Embed Size (px)
Citation preview

T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E
Time keeps on ticking into the future … past generations have dreamed of escaping the forces of time. Each time succumbing to the truth that we
need to embrace the present and learn to adapt to the inevitable future. Thus the only way we can move forward is though education as we heard from our presentation by Dr. Jeff Levy. Education can lift a soul from poverty to president in a single generation. The act of delivering education benefits the educator and “educatee”. Our speaker for next dinner meeting is one of the best in our field! He absolutely mesmerized us a few years ago when he presented an unforgettable
lecture on management of hypertension. Dr. Michael Foley will be presenting again next month. He will simplify the complex topic of Disseminated Intravascular Coagulation like no one else. We need to embrace educators like Dr. Foley who has the talent to lift
our knowledge from being a student to a professor! Be sure to not miss this opportunity. Looking forward to seeing you at our new venue: The National Liberty Museum (321 Chestnut Street) with discounted parking at the Bourse garage (400 Ranstead St.).
NewsletterF E B R U A R Y 2 0 1 7 V O L . 4 3 , N O . 2
T h e O b s t e t r i c a l S o c i e t y o f P h i l a d e l p h i a
PAGE 1 President’s Message
PAGE 2 Embrace Our Legacy
PAGE 3 Foster Collegiality
PAGE 4 January Meeting Photos
PAGE 7 Share Expertise
PAGE 9 Local Happenigs/Good News
PAGE 10 Improving Health of Women
PAGE 13 2017 Meeting Schedule
PAGE 14 Council Member Page
IN THIS Issue
President’s Message
1
To embrace our legacy, foster collegiality, and share expertise to improve the health of women in Philadelphia and beyond
Dr. Foley received his medical degree from The Chicago Medical School and completed his Obstetrics and Gynecology residency and his Maternal-Fetal Medicine fellowship at Ohio State University in Columbus, Ohio. He is board certified in Maternal-Fetal Medicine. Dr. Foley is a clinical professor of Obstetrics and Gynecology at the University of Arizona in Tucson. He is the director of obstetric intensive care at Banner Good Samaritan in Phoenix, Arizona. He is recognized as one of the world’s leading experts in the area of obstetric critical care. Dr. Foley is the editor of Obstetric Intensive Care: A Practical Manual, 1st and 2nd edition textbooks. He has been honored as one of the best doctors in America and locally as one of Phoenix’s top doctors.
Upcoming Lecture:“ABC’s of DIC”
Michael Foley, MDChair and Program Director, Banner Good Samaritan Medical Center, Arizona
Thursday,February 9, 2017
6:00pm Cocktails 6:30pm Buffet & Program
NEW VENUE! The National Liberty Museum
321 Chestnut Sreet, Philadelphia
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 2
Embrace Our Legacy
Commentary From Today’s Perspective. . .
The understanding of hemorrhage and shock in this time period was limited to practical experience. Certainly, obstetrics was an arena where practical understanding of bleeding was key to limiting bad outcomes, and indeed, the contributions of tone, tissue, and trauma to post-partum hemorrhage were well understood. Thrombus, on the other hand, was just being examined under the microscope, and clotting factors were only first described in 1905. Blood transfusion was still rare, since ABO typing and cross-matching were not elucidated until later in the decade, though saline transfusion was used to expand intravascular volume.
In the discussions of the Society in these years, there is a shift in focus, from post-partum hemorrhage, to the diagnosis and treatment of extrauterine or ectopic pregnancy. Providers feared the associated blood loss and anemia that led to mortality, but effective treatments were not yet established. Abdominal surgery was gaining in popularity, and anesthetic, irrigation, and suture techniques were frequently debated at Society meetings. Aside from suture ligation, the most effective technique involved irrigation of the bleeding surface with hot water!
This is what Dr. Davis is describing here: irrigation of the uterine cavity (with no anesthetic, please note) to treat hemorrhage. He notes that blood loss can be particularly heavy in septic patients, which demonstrates an understanding of coagulopathy. Remarkably, the pearls he gives in this paper are not completely different from current practice.
Do you have a contemporary comment to share? Join the conversation on our
Facebook page.
- Jasit Beausang. M.D.
When shall the uterus be douched and how shall it be done?- January 4, 1900
“Cases are occasionally seen where sepsis and haemorrhage are combined. In these patients, the infection has proceeded to such an extent that the blood is profoundly altered, and its coagulating power greatly reduced. Cases of incomplete abortion complicated by septic infection are sometimes among this class. In these patients, prolonged douching and intra-uterine manipulation must be avoided. The use of an anaesthetic is dangerous. While it is proper to douche and cl
eanse the uterus, this should be done as rapidly and gently as possible, the cavity firmly packed with gauze, and the patient stimulated in the most active manner. Such cases are occasionally lost through failure to rapidly perform the necessary manipulations.”-
- Read by Edward P. Davis, A.M., M.D. Professor of Obstetrics, Jefferson Medical College
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 3
Foster Collegiality
THE PAST TODAY, HAPPY 2017!
As we look ahead to 2017 and just a year away from 2018 our 150th, sesquicentennial celebration, it is important to recognize the history we have created in the last year and relate it back to the history of the distant past. In 1868 when the Society’s founding members decided that there should be a formal structure to their gatherings where they discussed relevant clinical and societal issues of the care of women in the Philadelphia region. They brought to the table the importance to have a Society that was academic, responsive and responsible. We have treasures in the published proceedings of the Society that allow us to look back and realize that what was important in 1868 is not so far from what we need to consider today; to be academic, responsive and responsible.
To be academic, the founders were largely part of community hospitals, and in 1868 there were many of them, however they recognized the importance of raising clinical scenarios in open forum to hopefully develop a consensus of treatment typically based on outcomes, but perhaps in their own way putting together current evidence in a manner to develop best practice for the time. Not unlike what we do today in our individual institutions and in a bigger way in the Society. They did not know that Philadelphia would become one of the most prominent cities for medicine and education and they played a part in establishing the foundation for outcomes and evidence based medicine.
To be responsive, the founders looked at issues affecting women and their families of Philadelphia specifically access to care, poverty and nutrition. One hundred and fifty years later, we still consider those issues but in ways that our founders would be surprised. How would they relate to the utilization of robotics, personalization of care of genetics and individualization of access through the internet and smart phones. Today’s young physicians are still learning about hypertension, diabetes and fibroids, but also need to understand world infections of HIV, Ebola and Zika as well as the local opioid use epidemic affecting our own region.
To be responsible, the founders started our Society off in a manner of most societies establishing Bylaws, setting up a museum and putting together a library. They established roles and traditions. They put forth procedures and policies to help the Society succeed and exist. The original library was deeded to the College of Physicians and became a part of one of the richest medical resources in the United States. Our artifacts from our museum are thought to have become the foundation for the world renown Mutter Museum. Today our Society continues to maintain standards, uphold the Bylaws and contribute to our history through the archives. Though the venue and the hospitals in the community may change, the mission of the Society lives on and we looking forward to much success in the upcoming year of 2017.
Mark B. Woodland, MS, MD, FACOG

T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 4
January Meeting
The Society would like to thank Dr. Levy for sharing his time and expertise. Members and Emeritus may view the lecture on our website www.obphila.org. We hope to see you in February at our NEW VENUE - The National Liberty Museum!
Drs. Galdi & Dougherty
Thank you Cooper Surgical!
Drs. Perriera, Wolf, Delvadia, Woodland & Sondheimer
Drs. Gocial, Zeidman & Brest
Thank you sponsors!
Drs. Wang, Williams & Patel
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 5
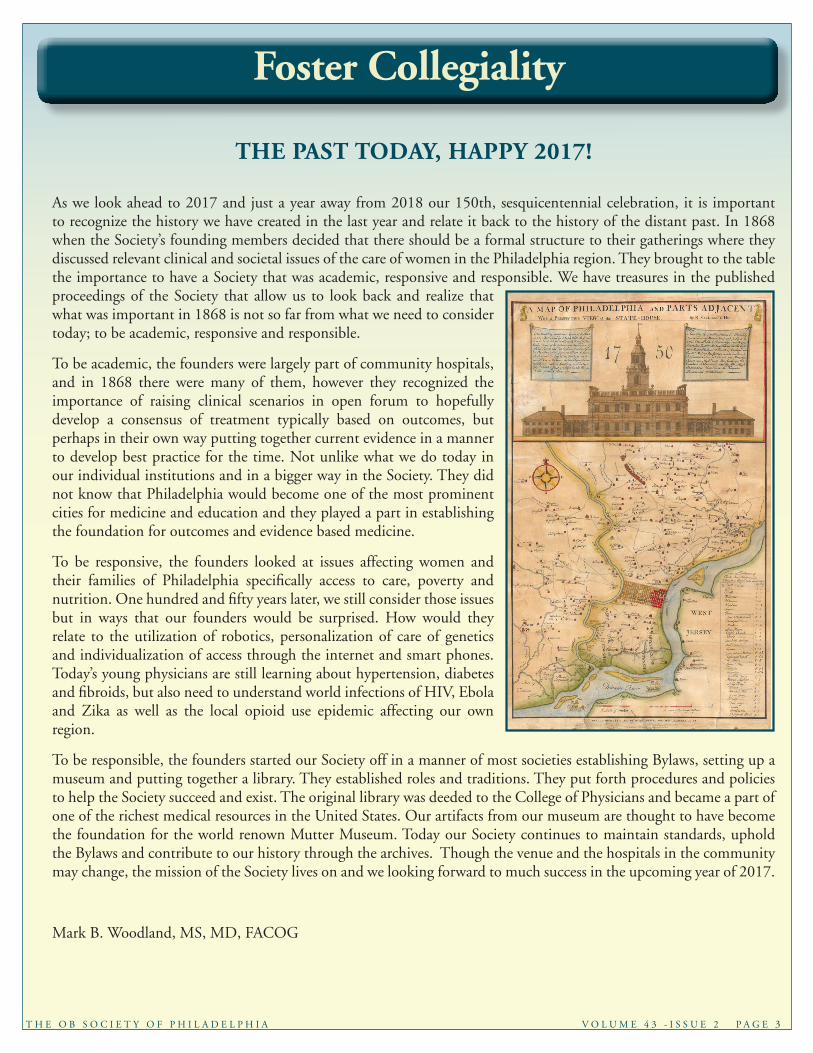
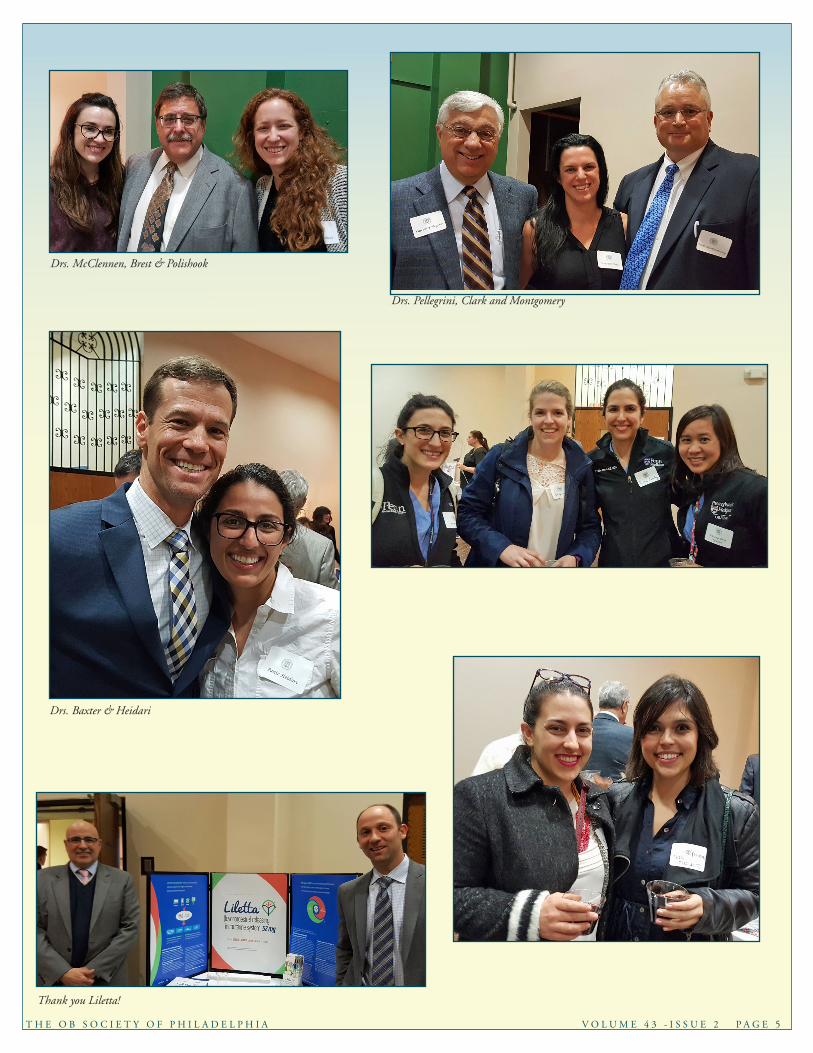
Drs. McClennen, Brest & Polishook
Drs. Pellegrini, Clark and Montgomery
Drs. Baxter & Heidari
Thank you Liletta!
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 6
Dr. Steven Sondheimer
Resident Presenter Sumra Tayebaly, M.D.
Drs. Delvadia, Levy & Woodland
Dr. Jeffrey Levy signs the Book!
Dr. Jeff Levy delivered a wonderful lecture!
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 7
Share Expertise
About four to five years ago, the Philadelphia Obstetrical Society teamed up with the March of Dimes for a conference hosted at the Pennsylvania Hospital to address Obstetrical Issues. The topics were wide ranging and included prevention of prematurity, hypertension and pre-eclampsia, shoulder dystocia, maternal hemorrhage and putting the “M” back in Maternal Fetal Medicine. Today the focus will be on maternal hemorrhage in keeping with this month’s Ob Society lecture on DIC.
Suggestions and ideas from that conference included education, preparation and drills. The educational component consisted of the obvious aspects of understanding maternal physiology, obstetrical hemorrhage and risk factors leading to these situations. This led to suggestions for assessing and communicating risk for hemorrhage and particularly postpartum hemorrhage. Another aspect was recognition that estimated blood loss is typically grossly underestimated. Education and training of all members of the health care team was encouraged to more appropriately evaluate patients experiencing hemorrhage at any stage of their care. The institution of the “massive transfusion protocol” was then recommended to be used when significant blood loss was noted. This takes the “thinking” out of the emergency situation to replace blood products in an appropriate fashion and help prevent adverse sequelae, such as DIC. Finally, drills to have staff trained to recognize and respond to these emergency situations in the quickest and most efficient manner were recommended. Drills have the added benefit of recognizing process issues before providers are found in the real emergency situation. These issues consist of items, such as, real time delivery of blood products or medications when seconds count.
One of the sequelae of the Philadelphia Obstetrical Society/March of Dimes conferences was the development of the Labor and Delivery Leadership ad hoc committee. This committee is composed of the Obstetrical Medical Director, Obstetrical Nurse Leader, and a safety officer from each of the six delivering teaching hospitals in Philadelphia. This group has met many times since the summit conferences to discuss and implement some “best practice” ideas that came out of the conference in all of the institutions for consistent education and care throughout the city. Some of the policies have included a more streamlined obstetrical record sharing process, urine drug screening policies and management of post-partum hemorrhage. It is the hope of this group to make available their suggestions and policies to the Delaware Valley region. One possible avenue for the dissemination of this information may be the Philadelphia Obstetrical Society web site.
Einstein Medical Center Montgomery experienced a fairly unique situation that required attention to development of these safety issues. This situation was the construction of a new hospital that drastically impacted the “delivery” of care by having a new physical structure. A new phone system, new “geography” of the triage, labor and delivery, postpartum and nurseries combined with rapid growth in census and staff led to the need to address emergency issues. New staff required the educational component. The department, as a whole, had to address the consistent and timely delivery of care in emergencies. Since the purview of this article is on hemorrhage, interventions for that will be the focus. The first item developed with the cooperation of the pharmacy was a hemorrhage kit. While some of these issues may seem easy, there are many technical details that need to be taken into account in our increasingly regulation driven delivery of health care. Simple needs of the refrigeration requirements for some medications make it almost impossible to have
Preventing Post-Partum Hemorrhage: The OB Society Puts It All Together
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 8
them immediately available in every delivery or operating room. When a real-time drill was performed, it took the nurse four to five minutes to travel from one of the delivery rooms to the med room (where the controlled refrigerator is kept) and back. In a severe postpartum hemorrhage, this is an unacceptable time. Therefore, EMCM’s hemorrhage kit starts simply with misoprostol, which is stable at room temperature and oxytocin which is generally stable at room temperature. These medications can be started while other uterotonics can be obtained from the med room refrigerator.
Cooperation with the anesthesia department, blood bank and the operating room, led to the implementation of the “massive transfusion protocol”. When severe or brisk blood loss is encountered, one verbal order to begin the “massive transfusion protocol” is all that is needed to provide multiple units of blood and blood products in a very timely fashion.
All staff were educated in assessment of risk for postpartum hemorrhage at admission and each patient gets assigned a risk level. If risk is rated at moderate to high, then the postpartum hemorrhage kit is brought into the delivery room. An additional nurse is physically present in the delivery room for the mother and one for the infant. Provider and nursing staff verify in the medical record that the patient’s blood type and screen is present. All staff have been educated in recognizing hemorrhage and assessing volume. Based on that assessment, response based on Stage of hemorrhage is then initiated. This response ranges from fundal massage and uterotonics to “massive transfusion protocol”.
After delivery, the consistent use of oxytocin is encouraged. On the postpartum unit, regular assessment of the bladder and fundus has been encouraged. When hemorrhage occurs, a “postpartum hemorrhage cart” has been assembled. This includes misoprostal, oxytocin, IV fluids and materials to start an IV, an IV pole, and Foley catheter. A notification system has also been established to bring all appropriate personnel to the patient’s room emergently.
Finally, a simulation mannequin and synthetic blood was able to be purchased to practice all of these education, assessment and response components.
The California Maternal Quality Care Collaborative has made available on their website a comprehensive guide for all aspects of identification and management of postpartum hemorrhage. This website can be accessed free of charge at www.cmqcc.org. They do require registration and answering a brief questionnaire to download all their information and protocols.
The response to postpartum hemorrhage is reminiscent of the movie “Sully” on two accounts. First, seconds count and the sooner you implement appropriate treatments, the more likely you will end with a better outcome. However, as Dr. Arnold Cohen pointed out in an email last fall, one must consider
the human element. Simulation does not account for the patient that “weighs 350 pounds, screaming, not cooperative”, possible substance abuse, no prenatal care, or undiagnosed medical issues. We are humans working on humans which introduces an infinite number of variables that can never be accounted for by simulation alone or simple protocol.
- Donald DeBrakeleer, DO
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 9
David M. Jaspan, DO, Einstein’s Chair of Obstetrics and Gynecology, Selected An Emerging Icon Awardee by The Philadelphia Inquirer
Davitd M. Jaspan, DO, FACOOG, Chair of the Department of Obstetrics and Gynecology at Einstein Healthcare Network has been selected as an Emerging Icon in Education and Medicine by The Philadelphia Inquirer. This is the first year of the Icon Awards, which honor leaders who have made significant contributions to the Philadelphia region in various industries. The winners were nominated by readers through an open nomination process on philly.com and selected by independent judging panels made up of experts in each of their fields.
As Chair of Obstetrics and Gynecology (Ob-Gyn) for Einstein Healthcare Network, Dr. Jaspan is responsible for patient care, including the delivery of babies, at Einstein Medical Center Philadelphia and at Einstein Medical Center Montgomery. More than 5,000 babies are born each year at both campuses.
In addition to obstetrics, Dr. Jaspan spearheaded the opening of the Pride Clinic, a program that offers the LGBT community a full range of Ob-Gyn services, including health maintenance exams; screenings; reproductive healthcare; counseling and treatment for menopause; and treatment for anxiety or depression. Opened in June 2015, the Pride Clinic is the only service of its kind in North Philadelphia or Montgomery County dedicated to the care of the LGBT community.
Honorees were recognized on November 16, 2016 at an awards event at Vie on North Broad
If you have anything to add to our newsletter, please contact Teri Wiseley at [email protected]. Your input to the newsletter is greatly appreciated.
Cell: 484-343-8199Email: [email protected]: Theresa B. Wiseley, CMM Executive Secretary Obstetrical Society of Philadelphia 308 Rolling Creek Rd. Swarthmore, PA 19081
Local Happenings & Good News
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 1 0
Improving Health of Women
THE PHILADELPHIA SODA TAX, OBESITY AND PUBLIC HEALTH- Sherry L Blumenthal MD, MSEd, FACOG
Mayor Kenney of Philadelphia proposed a 3-cent per ounce tax on sugar-sweetened beverages as a mechanism to fund Pre-K education and other city health and education programs. It was reduced to 1.5% before passage by City Council. While he did not tout this tax as a way to improve public health, there may be huge benefits (pun intended) and most municipalities and countries that have successfully levied this tax have done so to improve the health of the populace.
I have noted a slow increase in the weight of my Gynecologic patients at each of their yearly visits. I asked one obese patient to describe her diet and she responded “I do not eat that much”. In fact, her food consumption was not excessive. Then I asked what she drank, and found that she downed 2 liters of Cola a day! QED.
There are studies linking consumption of sugar and sugary beverages, soda in particular, to the “Obesity Epidemic”. Philadelphia has the distinction of being one of the fattest cities in the US, and our country is one of the fattest in the world. Obesity in children and adults has sky-rocketed. This has led to a substantial increase in Type II Diabetes, Coronary Artery Disease, Stroke, Obstetric complications, impact on offspring of obese women, and numerous orthopedic problems.
As Mark Bitman writes in the New York Times May 25, 2016, “There are those — including (one) presidential candidate— who oppose soda taxes as a regressive tax on the poor. But it is poor people who are disproportionately targeted in the
marketing of sugary foods, and poor people who most suffer the health consequences of consuming them. Furthermore, as Philadelphia’s plan demonstrates, this tax will benefit low-income residents in two ways: It will increase their services and decrease their likelihood of developing chronic disease. Nothing regressive about that.”
I agree with his comment, as the urban poor communities have less access to fresh fruits and vegetables and, because as humans we are drawn to sugar and simple carbohydrates, tend to purchase foods in convenience stores that provide minimal nutrition but maximal calories. Increasing funds for education also increases the opportunity to educate children about nutrition and encourage consumption of healthier options.
According to the CDC, the 2015 obesity rate in young adults has increased to 26.5%. The rate is 34.6% in adults between ages 40 and 59, and 30.1% in adults 60 and over.
There are more obese women than men. In Obstetrics, the risks of pregnancy in the obese are well known. There is an increase in Gestational Diabetes, Large-for-gestational age fetuses, Hypertension and Pre-eclampsia, Congenital anomalies, intra-uterine fetal demise and neonatal death, spontaneous abortion and recurrent miscarriage. Maternal obesity causes epigenetic changes in the fetus, predisposing him or her to obesity, metabolic syndrome, and earlier adult death than fetuses of normal-weight women. Obese pregnant women have a higher risk of delivering by Cesarean Section and also a higher risk of surgical complications such as infection and thrombotic episodes.
T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 1 1
Cancer risk is higher in obese women. There is a significant increase in Breast, Ovarian, and Endometrial cancers. In both sexes there is increased risk of kidney, pancreatic, stomach, and esophagus cancers and higher rates of prostate cancer in men. Among these are the most deadly cancers.
Cancer treatments are more difficult and may be less effective in the obese since Radiation treatment areas may be harder to localize and higher doses may be needed. Chemotherapy doses required may be higher also, and more toxic to the patient. Survival in some cancers, such as Cervix in women, are lower in the obese.
The cost of the morbidity in the obese, such as more need for joint replacement and higher complication rate of surgery, is significant. Equipment needs to be modified for obese patients and hospitals are purchasing larger wheelchairs, seats, operating tables, and surgical equipment.
It appears that weight loss is very difficult to sustain, especially in the extremely morbid obese category. Therefore our best strategy is prevention, which begins in childhood.“Soda producers and distributors, as well as the Teamsters members who deliver the product, argue that the tax is a job killer, and may spend as much as $10 million to make that case. There’s zero evidence to substantiate that claim; people who don’t buy soda will most likely buy other beverages, in most cases produced by the same companies.” Many cities, notably Berkeley CA have levied “Soda taxes” as a ballot initiative, but a notable “laboratory” for change has been Mexico,” which established a national tax on soda and junk food in January 2014. In that country of 120 million people, sales of sugary beverages have indeed declined, while those of bottled water have increased”, according to Mark Bitman.
The FDA has changed food labeling to include “added sugars”. Ingredient labels are highly deceptive-they may list sugar in many different ways, i.e. “evaporated cane juice”, brown rice syrup, and corn syrup. There may be four different names for sugar in one product, misleading the public as to how much they are consuming.
Sugar in our diets is not the only culprit- large portions, processed foods, and high fat foods as well as decreased exercise also contribute to the Obesity Epidemic. Sugar, however, is a large contributor, and there are multiple benefits to the public health by taxing consumption of sweetened beverages to reduce consumption and raise money for needed services. Shame on the beverage industry to misrepresent this tax as a “grocery tax”! I hope that soon this tax can be on the ballot for approval in Montgomery County and the rest of PA. It appears to be a win-win situation.
Addendum: Since this article was written, Mayor Kenney spoke to other lawmakers about how to get this tax through, citing that appealing to health concerns is ineffective! His tactic worked, but so far there has been no decrease in sales of sweetened beverages! No one has been hurt and money has been raised for education. Perhaps in the long-run, consumption will decrease.
Imag
e co
urte
sy o
f tiv
eryl
ucky
at F
reeD
igita
lPho
tos.n
et
The Philadelphia Obstetrical Society would like to thank Dr. Blumenthal for her expert article about the “Soda Tax” and the impact of the obesity epidemic. Through her position as Secretary and Legislative Liason, she has helped the Obstetrical Society improve women’s health in Philadelphia. The Ob Society has also supported Dr. Blumenthal’s efforts with ACOG District 3’s “ROUNDS” program. ROUNDS stands for Regional OB/Gyn Up to date New Didactic Series. These are a series of lectures and lecturers through ACOG District 3 that are available for your local hospital Grand Rounds free of charge. Dr. Blumenthal has an excellent lecture on Obesity in Women and there are many others that may be accessed by visiting http://www.acog.org/About-ACOG/ACOG-Districts/District-III/Educational-Outreach-ROUNDS-Project

T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 12
COLLATERAL DAMAGE: Increased incidence of emotional vulnerability when treatment fails
Andrea Mechanick Braverman, PhD
Associate Director of the Educational Core
Clinical Associate Professor of Obstetrics & Gynecology
Clinical Associate Professor of Psychiatry & Behavioral Medicine
Sidney Kimmel Medical College of Thomas Jefferson University
A recent study from a national registry of 47,500 Danish women found that those who do not have a child are three times more likely to divorce or end cohabitation with their partner than those who do (with odds ratios up to 3.13, 95% CI 2.88–3.41) regardless of their parity, after up to 12 years post infertility treatment.1 The study went on to find that almost 27% of the women were no longer living with the person with whom they had lived at the time of the fertility evaluation.
As we know from research (and clinical experience), infertility is counted among the greatest stresses many woman and men have encountered.1 For some it is the first significant major stressor they have encountered and often infertility presents itself relatively early on in a relationship as communication and navigating or negotiating differences are just developing. Infertility places more demands on the couple to communicate with each other about coping with stress, dealing with all the feelings that infertility may engender, and making decisions about treatment. Adding to these infertility demands is that couples come to infertility with their own with their own differing levels of psychological resources and vulnerabilities. Resilience, ability to cope and psychopathology will influence not only their individual path, should treatment be unsuccessful, but will also influence the dynamics of their relationship.
So what happens if treatment fails? If couples were not communicating well to begin with, then infertility can place a load on an already fractured infrastructure. Add to that couples may feel differently about their desire to have a child or may have different needs for a child, e.g. if one partner already has children from a previous relationship. Resentment and other negative feelings can develop over treatment time as differing coping or communication styles
The literature has been clear that bereavement as a result of trauma have negative psychological as well as health outcomes. Studies have shown the divorce rate for parents who have lost a child to be as high as 8 times greater.3
Perhaps the loss of the desired child may in part be understood through the literature on parental loss and the burden it places upon the relationship with a partner who has also lost a child. Increased awareness to the vulnerabilities of the infertility loss can lead to better psychoeducation and counsel.
The Danish study gives insight into the downstream sequelae of infertility and allows providers to have a heightened sensitivity to offering support to intended parents particularly when treatment has not been successful.
1) Kjaer, Trille, et al. “Divorce or end of cohabitation among Danish women evaluated for fertility problems.” Acta obstetricia et gynecologica Scandinavica 93.3 (2014): 269-276.)
2) T.H. Chen, S.P. Chang, C.F. Tsai, K.D. Juang. Prevalence of depressive and anxiety disorders in an assisted reproductive technique clinic. Hum Reprod 2004 ;(19):2313–2318.)
3) Rogers CH, Floyd FJ, Seltzer MM, Greenberg J, Hong J. Long-term effects of the death of a child on parents’ adjustment in midlife. Journal of family psychology. 2008 Apr;22(2):203.

T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 13
The venue for the evening program is at a NEW location: The National Liberty Museum
321 Chestnut Street
Cocktails – 6:00 p.m. Dinner and Program - 6:30 p.m.
Free parking in the lot next to the PCMS Building
Please visit the website for registration information.
2017 Meeting Schedule
February 9, 2017 Michael R. Foley, MD Professor & Chair - Obstetrics & Gynecology, University of Arizona ABC’s of DIC
March 16, 2017 Adele S. Schneider, MD Director Clinical Genetics, Einstein Medical Center, Philadelphia New Horizons for Expanded Carrier Screening
April 13, 2017 Barbara Schindler, MD Vice Dean Emerita, Educational and Academic Affairs; Professor of Psychiatry and
Pediatrics, Drexel University College of Medicine Opioid Addiction Under Our Noses – National Crisis
May 11, 2017 **President’s Night** Robert Debbs, DO Clinical Professor Ob/Gyn, Director, Pennsylvania Hospital Maternal-Fetal Medicine Dipak Delvadia, DO Clinical Assistant Professor Ob/Gyn, Associate Residency Director,
Drexel University College of Medicine The Evidence, the Art, and the Obstetrician
Resident education day - FRiday, May 5, 2017 8:00 a.M. to 3:00 p.M., thoMas JeFFeRson hospital
CALL FOR PAPERS – S. LEON ISRAEL AWARDThe S. Leon Israel Award was established to recognize excellence in research in the discipline of obstetrics and gynecology. The award is open to all current obstetrics and gynecology residents in programs associated with the Obstetrical Society of Philadelphia. Original research manuscripts not published prior to April 1, 2017 will be accepted for review.
The resident must be the first author, but not necessarily the only author of the paper. It is expected that the resident will have primary responsibility for the literature review, implementation of the study and final drafting of the discussion section. Review articles will not be accepted. Papers should be written in a scientific format to include title, authors, institution, abstract, introduction, materials and methods, results, and discussion and should conform to the instructions for the American Journal of Obstetrics and Gynecology.
Two copies should be submitted. One copy should have all institution and author information removed. The award and stipend ($500.00) will be conferred at the Annual Resident Day Bowl and Symposium on Friday, May 5, 2017. The author of the winning paper will be asked to present a brief summary of his/her work at the Resident Day Symposium and at President’s Night, Thursday, May 11, 2017.
Manuscripts must be received no later than April 1, 2017 to allow adequate time for review. Any manuscripts received after April 1, 2017 will be ineligible for consideration.
Manuscripts should be submitted to: Teri Wiseley, CMM, Executive Secretary via email to [email protected]

T H E O B S O C I E T Y O F P H I L A D E L P H I A V O L U M E 4 3 - I S S U E 2 P A G E 14
PRESIDENT Dipak Delvadia, DO
DUCOM - Dept. OB/GYN245 North 15th StreetPhiladelphia, PA l9l02-1192
IMMEDIATE PAST PRESIDENTHelen M. Widzer, MD
Women’s Associates for HealthcareEinstein Healthcare Network633 W. Germantown Pike Suite 203Plymouth Meeting, PA 19462
PAST PRESIDENT - 2nd YEARJason Baxter, MD
Thomas Jefferson University833 Chestnut Street, 1st FloorPhiladelphia, PA 19107
PRESIDENT ELECTA. George Neubert, MD
Geisinger Health System100 N. Academy Ave.Danville, PA 17822
VICE PRESIDENTPeter F. Schnatz, DO
The Reading Hospital and Medical CenterDepartment of OB/GYN6th Ave & Spruce StreetWest Reading, PA 19611
SECRETARY - 3rd YEARSherry. L. Blumenthal, MD
2701 Blair Mill Rd. Suite CWillow Grove, PA 19090
TREASURERHarish Sehdev, MD
Pennsylvania Hospital2 Pine east 800 Spruce StreetPhiladelphia, PA 19107
ASSISTANT SECRETARYNorman Brest, MD
Lankenau Medical Building, East100 East Lancaster Avenue, Suite 561Wynnewood, PA 19096-3450
ARCHIVESMark B. Woodland, MD
The Reading Hospital and Medical CenterDepartment of OB/GYN6th Ave & Spruce StreetWest Reading, PA 19611
RESIDENCT EDUCATION LIAISONGuy Hewlett, MD
Cooper University HospitalDept of Ob/GynOne Cooper PlazaCamden NJ 08103
RESIDENT EDUCATION COMMITTEEXuezhi Jiang, MDThe Reading Hospital and Medical Center, Department of OB/GYN 6th Ave & Spruce Street West Reading, PA 19611
RESIDENT EDUCATION COMMITTEEJasjit K. Beausang, MD
DUCOM – Dept. OB/GYN245 Norht 15th StreetPhiladelphia, PA 19102-1192
RESIDENT EDUCATION COMMITTEELarry Glazerman, MD
Planned Parenthood of Delaware 625 N. Shipley St. Wilmington DE 19801
RESIDENT REPRESENTATIVENEWSLETTER STAFFSumra Tayebaly, MD
MEMBERSHIP Fay D. Wright, MD
111 E. Levering Mill RoadBala Cynwyd, PA 19004
SOCIAL MEDIAAasta D. Mehta, MD
Lehigh Valley Health Network1245 Cedar Crest Blvd, Suite 201Allentown, PA 18103-6267
WEBSITE Albert El-Roeiy, MD
Crozer-Chester Medical CenterOne Medical Center BoulevardUpland, PA 19013-3995
BYLAWS Joan H. Zeidman, MD
919 Conestoga RoadBuilding 1, Suite #104Rosemont, PA 19010
SESQUICENTENNIAL COMMITTEESusan Kaufman, DO
Suite S-93, Executive Mews1930 State Hwy 70 EastCherry Hill, NJ 08003
FOUNDATIONArnold W. Cohen, MD
Albert Einstein Medical Center5500 Old York RoadPhiladelphia, PA l9l41
NEWSLETTER Donald DeBrakeleer, DO Center for Women’s Health of Montgomery County 1000 Walnut Street, Suite 122 Lansdale, PA 19446
MEMBER AT LARGE - 1st YEARDr. Abigail Wolf
833 Chestnut Street,1st FloorPhiladelphia, PA 19107-5127
MEMBER AT LARGE - 1st YEAR Lisa K. Perriera, M.D
833 Chestnut Street1st FloorPhiladelphia, PA 19107
NEWSLETTER COMMITTEELuisa Galdi, D.O.
216 N. Broad St.Feinstein 4th floorPhiladelphia, PA 19102
OBSTETRICAL SOCIETY OF PHILADELPHIACouncil Members: 2016-2017
MEDICO/LEGAL COMMITTEEJane Porcelan, MD, JD
Lankenau Medical Building, West100 Lancaster Avenue, Suite #433Wynnewood, PA 19096