-
8/8/2019 The Mandala of Psicoterapea
1/6
Psychotherapy Volume 26/Fall 1989/Number 3
THE MANDALA OF PSYCHOTHERAPY: THE UNIVERSALUSE OF PARADOXNEW
UNDERSTANDINGAND MORE CONFUSION
GERALD J. MOZDZIERZ, JOSEPH LISIECKI,AND FRANK J.
MACCHITELLIHines VA Hospital
Regardless of differences in definition,paradox is widely
practiced and writtenabout in the psychotherapy literature.This
article suggests a graphic"mandala" as a way of examiningparadox
based on three dimensionsinvolved in the paradoxicalintervention:
type of delivery ("hard" or"soft"); type of patient ("neurotic"
or"psychotic"); degree of explicitnessor implicitness. The
implications of thismanda la for therapists are discussedincluding
the need to heightenawareness of the little understood anddelicate
interaction between thetherapist's personality, the type ofclient,
and the strategic paradoxicalinterventions used in treatment.
The mandala in its various forms symbolizes thedifferent levels
of energy locked in the human or-ganism. . . . A properly drawn
mandala is a bookin itself containing a great deal of information
buthe who would read the symbols must learn the lan-guage. Jaco bs,
1961, cited in DeRopp, 1968Jay Haley (1963) described the paradox
in psy-
chotherapy in a s imple yet e legant way: "Whena therapist
indicates he will help a patient over aproblem and within that
framework he encourages
Correspondence regarding this article should be addressedto
Gerald J . Mozdzierz, Psychology Service, VeteransAdministration,
Edward Hines, Jr. Hospital, H ines, IL 60141.
the patient to have the problem, he is posing aformal paradox .
. . defining the situation as be-nevolent the therapist provides an
ordeal" (p. 66).Since Haley's landmark w ork, the
professionalliterature (e.g., Selvini-Palazzoli et al.,
1978;Watzlawick et al., 1974; Weeks & L'Ab ate, 1981)has been
inundated regarding the concept of par-adox in psychotherapy.
Controversy regardingprecisely what constitutes and what does not
con-stitute paradox in therapy has also been abundant(Dell, 1981;
Jessee & L'Abate, 1981; Selvini-Palazzoli, 1 981; Wa tzlawick,
1981).A number of attempts in the literature (Fisheret al., 1981;
Johnson & Alevizos, 1975; Om er,1982; Raskin & Klein, 1976;
Rohrbaugh et al.,1977, 1981; Weeks & L'A bate , 1979) have
beenmade to systematize thinking about the paradox.While the
paradox defies a definitive description,over the years it has
seductively invited descriptionsand elaborations of its essence in
what amountsto a "tower of theoretical B abe l." That is ,
paradoxis something that innumerable therapists have de-scribed
using different languages based on theidiosyncrasies of particular
theories, heuristicbiases, and so on to explain very much the
sameconcept. While specific use of paradoxical
strat-egies/approaches/techniques in psychotherapy forpurposes of
behavioral change has been discussedin the literature under a
variety of names for over70 years (Mozdzierz et al., 1976), we
agree withWatzlawick et al. (1974) that "little serious
andsystematic inquiry has been focused on this wholematter, which
has remained as puzzling and con-tradictory as ever" (p. XIII).A
num ber of years ago we began searching fora way of categorizing
what we considered to beaccounts of explicit paradoxical
strategies/inter-ventions in psychotherapy (Mozdzierz et al.,
1973).The essential purpose of the exercise was to develop
383
-
8/8/2019 The Mandala of Psicoterapea
2/6
G. J.Mozdzierz et al.some understanding of what we perceived to
bethe different ways in which a variety of practitionerseither
explicitly used paradoxical interventions orwere implicitly
paradoxical in their therapies asHaley (1963) suggested. Since we
were personallyacquainted with several of these practitioners
itseemed self-evident that some of them could neverdo with clients
what others of them did withaplomb. Over a period of time we
organized thework of a sample of clinicians with whose writingswe w
ere familiar into a threefold graphic schematicwhich we have
designated the "mandala of psy-chotherapy." The purpose of this
article is to de-scribe this mandala and some of the implicationsof
how it is organized for clinicians.The Universal Use of ParadoxMany
of the practitioners represented in themandala of Figure 1
practiced from widely di-vergent frames of reference, although some
arefrom the same school of psychotherapy. Para-doxically, even
though some of the practitionersin Figure 1 are from the same
school, they practicedin diverse ways. The reader will note that
thereare three basic reference dimensions to our mandala:the
Horizontal Axis, the Vertical Axis, and theConcentric Circle
Dimension.Horizontal Axis: Neurotic/Psychotic
The Neurotic/Psychotic horizontal axis of themandala represents
the basic continuum of patient
HARD
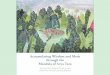
SOFTFigure 1. Proposed distribution of a sample of clinicians'
useof paradox along three dimensions: patient behavior
(neurotic/psychotic), personal approach of therapist (hard/soft),
andstructure of the paradoxical intervention
(implication/explicit).
behavior encountered by the therapist-theoreticiansdistributed
throughout the figure. Psychotic refersto the most stubborn,
confused, chaotic, aso cial,resistant, and at times bizarre
behaviors encounteredand written about by these authors; neurotic
refersto the more subtle sufferings of people anxiously(or
depressively) struggling to find their place inlife's arenas of
work, intimacy, family, and friends.The authors cited to the left
of the vertical axisdescribed patients who were primarily
neurotic.Those authors to the right of the vertical axisdescribed
(or worked with) psychotic patients.Milton Erickson can actually be
cited throughoutthe figure since his range of therapeutic
skill,talent, and flexibility in relating to a wide rangeof
patients under a variety of clinical circumstancesis legendary and
generally acknowledged to betruly exceptional (Barker, 1986;
Beahrs, 1971;Haley, 1977; Hammond, 1984). Farrelly is citedin both
the neurotic and psychotic dimensionssince Farrelly is presumably
paradoxically pro-vocative to all patients.Vertical Axis:
Hard/Soft
The Hard/Soft vertical axis represents the basiccontinuum of the
therapist's type of delivery orstyle of paradoxical intervention. W
e propose thatit is based, in part, on the characteristics of
thattherapist's personality. The delivery to or inter-vention with
the patient could be soft or hard.Soft refers to the gentle, kind,
persuasive, en-couraging, subtle, and rational, approaches
ofpractitioners such as Alfred Adler, Victor Frankl,Rudolph
Dreikurs, and Kurt Adler, who mightencourage patients to view their
anxiety as a reliablefriend who will be there when the need
arises.Hard refers to the more dramatic,
confrontational,challenging, provocative, and active
therapeuticapproaches such as those demonstrated by Rosen(1953) and
Kraupl-Taylor (1969) who deliberatelysought to provoke patients
into action or opposition.Hard interventions cited, in general,
tend tomatch the more dramatic and bizarre patient be-haviors, in
other words "meeting fire with fire."These interven tions are
proportionate to or greaterthan the degree of symptomatic patient
behaviorin question or offer the patient a
worse/differentalternative by placing the patient's behavior in
alarger context/frame. To summarize this hard/softdistinction,
Frankl might explain the rationale forhis intervention as if the
client were a colleague;he would attempt to persuade gently. On the
otherhand, Kraupl-Taylor advocated therapeuticallyprovoking patient
rebellion away from their
384
NEUROTIC
psYCHOTIC
-
8/8/2019 The Mandala of Psicoterapea
3/6
The Mandala of Psychotherapysymptomatic behavior by associating
their symp-toms with unacceptable sexual mean ings. W e
hy-pothesize that it is not simply a difference in the-oretical
perspective that allows for such hard versussoft differences in
delivery; we hypothesize thatthe personality of the practitioner
also plays arole. Some practitioners would be more comfortablewith
one type of approach and some more com-fortable with another.Circle
Dimension: Implicit/Explicit
To complete the description of our proposedmandala, paradoxical
interventions can either bevery explicit or subtle and implicit.
From the centerof the figure radiating outward are a series
ofconcentric circles. The center circle representspractitioners who
were implicitly paradoxical asHaley (1963) suggested. Thus Freud
and Rogersrepresent orientations that are intrinsically/im-plicitly
paradoxical; in effect, they are paradoxicalby the nature of their
activities. For example,Freud (1977) cautioned h is early audiences
to re-ceive his controversial psychosexual theories withskepticism
lest they become outcast from theirprofessional communities and
that psychic traumamust somehow be reexperienced (prescribed)
inorder to be resolved. That which patients havestruggled so much
to avoid must be reexperiencedin order to receive help a "benign
ordeal" (Haley,1963, 1984).At the outer circle, the use of paradox
by thepractitioners listed can be depicted as explicit.Haley (1963,
1984), Erickson (1959), and B eier's(1966) names are synonymous
with overt para-doxical interve ntions. Rosen (1953) at the
explicitperimeter of the circle talks about dealing withdelusions
("tricks") through use of exceptionallydramatic, deliberately
rehearsed, and orchestrated,paradoxical interventions which he
labeled a "trickagainst a trick." In locating Rosen within the m
an-dala, the reader w ill note that he is in the "ha
rd,""psychotic," and "explicit" axes of the figure re-garding his
unusual methods.Examples from Around the Mandala
At this point the reader may find it helpful tosee concrete
examples of how some of the therapistsin the mandala prac tice
their paradoxical/dialecticapproaches. A clinical sample of a
paradoxicalresponse to a patient and the rationale for thatresponse
from Farrelly & Brandsma (1974) andtheir Provocative Therapy we
locate in the "hard/explicit/neurotic" sector of the mandala. This
in-tervention is the exact dialectically opposite and
paradoxical response from what a client mightexpect:Another
patient asked, "Well, wh y am I this way?" Therapist(with
professional profundity): Well, it's very clear. Obviouslyyou had
crooked chromosomes to start off with, your motherblighted your
life, and your environment chew ed up what wasleft! So what the
hell chance do we have of changing you!"(p. 74)Their rationale for
this intervention is straight-forward:The inferences and constructs
used to provide answers are notimportant in themselves, only to the
extent that they takeimportant aspects o f behavioral and social
reality into account.The provocative therapist, therefore, will
offer and often bur-lesque explanations of all types. The burlesque
will clearlyindicate that behavior is more important than
explanation, (p.74 )
The hardness of this confrontation and its ex-plicitness
constitute what can be considered anoutrageously paradoxical
response to a patient en-quiry; it is a response and an explanation
to thepatient but not the kind that he expected. Webelieve that
Farrelly is not the least bit malevolentin responding this
way.Still another hard and explicit intervention, butthis time with
a psychotic patient, can be seenfrom the work of Rosen (1953) and
his "directpsychoanalysis":A patient had successfully denied his
psychotic behavior byinsisting his trouble was malformation of the
spine with anextra bone sticking out in back. He also had a most
unusualspringing step which he partly attributed to the spinal
defect.On the day when I recognized that I was admitted to
hispsychosis, I was impressed by two new things in his attitude.He
kept turning his head toward me instead of not looking atme as was
his custom and when I asked him to let me feelhis hand (cold and
moist), he extended his hand to me whereasheretofore I could only
examine it by force. Addressing myremarks to two other doctors and
his nurse, I stated: ''Let mesee, walking on my toes. I did that
when I was crazy. Whatwas it my psychiatrist said to me oh yes, I
recall. You'retrying to be a woman. You walk as though you had
high-heeled shoes on. But I don't believe in that nonsense. (To
thepatient): Would you like a cup of coffee? I think we have
somecake in the house." The patient remarked, 'Wo, were youreally
insane, Doctor? D id you really have that foot pull? Itseems to
pull up from the muscles of my leg. You never hada spine disease."
I replied: "Neither have you. A person whohas been through your
insanity understands these things, butenough of this psychology
nonsense." I then addressed myselfagain to the others, ignoring the
patient's manifest interest inmy alleged symptom. After a few
minutes of talk about baseballand politics, the patient
interrupted, "How can you believethat I want to be a girlT I bade
the patient good nigh t, offeringto shake his hand in leave-taking,
but he withdrew it, stating,"/ do that with ordinary people. I
don't care to leave. Youare the only one who has ever been
sincere." (pp. 19-20)
385
-
8/8/2019 The Mandala of Psicoterapea
4/6
G. J.Mozdzierz et al.The reader will observe that Rosen's
interventionis far from "benign" or "tame"; to the contrary,it is
very dramatic; in fact the above vignette isin our opinion not one
of the more dramatic ex-amples he cites. His explanation for
"lying" to
the patient represents a different view from thoseof Farrelly
& Brandsma (1974) but a paradoxicalone nevertheless:In every
case where the patient persists in denying the existenceof the
psychotic basis for his behavior, when I can, I makebelieve I was
once psychotic and had just those symptoms.The patient must face
the fact that I am not crazy now. If Iever was crazy with those
symptoms, I got well. Why shouldn'the get well too? If he thinks
that maybe I'm lying to him, hetakes it for a kindhearted lie and
many times after psychosis,with good humor and just a little
ashamed, he will assert, "Iknew it was a big lie. Maybe it wasn't
true, but it surelywarmed me toward you." (p. 20).A patient's
delusions are seen as a "trick devisedby his unconscious censorship
faculties to hidefrom consciousness something basically
moredangerous to him than the delusion itself" (p .148). In turn,
Rosen uses a "trick against thetrick" (his dramatic, staged,
rehearsed paradoxicalconfrontations) which don't "cure" but which
helpspush patients toward greater insight.As an example from the
explicit, soft, neuroticaxis of the mandala we offer a clinical
vignetteof a paradoxical redefining of symptoms fromKurt Adler
(1972):For this girl, for w hom her parents represented her only
security,to take a definitive step towards independence, away
fromthem, and join her life to a stranger (by getting married),
wasmore than she dared. H owever, social pressures, competitionwith
her sister, and her self-image of a mature, efficient person,which
she felt she had to uphold at any cost, put her on thehorns of a
dilemma. At that moment, her long trained andoften proven mechanism
of mobilizing anxiety came to heraid, like an old trusted friend.
Because no w, it was not herself,but her sickness that prevented
her from doing what she wasin reality not prepared to do. Since she
is not conscious ofthis, she can easily delude herself, and
hopefully also others.That was the time to tell her, "You know,
that reminds meof your early recollection, when you were little,
and yourmother wanted to leave you alone. You would cry, and
showsuch fears until your mother decided to stay home with you.And
now, you are thinking of leaving your mother, and avery similar
anxiety appears to come over you. You have,evidently, still not
really prepared yourself for sufficient in-dependence. Nobody can
do what he has not prepared himselffor. And you had alw ays been
such a good girl, different frommany others; you never rebelled
against your parents, whoover-protected you; where should you have
prepared for in-dependence.
Now she has official permission, doctor's advice to postponewhat
she is so afraid of doing, (p. 167)The reader will note that Adler
uses no humor
in this vignette, he is supportive of the patient'sbehavior,
gentle and persuasive but neverthelesssuggesting to this patient
that her anxiety is herfriend who returns to her when she really
needsit.Still another example from the soft, explicit,neurotic
sector of the mandala can be found inthe therapeutic w ork of
Victor Frankl (1955) whoutilizes a more grandfatherly approach in
dealingwith essentially neurotic, middle-class patients.His
patients are described as professional peoplewho fear public
speaking, airplane trips, socialengagements, operas, and so on. His
patientspresent three basic conditions: a "fear of fears,"which
produces avoidance patterns of behaviorsor a flight from fears; a
"fight against" obsessive-
compulsive behaviors or an attempt to suppressurges; and a
"fight for something," which attemptsto produce something but
actually prevents itsoccurrence.Frankl (1955) invites his patients
to seek whatthey have been avoiding, to invite what they'vebeen
fighting, and to replace a fear with a wish.He has instructed his
patients to "resolve delib-erately to show those whom he was with
at thetime how much he could really sweat . . . myheart should beat
even faster . . . or try very hard
to be as panicky as possible ." Symptoms w ere tobe exaggerated
to the point of absurdity.Frankl's paradoxical intentions were
alwaysdelivered with a good deal of humor w hich helpedto promote a
necessary self-detachment in viewingthe symptom as opposed to Kurt
Adler's approachnoted above, which was persuasive and
morestraightforward and "serious." Frankl (1955)maintained that
"when the patient began to laughabout his neurotic symptom, humor
entered inand helped to put distance between himself and
his neurosis." Hum or was antidote to what Franklidentified as
Heidegger's "sorrowful concern per-meating the human condition."
Frankl's collegialrelationship with his patients is captured in
hisadvice: "The therapist must never tire of encour-aging the
patient to continue to use paradoxicalintention over and over just
as his neurosis pro-duces the symptom over and ov er." As one
patientremarked , "W henever I deliberately tried to trembleI was
unable to do so."DiscussionTo this point in our presentation the
reader, asa devotee of the paradox, may ask, "So what?"In response
to this question we reply that our
386
-
8/8/2019 The Mandala of Psicoterapea
5/6
The Mandala of Psychotherapyintention in this article is to
expose the reader toseveral hypotheses, namely: 1) paradox is a
universal tool of encouragement in psychotherapythat is used and
written about by innumerablepractitioners under a variety of names
almost sincethe inception of psychotherapy; 2) of necessity,there
is an interaction between the type of patient/behavior, the
personality of the therapist, and thetype of paradoxical
intervention; 3) the mandalasimply represents one way of
graphically repre-senting this interesting dynamism; and 4)
theseobservations have implications for our under-standing of this
fascinating tool of therapy andits use with patients.Relative to
the last point above, obviously, thereare any number of
practitioners whose names andwritings have not been included in our
"ma ndala."Also a therapist of the stature and genius of M
iltonErickson could adopt paradoxical interventionsseemingly
without limit to any number of patientsand their behaviors. His
exceptional flexibilityand ability to form intense
rapport/relationshipswith patients appears to be the essential key
tounderstanding his phenomenal success with hispatients (Barker,
1986; Hammond 1984). Perhapsthat represents the essence of the
"world class"psychotherapist. Although it is probably difficultfor
us as a group to admit, most therapists havea more limited range of
abilities to relate andadapt interventions (paradoxical or
otherwise) tothe particular peculiarities and circumstances ofthe
patients, problems, and behaviors they en-counter. As Cummings
(1986) has said:It is a propensity of psychotherapy that every
patient whowalks into a therapist's office receives the type of
therapy thepsychotherapist has to offer. If the therapist is a
Freudiananalyst, he or she does not care what the patient
hasal-coholism, m arital problems, or job proble ms that patient
isgoing to get the couch. If the therapist is a Jungian analyst,the
patient is going to paint pictures. If the therapist is
abehaviorist, the patient is going to get desensitization.
(p.429)
Thus, as we see it, it is not unreasonable toexpect that the
limitations of therapists' framesof reference and their general
personalities certainlyinfluence not only what they practice bu t
also howthey practice and more specifically how they "de-liver"
paradoxical interventions to different pa-tients. A paradoxical
intervention/prescription canbe presented to a patient or client as
the truth; anoutrageous and absurd lie; simply another way
oflooking at things; a suggestion possibly havingvalue; a
challenge; a provocation; a twist of irony;
a humorous "nudging"; and so on.We believe that therapists are
most likely touse the type of paradoxical interventions that
arecompatible with their own personalities. For ex-ample, Farrelly
is probably more comfortable thanmost therapists in being ab le to
engage in the typeof nimble-tongued, witty, "burlesque"
paradoxicalinterventions for which he is noted. Correspond-ingly,
Frankl might be very uncomfortable in usingsuch interventions. On
the other hand, O'Connell's(1967, 1969) empathic, philosophical,
therapeuticuse of paradoxical wit is in keeping with the breadthof
his natural humanistic identification.We conjecture that effective
and caring therapistsmost likely modulate their paradoxical
interventionsin keeping with the vicissitudes of each
patient'sunique situation and the limitations of their
ownpersonalities. That is, if therapists are optimallyflexible (an
obviously ideal good toward whichwe strive but do not attain), they
are most likelyto modify the "delivery" of a paradoxical
inter-vention in keeping with and respect for the per-sonality of
the patient as well as their situation.If they are m inimally
flexible, therap ists are likelyto deliver paradoxical
interventions in a rathermechanistic cookbook manner as a
"technique."It is our opinion that paradox cannot be
mechan-istically applied but must rather be strategicallyrelated to
the patient and the dynamics of his orher personality and
situation. In this regard, wehave heard such naive practices
expressed by novicetherapists in comments such as, "I paradoxed
thatpatient!"We note with interest that, outside of MiltonErickson,
Farrelly, Rosen, Jackson, and Goldstein,the practitioners
distributed in our mandala tendto cluster themselves within the
neurotic/soft/ex-plicit quadrant, while few practitioners can
befound in the psychotic/hard/explicit quadrant. Wesuggest that
this may be so because paradoxicalinterventions with psychotics are
very difficult.Such patients are oftentimes so very concrete
intheir thinking, and therapists' personalities havelimitations in
the degree of flexibility and therange of interventions which they
can employwithin their theoretical frames of reference in re-sponse
to bizarre psychotic patient behaviors.The paradox is a powerful
and ubiquitous eh-couragenic therapeutic tool for promoting
change.In that regard it is not unlike the story of the blindmen
who each have hold of a different part of anelephant and therefore
describe and interpret thecreature at hand from their own point of
view. It
387
-
8/8/2019 The Mandala of Psicoterapea
6/6
G. J.Mozdzierz et al.is our contention that more attention needs
to begiven to the dynamism that we suggest is createdbetween the
patient, his or her situation, and thetherapist's personality in
understanding paradox.It is incumbent upon therapists who are
familiarwith the paradox as a therapeutic tool to examinethe
parameters within which they operate whenusing paradoxical
interventions. From a more co-herent understanding of this
ubiquitous vehiclefor change can emerge a more enlightened,
sen-sitive, effective, and ethical clinical use.ReferencesADLER, K.
(1972). Techniques that shorten psychotherapy:Illustrated with five
cases. Journal of Individual Psychology,28 , 155-168.BARKER, P.
(1986). Milton Erickson's contribution to psy-chiatry. British
Journal of Psychiatry, 148, 471-475.BEAHRS, J. O. (1971). The
hypnotic psychotherapy of MiltonH. Erickson. American Journal of
Clinical Hypnosis, 14,73-90.BEIER, E. (1966). The Silent Language
of Psychotherapy:Social Reinforcement of Unconscious Processes.
Chicago:Aldine.CUMMINGS, N. (1986). The dismantling of our health
system:Strategies for the survival of psychological practice.
AmericanPsychologist, 41 , 426-431.DELL, P. F. (1981). Some
irreverent thoughts on paradox.Family Process, 20, 37-42.DEROPP, R.
S. (1968). The Master Game: Beyond the Drug
Experience. New York: Delta Book/Dell Publishing.FISHER, L.,
ANDERSON, A. & JONES, J. (1981). Types ofparadoxical
interventions and indications/contraindicationsfor use in clinical
practice. Family Process, 20, 25-35.ERICKSON, M . (1959). Further
clinical techniques of hypnosis:Utilization techniques. American
Journal of Clinical Hyp-nosis, 1, 3-21.FARRELLY, F. & BRANDSMA,
J. (1974). Provocative Therapy.Cupertino, Calif.: Meta
Publications.FRANKL, V. (1955). The Doctor and the Soul. New
York:Alfred A. Knopf.FRANKL, V. (1960). Paradoxical intention: A
logotherapeutictechnique. American Journal of Psychotherapy, 14 ,
520-
535.FREUD, S. (1977). Introductory Lectures to Analysis on
Psy-choanalysis: A General Introduction to Psychoanalysis. NewYork:
Liveright.HALEY, J. (1963). Strategies of Psychotherapy. New
York:Grune & Stratton.HALEY, J. (1977). Uncommon Therapy; The
Psychiatric Tech-nique of Milton H. Erickson, M.D. New York: W.
W.Norton.
HALEY, J. (1984). Ordeal Therapy: U nusual Ways to
ChangeBehavior. San Francisco: Jossey-Bass.HAMMOND, C. (1984).
Myths about Erickson and Ericksonianhypnosis. American Journal of
Clinical Hypnosis, 26, 236-245.JACOBS , H. (1961). Western
Psychotherapy and Hindu Sadhana.
London: Allen & Unwin.JESSEE, E. & L'ABATE, L. (1981).
Comments on Dell's paper.Family Process, 20, 42-44.JOHNSON, S. M.
& ALEVIZOS, P. (1975). Strategic therapy:A systematic outline
of procedures. Unpublished manuscriptportions of which were
presented at the Ninth Annual Con-ference of the Association for
the Advancement of BehaviorTherapy, San Francisco.KRAUPL-TAYLOR, F.
(1969). Prokaletic measures derived frompsychoanalytic technique.
British Journal of Psychiatry,115, 407-419.MOZDZIERZ, G.,
MACCHITELLI, F. & LISEECKI, J. (1973).Workshop on The Paradox
in Psychotherapy. Howard John-son's Motor Lodge, Desplaines,
Illinois.MOZDZIERZ, G., MACCHITELLI, F. & LISIECKI, J. (1976).
Theparadox in psychotherapy: An Adlerian perspective. Journalof
Individual Psychology, 32, 169-184.O'CONNELL, W. E. (1967).
Spitting and stroking. IndividualPsychologist, 5, 29-31.O'CONNELL,
W. E. (1969). Humor: The therapeutic impasse.Voices, 25,
29-31.OMER, H. (1982). Paradoxical treatments: A unified
concept.Psychotherapy: Theory, Research and Practice, 18 ,
320-324.RASKIN, D. E. & KLEIN, Z. E. (1976). Losing a
symptomthrough keeping it: A review of paradoxical techniques
andrationale. Archives of General Psychiatry, 33,
548-555.ROHRBAUGH, M ., TENNEN, H., PRESS, S., W H I TE, L.,
RASKIN,P ., PICKERING, M . & WATZLAWICK, P. (1977).
Paradoxicalstrategies in psychotherapy. Symposium presented at
theAnnual M eeting of the Am erican Psychological Association,San
Francisco.ROSEN, J. (1953). Direct Psychoanalysis: Vols. I &
II. NewYork: Grune & Stratton.SELVINI-PALAZZOLI, M. (1981).
Comments on Dell's paper.Family Process, 20,
44-45.SELVINI-PALAZZOLI, M. S., BOSCOLO, L., CECCHIN, G. &
PRATA, G. (1978). Paradox and Counterparadox. NewYork: Jason
Aronson.WATZLAWICK, P. (1981). Comments on Dell's paper. Family
Process, 2 0 , 4 5 - 5 1 .WATZLAWICK, P., WEAKLAND, J. &
FISCH, R. (1974). Change:Principles of Problem Formulation and
Problem Resolution.New York: W. W. Norton.WEEKS, G. R. &
L'ABATE, L. (1979). A compilation of par-adoxical methods. American
Journal of Family Therapy,7, 61-76.WEEKS, G. R. & L'ABATE, L.
(1981). Paradoxical Psycho-therapy. New York: Brunner/Mazel.
388