Embed Size (px)
Citation preview

Listen to this manuscript’s
audio summary by
JACC Editor-in-Chief
Dr. Valentin Fuster.
J O U R N A L O F T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y V O L . 6 7 , N O . 1 5 , 2 0 1 6
ª 2 0 1 6 B Y T H E A M E R I C A N C O L L E G E O F C A R D I O L O G Y F O U N D A T I O N I S S N 0 7 3 5 - 1 0 9 7 / $ 3 6 . 0 0
P U B L I S H E D B Y E L S E V I E R h t t p : / / d x . d o i . o r g / 1 0 . 1 0 1 6 / j . j a c c . 2 0 1 6 . 0 1 . 0 7 1
REVIEW TOPIC OF THE WEEK
The Mitral Valve in ObstructiveHypertrophic Cardiomyopathy
A Test in ContextMark V. Sherrid, MD,a Sandhya Balaram, MD,b Bette Kim, MD,c Leon Axel, MD, PHD,d Daniel G. Swistel, MDe
ABSTRACT
Fro
Su
St.
an
Yo
rel
Ma
Mitral valve abnormalities were not part of modern pathological and clinical descriptions of hypertrophic cardiomyopathy
in the 1950s, which focused on left ventricular (LV) hypertrophy and myocyte fiber disarray. Although systolic
anterior motion (SAM) of the mitral valve was discovered as the cause of LV outflow tract obstruction in the M-mode
echocardiography era, in the 1990s structural abnormalities of the mitral valve became appreciated as contributing to
SAM pathophysiology. Hypertrophic cardiomyopathy mitral malformations have been identified at all levels. They occur
in the leaflets, usually elongating them, and also in the submitral apparatus, with a wide array of malformations of the
papillary muscles and chordae, that can be detected by transthoracic and transesophageal echocardiography and by
cardiac magnetic resonance. Because they participate fundamentally in the predisposition to SAM, they have increasingly
been repaired surgically. This review critically assesses imaging and measurement of mitral abnormalities and discusses
their surgical relief. (J Am Coll Cardiol 2016;67:1846–58) © 2016 by the American College of Cardiology Foundation.
L eft ventricular outflow tract (LVOT) obstruc-tion due to systolic anterior motion (SAM) ofthe mitral valve is a frequent cause of
disabling symptoms in hypertrophic cardiomyopathy(HCM). First-line therapy is pharmacological, withbeta-blockade, disopyramide, verapamil, or theircombinations (1). However, in patients with systolicgradients $50 mm Hg who fail to reach relief of symp-toms with pharmacotherapy or who have side effects,surgical myectomy is recommended by internationalguidelines as the primary and preferred modality forrelief of obstruction. An appreciation of mitral abnor-malities in HCM has accumulated over the past 20years (2–13). There has been a natural response bysurgeons to this greater understanding of the contri-bution of mitral pathology to SAM. At myectomy,they have tried to avoid leaving unrepaired pathologyby repairing the mitral valve (7–10,12–19). Diagnostic
m the aDivision of Cardiology, New York University Langone Medical
rgery, Mount Sinai St. Luke’s and Mount Sinai Roosevelt Hospitals, New Y
Luke’s and Mount Sinai Roosevelt Hospitals, New York, New York; dDep
d Physiology, New York University Langone Medical Center, New York, N
rk University Langone Medical Center, New York, New York. The auth
evant to the contents of this paper to disclose. Barry J. Maron, MD, serve
nuscript received November 18, 2015; revised manuscript received Janua
echocardiographic and cardiac magnetic resonance(CMR) discovery of mitral abnormalities in an elderlypatient may directly lead to a judgment for surgicalseptal myectomy rather than alcohol septal ablation(ASA), because ablation only addresses the septalthickening. Patients with mitral valve abnormalitiesmay be left with persistent SAM, gradients, and mitralregurgitation (MR) after ASA (20).
Guidelines support decisions to select surgery forpatients with mitral structural abnormalities. The2011 American guidelines state: “Additionally, spe-cific abnormalities of the mitral valve and its supportapparatus can contribute significantly to the genera-tion of outflow tract obstruction, suggesting thepotential value of additional surgical approaches(e.g., plication, valvuloplasty, and papillary musclerelocation) and making myectomy more appropriatethan alcohol septal ablation in some patients” (21). The
Center, New York, New York; bDivision of Cardiac
ork, New York; cDivision of Cardiology, Mount Sinai
artments of Radiology, Medicine, and Neuroscience
ew York; and the eDivision of Cardiac Surgery, New
ors have reported that they have no relationships
d as Guest Editor for this paper.
ry 3, 2016, accepted January 14, 2016.

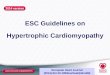
FIGURE 1 “Nightcap” Mitral Valve
Apical 3-chamber view in obstructive hypertrophic cardiomyopathy patient just after
leaflet coaptation. Tips of the elongated leaflets protrude 24 mm above the mitral annulus,
higher into the left ventricle than normal (double red arrow). As flow courses around the
septal bulge, it catches mitral leaflets and sweeps them into the septum.
AB BR E V I A T I O N S
AND ACRONYM S
CMR = cardiac magnetic
resonance
HCM = hypertrophic
cardiomyopathy
LV = left ventricle/ventricular
LVOT = left ventricular
outflow tract
MR = mitral regurgitation
MVR = mitral valve
replacement
SAM = systolic anterior motion
TEE = transesophageal
cardiography
J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6 Sherrid et al.A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8 Mitral Valve in Obstructive Hypertrophic Cardiomyopathy
1847
2015 European guidelines are more explicit: “Septalmyectomy, rather than SAA, is recommended in pa-tients with an indication for septal reduction therapyand other lesions requiring surgical intervention (e.g.,mitral valve repair/replacement, papillary muscleintervention) Class I, Level of Evidence: C” (22).
HISTORICAL APPRECIATION OF
MITRAL VALVE ABNORMALITIES IN HCM
In 1969, Shah et al. (23) reported with echocardio-graphy that LVOT obstruction in HCM was caused bySAM and mitral-septal contract. Anterior displace-ment of papillary muscles in the left ventricle (LV)was noted in 1974 (24) and was followed by relatedpublications (4,7,25,26). These investigatorsdescribed how this displacement positions mitralleaflets anteriorly into the flow stream and also re-duces their restraint, causing mitral slack, a necessarycomponent of dynamic SAM (25,27). Investigatorsfrom the National Institutes of Health (later fromMinneapolis) described direct insertion of an anom-alous anteriorly displaced papillary muscle into themiddle of the anterior mitral leaflet without inter-vening chordae (9). These displaced anterior papillarymuscles can contact the septum with each beat,causing submitral LV obstruction. Papillary muscle oranomalous chordae insertion into the midleaflet canalso tent the mitral leaflet anteriorly into the flowstream. Mitral leaflet elongation and its importancewas prominently brought to light by these same in-vestigators (2,3), who also described isolated poste-rior leaflet SAM occurring when this leaflet isparticularly elongated (28). At about the same time,transesophageal echocardiography (TEE) showedelongated leaflets in patients coming to surgery (29).
The most common cause of MR in obstructionoccurs when the posterior leaflet is not long or mobileenough to move anteriorly with the anterior leaflet,resulting in poor coaptation (29–31); MR is reduced oreliminated by abolition of SAM, either surgically orwith optimal pharmacological therapy (12,29,31). Theimportant point is that resolution of the SAM is thetherapeutic goal; this improves coaptation and theMR. In this review, mitral abnormalities are discussedaccording to their prominence and relative frequencyin patients coming to surgery. TEE is necessary toresolve any ambiguities about the cause of obstruc-tion when pre-operative imaging is suboptimal andalways in the operating room immediately before andafter cardiopulmonary bypass. The final operativeplan should be confirmed after review of TEE imme-diately before cardiopulmonary bypass. Because CMRhas been increasingly used to precisely demonstrate
abnormalities of the mitral apparatus in HCM,we will discuss its utility in detail.
ELONGATED ANTERIOR AND
POSTERIOR MITRAL LEAFLETS
The large majority of patients with obstruc-tive HCM have elongated anterior and pos-terior mitral leaflets, as compared withnormal subjects. Elongation has been notedpathologically, on echocardiography, and onCMR (2,3,5,6,12,29,32). In obstructive HCM,the anterior leaflet averages 34 mm versus 24mm in normal hearts (5,12,29). We havetermed this abnormality the “nightcap”
mitral valve because of its typical appearance onapical views at the moment of systolic coaptation(Figure 1). Elongated leaflets extend (protrude) intothe LV cavity well above the plane of the mitralannulus, a mean of 26 mm above the annuluscompared with 13 mm in normal hearts (5). Often, aresidual portion of the anterior mitral leaflet extendspast the point of coaptation (12,33), which is impor-tant in SAM pathophysiology because it is notecho

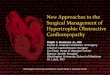
FIGURE 2 3-Dimensional TEE of the Residual Leaflet at the Moment of Mitral-Septal Contact
(Left) The 2-dimensional frame for orientation, showing systolic anterior motion and mitral-septal contact (white arrow). (Right)
Corresponding 3-dimensional frame; orientation is viewing mitral valve en face from left ventricular (LV) cavity, looking up at LV outflow tract.
Obstructing residual leaflet is shown with a white arrow. LV outflow tract orifices, displayed in black, are on either side of the residual leaflet,
shown with red arrows. High drag profile of the residual leaflet can be appreciated. TEE ¼ transesophageal echocardiography.
Sherrid et al. J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6
Mitral Valve in Obstructive Hypertrophic Cardiomyopathy A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8
1848
constrained by the LV–left atrium pressure differ-ence. Rather, it is only bounded by the LV and thusfreely moves with LV flow, even at low velocity (33).The residual leaflet usually contacts the septum first(Figure 2).
The protruding mitral leaflet plays an importantrole in the pathophysiology of SAM. Late diastolic andearly systolic flow strike the posterior surfaces of theprotruding leaflets with a high angle of attack andpush them into apposition with the septum (5,34,35).After mitral-septal contact, the pressure differenceitself pushes the obstructing mitral leaflet further intothe septum (34). Mitral leaflets are longer in patientswith obstructive HCM than with nonobstructiveHCM (5). An increased ratio of anterior leaflet lengthto LVOT diameter is associated with resting andprovocable obstruction (6). LVOT obstruction mayoccur after exercise in patients with completelynormal LV wall thickness; here the mitral leaflets areelongated and papillary muscles are anteriorly posi-tioned in the LV cavity (36). Echocardiographic andsome CMR reports have used different methods formeasuring the anterior mitral leaflet: echocardio-graphic papers have included the aortic-mitral conti-nuity (5,12,29), whereas some CMR papers haveexcluded this region (6).
A variety of surgical approaches have been devisedto correct anterior leaflet elongation. These haveincluded plication parallel to the long axis of thevalve, termed “vertical plication” (14); and plicationperpendicular to the long axis, termed “horizontalplication” (15,16,19,37,38). In short-axis views, thebody and tip of the anterior leaflet (usually A2) billow
out into the outflow tract, catching the forward flowof blood. Decreasing leaflet width in a medial/lateraldimension through vertical plication limits billowing(14). However, we have found that vertical plicationoften perturbs the coaptation line of the anteriorleaflet and causes central MR. With horizontalplication, as devised by Dr. Swistel, a line of suturesis placed horizontally across the pliable main body ofthe leaflet, within the aortomitral curtain. Thisstiffens the anterior leaflet, limits billowing, de-creases its area exposed to drag, shortens it, andprevents its leading edge from reaching the septum(12,16,19). Shortening of the leaflet is achievedwithout disturbing the coaptation line. Moreover,the procedure is quite simple. Done through theaortotomy, 4 or 5 sutures of 5-0 prolene are placed,using vertical mattress technique, horizontallyacross the leaflet, just superior to the bulk of thechordal attachments (Figure 3). The amount ofplication is easily chosen from 2 to 6 mm, dependingon need, as determined by pre-operative echocardi-ography (12) (Figure 4, Online Videos 1 and 2).
When excessive residual leaflet length contributesto obstruction, excision has been utilized as anancillary or alternative procedure to leaflet plication.A2 is often an isolated segment of excessive length,with 2 or 3 extremely slack and thinned-out chordae.Pre-operative analysis of the echocardiogram oftenreveals this segment to be inconsequential to coap-tation and competence, and direct examination in theoperative field suggests that these chordae play norole in preventing flail if removed. A segment of 2 to5 mm can at times be simply and safely excised

FIGURE 3 Horizontal Anterior Leaflet Plication
Reprinted with permission from Sherrid et al. (13). AML ¼ anterior mitral leaflet;
Ao ¼ aortic root; LCO ¼ left coronary ostium.
J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6 Sherrid et al.A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8 Mitral Valve in Obstructive Hypertrophic Cardiomyopathy
1849
(Figure 5). As in plication, judgment on the basis ofexperience must be exercised when determining thesafety of residual leaflet excision.
Another method to stiffen the mitral leaflet hasbeen termed anterior mitral leaflet extension. Here,the anterior leaflet is vertically incised and a stiffpericardial patch is inserted to prevent billowing ofthe leaflet (17). This underscores the principle thatalternate surgical approaches can be used in an indi-vidual patient to achieve optimal relief of LV outflowtract obstruction (18). However, inserting a pericardialpatch requires incising the valve, and can be time-consuming. The simplest, least time-consuming tech-nique should be used to repair mitral abnormalities, toavoid increasing the complexity of an already complexoperation. Note that virtually all leaflet repairsdescribed in this entire review are performed withoutinsertion of an annuloplasty ring.
ANTERIOR AND BASILAR DISPLACEMENT OF
THE ANTEROLATERAL PAPILLARY MUSCLE
Anterior displacement of the papillary musclesresults in an anterior position of the coaptation planeof the mitral valve in the LV cavity (4,7,26,39). Thiscauses a crucial overlap of the inflow and outflowportions of the LV that predisposes to SAM. We havemade direct surgical inspection of the papillarymuscles in HCM patients after extended myectomyand contrast them to those of hypertrophied patientswith aortic stenosis undergoing valve replacement.The 2 most common pathogenic abnormalities of thepapillary muscles in HCM are: 1) an anterior andbasilar displacement of the base of the anterolateral
FIGURE 4 Myectomy and Horizontal Anterior Leaflet Plication
(Left) Pre-operative apical 3-chamber frame in diastole showing elongat
dotted red line shows the site of extended myectomy. (Right) Post-ope
Online Videos 1 and 2. Reprinted with permission from Halpern et al. (1
papillary muscle (Figure 6); and 2) abnormal muscularconnections between its head and the anterolateralwall, inserting into or near the A1 scallop (12). RelatedCMR research reported by Kwon et al. (40) has shownanterior displacement of the anterolateral papillarymuscle and a higher frequency of bifid papillarymuscles; there was closer proximity between thesuperior papillary muscle and the septum in patientswith obstruction due to SAM (Figure 6). Obstruction
ed anterior mitral leaflet. Thickened bulging septum is shown, and the
rative frame showing shortened anterior leaflet and myectomy. See
2).

FIGURE 5 Residual Leaflet Excision
Surgical specimen from a patient who had an exceedingly long anterior leaflet and residual
leaflet. The residual leaflet was patulous and thin, and not contributing to coaptation. The
specimen is oriented with the leading edge (with its attached chordae) at the bottom.
Sherrid et al. J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6
Mitral Valve in Obstructive Hypertrophic Cardiomyopathy A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8
1850
magnitude correlated with anomalies, independentof septal thickness. Bifid papillary muscle, seen onCMR in Figure 6B, can appear on the echocardio-graphic short-axis view as an anterior extension anddisplacement (Figure 6A).
The extended myectomy, as described by Messmer(7) and by Schoendube et al. (8), includes release ofthe anterolateral papillary muscle by extending theresection laterally into the free wall above its baseand thinning the hypertrophied heads (12). Muscularconnections between the papillary muscle head andLV free wall are easily visualized when examining theventricular chamber during myectomy. We divideand excise these attachments, usually with a pituitaryrongeur (15,16,19). These techniques allow the ante-rior papillary muscle to fall posteriorly, drawing theanterior mitral leaflet with it, explicitly out of theejection stream. Papillary release brings the plane ofthe mitral annulus and aortic valve into a morenormal parallel orientation (41). Other surgeons havedevised novel surgical approaches for the contribu-tion of anomalous papillary muscles to SAM (40,42).
INSERTION OF ANTEROLATERAL PAPILLARY
MUSCLE DIRECTLY INTO THE MIDANTERIOR
MITRAL VALVE LEAFLET
Insertion of a head of the anterolateral papillarymuscle directly into the middle of the anterior mitral
valve leaflet without intervening chordae is demon-strated in Figures 7 to 9, by CMR in Online Videos 3and 4, and by 3-dimensional echocardiography inOnline Video 5. It may cause obstruction by apposi-tion of the papillary muscles with the septum onevery beat (9,18,43); when this occurs, flow acceler-ates in the submitral region. Off-axis echocardio-graphic views may be necessary for demonstration ofthis abnormality (18). CMR (through its superiorlateral resolution) and TEE can reliably demonstratethis morphological abnormality in the LVOT, whichcan alter management decisions. They should beperformed whenever there is ambiguity about thelevel of obstruction (43). With both techniques,tomographic planes can be chosen that show therelevant abnormalities and their anatomic relation-ships. Surgeons from the Mayo Clinic showed thataccessory papillary muscle heads and anomalouschordae could be removed if they did not support theleading edge of the valve leaflet (Figure 7) (18).Alternatively, the most anterior component can beexcised, leaving a posterior component attached tominimize the risk of flail leaflet. When the anomalouspapillary muscle is very large and directly obstructs,but excision is not possible, we have successfullyused a longitudinal resection to thin it, even to itsbase. This is combined with extended myectomy, tothe degree allowed by the septal thickness.
ANTERIOR MITRAL TENTING BY
PAPILLARY MUSCLES AND FIBROTIC,
RETRACTED SECONDARY CHORDAE
Anomalous anterior papillary muscles or fibrotic,retracted secondary mitral chordae may also con-tribute to obstructive pathophysiology and SAM, evenif they do not directly obstruct in the submitral area.They lift and tent the mitral valve anteriorly, so it ispre-positioned in the flow stream, predisposing toSAM (18,44) (Figure 9B).
ELONGATED POSTERIOR LEAFLET WITH SAM
When an isolated elongation of the posterior leafletcauses SAM, the residual leaflet protrudes through thespaces between the chordae to contact the septum (28)(Figure 10, Online Video 6). Although an uncommoncause of mitral-septal contact, it nonetheless cancause severe obstruction, and its identification beforesurgery is essential. Surgical alleviation has alwaysincluded some degree of septal resection; thus, theinitial exposure has been via the standard transaorticapproach. With this exposure, one can often access theposterior leaflet to excise a portion of the residualleaflet. Alternatively, if the posterior leaflet is not

FIGURE 6 Anterior Displacement of Hypertrophied Anterolateral Papillary Muscle
(A) Echocardiographic short-axis view of extra anteriorly displaced papillary muscles (red arrows). This bifid anteriorly displaced papillary
muscle positions the mitral valve leaflets anteriorly in the left ventricular chamber, where they overlap with the ejection flow stream.
(B) Cardiac magnetic resonance 4-chamber view showing hypertrophied bifid anterolateral papillary heads (red arrows), with the superior
head in close proximity to the septum (yellow arrows). Anterior displacement also decreases posterior restraint on mitral leaflets.
J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6 Sherrid et al.A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8 Mitral Valve in Obstructive Hypertrophic Cardiomyopathy
1851
accessible, we have approached the valve via left atrialincision and performed a narrow triangular resection,without an annuloplasty ring.
CALCIFICATION OF THE
MITRAL LEAFLETS OR ANNULUS
Occasionally, calcification of the mitral leaflets orannulus occurs in a patient who also has SAM withmitral-septal contact. It is generally the goal of 21st-century myectomy surgery to have patients leave the
FIGURE 7 TEE of Hypertrophied Anomalous Anterolateral Papillary
(A) Diastolic 0� view. Red arrows indicate anomalous papillary muscle i
muscle with the septum, causing severe obstruction. (C) Systolic frame,
obstruction. (D) Post-operative transthoracic parasternal view. Because
removed. Yellow arrowheads indicate septal myectomy. TEE ¼ transeso
operating room with their native mitral valves,to avoid the sequelae of mitral valve replacement(MVR) (i.e., chronic anticoagulation or late prosthesisdegeneration) (45). However, it is occasionallyimpossible to salvage the native mitral valve. A cluethat calcification or fibrosis is causing MR is anterioror mid-direction of the regurgitant jet. With regurgi-tation caused only by SAM, the jet is usually poste-riorly and laterally directed.
With even moderate annular calcification or ante-rior leaflet fibrosis, manipulation of the tissue is
Muscle Head Inserting Directly Into Midanterior Mitral Leaflet Without Intervening Chordae
n frames A to C. (B) Systolic frame, 0� view, showing apposition of the anomalous papillary
120�, showing apposition of the anomalous papillary muscle with the septum, causing severe
the papillary muscle did not support the leading edge of the anterior leaflet, it could be safely
phageal echocardiography.

FIGURE 8 CMR of Bifid Anomalous Anterolateral Papillary Muscle With Insertion Into the Midanterior Mitral Leaflet
(A) Early systolic 4-chamber view. Red arrows indicate anomalous muscle head in frames A and B. Note its proximity to the septum. (B) Early systolic 3-chamber view.
Note that papillary muscle tents up the middle of the anterior mitral leaflet (yellow arrow). (C) The 3-chamber view later in systole from a sequence demonstrating
flow velocities in outflow tract. Narrowing of the outflow tract between the papillary muscle and the septum causes flow acceleration due to obstruction. Note
that septal thickening is modest in this patient. See Online Videos 3, 4, and 5. CMR ¼ cardiac magnetic resonance.
Sherrid et al. J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6
Mitral Valve in Obstructive Hypertrophic Cardiomyopathy A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8
1852
not possible. On the basis of generalized results withmitral valve repair for other pathologies (i.e., rheu-matic disease), MVR might be necessary. However, ifthe primary pathology is an excessive residual leafletthat does not participate in coaptation, then residualleaflet excision with myectomy may be performed.
RELATIVELY THIN SEPTUM
Another situation in which MVR was previously theprimary option is the presence of a relatively thinseptum #18 mm. A limited myectomy would be per-formed because of concern that a ventricular septaldefect might result; alone, this would not be enoughof an intervention to alter flow adequately to relieve
FIGURE 9 Obstructing Anomalous Papillary Muscle
(A) Cardiac magnetic resonance (CMR) showing midsystolic apposition (
muscle (arrows) inserting directly into the anterior mitral leaflet (small
(B) Anomalous papillary muscle (red arrow) tapers and then inserts into
(yellow arrow). Orange arrow indicates leaflet coaptation. There was no p
anterior motion, and severe systolic anterior motion with high gradient a
SAM. However, these patients invariably have one ormultiple of the mitral valve abnormalities that lendthemselves to the operative repairs described previ-ously. Combined with a necessarily limited myec-tomy, this has sufficed to relieve SAM (12,42,44). Wenow routinely perform a limited myectomy on thesepatients, along with mitral repair without MVR. Arecent report of transaortic chordal cutting in patientswith relatively mild septal thickening has under-scored the utility of mitral repair in this group (44). In39 patients, intraoperative TEE and direct surgicalinspection detected that the anterior mitral leafletwas tented up into the outflow tract by retracted andfibrotic secondary chordae. A median of 3 secondarychordae were resected, in addition to necessarily
large arrowheads) of ventricular septum and anomalous papillary
arrowheads). Reprinted with permission from Rowin et al. (43).
the midportion of anterior leaflet and tents it anteriorly
apillary muscle-septal contact. Rather, there was mild resting systolic
fter exercise. Ao ¼ aorta; LA ¼ left atrium; VS ¼ ventricular septum.

FIGURE 10 Posterior Leaflet SAM, Mitral-Septal Contact, and Severe LVOT Obstruction
Apical transthoracic 5-chamber view. (A) Late diastole. Posterior leaflet is longer than the anterior leaflet. Friction lesion (from chronic mitral-
septal contact) on septum is indicated by the yellow arrow. (B) Moment of coaptation. There is a long residual leaflet from the posterior
leaflet that extends far past the anterior leaflet. Point of coaptation is indicated by the red arrow. (C) Next frame in systole showing coaptation
point with a red arrow and white arrow showing residual leaflet. (D) Posterior leaflet mitral-septal contact on septum at friction lesion. Resting
LVOT gradient was 80 mm Hg. Online Video 6 shows apical 3-chamber views from this patient. LVOT ¼ left ventricular outflow tract;
SAM ¼ systolic anterior motion.
J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6 Sherrid et al.A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8 Mitral Valve in Obstructive Hypertrophic Cardiomyopathy
1853
shallow myectomy; there was virtual abolition of highresting gradients and decrease in tenting. The CentralIllustration shows common anomalies of the mitralleaflets and papillary muscles that contribute toobstruction in HCM.
CLINICAL AND ECHOCARDIOGRAPHIC
RESULTS OF THE RESECT-PLICATE-RELEASE
OPERATION
From 1997 to 2015, we operated on 252 patientswith obstructive HCM for symptoms and gradientsresistant to pharmacological therapy (1,15,16). Theresect-plicate-release (RPR) techniques used were
adopted and modified from the reported surgicalexperience of others (7,8,9,14,18). The mean age was56 � 14 years; 55% were men. The average New YorkHeart Association functional class was 2.8 � 0.6. Themajority (96%) of these patients had surgery for SAMand mitral-septal contact. The remaining patients hadmid-LV obstruction.
In the patients who had SAM with mitral-septalcontact, LVOT gradients were 61 � 8 mm Hg andprovoked gradients were 111 � 41 mm Hg. Septalthickness was 24 � 5 mm (range 13 to 40 mm). Pre-operative echocardiography (both transthoracic andTEE) and now CMR provide the basis for the extent ofseptal resection; echocardiography and direct

CENTRAL ILLUSTRATION The Mitral Valve in Obstructive Hypertrophic Cardiomyopathy:Anomalies of the Mitral Valve and Papillary Muscle
Sherrid, M.V. et al. J Am Coll Cardiol. 2016;67(15):1846–58.
Continued on the next page
Sherrid et al. J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6
Mitral Valve in Obstructive Hypertrophic Cardiomyopathy A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8
1854

FIGURE 11 Algorithm of How Preoperative Echocardiography May Be Used to Guide Myectomy
ASA§
Frailty,Contraindication to
surgery, Aged
Obstructive HCM with rest orprovocable gradient ≥ 50 mm Hg
and symptoms refractory tooptimal medical therapy
MVR
ValvularCalcification
Anomalous papillary muscleinserting directly into the mid
anterior mitral leaflet
Extended myectomy andresect or thin anomalous
papillary muscle
Septal thickness ≤ 18 mmand AML > 30 mm
or > 17 mm/m2
Septal thickness > 18 mmand AML > 30 mm
or > 17 mm/m2
Septal thickness > 18 mmand AML ≤ 30 mm
or ≤ 17 mm/m2
Less aggressive myectomy,Plication of the AML*,
Release/resection of papillary muscles†or chordae
Extended myectomy,Plication of the AML*,
Release/resection of papillarymuscles†
Extended myectomy,Release/resection of papillary
muscles†, +/- Plication of AML asper surgical inspection for slack
“Plicate, Release” “Resect, Plicate,Release”
“Resect, Release”
Text in red and in quotations denote our shorthandmethod for categorizing our pre-operative assessment of which procedures should be done.
*Additionally, direct surgical inspection of anterior leaflet for slack determines indication for and extent of plication. Extensive mitral calcification
of anterior leaflet or annulus is a contraindication to plication. Patients with extensive calcification require mitral valve replacement. †Papillary
muscle release is predicted on pre-operative echocardiography by anterior extension of the lateral papillary muscle. §Dual-chamber pacing
with short AV delay is also a therapeutic option for frail elderly patients. AML ¼ anterior mitral leaflet; ASA ¼ alcohol septal ablation; AV ¼atrioventricular; HCM ¼ hypertrophic cardiomyopathy; MVR ¼ mitral valve replacement. Modified with permission from Halpern et al. (12).
J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6 Sherrid et al.A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8 Mitral Valve in Obstructive Hypertrophic Cardiomyopathy
1855
surgical inspection provide the basis for individualcase-by-case judgments regarding the need for mitralplication and papillary muscle release. Plication wasperformed in 66% of patients; papillary release was
CENTRAL ILLUSTRATION Continued
The top left image shows normal anatomy of mitral leaflets as they ap
shown underneath (A to C). The top right image shows normal papillar
anomalies are shown underneath on the right (D to F). (D to F) The aor
out-of-plane as well. Papillary muscles send chordae to both mitral lea
anterior mitral leaflet; arrow points to residual leaflet. (B) Elongation of p
of both mitral leaflets; the anterior leaflet is most often the longer of t
papillary muscle-bifid papillary muscle (white arrow). The vector of res
papillary muscle head (lower arrow) inserts directly into the middle of th
shown) and obstruct there, or may tent anterior leaflet into the LVOT. (
anterior leaflet and tents it into the LVOT (arrows), predisposing to sys
and papillary muscles may occur, but are not shown together for graphi
ventricle; LVOT ¼ left ventricular outflow tract; PW ¼ posterior wall.
performed in 86%. MVR was necessary in 6%.Concomitant procedures were performed in 35%,with coronary artery bypass graft as the most com-mon (16%).
pear on the apical long-axis view. Mitral valve anomalies are
y muscles as they appear on the 2-chamber view. Papillary muscle
tic valve is out-of-plane, its position shown as an oval; the septum is
flets but these are not shown for graphic clarity. (A) Elongation of
osterior mitral leaflet; arrow points to residual leaflet. (C) Elongation
he 2. (D) Additional thickened, anteriorly-displaced anterolateral
traint is now anterior (black arrow). (E) Anomalous anterolateral
e anterior mitral leaflet (top arrow). This may contact the septum (not
F) Abnormal chord, under tension, inserts into the midportion of the
tolic anterior motion. Combinations of anomalies of both the leaflets
c clarity. Ao ¼ aorta; AW ¼ anterior wall; LA ¼ left atrium; LV ¼ left

Sherrid et al. J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6
Mitral Valve in Obstructive Hypertrophic Cardiomyopathy A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8
1856
Operative mortality was 0.4%. The post-proceduralcomplication rate was 15%; the majority of compli-cations were respiratory compromise in older patientswith multiple comorbidities. Complete heart blockrequiring pacemaker insertion occurred in 6%. Earlyreoperation was required in 2 patients (0.4%): 1 forventricular septal defect repair and 1 for MVR.Length of stay was 7 � 5 days. There was markedimprovement in New York Heart Association func-tional class for 96%. In our 2012 report, survival at1, 5, and 10 years was 98%, 98%, and 92%, respec-tively (16).
We recently reported on detailed echocardiogra-phy before and after the resect-plicate-release repairin 77 patients. Pre-operative echocardiographicanterior mitral length provides a basis to recommendperformance of plication and defines its extent.We recommend plication when the anterior leaflet is>30 mm long or >17 mm/m2. Plication decreasesanterior leaflet length by 16%, residual leaflet lengthby 33%, and protrusion into the LV above the mitralannular plane by 24%. After papillary muscle release,there was a decrease in the distance from mitralcoaptation to the posterior LV wall. Surgery abolishedsevere SAM and resting gradients and reducedMR (12). An algorithm describing our use of echocar-diography, both transthoracic and TEE, to selectwhich of the “resect,” “plicate,” or “release” pro-cedures to apply in an individual patient is presentedin Figure 11.
SHOULD MITRAL SURGERY
ACCOMPANY MYECTOMY?
There is controversy about whether mitral valveabnormalities should be surgically repaired at thetime of myectomy (46). Some centers generallyperform mitral repair in addition to extended myec-tomy (8,10,14–17), whereas it is the judgment ofothers to usually just perform myectomy (1,47). Itmay be a natural surgical approach to comprehen-sively address all discovered contributors to apatient’s SAM, and to not leave unrepaired pathology.However, because a clinical trial has not been per-formed comparing results of myectomy plus mitralrepair versus myectomy alone, these decisionscurrently rest in the realm of clinical judgments.
Myectomy is considered to be among the mostchallenging of all surgical procedures for acquiredheart disease. The paucity of centers applying isolatedmyectomy provides silent evidence of a precipitouslearning curve; there is difficulty gauging “too muchversus too little myectomy.” Residual obstruction
requiring reoperation was previously reported afterisolated myectomy (48,49); which we have not seen inour experience (12,15,16). For inexperienced surgeons,isolated myectomy is an imprecise tool; there is a re-ported myectomy hospital mortality of 6% at non-referral centers in the U.S. Nationwide InpatientSample (50). In contrast, there is very low 30-day post-operative mortality, 0.5%, in patients operated on atdedicated HCM specialty centers (51).
Concomitant mitral surgery, particularly, RPRmyectomy operation, provides a buffer against failurethat may occur because of imprecision in depthand extent of myectomy. Mitral repair remediatesthe mitral half of obstructive HCM physiology;myectomy addresses only the flow abnormalityrelated to the septal bulge. The decision of whetherto repair detected abnormalities of the mitral valveat myectomy should be undertaken jointly by thereferring cardiologist and surgeon. Technical aspectsof mitral plication are undemanding and can bereadily learned. Papillary muscle release is moretechnically challenging and requires experience.However, echocardiographic and clinical resultsof its usefulness for relieving SAM suggest that aneffort to master the technique should be pursued.Given the experience required to master thesesurgical techniques, patients who are resistant tomaximal pharmacological therapy should be referredfor evaluation and treatment to dedicated HCMcenters (51).
WHY IS THE MITRAL VALVE ABNORMAL
IN HCM, WHICH IS CAUSED BY
MUTATIONS IN GENES CODING FOR
SARCOMERIC PROTEINS?
Leaflet elongation has been observed in subjects whohave an HCM-associated mutation but who have notyet developed thickening, suggesting that mitralelongation is a primary phenotypic expression ofHCM and is not acquired due to stretch from SAM (6).Elongated leaflets are not myxomatous (2). Abnormalcell lines that elongate to form valves appear tooriginate from epithelial-derived cells from coelomicmesothelium that migrate to endocardial cushions(52). These cells may respond to paracrine or to localmechanotransduction signals with the observeddevelopmental abnormalities (11,53).
CONCLUSIONS
In many patients with HCM, mitral valve abnormal-ities play a major contributing role in LV outflow

J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6 Sherrid et al.A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8 Mitral Valve in Obstructive Hypertrophic Cardiomyopathy
1857
obstruction. In patients who come to surgery at manycenters, the judgment is made to repair contributingmitral abnormalities whenever they are detected,regardless of the magnitude of septal hypertrophy.Mitral abnormalities play a particularly importantrole in patients with mild or moderate hypertrophy.These patients should not be treated by septalreduction alone (ASA in particular); surgical mitralvalve repair in association with septal myectomy isthe preferred approach. A number of surgical tech-niques are available to repair the mitral valve in HCM;given the great diversity of mitral abnormalities, the
proper technique should be selected for the individ-ual patient.
ACKNOWLEDGMENTS The authors thank Drs.Waseem Shami and Robert Nampiaparampil for theirtechnical expertise.
REPRINT REQUESTS AND CORRESPONDENCE: Dr.Mark V. Sherrid, Division of Cardiology, New YorkUniversity Langone Medical Center, Skirball 9N, 530First Avenue, New York, New York 10016. E-mail:[email protected].
RE F E RENCE S
1. Sherrid MV, Shetty A, Winson G, et al. Treat-ment of obstructive hypertrophic cardiomyopathysymptoms and gradient resistant to first-linetherapy with b-blockade or verapamil. Circ HeartFail 2013;6:694–702.
2. Klues HG, Maron BJ, Dollar AL, et al. Diversityof structural mitral valve alterations in hypertro-phic cardiomyopathy. Circulation 1992;85:1651–60.
3. Klues HG, Proschan MA, Dollar AL, et al. Echo-cardiographic assessment of mitral valve size inobstructive hypertrophic cardiomyopathy. Anato-mic validation from mitral valve specimen. Circu-lation 1993;88:548–55.
4. Jiang L, Levine RA, King ME, et al. An inte-grated mechanism for systolic anterior motion ofthe mitral valve in hypertrophic cardiomyopathybased on echocardiographic observations. AmHeart J 1987;113:633–44.
5. Ro R, Halpern D, Sahn DJ, et al. Vector flowmapping in obstructive hypertrophic cardiomyop-athy to assess the relationship of early systolic leftventricular flow and the mitral valve. J Am CollCardiol 2014;64:1984–95.
6. Maron MS, Olivotto I, Harrigan C, et al. Mitralvalve abnormalities identified by cardiovascularmagnetic resonance represent a primary pheno-typic expression of hypertrophic cardiomyopathy.Circulation 2011;124:40–7.
7. Messmer BJ. Extended myectomy for hyper-trophic obstructive cardiomyopathy. Ann ThoracSurg 1994;58:575–7.
8. Schoendube FA, Klues HG, Reith S, et al. Long-term clinical and echocardiographic follow-up af-ter surgical correction of hypertrophic obstructivecardiomyopathy with extended myectomy andreconstruction of the subvalvular mitral appa-ratus. Circulation 1995;92:II122–7.
9. Klues HG, Roberts WC, Maron BJ. Anomalousinsertion of papillary muscle directly into anteriormitral leaflet in hypertrophic cardiomyopathy.Significance in producing left ventricular outflowobstruction. Circulation 1991;84:1188–97.
10. Kaple RK, Murphy RT, DiPaola LM, et al.Mitral valve abnormalities in hypertrophic cardio-myopathy: echocardiographic features and surgi-cal outcomes. Ann Thorac Surg 2008;85:1527–35.
11. Hagège AA, Bruneval P, Levine RA, et al. Themitral valve in hypertrophic cardiomyopathy: oldversus new concepts. J Cardiovasc Transl Res2011;4:757–66.
12. Halpern DG, Swistel DG, Po JR, et al.Echocardiography before and after resect-plicate-release surgical myectomy for obstructive hyper-trophic cardiomyopathy. J Am Soc Echocardiogr2015;28:1318–28.
13. Sherrid MV, Chaudhry FA, Swistel DG.Obstructive hypertrophic cardiomyopathy: echo-cardiography, pathophysiology, and the con-tinuing evolution of surgery for obstruction. AnnThorac Surg 2003;75:620–32.
14. McIntosh CL, Maron BJ, Cannon RO III, et al.Initial results of combined anterior mitral leafletplication and ventricular septal myotomy-myectomy for relief of left ventricular outflowtract obstruction in patients with hypertrophiccardiomyopathy. Circulation 1992;86:II60–7.
15. Balaram SK, Tyrie L, Sherrid MV, et al.Resection-plication-release for hypertrophiccardiomyopathy: clinical and echocardiographicfollow-up. Ann Thorac Surg 2008;86:1539–44,discussion 1544–5.
16. Balaram SK, Ross RE, Sherrid MV, et al. Role ofmitral valve plication in the surgical managementof hypertrophic cardiomyopathy. Ann Thorac Surg2012;94:1990–7, discussion 1997–8.
17. Vriesendorp PA, Schinkel AF, Soliman OI, et al.Long-term benefit of myectomy and anteriormitral leaflet extension in obstructive hypertro-phic cardiomyopathy. Am J Cardiol 2015;115:670–5.
18. Minakata K, Dearani JA, Nishimura RA, et al.Extended septal myectomy for hypertrophicobstructive cardiomyopathy with anomalousmitral papillary muscles or chordae. J ThoracCardiovasc Surg 2004;127:481–9.
19. Swistel DG, DeRose JJ Jr., Sherrid MV. Man-agement of patients with complex hypertrophiccardiomyopathy: resection/plication/release. OperTech Thorac Cardiovasc Surg 2004;9:261–7.
20. Delling FN, Sanborn DY, Levine RA, et al.Frequency and mechanism of persistent systolicanterior motion and mitral regurgitation afterseptal ablation in obstructive hypertrophic car-diomyopathy. Am J Cardiol 2007;100:1691–5.
21. Gersh BJ, Maron BJ, Bonow RO, et al. 2011ACCF/AHA guideline for the diagnosis and treat-ment of hypertrophic cardiomyopathy: executivesummary: a report of the American College ofCardiology Foundation/American Heart Associa-tion Task Force on Practice Guidelines. J Am CollCardiol 2011;58:2703–38.
22. Elliott PM, Anastasakis A, Borger MA, et al.2014 ESC guidelines on diagnosis and manage-ment of hypertrophic cardiomyopathy. Eur Heart J2014;35:2733–79.
23. Shah PM, Gramiak R, Kramer DH. Ultrasoundlocalization of left ventricular outflow obstructionin hypertrophic obstructive cardiomyopathy. Cir-culation 1969;40:3–11.
24. Reis RL, Bolton MR, King JF, et al. Anterion-superior displacement of papillary muscles pro-ducing obstruction and mitral regurgitation inidiopathic hypertrophic subaortic stenosis. Oper-ative relief by posterior-superior realignment ofpapillary muscles following ventricular septalmyectomy. Circulation 1974;50:II181–8.
25. Cape EG, Simons D, Jimoh A, et al. Chordalgeometry determines the shape and extent ofsystolic anterior mitral motion: in vitro studies.J Am Coll Cardiol 1989;13:1438–48.
26. Levine RA, Vlahakes GJ, Lefebvre X, et al.Papillary muscle displacement causes systolicanterior motion of the mitral valve. Experimentalvalidation and insights into the mechanism ofsubaortic obstruction. Circulation 1995;91:1189–95.
27. Joshi S, Patel UK, Yao SS, et al. Standing andexercise Doppler echocardiography in obstructivehypertrophic cardiomyopathy: the range of gradi-ents with upright activity. J Am Soc Echocardiogr2011;24:75–82.
28. Maron BJ, Harding AM, Spirito P, et al. Systolicanterior motion of the posterior mitral leaflet: apreviously unrecognized cause of dynamic sub-aortic obstruction in patients with hypertrophiccardiomyopathy. Circulation 1983;68:282–93.
29. Grigg LE, Wigle ED, Williams WG, et al.Transesophageal Doppler echocardiography inobstructive hypertrophic cardiomyopathy: clarifi-cation of pathophysiology and importance inintraoperative decision making. J Am Coll Cardiol1992;20:42–52.

Sherrid et al. J A C C V O L . 6 7 , N O . 1 5 , 2 0 1 6
Mitral Valve in Obstructive Hypertrophic Cardiomyopathy A P R I L 1 9 , 2 0 1 6 : 1 8 4 6 – 5 8
1858
30. Schwammenthal E, Nakatani S, He S, et al.Mechanism of mitral regurgitation in hypertrophiccardiomyopathy: mismatch of posterior to anteriorleaflet length and mobility. Circulation 1998;98:856–65.
31. Yu EH, Omran AS, Wigle ED, et al. Mitralregurgitation in hypertrophic obstructive cardio-myopathy: relationship to obstruction and reliefwith myectomy. J Am Coll Cardiol 2000;36:2219–25.
32. He S, Hopmeyer J, Lefebvre XP, et al. Impor-tance of leaflet elongation in causing systolicanterior motion of the mitral valve. J Heart ValveDis 1997;6:149–59.
33. Shah PM, Taylor RD, Wong M. Abnormal mitralvalve coaptation in hypertrophic obstructive cardio-myopathy: proposed role in systolic anterior motionof mitral valve. Am J Cardiol 1981;48:258–62.
34. Sherrid MV, Chu CK, Delia E, et al. An echo-cardiographic study of the fluid mechanics ofobstruction in hypertrophic cardiomyopathy. J AmColl Cardiol 1993;22:816–25.
35. Sherrid MV, Gunsburg DZ, Moldenhauer S,et al. Systolic anterior motion begins at low leftventricular outflow tract velocity in obstructivehypertrophic cardiomyopathy. J Am Coll Cardiol2000;36:1344–54.
36. Alhaj EK, Kim B, Cantales D, et al. Symptom-atic exercise-induced left ventricular outflow tractobstruction without left ventricular hypertrophy.J Am Soc Echocardiogr 2013;26:556–65.
37. Patel P, Dhillon A, Popovic ZB, et al. Leftventricular outflow tract obstruction in hypertro-phic cardiomyopathy patients without severeseptal hypertrophy: implications of mitral valveand papillary muscle abnormalities assessed usingcardiac magnetic resonance and echocardiogra-phy. Circ Cardiovasc Imaging 2015;8:e003132.
38. Malik R, Rastegar H, Maron M, et al. Hyper-trophic cardiomyopathy patients undergoingmyectomy often require additional reparativeprocedures of mitral valvular and subvalvulardisorders: intraoperative findings and complex
surgical procedures (abstr). J Am Coll Cardiol2013;61 Suppl 10:E1226.
39. Henry WL, Clark CE, Griffith JM, et al. Mech-anism of left ventricular outflow obstruction inpatients with obstructive asymmetric septal hy-pertrophy (idiopathic hypertrophic subaortic ste-nosis). Am J Cardiol 1975;35:337–45.
40. Kwon DH, Setser RM, Thamilarasan M, et al.Abnormal papillary muscle morphology is inde-pendently associated with increased left ventric-ular outflow tract obstruction in hypertrophiccardiomyopathy. Heart 2008;94:1295–301.
41. Nakatani S, Schwammenthal E, Lever HM,et al. New insights into the reduction of mitralvalve systolic anterior motion after ventricularseptal myectomy in hypertrophic obstructive car-diomyopathy. Am Heart J 1996;131:294–300.
42. Kwon DH, Smedira NG, Thamilarasan M, et al.Characteristics and surgical outcomes of symp-tomatic patients with hypertrophic cardiomyopa-thy with abnormal papillary muscle morphologyundergoing papillary muscle reorientation.J Thorac Cardiovasc Surg 2010;140:317–24.
43. Rowin EJ, Maron BJ, Lesser JR, et al. Papillarymuscle insertion directly into the anterior mitralleaflet in hypertrophic cardiomyopathy, its identi-fication and cause of outflow obstruction by cardiacmagnetic resonance imaging, and its surgicalmanagement. Am J Cardiol 2013;111:1677–9.
44. Ferrazzi P, Spirito P, Iacovoni A, et al. Trans-aortic chordal cutting: mitral valve repair forobstructive hypertrophic cardiomyopathy withmild septal hypertrophy. J Am Coll Cardiol 2015;66:1687–96.
45. Roberts WC. Operative treatment of hyper-trophic obstructive cardiomyopathy. The caseagainst mitral valve replacement. Am J Cardiol1973;32:377–81.
46. Maron BJ, Nishimura RA. Revisiting arrhythmicrisk after alcohol septal ablation: is the pendulumfinally swinging.back to myectomy? J Am CollCardiol HF 2014;2:637–40.
47. Dearani JA, Ommen SR, Gersh BJ, et al. Sur-gery insight: Septal myectomy for obstructivehypertrophic cardiomyopathy—the Mayo Clinicexperience. Nat Clin Pract Cardiovasc Med 2007;4:503–12.
48. Roberts CS, McIntosh CL, Brown PS Jr., et al.Reoperation for persistent outflow obstruction inhypertrophic cardiomyopathy. Ann Thorac Surg1991;51:455–60.
49. Minakata K, Dearani JA, Schaff HV, et al.Mechanisms for recurrent left ventricular outflowtract obstruction after septal myectomy forobstructive hypertrophic cardiomyopathy. AnnThorac Surg 2005;80:851–6.
50. Panaich SS, Badheka AO, Chothani A, et al.Results of ventricular septal myectomy and hy-pertrophic cardiomyopathy (from NationwideInpatient Sample [1998–2010]). Am J Cardiol2014;114:1390–5.
51. Maron BJ, Dearani JA, Ommen SR. Low oper-ative mortality achieved with surgical septalmyectomy: role of dedicated hypertrophic car-diomyopathy centers in the management of dy-namic subaortic obstruction. J Am Coll Cardiol2015;66:1307–8.
52. Olivotto I, Cecchi F, Poggesi C, et al. Devel-opmental origins of hypertrophic cardiomyopathyphenotypes: a unifying hypothesis. Nat Rev Car-diol 2009;6:317–21.
53. Levine RA, Hagege AA, Judge DP, et al. Mitralvalve disease-morphology and mechanisms.Nature Rev Cardiol 2015;12:689–710.
KEY WORDS cardiac surgery, hypertrophicobstructive cardiomyopathy, left ventricularoutflow obstruction, mitral valve anomalies,mitral valve surgery, papillary muscles
APPENDIX For supplemental videos andtheir legends, please see the online version ofthis article.