Embed Size (px)
Citation preview

The National Kidney Foundation’s Kidney Early Evaluation ProgramTM
Essex-Passaic Wellness Coalition March 24, 2014
Ellen H. Yoshiuchi, MPS Division Program Director
National Kidney Foundation Serving Greater New York

Kidney Early Evaluation ProgramTM

10 Year Anniversary

KEEP Objectives
Identify those at risk for CKD using inclusion criteria:
Hypertension and/or Diabetes or family history of
HTN, DM or CKD in first order relatives.
Encourage participants at risk to seek
further medical evaluation.
Develop a referral network, such as free health clinics, for the uninsured identified as being at risk for CKD.
Develop a referral network of specialists for patients identified as being at risk for kidney disease.

KEEP Objectives
• To empower individuals to prevent or delay the onset of CKD or renal failure through education and appropriate disease management!

Chronic Kidney Disease is a Public Health Problem!
Rate of Kidney Disease Jumps by 30%

Chronic Kidney Disease is a Public Health Problem!
The devastating consequences of CKD are End Stage Renal Disease (ESRD),
which requires dialysis or transplantation, or leads to
cardiovascular disease & death.
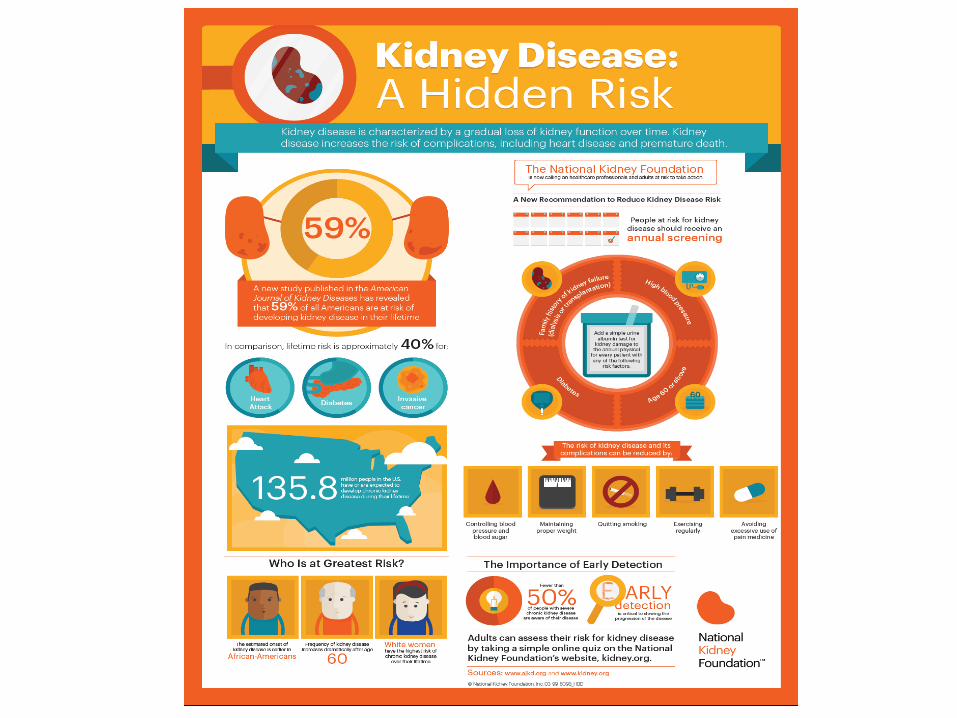
CKD is a Public Health Problem Worldwide!
• Early screening, diagnosis, and treatment should delay or prevent ESRD.
• 26 Million Americans have CKD. Most don’t know it.
• 73 Million Americans have HTN and/or DM.
• CKD is a worldwide public health problem.

KDOQI CKD Evaluation, Classification and Stratification (2002)
• Defined 2 independent criteria for CKD:
• Glomerular filtration rate (GFR) <60 ml/min per 1.73m2 for ≥3 months
• Presence of kidney damage [structural/functional/pathological abnormality; markers (i.e., albuminuria)] for ≥3 months
• Classified CKD by severity according to GFR
• Provided a common language for kidney disease that would:
• Facilitate new research
• Provide clinicians with a stage-specific clinical action plan
• Provide a framework for developing a public health approach toward resolution

KDOQI CKD Evaluation, Classification and Stratification (2002)
Concerns with KDOQI Definition and Classification (2002)
• New information on albuminuria and GFR and their association with mortality has become available since publication of the KDOQI CKD definition and staging.
• Increased recognition of limitations of the CKD definition and classification initiated debate that:
• Reflects changing knowledge
• Provides opportunities for improvement

Definition of CKD Identical to 2002
Classification of CKD
It is recommended that CKD be classified by:
• Cause
• GFR category
• Albuminuria category
• Referred to as “CGA Staging”
Represents a revision of the previous CKD guidelines, which included staging only by level of GFR

New Albuminuria Emphasis
• Most Family Physicians perform some type of office urine test.
• 90% perform a manual urine dipstick test.
• 53% perform an automated dipstick test.
• 58% perform an office-based urine microscopic exam.
American Academy of Family Physicians. Practice Profile II Survey. November 2009

Criteria for CKD
• Glomerular filtration rate (GFR) <60 ml/min/1.73 m2
• GFR is the best overall index of kidney function in health and disease.
• The normal GFR in young adults is approximately 125 ml/min/1.73 m2.
• GFR <15 ml/min/1.73 m2 is defined as kidney failure
• Can be detected by current estimating equations for GFR based on serum creatinine or cystatin C (estimated GFR) but not by serum creatinine or cystatin C alone
• Decreased eGFR can be confirmed by measured GFR, if required



3 Levels of Prevention in CKD
Primary – Prevent the development of CKD in the population at risk with Diabetes and/or Hypertension.
Secondary – Prevent the progression of CKD (loss of kidney function over time) and prevent or delay CKD complications.
Tertiary – Prevent adverse outcomes in those with chronic kidney failure treated with dialysis or kidney transplantation by optimizing care.
Am J Kidney Dis 2009:53:522-535

Conceptual Model of CKD: Continuum of Development,
Progression and Complications of CKD Each Arrow is a Target for Strategies to Improve Outcomes!

Referral to Nephrology by
CKD Stage

Primary Goals of CKD Care
• To prevent the progression of CKD to ESRD
• To prevent Cardiovascular Events & Death
Heart Attacks
Congestive Heart Failure
Sudden Cardiac Death


YOUR KIDNEYS and YOU

Did You Know?
• 1 in 3 American adults is at high risk
for developing kidney disease
• 1 in 9 American adults has kidney
disease and most don’t know it
• Early detection and treatment
can slow or prevent the
progression of kidney disease
• Kidney disease kills over
90,000 Americans every year

What You Will Learn Today
• What kidneys do
• Why kidneys are important
to your health
• What kidney disease is
• Who is at risk
• Actions you can take to
protect your kidneys

KEEP OVERVIEW
• KEEP is a free public health screening program.
• It was initiated in New York City by the National Kidney Foundation in August of 2000.
• Screenings were held in all areas of the US by local National Kidney Foundation divisions or affiliates.
• Over 180,000 people were screened as of 6/30/13.
• Visit www.KEEPonline.org for more information.

Criteria to Participate In KEEP
Anyone age 18 or older with one or more of
the following risk factors:
• History of diabetes
• History of high blood pressure
• Family history in first order relatives of
diabetes, high blood pressure and/or
kidney disease

Six Screening Stations
• Station One – Registration: Participant
receives paperwork packet
• Station Two – Screening Questionnaire &
Informed Consent: Filled out by a
professional volunteer
• Station Three – Physical Measurements:
Height, weight, waist circumference &
blood pressure

Six Screening Stations
• Station Four – Urine & Blood Testing
• Station Five – Clinician Consultation:
Interview with a physician, nurse
practitioner or physician assistant
• Station Six – Screening Review:
Participants receive copy of informed
consent & test results

KEEP Screening Evaluation
• Medical history: DM, HTN, CVD, CKD • Blood pressure • Height and weight • Waist circumference • Body mass index (BMI) • Blood glucose measurement • Serum creatinine • Hemoglobin

KEEP Screening Evaluation
• Albumin to Creatinine Ratio
• eGFR
• A1C for elevated glucose or self-reported diabetes
• Total Cholesterol:
HDL, LDL, Triglycerides
• For eGFR<60 ml/min
Calcium, Phosphorus & PTH
HEMOGLOBIN A1c Not affected by short-term fluctuations in blood
glucose levels Reliable measurement of blood glucose
concentrations over the prior 6 to 8 weeks • <7% of total hemoglobin Normal • > 7% is an indication of increased blood sugar levels High
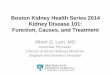
Waist Circumference
High Risk Groups
• Women with a waist circumference of more than 35 inches
• Men with a waist
circumference of more than 40 inches

Blood Pressure Classification KEEP uses the Blood Pressure Classifications according to The 7th National Report Guidelines on
Prevention, Detection, Evaluation & Treatment of High Blood Pressure from the National Heart, Lung
& Blood Institute of the National Institutes of Health, referred to as JNC 7.
BP Classification SBP mmHg DBP mmHg
Normal <120 and <80
Pre-hypertension 120–
139
or 80–89
Stage 1
Hypertension
140–159 or 90–99
Stage 2
Hypertension
>160 or >100
Blood Glucose Guidelines American Diabetes Association (ADA) 2008
Criteria for the Diagnosis of Diabetes Mellitus
Normal Fasting Glucose
FPG <100 mg/dl
Impaired Fasting Glucose
FPG 100–125 mg/dl
Provisional Diagnosis of Diabetes
FPG >126 mg/dl (The diagnosis must be confirmed. The KEEP consultant would recommend follow-up
testing & review by the participant’s primary care provider.)

Follow Up after the Screening
• 2 to 3 days: Participants with critical lab results are called by dedicated bilingual (Spanish/English) staff.
• 3 to 4 weeks: All screening results are mailed to participants and their physicians if participants wish to have their doctor receive a report.
• 2 to 3 months: A follow up survey is mailed out &
participants will be called if the survey is not received.
• 12 months: Invitations are sent by mail, phone or e-mail to attend an annual screening.

KEEP in Greater New York
9 Years/96 Screenings
2/1/2004 to 4/1/2013
• 8175 attended the screenings.
• 7373 met inclusion criteria & completed the screening.
• 2148 were repeat participants.
• Breakdown by gender: Male: 34.98% (2579)
Female: 64.91% (4786)

Of the 5967 who learned of a new problem…
• 3075 learned they may have kidney disease: 41.71%
• 763 learned they may have diabetes:
10.35%
• 861 learned they may have hypertension:
11.68%
• 1268 learned they may have high cholesterol: 17.20%

5461 (74.07%) individuals were aware of a pre-existing condition.
• 433 kidney disease: 5.86%
• 2,967 high cholesterol: 39.40%
• 2,276 diabetes: 30.41%
• 3,961 hypertension: 53.23%

Breakdown by Race & Ethnicity
• African American: 2355 31.94%
• Caucasian: 2062 27.97%
• Asian: 2037 27.63%
• Native American: 76 1.03%
• Pacific Islander: 11 0.15%
• Other: 777 10.54%
• Ethnicity—Hispanic: 1100 14.92%

Breakdown by Age Group
• 18 to 25: 219 (2.97%)
• 26 to 35: 463 (6.28%)
• 36 to 45: 1,035 (14.04%)
• 46 to 55: 1,734 (23.52%)
• 56 to 65: 1,927 (26.14%)
• Over 65: 1,979 (26.84%)
Who is coming to KEEP?
• 6511 (88.31%) have a physician.
• 5282 (71.64%) have health insurance.
• 2719 (36.88%) request that a report be sent to their doctor.
• Of 7274 with reported BMI:
Overweight: 2458 33.79%
Obese: 2490 34.23%

Follow-Up Survey
• 2333 (31.64%) responded!
• Of these, 71.50% reported seeing a physician post-screening.
• Of these, 10.97% had a doctor confirm that they had kidney disease.
• Of these, 90.61% indicated they were willing to participate in another screening.

YOU MAKE IT POSSIBLE. KEEP UP THE GOOD WORK!

CentraState Medical Center September 16, 2011

Trinitas Regional Medical Center October 18, 2011
New Jersey KEEP
Total screened: 1819
1 Nutley
1 Montclair
1 Sparta
1 East Orange
1 Toms River
1 Clifton
1 Paterson

New Jersey KEEP
• 6 Elizabeth • 5 Freehold • 5 Newark • 3 Lakewood

New Jersey KEEP ‘04 through ‘12
• 628 (34.52%) Male
• 1,191 (65.48%) Female
• 461 (25.34%) African-American
• 991 (54.48%) Caucasian
• 155 (8.52%) Asian
• 193 (10.61%) Other Race
• 370 (20.34% ) Hispanic

New Jersey KEEP ‘04 through ‘12
Breakdown of individuals that learned of a new problem:
• 152 (8.36%) learned they may have diabetes.
• 199 (10.94%) learned they may have hypertension.
• 278 (15.28%) learned they may have high cholesterol.
• 694 (38.15%) learned they may have kidney disease.

New Jersey KEEP ‘04 through ‘12
1,668 (91.70%) indicated that they have a doctor. 1,372 (75.43%) indicated that they have insurance. 906 (49.81%) requested that their report be sent to their doctors. 795 (43.71%) responded to the survey. 595 (74.84%) who responded to the follow- up survey reported seeing a doctor.
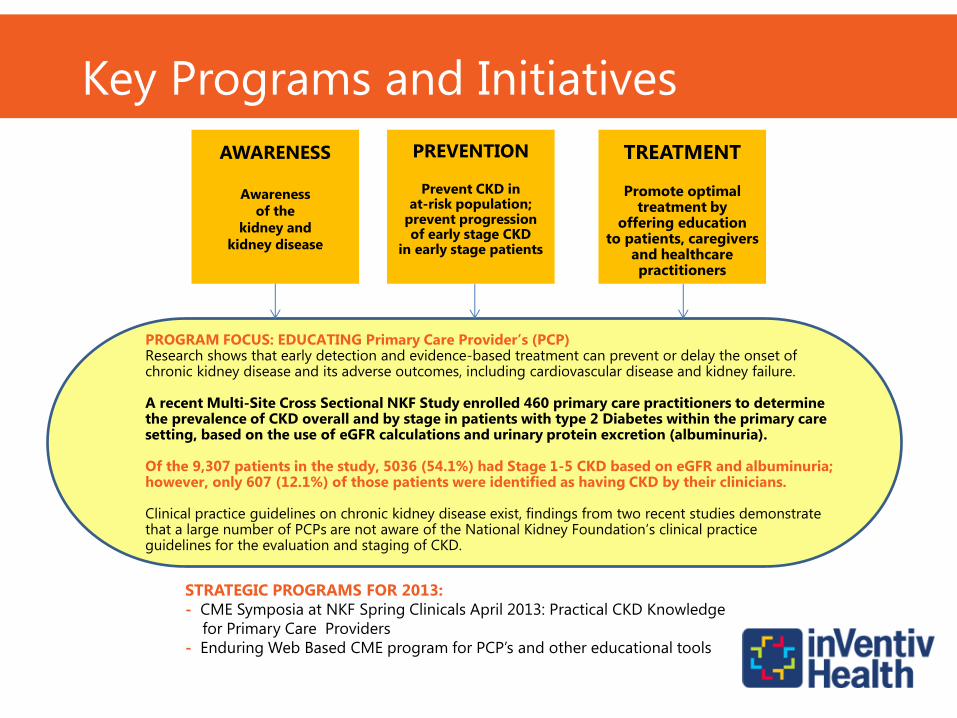
TREATMENT
Promote optimal treatment by
offering education to patients, caregivers
and healthcare practitioners
PREVENTION
Prevent CKD in at-risk population;
prevent progression of early stage CKD
in early stage patients
AWARENESS
Awareness
of the
kidney and
kidney disease
PROGRAM FOCUS: EDUCATING Primary Care Provider’s (PCP) Research shows that early detection and evidence-based treatment can prevent or delay the onset of chronic kidney disease and its adverse outcomes, including cardiovascular disease and kidney failure. A recent Multi-Site Cross Sectional NKF Study enrolled 460 primary care practitioners to determine the prevalence of CKD overall and by stage in patients with type 2 Diabetes within the primary care setting, based on the use of eGFR calculations and urinary protein excretion (albuminuria). Of the 9,307 patients in the study, 5036 (54.1%) had Stage 1-5 CKD based on eGFR and albuminuria; however, only 607 (12.1%) of those patients were identified as having CKD by their clinicians. Clinical practice guidelines on chronic kidney disease exist, findings from two recent studies demonstrate that a large number of PCPs are not aware of the National Kidney Foundation’s clinical practice guidelines for the evaluation and staging of CKD.
Key Programs and Initiatives
STRATEGIC PROGRAMS FOR 2013:
- CME Symposia at NKF Spring Clinicals April 2013: Practical CKD Knowledge
for Primary Care Providers
- Enduring Web Based CME program for PCP’s and other educational tools

KEEP Healthy
• For the general public
• Risk survey
• Height & weight measurement
• Body mass index (BMI)
• Blood pressure check
• Consultation with a clinician
• Over the age of 18

Programs for Patients
NKF Cares
• Patient information help line to answer questions & address concerns
• For any CKD, dialysis or transplant patient
• Staffed daily by social workers & information specialists for the majority of the day
• Toll-free number: 1-855-653-2273

Family Talk
• An informational packet to help patients talk to their families about kidney disease and its connection to diabetes and high blood pressure
• Includes booklets with basic information on CKD, Kidney Risk Quizzes, bracelets and stickers to distribute to the family
Family Talk
The “Family Talk” can take place in several ways:
• Talking one-on-one with family members at risk for CKD in person, via telephone or email
• Having a health discussion together with several family members
• Evaluation forms for patients and the social worker
• Pilot in dialysis centers
• Volunteers trained to go into the community to present “Your Kidneys & You”
• Trained live or via Webinar
• Receive a volunteer training manual, educational materials on kidneys & kidney disease
• Flash drive with presentation slides & training slides
• Documentation includes an agreement letter, sign-in sheets, participant evaluation & presenter evaluation
Kidney Community Educators

World Kidney Day!
• Protect & Prevent on World Kidney Day: Information on the NKF Web site
• Local events at many locations
• 2014 Grand Central Terminal Awareness & Education Event
• 2014 Social Media Campaign on Facebook, Instagram & Twitter

Facebook WKD Campaign

March 14, 2013

World Kidney Day Goes Viral!

Reach
• Reach: The number of people who saw content from our page through various channels.
• Viral Line: The number of unique people who saw a story about our page published by a friend.
• Peak: 229,587 total people reached from 3/9/13- 3/15/13!

Ask the Doctor!
Dr. Leslie Spry, MD, FACP • Are you concerned about yourself, a friend or
family member? Ask away. Dr. Leslie Spry is happy to provide answers to any questions.
• Dr. Spry practices consultative nephrology, is the medical director of the Dialysis Center of Lincoln in Nebraska, & participates in research/innovative projects to benefit dialysis patients.

PEERS Lending Support
For those who want more one-on-one support than a healthcare professional can provide in a brief office visit…
• A telephone-based peer support program
• Connects people who want support with someone who has been there
• Helps people adjust to living with any stage CKD, kidney failure, or a kidney transplant

WELCOME!
Seventh Annual Symposium on
Chronic Kidney Disease:
The Cardiac-Kidney-Diabetes Connection
The Roosevelt Hotel, New York City
April 4, 2014

Free CME Programs
Achieving Better Outcomes for Kidney Transplant Recipients: Optimizing Patient Management
• Available through February 25, 2015
• This web-based interactive virtual patient program will help participants: 1) consider available immunosuppressive therapies for kidney transplant recipients; 2) make optimal clinical decisions based on the needs and comorbidities of their patients; 3) individualize therapy for kidney transplant patients; and 4) provide the necessary patient teaching so that patients are more able to adhere to immunosuppressive regimens.
• Approved for 1.5 continuing education clock hours

What is “Living Well With Kidney Failure?”
• A six-part educational video series
• Created by the National Kidney Foundation to educate patients and their families about kidney failure and its treatment
• An update of the popular “People Like Us” Video series

Materials
• Caddy
• Letter to Clinician
• Leader’s Guide for Healthcare Professionals
• Educational DVD
• Patient Booklets
• Record of Participation