Embed Size (px)
Citation preview

ARTHRITIS & RHEUMATISMVol. 43, No. 3, March 2000, pp 568–575© 2000, American College of Rheumatology
THE MECHANISM OF THE EFFECT OF OBESITY IN KNEEOSTEOARTHRITIS
The Mediating Role of Malalignment
LEENA SHARMA, CONGRONG LOU, SEPTEMBER CAHUE, and DOROTHY D. DUNLOP
Objective. Obesity is most strongly linked toosteoarthritis (OA) at the knee. Varus malalignmentwas examined as a possible local mediator that mayincrease the impact of body weight at the knee, versusthe hip or ankle. Compartment load distribution ismore equitable in valgus than in varus knees, andvalgus knees may better tolerate obesity. We thereforetested whether 1) body mass index (BMI) is correlatedwith OA severity in varus knees, 2) the BMI–OA severitycorrelation is weaker in valgus than in varus knees, 3)BMI is correlated with the severity of varus malalign-ment, and 4) the BMI–medial tibiofemoral OA severityrelationship is reduced after controlling for varus mal-alignment.
Methods. In 300 community-recruited patientswith knee OA, 2 groups (varus and valgus) were identi-fied based on dominant knee alignment on a full-limbradiograph, i.e., the angle formed by the intersection ofthe femoral and tibial mechanical axes. Severity of kneeOA was assessed by measurement of the narrowest jointspace width on radiographs of knees in a fluoroscopy-confirmed semiflexed position.
Results. Alignment direction was symmetric (orneutral in 1 limb) in 87% of patients. One hundredfifty-four patients had varus knees and 115 had valgusknees. BMI correlated with OA severity in the varusgroup (r 5 –0.29, P 5 0.0009) but not in the valgusgroup (r 5 –0.13, P 5 0.17). BMI correlated withmalalignment in those with varus knees (r 5 0.26) but
not in those with valgus knees (r 5 0.16). The partialcorrelation of BMI and OA severity, controlling for sex,was reduced from 0.24 (P 5 0.002) to 0.04 (P 5 0.42)when varus malalignment was added to the model.
Conclusion. BMI was related to OA severity inthose with varus knees but not in those with valgusknees. Much of the effect of BMI on the severity ofmedial tibiofemoral OA was explained by varus mal-alignment, after controlling for sex. Whether it precedesor follows the onset of disease, varus malalignment isone local factor that may contribute to rendering theknee most vulnerable to the effects of obesity.
Obesity is a risk factor for both the development(1–14) and progression (15–19) of knee osteoarthritis(OA). Obesity may also be linked to hip and hand OA;at these sites, the association has been inconsistentlydetected (7,19–25). Hypotheses to explain theobesity–OA relationship fall into 2 categories, metabolicand mechanical.
The preponderance of studies has not supporteda metabolic link between obesity and OA. For example,controlling for body fat distribution, diabetes, serumcholesterol level, uric acid level, and blood pressure didnot reduce the association between obesity and knee OAin the First National Health and Nutrition ExaminationSurvey (NHANES-I) data (5). These studies, with rareexception (26), report no independent relationship be-tween metabolic correlates of obesity and the presenceof OA (5–7,14,22,23).
The mechanical hypothesis has received less at-tention in epidemiologic investigation. A widespreadassumption is that the link between obesity and OA isthe repetitive application of greater axial load. In itself,this theory does not explain the difference in OAprevalence among the lower extremity joints. An expla-nation is offered in a paradigm in which obesity in-
Supported by NIH grant AR-30692.Leena Sharma, MD, Congrong Lou, MS, September Cahue,
BS, Dorothy D. Dunlop, PhD: Northwestern University, Chicago,Illinois.
Address reprint requests to Leena Sharma, MD, Division ofRheumatology, Northwestern University, Ward Building 3-315, 303East Chicago Avenue, Chicago, IL 60611. Email: [email protected].
Submitted for publication May 24, 1999; accepted in revisedform September 24, 1999.
568

creases OA risk through 1) direct effects, and 2) theinfluence of local factors that mediate the mechanicalimpact of excess body weight at the knee (Figure 1). Akey local factor is the longer moment arm in reference tothe center of gravity at the knee than at the hip or ankleduring many activities (27). Knee malalignment is an-other factor that influences how load is distributed at theknee and may also help to explain the predisposition ofobesity-associated knee OA to be bilateral and symmet-ric in compartment involvement.
Varus malalignment intensifies the effect of ex-cess body weight on the medial tibiofemoral compart-ment. Knee alignment is reflected by the angle made bythe intersection of the femoral and tibial mechanicalaxes. The lower extremity joints are normally colinear ornearly colinear (28–30). Clinically, the direction of mal-alignment is often symmetric. Varus malalignment in-creases medial compartment load; valgus malalignmentincreases lateral compartment load (28,31,32). In thenormally aligned, ambulating knee, load is dispropor-tionately transmitted to the medial compartment (33).Varus malalignment further increases the total loadpassing medially during gait (30). Although valgus mal-alignment is associated with an increase in lateral com-partment peak pressures (32), the medial compartmentoften continues to bear more load than the lateralcompartment until severe valgus malalignment ispresent (34,35).
This difference in the impact of varus versusvalgus malalignment on load distribution is well estab-lished. However, the effect of this difference on the
relationship between obesity and OA has not beenexamined. First, the direction of malalignment is likelyto affect the potency of obesity as a factor leading toprogressive knee OA. Because load is distributed betterin valgus than in varus knees, obesity should have asmaller impact in those with valgus knees. Bruns et alspeculated that with varus, but not valgus, malalignment,weight may have a “multiplying effect on the deteriora-tion of the knee” (32). Whether the obesity–OA severityrelationship differs between patients with varus kneesand those with valgus knees has not been examined.
Second, varus malalignment, by focusing bodyweight forces medially, may be a mediating factor be-tween obesity and knee OA. If varus malalignment wereplaying this role, then body mass, the proximal factor,would correlate with varus malalignment, and the rela-tionship between body mass and severity of knee OAwould be reduced after accounting for varus malalign-ment.
In this study, we first examined whether varus/valgus alignment is symmetric within patients with kneeOA. We then tested the following hypotheses: 1) bodymass index (BMI) is correlated with radiographic dis-ease severity in OA patients with varus knees; 2) thecorrelation between BMI and disease severity is weakerin OA patients with valgus knees than in those with varusknees; 3) BMI is correlated with the severity of varusmalalignment; and 4) the relationship between BMI andthe severity of medial tibiofemoral disease is reducedafter controlling for the degree of varus malalignment.
PATIENTS AND METHODS
Patients. Three hundred patients with knee OA wereenrolled into the baseline phase of a longitudinal study exam-ining the contribution of mechanical, neural, and muscularfactors to radiographic progression and functional decline inknee OA. Patients were recruited from the community throughadvertising in 67 neighborhood organizations and senior cen-ters, local periodicals, press releases, letters to subjects in theAging Research Registry of the Buehler Center on Aging ofNorthwestern University, and referrals from local physicians.
Inclusion and exclusion criteria were based on consen-sus recommendations (36,37). Inclusion criteria were definedas definite osteophyte presence in the medial and/or lateraltibiofemoral compartment (i.e., Kellgren and Lawrence [K/L]radiographic grade $2) of 1 or both knees and at least a littledifficulty with knee-requiring activities. Exclusion criteria werethe following: intraarticular corticosteroid injection into eitherknee within the previous 3 months, uncomplicated knee sur-gery within the previous 6 months, complicated knee surgerywithin the previous year, bilateral total knee replacement,history of avascular necrosis, rheumatoid arthritis, or any othersystemic inflammatory arthropathy, periarticular fracture,
Figure 1. Paradigm of the link between obesity and osteoarthritis(OA) in weight-bearing joints, with illustration of a weaker relation-ship at the hip versus the knee. As shown, obesity may act through thedirect effect of body weight on load and also through the influence, atthe knee, of another factor (or factors) that mediates the mechanicalimpact of excess body weight at the knee.
ROLE OF MALALIGNMENT IN THE OBESITY–KNEE OA RELATIONSHIP 569

Paget’s disease, villonodular synovitis, joint infection, ochro-nosis, neuropathic arthropathy, acromegaly, hemochromatosis,Wilson’s disease, osteochondromatosis, gout or recurrentpseudogout, or osteopetrosis.
Measurement of alignment. To assess alignment, asingle anteroposterior radiograph of the entire lower extremitywas obtained. A 51 3 14–inch graduated grid cassette was usedas previously recommended (29). By filtering the x-ray beam ina graduated manner, this cassette accounts for the unique softtissue characteristics of the hip and ankle so that all landmarksin the lower extremity can be visualized well. The size of thecassette allows for inclusion of the full lower extremity of tallerpatients. The subject stood without footwear, positioned sothat the tibial tubercles faced forward. Because the tibialtubercle was a site adjacent to the knee that was not distortedby the presence of OA, this was used as the positioninglandmark (38); the patella is often used for this purpose instudies of normal knees (29), but is not appropriate in OAbecause patellofemoral subluxation may be present. The x-raybeam was centered at the knee at a distance of 8 feet. A settingof 100–300 milliampere-seconds and a kilovoltage of 80–90were used, depending on limb size and tissue characteristics, toensure landmark visualization.
Alignment was measured on the full-limb radiographas the angle formed by the intersection of the mechanical axesof the femur and the tibia, as previously recommended(28,30,38). Specifically, the angle measured was formed by theintersection of the line from the center of the femoral head tothe center of the femoral intercondylar notch, with the lineextending from the center of the ankle talus to the center of thetips of the tibial spines. A knee was defined as being varuswhen alignment (the intersection of the mechanical axes of thefemur and the tibia) was .0° in the varus direction, valguswhen alignment was .0° in the valgus direction, and neutralwhen alignment was 0°, as previously determined (29,30,39,40).The angle made by the intersection of lines drawn through thefemoral and tibial shafts on a knee radiograph was not used inthe present study since it does not account for variation in theproximal femur, femoral shaft, tibial shaft, or ankle (41), ishighly variable compared with full-limb measurements amongnormal subjects (30), and is not typically utilized in orthopedicclinical or biomechanical studies.
All measurements of alignment were made by a singleexperienced reader (LS). For this reader, reliability was highfor measurements of both varus (intraclass correlation coeffi-cient [ICC; model 1,1] 0.99) and valgus (ICC 0.98) alignment.
Measurement of BMI and leg dominance. BMI wasexpressed as the weight (in kg)/height (in m2). Leg dominancewas ascertained using the question: “In order to kick a ball,which leg would you use?”
Radiographic measurements of knee OA severity. Adetailed protocol (42) was followed for radiographic determi-nation of disease severity, including knee position, criteria forx-ray beam alignment relative to the center of the knee, use ofradiopaque markers to account for radiographic magnification,and definition of anatomic landmarks for measurement. Theanteroposterior view was obtained with knees in the weight-bearing, semiflexed position to superimpose the anterior andposterior joint margins. The heel was fixed and the foot rotateduntil the tibial spines were centered in the femoral notch. Kneeposition was confirmed by fluoroscopy.
Because this study required a compartment-specificmeasure of disease severity, the narrowest joint space widthwas utilized. The weight-bearing, semiflexed view is consideredoptimal for measurement of joint space (42,43). The elementsof the protocol used have been shown to enhance the precisionof these measurements (42,44,45). The femoral boundary usedwas the distal convex margin of the condyles. The tibialboundary was the line extending from near the tibial spine tothe outer margin, spanning across the center of the articularfossa in the midcoronal plane of the joint and defined by thesuperior margin of the bright radiodense band of the subchon-dral cortex (42,46). The interbone distance at the narrowestpoints of the medial and lateral compartments was measuredas previously recommended (36,46), using electronic calipers.Measurements were corrected for magnification.
All radiographs were obtained in the same unit by 1 of2 technicians who were trained in these protocols. One expe-rienced reader (LS) performed radiographic measurements ata different time than when alignment was measured. Duringreader sessions, the reader was blinded to all other data. Forthis reader, the reliability for minimum joint space measure-ment was calculated by analysis of variance with repeatedmeasures and by ICCs (model 3,1). The reliability was high formeasurements in both the medial and lateral compartments(r 5 0.95 and r 5 0.98, respectively).
Statistical analysis. Data on the dominant knee ofeach subject were used in statistical analyses to accountfor variation in how subjects load dominant versus nondomi-nant knees.
In patients with varus dominant knees, the correlationand the associated 95% confidence interval (95% CI) werecalculated for the relationship between BMI and the narrowestmedial joint space width, and between BMI and the narrowestof the medial or lateral joint space width. In patients withvalgus dominant knees, the correlation and 95% CI werecalculated for the relationship between BMI and the narrowestlateral joint space width, and between BMI and the narrowestof the medial or lateral joint space width. The correlation andassociated 95% CI were also calculated separately in varus andvalgus dominant knees for the relationship between malalign-ment and BMI, and between malalignment and joint spacewidth. Pearson’s method was used to calculate all correlations,except for those involving alignment. Due to the skeweddistribution of alignment, Spearman’s correlations were re-ported.
The relationships of BMI and malalignment to OAseverity were evaluated using partial correlations that were de-termined from multiple regression analysis. First, the partialcorrelation between BMI and OA severity was determined aftercontrolling for demographic factors. Second, the partial correla-tion between BMI and OA severity was determined after con-trolling for demographic characteristics and malalignment. Areduction in the partial correlation would indicate that malalign-ment explains part of the effect of BMI on OA severity.
RESULTS
Patient characteristics. Of the 300 patients, 8 hadundergone total knee replacement in the dominantknee. Among the remaining 292 dominant limbs, 154
570 SHARMA ET AL

knees (52.7%) had varus malalignment, 115 (39.4%) hadvalgus malalignment, and 23 (7.9%) had neutral (i.e., 0°)alignment; proportions were similar when only the 267dominant knees assigned a K/L grade of $2 wereconsidered (i.e., 53.9%, 39.0%, and 7.1%, respectively).Patient characteristics are provided in Table 1.
Is alignment symmetric? For the evaluation ofalignment symmetry, 10 patients who had undergonetotal knee replacement (8 in the dominant knee and 2 inthe nondominant knee) were excluded. Alignment direc-tion was either symmetric or neutral on one side in 253of 290 patients (87.2%, 95% CI 83.4–91.1%). Specifi-cally, both limbs were varus in 121 patients (41.7%),both limbs were valgus in 87 patients (30%), 1 limb wasvarus and the other neutral in 28 patients (9.7%), 1 limbwas valgus and the other neutral in 15 patients (5.2%),and both limbs were neutral in 2 patients (0.7%).Alignment direction was asymmetric (i.e., 1 knee varus,1 knee valgus) in 37 (12.8%) of 290 patients (95% CI8.9–16.6%). In 24 of these 37 patients, the malalignmentwas mild (i.e., #2°) in at least 1 limb. The distributionwas very similar when symmetry was examined in onlythose patients who had a K/L grade $2 in both knees.
Is BMI correlated with joint space width in thosewith varus knees and in those with valgus knees? Weevaluated the correlation between BMI and joint spacewidth within malalignment subsets. As shown in Table 2,in the 154 patients with varus dominant knees, BMIcorrelated with medial joint space width and with nar-rowest tibiofemoral joint space width. However, in the115 patients with valgus dominant knees, BMI was notcorrelated with either lateral joint space width or nar-rowest joint space width. In the 23 patients with neutraldominant knees, there was no correlation between BMI
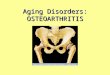
and narrowest joint space width. The regression lines forthe BMI–joint space width relationship in the varus,valgus, and neutral groups are shown in Figure 2.
Is BMI correlated with severity of malalignment?The correlations between malalignment and BMI, andbetween malalignment and joint space width are pre-sented in Table 3. BMI and malalignment were corre-lated in patients with varus knees, but not in those withvalgus knees. Due to the lack of correlation of BMI withmalalignment, and of BMI with disease severity, invalgus knees, subsequent analyses focused on the pa-tients with varus knees.
Are BMI and malalignment related in their effecton radiographic disease severity? We evaluated theimpact of BMI on disease severity in varus knees after
Table 2. Correlation of BMI with disease severity in malalignmentsubsets*
BMI, r (95% CI)
Varus group (n 5 154)Medial joint space width 20.27 (20.41, 20.11)Narrowest joint space width 20.29 (20.43, 20.14)
Valgus group (n 5 115)Lateral joint space width 20.10 (20.28, 0.09)Narrowest joint space width 20.13 (20.31, 0.05)
* Medial and lateral joint space widths are the width (in mm) of thenarrowest point in the medial and lateral compartments, respectively.Narrowest joint space width is the narrowest point of either tibiofemo-ral compartment. A 95% confidence interval (95% CI) that includes 0indicates that the correlation is not significant. See Table 1 for otherdefinitions.
Figure 2. Regression lines indicating the body mass index (BMI)–disease severity relationship for the varus, valgus, and neutral groups.The difference in the slope of the lines for varus and valgus groups wasstatistically significant (P , 0.0001). JSW 5 joint space width.
Table 1. Characteristics of patients with varus-aligned or valgus-aligned dominant knees*
Varus group(n 5 154)
Valgus group(n 5 115)
Age, years 64.9 6 10.8 64.0 6 11.4% women 60.4 86.1BMI 32.0 6 7.3 29.8 6 6.5Joint space width, mm
Medial 2.7 6 1.7 4.6 6 1.3Lateral 5.8 6 1.6 3.9 6 1.6Narrowest 2.6 6 1.6 3.4 6 1.3
* For age, body mass index (BMI), and joint space width, values arethe mean 6 SD. The BMI is the weight (in kg)/height (in m2). For jointspace width, “medial” refers to the narrowest joint space width in themedial compartment, “lateral” to the narrowest joint space width inthe lateral compartment, and “narrowest” to the narrowest width ofeither the medial or lateral compartments.
ROLE OF MALALIGNMENT IN THE OBESITY–KNEE OA RELATIONSHIP 571

controlling for demographic variables. An initial regres-sion analysis (data not shown) to evaluate demographicfactors on disease severity indicated that sex, but notage, was related to joint space width. Table 4 shows apartial correlation of 0.24 (95% CI 0.16–0.31) betweenBMI and disease severity after controlling for sex. Thepartial correlation between BMI and joint space widthwas reduced from 0.24 to 0.04 when malalignment wasadded to the model. This indicates that almost all of theeffect of BMI on disease severity was explained by varusmalalignment, after controlling for sex. The significantrelationship between sex and disease severity (i.e., beinga woman was associated with worse disease) was notaffected by adding malalignment to the model.
DISCUSSION
In patients with knee OA, a relationship betweenBMI and radiographic disease severity was found inthose with varus knees, but not in those with valgusknees. BMI correlated with varus malalignment. Thecorrelation between BMI and medial joint space widthwas greatly reduced by accounting for the severity ofvarus malalignment. This reduction indicates that muchof the variance in medial tibiofemoral disease severityexplained by BMI can also be attributed to varus mal-alignment; BMI did not have a relationship with diseaseseverity that was independent of malalignment in pa-tients with varus knees. Varus malalignment may ex-plain, in part, the uniquely strong association betweenBMI and OA at the knee versus OA at other lowerextremity sites. These findings support the role of varusmalalignment as a mediating factor, as depicted inFigure 1.
BMI and OA severity were correlated in patientswith varus knees, but not in those with valgus knees. It isestablished that compartment load distribution is moreequitable in valgus than in varus knees (34,35). Johnsonet al found that with progressively severe valgus mal-
alignment, medial compartment load gradually de-creased; only when fairly severe valgus malalignmentwas present was more load borne by the lateral compart-ment (34). With varus malalignment, medial plateauload rapidly approached 100% of total load; however,with valgus malalignment, load was still greater in themedial than in the lateral compartment in 71% of cases.As described by Harrington, the normal tendency was totransmit joint force through the medial side of the knee,so that a large valgus malalignment was required beforethe center of pressure shifted into the lateral compart-ment (35). The present study applies these biomechani-cal findings to the relationship in OA patients betweenbody weight and disease severity. Whether the strengthof the obesity–OA severity relationship is of comparablemagnitude in patients with varus versus valgus knees hasnot been previously examined.
In patients with varus knees, the relationshipbetween BMI and OA severity was greatly reduced afteraccounting for the malalignment, suggesting that muchof the BMI effect was explained by the severity of varusmalalignment. These cross-sectional results cannot re-veal the direction of relationships (i.e., obesity contrib-utes to varus malalignment which contributes to OA, orobesity leads to OA and varus malalignment developssubsequently). Body weight forces, which are alreadydisproportionately borne by the medial compartment,are further concentrated by progressive varus malalign-ment. Even if obesity-associated malalignment is sec-ondary to OA, it may be that obesity contributes toprogressive knee OA by amplifying and/or accelerating acycle of medial compartment cartilage loss and varusmalalignment (see Figure 3); this is a potential mecha-nism of disease progression in overweight subjects.
This study was not population based. However,patients were recruited from several community sourcesto maximize generalizability and efficiently target asufficient number of subjects with knee OA to allowanalyses in varus and valgus subsets and provide reason-
Table 3. Correlations of malalignment with BMI and jointspace width*
BMI Joint space width
Varus group (n 5 154) 0.26 (0.11, 0.40) 20.69 (20.77, 20.60)Valgus group (n 5 115) 0.16 (20.02, 0.35) 20.35 (20.51, 20.18)
* Values are the Spearman’s correlation coefficients with the associ-ated 95% confidence intervals (95% CI). Joint space width (in mm) isthe narrowest medial compartment width for the varus group andnarrowest lateral joint space width for the valgus-aligned group. A95% CI that includes 0 indicates that the correlation is not significant.See Table 1 for other definitions.
Table 4. Impact of BMI and varus malalignment on medialtibiofemoral disease severity*
Independentvariables Model R2, %
Partial r for BMI(95% CI)
Model 1 Sex, BMI 14.8 0.24 (0.16, 0.31)Model 2 Sex, BMI,
malalignment51.5 0.04 (20.04, 0.12)
* In these models, the dependent variable was narrowest medial jointspace width. The relationship between BMI and disease severity wasreduced after accounting for malalignment. 95% CI 5 95% confidenceinterval (see Table 1 for other definitions).
572 SHARMA ET AL

able distributions of BMI, malalignment, and OA sever-ity. This study was cross-sectional; how knee malalign-ment mediates the effect of body weight should befurther examined longitudinally.
Epidemiologic studies have strongly demon-strated that obesity is linked to the development of kneeOA (1–4,9) but have not revealed factors that might helpto explain the mechanism of the effect. In longitudinalstudies of the Framingham and Chingford populationsand in cross-sectional studies involving the NHANES,Baltimore Longitudinal Study of Aging, and Goteborgpopulations, the body weight–OA relationship was notreduced by adjusting for age (2,3,5,14), serum lipids(5,7), serum uric acid (1,5,7,14), blood glucose or diabe-tes (5,7), body fat distribution (5,6,23), blood pressure(5), smoking (2,3,14), chondrocalcinosis (3), hysterec-tomy (4), or estrogen replacement therapy (4). In theMichigan Bone Health Study involving younger women,the relationship between BMI and highest joint grade inthe knees was not attenuated by controlling for age,bone mineral density, hormone replacement therapy, orblood pressure (10). The relationship between weightand knee OA progression was not reduced by accountingfor age (9,15,17), sex (15,17,18), hand or multiple jointOA (9,15,17,18), calcium pyrophosphate dihydrate crys-tal deposition disease or chondrocalcinosis (15,18), orserum hyaluronic acid level (17). Among mechanicalfactors, adjustment for physical activity and injury didnot affect the relationship between body weight and OAdevelopment (1–4) or progression (9). These incidenceand progression studies, in contrast to the present study,did not reveal any factor that reduced the BMI–OArelationship.
Whether malalignment or any mechanical factor
other than injury or physical activity reduces the rela-tionship between obesity and knee OA severity has notpreviously been examined. Malalignment may developduring OA progression and may correlate with diseaseseverity. Varus malalignment and disease severity werecorrelated, though not perfectly. Sex continued to ex-plain a significant portion of disease severity afteraccounting for malalignment; BMI did not. Whetherknee malalignment develops before or after diseaseonset, it influences load distribution and is therefore alikely mediator in the obesity–OA relationship. Otherlocal factors that might either increase the vulnerabilityof the knee or decrease the vulnerability of the hip orankle to the effects of obesity should also be examined.Varus-valgus laxity was correlated with radiographicdisease severity, but not with BMI, making it less likelyto be a factor through which obesity acts (47).
If obesity were a more powerful risk factor invarus than in valgus knees, a stronger relationship wouldbe expected between obesity and OA in the medialcompartment compared with that in the lateral compart-ment in epidemiologic studies. Medial compartmentinvolvement is predominant in the studies that providethis information (11,18) and is the more common formof tibiofemoral OA (48,49). The published informationon the obesity–OA relationship is likely to be true formedial OA; little is known about this relationship inlateral OA.
A more modest association has been found be-tween measures of body weight and hip OA (19,20). Inanalyses of the NHANES-I data, obesity was not asso-ciated with hip OA overall, but was more closely asso-ciated with bilateral hip OA than with unilateral hip OA(19). Support for a link between heavier weight andhand OA comes from 1 longitudinal study (22) and somecross-sectional studies (7,20,23), but not from others(24,25).
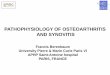
Figure 4. Paradigm of the relationship between obesity and osteoar-thritis (OA) at different joint sites. An obesity–hand association wouldsupport the existence of an unidentified systemic factor or mechanism.
Figure 3. Possible role of obesity in amplifying and/or acceleratingthe cycle of medial compartment cartilage loss and varus malalignmentin progressive knee osteoarthritis (OA).
ROLE OF MALALIGNMENT IN THE OBESITY–KNEE OA RELATIONSHIP 573

The paradigm in Figure 3 offers an explanationfor this combination of epidemiologic findings. If thereis no relationship between obesity and hand OA, theparadigm in Figure 3 is sufficient. An association be-tween obesity and hand OA would support the existenceof an as-yet-unidentified systemic factor or mechanism;through this factor, obesity may increase OA risk at bothnon–weight-bearing and weight-bearing sites (Figure 4).
The findings of the present study have implica-tions that should be examined. The relationship be-tween obesity and OA incidence and progression maybe stronger in varus knees than has been detected forknee OA as a whole. Change in weight may have agreater impact in varus knees. Patients who are obeseand have varus malalignment may be at particularlyhigh risk of rapid disease progression and may be lessresponsive to disease-modifying intervention. Thenatural history of OA, including the rate of progres-sion and factors contributing to progression, maydiffer significantly between varus and valgus knees.
In summary, a relationship between BMI andradiographic disease severity was present in those withvarus knees, but not in those with valgus knees. BMIcorrelated with the severity of varus malalignment. Therelationship between BMI and OA severity in varusknees was reduced after accounting for the severity ofmalalignment. Whether it precedes or follows the onsetof disease, varus malalignment is an attribute of theenvironment of the knee that may intensify the effect ofobesity on disease development and progression at themedial tibiofemoral joint versus other lower extremityjoints in patients with OA.
REFERENCES
1. Felson DT, Anderson JJ, Naimark A, Walker AM, Meenan RF.Obesity and knee osteoarthritis, the Framingham study. AnnIntern Med 1988;109:18–24.
2. Felson DT, Zhang Y, Anthony JM, Naimark A, Anderson JJ.Weight loss reduces the risk for symptomatic knee osteoarthritis inwomen: the Framingham study. Ann Intern Med 1992;116:535–9.
3. Felson DT, Zhang Y, Hannan MT, Naimark A, Weissman B,Aliabadi P, et al. Risk factors for incident radiographic kneeosteoarthritis in the elderly: the Framingham Study. ArthritisRheum 1997;40:728–33.
4. Hart DJ, Doyle DV, Spector TD. Incidence and risk factors forradiographic knee osteoarthritis in middle-aged women: theChingford Study. Arthritis Rheum 1999;42:17–24.
5. Davis MA, Ettinger WH, Neuhaus JM. The role of metabolicfactors and blood pressure in the association of obesity withosteoarthritis of the knee. J Rheumatol 1988;15:1827–32.
6. Hochberg MC, Lethbridge-Cejku M, Scott WW, Reichle R, PlatoCC, Tobin JD. The association of body weight, body fatness andbody fat distribution with osteoarthritis of the knee: data from theBaltimore Longitudinal Study of Aging. J Rheumatol 1995;22:488–93.
7. Bagge E, Bjelle A, Eden S, Svanborg A. Factors associated withradiographic osteoarthritis: results from the population study of70-year-old people in Goteborg. J Rheumatol 1991;18:1218–22.
8. Davis MA, Ettinger WH, Neuhaus JM, Cho SA, Hauck WW. Theassociation of knee injury and obesity with unilateral and bilateralosteoarthritis of the knee. Am J Epidemiol 1989;130:278–88.
9. Spector TD, Hart DJ, Doyle DV. Incidence and progression ofosteoarthritis in women with unilateral knee disease in the generalpopulation: the effect of obesity. Ann Rheum Dis 1994;53:565–8.
10. Sowers M, Hochberg M, Crabbe JP, Muhich A, Crutchfield M,Updike S. Association of bone mineral density and sex hormonelevels with osteoarthritis of the hand and knee in premenopausalwomen. Am J Epidemiol 1996;143:38–47.
11. McAlindon T, Zhang Y, Hannan M, Naimark A, Weissman B,Castelli W, et al. Are risk factors for patellofemoral and tibiofemo-ral knee osteoarthritis different? J Rheumatol 1996;23:332–7.
12. Cicuttini FM, Spector T, Baker J. Risk factors for osteoarthritis inthe tibiofemoral and patellofemoral joints of the knee. J Rheuma-tol 1997;24:1164–7.
13. Cicuttini FM, Baker JR, Spector TD. The association of obesitywith osteoarthritis of the hand and knee in women: a twin study.J Rheumatol 1996;23:1221–6.
14. Anderson JJ, Felson DT. Factors associated with osteoarthritis ofthe knee in the first National Health and Nutrition ExaminationSurvey (HANES I): evidence for an association with overweight,race, and physical demands of work. Am J Epidemiol 1988;128:179–89.
15. Schouten JSAG, van den Ouweland FA, Valkenburg HA. A 12year follow up study in the general population on prognosticfactors of cartilage loss in osteoarthritis of the knee. Ann RheumDis 1992;51:932–7.
16. Dougados M, Gueguen A, Nguyen M, Thiesce A, Listrat V, JacobL, et al. Longitudinal radiologic evaluation of osteoarthritis of theknee. J Rheumatol 1992;19:378–84.
17. Sharif M, George E, Shepstone L, Knudson W, Thonar EJ-MA,Cushnaghan J, et al. Serum hyaluronic acid level as a predictor ofdisease progression in osteoarthritis of the knee. Arthritis Rheum1995;38:760–7.
18. Ledingham J, Regan M, Jones A, Doherty M. Factors affectingradiographic progression of knee osteoarthritis. Ann Rheum Dis1995;54:53–8.
19. Tepper S, Hochberg MC. Factors associated with hip osteoarthri-tis: data from the First National Health and Nutrition ExaminationSurvey (NHANES-I). Am J Epidemiol 1993;137:1081–8.
20. Van Saase JLCM, Vandenbroucke JP, van Romunde LKJ,Valkenburg HA. Osteoarthritis and obesity in the general popu-lation: a relationship calling for an explanation. J Rheumatol1988;15:1152–8.
21. Croft P, Coggon D, Cruddas M, Cooper C. Osteoarthritis of thehip: an occupational disease in farmers. BMJ 1992;304:1269–72.
22. Carman WJ, Sowers M, Hawthorne VM, Weissfeld LA. Obesity asa risk factor for osteoarthritis of the hand and wrist: a prospectivestudy. Am J Epidemiol 1994;139:119–29.
23. Davis MA, Neuhaus JM, Ettinger WH, Mueller WH. Body fatdistribution and osteoarthritis. Am J Epidemiol 1990;132:701–7.
24. Hochberg MC, Lethbridge-Cejku M, Plato CC, Wigley FM, TobinJD. Factors associated with osteoarthritis of the hand in males:data from the Baltimore Longitudinal Study of Aging. Am JEpidemiol 1991;134:1121–7.
25. Hochberg MC, Lethbridge-Cejku M, Scott WW, Plato CC, TobinJD. Obesity and osteoarthritis of the hands in women. Osteoar-thritis Cartilage 1993;1:129–35.
26. Hart DJ, Doyle DV, Spector TD. Association between metabolicfactors and knee osteoarthritis in women: the Chingford Study.J Rheumatol 1995;22:1118–23.
27. Maquet PGJ. Theoretical analyses of the causes of knee OA. In:Biomechanics of the knee. Berlin: Springer-Verlag; 1984. p. 75–85.
574 SHARMA ET AL

28. Tetsworth K, Paley D. Malalignment and degenerative arthro-pathy. Orthop Clin North Am 1994;25:367–77.
29. Moreland JR, Bassett LW, Hanker GJ. Radiographic analysis ofthe axial alignment of the lower extremity. J Bone Joint Surg Am1987;69-A:745–9.
30. Hsu RWW, Himeno S, Coventry MB, Chao EYS. Normal axialalignment of the lower extremity and load-bearing distribution atthe knee. Clin Orthop 1990;255:215–27.
31. McKellop HA, Llinas A, Sarmiento A. Effects of tibial malalign-ment on the knee and ankle. Orthop Clin North Am 1994;25:415–23.
32. Bruns J, Volkmer M, Luessenhop S. Pressure distribution at theknee joint: influence of varus and valgus deviation without andwith ligament dissection. Arch Orthop Trauma Surg 1993;133:12–9.
33. Morrison JB. The mechanics of the knee joint in relation tonormal walking. J Biomech 1970;3:51–61.
34. Johnson F, Leitl S, Waugh W. The distribution of load across theknee: a comparison of static and dynamic measurements. J BoneJoint Surg Br 1980;62-B:346–9.
35. Harrington IJ. Static and dynamic loading patterns in knee jointswith deformities. J Bone Joint Surg Am 1983;65-A:247–59.
36. Dieppe P, Altman RD, Buckwalter JA, Felson DT, Hascall V,Lohmander LS, et al. Standardization of methods used to assessthe progression of osteoarthritis of the hip or knee joints. In:Kuettner KE, Goldberg VM, editors. Osteoarthritic disorders.Rosemont (IL): American Academy of Orthopaedic Surgeons;1995. p. 481–96.
37. Task Force of the Osteoarthritis Research Society. Special report:design and conduct of clinical trials in patients with osteoarthritis.Osteoarthritis Cartilage 1996;4:217–44.
38. Chao EYS, Neluheni EVD, Hsu RWW, Paley D. Biomechanics ofmalalignment. Orthop Clin North Am 1994;25:379–86.
39. Cooke TDV, Li J, Scudamore RA. Radiographic assessment ofbony contributions to knee deformity. Orthop Clin North Am1994;25:387–93.
40. Hilding MB, Lanshammar H, Ryd L. A relationship between
dynamic and static assessments of knee joint load: gait analysis andradiography before and after knee replacement in 45 patients.Acta Orthop Scand 1995;66:317–20.
41. Goldberg VM, Kettelkamp DB, Coyler RA. Osteoarthritis of theknee. In: Moskowitz RW, Howell DS, Goldberg VM, Mankin HJ,editors. Osteoarthritis: diagnosis and medical/surgical manage-ment. Philadelphia: WB Saunders; 1992. p. 599–620.
42. Buckland-Wright CB. Protocols for precise radio-anatomical po-sitioning of the tibiofemoral and patellofemoral compartments ofthe knee. Osteoarthritis Cartilage 1995;3 Suppl A:71–80.
43. Messieh SS, Fowler PJ, Munro T. Anteroposterior radiographs ofthe osteoarthritic knee. J Bone Joint Surg Br 1990;72:639–40.
44. Buckland-Wright JC, Macfarlane DG, Lynch JA, Jasani MK,Bradshaw CR. Joint space width measures cartilage thickness inosteoarthritis of the knee: high resolution plain film and doublecontrast macroradiographic investigation. Ann Rheum Dis1995;54:263–8.
45. Buckland-Wright JC, Macfarlane DG, Williams SA, Ward RJ.Accuracy and precision of joint space width measurements instandard and macroradiographs of osteoarthritic knees. AnnRheum Dis 1995;54:872–80.
46. Lequesne M. Quantitative measurements of joint space duringprogression of osteoarthritis: “chondrometry.” In: Kuettner KE,Goldberg VM, editors. Osteoarthritic disorders. Rosemont (IL):American Academy of Orthopaedic Surgeons; 1995. p. 427–44.
47. Sharma L, Lou C, Felson DT, Dunlop DD, Kirwan-Mellis G,Hayes KW, et al. Laxity in healthy and osteoarthritic knees.Arthritis Rheum 1999;42:861–70.
48. McAlindon TE, Snow S, Cooper C, Dieppe PA. Radiographicpatterns of osteoarthritis of the knee joint in the community: theimportance of the patellofemoral joint. Ann Rheum Dis 1992;51:844–9.
49. Thomas RH, Resnick D, Alazraki NP, Daniel D, Greenfield R.Compartmental evaluation of osteoarthritis of the knee; a com-parative study of available diagnostic modalities. Radiology 1975;116:585–94.
ROLE OF MALALIGNMENT IN THE OBESITY–KNEE OA RELATIONSHIP 575