Embed Size (px)
Citation preview

Volume 2 • Issue 5 • 1000150J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Nik Rosmawati et al., J Community Med Health Educ 2012, 2:5 DOI: 10.4172/2161-0711.1000150
Research Article Open Access
The Rate and Risk Factors for Anemia among Pregnant Mothers in Jerteh Terengganu, MalaysiaNH Nik Rosmawati1*, S Mohd Nazri2 and I Mohd Ismail3
1Environmental Health Unit, Department of Community Medicine, School of Medical Science, Health Campus, Universiti Sains Malaysia, Kelantan, Malaysia2Occupational Health unit, Department of Community Medicine, School of Medical Science, Health Campus, Universiti Sains Malaysia, Kelantan, Malaysia3Health System Management Unit, Department of Community Medicine, School of Medical Science, Health Campus, Universiti Sains Malaysia, Kelantan, Malaysia
AbstractBackground: Antenatal mothers with anemia are high risk to varieties of health implications as well
as to their off springs. Many studies show a high mortality and morbidity related to anemia in pregnancy. Methods: This cross-sectional study was designed to determine factors associated with anemia amongst forty seven antenatal mothers attending Antenatal Clinic at Klinik Kesihatan Kuala Besut, Terengganu in November 2009. Systematic random sampling was applied and information gathered based on patients’ medical records and through face-to-face interviewed by using a structured questionnaire.
Results: The mean age of respondents was 28.3 year-old. More than half of mothers were multigravidas. Of 47 respondents, 57.4% (95% CI: 43.0, 72.0) was anemic. The proportion of anemia was high for grand multigravidas mother (66.7%), those at third trimester of pregnancy (70.4%), did antenatal booking at first trimester (65.4%), poor haematinic compliance (76.5%), not taking any medication (60.5%), those with no co-morbid illnesses (60.0%), mothers with high education level (71.4%) and those with satisfactory monthly income (61.5%). The proportion of anemia was 58.3% and 57.1% for mothers with last child birth spacing of two years or less and more than two years accordingly. There was a significant association of haematinic compliance with the anemia (OR: 4.571; 95% CI: 1.068, 19.573).
Conclusions: Antenatal mothers in this area have a substantial proportion of anemia despite of freely and routinely prescription of haematinic at primary health care centers. Poor haematinic compliance was a significant risk factor. Health education programs regarding haematinic compliance and adequate intake of iron rich diet during pregnancy need to be strengthened to curb this problem.
*Corresponding author: NH Nik Rosmawati, Environmental Health Unit, Department of Community Medicine, School of Medical Science, Health Campus, Universiti Sains Malaysia, 16150 Kubang Kerian, Kelantan, Malaysia, E-mail: [email protected]
Received May 03, 2012; Accepted May 24, 2012; Published May 26, 2012
Citation: Nik Rosmawati NH, Mohd Nazri S, Mohd Ismail I (2012) The Rate and Risk Factors for Anemia among Pregnant Mothers in Jerteh Terengganu, Malaysia. J Community Med Health Educ 2:150. doi:10.4172/2161-0711.1000150
Copyright: © 2012 Nik Rosmawati NH, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords: Anemia; Risk factors; Pregnancy; Rate
IntroductionAnemia in pregnancy constitutes a major public health problem
in developing countries and a high morbidity and morbidity among antenatal mothers [1-3]. The average mortality attributed by anemia in Asia is estimated as 7.26% [4]. Most of anemias in pregnancy are due to iron deficiency [2]. It has been known contributes a risk to the fetus for preterm delivery, subsequent low birth weight, and inferior neonatal health [3,5].
Anemia amongst antenatal mothers is a worldwide health problem. Its prevalence in Africa was 57.1 % (95 % CI 52.8–61.3), South-East Asia was 48.2 % (95 % CI 43.9–52), Europe was 25.1 % (95 % CI 8.6–31.6), Western Pacific was 30.7 (95% CI 18.6–3) and 41.8% (95 % CI 39.9–43.8) worldwide for the year 1993 to 2005 affecting 56 million pregnant women [2]. In Malaysia, the prevalence was 35% and mostly of the mild type and more prevalent in the Indian and Malays communities [6].
World Health Organization (WHO) has categorized and emphasized on the significant health consequences based on the prevalence of the anemia. If the prevalence of anemia is 4.9% or less, it is considered as no public health problem for that country. The prevalence of anemia between 5.0% and 19.9% indicates a mild public health problem. Moderate public health problem is been considered when the prevalence is between 20.0% and 39.9%. If the prevalence is 40.0% or more, it is considered as severe public health problem [2].
Many studies explained the status of anemia in antenatal mothers was depend on the socioeconomic level [1,7], illiteracy, extremes of mother’s age, primigravida or grandgravida, short pregnancy intervals [7,8] and age of gestation [6,8]. In measuring the status of anemia in the population, hemoglobin (Hb) concentration is the most reliable indicator as opposed to clinical measures. Furthermore, it is cheaper and relatively easy to perform [2].
So far, only a few studies (6.7%; 8 out of 120 published and unpublished data) [9], has been done throughout Malaysia concerning this problem. Due to a significant risk for health of the mother as well as the fetus therefore, it is importance to carry out a study to determine the prevalence and factors associated with anemia amongst the most vulnerable group, antenatal mothers attending Antenatal Clinic at primary health care. Then, the magnitude of the problem and its epidemiology can be established. On top of that, this problem is easily preventable and treatable.
Operational definitions
The Hb thresholds used to define anemia in this study was based on WHO definition. Anemia is refer to the Hb concentration of less than 11 g/dL and non-anemia is refer to Hb concentration of 11 g/dL or more [2]. The level of educational status of respondents was grouped into low (refer to those with no education and those with education up to primary school), intermediate (refer to those with secondary school) and high (refer to those with tertiary education). Respondents who followed the haematinics prescription by health staffs were considered as good haematinics compliance.
Jour
nal o
f Com
munity Medicine & Health Education
ISSN: 2161-0711
Community Medicine & Health Education

Volume 2 • Issue 5 • 1000150J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Citation: Nik Rosmawati NH, Mohd Nazri S, Mohd Ismail I (2012) The Rate and Risk Factors for Anemia among Pregnant Mothers in Jerteh Terengganu, Malaysia. J Community Med Health Educ 2:150. doi:10.4172/2161-0711.1000150
Page 2 of 4
Monthly income was categorized into 3 levels. Poor income refer to those with income less than RM 720 (based on the poverty line index for West Malaysia in 9th Malaysia), satisfactory constituted of those with monthly income RM 720 to RM 1999 and good for those between RM 2000.00 and RM 4000. Respondents with known medical illnesses (including hypertension, diabetes, thallessemia, kidney, systemic lupus erythematous, others) are classified as having co-morbidities.
Patients and MethodStudy design and selection of participants
A cross-sectional study was conducted in November 2009 at Klinik Kesihatan Kuala Besut Terengganu, located about 60 km from Kota Bharu, a city of Kelantan or 150 km from Kuala Terengganu, a city of Terengganu. A Systematic random sampling was applied to antenatal mothers attending the clinic within study period (29th October to 26th November 2009) and excluding those with mental handicaps or in severe health conditions. The total numbers of antenatal mothers involved in this study was 47 respondents and the response rate was 100%.
Research instruments
Data collection was carried out by using a structured study questionnaire. The questionnaire consisted of socio-demography information (including age, education level and monthly income) and elicited risk factors (including parity, spacing with last child birth, haematinics compliance, time of antenatal booking, taking other medications and the presence of co morbidity problems. This questionnaire was constructed through series of discussions with experts and underwent face validity. Due to limited time, validity and reliability test was not done. The hemoglobin level was based on the current available results tested using the hemoglobinometer analysis of the blood samples drawn from either capillary or venous blood. All these information was gathered through face-to-face interviewed and from patients’ medical records. The average time taken for each interview session was fifteen minutes.
Statistical analysis
Data gathered were input into SPSS version 12.0 and analyzed using same software. Continuous variables were described as mean and standard deviation whereas, categorical variables were expressed by frequency and percentage. Simple logistic regression and multiple logistic regressions were used to determine the significant factors associated with hemoglobin levels. A p-value of less than 0.05 was judged to be statistically significant.
ResultsOf 47 respondents, 57.4% was anemic (95% CI: 43.0, 72.0). The
mean age of respondents was 28.3 year-old. More than half of the mothers were multigravidas and the least was grandmultigravidas. Nearly three-quarter had more than 2 years last child birth spacing and more than half were at third trimester, did antenatal booking at first trimester of pregnancy and good haematinics compliance. More than 80% of respondents did not take any other medications during pregnancy. Majority of antenatal mothers have no co-morbidity illnesses and their level of education were at intermediate level. About 46% of mothers had poor monthly income as shown in Table 1.
The rate of anemia was high for grandmultigravidas mother, those at the third trimester of pregnancy, did antenatal booking at first trimester, poor haematinic compliance, and did not taking any
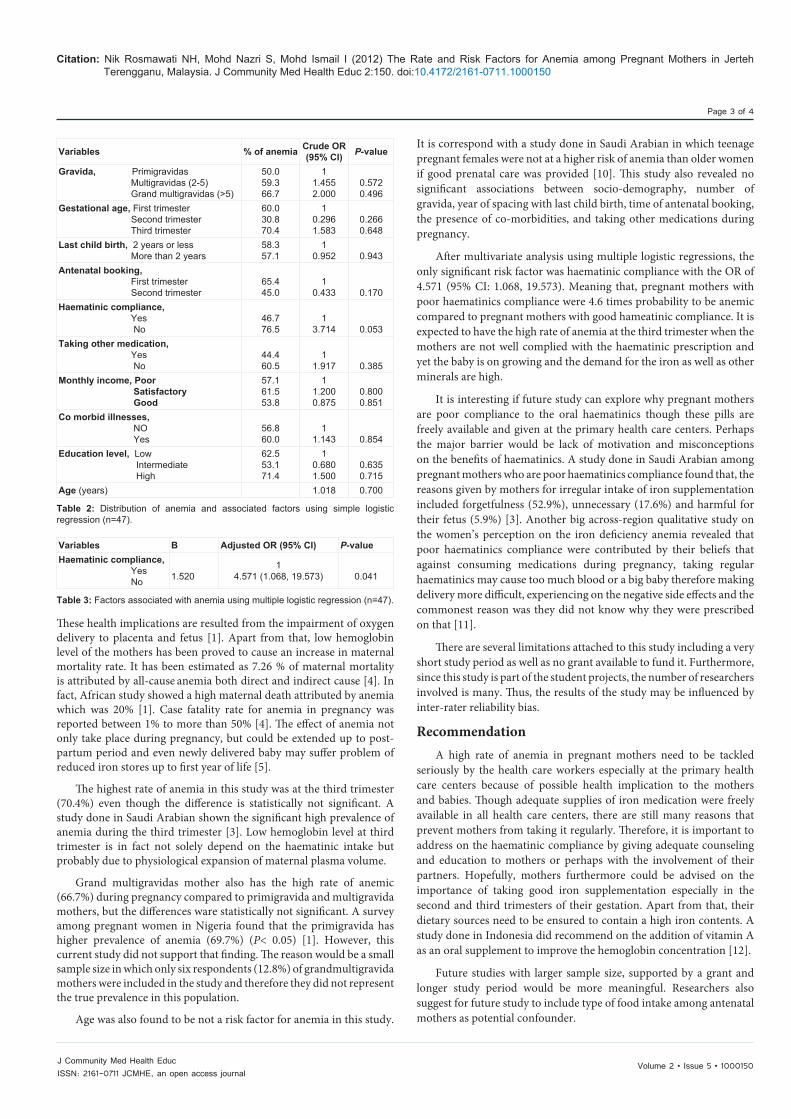
medication, those with no co-morbid illnesses, mothers with high education level and satisfactory monthly income. The proportion of anemia was 58.3% and 57.1% for mothers with last child birth spacing of two years or less and more than two years accordingly. Simple logistic regression revealed no significant different for the socio-demography and studied factors with the rate of anemia amongst antenatal mothers as illustrated in Table 2.
Table 3 shows the result of multiple logistic regressions. There was a significant association of haematinic compliance with the anemia among the respondents with the OR of 4.571 and 95% CI between 1.068 and 19.573.
DiscussionAn overall prevalence rate of anemia in pregnancy mothers in this
study was 57.4% (95% CI: 43.0, 72.0). This level is substantially high compared to previous study done in Kelantan where the prevalence was 47.5% [8]. The prevalence of anemia in Malaysia was 35% which is much lower than this study [6]. Other countries did show a lower prevalence of anemia such as 41.3% in Saudi Arabia [3], 48.2% in South-East Asia [2] and 41.8% worldwide [2]. However, the prevalence of anemia in developing countries such as Nigeria was higher, 76.5% [1]. The rate of anemia for pregnant mothers in this study is approaching to WHO estimation for developing countries and far behind from economically developed countries such as in Europe, where their prevalence was 25.1% [2]. This high figure is surprising considering the routine practice at all primary health care centers to provide pregnant women with prophylactic elemental iron. This reflects a poor nutritional health of antenatal mothers in this country.
Anemic state of mothers may predispose themselves as well as their off springs to several unwanted health outcomes such as preterm deliveries, low birth weight and prenatal mortality conditions [3].
Variable Frequency Percentage 95 % CIAnaemia, Yes No
2720
57.442.6
43.0, 72.0
Gravida, Primigravidas Multigravidas (2-5) Grand multigravidas (>5)
14276
29.857.412.8
Gestational age, First trimester Second trimester Third trimester
51327
10.627.757.4
Last child birth, 2 years or less More than 2 years
1235
25.574.5
Antenatal booking, First trimester Second trimester
2620
55.342.6
Haematinic compliance, Yes No
3017
63.836.2
Taking other medication, Yes No
938
19.180.1
Monthly income, Poor Satisfactory Good
211313
44.727.727.7
Co morbid illnesses, NO Yes
3710
78.721.3
Education level, Low Intermediate High
8327
17.068.114.9
Age (years) ‡28.3 (6.48)‡ Mean (sd)
Table 1: Descriptive profile among antenatal mothers (n= 47).
Volume 2 • Issue 5 • 1000150J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Citation: Nik Rosmawati NH, Mohd Nazri S, Mohd Ismail I (2012) The Rate and Risk Factors for Anemia among Pregnant Mothers in Jerteh Terengganu, Malaysia. J Community Med Health Educ 2:150. doi:10.4172/2161-0711.1000150
Page 3 of 4
These health implications are resulted from the impairment of oxygen delivery to placenta and fetus [1]. Apart from that, low hemoglobin level of the mothers has been proved to cause an increase in maternal mortality rate. It has been estimated as 7.26 % of maternal mortality is attributed by all-cause anemia both direct and indirect cause [4]. In fact, African study showed a high maternal death attributed by anemia which was 20% [1]. Case fatality rate for anemia in pregnancy was reported between 1% to more than 50% [4]. The effect of anemia not only take place during pregnancy, but could be extended up to post-partum period and even newly delivered baby may suffer problem of reduced iron stores up to first year of life [5].
The highest rate of anemia in this study was at the third trimester (70.4%) even though the difference is statistically not significant. A study done in Saudi Arabian shown the significant high prevalence of anemia during the third trimester [3]. Low hemoglobin level at third trimester is in fact not solely depend on the haematinic intake but probably due to physiological expansion of maternal plasma volume.
Grand multigravidas mother also has the high rate of anemic (66.7%) during pregnancy compared to primigravida and multigravida mothers, but the differences ware statistically not significant. A survey among pregnant women in Nigeria found that the primigravida has higher prevalence of anemia (69.7%) (P< 0.05) [1]. However, this current study did not support that finding. The reason would be a small sample size in which only six respondents (12.8%) of grandmultigravida mothers were included in the study and therefore they did not represent the true prevalence in this population.
Age was also found to be not a risk factor for anemia in this study.
It is correspond with a study done in Saudi Arabian in which teenage pregnant females were not at a higher risk of anemia than older women if good prenatal care was provided [10]. This study also revealed no significant associations between socio-demography, number of gravida, year of spacing with last child birth, time of antenatal booking, the presence of co-morbidities, and taking other medications during pregnancy.
After multivariate analysis using multiple logistic regressions, the only significant risk factor was haematinic compliance with the OR of 4.571 (95% CI: 1.068, 19.573). Meaning that, pregnant mothers with poor haematinics compliance were 4.6 times probability to be anemic compared to pregnant mothers with good hameatinic compliance. It is expected to have the high rate of anemia at the third trimester when the mothers are not well complied with the haematinic prescription and yet the baby is on growing and the demand for the iron as well as other minerals are high.
It is interesting if future study can explore why pregnant mothers are poor compliance to the oral haematinics though these pills are freely available and given at the primary health care centers. Perhaps the major barrier would be lack of motivation and misconceptions on the benefits of haematinics. A study done in Saudi Arabian among pregnant mothers who are poor haematinics compliance found that, the reasons given by mothers for irregular intake of iron supplementation included forgetfulness (52.9%), unnecessary (17.6%) and harmful for their fetus (5.9%) [3]. Another big across-region qualitative study on the women’s perception on the iron deficiency anemia revealed that poor haematinics compliance were contributed by their beliefs that against consuming medications during pregnancy, taking regular haematinics may cause too much blood or a big baby therefore making delivery more difficult, experiencing on the negative side effects and the commonest reason was they did not know why they were prescribed on that [11].
There are several limitations attached to this study including a very short study period as well as no grant available to fund it. Furthermore, since this study is part of the student projects, the number of researchers involved is many. Thus, the results of the study may be influenced by inter-rater reliability bias.
RecommendationA high rate of anemia in pregnant mothers need to be tackled
seriously by the health care workers especially at the primary health care centers because of possible health implication to the mothers and babies. Though adequate supplies of iron medication were freely available in all health care centers, there are still many reasons that prevent mothers from taking it regularly. Therefore, it is important to address on the haematinic compliance by giving adequate counseling and education to mothers or perhaps with the involvement of their partners. Hopefully, mothers furthermore could be advised on the importance of taking good iron supplementation especially in the second and third trimesters of their gestation. Apart from that, their dietary sources need to be ensured to contain a high iron contents. A study done in Indonesia did recommend on the addition of vitamin A as an oral supplement to improve the hemoglobin concentration [12].
Future studies with larger sample size, supported by a grant and longer study period would be more meaningful. Researchers also suggest for future study to include type of food intake among antenatal mothers as potential confounder.
Variables % of anemia Crude OR (95% CI) P-value
Gravida, Primigravidas Multigravidas (2-5) Grand multigravidas (>5)
50.059.366.7
11.4552.000
0.5720.496
Gestational age, First trimester Second trimester Third trimester
60.030.870.4
10.2961.583
0.2660.648
Last child birth, 2 years or less More than 2 years
58.357.1
10.952 0.943
Antenatal booking, First trimester Second trimester
65.445.0
10.433 0.170
Haematinic compliance, Yes No
46.776.5
13.714 0.053
Taking other medication, Yes No
44.460.5
11.917 0.385
Monthly income, Poor Satisfactory Good
57.161.553.8
11.2000.875
0.8000.851
Co morbid illnesses, NO Yes
56.860.0
11.143 0.854
Education level, Low Intermediate High
62.553.171.4
10.6801.500
0.6350.715
Age (years) 1.018 0.700
Table 2: Distribution of anemia and associated factors using simple logistic regression (n=47).
Variables B Adjusted OR (95% CI) P-valueHaematinic compliance, Yes No 1.520
14.571 (1.068, 19.573) 0.041
Table 3: Factors associated with anemia using multiple logistic regression (n=47).

Volume 2 • Issue 5 • 1000150J Community Med Health EducISSN: 2161-0711 JCMHE, an open access journal
Citation: Nik Rosmawati NH, Mohd Nazri S, Mohd Ismail I (2012) The Rate and Risk Factors for Anemia among Pregnant Mothers in Jerteh Terengganu, Malaysia. J Community Med Health Educ 2:150. doi:10.4172/2161-0711.1000150
Page 4 of 4
ConclusionOur study showed there was a substantial proportion of anemia
in this population. Despite of freely and routinely prescription of haematinic at primary health care centers, more than half of pregnant women were anemic. Poor compliance on haematinic intake by mothers was significantly associated with anemia by the OR of 4.571 (95% CI: 1.068, 19.573). This information is really valuable to initiate a further exploration to find the root cause of the high rate of anemia among pregnant mothers in our community.
Acknowledgement
The author wishes to thank to all staffs at Kuala Besut Health Clinic and All members in group 5 final year medical students 2009/2010 batch for completing the investigative assignment project during their Preventive Medicine Posting.
References
1. Idowu OA, Mafiana CF, Dapo S (2005) Anaemia in pregnancy: a survey of pregnant women in Abeokuta, Nigeria. Afr Health Sci 5: 295-299.
2. McLean E, Cogswell M, Egli I, Wojdyla D, Benoist Bd (2008)Worldwide prevalence of anaemia, WHO Vitamin and Mineral Nutrition Information System, 1993–2005. Public Health Nutrition 12: 444–454.
3. Rasheed P, Koura MR, Al-Dabal BK, Makki SM (2008) Anemia in pregnancy: A study among attendees of primary health care centers. Ann Saudi Med 28: 449-452.
4. Brabin BJ, Hakimi M, Pelletier D (2001) An analysis of anemia and pregnancy-related maternal mortality. J Nutr 131: 604S-614S.
5. Allen LH (2000) Anemia and iron deficiency: effects on pregnancy outcome. Am J Clin Nutr 71: 1280S-1284S.
6. Haniff J, Das A, Onn LT, Sun CW, Nordin NM, et al. (2007) Anemia in pregnancy in Malaysia: a cross-sectional survey. Asia Pac J Clin Nutr 16: 527-536.
7. Noronha JA, Bhaduri A, Vinod Bhat H, Kamath A (2010) Maternal risk factors and anaemia in pregnancy: A prospective retrospective cohort study. J Obstet Gynaecol 30: 132-136.
8. Ahmad Z, Jaafar R, Mohd Hassan MH, Othman MS, Hashim A (1997) Anaemia during pregnancy in rural Kelantan. Mal J Nutr 3: 83-90.
9. Ming KE, Lieng TC, Jenn NC, Jaafar S (2008) Bibliography of Primary Care Research in Malaysia. Kuala Lumpur: University of Malaya, Malaysia.
10. Mahfouz AA, el-Said MM, al-Erian RA, Hamid AM (1995) Teenage pregnancy: are teenagers a high risk group? Eur J Obstet Gynecol Reprod Biol 59: 17-20.
11. Galloway R, Dusch E, Elder L, Achadi E, Grajeda R, et al. (2002) Women’s perceptions of iron deficiency and anemia prevention and control in eight developing countries. Soc Sci Med 55: 529-544.
12. Muslimatun S, Schmidt MK, Schultink W, West CE, Hautvast JA, et al. (2001) Weekly supplementation with iron and vitamin A during pregnancy increases hemoglobin concentration but decreases serum ferritin concentration in Indonesian pregnant women. J Nutr 131: 85-90.





























