Embed Size (px)
Citation preview

THE PSYCHIATRIC MEDICAL HISTORY
Prof. Paz
García-Portilla

MEDICAL HISTORY (HX)
• Clinical data set gained by a physician by asking specific questions to the patient (or proxy), with the aim of obtaining information useful in formulating a diagnosis and providing medical care to the patient

MEDICAL HISTORY
• The information obtained in this way, together with the physical examination and additional evaluations, if needed, enables the physician to form a diagnosis, prognosis, and treatment plan
• Clinical reasoning based on facts elicited from symptoms and signs in the history-taking and examination has to be tested against basic scientific background and knowledge acquired during medical training

PSYCHIATRIC MEDICAL HISTORY
• A psychiatric history is frequently lengthy and in depth, as many details about the patient's life are relevant to formulating a management plan for a psychiatric illness.
• Mainly symptoms-based

HISTORY-TAKING IN PSYCHIATRY
• Based in the clinical interview
1. Initiation of a therapeutic alliance
2. Diagnotic data collection
3. Understand the views of the patients
4. Share the information
5. Reach agreements
6. Close the interview

HISTORY-TAKING PROCESS: 2. DIAGNOSTICDATA COLLECTION
• Identification and demographics of the patient
• Chief complaint (CC)
• History of the present complaint (HPC)
• Somatic history
• Substance use history
• Previous psychiatric history
• Family psychiatric history

HISTORY-TAKING PROCESS: 2. DIAGNOSTICDATA COLLECTION
• Psychopathological examination
Systematic questioning about the symptoms of the
psychiatric conditions
Observed behavior
Cognitive abilities
Inner experiences

COMPONENTS OF THE PSYCHOPATHOLOGICALEXAMINATION
• ABC STAMP LICKER
Appearance
Behavior
Cooperation
Speech
Thought – Form & Content
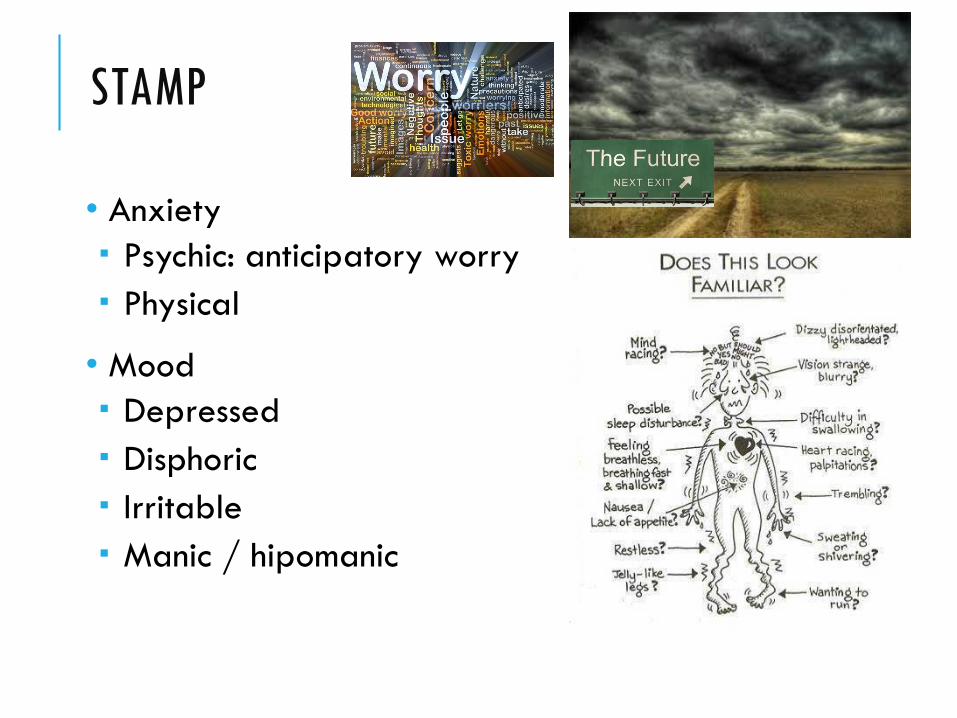
Anxiety
Mood
Perception
• ABC STAMP LICKER
Level of consciousness
Insight
Cognitive functioning
Orientation
Memory
Attention & Concentration
Abstract thinking
PsyKophisiology
Endings – suicidal or homicidal ideation
Reliability of informationModified from: Robinson DJ. Brain Calipers. 1997

ABC
• Appearance
• Behavior
Psychomotor
Restlesness
Agitation
Inhibition
Repetitive behaviors
Extrapiramidal Sx (EPS)
Social
……….
• Cooperation with the interview

STAMP
• Speech
Amount
Increased: loquacious, talkative, logorrhea, pressureof speech, …
Decreased: paucity of speech, impoverished, laconic, minimally responsive, mutism, …
Prosody (nonverbal communication)
Intonation, spontaneity/latency, rhythm, inflection
Mutism Pressure
of speech

STAMP
•Thought
Form: circumstantiality1, tangentiality2, flight of ideas3, loose associations4, thought derailment5 / blocking6, word salad7, incoherence, …..
1
2
35
4
6
7

STAMP
• Thought
Content: overvalued ideas, delusions, obsessions, homicidal / suicidal ideas
STAMP
• Anxiety
Psychic: anticipatory worry
Physical
• Mood
Depressed
Disphoric
Irritable
Manic / hipomanic

STAMP
• Perception
Hallucinations
Ilusions
Disturbances of self and environment
Depersonalization
Desrealization

LICKER
• Level of consciousness
• Insight
• Cognitive functioning
Orientation
Memory
Attention & Concentration
Abstract thinking
? ?

LICKER
• PsyKophysiology
Sleep-Wake
Feeding and eating
Sexual functioning
Gender identity
LICKER
• Endings – suicidal or homicidal ideation
• Reliability of information
?

• Demographics
• Medical Hx
• Psychiatric Hx
• Family psychiatric
Hx
• Psysical
examination
• Additional
investigations
(if needed)
Psychopathological
examination
DiagnosisProvisional + Differential dx
Treatment plan
Prognosis
• Additional investigations
Vital signs and Anthropometry
Lab analysis
EEG, EKG
Neuroimaging: CT scan, MRI, PET, SPECT
Psychometric evaluation

HISTORY-TAKING PROCESS: 3. UNDERSTANDTHE VIEWS OF THE PATIENTS
• Determine, acknowledge and appropriately explore
the patient’s
Ideas and concerns
Expectations
How each problem affects the patient’s life
• Encourage expression of the patient’s feelings
CLINICAL INTERVIEW: BASIC SKILLS
• It is not a conversation, but an active period of questioning and observation
• Be alert! Pursue suggestions and insinuations
• Display a neutral, calm, and objective/nonjudgmental manner
• Understand patients and empathize with them. Show an attitude of acceptance
• Be flexible, adjust your tone, vocabulary and type of questions to suit the patient
• At regular intervals, check your understanding of patient’s problems with them