Embed Size (px)
Citation preview

The need for imaging referral guidelines:
Introduction, components, requirements, appropriateness and
decision support
Denis RemediosClinical Radiologist,
Northwick Park Hospital, UK
On behalf of the IAEA

Imaging Referral Guidelines and Clinical Decision Support
Stakeholders• Referrers- medical practitioners, non-medical
professionals• Radiological medical practitioners• Radiographers• Medical physicists• Regulators• Payers• Patients and publicQuestions:• Why?• How?• When?

Why are Referral Guidelines needed?

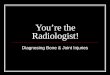
Health expenditure as % of GDP (2007)

0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
Ge
rma
ny
Be
lgiu
m
Sw
itze
rla
nd
Ice
lan
d
Fra
nc
e
No
rwa
y
Sw
ed
en
Ne
the
rla
nd
s
Lit
hu
an
ia
De
nm
ark
Fin
lan
d
UK
Per caput annual collective dose /mSvHart et al. 2010

Guidelines: for whom?
For referring practitioners: General Practitioners, doctors-in-training & non-medically qualified health professionals
For radiology practitioners: ICRP level 2 justification
For patients: reinforcement of advice
For Healthcare organisations: decision support, planning and provision

Levels of evidence for primary research question
Therapeutic studies—investigating the results
of treatment
Prognostic studies—investigating the effect of a patient
characteristic on the outcome of disease
Diagnostic studies—investigating a diagnostic test
Economic and decision analyses—
developing an economic or
decision model
Level I High-quality randomised controlled trial with statistically significant difference or no statistically significant difference but narrow confidence intervals Systematic review1 of level-I randomised controlled trials (and study results were homogeneous2)
High-quality prospective study3 (all patients were enrolled at the same point in their disease with ≥80% follow-up of enrolled patients) Systematic review1 of level-I studies
Testing of previously developed diagnostic criteria in series of consecutive patients (with universally applied reference "gold" standard) Systematic review1 of level-I studies
Sensible costs and alternatives; values obtained from many studies; multiway sensitivity analyses Systematic review1 of level-I studies
Level II Lesser-quality randomised controlled trial (eg, <80% follow-up, no blinding, or imperfect randomisation) Prospective3 comparative study4 Systematic review1 of level-II studies or level-I studies with inconsistent results
Retrospective5 study Untreated controls from a randomised controlled trial Lesser-quality prospective study (e.g., patients enrolled at different points in their disease or <80% follow-up) Systematic review1 of level-II studies
Development of diagnostic criteria on basis of consecutive patients (with universally applied reference "gold" standard) Systematic review1 of level-II studies
Sensible costs and alternatives; values obtained from limited studies; multiway sensitivity analyses Systematic review1 of level-II studies
Level III Case-control study6 Retrospective5 comparative study4 Systematic review1 of level-III studies
Case-control study6 Study of non-consecutive patients (without consistently applied reference "gold" standard) Systematic review1 of level-III studies
Analyses based on limited alternatives and costs; imperfect estimates Systematic review1 of level-III studies
Level IV Case series7 Case series Case-control study Poor reference standard
No sensitivity analyses
Level V Expert opinion Expert opinion Expert opinion Expert opinion

Dose information (from RCR iRefer, 2012)

NHS National Tariff Tariff
(£)Average
(£)Reporting
Fee(£)
MRI, one area, no contrast 154
MRI169*
26
MRI, one area, post contrast only 199
MRI, one area, pre and post contrast only 228
MRI, 2 or 3 areas, no contrast 171
MRI, 2 or 3 areas, with contrast 260
CT, one area, no contrast 105
CT131
24CT, one area, post contrast only 131
CT, one area, pre and post contrast only 152
CT, 2 or 3 areas, no contrast 132
CT, 2 areas with contrast 164
32CT, 3 areas with contrast 176
CT, More than 3 areas 223
Dexa Scans 49 49 13
Contrast fluoroscopy procedures <20 mins room usage 147159 N/A
Contrast fluoroscopy procedures >20 mins and <40 mins room usage 166
Ultrasound, scan 0-15 mins 63 US69
N/AUltrasound, scan > 15 mins 94
Nuclear Medicine Band 1 97
22823
Nuclear Medicine Band 2 151
Nuclear Medicine Band 3 302 64

Criteria for choice of investigations
For a given clinical problem, imaging modalities are listed in the following order:
1. Clinical effectiveness (evidence-based diagnostic/therapeutic impact)
2. Effective dose3. Cost-effectiveness
Essential for uniformity of practice

Clinical practice and clinical referral and imaging referral guidelines
• Clinical practice guidelines (‘guidelines’) are systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances. http://www.nus.edu.sg/irb/Articles/BMJ-Clinical%20Guidelines-Benefits%20and%20Limits.pdf
• Clinical referral guidelines/advice defines, as precisely as possible, the recommendations of the advisory group regarding the situations/conditions that should prompt specialist clinical referral. (from NICE) https://www.nice.org.uk/proxy/?sourceUrl=http%3A%2F%2Fwww.nice.org.uk%2Fmedia%2F94D%2FBE%2FReferraladvice.pdf
• Imaging referral guidelines recommend which imaging investigation is most likely to be helpful for a particular clinical scenario. Advisory not mandatory. (RCR iRefer)

Guidelines for guidelines?Appraisal of Guidelines for Research and Evaluation (AGREE) http://www.agreetrust.org/
AGREE Instrument :
1. assesses the quality of guidelines; 2. provides a methodological strategy for the
development of guidelines; 3. informs what information and how information
ought to be reported in guidelines.
Guidelines can play an important role in health policy formation and have evolved to cover topics across the health care continuum (e.g. screening, diagnosis).
Browman et al. Healthc Pap. 2003;3 http://www.ncbi.nlm.nih.gov/pubmed/12811083

Use of Appraisal of Guidelines for Research and Evaluation (AGREE) Instrument http://www.agreetrust.org/
• health care providers before adopting its recommendations into their practice;
• guideline developers to follow a structured and rigorous development methodology, to conduct an internal assessment to ensure that their guidelines are sound, or to evaluate guidelines from other groups for potential adaptation to their own context;
• policy makers to decide which guidelines could be recommended for practice or to inform policy decisions;
• educators to help enhance critical appraisal skills amongst health professionals and to teach core competencies in guideline development and reporting.

Making the best use of clinical radiology
The Royal College of Radiologists has published guidelines for 25 years since 1989. NHS Evidence accreditation for 7th edition (2012).

Guidelines App for smartphones and tablets

RCR iRefer App distribution • Europe: UK, Ireland, France, Norway,
Sweden, Belgium, Denmark, Portugal, Spain, Switzerland, Germany, Slovakia, Netherlands, Italy, Israel
• Western Pacific: Australia, New Zealand, Singapore, Hong Kong
• Eastern Mediterranean: UAE, Kuwait, Saudi Arabia
• Africa: South Africa• Americas: Brazil

Who should justify?
Radiological medical practitionerReferring medical practitioner(In consultation with the patient for complex or high
dose procedures)For asymptomatic individuals, justification by Health
Authority and Professional Body

Transfer of responsibility or delegation?
Responsibility for justification • lies ultimately or largely with the radiological
medical practitioner who may be a cardiologist etc.
• may be transferred to another medical practitioner eg in isolated, small facilities without a radiologist
Task of justification occasionally delegated to the radiographer for low dose procedures or those within an agreed pathway eg CT for stroke. Responsibility remains with the radiologist.

Adopting and adapting referral guidelines
• Adopting validated referral guidelines is a rapid process for implementation
• Adapting allows local issues to be incorporatedCurrent version of RCR Referral Guidelines adopted
by:CroatiaIrelandJapanRussia(Malaysia)
Over 20 years , adopted and adapted by >16 countries and 1 region (Europe)
Mostly adopted and translated without adaptation

ACR Appropriateness Criteriahttps://acsearch.acr.org/docs/69483/Narrative/

Similarities between ACR and RCR referral criteriaFeatures ACR RCR
Evidence-based + +
Based on common clinical problems
159 (800 var.) 315
Cycle of review 1 yr selective 4 yrs
Expert Panels 18 16
Consensus Technique Delphi Delphi
Level of agreement for consensus
80% 75%
Involvement of other organisations
15 through consensus
100 through consultation
Dose information Rel. radiation level (= ED)
Effective dose (ED)
Publication Web, Clinical Decision Support
Paper, App and restricted web

Western Australia HA: Diagnostic Imaging Pathwayshttp://www.imagingpathways.health.wa.gov.au/index.php/imaging-pathways/musculoskeletal-trauma/musculoskeletal/low-back-pain?tab=redflags#pathway

Canadian Association of Radiologists: adopt, adapt and translate http://www.car.ca/uploads/standards%20guidelines/car-fr-referralguidelines-d-20121011.pdf

Austrian Referral Guidelines: adopt and translate http://orientierungshilfe.vbdo.at/

EC Referral Guidelines 2000

articlestoryarticlestory Europe: EuroSafe Imaging Campaign. Collaborative efforts for Radiation Protection

USA Guidance for appropriate imaginghttp://www.acr.org/Quality-Safety/Appropriateness-Criteria

USA: Guidelines and clinical decision support

ACR- Clinical Decision Support

Clinical decision support for imaging referral guidelines in Europe ESR iGuide

Radiology, http://pubs.rsna.org/doi/abs/10.1148/radiol.2511081174
Christopher L. Sistrom; Pragya A. Dang; Jeffrey B. Weilburg; Keith J. Dreyer; Daniel I. Rosenthal; James H. Thrall; Radiology 2009, 251, 147-155.DOI: 10.1148/radiol.2511081174© RSNA, 2009
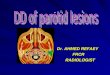
CT requests with Clinical Decision Support

Targeted CDS can reduce utilisation of lumbar MRI, head MRI and sinus CT.

Rand: MID report for Imaging and CDS 2014 http://www.rand.org/content/dam/rand/pubs/research_reports/RR700/RR706/RAND_RR706.pdf

Rand: MID report for Imaging and CDS http://www.rand.org/content/dam/rand/pubs/research_reports/RR700/RR706/RAND_RR706.pdf
Uptake“Approximately two-thirds of clinicians in the sample placed fewer than 20 orders”
Reduction in utilisation“largest decrease in the percentage of rated orders was for orders for CT and MRI of the lumbar spine, which decreased by 8 and 15%”. Overall 5%.
Coverage“percentage of orders that were successfully rated by DSSs ranged from as little as 17 percent for Convener D to a high of 58 percent for Convener A” Average c. 30%.

USA: Protecting Access to Medicare Act 2014
The bill sought to authorize a short-term Medicare SGR patch that extends authorization for physician reimbursement under Medicare under current law through March 31, 2015. The bill prevents a scheduled 24 percent reduction in Medicare physician reimbursement rates.
It also mandates that starting January 1, 2017, physicians ordering advanced diagnostic imaging exams (CT, MRI, nuclear medicine and PET) must consult government- approved, evidence-based appropriate-use criteria, namely through a CDS system. Physicians furnishing advanced imaging services will only be paid if claims for reimbursement confirm that the appropriate-use criteria was consulted, which CDS mechanism was used, and whether the exam ordered adhered or did not adhere to an acceptable CDS rating. It’s important to note that physicians ordering advanced diagnostic imaging services do not have to adhere to the appropriate-use criteria; however, they must confirm that the guidelines have been consulted.
Consultation of appropriate-use criteria is required prior to the ordering of advanced diagnostic imaging services in the physician office, hospital outpatient, and emergency department settings. Exams for inpatients and emergency services as defined under the Emergency Medical Treatment and Active Labor Act (EMTALA) will be exempt. Hardship exclusions, such as a lack of access to high speed Internet, will be allowed, presumably on a case-by-case basis.
The U.S. Department of Health and Human Services (HHS) through CMS is authorized to deem various accepted appropriate-use criteria by November 15, 2015.

Canadian Association of RadiologistsManitoba Demonstration Project in Physician Demand-Side Control forDiagnostic Imaginghttp://www.car.ca/uploads/about/manitoba%20i%20project_final%20report.pdf

Manitoba Demonstration Project: Why Such Limited Impact?
Low impact (5% accept rate) could be the result of several factors:
1. Insufficient guideline coverage of actual practice
• Would additional guidelines increase impact?
2. Good existing DI appropriateness at demonstration site
• Would guidelines be more useful for generalists (e.g. family
practitioners) rather than specialists?
3. Need for stronger clinical engagement about DI appropriateness
• Would more attention to demonstrating the “need” for guideline
adherence, influencing physician knowledge and attitudes lead
to more practice change?
4. Timing of advice
• Was this intervention placed “too late” in decision-making
process (after physician commitment to a course of action)?

Australia & New Zealand: Inclusive approach to imaging guidelines and decision support

UAE: Suggestions for next stepsIAEA Workshop on Patient Referral Guidelines, Sept. 2014
1. Adopt and adapt Imaging Referral Guidelines for use in the UAE
2. Encourage Clinician Champions to promote guideline introduction & use
3. Governmental endorsement and support for guideline availability & use
4. Educational initiatives for medical under-graduates & doctors in training, also CPD*
5. Clinical audit facilitation and training for monitoring guideline availability and use

Collaboration of Portuguese-speaking countries

Afrosafe campaign 2015AFROSAFE’s main objective is to address issues arising from radiation protection in medicine in Africa. This campaign is based on the Bonn Call-for-Action, 2013. The vision of AFROSAFE is: All radiation-based medical procedures in Africa appropriate and safely performed. AFROSAFE plans to achieve its goals through supporting adherence to policies, strategies and activities for the promotion of radiation safety.

Imaging referral guidelines: areas for consideration to help local implementation
• Imaging referral guidelines- what is available• Format- tabular or flow chart algorithm• Media- print copy, web-based, app-based for
tablets/smart phones, clinical decision support CDS• Barriers• Monitoring- audit, workflow, regulatory inspection• Tools for implementation- awareness campaigns,
education, CDS• Long term goals- reduced utilisation, effective
diagnostics, radiation safety culture, collective corporate responsibility for safety

Monitoring of guideline use in workflow
1. Clinic-radiological meetings (MDT meetings)Can influence:
i. Future imaging choices in the individual case
ii. Imaging referral behaviour.2. Educational messages in reports esp. to GPs
Sustained 20% reduction in referral possible “Lumbar imaging for low back pain without suggestion of serious underlying conditions does not improve clinical outcomes. See M04 http://www.rcr.ac.uk:2059/adult/#Tpc151
http://www.nice.org.uk/guidance/CG88/chapter/1-Guidance ”
3. Through CDS- dashboard can give ratings of appropriateness

Metrics esp. for Economic benefit?
Value of test not the same as the cost
Benefit to a health organisation within the constraints of resources
Essential to measure outcome for clinical guidance & patient protocols
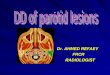
6. Societal benefit
5. Patient outcome
4. Therapeutic i
mpact
3. Diagnostic i
mpact
2. Diagnostic efficacy
1. Technical efficacy
The efficacy of diagnostic imagingFryback and Thornbury Med
Decis Making 1991;11:88 http://www.ncbi.nlm.nih.gov/pubmed/1907710

Evidence for referral guidelinesFollowing RCR guidelines, overall referrals fell
13% BMJ. 1993 Jan 9;306(6870):110-1
RCGP Randomised controlled trial showed fewer referrals and better conformance Oakeshott, Kerry, Williams. Br J Gen Pract. 1994 Sep;44:427-8.
Randomised trial with an educational reminder messages in reports is effective in reduction by up to 20% & does not affect quality of referrals. Eccles , Steen , Grimshaw , Thomas , McNamee , Soutter, Wilsdon , Matowe , Needham , Gilbert. The Lancet, 2001; 357: 1406 – 1409.
Over 12 consecutive months no evidence of the effect of the intervention wearing off Ramsay, Eccles, Grimshaw, Steen. Clin Radiol. 2003 Apr;58(4):319-21
Emerging evidence to show 2-20% improvement in conformance with clinical decision support tools.

Imaging Referral Guidelines: needs, components and clinical decision support
1. Awareness of value of appropriate imaging… referrers and patients
2. Adopting and adapting of guidelines to facilitate appropriate imaging
3. CDS in workflow simple & effective4. Clinical audit for monitoring,
identifying outliers, & feedback… Awareness, appropriateness & audit