Embed Size (px)
Citation preview

NUCLEAR CARDIOLOGY (V DILSIZIAN, SECTION EDITOR)
The Potential Utility of 123I-mIBG in Atrial Fibrillationand in the Electrophysiology Laboratory
Marc Ovadia & Kristin S. Duque
Published online: 16 February 2012# Springer Science+Business Media, LLC 2012
Abstract A novel indication for 123I-mIBG has recentlybeen proposed to risk stratify patients with atrial fibrillation.This review puts into perspective the utility and importanceof such a risk stratification modality, in the setting of theepidemic of atrial fibrillation, which also relates to theprevalence of heart failure, obesity, hypertension, andstroke. The authors argue that the epic cost of care forpatients with paroxysmal and more advanced forms of atrialfibrillation—including catheter ablation, heart failure, andstroke management—coupled with the poor efficacy of alltreatment modalities in advanced atrial fibrillation, makenecessary a paradigm shift where only paroxysmal atrialfibrillation that demonstrably will turn into permanentfibrillation should be targeted aggressively. If this prem-ise is accepted, then 123I-mIBG nuclear imaging for risk
stratification becomes a vital tool for the care of theindividual patient, as well as for disease control and costcontainment in the population, since 123I-mIBG scanningalone can predict (with hazard ratios of the order of 3.0–5.0) the future occurrence of permanent atrial fibrillationor heart failure.
Keywords I-123mIBG .meta-iodobenzylguanidinescintigraphy . Atrial fibrillation . Heart failure . Atrialfibrillation ablation . Pediatric atrial fibrillation ablation .
Uptake-1 . Noradrenaline transporter
Introduction
Atrial fibrillation ablation, an invasive procedure performedin the electrophysiology laboratory, is becoming the pre-ferred or definitive approach for therapy of atrial fibrillation,supplanting medical therapy, surgery, and observation withor without anticoagulation. This labor-intensive and expen-sive procedure has limitations on whom it can be performedupon successfully, and for it to be effective, it must beperformed early in the natural history of atrial fibrillation.In recognition of this, the indications for the procedure arelimited at present to performance in the earliest (paroxysmal)phase of atrial fibrillation, after failure of a limited trial ofpharmacotherapy. Further, its use in most clinics is limited topatients with no structural heart disease or with very limitedheart disease.
An essential problem is posed by this situation. For it isimpossible to predict reliably, in a patient with his or herfirst self-terminated episode of atrial fibrillation, that thisparticular patient will go on to have a recurrence. Thisstatement applies generally, but is especially true in theabsence of structural heart disease. And in the patient with
Curr Cardiol Rep (2012) 14:200–207DOI 10.1007/s11886-012-0249-y
M. OvadiaUniversity of Illinois College of Medicine Rockford,Rockford, IL, USA
M. OvadiaUniversity of Illinois College of Engineering Chicago,Chicago, IL, USA
M. Ovadia (*)Electrophysiology Section, Advocate LutheranGeneral Children’s Hospital,Advocate Lutheran General Hospital and Medical Center,1775 Dempster Street,Park Ridge, IL 60068, USAe-mail: [email protected]
K. S. DuqueDivision of Cardiology (Invasive Electrophysiology),St. Mary of Nazareth and St. Elizabeth’s Hospitals,and Resurrection Medical Center,7447 West Talcott Avenue, Suite 466,Chicago, IL 60631, USAe-mail: [email protected]

recurrent atrial fibrillation, it is similarly impossible to pre-dict reliably a progression to permanent atrial fibrillation.
The failure to identify correctly the patient who willbenefit from atrial fibrillation ablation will lead either tothe withholding of the therapy until there has been progres-sion to a stage where the procedure is far less likely to beefficacious or to the application of the procedure morewidely in a population than to those particular individualswho will derive benefit. In the first case, a failure to inter-vene early enough exposes patients to the important risks ofthe procedure with a low likelihood of benefit. In the secondcase, a large population is exposed to the procedure withbenefit for a minority, but with no benefit at all (or withdeleterious effects) for the majority who would never havehad progression of their condition.
And the procedure is expensive and has a real risk ofcomplications. Its complications include proarrhythmia withcreation of new permanent arrhythmias (eg, atypical atrialflutter or intra-atrial reentry), stroke, occult cardiac perfora-tion with pericardial effusion or tamponade with the needfor limited surgical intervention, and the serious risks ofimportant perforation with atrioesophageal fistula, extracar-diac (eg, intraabdominal) hemorrhage, and death.
Its expense is staggering, for atrial fibrillation is the mostcommon tachyarrhythmia in humans. If half the people withatrial fibrillation underwent atrial fibrillation ablation in ayear, or had a hospitalization for stroke, and the cost of theablation or hospitalization were $100,000, then $1.5 trillionwould be spent in that year on this alone. This is a largeamount of resources for the United States.
Against this backdrop, 123I-mIBG scintigraphy is emerg-ing as a risk stratification modality that can distinguishindividuals at the time of their first episode of atrial fibril-lation, who will progress to have permanent atrial fibrilla-tion or permanent atrial fibrillation and congestive heartfailure.
Background on Atrial Fibrillation Ablation
Since 2002 [1], catheter ablation for atrial fibrillation has beenavailable as an option for therapy of atrial fibrillation, and overthe years, the efficacy of this treatment has been proven in anexpanding number of populations. Controlled trials support itsutility in the adult with paroxysmal atrial fibrillation and nostructural heart disease [2, 3], and its use has been justified asprimary therapy [4] as well as in drug-refractory paroxysmalatrial fibrillation [2, 3]. The latter represents the sole US Foodand Drug Administration–approved indication for atrial fibril-lation at the time of this writing in early 2012. No study hasyet been done on the prophylactic employment of this tech-nique prior to first occurrence of sustained arrhythmia in anyhigh-risk population.
The electrophysiologic end point sought in ablation is pul-monary vein electrical isolation (entrance block to the pulmo-nary veins for impulse trains originating in the left atrium, in adrug-free state) and with the achievement of this end point,consistent superiority in outcome has been observed in allpatient populations reported.
The complications of this procedure are not minimal. Inaddition to vascular complications and hemorrhage, thereare complications peculiar to the procedure including phren-ic nerve palsy, pulmonary vein stenosis, and atrioesophagealfistula, as well as complications of cardiac or great vesselperforation with the need for urgent surgical intervention,sometimes performed on the catheterization table. Proar-rhythmia with creation of new incessant arrhythmia occursnot infrequently, and the need for repeat procedures furthercompounds the burden of this treatment option. The aggre-gate prevalence of the complications is reported to be inexcess of 6% [5]. Cappato et al. [6•] found a fatality rate of 1in 1000 patients even in very experienced hands (in a surveythat included data from 45,115 atrial fibrillation ablationprocedures). Death was caused most commonly by cardiactamponade proceeding to cardiac arrest, atrioesophagealfistula, and stroke [6•]. In De Ponti et al.’s [7] multicentersurvey of all electrophysiology procedures using transseptalcatheterization, a yet higher mortality was documented: 2 in1000 attributable to the transseptal catheterization alone, towhich may be added incremental mortality risk related to themany other parts of the procedure. Despite efforts to im-prove procedural safety [8••], there remains an irreduciblerisk of death with this elective procedure.
Thus, the specific targeting by ablation of the populationsat most risk for progression of atrial fibrillation is highlydesirable to avoid exposing patients whose course would bebenign, to these serious risks related to the procedure.
The Problem of Prediction of Atrial FibrillationProgression
The Framingham study showed that by age 40 years, individ-uals in normal sinus rhythm (up to that age) have a 1 in 4lifetime risk of atrial fibrillation [9]. This staggering statistic,coupled with the scientific support for considering atrial fi-brillation ablation as a first-line therapy for atrial fibrillation[4], shows the potential enormity of cost associated with theintroduction of atrial fibrillation ablation as a therapeuticmodality in the United States. This statement applies in theabsence of any risk stratification modality that can distinguishthe patient at enhanced risk for permanent atrial fibrillation orfor permanent atrial fibrillation and heart failure.
The crux of the problem of control of the use of the ablationmodality indiscriminately in patients many of whom will
Curr Cardiol Rep (2012) 14:200–207 201

derive no benefit, is the prediction of progression from parox-ysmal atrial fibrillation to a more advanced form of atrialfibrillation. Several studies have addressed this, of which weshall mention Al-Khatib et al.’s 4-year longitudinal study [10]and Kato et al.’s 14-year longitudinal study [11]. In thesestudies, the progression of atrial fibrillation was observed inapproximately 20% by 4 years to 70% by 14 years. However,for patients with no structural heart disease, only age was asignificant predictor, rendering the predictive utility for a par-ticular patient very low or nil. Although increased risk isassociated with congestive heart failure and valvular heartdisease, these two factors are typically absent in most of thepatients being considered for atrial fibrillation ablation. Thisgroup of patients forms the at-risk population under discussionhere.
Based on these considerations, it is evident that an easilyapplied clinical predictor of progression for the averagepatient with first-onset atrial fibrillation would be extremelyuseful.
Development of 123I-mIBG Scintigraphyand Its Introduction for Cardiac Sympathetic Imaging
123I-mIBG was first introduced for the imaging of adrenalmedullary tumors, pheochromocytoma and neuroblastoma[12]. Based on the sympathetic ganglionic blocking potencyof benzylguanidines [13], a radiolabeled series of variouslyderivatized congeners had been studied, and of these themeta-substituted species had kinetics most favorable forhuman imaging [14]. Subsequent research proved mIBG tobe a substrate for the noradrenaline transporter, the so-calleduptake 1 [15]. The ability of radiolabeled mIBG to imagecardiac sympathetic innervation was reported in 1987 [16],and broad application in cardiac imaging followed, culmi-nating in the finding that 123I-mIBG scintigraphy furnishedan independent risk factor for death in heart failure [17].
Use of 123I-mIBG Scintigraphy to Predict PermanentAtrial Fibrillation or Heart Failure
The seminal work on prediction of permanent atrial fibrilla-tion or heart failure for the individual patient with isolated newatrial fibrillation and normal left ventricular function is that ofAkutsu et al. [18••]. Additional important contributions, in-cluding those of Mabuchi et al. [19], are also noteworthy. Inthis section, we review the findings of these studies.
In the 2011 study by Akutsu et al. [18••], the authorsinvestigated the utility of 123I-mIBG scintigraphy prospec-tively in a large series of patients with new-onset atrialfibrillation and normal left ventricular function. Their goalwas to assess the utility of 123I-mIBG measures to predict
permanent atrial fibrillation, compared with other measures,in a well-conducted multivariable analysis.
The study population included 126 consecutive patientswith new onset of self-terminated (paroxysmal) atrial fibril-lation in structurally normal hearts in Showa UniversityHospital (昭和大学病院) in Tokyo, Japan. No patient hadclinical symptoms of congestive heart failure, and in factthis was an exclusion criterion. In addition, no patient hadpersistent atrial fibrillation; persistent atrial fibrillation wasan additional exclusion criterion. Other exclusion criteriaincluded left ventricular ejection fraction less than 0.5, his-tory of valvular, congenital, ischemic, rheumatic, or idio-pathic structural heart disease (the latter category includesidiopathic and genetic forms of dilated and hypertrophiccardiomyopathy), preexcitation syndrome, supraventriculartachycardia, implanted pacemaker or defibrillator, and his-tory of thromboembolism or vascular event. The averageage was 66 years, with predominance of males (73%). Fifty-three percent had a history of hypertension and 26% hadhyperlipoproteineria, with only rare obesity (5%). (Obesitywas defined as body mass index ≥31 kg/m2.) There wasappropriate pharmacotherapy for hypertension and intercur-rent conditions (eg, diabetes mellitus, which was present inapproximately 13% of patients), presumably similar to thatof background prevalence in the authors’ population.
In this group of patients, 123I-mIBG myocardial scintigra-phy was performed in sinus rhythm. Planar images wereacquired with 4-hour delay after intravenous injection of 123I-mIBG, 111 MBq, and heart/mediastinum activity ratio wascalculated from the delayed image.
Blinded to the results of scintigraphy, research personnelprospectively followed the patients up to 13 3/4 years (meanfollow-up, 4 years). The primary end point was the develop-ment of permanent atrial fibrillation and follow-up was con-ducted at least every 4 weeks. A second end point was theoccurrence of congestive heart failure requiring hospitaliza-tion, and a clinical diagnosis of congestive heart failure wasalso sought retrospectively “by dedicated research personnelusing a scripted review of the medical record” [18••]. Endpoints were confirmed separately by an independent commit-tee blinded by the patient’s medical history.
Results of this study (Fig. 1) were based on comparisonof the results of 123I-mIBG scintigraphy (as well as otherresults) in the two distinct subpopulations into which theoriginal homogeneous population segregated itself. Of theoriginal 126 patients, 35 patients made the transition topermanent atrial fibrillation and 91 did not. (It may be notedincidentally that of those 35, 14 went via an intermediatetransition stage of persistent atrial fibrillation managed withcardioversion and pharmacotherapy.)
Sixteen patients developed congestive heart failure, includ-ing 12 in the group with atrial fibrillation and 4 in the groupwithout. Not unexpectedly, the occurrence of heart failure was
202 Curr Cardiol Rep (2012) 14:200–207
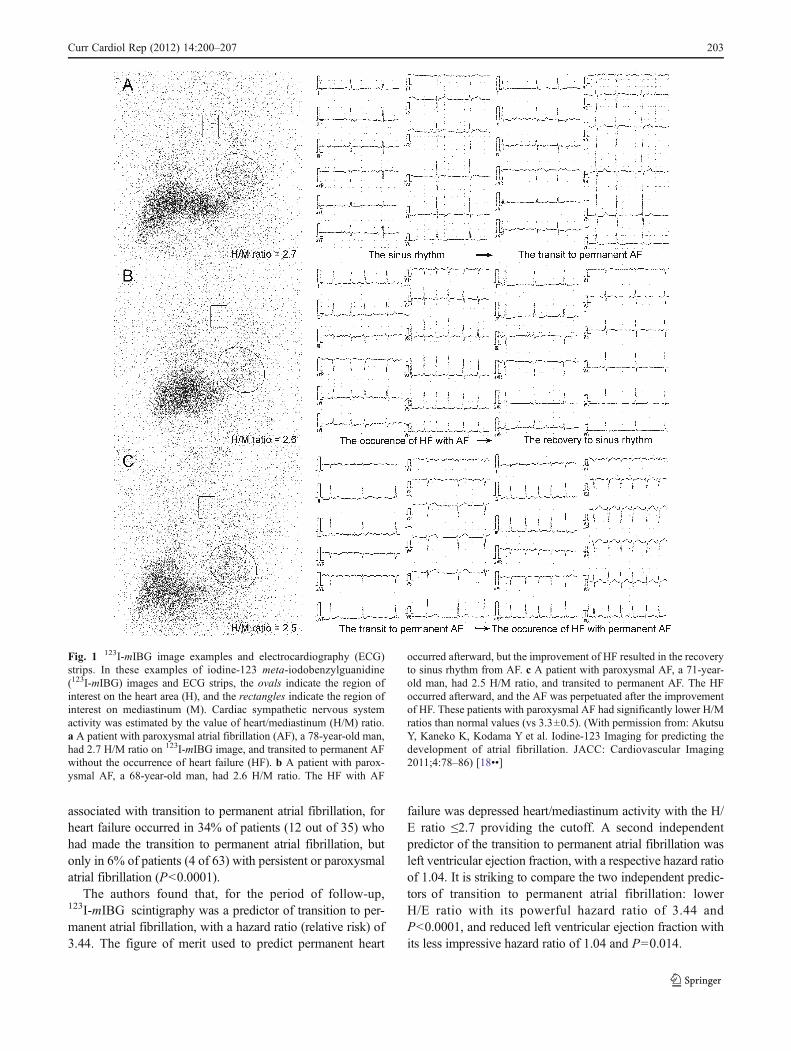
associated with transition to permanent atrial fibrillation, forheart failure occurred in 34% of patients (12 out of 35) whohad made the transition to permanent atrial fibrillation, butonly in 6% of patients (4 of 63) with persistent or paroxysmalatrial fibrillation (P<0.0001).
The authors found that, for the period of follow-up,123I-mIBG scintigraphy was a predictor of transition to per-manent atrial fibrillation, with a hazard ratio (relative risk) of3.44. The figure of merit used to predict permanent heart
failure was depressed heart/mediastinum activity with the H/E ratio ≤2.7 providing the cutoff. A second independentpredictor of the transition to permanent atrial fibrillation wasleft ventricular ejection fraction, with a respective hazard ratioof 1.04. It is striking to compare the two independent predic-tors of transition to permanent atrial fibrillation: lowerH/E ratio with its powerful hazard ratio of 3.44 andP<0.0001, and reduced left ventricular ejection fraction withits less impressive hazard ratio of 1.04 and P00.014.
Fig. 1 123I-mIBG image examples and electrocardiography (ECG)strips. In these examples of iodine-123 meta-iodobenzylguanidine(123I-mIBG) images and ECG strips, the ovals indicate the region ofinterest on the heart area (H), and the rectangles indicate the region ofinterest on mediastinum (M). Cardiac sympathetic nervous systemactivity was estimated by the value of heart/mediastinum (H/M) ratio.a A patient with paroxysmal atrial fibrillation (AF), a 78-year-old man,had 2.7 H/M ratio on 123I-mIBG image, and transited to permanent AFwithout the occurrence of heart failure (HF). b A patient with parox-ysmal AF, a 68-year-old man, had 2.6 H/M ratio. The HF with AF
occurred afterward, but the improvement of HF resulted in the recoveryto sinus rhythm from AF. c A patient with paroxysmal AF, a 71-year-old man, had 2.5 H/M ratio, and transited to permanent AF. The HFoccurred afterward, and the AF was perpetuated after the improvementof HF. These patients with paroxysmal AF had significantly lower H/Mratios than normal values (vs 3.3±0.5). (With permission from: AkutsuY, Kaneko K, Kodama Y et al. Iodine-123 Imaging for predicting thedevelopment of atrial fibrillation. JACC: Cardiovascular Imaging2011;4:78–86) [18••]
Curr Cardiol Rep (2012) 14:200–207 203
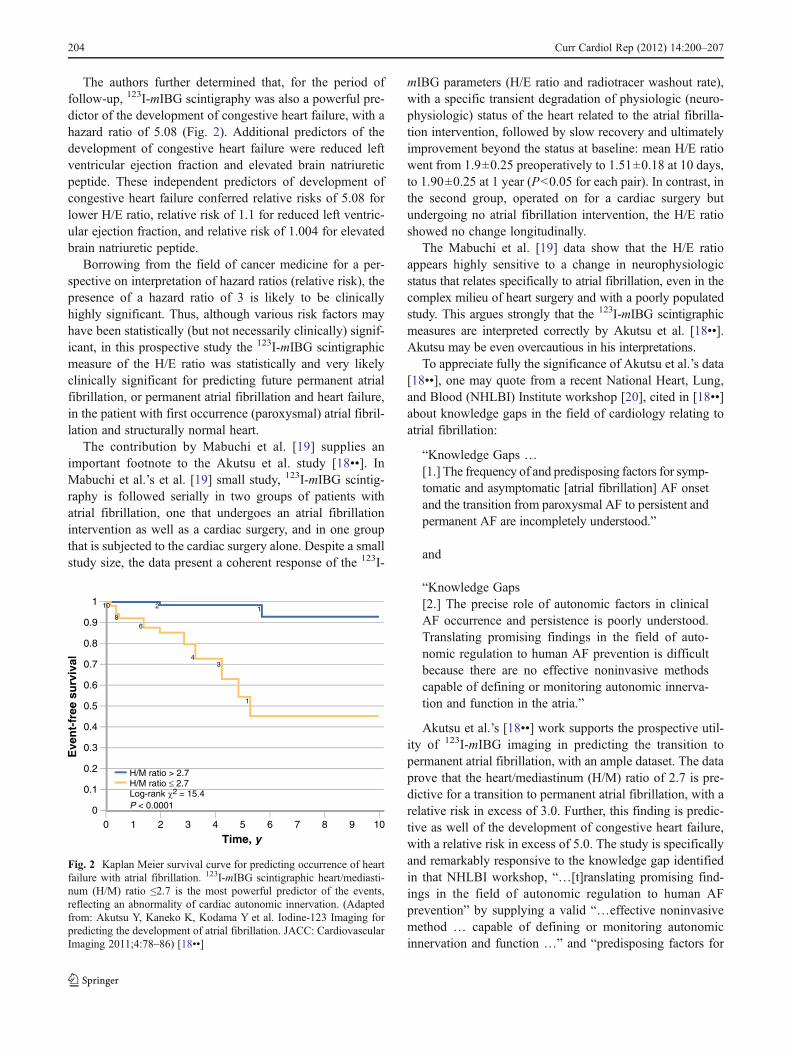
The authors further determined that, for the period offollow-up, 123I-mIBG scintigraphy was also a powerful pre-dictor of the development of congestive heart failure, with ahazard ratio of 5.08 (Fig. 2). Additional predictors of thedevelopment of congestive heart failure were reduced leftventricular ejection fraction and elevated brain natriureticpeptide. These independent predictors of development ofcongestive heart failure conferred relative risks of 5.08 forlower H/E ratio, relative risk of 1.1 for reduced left ventric-ular ejection fraction, and relative risk of 1.004 for elevatedbrain natriuretic peptide.
Borrowing from the field of cancer medicine for a per-spective on interpretation of hazard ratios (relative risk), thepresence of a hazard ratio of 3 is likely to be clinicallyhighly significant. Thus, although various risk factors mayhave been statistically (but not necessarily clinically) signif-icant, in this prospective study the 123I-mIBG scintigraphicmeasure of the H/E ratio was statistically and very likelyclinically significant for predicting future permanent atrialfibrillation, or permanent atrial fibrillation and heart failure,in the patient with first occurrence (paroxysmal) atrial fibril-lation and structurally normal heart.
The contribution by Mabuchi et al. [19] supplies animportant footnote to the Akutsu et al. study [18••]. InMabuchi et al.’s et al. [19] small study, 123I-mIBG scintig-raphy is followed serially in two groups of patients withatrial fibrillation, one that undergoes an atrial fibrillationintervention as well as a cardiac surgery, and in one groupthat is subjected to the cardiac surgery alone. Despite a smallstudy size, the data present a coherent response of the 123I-
mIBG parameters (H/E ratio and radiotracer washout rate),with a specific transient degradation of physiologic (neuro-physiologic) status of the heart related to the atrial fibrilla-tion intervention, followed by slow recovery and ultimatelyimprovement beyond the status at baseline: mean H/E ratiowent from 1.9±0.25 preoperatively to 1.51±0.18 at 10 days,to 1.90±0.25 at 1 year (P<0.05 for each pair). In contrast, inthe second group, operated on for a cardiac surgery butundergoing no atrial fibrillation intervention, the H/E ratioshowed no change longitudinally.
The Mabuchi et al. [19] data show that the H/E ratioappears highly sensitive to a change in neurophysiologicstatus that relates specifically to atrial fibrillation, even in thecomplex milieu of heart surgery and with a poorly populatedstudy. This argues strongly that the 123I-mIBG scintigraphicmeasures are interpreted correctly by Akutsu et al. [18••].Akutsu may be even overcautious in his interpretations.
To appreciate fully the significance of Akutsu et al.’s data[18••], one may quote from a recent National Heart, Lung,and Blood (NHLBI) Institute workshop [20], cited in [18••]about knowledge gaps in the field of cardiology relating toatrial fibrillation:
“Knowledge Gaps …[1.] The frequency of and predisposing factors for symp-tomatic and asymptomatic [atrial fibrillation] AF onsetand the transition from paroxysmal AF to persistent andpermanent AF are incompletely understood.”
and
“Knowledge Gaps[2.] The precise role of autonomic factors in clinicalAF occurrence and persistence is poorly understood.Translating promising findings in the field of auto-nomic regulation to human AF prevention is difficultbecause there are no effective noninvasive methodscapable of defining or monitoring autonomic innerva-tion and function in the atria.”
Akutsu et al.’s [18••] work supports the prospective util-ity of 123I-mIBG imaging in predicting the transition topermanent atrial fibrillation, with an ample dataset. The dataprove that the heart/mediastinum (H/M) ratio of 2.7 is pre-dictive for a transition to permanent atrial fibrillation, with arelative risk in excess of 3.0. Further, this finding is predic-tive as well of the development of congestive heart failure,with a relative risk in excess of 5.0. The study is specificallyand remarkably responsive to the knowledge gap identifiedin that NHLBI workshop, “…[t]ranslating promising find-ings in the field of autonomic regulation to human AFprevention” by supplying a valid “…effective noninvasivemethod … capable of defining or monitoring autonomicinnervation and function …” and “predisposing factors for
Fig. 2 Kaplan Meier survival curve for predicting occurrence of heartfailure with atrial fibrillation. 123I-mIBG scintigraphic heart/mediasti-num (H/M) ratio ≤2.7 is the most powerful predictor of the events,reflecting an abnormality of cardiac autonomic innervation. (Adaptedfrom: Akutsu Y, Kaneko K, Kodama Y et al. Iodine-123 Imaging forpredicting the development of atrial fibrillation. JACC: CardiovascularImaging 2011;4:78–86) [18••]
204 Curr Cardiol Rep (2012) 14:200–207
symptomatic and asymptomatic AF onset and the transitionfrom paroxysmal AF to persistent and permanent AF.”
Significance
In their paper, Akutsu et al. [18••] discussed the significanceof their work chiefly in relation to the physiologic elucida-tion of the relationship between the autonomic nervoussystem and specifically sympathetic innervation to atrialfibrillation at a critical point in the natural history of thedisease. However, the actual significance of their work ismore far-reaching. In the context of the epidemiology ofatrial fibrillation, which is of atrial fibrillation as a virtualepidemic, the introduction of 123I-mIBG scintigraphy allowsdetection of the population most at risk for progression topermanent atrial fibrillation and heart failure, which is pre-cisely the population that can benefit most from atrial fibrilla-tion ablation. Although at this time 123I-mIBG scintigraphyhas not been used to select patients for atrial fibrillationablation, the use of 123I-mIBG scintigraphy appears valid fordiscrimination of high-risk patients.
As noted earlier, the tailoring of therapy appropriate forthe individual patient would allow the application of atrial
fibrillation ablation to the patient at particular risk for pro-gression to permanent atrial fibrillation or atrial fibrillationand congestive heart failure. The avoidance of the compli-cations of the procedure for individuals who would derivelittle or no benefit has been detailed above. An economicargument can be articulated as well.
The expense of an ablation approach is staggering, foratrial fibrillation is the most common tachyarrhythmia inhumans. If half the people with atrial fibrillation underwentatrial fibrillation ablation in a year, or had a hospitalizationfor stroke, and the cost of the ablation or hospitalizationwere $100,000, then $1.5 trillion would be spent in that yearon this alone, a large amount of resources for the UnitedStates.
Yet if the 123I-mIBG technique (or an occupationally lesshazardous hypothetical 99mTc-based technique) were vali-dated and deployed, and allowed the targeting of only 1/10of that number of people with transcatheter ablation andtimely pharmacotherapy, then $1.3 trillion would be saved.This is the promise of any valid predictor of the transitionfrom paroxysmal or persistent atrial fibrillation, to perma-nent atrial fibrillation.
Based on these considerations, clinical management ofatrial fibrillation may be improved by introduction of
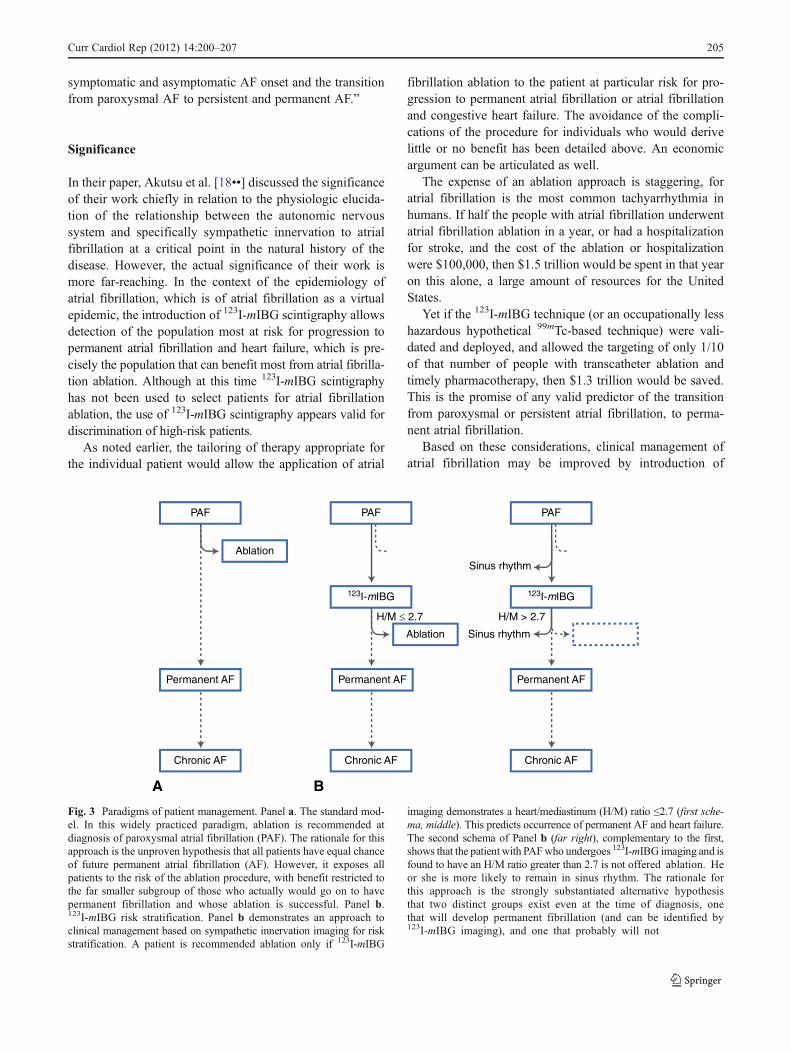
Fig. 3 Paradigms of patient management. Panel a. The standard mod-el. In this widely practiced paradigm, ablation is recommended atdiagnosis of paroxysmal atrial fibrillation (PAF). The rationale for thisapproach is the unproven hypothesis that all patients have equal chanceof future permanent atrial fibrillation (AF). However, it exposes allpatients to the risk of the ablation procedure, with benefit restricted tothe far smaller subgroup of those who actually would go on to havepermanent fibrillation and whose ablation is successful. Panel b.123I-mIBG risk stratification. Panel b demonstrates an approach toclinical management based on sympathetic innervation imaging for riskstratification. A patient is recommended ablation only if 123I-mIBG
imaging demonstrates a heart/mediastinum (H/M) ratio ≤2.7 (first sche-ma, middle). This predicts occurrence of permanent AF and heart failure.The second schema of Panel b (far right), complementary to the first,shows that the patient with PAFwho undergoes 123I-mIBG imaging and isfound to have an H/M ratio greater than 2.7 is not offered ablation. Heor she is more likely to remain in sinus rhythm. The rationale forthis approach is the strongly substantiated alternative hypothesisthat two distinct groups exist even at the time of diagnosis, onethat will develop permanent fibrillation (and can be identified by123I-mIBG imaging), and one that probably will not
Curr Cardiol Rep (2012) 14:200–207 205

123I-mIBG imaging. A schematic diagram of clinical man-agement of atrial fibrillation under the standard model, andwith the recognition of a potential role for 123I-mIBG imaging,is presented in Fig. 3.
Areas for Research
Among areas for research, the prospective testing of thehypothesis that the pathophysiologic correlate of provenatrial fibrillation identified by 123I-mIBG scintigraphy cor-rectly identifies most patients who will benefit from abla-tion, would be very valuable.
In addition, with the growth of large numbers of youngerpatients with first occurrence atrial fibrillation and specificrisk factors, the hypothesis suggests itself that possibly inthis separate group of patients (with risk factors not studiedin Akutsu et al.’s work [18••]) the same pathophysiologicmechanism could underlie progression to persistent or per-manent atrial fibrillation. Such populations include patientswith hypertrophic cardiomyopathy, patients with repairedcongenital heart defect (including atrial septal defect),patients with operated congenital heart defects or here-dofamilial diseases (eg, Marfan’s syndrome and longQT syndrome), and sufferers from obesity and sleepapnea, hypertension and insulin resistance (eg, polycysticovarian syndrome) who develop atrial fibrillation often intheir teenage years.
If validated as a predictor of permanent atrial fibrillationin these populations, the introduction of 123I-mIBG scintig-raphy could introduce a paradigm shift in atrial fibrillationtherapy in the young, leading to therapy for first occurrenceatrial fibrillation by ablation and avoiding a lifelong risk ofstroke and other debility.
Conclusions
The recent validation of the use of the widely availabletechnique of 123I-mIBG scintigraphy to risk stratify patientswith first occurrence and paroxysmal atrial fibrillation mayallow the discrimination of a population at high risk forprogression to atrial fibrillation or to atrial fibrillation andheart failure.
If this approach improves patient selection for atrialfibrillation ablation, the application of this expensive andcomplicated ablation technique could potentially be avoidedin patients who would derive little or no benefit, and theapplication of the atrial fibrillation ablation technique couldbe extended to more patient groups at high risk for perma-nent atrial fibrillation or for the complications of atrialfibrillation (eg, heart failure, death, and stroke), includingyounger patients.
Disclosure No potential conflicts of interest relevant to this articlewere reported.
References
Papers of particular interest, published recently, have beenhighlighted as:• Of importance•• Of major importance
1. Oral H, Knight BP, Tada H, et al. Pulmonary vein isolation for parox-ysmal and persistent atrial fibrillation. Circulation. 2002;105:1077–81.
2. Stabile G, Bertaglia E, Senatore G, et al. Catheter ablation treatmentin patients with drug-refractory atrial fibrillation. A Prospective,multi-centre, randomized, controlled study (Catheter ablation forthe cure of atrial fibrillation study). Eur Heart J. 2006;27:216–21.
3. Wilber DJ, Pappone C, Neuzil P, et al. Comparison of antiarrhyth-mic drug therapy and radiofrequency catheter ablation in patientswith paroxysmal atrial fibrillation. A Randomized controlled trial.JAMA. 2010;303:333–40.
4. Wazni OM, Marrouche NF, Martin DO, et al. Radiofrequency abla-tion vs antiarrhythmic drugs as first-line treatment of symptomaticatrial fibrillation. A Randomized trial. JAMA. 2005;293:2634–40.
5. Cappato R, Calkins H, Chen S-A, et al. Worldwide survey on themethods, efficacy, and safety of catheter ablation for human atrialfibrillation. Circulation. 2005;111:1100–5.
6. • Cappato R, Calkins H, Chen S-A, et al. Prevalence and causes offatal outcome in catheter ablation of atrial fibrillation. J Am CollCardiol. 2009;53:1798–803. This is a review of the most adverseoutcome in 45,000 procedures.
7. De Ponti R, Cappato R, Curnis A, et al. Trans-septal catheteriza-tion in the electrophysiology laboratory. Data from a multicentersurvey spanning 12 years. J Am Coll Cardiol. 2006;47:1037–42.
8. •• Chugh A, Oral H. Preventing serious complications during AFablation. Nat Rev Cardiol. 2009;6:562–3. A clinician-scientist withremarkable foresight reflects on the needed evolution of a proce-dure he was instrumental in introducing.
9. Lloyd-Jones DM, Wang TJ, et al. Lifetime risk for development ofatrial fibrillation: the Framingham heart study. Circulation.2004;110:1042–6.
10. Al-Khatib SM, Wilkinson WE, Sanders LL, et al. Observations onthe transition from intermittent to permanent atrial fibrillation. AmHeart J. 2000;140:142–5.
11. Kato T, Yamashita T, Sagara K, et al. Progressive nature of parox-ysmal atrial fibrillation. Observations from a 14-year follow-upstudy. Circ J. 2004;68:568–72.
12. Raffel DM, Wieland DM. Development of mIBG as a cardiacinnervation imaging agent. JACC Cardiovasc Imag. 2010;3:111–6.
13. Short JH, Darby TJ. Sympathetic nervous system blocking agents.III. Derivatives of benzylguanidine. J Med Chem. 1967;10:833–40.
14. Wieland DM, Mangner TJ, Inbasekaran MN, et al. Adrenal me-dulla imaging agents: a structure-distribution relationship study ofradiolabeled aralkylguanidines. J Med Chem. 1984;27:149–55.
15. Sisson JC, Wieland DM, Sherman P, et al. Metaiodobenzylguani-dine as an index of the adrenergic nervous system integrity andfunction. J Nucl Med. 1987;28:1620–4.
16. Sisson JC, Shapiro B, Meyers L, et al. Metaiodobenzylguanidineto map scintigraphically the adrenergic nervous system in man. JNucl Med. 1987;28:1625–36.
17. Jacobson AF, Senior F, Cerqueira MD, et al. Myocardial iodine-123 Metaiodobenzylguanidine imaging and cardiac events in heart
206 Curr Cardiol Rep (2012) 14:200–207

failure: results of the prospective ADMIRE-HF (AdreView Myo-cardial Imaging for Risk Evaluation in Heart Failure) study. J AmColl Cardiol. 2010;55:2212–21.
18. •• Akutsu Y, Kaneko K, Kodama Y, et al. Iodine-123 Imaging forpredicting the development of atrial fibrillation. JACC CardiovascImag. 2011;4:78–86. This paper is the seminal work in the field.
19. Mabuchi M, Imamura M, Kubo N, et al. Sympathetic denervationand reinnervation after the MAZE procedure. J Nucl Med.2005;46:1089–94.
20. Benjamin EJ, Chen P-S, Bild DE, et al. Prevention of atrialfibrillation: Report from a National Heart, Lung and Blood Insti-tute workshop. Circulation. 2009;119:606–18.
Curr Cardiol Rep (2012) 14:200–207 207