Embed Size (px)
Citation preview
THE MENOPAUSE AND HRT
THE MENOPAUSE AND HRT
Dr Jacqueline Guest Consultant Obstetrician
and Gynaecologist
Learning Objectives
• Physiology of the Menopause and Climacteric
• Role of Hormones in the Menstrual Cycle
• Symptoms of the Climacteric
• Hormone Replacement Therapy (HRT)
• Alternatives to HRT
Definition of the Menopause
The menopause is the last menstrual period (LMP).
The perimenopause or climacteric is the phase encompassing the menopause.
The climacteric lasts for about two years, but may last for 10 years or longer.
The menopause is the last menstrual period (LMP).
The perimenopause or climacteric is the phase encompassing the menopause.
The climacteric lasts for about two years, but may last for 10 years or longer.
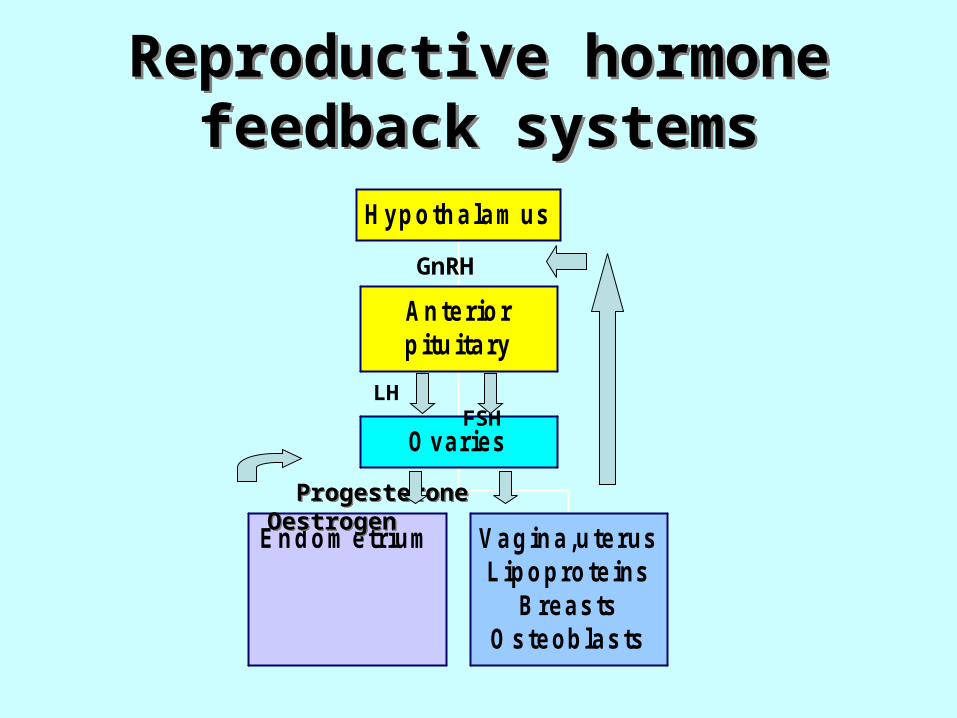
Reproductive hormone feedback systems
Reproductive hormone feedback systems
Endom etrium Vagina,uterusLipoproteins
BreastsOsteoblasts
Ovaries
Anteriorpituitary
Hypothalam us
GnRH
LH FSH
Progesterone Oestrogen Progesterone Oestrogen
The Role of Hormones in The Menstrual Cycle
Gonadotrophin hormonesGonadotrophin hormones stimulate the ovaries: stimulate the ovaries:follicle stimulating hormone (FSH) follicle stimulating hormone (FSH) luteinising hormone (LH)luteinising hormone (LH)
At the menopause ovaries run out of oocytes and they At the menopause ovaries run out of oocytes and they become resistant to the gonadotrophin hormonesbecome resistant to the gonadotrophin hormones
Levels of FSH and LH increase throughout the latter stages Levels of FSH and LH increase throughout the latter stages of the Climacteric and reach a peak 2 to 3 years after the of the Climacteric and reach a peak 2 to 3 years after the menopausemenopause
A level of FSH of more than 30IU/L on 2 separate occasions indicates Ovarian Failure
The Role of Hormones in The Menstrual Cycle
There are 3 important oestrogens in women: oestradiol,oestriol & oestrone
Oestradiol is predominant in premenopausal women: produced by the ovaries.
Oestrone is predominant in postmenopausal women : produced by peripheral conversion of androgens in the adipose tissue.
E1 is less biologically active than E2.E1 is less biologically active than E2.
There are 3 important oestrogens in women: oestradiol,oestriol & oestrone
Oestradiol is predominant in premenopausal women: produced by the ovaries.
Oestrone is predominant in postmenopausal women : produced by peripheral conversion of androgens in the adipose tissue.
E1 is less biologically active than E2.E1 is less biologically active than E2.
The Menopause - Acute Symptoms
• Hot flushesHot flushes• Night sweatsNight sweats• HeadachesHeadaches• Panic attacksPanic attacks• Mood swingsMood swings• IndecisivenessIndecisiveness
• Insomnia leading to:
• irritability • poor short term
memory• difficulty with
concentration
MEDIUM TERM SYMPTOMSMEDIUM TERM SYMPTOMS
• Vaginal drynessVaginal dryness• DyspareuniaDyspareunia• Reduced libidoReduced libido• Thinning skin/ hairThinning skin/ hair• Skin formicationSkin formication• Urethral syndrome (frequency, Urethral syndrome (frequency,
nocturia and urge incontinence)nocturia and urge incontinence)
LONG TERM SYMPTOMS
• CARDIOVASCULAR DISEASE
• OSTEOPOROSIS
• CEREBROVASCULAR DISEASE
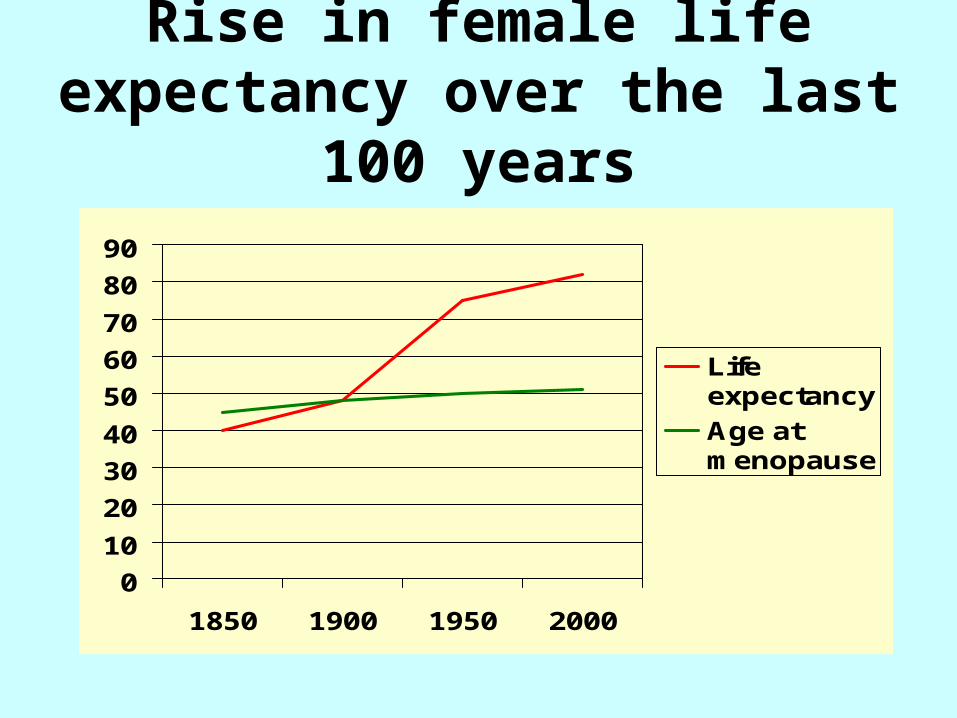
Rise in female life expectancy over the last 100 years
0
10
20
30
40
50
60
70
80
90
1850 1900 1950 2000
Lifeexpectancy
Age atmenopause
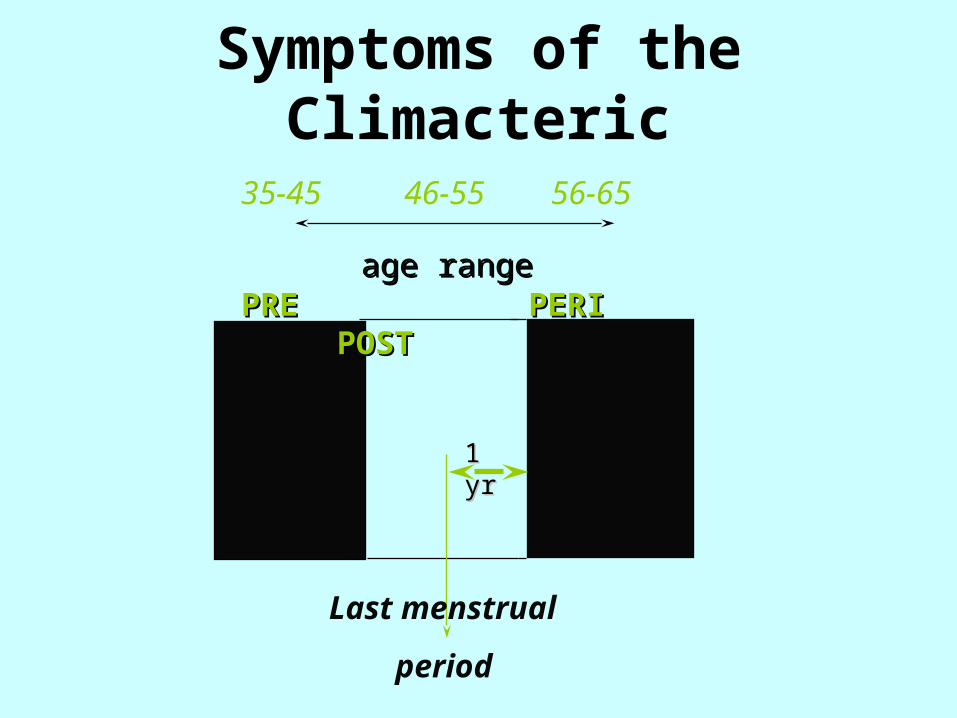
Symptoms of the Climacteric
age rangeage rangePRE PERI POSTPRE PERI POST
35-45 46-55 56-65
Last menstrual
period
1 yr1 yr
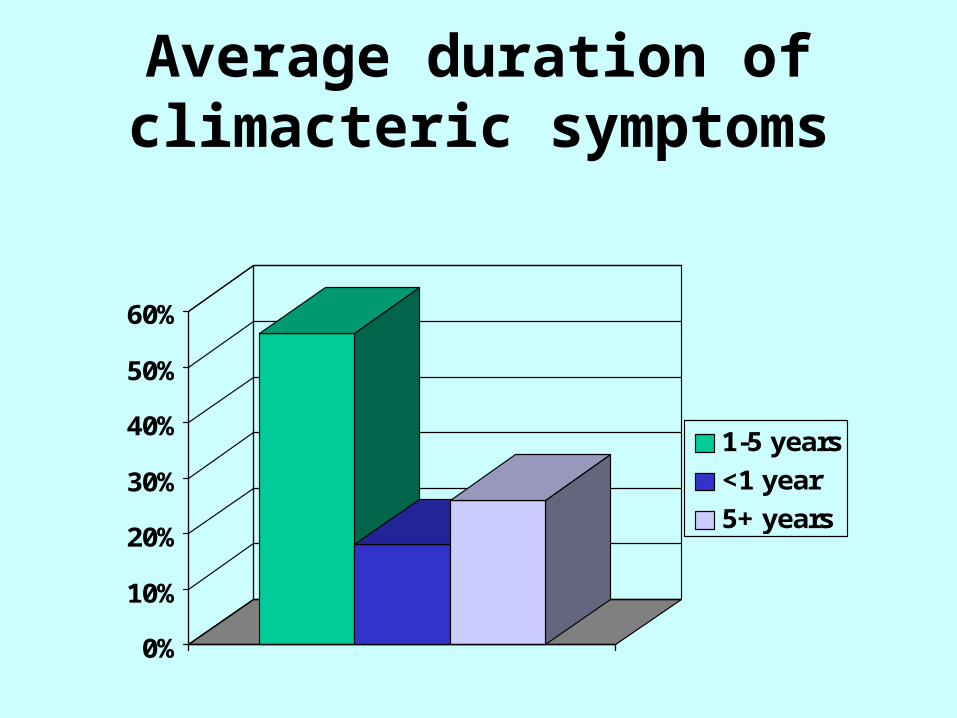
Average duration of climacteric symptoms
0%
10%
20%
30%
40%
50%
60%
1-5 years
<1 year
5+ years
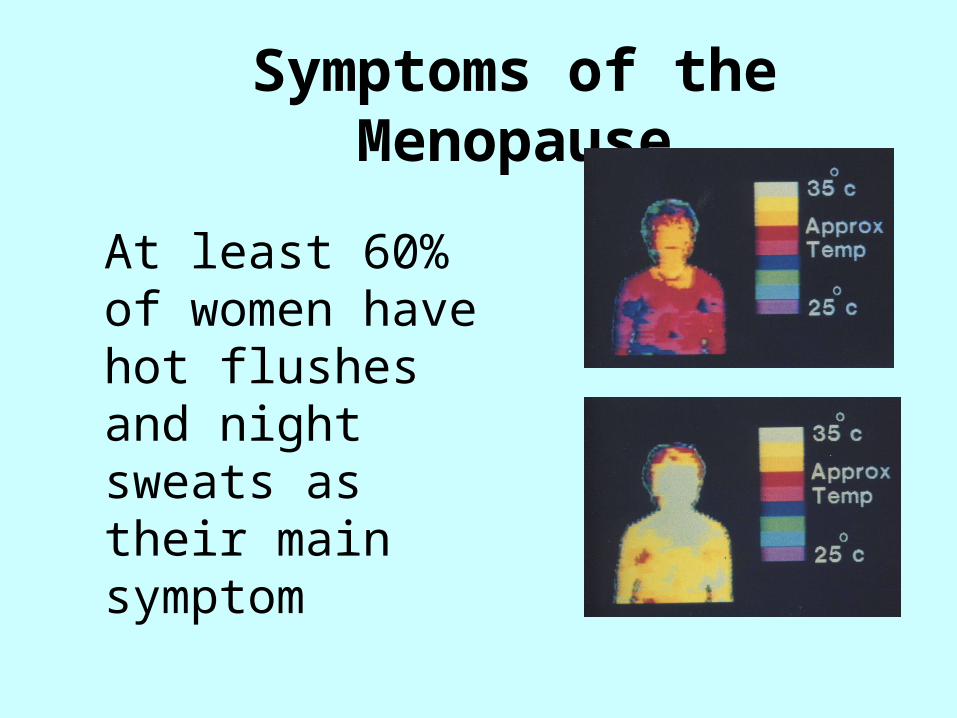
Symptoms of the Menopause
At least 60% of women have hot flushes and night sweats as their main symptom
Hormone Replacement Therapy (HRT)
OESTROGENS
• oestradioloestradiol
• oestradiol valerateoestradiol valerate
• conjugated equine oestrogensconjugated equine oestrogens
• oestrioloestriolThese should not be confused with the oestrogens used in the COC. They are used at a dose which is effectively 1/6th of the dose used in the COC.
PROGESTOGENS
19 NORTESTOSTERONE
DERIVATIVES
• norethisterone• levonorgestrel • norgestrel
17 HYDROXY-PROGESTERONE DERIVATIVES
• dydrogesterone• medroxy progesterone
acetate
Prescription of HRT: ROUTESPrescription of HRT: ROUTES
OralOralTransdermal: Transdermal: patch or gelpatch or gel
SubcutaneousSubcutaneous(implant)(implant)
Intramuscular Intramuscular (depot)(depot)
Intra-uterine Intra-uterine (Mirena)(Mirena)
Intra-vaginal Intra-vaginal (tablets, ring (tablets, ring or cream)or cream)
Preparations of HRT
• Oestrogen Only HRT (tablet, patch, gel, implant)
• Sequential Combined HRT - oestrogen and progestogens (tablets or patch)
• Continuous Combined HRT - oestrogen and progestogens (tablets or patch)
Oestrogen Only HRT
• Only to be used in women who have had a total hysterectomy
• If the hysterectomy was subtotal, then may need to use progestogens as well (some endometrium may be left behind)
• If the hysterectomy was for endometriosis, then progestogens continuously along with oestrogen should be used at least initially
Sequential Combined HRT
• Sequential oestrogen and progestogen
• The addition of the progestogen protects the endometrium and leads to a regular bleed
• Single named product available as patch or tablet but individualisation possible eg gel and IUS
Oestrogen for 28 days
Progestogen for 14 days
Continuous Combined HRT
• Continuous Combined HRT (CCT)
• This should not be started until 1 year after the LMP or aged 54. Should also be used after 2 years of cyclical therapy if under the age of 54.
• No monthly bleed
Oestrogen combined with progestogen for 28 days
Continuous Combined HRTContinuous Combined HRT
• This preparation leads to no bleeding after the first 6 months of use
• Single named product available as tablets or patches
• Any oestrogen continuously + any progestogen continuously
The Mirena is now licensed for use with Oestrogen only HRT for 4 years. The advantage is that it can be used in younger women to induce a no-bleed regime.
Tibolone or Livial
• This is an alternative CC HRT
• It is a gonadomimetic containing oestrogen, progestogens and androgens
• Licensed for vasomotor symptoms and osteoporosis
• The risk:benefit ratio similar to HRT in women under 60, but over 60 increased risk of stroke
• Slightly increased risk for endometrial cancer
• Less risk of breast cancer compared with CCT but increased over E2 only HRT
• May help libido due to androgen content
How long with sequential HRT?
• There are now several papers * that show that prolonged use of sequential HRT can increase the risk of endometrial cancer
• Relative risk of endometrial cancer rose from 1.3 to 2.9 for 5 years use
• For CCT HRT relative risk fell to 0.2*Beresford et al. Lancet 1997.
Wiederpass et al. J. of the National Cancer Institute 1999.
The advice is therefore
Do not keep women on cyclical therapies longer than 5 years
If the woman is over 54 or her periods have stopped for a year at any age start with CCT
Under the age of 54 continue on cyclical therapy for 2 years and then change to CCT
Local oestrogen preparations
• For women with vaginal and bladder symptoms who do not need systemic HRT local oestrogens can be used
• Vaginal creams and tablets are available
• There has been some concern that long term use without progestogens may cause endometrial hyperplasia or cancer
Long term treatment of atrophic vaginitis with low-dose oestradiol vaginal tablets*
• Women treated with twice weekly Vagifem tablets had an atrophic endometrium after 2 years
• Licensed for long term use as required
*L.Mettler and P.G.Olsen
Maturitas.14(1991) 23-31
MANAGEMENT OF HRT• Initial visit
• 3 months
• 6 months
• Yearly: BP, breast examination and BP, breast examination and vaginal examination (3 yearly vaginal examination (3 yearly smears to age 60 and 3 yearly smears to age 60 and 3 yearly mammography aged 50-64)mammography aged 50-64)
• Invite earlier visit for specific Invite earlier visit for specific problemsproblems

July 2002

Benefits of HRT
Benefits and HRT: Menopausal Symptoms
• HRT effectively relieves vasomotor symptoms
• In most cases, 2-3 years therapy is sufficient, but some women may need longer
• Symptoms may recur for a short time after stopping it.
Benefits and HRT: Coronary Heart Disease
• Re-analysis of WHI study suggests a cardio-protective effect if HRT taken in the early menopausal years
• No increased risk of CHD has been identified to date with oestrogen-only HRT
• RCT’s have shown an increased risk of CHD in women who started combined HRT more than 10 years after the menopause.
Healthcare professionals should assess carefully
every woman’s risk of CHD before prescribing HRT, irrespective of her age or time since menopause
Benefits and HRT: Colorectal Cancer
• HRT reduces the risk of colorectal cancer
• This is likely to be the anti-oxidant effect of oestrogen
Benefits and HRT: Osteoporosis
• “osteoporosis is a skeletal disorder characterised by compromised bone strength predisposing to an increased risk of fracture”
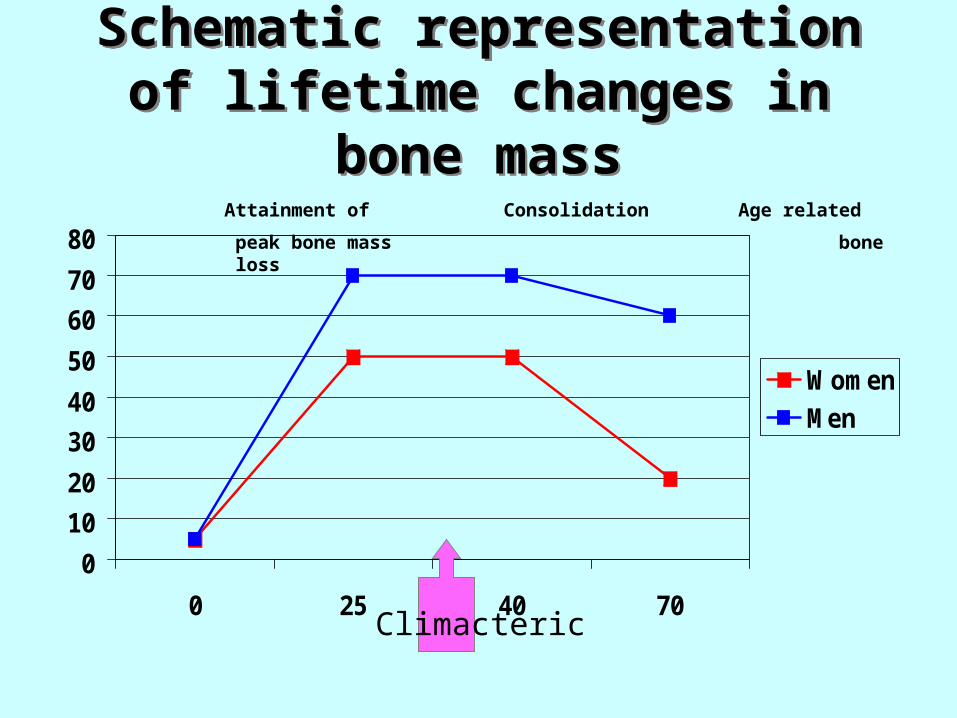
Schematic representation of lifetime changes in bone massSchematic representation of
lifetime changes in bone mass
0
10
20
30
40
50
60
70
80
0 25 40 70
Women
Men
Attainment of Consolidation Age related
peak bone mass bone loss
Climacteric
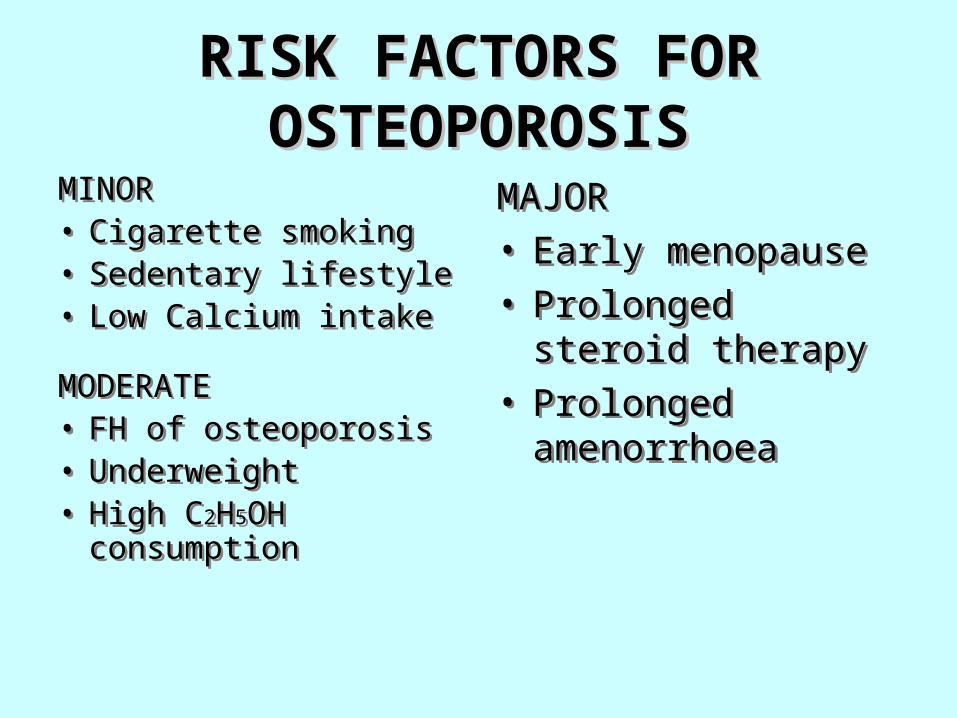
RISK FACTORS FOR RISK FACTORS FOR OSTEOPOROSISOSTEOPOROSIS
MINOR• Cigarette smoking• Sedentary lifestyle• Low Calcium intake
MODERATE• FH of osteoporosis• Underweight• High C2H5OH
consumption
MINOR• Cigarette smoking• Sedentary lifestyle• Low Calcium intake
MODERATE• FH of osteoporosis• Underweight• High C2H5OH
consumption
MAJOR• Early menopause• Prolonged steroid
therapy• Prolonged
amenorrhoea
MAJOR• Early menopause• Prolonged steroid
therapy• Prolonged
amenorrhoea
Management of patients at risk from osteoporosis
• Early diagnosis and treatment criticalEarly diagnosis and treatment critical
• Bone density screeningBone density screening
• Recommend lifestyle factors for self Recommend lifestyle factors for self helphelp
Benefits and HRT: Osteoporosis
• HRT is effective for the prevention of osteoporosis but its beneficial effect on bone diminishes soon after stopping treatment
• Because of the risks associated with long term use of HRT, it should only be used for prevention in women who are unable to use other medicines that are authorised for this purpose
• However HRT remains the treatment of choice in women with premature ovarian failure
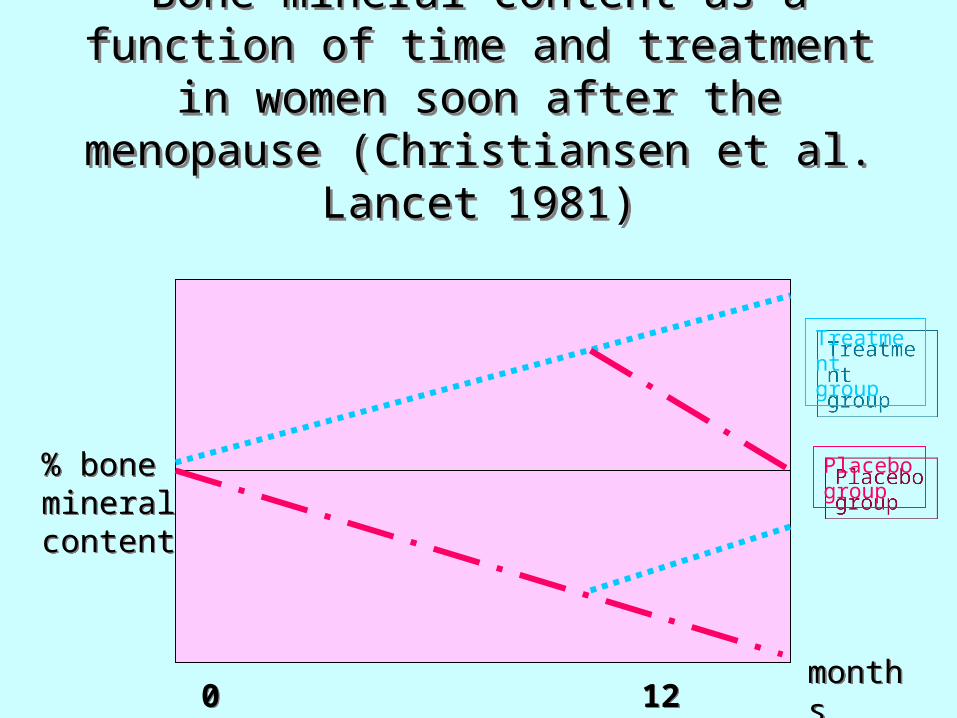
Bone mineral content as a function of time and treatment in women soon after
the menopause (Christiansen et al. Lancet 1981)
Bone mineral content as a function of time and treatment in women soon after
the menopause (Christiansen et al. Lancet 1981)
% bone mineral content
% bone mineral content
0 12 24 360 12 24 36monthsmonths
Treatment group
Treatment group
Placebo group
Placebo group
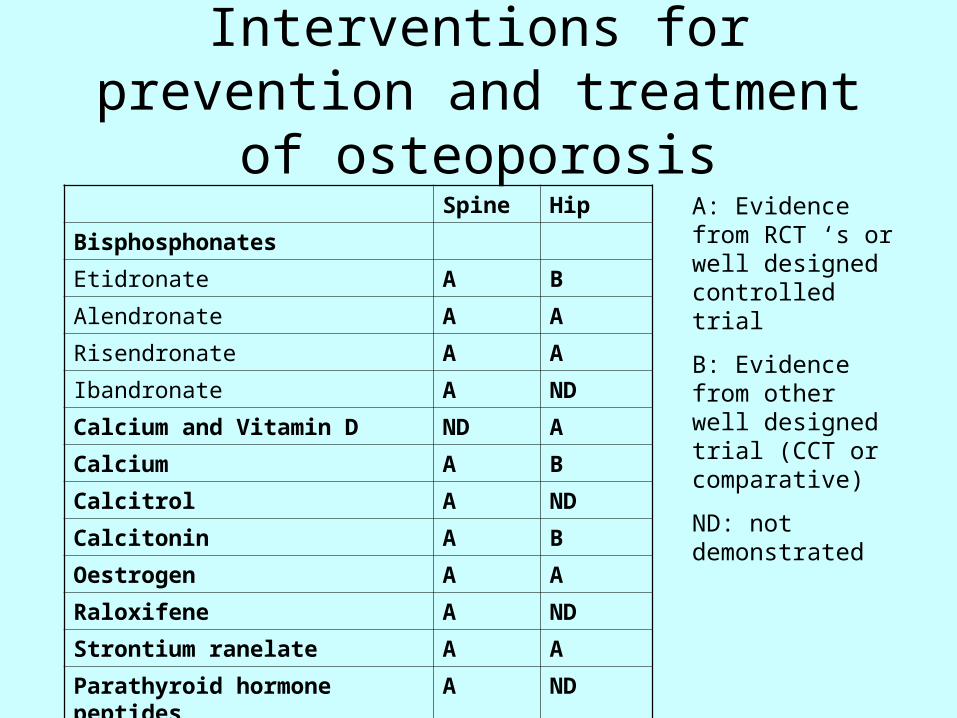
Spine Hip
Bisphosphonates
Etidronate A B
Alendronate A A
Risendronate A A
Ibandronate A ND
Calcium and Vitamin D ND A
Calcium A B
Calcitrol A ND
Calcitonin A B
Oestrogen A A
Raloxifene A ND
Strontium ranelate A A
Parathyroid hormone peptides A ND
Interventions for prevention and treatment of osteoporosis
A: Evidence from RCT ‘s or well designed controlled trial
B: Evidence from other well designed trial (CCT or comparative)
ND: not demonstrated
Risks and HRT: Stroke
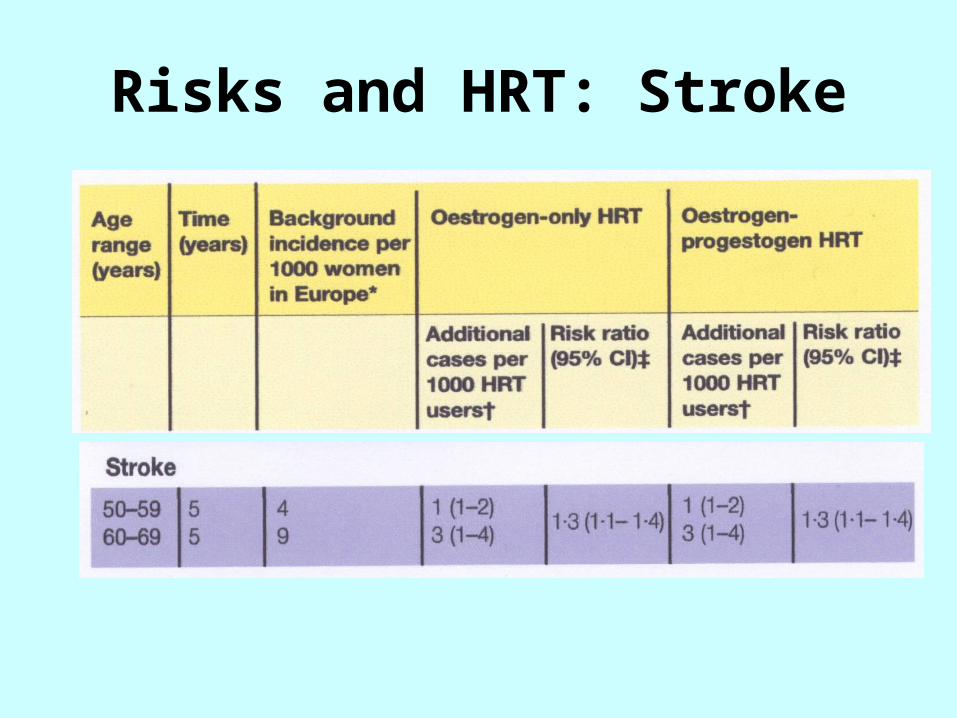
• In RCT’s HRT increased the risk of stroke (mostly ischaemic) compared with placebo
• Older women have a greater absolute risk of stroke
• Risk may depend on oestrogen dose
Risks and HRT: Stroke
Risks and HRT: Venous Thromboembolism
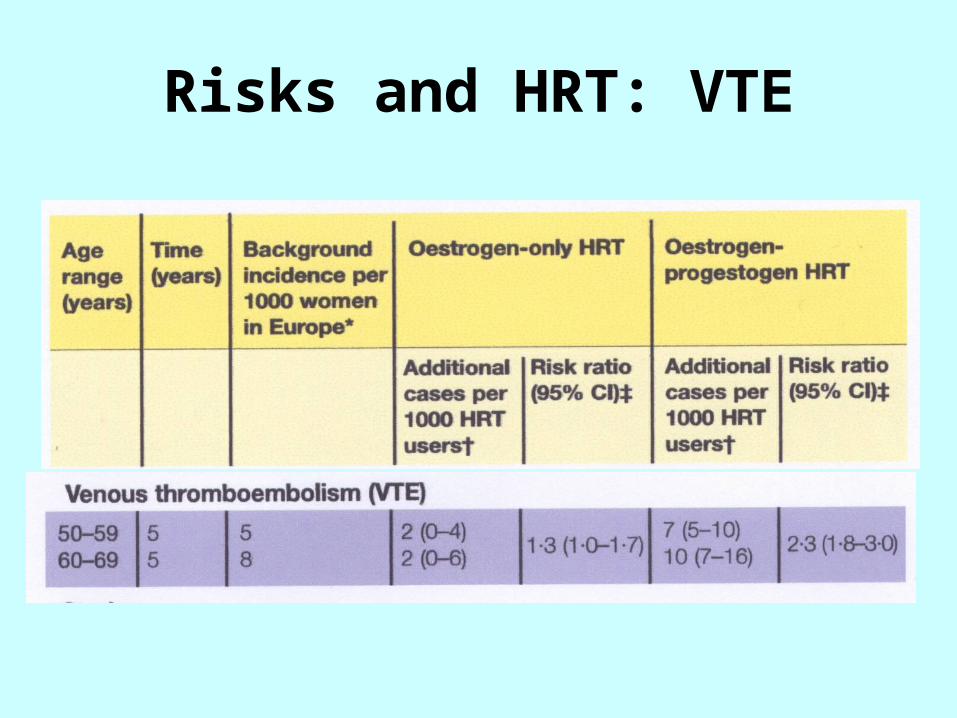
• Oral HRT has been associated with an increased risk of DVT and PE in RCT’s and observational studies.
• Evidence suggests that it is higher with combined HRT than oestrogen-only HRT and that these events are more likely in the first year of use
• One study suggests that risk may be lower with a non-oral route
Risks and HRT: VTE
Risks and HRT: Endometrial Cancer
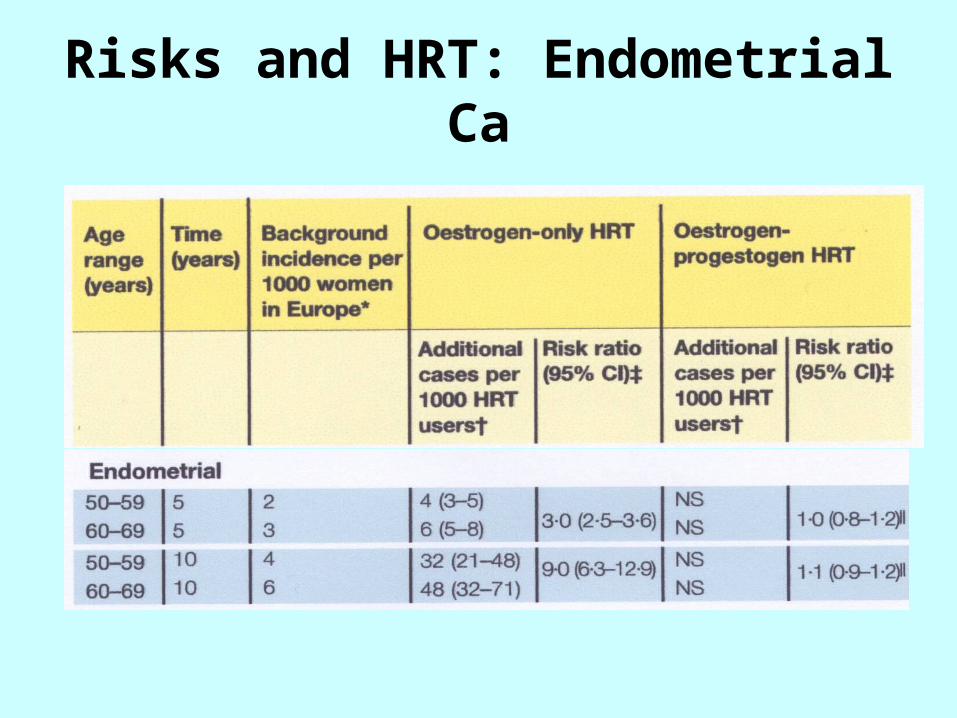
• In women with a uterus, use of oestrogen-only HRT substantially increases the risk of endometrial hyperplasia and cancer in a way that depends on dose and duration
• Addition of progestogen cyclically for at least 10 days per 28 day cycle reduces the risk and progestogen continuously eliminates risk
Risks and HRT: Endometrial Ca
Risks and HRT: Ovarian Cancer
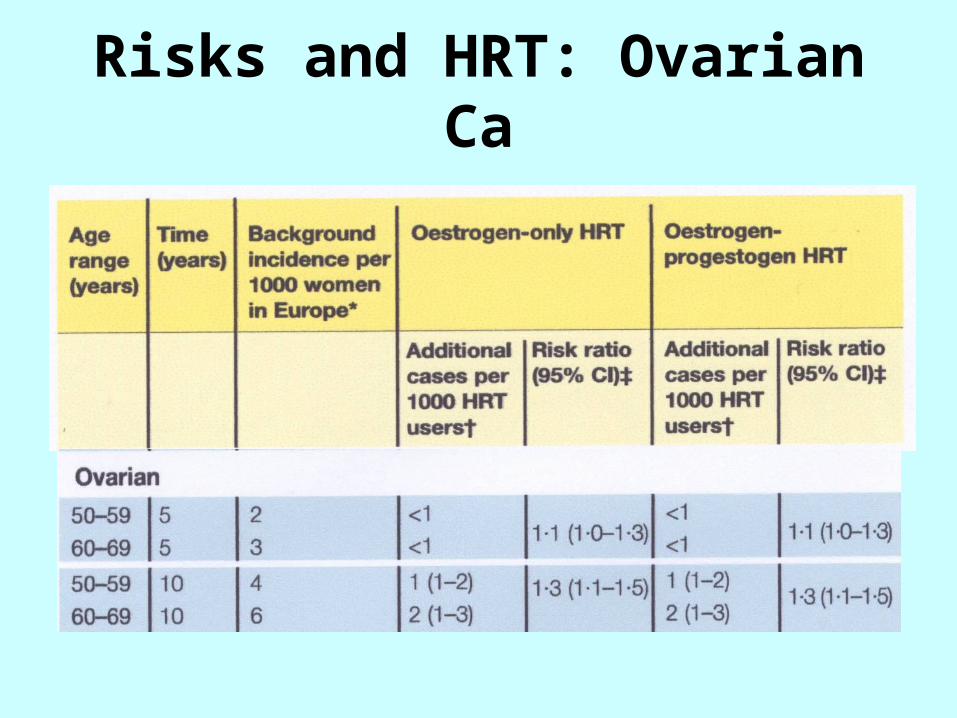
• Observational studies suggest that long-term use of all HRT’s may be associated with a small increased risk of ovarian cancer which returns to baseline a few years after stopping it.
Risks and HRT: Ovarian Ca
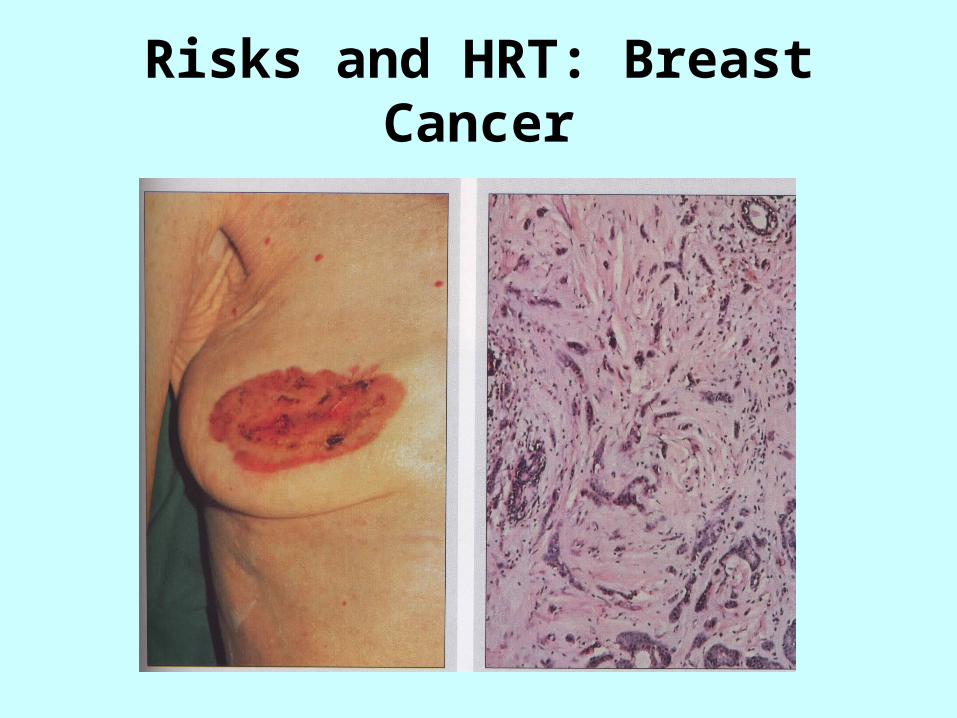
Risks and HRT: Breast Cancer
Risks and HRT: Breast Cancer
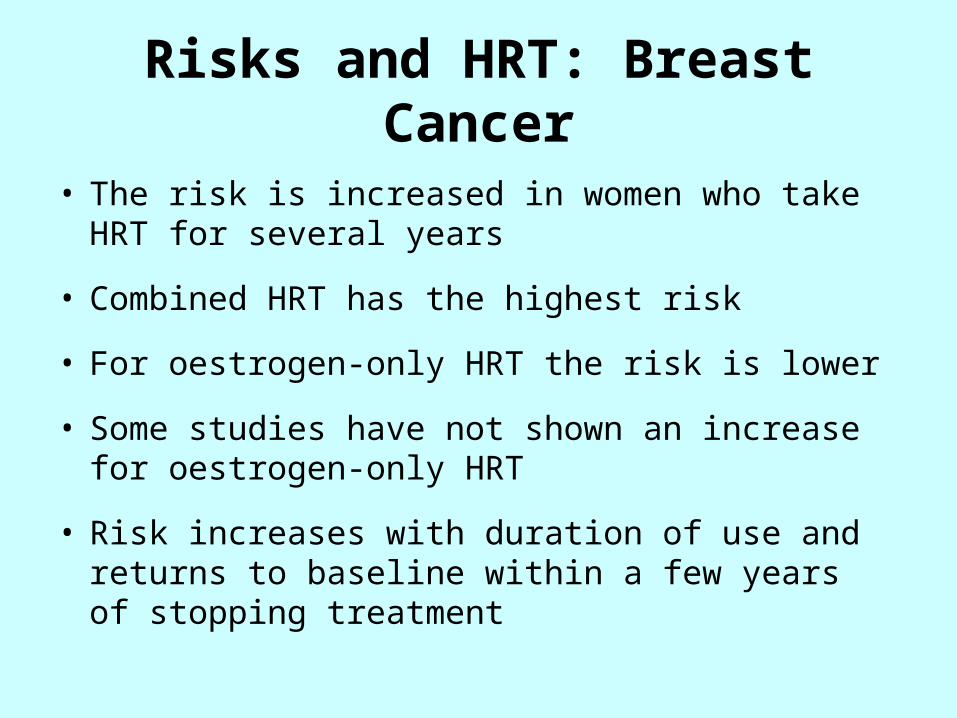
• The risk is increased in women who take HRT for several years
• Combined HRT has the highest risk
• For oestrogen-only HRT the risk is lower
• Some studies have not shown an increase for oestrogen-only HRT
• Risk increases with duration of use and returns to baseline within a few years of stopping treatment
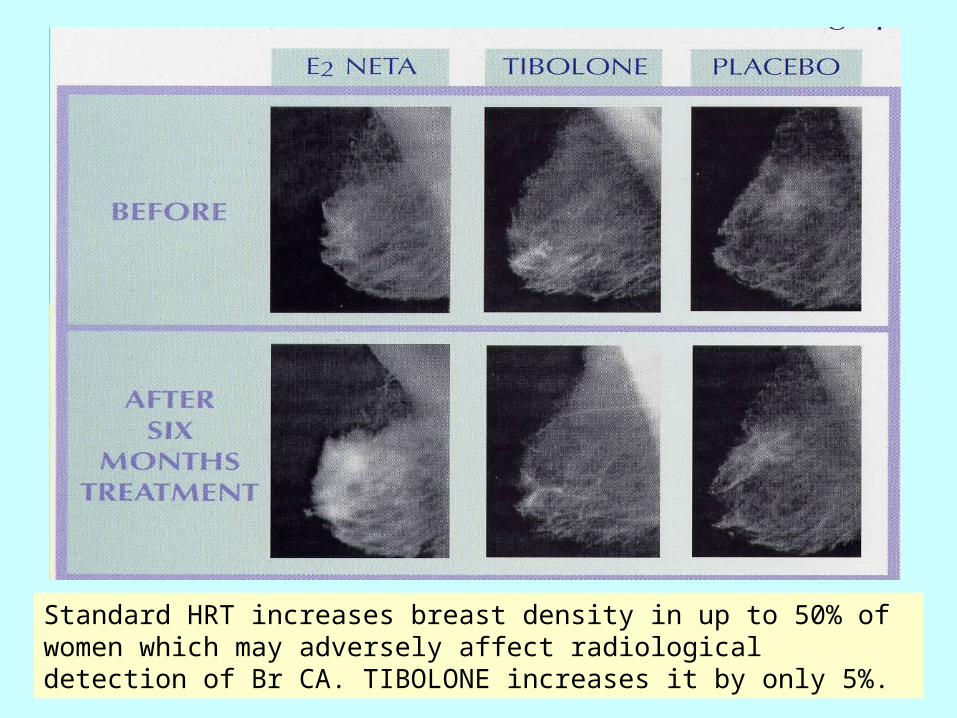
Standard HRT increases breast density in up to 50% of women which may adversely affect radiological detection of Br CA. TIBOLONE increases it by only 5%.
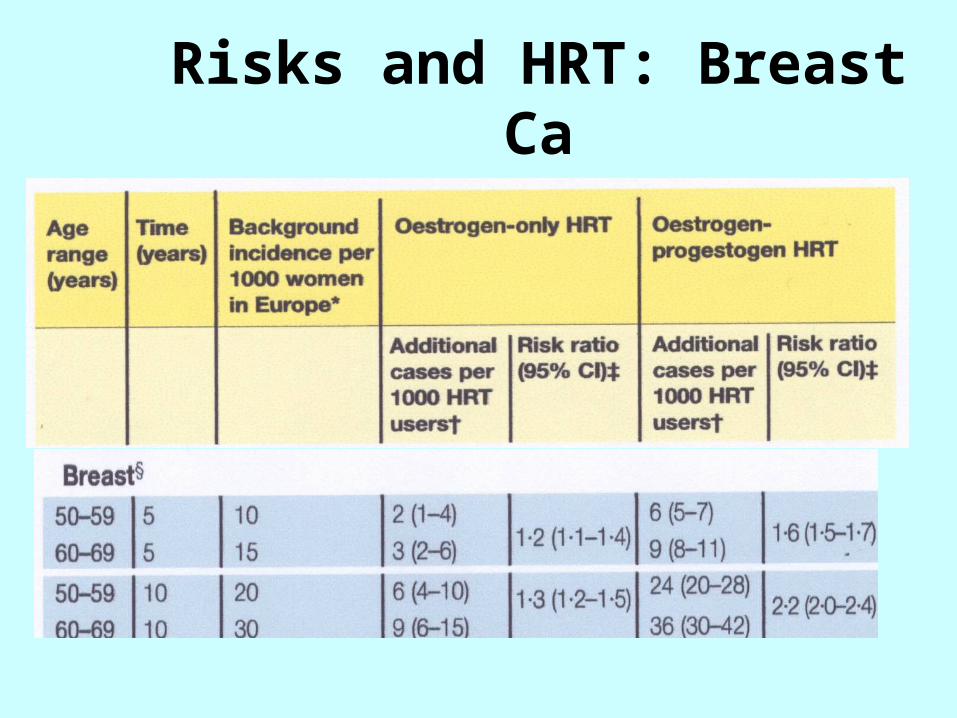
Risks and HRT: Breast Ca
Are there any alternatives to HRT?
SERMS
Specific
Estrogen
Receptors
Modulators
THE IDEAL ‘SERM’ WOULD:
• Give oestrogen agonism where it is needed
ie. skeleton, CVS and CNS
• Give oestrogen antagonism where it is needed ie. breast and uterus
TAMOXIFEN
• BONE probably favourable but no large trials
• CVS favorable effect on lipids but no effect on mortality
• UTERUS increase risk of endometrial proliferation, endometrial polyps and Ca body
RALOXIFENE
• Approved for the prevention of Approved for the prevention of non-traumatic vertebral non-traumatic vertebral fractures in post menopausal fractures in post menopausal women at increased risk of women at increased risk of osteoporosisosteoporosis
Summary of RaloxifeneSummary of Raloxifene
• Prevents bone loss• Favourable effect on lipid mechanism• Minor side effects • VTE risk similar to HRT• No endometrial stimulation• No increase in breast or endometrial cancer
riskBUT• Does not help menopausal symptoms
• Prevents bone loss• Favourable effect on lipid mechanism• Minor side effects • VTE risk similar to HRT• No endometrial stimulation• No increase in breast or endometrial cancer
riskBUT• Does not help menopausal symptoms
Alternatives to HRT: PHYTOESTROGENS
ISOFLAVONES
• red clover
• soy beanssoy beans
• soy productssoy products
• legumeslegumes
LIGNANS
• whole cereals
• oilseeds
• cereals
• berries
Phytoestrogens are plant substances that have effects similar to oestrogen
• Where isoflavones are an Where isoflavones are an integral part of the diet, integral part of the diet, menopausal symptoms, CHD, menopausal symptoms, CHD, osteoporosis, cancers of osteoporosis, cancers of breast, colon, endometrium breast, colon, endometrium and ovary are significantly and ovary are significantly lowerlower
• The isoflavone red clover is The isoflavone red clover is the only alternative treatment the only alternative treatment to have some trial evidence to have some trial evidence of benefit for menopausal of benefit for menopausal symptomssymptoms
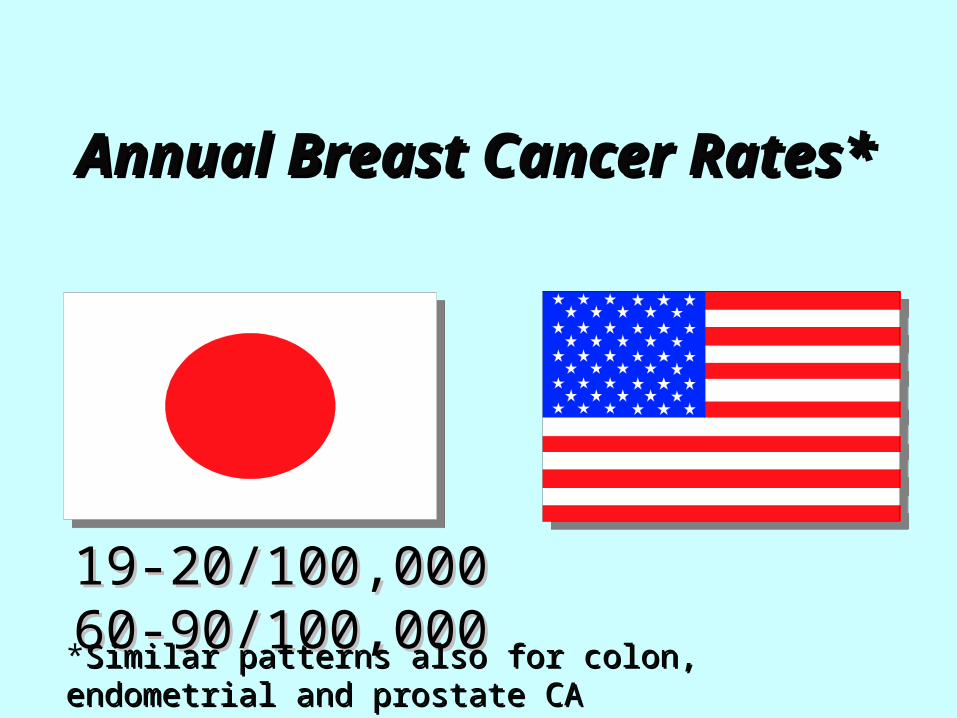
Annual Breast Cancer Rates*Annual Breast Cancer Rates*
19-20/100,000 60-90/100,00019-20/100,000 60-90/100,000
*Similar patterns also for colon, endometrial and prostate CASimilar patterns also for colon, endometrial and prostate CA
Other alternatives
• Herbalism: eg. Black cohosh, ginseng
• Homeopathy
• DHEA
• Acupuncture, magnets
None of these have definitively proven to be of benefit and drug interactions can occur
Read more: www.thebms.org.uk
Premature Ovarian Failure (Dysfunction)
• Cessation of menses before the age of 45
• Definition varies with the reference population (2SD below mean)
• Affects 1% women under 40
• Primary and secondary causes
Premature Ovarian Dysfunction
• Primary due to chromosome abnormalities eg Turner’s (XO); autoimmune disorders; enzyme defects
• Secondary due to chemotherapy, radiotherapy, surgery
• Spontaneous ovulation may occur with pregnancy rates up to 5-10%
Premature Ovarian Dysfunction
• Hormone replacement required to keep tissues healthy including bones and heart
• HRT (higher doses) or COCP to age 52
• Testosterone as patch or implant
• Risks are none use of HRT rather than use at this age. On HRT same risk as age equivalent population for breast Ca, VTE etc