Embed Size (px)
Citation preview
1
The Local Public Health Institute of Massachusetts
Progress Report
January 01, 2011 – June 30, 2012
Prepared by:
Hope Kenefick, MSW, PhD
Evaluator for the Local Public Health Institute of Massachusetts
2
Local Public Health Institute of Massachusetts
Progress Report
January 01, 2011 – June 30, 2012
Table of Contents
Page:
Executive summary 3
Introduction 6
Methodology 6
Problem 1 7
Problem 2 8
Problem 3 12
Problem 4 13
Problem 5 14
Problem 6 15
Intermediate and longer‐term outcomes 17
Conclusions and Next Steps 18
Appendix A: LPHI Logic Model 21
Appendix B: Competencies addressed by LPHI trainings
22
Appendix C: Emergency Preparedness Competencies and Capabilities Addressed by LPHI Trainings
24
Appendix D: Recommended Emergency Preparedness Training Courses
25
3
The Local Public Health Institute of Massachusetts
Progress Report
January 01, 2011 – June 30, 2012
Executive Summary
Introduction: Since January of 2010, the Boston University School of Public Health (BUSPH) has had the contract for and managed the Local Public Health Institute (LPHI) of Massachusetts. With support from
the Massachusetts Department of Public Health, the LPHI staff work with the LPHI Advisory Committee
to pursue the LPHI mission: To provide and ensure a competent workforce by strengthening and
sustaining the capacity of local boards of health to prepare for and respond to public health issues and
emergencies and to promote the health of residents of the Commonwealth. The LPHI is submitting an
18‐month report to align its reporting with the state fiscal year. Hereafter, the LPHI will resume
submission of annual progress reports cover July 1 through June 30. The full report describes the six
problems addressed by the LPHI and progress made between January 1, 2011 and June 30, 2012 in
addressing the problems and their associated objectives. Below is a description of the LPHI evaluation
methodology used to inform the progress report, as well as a summary of the major accomplishments of
the LPHI in the 18‐month timeframe and recommended next steps.
Methodology: The LPHI evaluator and LPHI management team devised several data collection and
tracking mechanisms to measure progress toward LPHI objectives and desired outcomes, including: (1)
standardized training evaluation forms; (2) A Foundations Course instructor evaluation survey; and (3)
administrative tracking by the LPHI Program Manager. Once the 18‐month accomplishments were
inventoried, the major accomplishments were presented to the members of the LPHI Advisory
Committee and members were polled to assess whether the progress failed to meet, met or exceeded
their expectations.
Accomplishments and Next Steps: It was a very productive 18 months with significant progress made
toward all program objectives, including:
The LPHI expanded its capacity for distance learning and offered seven new on‐line modules in
addition to the Orientation to Local Public Health: Bed Bugs; Dealing with Stress in Disasters:
Building Psychological Resilience; Legal Nuts and Bolts of Isolation and Quarantine, Parts 1 and
2; Lyme Disease; MAVEN and MAVEN TB Training Modules; and Swimming Pools. Like the
Orientation module, all but the MAVEN modules have a facilitator’s guide to assist in use of the
module as a teaching tool for classroom learning. Additionally, LPHI has 10 other modules
already in development and planned for completion in 2012.
The Foundations Course was run for the second time since BUSPH assumed the LPHI contract
and PPE, Surveillance and Legal Nuts and Bolts Parts 1 and 2 trainings were offered as well. In
April of 2012, a four‐day train the trainers event entitled Environmental Health Training in
4
Emergency Response (EHTER) was conducted. In all trainings, participants rated themselves as
better able to perform session learning objectives as a result of training and felt the training
content would be useful in their jobs. The mean quiz score in the EHTER course increased from
75% at pre‐test to 88% at post‐test and participants indicated their knowledge about all EHTER
topics increased as a result of the training. Additionally, statistically significant improvements in
learning took place in 14 of 17 sessions of the Foundations Course.
398 trainees received education in the LPHI’s training sessions over the 18‐month period.
Trainees represent all of the Public Health Emergency Preparedness Regions of the state,
although the lowest representation was among public health practitioners in Region 2: Central
MA at only 7.5%. The trainees are primarily local health directors/agents, public health nurses,
“other” positions (e.g., EP coordinators, regional public health staff), sanitarians/inspectors, and
BOH members/chairpersons.
The LPHI Fellows Program was launched and, based on evaluation results, was very successful in
meetings the program objective and in its marketing, application and selection criteria, and
recognition event.
The LPHI Advisory Committee met six times and has representation from all MDPH EP regions,
six public health associations, and five academic institutions.
Collaborative planning with LPHI partners took place and will expand LPHI offerings in 2012,
including additional on‐line modules which are in development, as well as basic and advanced
risk communications training.
The marketing and communications plan was implemented in 2011 and involved the use of the
LPHI website, use of Constant Contact, outreach via the public health associations, and
newsletters to market LPHI offerings. The number of registrations for trainings, applicants for
the Fellows Program, and attendance at the Fellows induction ceremony are all indicators that
marketing efforts were successful.
Data were collected via training evaluations to supply the LPHI with an on‐going assessment of
training needs among LPHI users. The LPHI evaluation strategy also allowed for the tracking of
progress toward LPHI objectives and the identification of next steps for the year ahead.
Overall, the LPHI’s progress met or exceeded the expectations of its Advisory Group Committee
members.
There are few recommended changes for the sake of quality improvement. Most of the
recommendations involve continuing to build on the successes to date, including:
Continuing to deliver and evaluate the blended and classroom sessions and begin to evaluate
the impact of the on‐line modules. Developing the additional modules scheduled for 2012 and
ensure each has an evaluation component.
Building on the successful launch of the LPHI Fellows Program.
Continuing collaborative planning with partners to deliver training and develop new offerings.
Continuing to use of the communications and marketing plan and implement products to
increase awareness of LPHI offerings and the Fellows Program.
5
Continuing to evaluate LPHI progress toward objectives and plan for evaluation of the
secondary/ long‐term outcome ‐ Improved agency performance in areas related to competencies
in which agency personnel have been trained by the LPHI.
Recommended changes or new initiatives for the next year are limited and include:
Exploring the relatively low utilization of LPHI offerings by those in Region 2: Central MA.
Analyzing the data associated with the existing on‐line modules to understand the impact of
distance learning options on LPH competencies.

6
The Local Public Health Institute of Massachusetts
Progress Report
January 01, 2011 – June 30, 2012
Introduction: Since January of 2010, the Boston University School of Public Health (BUSPH) has held the contract for and managed the Local Public Health Institute (LPHI) of Massachusetts. With support
from the Massachusetts Department of Public Health, the LPHI staff work with the LPHI Advisory
Committee to pursue the LPHI mission: To provide and ensure a competent workforce by strengthening
and sustaining the capacity of local boards of health to prepare for and respond to public health issues
and emergencies and to promote the health of residents of the Commonwealth. The LPHI Advisory
Committee identified six potential problems that pose barriers to achieving the LPHI mission, including
resources of which the LPHI has not taken full advantage. An objective was established to address each
of the identified problems and advance the LPHI toward its mission. This report is organized around the
six problems and provides a report of the progress made between January 1, 2011 and June 30, 2012.
The LPHI is submitting an 18‐month report to align its reporting with the state fiscal year. Hereafter, the
LPHI will resume submission of annual progress reports cover July 1 through June 30. The LPHI is
submitting an 18‐month report to align its reporting with the state fiscal year. Hereafter, the LPHI will
resume submission of annual progress reports cover July 1 through June 30. A logic model was drafted
to depict the relationship of the mission, problems, objectives, outputs and outcomes (See Appendix A).
For information about any of the educational offerings or documents referenced in this report, contact
Jennifer Tsoi, LPHI Project Manager at [email protected] or (617)638‐4825.
Methodology: The LPHI evaluator and LPHI management team devised several data collection and
tracking mechanisms to measure progress toward LPHI objectives and desired outcomes. Below are
descriptions of those utilized to inform this report.
Standardized training evaluation forms: All LPHI‐supported trainings must include an evaluation
component. Whenever possible, such evaluations include pre/post quiz questions to assess the
extent to which students acquired knowledge as a result of training. For the Foundations Course,
each of the 18 sessions began and concluded with an assessment of student preparedness to
perform session learning objectives and quiz questions assessing knowledge about the training
content. Students also provided data for use in quality improvement, including information about
what worked well and what could be improved. At the conclusion of the course, students
completed an overall course evaluation to provide data useful in quality improvement. In the
Environmental Health Training in Emergency Response (EHTER) course, a pre/post quiz covering all
training modules was used to assess knowledge gains. A standardized evaluation form was also
created for training sessions when a pre/post test is not feasible. The form is administered at the
conclusion of a training session and asks students to rate how their ability to perform the learning
objectives changed as a result of training. It further request data that for use in quality
7
improvement. In the case of on‐line learning modules, users are only required to complete the
pre/post quiz and evaluation if they intend to complete the module for a certificate of completion
and contact hours. It should be noted that these online modules were also designed to function as
easily accessible online reference manuals so not all users will be seeking contact hours or
certificates of completion. Google Analytics is used to track unique and returning hits to the
modules’ webpage.
Foundations Course Instructor evaluation survey: To gain additional insight about how the
Foundations Course can be improved in its next iteration, 13 of 19 (68.4%) instructors completed an
on‐line survey in February 2012 to provide information about what worked well and what could be
improved, as well as to assess instructor interest in proposed changes to the course.
Administrative tracking: The project manager routinely tracks data related to the size and
composition of the Advisory Committee and its meetings, the number and types of trainings and
demographics of training participants, the number and types of collaborating partners, the number
of trainings with a distance education component, and the status of the communications and
marketing plan, including the number of newsletters and training calendars disseminated.
Polling of LPHI Advisory Committee Members: The June LPHI Advisory Committee meeting was held
via webinar. Members were presented with evaluation findings about LPHI progress over the last 18
months and then asked a polling question to assess whether the LPHI activities presented failed to
meet, met, or exceeded their expectations.
Typically quantitative analyses for the LPHI are conducted using SPSS and qualitative analyses are
analyzed for common and divergent themes. For more detail on any of the data sources described
above or related evaluation documents, contact Hope Kenefick, the LPHI evaluator at
Problem #1: A group of individuals that understands the needs of local public health and that represents various segments of the workforce and geographic areas of the Commonwealth is needed to
advise MDPH and others (e.g., DEP, MEMA) about how to most effectively achieve the LPHI mission. To
address the problem, the Institute will accomplish the following objective: To rebuild and convene a
highly functioning Advisory Committee. The figure below shows progress made toward the objective in
2011.
# of associations represented
6 public health associations are represented, including: MA Association of Health Boards, MA Health Officers Association, Western MA Public Health Association, MA Environmental Health Association, MA Public Health Association, MA Association of Public Health Nurses
# of regions represented All emergency preparedness regions are represented on the LPHI Advisory Committee, including Regions 1, 2, 3, 4a, 4b, 4c , and 5
# of academic partners 5 academic partners are on the Committee: Harvard and Boston Universities
8
represented and University of MA Amherst were joined by the UMass Medical School and UMass Lowell during the 18‐month period.
# of meetings 6 in person meetings of the LPHI Advisory Committee in March, June, September, and December of 2011 and March and June of 2012. Additionally, 5 Meetings took place with the Bureau Directors at MDPH. Another 5 took place with training partners from the DelValle Institute of Emergency Preparedness, the Center for Excellence for Emergency Preparedness Education and Training (CEEPET) at UMass Medical School, and the Preparedness and Emergency Response Learning Center (PERLC) at the Harvard School of Public Health (HSPH). A workgroup of the LPHI Advisory Committee also met twice by conference call and had many email exchanges to develop the LPHI Fellows Program model.
The desired short‐term outcome of our work to address problem #1 is: Strengthened partnerships
among public health and academic partners to ensure that LPHI trainings and programs are aligned with
the learning priorities of the LPH workforce and are of high quality. Over the course of the reporting
period, several examples of active collaboration led to high quality training programs that meet the
needs of the LPH workforce. The 2011 Foundations Course featured academic partners at the Boston
University School of Public Health and representatives of local health with expertise in the various
content areas covered in the course. A high level of satisfaction among trainees and faculty, improved
ratings of ability to perform learning objectives by the trainees, and improved knowledge from pre to
post test for most sessions illustrate the high quality of this collaborative effort. Faculty and student
pairings developed initial content for several on‐line training modules in consultation with local public
health content experts. LPHI Advisory Committee members served as reviewers of the modules and/or
recruited others with content expertise to vet the modules. Six new modules were added addressing
dozens of cross‐cutting competencies at the awareness level. In total, 188 trainees completed these on‐
line modules to earn a certificate of completion. Additionally, 3,192 used the modules as on‐line
references through 3,719 hits to the LPHI website. MDPH Communications staff and four training
centers (LPHI, DelValle, CEEPET, and PERLC‐HSPH) collaborated on the review and designation of a
prerequisite Basic Risk Communication online course and on the development of an Advanced Risk
Communications training for delivery in 2012.
Problem #2: The LPH workforce may not possess the capabilities needed to prepare for and respond
to emerging public health issues and emergencies. Training is needed to ensure the LPH workforce has
the competencies necessary to protect the health of MA residents. To address problem #2, the LPHI will
accomplish the following objective: Provide training courses and education programs on Public Health
and Emergency Preparedness competencies. The figure below shows progress made toward the
objective in 2011.
# of trainings and programs
The 18 session Foundations Course ran from September through December of 2011. Seven new on‐line modules (Bed Bugs, Dealing with Stress in Disasters: Building Psychological Resilience; Legal Nuts and Bolts of Isolation and Quarantine; Lyme Disease; MA Virtual Epidemiological Network
9
(MAVEN) and MAVEN TB Training Modules; and Swimming Pools) were added to the Orientation to Local Public Health addressing dozens of cross‐cutting competencies at the awareness level. Classroom trainings covered Legal Nuts and Bolts of Isolation and Quarantine, Parts I and 2; Infectious Disease Surveillance, Reporting and Control, and Personal Protective Equipment. Additionally, LPHI support was extended to training partners to help underwrite the following conferences/trainings: MAPHN Annual Conference; MEHA Yankee Environmental Conference; MHOA Annual Conference; MAHB BOH Certificate Program; and WMPHA Title 5, Annual Conference, Food Protection, Introduce to local public health. Working in collaboration with MDPH and other training centers, LPHI also created 3 sets of training recommendations for new staff (see Appendix D), including at the awareness level for all entry level local public health practitioners, those with additional emergency response functions, and for practitioners at the performance level. In 2011, LPHI started to collaborate with DelValle, HSPH and CEEPET to prevent duplication of efforts in bringing Risk Communication training to MA health professionals. The Basic Risk Communication Curriculum was been finalized in early 2012, and efforts to develop the Advanced Risk Communication training will start in the summer of 2012.
The LPHI website also promoted additional training resources, trainings, updates, and 43 partner events/trainings.
# of competencies covered in trainings/programs
The Foundations Course addressed the 12/18 program area and 7/10 cross cutting competencies at the awareness level. The tables in Appendices B and C show the competencies addressed in existing and planned LPHI trainings.
# of registrants and # of participants (total, by region and role)
For Legal Nuts and Bolts, Part (LNAB1), 69 registered and 49 completed, a 71.0% completion rate.
For LNAB2, 57 registered and 34 completed, a 59.5% completion rate.
For Personal Protective Equipment (PPE), 36 registered and 32 completed, an 88.8% completion rate.
For Surveillance (Surv), 40 registered and 21 completed, a 52.5% completion rate.
For the 2011 Foundations Course, 36 registered and 31 completed, an 86.1% completion rate.
For the on‐line modules, 258 registered and 188 completed, a 72.9% completion rate.
For EHTER, 49 participants registered and 43 completed, a 87.7% completion rate.
The roles and regions of those who completed training are provided in
the tables below. In general, The trainees are primarily local health
10
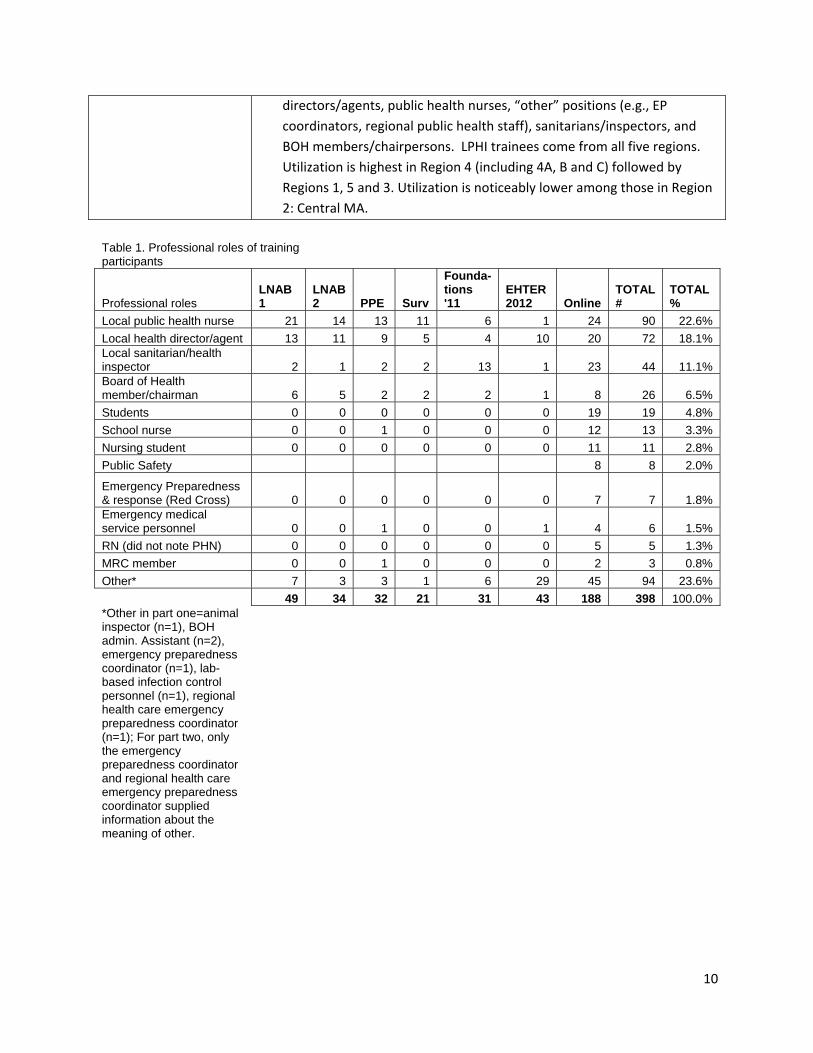
directors/agents, public health nurses, “other” positions (e.g., EP
coordinators, regional public health staff), sanitarians/inspectors, and
BOH members/chairpersons. LPHI trainees come from all five regions.
Utilization is highest in Region 4 (including 4A, B and C) followed by
Regions 1, 5 and 3. Utilization is noticeably lower among those in Region
2: Central MA.
Table 1. Professional roles of training participants
Professional roles LNAB 1
LNAB 2 PPE Surv
Founda-tions '11
EHTER 2012 Online
TOTAL #
TOTAL %
Local public health nurse 21 14 13 11 6 1 24 90 22.6%
Local health director/agent 13 11 9 5 4 10 20 72 18.1% Local sanitarian/health inspector 2 1 2 2 13 1 23 44 11.1% Board of Health member/chairman 6 5 2 2 2 1 8 26 6.5%
Students 0 0 0 0 0 0 19 19 4.8%
School nurse 0 0 1 0 0 0 12 13 3.3%
Nursing student 0 0 0 0 0 0 11 11 2.8%
Public Safety 8 8 2.0%
Emergency Preparedness & response (Red Cross) 0 0 0 0 0 0 7 7 1.8% Emergency medical service personnel 0 0 1 0 0 1 4 6 1.5%
RN (did not note PHN) 0 0 0 0 0 0 5 5 1.3%
MRC member 0 0 1 0 0 0 2 3 0.8%
Other* 7 3 3 1 6 29 45 94 23.6%
49 34 32 21 31 43 188 398 100.0% *Other in part one=animal inspector (n=1), BOH admin. Assistant (n=2), emergency preparedness coordinator (n=1), lab-based infection control personnel (n=1), regional health care emergency preparedness coordinator (n=1); For part two, only the emergency preparedness coordinator and regional health care emergency preparedness coordinator supplied information about the meaning of other.
11
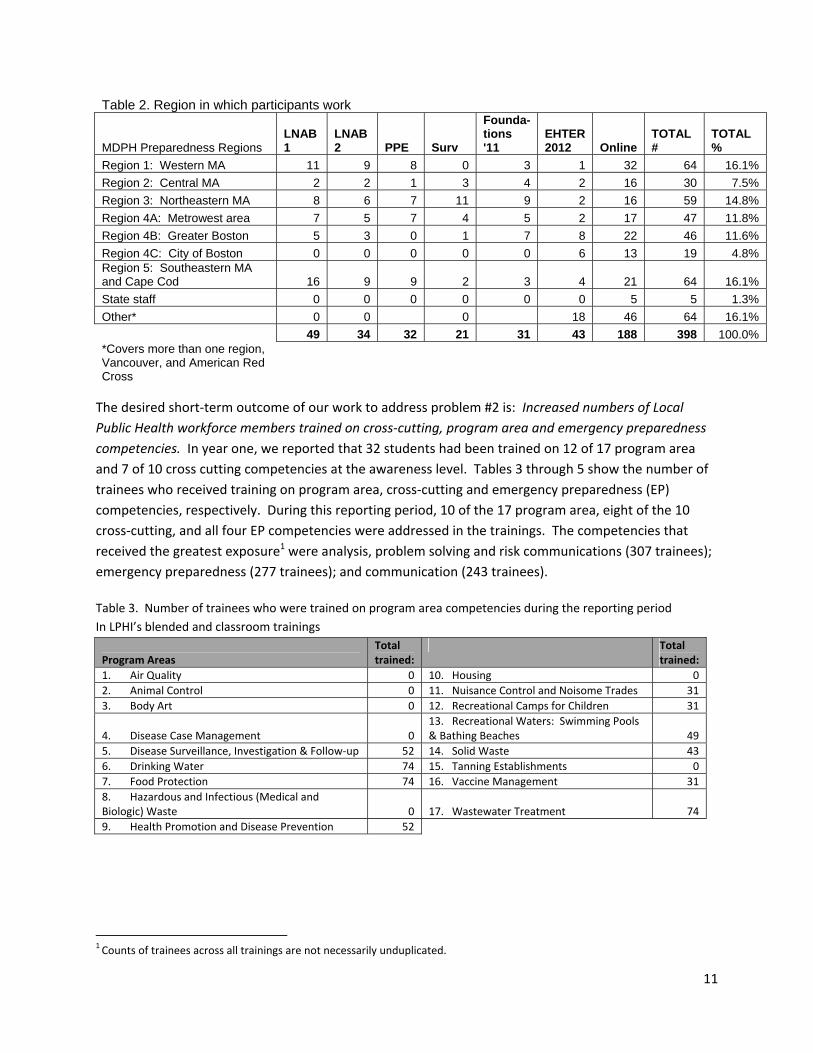
Table 2. Region in which participants work
MDPH Preparedness Regions LNAB 1
LNAB 2 PPE Surv
Founda-tions '11
EHTER 2012 Online
TOTAL #
TOTAL %
Region 1: Western MA 11 9 8 0 3 1 32 64 16.1%
Region 2: Central MA 2 2 1 3 4 2 16 30 7.5%
Region 3: Northeastern MA 8 6 7 11 9 2 16 59 14.8%
Region 4A: Metrowest area 7 5 7 4 5 2 17 47 11.8%
Region 4B: Greater Boston 5 3 0 1 7 8 22 46 11.6%
Region 4C: City of Boston 0 0 0 0 0 6 13 19 4.8% Region 5: Southeastern MA and Cape Cod 16 9 9 2 3 4 21 64 16.1%
State staff 0 0 0 0 0 0 5 5 1.3%
Other* 0 0 0 18 46 64 16.1%
49 34 32 21 31 43 188 398 100.0% *Covers more than one region, Vancouver, and American Red Cross
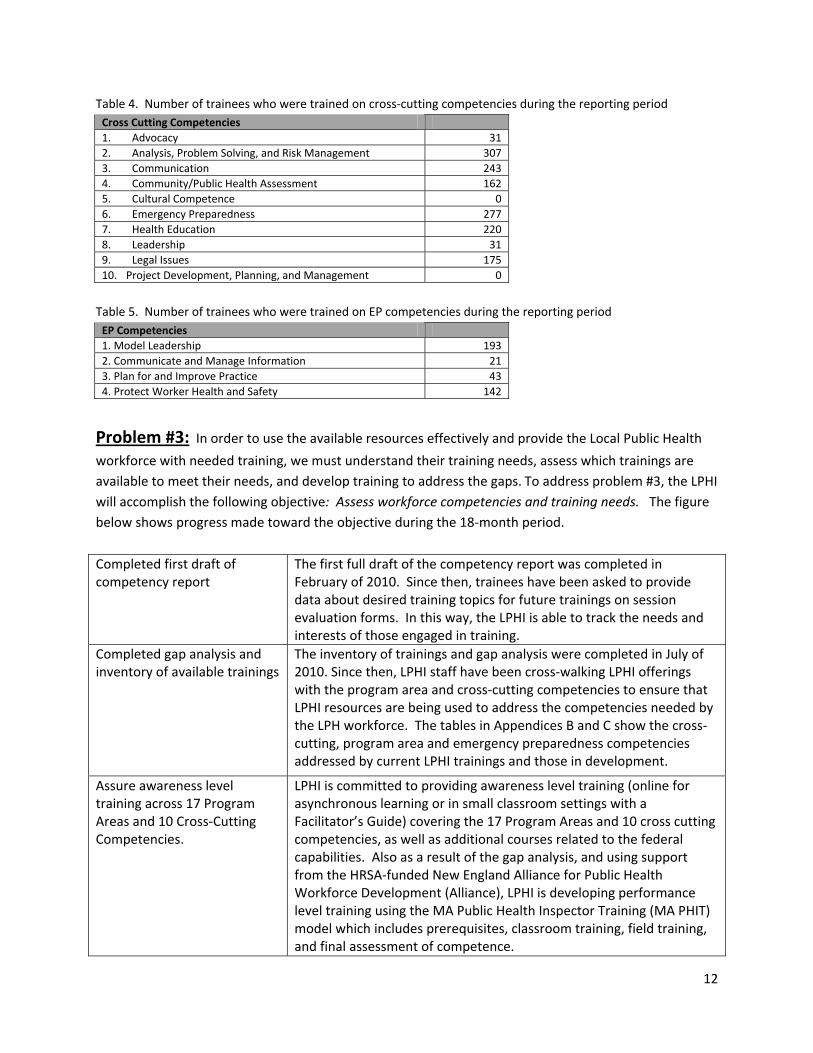
The desired short‐term outcome of our work to address problem #2 is: Increased numbers of Local
Public Health workforce members trained on cross‐cutting, program area and emergency preparedness
competencies. In year one, we reported that 32 students had been trained on 12 of 17 program area
and 7 of 10 cross cutting competencies at the awareness level. Tables 3 through 5 show the number of
trainees who received training on program area, cross‐cutting and emergency preparedness (EP)
competencies, respectively. During this reporting period, 10 of the 17 program area, eight of the 10
cross‐cutting, and all four EP competencies were addressed in the trainings. The competencies that
received the greatest exposure1 were analysis, problem solving and risk communications (307 trainees);
emergency preparedness (277 trainees); and communication (243 trainees).
Table 3. Number of trainees who were trained on program area competencies during the reporting period
In LPHI’s blended and classroom trainings
Program Areas Total trained:
Total trained:
1. Air Quality 0 10. Housing 0
2. Animal Control 0 11. Nuisance Control and Noisome Trades 31
3. Body Art 0 12. Recreational Camps for Children 31
4. Disease Case Management 0 13. Recreational Waters: Swimming Pools & Bathing Beaches 49
5. Disease Surveillance, Investigation & Follow‐up 52 14. Solid Waste 43
6. Drinking Water 74 15. Tanning Establishments 0
7. Food Protection 74 16. Vaccine Management 31
8. Hazardous and Infectious (Medical and Biologic) Waste 0 17. Wastewater Treatment 74
9. Health Promotion and Disease Prevention 52
1 Counts of trainees across all trainings are not necessarily unduplicated.
12
Table 4. Number of trainees who were trained on cross‐cutting competencies during the reporting period
Cross Cutting Competencies
1. Advocacy 31
2. Analysis, Problem Solving, and Risk Management 307
3. Communication 243
4. Community/Public Health Assessment 162
5. Cultural Competence 0
6. Emergency Preparedness 277
7. Health Education 220
8. Leadership 31
9. Legal Issues 175
10. Project Development, Planning, and Management 0
Table 5. Number of trainees who were trained on EP competencies during the reporting period
EP Competencies
1. Model Leadership 193
2. Communicate and Manage Information 21
3. Plan for and Improve Practice 43
4. Protect Worker Health and Safety 142
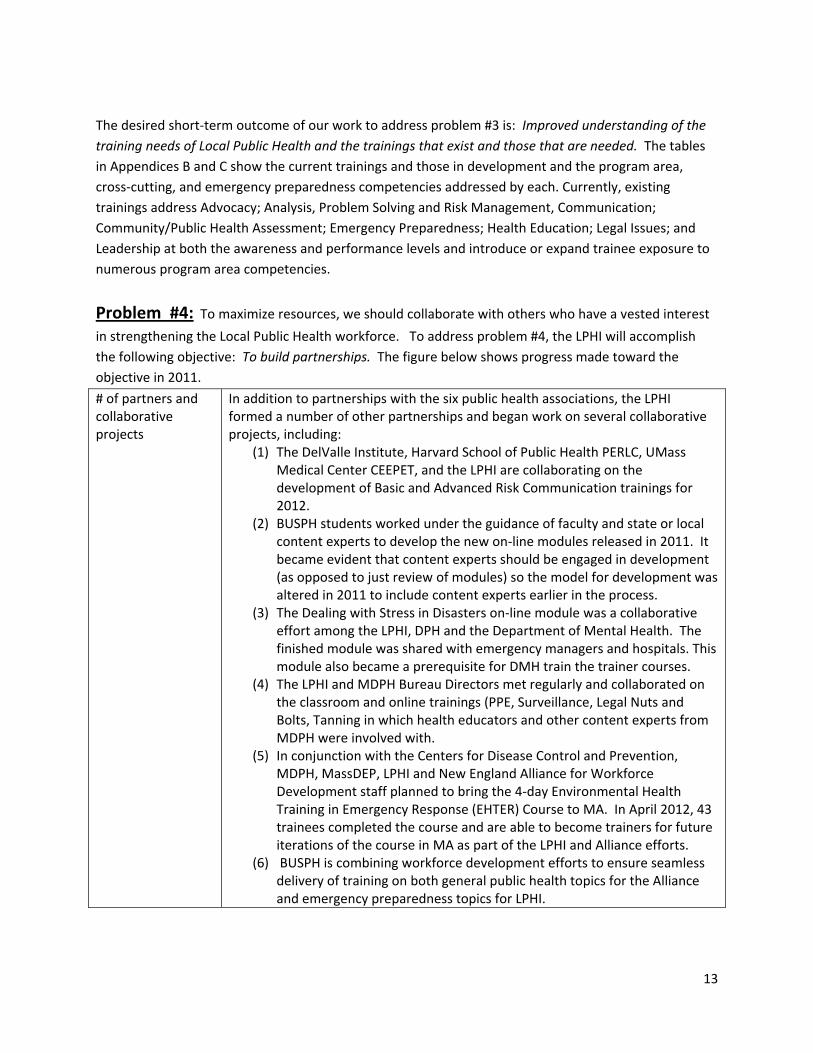
Problem #3: In order to use the available resources effectively and provide the Local Public Health workforce with needed training, we must understand their training needs, assess which trainings are
available to meet their needs, and develop training to address the gaps. To address problem #3, the LPHI
will accomplish the following objective: Assess workforce competencies and training needs. The figure
below shows progress made toward the objective during the 18‐month period.
Completed first draft of competency report
The first full draft of the competency report was completed in February of 2010. Since then, trainees have been asked to provide data about desired training topics for future trainings on session evaluation forms. In this way, the LPHI is able to track the needs and interests of those engaged in training.
Completed gap analysis and inventory of available trainings
The inventory of trainings and gap analysis were completed in July of 2010. Since then, LPHI staff have been cross‐walking LPHI offerings with the program area and cross‐cutting competencies to ensure that LPHI resources are being used to address the competencies needed by the LPH workforce. The tables in Appendices B and C show the cross‐cutting, program area and emergency preparedness competencies addressed by current LPHI trainings and those in development.
Assure awareness level training across 17 Program Areas and 10 Cross‐Cutting Competencies.
LPHI is committed to providing awareness level training (online for asynchronous learning or in small classroom settings with a Facilitator’s Guide) covering the 17 Program Areas and 10 cross cutting competencies, as well as additional courses related to the federal capabilities. Also as a result of the gap analysis, and using support from the HRSA‐funded New England Alliance for Public Health Workforce Development (Alliance), LPHI is developing performance level training using the MA Public Health Inspector Training (MA PHIT) model which includes prerequisites, classroom training, field training, and final assessment of competence.
13
The desired short‐term outcome of our work to address problem #3 is: Improved understanding of the
training needs of Local Public Health and the trainings that exist and those that are needed. The tables
in Appendices B and C show the current trainings and those in development and the program area,
cross‐cutting, and emergency preparedness competencies addressed by each. Currently, existing
trainings address Advocacy; Analysis, Problem Solving and Risk Management, Communication;
Community/Public Health Assessment; Emergency Preparedness; Health Education; Legal Issues; and
Leadership at both the awareness and performance levels and introduce or expand trainee exposure to
numerous program area competencies.
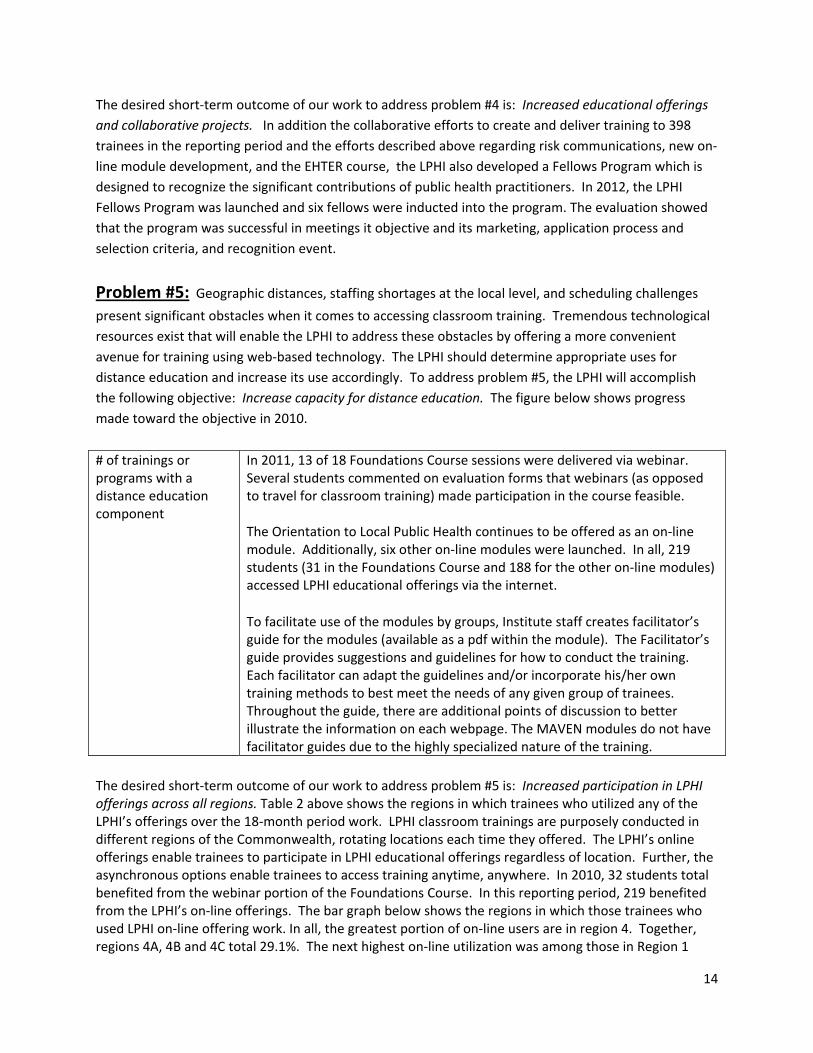
Problem #4: To maximize resources, we should collaborate with others who have a vested interest
in strengthening the Local Public Health workforce. To address problem #4, the LPHI will accomplish
the following objective: To build partnerships. The figure below shows progress made toward the
objective in 2011.
# of partners and collaborative projects
In addition to partnerships with the six public health associations, the LPHI formed a number of other partnerships and began work on several collaborative projects, including:
(1) The DelValle Institute, Harvard School of Public Health PERLC, UMass Medical Center CEEPET, and the LPHI are collaborating on the development of Basic and Advanced Risk Communication trainings for 2012.
(2) BUSPH students worked under the guidance of faculty and state or local content experts to develop the new on‐line modules released in 2011. It became evident that content experts should be engaged in development (as opposed to just review of modules) so the model for development was altered in 2011 to include content experts earlier in the process.
(3) The Dealing with Stress in Disasters on‐line module was a collaborative effort among the LPHI, DPH and the Department of Mental Health. The finished module was shared with emergency managers and hospitals. This module also became a prerequisite for DMH train the trainer courses.
(4) The LPHI and MDPH Bureau Directors met regularly and collaborated on the classroom and online trainings (PPE, Surveillance, Legal Nuts and Bolts, Tanning in which health educators and other content experts from MDPH were involved with.
(5) In conjunction with the Centers for Disease Control and Prevention, MDPH, MassDEP, LPHI and New England Alliance for Workforce Development staff planned to bring the 4‐day Environmental Health Training in Emergency Response (EHTER) Course to MA. In April 2012, 43 trainees completed the course and are able to become trainers for future iterations of the course in MA as part of the LPHI and Alliance efforts.
(6) BUSPH is combining workforce development efforts to ensure seamless delivery of training on both general public health topics for the Alliance and emergency preparedness topics for LPHI.
14
The desired short‐term outcome of our work to address problem #4 is: Increased educational offerings
and collaborative projects. In addition the collaborative efforts to create and deliver training to 398
trainees in the reporting period and the efforts described above regarding risk communications, new on‐
line module development, and the EHTER course, the LPHI also developed a Fellows Program which is
designed to recognize the significant contributions of public health practitioners. In 2012, the LPHI
Fellows Program was launched and six fellows were inducted into the program. The evaluation showed
that the program was successful in meetings it objective and its marketing, application process and
selection criteria, and recognition event.
Problem #5: Geographic distances, staffing shortages at the local level, and scheduling challenges present significant obstacles when it comes to accessing classroom training. Tremendous technological
resources exist that will enable the LPHI to address these obstacles by offering a more convenient
avenue for training using web‐based technology. The LPHI should determine appropriate uses for
distance education and increase its use accordingly. To address problem #5, the LPHI will accomplish
the following objective: Increase capacity for distance education. The figure below shows progress
made toward the objective in 2010.
# of trainings or programs with a distance education component
In 2011, 13 of 18 Foundations Course sessions were delivered via webinar. Several students commented on evaluation forms that webinars (as opposed to travel for classroom training) made participation in the course feasible. The Orientation to Local Public Health continues to be offered as an on‐line module. Additionally, six other on‐line modules were launched. In all, 219 students (31 in the Foundations Course and 188 for the other on‐line modules) accessed LPHI educational offerings via the internet.
To facilitate use of the modules by groups, Institute staff creates facilitator’s guide for the modules (available as a pdf within the module). The Facilitator’s guide provides suggestions and guidelines for how to conduct the training. Each facilitator can adapt the guidelines and/or incorporate his/her own training methods to best meet the needs of any given group of trainees. Throughout the guide, there are additional points of discussion to better illustrate the information on each webpage. The MAVEN modules do not have facilitator guides due to the highly specialized nature of the training.
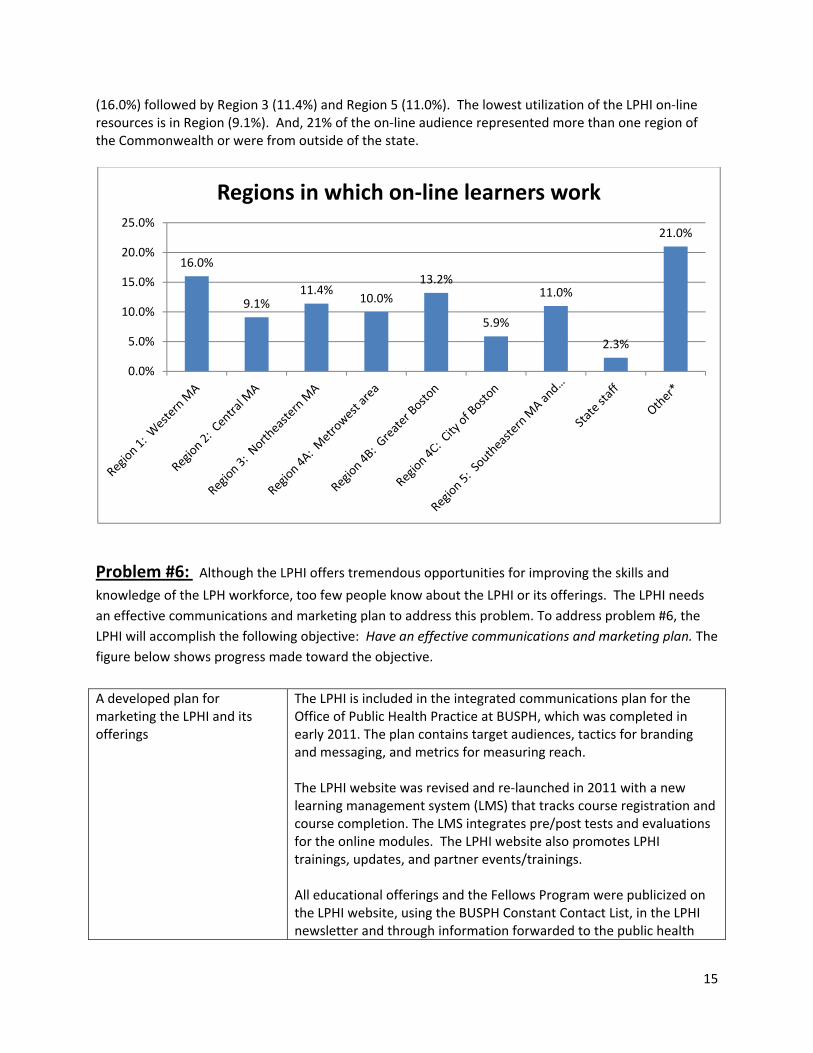
The desired short‐term outcome of our work to address problem #5 is: Increased participation in LPHI offerings across all regions. Table 2 above shows the regions in which trainees who utilized any of the LPHI’s offerings over the 18‐month period work. LPHI classroom trainings are purposely conducted in different regions of the Commonwealth, rotating locations each time they offered. The LPHI’s online offerings enable trainees to participate in LPHI educational offerings regardless of location. Further, the asynchronous options enable trainees to access training anytime, anywhere. In 2010, 32 students total benefited from the webinar portion of the Foundations Course. In this reporting period, 219 benefited from the LPHI’s on‐line offerings. The bar graph below shows the regions in which those trainees who used LPHI on‐line offering work. In all, the greatest portion of on‐line users are in region 4. Together, regions 4A, 4B and 4C total 29.1%. The next highest on‐line utilization was among those in Region 1
15
(16.0%) followed by Region 3 (11.4%) and Region 5 (11.0%). The lowest utilization of the LPHI on‐line resources is in Region (9.1%). And, 21% of the on‐line audience represented more than one region of the Commonwealth or were from outside of the state.
Problem #6: Although the LPHI offers tremendous opportunities for improving the skills and
knowledge of the LPH workforce, too few people know about the LPHI or its offerings. The LPHI needs
an effective communications and marketing plan to address this problem. To address problem #6, the
LPHI will accomplish the following objective: Have an effective communications and marketing plan. The
figure below shows progress made toward the objective.
A developed plan for marketing the LPHI and its offerings
The LPHI is included in the integrated communications plan for the Office of Public Health Practice at BUSPH, which was completed in early 2011. The plan contains target audiences, tactics for branding and messaging, and metrics for measuring reach. The LPHI website was revised and re‐launched in 2011 with a new learning management system (LMS) that tracks course registration and course completion. The LMS integrates pre/post tests and evaluations for the online modules. The LPHI website also promotes LPHI trainings, updates, and partner events/trainings. All educational offerings and the Fellows Program were publicized on the LPHI website, using the BUSPH Constant Contact List, in the LPHI newsletter and through information forwarded to the public health
16.0%
9.1%11.4%
10.0%
13.2%
5.9%
11.0%
2.3%
21.0%
0.0%
5.0%
10.0%
15.0%
20.0%
25.0%
Regions in which on‐line learners work
16
associations who disseminate the material to their members.
Explore incentives for training All graduates of the Foundations Course received a certificate of completion and nurses, sanitarians and health officers who completed all pre/post‐tests were awarded contact hours that are applicable toward their continuing education credits. A certificate of completion and contact hours are available to those who complete the on‐line modules if they also complete the evaluation component of the module. As further modules are developed, the LPHI staff are considering ‘bundling’ and issuing certificates for completion in sets (e.g., an environmental health certificate or a public health nursing certificate). The Fellows Program was launched in 2011 to recognize significant contributions to public health practice and to create an incentive among prospective fellows to attain more training and to provide more service. The program evaluation showed that the majority of fellows felt the fellows program motivated them to get more training.
# of newsletters, flyers and calendars
Three Community Engagement Newsletters and five promotional flyers were sent to the MA public health workforce to promote the work of the Institute. Additionally, a training calendar was developed to better coordinate training efforts with MDPH and the six public health associations.
The desired short‐term outcomes of our work to address problem #6 are described below. Increased awareness of the LPHI and its programs: During the 18‐month period, 496 people showed interest in LPHI trainings by registering for various educational offerings. Seven individuals began and six successfully completed the LPHI Fellows application process. The interest in training and the Fellows program demonstrate an awareness of the LPHI offerings. Additionally, more than 80 people attended the induction ceremony for the LPHI fellows thanks to the marketing efforts associated with the event. During the reporting period, 3,719 hits to the website enabled users to access on‐line training. Of those, 3,192 were unique users. To date, there have been more than 28,000 hits to the LPHI website, over 7,000 of which are returning visitors. Identify and utilize incentives when feasible: As noted above, the certificates of completion and contact hours for courses, classroom and on‐line serve as incentives for training. Additionally, most of the new LPHI Fellows indicated that the program motivated them to consider additional training in order to become a fellow.
Increased registrations for LPHI trainings: During the reporting period, 496 people registered for LPHI offerings, more than ten times the number that registered for courses in the first year in which BUSPH managed the LPHI contract, which indicates that the a solid foundation for marketing and training were built in the 2010 and that tremendous progress was made in the last 18 months to increase the educational offerings and ensure that the LPH workforce learned about the available LPHI training opportunities.
17
Intermediate and longer‐term outcomes:
As the LPHI progresses toward its objectives over time, we expect to achieve one intermediate and one
longer‐term outcome. The nature of the longer‐term outcome is that we must make progress toward
our objectives and achieve short‐ and intermediate‐term outcomes before we are able to see evidence
that our longer‐term outcome is coming to fruition. We did not expect to see such evidence in yet, but
will report on our ability to achieve the longer‐term objectives in subsequent annual reports.
The intermediate outcome is: Improved cross‐cutting, program area and emergency preparedness
competencies among the local public health workforce who have received training from the LPHI. It is a
“primary level outcome,” which means that we should see improved competencies among our primary
target (i.e., members of the local public health workforce who participate in LPHI trainings). In the
reporting period, the data related to this outcome comes from several trainings:
The Foundations Course: The 18 sessions of the course cover 12 of 17 program area and 7 of 10 cross
cutting competencies at the awareness level. The evaluation yielded the following results:
Likert scale ratings related to 100 course learning objectives showed that students perceived
that they were more capable of performing the learning objectives associated with each of the
sessions after training than before each session.
In 17 sessions, students completed quiz questions before training and again at the completion of
the session. The evaluation found improvements in 74 of 84 questions from pre‐test to post‐test
but only 25 of those improvements were statistically significant. Significant improvements from
pre‐ to post‐test took place in relation to 14 of 17 sessions.
For each session, students were asked to use a Likert scale (1=strongly disagree) to (5=strongly
agree) to rate their agreement with the following statement: The content will be useful to me in
my work. The ratings for the 18 sessions ranged between a low of 3.86 and a high of 4.75. The
utility of the course manual for trainees’ work received a mean score of 4.30.
All of these indicators of success are better than or equal to the success of the Foundations
Course in 2010.
Legal Nuts and Bolts: The participants in part I and part II rated their perceived ability to perform the
learning objectives associated with their respective training session prior to and after training.
Participants in both Parts I and II felt better prepared to perform their session learning objectives as a
result of training. Using a Likert Scale (5=strongly agree to 1=strongly disagree), participants were asked
to indicate their level of agreement with the statement “The content will be useful to me in my work.”
For Part I participants, the mean was 4.69. For Part II, the mean was 4.53.
Personal Protective Equipment (PPE): Participants in the PPE session rating their ability to perform the
session learning objective prior to and after training. For all three learning objectives, participants felt
better prepared to perform the objectives as a result of training. Using the 5‐point Likert scale used to
18
evaluate the other sessions, the mean level of agreement with the statement “The content will be useful
to me in my work” was 4.75.
Infectious Disease Surveillance, Reporting and Control: Participants in the surveillance session rating
their ability to perform the seven learning objectives before and after training. On all seven,
participants rated themselves as better prepared to perform the objectives as a result of training.
Additionally, 100% of trainees agreed with the statement “The content will be useful to me in my work.”
EHTER Course: The mean score of the pre‐test was 75% correct with a range of 50 to 90% whereas, at
post‐test, the mean increased to 88% with a range of 65 to 100% of correct responses. Participants
were asked to rate their knowledge of the training topics before and after training using a Likert scale of
(0=none to 4=extensive). On all topics, mean ratings increased from pre to post.
The longer‐term outcome is: Improved agency performance in areas related to competencies in which
agency personnel have been trained by the LPHI. It is a “secondary level outcome,” which means that an
expected result of LPHI training is that agencies will benefit from the increased competencies of their
staff that have been trained by the LPHI and that, consequently, agency performance related to those
competencies should improve. We expect to measure this outcome in future years of the LPHI.
The learning objectives and content of each session are tied directly the public health competencies.
Appendices B and C show which of competencies are addressed by current trainings and those in
planning. The evaluation findings associated with the blended and classroom sessions indicate that
trainees feel better prepared to perform the objectives associated with the training content as a result
of training and that the training will be useful in their work. And, in the case of the Foundations Course,
statistically significant improvements in learning took place. All of these positive findings are indications
of improved competencies among the trainees involved in the LPHI.
In 2012, we will begin to look at the evaluation data associated with the on‐line modules to understand
their impact on trainees and the associated competencies.
When presented information about the LPHI’s progress over the reporting period during a recent LPHI
Advisory Committee meeting conducted via webinar, Committee members were asked to indicate
whether the LPHI’s achievements failed to meet, met or exceeded their expectations for what the LPHI
was supposed to accomplish over the time period. Eight of 13 indicated that their expectations were
met and the remaining five said their expectations were exceeded.
Conclusions and Next Steps: The 18‐month reporting period was very productive with
significant progress made toward all six program objectives. Below, the major accomplishments are
summarized and are followed by a list of recommended next steps.
19
Summary of accomplishments:
The LPHI expanded its capacity for distance learning and offered seven on‐line modules in
addition to the Orientation to Local Public Health: Bed Bugs; Dealing with Stress in Disasters:
Building Psychological Resilience; Legal Nuts and Bolts of Isolation and Quarantine, Parts 1 and
2; Lyme Disease; MAVEN and MAVEN TB Training Modules; and Swimming Pools. Like the
Orientation module, all but the MAVEN modules have a facilitator’s guide to assist in use of the
module as a teaching tool for classroom learning. 10 additional modules are already in
development for 2012.
The Foundations Course was run for the second time since BUSPH assume the LPHI contract, the
EHTER was offered, and the PPE, Surveillance and Legal Nuts and Bolts Parts 1 and 2 were
offered in 2011. In all four trainings, participants rated themselves as better able to perform
session learning objectives as a result of training and felt the training content would be useful in
their jobs. Additionally, statistically significant improvements in learning took place in 14 of 17
sessions of the Foundations Course and quiz scores improved from pre‐ to post‐test in the
EHTER course.
398 trainees received education in the LPHI’s training sessions during the reporting period.
Trainees represent all of the Public Health Emergency Preparedness Regions of the state,
although the lowest representation was among public health practitioners in Region 2: Central
MA at only 7.5%. The trainees are primarily local health directors/agents, public health nurses,
“other” positions (e.g., EP coordinators, regional public health staff), sanitarians/inspectors, and
BOH members/chairpersons.
The LPHI Fellows Program was launched and, based on evaluation results, was very successful in
meetings the program objective and in its marketing, application and selection criteria, and
recognition event.
The LPHI Advisory Committee met six times and has representation from all MDPH EP regions,
six public health associations, and five academic institutions.
Collaborative planning with LPHI partners took place and will expand LPHI offerings in 2012,
including additional on‐line modules which are in development, basic and advanced risk
communications training.
The marketing and communications plan was implemented in 2011 and involved the use of the
LPHI website, use of Constant Contact, outreach via the public health associations, and
newsletters to market LPHI offerings. The number of registrations for trainings, applicants for
the Fellows Program, and attendance at the Fellows induction ceremony are all indicators that
marketing efforts were successful.
Data were collected via training evaluations to supply the LPHI with an on‐going assessment of
training needs among LPHI users. The LPHI evaluation strategy also allowed for the tracking of
progress toward LPHI objectives and the identification of next steps for the year ahead.
Overall, the LPHI’s progress met or exceeded the expectations of its Advisory Group Committee
members.

20
Recommended next steps for year two:
There are few recommended changes for the sake of quality improvement for the coming year. Most of
the recommendations involve continuing to build on the successes to date, including:
Continuing to deliver and evaluate the blended and classroom sessions and begin to evaluate
the impact of the on‐line modules. Developing the additional modules scheduled for 2012 and
ensure each has an evaluation component.
Building on the successful launch of the LPHI Fellows Program.
Continuing collaborative planning with partners to deliver training and develop new offerings.
Continuing to use of the communications and marketing plan and implement products to
increase awareness of LPHI offerings and the Fellows Program.
Continuing to evaluate LPHI progress toward objectives.
Recommended changes or new initiatives are limited and include:
Exploring the relatively low utilization of LPHI offerings by those in Region 2: Central MA.
Analyzing the data associated with the existing on‐line modules to understand the impact of
distance learning options on LPH competencies.
Plan for evaluation of the secondary/ long‐term outcome ‐ Improved agency performance in
areas related to competencies in which agency personnel have been trained by the LPHI.
21
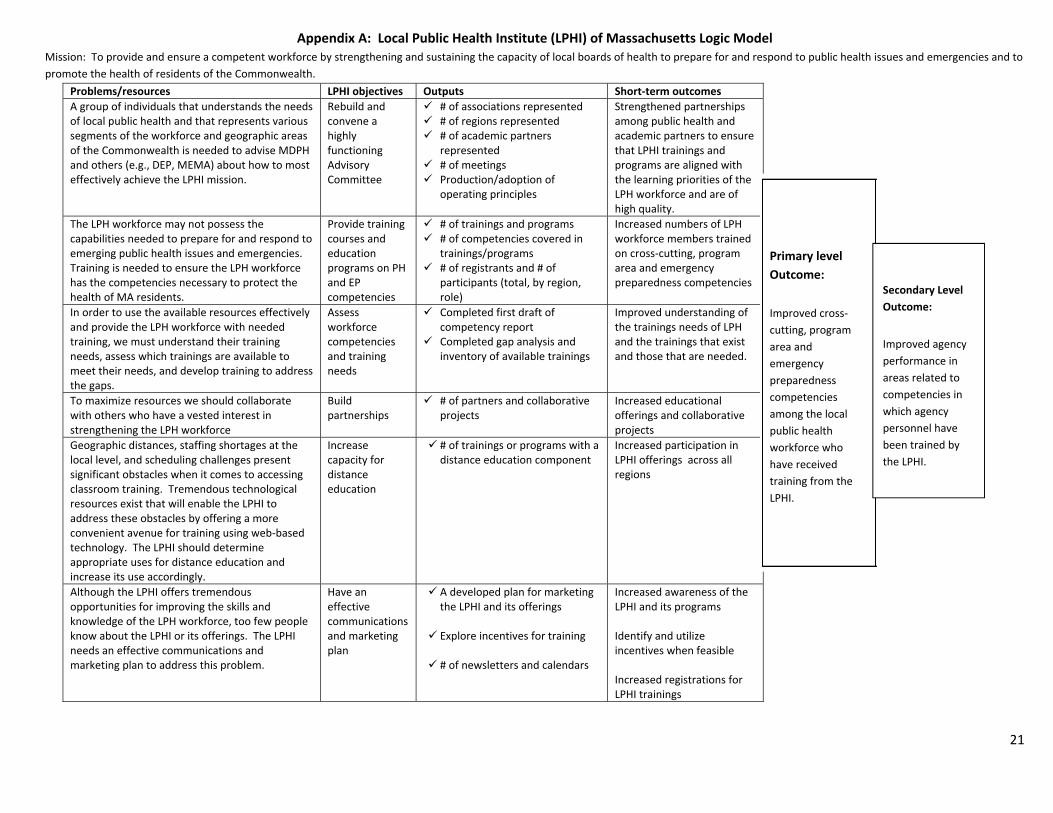
Appendix A: Local Public Health Institute (LPHI) of Massachusetts Logic Model Mission: To provide and ensure a competent workforce by strengthening and sustaining the capacity of local boards of health to prepare for and respond to public health issues and emergencies and to
promote the health of residents of the Commonwealth.
Problems/resources LPHI objectives Outputs Short‐term outcomes
A group of individuals that understands the needs of local public health and that represents various segments of the workforce and geographic areas of the Commonwealth is needed to advise MDPH and others (e.g., DEP, MEMA) about how to most effectively achieve the LPHI mission.
Rebuild and convene a highly functioning Advisory Committee
# of associations represented # of regions represented # of academic partners
represented # of meetings Production/adoption of
operating principles
Strengthened partnerships among public health and academic partners to ensure that LPHI trainings and programs are aligned with the learning priorities of the LPH workforce and are of high quality.
The LPH workforce may not possess the capabilities needed to prepare for and respond to emerging public health issues and emergencies. Training is needed to ensure the LPH workforce has the competencies necessary to protect the health of MA residents.
Provide training courses and education programs on PH and EP competencies
# of trainings and programs # of competencies covered in
trainings/programs # of registrants and # of
participants (total, by region, role)
Increased numbers of LPH workforce members trained on cross‐cutting, program area and emergency preparedness competencies
In order to use the available resources effectively and provide the LPH workforce with needed training, we must understand their training needs, assess which trainings are available to meet their needs, and develop training to address the gaps.
Assess workforce competencies and training needs
Completed first draft of competency report
Completed gap analysis and inventory of available trainings
Improved understanding of the trainings needs of LPH and the trainings that exist and those that are needed.
To maximize resources we should collaborate with others who have a vested interest in strengthening the LPH workforce
Build partnerships
# of partners and collaborative projects
Increased educational offerings and collaborative projects
Geographic distances, staffing shortages at the local level, and scheduling challenges present significant obstacles when it comes to accessing classroom training. Tremendous technological resources exist that will enable the LPHI to address these obstacles by offering a more convenient avenue for training using web‐based technology. The LPHI should determine appropriate uses for distance education and increase its use accordingly.
Increase capacity for distance education
# of trainings or programs with a distance education component
Increased participation in LPHI offerings across all regions
Although the LPHI offers tremendous opportunities for improving the skills and knowledge of the LPH workforce, too few people know about the LPHI or its offerings. The LPHI needs an effective communications and marketing plan to address this problem.
Have an effective communications and marketing plan
A developed plan for marketing the LPHI and its offerings
Explore incentives for training
# of newsletters and calendars
Increased awareness of the LPHI and its programs Identify and utilize incentives when feasible Increased registrations for LPHI trainings
Primary level
Outcome:
Improved cross‐
cutting, program
area and
emergency
preparedness
competencies
among the local
public health
workforce who
have received
training from the
LPHI.
Secondary Level
Outcome:
Improved agency
performance in
areas related to
competencies in
which agency
personnel have
been trained by
the LPHI.
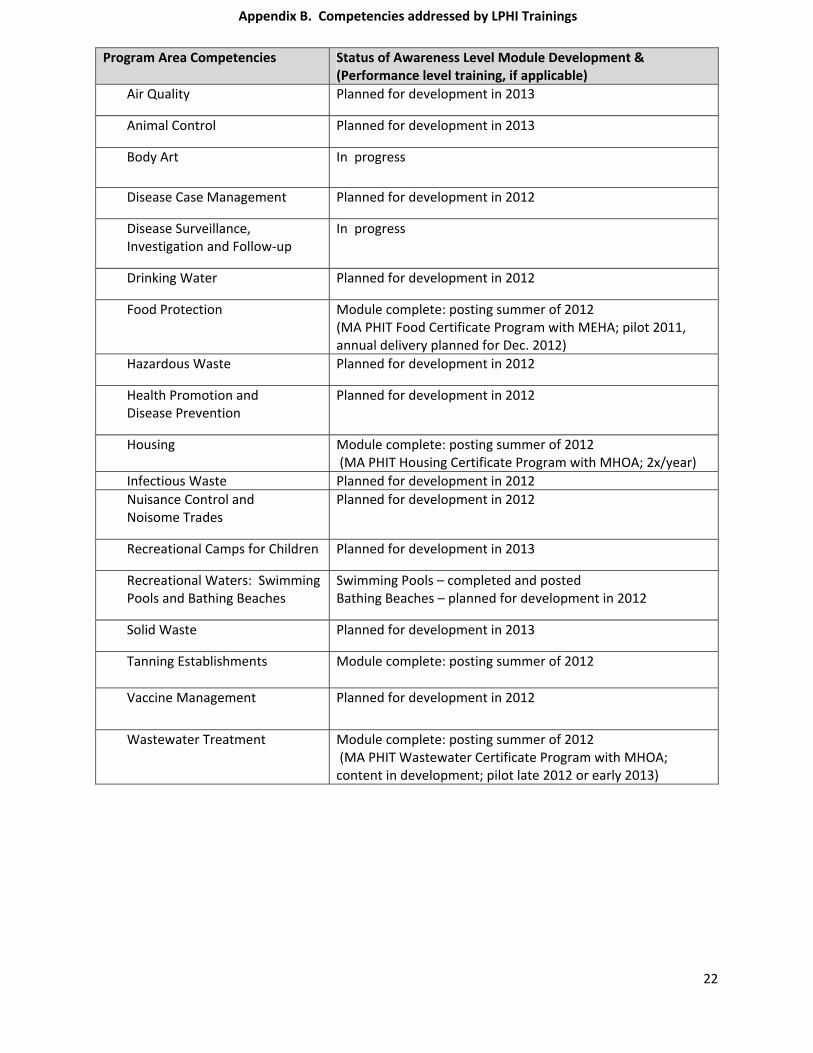
22
Program Area Competencies
Status of Awareness Level Module Development & (Performance level training, if applicable)
Air Quality
Planned for development in 2013
Animal Control
Planned for development in 2013
Body Art In progress
Disease Case Management
Planned for development in 2012
Disease Surveillance, Investigation and Follow‐up
In progress
Drinking Water
Planned for development in 2012
Food Protection
Module complete: posting summer of 2012 (MA PHIT Food Certificate Program with MEHA; pilot 2011, annual delivery planned for Dec. 2012)
Hazardous Waste
Planned for development in 2012
Health Promotion and Disease Prevention
Planned for development in 2012
Housing
Module complete: posting summer of 2012 (MA PHIT Housing Certificate Program with MHOA; 2x/year)
Infectious Waste Planned for development in 2012
Nuisance Control and Noisome Trades
Planned for development in 2012
Recreational Camps for Children
Planned for development in 2013
Recreational Waters: Swimming Pools and Bathing Beaches
Swimming Pools – completed and posted Bathing Beaches – planned for development in 2012
Solid Waste
Planned for development in 2013
Tanning Establishments
Module complete: posting summer of 2012
Vaccine Management
Planned for development in 2012
Wastewater Treatment Module complete: posting summer of 2012 (MA PHIT Wastewater Certificate Program with MHOA; content in development; pilot late 2012 or early 2013)
Appendix B. Competencies addressed by LPHI Trainings
23
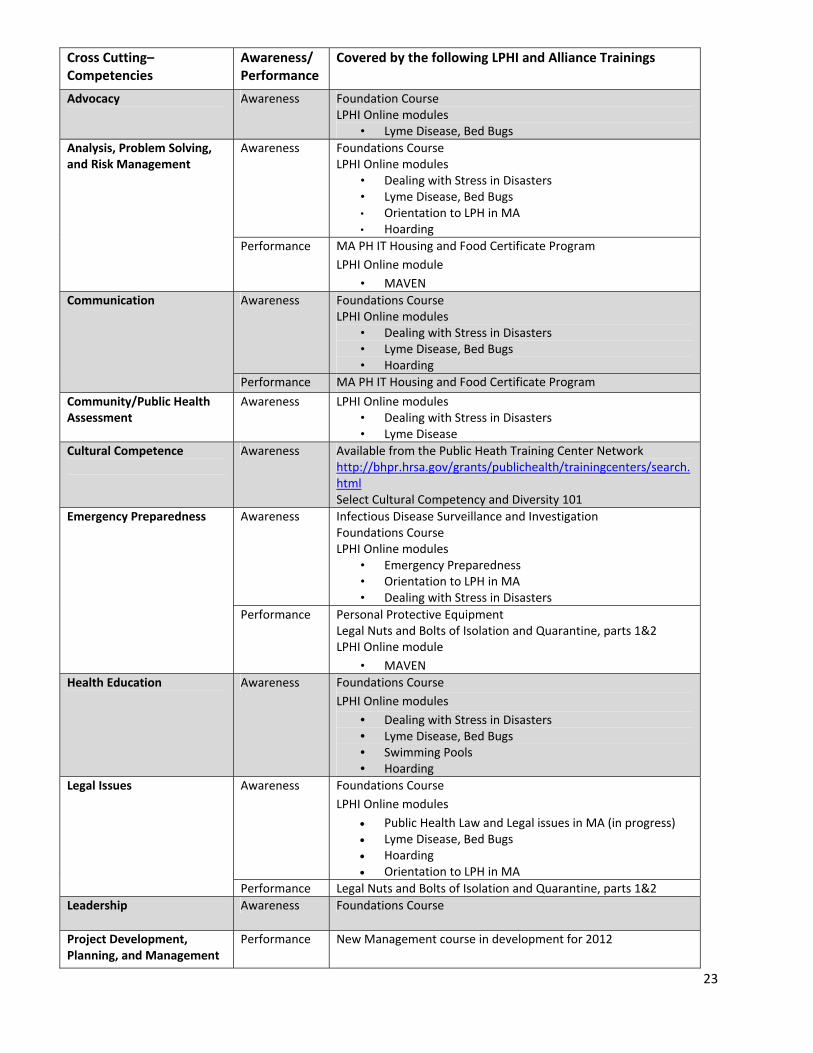
Cross Cutting– Competencies
Awareness/ Performance
Covered by the following LPHI and Alliance Trainings
Advocacy
Awareness Foundation Course LPHI Online modules
• Lyme Disease, Bed Bugs
Analysis, Problem Solving, and Risk Management
Awareness Foundations CourseLPHI Online modules
• Dealing with Stress in Disasters • Lyme Disease, Bed Bugs • Orientation to LPH in MA • Hoarding
Performance MA PH IT Housing and Food Certificate Program
LPHI Online module
• MAVEN
Communication Awareness Foundations CourseLPHI Online modules
• Dealing with Stress in Disasters • Lyme Disease, Bed Bugs • Hoarding
Performance MA PH IT Housing and Food Certificate Program
Community/Public Health Assessment
Awareness LPHI Online modules• Dealing with Stress in Disasters • Lyme Disease
Cultural Competence
Awareness Available from the Public Heath Training Center Network http://bhpr.hrsa.gov/grants/publichealth/trainingcenters/search.html Select Cultural Competency and Diversity 101
Emergency Preparedness Awareness
Infectious Disease Surveillance and Investigation Foundations Course LPHI Online modules
• Emergency Preparedness • Orientation to LPH in MA • Dealing with Stress in Disasters
Performance Personal Protective EquipmentLegal Nuts and Bolts of Isolation and Quarantine, parts 1&2 LPHI Online module
• MAVEN
Health Education
Awareness Foundations Course
LPHI Online modules
• Dealing with Stress in Disasters • Lyme Disease, Bed Bugs • Swimming Pools • Hoarding
Legal Issues
Awareness Foundations Course
LPHI Online modules
Public Health Law and Legal issues in MA (in progress) Lyme Disease, Bed Bugs Hoarding Orientation to LPH in MA
Performance Legal Nuts and Bolts of Isolation and Quarantine, parts 1&2
Leadership Awareness Foundations Course
Project Development, Planning, and Management
Performance New Management course in development for 2012
24
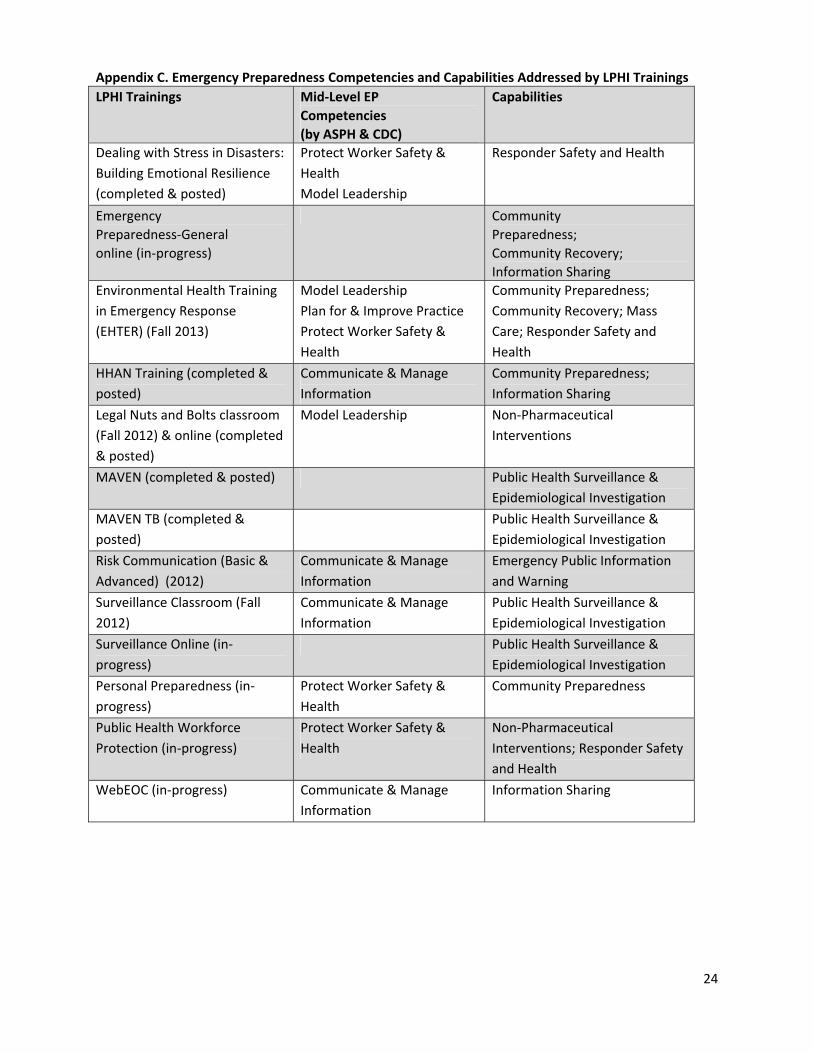
Appendix C. Emergency Preparedness Competencies and Capabilities Addressed by LPHI Trainings
LPHI Trainings Mid‐Level EP
Competencies
(by ASPH & CDC)
Capabilities
Dealing with Stress in Disasters:
Building Emotional Resilience
(completed & posted)
Protect Worker Safety &
Health
Model Leadership
Responder Safety and Health
Emergency
Preparedness‐General
online (in‐progress)
Community
Preparedness;
Community Recovery;
Information Sharing
Environmental Health Training
in Emergency Response
(EHTER) (Fall 2013)
Model Leadership
Plan for & Improve Practice
Protect Worker Safety &
Health
Community Preparedness;
Community Recovery; Mass
Care; Responder Safety and
Health
HHAN Training (completed &
posted)
Communicate & Manage
Information
Community Preparedness;
Information Sharing
Legal Nuts and Bolts classroom
(Fall 2012) & online (completed
& posted)
Model Leadership Non‐Pharmaceutical
Interventions
MAVEN (completed & posted) Public Health Surveillance &
Epidemiological Investigation
MAVEN TB (completed &
posted)
Public Health Surveillance &
Epidemiological Investigation
Risk Communication (Basic &
Advanced) (2012)
Communicate & Manage
Information
Emergency Public Information
and Warning
Surveillance Classroom (Fall
2012)
Communicate & Manage
Information
Public Health Surveillance &
Epidemiological Investigation
Surveillance Online (in‐
progress)
Public Health Surveillance &
Epidemiological Investigation
Personal Preparedness (in‐
progress)
Protect Worker Safety &
Health
Community Preparedness
Public Health Workforce
Protection (in‐progress)
Protect Worker Safety &
Health
Non‐Pharmaceutical
Interventions; Responder Safety
and Health
WebEOC (in‐progress) Communicate & Manage
Information
Information Sharing
25
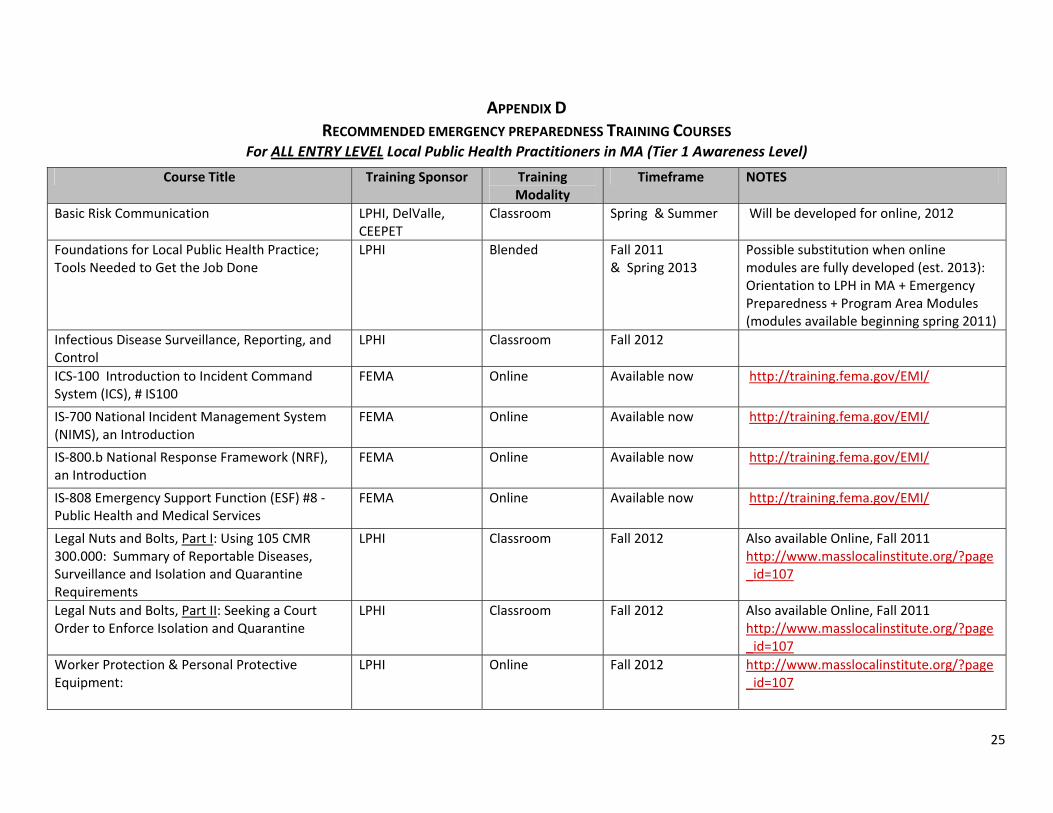
APPENDIX D RECOMMENDED EMERGENCY PREPAREDNESS TRAINING COURSES
For ALL ENTRY LEVEL Local Public Health Practitioners in MA (Tier 1 Awareness Level)
Course Title Training Sponsor Training Modality
Timeframe NOTES
Basic Risk Communication LPHI, DelValle, CEEPET
Classroom Spring & Summer Will be developed for online, 2012
Foundations for Local Public Health Practice; Tools Needed to Get the Job Done
LPHI Blended Fall 2011 & Spring 2013
Possible substitution when online modules are fully developed (est. 2013): Orientation to LPH in MA + Emergency Preparedness + Program Area Modules (modules available beginning spring 2011)
Infectious Disease Surveillance, Reporting, and Control
LPHI Classroom Fall 2012
ICS‐100 Introduction to Incident Command System (ICS), # IS100
FEMA Online Available now http://training.fema.gov/EMI/
IS‐700 National Incident Management System (NIMS), an Introduction
FEMA Online Available now http://training.fema.gov/EMI/
IS‐800.b National Response Framework (NRF), an Introduction
FEMA Online Available now http://training.fema.gov/EMI/
IS‐808 Emergency Support Function (ESF) #8 ‐ Public Health and Medical Services
FEMA Online Available now http://training.fema.gov/EMI/
Legal Nuts and Bolts, Part I: Using 105 CMR 300.000: Summary of Reportable Diseases, Surveillance and Isolation and Quarantine Requirements
LPHI Classroom Fall 2012 Also available Online, Fall 2011 http://www.masslocalinstitute.org/?page_id=107
Legal Nuts and Bolts, Part II: Seeking a Court Order to Enforce Isolation and Quarantine
LPHI Classroom Fall 2012 Also available Online, Fall 2011 http://www.masslocalinstitute.org/?page_id=107
Worker Protection & Personal Protective Equipment:
LPHI Online Fall 2012 http://www.masslocalinstitute.org/?page_id=107
26
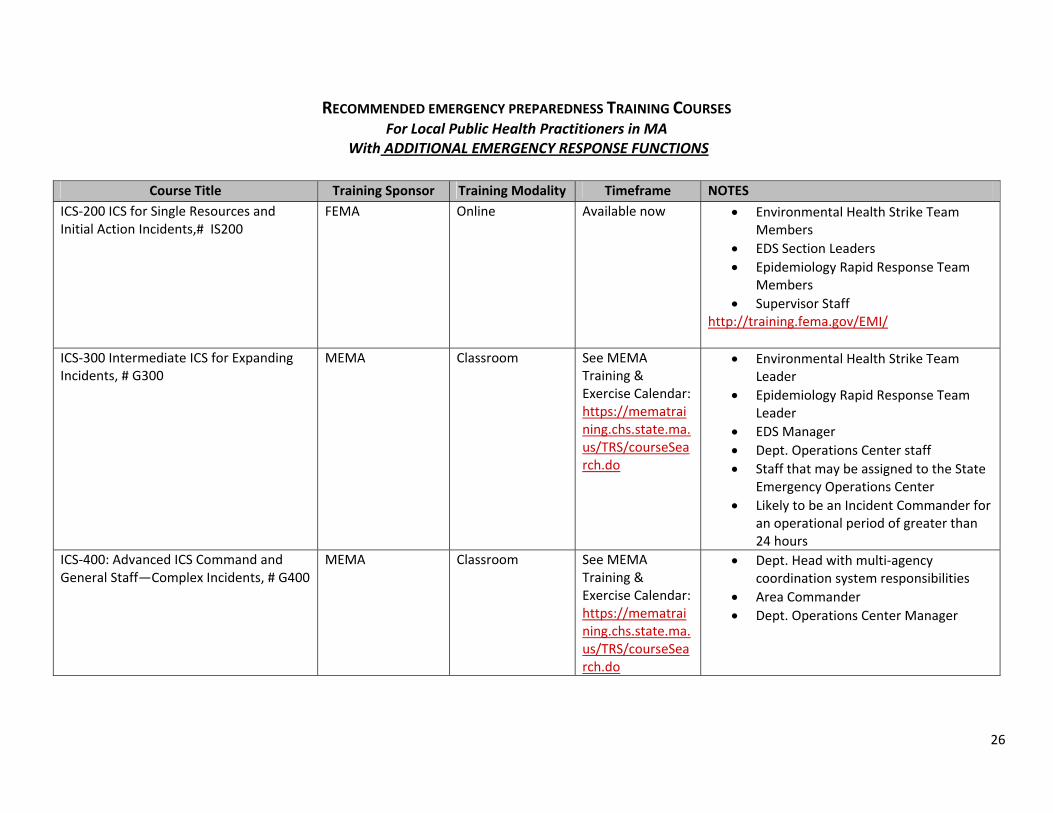
RECOMMENDED EMERGENCY PREPAREDNESS TRAINING COURSES For Local Public Health Practitioners in MA
With ADDITIONAL EMERGENCY RESPONSE FUNCTIONS
Course Title Training Sponsor Training Modality Timeframe NOTES
ICS‐200 ICS for Single Resources and Initial Action Incidents,# IS200
FEMA Online Available now Environmental Health Strike Team Members
EDS Section Leaders
Epidemiology Rapid Response Team Members
Supervisor Staff http://training.fema.gov/EMI/
ICS‐300 Intermediate ICS for Expanding Incidents, # G300
MEMA Classroom See MEMA Training & Exercise Calendar: https://mematraining.chs.state.ma.us/TRS/courseSearch.do
Environmental Health Strike Team Leader
Epidemiology Rapid Response Team Leader
EDS Manager
Dept. Operations Center staff
Staff that may be assigned to the State Emergency Operations Center
Likely to be an Incident Commander for an operational period of greater than 24 hours
ICS‐400: Advanced ICS Command and General Staff—Complex Incidents, # G400
MEMA Classroom See MEMA Training & Exercise Calendar: https://mematraining.chs.state.ma.us/TRS/courseSearch.do
Dept. Head with multi‐agency coordination system responsibilities
Area Commander
Dept. Operations Center Manager
27
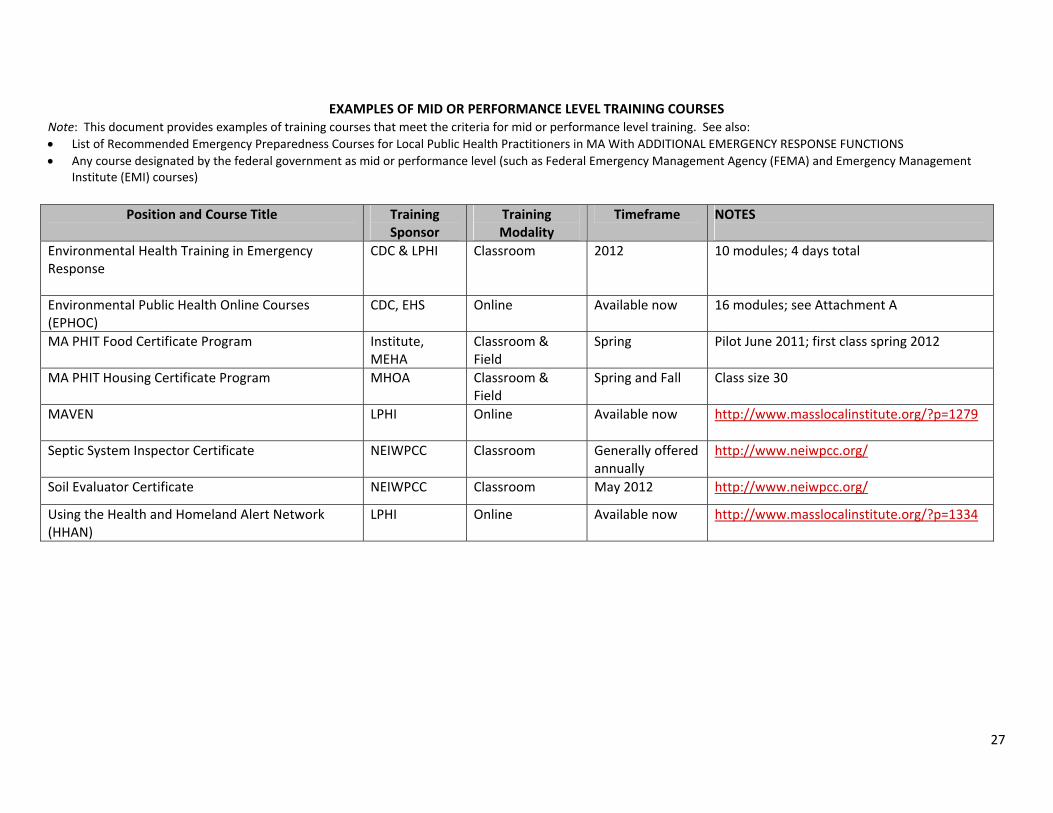
EXAMPLES OF MID OR PERFORMANCE LEVEL TRAINING COURSES Note: This document provides examples of training courses that meet the criteria for mid or performance level training. See also:
List of Recommended Emergency Preparedness Courses for Local Public Health Practitioners in MA With ADDITIONAL EMERGENCY RESPONSE FUNCTIONS
Any course designated by the federal government as mid or performance level (such as Federal Emergency Management Agency (FEMA) and Emergency Management Institute (EMI) courses)
Position and Course Title Training
Sponsor Training Modality
Timeframe NOTES
Environmental Health Training in Emergency Response
CDC & LPHI Classroom 2012 10 modules; 4 days total
Environmental Public Health Online Courses (EPHOC)
CDC, EHS Online Available now 16 modules; see Attachment A
MA PHIT Food Certificate Program
Institute, MEHA
Classroom & Field
Spring Pilot June 2011; first class spring 2012
MA PHIT Housing Certificate Program
MHOA Classroom & Field
Spring and Fall Class size 30
MAVEN LPHI Online Available now http://www.masslocalinstitute.org/?p=1279
Septic System Inspector Certificate NEIWPCC Classroom Generally offered annually
http://www.neiwpcc.org/
Soil Evaluator Certificate NEIWPCC Classroom May 2012 http://www.neiwpcc.org/
Using the Health and Homeland Alert Network (HHAN)
LPHI Online Available now http://www.masslocalinstitute.org/?p=1334