Embed Size (px)
Citation preview

4 - The Origin of Atherosclerosis/V) c c r6p^'YI'he monoclon 1 hypothesis, which holds that the proliferating
I? r, i' c1 t ^ ^ ,. ii
i 3R
all stern from one inutated cell, I-v,cells of ai -a Ierosclerotic plaque
suggests new lines of research on the causeI 1s of coronary disease;^ I r0n`101- — _^; ^;,,dCJ it.,'.' fi r C' h Ghp^ !h 1 1''^ rGh Gy I/ GI 1,
i n C
by Earl P. Benditt /'c t' ) cj f
C
ardiovascular disease has becomet he major cause of death in the
U.S. and other Western countriesnot just because people are living longerbut because some unknown aspects ofmodern life are increasing the incidenceof atherosclerosis, the chronic arterialdisorder that is the major cause of heartattacks and strokes. We cannot identifythose aspects until we know the true na-ture of the characteristic atheroscleroticlesion. The atherosclerotic plaque, alumpy thickening of the arterial wall,narrows the passageway and initiatesthe formation of a blood clot that canultimately close down a critical artery.
In the past 15 years it has becomeclear that the plaque is characterizedby an ac umulation smooth-musclecells. The important question is: W y do
Tcells accumulate? Some of its nowthink the cells of a plaque are the proge-ny of a single mutated smooth-musclecell from near the site of the plaque. Ifthat is so, the plaque is comparable toa benign tumor of the artery wall. Andif it is comparable, then the search forinitiating factors should be directedtoward the genetic and environmentalfactors that cause mutation—the samekinds of agents and conditions thattransform cells and thus initiate cancers.Here I shall review the theories thathave governed thinking about athero-sclerosis until recently. Then I shall re-port some experiments that led to thenew single-cell hypothesis and the evi-dence that tends to confirm it, and dis-cuss some implications of the proposednew approach.
Aterics are conduits with a specializedcell composition and structure that
enable them to conduct blood underpulsing pressure and to maintain and re-pair themselves. The artery wall hasthree layers: the intima, the media andthe adventitia. Lining the inner surfaceof the intima is a single layer of endothe-lial cells, which hold the blood cellswithin the artery and modulate the pas-sage of water and other substances from
the blood plasma into the tissues. Thecomposition of the remainder of the in-ti ma varies. It may consist only of non-cellular connective-tissue fibers or itmay include cells, depending on the typeof artery and the age and sex of the indi-vidual; the intima of coronary arteriestends to be thicker in males than in fe-males, and the thickness and the numberof cells increase with age in both sexes.It is in the intima that atherosclerosishas its effect.
A prominent region of clastic tissuecalled the internal elastic membraneseparates the intima from the media, theartery's main supporting layer. The cellsof the media are smooth-muscle cells, sodesignated because their contractile fi-bers lack the striated pattern of skeletal-muscle cells. In elastic arteries such asthe aorta the cells of the media are ar-ranged in small groups that spiral be-tween the coarse elastic fibers support-ing the artery wall; arteries that supplyorgans, such as the coronary arteries,have a similar structure but less elastictissue and relatively more ce ll s. The Ii-brous proteins elastin and collagen andthe carbohydrates (glycosaminogly-cans) of the media are all secreted by thesmooth-muscle cells.
The outermost layer of the arterywall, the adventitia, is composed of thecells called fibroblasts and their associ-ated intercellular collagen and glycos-aminoglycans. The adventitia carriesthe blood vessels that nourish the outerlayers of the artery wall and also an-chors the wall to the surrounding tis-sL1eS.
Like any other tissue the arteries aresubject to various disease processes suchas the reaction to injuries and their re-pair, infections, inflammations and tu-mors. It has been difficult to categorizethese disease processes because many ofthem look alike in their end stages andone is able to examine the minute struc-ture of their lesions on only two occa-sions: at autopsy and, less frequently,during surgery. One can differentiateamong various disease processes either
by following their development fromtheir inception, examining tissue sam-ples with a microscope, or by lookingfor special features that distinguish oneprocess from another. That is done bystudying animal diseases that mimic hu-man ones. Much can be learned fromanimal models, but there is always thequestion of how well a particular modelparallels the similar process in humanbeings.
The characteristic lesions of athero-sclerosis. at least as they are seen at
autopsy, are the raised fibrous plaques.They appear (in the dissected, undis-tended vessel) as discrete lumps, elevat-ed above the unaffected regions of theintima and ranging in color from pearlygray to yellowish gray. The main cellu-lar component of the plaque is, as I haveindicated, a smooth-muscle cell verysimilar to the major cell of the normalartery wall-, macrophages and otherwhite blood cells also infiltrate theplaque's dense connective tissue, whichconsists largely of collagen fibers. Theplaque usually contains glycosamino-glycans and sometimes elastin and suchblood proteins as fibrinogen. Lipopro-teins, the carriers of cholesterol in the
blood, are found both inside and outsidecells. Deep in the lesions there are debrisfrom dead and dying cells and varyingamounts of lipids (fats); crystals of cho-lesterol can sometimes be seen evenwith the unaided eye in the softened de-bris in advanced lesions. It is this fattydebris that suggested the name athero-sclerosis, from the Greek athera (gruel)and sclerosis (hardening).
The atherosclerotic plaque can closedown an artery by itself, but more of-ten its harmful effect is to predisposethe artery to occlusion by thrombosis.which represents an aberration in thedelicately balanced blood-clotting sys-tem that is essential for temporarilypatching leaks and injuries in blood ves-sels. A thrombus is a complex aggrega-tion of blood platelets, white cells andred cells in a network of fibrin. the main
74

^i, f^. ap kslew^
p f i
i^ ^il, 1
11 j +tl ^.
A t E* l e -!,L^ ,,^,j
L!
.s tl . s7
I
r.^; •'t ,tl., x,^
,µ1I t ^(uFh^^
I ^,+ ix'h{`'^'y^
t , 4 y1
dI1'N
^.I^r `'yr ^,.
P
ATHEROSCLEROTIC PLAQUE narrows the lumen, or passage- THROMBUS that formed just downstream of the narrowing causedway, of a human coronary artery, enlarged 19 diameters in this pho- by an atherosclerotic plaque blocked a coronary artery, shutting offtomicrograph made by the author. The plaque is a thickening of the the blood flow to part of the heart muscle and leading to a fatal heartartery wall composed mainly of connective tissue and smooth-muscle attack. The darker regions of the thrombus are composed of red bloodcells, with a region of cellular and fatty debris (lighter gray areas). cells and (lie lighter regions contain white blood cells and platelets.
ATHEROSCLEROTIC INNER SURFACE of an artery is seen at man-aorta segment that has been slit open. The plaques are seen toabout two and a half times natural size in this photograph of a hu- be discrete lumps that bulge into the lumen of the dissected artery.
75

COLLAGEN FIBERS ANDTISSUE CARBOHYDRATES
(II
ARTERY WALL is built up of several layers, whose precise composition varies with the par -ticular artery. A segment of a major etaslic artery of the type of the human aorta is diagrammed.
clotting protein. Thrombosis is commonin the veins of the leg, but for a throm-bus to form in the rapidly flowing blood-stream of an artery it appears that spe-cial conditions are required: either aslowing of the flow or a region of turbu-lence in it; injury to the inner lining ofthe vessel, causing platelets to stick to it,and perhaps increased stickiness of theplatelets themselves. Such conditionsmay be found on the downstream side ofa plaque, where there is a region of tur-bulence and sometimes an ulcerated en-dothelial surface. Platelets stick to thesurface and aggregate into a mass thatappears to successively recruit whiteblood cells, initiate the formation of fi-brin from fibrinogen in the plasma andthen recruit more platelets as well asred cells. The layered mass thus builtup may remain a relatively flat muralthrombus or may grow to become anoccluding thrombus that blocks the pas-sage of blood.
The theories that have guided the in-vestigation of atherosclerosis until re-cently are versions of two basic ap-proaches with origins in the 19th centu-ry. The dominant theory is associatedwith the German pathologist RudolfVirchow. It holds that the infiltration offatty substances from the bloodstreaminto the artery wall gives rise to depositsof cholesterol that act as an irritant.causing inflammation and the prolifer-ation of cells. This insudation theorywould appear to be supported by theincreased rate of coronary heart diseaseamong people with higher than normallevels of cholesterol in their blood. Ele-vated cholesterol levels have in turnbeen correlated geographically withdiets that are high in food fats and cho-lesterol, a finding that has given rise toefforts to prevent atherosclerosis by reg-ulating the diet. The insudation theoryseemed to be further reinforced by theexperiments of the Russian investigatorN. N. Anitschkow early in this century.He found that a disease resembling hu-man atherosclerosis could be producedin rabbits by adding egg yolks or cho-lesterol to their diet and hence raisingtheir blood levels of fat and cholesterol.In the experimental rabbit disease, itshould be noted, the lipids appear in thelesions early and can be shown to arisefrom the blood lipids. The rabbit modeland its data have strongly influencedinvestigators' perceptions of the humandisease.
The fact that autopsies of infants andyoung children show small fatty depos-its in the major blood vessels has givenfurther credence to the lipid-insudationtheory. It has also led people to assumethat the natural history of atherosclero-sis involves an evolution from the fattystreaks of childhood to the fully devel-oped fibrous plaques of the adult dis-ease. The trouble with such an assump-tion is that the fatty streaks appear to be
76

PLAQUE IN THE AORTA is further enlarged to 60 diameters and slained for cell nuclei(blue) and fat (orange). The cap is clearly composed of many cells embedded in an unstainedfibrous matrix. The debris includes cells that contain fat and, below them, extracellular fat.
SMOOTH-MUSCLECELLS
CELLS WITH FATTY •
DEGENERATION ,'I
DEBRIS
MEDIA
( I present to about the same extent in chil-LUMENJ dren of all populations, whereas adult
- INTIMAy
' atherosclerosis is rare in some popula-f r '
tions and common in others.Y^ ; ;^ ^`^^^`a^
rThe other basic concept of the origin
"^ t '^i of atherosclerosis, the encrustation the-u ^ I x ' f' ory, holds that the plaque begins with a
t , f ^ r y: PLAQUE
^`"^^? small mural thrombus that is converted
into a mass of tissue in the intima asg` r;' Y arterial-wall cells migrate to it, multipl
and then secrete the characteristic extra-'C cellular substances. Localized injuries
• to the arterial wall in experimental ani-
^` ADVENTITIA mall lead to a repair process of that
C r y kind, and substances that pass from the
CROSS SECTION OF PLAQUE in a human coronary artery is enlarged 24 diameters in plasma into the wall, along with debris
this photomicrograph, which is mapped at the right. The roughly oval atherosclerotic plaque, from dead and disintegrating elements
stained pink, is a thickening in the intima of the artery. The next layer is the media, stained of the thrombus, do cause such experi-
brownish black. The outer layer, the adventitia, contains connective collagen and fatty tissue, mental lesions to resemble atheroscle-rotic plaques in many ways- It is postulat-ed that in human atherosclerosis suchlesions grow large enough to obstruct anartery as the result of repeated episodes
}: r
--_ FIBROUS CAP of injury, each followed by the repara-
r
^tive clotting, migration and secretion.
^"„ Ideas about the nature and origin oatherosclerosis began to change when
x7'^^ k s the electron microscope revealed the
DEBRIS cellular composition of the plaque. Thefibrous, cellular cap covering the choles-terol-rich debris turned out not to con-tain ordinary fibroblasts, the cells that
MEDIA proliferate to heal a skin wound, butrather to contain month-m cle cellssimilar to those of the normal artery
4 wall. Then it was discovered that in its; , , early stages the human plaque does not
”"t ADVENTITIAcontain much lipid, which implied that
t 1,3 . r y
+, ^ li insudation is not the ri mar initi-idlipid primaryst+
+F y nisi E ', ' c ating factor. By now the major current
\', •: theories of the genesis of atherosclero-sis share the belief that the lesions beginas localized exces sive aecltmulati ns of
PORTION OF PLAQUE in the human aorta is enlarged 27 diameters, The fibrous cap of smooth-muscle cells in the intima. Thethe plaque, a mass of cells embedded in a matrix of collagen and other extracellular material, eurrenT—Ice is a O^b u^l1l initiatesis underlain by debris. The plaque is elevated above the adjacent intimal surface of the vessel, those accumulations and what makes
them grow.
Ater having worked with various ani-mal models of atherosclerosis in
our laboratory at the University ofWashington School of Medicine andhaving found them unsatisfactory, in19671 began, along with Ned S. Moss, tostudy atherosclerosis in chickens. Thatwas the animal in which Ruth Pick, Jere-miah Stamler and Louis N. Katz of theMichael Reese Hospital had discoveredthat the development of fatty lesions inchicken blood vessels after cholesterolfeeding could be prevented by treatmentwith a form of the female hormone es-trogen; their finding had led to trialsin which estrogen was administered t o
some male coronary patients in an effortto prevent a second occlusion. Moss andI fed cholesterol and administered es-trogen to chickens and examined theirvessels with the electron microscope.We found, first of all, that the lesionsthat cholesterol induced in the chickensdid not resemble human atherosclerotic
78

1 " • - 7 g - s..
CELLULAR NATURE of an early atherosclerotic plaque is dem-onstrated in this photomicrograph. A section of the media and the
E
3^. .r+ i. a;^h;6l,;d.y n 5x W
,S1^f) M b ^'}^uµi^^^::'. .^ .tY.' 7 Ct f .L R . J
^ i,•, ^GtSX^jd f i%^+. ^` ^ -.^ ^f- . , '^' y, ^^ ' ,',P i t.;,.^ "..rya .
flu• `. _ :. LY• d • O&..J._-., ^ ... .t.. ...
INDIVIDUAL CELLS of plaques appear in these electron micro-graphs made by Ned S. Moss. Cells from the base of an early lesion ina chicken artery are enlarged 15,000 diameters (top). Collagen fibers
COLLAGEN CELL MEMBRANE
DENSE-`;1300[ES
MYOFIBRILS
NUCLEOLUS
NUCLEUS s L•, - =
COLLAGEN
are seen head on and from the side, running between smooth-musclecells. A single smooth-muscle cell is enlarged 40,000 diameters ina micrograph of a plaque from a human coronary artery (bottom).
79

LUMEN
ENDOTHELIUM
INTIMA SMOOTH-MUSCLE CELLS
MEDIA INTERNAL ELASTIC LAMINA
- "1
GENESIS OF A PLAQUE as proposed by the monoclonal hypothe-sis is traced in these highly schematic drawings. The process beginsin the inner media. There are two cell types. A single cell (dark color)has undergone a mutation that gives it a selective advantage, andsome stimulus causes the mutated cell to divide (1). Its daughter cellmigrates into the intima (2). The progeny of the mutated cell, having
DAUGHTER CELL
O> j
a selective advantage and perhaps somehow freed of sonic curl) onproliferation, continue to multiply, thickening the intima (3, 4) andeventually forming a lumpy plaque (5) all of whose cells are progenyof the original cell that mutated. The last drawing (h) shows, by wayof contrast, a polyclonal plaque, which is the kind that would arisefrom the migration and proliferation of many cells of both cell types.

plaques. They appeared to be composedentirely of fat-fill ells derived fromblood macr es; there was cs-f ignificant smooth-muscle-cellproliferation. And none of the lesionsevo vc into the raised plaques char_ac-teristic of the ht an disease! We found,n the other hand, t at tSickens that
were not given cholesterol developed anarterial disease whose lesions did bear it
striking resemblance to the plaques ofhuman coronary atherosclerosis. Acttt-ally this naturally occurring disease ofchickens had been well described in theliterature of comparative pathology,but we had all tended to ignore it whenour attention was focused on the experi-mental disease produced by cholesterol.
Now we were able to observe theearliest stages of plaque formation inyoung, untreated chickens. The first signof a naturally occurring plaque was asmall group of cells in the intima, whichis normally populated by only an occa-sional cell. As we reconstructed the se-quence of events, one cell or possibly afew cells migrated from the media, pro-liferated and slowly gave rise to a massof cells in the intima. There was no evi-dence of cholesterol deposits in theseearly lesions. Degenerated and deadcells, intercellular debris and cholester-ol deposits did, however, appear in thelater stages. Why? What was the precisesource and nature of the cells that popu-lated the plaque? What initiated theirproliferation and what caused the con-tinued multiplication and degenerationthat produced the fully developed fi-brous plaque?
We noted that the cells of the earlyspontaneous plaque were subtly differ-ent from normal artery-wall cells. Theywere arrayed differently, they appearedto be smaller and to have few or no in-tercellular junctions, and in contrast tothe normal cells of the media they man-ufactu 11 ^raThUijnsoolini p an of e astin. Moreover, the early le-stons deve ope fatty vacuoles (cavities)when the chickens were on cholesterol:nearby normal artery-wall cells did notdevelop such vacuoles. Perhaps somemetabolic change stemming from themovement of the cells to a new locationwas responsible for the various differ-ences between artery-wall and plaquecells in chickens.
We decided next to see for ourselvesjust what the cells of a normal arterywall look like in the course of injury andrepair. John Poole (who was visiting ourlaboratory from the University of Ox-ford), Stephen Cromwell and I simulat-ed an injury by putting a fine suture inthe artery wall. A thrombus formedaround the part of the loop that was inthe flowing bloodstream, and smooth-muscle cells migrated from the mediainto the thrombus, where they multi-plied. These cells that populated the
0
CHOLESTEROL CRYSTALS DEGENERATING CELLS
ULCERATIONI ^ I
FAT j am' ^P^ *•^® \
ADVANCED MONOCLONAL PLAQUE is often ulcerated at the surface where endothelialand smooth-muscle cells hale died. The interior is filled with fat ty debris, the result of celldeath and degeneration as well as of migration of cholesterol and lipoproteins into the plaque.
thrombus had all the characteristics cells arise in response to injury or some(apart from some positional distortions) other stimulus, the stimulus would pre-of the normal smooth muscle cells of sumably have its effect on many normalthe media, including the formation of cells at many places, in which case theelastin and the development of inter- plaque cells should be polyclonal. Thecellular junctions. In other words, they question—monoclonal or polyclonal—iswere in sharp cont r ast to the modified susceptible to experimental testing insmooth-muscle cells we had seen in the humans by a genetic technique.spontaneous lesions in chickens. The technique, originally applied by
the geneticist A. H. Sturtevant to theWjjje realized then that various forms study of tissue development in fruit flies.W of the insudation-irritation theo- is based on the fact that an individual
rics had continued to dominate think- animal may be a "mosaic" composed ofing about the cellular proliferation ob- t wo distinguishable cell populations. Asserved in plaques. At one time it had Mary P. Lyon of the Medical Researchbeen assumed that the cells were wound- Council Radiobiology Unit at I-larwell,healing fibroblasts. and this fitted the England, first postulated, this is true ofidea of a response to irritation. Then all human females. In female cells thereelectron microscopy had revealed that are two X chromosomes, one derivedthe cells were smooth niusc!e cells, not from the father and one from the moth-fibroblasts, and yet no (ne had seriously er, only one of which is active in adultquestioned that the Its were there in cells: the other is inactivated early inresponse to some hint of irritation, embryonic development and remains in~T^c stuc y of tbt spt r.t,!ncous esions the nucleus as a dense bit of chromatinand the suture -induce ! '.c'ions empha- known as the Barr body. The inactiva-sized the unusual nat.u'e of the sponta- tion in any one cell is apparently ran-neous-plaque cells and ;'aintecl to one of dom, so that either the maternal Xchro-two origins for them: T hey could come mosome or the paternal one may remainfrom some small cell l r opulat i on that is active in a given cell and in a ll the proge-present but not oidu-.aril y observed in ny of that cell. If there is a "marker''the normal media and is caused to pro- gene, such as one for a particular en-liferate by a stimulant of some kind, per- zyme, in the maternal chromosome thathays one connected s itli injury, or they is different from the corresponding genecould be smooth muscle cells that have in the paternal chromosome, one canbeen altered by mutation. If they
are
distinguish between cell populations ingenetically altered cclls. then the cells of which one or the other chromosome isa given plaque would he expected to be active. There are several such poly-monoclonal: to have hcen derived, like morphic genes on the X chromosome.the cells of a benign tumor, from a single One of them codes for the enzyme glu-mutated cell. If. however. the plaque cosc-6-phosphate dchydrogenase (G-G-
81

MIXED CELLPOPULATION —+
A
B A
ALL B CELLS
I'.
B
ALL A CELLS-l-
A
ELECTROPHORE1'IC PATTERN reveals the presence of two cell populations with twoenzyme types. Enzyme solutions applied to a membrane migrate across it (arrmed) under the in-Iluence of an electric current. After 50 minutes the position of the enzyme hands is visualized( j r) by allowing the enzyme to react with its substrate, precipitating a dye. The presence oftwo separate bands shows there are two enzyme types; a photometric scan of the bands (blackcurie') allows one to estimate the proportions of the two enzyme types and thus of the cell types.
PD), and its two forms code for two ma-jor enzyme types that can be distin-guished by electrophoresis: when sub-jected to an electric field, one type (A)moves faster than the other type (B).
As in the well-known case of the sick-le-cell hemoglobin trait, a subset of theA type of G-6-PD confers resistance tomalaria and is relatively common in theU.S. black population, which originatedin malarious areas of Africa and contin-ued to live for a long time in malariousareas of the U.S. About 40 percent ofblack females are heterozygous for theG-6-PD gene, that is, some of their cellscarry each of the two enzyme types. R.G. Davidson. 1-1. M. Nitowsky and Bar-ton Childs of the Johns Hopkins Univer-sity School of Medicine capitalized onthe presence of the two enzyme types toestablish the fact that once a particularX chromosome is inactivated in a hu-man cell it remains inactivated. Theycultured bits of skin from black womenwho had the two enzyme types. The fi-broblast populations that grew in cul-ture manufactured both enzymes, show-ing that the cells were of both types.When the investigators isolated singlecells from the mixed population andcultu red them, however, each clone (theprogeny of a single cell) exhibited onlyone enzyme type. A or B; repeated sub-culturing of cells from a single clonecontinued to yield the same enzymetype. With the stability of the two cellpopulations' enzyme production thusestablished, it became possible to turnthe process around: to analyze extractsof tissue samples for their G-6-PD com-position by electrophoresis. and so todetermine their cell mixture. For exam-
plc. at the University of WashingtonSchool of Medicine. David Linder andStanley M. Gartler examined tumors ofuterine smooth muscle and found thateach tumor was of one cell type: PhilipJ. Fialkow and others extended the stud-ies to leukemia and other tumors.
In1973 we applied this analytic tech-nique to atherosclerotic plaques and
normal artery-wall tissue from vesselsobtained at autopsy. The first case yield-ed 15 plaques that could be analyzed.Four produced only the A type of theenzyme and eight produced only the Btype: three showed a mixed cell popula-tion. On the other hand, of 27 artery-wall samples that did not exhibit lesions,25 had a rather even mixture of the twotypes of cells. (The two samples with asingle enzyme pattern may have con-tained small plaques. but we could notbe sure.) Analysis of more cases boreout those first exciting findings: it wasclear that an atherosclerotic plaque fre-quently consists of cells of just one type.In 1975 nearly identical results were re-ported, based on a larger number ofcases, by T. A. Pearson. A. Wang, KimSolez and Robert I-I. 1-leptinstall ofthe Johns Hopkins School of Medicine.Similar results continue to be obtainedas the observations are extended in theselaboratories and in others- I shouldpoint out that it is not surprising thatsome atherosclerotic lesions appear notto be monoclonal. since several sour-ces of normally mixed cell populationsmay be in or close to a plaque. for ex-ample contaminating blood cells or in-growths of adjacent artery-wall con-nective tissue. Indeed. I had expected
that blood-cell contamination might pre-vent our seeing any clear distinctions,and the data were therefore surprisinglyunequivocal.
Before one can interpret the presenceof only one cell type in a particular cellgrowth in a mosaic organism as be-ing evidence of monoclonal origin, how-ever, several issues need to be settled.First, one must establish that the size ofthe patches of cells of one type that canbe found in normal tissue (patches thatare presumably the result of accidentsof cell growth and mixing during theformation of the embryo) is very smallcompared with the size of the putativelymonoclonal growth. We did this by tak-ing more than 1.000 samples of thesmallest possible size from the innerportions of normal artery walls and ana-lyzing the statistical variation in theircell populations. Our data suggest thatthe volume of a patch of cells of onlyone enzyme type in normal tissue isabout a ten-thousandth of a cubic milli-meter. which probably means it con-tains about 10 cells. A typical plaque, incontrast, has it volume of many cubicmillimeters.
Second. one must exclude the possi-bility that the usual proliferative re-sponse seen in healing processes stemsfrom a single cell. There are severalindications that such is not the case.Wounds are quite generally observed toheal by the simultaneous proliferationof cells all around the periphery; morespecifically, we found that many cellsaround a small injury to the aorta ofexperimental animals divided simulta-neously. Moreover, examination of thethickened intima seen in middle-agedand elderly people, which is thought tobe the result of repeated small injuries.reveals that the thickened areas arecomposed of mixed cell populations.
Some investigators have held that thepresence of just one cell type in athero-sclerotic plaques may be due to someprocess that favors the proliferation ofone of the two cell types present in amosaic individual. The fact that we reg-ularly find both lesions composed oftype-A cells and lesions composed oftype-B cells in the same individual in-dicates. however, that neither enzymetype is producing a selective advantageor disadvantage.
It seems reasonable to consider the sin-gle-cell plaque as being monoclonal
in origin and to propose that some eventprovides a single cell with an advantageover its neighbors, and that the progenyof that altered cell dominates an ensuingprocess of normal replacement multipli-cation or some kind of stimulated multi-plication. The commonly accepted rea-son for the appearance of such a selec-tive advantage in a body cell is an altera-tion in its genetic apparatus: a mutation.We have proposed that there are threestages in the pathogenesis of athero-
82

000
LI 1 200
cr,
ra
nIi
100
so
w
H60 ww
HzwHz
zz
H0)
20
40
—20 20 40 60 80MIGRATION (MILLIMETERS)
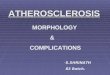
POTENTIAL MUI'AGENS are carried in the blood by the same blood proteins that carrychole
sterol. The black curve shows the electrophoretic pattern of lipoproteins in human bloodserum; the peaks at the left represent the chylomicrons and the low-density lipoproteins. Ra-dioactively labeled cholesterol dissolved in serum migrated mainly with those lipoproteins (col-or bars). A radioactive sample of the premutagen methylcholanthrene migrated in the samelipoproteins (hatching in bars) as cholesterol, lipoproteins known to move to cells of artery wall.
sclerosis. First comes an initiation stageduring which there is mutation in an ar-tery-wall cell. Then some factors or con-ditions promote the expression of theselective proliferative advantage con-ferred by the mutation, enlarging themass of cells: the mutation, in otherwords, may never be expressed as grossplaque formation unless something pro-motes cell multiplication and gives thealtered cells an opportunity to expresstheir altered capability for growth. Fi-nally, there is the stage of complication:the tendency of cells to degenerate andof lesions composed of those cells tobreak down and ulcerate is compatiblewith the presence of an altered cell pop-ulation.
If this general proposal is correct, oneought to consider as causes of athero-sclerosis the conditions and factors thatcause mutation or facilitate the ex-pression of advantageous mutations.Among the possible initiating factorsare intrinsic genetic ones that lead toexcessive mutations and such extrinsicones as chemical mutagens, viruses andpossibly ionizing radiation. The factorsthat might promote the subsequent de-velopment of atherosclerotic plaquesare those that promote cell multiplica-tion, such as certain chemical or physi-cal injuries. The possible causes of thethird stage, plaque degeneration, are notat all clear yet.
The primary value of the monoclonalhypothesis is that it provides a newframework within which one can asknew questions about the role of variousrisk factors. Cigarette smoking, dietaryhabits, changes in blood lipids (of genet-ic or dietary origin) and hypertension(high blood pressure) have all been im-plicated as contributing to the rising in-cidence of coronary disease and strokes.How does cigarette smoking, for exam-ple, tit into the monoclonal hypothesis?
The burning of cigarettes manufac-tures chemical substances that are
known to be precursors of mutagens;among them are the aryl hydrocarbons,such as benzpyrene and methylcholan-threne. The fact that the enzyme arylhydrocarbon hydroxylase, which con-verts these premutagens into mutagens,is induced (produced in extra amounts)in the liver and other tissues when thesubstances are administered shows thatthey are taken up by the blood and car-ried through the body. In what bloodelements are these noxious substancescarried? We have shown by electropho-resis that they are carried in the low-density and very-low-density lipopro-teins, the same fraction of the blood-protein spectrum in which cholesterol iscarried. It has also been noted that thehigher the concentration of lipoproteinsin the blood is, the more aryl hydro-carbons the blood will carry. Where dothe aryl hydrocarbons go'? Workers inseveral laboratories have established
that blood lipoproteins seem to be par-ticularly good nutrients for culturingsmooth-muscle cells from the humanartery wall. Mont Juchau, James Bondand I have found that the aryl hydrocar-bon hydroxylase enzyme system is pres-ent in the artery wall of rabbits, mon-keys and human beings—and that thesystem in the wall is induced, or turnedon, by aryl hydrocarbons.
What all of this means is that artery-wall cells are capable of converting intomutagens certain premutagenic sub-stances that come from the environmentand are transported to the cells by bloodlipoproteins. Does that happen and doesit cause atherosclerosis? Roy E. Albertand Martin Vanderlaan and their col-leagues at the New York UniversitySchool of Medicine administered twoknown mutagens, benzpyrene and di-methylbenzanthracene, to chickens. Themutagens gave rise to marked increasesin the number of plaques in the aortaand in the rate at which the plaques de-veloped, and they did so without therebeing any increase in the blood level ofcholesterol. The mechanism of plaque
formation in the chickens has not beenreconstructed, but the results are con-sistent with the monoclonal hypothesis.
Cholesterol, the centerpiece of the in-sudation theory, may also be found to fitthe monoclonal hypothesis. M. F. Gray,T. D. V. Lawrie and C. J. W. Brooks ofthe University of Glasgow noted thepresence of an epoxide derivative ofcholesterol in human blood serum andfound that the epoxide's level was ele-vated in people with high blood choles-terol. Cholesterol epoxide is known tobe able to produce connective-tissue tu-mors in mice and rats. Perhaps it isbecause epoxides or other substancesformed in the body from cholesterol aremutagens that cholesterol levels corre-late with the incidence of coronary dis-ease. Clearly it would be interesting tolook for evidence of mulagens in theblood serum of populations that havehigh and low risks of atherosclerosis.We have begun to do that, working withthe bacterial mutagen-screening systemdeveloped by Bruce N. Ames of theUniversity of California at Berkeley.There are also mammalian-cell-culture
83

00C0C_
rtwaz0
OU
OCrwUz
UwH
IF-Qw0
15
10
systems by means of which one can (indsubstances that are injurious to DNA,the genetic material, and hence likely tobe mutagenic for animal cells.
High blood pressure, which is knownto increase the risk of atheroscle-
rosis, may do so by exerting a chemicalor even hydrodynamic effect that makesartery-wall cells multiply faster; in ourlaboratory Stephen Schwartz is trying toidentify some such mechanism. Recent-ly R. W. Pero and his colleagues at theUniversity of Lund in Sweden foundthat the DNA of people with hyperten-sion is more susceptible to breakage incells by mutagens than the DNA of peo-ple with normal blood pressure. Thisfinding seems to conform with evidencethat the incidence of cancer is higher inindividuals with hypertension. Is it pos-sible that there are subsets of the humanpopulation with an increased propensityfor mutation in particular tissues, suchas the artery wall? An increased poten-tial for mutation, if it is combined withexposure to substances in the environ-ment that enhance the rate of muta-tion, could lead to a higher incidenceof plaque formation.
The epidemiologist Ernest L. Wynderhas pointed out an association on a geo-graphical basis between the death ratesfor cancer of the colon and for arterio-sclerotic heart disease [see illustrationabove]. Presumably there are either en-vironmental or genetic factors, or both,that effect such an association. A con-nection has been established between atleast one dietary factor and cancer aswell as atherosclerosis: breast-cancerrates have been found to be closely cor-related worldwide with dietary fat in-take, a correlation not unlike that foundfor deaths from heart disease.
I have alluded to therapeutic trials ofestrogens for preventing recurrent heartattacks in men. They were undertakenon the basis of experimental evidence inchickens and of the well-known obser-vation that before menopause womenhave fewer heart attacks and less ath-erosclerosis than men, whereas aftermenopause the incidence in women ofboth coronary disease and atherosclero-sis rises. When estrogen was tested inmen in a large and carefully designedstudy, the Coronary Drug Project, nooverall positive therapeutic effect of es-trogen could be discerned. On the con-
trary, the overall death rate for the mengiven estrogen was somewhat higherthan that for the control group, and sothe treatment was discontinued. The es-trogen group also showed an increasedincidence of cancer. The monoclonaltheory suggests a possible explanationfor these effects of estrogen.
Some of the chickens to which Mossand I administered the potent syntheticestrogen diethylstilbestrol developed tu-mors of the lymphatic system, an effectthat had been observed earlier. The ath-erosclerotic plaques also appeared to beworse in the diethylstilbestrol animals.And in the smooth-muscle cells of theplaques and artery wall of one of themwe discovered virus particles, some-thing we had not seen in a great manysamples from many animals not treatedwith estrogen. In some of the earlier ex-periments at Michael Reese Hospitalit had been noted that a combinationof cholesterol feeding and estrogen ad-ministration caused the spontaneousplaques of chickens to ulcerate. It is wellknown that diethylstilbestrol can rapid-ly elicit the proliferation of latent tumorviruses in mice. These various observa-tions suggest that the activation of latent
20
Q SCOTLAND
NORTH IRELANDCANADA
0 00DENMARK U.S. (WHITE)
0 0 0 0 AUSTRALIAENGLAND AND WALES NEW ZEALAND
BELGIUM
AUSTRIA SWEDENU.S. (NONWHITE) 0
SWITZERLAND0 SOUTH AFRICA
0 NETHERLANDS
WEST GERMANY 0 NORWAY0
0 ITALY0 ISRAEL
FINLAND 0
0 JAPAN
50 100 150 200 250 300
DEATH RATE, ARTERIOSCLEROTIC HEART DISEASE (PER 100,000)
CORRELATION between the death rates for cancer of the colon arrangement of points on this scatter chart, suggests that cancer and
and for arteriosclerotic heart disease, indicated by the roughly linear atherosclerosis are likely to have some causative factors in common.
84

,c.
viruses may be a possible mechanism bywhich some of the complications of hu-man atherosclerosis are induced.
The idea that atherosclerotic plaquesmay be some form of neoplasm, or
abnormally proliferating tissue, is quitestartling if one's concept of a neoplasmis limited to malignant cancers, whichspread. Many tumors, however, are be-nign: they remain localized. grow slowlyand may even regress. As a matter offact, a current concept of how cancersoriginate postulates that several succes-sive mutational steps are required be-fore extreme loss of control allows thetumor to spread [see "The Cancer Prob-lem." by John Cairns: SCIEN rir-Hc AMER-ICAN, November, 1975]: it appears thatmany more cells may undergo the firstchanges toward neoplasia than have upto now been considered. And even asmall potential of cells for enhancedgrowth would obviously have more seri-ous consequences in the narrow confinesof an artery than, say, in the skin.
New information is emerging aboutthe biology of the artery wall and itscells that should make it possible to trn-derstand how such loss of control maycome about. At the University of Wash-ington School of Medicine. Russell Rossand John A. Glomset and their co-work-ers have found a protein in blood plate-lets that promotes the multiplication ofarterial smooth-muscle cells and othercells in culture; it seems to have a role instimulating cell proliferation to repairan injury. One can envision the possibili-ty that a step in the evolution of an ath-erosclerotic plaque is the loss by a cell ofthe need for this protein. so that the celland its progeny divide when they shouldnot and thus produce the mass of theplaque. Pursuing a different line of re-search, George M. Martin in our depart-ment has been studying the aging in cul-ture of cells from animal and humanartery walls. Cells from different arter-ies age at different rates; cells from seg-ments of the aorta that are more proneto atherosclerosis tend to age more rap-idly. This may be an important clue towhat determines the unequal distribu-tion of atherosclerotic plaques through-out the arterial system.
The multifactorial nature of athero-sclerosis and its complications is evi-dent. The monoclonal hypothesis doesnot immediately simplify the problemof identifying the causes of heart attacksand strokes. What it does do, I believe, isto enrich the information and the ideasthat are available to investigators. Itthereby puts us in a much better positionfrom which to consider, test and identifythe multiple factors, genetic and envi-ronmental. that are responsible for thecurrent epidemic of these diseases,which not only shorten human life butalso impair its quality in our steadilyaging population.
' IMPOATYO
^:^: - I t<USHNI J