Embed Size (px)
Citation preview
The Lab's the Thing - What you should know about the clinical embryology lab
before signing a contract.
Richard T. Scott, Jr, MD, HCLDProfessor and Director, Reproductive Endocrinology
Robert Wood Johnson Medical SchoolClinical and Scientific Director,
Reproductive Medicine Associates of New Jersey
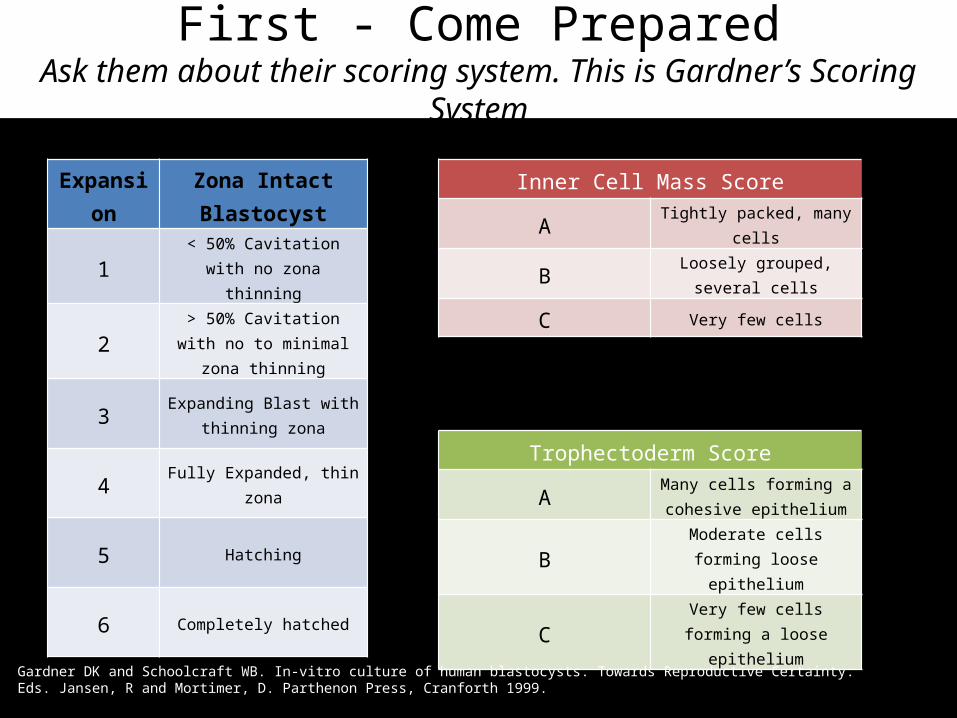
First - Come PreparedAsk them about their scoring system. This is Gardner’s Scoring System
Expansion Zona Intact Blastocyst
1 < 50% Cavitation with no zona thinning
2 > 50% Cavitation with no to minimal zona thinning
3 Expanding Blast with thinning zona
4 Fully Expanded, thin zona
5 Hatching
6 Completely hatched
Inner Cell Mass Score
A Tightly packed, many cells
B Loosely grouped, several cells
C Very few cells
Trophectoderm Score
A Many cells forming a cohesive epithelium
B Moderate cells forming loose epithelium
C Very few cells forming a loose epithelium
Gardner DK and Schoolcraft WB. In-vitro culture of human blastocysts. Towards Reproductive Certainty. Eds. Jansen, R and Mortimer, D. Parthenon Press, Cranforth 1999.
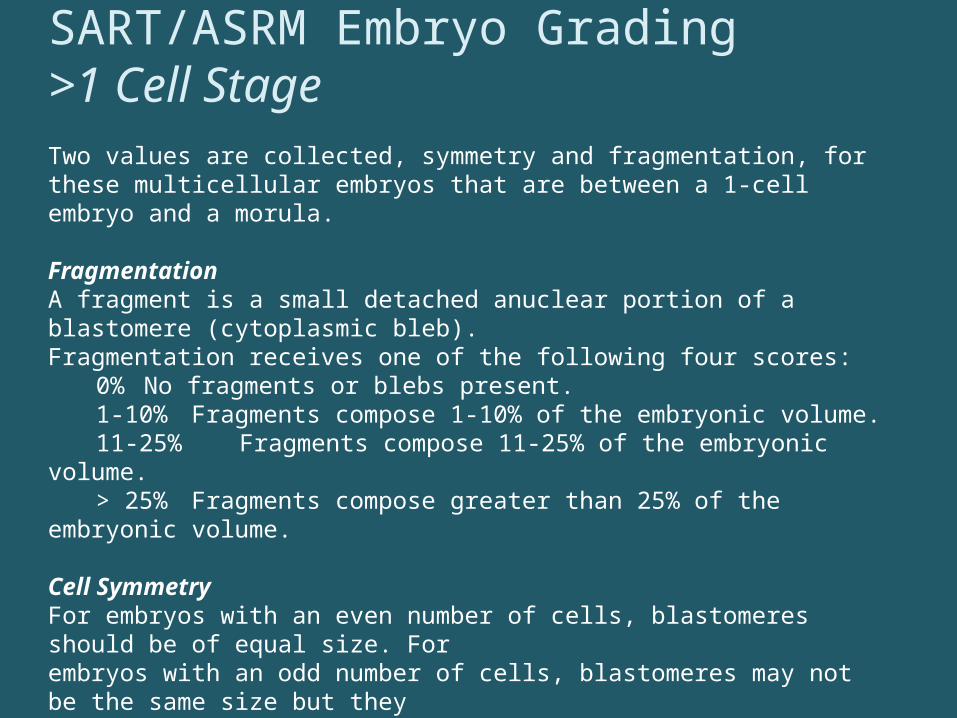
SART/ASRM Embryo Grading>1 Cell Stage Two values are collected, symmetry and fragmentation, for these multicellular embryos that are between a 1-cell embryo and a morula. Fragmentation A fragment is a small detached anuclear portion of a blastomere (cytoplasmic bleb). Fragmentation receives one of the following four scores:
0% No fragments or blebs present. 1-10% Fragments compose 1-10% of the embryonic volume. 11-25% Fragments compose 11-25% of the embryonic volume. > 25% Fragments compose greater than 25% of the embryonic volume.
Cell Symmetry For embryos with an even number of cells, blastomeres should be of equal size. For embryos with an odd number of cells, blastomeres may not be the same size but they should be of the appropriate size for their cleavage status.
Perfect All blastomeres are of the appropriate size and shape. Moderate 0-20% of the blastomeres are not of the appropriate size and
shape. Severe >20% of the blastomeres are not of the appropriate size and shape.
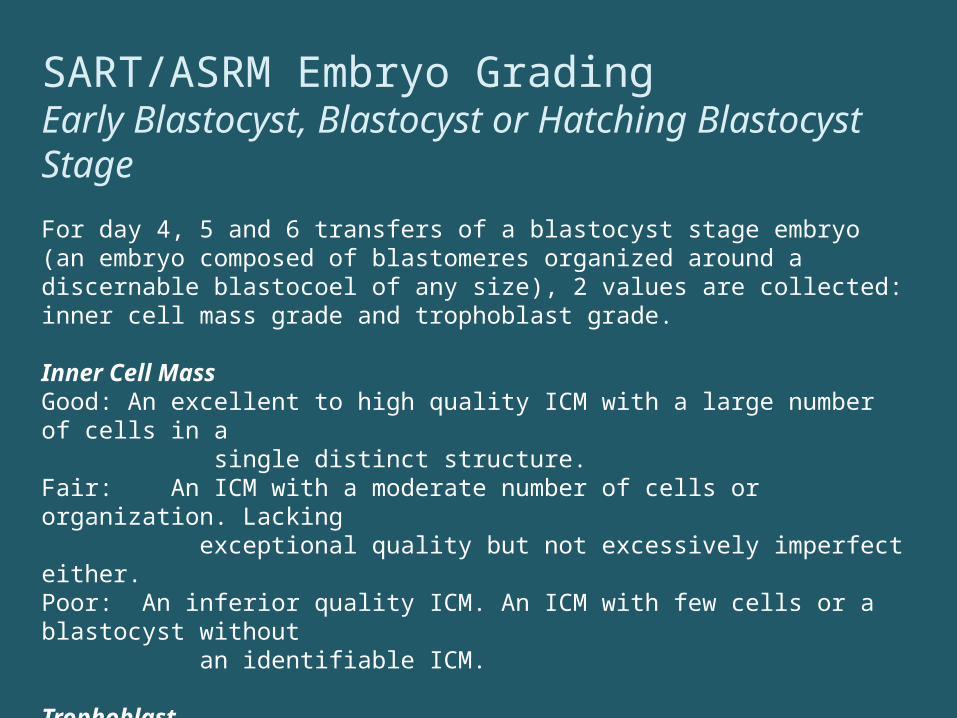
SART/ASRM Embryo GradingEarly Blastocyst, Blastocyst or Hatching Blastocyst Stage
For day 4, 5 and 6 transfers of a blastocyst stage embryo (an embryo composed of blastomeres organized around a discernable blastocoel of any size), 2 values are collected: inner cell mass grade and trophoblast grade. Inner Cell Mass Good: An excellent to high quality ICM with a large number of cells in a single distinct structure. Fair: An ICM with a moderate number of cells or organization. Lacking exceptional quality but not excessively imperfect either. Poor: An inferior quality ICM. An ICM with few cells or a blastocyst without an identifiable ICM.
Trophoblast Good: An excellent to high quality trophoblast with a large continuous and uniform layer of cells in a single distinct structure. Fair: A moderate number of cells that may have variable size and shape. Poor: An inferior quality trophoblast with few cells or gaps (non-contiguous areas)
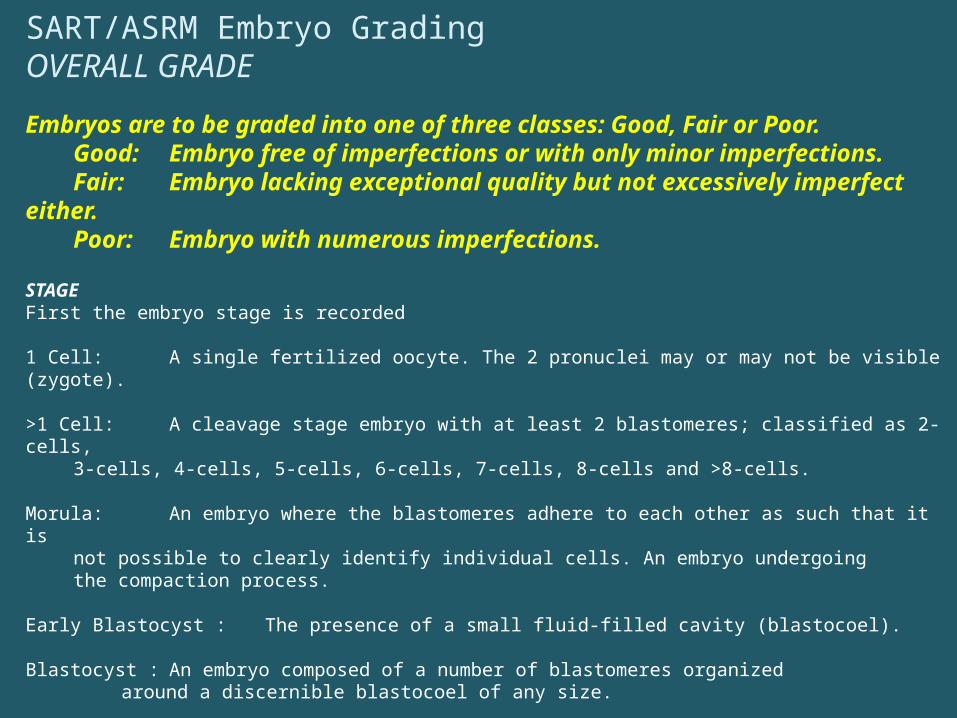
SART/ASRM Embryo GradingOVERALL GRADE
Embryos are to be graded into one of three classes: Good, Fair or Poor. Good: Embryo free of imperfections or with only minor imperfections. Fair: Embryo lacking exceptional quality but not excessively imperfect either. Poor: Embryo with numerous imperfections.
STAGE First the embryo stage is recorded
1 Cell: A single fertilized oocyte. The 2 pronuclei may or may not be visible (zygote).
>1 Cell: A cleavage stage embryo with at least 2 blastomeres; classified as 2-cells, 3-cells, 4-cells, 5-cells, 6-cells, 7-cells, 8-cells and >8-cells.
Morula: An embryo where the blastomeres adhere to each other as such that it is not possible to clearly identify individual cells. An embryo undergoing the compaction process.
Early Blastocyst : The presence of a small fluid-filled cavity (blastocoel).
Blastocyst : An embryo composed of a number of blastomeres organizedaround a discernible blastocoel of any size.
Hatching Blastocyst : Embryo partially or completely free of the zona pellucida. The embryo is composed of trophectoderm and inner cell mass cells and has a large expanded blastocoel

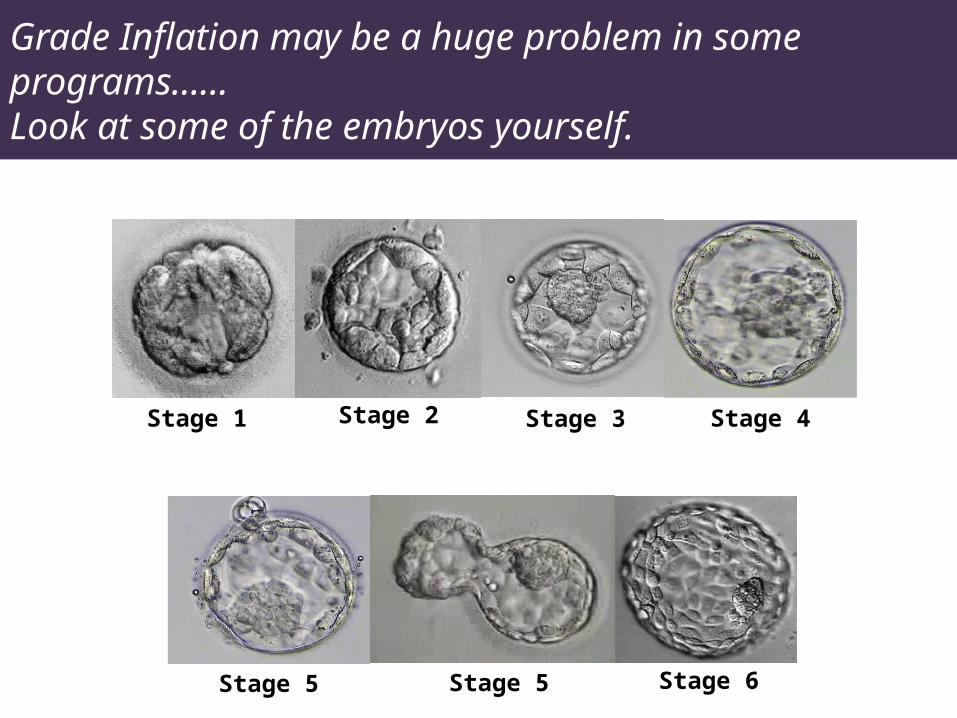
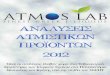
Grade Inflation may be a huge problem in some programs……Look at some of the embryos yourself.
Stage 1 Stage 2 Stage 3 Stage 4
Stage 5 Stage 5 Stage 6

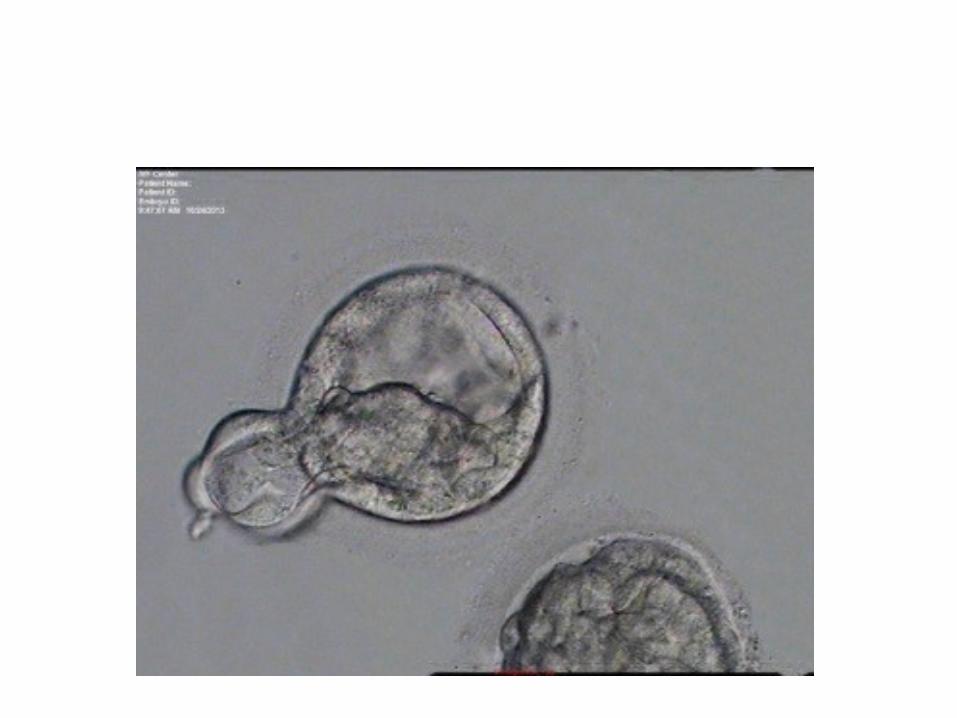




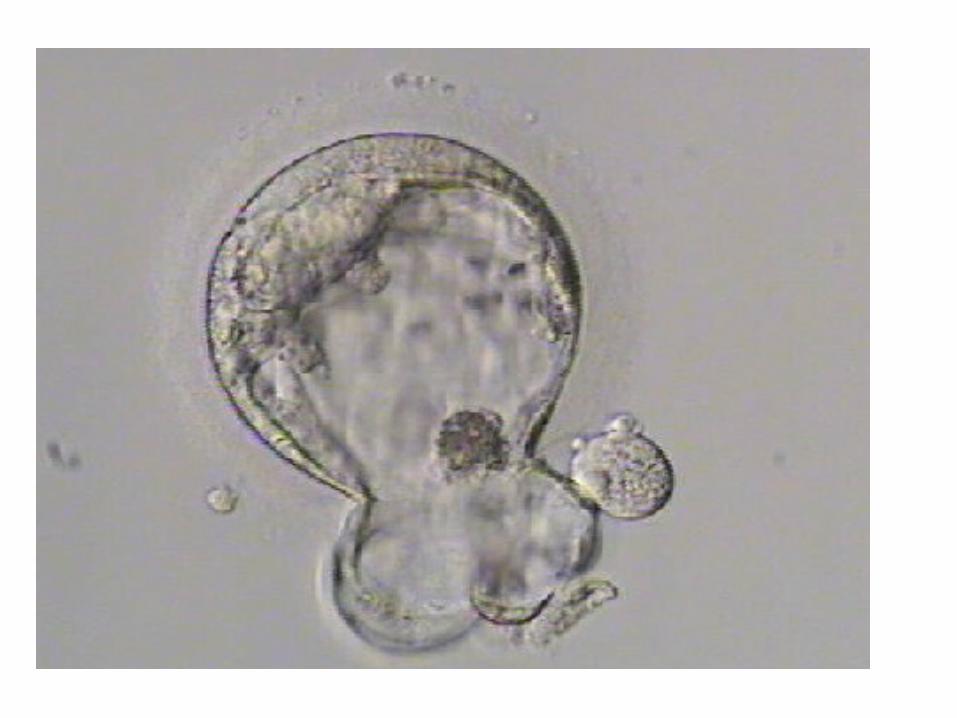





All of those were called 4BB’s
How can the laboratory help you build your practice?
• What do all young physicians lack when they start building their practice out of fellowship?
• Credibility– Some comes from the institution – but that tends to see
the patients migrate to the more established physicians– Leverage the lab
• World class care available through you equal to all others• Distinguishes you prior to have a track record
• Great labs = great outcomes– No questions that patients follow outcomes..

Do patients track rates?
www.fertilitysuccessrates.com

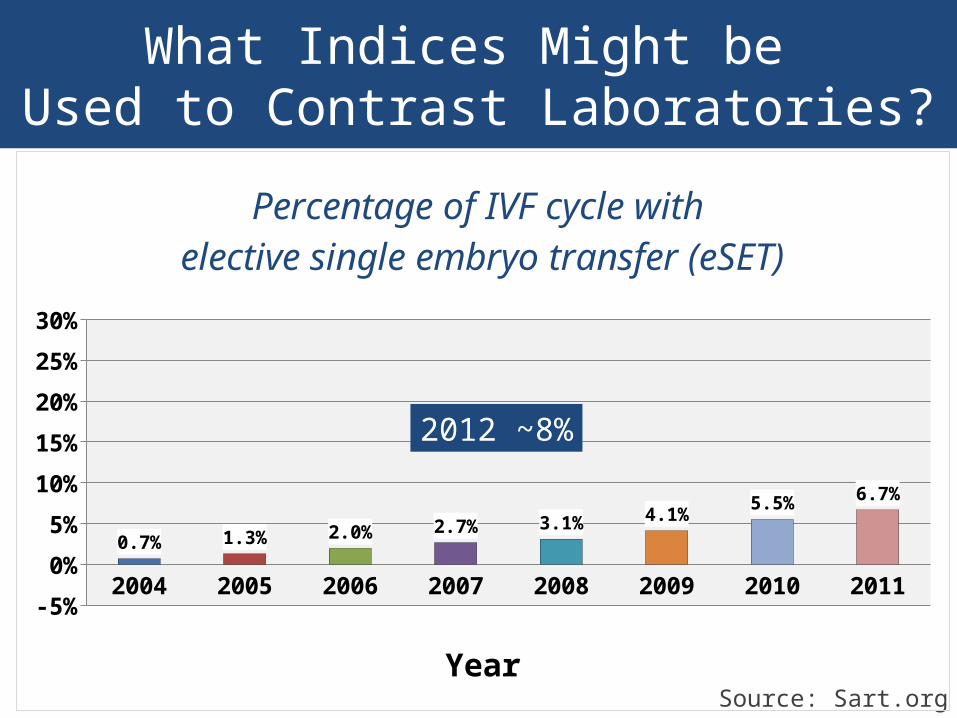
What Indices Might be Used to Contrast Laboratories?
Stage of Transfer
What Indices Might be Used to Contrast Laboratories?
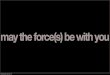
Source: Sart.org
2004 2005 2006 2007 2008 2009 2010 2011-5%
0%
5%
10%
15%
20%
25%
30%
0.7% 1.3% 2.0% 2.7% 3.1% 4.1%5.5% 6.7%
Percentage of IVF cycle with elective single embryo transfer (eSET)
Year
2012 ~8%
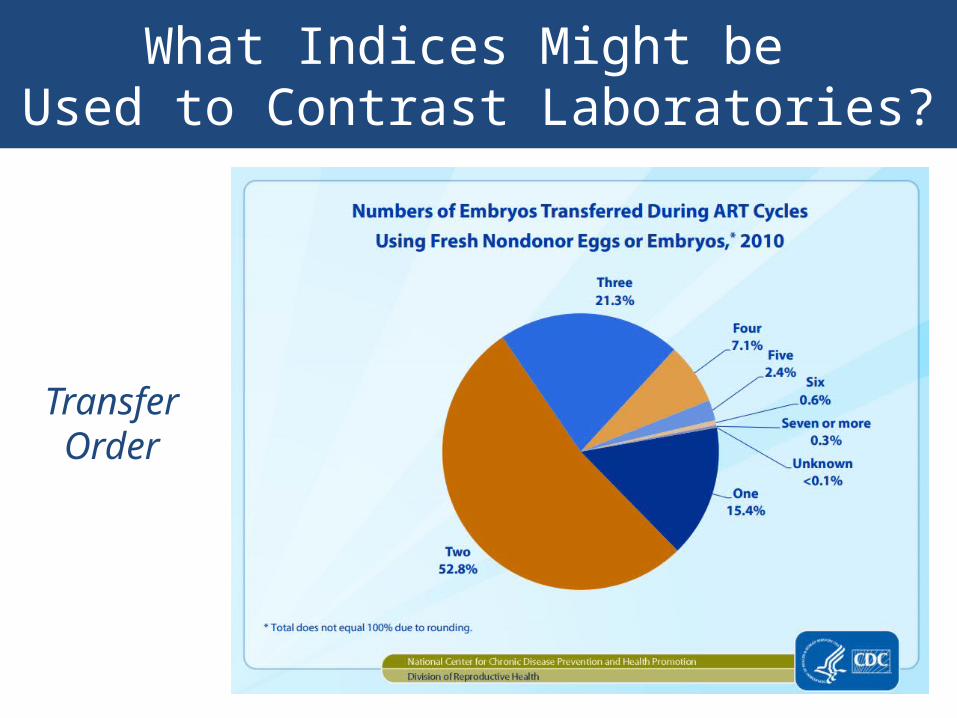
What Indices Might be Used to Contrast Laboratories?
TransferOrder
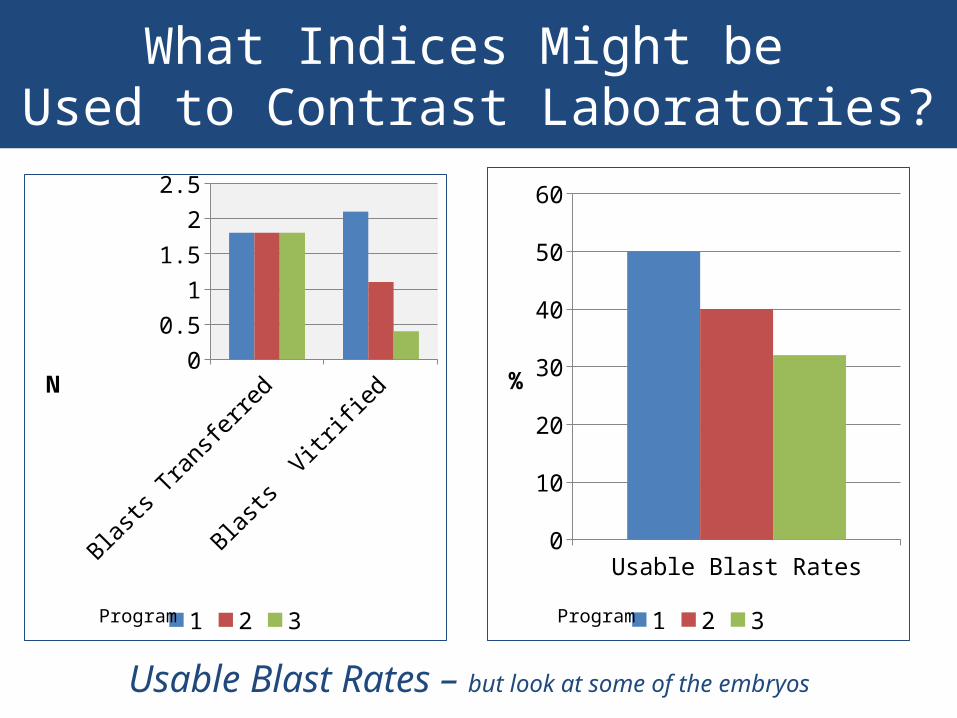
What Indices Might be Used to Contrast Laboratories?
Blasts
Transfe
rred
Blasts
Vitrified
0
0.5
1
1.5
2
2.5
1 2 3
N
Usable Blast Rates0
10
20
30
40
50
60
1 2 3
%
ProgramProgram
Usable Blast Rates – but look at some of the embryos
What Indices Might be Used to Contrast Laboratories?
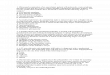
1 2 3 4 50
10
20
30
40
50
60
Program
Sust
aine
d Im
plan
tatio
n Ra
te (%
)
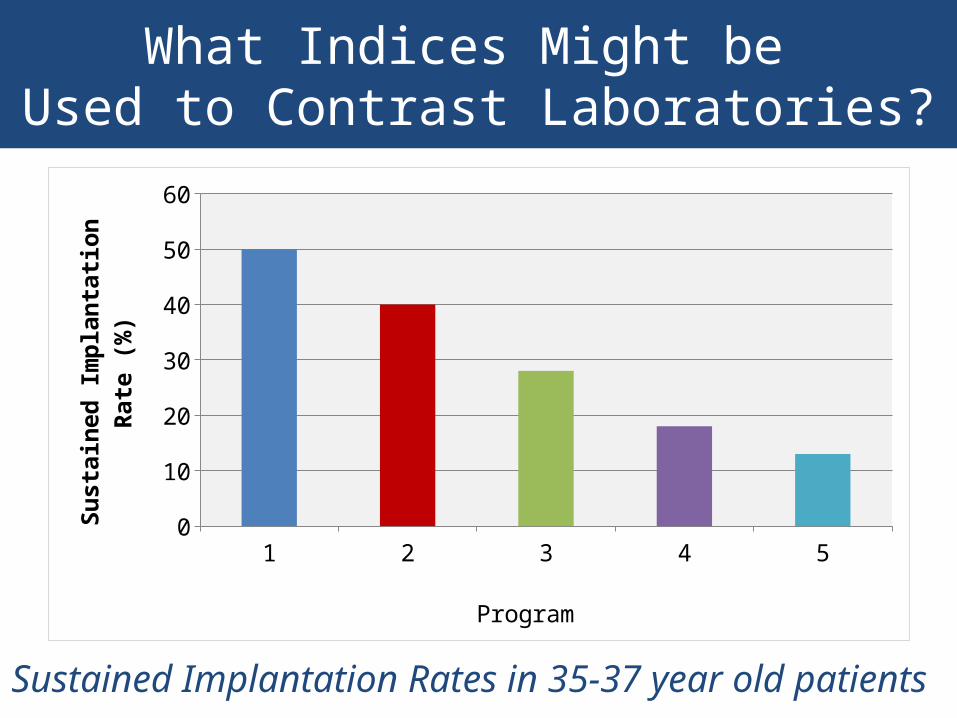
Sustained Implantation Rates in 35-37 year old patients
What Indices Might be Used to Contrast Laboratories?
Staffing Ratios
versus
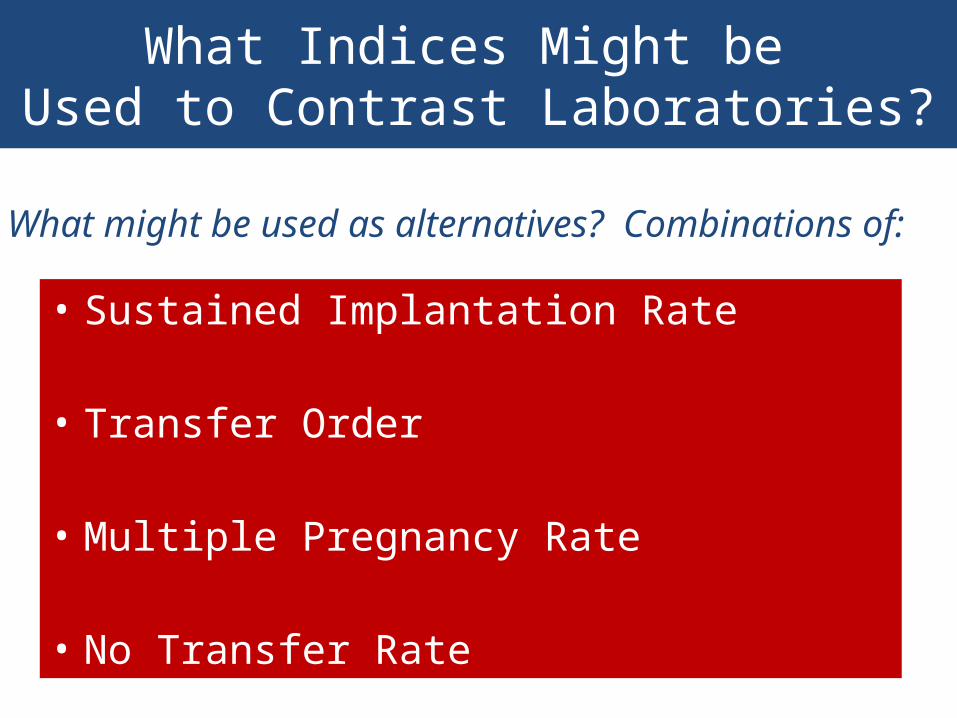
What Indices Might be Used to Contrast Laboratories?
• Sustained Implantation Rate
• Transfer Order
• Multiple Pregnancy Rate
• No Transfer Rate
What might be used as alternatives? Combinations of:
What Indices Might be Used to Contrast Laboratories?
• Most people contrast the youngest easiest patients
• May be compensated for by increased transfer order
• Does not consider the quality of the outcome
Pregnancy Rates are not as helpful…
Embracing New Technologies
InadequateLH
Too Fast:Adopts Unvalidated Tests with
Insufficient Evidence
Too Slow:Patients lose access to
beneficial adjuncts and program is less competitive
What is the Quality of the Interactions Between the Physicians and the Embryologists?
• Do they communicate openly about cases?
• Is “the lab” treated like a peer?– Not necessarily a business peer– Still, a clinical peer
• What type of data are reported back to the clinical program?
• What type of data are released to the patients?
What is the Quality of the Interactions Between the Physicians and the Embryologists?
How much does the clinical team know
about the lab?
Are you likely to have a voice in future decisions?

Things which may be less important in contrasting labs…
• Which media system is in use?
• Which incubators are used?
• Nature of proficiency testing?
• Academic credentials of the laboratory director

Ask to Spend a Day in the Embryology Lab
The Clinical Embryology Team