Embed Size (px)
Citation preview

1
INTRODUCTION
In the past, athletes who suffered a hit to the head during an athletic event were told to
“shake it off” and get back out there. Today, this would not be the case. Thousands of athletes
around the world, participating in various athletic events all suffer from a common injury. Unlike
a broken bone that can fully heal within months, the side effects of a concussion, both short and
long-term, can have a serious impact on an athlete’s future, and have high potential to
permanently end one’s career. Concussions are a constant, high-risk threat to athletes across the
sporting world, especially athletes in high contact sports such as football and hockey, where the
risk of head injury is increased due to the nature of the game. Although the concern for
concussions in today’s world of sports is much greater than it was 25 years ago, Cusimano’s
(2009) research suggests that still, a significant number of players and adults do not know what a
concussion is or how it occurs. She states that approximately one-quarter of adults, and ¼ to ½ of
young athletes who were surveyed could only recall one symptom of a concussion (Cusimano,
2009). Additionally, Cusimano (2009) found that ¼ of these athletes did not know if a player
experiencing symptoms of a concussion should forego participation. Without the most basic
understanding of concussions, one cannot possibly begin to fathom the serious impacts this
injury can have on one’s life.
To begin understanding the neuroanatomy and physiology of a concussion, one must first
grasp a basic understanding of the injury itself. According to the American Association of
Neurological Surgeons (2005) a concussion is “a clinical syndrome characterized by immediate
and transient alteration in brain function, including alteration of mental status and level of
consciousness, resulting from mechanical force or trauma.” In a more general sense, one may
describe a concussion as the brain hitting rigid areas of the skull violently, thus impairing normal

2
brain function. King (2003) states that post-concussion symptoms include, but are not limited to,
headache, dizziness, fatigue, poor memory and/or concentration, irritability, depression, sleep
disturbance, nausea, and potentially loss of consciousness. Research completed over the past two
decades has provided illustrations of the physical damage concussions have on the brain that can
lead to the risk of developing neurodegenerative disorders later in life.
REVIEW OF LITERATURE
Post-Concussive Pathophysiology
A cerebral concussion is not as simple as being described as a blow to the head that
causes the brain to hit off the projections of the skull, causing “bruising” to the brain that
requires time to heal. Although the previous statement has some validity, it does not accurately
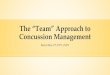
describe the neurometabolic cascade of a concussion. In 2001 Giza determined that immediately
following the impact to the head, an abrupt, involuntary release of neurotransmitters and ion
influxes occur. Glutamate, the main excitatory
neurotransmitter of the brain, is released in
large quantities, which essentially causes the
brain to overwork. The excessive increase in
glutamate concentration drives the Sodium-
Potassium Pump (Na+/K+ pump) to activate,
thus releasing potassium, and bringing more
sodium into the cell; a process that leads to increased neuronal depolarization (Giza, 2001).
Increased neuronal depolarization will offset the normal ranges of ionic concentrations,
membrane potential of cells, and permeability of ions in which the brain typically functions. The
Na+/K+ pump is a primary example of a pump that uses active transport; meaning this pump
Figure1.TheDisruptionofIonConcentration,andNeurotransmitterReleaseintheBrainImmediatelyFollowingaConcussion.

3
requires adenosine triphosphate (ATP) in order to function. Due to the sudden increase of
glutamate in the brain, there is a high demand on this pump, which results in the immediate
demand for a large supply of energy. How does the brain attain this much ATP with such short
notice? By reducing glutamate into glutamine and ATP (using glutamine synthase), the Na+/K+
pump is able to function. However, this does not occur without harm to the brain.
Giza’s research shows that after this initial period of hyperactivity and excess
neurotransmitter release comes a period of “depressed metabolism” (Giza, 2003). He found that
this cascade of events creates a severe energy crisis in the brain, which can lead to cell death and
impairment of neuronal connectivity (Giza, 2003). It is this impairment of neuronal function that
can lead to the loss of consciousness, blurred vision, and imbalance associated with traumatic
brain injury (Powell, 2001). Although these neuronal changes occur at the time of impact to the
head, they are unfortunately commonly accompanied by the later onset of additional life-
threatening changes in the brain. After the impact of the brain on the skull, the brain becomes
susceptible to bruising, torn blood vessels and nerve fibers damage (Frost, 2011). If any of these
sequelae occur, the individual suffering from a concussion may also be at a high risk for
developing a cerebral hemorrhage and/or elevated intracranial pressure as a result of cerebral
edema; very commonly characterized by prolonged suffering of concussion symptoms. As the
brain swells after impact with the skull, blood flow becomes more limited due to the brain and
blood vessels becoming compressed (Frost, 2011).
During this phase of the metabolic cascade of a concussion, the injured individual must
be extremely cautious that they do not suffer another blow to the head. If this were to occur,
cerebral edema could further increase, preventing oxygen and glucose reaching the brain, thus
having potential to prevent adequate blood supply to reach the brain, resulting in a stroke (Frost,

4
2011). If the concussed individual were to go back into competition before adequate healing time
was given the athlete could be at elevated risk to develop second impact syndrome. Second
impact syndrome is a rare condition in which a second concussion occurs before the first
concussion has properly healed. This results in rapid and severe cerebral edema, typically
resulting in sudden death. While it is true that many concussion symptoms fade within a few
days, it is extremely important to understand that if a second concussion occurs within the first
days or weeks after the initial concussion, the risk of developing second impact syndrome is very
high. Thus, caution needs to be taken post-injury in order to ensure the best possible healing of
the brain.
Physiological Damage
One of the hardest components of concussions to understand in the past was determining
the specific areas of the brain that are damaged when one suffers a traumatic brain injury (TBI).
The discussion and interest in sports related concussions received minimal attention until the
1990s, and since then it has been an ever-growing area of
concern in the world of sports and science. Perhaps the
reasoning behind this prior ignorance is that the actual damage
of a concussion cannot be seen like a broken arm; it is much
harder to determine the extent of a brain injury than it is a
broken bone or torn muscle. Although it was once thought that
a concussion was simply a temporary disturbance of
function without long-term consequences, it is now fully
understood that irreversible structural changes in the brain do occur (Jantzen, 2004). More
specifically, research completed by Kelly Jantzen (2004) had a strong focus on the functional
Figure2.BrainActivationinConcussedSubject(left)andControlSubject(right).

5
Magnetic Resonance Imaging (fMRI) differences between healthy and previously concussed
participants. Referring to Figure 1, Jantzen (2004) found that athletes who had suffered a
concussion during their season showed an increase in activation while being asked to perform a
bimanual sequencing task. While comparing those fMRI images of concussed individuals to the
control, it was determined that although non-concussed participants showed an increase in
activation of brain sites, the increase in concussed participants was significantly greater (Jantzen,
2004). The increases in brain activation in concussed participants were in regions that are
associated with executive functioning, including working memory and motor planning;
suggesting that it took concussed individuals more effort to properly execute the sequencing task
than it did the non-concussed participants (Jantzen, 2004). Jantzen’s reasoning for this increase
in activation in post-concussive participants is the axonal damage caused by concussions. Axonal
damage is thought to reduce the efficiency of processing in the brain once it suffers from a
concussion, meaning more neuronal resources are required to carry out the same function as a
healthy brain (Jantzen, 2004). The functional Magnetic Resonance Images produced showed
significant increase in activity in the medial frontal gyrus, inferior parietal lobe, and the bilateral
cerebellum (Jantzen, 2004). The functions of the parietal lobe include, but are not limited to:
working memory, storage and manipulation of numerical information. Additionally, the
cerebellum is significantly involved in preparing for, and carrying out complex motor
movements, as well as the timing of these tasks. As seen in the fMRI concussive forces damaged
these two areas of the brain, and thus the somatosensory cortex (in the parietal lobe) and the
cerebellum must create new pathways in order to carry out normal function.
The concern surrounding delayed, interrupted and/or excess brain activation and
sequencing has increased in recent years as evidenced by recent studies that show

6
neurophysiological changes in the brain after suffering from (a) concussion(s). In 2015, Coughlin
et al conducted a study on several National Football League players who had suffered several
concussions, specifically looking at the pathologic changes that produce chronic traumatic
encephalopathy (CTE). CTE, a
progressive degenerative disease of the
brain commonly found in athletes, raises
concern as researchers have found a
significant link between CTE and
neuropsychiatric consequences including
cognitive decline, mood and anxiety
orders (Coughlin et al, 2015). Similar to
the study completed by Jantzen in 2004, Coughlin et al (2015) also found changes in the medial
temporal, and parietal lobe structures, as well as cognitive deficits such as verbal learning and
memory. While analyzing functional Magnetic Resonance Images of the NFL players in
comparison to those of healthy controls, researcher’s observed a very significant difference, that
would later impact the development of neuropsychiatric problems (Coughlin et al, 2015). Images
showed that the translocator protein (TPSO), a marker of brain injury and repair, had an
increased amount of [11C] DPA-713 binding (Figure 2.) in the brain, which lead Coughlin and
her team (2015) to infer that the brain never truly heals after suffering from a concussion. Rather
than healing as a typical bone or muscle injury would, research shows that the neuroanatomical
damage caused by a concussion seldom reverses itself and heals back to 100% function (Iverson,
2012). This lack of healing can be seen in both short and long term examples of patients
suffering from mild head traumas. For example, Nigel King (2003) found diffuse microscopic
Figure3.Comparison of [11C]DPA-713 Binding in the Brains of Healthy Elderly Controls and Former NFL Players.

7
axonal injury in post mortem exams in patients who had suffered only one mild head injury.
Additionally, King (2003) states that within the first few weeks of injury, an MRI scan can show
cellular damage and metabolic abnormalities in various areas of the brain. The studies of King
and Iverson both suggest that more than just physical damage to the brain occurs during a
concussion, and that a great amount of evidence supports the idea that organic features, such as
diffuse microscopic axonal injury and abnormal cerebral blood flow, play a large role in the
neurophysical impairment of the brain post-concussion.
Short-Term Effects
Although medical professionals better understand many of the common short-term
symptoms of concussions, the importance of ensuring that adequate recovery time is given is of
utmost importance today in sports. As King (2003) stated, these post concussion symptoms
include headache, fatigue, poor memory and/or concentration, irritability, depression, sleep
disturbance, nausea and potentially loss of consciousness. Although it is most common that
many of these symptoms are present immediately after the time of impact, other symptoms may
take longer for the individual to fully notice (King, 2003). Each year, approximately 1.2 million
Americans report suffering from a head injury, and although the majority of these are classified
as mild traumatic brain injuries (MTBI), many people resume activity much too quickly and
jeopardize their own long-term health. Being that glucose is the main excitatory neurotransmitter
in the brain, this results in a lack of activation in many cortical pathways that develop our motor
movements and cognitive thinking abilities. More specifically, Giza et al (2001) found that
cerebral glucose is completely diminished by 24 hours after injury, and remains significantly low
for 5 to 10 days (in experimental animals).

8
The timeline of recovery for concussions must be assessed in regards to individual cases,
as recovery time strongly depends on several factors: the force of impact to the head, the prior
health of the individual, and history of previous concussions. For the majority, concussion
symptoms will subside within 7-10 days, however others are not so lucky. If the symptoms of a
concussion have not subsided within 10 days after the injury, the patient may be diagnosed with
Post Concussion Syndrome (PCS) (White, 2012). Patients with PCS may not continue to
experience all symptoms after 10 days, but generally experience severe headaches, dizziness and
irritability for weeks or months post-injury (White, 2012). The next level of damage is described
as having serious neurological deficits; severe brain swelling, bleeding in the brain, repeated
seizures and/or coma are common symptoms (White, 2012). Again, dependent on several factors,
these symptoms may be experienced up until one year post-injury for the patient to still be
classified as suffering from serious neurological deficits. Lastly, Chronic Traumatic
Encephalopathy (CTE) is a neurological disorder that is prevalent in individuals who have
suffered from multiple concussions. This neurological disorder may develop years to decades
after one’s last concussion, but can potentially have a serious impact on one’s quality of life.
Repeated concussions are the biggest worry for researchers today, as many individuals continue
to return to sport after suffering from one or more head injuries; a decision that may seem
acceptable at the time, but that one may regret in their later years of life.
Long-Term Effects- Neurological Disorders
Although more difficult to imagine, the real consequences of repeated concussions are
not usually experienced until ten to twenty years after the impact. The damage occurring to the
brain has a permanent impact on one’s neurological function, and with decreased function comes
the risk of developing several early-onset neurological disorders. Recent studies have shown a

9
correlation between TBI and chronic depression, with prevalence rates from 6% (mild TBI) to
77% (more severe TBI) (Guskiewicz, 2006). Although the studies of Guskiewicz et al (2006)
focused on World War II veterans, the concept of injury to the brain is still very relevant to the
world of sports. After accounting for several other possible causes for depression, Guskiewicz et
al (2006) discovered that there was an 18.5% lifetime prevalence of depression in individuals
who had suffered a head injury, versus the observed 13.4% lifetime prevalence for those with no
history of head injury. Applying these statistics to the world of sports, it can be simply stated that
repeated concussions permanently alter one’s brain function over time, and have the potential to
be a key risk factor in developing chronic depression later in one’s life.
Suffering from a Traumatic Brain Injury (TBI) opens up a new spectrum of possible
pathologic injuries if one continues to put
themselves in situations that make them
susceptible to repeated concussions. TBI,
causing diffuse axonal injury, mechanical tissue
damage, and neuronal dysfunction can quickly
become Mild Repetitive TBI or Severe TBI if
patients continue to re-injure the same areas of
their cortex (DeKosky et al, 2010). Figure 3
illustrates the progression of Traumatic Brain
Injury into later-onset, chronic
neurodegenerative disorders of the brain caused
by repeated concussions. As illustrated in this
diagram, Mild Repetitive TBI and Severe TBI both have a positive correlation for resulting in
Figure4.Spectrum of Pathologic Features and Outcomes of Traumatic Brain Injury

10
Dementia Pugilistica, CTE, Parkinson’s disease, and Alzheimer’s Disease- all of which are
classified as neurological disorders. Through research completed on human subjects, DeKosky et
al (2010) discovered that 20 to 30% of patients with Alzheimer’s or Parkinson’s disease have
suffered a single-incident traumatic brain injury, a statistic that is true in only 8 to 10% of the
control subjects. In an additional study completed by Hazrati et al (2013), researchers studied
post-mortem brains of six retired Canadian Football League players who all had history of
multiple concussions and significant neurological decline. Results showed all six subjects having
progressive cognitive decline prior to death, but the neuropathological findings varied (Hazrati et
al, 2013). Within the group of 6 participants Hazrati et al found three individual cases of
Alzheimer’s disease, a single case of Amyotrophic Lateral Sclerosis (ALS), and one case of
Parkinson’s disease. In addition to these findings, Hazrati et al also found that 50% of patients
showed post-mortem findings consistent with CTE. Since CTE can only definitively be
diagnosed in post-mortem autopsies, it is very important for researchers to document the cases in
which CTE correlates with multiple concussions. Symptoms of this neuropathological disorder
include memory loss, confusion, impaired judgment, impulse control problems, depression, and
eventually dementia (Hazrati et al, 2013). Hazrati’s research suggests that CTE is a disorder that
correlates to the onset of Alzheimer’s as each patient in this study that had CTE, also reported to
have many symptoms of this disease as well.
Alzheimer’s disease, a neurological disorder linked to severe traumatic brain injuries, is
another example of the long-term effects concussions may have on one’s life. Rudelli’s research
completed in 1982 was of the earliest to speculate that trauma to the head could potentially play
a provocative role in the alteration of neuroanatomy. These studies suggested that dementia may
be attributed to brain contusions formed following head injury as a result of a cerebral edema or

11
swelling (Rudelli, 1982). More recent studies, such as that of Lehman et al (2012), have
analyzed the prevalence of neurodegenerative disorders such as Alzheimer’s, Parkinson’s and
ALS. These studies found that the prevalence of death caused by neurodegenerative disorders is
3 times greater in a concussed population than that of the general US population, and that for
Alzheimer’s and ALS it is 4 times higher (Lehman et al, 2012). These results are consistent with
the physical damages that were previously discussed, in that the degeneration of cortical neurons
and disruption of neuronal pathways are what lead to these neurodegenerative disorders. With
more concussions one suffers the loss of more cortical neurons, decreasing the efficiency of the
brain and thus contributing to the generation of these neurodegenerative disorders. In 2009, de
Beaumont and his team of researchers assessed the cognitive abilities and electrophysiological
functions of former athletes with no history of sports concussion, and of former athletes who
sustained their last sports concussion over 30 years ago. In their research, it was found that those
who had sustained a concussion showed similar cognitive and motor system deficits as
asymptomatic individuals who were tested at three years post-concussion (de Beaumont et al,
2009). This aspect of the study agrees with previous statements arguing that the physical
alterations of the brain caused by concussions never fully regenerate and recover, and that
multiple concussions only worsen these problems. In addition to this, de Beaumont et al (2009),
found the previously concussed subjects showed significant reductions on both
neuropsychological and electrophysiological measures of episodic memory, and functions of the
frontal lobe; both of which are known as factors contributing to early-onset Alzheimer’s disease.
From the time an individual suffers a strong enough impact to the head, the
neurometabolic cascade of a concussion begins. Once the brain comes into contact with the skull,
the involuntary release of sodium, potassium and calcium ions, as well as glutamate begins. This

12
sudden influx results in increased neuronal depolarization, which is what kick-starts the period of
depressed metabolism. During the initial days of a concussion, this depressed period is when
symptoms are at highest prevalence, and brain function is at its worst. As the brain heals itself, it
is important for patients to refrain from physical activity, bright light, and other stimuli that
cause a change in the chemical makeup of the brain. Finally, the brain will never be able to fully
recover from the damage it suffered, and therefore new pathways must be formed that require
more energy than before. Although the brain is a very strong, resilient and powerful organ, the
neuroanatomical damage suffered during a concussion is impossible to fully heal, which can lead
to the development of several very serious neurological disorders.
Summary
The previous research was combined and presented in order to give a detailed outline of
the neurometabolic cascade of a concussion, and how that cascade may still affect individuals far
into the future. The resources used to compile this literature review were organized in a fashion
that allowed the timeline of events in a concussion to be followed chronologically, ending with
arguably one of the largest areas of focus for researchers today. Research included was used to
provide various perspectives on concussions in sport, ranging from history of the injury through
the neurological disorders associated with TBI. This approach was used to highlight the
important neurometabolic features of a concussion that are relevant to the development of these
neurological disorders.
DISCUSSION
Only 30 years ago, athletes who suffered a blow to the head in a contact sport were
expected to shake it off and be back in the lineup for the next game, if not the next shift. For
years concussions went undiagnosed, untreated and individuals did not take the time off to allow

13
for proper healing. Spectators at the highest level of sports events watched as athletes
continuously beat up their bodies, but rarely wondered about what effect these injuries had on
athletes’ cognitive abilities; because to them, these people were solely athletes. Today, that
mentality has changed for the better. There are more rules in high contact sports that attempt to
reduce the number of head injuries in sport, due in large part to the fact that today we understand
that concussions are not just a temporary injury, rather they are and injury that will one will
never be able to fully recover from.
According to ESPN, there are over 21.5 million kids between the ages of 6 and 17
playing a team sport in America alone. With contact sports being some of the most popular for
young children to participate in, the focus on concussion prevention a young age is of the utmost
importance. Although research completed by McCrory in 2004 proves that children are more
resilient to traumatic brain injuries than adults are, the most common cognitive sequencing of
concussive injuries is the same. Additionally, concussions also have the potential to affect a
child’s social, and educational success- processes critical throughout both childhood and
adolescence (McCrory, 2004). A child being more resilient to concussions than an adult means
that it takes a larger impact to a child’s head to produce the same neurological effects as an adult
who suffered a less forceful blow to the head. More specifically, McCrory (2004) found that “it
takes a two to three fold greater impact force to produce clinical symptoms in children compared
to adults.” This means that when a child shows symptoms of a concussion, it is reasonable to
assume that they sustained a far greater impact force in comparison to an adult showing the same
post-concussive symptoms (McCrory, 2004). Although the resilience of a child’s brain is
beneficial, it is still important that society takes control of these risks to help reduce the number
of brain injuries in the future of sport.

14
Though many of the results in literature cannot confidently conclude that there is a
definitive correlation between multiple concussions and early on-set neurological disorders, a
definite trend towards significance can be inferred. Results from these studies provide a
provocative body of material that suggests the protocol for concussion assessment and
management still may not be as developed as it should be in sports. If a history of repeated
concussions has been shown in patients with Alzheimer’s disease, Parkinson’s disease, as well as
other neurological disorders, then why are athletes allowed to choose to return to play after their
3rd and 4th concussions?
Practical Application
As previously stated, the fact that athletes who have suffered from multiple concussions
in their careers are still allowed to participate in high contact sports is astonishing, and creates a
greater risk for life threatening diseases with advancing age. A large issue with this is that the
research is not made available, and/or understandable to the right people. There is only so much
that scientists can do to make this information available and understandable to the affected
groups that include athletes, coaches, and parents. That being said, doctors, physical therapists,
and athletic trainers are trained to their best ability to detect, prevent and help concussion
recovery. However, it is up to the athletes themselves to decide their own future. Perhaps with
the appropriate guidance from qualified medical professionals, the important conclusions of
these studies could be presented to athletes who participate in high contact sports. By giving
athletes, coaches and parents this reliable information one can only hope that people would
become more aware of the risk they are taking when going back to their sport after already
having suffered from multiple concussions. Additionally, athletes educated on the long-term
effects of concussions would be more aware of how an illegal head check to another player could

15
have potential to severely change his/her life in the future. The neurometabolic cascade of a
concussion is initiated at the time of impact, and although the human brain is arguably the most
powerful mechanism in the world, it is impossible to use to it’s full potential when circuitry is
being disrupted and cerebral edemas are being formed. Many scientists have proven the
provocative role that concussions have on long-term neuroanatomical alteration, but it is not until
society understands this that the world of sports will then be forced to rethink the need for high
contact in athletics. At the end of the day, society needs to decide if seeing replays of big hits is
more important than an athletes mental health and quality of life 20 years later; and if one does
not choose the later option, this is an issue that will never be resolved.

16
BIBLIOGRAPHY
Coughlin,J.M.etal(2015).NeuroinflammationandBrainAtrophyinFormerNFL Players:AninvivoMultimodalImagingPilotStudy.NeurobiologyofDisease,74,58- 65.http://ac.els-cdn.com/S0969996114003325/1-s2.0- S0969996114003325-main.pdf?_tid=f576a062-75f7-11e5-a34a- 00000aab0f27&acdnat=1445214534_9773418293812cafeb298bf6820edc4 7Cusimano,M.D.,ChipmanM.L.Volpe,R.,Donnelly,P(2009).CanadianMinorHockey Participants’KnowledgeaboutConcussion.TheCanadianJournalof NeurologicalSciences,36(03),315-320. http://journals.cambridge.org/download.php?file=%2FCJN%2FCJN36_03%2 FS0317167100007046a.pdf&code=085ea5e64672c161d36eebf438633b36 DeBeaumont,L.,etal(2009).BrainFunctionDeclineinHealthyRetiredAthleteswho SustainedtheirLastSportsConcussioninEarlyAdultgood.Brain:AJournalof Neurology.132.695-708. http://brain.oxfordjournals.org/content/132/3/695.shortDeKosky,S.T.,etal(2010).TraumaticBraininjury-Football,WarefareandLong- TermEffects.TheNewEnglandJournalofMedicine,363,1293-1296. http://www.nejm.org/doi/full/10.1056/NEJMp1007051Frost,C(2011).AnatomyoftheConcussion:MoreSeriousthanMeetstheEye? https://honors.usf.edu/documents/Thesis/U78133303.pdf
Giza,C.C.,etal(2001).TheNeurometabolicCascadeofConcussions.Journalof AthleticTraining,36(3),228-235. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC155411/pdf/attr_36_03_0228.pdf
Guskiewicz,K.M.,etal(2007).RecurrentConcussionandRiskofDepressionin RetiredProfessionalFootballPlayers.JournalofMedicine&ScienceinSports &Exercise. http://indianasportsconcussionnetwork.com/recurrentriskofdepressionnfl.pdf
Hazrati,L.N.,etal(2013).AbsenceofChronicTraumaticEncephalopathinRetired FootballPlayerswithMultipleConcussionsandNeurological Symptomatology.JournalofHumanNeuroscience,7,222. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3662898/
Iverson,G.L.,etal(2012).PossibleLingeringEffectsofMultiplePastConcussions. JournalofRehabilitationResearchandPractice. http://www.hindawi.com/journals/rerp/2012/316575/

17
Jantzen,K.J.,etal(2004).AProspectiveFunctionalMRImagingStudyofMildTraumatic BrainInjuryinCollegeFootballPlayers.AmericanJournalofNeuroradiology,25, 738-745.http://www.ajnr.org/content/25/5/738.full.pdf+html
King,N.S(2003).Post-ConcussionSyndrome:ClarityAmidtheControversy?British JournalofPsychiatry,183,276-278. http://bjp.rcpsych.org/content/bjprcpsych/183/4/276.full.pdf
Lehman,E.J.,etal(2012).NeurodegenerativeCausesofDeathAmongNational FootballLeaguePlayers.TheOfficialJournaloftheAmericanAcademyofNeurology, 79(19),1970-1974.http://www.neurology.org/content/79/19/1970.short
McCroy,P.,etal(2015).SportPsychologyandConcussion:NewImpactstoExplore.British JournalofMedicine.http://bjsm.bmj.com/content/38/5/519.full.pdf+html
Powell,J.W(2001).CerebralConcussion:Causes,Effects,andRisksinSports.Journalof AthleticTraining,36(3),307-311. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC155423/pdf/attr_36_03_03 07.pdf
Rudelli,R.,etal(1982).PosttraumaticPrematureAlzheimer’sDisease.Journalofthe AmericanMedicalAssociation,39(9),570-575. http://archneur.jamanetwork.com/article.aspx?articleid=5811
White,J.(2012).CONCUSSION:ShortandLong-TermImpact.RetrievedNovember14, 2015,fromhttp://mnepilepsy.org/patient-information/concussion-short-and-long- term-impact/

![Bryan Concussion General Audience - 2015.pptx [Read-Only] · 2015-09-03 · CONCUSSION ‐16,400,000 MTBI and Post‐Concussion Syndrome ‐ 141,000 Concussion Management ‐1,550,000](https://img.pdfslide.net/doc/110x75/5fb548e39d237d0cb0684f4f/bryan-concussion-general-audience-2015pptx-read-only-2015-09-03-concussion.jpg)

























