Embed Size (px)
Citation preview

1
Tuberculosis in the world and in
Iraq
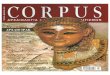
Nearly one third of the global population
i.e. two billion people is infected with
Mycobacterium tuberculosis and at risk of
developing the disease. More than eight
million people develop active Tuberculosis
(TB) every year, and about two million
die. (Figure 1)
More than 90% of global TB cases and
deaths occur in the developing world,
where 75% of cases are in the most
economically productive age group (15-54
years).An adult with TB loses on average
three to four months of work time, which
results in the loss of 20-30% of annual
household income.
Co-infection with human
immunodeficiency virus (HIV) significantly
increases the risk of developing TB.
250,000 deaths due to TB/HIV over the
world occur each year.
The main reasons for the increasing
burden of TB globally are: poverty,
collapse of health infrastructure, weak
national TB control programs and the
impact of HIV.
Iraq is considered to be a middle burden
country with TB, and occupies rank 108
globally and 7 in eastern Mediterranean
region among countries with TB burden
size. According to WHO report, the
estimated incidence of TB in Iraq is
45/100000 population (I.e. estimated
total new TB cases is around 15000 per
year), while the prevalence is
74/100000 and the mortality is
3/100000.
The real magnitude of MDR-TB in Iraq
is unknown as no drug resistance
survey (DRS) was conducted yet .With
reference to the Global TB Control WHO
Report 2009, the percentage of Multi-
Drug Resistance TB (MDR-TB) among new
cases in Iraq is 3%, and among
retreatment cases it is 38%. The
estimated number of MDR among all
cases is 988, and among smears positive
SS+ve cases is 719.
Introduction 1
Figure 1
Estimated TB incident rate 2011
Global tuberculosis report 2012.
Objectives of the curriculum
1. To incorporate national TB-DOTS control Program continuously into medical teaching curriculum as an initiative for comprehensiveness of public health programs in different health sectors.
2. To keep updating medical students in diagnosis, treatment and prevention of TB according to international standards.

2
Tuberculosis 2
What is Tuberculosis (TB)?
TB is a bacterial, infectious disease caused
by Mycobacterium Tuberculosis complex
(Human, Bovis and Africana), these
organisms are also known as tubercle
bacilli (because they cause lesion called
tubercle) or acid fast bacilli (AFB) because
it resist the acid decolorization during the
staining process (Figure 2).
TB affects all races all ages & all organs.
Infection occurs almost exclusively
through the respiratory system by
inhalation of tubercle bacilli. The lung is
the main organ affected. Each smear-
positive PTB (pulmonary TB) will transmit
infection to (10 – 15 persons) in year.
Those who will be infected with TB will
not necessarily get the disease; the
immune system "walls off" the TB bacilli,
which can remain dormant for years.
About 5 -10 % of the infected individuals,
have chance of developing TB disease
during their lifetime.
Transmission of Infection?
-Air Borne: When patients with PTB
speak ,and particularly when they cough
or sneeze, they produce an aerosol of
droplets from the bronchial tree, each of
which contains a number of bacilli ,The
number of infectious droplets projected
into atmosphere by a patient is very high
when coughing (3500) or sneezing (1
million).When they come in to contact
with air they rapidly dry and become very
light particles, however, they still
containing live bacilli, that remain
suspended in the air .In enclosed space,
the droplets can remain suspended for
long time, and the bacilli remain alive for
long time in the dark. The closer and more
prolonged the contact with an infectious
patient, the greater the risk of infection,
as this linked to the density of the bacilli
in the air the individual breaths and the
amount of the air inhaled.
-Ingestion: by contaminated un -
pasteurized milk (M. bovis).
-Rare routes of transmission:
cutaneous, trans placental, & transsexual
transmissions.
Incubation period:
Incubation period is 3-8 weeks in primary
TB, and up to years in post primary TB
(Table 1).
Table 1
Timetable of TB
Time from infection Manifestation
3-8 weeks Primary complex, positive tuberculin skin test
3-6 months Meningeal , miliary ,plural disease
Up to 3 years GI,bone and joint, lymph node
Around 8 years Renal tract inf.
From 3 years onwards
Post - primary disease due to reactivation of inf.
Figure 2 Mycobacterium Tuberculosis
Visualization using Ziehl-Neelsen stain.

3
Evolution of infection
1. Primary Tuberculosis:
When a few virulent tubercle bacilli
penetrate the pulmonary alveoli of a
healthy person, they are phagocytosed by
the alveolar macrophages, in which they
multiply. Other macrophages and
monocytes are attracted and Participate
in the process of defense against
infection. The resulting (infectious focus)
made up of inflammatory cells, is referred
to as primary focus. The bacilli and the
antigens that they liberate are drained by
the macrophages through the lymphatic
system to the nearest lymph nodes. Inside
the lymph node, the T lymphocytes
identify the M. tuberculosis antigens and
are transformed in to specific T
lymphocytes, leading to liberation of
lymphokines and activation of
macrophages that inhibit the growth of
the phagocytosed bacilli. The
inflammatory tissue formed in the
primary focus is replaced by fibrous scar
tissue in which the macrophages
containing bacilli are isolated and die. This
primary focus is the site of tuberculosis-
specific caseating necrosis. This focus
contains (1000-10000) bacilli which
gradually lose their viability and multiply
more and more slowly. Some bacilli can
survive for months or years, these are
known as (Latent bacilli) this is indicated
by the development of a delayed-type
hypersensitivity which can be
demonstrated by tuberculin skin test and
this process takes period about 6-8weeks
from the beginning of the infection.
2. Secondary focus: Post primary
Before immunity is established, bacilli
from the primary infectious focus or from
the nearest lymph node are transported
and disseminated throughout the body by
lymph system and then via the blood
stream. Secondary foci containing a
limited number of bacilli are thus
constituted, particularly in the lymph
nodes, serous membranes, meninges,
bones, liver, kidneys and lungs. As soon as
an immune response is mounted most of
these foci spontaneously resolve.
However, a number of bacilli may remain
latent in the secondary foci for months or
even years.
Primary TB is mostly pulmonary and may
be extra- pulmonary e.g. intestinal
primary TB.
80 – 90 % of infected individual's
immunity will take the upper hand,
ending in spontaneous healing, resolution
fibrosis and calcification.
In 10 – 20 % of infected individual
virulence takes the upper hand and may
result in active disease. This results in
primary TB when initial infection causes
the individual to develop clinical disease.
In most instances, even where there are
clinical signs present, immunity will get
the role to play and the disease will
regress spontaneously. Where it does not,
progressive primary TB or disseminated
TB may occur.
When should tuberculosis be
suspected?
The onset of the disease is often
insidious; symptoms often develop slowly,
on several weeks. Chest symptoms are
often nonspecific, cough is almost always
present with sputum production. Possibly
chest pain & or dyspnoea. Less commonly
haemoptysis may occur.
Systemic symptoms: fever in the evening
(on average 38°C) heavy night sweat, loss
of appetite, loss of weight & a general
sense of malaise.

4
Suspected TB patient is any patient have
cough more than 3 weeks not responding
to ordinary treatment (figure 5).

5
Case definition 3
A case of TB is defined as a patient on
whom tuberculosis has been confirmed by
bacteriology or diagnosed by a clinician.
Purpose of case definition
1. Proper patient registration and case
notification. 2. To evaluate the trend in the
proportion of the new smear positive cases & smear positive relapse & other retreatment cases.
3. Commencement of appropriate treatment categories for TB cases & cohort analysis of treatment outcome.
What determines case
definition?
1. Site of TB disease:
TB affects the lungs in more than 80% of
cases & called pulmonary TB. TB can
affects a various organs & called extra
pulmonary TB.
2. Severity of TB disease:
Bacillary load, extent of the disease &
anatomical site is considered in
determining TB disease severity.
3. Bacteriological result of sputum smear examination:
a. Smear positive pulmonary
tuberculosis (PTB)
- Either a patient with at least two
sputum specimens positive for AFB by
microscopy.
- Or patient with one sputum specimen
positive for AFB & radiographic
abnormalities consistent with active
pulmonary TB . Decision by a physician
to treat with a full curative course of anti
TB chemotherapy.
- Or with at least one sputum specimen
positive for AFB with culture positive for
AFB.
- Under programmed conditions when
microscopy lab services are available and
diagnostic criteria are properly applied,
Pulmonary T.B smear positive case
represent at least 65% of the
total(PTB)cases in adults and 50% or more
of all TB cases.
b. Smear negative (PTB):
Either a patient fulfills all the following
criteria.
- Two sets (taken at least 2 weeks apart)
of at least two sputum specimen negative
for AFB.
- Radiographic abnormalities consistent
with active pulmonary TB & a lack of
clinical response despite one week of
broad spectrum antibiotics (except
quinolones).
- A decision by a physician to treat with
full curative course of anti TB
chemotherapy.
Or a patient who fulfills the following
criteria with three specimen of sputum
smear negative for AFB radiographic
abnormalities consistent with active
pulmonary TB and a decision by physician
to treat with full curative course of anti-
TB chemotherapy.
c. Extra – pulmonary TB: Are patients with tuberculosis in organs
other than the lungs (e.g. pleura, lymph
nodes, abdomen, genitourinary tract,
skin, joints and bones, meninges).
Diagnosis should be based on one culture
positive specimen or histological or strong
clinical evidence consistent with active
extra-pulmonary disease, followed by a

6
decision by a clinician to treat with a full
course of anti-TB chemotherapy.
A patient in whom both pulmonary and
extra-pulmonary tuberculosis has been
diagnosed should classify as pulmonary
case.
4. Case classification according to
previous treatment.
On diagnosis, patients are classified for
registration according to previous TB
treatment:
New case: Patient who has never had
treatment for tuberculosis or who has
taken anti TB chemotherapy for less than
4 weeks.
Relapse: patient who has been declared
cured from T.B in the past by a physician
after one full course of chemotherapy &
now has become bacteriologically positive
(at least one smear or culture)
tuberculosis.
Treatment failure: Patient who while on
treatment remained or become again
smear positive 5 months after
commencing treatment. It is also a patient
who was initially smear negative before
starting treatment and become smear
positive after second month of treatment.
Treatment defaulter: patient who does
not take drugs or interrupts treatment for
two months or more & return to the
health services with smear positive
sputum consider as treatment failure or
return with smear negative in this case
continues his treatment but from the
start.
Chronic cases: Patient who remained or
became again smear positive after
completing a fully supervised retreatment
regimen.

7
Diagnosis of TB 4
Diagnosis of pulmonary TB in
adult:
a. If after interview and clinical
examination there is no evidence of
another cardio pulmonary condition in a
patient who presents with cough lasting
for more than 3 weeks pulmonary
tuberculosis should be suspected.
Bacteriological examination of the sputum
must be performed on 3 consecutive
sputum for direct smear examination of
AFB.
b.Certain radiological abnormalities are
consistent with TB:
Nodules: round shadow with clearly
defined borders. (Figure 3).
Patchy shadow: irregular border
infiltration.
Cavities are the most characteristic
sign of TB. (Figure 4 ).
Some radiographic shadow show TB
sequel:
Nodules that are fully or partially
calcified.
Satellite abnormalities.
Fibrosis.
Fine walled bullae /Cavities.
Specific aspects of childhood TB: a. Primary pulmonary TB: Primary
infection is asymptomatic. In (10%) of cases primary infection has clinical manifestation. b. Generalized symptoms. c. Mucocutaneous manifestation (Erythèma Nodosum, Phlyctenular conjonctivites). d. Radiological sign: typical primary complex.
Isolated mediastinal lymphadenopathy
Segmental consolidation associated
with mediastinal lymphadenopathy.
e. History contact to index case.
f. Positive tuberculin skin test.
Figure 4
Upper lobe cavitary lesion
Figure 3 A rounded opacity in the left lung apex. Partially overlapping with the left anterior first rib. This abnormality is consistent with a pulmonary nodule.
Figure 3 A rounded opacity in the left lung apex. Partially overlapping with the left anterior first rib. This abnormality is consistent with a pulmonary nodule.
Figure 3 A rounded opacity in the left lung apex. Partially overlapping with the left anterior first rib. This abnormality is consistent with a pulmonary nodule.

8
Diagnosis of pulmonary TB
Points to be remembered in the diagnosis of pulmonary TB: 1. Over 80% of patients with smear
positive pulmonary T.B have at least one or more respiratory symptoms for more than three weeks.
2. The most frequent respiratory symptom is the cough followed by expectoration. Over 90% of patients with smear positive pulmonary TB develop cough while only 20% of them have haemoptysis.
3. The bacteriological examination of the sputum is the only way in which the diagnosis of pulmonary TB can be confirmed.
4. X- Ray diagnosis of TB is unreliable because other chest disease can look like TB on x- ray.
5. The tuberculin test has a limited value in clinical work in adult but it helps in diagnosis TB in children.
Over 90% with a cavitory pulmonary T.B
or with extensive abnormal infiltration are
smear positive, therefore a patient with
cavitations on chest x ray & repeated
specimen smear for AFB were negative,
probably has a disease other than TB.

9
Management of TB 5
Disciplines in the management of T.B
1. Physician should manage TB cases
without any deviation in combination
of drugs, dosage, duration of
treatment & type of regimen used.
2. Physician demands not only a
detailed knowledge of the drugs
available but also of the most
appropriate regimen for the
individual patient.
3. The available drugs must not be
abused by inadequately trained
doctors.
4. Anti TB chemotherapy is by far the
most important measures in the
treatment of all form of TB and
should be given to every patient with
active disease while surgery plays a
minor role.
5. It is wasteful to treat patients who do
not need it and expose them to the
risk of drug toxicity and to the
domestic penalties as being labeled
tuberculosis.
6. Hospitalization in itself has little or
no effect on the outcome of
treatment. A patient who takes the
drugs regularly will do equally well
whether treatment in or out of the
hospital. However, regular & direct
supervision of patients is of Para
most important.
7. Inpatients treatment is indicated for
severely ill, and for those with
complications of TB (e.g.
haemoptysis, spontaneous
pneumothorax) as for those with
other serious co-existent disease
requiring hospitalization.
8. Pregnant women with TB should
start or continue their treatment for
TB in the same way as other patients;
however, Streptomycin should not be
used because of the risk of toxicity to
the inborn child.
9. The use of Rifampicin or
Streptomycin for diseases other
than mycobacterium diseases
should be avoided or limited to very
carefully considered indication.
10. Anti TB drugs are relatively toxic &
mild side effects are not
uncommon, but in most case no
need for drug withdrawal. Minor
side effects are relatively few
cause, discomfort, they often
respond to symptomatic or simple
treatment. Major side effects are
those giving rise to serious health
hazard & required discontinuation
of the drug & referral to chest
physician.
11. Major (essential) anti TB drugs are:
There are three main properties of
anti TB drugs; bactericidal ability,
sterilizing ability and ability to prevent
resistance.
The essential anti TB drugs possess
these properties to different extent.
Isoniazide (H), Rifampicin (R),
streptomycin (S), Ethambutol (E),
Pyrazinamid (Z), all are able to cure
100% of new T.B cases with sensitive
bacilli. Treatment of T.B is the main
weapon against the fight of the
disease. The bases of TB treatment is
chemotherapy.
Aims of the treatment:
To cure TB patients.
To prevent death.
To prevent relapse.
To decrease transmission to others.
To prevent drug resistance.

10
Figure 5
How to manage a suspected TB patient.
Suspected TB patient
Microscopical
examination of Sputum
for AFB
AFB +ve AFB -ve
Broad spectrum antibiotics
except Quinolones
Improvement No improvement
Repeated AFB
microscopy
AFB -ve AFB +ve
Clinical and radiological
assessment
Not TB TB
Consider other diagnosis Treat as smear –ve
pulmonary TB Treat as smear +ve
pulmonary TB

11
Requirements for adequate
chemotherapy:
1. Good chemotherapy, which is designed to kill mycobacterium & sterilize the body tissues.
2. Prescribed in a correct dosage. 3. Taken regularly by the patients. 4. For a sufficient period of time.
Effects of anti TB chemotherapy:
A good chemotherapy is designed to kill
TB bacilli rapidly, prevent the
development of drug resistance, and
sterilize the host's tissues. The
achievement of these effects requires a
combination of drugs.
Failure of chemotherapy is due to the
irregularity of drugs taking & the high
dropout rate during treatment.
This would be prevented by good health
education, involve whole family in
observing the patients, using special pack
for anti TB drugs & using the latest DOTS
strategy (see p21).
Drug Action:
How do anti tuberculosis drugs work?
(Table 2)
1. Bactericidal action which is defined as
their ability to kill large numbers of
actively metabolizing bacilli rapidly.
2. Sterilizing action- defined as their
capacity to kill special populations of
slowly or intermittently metabolizing semi
dormant bacilli the so called per sisters.
3. Their ability to prevent the emergence
of acquired resistance by suppressing
drug resistant mutants present in all large
bacteria population.
4. Their suitability for intermittent use.
Bactericidal action:
Most of the anti TB drugs with the
exception of Ethambutol have some
bactericidal action but INH is the most
potent bactericidal drug. Rifampcin is also
an important bactericidal drug;
streptomycin and Pyrazinamid are less
potently bactericidal.
Sterilizing action:
Rifampcin and Pyrazinamid are the most
important sterilizing drugs because of
their ability to kill semi dormant bacilli.
The WHO recommended certain
regimens for each patient category:
Category I: Smear positive case or smear
negative severely ill patient or seriously ill
extra pulmonary T.B, e.g. T.B meningitis,
Miliary T.B, T.B pericarditis& T.B peritonitis.
New cases that are not treated previously as
pulmonary TB or serious extra pulmonary T.B
(meningitis). First line standard regimen (2HRZ
E or (S) +4RH).
Category II: Failure, after failure of a
default, defaulter, Relapses First line
treatment regimen (2HRZES + 1HRZE + 5HRE).
Category III:Less severe sputum smear
negative pulmonary TB and less severe type of
extra pulmonary TB. First line standard
regimen (2HRZ + 4RH).
Category IV: Chronic or drug resistant TB
cases. Second line regimens.

12

13
Optimal management of new
cases of TB
The Iraqi National TB Program (NTP)
(see page 19) committee adapted a new
WHO strategy since October 2000 and
this consists of:
1. Initial daily intensive phase:is
supervised by medical staff or
(patient's family or others). Containing
Rifampcin 450 mg if the patient weight
less than 50 Kg & 600mg if his weight is
more than 50 Kg. Plus INH 300 mg .
Plus 1.5 gm of Pyrazinamid if patient's
weight is less than 50 Kg and 2gm for
patient weighing more than 50 Kg Plus
either Ethambutol 25 gm/Kg or
streptomycin 0.75 gm daily.
2. Continuation phase: Preferable to be
supervised .On the day of receiving
the drug, contain daily Rifampcin and
INH for next 4 months.(Table 3)
Table 3 Possible alternative regimens for treatment category
Alternative TB Treatment regimens
T.B. Patient TB Treatment
category
Continuation phase
Initial Phase
4HR or 6HE
2HRZ E or (S)
New smear + ve patient (Figure 6)
PTB
New smear – ve patient
PTB with extensive parenchyma involvement
New cases of severe forms of extra PTB
I
5HRE
2HRZES +
1HRZE
Sputum smear + ve
Relapse
Treatment failure
Treatment after interruption
II
4HR or 6HE 2HRZ
New s – ve PTB (other than in category I)
New less severe forms of extra PTB
III
NOT APPLICABLE
(refer to WHO guidelines for use of second line drugs in specialized
centers)
Chronic cases (still sputum positive after supervised retreatment)
IV

14
Figure 6
Treatment for the New Pulmonary and extra pulmonary cases
New Pulmonary and extra pulmonary cases
The initial phase 2 HRZE
pulmonary cases
Sputum smear examination (for pulmonary TB cases) at the end of 2nd, 5th, 6th months
For extra pulmonary cases: clinical assessment and other measures e.g. radiology, biopsy, etc.
If smear negative
cases
If smear positive at
5th months
Continuation phase
4HR Retreatment

15
DR TB is a man-made disease (due to non-
compliance, improper drug regimen,
etc.).Primary resistance is prevented by
giving the patient combination of drugs.
Secondary (acquired) TB resistance is
expected to be developed in:
1. A large bacillary population such as
patient with cavitations.
2. Inadequate drug regimens
(inappropriate drugs, insufficient
dosage), drug side effects and
complications.
3. Treatment of DR TB should be done
by or in close consultation with an
expert in the management of these
cases & on hospitalization bases.
4. A single new drug should never be
added to a failing regimen.
5. Treatment duration for DR TB patient
may last 18-24 months by using 4-6
drugs (capriomycin, cyclocerin,
ethionamide, levofloxacine, and PAS).
6. Second line regimens often represent
the patient's last hope for being cured
inappropriate management can thus
have life threatening sequences.
Drug resistance TB patients (DR)
6

16
Figure 7
Retreatment Cases
Relapse, Failure, after Defaulters
Check sputum smear at the end of 3rd, 5th, 8th months
If smear - ve continue on HRE for 5 months
If smear + ve continue on HRZE
Check sputum after 5 months
If smear + ve at the 5th month
If smear + ve at the end of treatment
Culture and sensitivity C/S
If C/S show resistant to 2 or more of the drugs
Drug resistant (DR) case .start
2nd line drugs

17
Management of contacts of
smear positive cases
Children age & adults: any person who
coughs & who was in contact with smear
positive index case (smear positive
pulmonary TB patient) should have three
sputum examinations (Fig.8)
Children aged less than 5 years: any
contact aged less than 5 years who has a
positive tuberculin that not previously
vaccinated with BCG with signs or
symptoms of TB should be treated as
suffering from active TB.
Those without signs or symptoms of
disease should be given preventive
chemotherapy (INH for 6 months)
Children under one year of age with
mothers who are being treated for smear
positive pulmonary TB should be given
Isoniazid if the tuberculin test is negative
at the end of three months, INH may be
stopped & BCG may be given .
Treatment regimens in special
situation:
Treatment for pregnant women: most
anti-TB drugs are safe for use in pregnant
women the exception is streptomycin
which is auto toxic to the fetus should not
be used in pregnancy.
Treatment for breast feeding women: all
the anti-TB drugs are compatible with the
breast feeding.
Patient with liver disease: should not
receive Pyrazinamid. The recommended
regimen are 2 S.H.R.E./6 H.R. OR 2
S.H.E./10 H.E.
Acute viral hepatitis: combination of
Streptomycin and Ethambutol up to a
maximum duration of 3 months until the
acute hepatitis has resolved then
continuation phase of 6 months of INH
and Rifampcin.
Treatment of patients with renal failure:
the safest regimen is 2 H.R.Z. /6 H.R.
Assessment of the Patient:
The three approaches to monitoring progress of patient during treatment are: 1. Clinical Assessment:
Clinical assessment of progress is largely subjective. Disappearance of clinical symptoms, general wellbeing and ability to resume normal activities and weight gain are all pointers to clinical progress. ESR and other tests are unreliable and unnecessary in monitoring progress.
2. Assessment by bacteriology:
The management of patients is generally based on smear microscopy. It is not necessary to examine the sputum every month. The WHO and I.U.A.T.L.D recommended monitoring progress during treatment in smear positive patients through sputum. Smears on three occasions, at second month, fifth month and at the end of treatment. This allows decisions on treatment management to be made with a minimum of tests.
3. Assessment by Radiography:
Assessment by radiographic changes alone can be very misleading.
Management of contacts of smear positive cases and in special situations
7

18
Figure 8
How to manage a child contact of a newly diagnosed patient with tuberculosis
Tuberculin Test is possible
Tuberculin +ve Tuberculin - ve
Child is well Child is well Child is unwell
Full clinical
assessment
Preventive isoniazid for 2
months
Preventive isoniazid for 2
months
Possibility of tuberculosis
possible Possibilityof tuberculosis
possible
Tuberculin - ve Tuberculin +ve
Full treatment for
tuberculosis
Isoniazid for 6 months
Stop isoniazid and
Give BCG

19
National TB program (NTP)
9
Iraq has an estimated 32,249,932
inhabitants. The country is
administratively divided into 18
governorates with varying population
sizes ranging from around 800 thousand
to 7 million. The Ministry of Health has
established the National Tuberculosis
Control Programme (NTP) in 1989 with
WHO support, and introduced the DOTS
strategy in 1998. By 2000, the DOTS
strategy was implemented at all the
Governorate Respiratory and Chest
Disease Clinics – except for the three
northern governorates of Kurdistan Iraq –
assuming 100% population DOTS
coverage regardless of the actual number
of people who have real access to that
clinic. By 2008, the three northern
governorates had started DOTS
implementation.
The Government of Iraq considers TB as a
major public health problem, and keeps
TB control high in the national health
agenda. Currently, many health reforms
are ongoing including the expansion of
the DOTS services into the Basic Package
of Health Services to be delivered
through the nationwide network of
Primary Health Care Centers (PHCCs). The
Government of Iraq invests strongly in
the rebuilding of the health infrastructure
that was damaged during the war and
encourages recruitment of qualified
health personnel. The NTP enjoys the full
support of the Government of Iraq. In
addition to the strong political
commitment to the National TB Control
Program, the government also supports
the procurement of first and second-line
anti TB drugs and the strengthening of
the storage and distribution
infrastructure.
The overall responsibility for TB control
rests with the NTP within the MoH. NTP is
responsible for policy and strategy
formulation, coordination with partners,
as well as planning, implementation and
monitoring of control activities. The
organizational structure of NTP is based on
4 levels:
1. Chest & Respiratory Diseases
Specialized Center at the national
(central) level in Baghdad: It is
responsible for training of staff,
implementation of the national TB
control plan and supervision of
activities in governorates.
2. Nineteen Governorate Respiratory and
Chest Disease Consultation Clinics at
the governorate (intermediate) level:
the governorate clinics are responsible
for diagnosis and registration of TB
cases detected in their geographic
areas. These clinics provide treatment
to their patients or refer them to the
district TB Management Unit for
treatment follow up.
3. There are 126 health districts in Iraq
(peripheral level). The health district’s
core organizational entity is the TB
Management Unit (TBMU)/ District TB
Coordinator (DTC). In each one of
these districts, the main Primary
Health Care Center has a TBMU which
ensures TB diagnosis and treatment.
The TBMUs also have TB register and
reporting facilities. TBMUs are also
responsible for the referral of TB
patients to a PHCC that is the nearest
to the patient’s residence – if available
– and for treatment follow-up of
patients. The TBMU is the basic
management unit in NTP.
4. There are Primary Health Care Centers
(PHCCs) throughout Iraq (some are
directed by Doctors and others are
directed by paramedical staff) in
addition to a number of main PHCCs
with training functions (peripheral

20
level). The role of PHCCs, other than
main centers, is limited to the
monitoring of patients’ treatment
intake under DOT.
National TB program in Iraq
Vision:A TB-free country, with
elimination of the disease as a public
health problem by 2050.
Goal: To reduce dramatically the country
burden of TB by 2015, in line with the
MDGs and Stop TB partnership targets.
Objectives:
Achieve universal access to high
quality care for all TB patients
including vulnerable populations.
Ensure universal access to diagnosis,
treatment and care for Drug-Resistant
TB (DR-TB).
Protect and promote human rights in
TB prevention, care and control.
Targets:
Halt and begin to reverse the
incidence of TB by 2015;
Reduce the prevalence of and deaths
due to TB by 50% by 2015
STRATEGIC DIRECTIONS
These strategic directions are designed
according to the key component of
International Stop TB Strategy:
1. The political will of the government
Political commitment with increased
and sustained financing
Improving quality and efficiency of
general services in respiratory
illnesses in Primary Health Care
facilities through strengthening DOTS
integration into the Basic Package of
Health Services (BPHS)
Case detection through quality-
assured bacteriology
An effective drug supply and
management system
Strengthening the Monitoring and
Evaluation (M&E) System and impact
measurement
2. Scale-up the prevention and management of Drug-Resistant TB (DR-TB)
3. Addressing TB/HIV, and the needs of
poor and vulnerable populations
Scale-up collaborative TB/HIV activities
Address the needs of TB contacts, and poor and vulnerable populations
4. Engaging all care providers, public, non-governmental and private, by scaling up public-private mix (PPM) approaches to ensure adherence to the International Standards of TB Care.
5. Empowering patients and
communities by scaling up community TB care and creating demand through context-specific advocacy, communication and social mobilization, for the patient empowerment, community involvement and Community Health Worker (CHW) training for community-based DOTS.
6. Enabling and promoting research to improve programme performance.
Developing a national framework for operational research and building local capacity in operational research.

21
DOTS 8
What is DOTS?
Direct Observation Treatment Short
Course (DOTS). DOTS is the new WHO
strategy, it is based on one priority, to
ensure that all sputum smear positive
pulmonary TB complete a full course of
short course chemotherapy with direct
observation of swallowing the drug during
the period of treatment or at least during
the initial phase of treatment. The main
advantage of DOTS is that treatment is
carried out entirely under programed
supervision, only when a second person
directly observes a patient swallowing the
given medication then can be certain that
the patient is actually receiving the
prescribed treatment regimen. No
concealed irregularity can occur as it can
in self-administration regimen, the
treatment observer ensures that
medicines are taken at the correct interval
& in the correct dosage & with that
certainly come benefits both for the
patient & the community. Perhaps the
most immediately apparent is the high
cure rate associated with assured
completion of treatment. Equally
important is the dramatic reduction in the
development of drug resistance.
Adverse effects and treatment
complications can be quickly identified &
addressed.
The basic rules for efficient TB treatment
an initial intensive phase associating at
least four major anti T.B drugs
administrated daily during two months
followed by continuation phase during the
next four months with two major anti T.B
drugs.
The DOTS strategy required five
conditions:
1. The political will of the government.
2. Existence of laboratories network to
identify smear positive pulmonary TB
patients.
3. A network of peripheral health
centers.
4. Regular supply of drugs and reagents.
5. Organization of permanent
surveillance system in order to
supervise the tasks of program and to
evaluate its epidemiological impact.
10 Reasons to use DOTS
1. Cure the patient.
2. Prevents new infection.
3. Stop MDR tuberculosis.
4. Cost effective.
5. Community based.
6. Extends lives of AIDS patients.
7. Protects the workforce.
8. Protects the international travelers.
9. Stimulates economies.
10. Proven effectiveness.

22
Figure 9
DOTS program implementation profile
Diagnosis
Supplies
Training
Supervision
Monitoring and Evaluation
Patient
Chest and Respiratory
Diseases institute Chest and Respiratory
Diseases clinic
Baghdad Governorate
District TB coordinator District TB coordinator
PHCC
Daily treatment
supervisor

23
The bacille Calmette-Guérin BCG was
first used to immunize humans in
1921, and following its introduction
into the WHO Expanded Program on
Immunization in 1974, BCG soon
reach global coverage rates exceeding
80% in countries endemic for TB.
Extensive clinical trials have been
conducted to assess the protective
efficacy of BCG against pulmonary
TB, but a wide range of vaccine
efficacy values have been observed
probably due in part to differences in
study design and geographical
location. BCG vaccination does not
prevent reactivation of latent TB, the
main source of bacillary dissemination
in the community. Despite these
limitations, and particularly in light of
the growing HIV/AIDS pandemic and
the appearance of multidrug-resistant
M. tuberculosis strains, BCG vaccines
will continue to represent an important
tool in the global fight against TB until
new vaccines are available.
BCG vaccine is part of the national
childhood immunization program.
BCG vaccine has a documented
protective effect against meningitis and
disseminated TB in children. It does
not prevent primary infection. The
impact of BCG vaccination on
transmission of TB is therefore limited.
WHO recommendations on the
use of BCG vaccine
• In countries with a high burden of
TB, a single dose of BCG vaccine
should be given to all infants as soon
as possible after birth. Since severe
adverse effects of BCG vaccination are
extremely rare, all healthy neonates
should be BCG -vaccinated, even in
areas endemic for HIV.
• BCG vaccination should not be given
to (i) infants and children with AIDS,
(ii) infants and children known to be
HIV-infected or (iii) children known to
have other immunodeficiencies.
• In situations where infants have been
exposed to smear-positive pulmonary
TB shortly after birth, BCG
vaccination should be delayed until
completion of six months of INH
preventive therapy (IPT).
• Vaccination of health staff, and
particularly laboratory, is an option
in high-risk environments (in particular
if staff are in close contact with cases
of drug-resistant TB).
• There is no evidence that
revaccination increases protection, and
revaccinationis not recommended.
• Countries with a low burden of TB
may choose to limit BCG vaccination
to neonates and infants of recognized
high-risk groups for the disease or of
tuberculin skin test (TST)-negative
older children. In some low-burden
populations, BCG vaccination has been
replaced by intensified case detection
and supervised early treatment
Until an improved anti-TB vaccine
becomes available, efforts to control
the spread of the disease will continue
to rely on currently available tools,
namely early diagnosis and treatment,
appropriate preventive treatment, and
other public health and infection
control measures
BCG Vaccines 9

24
1- The new rapid TB test – known as
Xpert MTB/RIF- is a fully-automated
diagnostic molecular test. It has the
potential to revolutionize and
transform TB care and control. The
test:
• simultaneously detects TB and
rifampicin drug resistance
• provides accurate results in less than
two hours so that patients can be
offered proper treatment on the same
day
• has minimal bio-safety requirements,
training, and can be housed in non-
conventional laboratories
WHO recommendations on the
use of Xpert MTB/RIF test
• Strong recommendation: Xpert
MTB/RIF rapid test should be used as
the initial diagnostic test in individuals
suspected of MDR-TB or HIV/TB
• Conditional recommendation:
Xpert MTB/RIF rapid test may be used
as a follow-on test to microscopy in
settings where MDR-TB and or HIV is
of lesser concern, especially in smear-
negative specimens (recognizing major
resource implications)
EXPECTED IMPACT
• A three-fold increase in the diagnosis
of patients with drug-resistant TB
• A doubling in the number of TB/HIV
cases diagnosed in areas with high
rates of TB and HIV (compared to
microscopy diagnosis)
2-The use of molecular line probe
assay for detection of resistance anti-
tuberculosis drugs
Genotypic (molecular) methods have
considerable advantages for scaling up
programmatic management and
surveillance of drug-resistant TB,
offering speed of diagnosis,
standardized testing, potential for high
through-put, and fewer requirements
for laboratory biosafety. Molecular line
probe assay (LPA) technology for
rapid detection of multi-drug resistant
tuberculosis (MDR-TB) was endorsed
by WHO in 2008.
New modality in TB diagnosis
10

25
References 1- Global TB control/WHO report
2000.
2- Global tuberculosis report 2012
/WHO 2012.
3- Global tuberculosis report 2009
/WHO 2009.
4- Implementing the WHO stop TB
strategy –A handbook for national
tuberculosis control programs-
WHO/HTM/TB/2008.401.
5- What is DOTS ? WHO / CDSCPC
/ TB / 99 ; 270.
6- You can stop TB ,EMRO , world
TB day 24 march 2000.
7- Stop TB at the source .WHO
report on TB epidemic , 1995.
8- Treatment of TB guideline for
national program ,WHO,97.
9- Fighting TB,WHO/TB/1995.
10- Fiona GTB is global emergency
BMJ ,1993.
11- Horne-N modern drug treatment
of TB oxford university
press,1992
12- Kochi.A.TB control is not what is
used to be ,the TB treatment
observed TB WHO,1996
13- Nadia AIT .Khalid and Donald ,
Enarson .TB a manual for medical
students , WHO,1999.
14- Croften , Horne , Miller. Clinical
TB, IUAT.1992
15- fact sheet- tuberculosis diagnostics
, Xpert MTB/RIF Test-WHO
February 2013
16- The use of molecular line probe
assay for the detection of
resistance to second – line anti –
tuberculosis drug ,expert group
meeting report :Geneva ;February
2013. WHO/HTM/TB/2013.01.




















![the Path Forward in Iraq [COIN in Northern Iraq]](https://img.pdfslide.net/doc/110x75/58a2c7391a28ab724d8b5927/the-path-forward-in-iraq-coin-in-northern-iraq.jpg)