Embed Size (px)
Citation preview

Injury Prevention 1997; 3: 282-287
METHODOLOGIC ISSUES
The PRECEDE-PROCEED model: application toplanning a child pedestrian injury preventionprogram
Peter Howat, Steve Jones, Marg Hall, Donna Cross, Mark Stevenson
AbstractObjectives-The objectives were first, tomodify the PRECEDE-PROCEED modeland to use it is as a basis for planning athree year intervention trial that aims toreduce injury to child pedestrians. Asecond objective was to assess the suit-ability of this process for plannng such arelatively complex program.
Setting-The project was carried out in 47primary schools in three local governmentareas, in the Perth metropolitan area.
Methods-The program was developed,based on extensive needs assessment in-corporating formative evaluations. Epide-miological, psychosocial, environmental,educational, and demographic informa-tion was gathered, organised, and priori-tised. The PRECEDE-PROCEED modelwas used to identify the relevant beha-vioural and environmental risk factorsassociated with child pedestrian injuriesin the target areas. Modifiable causes ofthose behavioural and environmental fac-tors were delineated. A description ofhowthe model facilitated the development ofprogram objectives and subobjectiveswhich were linked to strategy objectives,and strategies is provided.Results-The process used to plan thechild pedestrian injury prevention pro-gram ensured that a critical assessmentwas undertaken of all the relevant epide-miological, behavioural, and environmen-tal information. The gathering, organ-ising, and prioritising of the informationwas facilitated by the process.
Conclusions-The use of a model such asPRECEDE-PROCEED can enhance thedevelopment of a child injury preventionprogram. In particular, the process canfacilitate the identification of appropriateobjectives which in turn facilitates thedevelopment of suitable interventionsand evaluation methods.(Injury Prevention 1997; 3: 282- 287)
Keywords: child pedestrian injury; health promotionplanning; models
Injury prevention is recognised as a majorpublic health priority in Australia and othercountries.' 2 Pedestrian injury is a leading cause
of injury death for Western Australian childrenwith 3.2/100 000 fatalities per year.'-4 Forthose who survive being hit by a vehicle, theinjuries are usually severe. About 80% ofcritically injured child pedestrians have severehead injuries.5 Children aged 5-9 years whosuffer a pedestrian injury spend an average of30 days in hospital and the direct costs aresubstantial.6 7
Pedestrian safety is a complex problem thatrequires multiple interventions at national,state, and local levels. A multifaceted locallevel approach can involve a combination of:pedestrian skills training, parent education,teacher education, legislation, environmentalmodifications, and vehicle design changes.This combined approach is more likely to yieldeffective outcomes than any single strategy.8I "
Program planning is an aspect of injurycontrol that has attracted recent debate. Itseems that inadequate planning has been oneof the major reasons for ineffective injurycontrol and other health promotion interven-tions in the past.12 Increasing attention hasbeen given, therefore, to the use of recognisedplanning models to enhance the quality ofinjury control interventions. A significantproportion of programs, however, are devel-oped with relatively little consideration givento planning frameworks or theoreticalmodels.8 13 14
One of the benefits of using planning modelsand relevant theories is the likelihood ofimproved rigour in identifying factors on whichinterventions can be based and to establishmore appropriate objectives. This, in turn,influences better quality evaluation designs forprograms. Planning models can also provide aholistic picture of a health promotion programand thereby ensure that key components areappropriately and adequately addressed andevaluated. 14-16The purpose of this paper is to demonstrate
how the PRECEDE-PROCEED model17 wasadapted and applied as a framework forplanning the Child Pedestrian Injury Preven-tion Project (CPIPP).CPIPP has been planned as a three year
intervention trial to assess the effect of acomprehensive program aimed at reducingpedestrian injuries in schoolchildren aged 5-9 years. The program includes variable appli-cations of school based student, parent, tea-cher, and community education, as well asenvironmental interventions. The interven-tions are based on relevant components of
Centre for HealthPromotion Research,School of PublicHealth, CurtinUniversity ofTechnology,Perth 6001,GPO Box U 1987,AustraliaP HowatM HallS JonesD CrossM Stevenson
Correspondence to:Dr Howat.
282
The PRECEDE-PROCEED model
behavioural learning theories and involveaspects of community development to ensurethe active involvement of the schools and theircommunities."3 14 16-18Two communities in the Perth metropolitan
area are receiving CPIPP interventions. Onecommunity is receiving the school basedprogram only and the other, the school basedprogram plus community and environmentalinterventions. A third community is being usedas a comparison group. In total, 47 schools,2440 children, 103 teachers, and 2440 parentsare involved in the project. Extensive process,impact, and outcome evaluation proceduresare being utilised.
A framework for planning an injuryprevention programWith increasing experience in developinginjury prevention programs there has also beenan improvement in the sophistication of theplanning process. As program planners im-prove their planning skills more of the betterplanned programs are likely to be based onsound theory. Haddon's injury countermea-sures, for example, have been widely used andthere has been some recent application of thePRECEDE-PROCEED model.8The PRECEDE model, and its more recent
updated version known as PRECEDE-PRO-CEED, have been referred to in over 500publications, and used as the basis of planningnumerous other health and injury preventionprograms.'7 II A value of the model is that itforces the planner to assess thoroughly thefactors associated with the problem that is thefocus of concern. A series of diagnosesprecedes the development of the interventions,their implementation, and evaluation.
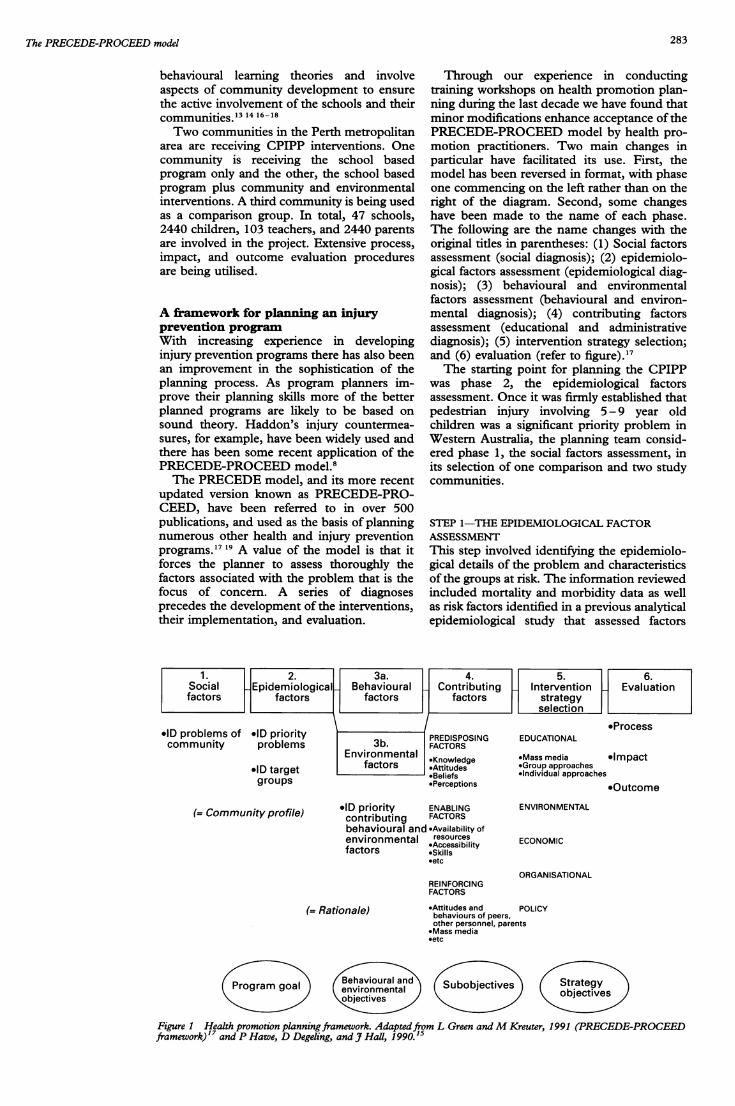
Through our experience in conductingtraining workshops on health promotion plan-ning during the last decade we have found thatminor modifications enhance acceptance of thePRECEDE-PROCEED model by health pro-motion practitioners. Two main changes inparticular have facilitated its use. First, themodel has been reversed in format, with phaseone commencing on the left rather than on theright of the diagram. Second, some changeshave been made to the name of each phase.The following are the name changes with theoriginal titles in parentheses: (1) Social factorsassessment (social diagnosis); (2) epidemiolo-gical factors assessment (epidemiological diag-nosis); (3) behavioural and environmentalfactors assessment (behavioural and environ-mental diagnosis); (4) contributing factorsassessment (educational and administrativediagnosis); (5) intervention strategy selection;and (6) evaluation (refer to figure)."7The starting point for planning the CPIPP
was phase 2, the epidemiological factorsassessment. Once it was firmly established thatpedestrian injury involving 5-9 year oldchildren was a significant priority problem inWestern Australia, the planning team consid-ered phase 1, the social factors assessment, inits selection of one comparison and two studycommunities.
STEP 1-THE EPIDEMIOLOGICAL FACTORASSESSMENTThis step involved identifying the epidemiolo-gical details of the problem and characteristicsof the groups at risk. The information reviewedincluded mortality and morbidity data as wellas risk factors identified in a previous analyticalepidemiological study that assessed factors
(=Community profile) IlD priority ENABLING ENVIRONMENTAL(=Comuniy proile) contributing FACTORSbehavioural and -Availability ofenvironmental resources ECONOMICfactors *Skills
*etc
OFREINFORCINGFACTORS
Beavioura an
environmentalobjectives
*Attitudes and PObehaviours of peers,other personnel, parents*Mass media*etc
u bjecives
RGANISATIONAL
)LICY
Strateg
objectives
Figure 1 Health promotion planningframework. Adaptedfrom L Green andM Kreuter, 1991 (PRECEDE-PROCEEDframework)'7 and P Hawe, D Degeling, and _' Hall, 1990.15
(= Rationale)
rogram goal
283

Howat, _Jones, Hall, Cross, Stevenson
contributing to childhood pedestrian injury inWestern Australia.20 This was supported bydata from health department records and otherrelevant literature.2 Some of the key informa-tion identifying child morbidity and mortalitydue to traffic related trauma as a priorityproblem included:
* Pedestrian injury was the main cause ofinjury death for Western Australian children
* The rate of child pedestrian injury deathsper year in Western Australia was 3.2/100 000, which was higher than the meanAustralian rates
* The injuries sustained by child pedestrianshit by a vehicle are usually severe
* 80% of critically injured child pedestrianshave severe head injuries
* The average hospitalisation of 5 - 9 year oldpedestrian injury victims is 30 days
* The direct cost per child pedestrian injuryvictim is estimated at A$ 100 0006 7
It was also found that parents and teachersof young children perceived pedestrian injuryto be a significant health problem.
This information was used to help define thetarget groups for the CPIPP. These two groupswere: primary target groups-5 -9 year oldchildren, their teachers, and parents andsecondary target groups-school administra-tors, city officials, legislators, police, roadsafety advisory committee, and other residents.Based on this information a program goal wasestablished: a reduction in 5-9 year old childpedestrian injuries in community A withinthree years. While it is usually preferable toset a specific rate of change, it was not possiblein this case. Injury reporting systems are stillinsufficiently developed in Western Australiato allow meaningful comparison of injurymortality and morbidity data between the threesurburban communities selected for theCPIPP.
STEP 2-THE BEHAVIOURAL ANDENVIRONMENTAL ASSESSMENTIn this phase of the planning process, factorscausally associated with child pedestrian in-juries were identified. First, behavioural andsecond, environmental factors were consideredas risk factors, and behavioural and environ-mental objectives were developed for each riskfactor. It is standard practice to state theamount of change expected for each of therisk factors. However, this is usually notpossible until substantial baseline data havebeen collected on the target groups and therelevant environments in which they performthe at-risk behaviours. The planning of allprograms should entail the compilation ofsome data. However, many programs are notwell enough funded to conduct adequate datacollection to allow all the objectives to be statedwith precise, expected rates of change. Thislimitation was experienced to some extent forthe CPIPP even though extensive data werecollected at baseline. The amount of changeexpected by the intervention was incorporated
into the objectives discussed below, whereverthe baseline data were sufficient for an estima-tion to be made.As well as the baseline data, reference was
made to the relevant literature and officialhealth statistics to identify factors causallyrelated to child pedestrian injuries. The relativeimportance and changeability of each factorwas assessed based on procedures recom-mended by Green and Kreuter.'7
For the behavioural assessment, the main riskfactors and behavioural objectives were identi-fied for the two primary target groups, childpedestrians aged 5 - 9 years, and their parentsor guardians. Two main risk factors wereidentified: inappropriate road crossing beha-viours, and children not seeking help to crossthe roads. Five behavioural objectives wereformulated to guide interventions aimed atreducing the effect of the risk factors.Three risk factors were seen to be most
relevant as parental influences on the roadcrossing behaviours of the children. Theseincluded: parents failing to supervise thechildren at road crossing; parents not teachingtheir children appropriate road crossing proce-dures; and parents not modelling appropriateroad crossing behaviours. One behaviouralobjective was developed for each of these riskfactors.
For the environmental assessment, a total offive main risk factors and eight environmentalobjectives were identified for the three generalgroups of relevant environmental factors:traffic volume and speed, road design, androadside obstacles.
STEP 3-CONTRIBUTING FACTORS ASSESSMENTMultiple factors contribute to each of thebehavioural and environmental risk factorsidentified in the preceding step. These con-tributing factors are classified into predispos-ing, enabling, and reinforcing factors. Thepredisposing factors are antecedents to beha-viour that provide motivation for actions. Theyinclude knowledge, attitudes, beliefs, andperceived needs and abilities, including selfefficacy. Enabling factors are regarded asconditions of the environment that facilitatethe performance of action by individuals ororganisations. They make it possible formotivation to be realised; that is they enablepeople to act on their predispositions. Includedare availability, accessibility and affordability ofresources, supportive policies, as well as newskills that are needed for behavioural orenvironmental changes. The reinforcing fac-tors provide rewards or incentives for thecontinuation of behaviours. Social support,peer influences, and influences from othersignificant people such as health professionals,parents and teachers, are all reinforcing factors.They also include social benefits, physicalbenefits, tangible or imagined rewards, andmass media promotions. The various predis-posing, enabling, and reinforcing factors maybe either barriers or facilitators to action.'4 17The PRECEDE-PROCEED model recom-
mends identifying these factors for each
284

The PRECEDE-PROCEED model
behavioural and environmental risk factor.This is a relatively straightforward processwhen only a few risk factors are identified aspriorities for action. However, today mosthealth problems are multicausal and thereforerequire multiple interventions.A total of 10 behavioural and environmental
risk factors were identified to explain themajority of pedestrian injuries. The maincontributing factors for the two primary targetgroups and for each of the three main groups ofenvironmental factors, are listed below. Sub-objectives were identified for each contributingfactor. 15
In total, 20 predisposing, enabling, andreinforcing factors were found to effect thebehavioural and environmental risk factors andsome contributing factors are common to morethan one risk factor. Predisposing factorsrelated directly to child pedestrians included:lack of knowledge about safe road crossingbehaviour, and perception of low risk of injurywhile crossing busy roads. The enabling factorsfor this group included: inability to identifysafer road crossing sites; poorly developed roadcrossing skills; lack of social skills required toask people to help them cross roads; andinadequate school road safety education. Tworeinforcing factors were: parents allowingchildren to cross roads alone, and* parents'perceptions that their children have adequateabilities to cross roads safely, unaccompanied.
STEP 4-INTERVENTION STRATEGY SELECTIONBy this stage of the planning sequence, themain factors that seem to be associated withthe injury problem, in this case the injuries tochild pedestrians, have been identified. Therelevant factors have become more specificwith each step in the sequence, that is the two
The CPIPP interventions
Strategies Channel of communication Purpose
School basedStudents Nine pedestrian safety classroom To provide students with safety
lessons per year for three years. related:Booster sessions during the year Knowledge
Affective educationSocial skills development
Decision makingAssertive communication
Opportunities to practice road-crossing behaviour
Parents Nine home activities per year To actively involve parents in thepedestrian safety education of theirchildren and reinforce messageslearnt at school
Teachers Pedestrian safety teaching resource. To familiarise teachers with theHalf day teacher training. Follow pedestrian safety education re-up support source 'Crossing Roads' and
provide support for itsimplementation
Community basedMedia Community newspapers and other To raise community awareness of
local media pedestrian safety
Community Monthly meetings of relevant To increase communityadvisory group community opinion leaders Awareness of pedestrian safety!
To identify and recommendenvironmental and policy changesconcerning pedestrian safety
Safe routes to Monthly meetings of community To identify safer routes for childrenschool project advisory committee. Newsletters to travel to school
to parents of all primaryschoolchildren
behavioural and the five environmental factorswere quite broad. They were then furtherrefined as specific predisposing, enabling, andreinforcing factors. Similarly, a broad programgoal was identified in the epidemiologicalfactors assessment, followed by more specificbehavioural and environmental objectives,which were examined further by subobjectives.During step 4, strategy objectives were devel-oped to address each of the subobjectives.
Thirteen main strategy objectives weredeveloped to enable the subobjectives to bemet. Some of the strategy objectives relate tomore than one of the subobjectives. 'Create aquality school based pedestrian safety educa-tion program' is an example of this.The intervention strategies were then se-
lected to address these strategy objectives.Successful attainment of these strategy objec-tives should lead to a change in the subobjec-tives (phase 4), behavioural and environmentalobjectives (phase 3), and ultimately in a changein the program goal (phase 2). The CPIPPaims to test whether there were significantchanges in all of the objectives due to the threeyear intervention program.To maximise the likely impact of the
intervention strategies, it was recognised thata combination of educational and environ-mental approaches were needed. The educa-tional strategies referred to here can beclassified into two main types. First, there arethose activities that aim to directly influenceroad crossing behaviour. This education isbeing delivered by mass media, group ap-proaches, and individual approaches. Themain target groups here are children, theirparents or guardians, as well as their teachers.In-service training of teachers to effectivelyconduct road safety education for the studentsin schools is an example of this education.The second type of education involves
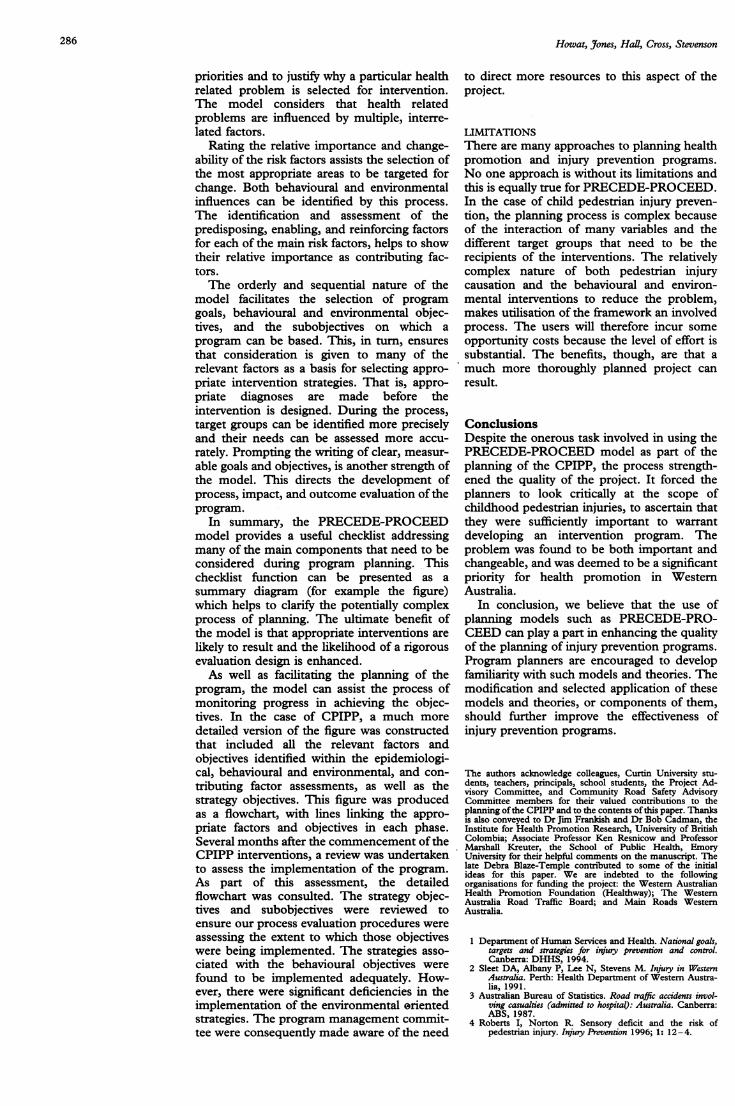
support for the children's road crossing beha-viours by influencing environmental changesthat help make the roads safer. Individualcommunication with appropriate opinion lea-ders in the study community, including citycouncillors and staff, and members of the RoadSafety Advisory Committee, are examples. Italso includes the provision of mass mediainformation directed to residents to increasetheir awareness about the need for environ-mental changes, such as lowering speed limitsand the installation of roundabouts, and toincrease their support for such changes.The table summarises the intervention stra-
tegies that were developed based on thestrategy objectives. Specific details of thesestrategies are presented elsewhere (D Cross etal; paper presented at the Third InternationalConference on Injury Prevention and Control,Melbourne, 18-22 February 1996).
DiscussionThe use of PROCEED-PRECEDE as a basisfor planning injury prevention interventionscan facilitate the process in several ways. Use ofthe model forces the planner to assess bothqualitative and quantitative data to identify
285
Howat, Jones, Hall, Cross, Stevenson
priorities and to justify why a particular healthrelated problem is selected for intervention.The model considers that health relatedproblems are influenced by multiple, interre-lated factors.
Rating the relative importance and change-ability of the risk factors assists the selection ofthe most appropriate areas to be targeted forchange. Both behavioural and environmentalinfluences can be identified by this process.The identification and assessment of thepredisposing, enabling, and reinforcing factorsfor each of the main risk factors, helps to showtheir relative importance as contributing fac-tors.The orderly and sequential nature of the
model facilitates the selection of programgoals, behavioural and environmental objec-tives, and the subobjectives on which aprogram can be based. This, in turn, ensuresthat consideration is given to many of therelevant factors as a basis for selecting appro-priate intervention strategies. That is, appro-priate diagnoses are made before theintervention is designed. During the process,target groups can be identified more preciselyand their needs can be assessed more accu-rately. Prompting the writing of clear, measur-able goals and objectives, is another strength ofthe model. This directs the development ofprocess, impact, and outcome evaluation oftheprogram.
In summary, the PRECEDE-PROCEEDmodel provides a useful checklist addressingmany of the main components that need to beconsidered during program planning. Thischecklist function can be presented as asummary diagram (for example the figure)which helps to clarify the potentially complexprocess of planning. The ultimate benefit ofthe model is that appropriate interventions arelikely to result and the likelihood of a rigorousevaluation design is enhanced.As well as facilitating the planning of the
program, the model can assist the process ofmonitoring progress in achieving the objec-tives. In the case of CPIPP, a much moredetailed version of the figure was constructedthat included all the relevant factors andobjectives identified within the epidemiologi-cal, behavioural and environmental, and con-tributing factor assessments, as well as thestrategy objectives. This figure was producedas a flowchart, with lines linking the appro-priate factors and objectives in each phase.Several months after the commencement of theCPIPP interventions, a review was undertakento assess the implementation of the program.As part of this assessment, the detailedflowchart was consulted. The strategy objec-tives and subobjectives were reviewed toensure our process evaluation procedures wereassessing the extent to which those objectiveswere being implemented. The strategies asso-ciated with the behavioural objectives werefound to be implemented adequately. How-ever, there were significant deficiencies in theimplementation of the environmental erientedstrategies. The program management commit-tee were consequently made aware of the need
to direct more resources to this aspect of theproject.
LIMITATIONSThere are many approaches to planning healthpromotion and injury prevention programs.No one approach is without its limitations andthis is equally true for PRECEDE-PROCEED.In the case of child pedestrian injury preven-tion, the planning process is complex becauseof the interaction of many variables and thedifferent target groups that need to be therecipients of the interventions. The relativelycomplex nature of both pedestrian injurycausation and the behavioural and environ-mental interventions to reduce the problem,makes utilisation of the framework an involvedprocess. The users will therefore incur someopportunity costs because the level of effort issubstantial. The benefits, though, are that amuch more thoroughly planned project canresult.
ConclusionsDespite the onerous task involved in using thePRECEDE-PROCEED model as part of theplanning of the CPIPP, the process strength-ened the quality of the project. It forced theplanners to look critically at the scope ofchildhood pedestrian injuries, to ascertain thatthey were sufficiently important to warrantdeveloping an intervention program. Theproblem was found to be both important andchangeable, and was deemed to be a significantpriority for health promotion in WesternAustralia.
In conclusion, we believe that the use ofplanning models such as PRECEDE-PRO-CEED can play a part in enhancing the qualityof the planning of injury prevention programs.Program planners are encouraged to developfamiliarity with such models and theories. Themodification and selected application of thesemodels and theories, or components of them,should further improve the effectiveness ofinjury prevention programs.
The authors acknowledge colleagues, Curtin University stu-dents, teachers, principals, school students, the Project Ad-visory Committee, and Community Road Safety AdvisoryCommittee members for their valued contributions to theplanning ofthe CPIPP and to the contents ofthis paper. Thanksis also conveyed to Dr Jim Frankish and Dr Bob Cadman, theInstitute for Health Promotion Research, University of BritishColombia; Associate Professor Ken Resnicow and ProfessorMarshall Kreuter, the School of Public Health, EmoryUniversity for their helpful comments on the manuscript. Thelate Debra Blaze-Temple contributed to some of the initialideas for this paper. We are indebted to the followingorganisations for funding the project: the Western AustralianHealth Promotion Foundation (Healthway); The WesternAustralia Road Traffic Board; and Main Roads WesternAustralia.
1 Department of Human Services and Health. National goals,targets and strategies for injury prevention and control.Canberra: DHHS, 1994.
2 Sleet DA, Albany P, Lee N, Stevens M. Injury in WesternAustralia. Perth: Health Department of Western Austra-lia, 1991.
3 Australian Bureau of Statistics. Road traffic accidents invol-ving casualties (admitted to hospital): Australia. Canberra:ABS, 1987.
4 Roberts I, Norton R. Sensory deficit and the risk ofpedestrian injury. Injury Prevention 1996; 1: 12-4.
286

The PRECEDE-PROCEED model
5 Harris BH, Schwaitzberg SD, Seman TM, Herrman C. Thehidden morbidity of pediatric trauma. Jf Pediatr Surg1989; 24: 103-6.
6 Andreassen DC. Preliminary costs for accident types: accidentcosts for project planning and evaluation. Melbourne:Australian Road Research Board, 1992. (Report NoARR 217.)
7 Andreassen DC. Vehicle repair costs: accident costs for projectplanning and evaluation. Melbourne: Australian RoadResearch Board, 1992. (Report No ARR 218.)
8 Gielen A. Health education and injury control: integratingapproaches. Health Educ Q 1992; 19: 203-18.
9 Roberts I, Norton R, Dunn R, Hassall I, Lee-Joe T.Environmental factors and child pedestrian injuries. AustJfPublic Health 1994; 18: 43 - 6.
10 Roberts I, Ashton T, Dunn R, Lee-Joe T. Preventing childpedestrian injury: pedestrian education or traffic calming.Aust
_JPublic Health 1994; 18: 209 - 12.
11 Howat P, Binns C, Blaze-Temple D, Corti B. Prevention ofalcohol related problems: an overview of health promo-tion measures. Drug Education Journal of Australia 1987;1: 87-99.
12 Kok G. Why are so many health promotion programsineffective? Health Promotion Journal ofAustralia 1993; 3:12-7.
13 Simons-Morton B, Brink S, Simons-Morton D, et al. Anecological approach to the prevention of injuries due todrinking and driving. Health Educ Q 1989; 16: 397-411.
14 Glanz K, Rimer B. Theory at a glance: a guide for healthpromotion practice. Washington DC: USDHHS, 1995.
15 Hawe P, Degeling D, Hall J. Evaluating health promotion: aguide for health workers. Sydney: MacLennan and Petty,1990.
16 Bjaras G. The potential of community diagnosis as a tool inplanning an intervention program aimed at preventinginjuries. Accid Anal Prev 1993; 25: 3-10.
17 Green L, Kreuter M. Health promotion planning: aneducational and environmental approach. Mountain View:Mayfield, 1991.
18 Tones K. Mobilising communities: coalitions and theprevention of heart disease. Health Educ J 1994; 53:462-73.
19 Institute of Health Promotion Research, University ofBritish Columbia. Second Annual Summer Institute onHealth Promotion Planning and Evaluation, June 12- 16.Vancouver, IBHR, 1995 (course manual).
20 Stevenson M, Jamrozik K, Spittle J. A case control study oftraffic risk factors and child pedestrian injuries. Int JfEpidemiol 1995; 24: 1-8.
Editorial Board Member: brief biography
JOCELYN PEDDER
Jocelyn Pedder is the Pre-sident of RONA Kineticsand Associates Ltd, an in-dependent safety researchgroup in Vancouver, Cana-da. Born in New Zealand,her interest in injury preven-tion research was initiated asa researcher at the School ofMedicine at the University of
.wrw "4 .&0t Auckland when she con-ducted a study of singlevehicle crashes. In 1975 shemoved to England to work atthe Accident Research Unit
of the University of Birmingham. For the next eight yearsshe was involved in the study of real crashes and resultinginjuries. Some of this work formed the basis of herdoctorate dissertation on the characteristics of motorcyclecrashes and the potential for injury prevention.
In 1983 Dr Pedder moved to Canada to join Biokineticsand Associates Ltd, a bioengineering consulting firm inOttawa. Her work at Biokinetics included the design anddevelopment of personal protective equipment and safetyspecifications. She moved to Vancouver in 1992 toestablish RONA Kinetics where her work in the field ofsafety research continues. Dr Pedder has many publishedresearch papers in the field of road trauma and safety,notably on kinematics and injury control in motor vehiclecrashes as well as impacts involving pedestrians andbicyclists.Dr Pedder is actively involved in efforts to advance the
state of knowledge on the biomechanics of injury andinjury prevention through studies of real crashes. Sheparticipates in a number of related national and interna-tional technical committees and is a member of the Societyof Automotive Engineers. She is currently on the board ofdirectors of the Association for the Advancement ofAutomotive Medicine. Dr Pedder is also involved in localefforts to reduce road trauma and the incidence of motorvehicle crashes through the implementation of existingresearch findings and appropriate legislation.
287