Embed Size (px)
Citation preview
Journal of Clinical Narsin« l'>9.i; 2: l.S.S
The participation of hospital nurses in the multidisciplinary wardround on a cancer-therapy ward
ZOI'. WlL'XLi: liSc, MN, One. Cal.U aril Sislcr, Opiiorc and Isk tlarj, Iclnulrc Hospital, ll'Inl.harch. Cardiff CF-l 7\f, Ik
•Icccplcd for puhliciilion l> Dcccinhcr l'>')2
Summ-.iry
• The aim of ihis study is lo describe the puriicipation of a gniup ol hospimlnurses in the nuiltidisciplinary ward rounds oti a cancer-tliei-ap\ ward.
• Thirteeti tiuiltidisciplinary gt-oup meetings (which took place belore the 'walkfouiur ineetitig- with the patietits at the bedside) wet-e tape recorded over a periodof 4 weeks. The pat-ticipatitig nurses were ititerviewed imtnediately alter eachward round, yielding 2.i interviews \n total. Iti additioti, three niuhidisciplinarvteam meetings were oh.served by the researcher.
• Tlie verbal contribtttions ofthe nurses are categorized. Tbe beba\iour and ibeviews of tlie participatitig nurses about ward routuls are described.
• .'\spects of decision making atid titne tnanagetiient at-e highlighted. Barriers tothe participation of nttrses in ward rounds are identifted.
• Recommendations which tnay itnprove the participation of nurses in wardroittids are maile.
Keywords: cancer, doctor nurse t-elationsbip, conitnunication. ward round.
Introduclion and aim of the study
'I'he ]iurii()se ol this study was to explore and describe (asobserveil by tbe leseaiclier atul reiiorteti by a satnple olntn-ses) tbe participatioti ol tutrses in a weekly tiiulliiiiscip-linary bospital ward routid. Tbe settitig is otie ward m aregiotial caticer-treatment cetitre wbere |iatietits at-e mostlyadmilted for railiotberaiiy and/or cbetnotlierapy.
The wat-d iti question bad t-ccctitly changed tbe tnctbodot delivery ol tiursitig eare to one ol pritnary mn-sing(Mantbey, 197.S). One outcome of tliis tnetbod ot nursingwas thai (be wat-d sister tio longer attended tbe wardt-()unds, except in ber capacity as pritnary or associatetiurse. It was bebevetl to be itnportatit to establish wbat
Ciirrcspiinilcihi-: JJinnlion Ti-rraii-, Railyr, CarJiJf Ct'-l Sl'.l),
was bappetiitig to tbese nurses during tbe ward rounds.
Perbaps tben sotne liglit could be slied oti bow etierg\
sbould be dit-ected to enable tbetn to contribute fully to tbe
team for tbc betielit oi' tbeir patietits, tlieir owti practice
and tbeir tnultidi.sciplinat-y colleagues. It was boped tbis
study would getierate I'urtber ititerest in wbat tbe autbor
views as ati importatit isstic wbicb is vital to tbc dexelop-
tnetit of nursing roles and critical atialysis ot accepted
practice.
Li tcr -a ture rex icw
A diagnosis ot caticer is a tnajor, bte-tbreatcnuig cxetit. .\
study publisbed in l')8,S (Cancer Relief Macmillan l'utul)
found tbat caticer was tlu- tnost learetl ot all diseases, and
tbat the treattnents wet-e genet-all\ pcrccixcii lo be ' \cr\
/ . Whale
paitituT. Respondents were poorlv intbrtned about recent
advances in patietit c:()mf()rt and attitttdes were found to be
'unilttl} negative and learluF.
It bas beeti estitnated (bat between 25 and 45",, of
people witb cancer recei\ea lortnal psycbological diagnosis
of anxiet) (Maguire, 1978; \ \ elcb-McCallery, 1985).
Anxiet) was associated witb insotnnia, social witbcb-awal,
bel|ilessiu-ss, atnicijiatory nausea anil vomiting, sexual
probletns atul nHilti|ile side-edects to cancer (berapy.
Tbere bave been nio\es iti cancer researcb to tneastn'e tbe
tbstrcss causeti by tbe symptoms of cancer and its treat-
ments (Holmes & Dickerson, 1987; I lohnes. 1989). Tbe
aim was to make some judgetneiit ot 'qualit\ ot lite' toi'
caticcr palienls. .Svmptotns reported by patietits tliat affec-
ted tbeir distress included tiredness, tnooil, ap]ietite, pain,
appearance, conccntratioti, tnobtbty, constipaiioti, sleep,
diarrboea and nat.isea.
Idctitilying patient needs is certaitih a growitig area of
nursmg researcb (l.illey, 1987; \c)n I'.ssen & Sjoden, 1991).
l''or example, Derdiarian (1987) tbund tbat cancer patients
generally seek tnaxitnum mtortnatioti in tbeir tn-sl steps
lowartis c<)[iing. Nevertbeless, cancer patients continue to
report ibat tbey arc not getting ibc intbrmalion trotn
bealtb-carc professionals tbat tbey feel tbey need (Wiggitis
<•/ ,//., 199(1).
Defining nursing ktiow ledge atui identifying tbe nurse's
role bas rctnained a ditlicult pr(iblctii (Perry, 1985). 111-
detined role delinition, lack ot exjiet-tise and poor pet-cep-
tion ot role by oibcr bealtb-care prolessiotials and patients
ba\c l)ecn cited as barriers to idetitilying tbe domaiti of
nut-sing (Weiss, 1985). Tbe role ot tbe cancer nurse tnay
inilced be witle ranging, reqttiring specitic skills in ot-der to
respond ctlectivel) atul ediciently lo (be tieeds ol palienls.
Additionalh, tbe cancer tun'se will interact witb otber
protessionals wbo are specialtsts in cancer cat-e. Indeed,
(luTc is a growing bod} ol literature su]i]iorting tiie
cllcctneness ot tnultidisciplinary work oti jiatient out-
totncs (Molnar l-'eiger & .Scbtnitt, 1979; I'.ngstrotn, 1986).
II eflccttve teamwork is (o be acbieved tor tbe benetit of
patients, it coukl be argtietl tbat llie tutrse bas a lui(ber
responsibilit} to be a iLilly participating member ol' tbat
(catn.
Flu- expert nurse ma\ well be visible in clinical areas in
direct intet-action witb patictKs (Benner, 1984). Tbe degree
to whicb tins same expertise nianilesls itsclt in tbe pres-
ence ot other tliscipbnes may be \c-ry ditlei-eiit. l''or
example, tbc work ot Prescott cl al. (1987) dcniotistrated
that there was a Jack ot av\arcncss among doctors about thc
(\pcs ol ilccisions nurses made, both in tbc course o l tbci r
prailicc anti prior lo ibcu' rc(.|ucsts lor a tiictlical opitiion.
\ u r s c s ucrc aclnc in providing inffji niation arul makinu
suggestions lo doctors, but tbis was not sytionymous in
tloctors' eyes witb tbe nurse as decisioti tnaker. Tbis is
des]iite tbe lad (ba( galbering itilbrmation and considering
available options are essential cotnponents ol tbe decision-
makitig process.
It bas been argued (Kinston, 1983) ibat doctors feel tbey
sbould retain 'pi-escribitig autbority' over nurses, i.e. ibey
have a rigbt to determitie tbe execution of particular
nursing tasks, in a way that does not apply to otber
disciplines. Weiss (1983) observed tbat altbougb both
doctors and tnirses accept i-esponsibility for patient cat-e,
doctors see themselves as more responsible tban nurses.
'I'bis may e.xplaiii why doctors feel they can Icgiliniately
detnand gt-eatcr authority for decision tnaking in ihi-'
health-care setting. The complexities and dilliculties of tbe
doctor nurse relalionsbip bave beeti well documented
(Catnpbell-lleider & Pollock, 1987; Stein ei al., 1990).
1 lowever, the litei-ature genet-ally pays little regard to any
view tbat (bere niigbt be quite a large ovei-lap in 'he
demands ol tbe (wo |irolessiotis.
Ward rounds bave been described as a 'regular ritual of
ward b'le' (Walsli & I'ord, 1989), and anecdotal evidence of
tbe tnisct-ics of wat-J t-ounds for nurses arc comtnon (Walsb
& I'ord, 1989; Webb, 1987). Criticisms Irom patients bave
also been docutnetited (.Steele& Niortoti, 1978). Ciadboisc/
al. (1988) studied ward t-outuls in a general bospital and
tbund tbat because medical scbedules wet-e given tbe
bigbest priorit), otber discijilines anil deiiartments, no-
tably nursing, used their time poorly. Brink (1972)
observed psycbiatric nmses iti a multidisciplinary ward
round and found ibeir behaviour both passive and unpro-
tessional. I'jigstt-otn (1986), Weiss (1983) and Mallik
(1992) also noted this passivitv of nurses during ward
rounds. Weiss noted this passivity in patietits as well. It
cotild be argued lliai if ntn-ses are cotn|iliatit iti the
concentratton on medical aspects of a patient's care,
patient needs are going to be overlooked. Tbese studies
reinlorce tbe view tbat iticreased o]iportunity alone does
not necessaril} toslei- collaboration.
Ptice (1985) usefully described ward routuls as botb
TunctionaT and 'tlyslunctiotiar. Tbe functional aspects
incluile decision tnaking, infontiing, teacbitig, tnaititaitiitig
relationsbips witbiti tbe ward atul ratiotiitig ati expensive
resource (llie consttltant). The dyslunclional aspects cottid
include tbe use of jargon witb patients, litniting tbe time
aiitl scope ol ilecision making and rigiilly controlbtig the
tiattire ol consul(an( pa(ient interactiotis. Mobiar-T'ciget-
& Scbtnitt (1979) reported ibat (be dillcritig cbai-actcristics
ol doctors were a major inlluetu-c oti ibc way ntirses
contribtilcil to ward rouiuls.
Thci-c ilo appear to be tbflc-rcrues in the organization.
Nurses' participatioti iti ward rounds 157
function and expectations of tbe ward round across tbelitet-atut-e t-eviewed wbich points to the coticlusioti tbateacb study is contextual. Nevertheless, tbetnes emergedwbich pt-esented an interesting background for tbe platniedstudy.
Aims of the study
• To identify tiurses' verbal contribution lo ward t-oundsby audiotaping a satnple ol ward rounds.
• To exatnine nurses' petceptions of ward rounds (byinterview).
• To observe tbe intetaction of tbe tnultidisciplinary teatnduring the ward rounds (by non-participant observa-tion).
• '1\) analyse and discuss tbe findings.A pilot study was undertaken to provide pointers to tliefeasability ol tbe tnain study. Tbe tnultidisciplinary wardt-outul was a weekly event wbicb (iti this context) entailedeacb tnedical consultant meeting with tbeir owti tnedicalteatn iti conjunction with a qualified ward tuttse, a socialworker atul a cotntnutiity liaisoti tutrse. Individual patientsare discussed privately atiiong tbis group, l'̂ ollowing tbismeeting, tbe medical teatn and tbe ward nutse met thepatient, either in an examination rootn or by tbe bedside.
Tape recording tbe tnultidisciplinary group tneetingsyielded ricb data. Observing the multidisciplinary meet-ings illumitiated tbe tajie recordings. Tbe tneeting witb tbepatient was overwhebningly an interaction betweeti con-sultant and patient and, tbetefote, data gleaned to lullil theaitns ofthe study wete spatce. b'or tbis teason, tbe meetingwitb tbe i^atient was not included iti tbe study. Tbeinterview Ibrtnat for eliciting the views of nut-ses wasdeveloped considerably during tbe pilot study.
Design of the main study
Tbe ward selected for tbe study was in a regional cancet-treattnent centre. Tiie cancer tteattnents involved radio-tberapy and/or cbemotbetapy atui patients were adtnittedto tbe ward for palliative or curative tberapy. Tbere werethtee fortnal tnultidisciplinary ward t-ounds per weekwbicb involved tht-ee different tnedical cotisultants. Tbit-teen of tbe tnultidisciplitiary tncetitigs wbicb took placeprior to tbe meeting ot tbe patients were tape t-ecorded. Inadditioti, tbtee of tbe tnultidisciplinary group meetingswere observed using tion-participant observation.
These ward t-ounds involved a satnple of 12 differentnurses (botb pritnary and associate nurses) participating intbe ward rounds on 23 occasions yielding 2?i interviews.'f'he nurses consented formally to participating in the
study. Tbe data wet-e analysed in a nutnber of ways and aresutntnarized below.• Starting and finisbing times ol ward routids.• Total nutnber of patient cases atul frequency of nurse
cotitributions.• C>)ntent analysis of tbe nurses' verbal contributions to
tbe (13) multidisciplinary tneetings.• Tbetnatic analysis of tbe (23) post-round interviews.• Analysis of tbe field notes taken during observation of
tbe (3) multidiscipiitiary reatn tneetings.• Tbe natut-e and pattern of tbe nurses' verbal contribu-
tiotis.• Atialysis of findings for palliative and curative tbet-apy.• Reportitig of probletns by nurses and subsequent de-
cision tnaking by the tnultidisciplinary team.• Differetices act-oss wat-d rounds..A.S tbe data covet-ed a wide range of issues, and botbqualitative and quantitative analyses were used, the resultsand discussion are presented concurretitly.
Results and discussion
• .ST.VRTtNG AND t'lNtSIUNG TtMKS Ot- \V.\RD RCH'NDS
Tbe ward rounds tt-aditiotially occurt-ed at a set titne on aset day of tbe week. Wbile tbe ward rounds started witbin afew tninutes of the scheduled titne, tbe finishing titnesvaried considerably. Tbe sbortest ward round in tbesatnple was 35 tninutes; tbe longest 2 bours.
• TOTAt, NUNttita? ot- PAftKNT CASKS ANt> t'Rt-.Ql KNCY Ot'
NTRSt-: c:ON TRlBr rtONS
Tbe ward tiurses participating in tbe tnultidisciplinarygt-()up tneetitigs contributed verbally to 81' \ , (107) of tbepatient cases, ln 19",, (25) of patient cases, tbe nurse tnadeno verbal cotitribution. Tbis supports finditigs by otberauthors (Brink, 1972; Kngstt-otn, 1986), tbat nut-ses werenot routitiely expected to present tbeir view for everypatient case. Tbis raises tbe question of tbe value given totbe nursitig input by tbe team.
• CONTt'.NT ANAt.Y.StS Ot'' N'l RSKS' VKRHAl.
CONTRllUlTtONS TO TtlK (13) Ml'I.TlDISCIPl.lNARV
Mt-',t'.TtN(;S
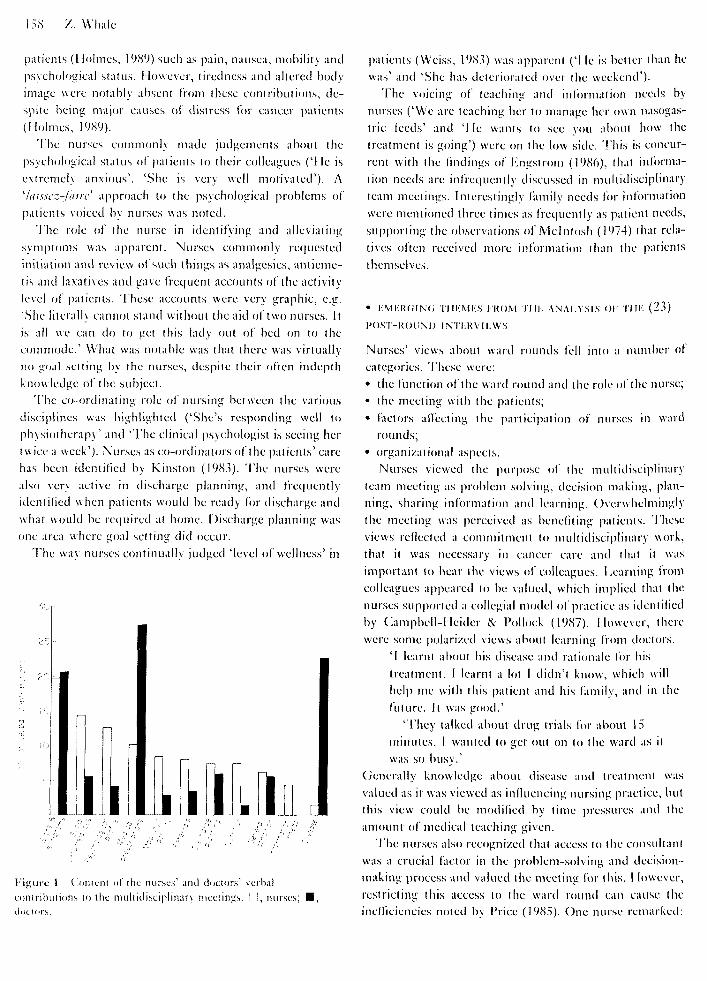
Tbe content atialysis of tlie verbal contributions ot thenurses present at tbe tnultidisciplinary tneetings is pre-sented in Figut-e 1, witb tbe doctot-s' contributions in-cluded lor comparison. Tbe nurses" contributions covet-eda tutniber of 'quality of life' itidicatot-s identified b\ caticer
158 Z. Whale
pattetits (I lolmes, 19<S9) such as pain, nausea, mobility andpsycholotjical slalus. liowever, lireilness and altered bodyimage were notably absent (roni ihe.se contributions, de-spite being- major causes of distress for cancer patients(Holtnes, 1989).
The nurses cotiitnonly made judgements about thepsychological status ol patients to their colleagues ('lie isextremely anxious'. 'She is very well motivated'). A'latsscz-latrc' approach to the psychological ]iroblems ofpatients voiced by nurses was noted.
The role of the nurse in identifying and alleviatingsymptotns was apparent. Nurses commonly requestedmiliation and review of sucb tbings as analgesics, antieme-tis and laxatives and gave frequent accounts of the activitylevel of patients. These accounts were very graphic, e.g.'She literally cannot stand without the aid of two nurses. Itis all we can do to get this lady out of bed on to thecommode.' What was notable was that there was virtuallyno goal setting by the nurses, despite their often itidepthknowledge of the subject.
The co-ordinating role of nursing between the variousdisciplines was highlighted ('She's respontling well tophysiothenipv' and 'The clinical psychologist is seeing hertwice a week'), .\urses as co-ordinators of the patietits' carehas been identified by Kinston (1983). The nurses werealso very active in discharge platTning, and frequentlyidentified when patients would be ready for discharge andwhat would be required at home. Discharge planning wasone area where goal setting did occur.
The way nurses continually judged 'level ofvvellness' in
UMHMgurc 1 Cotitcnt ol tlic nurses' and diicturs' verbalLontrihutions to the tnultitlisciplinary meetings. I :, nurses;tloctors.
patients (Weiss, 1983) was apparent ('I le is better than hewas' and '.She has deteriorated over the weekend').
The voicing of teaching and information needs bynurses ('We are leaching her to manage ber own nasogas-tric feeds' and 'I Ie wants to see you about how thetreatment is going') were on the low side. I'his is concur-rent with the findings of I'jigstrom (19(S6), that informa-tion needs are infrequently discussed in multidisciplinaryteam meetings. Interestingly family needs for informationwere mentioned three times as frequently as patient needs,supporting the observations of Mclntosh (1974) that rela-tives often received more information than the patientsthemselves.
• t ; . M t : R ( ; i N < i • i - t t i ; M t ; . s t ' K O M 't t t i - ; A N A t . ' i . s t . s o t ' t t t t : ( 2 3 )
t ' O . S t - t i O t j ' N t ) t N T t J i V I t A V . S
Nurses' views about ward rounds fell into a number ofcategories. These were:• the ftinction of the ward round and the role of the nurse;• the meeting with the patients;• factors affecting tbe partieipation of nurses in ward
rounds;• organizational as|K'cts.
Nurses viewed the |-)tirpose of the multidiseiplinaryteam meeting as problem solving, decision making, plan-ning, sharing information and learning. Overwhelminglythe meeting was perceived as benefiting patients. Theseviews reflected a commitment to multidisciplinary work,that it was necessary in cancer care and that it wasimportant lo hear the views of colleagues. Learning iVonicolleagues ajipeared to be valued, which implied that thenurses su|iported a collegial model of jiiactice as identifiedby Canipbell-lleider & Pollock (1987). However, therewere some polarized views about learning from doctors.
'I learnt about his disease and rationale for fiistreatment. I learnt a lot I didn't know, which willhel]:) tTie with this patient and his family, ancl in thefuttire. It was good.'
'They talked about drug trials for about 15minutes. I wanted to get out on to the ward as itwas so busy.'
(jenerally knowledge about disease and treatment wasvalued as it was viewed as influencing nursing practice, butthis view could be modified by time presstires and theatnount of medical teaching given.
The ntirses also recognized that access to the eonstiltantwas a crucial factor in the problem-solving and deeision-tnaking process and valued the meeting for tbis. 1 lowever,restricting thjs access to the ward round can caitse theinetlieieneies noted by I'rice (1985). One nurse remarked:

Nm-scs" p;n-tici|-)alii)n in wartl rounds
'Decisions can be delayed because you are waitinglor the i-otuul. Let's lace il, jtuiior doctors cati'tchange anytiiitif!;. You know what should be dotiebut yott can't act on it straight away.'
Goal scttmg was \icwed as an important Ititictioti ol tbeward round. .Althottgli goal .setting can be seen as animportant cotii]ioticnt ol clccisioti tnakitig (Pt-cscott cl ni,1987), it bad been tioted Irotn tbe tape recordings tbat theconsultants, rather tban the nurses, were the goal setters.
Nurses viewed tiic t-olc o( tiic tutt-sc in the ward t-oundsin tlic followitig way:• being itivolved in decision niakitig,• puttitig forward nurstng knowledge,• speaking on behalf ofthe patient,• learning,• co-orditiatitig the diseiplities,• guiding nunsiiig practice.
ISeitig itivolved iti tleeision making was expressed repea-tedly by niu-ses. Some nurses idcntilicd their pivotal role indeeision making as they felt able to make or bt-eak adecision by 'manipulation' or 'blocking'. Awareness ofthehumanizing r-olc ol nursing input (Pctci-son, I9(S(S) wasnoted in ibc conmioti phrase 'presenting patietits aspeople'. There was also awnrcncss of knowledge thai onl}nurses held, whieb supports the iinditigs of Mallik (1992)..'\n example was the discussion abotit an elderly palient theconsultant wanted to keep in hospital until her radiother-apy reactioti bad stibsided (jiossibly a lurlber Ibrttiigbt).The nurse contribtitcd: 'She is eating very littie het-e. Sheis still sore. Hut she actually cats tnore at home when she ison weekend leave than she does bcrc. I ler daughter is tlict-cand j-it-eparcs all ber food. 1 think she'd be belter olV alhotnc'
Nurses did see thetnselvcs as co-ortlinators of patientcat-c, a view that bas beeti t-ecognized by organizatiotialstudies inio hospital cat-c (kinstoti, ]9(S.i).
Tlic meeting wilh tbe palients was seen as overwliehii-itigly ttnsalislactory, producing barriers to conmuniicationand confidentiality. These views are reflected in the com-ments of jiatietiis (.Steele &: Morton, 1978). Sotne a.s]ieetsre]iorled by nurses, such as misleading ]iaticnts or detncan-ing them, appear so cxlreme as to sup]iorl the observationsol f figh (19cS9) that pr-oicssioiials arc tiot sensitive to theauthority and power ihey possess. Certainly the cancerpatieni is vulnerable (l'urlong, 1982) and eointnunieationwilh ]iatieiits docs seem an important area of collaborationbetween doctors and nurses. However, the views ol thenurses in ihc present study suggest that the ward roundfortnat is totally inappropriale for conitntinicatitig eflecti-vely wilh cancer patients. Otie nurse said:
' I he patieni will not tell ihe cotisultant what's on
their mind because there are six people routui thebed. lake |the patietii's natiie] today. She is verytiept-cssed atu! there was no wa> he |the constiltant|was goitig 10 get an\ thing out of her. She told himshe was line. 1 had lo point this out to himfollowing ihe roiuul. 1 le agreed he should see herlater on his own. The walk round is a sham. Itachieves nothing."
Positive aspects ot the meeting with the patients wereexpre.s.scd tnuch less bul iinohcd the iiiiporlancc o/ ihcconsuUanr meeting and talking with the patietits. Onentirse commented:
Tie is incredibly anxious. I've spent a lot of timewilh him and his family, atid he's spoken to |tliejunior doctor |, but he really needed to hear it fromthe horse's mouth. He got that today and he'sbctier for it.'
l'actors allecting partieijiation in ihe ward round asperceived by these nurses could be summarized as doctornurse relationships, personal eharactcrislics ot the nurses,and relationships with jiatients. The consultant's be-haviour was v'lcwcd as a major factor afiecting participa-tion, detnonstraied in comments sucb as being 'ignored','.spoken 10 abruptl}' or 'allowed to speak". Relationshipswith the junior doetor and the nurse were also iVequentlymenlioncd. l'"ivc nurses described how the junior doctorpresciited intbrmation which they had got from die nursebefore the ward round began.
i"tl iiaci a cluu with |thc junior iloctor( hcfbt-chatul.She then knew everything 1 knew about thosepatients, aiul we decided what we wanted iloneanyway, belore we got to the ward round. So 1il!dti"t cotilribute much, and that"s that."
'lie said all these things which had come rrt)inme live minutes belore the wartl rt)utul began . . . sowhen he |the coiisullant| asks il \()u"\c got anythint;10 add, lie"s already said il all! ll makes me teel verysubmissive."
The degree to which the nurse contributes to theknowledge ofthe junior doctor then goes oti to afiect theparticiiiation of that nurse in the ward round.
Persotial factors such as confKleticc, experience, asscri-i\eness and beliefs about nursing were ideniilied as alFeci-lng participation. Nurses were cotisctous oftheir pet-sotiallimitations and the way it afleeted their behaviour. Somentirses also showed some awareness of ihcir limited contri-butions, even when llie\ had gone into the round withspecilic intentions. This showed some awareness oC Mal-lik's (1992) observations ihal tuirscs' expcctatiotis wet-e notalways matched by their behaviour.
Knowing jiaticnts and their taniilics, caring for them

160 Z. Whale
ami being adie to speak with conviction and confidence ontheir behalf were seen as major factors influencing partici-pation. This sup|iorts the findings of Mallik (1992) andHusb\ & (iilchrist (1992).
Organizationally, time managenietit was seen as a prob-lem in ward rounds due to conflicting demands, variablelength of ward rounds ant] fragmentation of care caused bymore than one nurse participating in the round. Sugges-tions for minimizing these jirobletns included reviewingthe starting times of ward rounds and holding them duringthe overlap of nursing shifts (the afternoon). Obstacles tochange were fbrseen, which tnainly involved tbe threat !omedical prestige. However, it was suggested hy somenurses that dialogue with doctors might open the debateand enable changes to be piloted.
• ( ) l i S l . t ( \ \ r i ( ) \ O l - t l l K ( 3 ) M l t . t t D t S C t l ' t . I N A K V t l ' : A : V t
\ t l . l . t l \ ( i . S
Ohscrsation of the mtiltidisciiilinary tneetings illutninatedthe wa\ in which the consultant directetl the group indialogue and decision making. This supports the observa-tions of Weiss & Remens (1983). The behaviour of theconsuhants demonstratetl, to a greater or lesser degree,'chairntanship skills' (Rackham & Morgan, 1977). Theyinvited contributions from other tnembers of the group bydirect questioning of individuals, or general questioningcoupled vviih scanning of the group. Other behavioursnoted from the consultants were prolonged eye contact,active listening and supportive gestures stich as noddingand smiling. By encouraging dialogue in this manner, theavailable infortiiation could be summarized and a decisionciirectecl. The nurses demonstrated active listening, pro-longed eye contact with speakers, supportive gestures andnote taking. The nurses continually responded to bothverbal and non-verbal cues from the consultant. Speakingwithout a CLie (e.g. a direct question or establishment of eyecontact) was virtually absent, Weiss (1985) and Mallik(1992) tertned nurse behaviour in ward rounds as ']xissive'.In the present sttid\, a more accurate term for the nurses'bcliaviour was lelt to be 'reactive', contrasting with tbeproactive l)ehaviouf of the consultant.
t t l . . \ A t t k i : A.Xt) t'A I t t . t ( \ '
t R t l t t l ' I O N S
l'' II tl-: .\'t KSF.S VKIUiAI.
.'\nalysis of the verbal contributions confirmed the reactivenature of the nurses' behaviour. (Contributions were codedas 'reactive' or 'proactive'. In a reactive contribution thenurse responded to a problem or agenda introtluced byanother member of the team. In a proactive contribution
the nurse introduced a new problem or agenda into thedisctission. I'jghty-three per cent of all nurse contributionswere coded as reactive and, conversely, 17",) as ])roactive.Nurses' reluetance to contribute proactively may well haveimplications for jiatient eare, for example failing to alertthe multidisciplinary team to patient problems.
Despite the reactive nature of their contributions, thenurses consistently gave detailed elaborations of patientexperiences whieh enriched, htimani/ed and justified thetnultidisciplinary discussion. The use of elaboration bynurses gave a unique insight into the patient as anindividual by recounting wbat tbey bad achieved, what tbepatient felt and had said abotit their circumstances. lMfty-five per cetit of the tiurses' contributions were coded aselaborative and 45",, non-elaborative. Cotnpare these non-elaborative and elaborative responses:
ctJt;. Do the relatives know the situation.''NI:RSK. Yes.
c:t_iK. We need to aim for home.NURSK. Yes.
ctii',. This man is dying, do you know what he thinks.'NURSF.. I think he does know, but he wouldn't volunteerhow he is feeling, you have to sqtieeze it out of him. lieknows . . . to me he just says he is miserable, but he hastalked to liis family, he has made his will, he has told hiswife he wants to stay here. I le's a very private gentletnan,not very emotional . . . bttt he does know.
cm;. I low is he doing.'NUR.si-:. I hope his mental state improves, as I think he willthen be more positive about eating . . . I ho]ie that's goingto be (he case, but talking to the family, this is reallygetting dreadftil for them now, beeause they feel he has gota change in personality. This isn't their father at all, he'ssnappy and aggressive towards them, lie's a different tiianthan when he came in. I Ie needs rehabilitation, he feels wehave created his ]iroblems rather than treated them, andhe's so unhappy.
Although other membets of the team occasionallyoflered elaborative contributions about individual patients,all nurses regttlarly and consistently provided this sort ofinsight for the rest of the mttltidisciplinary team. Thistnaybe evidence ol nurses' abilities to 'think nursing'(Ferry, 1985), yet ironically, this ability was demonstratedmainly in res]:)onse to cues from the medical stall. NursingIS characterized by direct, at times prolonged, unstruc-tured and intimate contact with patients, whereas, forexample, tnedicine is characterized by 'brief, highly struc-tuted, almost ceretiiotiial interactions' ((.atiipbell-I leider& Polloek, 1987). (Certainly, the elaborations coded for
Nurses' partici]iation in ward rounds 161
junior doctors and consttltants were of a different nature.Junior doctors' elaborations were primarily concernedwith pathophysiology, i.e. ittdividualized but impersonal.Consultants elaborated at length, in a way that reflectedboth their confidence in their teaching role and tbeirawareness of their accountability in decision making. Theirelaborations were of a more general nature btit took a moreholistic view of patietit care, e.g. 'treatmetit of the elderlypatient with lymphoma shotild consider. . .'.
The elaborations b\ the nurses seemed particularly.sought by the consultants, rather than the junior doctor, toassist in decision making about longer-tertii goals for thepatient who they live with, how they manage at home,how disabling is their condition, etc. Indeed, this know-ledge had sometimes to be prised otit of the nurse! Thiswas evidenced by often lengthy and detailed dialoguebetween the cotisultant and ntirsc. What atithors such asPerry (1985) describe as the domain of tiursing (interactingand meeting the psychosocia! atul physical needs of indi-vidttals and groups) seem crttcial for the execution of acancer specialists' work. The cotisultants seem consistentlypatietit-centied in a way that the jtmior doctor did not, andthis resulted in a difVetencc in dialogtie between nurses andjunior and senior doctors. These observed differences hadnot been suggested by the review of the tloctor nurseliterature.
• A N A t . ' i S t S o t ' ' l ' t N t ) t N < ; S I ' O R c ; t I R A f t Vts A N t ) t ' A l . t . t A T t \ I .
T I t t ' . R A P Y
The rationale for this analysis stemmed from the argu-tnents abotit cute atid care, which are often presentedhistorically as a ftindatiiental difference in the approach ofmedicine and ntirsing, atid which has become the focus oftiiuch nursing literatttre (Watson, 1985; (iadow, 1988). Itcould be argued that iti ]iallative care, where conilort goalsare a priority and medical intervention is limited, nursesmay have a more active role to jilay.
However, there was no difTerence in the content ornature of the ntirses' contributions for palliative andcurative patient cases. The contributions only varied in sotnttch as iisychophysiological ]iroblems discussed wereusually treatment-related in curati\e care and disease-related in palliative care. Many of the lengthiest contribu-tions by nurses, and the richest dialogue, concerned elderlypatients having curative treatment. The disabling cHect oflong courses of treatment on the elderly came over timeand time again.
(-aritig may be the legitimate domain of tittrsitig btitwbetlier professional caring is, or should be, the doniaiti ofone discipline is a point worthy of debate.
• Rt'.PORTtNCi OF PATIF.NT PROIit.KMS liY N l KSFS AND
St'tiSt ' .Qlt ' .NI' t)FC:tStON .MAt^lNCi
There were a total of 91 reports of patient probletns b\ thenurses involved in the tiitiltidisctplinary team meeting.Seventy-one (78",,) of these reports progressed to a de-cision being made abotit how to deal with the problem.This reflects an important role of the nurse in the manage-ment of patietit problems. This input of the nurses, astioted previously, was tiot synonytnous with making thedecision. This role was reversed tnainly for the consultantand supports finditigs by Prescott (7 al. (1987). Conversely,20 of the 91 ]iroblems raised b\ nurses (22'-\^) appeared notbe acknowledged by the group and did not result in adecision. This commonly involved idetitification of a ps\-cbological problem in a patient such as 'extremely anxious'or 'very depressed'.
• tMFhKRt'NCF.S ACROSS W ARt) ROl NDS
:\nalysis was not possible as a breakdown of the differentward rounds ]irodticcd very small numbers of incidencesfor contributions, decision making and content. However,as a general itnpression, the main difTcrenccs across wardrounds were the \ariation in cbairmanship skills of theconsultant and the tnarked variation iti the performance ofthe participating ntirse. .'\t otie extreme the nurse seemedto perform poorly on behalf of patients by responding onlyto direct questioning and giving minimal elaboration. .\tthe otber extreme the ntirse used the ctie from tlicconsultant, tiot only to elaborate the point under discus-sion, but as a platfbrtn to present other issues and prob-letns. The 'good performers' were observed at times tocontribute without any identifiable cue although tliis wasrare in the data.
Conclusions and reconinicndatiotis for clinicalpractice
The speciality of cancer care, the ward organization andthe attributes of the multidisciplinarx team make tlicfinditigs of this study contextual. Thetnes ha\c emergedwhich find support in the literature and new areas forstudy have been highlighted.
Harriers to tbe participation of nurses in ward roundscould be personal, notabh lack of asserti\encss, lack oiexperience and lack of clarity of role. Ikiia\iour of theconsultant was also a major factor affecting participation.Knowing and directiv caring for patients and their fatiiilieswas viewed by nurses as itifluencing participation.
The performance of the nurses dttring the warii rounds
162 Z. Wha
varied etiortnotislx. \e \er t l ieless , llie detailed elaboratiotis
ijivcti h\ nurses about patients played a tnajor role iti tlie
t;'r()Li|)s' decisioti tuakitig'. The nieetitii^ with the jiatients
was seen h\ ntn-ses as overwhelmingly un.satislactory,
producinu' harriers to comtntniicatioti and cotilidenttahty.
There ajipears to he a great need lor the Ititictioti o l t he
vsai'd routid to he iitiilerstood by the disci|)line.s. This
wDuld enable each participant to be clear about their role.
Such issues as tutrse i')articipalion, consultation between
paueni and tonsiihant, decision making and medical
teachnig need to considered. Nurses could then submit a
clear statement of their i'>hilosoj')hy anti intent regarding
their participation in ward round.s.
It shuuii.! tidt, however, be assutned that nurses will
])erlorni well in ward rountls ll they at-e 'allowed' to by the
other disciplines. Training needs should also he coti-
sitlcrcd. These nia\ encompass assertiveness, negotiation
anil chairmanship skills. Nurses traditiotialh pt-csetit writ-
ten care studies during their training, but also need to be
competent in verbal case presentation, (lonlidence in the
unic|ueness ofthe nursing input, an awareness of nursing
knovvleclgc and the benefit ol this approach to patients
needs to be nurtured, further research into the relation-
ship between nursing input and patient otitcomes will he
necessary to add strength to this argument.
I he study also highhghted the time and resources
investetl in ward rounds. Understatuling ol roles atul
training needs ma\ indeed tnake the ward round a mot-e
efiectivc meeting (or all involved. I lowever, changes in
wartl round format will almost certainly be necessary as
well. One example would be a private consultation
between ]iatient and consultant after the multidisciplinary
meeting. .Another tormat coukl involve both the consultant
antl the tiurse meeting the patient. Options therelore need
to be considcretl and |)iloted.
It is suggested thai these changes would im|')rove the
qualits ofinteraciions between disciplines and improve the
etleclivcticss of the cancel- service.
.Acknovvlcdgmcnt.s
The author acknowledges Hriati Millar and Angie Tilchen.
The lull text (if this studs is available at the University of
Wales' College of Medicine Library, Heath I'ark, (lardilF.
Ihis stmly was funded by the Institute of Nursitig,
Oxford, via the WOrshiplul (Company ol Barber .Surgeons'
Postgraduate Scholarship in (llinical Nursing (1991 92).
Refe rences
Ik'iincr P. (I''>S4} from \ovuc lo l',\fieri: l.xrcllcncc ami Power inC.litnial N'ld'.im! I'l'iii llie. AtUlisiin Wcslcv, (.alilorni.i.
Brink P . | . (1V72) Kolc ilislancc: a inaiKicuvcr in nur.sinii. Nursing
forum 111(2), M:-, :-,.U.
l i u s b v A . & ( i i k h r i s l l i . ( 1 9 9 2 ) T l u - r o l e of l l i c l u i r s e i n l l i c m e d i c a l
u;ir(l rmmd. Journal of .lilvaiiccil Nursing 17, .t.^'' 346.Canipbcll-I Iciik-r N. & Pollock I) . (]'),S7) l iarricrs lo phy.sician
nurse colk-j^ialilv: an aiillinipological pcrspccl ivc. .Sonal Science
and Medicine 25(.s), 421 42.S.
C.anct-r Relief Macmil lan I-'uiuI (l'),S,S) Public alliludc-s lo and
kn()v\Ictljic (li cancer u\ ihe i j . K . Nursing Iniu's 84(1K), 22.
I )er(.liarian A. (I9(S7) liif'Drinalion needs o l r eccn l ly diaj;iii).scd cancer
pal ienls . P a n s I and I I . Cancer Niirsiiit; lf)(2 and 3), 107, 156.
la igsl roni H. (19(S6) Coninuinical ion ami decision-niakinn in a study
(if ihe mullicliscipliiiarv leani conference wilh ibe regislcred nurse
as eonlerenee cbairnian. hilcrualional Journal oj Nursing Studies
2.3(4), 2'W .?!-!.
I'uriono; R.C..S. (19(S2) Personal meanings in cancer. In Personal
Alcanings (.Shepherd !•;. cS; Watson J.P., eds). John Wiley and.Sdiis, ( Jiichesler.
(Jadbdis (;., l.ogeay P. cV Maline J. (I9K8) Medical sebednles andlime nianaj^emenl in luirsinf!;. In Stress and Oriiaiiisalionat Priih-
Icnn ill IlitipUiih, (Wallis 1). & dc WollVC.J., eils). Crodiii Helm,London.
(iadovv S. (19H.S) Cdvenani wiihout eure: leiiing go and boUling (inin chrdnie illness. In The h'thics of Care and ihc i'.tliics oJ (>nre:
Synthesis and Chronicity (Walsdii j . & Ray M , eds). Nalional
l.caiiue lor Nursinp;, New York.
IIif!;li D . M (1989) Tri i l l i lc l l ing, cdiirulenliality und ibe dying
p.\licnl: lKSv dilcninias ior llie nurse . A''//r.s;;/i; I'lirinii 24(1), 5 I I .
I lolnies .S. (1989) Use (if a mollified synipKini i l isuess .scale in
assessmeni df the canecr palienl. liitcriiiitional Journal of Nursing
Sliiilies 2(>{ 1), W 79.I I d l n i c s .S. & D l c k e r s o n J . W . ' I ' . ( 1 9 8 7 ) T b e q u a l i l y o f l i fe : d e s i g n
a n d e v a l u a l i d i i o l a s e l l - a s s e s s n i c n l i n s l r u n i e n l l o r u s e \ \ i l l i c a n c e r
palienls. International Journal of Niirsiiif, Studies 24, 15 24.KinsKin \\\ (1983) I lospilal orj^anisatidn ami strucuire, anil its ellcct
on inlerprotessioiial belnivioLir and llie delivery dl care. Social
Scicmc and Medicine 17(16), 1 159 1 170.l.illey I,. (1987) I lunian need fullillnienl alteralion in l l iecl icnl vvilli
u ter ine cancer. Cancer Nursing 10(6), 327.
Mallik ;V1. (19<)2) T b e role dl tbe nurse on ihe consul tan t ' s ward
round . Niirsiiii; Times 88(5), 49 52.
Vlajjuire P. (1978) T h e psyebdlogical ellccls of cancers and llicir
Irealnienls. In Oncology /or Nurses and Ilealtluare Projcssiouiils,
(Tillany R. eil.). Vol. 2. I larper and Rdvv, l.onddii.Manllicy M (1978) flic Practice of Primary Nursing, Blackwell
Scienli l ie Publicalidiis, Oxford.
Miilnar l'"eif!;er S. & Schni iu M.I I. (1979) Colicj'ialily in iiUertliscip-
linary lieallh leanis: ils nicasureiiicnl and ils edec ls . Social Science
and Medicine I .M, 217 22').
Perry (. (1985) l i a s (he discipline of nursing ilevelopeil Id the slage
where nurses d(i ' think nurn\ny:'? Journal oJ Idvanccd Nursing 10,
31 37.
Pelersen M. (1988) T h e iidrnis anil values liekl by llirc-e grouiis (if
nurses e(incerniii[i; psychdSdcial nursinp; jiraclice. Inleriiational
Journal of Niirsiny, Studies 25(2), 85 103.Prescdll P.A., Denn i s K.\\. & jacox A.K. (1987) Clinical decision
making df stall nurses. tM.IGt;: Journal of Nursing Scholarship
19(2), 56 62.I'riee li. (19X5) Your movi-, nurse. Nursing Times H4(41), 24 2().

Nurses' participation in ward rounds 163
Rackham N, S; Motgan T, (197/) Behaviour .-Inalysis in 'Praining.
,Vlc(itaw-l lill, I,ondon,Steele S,J, & Motion I), | ,l!, (1978) The ward round, LanccI, i,
8,S- 86,Stein L,, Watts n , T , & I lowell T, (1990) The doetor ntu-se gatiie
revisited. Nursing Outlook ib, 264 268,Von Mssen I., & Sjodeti P, (1991) Tbe itnportance of nurse earing
bebaviouts as perceived by Swedish hospital patients atul nursingstall, Inlernalional Jmirnal of Nursing Studies 28(.i), 267 281,
Walsh M, & I'ord P, (l')89) Nursing Rituals: Research and Rational
.Ictioiis. I leinetiianti Nursing, Oxford,Watson J, (198,S) Nursing: Human Science and Human Care. Apple-
ton-(x'ntury-('n)lts. New ^'ork,Webb (!, (1987) Frofessionalistn revisited. Nursing Tunes 8.3, M) 41,
Weiss S,l, (198.i) Role ditrcrcntiation between tuirse and physician;itiiplications for nursing. Nursing Research 32(,i), I,i,v-Li9,
Weiss S,], (198,^) The inlluence of discourse on collaborationamongst nutvses, physicians and eon.sumers. Research ni \ursingand Ileallh 8, 49-59,
Weiss S,l, &; Retnen N, (1983) Self limiting patterns of tiursingbehaviour wilhin a tripartite context involving cotisuniers andphysicians, Western Journal oj \ursing Research 5, // 89,
Weleh-McCailVey D, (198,S) Cancer, anxiety anti the quality ol'life.Cancer .\iirsing 8(.i), >\.
Wiggins |,11,, Donovan li,. Redman S, & Saiison-l"islier R,W,(1990) Cancer patients" satisfaction with cate. Cancer 66(1),610 626,






























