Embed Size (px)
Citation preview
The Offender Personality Disorder Strategy Commissioning the pathway
12th April 2012
Nick Joseph & Nick Benefield
Department of Health/NOMS personality disorder policy team
Objective
To set out the DH/NHS/NOMS commissioning
intentions, by presenting:
• The context
• The strategy
• Thinking on commissioning community
services
• Practical examples of community based
services
The wider picture
The PD ‘Project’
Life Course Development and Pathway
The diagnosis problem & a biopsychosocial model
Partnership Programme
The vision
Reduce the risk of serious harm to others and serious further offending
Improve psychological health and wellbeing, and tackle health inequalities
Develop leadership in the fields of health, criminal justice and social care, and create a workforce with
appropriate skills, attitudes and confidence
Coalition Government’s policy For NOMS & the NHS to improve the management of
offenders with PD through:
Predominantly based in the CJS
Whole systems approach
Psychologically informed approaches focussing on relationships and the social context in which people
live
Shared responsibility
Joint operations
Coalition Government’s policy (2) For NOMS & NHS specialised commissioning to deliver:
A focus on assessment, case formulation and sentence planning
PD treatment units in prisons & PIPES to improve progression
Improved targeting of resources for screening & early identification
Access to secure psychiatric hospitals
Strategic context 1999
2011
2009
“In conjunction with other
government departments, the
Department of Health, the
National Offender Management
Service and the NHS should
develop an inter-departmental
strategy for the management of
all levels of personality disorder
within both the health service
and the criminal justice system,
covering the management of
individuals with personality
disorder into and through
custody, and also their
management in the community.”
Strategic context 1999
2011
2011
Published 21st October 2011
Historical context 1999
2011
Labour party manifesto (2001)
‘those with a dangerous severe personality disorder
– we will pass new legislation and
create over 300 more high-security prison and hospital
places’
2001
Led to DSPD units at: Whitemoor (2003), Frankland (2004), Rampton (2004) Broadmoor (2005) & Primrose (2007)
Context – some things that may still be useful
1999
2011
2003
Context – some things that may still be useful
1999
2011
2004/5
2007
• The Knowledge
and Understanding
Framework
• Basic training about
attitudes and
leadership through
a BSc & MSc
programme
Context 1999
2011
2009
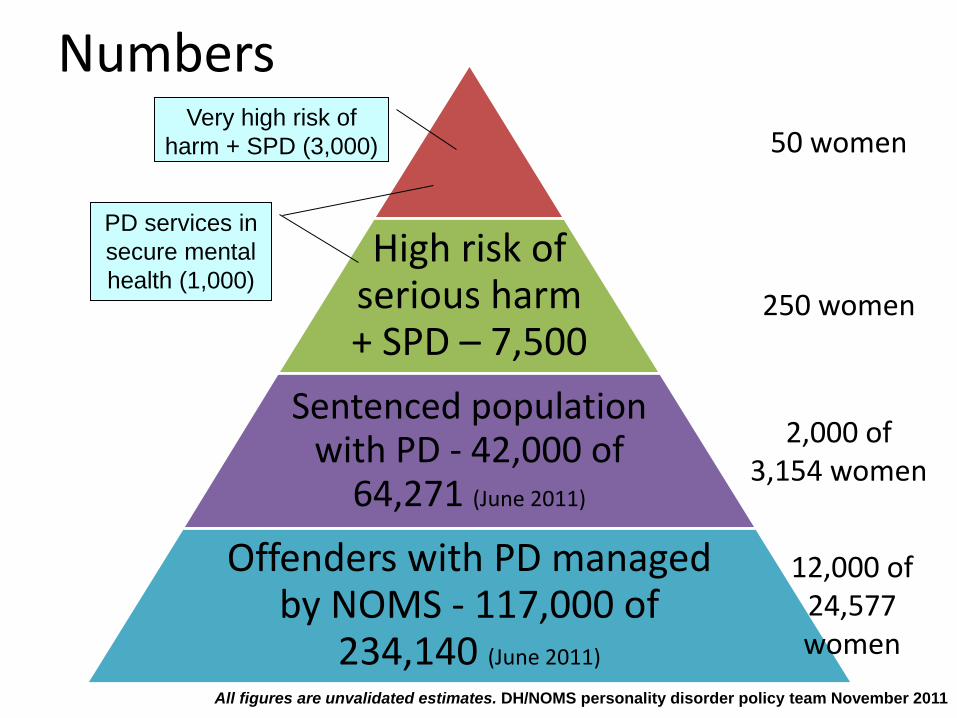
High risk of serious harm + SPD – 7,500
Sentenced population with PD - 42,000 of
64,271 (June 2011)
Offenders with PD managed by NOMS - 117,000 of
234,140 (June 2011)
Very high risk of
harm + SPD (3,000)
PD services in
secure mental
health (1,000)
All figures are unvalidated estimates. DH/NOMS personality disorder policy team November 2011
Numbers
12,000 of 24,577 women
2,000 of 3,154 women
250 women
50 women
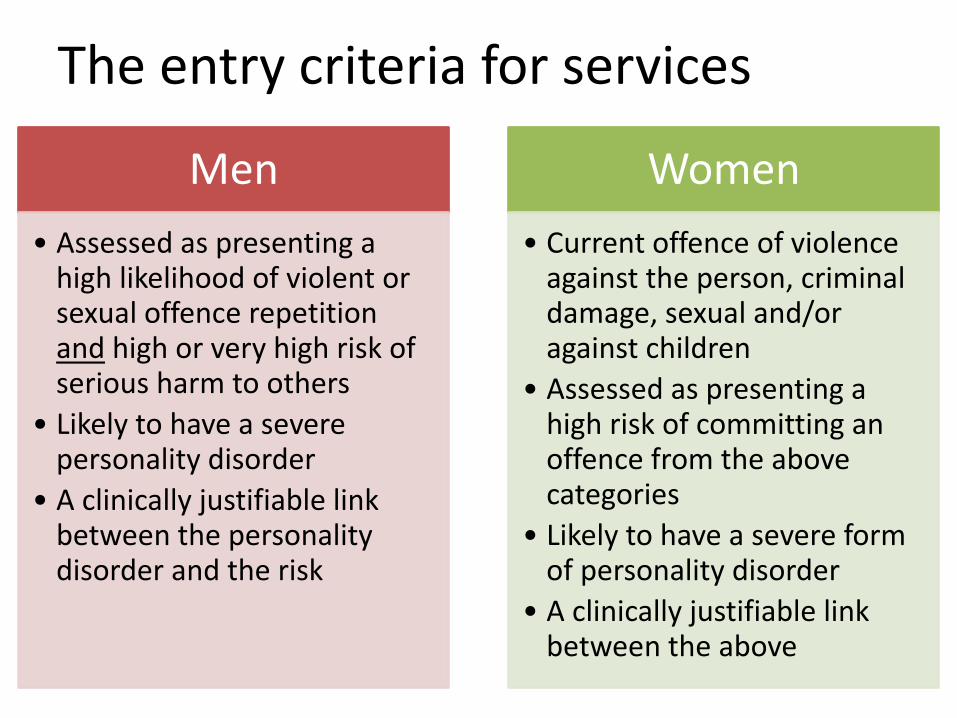
The entry criteria for services
Men
• Assessed as presenting a high likelihood of violent or sexual offence repetition and high or very high risk of serious harm to others
• Likely to have a severe personality disorder
• A clinically justifiable link between the personality disorder and the risk
Women
• Current offence of violence against the person, criminal damage, sexual and/or against children
• Assessed as presenting a high risk of committing an offence from the above categories
• Likely to have a severe form of personality disorder
• A clinically justifiable link between the above
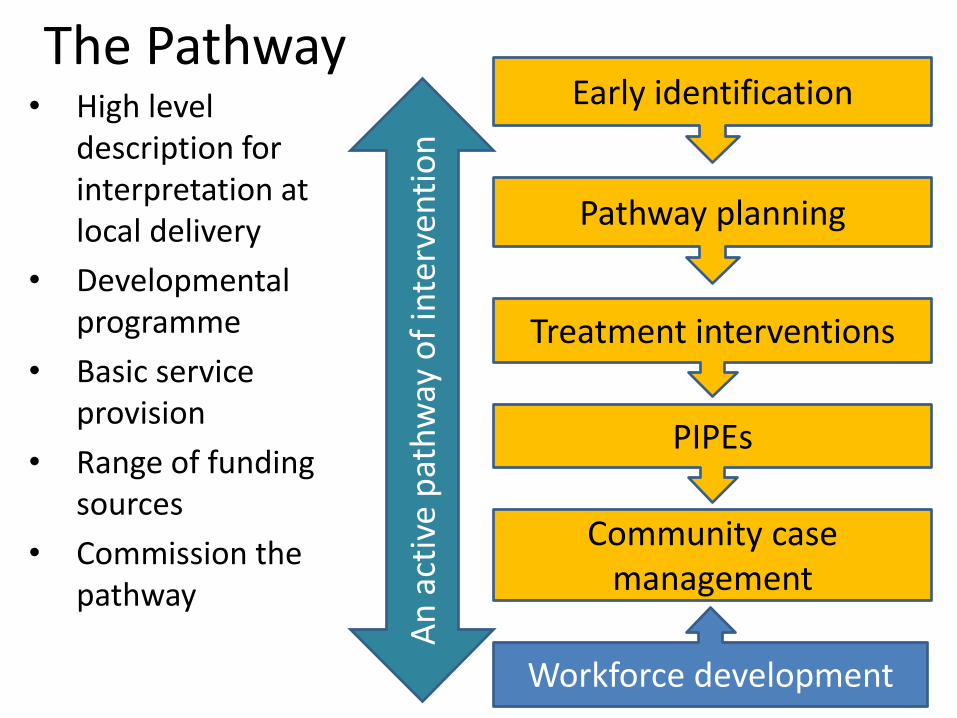
Early identification
Pathway planning
Treatment interventions
Community case management
An
act
ive
pat
hw
ay o
f in
terv
enti
on
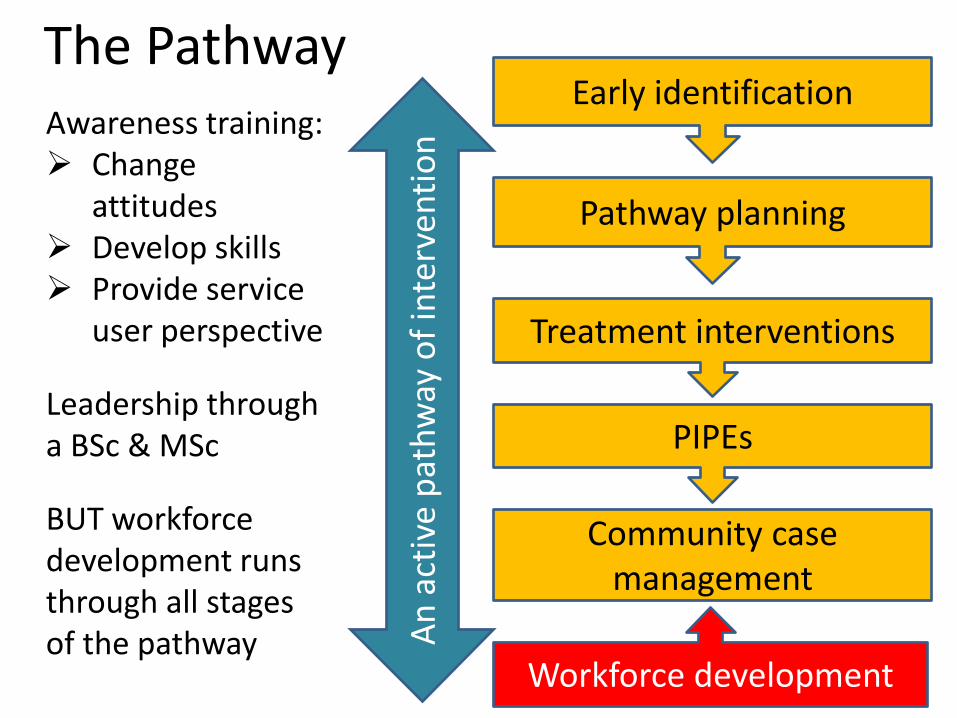
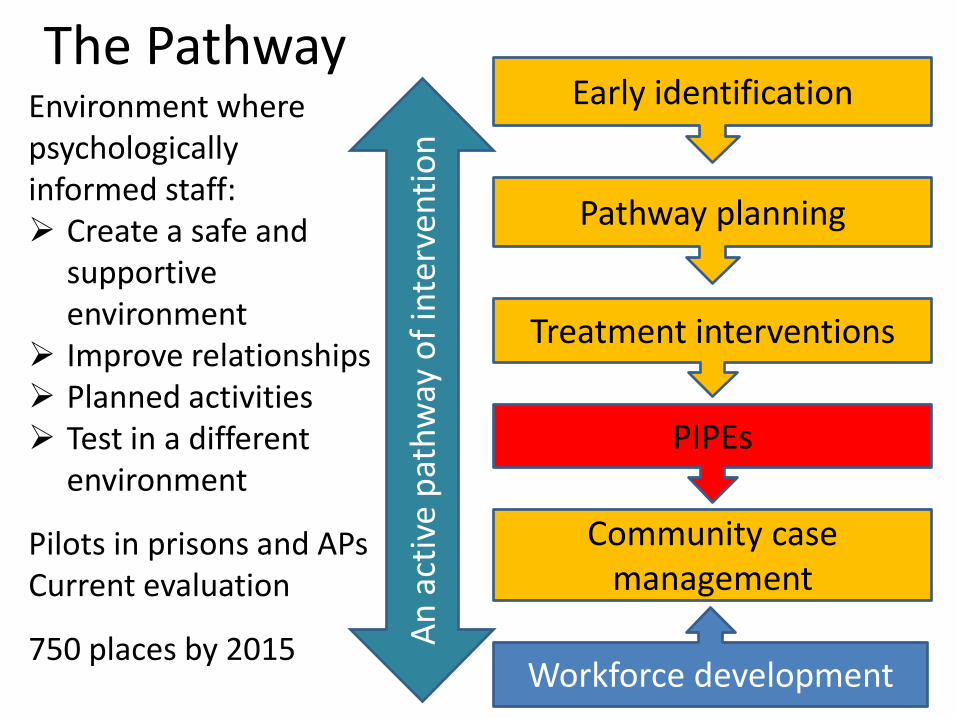
The Pathway
PIPEs
Workforce development
• High level description for interpretation at local delivery
• Developmental programme
• Basic service provision
• Range of funding sources
• Commission the pathway
Early identification
Pathway planning
Treatment interventions
Community case management
An
act
ive
pat
hw
ay o
f in
terv
enti
on
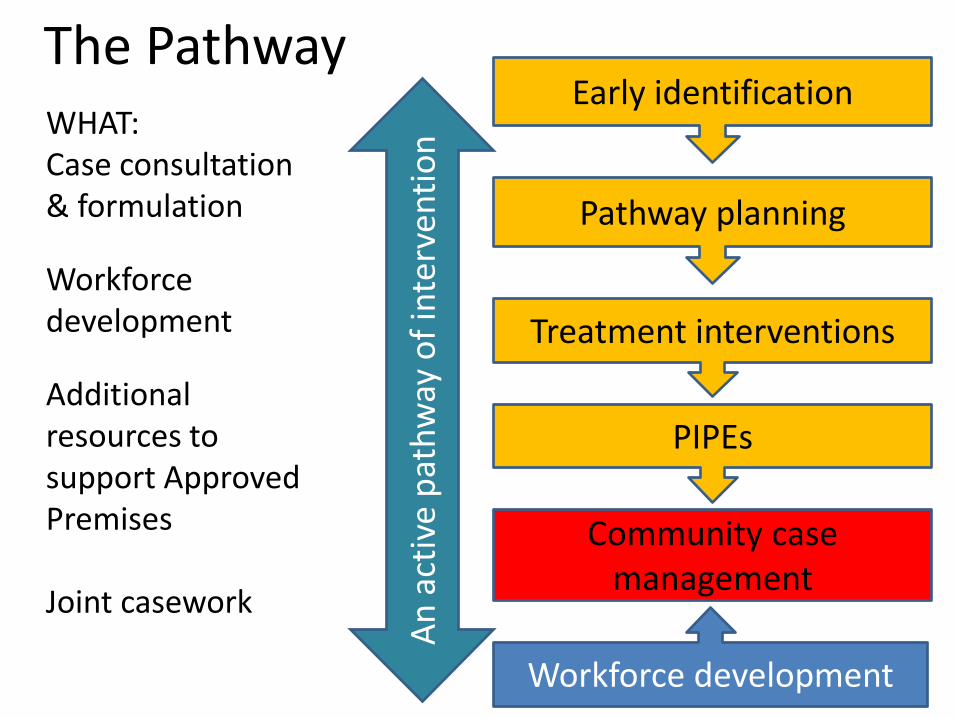
The Pathway
PIPEs
Workforce development
Awareness training: Change
attitudes Develop skills Provide service
user perspective
Leadership through a BSc & MSc
BUT workforce development runs through all stages of the pathway
Early identification
Pathway planning
Treatment interventions
Community case management
An
act
ive
pat
hw
ay o
f in
terv
enti
on
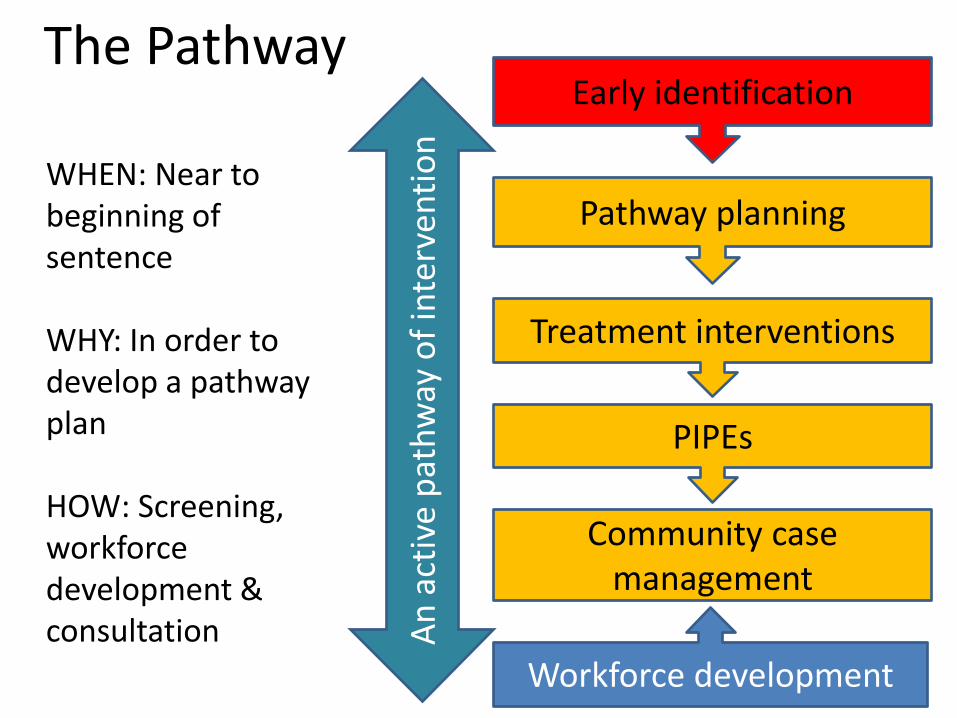
The Pathway
PIPEs
Workforce development
WHEN: Near to beginning of sentence WHY: In order to develop a pathway plan HOW: Screening, workforce development & consultation
Early identification
Pathway planning
Treatment interventions
Community case management
An
act
ive
pat
hw
ay o
f in
terv
enti
on
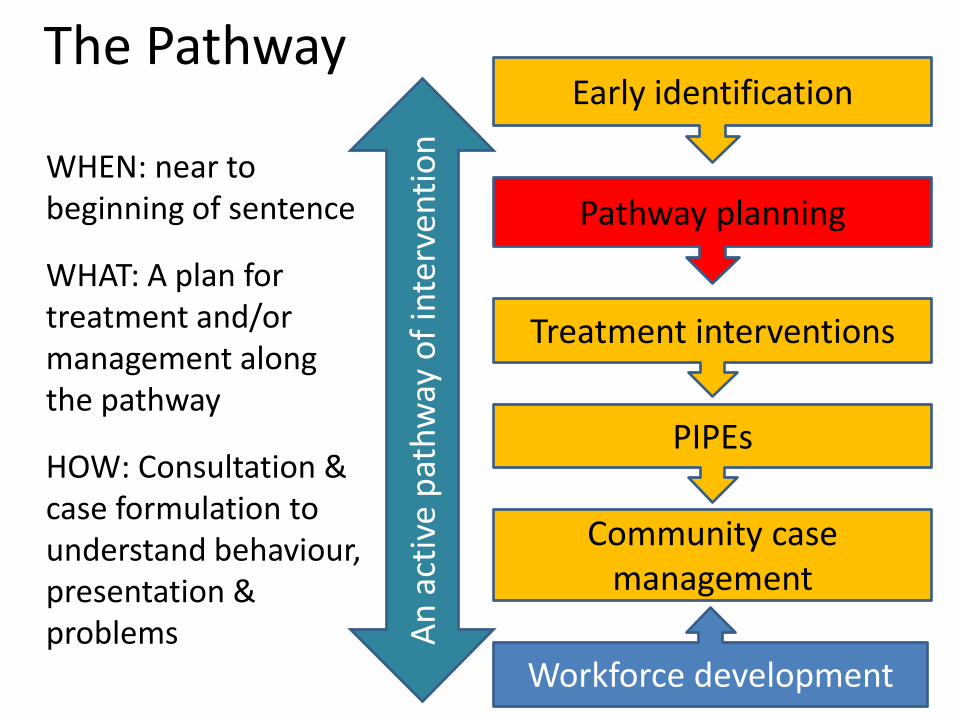
The Pathway
PIPEs
Workforce development
WHEN: near to beginning of sentence
WHAT: A plan for treatment and/or management along the pathway
HOW: Consultation & case formulation to understand behaviour, presentation & problems
Early identification
Pathway planning
Treatment interventions
Community case management
An
act
ive
pat
hw
ay o
f in
terv
enti
on
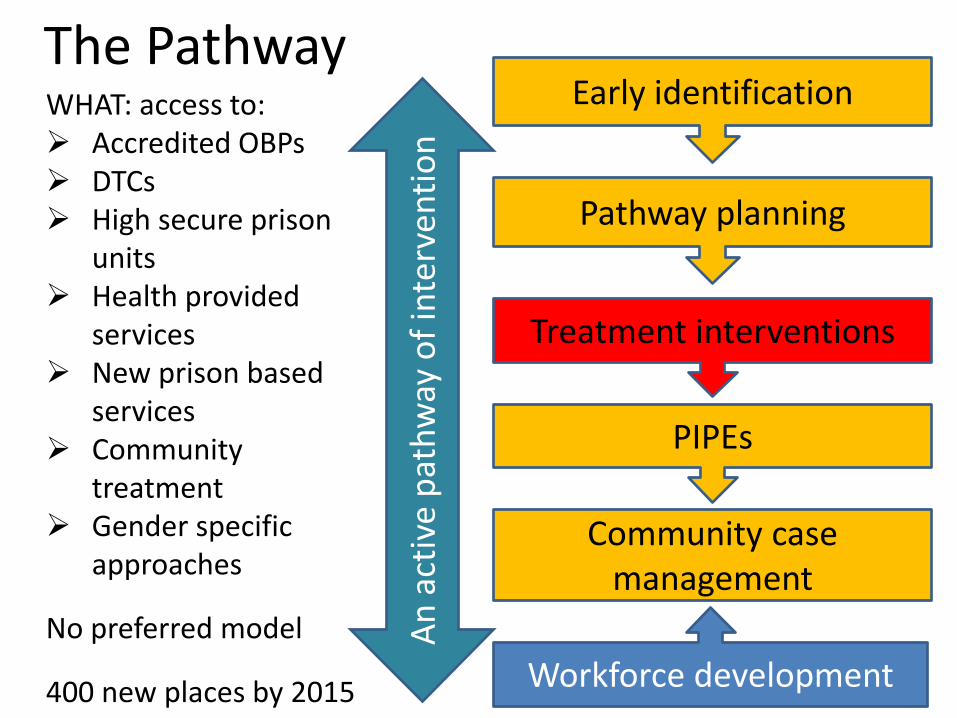
The Pathway
PIPEs
Workforce development
WHAT: access to: Accredited OBPs DTCs High secure prison
units Health provided
services New prison based
services Community
treatment Gender specific
approaches
No preferred model
400 new places by 2015
Early identification
Pathway planning
Treatment interventions
Community case management
An
act
ive
pat
hw
ay o
f in
terv
enti
on
The Pathway
PIPEs
Workforce development
Environment where psychologically informed staff: Create a safe and
supportive environment
Improve relationships Planned activities Test in a different
environment
Pilots in prisons and APs Current evaluation
750 places by 2015
Early identification
Pathway planning
Treatment interventions
Community case management
An
act
ive
pat
hw
ay o
f in
terv
enti
on
The Pathway
PIPEs
Workforce development
WHAT: Case consultation & formulation
Workforce development
Additional resources to support Approved Premises Joint casework
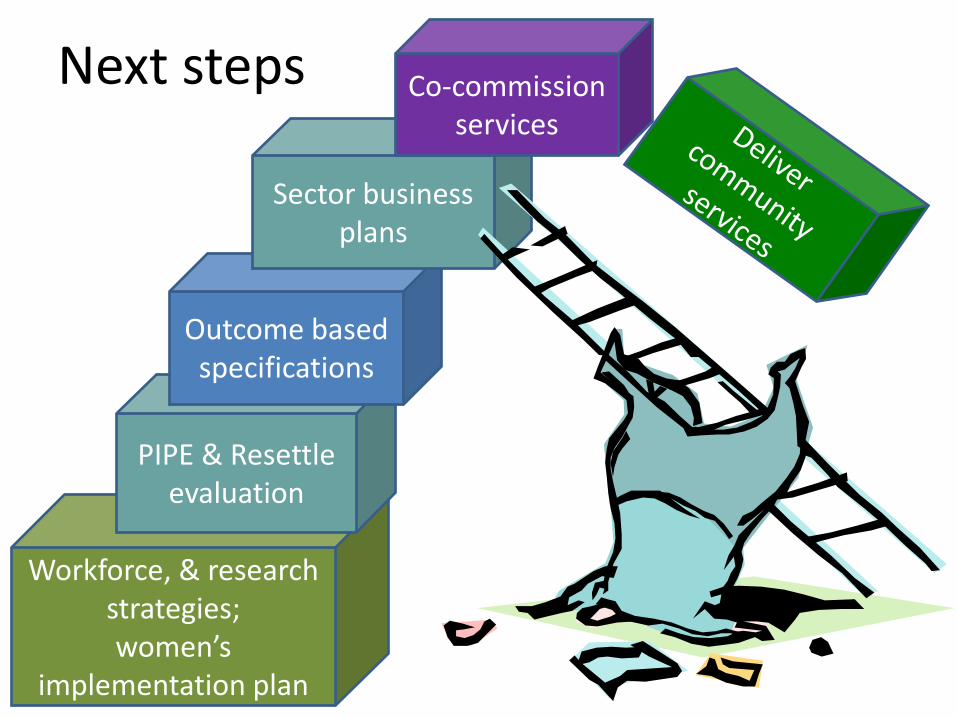
Next steps
Workforce, & research strategies; women’s
implementation plan
PIPE & Resettle evaluation
Outcome based specifications
Sector business plans
Co-commission services

Commissioning the community services specification
Objectives:
1. To enable selected trusts and health
providers to implement the service in one
or two LDUs (including APs) in order to
develop a localised approach for later roll
out
2. To deliver the community specification in
about 20 probation trusts in 2012/13
Key points
• Probation Trust & health provider(s) submit a
business case for consideration
• Nationally co-ordinated approach, but decisions
made in the sectors by co-commissioners
• 20 PTs, but 6 prioritised: (London, A&SPT,
Lancashire, Wales, S&WMPT, Northumberland)
• Clarity required for the process to select the
health provider
• Resources: £45-55k per LDU
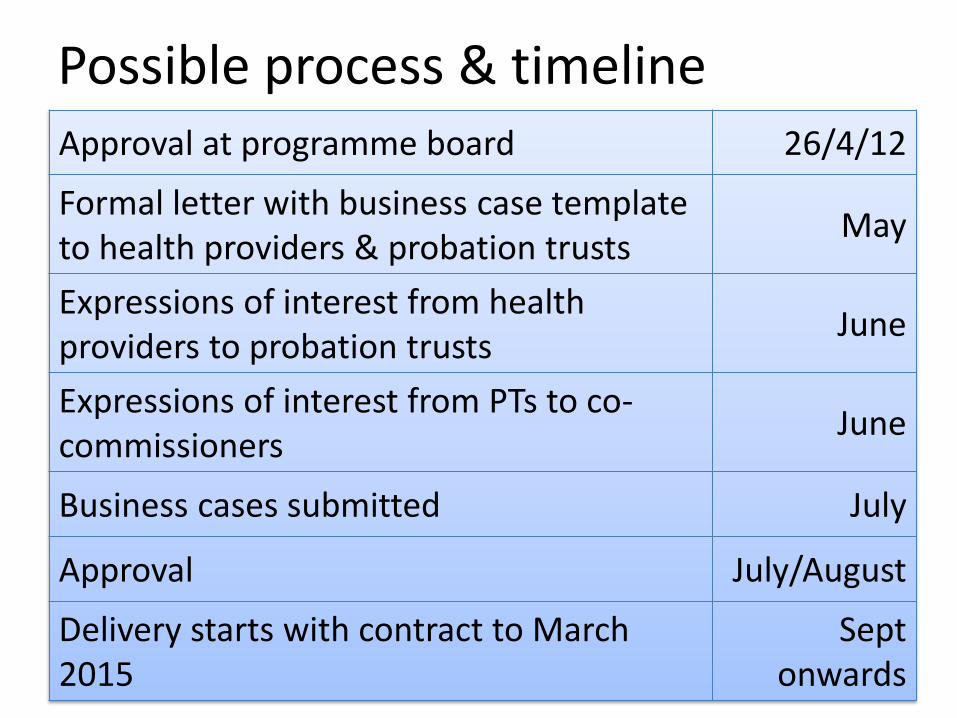
Possible process & timeline Approval at programme board 26/4/12
Formal letter with business case template to health providers & probation trusts
May
Expressions of interest from health providers to probation trusts
June
Expressions of interest from PTs to co-commissioners
June
Business cases submitted July
Approval July/August
Delivery starts with contract to March 2015
Sept onwards
Questions? Contact: [email protected]
Information: www.personalitydisorder.org.uk Department of Health/NOMS personality disorder
policy team
The London PD Pathway Project
Jackie Craissati
Why worry about PD offenders?
• PDO’s are more likely to – Commit an SFO
– Re-offend whilst on probation
– Drop out of accredited programmes
– Die of an overdose
– Get recalled
– Leave a hostel prematurely
– Stay in segregation and/or receive adjudications
– Make complaints
– Cause staff burnout
Basic premise
• Caseloads high (60)
• 50% will be PD (but not all high harm)
• Variable skills & training
• Assume an innate curiousity about what makes offenders do what they do
• Any intervention must be non-specialist (accessible)
• Any intervention must increase effectiveness AND reduce workload (efficient)
Resources
• 2 chartered psychologists (forensic & clinical)
• 1 assistant psychologist
• 1 laptop + statistical package
• 1 north London cluster (T Hamlets & Hackney)
• 1 south London cluster (Lambeth & S’wark)
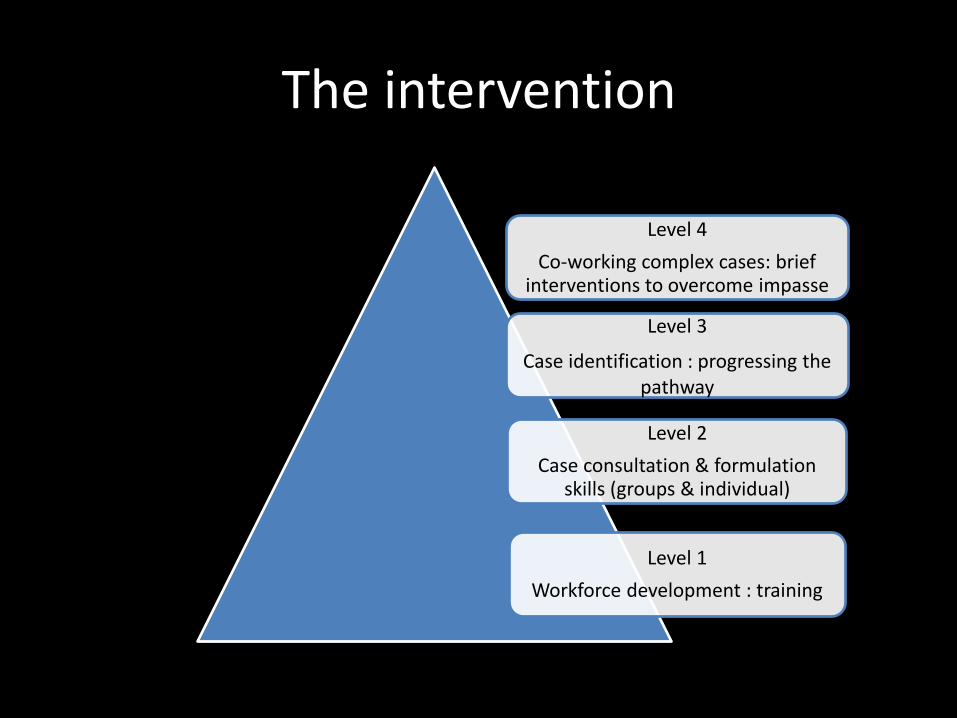
The intervention
Level 4
Co-working complex cases: brief interventions to overcome impasse
Level 3
Case identification : progressing the pathway
Level 2
Case consultation & formulation skills (groups & individual)
Level 1
Workforce development : training
Outcomes – workforce development
• Project succeeds or fails on basis of senior probation skills, confidence & support
• Staff significantly more knowledgeable & confident about PD and link to offending
• Little and often probably most effective
• Skills focussed most helpful
Outcomes – case consultation
• PO’s most in need, tend to avoid it
• Experienced as useful (as long as it doesn’t result in more work)
• Still learning to ‘take a history’ – the narrative approach
• Informal consultation as important as the planned group events (embedded in the office)
Outcomes – case identification
1. PO’s bring offenders who worry them Tend to over include low risk sex offenders and focuses on reactive (rather than proactive) anxieties
2. DSPD variables in OASys (10) Identifies a highly antisocial, prolific offending group, who may or may not have violent index offences
3. Flow chart (sex/violence + ISP + DSPD or childhood abuse)
Identifies a low frequency, high harm group
Outcomes – co-working
• 46% had contact with psychologists – Letter writing/Phone calls/Video conferencing/ Face to face
• 157 (46%) moved on pathway, & 31 entered prison/health therapeutic communities
• Those with contact significantly more likely to – Progress into appropriate treatment – Succeed when out in the community
The Camden & Islington Experience Impact Personality Disorder Project
Kate Smith Stuart John Chuan Acting ACO Camden & Islington LDU Forensic Psychologist
[email protected] [email protected]
PCA presentation Skipton House – London – 12 April 2012
Mission statement
To enable and empower frontline staff to work more effectively with offenders with PD
What we set out to do Mission statement
To enable and empower frontline staff to work more effectively with offenders with PD
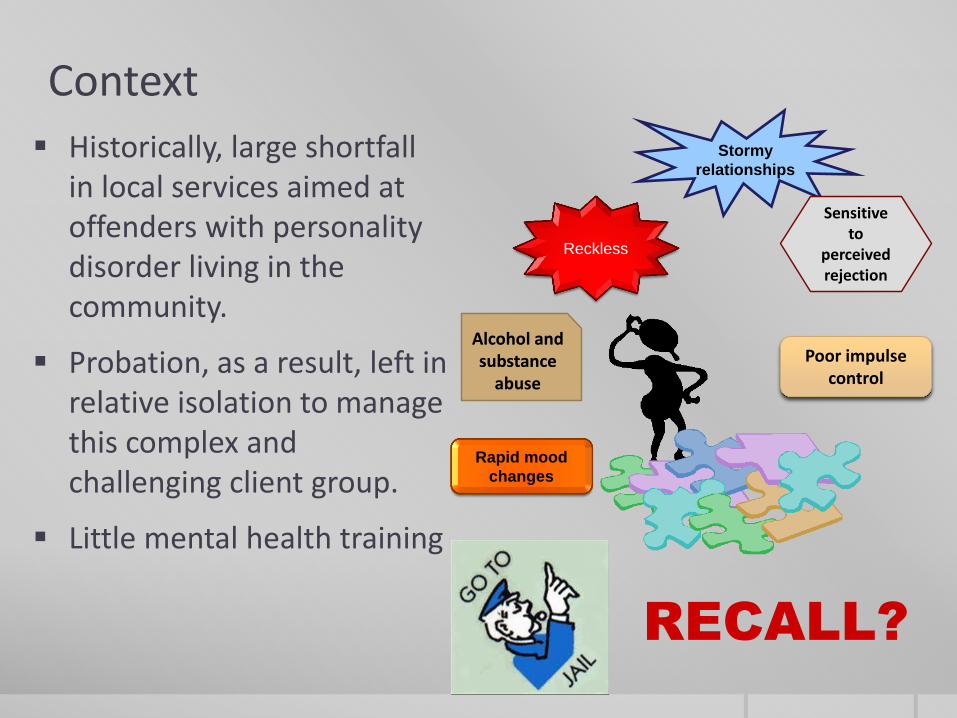
Context
Historically, large shortfall in local services aimed at offenders with personality disorder living in the community.
Probation, as a result, left in relative isolation to manage this complex and challenging client group.
Little mental health training
RECALL?
Stormy
relationships
Sensitive to
perceived rejection
Reckless
Poor impulse control
Alcohol and substance
abuse
Rapid mood
changes
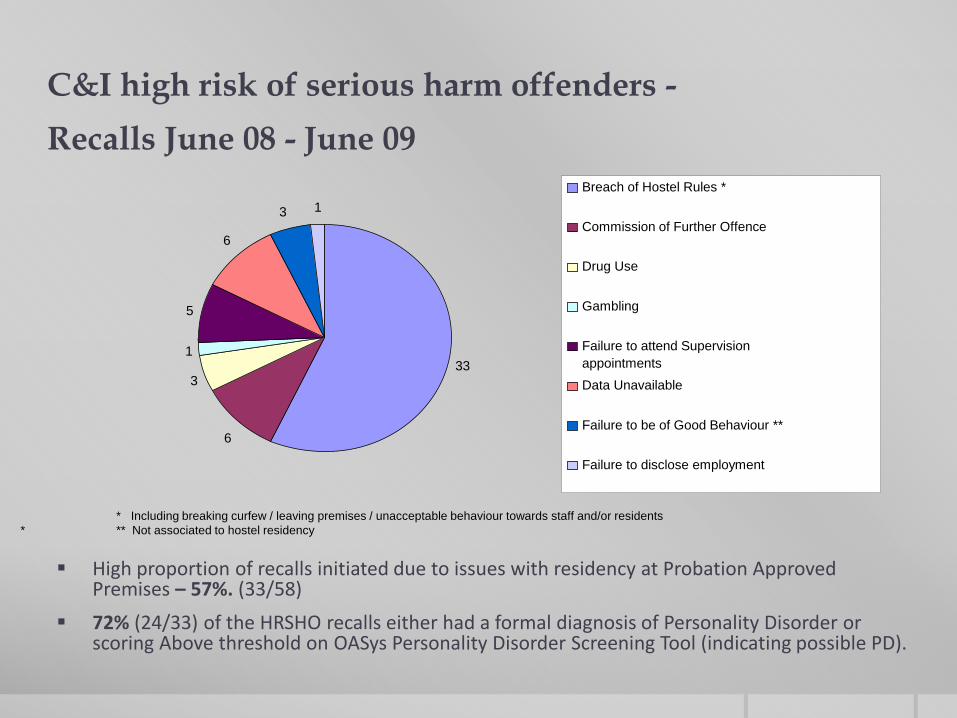
C&I high risk of serious harm offenders -
Recalls June 08 - June 09
High proportion of recalls initiated due to issues with residency at Probation Approved Premises – 57%. (33/58)
72% (24/33) of the HRSHO recalls either had a formal diagnosis of Personality Disorder or scoring Above threshold on OASys Personality Disorder Screening Tool (indicating possible PD).
33
6
3
1
5
6
3 1
Breach of Hostel Rules *
Commission of Further Offence
Drug Use
Gambling
Failure to attend Supervision
appointments
Data Unavailable
Failure to be of Good Behaviour **
Failure to disclose employment
* Including breaking curfew / leaving premises / unacceptable behaviour towards staff and/or residents
* ** Not associated to hostel residency
How we did it 1. Quick set-up
2. Economically viable
3. Sustainable benefits
1. Establish local need - OMs and AP staff
WHAT they wanted
Better understanding of PD (beyond diagnosis)
Better understanding of how to access Mental Health services
Tell me what to do
Help me with my emotional reactions
HOW can we help you?
Provide workforce with strategies that: - are relevant - can be used immediately - improving engagement - make use of existing community resources - focus on staff wellbeing
2. The Portfolio of Helping Interventions:
Strengthening Pathways to existing mainstream
services
THE TEAM Psychologist – case consultation; training, NHS translator Probation Officer Specialist – consultation, CJS translator Assistant Psychologist - evaluation Kate Smith – C&I Acting ACO Dr Win Bolton – C&I NHS Trust
A B C
D
Joint case working: a. Build credibility b. Demonstrate
approach
A. Upskilling examples
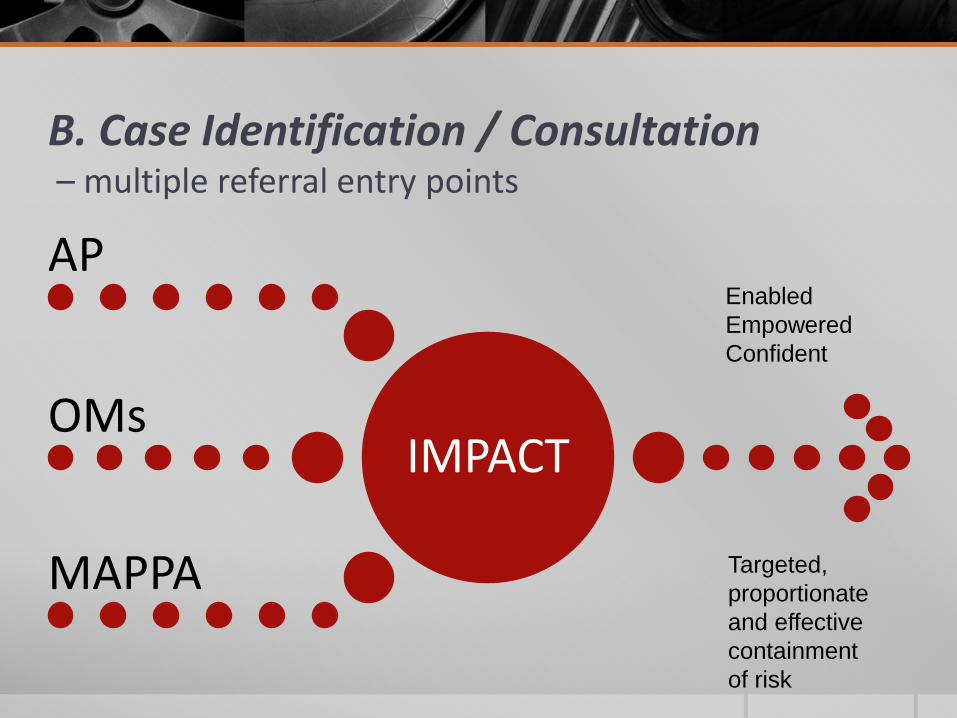
B. Case Identification / Consultation – multiple referral entry points
IMPACT
AP
OMs
MAPPA
Enabled
Empowered
Confident
Targeted,
proportionate
and effective
containment
of risk
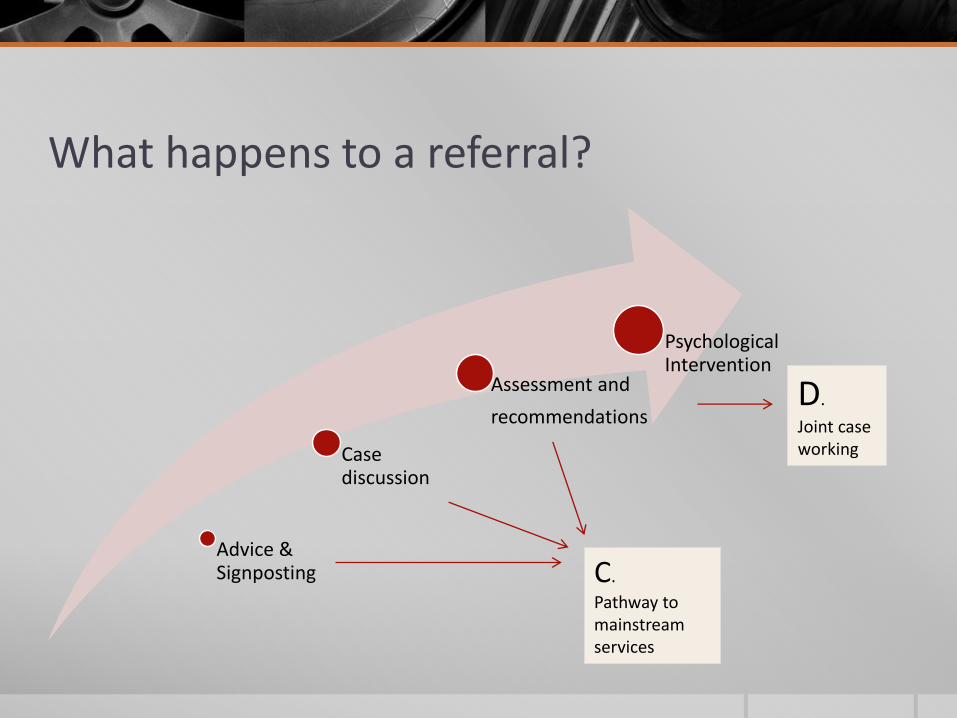
What happens to a referral?
Advice & Signposting
Case discussion
Assessment and
recommendations
Psychological Intervention
C.
Pathway to mainstream services
D.
Joint case working
Outcomes Can the delivery model enable and empower to work more effectively with PD?
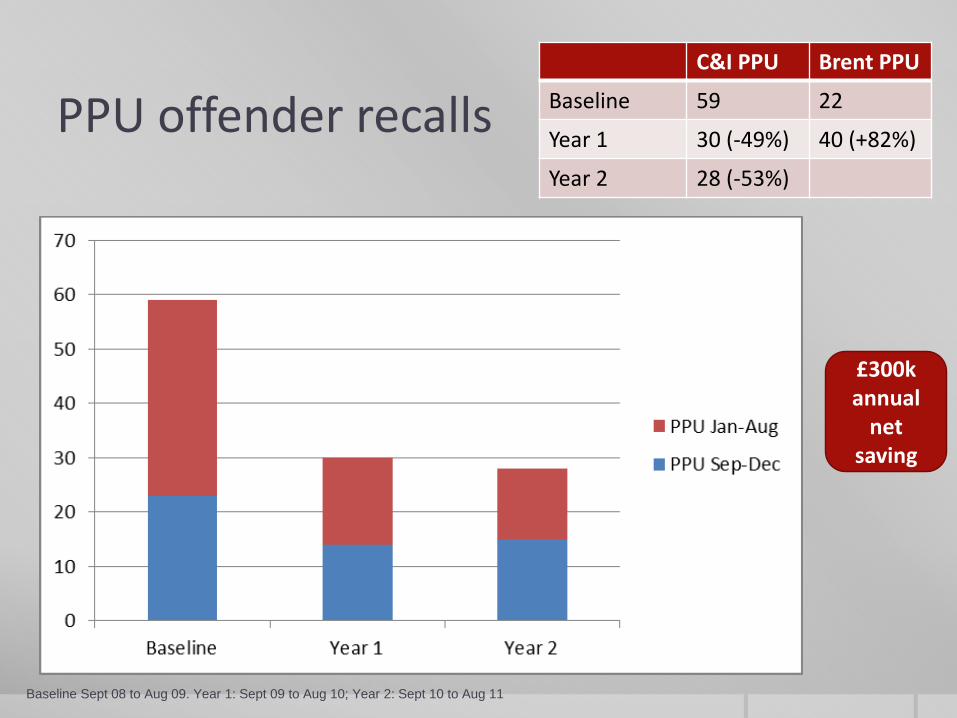
PPU offender recalls
Baseline Sept 08 to Aug 09. Year 1: Sept 09 to Aug 10; Year 2: Sept 10 to Aug 11
C&I PPU Brent PPU
Baseline 59 22
Year 1 30 (-49%) 40 (+82%)
Year 2 28 (-53%)
£300k annual
net saving
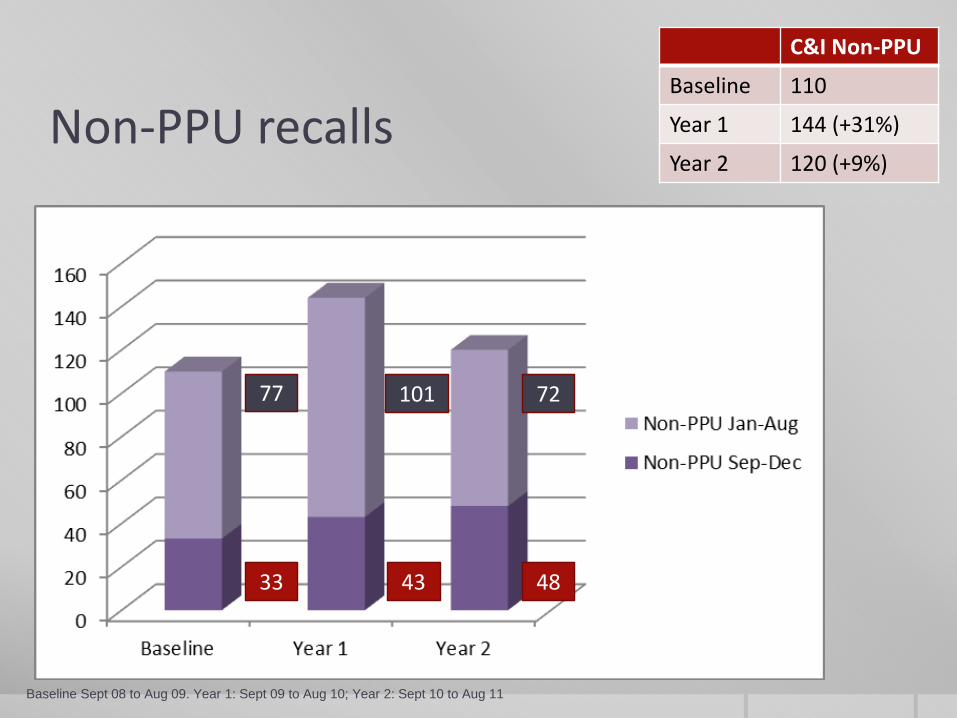
Non-PPU recalls
C&I Non-PPU
Baseline 110
Year 1 144 (+31%)
Year 2 120 (+9%)
Baseline Sept 08 to Aug 09. Year 1: Sept 09 to Aug 10; Year 2: Sept 10 to Aug 11
33 43 48
77 101 72
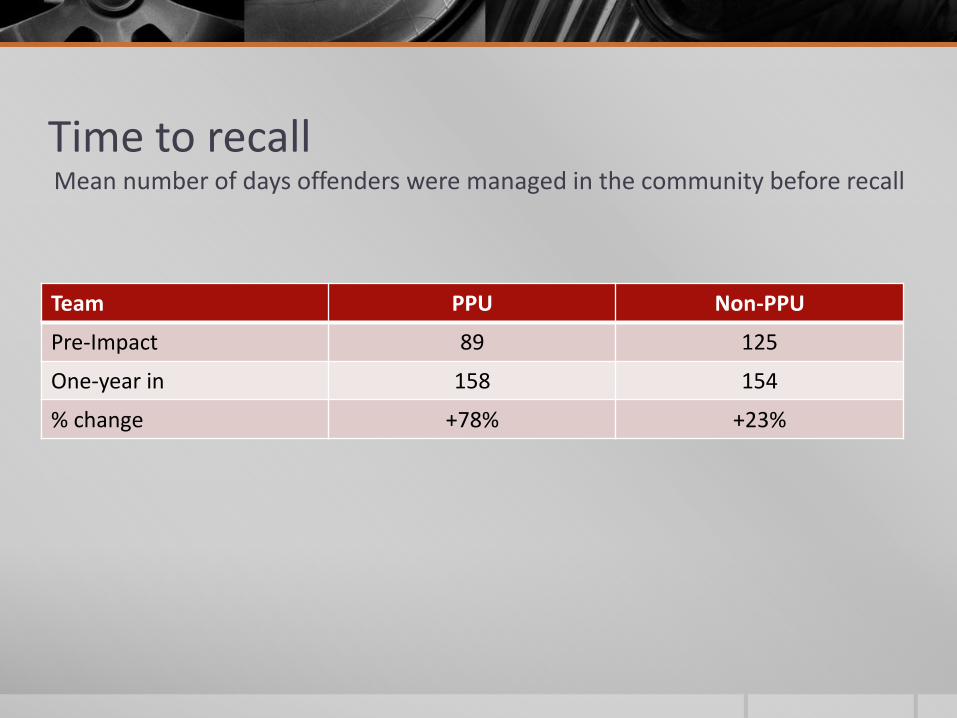
Time to recall Mean number of days offenders were managed in the community before recall
Team PPU Non-PPU
Pre-Impact 89 125
One-year in 158 154
% change +78% +23%
Training needs analysis PPU and the two APs
45 min semi-structured interviews (1-year follow-up)
“they are able to see things that I can’t see and
tell me how to work specifically with that
from a different perspective”
“When I was asked this before and I didn’t really understand it. I was like “well I can’t deal with those offenders cause they annoy me, they wind me up, they make me angry and I want to say something back to them.” Whereas now my experience is different cause I don’t take it personally. I can take a step back which stops me from getting so stressed out, it’s quite a big change for me”.
“it gives you more confidence, it relieves stress, and I think it makes you less likely to go off sick, because you are actually dealing with the stuff here and you feel capable whereas when you’re floundering in the dark it’s really scary … he is able to see things that I can’t see and tell me how to work specifically with that from a different perspective”.
KUF Training Feedback Post Training Questionnaires
“Very good. It is a surprise this training isn’t more widespread.
Good online support too.”
“Thought the training was excellent and will be useful when I’m working with all my cases.”
“It was a supportive and reflective space. It was non-judgemental and very interesting to hear everyone’s experiences.”
“A very empowering training. I think most practitioners who work directly with people should attend this course.”
Lessons learned from the Impact Project
Identify and respond sensitively to local needs but stick to your mission statement
Target intervention at staff – economical and sustainability
It’s better to identify and intervene early rather than crisis manage
Model a Probation/NHS partnership approach within team – if you can’t do it how can you expect that of local services
‘Treatment’ for PD is not the only option – think creatively to meet offender needs using community resources
Upskill managers too!
Introducing PIPEs
Psychologically
Informed
Planned
Environments
Introducing PIPEs
• Specifically designed environments
• Additional Staff Training
• Promoting a Psychological Understanding
• Focus on the ‘social’ environment
• Relationships and interactions.
• Maximise ordinary situations
• Psychologically Informed
PIPEs explained…
Psychologically Informed
• Training, support and supervision
• Understanding personality pathology
Planned
• Opportunities to practice/maintain gains made earlier in an offender’s sentence
• Support pathway and transition needs
Environment
• Enabling Environments
• Quality relationships and interactions
A pathway of progression
• Supporting Transition
• Facilitating ‘Progression’
• Bridging the Gap
• Provide a ‘Good enough’
and validating experience
• Not a treatment intervention
• Not exclusively for
Personality Disorder (PD)
Benefits – supporting outcomes
• Effective movement through a clear pathway of intervention
• Maintain, support and evidence improvements in risk of harm and risk of reoffending
• “Tested" Change in Individuals
• Recognised development of an ‘Enabling Environment’
• Career Development opportunities for staff
• Improved Staff/Offender Relationships
• Enhance the local range of services for offenders
• Improved Optimism in Staff, Offenders, Management
• Settled Prison / Hostel Environments
Evaluation of the model
Evaluative Field Test
• Four strands – experience, climate, risk, staff
• October 2012
Seven Progression Unit Pilots
• Leicestershire and Rutland Probation Trust
• Merseyside Probation Trust
• HMP Hull, Gartree and now Frankland
• HMP Low Newton and Send
Governance and Development
• Clinical Network / Structures / Support
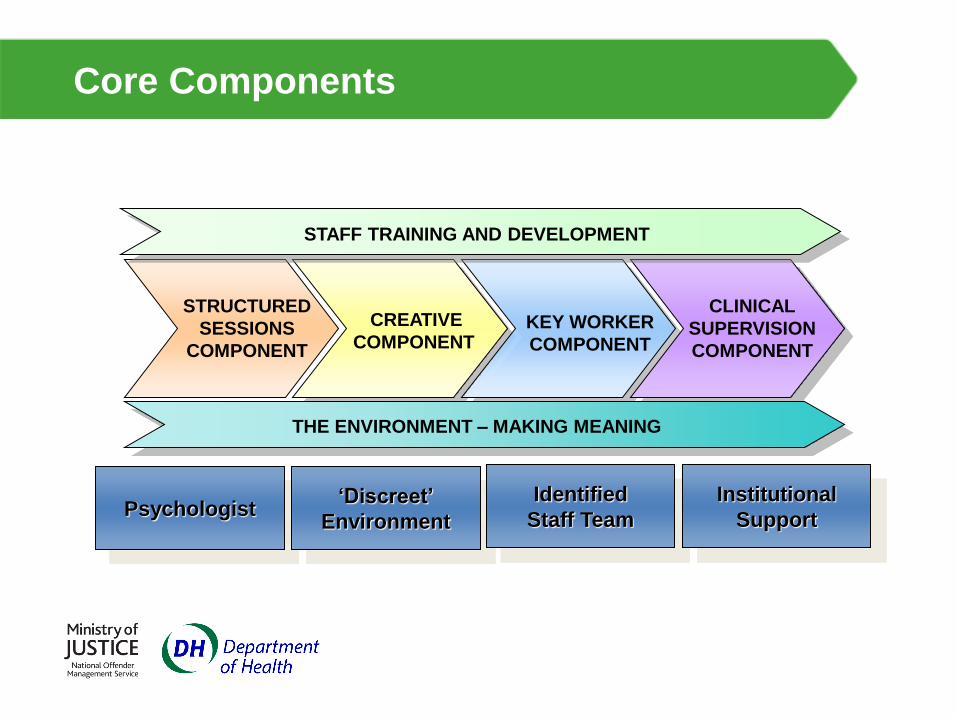
Core Components
STRUCTURED
SESSIONS
COMPONENT
CREATIVE
COMPONENT KEY WORKER
COMPONENT
CLINICAL
SUPERVISION
COMPONENT
THE ENVIRONMENT – MAKING MEANING
STAFF TRAINING AND DEVELOPMENT
Psychologist ‘Discreet’
Environment
Identified
Staff Team
Institutional
Support
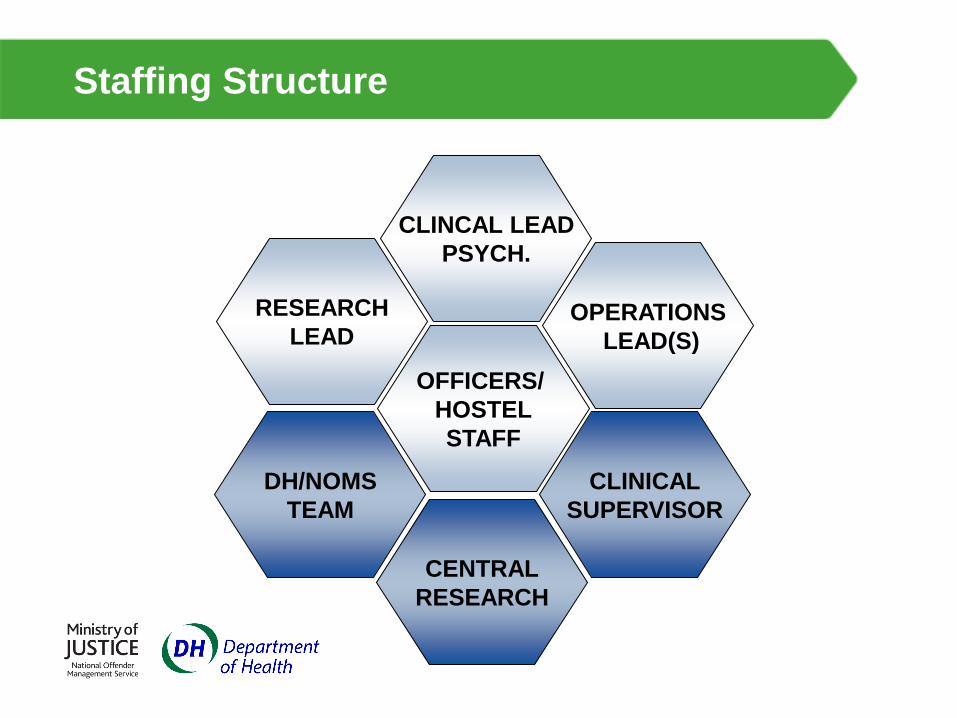
Staffing Structure
RESEARCH
LEAD
OFFICERS/
HOSTEL
STAFF
CLINCAL LEAD
PSYCH.
OPERATIONS
LEAD(S)
CLINICAL
SUPERVISOR
DH/NOMS
TEAM
CENTRAL
RESEARCH
Referral Criteria
Prison PIPE
• Completed high intensity offending behaviour programmes/intervention
• Has a minimum of 6 months to serve in custody
• Not currently suffering from active mental illness
• Not required an adapted treatment intervention
• Offence type – as per individual unit
Approved Premises PIPE
• Management of existing AP population
Some challenges
• Adapting and developing an existing culture
• Understanding Personality Disorder / Needs
• Developing knowledge, skills and attitudes
• Embedding into the host institution
• Awareness
Does PIPE work?
• The evaluation strategy hopes to provide some answers.
• But until then....
– Reduction to self-harm incidents
– Improvements in behaviour / stability
– Increased participation in hostel activity (e.g. Fairshare)
– Improved relationships between staff and residents
– Residents developing realistic plans for the future
– Staff say they feel more satisfied in their jobs. They feel like they are making a real difference.
...the observations are promising.
Summary
PIPEs:
• Facilitating a ‘good enough’ experience through a
structured and planned environment
• Maximising ‘ordinariness’, promoting pro-social living
• Supporting progression and transition
• Supporting staff to work with complex needs
• Supporting a system-wide offender pathway
65
Resettle : The Way Ahead?
Joint PCA / DH / NOMS Event
Commissioning Personality Disorder Services
12th April 2012
Diana Johnson
Service Director, Resettle
0151 494 4390
66
Aims of Resettle Pilot To establish whether co-ordinated community
psychosocial provision for personality
disordered offenders is effective in :
i) Reducing reoffending and social exclusion,
ii) Managing risk in the community and
iii) Enhancing the quality of lives of individuals.
UNCLASSIFIED
67
Resettle
• Jointly commissioned / funded / delivered
• Subject to Randomised Controlled Trial
Research
• MAPPA cases: adult males
• High risk of serious harm linked to violent /
sexual offending and P.D.
• Consent and high level commitment
68
Four stage approach
1. Prison in-reach work; both prior to release and, where appropriate, subsequent to recall;
2. Induction and intensive support on release; involving a range of other services;
3. Targetted and sequenced interventions, involving a multi modal approach;
4. Managed endings, with potential for ongoing support.
69
Good Lives
(Ward and Marina 2007)
• Healthy living
• Knowledge
• Excellence in work and play
• Excellence in agency (self management) Inner peace
• Relatedness (relating to others)
• Spirituality
• Creativity
70
Desistance
• Realistic: recognising that entrenched behaviours take a long time to change, lapses and relapses are to be expected and planned for
• Focus on strengths and resources: support positive potential
• Build positive relationships: which are valuing, respectful and supportive involving individuals, workers, families and social networks
• Respect individuality: each individual, their path into and out of offending, their goals and needs will be different: interventions need to reflect this
• Recognise the significance of social context: society and the individual offender need to see the potential for social reintegration and acceptance
• Promote motivation and hope: For the individual and their capacity for change and for the future. Encourage self-determination.
71
Resettle : Workforce Development
– A capacity to maintain boundaries whilst also being flexible and responsive
– Emotional maturity and personal resilience
– A capacity to empower the service user
– Maintenance of a positive attitude and an acceptance of what is (and is not) possible.
– Capacity for reflection and willingness to be open about uncertainties
– Capacity for team and shared working
– Positive and rewarding approaches are more likely to be effective in engaging and keeping people in services than negative and punitive ones.
72
Resettle : Resources
• Health and Criminal Justice staffing / skills
• Groupwork / individual work
• Therapeutic interventions and Risk Management integrated
• Crisis Line
• Resettle Plus
• Other contracted services to meet offending related needs
• Community reintegration
• Approved Premises
73
Resettle : some headline
information
• Resettle cases 49 (plus 12 referral post
RCT) : Control Group 33
• 21 Recalls : 15 for escalating risk (71%)
• 12 Re-Releases in 17 cases
• 1 case on 4th re-release
• 1 case 11 months in community
• 3 cases 18 months in community
74
Resettle : Some Lessons Learned
• Merits of investment in In-Reach
• Benefits to Risk Management of
integrating Case Formulation
• Strengths of multi-agency workforce skills
and perspectives
• Experience of Recalls and Re-Release
• Long term commitment by all : including
participants
75
Key Messages
• Benefits of Health / Criminal Justice collaboration at all levels
• Psychologically informed practice / risk management
• Complexity and challenge requires appropriate workforce expertise and support
• Enhanced risk assessment / management in multi agency setting
• Service User engagement in intensive programme

76
Think Pathway
• Shared population
• Early Identification and Assessment
• Community to community – and round again
• Enhanced services
• Resources for consultation and workforce development
• New Opportunities for authentic progression through a pathway.