Embed Size (px)
Citation preview
Dedicated to Respiratory Health Care www.pulmonarypaper.org • Volume 22, Number 1
PaperThePulmonary
January/February 2011
MedicareChangesTax Time HelpAlso inside:
Calling Dr. Bauer
Sharing the Health
MedicareChangesTax Time HelpAlso inside:
Calling Dr. Bauer
Sharing the Health
contents
“Imagination is the beginning of creation.You imagine what you desire, you will what you imagine
and at last you create what you will.”– George Bernard Shaw
Imagination is a powerful thing. Twentyyears ago, we could only imagine that
we could go shopping, run a business,talk face to face, or find a date from ourown homes using a computer. Millionsof you are now using the Internet toconnect with others for support and tolearn about lung problems.
Imagine we can solve the main cause ofChronic Obstructive Lung Disease.There are an estimated 46 millionsmokers in the United States. The realityis cigarette and tobacco tax revenuessupplied our 50 states with over 16.5billion dollars in 2008 (according to theUrban Institute-Brookings InstitutionTax Policy Center). Imagine we could geta smidgeon of that revenue for researchor figure out a way for states to balancebudgets without cigarette money. It onlytakes one person’s imagination to makereality happen!
www.pulmonarypaper.org Volume 22, Number 1
346789
Sharing the Health
Traveling NewsTSA Tips
Get Up & Go2 CruisesMake some memories!
Flu News
2010 Tax Deductions
Respiratory NewsLatest researchinformation!
101213141516
COPD Is Now Number Threein Cause of Deaths in US
Medicare Changesin 2011
Calling Dr. Bauer …Thoracentesis explained
Alternative to SpirivaNews on Smoking
Ask Mark …Purchasing an oximeter
Fibrosis FileIPF medication and newsStart your exercise routine!
Dedicated to Respiratory Care
Volume 22, No. 1January/February 2011
On the cover: Carolyn Blackwell ofTexas does not let lung problemskeep her home!
The Pulmonary PaperPO Box 877Ormond Beach, FL 32175Phone: 800-950-3698Email: [email protected]
The Pulmonary Paper is a 501(c)(3)not-for-profit corporation supportedby individual gifts.Your donation istax deductible to the extent allowedby law.
All rights to The Pulmonary Paper(ISSN 1047-9708) are reserved andcontents are not to be reproducedwithout permission.
As we cannot assume responsibility,please contact your physician beforechanging your treatment schedule.
PaperThePulmonary
The Pulmonary Paper StaffEditorCeleste Belyea, RN, RRT, AE-CAssociate EditorDominic Coppolo, RRT, AE-CMedical DirectorMichael Bauer, MD
The Pulmonary Paper is a member-ship publication. It is published sixtimes a year for those with breathingproblems and health professionals.The editor encourages readers tosubmit information about programs,equipment, tips, or services.
Phone: 800-950-3698Fax: 386-673-7501www.pulmonarypaper.org
John Lennon’s Imagine in Central Park.Imagine evokes a vision and hope for aworld without strife, war and conflict. Itcan also mean whatever we want it to be!

January/February 2011 www.pulmonarypaper.org 3
A Race We Do Not Want To Win!
It wasn’t supposed to happen until 2020, butChronic Obstructive Lung Disease (COPD) is now thethird leading cause of death in the United States. The
Centers for Disease Control released a report, “Deaths:Preliminary Data for 2008,” confirming that COPDbecame the third leading cause of death in theUnited States for 2008. The report states that themortality rates are the result of chronic lower respiratorydiseases (CLRD), such as chronic bronchitis, emphy-sema and bronchiectasis, which increased by 7.8 percent.The report notes that the increase could be due to a changein rules governing the coding and classification ofdeaths in 2008. Before the change, many deaths that werepreviously assigned to COPD/unspecified, pneumonia andother acute lower respiratory infections are nowclassified under CLRD.
Experts agree COPD and its related conditions havenot experienced the same decrease we have seen inmortality rates for heart disease, cancer and stroke.(Mortality rates for stroke fell 3.8 percent.) There is a needfor additional resources to target COPD research andinterventions.
“It’s unacceptablethat COPD has gonefrom fourth to the thirdleading cause 12 yearssooner than originallyprojected,” says John W.Walsh, president andco-founder of the COPDFoundation. “This in-tensifies our declarationof war on COPD andpoints to the importanceof increased awareness, prevention, detection and treat-ment to reduce the burden of COPD.”
“COPD is almost always preventable and almostalways treatable, but in order to treat it, it must bediagnosed,” says Byron Thomashow, M.D. With asimple test, individuals experiencing the symptoms ofCOPD (including breathlessness, wheezing and chroniccoughing) can take action to prevent the worsening ofsymptoms. Those of us that have been diagnosed can takealso take action to prevent COPD from moving upanother notch!
Cooking with COPDAdvance for Respiratory Care and Sleep Medicine
brings you Save Your Breath: Cookbook for People withCOPD, written by Elizabeth Page, respiratory wellnesscoordinator for YavapaiRegional Medical Center,Prescott, AZ.
For more than 40 years,Elizabeth has cared forpatients with respiratoryailments as an RT and asth-ma educator. This 40-pluspage cookbook includesnearly 50 recipes foreasy-to-make, nourishingdinners, soups, salads,breakfasts and desserts,plus substitutions to turn your favorite dish into a deli-cious low-salt or low-sugar treat and tips for savingenergy in the kitchen. View and download this free e-bookat http://tinyurl.com/64r7j6r.
Those with chronic lung problems often have troublemaintaining weight since their bodies need extra caloriesto breathe.
Tips from the experts about meals and COPD:• You should include fiber in your diet and decrease
your salt intake.• Avoid overeating and foods that cause gas and
distention as cauliflower and cabbage.• If you use supplemental oxygen, be sure to wear it
while eating to give you extra energy for digestion.• If you sit upright rather than slouching, there will be
less pressure on your diaphragm.• Use pursed-lip breathing to help with shortness of
breath while eating.• Drink plenty of liquids but wait until after your meal
to avoid feeling bloated.• Many people say the best tip they can share about
meal time is to eat smaller meals 4 to 6 times a dayrather than larger ones.

4 www.pulmonarypaper.org Volume 22, Number 1
The healthcare reform legislation signed into lawby President Barack Obama profoundly changesthe way care is provided. According to Medscape,
“The Affordable Care Act seeks to dramatically expandthe number of people who can afford healthcare. It doesthat by subsidizing the cost for those who can’t afford it,penalizing those who refuse to buy it, and limiting thecases in which insurers can deny coverage. Among scoresof other provisions, it boosts pay for primary carephysicians, encourages compensation based on quality ofcare and bars copayments for most preventive services.”
The Durable Medical Equipment, Prosthetics,Orthotics, and Supplies (DMEPOS) CompetitiveBidding program is now in effect. Medicare beneficiariesin nine areas around the country will have to getmedical equipment and supplies through suppliers thathave a contract with Medicare.
This requirement applies to beneficiaries who live inone of the areas or who travel to that area. Areas affected:
Charlotte-Gastonia-Concord, NC-SCCincinnati-Middletown, OH-KY-INCleveland-Elyria-Mentor, OHDallas-Fort Worth-Arlington, TXKansas City, MO-KSMiami-Fort Lauderdale-Pompano Beach, FLOrlando-Kissimmee, FLPittsburgh, PARiverside-San Bernardino-Ontario, CA
You have probably already talked to your supplierabout these changes if you are in one of these areas. Youare able to continue getting your oxygen from yourcurrent supplier if they chose to become a grandfatheredsupplier by agreeing to supply equipment under the termsof the Competitive Bidding program.
Besides oxygen, oxygen equipment and supplies, thefollowing product categories are included in theCompetitive Bidding program:
• Standard power wheelchairs, scooters and relatedaccessories;
• Complex rehabilitative power wheelchairs and relatedaccessories;
• Mail-order diabetic supplies;• Enteral nutrients, equipment and supplies;• Continuous Positive Airway Pressure (CPAP) devices
and Respiratory Assist Devices and related suppliesand accessories;
• Hospital beds and related accessories;• Walkers and related accessories; and• Support surfaces.
You may call 1-800-Medicare with questions, or youcan use the online supplier tool to find a supplier whois in your area. Go to www.medicare.gov/supplier andfollow the steps below:
• Enter your zip code and click “Submit;”• A list of product categories will appear; those
product categories with a star icon next to them areincluded in the competitive bidding program;
• After selecting a Competitive Bidding productcategory, click “View Results;”
• A page will display stating you’ve selected aCompetitive Bidding product category and brieflyexplain the program; click “Continue;”
• A list of all Medicare contract supplier locations inthe Competitive Bidding area will appear.
Getting items repaired: You may be able to get an itemon the above DMEPOS list that you owned beforeJanuary 1, 2011, repaired or replaced by a non-contractsupplier.
The Centers for Medicare & Medicaid Services (CMS)has developed a fact sheet that describes the rules forrepairs which you can access at http://tinyurl.com/6akt69g.
Medicare Changes in 2011

If you are traveling and need equipment repairs, visitthis site: http://tinyurl.com/6bzusnc.
The CMS tool kit on DMEPOS Competitive Biddingcontains a number of useful fact sheets. It is available athttp://tinyurl.com/4t4kd3n.
Other provisions of the health law that may affect youthis year:
• Prescription drug costs could shrink $700 for atypical Medicare beneficiary in 2011, as the dough-nut hole – the gap in prescription coverage whenmillions of seniors must pay full price at the pharmacy– begins to close. Drug companies will give seniors50 percent off brand drugs while in the gap, excludingthose low-income people who already get subsidies.Generics will also be cheaper.
• Chain restaurants with 20 or more locations, andowners of 20 or more vending machines, will haveto display calorie infor-mation on menus,menu boards anddrive-thru signs.Restaurants must alsoprovide diners with abrochure that includesdetailed nutritional in-formation, like the fatcontent of their dishes.
• Medicare premiums in 2011 will take a bigger bitefrom wealthier beneficiaries. Beneficiaries payinghigher premiums will rise from 2.4 million in 2011to 7.8 million in 2019. Also, premiums for MedicarePart D which covers prescription drugs, will be linkedto income for the first time.
• Consumers with flexible spending accounts in whichpre-tax income can be used for medical purchases canno longer spend the money on over-the-counter drugsunless they have a doctor’s prescription.
• Medicare is bumping up payments for primary careby 10 percent from January 1 through the end of2015. It’s an incentive for doctors and others whospecialize in primary care – including nurses, nursepractitioners and physician assistants – to see theswelling numbers of seniors and disabled peoplecovered by the program.
• Payment for Medicare Advantage plans is beingrestructured. Rates this year will be frozen at 2010levels and lower rates will be phased in beginningin 2012.
• For the calendar year 2011, the payment rate forpulmonary rehabilitation in a hospital setting willincrease to $62.98 (Ambulatory Payment Classifi-cation 0102) (co-payment $12.60).
One of the benefits that we thinkwill be very effective is Medicare nowwill cover two types of physicalexams – one when you’re new toMedicare and one each year afterthat.
Medicare covers aone-time “Welcome toMedicare” physicalexam, if you get it with-in the first 12 months youhave Part B. It’s a review ofyour health, plus educationand counseling about pre-ventive services, and referrals for oth-er care you may need. Before January1, 2011, you pay 20% of the Medicare-approvedamount. Now you pay nothing for the “Welcome toMedicare” exam if the doctor accepts assignment. Whenyou make your appointment, let your doctor’s office knowyou’d like to schedule your “Welcome to Medicare” exam.
If you’ve had Part B for longer than 12 months, youcan get a yearly wellness visit to develop or update aprevention plan just for you based on your current healthand risk factors. Medicare has not cover this exambefore; again you’ll pay nothing for this exam if thedoctor accepts assignment. This exam is covered onceevery 12 months.
January/February 2011 www.pulmonarypaper.org 5
6 www.pulmonarypaper.org Volume 22, Number 1
Pulse Oximetry at a low discount price!
Call for special pricing forPulmonary Paper members.
Calling Dr. Bauer …
Dr. Michael Bauer
Dear Dr Bauer,My father’s doctor wants to put a
needle through his lung to get fluidout. Could you give me some infor-mation about this procedure and ifit is safe and effective?
Laura from Florida
A pulmonary specialist usuallyperforms this special test. Normally,there is only a small amount oflubricating fluid surrounding thesurface of the lung. In diseaseconditions, large amounts of fluid
may accumulate on one or bothsides of the lung. When this occurs,a person will also feel discomfort andshortness of breath. A thoracentesisis done either to remove fluid forpatient comfort or to help the physi-cian establish the diagnosis or causeof the fluid accumulation. Some ofthe more common reasons would bepneumonia, heart failure or cancer.Once we know the cause, an appro-priate treatment plan can be started.Uncommon side effects might includemild discomfort, bleeding or a smallcollapse of the lung itself. A thora-centesis is considered a safe andvery low risk procedure.
Dear Dr. Bauer,I do not understand the difference
between asthma and emphysema –can you help?
Anthony from North Carolina
Many use these terms inter-changeably. This is usually notcorrect. Although there are manysimilarities between asthma andemphysema, they remain twodistinctly different lung diseases.
Asthma results from a condition ofchronic inflammation affecting thebronchial passages. This causesswelling, irritation and mucus pro-duction in the lung. There are manypotential causes or “triggers” forasthma, including allergies, exercise,cold air and exposure to dusts, fumesor strong smells. Emphysema resultsfrom actual destruction of smallalveoli or lung sacs. Lung damage inemphysema is almost always a directresult of exposure to cigarette smokeover many years.
Asthma and emphysema are bothcalled obstructive lung disease.People with either condition havemore difficulty exhaling their air.Many of the same medications areused to treat both diseases. Drugsaimed at fighting inflammation, suchas inhaled corticosteroids, are themost effective at controlling asthma.Bronchodilating inhalers are themainstays of emphysema treatment.
Question for Dr. Bauer? You maywrite to him at The Pulmonary Paper,PO Box 877, Ormond Beach, FL32175 or by email at [email protected].
January/February 2011 www.pulmonarypaper.org 7
Alternative to Spiriva Being DevelopedForest Laboratories Inc. and Almirall SA recently
announced their chronic lung disease drug, AclidiniumBromide, met its main goals in its third late stageclinical trial. Aclidinium is a long-acting inhaledanticholinergic bronchodilator, currently beingdeveloped as a maintenance treatment for those withCOPD. Aclidinium, which will be an alternative toSpiriva, is also delivered by the Genuair dry powderinhaler.
The companies enrolled a total of 828 patients inthe trial. Aclidinium was found to be effective ateducing breathlessness and improving a patient’shealth status. Many participants showed an increaseof 30% in their FEV-1 for 12 hours while takingAclidinium. The companies plan to file for marketing ap-proval of Aclidinium in the United States and Europemid-2011.
The patent on Spiriva (Tiotropium Bromide) expiresin 2012 and Tiotropium will become available in theUnited States as a generic. This generic version will be lessexpensive and can be offered by several sources.
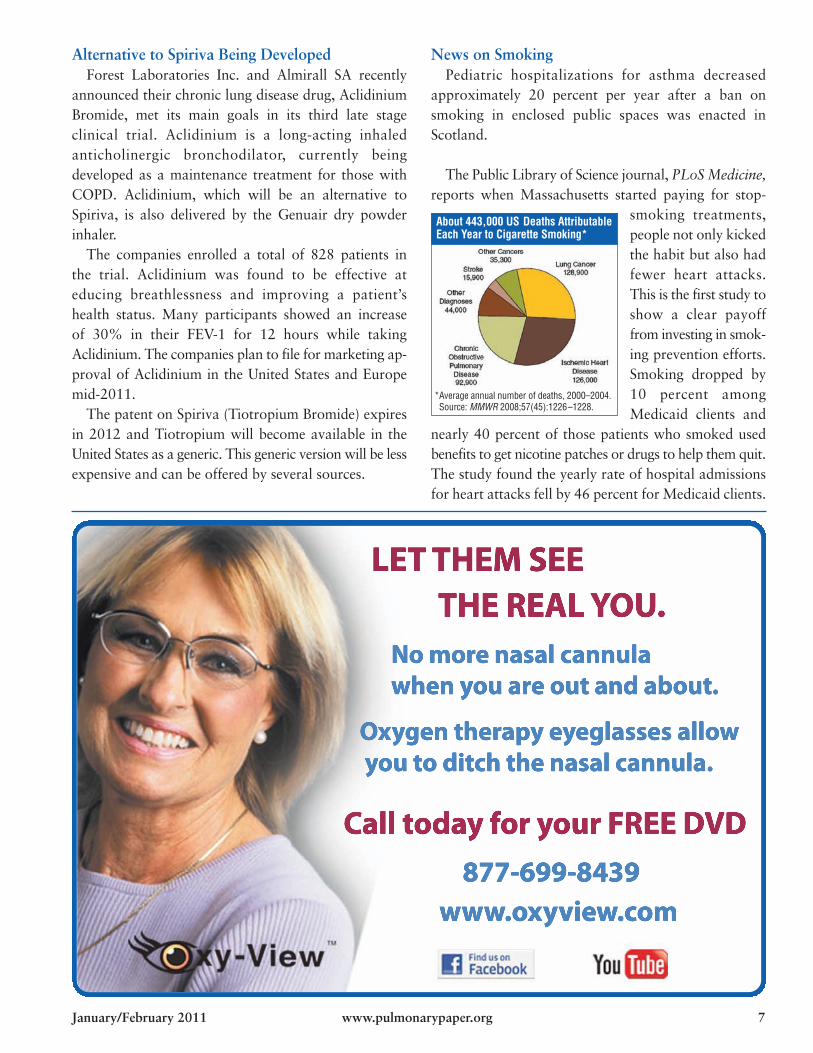
News on SmokingPediatric hospitalizations for asthma decreased
approximately 20 percent per year after a ban onsmoking in enclosed public spaces was enacted inScotland.
The Public Library of Science journal, PLoSMedicine,reports when Massachusetts started paying for stop-
smoking treatments,people not only kickedthe habit but also hadfewer heart attacks.This is the first study toshow a clear payofffrom investing in smok-ing prevention efforts.Smoking dropped by10 percent amongMedicaid clients and
nearly 40 percent of those patients who smoked usedbenefits to get nicotine patches or drugs to help them quit.The study found the yearly rate of hospital admissionsfor heart attacks fell by 46 percent for Medicaid clients.
About 443,000 US Deaths AttributableEach Year to Cigarette Smoking*
*Average annual number of deaths, 2000–2004.*Source: MMWR 2008;57(45):1226–1228.

8 www.pulmonarypaper.org Volume 22, Number 1
Carole from Canada writes, I’vebeen thinking of purchasing anoximeter. My doctor doesn’t think it’snecessary and I might obsess with it.I would like to check my saturationand heart rate when I’m exercising athome, when I have the oxygen off andwhen I feel light headed. I would alsolike to know if pursed lip breathingis as effective as simply exhaling.
Mark replies, Your doctor seems tosport the attitude of the ‘olde guarde’which the likes of Dr. Tom Petty andmany others, including myself, haveworked hard for years to change. It’snonsense for medical professionalsto presume that you not only “don’tneed” an oximeter, but “shouldn’thave” one! That’s like expectingdiabetics to dose themselves withinsulin without first measuring theirblood sugar to determine how muchthey need.
As we know, folks do not do wellwith a single order for an oxygen dose.Oxygen flow requirements can varysignificantly from rest to ambulationto sleep. It is common to observe thata person can maintain an adequatesaturation with no oxygen or 1/2 literor 1 liter when sitting still. When they
get up and move, they require 4, 5 or6 liters and may still not be able tohold a saturation of 90% or more.You should let your shortness ofbreath be your guide while exercising,rather than any target or arbitrarymaximum heart rate.
In the book, Adventures of anOxyphile 2, Dr. Petty explained whywe advocate patients have and usetheir own oximeters. Maybe you cangive a copy to your doctor! You canfind it online at Dr. Petty’s website,http://drtompetty.org or send checkfor $19.99 to:
Snowdrift Pulmonary Conference1305 Krameria St. #HPMBDenver, COThe first version of the book,
Adventures of an Oxy-Phile, is avail-able free to download at the web siteas well as his book, From Both Endsof the Stethoscope.
As COPD reaches the more severestages (FEV1 – Forced ExpiratoryVolume in One Second below 25%),the risk for carbon dioxide retentionincreases.
Because of the destruction to theairways, the problem is not getting airinto the lungs but getting stale air out!When one breathes out, air cannotleave the air sac before another breathis taken in. Increased amounts of airare trapped at the end of expirationand the diaphragm gets pushed down-ward (flattened) from the trapped air.The belly pooches out as the contentsof the abdomen are displaced down-ward and outward and the chestexpands in diameter.
Pursed lips breathing (PLB) helpsexpand the airways by splinting themwith positive pressure during exhala-tion. This increases the efficiency of
exhalation, allowing more air to beexhaled with each breath. Some folkscan do PLB with enough efficiency toraise their oxygen saturation. It helpsreduce air trapping, though that isonly relative in magnitude.
PLB is most useful when movingor exerting, as that is when youincrease both respiratory effort andrate. The more your respiratory rateincreases, the more air becomestrapped per-unit-of-time. We call thisdynamic hyperinflation.
It is unavoidable as your FEV1drops to very low levels. Folks whoare new to PLB should practice it asmuch as they can to gain bettercontrol and mastery of the technique.It is very helpful to pull you out ofpanic and anxious moments.
Don’t beat yourself up for what youcannot change! Yes, you do have astruggle ahead of you. By approach-ing your challenges with hope anddetermination, a 25% FEV1 cancarry you a long way for a long timewithout as much misery as you mightfear. Work hard to maximize whatfunction and capacity you haveremaining. Life can be good – no,GREAT! – despite the challenge ofadvanced COPD.
Mark Mangus RRT, BSRC, is a member ofthe Medical Board of EFFORTS (the onlinesupport group, Emphysema Foundation ForOur Right To Survive, www.emphysema.net). He generously donates his time toanswer members’ questions.
Ask Mark …
Mark Mangus, RRTEFFORTS Board
IPF Medication and Research NewsGilead Sciences Inc. is halting the Phase III clinical
trial of Ambrisentan in patients with idiopathic pulmonaryfibrosis (IPF) “due to lack of efficacy.” The biopharma-ceutical company said the decision follows an analysis ofefficacy and safety data “which did not show evidenceof a treatment benefit in the group of patients that receivedAmbrisentan.”
Eight months after the Food and Drug Administrationrejected Pirfenidone as a treatment for IPF, InterMune Inc.said it will undertake a Phase III study of the drug. Thecompany said it would enroll the first patient in a late-stage trial of Pirfenidone (also known as Esbriet) inpatients with IPF in the first half of this year. InterMunesaid it has a March meeting scheduled with the FDA todiscuss the new study – that is required for their approvalof the drug. There is no current treatment in the UnitedStates for IPF. Esbriet last month won a positive recom-mendation from a European advisory group and isexpected to be marketed, starting in Germany, in thethird quarter.
Another company, FibroGen Inc., based in San Fran-cisco, will also target IPF in a mid-stage study. The 48-pa-tient study will test human monoclonal antibody, FG-3019,which it has developed to combat connective tissuegrowth factor.
FibroGen hopes to show that blocking connectivetissue growth factor, or CTGF, is key to stopping andperhaps even rolling back damage caused after injuredlungs heal improperly.
Patients in the study will receive intravenous doses ofFG-3019 every three weeks for 45 weeks. The trial willjudge safety, tolerability and the effectiveness of the drugon the extent of lung fibrosis, lung function and shortnessof breath. FG-3019 also is being studied in two Phase IIstudies against advanced liver fibrosis due to chronicinfection with Hepatitis B virus and in patients withpancreatic cancer.
For more information on this clinical trial, go towww.clinicaltrials.gov and search for NCT01262001. Youmay also contact Loredie Lugos RN at 415-978-1353.
The new year is a great time to start a new exerciseroutine! If you do not have access to a pulmonary
rehabilitation program, ask your physician whichexercises would be appropriate for you. When youbegin to exercise at home, start for short periods, evenif for only a few minutes. Work toward a goal ofexercising once a day, four to five times per week for fiveto 15 minutes at a time. Increase the duration of yourexercise by a few minutes each time with a goal of 20 to40 minutes of continuous exercise.Aerobic exercise like cycling, swim-ming and walking is best for thelungs, heart and circulatory system.
Resistance or strength training shouldbe performed at light intensity forbeginners with one or two repetitions.Examples of chest and shoulder exercises:
Wall Push-Ups• Stand facing a wall with your feet about 1 to 2 feet
back from it. The farther you stand back, the moredifficult the exercise becomes.
• Place your hands on the wall a bit wider thanshoulder-width apart.
• Bending only at the elbows, lower yourself forwardtowards the wall then push yourself away from it,keeping your body straight.
• Exhale while you exert.
Seated Shoulder Presses• Use something around the house for weight, as canned
goods if you do not have one or two pounddumbbells.
• From a seated or standing position, hold the weightsjust above your shoulders.
• Push weights up overhead slowly.
January/February 2011 www.pulmonarypaper.org 9
Fibrosis File

Good Times!
I have a hint for users of BiPaP devices. I use a wig capto keep the Velcro on the straps from snagging in my hair.I also heard about a valve that is placed between the can-nula and the concentrator tubing that allowsyou to adjust the flow without having to do it at theconcentrator. It is from www.softhose.com and costs $10plus shipping and handling. They also have very softcannulas and tubing you may order by calling1-858-748-5677.
RVD, Colorado
One of our biggest changes in recent years came withthe change to HFAmetered dose inhalers. Since old habitsare hard to break and you may still be wondering aboutthe differences, you can download information and achart on the inhalers, number of doses in the inhaler andhow to clean and prime it from National Jewish Healthat http://tinyurl.com/64jsvdr.
For those without access to the Internet, send a requestwith a self-address, stamped envelope to The PulmonaryPaper, PO Box 877, Ormond Beach, FL 2175 and wewould be happy to send you a copy.
Today’s Internet users have a host of acronyms that theyuse in conversations that might seem like a foreignlanguage, as LOL is Laughing Out Loud.
Gail Keller of Westfield, NJ, sent us this list, developedespecially for seniors, some of which you might want touse in your next email!
ATD: At the Doctor’sBFF: Best Friend FartedBTW: Bring The WheelchairBYOT: Bring Your Own TeethCBM: Covered By MedicareDWI: Driving While IncontinentFWBB: Friend With Beta BlockersFWIW: Forgot Where I WasFYI: Found Your InsulinGGLKI: Gotta Go, Laxative Kicking InGHA: Got Heartburn AgainHGBM: Had Good Bowel MovementIMHO: Is My Hearing-Aid On?LMDO: Laughing My Dentures OutLOL: Living On LipitorOMG: Oh, My Grandchildren!ROFLCGU: Rolling On The Floor LaughingAnd Can’t Get Up
SGGP: Sorry, Gotta Go PoopTGIF: Thank Goodness It’s Four O’Clock(for early bird specials)
TTYL: Talk To You LouderWAITT: Who Am I Talking To?WTP: Where’re The Prunes?
I have excessive mucus. First thing in the morning,I drink 1-1/2 to 2 tablespoons of lemon juice, sweetenedwith honey in a glass of hot water. This clears my throatand is also a natural laxative. Another plus is that it tastesgood! I think people with diabetes should check witha health professional about using this.
Janet McLees, Flint, MI
Sharing the Health
10 www.pulmonarypaper.org Volume 22, Number 1
Receive a Free One Year MembershipContribute a picture or tip on how you COPE with
COPD! Send to The Pulmonary Paper, PO Box 877,Ormond Beach, FL 32175. Include your name/address.
Jeri Mondloch (right) with friend, Annie Bale, enjoys rootingfor her University of Minnesota Gophers. She dressed up forHalloween as a Conehead! Jeri uses trans-tracheal oxygen.
January/February 2011 www.pulmonarypaper.org 11
Julia Steitz of Penfield, NY, ordered a lung flute fromMedical Acoustics (http://medicalacoustics.com), a newproduct to help clear secretions. Because of her low flowrates when breathing through the device, she was unableto get it to work properly. Her husband tried and withnormal lung values had no problems. The company gaveher a complete refund and told her they were workingon improving the product.
She also wants to share a tip for doing laundry. Juliasits on a chair and uses a “grabber” to get the clothes outof the washer and dryer.
The American Association for Respiratory Care haspublished an informative 56-page booklet entitledA Patient’s Guide to Aerosol Drug Delivery. Thepublication covers each type of medication device withinstructions on how to clean them and solve problemsthat may arise.
You may see it on the Internet at www.yourlunghealth.org/healthy_living/aerosol/
Jenna from Florida found she had problems with herSpiriva capsules when she stored her medication in thebathroom. The humidity may have been causing themedication to stick together and the capsule did not seemas easy to break. Once she moved her medicines to adifferent room the problem solved itself.
If your oximeter mistakenly gets wet, take the batteriesout immediately and cover the oximeter in a small con-tainer with rice. Cover the container and leave itovernight. The rice will absorb the water and your oxime-ter will be fine with new batteries! Maggie B., Illinois
1-888-648-7250www.rxstat.net
Sequal’s EclipseSmallestcontinuous
flow POC. 3LPMcontinuousand 6LPMpulse
Respironic’sEverGoBest battery life,8 hours at 2LPM6LPM pulse
Respironic’sEverflo™ Quiet withOxygen Purity IndicatorSmall form, 30 lb.stationary unit ($799delivered). Great for afteryour Medicare rental!
Invacare® XPO2™Lightest POC at6 lbs.! 5LPM pulse
Rx Stat Respiratory will match or beat anyone’s prices on oxygen equipment!
Rx Stat will beat anyone’s priceon a new portable concentrator.
We also rent POCs for travel:$395 for first 10 days, $295 for eachadditional 10 days–includes shipping!
And we buy and sellused portable concentrators.
Call for availability!
See demos of POCson YouTube.com,search “Rx Stat”
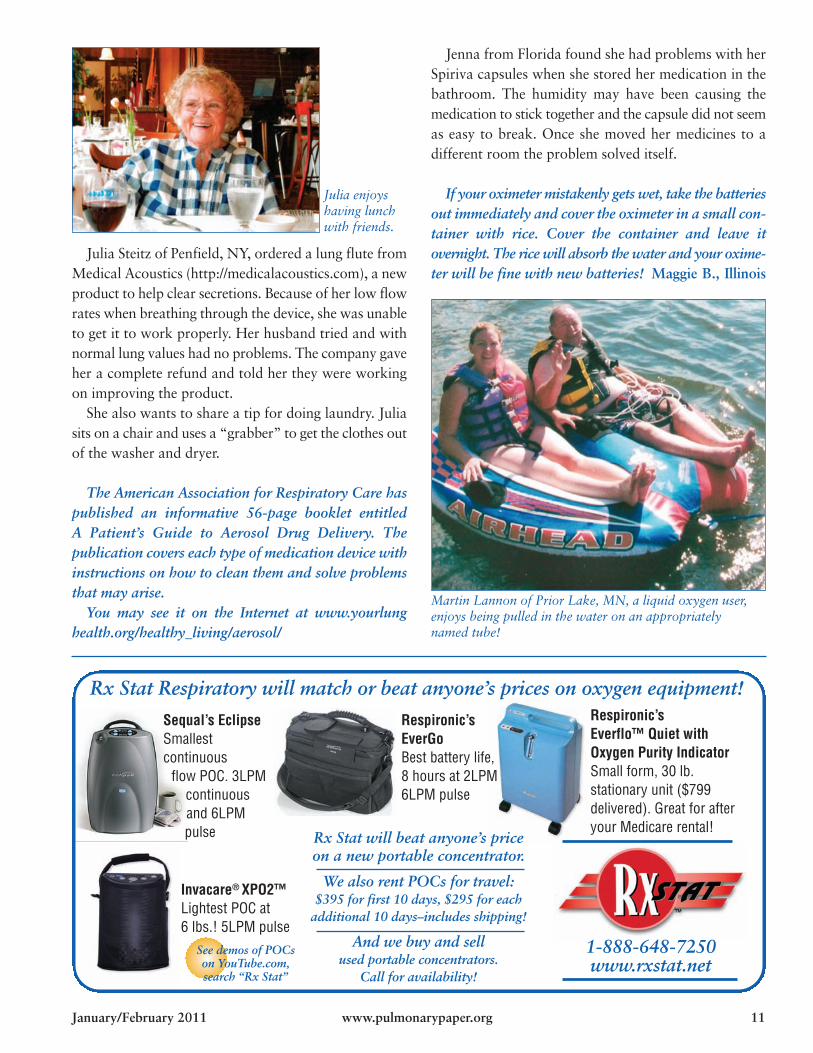
Martin Lannon of Prior Lake, MN, a liquid oxygen user,enjoys being pulled in the water on an appropriatelynamed tube!
Julia enjoyshaving lunchwith friends.
Traveling by Air: Key Travel Tips fromTransportation Security Administration (TSA)
There are times when TSAwill physically inspect a piece ofchecked luggage. Locks thatcan be opened by security offi-cers using universal “master”keys are available at airportsand travel stores nationwide.
Do not pack wrapped gifts or bring wrapped gifts tothe checkpoint as TSA may have to unwrap packages forsecurity reasons.
Footwear is required to be removed and placedthrough the X-ray machine for screening. Wearing slipon rather than tie shoes will cut down on efforts at thescreening. Persons with medical conditions who keep theirshoes on will be subjected to additional screening.
Place the following items in your carry-on baggage orin a plastic bag prior to entering the screening checkpoint:
Mobile phones and keysLoose change and money clipsMetal hair decorations and large belt bucklesMedications needed (in case your luggage is delayed
at arrival)
Prescription liquid medications and other liquidsneeded by travelers with medical conditions are permit-ted which includes:
• All prescription and over-the-counter medications (liq-uids, gels and aerosols) including petroleum jelly, eyedrops and saline solution for medical purposes
• Liquids including water, juice, or liquid nutritionor gels for passengers with a disability or medicalcondition
However, if the liquid medications are in volumes larg-er than 3.4 ounces (100 ml) each, they must be declaredto the Security Officer either verbally or in writing.
Once cleared through screening, you can bringwheelchairs, scooters, canes, walkers, support braces,diabetes-related medication, equipment and supplies,orthopedic shoes, exterior medical devices, hearing aids,CPAP machines, respirators and personal oxygenconcentrators among other items.
Seen while traveling:You always have to keep the right balance in life!
12 www.pulmonarypaper.org Volume 22, Number 1
Traveling News
The next generationof portable oxygenconcentrators –
• Small in size –only 7 lbs.
• Virtually silent,discreet
• No refills needed• A/C, D/C power• 4-hour or
8-hour battery• $3,200 with
8-hour battery(Special sale pricefor PulmonaryPaper readers!)*If you qualify
Regain Your Quality of Lifewith Inogen One G2!
No more cylinders,no more refills!
Covered byMedicare*
The width ofa coffee mug,the height oftwo stacked!Very discreet.Covered byMedicare*
Call today!RxStat Respiratory
1-888-648-7250 • www.rxstat.net
October 1Sapphire Princess7-day CaliforniaCoast cruise fromLos Angeles, CA
February 12, ’12Norwegian Spirit7-day cruise to theWestern Caribbeanfrom New Orleans, LA(Stay for Mardi Grason February 21!)
July 1Celebrity In5nity7-day cruise to Alaskafrom Seattle, WA
Visit www.seapuffers.com or call 1-866-673-3019 to join the fun! FST: ST36334
January/February 2011 www.pulmonarypaper.org 13
March 13Holland America’sNieuw Amsterdam7-day cruise to theWestern Caribbeanfrom Fort Lauderdale
June 4Emerald Princess
11-day cruise toScandinavia and Russia
from Copenhagen
April 15, ’12Carnival Pride
See the Cherry Blossomsin Washington, DC
7-day Caribbean cruisefrom Baltimore, MD
September 2Norwegian Dawn
7-day cruiseto Bermuda
from Boston,MA
January 15, ’12Royal Caribbean
Mariner of the Seas7-day cruise to theWestern Caribbean
from Galveston, TX
April 4Coral Princess
10-day cruise to thePanama Canal
from Fort Lauderdale
Call to book your individualtrip or join us on our roundtripSea Puffers group cruises!We take the worry out oftraveling with oxygen!
You will always get the lowest possible price available at timeof booking with Cruise Planners – Get Up & Go2! All trips areroundtrip from the port city.
Pack Your Bags! Let’s Make Memories!Pack Your Bags! Let’s Make Memories!
14 www.pulmonarypaper.org Volume 22, Number 1
Bumps and Bruises!A bruise here, a bruise thereI have bruises everywhere!Sharp edges and cornersare not my friend,No matter how careful,they find me again and again!On my arm or on my elbow,Oh where will the next one go?The tattooed youth havenothing on me!On my arm, I have thelikeness of Sicily.First, it was blackand now it is not.It’s sort of the color of an apricot!The best part is, it will soon be gone,probably replaced by another one.I won’t be surprised, only amused!
Susan Forte, Nevada City, CA
Flu UpdateLast flu season, the world went through the first
influenza pandemic in more than 40 years. Many researchteams are working on an universal flu shot that couldprotect people from all flu strains for decades or even life.People who were infected in the H1N1 pandemicdeveloped an unusual immune response, making anti-bodies that could protect them from all seasonal H1N1flu strains from the last decade and maybe even the dead-ly Spanish flu from 1918 and a strain of the avian flu.
As of early January, reported flu cases were mild formost of the country except for Louisiana, Mississippi,Alabama and Georgia, who reported high incidence ofthe flu. The New York City area also showed moderateactivity.
As many as 49,000 people in the United States die fromthe flu every year. The Centers for Disease Control haverecommended everyone 6 months and older be vaccinated.Please get your vaccination if you haven’t already!

It’s time for our annual income tax article! TheInternal Revenue Service lets you deduct medical costsas long as they are more than 7.5 percent of your
adjusted gross income.If you paid for travel oxygen, a portable nebulizer or
oximeter, it may be considered a medical expense. Otherpossible deductions you may want to investigate:
• An air conditioner or humidifier that is added to yourhome’s heating/air conditioning system that is neces-sary for relief from allergies or other respiratorysymptoms.
• Medical equipment/supplies sold without a prescrip-tion, including needles, bandages or devices such asa glucometer.
• Uninsured medical treatments, such as an extra pairof eyeglasses or set of contact lenses, false teeth,hearing aids and artificial limbs.
• Smoking cessation programs and prescribed drugs andweight-loss programs.
• Travel expenses to and from medical treatmentssuch as ambulance service, bus, taxi, train, plane fares,parking fees, tolls and use of personal vehicle. For2009, you can deduct eligible medical travel at 24 centsper mile. In 2010, the mileage rate deduction is 16.5cents. You may also be able to deduct the cost ofequipment for your car needed to transport ascooter or wheelchair.
• Wheelchairs/motorized scooters if not already paid forby insurance. Cost of ramps, wider doorways or hall-ways, railings, support bars, modified door hardwareand other modifications to accommodate yourscooter or wheelchair. A chair lift to get up and downthe stairs as well as adjusting electrical outlets andfixtures and grading exterior landscape to ease accessto the house.
• In calculating residential remodeling as a medicaldeduction, you won’t be able to write off the full costson your tax return. If the improvement increases thevalue of your property, that amount is subtracted fromthe project’s cost and the difference counts as amedical expense.
• Insurance payments from already taxed income. Thisincludes the cost of long-term care insurance up tocertain limits based on your age.
• If you are an oxygen or CPAP user, you may be ableto take the cost of the electricity used to operate yourconcentrator as a medical deduction. Check withwhomever prepares your annual income tax return ifyou can or would benefit from taking this deduction.
How to compute the cost of electricity used:1. Look at the label on your concentrator. It states the
number of volts and amps the concentrator uses. If notfound on the concentrator, look for it in the manual orask your oxygen provider. As an example, we will use115 volts at 4 amps. To convert to watts (W), multiplyvolts and amps: 115 volts x 4 amps = 460W.
2. Next, calculate the number of kilowatt (KW) hours youuse per year. Multiply the watts your concentrator usesby .001 KW/W to convert watts to kilowatts. In ourexample, 460 W x .001 KW/W = 0.46 W.
3. Multiple this answer by 24 hours/day x 365 days/yearif you are a continuous user. If you do not always haveyour oxygen on, multiply by the average number ofhours used per day and then by 365 days/year. Tocontinue the example, 0.46 KW x 24 hours/day x 365days/year = 4,029.6 KWH/Y. This is the kilowatt hoursyou have used to run your concentrator the past year.
4. Now multiply the above result by the cost per kilowatthour your electric company charges you. It may belisted on your bill or you could call their office. Let’s saythey charge you 8 cents per kilowatt hour (prices varywidely depending on the region in which you live).To finish our example, 4,029.6 KWH/Y x $0.08 =$322.27. This is the amount of electricity you paid torun your concentrator.
For a complete list of what medical deductions the IRSwill and will not allow, check out Publication 502, whichcan be seen on the Internet at www.irs.gov/pub/irs-pdf/p502.pdf.
Tax Time Rolls Around Again!
January/February 2011 www.pulmonarypaper.org 15

Dedicated to Respiratory Health Care
PaperPO Box 877, Ormond Beach, FL 32175-0877
ThePulmonary Non-ProfitOrganizationUS Postage
PAIDDaytona Beach, FL
Permit #275
Respiratory NewsRecently, doctors at the Canadian Heart and Stroke
Foundation discovered an early warning system in aprotein called PIM-1. Dr. Sébastien Bonnet has establishedthat PIM-1 cells can be used as markers of pulmonaryhypertension. Physicians found the greater the PIM-1levels, the more severe the pulmonary hypertension. Withblood tests to look at these levels and blocking thePIM-1 protein, a cure might be possible!
Researchers at New York Presbyterian/Weill CornellMedical Center have discovered a breakthrough exper-imental treatment for lung cancer. The treatment is partof a lung cancer vaccine that exposes the body to aprotein that the lung cancer produces. This proteinproduction helps the body build up protection against thecancer that’s attacking it. Lung cancer is the leading causeof cancer deaths throughout the world, and if the vac-cine works, countless lives could be saved. More than 400centers worldwide are taking part in the study. Thevaccine is given as a series of injections over two years.
The Canadian Medical Association Journal reportspopular heartburn drugs, such as Prilosec, Prevacis andNexium as well as Tagamet, Pepcid, Acid and Zantac, areassociated with an increased risk of pneumonia. Thesedrugs are very popular in the United States and are thesecond best-selling category of medications worldwide. Themost plausible reason why suppressing acid in the stom-ach might raise the risk of pneumonia is that stomach acidacts as a barrier helping to control harmful bacteria andpathogens. Not enough stomach acid to do the job mayallow pathogens to flourish and end up in the lungs. Butthe drugs are very important since reflux can also causeacids from the stomach to get into the airways and inflamethe bronchial tubes, raising the risk of infection.
Prescription pain meds Darvocet and Darvon have beenrecalled after research linked them to serious or poten-tially fatal heart rhythm abnormalities. A voluntaryrecall was issued by manufacturer Xanodyne Pharma-ceuticals Inc. in November at the request of the FDA.
![Untitled-4 [] · So, you are not comfortable with specialization. ... are motivated. We specialize in graphic design and packaging, we specialize in product design, we specialize](https://img.pdfslide.net/doc/110x75/5ee2fe07ad6a402d666d2425/untitled-4-so-you-are-not-comfortable-with-specialization-are-motivated.jpg)