Embed Size (px)
Citation preview

The Pediatrics Milestones: Conceptual
Framework, Guiding Principles, and
Approach to Development
Patricia J. Hicks, MD
Daniel J. Schumacher, MD
Bradley J. Benson, MD
Ann E. Burke, MD
Robert Englander, MD, MPH
Susan Guralnick, MD
Stephen Ludwig, MD
Carol Carraccio, MD, MA
Editor’s Note: The online version of this article contains 3
APPENDICES on practice-based learning, personal and
professional development, and patient care, respectively.
The ACGME Outcome Project Evolves Into theMilestone Project
The Accreditation Council for Graduate Medical Education
(ACGME) Outcome Project shifted the focus of the
accreditation aspects of residency training from the process
of education to the outcomes of programs. The Assessment
Toolbox, a product of collaboration between the ACGME
Patricia J. Hicks, MD, is Director of the Pediatric Residency Program at TheChildren’s Hospital of Philadelphia and Professor of Clinical Pediatrics in theDepartment of Pediatrics at University of Pennsylvania School of Medicine;Daniel J. Schumacher, MD, is a Clinical Fellow in Emergency Medicine atCincinnati Children’s Hospital Medical Center and in the Department ofPediatrics at the University of Cincinnati College of Medicine; Bradley J. Benson,MD, is Med-Peds Program Director at the University of Minnesota AmplatzChildren’s Hospital and Director of the Division of General Internal Medicine andAssociate Professor of Internal Medicine and Pediatrics at the University ofMinnesota School of Medicine; Ann E. Burke, MD, is Director of the PediatricResidency Program at Wright State University, Boonshoft School of Medicineand in the Department of Pediatrics, at the Dayton Children’s Medical Center;Robert Englander, MD, MPH, is Senior Vice President of Quality and PatientSafety at the Connecticut Children’s Medical Center and Professor of Pediatricsat University of Connecticut School of Medicine; Susan Guralnick, MD, isdesignated institutional official (DOI) and Director of Graduate MedicalEducation at Winthrop University Hospital, Associate Professor in theDepartment of Pediatrics at Winthrop University Hospital, and AssociateProfessor in the Department of Pediatrics at Stony Brook University School ofMedicine. Stephen Ludwig, MD, is designated institutional official (DOI) andChairman of Graduate Medical Education at Children’s Hospital of Philadelphiaand Professor of Pediatrics and Professor of Emergency Medicine at University ofPennsylvania School of Medicine; Carol Carraccio, MD, MA, is Associate Chair forEducation at University of Maryland Hospital for Children, and Professor in theDepartment of Pediatrics, University of Maryland School of Medicine.
DOI: 10.4300/JGME-D-10-00126.1
Abstract
Background The Accreditation Council for GraduateMedical Education (ACGME) and the American Board ofPediatrics (ABP) have partnered to initiate the PediatricsMilestone Project to further refine the 6 ACGMEcompetencies and to set performance standards as partof the continued commitment to document outcomes oftraining and program effectiveness.
Intervention Members of the Pediatrics MilestoneProject Working Group searched the medical literatureand beyond to create a synopsis of models andevidence for a developmental ontogeny of the elementsfor 52 subcompetencies. For each subcompetency, wecreated a series of Milestones, grounded in theliterature. The milestones were vetted with the entireworking group, engaging in an iterative process ofrevisions until reaching consensus that their narrativedescriptions (1) included all critical elements, (2) werebehaviorally based, (3) were properly sequenced, and
(4) represented the educational continuum of trainingand practice.
Outcomes We have completed the first iteration ofmilestones for all subcompetencies. For each milestone, asynopsis of relevant literature provides background,references, and a conceptual framework. Thesemilestones provide narrative descriptions of behaviorsthat represent the ontogeny of knowledge, skill, andattitude development across the educational continuumof training and practice.
Discussion The pediatrics milestones take us a stepcloser to meaningful outcome assessment. Next stepsinclude undertaking rigorous study, making appropriatemodifications, and setting performance standards. Ouraim is to assist program directors in making more reliableand valid judgments as to whether a resident is a ‘‘gooddoctor’’ and to provide outcome evidence regarding theprogram’s success in developing doctors.
The working group would like to thank Ms Lisa Johnson and Dr Jerry Vasiliasfor their support and constant encouragement of the group. Theircommitment to the Milestones Project has been invaluable.
Corresponding author: Patricia J. Hicks, MD, Children’s Hospital of Philadelphia,Main Hospital 9NW, Room 64, 34th & Civic Center Boulevard, Philadelphia, PA19104, 215.764.7973, [email protected]
Received July 12, 2010; revision received July 23, 2010; accepted July 28, 2010.
PRACTICAL ARTICLE
410 Journal of Graduate Medical Education, September 2010

and the American Board of Medical Specialties (ABMS) was
offered to the graduate medical education (GME)
community as a resource and to stimulate further work on
assessment.1,2 Despite the availability of this and other
resources, individuals and institutions continue to struggle
to define the optimal method for measuring achievement in
the competencies.3 Hence, the work of the ACGME
Milestone Project, which seeks to take the next steps in
advancing educational outcome assessment in GME, is of
critical importance. These benchmarks, or milestones of
knowledge, skills, and attitudes (KSA), will document
increasing mastery of the 6 competencies.2,4 The ACGME
goal in creating milestones for every specialty is to ensure
that programs and the ACGME will collectively be able to
certify to the public that the residents are competent to
practice in their specialty without direct supervision at the
end of their training.
The Pediatrics Milestone Project BeginsIn early 2009, the ACGME and the American Board of
Pediatrics (ABP) jointly launched the Pediatrics Milestone
Project. The goals of the project are to (1) reframe and
further define the 6 competencies in the context of the
specialty of pediatrics, (2) identify markers of achievement
along the continuum of GME, and (3) identify tools that
could be embraced by the pediatric community as
meaningful measures of performance. We assembled a 10-
member working group (2 of the 10 were staff members),
composed of members of the Association of Pediatric
Program Directors (APPD), 1 member of the Medicine-
Pediatrics Program Directors Association (MPPDA), 2
representatives of the ACGME, and 1 resident member. We
also created an advisory board, whose members were
selected from the sponsoring organizations and from other
highly regarded national leaders in medical education, to
guide us in our work, which began in April 2009.
Foundational Work for the Project: Guiding Principles andConceptual Considerations
The first task of the Pediatrics Milestone Project Working
Group (the authors of this article) was to construct Guiding
Principles and Conceptual Considerations. These
foundational documents, drafted in May 2009, provided the
scaffolding for the working group, guiding us in both the
approach to the work and in the actual construction of the
milestones. The importance of defining the continuum, from
undergraduate medical education (UME) through GME to
the continuous professional development (CPD) of
Maintenance of Certification (MOC), is reflected as a
central goal of the working group in both of these
documents (T A B L E S 1 and 2 ). An example of a key
guiding principle is that ‘‘the ACGME competencies are
PRACTICAL ARTICLE
Journal of Graduate Medical Education, September 2010 411
necessary, but may not be sufficient, in defining milestones
for professional formation of pediatricians.’’ Although not
part of the original charge, the working group saw this
reflective process to identify implicit subcompetencies that
should be made explicit as the first essential step in
addressing the refinement of the competencies for our
specialty. As such, we began an ongoing dialogue with the
membership of APPD at their spring 2009 meeting.
Attendees were asked to consider possible subcompetencies
that are not explicitly articulated in the current ACGME
competencies. Coding responses and discerning major
themes produced the personal and professional
development subcompetencies displayed in T A B L E 3 ,
which were added to the subcompetencies included in the 6
ACGME competency domains of our program
requirements.
A key area of focus for the conceptual considerations
was a developmental model, both in creating the milestones
and in setting performance standards. We anticipated
creating narrative anchors of behaviors to serve as a
learning roadmap for trainees and to contribute to the
establishment of normative ranges of behaviors to help
educators define performance standards, recognizing that
there would be some variation across learners and contexts.
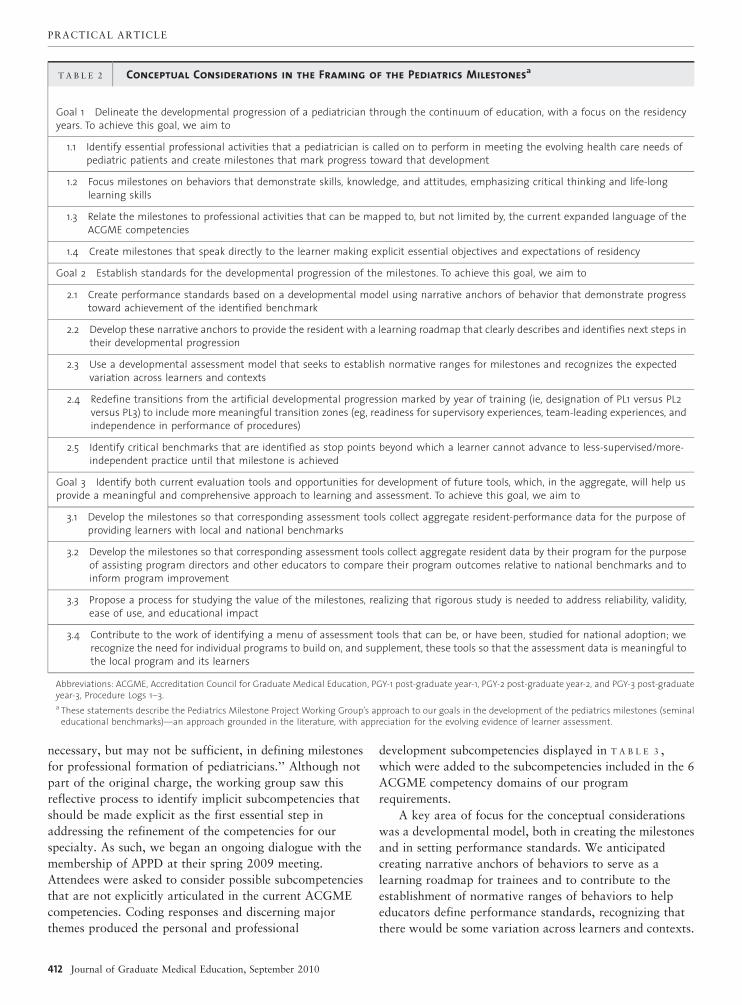
T A B L E 2 Conceptual Considerations in the Framing of the Pediatrics Milestonesa
Goal 1 Delineate the developmental progression of a pediatrician through the continuum of education, with a focus on the residencyyears. To achieve this goal, we aim to
1.1 Identify essential professional activities that a pediatrician is called on to perform in meeting the evolving health care needs ofpediatric patients and create milestones that mark progress toward that development
1.2 Focus milestones on behaviors that demonstrate skills, knowledge, and attitudes, emphasizing critical thinking and life-longlearning skills
1.3 Relate the milestones to professional activities that can be mapped to, but not limited by, the current expanded language of theACGME competencies
1.4 Create milestones that speak directly to the learner making explicit essential objectives and expectations of residency
Goal 2 Establish standards for the developmental progression of the milestones. To achieve this goal, we aim to
2.1 Create performance standards based on a developmental model using narrative anchors of behavior that demonstrate progresstoward achievement of the identified benchmark
2.2 Develop these narrative anchors to provide the resident with a learning roadmap that clearly describes and identifies next steps intheir developmental progression
2.3 Use a developmental assessment model that seeks to establish normative ranges for milestones and recognizes the expectedvariation across learners and contexts
2.4 Redefine transitions from the artificial developmental progression marked by year of training (ie, designation of PL1 versus PL2versus PL3) to include more meaningful transition zones (eg, readiness for supervisory experiences, team-leading experiences, andindependence in performance of procedures)
2.5 Identify critical benchmarks that are identified as stop points beyond which a learner cannot advance to less-supervised/more-independent practice until that milestone is achieved
Goal 3 Identify both current evaluation tools and opportunities for development of future tools, which, in the aggregate, will help usprovide a meaningful and comprehensive approach to learning and assessment. To achieve this goal, we aim to
3.1 Develop the milestones so that corresponding assessment tools collect aggregate resident-performance data for the purpose ofproviding learners with local and national benchmarks
3.2 Develop the milestones so that corresponding assessment tools collect aggregate resident data by their program for the purposeof assisting program directors and other educators to compare their program outcomes relative to national benchmarks and toinform program improvement
3.3 Propose a process for studying the value of the milestones, realizing that rigorous study is needed to address reliability, validity,ease of use, and educational impact
3.4 Contribute to the work of identifying a menu of assessment tools that can be, or have been, studied for national adoption; werecognize the need for individual programs to build on, and supplement, these tools so that the assessment data is meaningful tothe local program and its learners
Abbreviations: ACGME, Accreditation Council for Graduate Medical Education, PGY-1 post-graduate year-1, PGY-2 post-graduate year-2, and PGY-3 post-graduateyear-3, Procedure Logs 1–3.a These statements describe the Pediatrics Milestone Project Working Group’s approach to our goals in the development of the pediatrics milestones (seminal
educational benchmarks)—an approach grounded in the literature, with appreciation for the evolving evidence of learner assessment.
PRACTICAL ARTICLE
412 Journal of Graduate Medical Education, September 2010

Establishing the Scholarly Approach for the Development ofthe Pediatrics Milestones
The Pediatrics Milestone Project Working Group’s
approach was grounded, in part, by Glassick’s second
standard for assessing scholarship, calling for adequate
preparation whereby scholars show their understanding of
existing scholarship in the field.5 For our work, this
translated to grounding the milestones in the literature.
Specifically, we searched the literature for conceptual
frameworks6—theories or models that represent or inform
the approach to the developmental progression of KSA
within a subcompetency.
In this search, we sought the ontogeny of behaviors that
would represent the does level in the Miller pyramid.7
Although difficult, it was important to identify and define
constructs, or observable traits that help to represent
components of real world performance, for each
subcompetency considered. In addition, case specificity,8
one’s inability to translate learner performance from one
context to another, contributed a layer of complexity to the
design of the milestones. The complexity of case specificity
contributed an additional challenge to the design of the
milestones. Therefore, we intentionally wrote the milestones
as generic items with the addition of examples of behavioral
descriptors in a specific clinical setting, providing real-world
context. We recognize that assessment using the specific
examples offered in each milestone would yield outcomes
that may not be transferable to another context.8
In searching the literature to inform the development of
the milestones, the primary authors came to appreciate the
paucity of evidence for defining the ontogeny of the
development of KSAs for many milestones. This resulted in
an iterative process of (1) piecing together various theories
and models to address the different facets of a
subcompetency, (2) translating the models and theories
gleaned from the literature into behaviors that marked
development over time, (3) testing the sequence of behaviors
against our own empirical evidence gained from years of
working with learners, and (4) often starting the process
over again when vetting within our working group added a
different lens to the primary author’s work. This resulted in
the construction of each milestone through a process using a
‘‘succession of lenses,’’ as Harris9 describes in the
deliberative inquiry approach to curriculum design. This
iterative approach of searching the literature, building on
relevant theories and models, and then revising to
accommodate the perspectives or lenses of the working
group is a critical contribution to the construct validity of
the Pediatrics Milestone Project.10
Construction of a Pediatrics Milestone
For each subcompetency, we created a milestone document
that features a background or synopsis of the literature with
references and a sequence of narrative descriptions of
observable behaviors at advancing levels of development
across the educational continuum of training and practice.
Of note, we intentionally did not label (eg, novice,
competent) these descriptors, wanting the focus to be on the
behavior and not on the label. Illustration of the format for
the Pediatrics Milestones is shown in the F I G U R E The
Anatomy of a Pediatrics Milestone.
Initial Work in the Development of a Pediatrics Milestone
As discussed in the section on scholarship, authors initiated the
development of milestones through a thorough literature search
to identify relevant theories or models that would help to
identify a sequence of observable behaviors that would illustrate
the essential KSA embodied in the specific subcompetency.
T A B L E 3 Personal and Professional Development
Residents must demonstrate a commitment to engage in personal and professional development that will sustain them in balancing acommitment to their profession with a healthy and productive personal life. Residents are expected to demonstrate
N Self-awareness (of one’s own knowledge, skills, and emotional limitations) that leads to appropriate help-seeking behaviors
N Healthy responses to stressors
N Flexibility and maturity in adjusting to change, with the capacity to alter one’s own behaviors
N The ability to manage conflict between one’s personal and one’s professional responsibilities
N Trustworthiness (ie, a combination of clinical knowledge/skill, discernment, conscientiousness, and truthfulness) that makescolleagues feel secure when one is responsible for the care of patients
N Leadership skills that enhance team function, the learning environment, and/or the health care delivery system/environment, with theultimate intent of improving care of patients
N Self-confidence that puts patients, families, and members of the health care team at ease
N The capacity to accept that ambiguity is part of clinical medicine and to recognize the need for and to use appropriate resources indealing with uncertainty
PRACTICAL ARTICLE
Journal of Graduate Medical Education, September 2010 413

For example, in the Practice-Based Learning and
Improvement (PBLI) subcompetency of ‘‘identify strengths,
deficiencies and limits in one’s knowledge, and expertise’’
(see APPENDIX A online), the primary author first looked at
literature regarding residents’ abilities to identify their own
level of understanding, knowledge, and expertise. The
exploration of the literature on this subject reached back to
the original theory constructed by John Dewey,11 moved
through the learning theories of Kolb,12 and explored the
more recent literature by Davis13 regarding the significant
limitations to self-assessment.
As a second step, the primary author then reframed
what was gleaned from the literature in the context of
clinical practice to make it meaningful to learners, faculty,
and program directors. For example, in the PBLI
subcompetency discussed above, the author used a set of
questions that stimulates specific elements of critical
thinking14 when describing progression of developmental
milestones about ‘‘the learner’s ability to identify strengths,
deficiencies and limits in one’s knowledge and expertise’’
(see APPENDIX A online).
Using the multiple literature sources searched, the
experience with learners at different levels of education and
training, and the conceptual framework that had been
formed, the authors’ next step was to construct a
developmental progression of the individual elements of the
developmental milestones (T A B L E 2 of APPENDIX A). Careful
consideration was given to constructing the spectrum of
behaviors for each element of a given subcompetency. This
spectrum was ultimately the judgment of the primary author,
based on her understanding of the subject of self-assessment
and other relevant literature and experience with learners at
each developmental stage. Even with later vetting of these
judgments with the working group, it became clear early in
this process that the initial iteration of milestones would
require expert input regarding these judgments.
For the more complex milestones, an example was often
constructed to illustrate each developmental level. Where
F I G U R E Anatomy of a Pediatrics Milestone
Note: This example uses the Making Informed Diagnostic and Therapeutic Decisions That Result in Optimal Clinical Judgment milestone to provide select specificexamples. To view this full milestone document, with the references 2 and 3 cited in the developmental milestones below, please see APPENDIX E online.
PRACTICAL ARTICLE
414 Journal of Graduate Medical Education, September 2010

possible, a consistent context for these examples was used
along the continuum of levels within a given milestone to
aid in clarity. It is hoped that such examples may be built on
as we move forward and compile resources, such as
standardized patients or video recordings to train and
calibrate raters. These same resources could be used for
faculty development efforts.
At the end of these first 3 steps, the primary author
would then develop a written document, the components of
which are illustrated in the F I G U R E .
Working Group Vetting of a Pediatrics Milestone
Once the primary author had finished the initial
development of a milestone, this document was distributed
to the entire working group, and the process of vetting took
place during every two weeks phone calls and occasional
face-to-face meetings during the past 18 months.
In vetting the milestones, the working group applied a
modified standard-setting approach.15 In this process,
judgments about scoring of the developmental milestone
anchors within each milestone are constantly compared to
the known or familiar population of learners as they
develop from undergraduate medical education through the
level of being ready to perform without direct supervision
(graduating third-year residents) and beyond into practice.
This included defining and describing minimum cutoffs for
acceptable beginning-intern performance and the endpoints
for GME, at which the absolute minimum readiness to
practice without direct supervision is achieved.
Other important considerations during the vetting
process are included in paragraphs 1 through 5 below.
1. Close examination of the developmental milestone
anchors in the milestone document reveals that
each embraces a number of different behavioral
elements. Careful consideration was given to these
clusters of elements and whether they develop
synchronously or asynchronously, whether some
elements are ordinal (yes or no; present or absent),
or whether some elements take large jumps across
anchors versus changing in small, granular ways
within a given anchor or among anchors.16 The
nature of developmental progression for each
element was important to consider because not all
elements would progress along their specific
trajectories at the same rate. Furthermore, all
elements may not be measurable in quantitative
terms. Much like the Denver Developmental
Screening Test for assessing elements of fine motor,
gross motor, language, and social development of
children,17 progress along 1 element of development
may take place at a different rate than progress on
other elements. The measure of the learner’s
performance may also fall between specified
behavioral descriptions because the milestones
represent points along a continuum.
1. For example, we found in the milestone addressing
Competency in the Performance of Procedures that
development in some cognitive aspects of procedures
(knowing some of the steps it takes to perform a
procedure, such as contraindications, indications,
risks, benefits, etc) may develop before the
psychomotor procedural skills are developed.
2. The working group considered whether elements
within a developmental milestone anchor were
required elements and were necessary in defining a
particular developmental stage.
2. For example, the milestone of Making Informed
Diagnostic and Therapeutic Decisions That Result in
Optimal Clinical Judgment (APPENDIX C online)
speaks directly to the concept of clinical reasoning,
on which much has been written in the literature.18–21
Incorporating well-studied and delineated concepts
from this literature was thought to be a requirement
and necessary for defining particular developmental
stages, and this milestone includes a number of these
concepts, including analytic reasoning to describe the
earliest stage in clinical reasoning22 and the use of
semantic qualifiers18 (paired opposites to describe
clinical information, such as acute and chronic) and
illness scripts (narrative scripts in which the
characteristic features of specific illnesses form
clinical patterns in memory) to describe components
of more advanced stages.21,23
3. The working group also considered whether some
behavioral elements within a given cluster of a
milestone are compensatory in nature and thus, if
present, would allow a rater to assign that particular
anchor level, even if other elements of that level were
not met. The subcompetency addressing patient and
family education provides an illustration of where
some elements of an anchor might not be met but the
resident would still be able to pass to the next
developmental level. For example, if a resident
struggles with oral communication with families,
often finding it difficult to translate complex medical
concepts into simple language that can be
understood by the family, but that resident has very
strong skills in graphical representation of
information, that resident may be very effective in
explaining the diagnosis and treatment options
through drawings or other graphical representations
of the situation. Thus, this resident could achieve a
milestone that describes oral communication skills
leading to patient and family understanding, without
the possession of superior oral communication skills.
Caution should be applied when allowing for
compensatory scoring; that is, one should be sure
that what one is considering as compensatory is truly
part of the construct of that individual milestone and
PRACTICAL ARTICLE
Journal of Graduate Medical Education, September 2010 415

not a character trait, impression, or other subjective
element giving favor to the resident in the eyes of the
assessor (a halo effect).24
4. The working group next reviewed all developmental
milestone anchors to be sure they were written as
observable or demonstrable (even if not measurable)
statements. These anchors may or may not relate
directly to the learning objectives for an associated
curriculum. A simple Tylerian approach, where
evaluation is linked to specified curricular learning
goals and objectives, was not desired.25 Many
subcompetencies address learning that takes place
through the hidden (or implicit) curriculum or through
the explicit curriculum. However, even in the latter
case, the objectives themselves may not be explicitly
stated. Therefore, although people are accustomed to
assessing discrete objectives, we appreciate that, for
the milestones to be meaningful, it is necessary to
embrace and capture the complexity that is present in
performing and assessing these complex tasks. The
working group, therefore, acknowledged the
importance of the milestones as a roadmap to learning
for residents. Although the milestones are being
constructed for the purpose of program outcomes,
they are intended to measure the individual resident
performance and, as such, should be carefully written
to be useful as a guide to the learner. The working
group thus reflected on how the milestone document,
especially the developmental anchors, were written to
speak to learners in an understandable, meaningful,
and nonthreatening manner.
5. For some milestones, the working group looked for
critical transition points in the middle section of the
range of developmental milestone anchors, from the
beginning intern to the graduating resident. These
stopping points reflect the developmental level that
would need to be reached before the resident could
perform certain duties, such as supervise more junior
residents or care for patients without direct (in-house
or immediately available) supervision.
An example of such a stopping point is illustrated in the
Trustworthiness milestone (APPENDIX B, BOX), where a
specific level of discernment or conscientiousness26 (terms
defined in the milestone) must be met before the resident
could move to a less directly supervised setting.
Further Refinement of the Pediatrics Milestone by the
Primary Author
After thoughtful vetting by the entire working group, the
primary author would revise the milestone based on written
(e-mail) review and input from discussion (via conference
call or face-to-face meeting). The process of discussion,
editing, and revising was repeated for many milestones,
illustrating the highly iterative nature of our work.
Emerging Themes and Discoveries
1. The development of each milestone prompted the
working group to consider the curriculum design
that would prepare a pediatric resident to make
B O X Pediatrics Milestone Project Working Group
Guiding Principles
The working group of the Pediatrics Milestone Project seeks to (1)delineate the developmental progression of a pediatrician through thecontinuum of education, with a focus on the residency years; (2)establish standards for that developmental progression; and (3) identifyboth current evaluation tools and opportunities for development offuture tools that in the aggregate will help us provide a meaningful andcomprehensive approach to learning and assessment.
The outcome of the Pediatrics Milestone Project will be the first step inwhat we hope will be an iterative process of quality improvement inresidency training within the evolving context of the continuum ofmedical education. It represents a starting point rather than an endpoint, a new way of thinking about medical education using adevelopmental approach.
Below are critical assumptions and beliefs that are central to helpingus navigate the Pediatrics Milestone Project:
Creating the Milestones
1. Our ultimate goal and driving force is meeting societal needs forquality patient care and safety through better education and trainingas measured, where possible, through patient care outcomes.
2. The Pediatrics Milestone Project will focus on core skills butrecognizes the pediatrician of tomorrow will need some flexibilityin training to achieve skills in the context of their specific careerpaths.
3. We will engage the patient to inform the development of themilestones.
4. The Pediatrics Milestone Project strives to develop a work productthat recognizes the natural tension between the values ofautonomy and personal ownership associated with the privilege ofcaring for patients and the increasing focus on interdependenceand teamwork necessary for optimal care.
5. Professional formation requires the development of behaviors throughdeliberate practice, which define a ‘‘good doctor’’ as well as longitudinalassessment to ensure that these behaviors become habits.
Embedding the Milestones in the Context ofMedical Education
1. The Accreditation Council for Graduate Medical Education(ACGME) competencies are a necessary, but not sufficient,framework for our work. For example, not all competencies arecreated equal, and they are inseparable in real world practice.
2. In developing the products of the Pediatrics Milestone Project, wewill look to the continuum of undergraduate medical education,Graduate Medical Education, and Continuing ProfessionalDevelopment to inform our work.
Assessing the Milestones
1. Evaluation and assessment of residents is optimized when it ispractical, flexible, and done with, rather than to, the learner.
2. In the assessment of performance, there needs to be balancebetween deconstructing the complex tasks of a physician intodiscrete learning objectives and reconstructing these objectives tocapture how they are integrated into a complex task.
Implementing the Milestones
1. The Pediatric Milestone Project will strive to develop work productsthat can be successfully implemented by all program directors,other educators, and learners at the grassroots level.
2. We will need to incorporate ongoing assessment of the projectinto the implementation process.
3. We will engage stakeholders throughout the pediatrics and laycommunities into the implementation phase.
PRACTICAL ARTICLE
416 Journal of Graduate Medical Education, September 2010

progress in demonstrating the desired behaviors
captured in the milestones. Often, the chosen
conceptual framework for the elements of the
milestones was derived from published literature
describing the rationale for a curricular design.
2. There were consistent themes in the developmental
ontogeny of many milestones, elaborated in a recent
article by the Pediatrics Milestone Project Working
Group.27 Some are listed here:
a. The developing physician moves from a
dependent learner to a more independent
learner.
b. The developing physician becomes more
intrinsically motivated or directed as he or she
matures.
c. The development of an appreciation of the need
for teamwork and dependency on resources
outside of self allows the mature learner to
practice without direct supervision (but with
awareness of the need for assistance).
d. There is a developmental progression of comfort
with uncertainty and development of effective
strategies to manage ambiguity.
3. It is important to make explicit the implicit goal that
the development of personal and professional growth
is an essential domain for the physician entrusted
with the care of children and adolescents.28
4. The elements of one subcompetency often overlap
with the elements of another, making the
achievement of one subcompetency interdependent
on the other.
5. None of the milestones, by themselves, will speak to
the consistency or habit with which a resident
demonstrates the behaviors of that milestone.
Individual milestones capture observable behaviors
for only 1 specified time and context. Consistency,
habits, and professionalism are optimally inferred
from performance data across a number of contexts
and observations over time.
Challenges and Next Steps
Although every attempt was made to construct the
pediatrics milestones using the best evidence for assessment
of the competencies, the working group’s expertise is
limited by the education and experiences of the group and
the literature we explored. Outcome evidence or
assessment results that provide the type of reassurance that
residents, programs, the ACGME, and the public expect
will require further work on the milestones themselves and
on the approach to measurement and reporting. The
Pediatrics Milestone Working Group looks forward to the
opportunity to collaborate with a variety of experts to
improve this first iteration of the pediatric milestones. We
hope to consult content experts for the more complex
milestones, where the ontogeny of skill development was
difficult to frame. We also look forward to engaging in
discussion with a newly appointed ACGME Advisory
Group on Assessment that is dedicated to the Milestone
Project.
A guiding principle that directed our development of the
behavioral narrative anchors stated, ‘‘in the assessment of
performance, there needs to be balance between
deconstructing the complex tasks of a physician into
discrete learning objectives and reconstructing these
objectives to capture how they are integrated into a complex
task.’’ The latter presented the greatest challenge. To
accomplish this in measurement and reporting efforts, we
plan to embrace the complexity and capture the continuum
of behaviors that underlie the developmental progression
through a series of developmental milestones rather than
focus only on the 4 to 5 milestones in a series as discrete
anchors.
Another challenge that we face is reporting achievement
of milestones. Our plan is to weigh all of the elements of a
milestone that describe a given subcompetency, so that,
rather than reporting yes or no to the question of
achievement, we will be able to report proximity to a target
of the aggregated elements within a series of developmental
milestones. In a subsequent article, we will share ideas for
next steps as we work to not only improve the pediatrics
milestones but also to hopefully contribute in a meaningful
way to the milestones work for many other specialties
through the lessons learned from our own work.
References
1 [ACGME/ABMS] Accreditation Council for Graduate Medical Education/American Board of Medical Specialties. Toolbox of assessment methods.http://www.acgme.org/Outcome/assess/Toolbox.pdf. Accessed June 1, 2010.
2 [ACGME] Accreditation Council for Graduate Medical Education. TheACGME outcome project: an introduction. http://www.acgme.org/outcome. Accessed June 1, 2010.
3 Lurie SJ, Money CJ, Lyness JM. Measurement of the general competencies ofthe Accreditation Council for Graduate Medical Education: a systematicreview. Acad Med. 2009;84(3):301–309.
4 Nasca T. CEO’s Welcoming Address at the ACGME Annual EducationalConference, 2010. http://www.acgme.org/acWebsite/newsReleases/newsRel_3_23_10_1.asp. Accessed June 1, 2010.
5 Glassick CE. Boyer’s expanded definition of scholarship, the standards ofassessing scholarship and the elusiveness of the scholarship of teaching.Acad Med. 2000;75(9):877–880.
6 Bordage G. Conceptual frameworks to illuminate and magnify. Med Educ.2009;43(4):312–319.
7 Miller GE. The assessment of clinical skills/competence/performance. AcadMed. 1990;65(suppl 9):563–567.
8 Norman G, Bordage G, Page G, Keane D. How specific is case specificity?Med Educ. 2006;40(7):618–623.
9 Harris IB. Deliberative inquiry: the art of planning. In: Short EC, ed. Forms ofCurriculum Inquiry. Albany, NY: State University of New York, 1991:285–307.
10 Downing SM. Validity: on the meaningful interpretation of assessmentdata. Med Educ. 2003;37(9):830–837.
11 Dewey J, ed. How We Think? A Restatement of the Relation of ReflectiveThinking to the Educative Process. Boston, MA: DC Heath & Co; 1933.
12 Kolb DA. Experiential Learning as the Science of Learning and Development.Englewood Cliffs, NJ: Prentice Hall; 1984.
PRACTICAL ARTICLE
Journal of Graduate Medical Education, September 2010 417

13 Davis DA, Mazmanian PE, Fordis M, Van Harrison R, Thorpe KE, Perrier L.Accuracy of physician self-assessment compared with observed measuresof competence: a systematic review. JAMA. 2006;296(9):1094–1102.
14 King A. Designing the instructional process to enhance critical thinkingacross the curriculum. Teach Psychol. 1995;22(1):13–17.
15 Cizek CJ, ed. Setting Performance Standards: Concepts, Methods andPerspectives. Mahwah, NJ: Lawrence Erlbaum Associates, Inc; 2001.
16 Downing SM, Yudkowsky R. Assessment in Health Professions Education.New York, NY: Routledge; 2009.
17 American Academy of Pediatrics, Committee on Children with Disabilities.Developmental surveillance and screening of infants and young children.Pediatrics. 2001;108(1):192–196.
18 Bordage G. Prototypes and semantic qualifiers: from past to present. MedEduc. 2007;41(12):1117–1121.
19 Coderre S, Mandin H, Harasym PH, Fick GH. Diagnostic reasoning strategiesand diagnostic success. Med Educ. 2003;37(8):695–703.
20 Bowen JL. Educational strategies to promote clinical diagnostic reasoning.N Engl J Med. 2006;355(21):2217–2225.
21 Schmidt HG, Rikers RM. How expertise develops in medicine: knowledgeencapsulation and illness script formation. Med Educ. 2007;41(12):1133–1139.
22 Schmidt HG, Boshuizen HPA. On acquiring expertise in medicine. EducPsychol Rev. 1993;5(3):205–221.
23 Schmidt HG, Norman GR, Boshulzen HP. A cognitive perspective on medicalexpertise: theory and implications. Acad Med. 1990;65(10):611–621.
24 Downing SM, Yudkowsky R. Validity and Its Threats: Assessment in HealthProfessions Education. New York, NY: Routledge; 2009.
25 Stufflebeam DL, Shinkfield AJ. Evaluation Theory, Models and Applications.San Francisco, CA: John Wiley and Sons, Inc.; 2007.
26 Kennedy TJ, Rehehr G, Baker GR, Lingard L. Point-of-care assessment ofmedical trainee competence for independent clinical work. Acad Med.2008;83(suppl 10):S89–S92.
27 Englander R, Hicks P, Benson B, et al. Pediatric milestones: a developmentalapproach to the competencies. Pediatrics. 2010. In press.
28 Cooke M, Irby DM, O’Brien BC. Educating Physicians—A Call for Reform ofMedical School and Residency. San Francisco, CA: Jossey-Bass; 2010.
PRACTICAL ARTICLE
418 Journal of Graduate Medical Education, September 2010





























