Embed Size (px)
Citation preview
JOHNSTON AND ROBINSON: MAXIMAL HISTALOG TEST 207
cent, whereas when saline was given there was an average fall in metabolic rate of 4 per cent. In all the cases shown in Table 11 there is an increase in oxygen consumption during and after the infusion. The maximum increase in metabolic rate recorded was 28.4 per cent with a dose of intralipid of 2 g. per kg. body-weight. In some cases the effect on the meta- bolic rate was very much less with a maximum increase of 12.4 per cent. The maximum figures recorded for the increase in metabolic rate of the 10 patients were 28.4, 28.1, 25.6, 19'5, 13.0, 12.4, 21.3, 23.1, 26.1, and 20.1 per cent. The average increase in metabolic rate of the patients was 21 per cent. The results in Cases 5 and 9 are shown in graphic form together with triglyceride and non-esterified free fatty acid levels (Figs. I, 2).
The respiratory quotient results all show some fall during or after infusion compared with the average figure before the start of the infusion. Some patients had a low resting respiratory quotient. This was noted particularly in Case 6 (0.72), who was suffering from carcinomatosis, and Case 10 (0.75), a case of achalasis of the cardia. A low respiratory quotient in debilitated patients might be expected as they are probably burning endogenous fat as a major source of calories. In these cases a further drop in respira- tory quotient has occurred, although the fall is small, from 0.72 to 0.70 and from 0.75 to 0.73. The fall in respiratory quotient does not persist throughout the experiments and, although the oxygen consumption usually remains elevated throughout the experimental periods, the respiratory quotient often rises later in the experiment, in some cases above the resting level. In Case 2 a respiratory quotient above I was recorded. This must be due to persistent overbreathing. This case did, however, show a significant increase in oxygen consumption.
DISCUSSION The results shown in this investigation demon-
strate that intralipid acts as a metabolic stimulus and causes an increase in oxygen consumption during and after infusion. The increased heat production from this will cause a feeling of well-being in the debilitated patient with a low basal metabolic rate.
The increase in oxygen consumption during and after infusion confirms that the emulsion is utilized. Only one patient has been studied with both saline and intralipid infusions, and the results show quite clearly the difference in oxygen consumption and metabolic rate with these two infusions.
It seems therefore that a fat emulsion is now available which is well tolerated in human beings. This has never been available before and there are many cases, mainly surgical, who will benefit from its use. Its use is not indicated unless the patient is in negative nitrogen balance and it should be given slowly. Protein, fat, and carbohydrate metabolism are so closely linked that the ideal form of parenteral nutrition would consist of all three, not necessarily in the same preparation, but delivered either on the same day or synchronously through a Y-connection to a single venous cannula.
SUMMARY Intralipid infusion stimulates oxygen consumption.
An average maximum increase in metabolic rate of 21 per cent occurred in the 11 patients studied. A saline infusion caused no rise in oxygen consumption or metabolic rate.
A fall in the respiratory quotient occurred in all the patients either during or after intralipid infusion. The respiratory quotient did not remain lowered, but often rose even above the resting level later in the experiment.
A drop in the respiratory quotient and evidence of metabolic stimulation during intralipid infusion add evidence that the emulsion is metabolized,
Acknowledgement.-I am grateful to Dr. W. J. Griffiths, Ph.D., St. Thomas's Hospital, London, for the gas-analysis estimations.
REFERENCES KINSELL, L. W., MICHAELS, G. D., and IMAIGHI, K.
SHAFIROFF, B. G. P., MULHOLLAND, J. H., and BAKER, J.
--- - Co TUI, ROTH, E., and BARON, H. C. (1949),
(1969, Am. 3. clin. Nutr., 16, 97.
(I951),3. exp. Med., 9, 185.
Surgery Gynec. Obstet., 89, 398.
THE MAXIMAL HISTALOG TEST OF GASTRIC SECRETION* A COMPARISON WITH THE HISTAMINE INFUSION TEST IN MAN
BY DAVID JOHNSTON AND D. W. ROBINSON UNIVERSITY DEPARTMBNT OF SURGERY, ROYAL INFIRMARY, SHEFFIELD
IMPROVED methods of measuring the maximal secretory capacity of the human stomach are being sought, following the demonstration that the aug- mented histamine test (Kay, 1953) elicits an acid out- put 25-30 per cent less than the maximum (Lawrie, Smith, and Forrest, 1964; Makhlouf, McManus, and Card, 1965). Pure gastrin will doubtless prove to be
* Based on a communication to the Surgical Research Society, July, 1966.
the ideal stimulus in the future, because it has no side-effects and because it alone elicits maximal secretion of acid from the human stomach (Makhlouf and others, 1969, but at present it is unobtainable. For practical purposes the choice seems to lie between the histamine infusion test, introduced in Britain by Lawrie and others (1964), and the histalog test, which has long been popular in North and South America, although it was only in 1965 that Laudano and Roncoroni defined the dose of histalog which
208
17'7
20'0
BRIT. J. SURG., 1967, Vol. 54, No. 3, MARCH
-___ -~ 17'1
22.6
produced maximal levels of gastric secretion. This paper presents the results of a comparative study of the maximal histalog test and the histamine infusion test, aimed at discovering which is the better for routine use. Particular attention was paid to the levels of secretion elicited by either method and to the incidence of side-effects.
lMATERIAL AND METHODS The subjects were 17 male patients, of whom 12
had duodenal ulcer, 2 gastric ulcer, and 3 dyspepsia without radiological evidence of gastro-intestinal abnormality. Their ages ranged from 24 to 67 years, with a mean of 40 years.
Histamine and Hista1og.-Histamine acid phos- phate, containing 36 per cent histamine base, was administered intravenously in a dose of 0.04 mg. per kg. per hour, by means of a slow injection pump, for 2 hours. Mepyramine maleate (anthisan), 50 or IOO mg., was injected intramuscularly 15 minutes before the start of the histamine infusion: the larger dose was given to subjects weighing more than 70 kg. Histalog (3-/hninoethylpyrazole dihydrochloride) was given subcutaneously into the flexor surface of the forearm in a dose of 2 mg. per kg. No antihistamine was given with it.
Procedure.-Each subject underwent the hista- mine and the histalog tests. There was an interval of at least a day between the tests and the order in which the tests were done was varied in random fashion. In the fasting subject a 16 F.G. neoplex tube was
passed through the nose into the stomach, the contents of which were aspirated and discarded. Continuous suction was then exerted, apart from frequent occasions when air was injected down the
4'0 5.3
13.2 28.0 20.7
- PATIENT
- - I
2
3 4 5 6 7
8 9
10
I1 12
13 14
1s 16 17
4'3 3'8
17.8 27.6 22'1
Mean -
22'2 23.0
28.2
18.3 12'0
tube to keep its lumen clear. Although the tube was not usually placed in position under radiological control, no effort was spared to ensure maximum recovery of the gastric juice secreted. Apart from close personal supervision, with frequent injection of air down the tube, the most useful measure was found to be that of asking the subject to take deep breaths and to tighten the abdominal muscles to 'pump' the acid out: small alterations of the position of the tube or of the patient were frequently rewarded by an increased aspirate in the ensuing minutes. In all the tests the stomach was emptied completely before the stimulant drugs were given, and in 12 of the 17 subjects aspiration of the spontaneous secretion for at least 30, and usually 45, minutes permitted a com- parison to be made between spontaneous and 'maximal ' secretion. Separate specimens representing 15-minute collections were taken throughout.
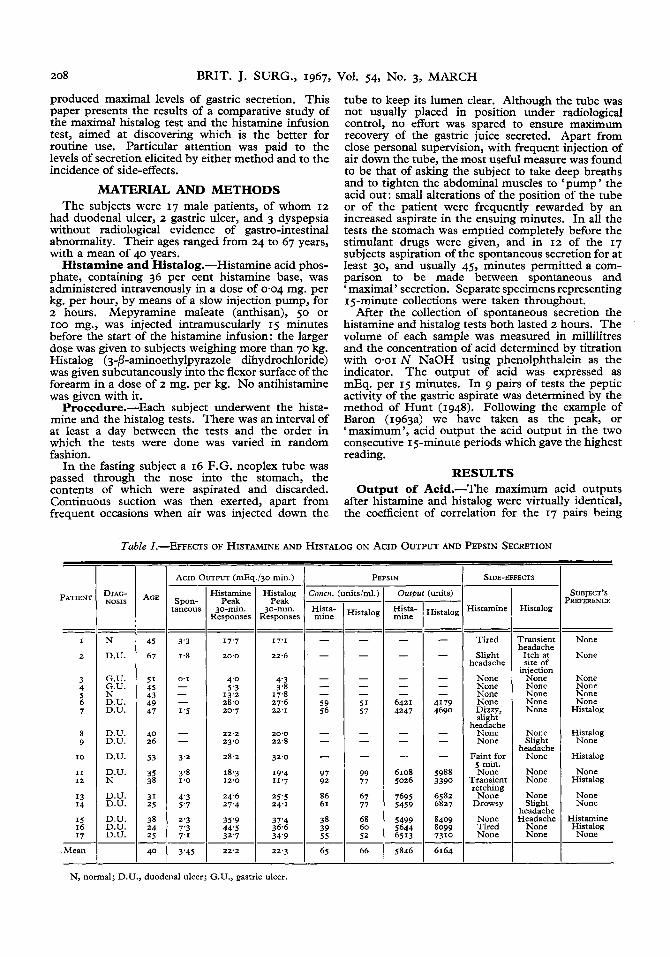
After the collection of spontaneous secretion the histamine and histalog tests both lasted 2 hours. The volume of each sample was measured in millilitres and the concentration of acid determined by titration with 0.01 N NaOH using phenolphthalein as the indicator. The output of acid was expressed as mEq. per 15 minutes. In 9 pairs of tests the peptic activity of the gastric aspirate was determined by the method of Hunt (1948). Following the example of Baron (1963a) we have taken as the peak, or 'maximum', acid output the acid output in the two consecutive 15-minute periods which gave the highest reading.
RESULTS Output of Acid.-The maximum acid outputs
after histamine and histalog were virtually identical, the coefficient of correlation for the 17 pairs being
20'0 22.8
32'0
19'4 11.7
Table I.-EFFECTS OF HISTAMINE AND HISTALOG ON ACID OUTPUT AND PEPSIN SECRETION - DIAG- NOSIS
- - N
D.U.
G.U. G.U. N D.U. D.U.
D.U. D.U.
D.U.
D.U. N
D.U. D.U.
D.U. D.U. D.U.
=
AGE
- - 45
67
5 1 45 43 49 47
40 26
53
35 38
31 25
38 24 25
40
- Spon- aneous
- - 3'3
1.8
0'1 - - - I ' 5
- - 3'2
3 4
4'3 5'7
2'3 7'3 7'1
I '0
~~~ ~
Histamine Histalog
30-mm. 30-min. Responses Responses I Peak
24.6 I 25'5 27'4 24.1
3'45
35'9 371'4 44'5 36.6 32'7 1 34'9
22'2 22'3 ~~
PEPSIN - dtslml.)
66
- outp1 -
Hista- mine - - - -
- - -
642 I 4247
- - -
6108 5026
7695 5459
5499 5644 6513
5846
- :units)
listalog -
- - - -
- - -
4179 4690
- - -
5988 3390
6582 6827
8099 7310
8409
6164
SIDE-EFFECTS
Histamine
Tired
Slight headache
None None None None Dizzy, slight
headache None None
Faint. for 5 min. None
Transient retching
None Drowsy
None Tired None
Histalog
Transient headache
Itch at site of
inlection None None None None None
None Slight
he a da ch e None
None None
None Slight
headache Headache
None None
SUBJECT'S ?REFERENCE
None
None
None None None None
Histalog
Histalog None
Histalog
None Histalog
None None
Histamine Histalog None
N, normal; D.U., duodenal ulcer; G.U., gastric ulcer.
JOHNSTON AND ROBINSON:
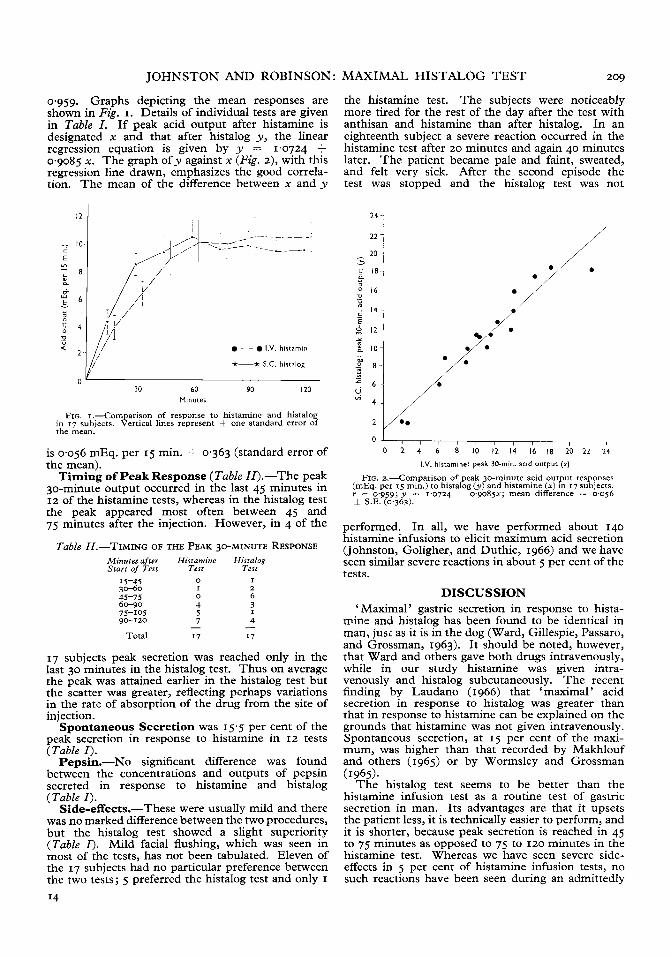
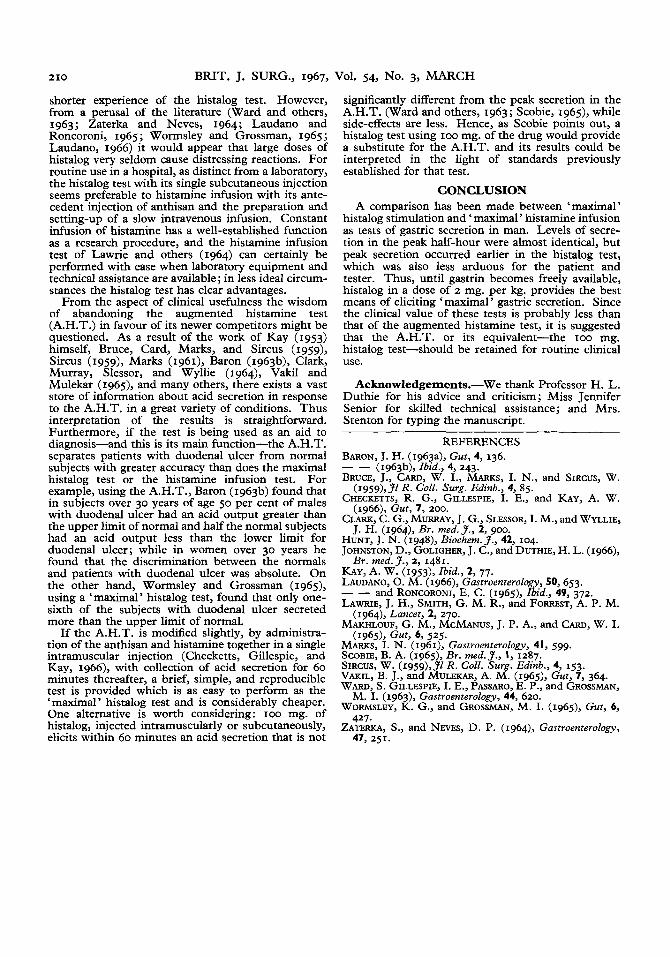
0.959. Graphs depicting the mean responses are shown in Fig. I . Details of individual tests are given in Table I . If peak acid output after histamine is designated x and that after histalog y, the linear regression equation is given by y = 1.0724 + 0.9085 x. The graph of y against x (Fig. z), with this regression line drawn, emphasizes the good correla-
The mean of the difference between x and y tion.
- E ?
0
w E
a
Y - ” 0 -2
2
I2 I I / I
_.-- , 10.
- ,
8
- - I.V. histamin
*-* S.C. histalog
6
30 60 90 I20
’Yf’ 2
0 30 60 90 I20
- - I.V. histamin
*-* S.C. histalog
Minutes
FIG. I .-Comparison of response to histamine and histalog in 17 subjects. Vertical lines represent & one standard error of the mean.
is 0.056 mEq. per 15 min. & 0.363 (standard error of the mean).
Timing of Peak Response (Table II).-The peak 30-minute output occurred in the last 45 minutes in 12 of the histamine tests, whereas in the histalog test the peak appeared most often between 45 and 75 minutes after the injection. However, in 4 of the
Table ZZ.-TIMING OF THE PEAK 30-MINUTE RESPONSE Minutes after Histamine Histalos Start of Test Test Test
15-45 0 I 30-60 I 2 45-75 0 6 60-90 4 3 75-105 5 I
4 90-120
Total I7 I7 - 7 -
17 subjects peak secretion was reached only in the last 30 minutes in the histalog test. Thus on average the peak was attained earlier in the histalog test but the scatter was greater, reflecting perhaps variations in the rate of absorption of the drug from the site of injection.
Spontaneous Secretion was 15.5 per cent of the peak secretion in response to histamine in IZ tests (Table I ) .
Pepsin.-No significant difference was found between the concentrations and outputs of pepsin secreted in response to histamine and histalog (Table I ) .
Side-effects.-These were usually mild and there was no marked difference between the two procedures, but the histalog test showed a slight superiority (Table I ) . Mild facial flushing, which was seen in most of the tests, has not been tabulated. Eleven of the 17 subjects had no particular preference between the two tests; 5 preferred the histalog test and only I I4
MAXIMAL HISTALOG TEST 209
the histamine test. The subjects were noticeably more tired for the rest of the day after the test with anthisan and histamine than after histalog. In an eighteenth subject a severe reaction occurred in the histamine test after 20 minutes and again 40 minutes later. The patient became pale and faint, sweated, and felt very sick. After the second episode the test was stopped and the histalog test was not
24 1
O I , , , , , , , , I
0 2 4 6 8 10 I2 14 16 18 20 22 24
I.V. histamine: peak 30-mi”. acid output (x)
FIG. 2.-Comparison of peak 30-minute acid output responses (mEq. per 15 min.) to histalog ( y ) and histamine (x) in 17 subjects. r = 0,959; y = 1.0724 +~ 0 , 9 0 8 5 ~ ; mean difference -= 0.056 & S.E. (0.363).
performed. In all, we have performed about 140 histamine infusions to elicit maximum acid secretion (Johnston, Goligher, and Duthie, 1966) and we have seen similar severe reactions in about 5 per cent of the tests.
DISCUSSION ‘ Maximal ’ gastric secretion in response to hista-
mine and histalog has been found to be identical in man, jusi as it is in the dog (Ward, Gillespie, Passaro, and Grossman, 1963). It should be noted, however, that Ward and others gave both drugs intravenously, while in our study histamine was given intra- venously and histalog subcutaneously. The recent finding by Laudano (1966) that ‘maximal’ acid secretion in response to histalog was greater than that in response to histamine can be explained on the grounds that histamine was not given intravenously. Spontaneous secretion, at 15 per cent of the maxi- mum, was higher than that recorded by Makhlouf and others (1965) or by Wormsley and Grossman
The histalog test seems to be better than the histamine infusion test as a routine test of gastric secretion in man. Its advantages are that it upsets the patient less, it is technically easier to perform, and it is shorter, because peak secretion is reached in 45 to 75 minutes as opposed to 75 to 120 minutes in the histamine test. Whereas we have seen severe side- effects in 5 per cent of histamine infusion tests, no such reactions have been seen during an admittedly
(1965).
210 BRIT. J. SURG., 1967,
shorter experience of the histalog test. However, from a perusal of the literature (Ward and others, 1963; Zaterka and Neves, 1964; Laudano and Roncoroni, 1965; Wormsley and Grossman, 1965; Laudano, 1966) it would appear that large doses of histalog very seldom cause distressing reactions. For routine use in a hospital, as distinct from a laboratory, the histalog test with its single subcutaneous injection seems preferable to histamine infusion with its ante- cedent injection of anthisan and the preparation and setting-up of a slow intravenous infusion. Constant infusion of histamine has a well-established function as a research procedure, and the histamine infusion test of Lawrie and others (1964) can certainly be performed with ease when laboratory equipment and technical assistance are available; in less ideal circum- stances the histalog test has clear advantages.
From the aspect of clinical usefulness the wisdom of abandoning the augmented histamine test (A.H.T.) in favour of its newer competitors might be questioned. As a result of the work of Kay (1953) himself, Bruce, Card, Marks, and Sircus (1959), Sircus (I959), Marks (1961), Baron (1963b), Clark, Murray, Slessor, and Wyllie (1964), Vakil and Mulekar (1969, and many others, there exists a vast store of information about acid secretion in response to the A.H.T. in a great variety of conditions. Thus interpretation of the results is straightforward. Furthermore, if the test is being used as an aid to diagnosis-and this is its main function-the A.H.T. separates patients with duodenal ulcer from normal subjects with greater accuracy than does the maximal histalog test or the histamine infusion test. For example, using the A.H.T., Baron (1963b) found that in subjects over 30 years of age 50 per cent of males with duodenal ulcer had an acid output greater than the upper limit of normal and half the normal subjects had an acid output less than the lower limit for duodenal ulcer; while in women over 30 years he found that the discrimination between the normals and patients with duodenal ulcer was absolute. On the other hand, Wormsley and Grossman (1965), using a ‘maximal’ histalog test, found that only one- sixth of the subjects with duodenal ulcer secreted more than the upper limit of normal.
If the A.H.T. is modified slightly, by administra- tion of the anthisan and histamine together in a single intramuscular injection (Checketts, Gillespie, and Kay, 1966), with collection of acid secretion for 60 minutes thereafter, a brief, simple, and reproducible test is provided which is as easy to perform as the ‘ maximal ’ histalog test and is considerably cheaper. One alternative is worth considering: 100 mg. of histalog, injected intramuscularly or subcutaneously, elicits within 60 minutes an acid secretion that is not
Vol. 54, No. 3, MARCH
significantly different from the peak secretion in the A.H.T. (Ward and others, 1963; Scobie, 1969, while side-effects are less. Hence, as Scobie points out, a histalog test using zoo mg. of the drug would provide a substitute for the A.H.T. and its results could be interpreted in the light of standards previously established for that test.
CONCLUSION A comparison has been made between ‘maximal’
histalog stimulation and ‘ maximal’ histamine infusion as tests of gastric secretion in man. Levels of secre- tion in the peak half-hour were almost identical, but peak secretion occurred earlier in the histalog test, which was also less arduous for the patient and tester. Thus, until gastrin becomes freely available, histalog in a dose of 2 mg. per kg. provides the best means of eliciting ‘maximal’ gastric secretion. Since the clinical value of these tests is probably less than that of the augmented histamine test, it is suggested that the A.H.T. or its equivalent-the IOO mg. histalog test-should be retained for routine clinical use.
Acknowledgements.-We thank Professor H. L. Duthie for his advice and criticism; Miss Jennifer Senior for skilled technical assistance; and Mrs. Stenton for typing the manuscript.
~
REFERENCES BARON, J. H. (1963a), Gut, 4, 136. -- (1963b), Ibid., 4, 243. BRUCE, J., CARD, W. I., MARKS, I. N., and SIRCUS, W.
CHECKETTS, R. G., GILLESPIE, I. E., and KAY, A. W.
CLARK, C. G., MURRAY, J. G., SLESSOR, I. M., and WYLLIE,
HUNT, J. N. (1948), Biochem. 3., 42, 104. JOHNSTON, D., GOLIGHER, J. C., and DUTHIE, H. L. (1966),
KAY, A. W. (I953), Ibid., 2, 77. LAUDANO, 0. M. (1966), Gastroenterology, 50, 653. _ - and RONCORONI, E. C . (1969, Ibid., 49, 372. LAWRIE, J. H., SMITH, G. M. R., and FORREST, A. P. M.
MAKHLOUF, G. M., MCMANUS, J. P. A., and CARD, W. I.
MARKS, I. N. (1961), Gastroenterology, 41, 599. SCOBIE, B. A. (1965), Br. med. J., I , 1287. SIRCUS, W. (1959),Jl R. Coll. Surg. Edinb., 4, 153. VAKIL, B. J., and MULEKAR, A. M. (1969, Gut, 7 , 364. WARD, S . GILLESPIE, I. E., PASSARO, E. P., and GROSSMAN,
WORMSLEY, K. G., and GROSSMAN, M. I. (1969, Gut, 6,
(1959),31 R. Coll. Surg. Edinb., 4, 85.
(1966), Gut, 7 , 200.
J. H. (1964, Br. med.J., 2, 900.
Br. med.J., 2, 1481.
(1964), Lancet, 2, 270.
(196519 Gut, 4 525.
M. I. (1963), Gastroenterology, 44, 620.
427.
47, 251. ZATERKA, S. , and NEVES, D. P. (1964, Gastroenterology,