Embed Size (px)
Citation preview
The Relationship between Burnoutand Role Stress in TherapeuticRecreation Specialists
Leandra A. Bedini, Lavon Williams, and Deanna Thompson
Professionals in health care must face pressures of accountability, justification of worth, andcost containment in addition to every- day responsibilities of working with people in humanservices and of providing quality health care. As a result, the possibility of burnout amonghealth care professionals is a concern. Since therapeutic recreation specialists (TRS) are partthe health care process, this study examined burnout and role stress among TRSs in theUnited States. Research problems addressed: (a) existence and extent of burnout, specifi-cally emotional exhaustion, depersonalization, and personal accomplishment; (b) existenceand extent of role stress, specifically role conflict and role ambiguity; (c) relationship be-tween burnout and role stress; and (d) contributing factors to burnout in TRSs. Mailedsurveys were analyzed by descriptive and interpretive analysis such as canonical correlationand regression. Results indicated that TRSs experienced moderate burnout, and a positiverelationship was determined between the burnout and role stress. Discussion and implica-tions for therapeutic recreation professionals are addressed.
KEY WORDS: Burnout, Role Stress, Role Conflict
Bedini is an Assistant Professor in the Department of Leisure Studies and Williams is aDoctoral Candidate in the Department of Exercise and Sport Science, both at University ofNorth Carolina at Greensboro. Thompson is a Therapeutic Recreation Specialist inDurham, North Carolina.
This paper was presented at the NRPA Symposium on Leisure Research in San Jose, CA inOctober, 1993. This research was funded in part by the North Carolina Recreation andPark Society's Therapeutic Recreation Division.
Third Quarter 1995 163
Recently, professionals in the health carearena have been presented with new pres-sures regarding accountability, justificationof worth, and cost containment. These pres-sures are being added to the every day re-sponsibilities and stress of working withpeople in human services and providingquality health care. Stressors, such as thosementioned, that exist in most work settingscan have a negative impact on one's job per-ception and performance. The cumulativeeffect of these stressors can be overwhelmingto health care professionals, potentially con-tributing to burnout.
Burnout among health care professionalscan be one of the most destructive elementsin one's work environment. Burnout causesperceptions and symptoms that ultimatelyreduce effectiveness on the job (Maslach,1982a; Pines & Aronson, 1988). While re-search has been conducted on the impact ofburnout on a myriad of specific health careprofessionals ranging from child life workers(Holloway & Wallinga, 1990), to physicaltherapists (Deckard & Present, 1989), littleattention has been given to therapeutic rec-reation professionals. Specifically, studiesabout burnout among therapeutic recre-ation professionals and its relationship torole stress are sparse.
Thompson (1990) examined the rela-tionship of role stress and burnout in a pilotstudy of 52 therapeutic recreation specialists(TRS) in North Carolina. Her findings sug-gested moderate levels of burnout and a re-lationship between burnout and role stressin these TRSs. Based on these preliminaryresults and since therapeutic recreation spe-cialists today are subject to mounting pres-sures of health care services, the potential forrole stress and burnout in therapeutic recre-ation specialists warranted examination.The present study examined burnout androle stress among therapeutic recreationspecialists in the United States. Specific re-search problems addressed: (a) existenceand extent of burnout, specifically emo-tional exhaustion, depersonalization, and
personal accomplishment among TRSs; (b)existence and extent of role stress in theform of role conflict and role ambiguityamong TRSs; (c) relationship between burn-out and role stress among TRSs; and (d)contributing factors to burnout in TRSs.
LiteratureThe underlying conceptual framework
for this study was Merton's (1976) theory ofambivalence. This theory suggests thatwithin a social system," strain, tension, andinconsistencies regarding roles exist. Thesediscrepancies in how an individual defineshis or her roles can result in dysfunctionalbehaviors and manifestations. In otherwords, incompatible expectations or beliefsassigned to one's status or position withinone's professional and social structures (am-bivalence) can contribute to role stress. Sub-sequently, role stress, if unresolved, has thepotential to impact how an individual per-ceives and reacts to his or her status andstrain (Maslach, 1982b). Based on this prop-osition, the relationship between role stressand burnout is an important concept to ex-plore for many human service professionals.
Role StressPeople take on many roles throughout
their lives. Within the work environment,one's role is very important. According toHardy and Hardy (1988), the term role" isdefined as expected and actual behaviors as-sociated with a position" (p. 165). Rolestress, then, relates to a social structurerather than to an individual within the socialstructure. Role stress is a condition whererole obligations are vague, irritating, diffi-cult, conflicting, or impossible to meet"(Hardy & Hardy, 1988, p. 165). Accordingto Deckard and Present (1989), there aretwo major components of role stress: roleconflict and role ambiguity. Role conflictoccurs when role demands are inconsistentwith the person's goals, abilities, values, orbeliefs. Hardy and Hardy (1988) noted that
164 Therapeutic Recreation Journal

research on role conflict indicated that it isinevitable in most organizations. Role am-biguity results from lack of adequate infor-mation for an individual to perform a role(Deckard & Present, 1989). As Hardy andHardy (1988) suggested, disagreement onrole expectations in the work communitywithout proper understanding of the expec-tations by the worker creates role ambiguity.
BurnoutMaslach (1982b) denned burnout as a
syndrome of emotional exhaustion, deper-sonalization, and reduced personal accom-plishment that can occur among individualswho do people work' of some kind" (p. 30).She further characterized burnout as ameans of coping with the strain of dealingextensively with other people, especiallypeople who are experiencing difficulties.This definition served as a basis for the de-velopment of the Maslach Burnout Inven-tory (Maslach & Jackson, 1981, 1986)which measures three subcategories of burn-out: emotional exhaustion, depersonaliza-tion, and personal accomplishment. Ac-cording to Maslach and Jackson (1986),emotional exhaustion is defined as feelingsof being emotionally overextended and ex-hausted by one's work"; depersonalizationas an unfeeling and impersonal response to-wards recipients of one's service, care, treat-ment, or instruction"; and personal accom-plishment as feelings of competence andsuccessful achievement in one's work withpeople" (p. 2).
Organizational Factors Leadingto Burnout in HealthCare Professionals
Dailey (1990) demonstrated a direct cor-relation between increasing role conflict androle ambiguity (role stress) and negativework attitudes. Similarly, Deckard andPresent (1989) found that the emotional andphysical well-being, as well as the degree ofburnout experienced by physical therapists,
was at least a partial result of role ambiguityand role conflict in the organizational envi-ronment. Additionally, conflict regardingprofessional values was a significant predic-tor of job satisfaction and thus had potentialties to burnout (Siefert, Jayaratne, & Chess,1991).
Perlman and Hartman (1982) reviewedprofessional literature on burnout to deter-mine that organizational variables were moreoften a source of burnout than individualvariables. Organizational sources of stressleading to burnout including lack of auton-omy, insufficient resources, inadequate staff,overwhelming workload, and a lack of sup-port were studied among nurses (Firth, Phil,McKeown, Mclntee, & Britton, 1987;McGrath, Reid & Boore, 1989; Williams,1989), paramedics (Grisby & McKnew,1988), physical therapists (Deckard & Pres-ent, 1989), medical social workers (Coady,Kent, & Davis, 1990) and child life special-ists (Holloway & Wallinga, 1990). It is ap-parent from these studies that an under-standing of organizational variables such asrole stress (Schwab & Iwanicki, 1982) is nec-essary to address burnout adequately.
Individuals Factors AffectingBurnout
Although most research has focused onthe environmental and occupational factorsthat might contribute to role stress andburnout, several studies exist that noted per-sonal factors that may affect one's predispo-sition to burnout. For example, Maslach(1982b) as well as Hardy and Hardy (1988)noted that a relationship existed betweenage and burnout in health care workers.Findings showed that the younger the healthcare workers were, the more likely theywould experience burnout. Additionally,Maslach (1982b) found that level of educa-tion showed significant differences in burn-out levels. Health care workers with a col-lege education but no post college trainingwere more likely to become burned out. In-
Third Quarter 1995 165
dividuals with less than a college education,however, had the lowest level of burnout.
Consequences of Burnout and RoleStress in Health Care Services
The effect of burnout on physical andemotional well being of health care profes-sionals can be overwhelming. For example,burnout has been associated with such phys-ical consequences as fatigue, headaches, andflu (Pines & Aronson, 1988); chronic fatigueand tension which can increase susceptibil-ity to illness, lingering colds, persistentheadaches (Maslach, 1982a); and gastroin-testinal disorders and muscular pain (Car-roll & White, 1982). Psychological healthalso can be affected by burnout. Indicatorsof this effect include paranoia, depression,tics," inability to concentrate (Carroll &White, 1982); low self esteem, irritability,and poor relations with family and friends(Maslach, 1982a). Functionally in the work-place, Maulday (1983) noted an impairedability to meet demands, decreased enthusi-asm and motivation at work, decreased abil-ity to solve problems, decreased empathyand compassion for clients, increased abuseof substances, and increased turnover in theworkplace.
Role Stress and Burnout inTherapeutic Recreation Specialists
Therapeutic recreation specialists sharethe pressures health care work environmentwith many health care professionals (e.g.,nurses, physical and occupational thera-pists, child life specialists). Additionally,TRSs face the frustration of sometimes be-ing perceived as less important than otherdisciplines in health care (e.g., Smith, Perry,Neumayer, Potter, & Smeal, 1991). As a re-sult, it is logical to assume that TRSs are es-pecially vulnerable to the elements thatmight contribute to burnout. Few studiesaddress burnout or role stress specifically fortherapeutic recreation specialists. Cunning-ham and Bartuska (1989) explored the rela-
tionship between overall stress and leisuresatisfaction in therapeutic recreation profes-sionals finding that TRSs experienced sim-ilar stress as others in related occupations.Wade-Campbell and Anderson (1987) stud-ied therapeutic recreation personnel whoworked in Veteran's Administration agen-cies. They found that while TRSs experi-enced low levels of emotional exhaustion,they demonstrated moderate levels of de-personalization, and low levels of personalaccomplishment leading to burnout. Sim-ilarly, Thompson's (1990) pilot study, spe-cifically on the relationship between rolestress and burnout in therapeutic recreationprofessionals in North Carolina, suggestedsome commonalities between TRSs andother health care professionals. These find-ings indicated the need for a more generaliz-able study on the national level across set-tings to determine the status of burnout andthe relationship between burnout and rolestress for TRSs in the United States.
Methods
SampleSubjects consisted of therapeutic recre-
ation specialists (TRS) identified throughrandomized sampling of those certified atthe professional level with the NationalCouncil on Therapeutic Recreation Certi-fication (NCTRC). Subjects were of bothsexes and varied demographically (a de-tailed breakdown can be found in the resultssection).
A sampling frame of 10,000 professionalmembers warranted at least 375 subjects toapproach generalizability of the sample(Krejcie & Morgan, 1970). At the time of themailing, the National Council for Thera-peutic Recreation Certification had no ca-pacity to select individuals randomly fromits member" list, however, all individualswere listed by state. Therefore, a multistagecluster sampling procedure was used. Amultistage cluster sampling procedure is ap-
166 Therapeutic Recreation Journal
propriate in cases where the sampling frameis too large or impractical for individual sys-tematic sampling and the subjects are al-ready grouped in subpopulations (i.e.,states) (Babbie, 1986). For this study, clustersampling consisted of a two-stage listing andsampling technique. The first stage em-ployed a random selection of states chosenfrom the original mailing list. In the secondstage, a sample of 400 subjects was selectedfrom the list of states generated in the firststage using a systematic random samplingprocedure choosing every 7th name.
InstrumentsQuestionnaire packets were mailed to
400 TRSs. The questionnaire packets in-cluded three instruments: a Maslach Burn-out Inventory (MBI), a Role Stress Scale(RSS), and a Respondent Profile Survey(RPS). The MBI (Maslach & Jackson, 1986)is a 22 item measure of perceived burnout inthe helping professions and consists of threesubscales: emotional exhaustion, deperson-alization, and personal accomplishment.The nine item Emotional Exhaustion scaledescribes feelings of being emotionally over-extended and exhausted by one's work"(Maslach & Jackson, 1986, p. 7). The fiveitem Depersonalization subscale describesan unfeeling or impersonal response towardrecipients of one's care or service" (Maslach& Jackson, 1986, p. 7). The eight item Per-sonal Accomplishment subscale describesfeelings of competence and successfulachievement in one's work with people"(Maslach & Jackson, 1986, p. 7). Accordingto Maslach and Jackson (1981), the Per-sonal Accomplishment subscale should notbe viewed as opposite of Emotional Exhaus-tion and Depersonalization, rather as inde-pendent of the other two subscales. ThisPersonal Accomplishment subscale is re-versed with the lower mean scores indicat-ing higher burnout. Each subscale wasscored using a 7-point Likert scale rangingfrom never" = 0 to every day" = 7 statinghow often one experienced a particular con-
cept related to burnout. Total scores canrange from 0 to 154 with subscales rangingfrom 0 to 63, 35, and 56 respectively. In-ternal consistency of the three subscales hasbeen demonstrated in prior research with1316 human service professionals. Cron-bach alpha coefficients were .90 for Emo-tional Exhaustion, .79 for Depersonaliza-tion, and .71 for Personal Accomplishment(Maslach & Jackson, 1981).
The Role Stress Scale (Rizzo, House, &Lirtzman, 1970) is a 30 item instrument us-ing a 7 point Likert scale ranging from 1= very false" to 7 = very true" in responseto questions about conflicts and ambiguitiesin work responsibilities. No score is deter-mined for role stress overall, however, theinstrument measures the subscales of roleambiguity (six questions) and role conflict(eight questions). The total scores can rangefrom 7 to 42 for role ambiguity and from 7to 56 for role conflict. The established Cron-bach alpha reliability coefficient for the sub-scales were .86 for role ambiguity and .85for role conflict (Rizzo, House, & Lirtzman,1970).
The Respondent Profile Survey (RPS)was demographic information checklist de-signed for this study. Comprised of 15 ques-tions, the RPS identified information suchas setting/service area, age, sex, years inpractice, years in present position, clientload, and educational level.
ProcedureThe Total Design Method (Dillman,
1978) was used for conducting mail surveyresearch. This method employs personaliz-ing techniques proven to encourage good re-sponse rates. Based on the techniques of theTDM, each packet contained the three in-struments, a personal cover letter explainingthe purpose of the study, and a stamped,self-addressed return envelope. Based on theTDM, a follow-up postcard was sent ap-proximately two weeks after the initial mail-ing to those who had not responded. A sec-ond cover letter and packet were sent two
Third Quarter 1995 167
weeks after the card for those subjects whoremained unaccounted.
Analysis and ResultsBoth descriptive and interpretive statis-
tics were used with this study. Frequenciesand percentages were determined for the de-mographic portions of the study. Univariateand multivariate analyses such as corre-lations and regression analyses also wereused to determine relationships betweenburnout variables and role stress variables.
From a mailed sample of 400 surveys, atotal of 236 (59%) were returned, 219 (55%)of which were usable. Seventeen of the re-turned surveys could not be used because ei-ther the respondents were not currentlypracticing in therapeutic recreation (i.e., re-lated fields, leave of absence, educators) orfailed to complete the surveys properly. Thedemographics of the subjects revealed asample reflective of the field of therapeuticrecreation (e.g., Brasile, 1992) with 45(20.5%) of the respondents being male and174 (79.5%) female. Additionally, fiftyseven percent (n = 121) of those who re-sponded were therapists, while 43% (n = 90)held dual roles or were administrators. Theage ranged from 21 to over 66 years with themean age in the 31-35 years category.
Fifty-four percent (n = 118) of the re-spondents indicated that they worked inmore than one setting or service area. Ser-vice areas most commonly represented werepsychiatric (49.5%), followed by physical re-habilitation (30.6%), geriatrics (14.6%), de-velopmentally disabilities (8.7%), pediatrics(8.2%), medical surgery (6.8%), and other"(22.3%) which included head injury, dualdiagnosis, burn, school, and community. Asa group, the respondents practiced thera-peutic recreation for an average of 10 to 15years with an average of 5 to 8 years in theirpresent position. They worked with a me-dian of 40 clients a week, averaging 20 to25 hours of client contact per week. Whenasked what the most stressful part of theirjob was, the two most frequently cited re-
sponses were case load (22.4%), and lack ofsupport (15.2%). Problems with coworkers(9.5%), poor salary (8.6%), poor job security(7.1%), ungrateful/non-compliant clients(7.1%), problems with boss (4.8%), and deadend job (4.8%) were also identified. Most ofthe remaining respondents selected other"(13.9%), which included concerns such aslack of time off, lack of supervision, or work-ing with terminally ill clients. The remain-ing 6.7% chose more than one stress factor.
Existence and Degree of BurnoutScores on the Maslach Burnout Inven-
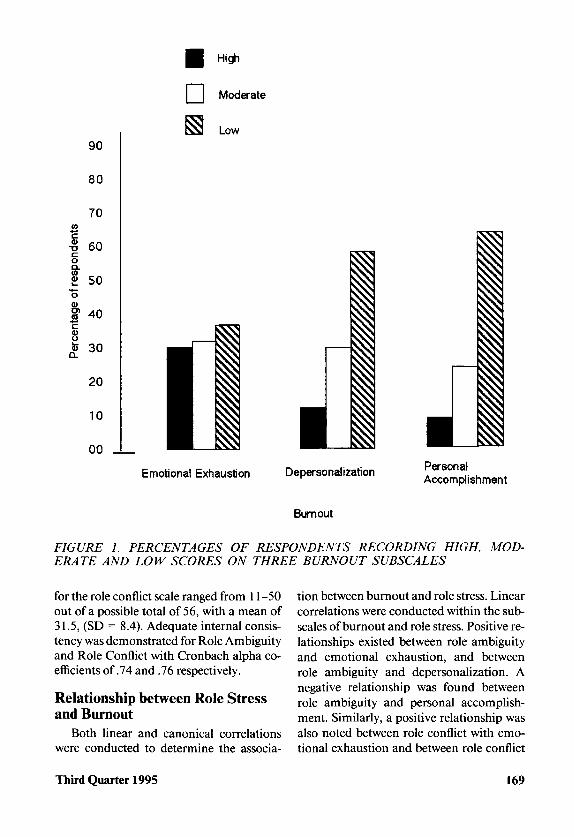
tory for this sample ranged from 42 to 104,out of a possible total of 154, with a meanscore of 67.1 (SD = 12.46). The three sub-scales of the Maslach Burnout Inventory,Emotional Exhaustion, Depersonalization,and Personal Accomplishment, demon-strated internal consistency with Cronbachalpha coefficients of .80, .76, and .73 respec-tively. According to the category ranges oflow, moderate, and high identified by theMBI (Maslach & Jackson, 1986), results in-dicated that the subjects' responses on emo-tional exhaustion were evenly distributed.Responses indicated that 30.1 % of the re-spondents scored in the high" category,31.5% in the moderate" category, and36.5% scored in the low" category for emo-tional exhaustion. The respondents' deper-sonalization scores showed 10.5% of thesample in the high category, 27.4% in themoderate category, and 58.4% in the lowcategory of depersonalization. Finally, thesubjects' personal accomplishment scoresshowed 6.8% in the high category, 24.7% inthe moderate category, and 63.5% in the lowcategory of personal accomplishment (seeFigure 1).
Existence and Extent of RoleStress
Subcategory scores for role ambiguityranged from 6-37 out of a possible total of42, with a mean of 16.2, (SD = 5.7). Scores
168 Therapeutic Recreation Journal
CO
1
90
80
70
60
£ 50
I 40<D
I 30
20
10
00
High
Moderate
Low
Emotional Exhaustion Depersonalization
Burnout
PersonalAccomplishment
FIGURE 1. PERCENTAGES OF RESPONDENTS RECORDING HIGH, MOD-ERATE AND LOW SCORES ON THREE BURNOUT SUBSCALES
for the role conflict scale ranged from 11 -50out of a possible total of 56, with a mean of31.5, (SD = 8.4). Adequate internal consis-tency was demonstrated for Role Ambiguityand Role Conflict with Cronbach alpha co-efficients of .74 and .76 respectively.
Relationship between Role Stressand Burnout
Both linear and canonical correlationswere conducted to determine the associa-
tion between burnout and role stress. Linearcorrelations were conducted within the sub-scales of burnout and role stress. Positive re-lationships existed between role ambiguityand emotional exhaustion, and betweenrole ambiguity and depersonalization. Anegative relationship was found betweenrole ambiguity and personal accomplish-ment. Similarly, a positive relationship wasalso noted between role conflict with emo-tional exhaustion and between role conflict
Third Quarter 1995 169
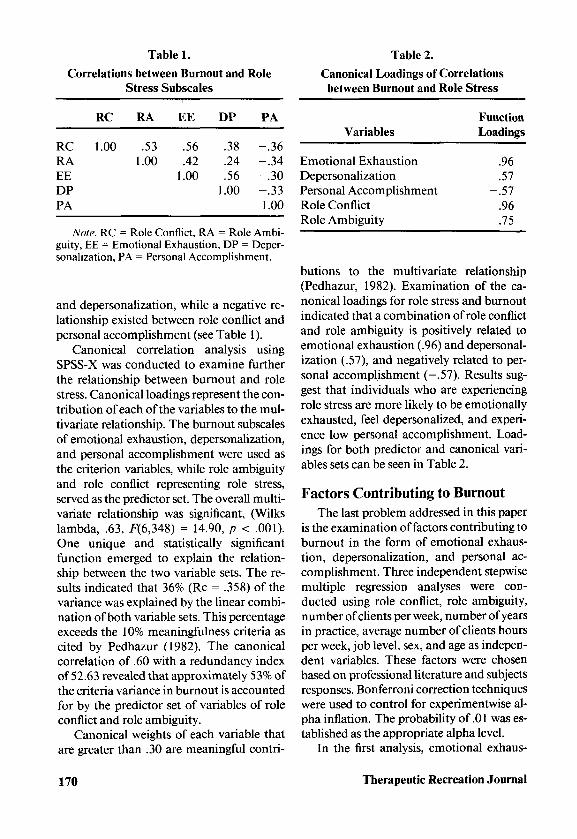
Table 1.
Correlations between Burnout and RoleStress Subscales
Table 2.
Canonical Loadings of Correlationsbetween Burnout and Role Stress
RCRAEEDPPA
ATs-
RC
1.00
RA
.531.00
EE
.56
.421.00
DP
.38
.24
.561.00
A Ortl^
PA
-.36-.34-.30-.331.00
Variables
Emotional ExhaustionDepersonalizationPersonal AccomplishmentRole ConflictRole Ambiguity
FunctionLoadings
.96
.57- .57
.96
.75
guity, EE = Emotional Exhaustion, DP = Deper-sonalization, PA = Personal Accomplishment.
and depersonalization, while a negative re-lationship existed between role conflict andpersonal accomplishment (see Table 1).
Canonical correlation analysis usingSPSS-X was conducted to examine furtherthe relationship between burnout and rolestress. Canonical loadings represent the con-tribution of each of the variables to the mul-tivariate relationship. The burnout subscalesof emotional exhaustion, depersonalization,and personal accomplishment were used asthe criterion variables, while role ambiguityand role conflict representing role stress,served as the predictor set. The overall multi-variate relationship was significant, (Wilkslambda, .63, F(6,348) = 14.90, p < .001).One unique and statistically significantfunction emerged to explain the relation-ship between the two variable sets. The re-sults indicated that 36% (Re = .358) of thevariance was explained by the linear combi-nation of both variable sets. This percentageexceeds the 10% meaningfulness criteria ascited by Pedhazur (1982). The canonicalcorrelation of .60 with a redundancy indexof 52.63 revealed that approximately 53% ofthe criteria variance in burnout is accountedfor by the predictor set of variables of roleconflict and role ambiguity.
Canonical weights of each variable thatare greater than .30 are meaningful contri-
butions to the multivariate relationship(Pedhazur, 1982). Examination of the ca-nonical loadings for role stress and burnoutindicated that a combination of role conflictand role ambiguity is positively related toemotional exhaustion (.96) and depersonal-ization (.57), and negatively related to per-sonal accomplishment (—.57). Results sug-gest that individuals who are experiencingrole stress are more likely to be emotionallyexhausted, feel depersonalized, and experi-ence low personal accomplishment. Load-ings for both predictor and canonical vari-ables sets can be seen in Table 2.
Factors Contributing to BurnoutThe last problem addressed in this paper
is the examination of factors contributing toburnout in the form of emotional exhaus-tion, depersonalization, and personal ac-complishment. Three independent stepwisemultiple regression analyses were con-ducted using role conflict, role ambiguity,number of clients per week, number of yearsin practice, average number of clients hoursper week, job level, sex, and age as indepen-dent variables. These factors were chosenbased on professional literature and subjectsresponses. Bonferroni correction techniqueswere used to control for experimentwise al-pha inflation. The probability of .01 was es-tablished as the appropriate alpha level.
In the first analysis, emotional exhaus-
170 Therapeutic Recreation Journal
tion served as the dependent variable. Re-sults revealed that 36% (R = .60, F (2,174)= 49.15, p = .001) of the variance in emo-tional exhaustion was explained by role con-flict (Beta = .56, p = .001) and age (Beta= -.22, p = .001). These results indicatethat younger therapeutic recreation profes-sionals and those feeling greater role conflictare more likely to experience emotional ex-haustion in the work place than older pro-fessionals with less role conflict.
Depersonalization served as the depen-dent variable in the second multiple regres-sion. Results show that together role conflict(Beta = .37, p = .001) and number of clienthours per week (Beta = .24, p = .001) ex-plained 20% (R = .44, F(2,172) = 2\.\l,p= .001) of the variance in depersonalization.These results indicate that individuals whoexperience greater role conflict and whohave more client hours per week, experiencegreater depersonalization than those whoexperience less role conflict and have fewerhours of client contact per week.
The last multiple regression employedpersonal accomplishment as the dependentvariable. In this analysis, role conflict (B= -.36, p = .001) alone explained 13% (R= .36, JP (1,171) = 25.68, p = .001) of thevariance in personal accomplishment.These results indicate that individuals expe-riencing less role conflict experience greaterpersonal accomplishment than those whoexperience greater role conflict.
ConclusionThe present study examined the relation-
ship between burnout and role stress amongtherapeutic recreation specialists (TRS) inthe United States. Four research questionswere addressed.
The first specific research problem ad-dressed the existence and extent of burnoutusing subfactors of Emotional Exhaustion,Depersonalization, and Personal Accom-plishment among therapeutic recreationspecialists. Similar to Thompson's (1990)study, the results indicated a moderate exis-
tence of overall burnout in TRSs specificallymoderate emotional exhaustion, and lowdepersonalization. Contrary to the results ofThompson (1990), however, it is notablethat the subjects in this study experiencedparticularly low perceptions of personal ac-complishment. This result raises questionsregarding why the subjects did not experi-ence feelings of competence and success re-garding their work.
The second research problem addressedthe existence and extent of role stress, spe-cifically role conflict and role ambiguity,among TRSs. While the subjects experi-enced relatively low role ambiguity, theirscores for role conflict were more substan-tial. According to Hardy and Hardy (1988),role conflict can occur from role obligationsbeing unclear as well as from experiencingcontradictory expectations.
The third research problem addressedthe relationship between role stress andburnout among TRSs. The results identifieda positive relationship between burnout androle stress. These findings suggest the possi-bility that role demands of TRSs that are in-consistent with their individual abilities,values, goals, or beliefs as noted by Deckerdand Present (1989).
The last research problem addressed thecontribution of specific demographic factorsto the constructs of burnout. The multipleregression analyses showed that role conflictwas the most substantial predictor variableacross each subscale of burnout. Addition-ally, demographic factors of age and numberof client hours/week accounted for much ofthe remaining variance in the burnout sub-scales. Therefore, the data suggests thatyounger practitioners with higher client con-tact are more susceptible to burnout thanolder practitioners with fewer hours of clientcontact. The results dealing with age areconsistent with Maslach (1982a) who iden-tified a similar relationship between age andburnout. She attributed this relationship toyounger practitioners having less work ex-perience as well as life experience in terms
Third Quarter 1995 171
of maturity and stability. Similarly, Hardyand Hardy (1988) described the new profes-sionals as experiencing reality shock" uponentering a new job. They attributed this inpart to different role expectations betweeneducators and service administrators per-ceptions of their jobs. Number of clienthours reflects a potential overload of time,abilities, and responsibilities. In combina-tion with age, this result suggests that expe-rience and maturity might be a factor man-aging increased numbers of client hours.Conversely, a this result may suggest a rela-tionship between age and hours of clientcontact.
Implications and RecommendationsThe positive relationship between burn-
out and role stress, specifically role conflict,generates several implications for therapeu-tic recreation professionals in terms of prac-tice, education, and research. First, for prac-tice, inconsistencies need to be identifiedand addressed between actual role demandsby supervisors and the TRSs' perceived rolefactors such as goals and values. The consis-tency between job responsibilities and thetherapists' professional goals should be ex-amined. This may be accomplished by de-veloping structured meetings during whichsupervisors and therapists discuss yearlygoals and how they were or were not met.Additionally, issues of role conflict shouldbe the focus of professional developmentefforts within individual agencies. In-ser-vices and workshops could be arranged toallow staff to express feelings of inconsisten-cies between their expectations and valueswith those of the agency and supervisors.
Second, since younger TRSs seemed tobe more susceptible to burnout, the expec-tations of entry level practitioners should bemonitored to prevent possible role conflict.Educators who prepare college and univer-sity students should pay particular attentionto providing current and accurate informa-tion about expectations and potential expe-riences in practical settings. Providing a ros-
ier" picture than the one that actually existsor providing no picture" at all can contrib-ute to disillusionment and disappointmentas well as frustration for new practitioners.Agency supervisors can help represent thefield accurately by guest lecturing in collegeand university classes and interacting withinterns during the interview phase of job so-licitation. Additionally, educators and prac-titioners should be sure to establish andmaintain communication with each otherto facilitate a student's transition from aca-demic to professional environments.
Third, the low personal accomplishmentscores raise particular concerns. Causesleading to TRSs' feelings of low personal ac-complishment need to be investigated.Managers in therapeutic recreation shouldexplore the therapists' feelings of compe-tence and perceptions of barriers to successon the job. Methods to provide opportuni-ties for meeting both professional and per-sonal goals through the work environmentshould also be pursued.
In addition to implications for practiceand education, several implications for fur-ther research are suggested. One limitationof this study was the absence of an adequatenumber of subjects from each setting/ser-vice area to be considered in multivari-ate analysis. This prohibited comparisonswithin this particular variable. Future re-search should be conducted on a larger sam-ple with particular attention to variablessuch as settings/service areas to determinewhether specific areas are more susceptibleto burnout and role stress. Further study inthese areas may provide information thatcan enhance curriculum development thatcould be helpful in preparing students betterfor the transition from school to work.
Second, other factors not examined inthis study such as perceptions of stress caus-ing factors should be researched. Smith,Perry, Neumayer, Potter, and Smeal (1991)identified that both therapeutic recreationspecialists and occupational therapists havea low perception of the status of therapeutic
172 Therapeutic Recreation Journal
recreation in health care. The contributionof TRSs' perceptions of the influence andstatus of therapeutic recreation to levels ofburnout and role stress may yield additionalinsight to this line of study.
Third, non-traditional research approachesshould be considered for more in-depth pur-suit of specific issues raised by this studysuch as causes of negative perceptions re-garding personal accomplishment or factorscontributing to role conflict in TRSs. Quali-tative research approaches (i.e., in-depth in-terviewing, case studies, or participant ob-servation) might be useful in gleaning infor-mation not attainable through quantitativeapproaches.
Finally, longitudinal research might bewarranted to identify and examine those in-dividuals who either did not reply or werenot accessible to this study. It is likely thatTRSs who were burned out did not respondto this survey. Additionally, those individu-als who perhaps left the field of therapeuticrecreation due to burnout were not identi-fied as potential respondents. Longitudinalstudies that would follow new TRSs intoand through their jobs in therapeutic recre-ation have potential for tracking levels ofburnout in different stages of the profes-sional career of a therapeutic recreation spe-cialist.
Much more research as well as the testingof strategies to explore and ameliorate cur-rently identified problems of burnout androle stress are warranted. Therapeutic recre-ation specialists make up a significant partof the health care team. Understanding thenature and causes of burnout and role stresscan help initiate appropriate changes in thedelivery of therapeutic recreation services.Not only can these potential changes helpkeep professionals healthy and in the field,they in turn can contribuyr to quality healthcare delivery to all consumers.
References
Babbie, E. (1986). The practice of social research,(4th ed.). Belmont, CA: Wadsworth Publishing.
Brasile, F. M. (1992). Professional preparation:Reported needs for a profession in transition.Annual in Therapeutic Recreation 3, 58-71.
Carroll, J. F. X. & White, W. L. (1982). Theorybuilding: Integrating individual and environ-mental factors within an ecological frame-work. In W. S. Paine (Ed.). Job stress andburnout; Research, theory, and interventionperspectives, (pp. 41-60). Beverly Hills: SagePublications.
Coady, C. A., Kent, V. D., & Davis, P. W. (1990).Burnout among social workers working withpatients with cystic flbrosis. Health & SocialWork, 15(2), 116-124.
Cunningham, P. H. & Bartuska, T. (1989). Therelationship between stress and leisure satis-faction among therapeutic recreation person-nel. Therapeutic Recreation Journal, 23 (3),65-70.
Daily, R. C. (1990). Role perceptions and job ten-sion as predictors of nursing turnover. Nurs-ing Connections, 3 (2), 33-42.
Deckard, G. J. & Present, R. M. (1989). Impactof role stress on physical therapists' emotionaland physical well-being. Physical Therapy, 69,713-718.
Dillman, D. (1978). Mail and telephone surveys;The total design method. New York: John Wi-ley and Sons.
Firth, H., Phil, B., McKeown, P., Mclntee, J., &Britton, P. (1987). Professional depression,burnout" and personality in long stay nursing.International Journal of Nursing Studies, 24,227-237.
Grisby, D. W. & McKnew, M. A. (1988). Workstress burnout among paramedics. Psycholog-ical Reports, 63 (1), 55-64.
Hardy, M. E. & Hardy, W. L. (1988). Role stressand role strain. In M. E. Hardy & M. E. Con-way (Eds.). Role theory: Perspectives for healthprofessional s (pp. 159-239). Norwalk, CT:Appleton Thayer.
Holloway, D. & Wallinga, C. R. (1990). Burnoutin child life specialists: The relation of rolestress. Children's Health Care: Journal of theAssociation for the Care of Children's Health,19(1), 10-18.
Krejcie, R. V. & Morgan, D. W. (1970). Deter-mining sample size for research activities. Ed-ucational and Psychological Measures, 30,601-610.
Third Quarter 1995 173
Maslach, C. (1982a). The cost of caring. Engle-wood Cliffs, NJ: Prentice Hall.
Maslach, C. (1982b). Understanding burnout:Definitional issues in analyzing a complexphenomenon. In W. S. Paine (Ed.). Job stressand burnout: Research, theory, and interven-tion perspectives, (pp. 29-40). Beverly Hills:Sage Publications.
Maslach, C. & Jackson, S. E. (1981). The MaslachBurnout Inventory. Palo Alto, CA: ConsultingPsychologists Press.
Maslach, C. & Jackson, S. E. (1986). The MaslachBurnout Inventory. (2nd ed.). Palo Alto, CA:Consulting Psychologists Press.
Maulday, T. W. (1983). Burnout and health pro-fessionals: Manifestations and management.Norwalk, CT: Appleton-Century-Crofts.
McGrath, A., Reid, N., & Boore, J. (1989). Occu-pational stress in nursing. International Jour-nal of Nursing Studies, 26, 343-358.
Merton, R. K. (1976). Sociological ambivalenceand other essays. New York: The Free Press.
Pedhazur, E. J. (1982). Multiple regression in be-havioral research. Fort Worth: Harcourt,Brace, Jovanovich, College Publishers.
Perlman, B. & Hartman, E. A. (1982). Burnout:summary and future research. Human Re-lations, 35, 283-305.
Pines, A. & Aronson, E. (1988). Career burnout:Causes and cures. NY: Free Press.
Rizzo, J. R., House, R. J., & Lirtzman, S. I.(1970). Role conflict and ambiguity in com-plex organizations. Administrative SciencesQuarterly, 15, 150-163.
Schwab, R. L. & Iwanicki, E. F. (1982). Perceivedrole conflict and role ambiguity and teacher'sburnout. Educational Administration Quar-terly, 18, 60-74.
Siefert, K., Jayaratne, S., & Chess, W. A. (1991).Job satisfaction, burnout, and turnover inhealth care social workers. Health and SocialWork, 16, 193-202.
Smith, R. W., Perry, T. L., Neumayer, R. J., Pot-ter, J. S., & Smeal, T. M. (1992). Interprofes-sional perceptions between therapeutic recre-ation and occupational therapy practitioners:Barriers to effective interdisciplinary teamfunctioning. Therapeutic Recreation Journal,26, (4), 31-42.
Thompson, D. L. (1990). Burnout and role stressin therapeutic recreation specialists in healthcare settings. Unpublished manuscript.
Wade-Campbell, K. N. & Anderson, S. C. (1987).Perceived levels of burnout of Veteran Ad-ministration therapeutic recreation person-nel. Therapeutic Recreation Journal, 21 (3),52-63.
Williams, C. A. (1989). Empathy and burnout inmale and female helping professionals. Re-search in Nursing and Health, 12 (3), 169-178.
174 Therapeutic Recreation Journal