Embed Size (px)
Citation preview

288
THE PROBLEM OF TUBERCULOSISIN CHILDHOOD
By A. MARGARET MACPHERSON, M.D., F.R.C.P.Physician, Elizabeth Garrett Anderson Hospital, London; Assistant Physician, Children's Contact Dept.,
Brompton Hospital
Tuberculosis in children has to be consideredfrom more points of view than has tuberculosis inadult life. Since congenital tuberculosis is of rareoccurrence, virtually all children begin life freefrom tuberculous infection but during childhoodan appreciable number become infected. Theproblem of infection by the tubercle bacillus inchildhood may present itself from the epidemio-logical standpoint, from the aspect of case findingamong the child's associates, and gradually mergesinto problems connected with tuberculousmorbidity resulting from the primary infection.How many children are likely to be infected at
various ages, how seriously must this infection betaken; how should primary lesions be dealt withand how often may serious consequences beexpected to arise ?These are some of the questions which are
frequently asked.
InfectionAlthough there is evidence to show that fewer
children now become infected compared with20 years ago, primary tuberculosis in childhoodis still a problem of some magnitude. The mostrecent general survey of the incidence of tuber-culous infection, as shown by tuberculin testing,indicates that between 40 to 57 per cent. of childrenat I5 years of age in England and Wales have had aprimary infection.'
In the population as a whole the rate of infectionvaries in different age groups. Younger childrenwhose horizon is limited are less likely to beinfected than older children. Immediately afterleaving school, the rate of infection, in urbandistricts, rises more sharply. The figures quotedabove represent the condition present in 1949 andI950. Improvements in the early diagnosis ofactive cases and in treatment of sputum-positivecases, together with the wider use of B.C.G.inoculation may result in considerable alterationof these rates in the not too distant future.
Since roughly half of the population of children
in England and Wales have primary tuberculouslesions it is obvious that the majority of theselesions give rise to no clinical symptoms. Theproblem then presents itself, how many of theseprimary lesions are likely to cause trouble andwhich are the ones that are likely to do so?
Incidence of Clinical Manifestations inInfected Children
It is clear that the age at which primary tuber-culous infection takes place is of great importance.Infection under 3 years of age must be regardedseriously; primary lesions at this age may bequickly followed by serious and not infrequentlyfatal complications. Between the ages of 5-10years, primary infection is less likely to give riseto clinical symptoms and signs. Tuberculosis,even in this age group is significant and althoughdeath rates at this age are at a lower level for alldiseases, tuberculosis is still high in proportion toother diseases. The findings of Hyge amongschoolchildren in contact with a teacher withpositive sputum show that tuberculous infectionat this age cannot be treated lightly. He foundthat of the 70 children infected, 4I had pulmonarytuberculosis and of these 37 had tubercle bacillirecovered from gastric lavage.2
In later childhood and adolescence, it appearsthat primary infection may not infrequently beresponsible for pulmonary lesions of the infiltrativetype usually associated with young adult life.These lesions, though less dramatic in the im-mediate post-primary stage, lead eventually tochronic tuberculous lesions with long periods ofinvalidism and insecurity.
Other factors also no doubt have their place inthe aetiology of tuberculous morbidity such asextent of exposure to infection, environment,heredity and nutrition.The incidence of morbidity due to tuberculous
infection in children is difficult to measure. Therelation between the mortality and morbidityfigures is altering and mortality figures are a less
by copyright. on S
eptember 16, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.344.288 on 1 June 1954. Dow
nloaded from

June 1954 MACPHERSON: Problbm of Tuberculosis in Childhood 289
useful guide than they used to be to the significanceof tuberculous disease hii childhood. This isspecially so in the case of tuberculous meningitis.Before the use of streptomycin all established casesof meningitis had a fatal outcome, the rate ofincidence and the mortality rate for this type oftuberculous lesion corresponding to each other;now the gap between them is widening, as nodoubt it is for other forms of tuberculosis inyoung children.A recent attempt to estimate morbidity figures in
children infected before 5 years of age has beenmade in Newcastle by Cammock and Miller.They consider that of children under 5 years whohave had primary tuberculous infection, 3 to 5 percent. are liable to develop serious complications.Of the 258 infected children in Newcastle, whowere traced, it was found that 1.5 per cent.developed bone lesions and 4. I per cent. developedtuberculous meningitis or miliary tuberculosiswithin a minimum of two years from infection.3Apart from these there are the children who sufferfrom general ill-health as a result of gross glandularinfection or caseating tuberculous lesions in thelung and those who, although they eventuallyrecover from the tuberculous lesions, are left withchronic pulmonary lesions resulting from bron-chial occlusion.
In Rochester, New York, Beaven found in theo to I4 years age group that there were 78.7clinical cases of tuberculosis per i,ooo infectedpersons, a morbidity rate which was considerablyhigher than that in older age groups.
Looking at the problem from the point of viewof the individual child, the first question is toestablish whether or not the child is infected; ifinfected, to consider the likelihood of lesion togive rise to trouble. If the child is under 3 to 5years, there is considerable risk of illness of greateror less severity: if the child is over 5 years andunder i o years there is much less chance ofdeveloping clinical tuberculosis: if over io years,and more especially if I5 to 17 years, the outcomewill to a large extent depend on w;hether theprimary infection is recent .otf not. It may bepossible to establish this if previous tuberculintests have been negative, or the history of recentexposure to infection may make recent infectionlikely. If this is so, then there is a risk tihat therecent lesion may sprea4 rgiving- rise to chronicinfiltration.
DiagnosisThe classical pictures of acute tuberculous
bronchopneumonia, pleurisy, miliary andmeningeal tuberculosis, peritonitis and bonelesions need not be described here. Theseobvious lesions, apart from bronchopneumonia and
pleurisy, are in reality complications of a primarylesion which in itself may be much less easilyrecognized.A primary lesion may develop and resolve
without its presence being suspected; it maycause ill-health which is not readily recognizedas being due to tuberculous infection, or it maygive rise to persisting lesions in the lungs, non-tuberculous in themselves but resulting from theoriginal primary lesion. From the primarycomplex, tubercle bacilli may enter the bloodstream in small or large numbers, giving rise to thehaematogenous lesions. It is considered by manyobservers that haematogenous infection is commonalthough usually not manifest.
X-ray FindingsSymptoms and clinical signs although they may
be aids are usually too indefinite to be of any use inmaking a diagnosis of early primary tuberculosis.Radiography will provide the most useful evidenceof a primary lesion. On the other hand the absenceof any evidence in the radiogram does not neces-sarily exclude a primary lesion; the lesion may betoo small to show, or at too early a stage to show,or may be hidden by the mediastinal or heartshadows. Evidence of a primary complex when
X-RAY I. - Primarytuberculosis withenlargement ofglands at the lefthilum.
X-RAY 2.- Samechild, threeyears later,showing calcifi-cation in thehilar glands andin the lunglesion.
(X-Ray I & 2 reproduced by courtesy of the Royal Society ofMedicine).
by copyright. on S
eptember 16, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.344.288 on 1 June 1954. Dow
nloaded from

290 POSTGRADUATE MEDICAL JOURNAI--- - June i954visible is shown by the enlargement of glands at thehilum or supra-hilar region. The primary lesionin the lung may or may not be seen. It is oftennot possible to detect it until healing with calcification develops and makes it more visible in theradiogram (X-ray i and 2). When the early lunglesion can be seen it is small and localized, some-times slightly flocculent and sometimes homo-genous and demarcated from surrounding lung.There is, however, much variation in size of whatappears to be the primary lesion.The size of the enlarged glands also varies
greatly. The glands tend to be larger in the
e. ......
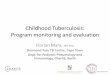
X-RAY 3a.-V.C., girl, 8 months old, October 5, 1953.Primary tuberculosis. Tension emphysema rightside with displacement of trachea and widenedcarina. Bronchoscopy showed right and left mainbronchi much narrowed; no ulceration seen.
X-RAY 3c.-Same child, December 2, I 95 3, three weekslater showing re-expansion of right lower lobe andcollapse of right middle lobe.
infants and young children. These glands owingto their anatomical relation to the bronchi, mayulcerate through the bronchial wall, or bulge thebronchial wall, altering the size of the lumen of oneof the larger bronchi. If the lumen is occluded,collapse of the lung segment beyond will resultand the X-ray will show an opacity due to thecollapsed lobe or segment. Incomplete obstruc-tion may give rise to tension emphysema of theaffected lobe. Collapse of one lobe or segmentmay be found together with tension emphysemain another part of the lung. (X-ray 3 a, b, c & d).
X-rays may show a homogenous shadow suggesting consolidation of a lobe or segment in whichthere may be cavitation. This appearance occurs
X-RAY 3b.-Same child, November 13, 1953, five weekslater and ten days after bronchoscopy, showingcollapse of right lower lobe.
X-RAY 3d.-December 2, 1953. Lateral view, showingcollapse of middle lobe.
by copyright. on S
eptember 16, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.344.288 on 1 June 1954. Dow
nloaded from

MACPHERSON: Problem of Tuberculosis in Childhood
in subacute or chronic caseating pneumoniadeveloping either from primary pulmonary lesionsor by bronchial spread.
Symptoms and SignsAlthough radiograms may show large hilar
shadows, there may be no symptoms and the childmay appear to be quite healthy and the X-rayfindings come as a surprise. It is not infrequent,however, to find evidence of some ill-health, suchas loss of energy, failure to gain weight normallyand slight irregular pyrexia.
Involvement of bronchi usually gives rise tolocalizing symptoms. Cough which is oftenparoxysmal may develop and a characteristicwheezing is noticed, becoming more marked afterexertion or crying. If large sections of lung areinvolved by collapse or emphysema there may becyanosis and distressed breathing or reluctance tomake any physical effort, even crying, whichrequires extra exertion. Babies who have not beenweaned may not be able to suck properly.Abnormal physical signs due to primary pulmon-
ary lesions are only evident when there is acutebroncho-pneumonia and miliary tuberculosis,collapse, emphysema or caseating pneumoniainvolving large areas of lung. The involvement ofthe bronchial wall due to ulceration or pressurefrom tuberculous glands may give rise to persistentrhonchi in the corresponding bronchus or apersistent inspiratory wheeze.
Collapse, involving large segments or even acomplete lobe of a lung may give rise to fewabnormal signs. Emphysema of the other portionsof lung and possibly fixation of mediastinum dueto adenitis may mask the presence of collapse.
Tension emphysema may be detected by fulnessof the affected side, displacement of the apex beatand hyper-resonance with absent breath sounds.
Large areas of caseating pneumonia which maybe associated with areas of collapse give rise tosigns of consolidation and the discrepancy betweenthe signs of consolidation and the general conditionof the child, with little malaise and often onlyslight pyrexia is remarkable and often gives thefirst clue as to the type of lesion present in the lung.
Management and Treatment of PrimaryTuberculosis in Children
For acute tuberculosis in childhood, includingacute bronchopneumonia, miliary tuberculosisand meningitis, treatment usually follows orthodoxlines. Streptomycin, para-amino salicylic acidand isoniazide are used in varying combinationswith the addition of tuberculin in meningitis, theresults of treatment varying more consistently withthe stage of the disease at which treatment is begun
than with the variations in technique or treatment.Details of such treatment need not be discussedhere.The management of primary tuberculous lesions
with less marked constitutional disturbance or withnone at all, gives rise to a greater degree of dif-ference of opinion.
It is, however, clear that the risks involved as aresult of contact with open cases of tuberculosis inearly childhood and probablv also in adolescence,are so serious that measures should be taken toprevent heavy infection, especially at these ages.
PreventionBovine infection is preventable and in large
towns is probably of insignificant account as a sourceof tuberculous disease. By adequate pasteurisa-tion of milk and by the use of milk from tuberculintested herds infection due to bovine tuberculosisdisappears. In country districts where un-pasteurized milk is provided from non-attestedherds, the risk of infection can be reduced orabolished by boiling milk before use.
Infection from human sources is more difficultto control. As soon as a source of active tuber-culosis is discovered, any young child in thehousehold or in close proximity should be keptaway until such time as the tuberculous patient isremoved elsewhere. Isolation of the child fromthe possible source of infection may be impossibleowing to inco-operation of parents, or, unfortu-niately, to lack of hospital accommodation and topoor housing.A considerable number of children are infected
by the time diagnosis of tuberculosis is made in the'contact ' case: this fact stresses the importanceof detecting active tuberculosis as early as possibleand justifies regular radiographic examination aswell as early investigation of any symptom whichmay be suspicious of tuberculosis in persons whocome into contact with young children..
In late childhood and adolescence it is less easyto control contact with infection where the sourceof infection is often undetectable.
B.C.G. InoculationB.C.G. inoculation is indicated when it is
impossible to remove the child from infection andwhen there is a possible risk of infection due toreactivity of a quiescent case in the child'senvironment. It is also desirable in late childhoodand adolescence when the possibility of infectionincreases with a widening of the young person'shorizon. By providing the child with a degree ofimmunity, the inoculation guards it from undesi-rable complications of primary infection of thelungs or intestine due to a heavy and uncontrolledfirst infection. It should however be impressed on
_7une I1954 2grby copyright.
on Septem
ber 16, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.344.288 on 1 June 1954. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
parents that this immunity is not complete anddoes not obviate care in the prevention of frequentand heavy infection, nor is the immunity perman-ent. Repetition at yearly intervals of tuberculintests should be carried out to ensure that theB.C.G. inoculation is still effective. In olderchildren, small exogenous reinfections frequentlymaintain hypersensitivity to tuberculin tests, butat this age also heavy and repeated infectionsshould be avoided. When there is known risk ofinfection, special care must still be taken insupervising such inoculated children and adoles-cents by regular radiographic examination.
Treatment of Primary Tuberculous LesionsMany children with primary lesions do not
require treatment. An analysis of 224 contactchildren between ages of birth to IS years whoattended the contact clinic at Brompton Hospitalduring the years I948 to I95I gives some indicationof the number who were considered to need someform of treatment or special care. These childrenwere all known to have been in close contact withsomeone with positive sputum or with evidence ofa tuberculous cavity; the group contains only those'Who were positive to tuberculin tests when first-examined.
Of these 224 children, II 7 (52.8 per cent.) hadno radiographic evidence of primary lesions; 41(18.7 per cent.) had evidence of calcification only,and 63 (28.5q per cent.) had signs which wereinterpreted as being due to active tuberculouslesions. The 4I children with calcified lesions hadnot had any treatment and therefore they had dealtwith their primary lesions satisfactorily withouttreatment. The II7 with no radiographic evi-dence of primary lesions were followed for aminimum of one year and developed no evidenceduring that time of further disease, therefore it mayfairly be presumed that there was no indication fortreatment in this group. Sixty-three (28.5 percent.) children had evidence of active tuberculouslesions, but in only 49 (2I.9 per cent.) of these wasthe lesion such that it was considered to requirespecial care.
Brian Thcmpson gives figures for childrenunder 14 years attending Ealing Club Clinic duringthe years 1942 to I945.4 There were 604children with positive tuberculin tests on firstexamination and 51 who converted from negativeto positive tests. Among these 655 infectedchildren there were 130 (19 per cent.) with lesions' which would reasonably be regarded as part of aprimary infection' on first examination or onconversion, a figure which corresponds closely tothat of 2I.9 per cent. quoted above. These figaresgive an indication of the significance which should
be attached to tuberculous infection during child-hood as a whole.From what has already been said, however, it is
obvious that the significance of tuberculous infec-tion is closely linked with the age at which it takesplace.Whether or not treatment is indicated will have
to be decided in each case which presents itself,according to its circumstances as well as to its age.Consideration will have to be given to degree andfrequency of infection, social and economicconditions, and also to the character and extent ofthe lesion found.The possible existence and the extent of the
lesion should not be gauged by one X-ray examina-tion. The radiogram may have been taken soonafter infection had taken place and before thelesion had fully developed, so that it is advisableto make a second X-ray examination within twoor three months of the first.When the only evidence of primary tuberculosis
is a moderate degree of hilar adenitis, regularsupervision with repetition of radiograms at regularintervals is all that is indicated as a rule. Thesechildren are very unlikely to be a source ofinfection and need not be segregated from otherchildren. When of school age they can usuallycontinue to attend school.
Gross hilar enlargement and any complicationsindicating bronchial involvement will requiremore definite treatment. Opinions at the presenttime are not unanimous concerning the value of-rest in bed for these lesions. Tne experience ofwise clinicians in the days before antibiotics andsurgical treatment were available should not, Ithink, be lightly cast aside and they were fullyaware of the value of rest in healing activetuberculous lesions. Insistence on rest in bed inthe early stage of large lesions, if necessary for aperiod of months, may prevent further compli-cations and may result in complete recovery oflesions which at first were extensive. A periodof rest in bed of four or six months in congenialsurroundings is no great hardship for a young child,and is worth while if the child is saved even aminimal risk of serious complications.Whether rest is provided at home or in hospital
or sanatorium will depend largely on homecircumstances. Apart from necessary room, freshair and good food a child must have company andentertainment or employment if it is going to stayin bed at all.
In the more acute cases and in those withstridor, it is advisable to have the child undersupervision and in expert care. Early signs ofcomplications such as meningitis or bone lesionsare usually more readily detected vhen the childis in an institution.
June 1954292by copyright.
on Septem
ber 16, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.30.344.288 on 1 June 1954. D
ownloaded from

June 1954 MACPHERSON: Problem of Tuberculosis in Childhood
Streptomycin, para-amino salicylic acid andisoniazide
In the acute forms of tuberculosis antibiotics areof great value. It is doubtful whether they haveany definite use in the treatment of large caseatingglands or chronic caseating pneumonia. Neitherthe size of the caseating lesions nor the rate ofhealing is dramatically influenced. There is notat present sufficient evidence to assess their valuein those cases where ulceration of a bronchus ispresent.
Since it is probable that haematogenous infec-tion to a greater or less degree arises in manyprimary lesions, especially in infants, antibioticsare given by some physicians to young childrenwho have evidence of recent infection with definiteprimary lesions, hoping in this way to reduce thepossibility of miliary lesions both evident andoccult.
Bronchoscopy and Surgical TreatmentTreatment when a bronchus has become
involved in the primary lesion presents manyproblems. It may be necessary, though rarely, as anemergency measure to clear the lumen of a bronchusof tuberculous material when stridor is marked andendangering a child's life. Bronchoscopic removalof the material may be attempted or, alternatively,thoracotomy and removal of the mass of glandsinvading the bronchial wall. Bronchoscopy maybe indicated for removal by suction of pus frombronchi, beyond the partial obstruction, whichhave become secondarily infected. RichardsandBlair6 recommend routine bronchoscopy in orderto reduce the possibility of bronchiectasis de-veloping in the collapsed lobe.How to treat the collapsed lobe is still a debatable
point. That bronchiectasis may result from suchcollapse is an established fact. As yet the numberof cases with collapse which develop bronchiectasiswith symptoms in later life is not known. Preven-tion and treatment of secondary infection in the
collapsed segment is no doubt of importance.The problem of the collapsed lobe is at presentbeing dealt with usually in one of three ways.Expectant treatment is advocated by some on theassumption that the majority heal sufficiently to-allow complete or partial re-expansion of thecollapsed lobe and, in only a few cases, willbronchiectasis develop later; others recommendresection of the collapsed lobe, or segment,either at an early stage or after a period of a year ormore if there has not been complete recovery, sopreventing future trouble in an unexpanded orpartially re-expanded segment. The third formof treatment is thoracotomy and removal of themass of caseating glands in order to preventpossible irreversible collapse and development ofbronchiectasis.The treatment of chronic caseating lesions
occupying large areas of the lung is also varied.With our present knowledge of this type of lesionit is not possible to say how many of them healcompletely, although apparently there are somewhich do so. It is clear that many of them remainin a chronic state for a year or more. It has beensuggested that parts of these lesions may remainunhealed and, in later life, give rise to clinicalpulmonary tuberculosis. On this assumption, itis suggested that removal of such caseating lunglesions is preferable to a ' wait and see ' policy.7On the one hand there is the risk of the operationand the possible disadvantage to a child of the lossof a lobe or even a complete lung and, on theother, the disadvantage of a long period oftreatment probably away from home and thepossible relationship of these lesions to clinicaltuberculosis in later life.
REFERENCESI.MEDICAL RESEARCH COUNCIL, National Tuberculin
Survey (1952), Lancet, i, 775.2. HYGE, T. V. (I945), Ugesk. f. Iacger, 105, 779.3. CAMMOCK, R. M., and MILLER, F. J. W. (I953), Lancet,
i, is8.4. BEAVEN, P. W. (igso), Dis. of Chest, 17, 28o.5. THOMPSON, B. C. (1952), Proc. Roy. Soc. Med., 45, 74I.6. BLAIR, L. G., and ROBBERTS, S. C. (I950), Lancet, i, 386.7. THOMAS, D. (I952), Proc. Roy. Soc. Med., 45, 743.
Continuation of Biblio-rabhv-Yohn C. Roberts, M.D., M.R.C.P., from page 287.BIBLIOGRAPHY
-MAHER-LOUGHNAN, G. P. (1952), Tubercle, 33, 342.BIGNALL, J. R., CROFTON, J. W., and THOMAS, J. A. B.
(i95i), Brit. med J7 i, 554.NHECK, W., and CORk IN HINSHAW H., i2th U.S. Dept. Vet.Admin. Cont. on Chemotherapy of Tuberculosis.
SUMNER, J. (i949), Tubercle, 3, 62.CROFTON, J. (1952), Brit. med. J., ii, IOI4.ANNOTATION (I9S3), Lancet, i, 23I.PUGH, D. L., EDWARDS, G. F., McLAREN, R. G., and
JONES, E. R. (1952), Tubercle, 33, 369.HOUGHTON, L. E. (1952), Ibid., 33, 381.RUBIN, B. HASSETT, G. L.Jun.,THOMAS, B. G. H., and
BURKE, J. C. (1952), Amer. Ret. Tthberc., 65, 392.LUNTZ, G. R. W. N., and SMITH, S. G. (1953), Brit. med. J7.,
i, 296.ROSS-COSBIE, J., GOW, J. G., and ST. HILL, C. A. (I953),
Ibid i, 901TURIBJULL, F. W. A., WALLACE, A. T., STEWART,SHEILA, and CROFTON, J. W. (I953), Ibid., i, 1244.
MIcCARTHY, D., and MANN, T. P. (I950), Ibid., i, 341.
BARNETT, MARGARET, BUSHBY, S. R. M., and MIT-CHESON, D. A. (I953), Lancet, i, 314.
JOINER, C. L., MACLEAN, K. S., PRITCHARD, E. K., ANDER-SON, K., COLLARD, P., KING, M. B., and KNOX, R.(1952), Ibd., ii, 843.
MEDICAL RESEARCH COUNCIL REPORT No. 4 (1953),Ibid., ii, 217.
LORBER, J. (i950), Ibid., i, 389.ANDERSON, T., KERR, MIARY, and LANDSMAN, JOAN
(1953), Ibid., ii, 69i.RITCtilE, M., TAYLOR, R. M., and DICK, J. C. (1953), Ibid.,
ii, 4I9.TORRES-GOST,-J. (I953), Ibid., ii, 693.FLETCHER, A. P. (I953), Ibid., ii, 694.CATHIE, L. A. P. (i950), Ibid., i, 44I.SMITH, HONOR V., and VOLLUM, R. L. (I950), Ibid., ii, 275.EVANS, E. T. (1952), J. Bone and yoint Surg., 2, 267.DEROY, M. S., and FISHIER, H. (1952), Ibid., 2, 299.DICK, J. C. (I953), Lancet, i, 8o8.BURNS, T., SMITH, H. G. M., and SNAITH, L. M. (I953),
Ibid., i, 8I7.
by copyright. on S
eptember 16, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.30.344.288 on 1 June 1954. Dow
nloaded from