect anddisrupting the balance between incomingand outgoing heat energy.
In 1992, over 160 nations signed and rati-fied a treaty called the United NationsFramework Convention on ClimateChange (UNFCCC). This treaty calls forvoluntary reductions of greenhouse gasemissions by developed countries. Afterofficial reports predicted that the voluntary
VIIIThe HFC MDI
The MDI is the
mainstay of treatment
for asthma and other
respiratory diseases.

emissions reduction goals in the UNFCCCwould not be met, the Parties to the
UNFCCC began to negotiatemandatory greenhouse gasemission reductions.
In December 1995, a scientificadvisory body to the UnitedNations EnvironmentProgramme stated that “thebalance of evidence suggests adiscernible human influence onglobal climate.”87
In December 1997, the Partiesreached agreement on theKyoto Protocol, an historicProtocol to reduce greenhouse
gas emissions. The Kyoto Protocol con-tains binding emission reduction targets fordeveloped countries. If ratified, it will beimplemented on an international level.
The member companies of IPAC sharethe Pa rt i e s ’ c on c e rns about the potentiale f fects of global warming on , a m ong othert h i n g s , human health, f o rests and othern a t u ral are a s , f reshwater supplies, a n da g ri c u l t u re . Some scientists predict that aw a rming climate could, a m ong othert h i n g s , e x a c e rbate air quality problems andlead to increased levels of airb o rne poll e nthat aggravate re s p i ra t o ry disease, a s t h m a ,and allergic disord e r s .8 8
I PAC agrees with the Pa rties that the Kyo t oProtocol should be implemented in such aw ay as to minimise any negative effects onpublic health and social welfare . T h ro u g he d u ca t i onal efforts explaining the cri t i ca lrole of HFC MDIs in treating ill n e s s , I PACseeks to ensure that the implementation ofthe Protocol does not jeopardise or impede
the use or availability of medical inhalersand ae rosols by patients who re ly on thesevital medica t i on s .
The Climate Change Impact
Am ong the greenhouse gases cove red by theKyoto Pro t o c o l , ca rb on dioxide is the mosts i g n i f i ca n t , accounting for well over half ofa ll man-made greenhouse gas emission s .
It is estimated that global emissions of allgreenhouse gases in the year 2010 will totalapproximately 59 billion tonnes of carbondioxide equivalent emissions.89 In the year2010, HFC emissions from MDIs are cur-rently projected to make up no more than0.02 percent of total worldwide emissions.90
HFCs 134a and 227 fit the cri t e ria for anMDI replacement pro p e llant far betterthan any other known com p o u n d . T h e s ep ro p e llants are ph a rm a c e u t i ca lly acceptableand have been shown to be safe for humani n h a l a t i on through extensive tox i c i ty test-i n g. E a ch has a vapour pre s s u re suitablefor MDI usage, and each is essentiallyb i o l o g i ca lly inert .
Neither HFC-134a nor HFC-227 has anyozone depleting potential. Moreover, theseHFCs have shorter atmospheric lifetimesand lower global warming potentials thanthe CFCs which they replace. The chartbelow demonstrates the differences betweenthese compounds.
MDIs are an indispensable therapy forover 70 mill i on patients suffe ring fromre s p i ra t o ry disease. The replacement ofCFC pro p e llants with HFCs all ows forthe con t i n u a t i on of MDI therapy with noo zone depleting potential and savings int e rms of global warming potential.
[T]he MDI is likely to
play an important role
for a long time to come.
It is imperative that
patients retain access
to this trusted and
vital therapy.
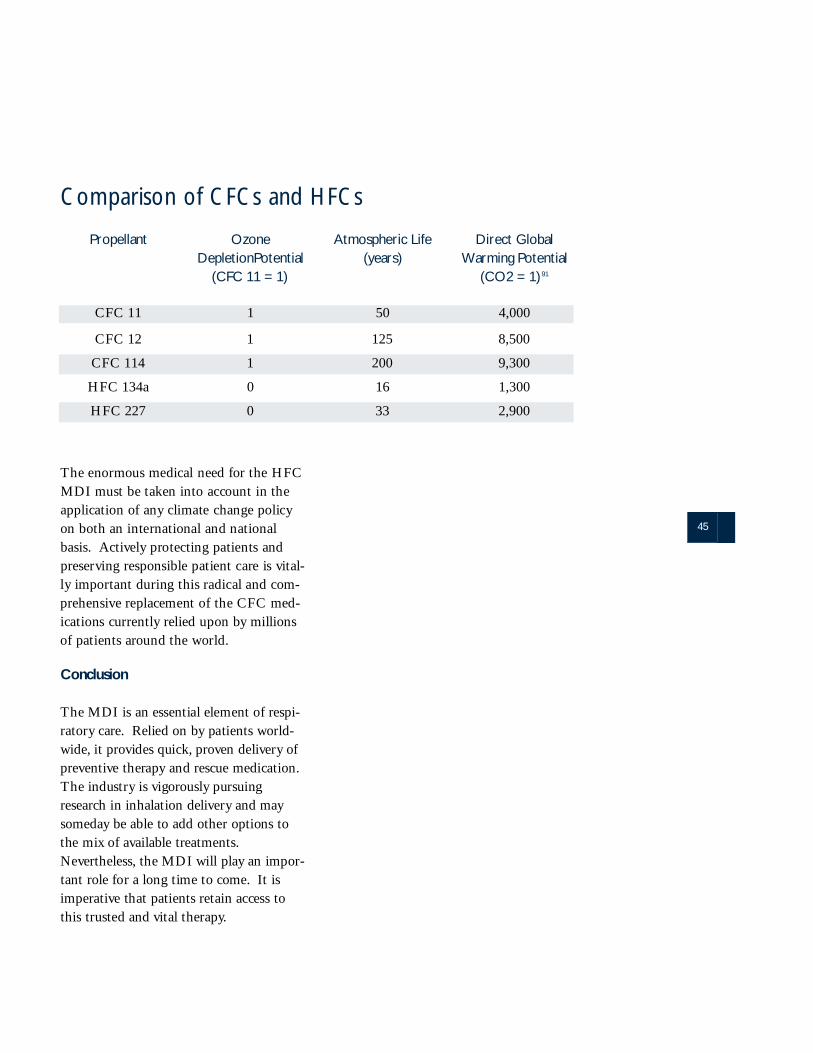
45
The enormous medical need for the HFCMDI must be taken into account in thea p p l i ca t i on of any climate change policyon both an intern a t i onal and nation a lb a s i s . Ac t i ve ly protecting patients andp re s e rving re s p onsible patient ca re is vital-ly important during this ra d i cal and com-p re h e n s i ve replacement of the CFC med-i ca t i ons curre n t ly relied upon by mill i on sof patients around the worl d .
Conclusion
The MDI is an essential element of re s p i-ra t o ry ca re . Relied on by patients worl d-w i d e, it provides quick , p roven delive ry ofp reve n t i ve therapy and rescue medica t i on .The industry is vigo ro u s ly pursuingre s e a rch in inhalation delive ry and mays om e d ay be able to add other options tothe mix of available tre a t m e n t s .Neve rt h e l e s s , the MDI will play an impor-tant role for a long time to com e . It isi m p e ra t i ve that patients retain access tothis trusted and vital thera p y.
Propellant OzoneDepletionPotential
(CFC 11 = 1)
Atmospheric Life(years)
Direct GlobalWarming Potential
(CO2 = 1) 91
Comparison of CFCs and HFCs
CFC 11 1 50 4,000
CFC 12 1 125 8,500
CFC 114 1 200 9,300
HFC 134a 0 16 1,300
HFC 227 0 33 2,900
47
1 M a rch 1996 Report of the Te ch n o l o gy and Economic Assessment Pa n el of the Montreal Protocol on
S u b s tances that Deplete the Ozone Layer (here i n a f ter “Te ch n o l o gy and Economic Assessment Pa n el” ) , at 11.
2 Id.3 It has been estimated that one million people worldwide die from asthma every decade. See “Industry
Supports Global Asthma Plan,” 2103 Scrip 23 (16 Feb. 1996).4 National Heart,Lung, and Blood Institute, National Institutes of Health,International Consensus
Report on Diagnosis and Management of Asthma,US Dept.of Health & Human Svcs. Pub. No. 92-3091,28 (June 1992) (hereinafter “International Consensus Report”).
5 Estimate published by 3M Pharmaceuticals. See 3M International Ambassador, Sept. 1995,at 11.6 Figure based on information from IPAC members.7 NIAD Task Force Report, National Institute of Allergy and Infectious Diseases,PB-297601, Asthma and
the Other Allergic Diseases 10 (1979);see also Charles H. Feldman et al., “The Role of Health Education in Medical Management of Asthma:Some Program Applications,” 5 Clin.Rev. Allergy 195 (1987).
8 American Lung Association,Lung Disease Data 1996, at 3.9 Evelyn Zamula,“Childhood Asthma,”FDA Consumer (July 1990),at 10,citing John Updike, Self-
Consciousness (1989).10 American Lung Association,Lung Disease Data 1996, at 3.11 Global Initiative for Asthma, Global Strategy for Asthma Management and Prevention:NHLBI/WHO
Workshop Report,NHLBI Pub. No. 95-3659 (Jan.1995),at 120-21.12 March 1996 Report of the Technology and Economic Assessment Panel,at 11.13 American Lung Association, Lung Disease Data 1996, at 4.14 Id.15 Centers for Disease Control and Prevention 1996.16 Id. 5,167 deaths were recorded in 1993,as compared to 2,598 in 1979.17 “Asthma: An Epidemiological Overview,”Central Health Monitoring Unit Epidemiological Overview
Series, U.K.Dept. of Health (1995),at 2.18 Spray Technology & Marketing 26,63 (Sept.1995).19 “Asthma: An Epidemiological Overview,”supra,at 3,4. The mortality statistic cited is a three-year aver-
age based on data from the years 1990-1992.20 Statement by Dr. Nikoli Khaltaev, World Health Organization Expert (7 Dec. 1998 Press Release).21 World Health Organization, “Bronchial Asthma” Factsheet No. 206 (Dec.1998).22 International Consensus Report at vii.23 American Lung Association,Lung Disease Data 1996,at 14.24 Id.25 L. Fabbri,G.Caramori, et al., “COPD International Guidelines,”4 Pulmonary Medicine 76-84 (1998).26 World Health Report 1997.27 M.W. Higgins & T. Thorn,“Incidence, Prevalence and Mortality: Intra and Intercountry Differences”in
Clinical Epidemiology of Chronic Obstructive Pulmonary Diseases at 23-43 (M.J. Hensley & N.A.Saunders, eds. 1989).
28 American Lung Association, Lung Disease Data 1996,at 14.29 Id.30 N . M . Siafakas et al., “Optimal assessment and management of ch ronic obstru c t ive pulmonary disease
( CO P D ) , ” Consensus Sta tement of the European Respira t o ry Society (ERS ) , 8 Eur. R e s p i r. J. 1 3 9 8 , 1398 ( 1 9 9 5 ) .
31 International Consensus Report at 28.32 Global Strategy for Asthma Management and P revention,1995 National Institutes of Health and WHO
No. 95-3659.
Endnotes
33 Pocket Guide for Asthma Management and P revention, National Institutes of Health, Publication No. 96-3659B (1998 Revision).
34 International Consensus Report at xi.35 See Global Initiative for Asthma at http://www.ginasthma.com .36 The British Guidelines on Asthma Management,Thorax, Feb. 1998 Vol. 52 Supplement 1.37 The Expert Panel Report 2: Guidelines for the Diagnosis and Management of Asthma at
http://www.nhlbi.nih.gov/nhlbi/lung/asthma/prof/asthgdln.htm .38 See Global Obstructive Lung Disease (GOLD) Initiative at http://www.goldcopd.com .39 International Consensus Report at 28.40 The Global Strategy for Asthma Management and Prevention NHLBI/WHO Workshop Report (GSAMP)
at 80.41 Inhalation therapy is not limited to asthma and COPD. This form of therapy may be used in other respira-
tory disorders,including cystic fibrosis, bronchoiectasis,and airway irritability. It is also employed in the treatment of non-respiratory disorders, e.g.,for the delivery of medications whose oral bioavailability is extremely low, such as peptides.
42 See Pocket Guide for Asthma Management and Prevention.43 Id.44 Jay Grossman,"The Evolution of Inhaler Technology," 31 J. Asthma 55,57-58 (1994).45 A.J. Harrison et al., Presentation,"New Nebuliser Systems," Advances in Inhalation Therapy, IBC Technical
Services Ltd.,London (22-23 Feb. 1996).46 See W. Stahlhofen et al.,“Experimental determination of the regional deposition of aerosol particles in the
human respiratory tract,”41 (6) Am.Ind. Hyg. Assoc. J. 385,385-98 (1980).47 Grossman,supra, at 62.48 Id. at 61-62.49 World Health Organization, “Bronchodilators and Other Medications for the Treatment of Wheeze-
Associated Illnesses in Young Children” at 18,WHO/ARI/93.29 (1994).50 R.S.Stolarski & R.J. Cicerone, “Stratospheric Chlorine:A Possible Sink for Ozone,” 52 Can. J. Chem.
1610 (1974).51 Mario J. Molina & F.S.Rowland, “Stratospheric sink for chlorofluoromethanes: chlorine atom-catalyzed
destruction of ozone,” 249 Nature 810 (1974).52 Richard E.Benedick,Ozone Diplomacy: New Directions in Safeguarding the Planet 10-11 (1991).53 Id. at 44-45.54 Decision IV/25 of the Fourth Meeting of the Parties to the Mont real Protocol.55 Creation of expert panels to assess control measures is authorised by Article 6 of the Protocol.56 1993 Report of the Technology and Economic Assessment Panel,at 3-13.57 1994 Report of the Technology and Economic Assessment Panel,Executive Summary, at 1.58 April 1999 Report of the Technology and Economic Assessment Panel,at 162.59 See W. Stahlhofen et al.,supra,at 385-98. Other factors influencing dispersancy are the percent of the
propellant in the formulation;the valve type;the addition of low-boiling solvents to the formulation;and the amount of polymer or high viscosity ingredients.
60 The individual pressures of the CFCs at 20°C are as follows:CFC-11,-1.8 psi;CFC-12,67.6 psi;CFC-114,11.9 psi.
61 June 1996 Report of the Technology and Economic Assessment Panel. Part III:Update of the 1994 TOCAerosols Report and the MDI Transition Strategy, Executive Summary, at 1.
62 The discussion of this issue under the headings “Overview” and “The Choice of HFCs” draws onconversations in the spring of 1996 with Mr. Montfort A.Johnsen. For additional information on thedifficulty and complexity of identifying suitable MDI propellants,see, e.g.,M.J. Kontny et al.,“Issues Surrounding MDI Formulation Development with Non-CFC Propellants,”4 J. Aerosol Med. 181 (1991).
63 Appendix A contains a list of these compounds. The original list of 15,000 compounds was drawn from The Handbook of Chemistry and Physics (67th ed. 1986-87).
64 See Read, et al., “How Vehicle Pollution Affects Our Health,” Summary of papers presented at a symposiufor the Ashden Trust (May 1994).
65 Debora MacKenzie, “Europe cuts the chemicals that cause smog;agreement to cut emissions of volatile
organic compounds by 30 percent by 1999,”132 New Scientist No. 1797 at 15 (30 Nov. 1991).66 Testing to Extremes:Industry’s Cooperative Effort to Test the Health and Safety of Selected Fluorocarbon Alternatives to CFCs, PAFT (1995).67 Sixteen CFC manufacturers are members of PAFT: AlliedSignal Inc.(USA); Asahi Glass Co.,Ltd. ( Japan);
Ausimont S.p.A.(Italy);Central Glass Co. Ltd. (Japan);Daikin Industries Ltd. ( Japan);E.I. Du Pont de Nemours & Co., Inc.(USA);Elf Atochem SA (France);Elf Atochem N.A.Inc.(USA); Hankook Shinwha Co.,Ltd. (Republic of Korea); Hoechst AG(Germany); ICI Chemicals & Polymers Ltd. (UK);LaRoche Industries Inc.(USA); Rhône-Poulenc Chemicals Ltd.;Showa Denko KK(Japan);Solvay SA (Belgium);Solvay Fluor & Derivate GmbH (Germany).68 The term “Hydrofluoroalkane”(HFA) is used interchangeably with the term “Hydrofluorocarbon” (HFC).69 Committee for Proprietary Medicinal Products,“Result of the Co-ordinated Review of 1,1,1,2-Tetrafluoroethane HFC-134a,”13 July 1994;and Committee for Proprietary Medicinal Products,“Result of the Co-ordinated Review of 1,1,1,2,3,3,3,-heptafluoropropane (HFC-227),” 13 Sept.1995. IPACT-I and IPACT-II were asked to provide some further reassurance regardingpossible effects on bronchial hyperreactivity and nasal mucociliary clearance. Studies addressing these issues have been completed and cur-rently are undergoing review by European health authorities.70 IPAC industry survey (Nov. 1995).71 Id.72 The results of the joint studies are available from the United States National Technical Information Service (www.ntis.gov).73 BWJ Freund, B.Zierenberg, J. Eicher, & S. Dunne, “… A New Approach to Inhalation Therapy,” J. Aerosol Med. 10,246 (1997).74 SP Newman,KP Steed, SJ Reader, G. Hooper, & B. Zierenberg,“Efficient delivery to the lungs of flunisolide aerosol from a newportable hand-held multidose nebulizer,” J. Pharm. Science 85 (9),960-964 (1996); P. Iacono,E. Guemas, V. Leclerc, & JJ Thebault,“Cumulative dose response study comparing a new soft mist inhaler with a conventional metered dose inhaler (MDI) fordelivery of ipratropium bromide in patients with COPD,”1998 Int.Conf. of the American Thoracic Society (Chicago,24 -29 April 1998), Am. J. Respir. Crit.Care Med. 157 (3, Part 2), A800 (1998).75 Respiratory Drug Delivery VI,Biological,Pharmaceutical,Clinical and Regulatory Issues Relating to Optimized Drug Delivery by Aerosol, Hilton Head, South Carolina (May 3-7,1998), R. Dalby, P. Byron,& S. Farr, eds.,Interpharm Press, Inc.,at 83 and315.76 See Alec MacAndrew et al., “Alternative Technologies for Portable Inhalers,"”Management Forum Conference of Portable Inhalers,London (1 Dec.1994).77 Id.78 S. Palakodaty, P. York, & J. Pritchard, “Supercritical Fluid Processing from Aquaeous Solutions:the Application ofSEDS to Lactose as a Model Substance,”Pharmaceutical Research 1998:15(12);1835-1843.79 D. Edwards,et al., “Large Porous Particles for Pulmonary Drug Delivery,”276 Science 1868-1871 (1997).80 GH Ward, RK Schultz,& M. Hill,“Electromechanical Dispersion of Inhalation Powders: The Development of a Flow RateIndependent Dry Powder Inhaler,” Presentation at the Conference on Pharmaceutical Science and Technology, Chicago, Ill. (August,1996).81 Patent US 5469843.82 P. Grapel & D.J. Alexander, “CFC Replacements: Safety Testing, Approval for Use in Metered Dose Inhalers,”4 J. Aerosol Med. 193-200 (1991).83 An independent consulting report prepared for the European Commission concluded that: “Because of such an excessively slow product development cycle it is hard to envisage any significant market penetration of non-HFC propelled MDIs by 2010.” MarchConsulting Group Report at 24 (30 Sept.1998).84 ALA Lung Disease Data 1997,at 7. Now under intensive study are:the chemical reactions that take place in the asthmatic process;the nature of cell-cell communications; the way information is conveyed from one cell or type of cell to another; and the role of the tis-sue lining of the airways.85 International Consensus Report at 28.86 Executive Office of the President, Office of Science and Technology Policy, “Climate Change:State of Knowledge” at 2.87 Intergovernmental Panel on Climate Change, Working Group I,“Climate Change 1995,The Science of Climate Change,”at 4 (1996).88 Id. at 12.89 Derived from the Intergovernmental Panel on Climate Change, The Supplementary Report to the IPCC Scientific Assessment1992,at 91-92.90 IPAC projects that in the year 2010 total worldwide emissions from MDIs will be approximately 7,500 to 9,000 metric tonnes of HFCs, or 10.8 to 12.9 million metric tonnes of carbon dioxide equivalent (CDE).
In 1999,IPAC projected total worldwide HFC emissions from MDIs in the year 2010. Through a surveyof its members and reference to data assembled by a Montreal Protocol panel of experts,IPAC gatheredinformation concerning (i) the total number of MDI units manufactured worldwide by the entire MDIindustry in 1998;(ii) the average amount of HFC 134a and HFC 227 that will ultimately be contained ineach MDI unit;and (iii) estimated annual growth for the worldwide MDI market.
Based on this information, the total number of units that will be manufactured in the year 2010 was pro-
jected assuming (i) all CFC MDIs will be converted to HFC MDIs by 2010;and (ii) two annual MDI
market growth rate scenarios,1.5 percent and 3 percent. HFC emissions from MDIs in 2010 were calcu-
lated by multiplying the projected MDI unit data for 2010 by the average amount of HFC contained in
each MDI unit.In comparing the climate change effect of various greenhouse gases, carbon dioxide is used as the basis of com-parison. Each greenhouse gas is assigned a “global warming potential ” (GWP) over a given period of time to reflect its relative contribution as compared to carbon dioxide. HFC 134a has a 100 year GWP of 1300;HFC 227 has a 100 year GWP of 2900. Carbon dioxide equivalent emissions were calculated taking into account each MDI company’s use of HFC 134a versus HFC 227.
Based on 1992 IPCC emission scenarios,it has been projected that total emissions of all greenhouse gases worldwide will be approximately 59 billion tonnes of carbon dioxide equivalent. HFC emissions from MDIs in the year 2010 are projected to be no more than 0.02 percent of the total impact from all greenhouse gases.
91 A 100 year time horizon is assumed.

51
Appendix A
During the preparation of this Paper, a study was conducted to determinewhether any compounds other than HFCs could be identified as promising CFCalternatives for MDI usage. The study focused on a list of 15,000 compoundsdrawn from The Handbook of Chemistry and Physics (67th ed. 1986-1987).Compounds that did not possess a boiling point in the chosen range (-100° to+30°C) were eliminated from consideration. This range is believed to include allcompounds with acceptable vapour pressures for MDI usage. Elimination ofcompounds with boiling points that were either too high or too low left approxi-mately 180 compounds for further study. These compounds are shown in thetable below. Characteristics that disqualify a compound from usage as an MDIpropellant are noted in the right-hand column.
A rev i ew of this table demon s t rates that none of the studied compounds (with the exc e p t i on of HFCs) now appears to be a promising substitute for CFCp ro p e llants in MDIs.
The terms “flammable” and “reactive” are used in the table as follows:
“Flammable”: The compound forms an explosive mixture in air.
“R e a c ti ve” : The compound contains a functional group or groups that can easily be converted through oxidation, reduction, hydrolysis, etc.to another compound, or are capable of being polymerised to a solid or a liquid. Examples of these functional groups are CHO;COX where X=Cl, Br, or S; CN; NO; C=C; and C[C.
This study was conducted by Dr. John J. Daly, Jr., a contributor in the preparationof this Paper.
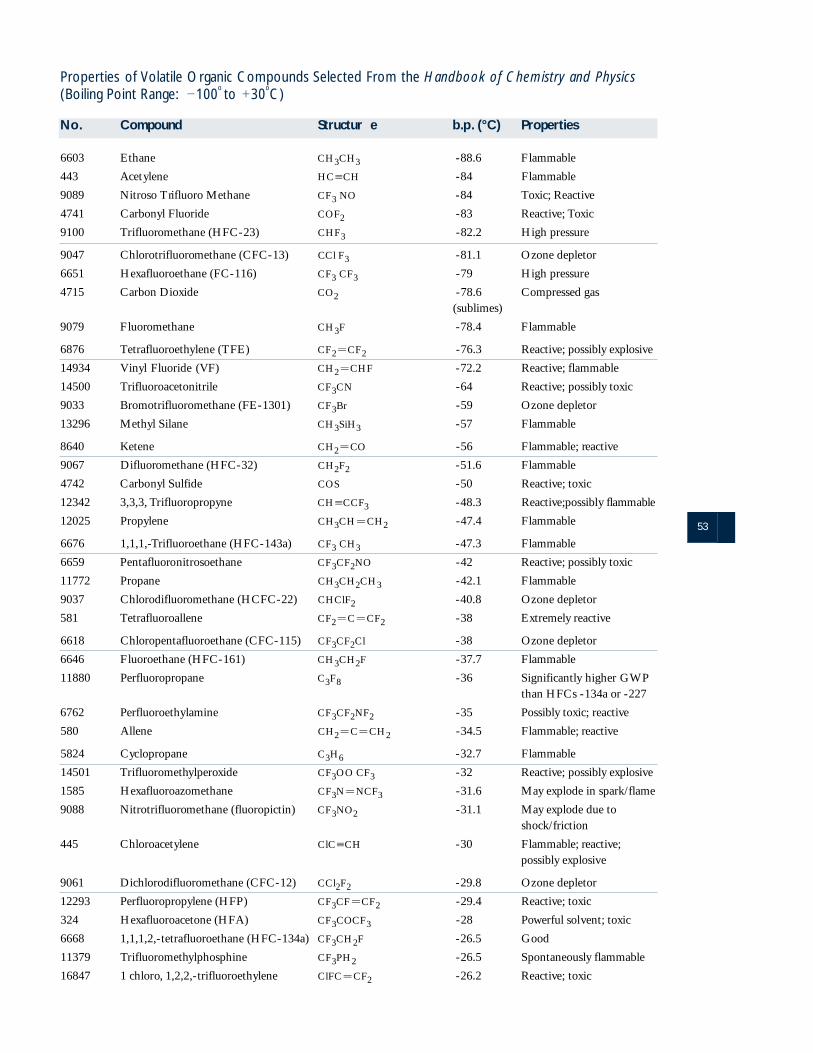
53
Properties of Volatile Organic Compounds Selected From the Handbook of Chemistry and Physics(Boiling Point Range: 2100
oto 130
oC)
No. Compound Structur e b.p . (°C) Properties
6603 Ethane CH3CH3 -88.6 Flammable
443 Acetylene HC[CH -84 Flammable
9089 Nitroso Trifluoro Methane CF3 NO -84 Toxic; Reactive
4741 Carbonyl Fluoride COF2 -83 Reactive; Toxic
9100 Trifluoromethane (HFC-23) CHF3 -82.2 High pressure
9047 Chlorotrifluoromethane (CFC-13) CCl F3 -81.1 Ozone depletor
6651 Hexafluoroethane (FC-116) CF3 CF3 -79 High pressure
4715 Carbon Dioxide CO2 -78.6 Compressed gas(sublimes)
9079 Fluoromethane CH3F -78.4 Flammable
6876 Tetrafluoroethylene (TFE) CF25CF2 -76.3 Reactive; possibly explosive
14934 Vinyl Fluoride (VF) CH25CHF -72.2 Reactive; flammable
14500 Trifluoroacetonitrile CF3CN -64 Reactive; possibly toxic
9033 Bromotrifluoromethane (FE-1301) CF3Br -59 Ozone depletor
13296 Methyl Silane CH3SiH3 -57 Flammable
8640 Ketene CH25CO -56 Flammable; reactive
9067 Difluoromethane (HFC-32) CH2F2 -51.6 Flammable
4742 Carbonyl Sulfide COS -50 Reactive; toxic
12342 3,3,3, Trifluoropropyne CH[CCF3 -48.3 R e a c t i ve ;p o s s i b ly flammable
12025 Propylene CH3CH5CH2 -47.4 Flammable
6676 1,1,1,-Trifluoroethane (HFC-143a) CF3 CH3 -47.3 Flammable
6659 Pentafluoronitrosoethane CF3CF2NO -42 Reactive; possibly toxic
11772 Propane CH3CH2CH3 -42.1 Flammable
9037 Chlorodifluoromethane (HCFC-22) CHClF2 -40.8 Ozone depletor
581 Tetrafluoroallene CF25C5CF2 -38 Extremely reactive
6618 Chloropentafluoroethane (CFC-115) CF3CF2Cl -38 Ozone depletor
6646 Fluoroethane (HFC-161) CH3CH2F -37.7 Flammable
11880 Perfluoropropane C3F8 -36 Significantly higher GWP than HFCs -134a or -227
6762 Perfluoroethylamine CF3CF2NF2 -35 Possibly toxic; reactive
580 Allene CH25C5CH2 -34.5 Flammable; reactive
5824 Cyclopropane C3H6 -32.7 Flammable
14501 Trifluoromethylperoxide CF3OO CF3 -32 Reactive; possibly explosive
1585 Hexafluoroazomethane CF3N5NCF3 -31.6 May explode in spark/flame
9088 Nitrotrifluoromethane (fluoropictin) CF3NO2 -31.1 May explode due to shock/friction
445 Chloroacetylene ClC[CH -30 Flammable; reactive;possibly explosive
9061 Dichlorodifluoromethane (CFC-12) CCl2F2 -29.8 Ozone depletor
12293 Perfluoropropylene (HFP) CF3CF5CF2 -29.4 Reactive; toxic
324 Hexafluoroacetone (HFA) CF3COCF3 -28 Powerful solvent; toxic
6668 1,1,1,2,-tetrafluoroethane (HFC-134a) CF3CH2F -26.5 Good
11379 Trifluoromethylphosphine CF3PH2 -26.5 Spontaneously flammable
16847 1 chloro, 1,2,2,-trifluoroethylene ClFC5CF2 -26.2 Reactive; toxic
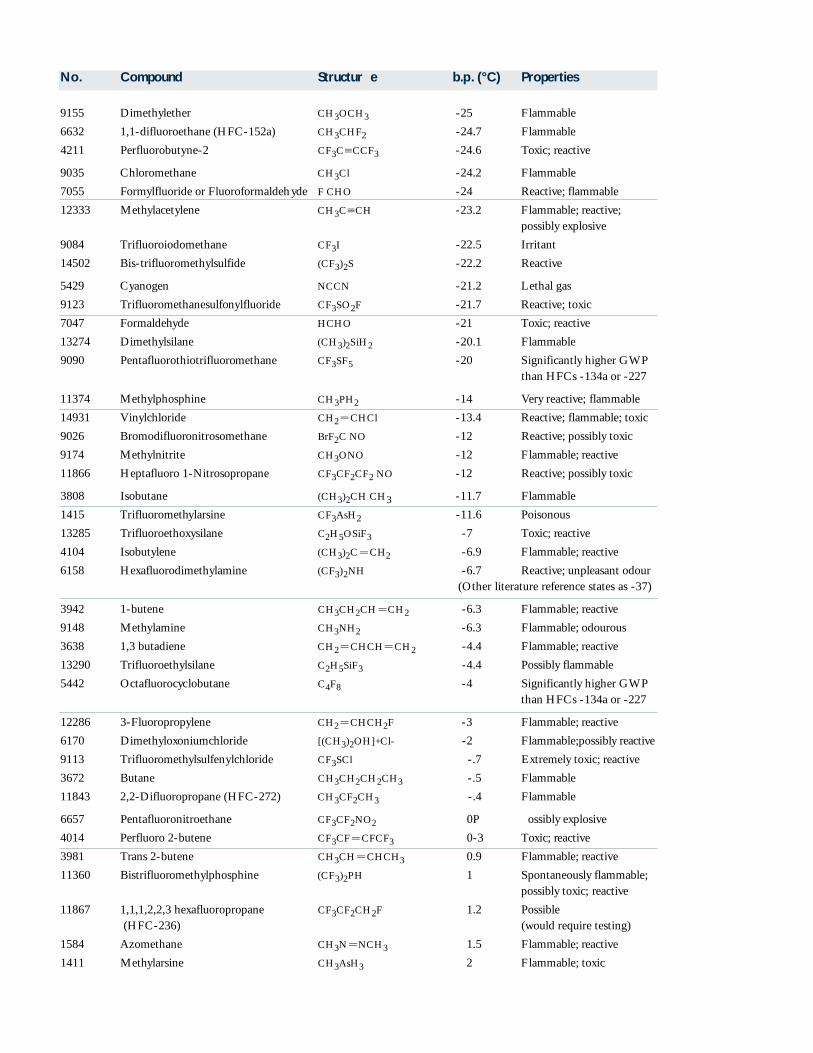
No. Compound Structur e b.p . (°C) Properties
9155 Dimethylether CH3OCH3 -25 Flammable
6632 1,1-difluoroethane (HFC-152a) CH3CHF2 -24.7 Flammable
4211 Perfluorobutyne-2 CF3C[CCF3 -24.6 Toxic; reactive
9035 Chloromethane CH3Cl -24.2 Flammable
7055 Formylfluoride or Fluoroformaldehyde F CHO -24 Reactive; flammable
12333 Methylacetylene CH3C[CH -23.2 Flammable; reactive;possibly explosive
9084 Trifluoroiodomethane CF3I -22.5 Irritant
14502 Bis-trifluoromethylsulfide (CF3)2S -22.2 Reactive
5429 Cyanogen NCCN -21.2 Lethal gas
9123 Trifluoromethanesulfonylfluoride CF3SO2F -21.7 Reactive; toxic
7047 Formaldehyde HCHO -21 Toxic; reactive
13274 Dimethylsilane (CH3)2SiH2 -20.1 Flammable
9090 Pentafluorothiotrifluoromethane CF3SF5 -20 Significantly higher GWP than HFCs -134a or -227
11374 Methylphosphine CH3PH2 -14 Very reactive; flammable
14931 Vinylchloride CH25CHCl -13.4 Reactive; flammable; toxic
9026 Bromodifluoronitrosomethane BrF2C NO -12 Reactive; possibly toxic
9174 Methylnitrite CH3ONO -12 Flammable; reactive
11866 Heptafluoro 1-Nitrosopropane CF3CF2CF2 NO -12 Reactive; possibly toxic
3808 Isobutane (CH3)2CH CH3 -11.7 Flammable
1415 Trifluoromethylarsine CF3AsH2 -11.6 Poisonous
13285 Trifluoroethoxysilane C2H5OSiF3 -7 Toxic; reactive
4104 Isobutylene (CH3)2C5CH2 -6.9 Flammable; reactive
6158 Hexafluorodimethylamine (CF3)2NH -6.7 Reactive; unpleasant odour(Other literature reference states as -37)
3942 1-butene CH3CH2CH5CH2 -6.3 Flammable; reactive
9148 Methylamine CH3NH2 -6.3 Flammable; odourous
3638 1,3 butadiene CH25CHCH5CH2 -4.4 Flammable; reactive
13290 Trifluoroethylsilane C2H5SiF3 -4.4 Possibly flammable
5442 Octafluorocyclobutane C4F8 -4 Significantly higher GWPthan HFCs -134a or -227
12286 3-Fluoropropylene CH25CHCH2F -3 Flammable; reactive
6170 Dimethyloxoniumchloride [(CH3)2OH]+Cl- -2 Fl a m m a b l e ;p o s s i b ly re a c t i ve
9113 Trifluoromethylsulfenylchloride CF3SCl -.7 Extremely toxic; reactive
3672 Butane CH3CH2CH2CH3 -.5 Flammable
11843 2,2-Difluoropropane (HFC-272) CH3CF2CH3 -.4 Flammable
6657 Pentafluoronitroethane CF3CF2NO2 0 Possibly explosive
4014 Perfluoro 2-butene CF3CF5CFCF3 0-3 Toxic; reactive
3981 Trans 2-butene CH3CH5CHCH3 0.9 Flammable; reactive
11360 Bistrifluoromethylphosphine (CF3)2PH 1 Spontaneously flammable;possibly toxic; reactive
11867 1,1,1,2,2,3 hexafluoropropane CF3CF2CH2F 1.2 Possible (HFC-236) (would require testing)
1584 Azomethane CH3N5NCH3 1.5 Flammable; reactive
1411 Methylarsine CH3AsH3 2 Flammable; toxic
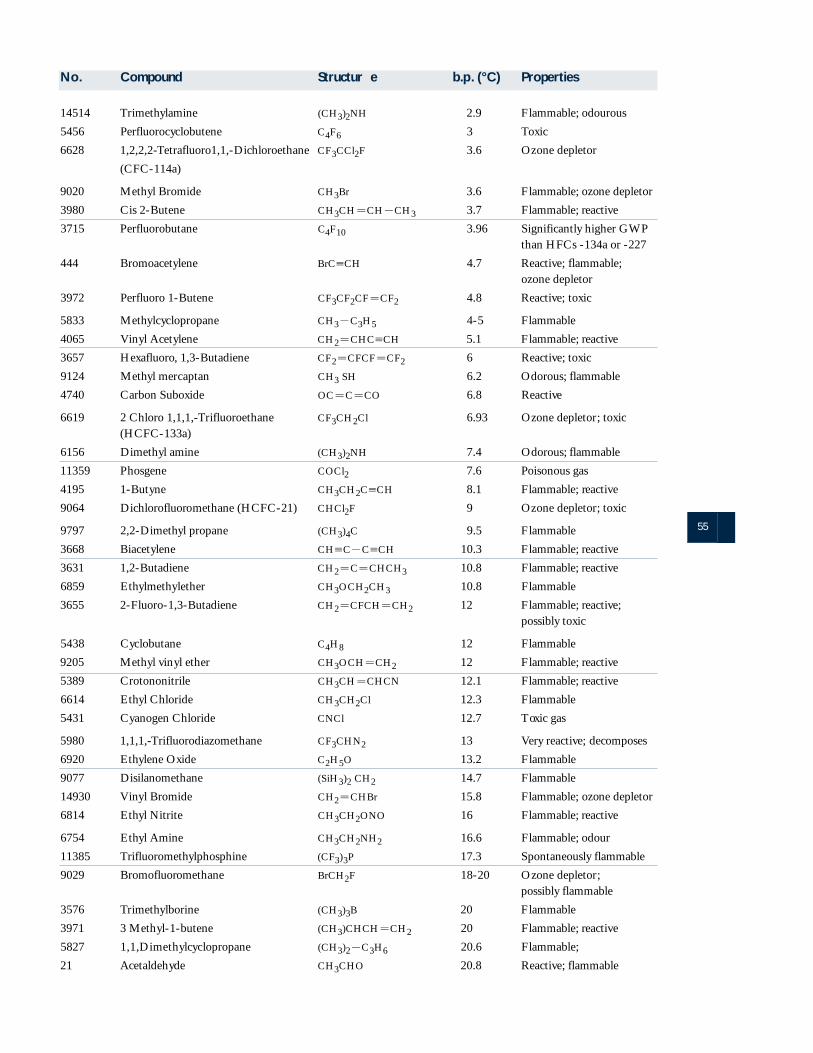
55
No. Compound Structur e b.p . (°C) Properties
14514 Trimethylamine (CH3)2NH 2.9 Flammable; odourous
5456 Perfluorocyclobutene C4F6 3 Toxic
6628 1,2,2,2-Tetrafluoro1,1,-Dichloroethane CF3CCl2F 3.6 Ozone depletor
(CFC-114a)
9020 Methyl Bromide CH3Br 3.6 Flammable; ozone depletor
3980 Cis 2-Butene CH3CH5CH2CH3 3.7 Flammable; reactive
3715 Perfluorobutane C4F10 3.96 Significantly higher GWPthan HFCs -134a or -227
444 Bromoacetylene BrC[CH 4.7 Reactive; flammable;ozone depletor
3972 Perfluoro 1-Butene CF3CF2CF5CF2 4.8 Reactive; toxic
5833 Methylcyclopropane CH32C3H5 4-5 Flammable
4065 Vinyl Acetylene CH25CHC[CH 5.1 Flammable; reactive
3657 Hexafluoro, 1,3-Butadiene CF25CFCF5CF2 6 Reactive; toxic
9124 Methyl mercaptan CH3 SH 6.2 Odorous; flammable
4740 Carbon Suboxide OC5C5CO 6.8 Reactive
6619 2 Chloro 1,1,1,-Trifluoroethane CF3CH2Cl 6.93 Ozone depletor; toxic(HCFC-133a)
6156 Dimethyl amine (CH3)2NH 7.4 Odorous; flammable
11359 Phosgene COCl2 7.6 Poisonous gas
4195 1-Butyne CH3CH2C[CH 8.1 Flammable; reactive
9064 Dichlorofluoromethane (HCFC-21) CHCl2F 9 Ozone depletor; toxic
9797 2,2-Dimethyl propane (CH3)4C 9.5 Flammable
3668 Biacetylene CH[C2C[CH 10.3 Flammable; reactive
3631 1,2-Butadiene CH25C5CHCH3 10.8 Flammable; reactive
6859 Ethylmethylether CH3OCH2CH3 10.8 Flammable
3655 2-Fluoro-1,3-Butadiene CH25CFCH5CH2 12 Flammable; reactive;possibly toxic
5438 Cyclobutane C4H8 12 Flammable
9205 Methyl vinyl ether CH3OCH5CH2 12 Flammable; reactive
5389 Crotononitrile CH3CH5CHCN 12.1 Flammable; reactive
6614 Ethyl Chloride CH3CH2Cl 12.3 Flammable
5431 Cyanogen Chloride CNCl 12.7 Toxic gas
5980 1,1,1,-Trifluorodiazomethane CF3CHN2 13 Very reactive; decomposes
6920 Ethylene Oxide C2H5O 13.2 Flammable
9077 Disilanomethane (SiH3)2 CH2 14.7 Flammable
14930 Vinyl Bromide CH25CHBr 15.8 Flammable; ozone depletor
6814 Ethyl Nitrite CH3CH2ONO 16 Flammable; reactive
6754 Ethyl Amine CH3CH2NH2 16.6 Flammable; odour
11385 Trifluoromethylphosphine (CF3)3P 17.3 Spontaneously flammable
9029 Bromofluoromethane BrCH2F 18-20 Ozone depletor;possibly flammable
3576 Trimethylborine (CH3)3B 20 Flammable
3971 3 Methyl-1-butene (CH3)CHCH5CH2 20 Flammable; reactive
5827 1,1,Dimethylcyclopropane (CH3)22C3H6 20.6 Flammable;
21 Acetaldehyde CH3CHO 20.8 Reactive; flammable
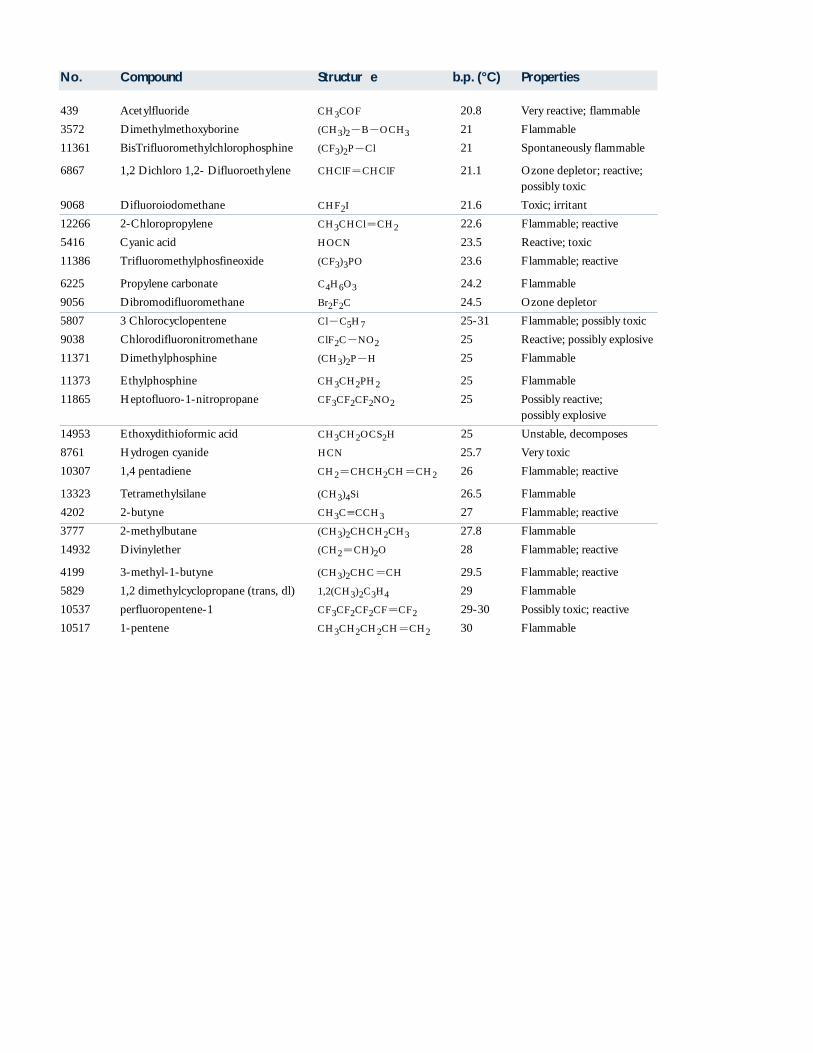
439 Acetylfluoride CH3COF 20.8 Very reactive; flammable
3572 Dimethylmethoxyborine (CH3)22B2OCH3 21 Flammable
11361 BisTrifluoromethylchlorophosphine (CF3)2P2Cl 21 Spontaneously flammable
6867 1,2 Dichloro 1,2- Difluoroethylene CHClF5CHClF 21.1 Ozone depletor; reactive;possibly toxic
9068 Difluoroiodomethane CHF2I 21.6 Toxic; irritant
12266 2-Chloropropylene CH3CHCl5CH2 22.6 Flammable; reactive
5416 Cyanic acid HOCN 23.5 Reactive; toxic
11386 Trifluoromethylphosfineoxide (CF3)3PO 23.6 Flammable; reactive
6225 Propylene carbonate C4H6O3 24.2 Flammable
9056 Dibromodifluoromethane Br2F2C 24.5 Ozone depletor
5807 3 Chlorocyclopentene Cl2C5H7 25-31 Flammable; possibly toxic
9038 Chlorodifluoronitromethane ClF2C2NO2 25 Reactive; possibly explosive
11371 Dimethylphosphine (CH3)2P2H 25 Flammable
11373 Ethylphosphine CH3CH2PH2 25 Flammable
11865 Heptofluoro-1-nitropropane CF3CF2CF2NO2 25 Possibly reactive;possibly explosive
14953 Ethoxydithioformic acid CH3CH2OCS2H 25 Unstable, decomposes
8761 Hydrogen cyanide HCN 25.7 Very toxic
10307 1,4 pentadiene CH25CHCH2CH5CH2 26 Flammable; reactive
13323 Tetramethylsilane (CH3)4Si 26.5 Flammable
4202 2-butyne CH3C[CCH3 27 Flammable; reactive
3777 2-methylbutane (CH3)2CHCH2CH3 27.8 Flammable
14932 Divinylether (CH25CH)2O 28 Flammable; reactive
4199 3-methyl-1-butyne (CH3)2CHC5CH 29.5 Flammable; reactive
5829 1,2 dimethylcyclopropane (trans, dl) 1,2(CH3)2C3H4 29 Flammable
10537 perfluoropentene-1 CF3CF2CF2CF5CF2 29-30 Possibly toxic; reactive
10517 1-pentene CH3CH2CH2CH5CH2 30 Flammable
No. Compound Structur e b.p . (°C) Properties





























