Embed Size (px)
Citation preview

The Prognostic Value of CD38 Expression and
its Quantification in B Cell Chronic Lymphocytic
Leukemia (B-CLL)
TRYFONIA MAINOU-FOWLER*, HELEN M. DIGNUM, STEPHEN J. PROCTOR andGEOFFREY P. SUMMERFIELD
Haematological Sciences, School of Clinical and Laboratory Sciences, The Medical School, Leech Building, Framlington Place, Newcastle uponTyne NE2 4HH, UK
(Received 11 September 2003)
A large number of prognostic factors are available to help predict the outcome of patients who presentwith B-cell chronic lymphocytic leukemia (B-CLL). These include clinical stage, leukemic cellmorphology, lymphocyte doubling time, the pattern of infiltration in bone marrow trephine biopsies,cytogenetic abnormalities, p53 function and serum factors such as beta-2 microglobulin. Two recentlydescribed major prognostic factors are immunoglobulin heavy chain variable region (IgVH) mutationstatus and cell membrane expression of CD38. These are both highly significant independentprognostic factors, but are not closely correlated.
Whereas IgVH mutational status is a time consuming and demanding technique, only available in alimited number of centres, CD38 expression by flow cytometry is relatively simple and rapidlyobtained in most diagnostic laboratories. The predictive value of CD38 expression is enhanced bymeasurement of antigen density in terms of antibody binding capacity (ABC) rather than as thepercentage of cells expressing the antigen. ABC correlates closely with relative median fluorescence(RMF), a parameter which is even more simply and cheaply obtained by flow cytometry. One of thesemethods of determining CD38 expression should be employed routinely.
Recent work suggests that membrane ZAP-70 expression determined by flow cytometry will proveto be an accurate proxy for IgVH mutational status and this assay will be within the reach of anylaboratory skilled in flow cytometry. The combination of ZAP-70 expression, CD38 antigen density,p53 function and the concentration of serum factors such as soluble CD23, is likely to provideextremely accurate prognostic information in future studies. This will assist in identifying Stage Apatients who may benfit from early and/or more intensive treatment, as well as Stage B and C patientswho may require alternative treatment strategies at the outset.
Keywords: Chronic lymphocytic leukemia; CD38 quantification
INTRODUCTION
B-cell chronic lymphocytic leukemia (B-CLL) is the
commonest leukemia in the developed world, accounting
for about 40% of all leukemias [1]. It is a malignant B-cell
proliferation with a wide clinical spectrum of disease,
course and prognosis. The disease is characterized by the
clonal accumulation in the peripheral blood and bone
marrow of small, mature-looking CD5+ B-lymphocytes
with a distinct immunophenotype [2,3]. Originally, B-
CLL was considered to be a disease of antigen-
inexperienced (pre- germinal center) or naı̈ve B-lympho-
cytes. Sequence analysis of the immunoglobulin (Ig)
variable heavy (VH) region genes of leukemic cells from
patients with B-CLL showed that these cells bear the
germline configuration [4,5]. However, recent data
suggest that in some B-CLL cases the B-cells may arise
from post-germinal centre, memory B-cells. Sequence
analysis of VH and light chain variable regions of the Ig
genes showed that 57% of IgG+ CD5+ [6] and about
50% of IgM+ cases [7] possess somatic mutations. These
findings indicate that depending on the mutational status
of the Ig VH genes, patients with B-CLL can be divided
into two groups; those with unmutated (pre-germinal
center) and those with mutated genes (post-germinal
center).
*Corresponding author. Tel.: +44 (0)191 282 0641/282 0451. Fax: +44 (0)191 222 5524. E-mail: [email protected]
Leukemia & Lymphoma, March 2004 Vol. 45 (3), pp. 455–462
ISSN 1042-8194 print/ISSN 1029-2403 online # 2004 Taylor & Francis LtdDOI: 10.1080/1042819032000141275
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.

B-CLL is predominantly a disease of the middle-aged
and elderly, but a proportion of patients are of an age
when more intensive treatment, even potentially curative
high dose therapy, can be considered. The clinical course
of B-CLL is highly variable. Most patients present with
stable non-progressive disease and survive for prolonged
periods without requiring treatment. In others, the
disease progresses rapidly and patients die despite
aggressive treatment [8]. The two staging systems that
were introduced almost three decades ago have been
effective in classifying patients with B-CLL into different
prognostic groups [9,10]. While both systems are useful in
assessing prognosis, they fail to identify the subsets of
early stage patients (Rai 0 and 1, Binet A) that may
progress rapidly and therefore benefit from early or more
intensive therapy. The clinical management of CLL
therefore requires the identification of clinically useful
prognostic markers to guide therapy.
A large number of studies have been performed in
recent years to identify factors of prognostic value in B-
CLL (reviewed by Zwiebel and Cheson [8]). Clinical (11)
and hematological parameters including morphological
variants and type of pattern of bone marrow infiltration
[12], kinetic variables [13,14], immunological markers
[15 – 21] and genetic abnormalities (reviewed by Stilgen-
bauer et al.) [22] are useful independent prognostic
factors, with some of them being able to identify patients
who present with low tumor load but have a poor
outcome [19 – 21]. However, while most of these have
proven to be valuable indicators of poor prognosis, they
do not always provide useful information for all patients
and remain imperfect in individual cases. Recently,
studies have reported that both the mutational status of
Ig VH genes and the phenotypic expression of CD38 by
the leukemic clone are powerful prognostic factors in B-
CLL.
THE CD38 ANTIGEN
The human CD38 antigen, initially described as a T-cell
differentiation antigen (T10) [23], is a non-lineage
restricted type II glycoprotein involved in lymphocyte
activation [24]. The molecule consists of a single chain of
46 kDa spanning the membrane with its carboxyl
terminus located in the extra-cellular compartment [25].
Its ligand has recently been identified as the platelet
endothelial cell adhesion molecule-1 (CD31) [26].
The CD38 antigen is a member of the family of the
leukemic multi-lineage markers [23] and has a multi-
functional activity [27]. It mediates several diverse
functions including signal transduction, cell adhesion, in
particular adhesion to endothelium, and plays an
important role in lymphocyte homing [28]. CD38
specifically interacts with the CD31 molecule, a cell
surface glycoprotein expressed on hemopoietic and
endothelial cells [26]. Ligation of CD38 has been reported
to inhibit normal human B-cell lymphopoiesis [29] while
CD38 signaling mediated by agonistic antibodies prevents
apoptosis of germinal centre B cells [30]. This finding
suggests that the level of CD38 expression may affect the
overall survival of B-cell clones. In addition, CD38 has
enzymatic properties; it is an ecto-enzyme whose extra-
cellular domain has activities which lead to synthesis and
hydrolysis of cyclic adenosine di-phosphate – ribose [31].
Expression of the CD38 antigen is not restricted to a
specific lineage nor to a discrete activation stage. It is
expressed on CD34+ precursor cells, un-stimulated pre-
germinal center B-cells, germinal center B-cells, myeloid
precursors, peripheral blood NK cells, activated T and B
lymphocytes and terminally differentiated cells including
plasma cells [32,33].
Although the exact function of the CD38 antigen
remains unclear, its expression has been used as a marker
to study leukocyte activation and differentiation [32].
Analysis of CD38 and Ig gene expression has been used to
assign B-cells to various stages of differentiation from
naı̈ve to memory cell [34]. Also CD38 expression has been
useful in the systemic classification of T- and B-cell
malignancies [23]. It has been reported that leukemias
which result in immortalization of early differentiation
stages are CD38+, while differentiated phenotypes are
CD38– [32]. In recent years, expression of CD38 has been
associated with disease progression and outcome in many
different types of leukemia, including B-CLL [35 – 37].
Ig VH GENE MUTATIONS IN B-CLL
In 1999, the pivotal studies of Hamblin et al. [38] and
Damle et al. [37] mutually demonstrated that the
mutation status of the Ig VH genes predicts the natural
history of B-CLL. Both studies showed that the presence
of unmutated VH genes was associated with inferior
clinical course, even within the group of patients with
Binet Stage A [38] or Rai intermediate risk group [37]. By
contrast, patients with mutated genes followed a more
indolent course of B-CLL [37,38]. Others have since
confirmed these findings [39 – 45]. Collectively these
studies have shown that patients with B-CLL can be
divided into two prognostic groups; those with unmu-
tated genes who have a poorer prognosis and require
more treatment while patients with mutated genes
experience a more indolent course. In addition, some of
these studies have provided new important information
regarding patients’ survival in relation to mutation status.
Retaining responsiveness to IgM ligation has been
suggested to contribute to the poor prognosis associated
with the unmutated group [46]. Oscier and colleagues
reported that the unmutated Ig VH genes were associated
with previously known adverse abnormalities including
complex karyotype, atypical cell morphology, stage and
unfavorable genetic defects such as trisomy 12 and
deletion 11q23 [40]. The more favorable genetic aberra-
tion 13q14 was over represented in the mutated group
[40]. This finding was confirmed by Krober et al. who also
456 T. MAINOU-FOWLER et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.

demonstrated that the high-risk genetic alterations 17p
and 11q23 are almost exclusively found in patients with
unmutated genes [43].
It is clear from these studies that the relative lack of Ig
VH gene mutations is linked to a poorer disease outcome.
Thus, knowledge of the mutational status at diagnosis
could prove valuable in identifying patients whose disease
is destined to progress and, consequently, to clinically
manage these patients more efficiently. Investigating Ig
VH gene mutations as part of the routine diagnostic work
up of B-CLL could be problematic; the procedure is
complex and expensive and not all laboratories are
suitably equipped. The identification of a phenotypic
surrogate marker for mutational status would prove
valuable.
PROGNOSTIC SIGNIFICANCE OF CD38
EXPRESSION IN B-CLL
In 1999, Damle et al. in their pivotal study found a strong
correlation between VH gene mutations and phenotypic
CD38 expression in B-CLL [37]. They demonstrated that:
(1) leukemic clones from patients with unmutated
genes almost always express CD38 at a level
5 30%.
(2) identified the group of patients with inferior
clinical course and
(3) were able to segregate the Rai intermediate risk
group who followed a more aggressive course
from those with indolent disease.
Damle et al. proposed that the VH gene mutation status
and CD38 expression should be used as prognostic
indicators of disease progression and outcome in B-
CLL [37]. In addition, CD38 expression, a phenotypic
marker easily measured in the clinical setting, could be
used as a surrogate for the Ig VH gene mutation state.
In their follow-up study, Hamblin et al. were unable to
confirm the above findings [41]. Hamblin et al. reported
an association between the percentage of CD38 expres-
sion and VH Ig gene mutations, but the results were
discordant in about 30% of cases [41]. In a multivariate
analysis, CD38 expression and mutational status were
shown to be independent prognostic factors [41].
Similarly, other studies have since reported that CD38
expression is not a good predictor of Ig gene mutational
status [42,43,45,47 – 49]. In addition, while some of these
studies have reported CD38 expression to have indepen-
dent prognostic value [42,43,45,48], others were unable to
demonstrate such a finding [40, 47]. Nevertheless, recent
studies have provided evidence to confirm that CD38
expression is an important prognostic factor in B-CLL.
CD38+ B-cell percentage positivity was shown to
predict for overall survival [37,50 – 57], progression-free
survival [50,53], event-free survival after first-line therapy
[58], requirement for treatment [37,55,59], time to first
treatment [51,53,56] and response to therapy [50]. In one
study, measurement of CD38 expression identified a sub-
group of patients with either better or poorer prognosis
within the poor or good prognostic groups, respectively
[52]. Recently, CD38 positivity in association with
increased expression of its ligand CD31, has been
reported to identify a subset of cases with inferior
outcome than CD38 alone [60]. Moreover, the percentage
of CD38 positivity was reported to be significantly
associated with known factors of poor prognosis,
including gender, stage, lymphocyte doubling time,
lymphadenopathy, atypical morphology, diffuse pattern
of bone marrow infiltration and serum levels of beta-2
microglobulin (b2M) and soluble CD23 [50,52 – 55,59,61].
The known favorable chromosomal deletion 13q14 was
shown to occur mainly in the CD38– group [54] while
trisomy 12 was detected in the CD38+ group [54]. By
contrast, 17p and 11q23 deletions were undetectable in
the CD38– cases [62]. In addition, recently it has been
reported that the combination of CD38 positivity and/or
evidence of p53 dysfunction identifies poor risk cases
more effectively than Ig VH mutation alone [39].
Unmutated Ig VH with normal p53 function and CD38
expression of 5 20% showed no survival disadvantage
compared to mutated Ig VH cases. Dysfunction of p53
and/or CD38 positivity 4 20% correctly identified all
poor risk patients, and was more specific than the Ig VH
mutation [39]. There was no significant correlation
between p53 dysfunction and CD38 positivity [39].
Collectively, all the above studies show that the
percentage of CD38 expression is an excellent indepen-
dent prognostic marker and measurement of CD38
should be used in the routine work up of B-CLL to
identify the poor risk cases. However, despite the
usefulness in predicting for poor outcome, investigating
CD38 expression can be problematic.
CD38 expression can change with time and under
different conditions. The percentage of CD38 expression
may increase with disease progression [41,63] or during
infections; chemotherapy selectively eliminates the
CD387 clone [41]. Moreover, depending on the cut off
levels chosen, some patients could be classified to different
prognostic groups at different time points according to
the level of CD38 expression [43]. It is important
therefore for the accurate assessment of the prognostic
significance of CD38 positivity to ensure that only
samples close to or at the time of presentation are tested.
The cut off level that predicts for poor outcome has
been disputed. Although the 30% cut off point in the
study by Damle et al. [37] was selected arbitrarily, this
was subsequently identified as a statistically valid cut off
level for predicting disease progression and outcome
[41,51]. Other studies also used the 30% cut off point
[40,42,47,48,50,51,53 – 55,61], while some reported that
the lower levels of 20% [39,56,57] or 15% [59] predicted
for poor outcome. None of these studies has reported any
modifications of the findings if different cut off levels are
used. By contrast Hamblin et al. [41] and Domingo-
457PROGNOSTIC VALUE OF CD38 EXPRESSION
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.

Domenech et al. [55] reported no alterations in their
results between the two cut off points of 20% and 30%.
Similarly, in another study, both 20% and 30% CD38
positivity were significant predictors of progression-free
survival, albeit the latter had a slightly better predictive
value [42]. In this study, the optimal cut off point was 7%.
The sensitivity and specificity of this level, however, were
greatly reduced [42]. When 30% CD38 expression was
used to predict Ig VH mutational status, the specificity
also fell significantly [42]. A level of 7% of CD38
positivity has since been reported to be a better predictor
of inferior outcome than the 30% cut off point [43].
Recently, Ghia et al. [45] were unable to demonstrate
the predictive value of CD38 expression based on the
percentage positivity. They reported a bimodal expression
of CD38 [45]. In their elegant studies, these authors
showed that the presence of a distinct CD38+ population
within the leukemic clone, irrespective of its size,
identified the cases with progressive disease rather than
the numerical cut off definitions used by others [45].
Bimodal CD38 expression was previously reported by
Jelinek et al. [42] who, in addition, demonstrated that the
CD38+ and CD387 cells belonged to the same clone.
The greatest value of CD38 expression and other
factors of prognostic value in B-CLL is to assess the
likelihood of future disease progression in early stage
patients. To date, few studies have shown that the
percentage of CD38 positivity can identify early stage
patients that are likely to progress or die from B-CLL.
Damle et al. were the first to report that CD38 positivity
5 30% identified those cases in the Rai intermediate risk
group with inferior course of disease [37]. Similarly,
others have reported that the percentage CD38 of 5 30%
or 5 20% identified the patients that belonged to Rai
stage 0 – I [55] or 0 – III [52] respectively, who had a
poorer outcome. By contrast, other investigators were
unable to show a significant association between CD38
positivity and inferior clinical course in the Binet Stage A
group. Heintel et al. [61] reported discordant findings
between risk factors including b2M, sCD23, lymphocyte
doubling time, time to therapy, and WBC in the CD38+
Binet Stage A patients. None of these patients progressed
to higher Binet stage [61]. Our group also reported that
5 30% CD38 expression did not predict for survival or
treatment requirement for Binet Stage A or younger
patients [51]. We found, however, that quantification of
CD38 by flow cytometry significantly improved the
prognostic value of percentage CD38 expression [51].
QUANTIFICATION OF CD38 AND ITS
SIGNIFICANCE IN B-CLL
Despite the usefulness of flow cytometric evaluation of
CD38 in the prognostication of B-CLL, the subjective
determination of positive percentages may result in
ambiguity of the test. In addition, controversy exists
between different centers in connection with the predictive
cut off levels. Ghia and colleagues have overcome this
problem by evaluating the CD38 positive cell population
within the leukemic clone [45]. However, the distinction
between positive and negative populations is not always
as clear as these authors have indicated and, conse-
quently, discordant cases will add ambiguity to the
method. Moreover, if evaluation of CD38 expression is
to enter the clinical arena, a reproducible method must
exist that gives similar results in different laboratories.
Quantification of CD38 antigen overcomes the problem
of subjectivity and also has the potential to yield less
variation [64,65] and therefore more reproducible results.
Several methods for antigen quantification have been
described [66,67]. The majority of studies have used beads
coated with known amounts of antibody conjugated with
a specific fluorochrome which serves as a control for the
immunofluorescence analysis. The quantiBRITE system
makes use of a fluorochrome antibody reagent that has a
1:1 fluorochrome to protein ratio and also uses multi-
leveled calibrated beads with known and incremental
fluorochrome fluorescence [67]. This method measures
absolute levels of antigen as antibodies bound per cell.
The quantum simply cellular (QSC) antibody binding
capacity employs a cocktail of five highly uniform
microbead populations, one blank and four coated with
a defined and different quantity of anti-mouse polyclonal
antibody which has balanced reactivity against all Ig
isotypes [67]. The beads by having incremental antibody
binding capacity, can place a check on the degree of
compensation across the entire range of fluorescence
intensity. Also, the beads are labeled with the same
antibody/conjugate as the cells. This provides a high
degree of spectral matching. The intensity of the antigen
is expressed as antibody binding capacity (ABC).
Recently, Hsi et al. reported that the intensity of CD38
expression, evaluated using the quantiBRITE system,
identified a higher percentage of CD38 positive patients
than percentage expression alone [68]. Moreover, these
authors provided evidence to suggest that a subgroup of
B-CLL patients with 5 30% CD38 and poor overall
survival could only be identified by CD38 quantification
[68]. In addition, in an earlier study, CD38 intensity in
association with the percentage CD38 positivity had a
higher predictive power for overall survival than the
positive percentage alone [57]. Our group used QSC ABC
to show that the intensity of CD38 expression and not the
percentage positivity predicted for disease-specific survi-
val and time to treatment of Binet Stage A patients and
also for disease-specific survival of patients under 60 years
[51].
Quantification of CD38 expression using commercially
available beads involves an added expense and complex-
ity in the day to day clinical work up of B-CLL. Antigen
expression can also be quantified using relative median
fluorescence (RMF) [69]. RMF can be defined as the ratio
of median value of the fluorescence of the test over that of
the control; these values are based on flow cytometer
readings. RMF may not be as accurate as quantification
458 T. MAINOU-FOWLER et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.

using beads but is easy to perform and involves no
expense. Our group has recently completed a study to
investigate whether the intensity of CD38 expression
evaluated using RMF has a predictive value similar to
that of ABC. We found that only the intensity by either
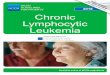
ABC or RMF predicted for:
(1) disease-specific survival of Binet Stage A patients
(Fig. 1)
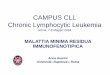
(2) survival of Binet Stage A patients under 60 years
(Fig. 2) and
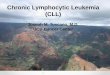
(3) time to treatment for patients in Binet Stage A and
under 60 years (Fig. 3).
The RMF was as good a predictive marker as the ABC
(Figs. 1 – 3).
It is clear from the above studies that quantification of
CD38 expression is a better method to identify higher risk
cases. We recommend the adoption of CD38 quantifica-
tion wherever CD38 positivity is currently measured as
part of the assessment of B-CLL patients. Trials could
verify the predictive value of quantification by using
either ABC or RMF or any other antigen quantification
method.
CONCLUSIONS AND FUTURE DIRECTIONS
The expression of CD38 is an excellent prognostic marker
in B-CLL and it should be used clinically in the routine
��
��
��
� ��� ��� ��� ����
��
��
��
������
����
�� ����
������
��������
� ��� ��� ��� ����
��
��
��
���������
�������
��� ����
������
��������
� ��� ��� ��� ����
��
��
��
������� ��
���� ���
��� ���� ��
������
��������
FIGURE 1 Disease-specific survival of Binet Stage A patients. (A)RMF: median survival: RMF 4 3: 103 months; RMF 5 3: undefined.(B) ABC: median survival: ABC 4 250: 214 months; ABC 5 250:undefined. (C) Percentage CD38: median survival: CD38 4 30%:undefined; CD 38 5 30%: undefined. n=158 ; the cut off level forRMF was 3 (Fisher’s Exact test).
��
��
��
� ��� ��� ��� ����
��
��
��
������
����
� ������
������
��������
� ��� ��� ��� ����
��
��
��
���������
�������
� ������
������
��������
� ��� ��� ��� ����
��
��
��
������� ��
���� ���
� ������ ��
������
��������
FIGURE 2 Disease-specific survival of Binet Stage A patients less than60 years. (A) RMF: median survival: RMF 4 3: 102 months; RMF 5 3:undefined. (B) ABC: median survival: ABC 4 250: 102 months; ABC5 250: undefined. (C) Percentage CD38: median survival: CD38 4 30%:undefined; CD 38 5 30%: undefined. n=158; the cut off level for RMFwas 3 (Fisher’s Exact test).
459PROGNOSTIC VALUE OF CD38 EXPRESSION
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.

work up of CLL. Quantification of the CD38 antigen by
flow cytometry greatly improves the prognostic value of
the percentage expression, especially for the early stage
and younger patients. Trials should be performed in
different centers to evaluate the prognostic significance of
quantification of CD38. Furthermore, if the expression of
CD38 should enter the clinical field, it is advisable that
other parameters including type of reagents, methodology
and instrumentation are evaluated in order to minimize
the inter-laboratory variation.
Recently, studies have suggested that the expression of
the tyrosine kinase ZAP-70 may be a better surrogate for
the Ig VH mutational status than the expression of CD38.
Gene expression profiling in patients with B-CLL, has
shown that ZAP-70 expression predicts the mutational
status of the Ig VH genes [70 – 72]. Furthermore, recently
it has been reported that the expression of ZAP-70 is
associated with increased signalling though the B cell
receptor [73] and identifies patients in the poor risk group
[71,72,74].
Clearly, ZAP-70 expression has a great potential.
However, until the prognostic value of this marker is
assessed in different centers, and a method suitable for its
routine evaluation is developed, measurement of CD38
antigen density on the leukemic cell surface is likely to
retain its prognostic utility in B-CLL.
It is suggested that measurement of CD38 and ZAP-70
expression in association with other factors of prognostic
value including serum CD23 [19] and p53 expression [39]
are used to develop a prognostic profile that will assist in
treatment decisions for patients with this common
lymphoproliferative disorder.
Acknowledgements
Dr T. Mainou-Fowler has been supported by The
Tyneside Leukaemia Research Association and the
Leukaemia Research Fund.
References
[1] Rai, K. and Patel, D. (1995) Chronic lymphocytic leukaemia. InHematology: Basic Principles and Practice, edited by R. Hoffman, E.Benz, S.Shattil, B. Furle, H. Cohen and L. Silberstein. Pp. 1308 –1321. New York: Churchill Livingstone.
[2] Matutes, E., Owusu-Ankomah, K., Morilla, R., Marco, J.G.,Houlihan, A., Que, T.H., et al. (1994) ‘‘The immunological profileof B cell disorders and proposal of a scoring system for the diagnosisof CLL’’, Leukemia, 8, 1640 – 1645.
[3] Matutes, E. and Polliack, A. (2000) ‘‘Morphological and immuno-phenotypic features of chronic lymphocytic leukemia’’, Reviews inClinical and Experimental Hematology, 4, 22 – 47.
[4] Kipps, T.J., Tomhave, E., Pratt, L.F., Duffy, S., Chen, P.P. andCarson, D.A. (1989) ‘‘Developmentally restricted immunoglobulinheavy chain variable region gene expressed at high frequency inchronic lymphocytic leukemia’’, Proceedings of the NationalAcademy of Science USA, 86, 5913 – 5917.
[5] Deane, M. and Norton, J.D. (1991) ‘‘Preferential rearrangement ofdevelopmentally regulated immunoglobulin VH1 genes in human B-lineage leukemias’’, Leukemia, 5, 646 – 650.
[6] Hashimoto, S., Dono, M., Wakai, M., Allen, S.L., Lichtman, S.M.,Schulman, P., et al. (1995) ‘‘Somatic diversification and selection ofimmunoglobulin heavy and light chain variable region genes inIgG+ CD5+ chronic lymphocytic leukemia B cells’’, Journal ofExperimental Medicine, 181, 1507 – 1517.
[7] Fais, F., Ghiotto, F., Hashimoto, S., Sellars, B., Valleto, A., Allen,S.L., et al. (1998) ‘‘Chronic lymphocytic leukemia B cells expressrestricted sets of mutated and unmutated antigen receptors’’,Journal of Clinical Investigation, 102, 1515 – 1525.
[8] Zwiebel, J.A. and Cheson, B.D. (1998) ‘‘Chronic LymphocyticLeukemia: staging and prognostic factors’’, Seminars in Oncology,25, 42 – 59.
[9] Rai, K., Sawitksy, A., Cronkite, E.P., Chanana, A.D., Levy, R.N.and Pasternack, B.S. (1975) ‘‘Clinical staging of chronic lympho-cytic leukemia’’, Blood, 46, 219 – 234.
[10] Binet, J.L., Auquier, A., Dighiero, G., Chastang, C., Piguet, H.,Goasguen, J., et al. (1981) ‘‘A new prognostic classification ofchronic lymphocytic leukaemia derived from multivariate survivalanalysis’’, Cancer, 48, 198 – 206.
��
��
��
� ��� ��� ����
��
��
��
�������
����
��� ����
������
��������
� ��� ��� ����
��
��
��
���������
������
��� ����
������
��������
� ��� ��� ����
��
��
��
������� ��
���� ��
��� ���� ��
������
��������
FIGURE 3 Time to treatment of Binet Stage A patients less than 60years. (A) RMF: median time to treatment: RMF 4 3: 44 months; RMF5 3: 116 months. (B) ABC: median time to treatment: ABC 4 250: 33months; ABC 5 250: 116 months. (C) Percentage CD38: median time totreatment: CD38 4 30%: 54 months; CD 38 5 30%: 116 months.n=158; the cut off level for RMF was 3 (Fisher’s Exact test).
460 T. MAINOU-FOWLER et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.

[11] Lee, J.S., Dixon, D.O., Kantarjian, H.M., Keating, M.J. andTalpaz, M. (1987) ‘‘Prognosis of chronic lymphocytic leukemia: Amultivariate regression analysis of 325 untreated patients’’, Blood,69, 929 – 936.
[12] Frisch, B. and Bartl, R. (1988) ‘‘Histologic classification and stagingof chronic lymphocytic leukaemia’’, Acta Haematologica, 79, 140 –152.
[13] Molica, S. and Alberti, A. (1987) ‘‘Prognostic value of thelymphocyte doubling time in chronic lymphocytic leukemia’’,Cancer, 60, 2712 – 2716.
[14] Christiansen, I., Gidlof, C., Wallgren, A.C., Simonsson, B. andTotterma, T.J. (1994) ‘‘Serum levels of soluble intercellular adhesionmolecule 1 are increased in chronic lymphocytic leukemia andcorrelate with clinical stage and prognostic markers’’, Blood, 84,3010 – 3016.
[15] Kay, N.E., Burton, J., Wagner, D. and Nelson, D.L. (1988) ‘‘Themalignant B-cells from chronic lymphocytic leukemia patientsrelease TAC soluble interleukin-2 receptors’’, Blood, 72, 447 – 450.
[16] Molica, S., Levato, D., Olio, M.D., Cascavilla, N., Matera, R.,Minervini, M., et al. (1997) ‘‘Clinico-prognostic implications ofincreased levels of soluble CD54 in the serum of B-cell chroniclymphocytic leukaemia patients. Results of a multivariate survivalanalysis’’, Haematologica, 82, 148 – 151.
[17] Christiansen, I., Sudstrom, C. and Totterman, T.H. (1998)‘‘Elevated serum levels of soluble vascular cell adhesion molecule-1 (sVCAM-1) closely reflect tumour burden in chronic lymphocyticleukaemia’’, British Journal of Haematology, 103, 1129 – 1137.
[18] Ferrajoli, A., Keating, M.J., Manshouri, T., Giles, F.J., Dey, A.,Estrov, Z., et al. (2002) ‘‘The clinical significance of tumor necrosisfactor-a plasma level in patients having chronic lymphocyticleukemia’’, Blood, 100, 1215 – 1219.
[19] Sarfati, M., Chevret, S., Chastang, C., Biron, G., Stryckmans, P.,Derespesse, G., et al. (1998) ‘‘Prognostic importance of serumsoluble CD23 levels in chronic lymphocytic leukemia’’, Blood, 88,4259 – 4264.
[20] Keating, M.J., Lerner, S., Kantarjian, H., Freireich, E.J. andO’Brien, S. (1995) ‘‘The serum b2-microglobulin level is morepowerful than stage in predicting response and survival in chroniclymphocytic leukemia’’, American Society of Haematology AnnualMeeting, Blood, 86, 606a.
[21] Hallek, M., Langenmayer, I., Nerl, C., Knauf, W., Dietzfelbinger,H., Adorf, D., et al. (1999) ‘‘Elevated serum thymidine kinase levelsidentify a sub-group at high risk of disease progression in early nonsmoldering chronic lymphocytic leukemia’’, Blood, 93, 1732 – 1737.
[22] Stilgenbauer, S., Bullinger, L., Lichter, P., Dohner, H. and TheGerman CLL Study Group (GCLLSG) (2002) ‘‘Genetics of chroniclymphocytic leukemia: genomic aberrations and V(H) gene muta-tion status in pathogenesis and clinical course’’, Leukemia, 16, 993 –1007.
[23] Reinherz, E.L., Kung, P.C., Goldstein, G., Kumagai, M., Coustan-Smith, E. and Murray, D.J. (1980) ‘‘Discrete stages of intrathymicdifferentiation: analysis of normal thymocytes and leukemiclymphoblasts of T lineage’’, Proceedings of the National Academyof Sciences of the United States of America, 77, 1588 – 1592.
[24] Funaro, A., Horenstein, A.L. and Malavasi, F. (1995) ‘‘HumanCD38: a versatile leukocyte molecule with emerging clinicalperspectives’’, Fundamental and Clinical Immunology, 3, 101 – 113.
[25] Malavasi, F., Funaro, A., Alessio, M., De Monte, L.B., Ausiello,C.M., Dianzani, U., et al. (1992) ‘‘CD38: a multilineage cellactivation molecule with a split personality’’, International Journalof Clinical and Laboratory Research, 22, 73 – 80.
[26] Deaglio, S., Morra, M., Mallone, R., et al. (1997) ‘‘Humal CD38(ADP-ribosyl cyclase) is a counter-receptor of CD31, an Igsuperfamily member’’, Journal of Immunology, 160, 395 – 402.
[27] Mehta, K., Shahid, U. and Malavasi, F. (1996) ‘‘Human CD38, acell surface protein with multiple functions’’, FASEB Journal, 10,1408 – 1417.
[28] Dianzani, U., Funaro, A., Di Franco, D., Garbarino, G., Bragardo,M., Redoglia, V., et al. (1994) ‘‘Interaction between endotheliumand CD4+/CD45RA+ lymphocytes’’, Journal of Immunology,153, 952 – 959.
[29] Kumogai, M., Cousan-Smith, E., Murray, D.J., Silvennoinen, O.,Gopal Murti, K., Evans, W.E., et al. (1995) ‘‘Ligation of CD38suppresses human B lymphopoiesis’’, Journal Experimental Medi-cine, 181, 1101 – 1110.
[30] Zupo, S., Rugari, E., Dono, M., Tamborelli, G., Malavasi, F. andFerrarini, M. (1994) ‘‘CD38 signalling by agonistic monoclonalantibody prevents apoptosis of human germinal center B cells’’,European Journal of Immunology, 24, 1218 – 1222.
[31] Gelamn, I., Dettere, P., Gouy, H., Boumsell, L., Debre, P. andBismuth, G. (1994) ‘‘The lymphocyte antigen CD38 acts as anicotinamide adenine dinucleotide glycohydrolase in human Tlymphocytes’’, European Journal of Immunology, 23, 3361 – 3364.
[32] Malavasi, F., Funaro, A., Roggero, S., Horenstein, A., Calosso, L.and Mehta, K. (1994) ‘‘Human CD38: a glycoprotein in search of afunction’’, Immunology Today, 15, 95 – 97.
[33] Oertel, J., Oertel, B., Schliecher, J., Schleicher, J. and Huhn, D.(1996) ‘‘Immunophenotyping of blasts in human bone marrow’’,Annals in Hematology, 72, 125 – 129.
[34] Pascual, V., Liu, Y.J., Magalski, A., de Bouteiller, O., Banchereau,J. and Capra, J.D. (1994) ‘‘Analysis of somatic mutation in five Bcell subsets of human tonsil’’, Journal Experimental Medicine, 180,329 – 333.
[35] Omede, P., Boccadoro, M., Gallone, G., Frieri, R., Battaglio, S.,Redoglia, V., et al. (1990) ‘‘Multiple myeloma: increased circulatinglymphocytes carrying plasma cell-associated antigens as an indi-cator of poor prognosis’’, Blood, 76, 1375 – 1379.
[36] Keyhani, A., Huh, Y.O. and Jendiroba, D. (1999) ‘‘Increased CD38expression is associated with favourable prognosis in adult acuteleukemia’’, Leukemia Research, 24, 153 – 159.
[37] Damle, R.N., Wasil, T., Fais, F., Ghiotto, F., Valetto, A., Allen,S.L., et al. (1999) ‘‘Ig V gene mutation status and CD38 expressionas novel prognostic indicators in chronic lymphocytic leukemia’’,Blood, 94, 1840 – 1847.
[38] Hamblin, T.J., Davis, Z., Gardiner, A., Oscier, D.G. and Stevenson,F.K. (1999) ‘‘Unmutated Ig VH genes are associated with a moreaggressive form of chronic lymphocytic leukemia’’, Blood, 94,1848 – 1854.
[39] Lin, K., Sherrington, P.D., Dennis, M., Matrai, Z., Cawley, J.C.and Pettitt, A.R. (2002) ‘‘Relationship between p53 dysfunction,CD38 expression and IgVH mutation in chronic lymphocyticleukemia’’, Blood, 100, 1404 – 1409.
[40] Oscier, D.G., Gardiner, A.C., Mould, S.J., Glide, S., Davis, Z.A.,Ibbotson, R.E., et al. (2002) ‘‘Multivariate analysis of prognosticfactors in CLL: clinical stage, IGVH gene mutational status, andloss or mutation of the p53 gene are independent prognosticfactors’’, Blood, 100, 1177 – 1184.
[41] Hamblin, T.J., Orchard, J.A., Ibbotson, R.E., Davis, Z., Thomas,P.W., Stevenson, F.K., et al. (2002) ‘‘CD38 expression andimmunoglobulin variable region mutations are independent prog-nostic variables in chronic lymphocytic leukemia, but CD38expression may vary during the course of the disease’’, Blood, 99,1023 – 1029.
[42] Jelinek, D.F., Tschumper, R.C., Geyer, S.M., Bone, N.D., Dewald,G.W., Hanson, C.A., et al. (2001) ‘‘Analysis of clonal B-cell CD38and immunoglobulin variable region sequence status in relation toclinical outcome for B-chronic lymphocytic leukaemia’’, BritishJournal of Haematology, 115, 854 – 861.
[43] Krober, A., Seiler, T.l., Benner, A., Bullinger, L., Bruckle, E.,Lichter, P., et al. (2002) ‘‘VH mutation status, CD38 expressionlevel, genomic aberrations, and survival in chronic lymphocyticleukemia’’, Blood, 100, 1410 – 1416.
[44] Maloum, K., Davi, F., Merle-Beral, H., Pritisch, O., Magnac, C.,Vuillier, F., et al. (2000) ‘‘Expression of unmutated VH genes is adetrimental prognostic factor in chronic lymphocytic leukemia’’,Blood, 96, 377 – 379.
[45] Ghia, P., Guida, G., Stella, S., Gottardi, D., Geuna, M., Strola, G.,et al. (2003) ‘‘The pattern of CD38 expression defines a distinctsubset of chronic lymphocytic leukemia (CLL) patients at risk ofdisease progression’’, Blood, 101, 1262 – 1269.
[46] Lanham, S., Hamblin, T., Oscier, D., Ibbotson, R., Stevenson, F.and Packham, G. (2003) ‘‘Differential signalling via surface IgM isassociated with VH gene mutational status and CD38 expression inchronic lymphocytic leukemia’’, Blood, 101, 1087 – 1093.
[47] Thurnberg, U., Johnson, A., Roos, G., Thom, I., Tobin, G.,Sallstrom, J., et al. (2001) ‘‘CD38 expression is a poor predictor forVH gene mutational status and prognosis in chronic lymphocyticleukemia’’, Blood, 97, 1892 – 1893.
461PROGNOSTIC VALUE OF CD38 EXPRESSION
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.

[48] Matrai, Z., Lin, K., Dennis, M., Sherrington, P., Zuzel, M., Pettitt,A.R., et al. (2001) ‘‘CD38 expression and VH gene mutation in B-cell chronic lymphocytic leukemia’’, Blood, 97, 1901 – 1902.
[49] Vilpo, J., Tobin, G., Hulkkonen, J., Hurme, M., Thunberg, U.,Sundstrom, C., et al. (2003) ‘‘Surface antigen expression andcorrelation with variable heavy-chain gene mutation status inchronic lymphocytic leukemia’’, European Journal of Haematology,70, 53 – 59.
[50] Del Poeta, G., Maurillo, L., Venditti, A., Buccisano, F., Epiceno,A.M., Capelli, G., et al. (2001) ‘‘Clinical significance of CD38expression in chronic lymphocytic leukemia’’, Blood, 98, 2633 –2639.
[51] Mainou-Fowler, T., Dignum, H., Taylor, P.R.A., Dickinson, A.,Saunders, P.W.G., Proctor, S.J., et al. (2002) ‘‘Quantificationimproves the prognostic value of CD38 expression in B-cell chroniclymphocytic leukaemia’’, British Journal of Haematology, 118, 755 –761.
[52] Ibrahim, S., Keating, M., Do, K.A., O’Brien, S., Huh, Y.O., Jilani,I., et al. (2001) ‘‘CD38 expression as an important prognostic factorin B-cell chronic lymphocytic leukemia’’, Blood, 98, 181 – 186.
[53] Chevallier, P., Penther, D., Avet-Loiseau, H., Robillard, N., Ifrah,N., Mahe, B., et al. (2002) ‘‘CD38 expression and secondary 17pdeletion are important prognostic factors in chronic lymphocyticleukaemia’’, British Journal of Haematology, 116, 142 – 150.
[54] D’Arena, G., Musto, P., Cascavilla, N., Dell’Olio, M., Di Renzo,N., Perla, G., et al. (2001) ‘‘CD38 expression correlates with adversebiological features and predicts poor clinical outcome in B-cellchronic lymphocytic leukaemia’’, Leukemia and Lymphoma, 42,109 – 114.
[55] Domingo-Domenech, E., Domingo-Claros, A., Gonzalez-Barca, E.,Beneitez, D., Alonso, E., Romagosa, V., et al. (2002) ‘‘CD38expression in B-cell chronic lymphocytic leukemia: association withclinical presentation and outcome in 155 patients’’, Haematologica,87, 1021 – 1027.
[56] Durig, J., Naschar, M., Schmucker, U., Renzing-Kohler, K.,Holter, T., Huttmann, A., et al. (2002) ‘‘CD38 expression is animportant prognostic marker in chronic lymphocytic leukemia’’,Leukemia, 16, 30 – 35.
[57] Morabito, F., Mangiola, M., Oliva, B., Stelitano, C., Callea, V.,Deaglio, S., et al. (2001) ‘‘Peripheral blood CD38 expressionpredicts survival in B-cell chronic lymphocytic leukemia’’, LeukemiaResearch, 25, 927 – 932.
[58] Morabito, F., Mangiola, M., Stelitano, C., Deaglio, S., Callea, V.and Malavasi, F. (2002) ‘‘Peripheral blood CD38 expression predictstime to progression in B-cell chronic lymphocytic leukaemia afterfirst-line therapy with high-dose chlorambucil’’, Haematologica, 87,217 – 218.
[59] Benet, I., Terol, M.J., Marugan, I., Martinez-Climent, J.A.,Sarsotti, E., Ivars, C., et al. (2000) ‘‘CD38 expression definesclinical and biological characteristics in B-CLL’’, American Societyof Hematology Annual Meeting, Blood, 96, 1600a.
[60] Ibrahim, S., Jilani, I., O’Brien, S., Rogers, A., Manshouri, T., Giles,F., et al. (2003) ‘‘Clinical relevance of the expression of the CD31ligand for CD38 in patients with B-cell chronic lymphocyticleukemia’’, American Cancer Society, 97, 1914 – 1919.
[61] Heintel, D., Schwarzinger, I., Chizzali-Bonfadin, C., Thalhammer,R., Schwarzmeier, J., Fritzer-Szekeres, M., et al. (2001) ‘‘Associa-tion of CD38 antigen expression with other prognostic parametersin early stages of chronic lymphocytic leukemia’’, Leukemia andLymphoma, 42, 1315 – 1321.
[62] Guarini, A., Gaidano, G., Mauro, F.R., Capello, D., Mancini, F.,De Propris, M.S., et al. (2003) ‘‘Chronic lymphocytic leukemiapatients with highly stable and indolent disease show distinctivephenotypic and genotypic features’’, Blood, 102, 1035 – 1041.
[63] Chang, C.-C. and Cleveland, R. (2002) ‘‘Conversion of CD38 and/or myeloid-associated marker expression status during the course ofB-CLL: association with a change to an aggressive clinical course’’,Blood, 100, 1106.
[64] Gratama, J.W., D’hautcourt, J.L., Mandy, F., Rothe, G., Barnett,D., Janossy, G., et al. (1998) ‘‘Flow cytometric quantification ofimmunofluorescence intensity: problems and perspectives’’. Eur-opean Working Group on Clinical Cell Analysis, Cytometry, 33,166 – 178.
[65] Hultin, L.E., Matud, J.L. and Giorgi, J.V. (1998) ‘‘Quantification ofCD38 activation antigen expression in CD8+ T cells in HIV-1infection using CD4 expression on CD4+ T lymphocytes as abiological calibrator’’, Cytometry, 33, 123 – 132.
[66] Schwartz, A., Marti, G.E., Poon, R., Gratama, J.W. andFernandez-Repollet, E. (1998) ‘‘Standardazing flow cytometry: aclassification system of fluorescence standards used for flowcytometry’’, Cytometry, 33, 106 – 114.
[67] Barnett, D., Storie, I., Granger, V., Whitby, L., Reilly, J.T., Brough,S., et al. (2000) ‘‘Standardization of lymphocyte antibody bindingcapacity-amulti-centre study’’,Clinical andLaboratoryHaematology,22, 89 – 96.
[68] Hsi, E.D., Kopecky, K.J., Appelbaum, F.R., Boldt, D., Frey, T.,Loftus, M., et al. (2003) ‘‘Prognostic significance of CD38 andCD20 expression as assessed by quantitative flow cytometry inchronic lymphocytic leukaemia’’, British Journal of Haematology,120, 1017 – 1025.
[69] Mainou-Fowler, T., Proctor, S.J., Miller, S. and Dickinson, A.M.(2001) ‘‘Expression and production of interleukin 4 in B-cell chroniclymphocytic leukemia’’, Leukemia and Lymphoma, 42, 689 – 698.
[70] Rosenwald, A., Alizadeh, A.A., Widhopf, G., Simon, R., Davis,R.E., Yu, X., et al. (2001) ‘‘Relation of gene expression phenotypeto immunoglobulin mutation genotype in B cell chronic lymphocyticleukemia’’, Journal of Experimental Medicine, 194, 1639 – 1648.
[71] Wiestner, A., Rosenwald, A., Barry, T.S., Wright, G., Davis, R.E.,Henrickson, S.E., et al. (2003) ‘‘ZAP-70 expression identifies achronic lymphocytic leukemia subtype with unmutated immunoglo-bulin genes, inferior clinical outcome, and distinct gene expressionprofile’’, Blood, 101, 4944 – 4951.
[72] Crespo, M., Bosch, F., Villamor, N., Bellosillo, B., Colomer, D.,Rozman, M., et al. (2003) ‘‘ZAP-70 expression as a surrogate forimmunoglobulin-variable region mutations in chronic lymphocyticleukemia’’, New England Journal of Medicine, 348, 1764 – 1775.
[73] Chen, L., Widhopf, G., Huynh, L., Rassenti, L., Rai, K.R., Weiss,A., et al. (2002) ‘‘Expression of ZAP-70 is associated with increasedB cell receptor signalling in chronic lymphocytic leukemia’’, Blood,100, 4609 – 4514.
[74] Orchard, J.A., Ibbotson, R.E., Davis, Z.A., Gardiner, A., Hamblin,T.J. and Oscier, D.G. (2002) ‘‘Zap-70 Evaluation by flow cytometryis a significant prognostic marker in B-CLL, American Society ofHematology Annual Meeting’’, Blood, 100, 168a.
462 T. MAINOU-FOWLER et al.
Leu
k L
ymph
oma
Dow
nloa
ded
from
info
rmah
ealth
care
.com
by
Uni
vers
ity o
f U
lste
r at
Jor
dans
tow
n on
11/
13/1
4Fo
r pe
rson
al u
se o
nly.