Embed Size (px)
Citation preview

CLINICAL TRIAL
The MSKCC nomogram for prediction the likelihoodof non-sentinel node involvement in a German breastcancer population
M. Klar Æ A. Jochmann Æ M. Foeldi Æ M. Stumpf ÆG. Gitsch Æ E. Stickeler Æ D. Watermann
Received: 21 December 2007 / Accepted: 21 December 2007 / Published online: 3 January 2008
� Springer Science+Business Media, LLC. 2008
Abstract Objective To assess whether the Memorial
Sloan Kettering Cancer Center (MSKCC) nomogram for
prediction of NSLN metastasis is useful in a German breast
cancer population and whether the characteristics of the
breast tumor and the sentinel lymph node (SLN) are able to
predict the likelihood of non-sentinel lymph node (NSLN)
metastasis. Methods A total of 545 patients with primary
breast cancer and SLN examination were evaluated. The
MSKCC nomogram was applied to 98 patients with a
positive SLN who subsequently had completion axillary
lymph node dissection (ALND). Predictive accuracy was
assessed by calculating the area under the receiver-operator
characteristic (ROC) curve. The collective was evaluated
by correlating the prevalence of NSLN and SLN metastasis
to pathological features. Results The MSKCC nomogram
achieved a ROC of 0.58 indicating a bad accuracy of the
nomogram. Tumor size, histology, lymphovascular infil-
tration, multifocality, Her-2-neu positivity, and nuclear
grade correlated with the probability of SLN metastasis.
Histology and primary tumor localization correlated
significantly with the probability of NSLN metastasis.
Conclusions The MSKCC nomogram did not provide a
reliable predictive model in our study population. How-
ever, the likelihood of SLN metastasis correlated with the
presumed risk factors and no obvious differences between
the MSKCC population and our population could be seen.
In order to achieve interinstitutional reproducibility,
standardization of surgical procedure and of the patholog-
ical assessment of the SLN is desirable.
Keywords Breast cancer � Sentinel lymph node biopsy �Non sentinel lymph node metastasis � Axillary lymph
node dissection � Breast cancer nomogram
Introduction
Sentinel lymph node (SLN) biopsy is a valid method of
assessing axillary lymph node involvement in patients with
early breast cancer [1]. Although axillary lymph node
dissection (ALND) is still standard of care in any case of
SLN metastasis [2–8], there is an ongoing debate about the
necessity for complete ALND in every patient with meta-
static SLN, especially in those with little risk of additional
disease since 40–60% of patients have no disease in axil-
lary lymph node other than SLN itself [1, 9, 10]. These
patients, therefore, are unlikely to benefit from further
surgery that results in a longer period of hospitalization,
higher costs and higher postoperative morbidity [11].
Opponents of ALND after proven metastatic SLN fur-
thermore argue that the therapeutic impact is minimal [12]
and that SLN positive patients will receive systemic ther-
apy, regardless of the presence of any additional nodal
metastasis. Proponents, however, support more aggressive
treatment referring to the survival data from the National
Cancer Database for women with stage I and stage II breast
carcinoma demonstrating a significant worse 10-year
survival when ALND was omitted [13].
Within the last years a number of studies investigated
the risk of additional axillary involvement in early breast
cancer. The most powerful independent predictor described
in theses studies is the size of the primary tumor and the
M. Klar � A. Jochmann � M. Foeldi � M. Stumpf � G. Gitsch �E. Stickeler � D. Watermann (&)
Department of Obstetrics and Gynecology,
University of Freiburg, Medical School, Hugstetter Str. 55,
79106 Freiburg, Germany
e-mail: [email protected]
123
Breast Cancer Res Treat (2008) 112:523–531
DOI 10.1007/s10549-007-9884-1

size of SLN metastasis [14–19]. However, up to now,
metaanalyses have failed to quantify the predictive value of
these features [20]. One reason might be the heterogeneity
in the investigational procedures, another the different
patient population. Therefore, validation of predictive
characteristics of the primary tumor and the SLN in dif-
ferent settings is still needed and represented the first goal
of this study.
Van Zee et al. from the Memorial Sloan Kettering
Cancer Center (MSKCC) assessed potential independent
predictors of non-sentinel lymph node metastasis (NSLN)
by creating a nomogram. The chosen variables (pathologic
size, tumor type, nuclear grade, multifocality, estrogen
receptor status, method of detection of the SNL, number of
positive and negative SLN) were based on a review of
literature and their own data [21]. The analyses showed a
receiver–operator characteristic curve (ROC) of 0.76. The
same model used in a prospective setting in the same center
revealed a ROC of 0.77. Breast cancer specialists, in
comparison, when asked to predict the likelihood of
NSLN-metastasis with the same given characteristics,
achieved only a ROC of 0.54 [22]. A model with a ROC of
0.5 is equal to the toss of a coin. A model with a ROC of
0.7–0.8 is considered good, whereas an ROC of 0.81–0.9
has excellent discrimination.
Interinstitutional differences exist concerning SLN
mapping, removal, pathological assessment and staining.
This might influence the accuracy of the nomogram.
Therefore, a validation of the nomogram is obligatory
before its use as a predictive tool. The purpose of this study
was to validate the MSKCC nomogram in a community
breast cancer center patient population in Germany.
Materials and methods
From January 1999 to December 2005, 1,612 patients with
histologically proven breast cancer were treated in our
department. Of these, 577 underwent breast-conserving
surgery or mastectomy with SLN biopsy since they met the
inclusion criteria for SLN biopsy (histologically proven
breast cancer, negative axillary lymph nodes on palpation
and sonography, informed consent for sentinel lymph node
procedure). Patients were excluded from SNL biopsy in case
of failed SLN mapping, inflammatory breast cancer, ductal
carcinoma in situ (DCIS), no informed consent, clinically
suspicious axillary lymph nodes, pregnancy and lactation,
allergies against nanocol or dye stuffs, or previous operation
of the axilla. A total of 32 patients were excluded because of
lacking follow-up-data or failed SLN detection.
For SLN mapping, we used either the radiotype (97.5%)
or the blue dye (2.5%) technique. Both techniques have been
described elsewhere in detail [23, 24]. For radioisotope
technique, 99mTc-nanocol was injected subcutaneously
around the tumor 1 day prior to surgery and lymphoscin-
tigraphy was performed. Intraoperatively, the SLN were
detected by using a hand held gamma probe. Any lymph
node with radioactivity was regarded as SLN and sent to
immediate intraoperative pathological evaluation using
frozen section. ALND was performed in any case of tumor
detected intraoperatively or at final pathological diagnosis.
The remaining SLN material was further analyzed by
hematoxylin–eosin staining (H&E) and immunohistochem-
istry (IHC). If tumor cell clusters were detected by these
techniques secondary ALND was performed. The tumor
stage was classified according to UICC classification.
Hormone receptor and Her-2/neu status was determined by
immunohistochemistry, a Her-2/neu score of +++ was
classified as positive.
Data from all patients were entered into a database. This
database included for each patient: personal data, data on
surgery, data on the tumor, SLN data, NSLN data, data on
adjuvant treatment, date of recurrence, time of follow up
and nomogram-specific data (tumor type, pathological size
in cm, grading, presence of lymphovascular invasion,
multifocalilty and multicentricity, estrogen and progesteron
receptor status, method of detection of SLN metastasis and
number of positive SLN).
A total of 118 patients (of 545 patients meeting the
inclusion criteria of our study) were SLN positive. Of
these, 98 patients underwent ALND with at least 10 lymph
nodes removed from the axilla. Standard of care by com-
pletion via ALND with at least 10 nodes after positive
SLN, however, was not performed in the remaining 20
patients. This was due to several reasons, like treatment
with radiotherapy for tumor control in the axilla instead of
surgery, metastatic disease or severe comorbidity. In
addition, in 6 patients ALND was performed, but less than
10 lymph nodes were removed. A total of 427 patients were
SLN negative. Of these 125 underwent ALND during our
initial training period, when the SLN-technique was
introduced at our institution.
Patients were categorized in three groups: SLN-negative
without ALND (n = 302), SLN-negative with ALND
(n = 125) and SLN-positive (n = 118).
All analyses were conducted with SPSS12.1. For numeric
data, values are expressed in mean and median val-
ues ± standard derivation (SD). Numeric data was analysed
with Student’s-t-Test if normal distribution and equality of
variances were given. If not, the Mann–Whithney-Test was
used for comparison of data. Categoric data was analysed
with the Chi-Square-test or with Fisher’s-Exact-Test.
In order to calculate the risk of NSLN metastasis, we
evaluated the MSKCC nomogram provided in a free online
version (http://www.mskcc.org/nomograms). The predic-
tive power of the nomogram was assessed by calculating the
524 Breast Cancer Res Treat (2008) 112:523–531
123

area under the receiver–operator characteristic (ROC) curve.
Further information on the methods of development and
internal validation are available on the above internet site and
the corresponding publication [21].
Results
The MSKC nomogram in our collective
of SLN-positive patients
The overall descriptive clinical and histopathological char-
acteristics of patients with SNL biopsy (n = 545) are shown
in Table 1. Adjuvant treatment of theses patients included
chemo- (52%), radio- (72%) and endocrine therapy (72%).
The overall survival (OS) in the whole cohort (n = 545)
in the mean follow up time of 32.5 months was 97.6%, the
disease free survival (DFS) was 93.6%.
Clinical data collected for MSKC nomogram included:
size of primary tumor, tumor type and nuclear grade,
multifocality, lymphovascular invasion, estrogen receptor
status, method of metastasis detection, number of positive
SLN and number of negative SLN. Inclusion criteria were:
Invasive breast cancer, no neoadjuvant chemotherapy, SLN
metastasis and at least 10 lymph nodes removed at ALND.
Of the 118 SLN positive patients 98 could be included in
the MSKC calculation. In comparison to the population of
the original publication of the MSKC nomogram [21] our
collective showed no major differences (Table 2).
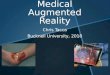
In order to assess the accuracy of the nomogram in our
collective, actual probabilities were plotted against the
calculated probabilities for each decile of patients. The
trend line differed in a few deciles more than 50% (Fig. 1).
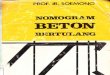
The ROC was 0.58 (Fig. 2).
In conclusion, the MSKC nomogram does not provide
an accurate prediction of the probability of NSLN-metas-
tasis in our cohort of SLN-positive breast cancer patients.
Collective assessment
Data on survival and recurrences
During the follow-up time, within the group of SLN-
negative-patients receiving no ALND (n = 302) nine
recurrences (3.0%) were observed: five local recurrences at
the breast, one axillary recurrence and three distant
metastasis.
Within the group of SLN-positive (n = 118), 18 recur-
rences (15.2%) were observed: four local recurrences at the
breast and 14 distant metastasis. Three patients with distant
metastasis died within the follow-up time. No axillary local
recurrence was observed in this group.
Within the group of patients receiving ALND after
negative SLN (n = 125), eight recurrences occurred
(6.4%) during follow up time, including three local recur-
rences at the breast, two axillary recurrences and three
distant metastasis.
Table 1 Overall patient and tumor characteristics of the patient
population
Variable Frequency
n %
Age (at the time of operation)
\50 years 121 22
C50 years 424 78
Tumor size (cm)
\1 130 24
1–3 370 68
[3 43 8
Tumor location
UIQ 106 19
UOQ 251 47
LIQ 44 8
LOQ 91 17
Central 43 8
Histology
Ductal 344 63
Lobular 116 21
Other 85 16
Nuclear grade
I 64 12
II 332 61
III 146 27
Centricity
Multifocal 165 73
Unifocal 380 27
Receptor status
ER positive 407 75
PR postitive 362 66
Her-2/neu
0–2 375 69
3 59 11
Unknown 111 20
Lymphovascular invasion
Negative 430 79
Positive 115 21
No. of positive lymph nodes
0 427 78
1 82 15
2 26 5
C3 10 2
LIQ, Lower inner quadrant; LOQ, Lower outer quadrant; UIQ, Upper
inner quadrant; UOQ, Upper outer quadrant
Breast Cancer Res Treat (2008) 112:523–531 525
123

SLN metastasis
As presumed, tumor size, histology, lymphovascular infiltra-
tion, multifocality, Her-2-neu positivity, and nuclear grade
correlated with the probability of SLN metastasis (Table 3).
118 of the 545 patients (22%) had at least one positive
SNL (characteristics shown in Table 2). 178 positive SLN
were obtained (mean 1.51 SNL per patient). Of the 118
SNL-positive patients, 16 (13.5%) had isolated tumor cells
(ITC) in the SNL, whereas 60 (50.8%) and 28 (23.7%) had
Table 2 Comparison of descriptive characteristics of the prospective and retrospective patient collectives: UFK, Freiburg; MSKCC, New York;
CWH Nijmegen and MD Anderson, Houston
Variable UFK
Freiburg retrospective
group (n = 98)
MSKCC
New York prospective
group (n = 373)
CWH
Nijmegen prospective
group (n = 222)
MD Anderson
Houston retrospective
group (n = 200)
n % n % n % n %
Age (years)
B50 30 30.6 157 35.1 78 35.1 123 62
Tumor size (mm)
B0.5 5 5.1 13 3.5 1 0.5 5 3
0.6–1.0 7 7.1 49 13.1 13 5.9 25 13
1.1–2.0 45 46.0 166 44.5 90 40.5 91 46
2.1–3.0 25 25.5 93 24.9 69 31.1 39 20
3.1–5.0 11 11.2 41 11 40 18.0 20 10
[5.1 5 5.1 11 2.9 9 4.0 20 10
Tumor type and nuclear grade
Ductal, I 2 2 11 2.9 30 13.5 14 7
Ductal, II 50 51 175 46.9 78 35.1 86 43
Ductal, III 20 20.4 129 34.6 65 29.3 63 32
Lobular 26 26.5 58 15.5 49 22.1 20 10
Lymphovascular invasion 46 46.9 154 41.3 72 32.4 60 30
Multifocality 38 34.7 132 35.4 55 24.8 19 9
Estrogen receptor pos. 74 76.3 290 77.7 190 85.6 160 80
Method of detection
IHC only 10 10.2 18 4.8 49 22.1 8 4
Serial H&E 24 24.5 40 10.7 38 17.1 99 50
Routine H&E – – 296 79.4 135 60.8 35 18
Frozen section 64 65.3 128 47 – – – –
Number of positive SLN
1 66 67.3 265 71 163 73.4 150 75
2 24 24.5 75 20.1 48 21.6 42 21
3 3 3.1 21 5.6 7 3.1 6 3
4 4 4.1 8 2.1 3 1.4 1 0.5
5 3 0.8 0 0 1 0.5
C6 1 1 1 0.3 1 0.5 – –
Number of negative SLN
0 50 51 132 35.4 131 59 77 39
1 22 22.4 79 21.2 64 28.8 50 25
2 12 12.2 72 19.3 19 8.6 39 20
3 6 6.1 41 11 7 3.1 14 7
4 3 3.1 22 5.9 0 0 7 4
5 2 2 7 1.9 1 0.5 6 3
C6 3 3 20 5.3 0 0 7 4
IHC, Immunohistochemistry; H&E, Hematoxylin and eosin; SLN, Sentinel lymph node
526 Breast Cancer Res Treat (2008) 112:523–531
123

macro ([2 mm)- and micrometastasis (B2 mm), respec-
tively. In 14 patients the size was not specified.
NSLN metastasis
A total of 55 patients of the 545 patients (10%) showed
NSLN-metastasis. The prevalence of NSLN metastasis in
the group of SLN positive patients was 46.6% (55 of 118
patients), with a mean number of 3.47 involved lymph
nodes.
Only histology (P \ 0.023) and primary tumor locali-
zation (P \ 0.049) correlated significantly with NSLN-
metastasis. Tumor grade, lymphovascular infiltration, SNL
capsular infiltration, centricitiy and biologic features
(estrogen and progesterone receptor status, Her2/neu
expression) of the primary tumor did not correlate with the
prevalence of NSLN metastasis (Table 4).
Discussion
The MSKCC nomogram has already been evaluated by
numerous centers (Table 5) [25–34]. Interestingly, whereas
the nomogram seems to provide a useful predictive tool in
the North American [25, 34], and Australian [26, 27]
population, the results from European institutions are
heterogenous: Kocscis et al. [28] (Hungary) found the
correlation between the predicted and observed proportions
weaker for their patients than for the patients assessed at
the MSKCC. Alran et al. (France) warned against the use
of the nomogram for patients with micrometastatic positive
SLN and proposed the integration of age, proliferation
0%1 to10
11 to20
21 to30
31 to40
41 to50
51 to60
61 to70
71 to80
81 to90
91 to100
20%
40%
60%
80%
100%
120%
Groups (%)
)%(
ytilib
ab
orP
BCN predicted probability
actual probability
Fig. 1 Comparison between actual and predicted probability
Fig. 2 Receiver–operator characteristic (ROC) curve calculation for
the MSKCC nomogram applied to the Freiburg data (n = 98)
Table 3 Clinicopathologic correlation in patients with SLN-
metastasis
Variable SLN neg. SLN pos. P-value
Number of patients 427 118
Primary tumor size (mean in mm) 16.5 20.82 \0.001
Age (mean) 59 58 0.28
Histology \0.001
Ductal 265 (62%) 79 (67%)
Lobular 81 (19%) 35 (30%)
Other 81 (19%) 4 (3%)
Nuclear grade 0.015
I 59 (14%) 5 (4%)
II 255 (60%) 77(65%)
III 110 (26%) 36 (31%)
Primary tumor location 0.079
UOQ 185 (44%) 66 (57%)
UIQ 91 (22%) 15 (13%)
LOQ 71 (17%) 20 (17%)
LIQ 38 (9%) 6 (5%)
Central 34 (8%) 9 (8%)
ER receptor pos. 323 (76%) 90 (76%) 1.0
PR receptor pos. 289 (68%) 76 (64%) 0.509
Her-2/neu pos. (Score +++) 143 (34%) 52 (44%) 0.039
Lymphovascular invasion positive 58 (14%) 57 (48%) \0.001
Multifocality 117 (27%) 48 (41%) 0.007
Breast Cancer Res Treat (2008) 112:523–531 527
123

index and hormone receptors in the present nomogram
[29]. Zgajnar et al. (Slovenia) found that the MSKCC
nomogram overestimates the probability of NSLN metas-
tasis [32]. Pal et al. (UK) suggested a revised predictive
model using more detailed pathologic features and
achieved a ROC curve of impressive 0.84 [33]. Smidt et al.
(The Netherlands) and Ponzone et al. (Italy), found the
MSKCC nomogram helpful to predict an individual’s risk
of NSLN involvement, although their collectives differed
significantly from the one’s of the MSKCC (Table 2) [30,
31]. It is thus questionable, whether the discrepancies in the
study population alone make it difficult to recommend the
nomogram as a world-wide prediction tool. Most presum-
ably some other factors contribute as well to the lack of
reproducibility of the nomogram.
Firstly, the methods of pathological assessments vary
among the present studies [21, 25, 28–30]. Lambert et al.
showed accurate results of the nomogram by using touch
imprint cytology (TIC) for intraoperative assessment of
SLN and suggested the suitability of substituting TIC for
frozen section within the nomogram [25]. However, Kocsis
et al., who also used TIC, failed to successfully validate the
nomogram in their collective [28]. Although the two
techniques appear to be roughly equivalent [35], we con-
sider (and so do Kocsis et al.) the differences in the
intraoperative assessment (frozen section vs TIC, interin-
dividual differences of microscopic assessment) to partly
explain the lower correlation between predicted and
observed probability. The final diagnosis of SLN metasta-
sis is often based on H&E staining, whereas the MSKCC
uses frozen section as the method of choice for SLN
metastasis-detection.
Secondly, the diameter of the SLN metastasis is not
included in the calculation of the MSKCC nomogram,
although the size of SNL metastasis is described to be one
of the most powerful independent predictor for additional
axillary involvement [13–18]. In this context it would be
Table 4 Clinicopathologic correlation in patients with NSLN-
metastasis
Variable NSLN neg. NSLN pos. P-value
Total number of ALND
with more than 10 nodes
61 37
Age 58.3 56.4 0.495
Primary tumor diameter
(mean in mm)
21.2 21.0 0.918
Total number of lymph nodes 15.6 16.9 0.251
Number of pos. SLN 1.4 1.7 0.919
Size of SLN metastasis 0.08
Macrometastasis 30 24
Micrometastasis 19 5
Histology 0.023
Ductal 37 (61%) 31 (84%)
Lobular 22 (36%) 4 (11%)
Other 2 (3%) 2 (5%)
Nuclear grade 0.278
I 4 0
II 41 26
III 16 11
Lymphovascular invasion 0.129
Neg. 36 16
Pos. 25 21
SNL capsule infiltration 0.347
Neg. 48 26
Pos. 13 11
Primary tumor location 0.049
UOQ 37 21
UIQ 8 3
LOQ 5 10
LIQ 5 0
Central 6 2
Centricity 0.522
Unifocal 40 20
Multifocal 17 14
Multicentric 4 3
Histology and primary tumor localisation correlates significantly with
NSLN-metastasis. All other clinicopathologic parameters had no
predictive value (control: NSLN-metastasis to size of NSLN metas-
tasis, P: 0.000)
* Quotient of number of positive SLN to total number of removed
axillary lymph nodes
Table 5 Results of validations of the MSKCC nomogram
References Patients (n) ROC Correlation
coefficient (r)
Van Zee, USA (2003) 373 0.77 0.97
Without frozen section data 373 0.78
Kocsis, Hungary (2004) 140 NA 0.84–0.87
Smidt, The Netherlands (2005) 222 0.78 NA
Soni, Australia (2005) 149 0.75 NA
Degnim, USA (2005)
Mayo Clinics dataset
465 0.72 NA
Degnim, USA (2005)
Michigan dataset
89 0.86 NA
Dauphine, USA (2006) 51 0.63 NA
Cripe, USA (2006) 92 0.82 0.86
Lambert, USA (2006) 200 0.71 0.97
Zgainar, Slovenia (2007) 276 0.72 NA
Ponzone, Italy (2007) 186 0.71 NA
Alran, France (2007) 588 0.72 NA
Pal, UK (2007) 118 0.68 NA
528 Breast Cancer Res Treat (2008) 112:523–531
123

interesting to determine if the inclusion of the criteria ‘‘size
of SLN metastasis’’ would contribute to a better accuracy
among the different institutions.
Thirdly, the number of removed SLN varies among the
different studies. We have removed a mean 1.51 SLN per
patient which corresponds to the number of Kocsis et al.
[28]. In contrast, Lambert et al. removed a mean 2.0 SLN
per patient. It is plausible that with fewer SLNs removed,
the number of positive NSLN increases. According to the
Axilla Management Consensus Group there is general
consensus that SLN biopsy should aim to remove all nodes
that are blue, hot, blue and hot or palpably suspicious [36].
In this context, further studies on the validation on the
nomogram should standardize their protocol of the surgical
approach of SLN mapping and removal.
Breast cancer has a long natural history and relatively
small residual disease might become clinically apparent
later than during our follow-up time. We also cannot dis-
tinguish the effects of surgery, chemotherapy, radiotherapy
and antihormonal treatment on local and distant relapses.
Therefore, we did not compare DFS and OS between the
groups of patients since an appropriate stratification in
tumor stage and adjuvant treatment was not reasonable due
the limited number of patients.
Our study confirms that axillary recurrence after SLN
biopsy is a rare event. Studies on SLN biopsy followed by
ALND have shown this technique to be a reliable method
of staging in patients with clinical node-negative disease
[37]. Moreover, SLN biopsy allows enhanced pathologic
analyses to increase accuracy of staging and decrease false-
negative results, ranging between 5 and 10% [38–40]. In
this view, it is not astonishing that no axillary recurrence
occurred within 32.5 months after positive SLN biopsy and
consecutive ALND. This is probably not only an effect of
the completion of dissection in the axilla, since there was
also no axillary recurrence within the SLN-negative group
of patients without ALND (n = 302). Naik et al. from the
MSKCC have similar data on axillary recurrence after SNL
biopsy with or without ALND, 0.35 and 1.4%, respectively
[39]. Veronesi et al., Louis-Sylvestre et al. and Chua et al.
provide similar data of axillary recurrence after SLN
biopsy followed by ALND (0–2.1% at a follow up time of
40–180 months) [41–43].
Size of the tumor, histology, lymphovascular infiltration,
multifocality, Her-2/neu positivity, and nuclear grade corre-
late with the probability of SLN metastasis (Table 3). The
likelihood of SLN metastasis correlated with the presumed
risk factors mentioned above. These findings are consistent
with the recently published prediction model for the presence
of SLN metastasis [44]. Based on a large dataset (n = 3,786)
of the MSKCC Beilacqua et al. described the association of
SLN metastasis with the variables age, tumor size, tumor type,
lymphovascular invasion, tumor location, multifocality and
estrogen and progesterone receptors. The subsequently
developed SLN-nomogram will soon be available on the same
web-page of the MSKCC as the NSLN-nomogram we have
used in our study.
We have conducted a validation of the MSKCC nom-
gram for the prediction of NSLN involvement in early
breast cancer in a German breast cancer population. In our
analyses, the MSKCC nomogram did not provide a reliable
predictive model for identifying patients with a low or a
high risk for NSLN metastasis. Therefore, further testing in
different institutions are needed. We recommend the vali-
dation of the original [21] or the modified [33] nomogram.
Given the relevant variations in SLN surgical procedures
and pathological assessment of the SLN, we advise caution
against the unvalidated use of this prediction tool.
References
1. Veronesi U, Paganelli G, Galimberti V, Viale G, Zurrida S,
Bedoni M, Costa A, de Cicco C, Geraghty JG, Luini A, Sacchini V,
Veronesi P (1997) Sentinel-node biopsy to avoid axillary dissection
in breast cancer with clinically negative lymph-nodes. Lancet
349:1864–1867
2. Wong SL, Edwards MJ, Chao C, Tuttle TM, Noyes RD, Woo C,
Cerrito PB, McMasters KM (2001) Predicting the status of the
nonsentinel axillary nodes: a multicenter study. Arch Surg
136:563–568
3. Rahusen FD, Torrenga H, van Diest PJ, Pijpers R, van der Wall
E, Licht J, Meijer S (2001) Predictive factors for metastatic
involvement of nonsentinel nodes in patients with breast cancer.
Arch Surg 136:1059–1063
4. den Bakker MA, van Weeszenberg A, de Kanter AY, Beverdam
FH, Pritchard C, van der Kwast TH, Menke-Pluymers M (2002)
Non-sentinel lymph node involvement in patients with breast
cancer and sentinel node micrometastasis; too early to abandon
axillary clearance. J Clin Pathol 55:932–935
5. Sachdev U, Murphy K, Derzie A, Jaffer S, Bleiweiss IJ, Brower S
(2002) Predictors of nonsentinel lymph node metastasis in breast
cancer patients. Am J Surg 183:213–217
6. Mignotte H, Treilleux I, Faure C, Nessah K, Bremond A (2002)
Axillary lymph-node dissection for positive sentinel nodes in
breast cancer patients. Eur J Surg Oncol 28:623–626
7. Nos C, Harding-MacKean C, Freneaux P, Trie A, Falcou MC,
Sastre-Garau X, Clough KB (2003) Prediction of tumour
involvement in remaining axillary lymph nodes when the sentinel
node in a woman with breast cancer contains metastasis. Br J
Surg 90:1354–1360
8. de Widt-Levert L, Tjan-Heijnen V, Bult P, Ruers T, Wobbes T
(2003) Stage migration in breast cancer: surgical decisions con-
cerning isolated tumour cells and micro-metastasis in the sentinel
lymph node. Eur J Surg Oncol 29:216–220
9. Abdessalam SF, Zervos EE, Prasad M, Farrar WB, Yee LD,
Walker MJ, Carson WB, Burak WE Jr (2001) Predictors of
positive axillary lymph nodes after sentinel lymph node biopsy in
breast cancer. Am J Surg 182:316–320
10. Barnwell JM, Arredondo MA, Kollmorgen D, Gibbs JF,
Lamonica D, Carson W, Zhang P, Winston J, Edge SB (1998)
Sentinel node biopsy in breast cancer. Ann Surg Oncol 5:126–130
11. Veronesi U, Paganelli G, Viale G, Luini A, Zurrida S, Galimberti
V, Intra M, Veronesi P, Robertson C, Maisonneuve P, Renne G,
Breast Cancer Res Treat (2008) 112:523–531 529
123

De Cicco C, De Lucia F, Gennari R (2003) A randomized
comparison of sentinel-node biopsy with routine axillary dis-
section in breast cancer. N Engl J Med 349:546–553
12. Cady B. (1997) Case against axillary lymphadenectomy for most
patients with infiltrating breast cancer. J Surg Oncol 66:7–10
13. Bland KI, Scott-Conner CE, Menck H, Winchester DP (1999)
Axillary dissection in breast-conserving surgery for stage I and II
breast cancer: a national cancer data base study of patterns of
omission and implications for survival. J Am Coll Surg 188:586–
595; discussion 595–596
14. Hwang RF, Krishnamurthy S, Hunt KK, Mirza N, Ames FC,
Feig B, Kuerer HM, Singletary SE, Babiera G, Meric F, Akins JS,
Neely J, Ross MI. (2003) Clinicopathologic factors predicting
involvement of nonsentinel axillary nodes in women with breast
cancer. Ann Surg Oncol 10:248–254
15. Cserni G (2001) Sentinel lymph-node biopsy-based prediction of
further breast cancer metastasis in the axilla. Eur J Surg Oncol
27:532–538
16. Turner RR, Chu KU, Qi K, Botnick LE, Hansen NM, Glass EC,
Giuliano AE (2000) Pathologic features associated with nonsen-
tinel lymph node metastasis in patients with metastatic breast
carcinoma in a sentinel lymph node. Cancer 89:574–581
17. Reynolds C, Mick R, Donohue JH, Grant CS, Farley DR, Callans
LS, Orel SG, Keeney GL, Lawton TJ, Czerniecki BJ (1999)
Sentinel lymph node biopsy with metastasis: can axillary dis-
section be avoided in some patients with breast cancer? J Clin
Oncol 17:1720–1726
18. Weiser MR, Montgomery LL, Tan LK, Susnik B, Leung DY,
Borgen PI, Cody HS 3rd (2001) Lymphovascular invasion
enhances the prediction of non-sentinel node metastasis in breast
cancer patients with positive sentinel nodes. Ann Surg Oncol
8:145–149
19. Viale G, Maiorano E, Pruneri G, Mastropasqua MG, Valentini S,
Galimberti V, Zurrida S, Maisonneuve P, Paganelli G, Mazzarol
G (2005) Predicting the risk for additional axillary metastasis in
patients with breast carcinoma and positive sentinel lymph node
biopsy. Ann Surg 241:319–325
20. Degnim AC, Reynolds C, Pantvaidya G, Zakaria S, Hoskin T,
Barnes S, Roberts MV, Lucas PC, Oh K, Koker M, Sabel MS,
Newman LA (2005) Nonsentinel node metastasis in breast cancer
patients: assessment of an existing and a new predictive nomo-
gram. Am J Surg 190:543–550
21. Van Zee KJ, Manasseh DM, Bevilacqua JL, Boolbol SK, Fey JV,
Tan LK, Borgen PI, Cody HS 3rd, Kattan MW (2003) A
nomogram for predicting the likelihood of additional nodal
metastasis in breast cancer patients with a positive sentinel node
biopsy. Ann Surg Oncol 10:1140–1151
22. Specht MC, Kattan MW, Gonen M, Fey J, Van Zee KJ (2005)
Predicting nonsentinel node status after positive sentinel lymph
biopsy for breast cancer: clinicians versus nomogram. Ann Surg
Oncol 12:654–659
23. Gipponi M, Bassetti C, Canavese G, Catturich A, Di Somma C,
Vecchio C, Nicolo G, Schenone F, Tomei D, Cafiero F (2004)
Sentinel lymph node as a new marker for therapeutic planning in
breast cancer patients. J Surg Oncol 85:102–111
24. Varghese P, Mostafa A, Abdel-Rahman AT, Akberali S,
Gattuso J, Canizales A, Wells CA, Carpenter R (2007) Methylene
blue dye versus combined dye-radioactive tracer technique for
sentinel lymph node localisation in early breast cancer. Eur J Surg
Oncol 33:147–152
25. Lambert LA, Ayers GD, Hwang RF, Hunt KK, Ross MI, Kuerer
HM, Singletary SE, Babiera GV, Ames FC, Feig B, Lucci A,
Krishnamurthy S, Meric-Bernstam F (2006) Validation of a
breast cancer nomogram for predicting nonsentinel lymph node
metastasis after a positive sentinel node biopsy. Ann Surg Oncol
13:310–320
26. Degnim AC, Griffith KA, Sabel MS, Hayes DF, Cimmino VM,
Diehl KM, Lucas PC, Snyder ML, Chang AE, Newman LA
(2003) Clinicopathologic features of metastasis in nonsentinel
lymph nodes of breast carcinoma patients. Cancer 98:2307–2315
27. Soni NK, Carmalt HL, Gillett DJ, Spillane AJ (2005) Evaluation
of a breast cancer nomogram for prediction of non-sentinel lymph
node positivity. Eur J Surg Oncol 31:958–964
28. Kocsis L, Svebis M, Boross G, Sinko M, Maraz R, Rajtar M,
Cserni G (2004) Use and limitations of a nomogram predicting
the likelihood of non-sentinel node involvement after a positive
sentinel node biopsy in breast cancer patients. Am Surg 70:1019–
1024
29. Alran S, De Rycke Y, Fourchotte V, Charitansky H, Laki F,
Falcou MC, Benamor M, Freneaux P, Salmon RJ for the Institut
Curie Breast Cancer Study Group, Sigal-Zafrani B (2007) Vali-
dation and limitations of use of a breast cancer nomogram
predicting the likelihood of non-sentinel node involvement after
positive sentinel node biopsy. Ann Surg Oncol 14:2195–2201
30. Smidt ML, Kuster DM, van der Wilt GJ, Thunnissen FB, Van Zee
KJ, Strobbe LJ (2005) Can the Memorial Sloan-Kettering Cancer
Center nomogram predict the likelihood of nonsentinel lymph
node metastasis in breast cancer patients in the Netherlands? Ann
Surg Oncol 12:1066–1072
31. Ponzone R, Maggiorotto F, Mariani L, Jacomuzzi ME, Magistris
A, Mininanni P, Biglia N, Sismondi P (2007) Comparison of two
models for the prediction of nonsentinel node metastasis in breast
cancer. Am J Surg 193:686–692
32. Zgajnar J, Perhavec A, Hocevar M, Podkrajsek M, Hertl K,
Frkovic-Grazio S, Pohar M, Besic N (2007) Low performance of
the MSKCC nomogram in preoperatively ultrasonically negative
axillary lymph node in breast cancer patients. J Surg Oncol
96:547–553
33. Pal A, Provenzano E, Duffy SW, Pinder SE, Purushotham
AD(2007) A model for predicting non-sentinel lymph node
metastatic disease when the sentinel lymph node is positive. Br J
Surg: Epub ahead of print
34. Cripe MH, Beran LC, Liang WC, Sickel-Santanello B (2006) The
likelihood of additional nodal disease following a positive sen-
tinel lymph node biopsy in breast cancer patients: validation of a
nomogram. Am J Surg 192:484–487
35. Aihara T, Munakata S, Morino H, Takatsuka Y (2004) Com-
parison of frozen section and touch imprint cytology for
evaluation of sentinel lymph node metastasis in breast cancer.
Ann Surg Oncol 11:747–750
36. Benson JR, della Rovere GQ, Axilla Management Consensus
Group (2007) Management of the axilla in women with breast
cancer. Lancet Oncol 8:331–348
37. Cody HS 3rd (2003) Sentinel lymph node biopsy for breast
cancer: does anybody not need one? Ann Surg Oncol 10:1131–
1132
38. Liberman L (2000) Pathologic analysis of sentinel lymph nodes
in breast carcinoma. Cancer 88:971–977
39. Naik AM, Fey J, Gemignani M, Heerdt A, Montgomery L, Petrek
J, Port E, Sacchini V, Sclafani L, VanZee K, Wagman R, Borgen
PI, Cody HS 3rd (2004) The risk of axillary relapse after sentinel
lymph node biopsy for breast cancer is comparable with that of
axillary lymph node dissection: a follow-up study of 4008 pro-
cedures. Ann Surg 240:462–468; discussion 468–471
40. Martin RC, Derossis AM, Fey J, Yeung H, Yeh SD, Akhurst T,
Heerdt AS, Petrek J, VanZee KJ, Montgomery LL, Borgen PI,
Cody HS 3rd (2001) Intradermal isotope injection is superior to
intramammary in sentinel node biopsy for breast cancer. Surgery
130:432–438
41. Veronesi U, Salvadori B, Luini A, Banfi A, Zucali R, Del
Vecchio M, Saccozzi R, Beretta E, Boracchi P, Farante G et al
(1990) Conservative treatment of early breast cancer. Long-term
530 Breast Cancer Res Treat (2008) 112:523–531
123

results of 1232 cases treated with quadrantectomy, axillary dis-
section, and radiotherapy. Ann Surg 211:250–259
42. Louis-Sylvestre C, Clough K, Asselain B, Vilcoq JR, Salmon RJ,
Campana F, Fourquet A (2004) Axillary treatment in conserva-
tive management of operable breast cancer: dissection or
radiotherapy? Results of a randomized study with 15 years of
follow-up. J Clin Oncol 22:97–101
43. Chua B, Ung O, Boyages J (2002) Competing considerations in
regional nodal treatment for early breast cancer. Breast J 8:15–22
44. Bevilacqua JL, Kattan MW, Fey JV, Cody HS 3rd, Borgen PI,
Van Zee KJ (2007) Doctor, what are my chances of having a
positive sentinel node? A validated nomogram for risk estima-
tion. J Clin Oncol 25:3670–3679
Breast Cancer Res Treat (2008) 112:523–531 531
123