Embed Size (px)
Citation preview

The Learning Curve for the Laparoscopic Approachfor Colorectal Cancer: A Single Institution’s Experience
Gang Chen, MSc,1,* Zheng Liu, MD,2,* Peng Han, MSc,1 Jing-Wen Li, MSc,1 and Bin-Bin Cui, MD1
Abstract
Background: The purpose of this study was to evaluate the learning curve of the laparoscopic approach forcolorectal cancer and generate a focused training program for more junior surgeons.Subjects and Methods: This study analyzed data from 100 consecutive laparoscopic surgeries for colorectalcancer between January 2009 and July 2010. The learning curve was compared between the first 50 surgeries(study group 1) and the subsequent 50 surgeries (study group 2).Results: Age, gender, mean body mass index, history of abdominal surgery, and tumor stage were not signi-ficantly different between the two study groups. Operative time decreased with increasing experience andreached a plateau after 23 patients. The operative time in study group 2 tended to be shorter than in study group1 (P = .06). Other parameters including blood loss, average number of retrieved lymph nodes, conversion rate,and intraoperative complication rates were not different between the two study groups.Conclusions: More junior surgeons can be safely trained if they are exposed to a focused training program.Supervision by an experienced surgeon and considerable experiences in open colorectal surgery are assets for anaccelerated learning curve.
Introduction
The first laparoscopic colectomy was performed byJacobs et al.1 in 1991. Since then, especially in the last
decade, minimal access surgery has made substantial ad-vances.2 Indications for laparoscopic surgery now range fromcholecystectomy to nearly all gastrointestinal surgeries and,especially, colorectal cancer surgery.3,4 Because of adequateoncological clearance, laparoscopic colorectal cancer surgeryhas been accepted as an alternative to open surgery.
In general, laparoscopic colorectal surgery is safe andfeasible5–8; however, there are still some surgical challenges.Inadequate laparoscopic procedures may lead to complica-tions and poor survival. Several studies indicated that com-plication rates decrease as surgeons gain experience.9–11 Oneof the most common methods to gauge the learning process isevaluation of the ‘‘learning curve.’’12 An accelerated learningcurve is the key to improving short-term outcomes.13 Bothoperative risks and oncological results should be taken intoconsideration during the initial learning curve. To date, thelearning process for the laparoscopic approach to colorectalcancer has not yet been clearly described.
In general, trainees start in a conventional training programwith basic procedures such as appendectomy, cholecystec-
tomy, and hernia repair.14–16 It was not clear whether thetraining program for the more junior surgeons should bedifferent from a conventional training program. Indeed, aconventional training program may not be necessary forthem. The objective of this study was to evaluate the feasi-bility and short-term outcomes of laparoscopic surgery forcolorectal cancer performed by the more junior surgeons andto assess the learning curve. We further discuss the need togenerate a focused training program for more junior surgeonsat a cancer-specializing center.
Subjects and Methods
Patient selection for laparoscopic surgery
From January 2009 to July 2010, 100 patients underwentlaparoscopic colorectal cancer surgery at The Tumor Hospitalof Harbin Medical University, Harbin, China. Patients re-ceived preoperative intravenous antibiotics and a mechanicalbowel preparation. All patients were encouraged to eat anddrink as soon as possible after the surgery. Informed consentswere obtained for all procedures.
Because the present study was designed to evaluate thelearning curve for laparoscopic colorectal surgery, difficultcases were excluded from the present study. Exclusion criteria
1Department of Colorectal Surgery, The Affiliated Tumor Hospital of Harbin Medical University, Harbin, China.2Department of Colorectal Surgery, The Second Affiliated Hospital of Harbin Medical University, Harbin, China.*The first two authors contributed equally to this work.
JOURNAL OF LAPAROENDOSCOPIC & ADVANCED SURGICAL TECHNIQUESVolume 23, Number 1, 2013ª Mary Ann Liebert, Inc.DOI: 10.1089/lap.2011.0540
17

were as follows: body mass index of >35 kg/m2, extensiveprevious abdominal surgery, palpable fixed tumors, tumorof splenic flexure, and intestinal obstruction. The morejunior surgeons had more than 10 years of experience in opencolorectal surgery and had performed more than 300 opencolorectal surgeries per year for the past 3 years. Furthermore,they had completed the laparoscopic training program in ourhospital and had been an assistant in more than 100 laparo-scopic colorectal operations during the laparoscopic trainingprogram. All surgeries were supervised by experienced staffsurgeons who previously had performed more than 300 lap-aroscopic surgeries.
Patient characteristics included age, gender, body massindex, American Society of Anesthesiologists score, historyof abdominal surgery, tumor stage, and tumor location.Operative procedures, operative time, intraoperative com-plications, blood loss, number of lymph nodes harvested,positive resection margin, conversion to open surgery, andsurgical outcomes were prospectively recorded. Conversionto open surgery was defined as any case that could not becompleted laparoscopically as planned.
To evaluate the learning curve, surgeries were grouped intothe first 50 cases (study group 1) and subsequent 50 cases(study group 2). The aforementioned outcome parameterswere compared between the twoh study groups.
Technical considerations and operative strategy
Standardized procedures were performed in all cases.Laparoscopic left-sided colon resection began with ligationof proximal vascular pedicles followed by mobilization andresection of bowel with anastomosis. For right-side surgery,the bowel was laparascopically mobilized, and division ofblood vessels, bowel resection, and anastomosis were per-formed extracorporeally through a small extension of themidline trocar incision.
For rectal cancer, the total mesorectal excision was com-pleted intracorporeally. The rectum was mobilized as fardistally as required by tumor location with attempts to keepthe mesorectal fascia intact. The rectum was divided usingarticulating endoscopic linear staplers to achieve a distalmargin of q2 cm. After placement of the anvil of the en-doluminal circular stapling device in the proximal bowelsegment, an anastomosis was performed intracorporeallyusing a standard double-stapling technique.17 A perinealdissection for abdominoperineal excision of rectum was thenperformed, and the resected specimen was retrieved throughthe perineal wound. The D3 dissection was performed whenindicated.
Statistical analysis
We used the moving average method (specifically, amoving average of four) to analyze the data. For example, anaverage of the first four values was calculated (= first movingaverage); with the addition of another variable, an average ofthe last four values was calculated (= second moving average),and so on. For construction of a smoothed learning curve andanalysis of the operating time, these moving averages wereused. All numerical values are expressed as median (range).The differences between study groups 1 and 2 were analyzedusing Fisher’s exact test, chi-squared test, or Mann-Whitney Utest where appropriate. Analysis was performed with statis-tical software (SPSS version 13.0; SPSS Inc., Chicago, IL), anddifferences were considered significant at P < .05.
Results
In total, 100 patients were included in this study. Demo-graphic characteristics of study patients are shown in Table 1.The age, gender, body mass index, history of abdominalsurgery, and tumor stage were not significantly differentbetween study group 1 (first 50 laparoscopic surgeries) and 2
Table 1. Demographic Characteristics of Study Patients
Study group 1 (n = 50) Study group 2 (n = 50) P
Median (range) age (years) 63.3 – 9.3 (30–80) 63.8 – 9.5 (28–81) NSMale/female ratio 26/24 29/21 NSMedian (range) BMI (kg/m2) 21.6 – 3.0 (15.9–29.6) 22.1 – 3.2 (16.1–30.1) NSPrevious abdominal surgery 3 (6%) 4 (8%) NSASA grade NS
1 17 (34%) 17 (34%)2 29 (58%) 31(62%)3 4 (8%) 2 (4%)4 0 (0%) 0 (0%)
TNM stage NSI 3 (6%) 2 (4%)II 21 (42%) 18 (36%)III 25 (50%) 27 (54%)IV 1 (2%) 3 (6%)
Tumor location .02Cecum 5 (10%) 4 (8%)Ascending 6 (12%) 10 (20%)Transverse 0 (0%) 1 (2%)Descending 3 (6%) 2 (4%)Sigmoid 23 (46%) 8 (16%)Rectum 13 (26%) 25 (50%)
Data are number of patients (%) unless indicated otherwise.ASA, American Society of Anesthesiologists; BMI, body mass index; NS, not significant.
18 CHEN ET AL.

(last 50 laparoscopic surgeries). Sixty-two (62%) patientssuffered from colon cancer, whereas another 38 (38%) patientshad rectal cancer. According to the clinical TNM classification,there were 5 cases with stage I, 39 with stage II, 52 with stageIII, and 4 cases with stage IV tumors (Table 1). Tumor loca-tions were significantly different between study groups 1 and2. Specifically, the percentage of tumors in the ascending ortransverse colon and rectum was lower, whereas the per-centage of tumors in the cecum or descending and sigmoidcolon was higher, in study group 1 compared with studygroup 2 (P = .02) (Table 1).
Operative procedures were significantly different betweenthe two study groups (Table 2). Specifically, the percentagesof right hemicolectomies, transverse colectomies, anterior re-section, and abdominoperineal excision of rectum were lower,whereas the percentages of left hemicolectomies and sigmoi-dectomies were higher, in study group 1 compared withstudy group 2 (P = .04) (Table 2). Average operating time,blood loss, and number of retrieved lymph nodes werecomparable between the two study groups (Table 2). No in-
traoperative complications or patients with positive resectionmargins were found in either study group. Conversion toopen surgery was required in 1 patient in study group 2 (2%)because of locally advanced disease.
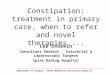
The moving average of the learning curve for study group 1is shown in Figure 1. The operative time was longer than 240minutes in the first 8 cases. The operative time gradually de-creased with increasing experience (Fig. 1).
Surgical outcomes are presented in Table 3. The time toflatus, time to bowel opening, and postoperative hospital staywere similar between the two study groups. Anastomoticleakage occurred in 1 patient who underwent a sphincter-saving surgery in study group 2. Postoperative complicationswere not significantly different between the two study groups,although they tended to be slightly higher in study group 1compared with study group 2 (20% versus 14%, P = .06) (Table3). There was no mortality in either study group.
Discussion
Laparoscopic procedures used for colorectal cancer haverecently become a standard in many hospitals. Several ran-domized controlled trials demonstrated the benefits andsafety of laparoscopic colorectal surgery, making it now thepreferred approach in the surgical management of colorectalcancer.18,19 Although laparoscopic colorectal surgery is per-formed more frequently, implementation of laparoscopiccolorectal procedures is still challenging because they requirea longer training period.20
Various laparoscopic training programs are available,but their efficiency is not clear.21 The traditional trainingparadigm is being challenged in many centers. As a result,clinicians are trying to define the most cost-effective andefficient training program in order to shorten the learningcurve.22 In addition, a traditional training program does notfit all trainees. Surgeons in traditional training will need tolearn laparoscopic techniques without ever having performedthe procedure in the open way. The shape of the learningcurve may vary depending on individual experiences andinnate skills. We hypothesized that this laparoscopic trainingprogram would help to shorten the learning curve for train-ees. The purpose of this study was to assess the learning curveof the training program. In the present study, intensive
Table 2. Operative Results
Study group 1 (n = 50) Study group 2 (n = 50) P
Median (range) operating time (minutes) 205.0 – 35.6 (135–330) 194.9 – 37.6 (120–350) .06Median (range) blood loss (mL) 23.1 – 24.5 (0–150) 20.0 – 28.9 (0–200) NSMedian (range) number of retrieved lymph nodes 14.4 – 4.8 (4–27) 14.7 – 5.0 (3–30) NSPositive resection margins 0 (0%) 0 (0%) NSConversion to open surgery 0 (0%) 1 (2%) NSIntraoperative complications 0 (0%) 0 (0%) NSOperative procedure .04
Right hemicolectomies 11 (22%) 14 (28%)Transverse colectomies 0 (0%) 1 (2%)Left hemicolectomies 3 (6%) 2 (4%)Sigmoidectomies 22 (44%) 8 (16%)Anterior resections 7 (14%) 9 (18%)APER 7 (14%) 16 (32%)
Data are number of patients (%) unless indicated otherwise.APER, abdominoperineal excision of rectum; NS, not significant.
Ope
rativ
e tim
e (m
in)
Number of cases
FIG. 1. Learning curve in study group 1 calculated usingthe moving average method (see Statistical analysis for moredetails).
LEARNING CURVE FOR LAPAROSCOPIC COLORECTAL SURGERY 19

training of surgeons may be an important key to shorten thelearning curve and limit its impact on the outcome of thepatient.
First, trainees in this program start with basic laparoscopictraining. Previous studies demonstrated that initial masteringof basic skills enhances skill acquisition and reduces resourcerequirements for training.22 During this process, using theoperating room for basic skill training in laparoscopy may beinefficient and expensive. A simulation on inanimate or ani-mate models allows trainees to acquire new skills and learnnew procedures in a safe and non-threatening environmentbefore performing these tasks on patients. Trainees practicethe video trainer and animal dissection tasks, during whichthey are personally guided by an experienced staff surgeon.According to our experience, an intense laparoscopic trainingimproves the video–eye–hand skills, and trainees obtain adeeper understanding of anatomy, gain experience in lapa-roscope manipulation, and learn to provide countertraction. Ithas previously been reported that surgeons who regularlyplay video games are generally more skilled at performinglaparoscopic surgery.23 We downloaded video games fromthe World Laparoscopy Hospital (http://training.laparoscopyhospital.com) to develop the trainees’ laparoscopic skills.
Second, the trainees attend advanced laparoscopic trainingcourses, once they become familiar with basic laparoscopy.After attending these courses, laparoscopic surgeons shouldbe able to confidently perform all procedures taught bythemselves on their patients. Through skill laboratories in-volving surgical trainers, animal models, or other simulatedoperating conditions, many advanced laparoscopic skills,such as intracorporeal suturing, are acquired. It is generallybelieved that laparoscopic colorectal surgery requires expe-rience of laparoscopic cholecystectomy. However, the traineesin our program start with assisting in laparoscopic colorectalsurgeries performed by an experienced surgeon instead ofstarting with laparoscopic cholecystectomy or appendec-tomy. As an assistant, it is important to accumulate a suffi-cient number of cases within a short time.24 The trainees arerequired to assist more than 100 laparoscopic colorectal sur-geries before being able to independently start their first caseas operators.
Previous publications suggested that the learning curve forlaparoscopic colorectal surgery ranges from 30 to 100cases.20,25 In our study, the moving average stabilized after 23cases. Our results, therefore, suggest that a surgeon is able tosafely perform the operation at a relatively early stage. It
needs to be mentioned, though, that initial cases were highlyselected. In general, sigmoidectomy is regarded as a simplerprocedure to perform; therefore, the percentage of sigmoid-ectomies was higher in study group 1 (i.e., the beginner’sphase) than in study group 2 (44 versus 16%, respectively).
There are several reasons why we were able to acceleratethe learning curve in our training program. Our more juniorsurgeons were already extremely experienced in open colo-rectal surgery. With this experience, the trainee exhibited anexcellent ability to identify and dissect tissue planes with theusual tactile clues and a capability to control multiple bloodvessels. Additionally, the supervision by experienced sur-geons certainly helped to solve laparoscopic surgery prob-lems in the beginning of the learning curve, especially in theidentification of anatomical structures and planes of dissec-tion. Under proper supervision, good results can be obtainedeven when a surgeon is relatively inexperienced. The newtraining program and the considerable experience of opensurgery made a significant influence to the length of thelearning curve.
The patient’s safety is the major concern during the trainingprogram.14 Our study provides evidence that skills of lapa-roscopic colorectal surgery can be taught and acquired safelyunder the proposed training program. It is important toevaluate operative times, complication rates, conversion rate,and blood loss to evaluate the learning curve. In our study,operative time decreased as the surgeon became more expe-rienced and was slightly shorter during the later stages of thetraining (i.e., study group 2). Several other studies have alsodemonstrated the impact of the surgeon’s experience oncomplications, showing a significant decrease in the compli-cation rate as trainees gain experience.26,27 The conversionrate during the learning curve was notably low in our study.Specifically, only 1 case of conversion to open surgeryoccurred in study group 2 and none in study group 1. Therewere no serious complications during the entire trainingprogram. Complications were seen more often initially (i.e.,study group 1), although no significant differences werefound between the two study groups.
Our study had several limitations. It was not primarilydesigned to analyze long-term oncological outcomes oflaparoscopic colorectal surgery, which would require asubsequent follow-up. Because our center is a high-volumecancer-specializing center, the results of this study may not bedirectly applicable to the training of surgeons in a generalhospital with a low volume of laparoscopic colorectal surgery.
Table 3. Surgical Outcomes
Study group 1 (n = 50) Study group 2 (n = 50) P
Median (range) time to flatus (days) 2.2 – 1.2 (1–7) 1.9 – 0.9 (1–6) NSMedian (range) time to bowel opening (days) 3.0 – 0.8 (2–6) 2.9 – 0.9 (2–7) NSMedian (range) postoperative hospital stay (days) 8.3 – 4.6 (5–35) 7.7 – 3.5 (6–28) NSWound infection 5 (10%) 4 (8%) NSBowel obstruction 1 (2%) 1 (2%) NSUrinary tract infection 3 (6%) 2 (4%) NSAnastomotic leakage 1 (2%) 0 (0%) NSDeath 0 (0%) 0 (0%) NSPostoperative complications 10 (20%) 7 (14%) NS
Data are number of patients (%) unless indicated otherwise.NS, not significant.
20 CHEN ET AL.

In conclusion, we demonstrated that laparoscopic colorec-tal surgery can be safely taught to more junior surgeons.Supervision by an experienced surgeon and extensive expe-rience in open colorectal surgery are required for an acceler-ated learning curve.
Disclosure Statement
No competing financial interests exist.
References
1. Jacobs M, Verdeja JC, Goldstein HS. Minimally invasivecolon resection (laparoscopic colectomy). Surg LaparoscEndosc 1991;1:144–150.
2. Row D, Weiser MR. An update on laparoscopic resection forrectal cancer. Cancer Control 2010;17:16–24.
3. Luglio G, Nelson H. Laparoscopy for colon cancer: State ofthe art. Surg Oncol Clin North Am 2010;19:777–791.
4. Nandakumar G, Fleshman JW. Laparoscopy for rectal can-cer. Surg Oncol Clin North Am 2010;19:793–802.
5. Hewett PJ, Allardyce RA, Bagshaw PF, Frampton CM,Frizelle FA, Rieger NA, Smith JS, Solomon MJ, Stephens JH,Stevenson AR. Short-term outcomes of the Australasianrandomized clinical study comparing laparoscopic andconventional open surgical treatments for colon cancer: TheALCCaS trial. Ann Surg 2008;248:728–738.
6. Jayne DG, Guillou PJ, Thorpe H, Quirke P, Copeland J,Smith AM, Heath RM, Brown JM. Randomized trial of lap-aroscopic-assisted resection of colorectal carcinoma: 3-yearresults of the UK MRC CLASICC Trial Group. J Clin Oncol2007;25:3061–3068.
7. Veldkamp R, Kuhry E, Hop WC, Jeekel J, Kazemier G,Bonjer HJ, Haglind E, Pahlman L, Cuesta MA, Msika S,Morino M, Lacy AM. Laparoscopic surgery versus opensurgery for colon cancer: Short-term outcomes of a rando-mised trial. Lancet Oncol 2005;6:477–484.
8. Fleshman J, Sargent DJ, Green E, Anvari M, Stryker SJ, BeartRW Jr, Hellinger M, Flanagan R Jr, Peters W, Nelson H.Laparoscopic colectomy for cancer is not inferior to opensurgery based on 5-year data from the COST Study Grouptrial. Ann Surg 2007;246:655–662.
9. Kayano H, Okuda J, Tanaka K, Kondo K, Tanigawa N.Evaluation of the learning curve in laparoscopic low anteriorresection for rectal cancer. Surg Endosc 2011;25:2972–2979.
10. Sanchez-Santos R, Estevez S, Tome C, Gonzalez S, Brox A,Nicolas R, Crego R, Pinon M, Masdevall C, Torres A.Training programs influence in the learning curve of lapa-roscopic gastric bypass for morbid obesity: A systematicreview. Obes Surg 2012;22:34–41.
11. Kim SY, Hong SG, Roh HR, Park SB, Kim YH, Chae GB.Learning curve for a laparoscopic appendectomy by asurgical trainee. J Korean Soc Coloproctol 2010;26:324–328.
12. Park IJ, Choi GS, Lim KH, Kang BM, Jun SH. Multi-dimensional analysis of the learning curve for laparoscopicresection in rectal cancer. J Gastrointest Surg 2009;13:275–281.
13. Rogers DA, Elstein AS, Bordage G. Improving continuingmedical education for surgical techniques: Applying thelessons learned in the first decade of minimal access surgery.Ann Surg 2001;233:159–166.
14. Li JC, Hon SS, Ng SS, Lee JF, Yiu RY, Leung KL. Thelearning curve for laparoscopic colectomy: Experience of a
surgical fellow in an university colorectal unit. Surg Endosc2009;23:1603–1608.
15. Choi DH, Jeong WK, Lim SW, Chung TS, Park JI, Lim SB,Choi HS, Nam BH, Chang HJ, Jeong SY. Learning curves forlaparoscopic sigmoidectomy used to manage curable sig-moid colon cancer: Single-institute, three-surgeon experi-ence. Surg Endosc 2009;23:622–628.
16. Lin YY, Shabbir A, So JB. Laparoscopic appendectomy byresidents: Evaluating outcomes and learning curve. SurgEndosc 2010;24:125–130.
17. Kuroyanagi H, Akiyoshi T, Oya M, Fujimoto Y, Ueno M,Yamaguchi T, Muto T. Laparoscopic-assisted anteriorresection with double-stapling technique anastomosis: Safeand feasible for lower rectal cancer? Surg Endosc 2009;23:2197–2202.
18. Clinical Outcomes of Surgical Therapy Study Group. Acomparison of laparoscopically assisted and open colectomyfor colon cancer. N Engl J Med 2004;350:2050–2059.
19. Weeks JC, Nelson H, Gelber S, Sargent D, Schroeder G:Short-term quality-of-life outcomes following laparoscopic-assisted colectomy vs open colectomy for colon cancer: Arandomized trial. JAMA 2002;287:321–328.
20. Schlachta CM, Mamazza J, Seshadri PA, Cadeddu M,Gregoire R, Poulin EC. Defining a learning curve for lapa-roscopic colorectal resections. Dis Colon Rectum 2001;44:217–222.
21. Stolzenburg JU, Truss MC, Rabenalt R, Do M, SchwalenbergT, Katsakiori PF, McNeill A, Liatsikos E. Training in lap-aroscopy. EAU-EBU Update Series 2007;5:53–62.
22. Stefanidis D, Hope WW, Korndorffer JR Jr, Markley S, ScottDJ. Initial laparoscopic basic skills training shortens thelearning curve of laparoscopic suturing and is cost-effective.J Am Coll Surg 2010;210:436–440.
23. Rosser JC Jr, Lynch PJ, Cuddihy L, Gentile DA, Klonsky J,Merrell R. The impact of video games on training surgeonsin the 21st century. Arch Surg 2007;142:181–186.
24. Lai PS, Hou YC, Chang TC, Hung CH, Lin HM, Liang JT.The learning curve of laparoscopic colorectal surgery inregional hospital. J Soc Colon Rectal Surgeon (Taiwan)2010;21:1–8.
25. Reissman P, Cohen S, Weiss EG, Wexner SD. Laparoscopiccolorectal surgery: Ascending the learning curve. WorldJ Surg 1996;20:277–281.
26. Agachan F, Joo JS, Weiss EG, Wexner SD. Intraoperativelaparoscopic complications. Are we getting better? DisColon Rectum 1996;39:S14–S19.
27. Agha A, Moser C, Iesalnieks I, Piso P, Schlitt HJ: Combi-nation of hand-assisted and laparoscopic proctocolectomy(HALP): Technical aspects, learning curve and early post-operative results. Surg Endosc 2008;22:1547–1552.
Address correspondence to:Bin-Bin Cui, MD
Department of Colorectal SurgeryThe Affiliated Tumor Hospital of
Harbin Medical University150 Haping Road
Harbin 150081China
E-mail: [email protected]
LEARNING CURVE FOR LAPAROSCOPIC COLORECTAL SURGERY 21










![LAPAROSCOPIC SURGERY FOR COLONIC CANCERincluding surgery for colorectal malignancies, has been demonstrated [1-7]. Currently, indications for laparoscopic surgery are continuing to](https://img.pdfslide.net/doc/110x75/5f088a2f7e708231d4228374/laparoscopic-surgery-for-colonic-cancer-including-surgery-for-colorectal-malignancies.jpg)

















