Embed Size (px)
Citation preview

INTRODUCTIONOrthodontic temporary anchorage devices (OrthoTADs™), andminiscrew implants (MSIs) in particular, have gained acceptancerapidly in the past few years in orthodontics. MSIs provide a costeffective means of overcoming traditional anchorage limitationswithout sacrificing quality results while providing minimal riskto the patient. Moreover, because of their simplicity andflexibility in use, many orthodontists have begun placing MSIsthemselves in their own offices. The Imtec Ortho Implant® offersespecially unique features making it applicable for most anyorthodontic case.
IMTEC ORTHO IMPLANTThe Ortho Implant® (IMTEC Corp., Ardmore, Oklahoma) is arecently developed miniscrew implant (MSI) designed forenhancing orthodontic anchorage. Simplicity of use andintegration into the daily orthodontic practice were the primarygoals when designing the Ortho Implant. With those goals inmind, only one head design and one diameter with three differentlengths were chosen. Three different lengths are necessary tofacilitate placement in different locations within the oral cavitybased on gingival thickness and bony depth. The smalldimensions allow placement in a wide variety of intraorallocations, which permits stable anchorage in the treatment ofmany different malocclusions. Placement and removal of theOrtho Implant is technically easy and can be accomplished bythe orthodontist, and in most instances, without injections orpilot holes.
Threaded Body
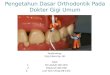
The threaded body was designed with a sharp tip so that it isdrill-free, thereby eliminating the necessity of a pilot hole. Inlieu of a thread-cutting cutting flute, the apical 4 mm of theOrtho Implant is tapered from 0.1 mm to the full 1.8 mm (Fig. 1)so that bone is compressed in and around the screw threads
during thread-forming instead of the cutting and removing ofbone common with other self-tapping screws. The outerdiameter is 1.8 mm with a core diameter of 1.6 mm. Threethreaded lengths are available: 6, 8, and 10 mm. The surface ismachine-polished to prevent osseointegration but allow bone apposition.
Transmucosal Collar
The transmucosal collar is 1.0 mm tall. The surface is highlypolished to allow intimate gingival adaptation, thereby creatinga seal between the oral cavity and the underlying bone.
The Ortho Implant Using the Cope PlacementProtocol™: Big Results From a Tiny Implantby Jason Bryan Cope, D.D.S., Ph.D.
Jason B. Cope received his dental training at Baylor College of Dentistry - DDS (‘95), orthodontic certificate (‘97), and PhD(‘99) in distraction osteogenesis. Upon completion of his orthodontic certificate, he was invited to join the department as anadjunct clinical assistant professor.
During his career, Dr. Cope has published 18 refereed journal articles, 34 book chapters, a research handbook, and co-editeda 600-page textbook on distraction osteogenesis. In addition, he has given over 100 lectures nationally and internationally. Dr. Cope is an ad hoc reviewer for the American Journal of Orthodontics, the World Journal of Orthodontics, The AngleOrthodontist, the Journal of Clinical Orthodontics, and was the guest editor for the March 2005 issue of Seminars InOrthodontics on OrthoTADs. Currently, he is writing a textbook OrthoTADs: The Clinical Guide and Atlas. Dr. Cope’s privatepractice is located in University Park, Texas, where he treats patients 4 days a week. In March 2002, he passed the AmericanBoard of Orthodontics exam, becoming the first person to complete ABO Option 2, and one of the youngest orthodontistsever to become a Diplomate. In July 2004, he presented his scientific paper to become a full member of the SW componentof the Edward H. Angle Society of Orthodontists.
Figure 1: IMTEC Ortho Implant
1

Abutment Head
The abutment head of the Ortho Implant is designed more like adental implant than a miniscrew and is placed into bone byapplying seating force to the square head, which is 1.5 mm tall.The grooved neck and O-Ball combined are 2.4 mm tall. Two0.75-mm (0.030-inch) holes in the O-Ball are oriented at 90degrees to each other and perpendicular to the long axis of thescrew. The Ortho Implant can be attached to either through theholes in the O-Ball or around the grooved neck. The O-Ball headmakes the system universally adaptable; it serves as onecomponent in a ball and socket joint, the other being the Ortho Cap.
Ortho Cap
The Ortho Cap (O-Cap) is a stainless steel abutment componentwith an internal O-ring that locks in place around the O-Ball(Fig. 2). The O-Cap can be placed and removed with little effortbut is stable enough that a patient cannot inadvertently dislodgeit. If the clinical situation warrants, the O-Cap can be placed tosuppress the soft tissues and prevent mucosal overgrowth, asituation not uncommon with other MSI systems. A groove islocated around the circumference of the O-Cap so that ligatures,elastics, or power chain can be attached directly to the O-Cap.And because the O-Cap is made of stainless steel, it can besoldered to, thereby allowing different attachments to be fabricated.
SURGICAL PROCEDUREThe surgical procedure is as follows (Cope Placement Protocol™):
1. Patient brushes teeth without fluoridated toothpaste.
2. Patient rinses with 15 mL of 0.12% chlorhexidinegluconate for 30 seconds.
3. Apply Oraqix® anesthetic topically.
4. Apply local anesthetic (optional).
5. Determine the Ortho Implant insertion site.
6. Perform bone sounding with periodontal probe to measuresoft tissue thickness.
7. Determine Ortho Implant length based on both soft tissueand bone thicknesses.
8. Place punch incision with 1.5-mm soft tissue biopsy punch(alveolar mucosa only).
9. Place pilot notch with No. 2 round bur or pilot hole with1.1-mm pilot drill bit (optional).
10. Insert Ortho Implant with O-Driver or contra-angle LT-Driver.
11. Place O-Cap to prevent soft tissue overgrowth (optional).
12. Load Ortho Implant immediately either by attaching to O-Cap or directly to implant head.
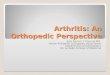
ORTHODONTIC MECHANICSAfter placement, the Ortho Implant can be loaded immediately.There is no need to wait days or even weeks to load for softtissue or bony healing. Attachment mechanics can be placeddirectly through the 0.030-inch holes (Fig. 3A), around theOrtho Implant neck (Fig. 3B), around a cotter pin placed throughthe 0.030-inch holes (Fig. 3C), around the groove in the O-Capif placed (Fig. 3D), or to attachments soldered to the O-Cap (Fig. 3E). Postoperative pain is negligible, and at most 400-800mg of ibuprofen is administered. Postoperative antibiotics forprophylactic reasons are not necessary unless the patientotherwise would be covered under the American HeartAssociation guidelines.
Ortho Implants can be used to overcome anchorage limitationsin several different case categories. Moreover, they can also beused to increase treatment efficiency (decrease total treatment
Figures 3A-E: Methods of attachment. A, Directly through the0.030-inch holes. B, Around the implant neck. C, Around a cotter pin placed through the 0.030-inch holes. D, Around the groove in O-Cap. E, To soldered O-Caps.
Figure 2: Ortho Cap forplacement around the O-Ball head.
3A
3B 3C
3D 3E
2

time) in cases that can be treated by traditional orthodonticmechanics. Several different examples of OrthoTADs™
treatment mechanics are illustrated below.
Anterior Retraction
Maximum anchorage is a primary indication of MSIs inpremolar extraction cases. When maximum retraction of theanterior segment is desired, the Ortho Implant can be placedlaterally in the alveolar ridge mesial to the first molar (Fig. 4).Locking closed coil springs are placed around the head of the O-Ball so that it does not have to be ligated and the patient cannotinadvertently dislodge it.
Arch Distalization
Mechanics to distalize the entire arch for avoiding extractionsand/or correcting buccal segment relationships can be designedeither to pull or push the arch distally. In pulling mechanics theimplants must be placed posteriorly so that ample distance existsfor active mechanics (Fig. 5A). In pushing mechanics theimplants must be placed more anteriorly (Fig. 5B).
Posterior Protraction
Ortho Implants used for protraction require additionalconsideration. In these situations, a full-sized rectangularstainless steel arch wire (rounded posteriorly to ease slidingmechanics) is used. In addition, the force should pass throughthe center of resistance on the facial, and a light force should alsobe applied on the lingual (Fig. 6). The lingual force is notnecessarily for protraction but simply to minimize any rotationaltendency and decrease friction.
Molar Uprighting
Traditional orthodontic mechanics for uprighting mesially tippedmolars usually cause relative extrusion of molars and placingthem in traumatic occlusion with the opposing molars. In thesecases, the Ortho Implant is placed distal to the tipped molar andin line with the central fossa (Fig. 7). The molar is pulled distallyand intruded simultaneously, thereby preventing extrusion.
Molar Intrusion
For supererupted teeth, molar intrusion is relatively simple. AnOrtho Implant can be placed on both the facial and palatalsurfaces or just on the facial surface (Fig. 8). The reason it ispossible to place an Ortho Implant on the facial surface only isbecause of the additional root surface area of the molars.
Incisor Intrusion
Although anterior bite opening is possible with traditionalmechanics using reverse curve of Spee wires, bite openingusually takes upward of 8-12 months, unless bite openingauxiliaries are bonded to the molars or incisors. The OrthoImplant can be used in these cases to open the bite in less thanhalf the time, thereby allowing lower bonding sooner (Fig. 9).
Figure 4A-B: Anterior en masse retraction. A, Buccal photograph atinitial placement and loading. B, Buccal photograph after 6 months ofloading. Note the new locking closed coil spring that does not requireligation and locks in place over the Ortho Implant so that it cannot bedislodged by the patient. (Courtesy Dr. Jason B. Cope, Dallas, Tex.Patent pending.)
4A 4B
Figure 5A-B: Arch distalization. A, Occlusal photograph of pullingmechanics. B, Occlusal photograph of pushing mechanics.
5A 5B
Figure 6A-D: Posterior protraction. A, Buccal photograph at initialOrtho Implant placement and loading. B, Buccal photograph after 2 months of loading. C, Occlusal photograph at initial Ortho Implantplacement and loading. D, Occlusal photograph after 2 months of loading.
6C 6D
Figure 7A-7C: Molar uprighting. A, Pretreatment occlusalphotograph. Note third molars were extracted. B, Ortho Implantlocation in line with central fossa. C, Progress occlusal photographafter 5 months of molar uprighting.
7A 7B 7C
6A 6B

Excerpted from Cope JB, Herman RJ. The Ortho Implant System.In: Cope JB, ed. OrthoTADs: The Clinical Guide and Atlas. UnderDog Media, LP, Dallas, In Press, April 2006, with permission fromUnder Dog Media, LP, www.orthotads.com.
Figure 8A-B: Molar intrusion. A, Buccal photograph of OrthoImplant at initial loading. B, Buccal photograph of Ortho Implant after7 months of loading. Note overintrusion of first and second molars(Photographs taken in maximum intercuspation).
8A 8B
Figure 9A-D: Incisor intrusion. A, Anteriorphotograph at initial Ortho Implant placement andloading. B, Anterolateral photograph at initial OrthoImplant placement and loading. C, Anteriorphotograph after 5 months of loading allowing lowerbracket placement. D, Anterolateral photographafter 5 months of loading.
9A 9B
9C 9D
10A 10B
10C 10D
Figure 10: Posterior intrusion using palatalmechanics. A, Anterior photograph at initial OrthoImplant placement and loading. B, Anterolateralphotograph at initial Ortho Implant placement andloading. C, Occlusal photograph of Ortho Implantlocation and attachment mechanics. D, Close-upphotograph of Ortho Implant location and attachmentmechanics (Courtesy Dr. Jason B. Cope, Dallas, Tex.Patent pending). E, Anterior photograph after 3months of loading. F, Anterolateral photograph after 3months of loading. Note that the overbite has closedand overjet decreased due to autorotation.
10E 10F
Posterior Intrusion
Perhaps the best location for MSI placement in hyperdivergentskeletal open bite case being treated by dental intrusion is in thepalatal bone, but only if the patient does not have a narrowintermolar width. These patients characteristically have a highpalatal vault such that placement of an MSI at the junction of thepalatal bone and palatal alveolar ridge is high enough forintrusion mechanics (Fig. 10). Moreover, these patients usuallyhave hanging lingual cusps that need more intrusion than thefacial cusps.
REMOVAL PROCEDUREOrtho Implant removal is indicated after its use for anchorageand tooth movement is complete. Ortho Implant removal occurswithout topical or local anesthetic by simply unscrewing theOrtho Implant. No pain is associated with the Ortho Implantremoval; therefore, analgesics are not indicated.
Reprinted from Orthodontic Perspectives Vol. XIII No. 1.© 2006 3M. All rights reserved.














![[Ortho] 106Quiz](https://img.pdfslide.net/doc/110x75/55cf860e550346484b93d4c4/ortho-106quiz.jpg)