Embed Size (px)
Citation preview

THE RELATIONSHIP BETWEEN TEMPERATURE AND 911 MEDICAL DISPATCH
DATA FOR HEAT-RELATED ILLNESS IN TORONTO, 2002-2005:
AN APPLICATION OF SYNDROMIC SURVEILLANCE
by
Katherine L. Bassil
A thesis submitted in conformity with the requirements
for the degree of Doctor of Philosophy
Graduate Department of Public Health Sciences
University of Toronto
© Copyright by Katherine L. Bassil (2008)

ii
Abstract The Relationship Between Temperature and 911 Medical Dispatch Data for Heat-Related Illness
in Toronto, 2002-2005: An Application of Syndromic Surveillance
Thesis for the Degree of Doctor of Philosophy in Epidemiology
Graduate Department of Public Health Sciences
University of Toronto, 2008
Katherine L. Bassil
Heat-related illness (HRI) is of growing public health importance, particularly with
climate change and an anticipated increased frequency of heat waves. A syndromic surveillance
system for HRI could provide new information on the population impact of excessive heat and
thus be of value for public health planning. This study describes the association between 911
medical dispatch calls for HRI and temperature in Toronto, Ontario during the summers of 2002-
2005.
A combination of methodological approaches was used to understand both the temporal
trend and spatial pattern in the relationship between 911 medical dispatch data and temperature.
A case definition for HRI was developed using clinical and empirical assessments. Generalized
Additive Models (GAM) and Zero inflated Poisson regression (ZIP) were used to determine the
association between 911 calls and mean and maximum temperature. The validity of the HRI case
definition was investigated by making comparisons with emergency department visits for HRI.
Descriptive, aberration detection, and cross-correlation methods were applied to explore the
timing and volume of HRI calls in relation to these visits, and the declaration of heat alerts.

iii
Finally, the existence of neighbourhood level spatial variation in 911 calls for HRI was analyzed
using geospatial methods.
This is the first study to demonstrate an association between daily 911 medical dispatch
calls specifically for HRI and temperature. On average, 911 calls for HRI increased up to a
maximum of 36% (p<.0001) (median 29%) for each 1°C increase in temperature. The temporal
trend of 911 calls for HRI was similar to emergency department visits for HRI and heat alerts,
improving confidence in the validity of this data source. Heterogeneity in the spatial pattern of
calls across neighbourhoods was also apparent, with recreational areas near the waterfront
demonstrating the highest percentage increase in calls.
Monitoring 911 medical dispatch data for HRI could assist public health units carrying
out both temporal and geospatial surveillance, particularly in areas where synoptic based
mortality prediction algorithms are not being utilized. This previously untapped data source
should be further explored for its applications in understanding the relationship between heat and
human health and more appropriately targeting public health interventions.

iv
Acknowledgements There are several people I would like to extend my sincere gratitude to for their contributions to this thesis. To my supervisor, Dr. Donald Cole, for providing endless encouragement and support. His wise counsel and mentorship guided this doctoral work and have been an invaluable part of my academic training. To Dr. Rahim Moineddin, for his generosity of time and patience in supporting my statistical learning curve. To Drs. Elizabeth Rea and Wendy Lou for their enthusiasm and dedication as committee members. To my examiners, Drs. Scott Sheridan, Andrea Sass-Kortsak, Rick Glazier, and Pat O’Campo for their helpful comments and contributions to my thesis. To my wonderful colleagues at Toronto Public Health and Toronto Emergency Medical Services, without whom this collaborative work would not have been possible or nearly as enjoyable. My most heartfelt thanks goes to Brian, Mum, Dad, and James, to whom this thesis is dedicated.

v
Table of Contents Abstract ii Acknowledgements iv List of Tables vii List of Figures viii 1 Introduction 1 1.1 Purpose 1 1.2 Study Objectives 3 2 Review of the Literature 5 2.1 The Adverse Impacts of Heat on Human Health 5 2.1.1 Physiological Effects of Heat 5 2.1.2 Heat-Related Illness (HRI) 6 2.2 Epidemiological Studies of Heat and Health – Approaches and Challenges 8 2.2.1 Exposure Assessment 8 2.2.2 Outcome Assessment 11 2.2.3 Study Designs 13 2.3 Epidemiological Studies of Heat Health Impacts– Evidence 14 2.3.1 Mortality 14 2.3.2 Morbidity 15 2.3.3 Population Vulnerability to HRI 16 2.3.3.1 Physiologic 16 2.3.3.2 Socioeconomic 17 2.3.3.3 Geospatial 18 2.4 Surveillance for HRI 19 2.4.1 Heat Health Warning Systems (HHWS) 20 2.4.1.1 Toronto’s HHWS 22 2.4.2 Syndromic Surveillance 23 2.4.3 Geographic Information System Application to Surveillance 28 2.5 Chapter Summary 29 3 Methods and Approach 30 3.1 Study Design 30 3.2 Data Sources 30 3.2.1 Toronto EMS Dispatch System 31 3.2.2 Emergency Department Visits, National Ambulatory Care
Reporting System (NACRS) 36 3.2.3 Meteorological Data 38 3.2.4 Toronto Heat Health Warning System (HHWS) 38
3.3 Data Acquisition 39

vi
3.3.1 Partner Agencies 39 3.3.2 Institutional Reviews & Privacy Issues 39
3.4 Software 40 3.5 Data Preparation and Extraction 41 3.6 Data Interpretation and Analysis 42
3.6.1 Descriptive Analysis 43 3.6.2 Development of a Case Definition 43 3.6.3 Assessing the Relationship between Temperature and HRI 45 3.6.4 Validation and Timing Assessment 48 3.6.5 Geospatial Approach 50
4 Results 53
4.1 Descriptive Statistics 53 4.2 Study Objective 1a: Developing a Case Definition for HRI 56 4.3 Study Objective 1b: Time Series of the Relationship of 911 HRI Calls
and Temperature 66 4.4 Study Objective 2a: Validity Assessment 80 4.5 Study Objective 2b: Timing Assessment 88 4.6 Study Objective 3: Geospatial Distribution of HRI in Toronto 96
5 Discussion 106
5.1 Study Objective 1a: Developing a Case Definition for HRI 106 5.2 Study Objective 1b: Time Series of the Relationship of 911 HRI Calls
and Temperature 112 5.3 Study Objective 2a: Validity Assessment 116 5.4 Study Objective 2b: Timing Assessment 117 5.5 Study Objective 3: Geospatial Distribution of HRI in Toronto 118 5.6 Study Limitations 121 5.7 Future Research 123 5.8 Contributions of this Research 126 5.9 Conclusions 127
References 129 Appendices 155 Appendix A: Summary of epidemiological studies of the relationship between heat and mortality Appendix B: Influencing factors and underlying assumptions in the 911 call process for HRI Appendix C: Heat alerts and extreme heat alerts, Toronto, 2002-2005 Appendix D: 911 MPDS determinants potentially representing HRI Appendix E: Comparison of different smoothers for GAM models Appendix F: Percentage of heat-related calls and mean daily temperature by determinant grouping, 2002-2005 (June 1-August 31) Appendix G: Investigation of associations between different spike thresholds for 911 calls and emergency department (ED) visits and public health heat alert notifications (based on synoptic weather system mortality projections)

vii
List of Tables
3.1 Data variables from the 911 EMS database 35
3.2 ICD-10-CA codes used in construction as the case definition of HRI for ED visits 37
4.1 Descriptive meteorological statistics by summer, Toronto 2002-2005 55
4.2 Correlations between daily % 911 calls for HRI and mean temperature for
selected determinant groupings 61
4.3 Correlation between daily % 911 calls for HRI and mean and maximum
temperatures for selected individual determinants 64
4.4 911 determinants used in construction of the case definition of HRI 66
4.5 Descriptive 911 call statistics by summer, Toronto 2002-2005 67
4.6 Number of total calls for heat-related illness occurring on days with a
maximum temperature above or below 28°C 71
4.7 Number of total calls for heat-related illness occurring on days with a
mean temperature above or below 24°C 71
4.8 Regression analyses associating daily meteorological variables and the
proportion of HRI among all ambulance emergency calls 73
4.9 Regression analyses associating the interaction between temperature and relative
humidity with the proportion of HRI among all ambulance emergency calls 75
4.10 Comparison of BIC and AIC values between models with and without the
interaction term (relative humidity and mean or maximum temperature) 77
4.11 Regression analyses associating daily meteorological variables and the
proportion of HRI among all ambulance emergency calls with a 1 day lag 78
4.12 Descriptive emergency department visit statistics by summer,
Toronto 2002-2005 81
4.13 Regression analyses associating daily meteorological variables and the proportion
of HRI among all emergency room visits 82
4.14 Comparisons of classifications of days with excess HRI by different systems,
across all four summers 87

viii
List of Figures 2.1 Heat-related illness pyramid of health effects 7
3.1 MPDS code categorization process 32
4.1 All daily 911 emergency calls, Toronto 2002-2005 (June 1- August 31) 54
4.2 911 call “determinant” selection summary – focus groups 56
4.3 Percentage of heat-related calls and mean daily temperature by determinant,
2002-2005 (June 1-August 31) 58
4.4 Proportion of heat-related calls among total calls graphed co-temporaneously
with maximum daily temperature, 2002-2005 (June 1-August 31) 68
4.5 Heat-Related Illness, 911 calls, emergency room visits, and heat alert days,
by summer, Toronto 2002-2005 84
4.6 Receiver Operating Curve (ROC) plot of 911 and NACRS thresholds
vs. heat alerts 87
4.7 Output from EARS analysis of aberrations for 911 and ED HRI visits 89
4.8 Cross-correlation between 911 and NACRS data – All summers 93
4.9 Cross-correlation between 911 and NACRS data – Individual study summers 94
4.10 Percentage of 911 calls for HRI by neighbourhood 98
4.11 Mean percentage of 911 HRI calls for Toronto summers, 2002-2005 102
4.12 Spatial autocorrelation: Moran’s I and significance map 103
4.13 Low-income families (number of families under Low Income Cut-Off (LICO)
as a percentage of all economic families (2001) 105

1
Chapter 1
Introduction 1.1 Purpose
Exposure to extreme heat is associated with a diverse range of adverse health effects,
ranging from non-specific and specific symptoms to excess mortality, all of which fall under the
broad umbrella of “heat-related illness” (HRI). Although these effects are most marked in
vulnerable populations like the elderly and socially isolated, everyone is at risk to a varying
extent. The impact of heat on health was clearly evident during and following the Chicago heat
wave in 1995, which resulted in over 700 excess deaths1, and, more recently, the heat waves in
Europe in 2003, which resulted in over 70,000 heat-related deaths.2 These negative impacts of
heat on health continue to be a persistent concern. They are expected to become even more
pressing in the future with predicted meteorological changes linked to climate change, as
outlined in the recent IPCC (Intergovernmental Panel on Climate Change) report.3 Of particular
concern for North America are the additional risks associated with rapid urbanization and the
growing population over the age of 65. As Baby Boomers join the ranks of the elderly, the
segment of the population most at risk of the effects of heat, health impacts will most likely
increase.4
Thus, mitigating negative health impacts is an important task for public health
practitioners. Practitioners are faced with the challenge of developing and implementing
effective interventions to address both the immediate effects of heat and to devise longer-term

2
strategies to mitigate future heat events. One of the emerging priorities that has been
recommended is the development of syndromic surveillance systems for the monitoring of
environmental health conditions. A syndromic surveillance system that is able to provide
information of populations at risk and quantify health impacts has the potential to facilitate the
development and implementation of targeted public health interventions, and thus reduce
associated morbidity and mortality. However, a challenge in developing these systems is
determining the most appropriate data source to provide morbidity information. One of the
recommendations from the evaluation of the syndromic surveillance network implemented in
Toronto during World Youth Day in 2002 was to further explore the potential of 911 medical
dispatch data for on-going public health surveillance.5
Despite recommendations to explore 911 medical dispatch data as a syndromic
surveillance data source, very limited work has been conducted to date, particularly in Canada.
The majority of the research so far has been conducted in New York City and in parts of Europe,
primarily for influenza-like-illness.6-8 A few studies of medical dispatch data have considered
increases in all calls with high temperatures and the results have been very promising.9, 10
This study builds on previous work and is a direct response to recommendations to
develop surveillance for heat-related conditions; thus it is timely and highly relevant to current
public health system priorities. This research used a combination of methodological approaches
to understand both temporal trends and spatial patterns in the relationship between 911 medical
dispatch data and temperature in Toronto.

3
1.2 Study Objectives
The purpose of this research can be divided into three key study objectives, each with its
own a priori hypothesis.
Study Objective 1
a) To develop a case definition for HRI by examining temporal trends with temperature
measures of a variety of combinations of 911 call determinants and sub-groupings, varying in
specificity.
b) To make comparisons of daily temporal trends in HRI with temperature measures (mean
and maximum) using time series analysis across four summers in Toronto using the HRI case
definition.
The a priori hypothesis is that HRI 911 calls will follow a similar temporal pattern with
temperature, and more specific codes will co-vary more strongly with temperature indicators
than less specific codes. Further, there will be stronger positive correlations for 911 call
determinants which represent: greater recognition, labeling or occurrence of HRI per se;
aggravation of pre-existing conditions; and de-compensation of already vulnerable individuals.
Study Objective 2
a) To assess the validity of the HRI case definition using 911 determinants by making
comparisons with data on emergency department visits for HRI during the same time period.

4
b) To explore the timing and volume of HRI calls in relation to visits to emergency departments
for HRI, and declaration of heat alerts (i.e. based on an algorithm of predicted excess mortality)
using descriptive, aberration detection, and cross-correlation methods.
Given the broad spectrum of HRI, it is anticipated a priori that 911 calls for HRI, which
capture morbidity data, will peak earlier than current alerts based on predicted mortality. The
temporal trend of emergency visits and 911 calls for HRI will likely be similar given they both
represent morbidity.
Study Objective 3
a) To investigate the existence of neighbourhood level spatial variation of 911 calls for HRI.
The a priori hypothesis is that there will be heterogeneity in the burden of 911 calls for
HRI between different neighbourhoods. This variability will flag “hot spots” where further
investigation of relevant factors can occur and public health resources can be appropriately
directed.

5
Chapter 2
Review of the Literature 2.1 The Adverse Impacts of Heat on Human Health
The dramatic effect of heat on human health was clearly demonstrated during recent
major heat waves including Chicago in 1995, the North American mid-west in 1999, and across
Europe in 2003, which together have resulted in thousands of excess deaths.1, 2, 11 In Toronto
alone, it has been estimated that there are currently approximately 120 heat-related deaths per
year.12 There is mounting evidence to suggest that these negative impacts will increase with
climate change. Warmer climates are expected to result in higher summer temperatures and more
dramatic fluctuations, which will result in more frequent, longer duration, and more intense heat
waves with their associated health risks.13-15 In Canadian cities, heat-related mortality is
predicted to double by 2050, and triple by 2080.16 Increasing urbanization and a rapidly ageing
population are expected to exacerbate these effects. This potentially growing attributable health
burden has led to a growing body of research examining the relationship between heat and
human health.
2.1.1 Physiological Effects of Heat
The human body uses several mechanisms to maintain a healthy core body temperature
close to 37°C at rest, in a process called thermoregulation.17-19 These mechanisms attempt to
balance the amount of heat produced by the body as a result of metabolic activity and gained

6
from the external environment, with the amount lost. Methods of thermoregulation include sweat
production to lose heat from the skin and cutaneous vasodilation which increases blood flow to
transport heat from the body core to the skin and then to the surrounding environment.20-22
However, during excessive levels of heat stress (e.g. overall heat burden on the body) these
mechanisms may be overwhelmed and no longer be capable of effectively dissipating heat,
resulting in excess heat production and increased body temperature.19, 23 Consequently, heat-
related illness may result.17, 19-23
2.1.2 Heat-Related Illness (HRI)
Heat-related illness (HRI) refers to a broad clinical spectrum that ranges from mild
symptoms through heat exhaustion to more serious illnesses including heat stroke. Although
there is not a universal definition for HRI, it is typically classified according to increasing
degrees of severity. Mild symptoms may include cramps, fatigue, and weakness that are
generally not life threatening.20, 23 Heat exhaustion and heat stroke are more serious
manifestations of HRI. The former is characterized by intense thirst, heavy sweating, headache,
dizziness, weakness, nausea and vomiting. The latter is generally defined by fever, severe
headache, confusion, and red, hot, and dry skin.24 Heatstroke can result in complications
including kidney, liver, and brain damage, and ultimately death.17, 19, 23, 25, 26 There is evidence to
suggest that survivors of HRI may experience subsequent functional impairment up to 1 and 2
years after the HRI episode.27 While the case-fatality ratio is uncertain, a recent study suggests
an approximate mortality rate of 30% for all cases of HRI presenting to an emergency
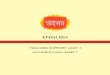
department.28 Figure 2.1 illustrates the range of HRI severity in relation to the proportion of the
population affected and the kinds of health-seeking practices employed.

7
Figure 2.1: Heat-Related Illness Pyramid of Health Effects
Adapted from sources29, 30
Aside from HRI, high ambient temperatures have been associated with increased
violence,31 suicide,32 and psychiatric emergencies.33-35 Heat can aggravate pre-existing
conditions, particularly chronic cardiovascular and respiratory disorders by placing excess stress
on already strained bodily systems. Exacerbations of other conditions, like diabetes is an
additional risk.36 There is also evidence to suggest that serious adverse drug reactions are higher
during heat waves, particularly in the elderly.37 Thus, extreme heat has a broad range of adverse
effects on health.
Mortality
Mild symptoms, discomfort, subtle effects
Heat cramps, heat exhaustion, heat stroke; Aggravation of pre-existing conditions
Medical seeking behaviour: ER, physicians office, 911,
Telehealth, clinic
Hospital admission
Proportion of Population
Severity of Effect

8
2.2 Epidemiological Studies of Heat and Health – Approaches and
Challenges
In critically reviewing evidence from the epidemiological literature on heat and health it
is necessary to first understand challenges inherent in the methods and study designs, particularly
with regards to exposure and outcome assessment.
2.2.1 Exposure Assessment
A key methodological challenge in epidemiological studies of the effect of heat on
human health is assessing exposure. Two approaches are commonly used. The first is defining a
specific period of high temperature, often termed a “heat wave”, and then analyzing health
outcomes in heat wave versus non-heat wave conditions. The occurrence of several heat waves
in recent years has provided the opportunity to conduct such studies.11, 38-46 However, a number
of different terms are used in the literature to define a time period of high ambient temperature
including: heat event, heat episode, heat wave, heat stress, hot weather, heat period, and
excessive weather. Furthermore, heat waves are rare events and no two are the same; they differ
in both magnitude and impact depending on characteristics of the population. These
inconsistencies in terminology and inherent variability in episodes make between study
comparisons difficult.
A second approach is to assign exposure using meteorological variables. These include
minimum, mean, maximum, dew point temperature, and apparent temperature. Other researchers
create an index using a combination of these variables including humidity such as Humidex. The
synoptic measure and energy balance models also incorporate additional meteorological as well

9
as physiological variables to assess the impact of heat on the human body. These daily
meteorological variables or indices can then be applied in a time series approach thereby
overcoming some of the problems associated with comparing heat event periods, such as
uncertain baselines. However, using temperature measures assumes that everyone in a specified
geographic area experiences the same exposure. This is not the case particularly given variations
in temperature within the urban environment due to the urban heat island effect, and differences
in individual susceptibility and adaptive behaviours such as the use of air conditioning.
Nevertheless, temperature measurements have been deemed to be the strongest determinant of
variation over time in population exposures to heat.47
There is a lack of consensus regarding the most appropriate temperature measure to use
in research on heat and health. It has been suggested that daily mean temperature is the most
suitable meteorological variable to assess heat exposure because it incorporates the impact of
high night-time temperatures (minimum temperature). Reflection of overnight periods of
persistent heat or relief may provide a more complete picture of heat exposure.48-50 On the other
hand, the use of daily mean temperature may mask the effect of large peaks in temperature that
are captured by measures of maximum temperature.51 It seems reasonable that the most
appropriate measure of exposure will be influenced by factors specific to the geographic area and
population under study. Consequently, both mean and maximum temperatures are used as
measures of heat exposure in the epidemiological literature.
The timing of high temperatures within a season must also be considered in
epidemiological studies of impacts of heat on health. Hot days occurring early in the season

10
typically have a larger effect than those occurring later on because the affected population has
not had the opportunity to acclimatize to the changed conditions.49 Prolonged periods of high
temperatures have a stronger impact on health compared with periods with extreme peak values
but shorter duration and lower mean.50, 52-54 This is thought to be due to the fact that the
population does not have the opportunity to have relief from the heat, for example, when
overnight temperatures drop.
An additional challenge in assessing exposure in epidemiological studies is in taking into
consideration the possible influence of other meteorological variables, including relative
humidity, and air pollutant indicators, including smog-related pollutants such as ozone. Studies
regarding the relationships among air pollutant levels, temperature, and mortality have produced
conflicting results. High temperatures have been associated with poor air quality, specifically
increased smog in urban environments. This is primarily a result of increases in ozone, a
photochemically induced air pollutant which is formed rapidly under warm and sunny conditions
and which is the primary contributor to smog. Heat and poor air quality both carry their own
burden of illness and are associated with increased mortality. For example, in Toronto it has been
estimated that on average from 1954 to 2000, of the acute deaths that occurred annually
approximately 120 were heat-related and 822 related to air-pollution.12, 16 This effect may be
independent, or the result of the interaction between high temperatures and air pollutants to
produce a combined effect on mortality that is greater than each factor acting alone.47, 51, 55-59 It is
uncertain whether air pollutants are confounders, effect modifiers, or unimportant covariates in
examinations of the effects of temperature on mortality.47, 60, 61 However, it is important to

11
consider the possible combined effects of heat and smog on human health as they have
implications for the delivery of public health interventions for both.
The influence of relative humidity on the relationship between heat and health is also
unclear. One might expect that high relative humidity would enhance the health impacts of hot
weather because it reduces the evaporation of sweat and in this way, impairs body cooling
mechanisms. This relationship is supported by some studies.62 However, others have found no
clear influence of humidity on health outcomes.63-65 Some suggest that the effects of heat are
actually diminished, as opposed to increased, by humid weather.66 There is high variability in the
literature of the role played by relative humidity, and this role is likely influenced by local
weather conditions.
2.2.2 Outcome Assessment
There are also challenges in measuring outcomes in the heat/health literature. The vast
majority of the research on the effect of heat on health considers mortality measures. However,
determining the method for attributing deaths to heat is a key challenge. Two approaches are
commonly used: measuring mortality specific to heat-related causes, and measuring “excess
mortality”.
Although there are advantages to measuring mortality specifically due to heat, this
measure is subject to misclassification. Several studies have shown that deaths from heat-related
causes are underreported in mortality statistics. A heat wave in Athens in 1987 resulted in
approximately 900 deaths classified as heat-related. However, the attributable excess mortality

12
was estimated to be more than 2000.56 In general, although heat may contribute to death it is
often not listed on the death certificate unless it is considered the underlying cause of death.47, 67
For example, a study that counted deaths in which hyperthermia was listed as a contributing
factor on the death certificate, but not the underlying cause, revealed that these deaths increased
the number of heat-related deaths by 54%.68 Furthermore, in the cases of isolated elderly who
are found days after they have died, it is difficult to attribute death to heat as it must be assigned
at the point of death. The lack of widely accepted systematic criteria for determining a heat-
related death also create outcome definition challenges.47
Given these challenges in attributing deaths to heat-related causes and wanting to more
broadly capture aggravation of pre-existing conditions, researchers have often used measures of
“excess mortality”.22 Excess mortality is calculated by subtracting the expected mortality from
what is observed, using a variety of methods including moving averages and averages from
similar time periods in previous years.69 One of the advantages of this indicator is that it captures
a broader set of deaths that may be caused by heat, such as those due to exacerbations of
cardiovascular and respiratory conditions.
The potential effect of “harvesting” must also be considered in measuring mortality due
to heat. This phenomenon refers to a mortality displacement effect whereby deaths that would
have occurred anyway, are brought forward as a result of triggering or exacerbating medical
conditions that can be exacerbated by the heat (e.g. cardiovascular). Evidence to support such an
effect can be seen in the lower than expected mortality that sometimes occurs immediately
following a heat episode.70 Most studies suggest that this mortality displacement is quite brief. 41,

13
64, 66, 71A large multi-city lag model in the United States suggests that this lag effect is usually
restricted to bringing deaths ahead by one day and that the impact of heat on mortality is usually
at lag 0 (i.e. the same day).63, 64 A study of the impact of harvesting among the elderly in Italy
during the 2003 European heat waves found a correlation between excess mortality and
maximum temperature for a slightly longer time period, of the three preceding days.41 Robust
methods to quantify the mortality displacement effect have not yet been developed, so the issue
of “harvesting” has yet to be resolved.70
Morbidity is a less commonly studied outcome in heat studies. Data on non-fatal heat
health outcomes are not routinely collected making these studies more difficult. Of the available
data sources, the most frequently used are hospital admissions. Similar methodological
challenges apply to morbidity studies, particularly the lack of a universal case definition of
HRI.72, 73 As a result, morbidity studies typically include measurements of all hospital
admissions, rather than specific diagnoses. The development of case definitions for HRI based
on different health services data would improve methods and the ability to make between-study
comparisons.
2.2.3 Study Designs
Several study designs are used to assess the effects of heat on health. Descriptive studies
include comparisons of mortality or morbidity counts before and after a major heat event. While
these provide useful information, analytical techniques including time series are increasingly
being used to quantify the association between temperature and health outcomes. The time series
approach is an efficient design for examining the temperature-mortality/morbidity relationship

14
for populations over a substantial period of time.47 Temperature measurements collected at
consecutive intervals over time (e.g. daily) and health outcome counts or rates are used as the
variables of interest. Potentially confounding factors usually include air pollutant information
and other meteorological variables. Finally, geospatial approaches are starting to be applied to
describe the geospatial burden of illness due to heat. These range from descriptive maps to
cluster detection techniques that can highlight “hot spots” or areas with a disproportionate
burden of illness where public health interventions should be targeted.10, 74-79
2.3 Epidemiological Studies of Heat and Health Impacts – Evidence
2.3.1 Mortality
There is a strong relationship between extreme temperatures and mortality. This
relationship is often described as a V- or U-shaped curve, with increased mortality at both low
and high temperature extremes.66, 80 Appendix A summarizes some of the key studies of the
impacts of heat on mortality; all demonstrate a positive association between heat and mortality of
varying magnitudes.35, 41, 43-45, 48, 49, 51, 80-87 The majority of these studies consider excess
mortality, usually compared before and after a major heat event. However, there is also research
that examines mortality in relation to daily time series of temperature. A range of increased
mortality for each degree increase in temperature is apparent in the research, varying from 1 or
2% to higher values of 35%. In studies that have looked at mortality due to specific causes, the
greatest increases are seen in deaths due to respiratory and cardiovascular causes.45, 51, 86
Furthermore, mortality is typically greatest in elderly age groups.43, 48, 80

15
2.3.2 Morbidity
Few studies have investigated the impact of heat on morbidity. Of those that have, the
majority consider increases in emergency hospital admissions during heat waves. During the
1995 Chicago heat wave, emergency hospital admissions increased by 11% in total, and by 35%
in the over 65 age group.88 Increases in hospital admissions were also evident during the 2003
heat waves across Europe. A 16% increase in admissions in those over 75 was detected in
London.43 In Spain, during this time, approximately 40% of admissions were identified as heat-
related. France, which was the most severely affected, also experienced large increases in
hospital admissions. One hospital in Paris reported 2600 excess emergency department visits and
1900 excess hospital admissions in August alone.89
There is a contrast between the evidence reported in morbidity and mortality studies.
Overall, the increases in hospital admissions during heat events are smaller in magnitude than
excess mortality.90, 91 A time series analysis of daily emergency hospital admissions in the UK
between 1994-2000 found no clear evidence of an association between elevated temperature and
increased admissions.90 This was in marked contrast to other research by this group that found a
3% increase in all-cause mortality in London for every 1 degree increase in temperature above
21.5°C.49 This phenomenon is further supported by evidence from the 1995 heat wave in
Chicago where all-cause mortality increased by 147% and hospital admissions only by 11%.91
Further evidence includes the consistently reported excess of deaths due to cardiovascular
disease during heat waves, but lack of such increases in morbidity studies.92 This suggests that
people who die during heat waves are not reaching the attention of medical services either
because they die quickly, live alone, or due to some other reason do not reach medical care.69, 93

16
This has important implications for prevention, including the need for surveillance to detect HRI
before it advances to severe fatal outcomes, and to identify vulnerable groups quickly.93, 94
2.3.3 Population Vulnerability to HRI
Although the risk of HRI exists for everyone, the effect of heat on health is not
experienced equally among all members of the population. Vulnerability is influenced by
physiological, socioeconomic, and geospatial factors. It is important to note the distinction
between this kind of population vulnerability versus that experienced by other at-risk
populations. In addition to the vulnerable groups described below, otherwise healthy individuals
are also at-risk of the effects of heat in situations of excess exposure or physical exertion (e.g.
recreational, occupational).
2.3.3.1 Physiologic
There is substantial evidence to suggest that heat-related mortality is greatest among high
risk groups like the elderly, infants and young children, and people with pre-existing illness. 20, 35,
80, 95
It has been suggested that the effect of heat on health varies considerably with age, and
that this is primarily related to the pathophysiology of HRI.35, 36, 96, 97 Infants and young children
have a greater body surface area-to-mass ratio compared to adults, thus providing a greater
surface for heat gain.98 They are also at an increased risk of dehydration and therefore heat stress
due to the relative higher volume of fluid in their bodies compared to an adult.70 In addition, they
have less efficient cooling mechanisms when compared with adults, lessening their ability to

17
dissipate body heat. However, a substantial proportion of the reported heat-related deaths in
children are the result of being left in cars on hot days.
Elderly populations, particularly those over the age of 65, have a weaker
thermoregulatory system and impaired kidney function, making them particularly susceptible to
the effects of heat.41, 81, 99, 100 They may be unable to increase their cardiac output sufficiently
during very hot weather. Furthermore, sweating efficiency decreases with age. The elderly are
also more likely to have a pre-existing chronic condition or be taking medications that interfere
with normal functioning of the thermoregulatory system, another risk-factor for mortality from
heat.27, 35, 72, 97, 101, 102 Consequently, they may not be as aware that they are becoming ill because
of high temperatures, and therefore not take action to reduce exposure. The highest death rates
from HRI are typically seen in the elderly and in particular, in those that have a pre-existing
chronic disease, and a lack of mobility.99 This was evident during the 1995 Chicago heat wave
where heat-related mortality increased with age, ranging from 3 per 100,000 for individuals
under 55 years of age, to 258 per 100,000 for those over 84.1 Studies of the elderly in institutions
also support these findings; this population is likely to be particularly frail, and some of these
institutions, particularly in northern Europe, may not have access to air-conditioning.27, 35 In
France, death rates in nursing homes doubled during the heat-wave in 2003.
2.3.3.2 Socioeconomic
A socioeconomic gradient for heat-related mortality has been suggested. Some studies
report that individuals of lower socioeconomic status (SES) are at an increased risk of mortality
from HRI.39 There are a few plausible reasons for this association. One of the strongest

18
protective factors of heat-related mortality that has been cited is access to air conditioning.103
However, individuals from lower SES backgrounds do not have the same access to air
conditioners, and even in circumstances where air conditioners have been provided, these
individuals cannot necessarily afford the maintenance and utility fees. Individuals of low SES are
also more likely to live in impoverished neighbourhoods, in poor quality housing, that exacerbate
the impacts of high ambient temperatures. 36, 104, 105 They may also be more likely to have a
higher prevalence of chronic diseases than are exacerbated in hot weather. Living conditions and
social networks also contribute to overall vulnerability to extreme temperature. Living alone,
being confined to a bed, and not leaving home daily have been associated with increased risk.39,
103 It is also plausible that the marginally housed/homeless have a greater exposure to
environmental hazards, making them particularly vulnerable.
2.3.3.3 Geospatial
There is geospatial heterogeneity in the impacts of heat. The effects of heat appear to be
greater in urban than in rural populations.46, 56 Urban settings typically include high-rise
apartments and people residing on the top floors, who are at greater risk of heat exposure.20, 99
Cities with older structures, typically multi-family, brick dwellings with poor ventilation and a
high heat load, are especially at risk. High settlement density, sparse vegetation, and limited open
space in a neighbourhood have been significantly correlated with greater human heat stress.106
Further, the urban environment may also contain a larger proportion of people of lower
socioeconomic status as compared with more rural regions, who are at greater risk. People living
in high crime areas may be more vulnerable because they are afraid to leave their window open

19
at night, which would increase indoor air circulation.107 However, it is the urban heat island
effect that greatly contributes to the particular risk of the urban environment.
Urban heat islands are metropolitan areas that are significantly warmer than their
surroundings due to a combination of factors that may include the presence of large expanses of
concrete, intensive use of asphalt, and other diverse construction materials that retain heat.108
Urban heating is largely attributed to excess heat absorbed and released from urban
infrastructure, such as buildings, streets, and parking lots.109 In fact, in major urban regions, the
increase in temperature in these urban heat islands has been recorded up to 11ºC warmer than
surrounding areas.110 In Toronto, efforts are being made to quantify this impact and identify
urban heat island locations, through the use of remote sensing technologies in an initiative led by
Natural Resources Canada (personal communication, David Mate, Scientific Communications
Officer, Natural Resources Canada).
There are clearly a variety of factors that influence an individual’s vulnerability to the
harmful effects of heat. Public health surveillance is an important tool that can be used to detect
and monitor HRI in the community as a whole, as well as these vulnerable groups, so that
interventions can be initiated and appropriately targeted.
2.4 Surveillance for HRI
The limitations of existing surveillance for HRI were clearly demonstrated during the
heat wave in 2003 in France, one of the countries where the effects were most extreme. It was
nearly a week after substantial impacts on mortality had developed that an official public health

20
response was started.111, 112 This has been largely attributed to the lack of a warning system to
trigger the implementation of public health action. A retrospective assessment found that there
had been an excess of approximately 3,900 deaths at the time when only 10 specific deaths had
been reported during the episode.113 In response, many cities and countries have implemented
heat health warning systems.
2.4.1 Heat Health Warning Systems (HHWS)
A HHWS is an early warning system for heat events that is designed to alert the population
and relevant authorities in advance about developing adverse meteorological conditions, and then
to implement effective measures that are designed to reduce adverse health outcomes during and
after the events.113 Several necessary components of HHWS systems include:114
• Reliable and valid meteorological forecasts for the region and population of interest
• Robust understanding of the cause-and-effect relationships between the thermal
environment and health outcomes at the population level, including the evidence-based
identification of “high risk” meteorological conditions to activate and deactivate the
response activities
• Effective response measures to implement within the window of lead-time provided by
the warning
• The involvement of institutions that have sufficient resources, capacity, and knowledge to
undertake the specific response measures

21
HHWS are typically implemented at the municipal (or, in Europe, national) level. As a result,
they often vary in the structure, stakeholder agencies, and associated interventions implemented.
One of the advantages of location-based approaches is that interventions can be tailored to the
specific population. However, the downside is that if local levels each create their own criteria
and method they may not be taking advantage of existing knowledge and previous work. To
address these challenges, some systems, like the synoptic approach developed by Kalkstein and
colleagues, use standard criteria for defining air masses, but the heat warning criteria for each
locale are based on their own unique historical heat/mortality relationships.60, 108, 115 This system
is currently used in several European countries that are linked to national systems in this way. In
addition, the US National Weather Service is currently developing a national HHWS (personal
communication, Larry Kalkstein, Director of the Center for Climatic Research, University of
Miami).
Surprisingly few countries and cities have a HHWS, although the numbers have increased
since the 1995 heat wave in Chicago and the 2003 heat waves in Europe. A recent survey of 45
countries in Europe found that 15 had a HHWS in operation.22 Toronto, Montreal, Philadelphia,
Shanghai, France, Portugal, Italy, Germany, Phoenix, and Dayton, Ohio are among those that do
have a HHWS in place. These systems use different approaches for determining thresholds for
action, including Humidex, apparent temperature, and the synoptic classification method. A
synoptic approach considers a number of meteorological conditions including air temperature,
dew point temperature, visibility, cloud cover, wind speed, and wind direction, to group
conditions into air mass types.60, 108, 115 Certain air masses are linked to higher mortality so that it
is possible to predict the likelihood of excess mortality based on the predicted arrival of an

22
offensive air mass categorized with local weather forecast data. In this way, the synoptic
approach recognizes the fact that people respond to the total effect of all weather variables
interacting simultaneously on the body.108
2.4.1.1 Toronto’s HHWS
The HHWS in Toronto is based on the synoptic classification approach. It was developed
in 2000 in collaboration with the Toronto Atmospheric Fund and researchers at Kent State
University. The HHWS was developed using 46 years of meteorological data and 17 years of
daily mortality counts for May 1st through September 30th (personal communication, Nancy Day,
Epidemiologist, Toronto Public Health). Environment Canada sends meteorological information
to the system, which is housed at Kent State University. A “heat alert” is called when an
oppressive air mass is forecast and the likelihood of excess mortality exceeds 65%. An “extreme
heat alert” is declared when this likelihood is 90%. The system is checked by Toronto Public
Health staff four times a day on a password-protected website (personal communication, Elaine
Pacheco, Manager, Hot Weather Response Plan, Toronto Public Health).
When a heat alert or extreme heat alert is declared, a number of interventions are initiated
through the Hot Weather Response Plan. These include mass media broadcast messages, opening
of cooling centres, and distribution of water by the Canadian Red Cross. The hours of
community organizations like libraries and pools are extended.116 Over 800 partner agencies are
contacted so that they can advise vulnerable populations that they work with of precautions to
take (personal communication, Marco Vittiglio, Manager, Emergency Planning and
Preparedness, Toronto Public Health).

23
While HHWS are invaluable for initiating a timely public health response, many do not
include health indicator data and of those that do, they are typically based on predicted excess
mortality, like the synoptic approach used in Toronto. Incorporating morbidity syndromes into
routine public health monitoring through syndromic surveillance systems is a rapidly developing
field.
2.4.2 Syndromic Surveillance
The practice of public health surveillance is changing to address new and emerging
diseases as well as take advantage of the increasing availability of routinely collected electronic
health-related data.117 New approaches to surveillance are being explored to complement, rather
than replace, traditional surveillance. One of these approaches is syndromic surveillance, a new
and quickly developing method in epidemiological surveillance. Although initially driven in the
USA by potential bioterrorism threats, syndromic surveillance systems have increasingly been
applied to the early detection of new and re-emerging diseases, and more recently, to
environmental health problems.118
Syndromic surveillance traditionally uses health-related data that precede diagnosis to
signal occurrence of a case or cluster of illness.119-121 Routinely collected electronic data, such as
clinical, administrative, or pharmacy, are extracted and analyzed by automated systems, typically
on a daily basis. The reliance on pre-existing data streams is important as these health systems do
not require the development of new datasets but rather make use of available data. This system
generates an alert when the number of cases meeting a syndrome definition exceeds what is
expected based on historical data. In this way, near real-time analysis is provided. For many

24
diseases, the effectiveness of an intervention is linked to the rapidity of detection; the timeliness
of syndromic surveillance represents its true potential benefit as appropriate public health action
can be initiated before confirmation by a laboratory or more extensive clinical diagnosis.
Aside from the ability to detect infectious disease in the early stage of an outbreak,
syndromic surveillance systems are being recognized for their potential to provide enhanced
“situational awareness”.122 Public health practitioners can use syndromic surveillance systems to
get a picture of the health status of the community in near real-time by monitoring a number of
syndromes. Areas with a higher burden of illness can be targeted for delivery of public health
interventions. This is of great value to clinicians and public health practitioners, particularly in
terms of organizing and retaining resources.
While there have been significant advances, the area of syndromic surveillance is still
very much in its infancy and much remains unknown regarding its effectiveness. Important
research needs include: understanding which is the most appropriate data source (or combination
of sources), developing valid approaches to classifying symptoms into syndrome categories,
assessing appropriate analytical methods, and determining thresholds for public health action.
There are several data streams that are currently being explored as potential sources for
syndromic surveillance systems. The most commonly studied are emergency department visits,
coded by chief complaint or ICD (International Statistical Classification of Diseases) codes.123-126
Other data sources under evaluation include:
- pharmacy over-the-counter sales127-130

25
- school/workplace absenteeism 124, 131
- physician/clinic visits124, 132
- insurance/Health Maintenance Organization claim data133, 134
- nurse-led help lines like Ontario Telehealth126, 135 and National Health Service Direct in
the UK112, 136-140
- 911 medical dispatch data6-8
In Toronto during World Youth Day in 2002, a syndromic surveillance network was
implemented that included monitoring of most of these aforementioned data sources. The
information captured by the surveillance network was used to detect potential infectious disease
outbreaks as well as target interventions and medical assistance for other syndromes, including
environmental-related conditions. Of these data sources and syndromes, it was suggested that
monitoring of 911 medical dispatch data holds significant potential for on-going public health
surveillance in the near future, particularly for HRI, and further exploration of this source was
strongly recommended.5
There are several features of 911 medical dispatch data that make it a suitable source for
syndromic surveillance systems. 911 call records include at least some information about the
caller, location, and category of health complaint. Data are entered in real-time into a
computerized database, with a single record created for each call. The automated nature of the
system facilitates a timely and relatively simple method of transferring the data for analysis
either continuously or in discrete time intervals. Further, methods developed with 911 data can

26
be reproduced with comparable emergency medical services data systems and implemented at
minimal cost.
One of the greatest features of 911 data is the detailed geospatial information available for
each record. Each call has an associated latitude and longitude, recorded at the location of the
caller where they have become ill. This differs from other traditional health databases that do
provide geospatial information, but this is typically residential address. By capturing geospatial
details at the point of illness, information regarding environmental exposures can be monitored.
This is particularly important for syndromes where place matters such as those related to
temperature-exposure (e.g. HRI) and those related to air quality (e.g. respiratory health effects).76
Practitioners involved in prevention services can use this geospatial information to assimilate
large quantities of data to determine both overall patterns of illness as well as drill down to finer
granularity if counts warrant closer examination.
Despite the growing interest in this area, there has been limited formal evaluative work to
date exploring the use of 911 medical dispatch data, particularly in Canada. Of the work that has
been done, however, the results are very promising. Since 1999, the New York City Department
of Health has been monitoring 911 medical dispatch calls on a daily basis to identify temporal
increases in respiratory illnesses. The system provides a tool to detect unusual 911 activity and
investigate the potential causes. This system has been validated on an annual basis and each year,
the first surveillance indicator at the start of the influenza season has been an increase in 911
calls, generally 2 to 3 weeks before notification from traditional surveillance systems.7, 8 Similar

27
results have been reported from Danish research where an increase in medical dispatch calls
corresponded to the first influenza outbreak of the season.6
More recently, syndromic surveillance systems using 911 medical dispatch data are being
explored for their application to environmental health conditions, such as HRI. It is anticipated
that with climate change, the impact of hot weather on health will become a major public health
concern. Many of these health conditions are not routinely monitored within the community, one
of the challenges being the difficulty in obtaining morbidity indicators on a timely basis.
Appendix B provides a logic model of the process by which HRI may be captured by 911
medical dispatch data. Conceptually, it seems plausible that 911 medical dispatch data captures
some proportion of the heat-related burden of illness and therefore could quantify some of the
health impact. The limited work examining 911 medical dispatch data as an indicator of heat-
related illness has shown encouraging results. Total ambulance response calls were observed to
increase with temperatures higher than expected in a study in Switzerland,9 and approximately
10% on heat alert days in earlier Toronto research.10 However, both studies examined all total
ambulance calls, rather than those specifically for heat. Further, the Swiss study only considered
the population over the age of 65 years. The Toronto study used census population information
as the denominator for rates of 911 calls; therefore, it is unclear whether the reported effects
were the result of changes in population size brought about by summer tourist and visitors to the
city.
The location of ambulance calls can be mapped to illustrate vulnerable neighbourhoods.10
This information is important for public health practitioners in planning locations for

28
interventions. It is particularly important for illnesses such as HRI where there are known
vulnerable groups such as the elderly, socially isolated, and those with pre-existing illness. A
surveillance system that can identify and locate these vulnerable populations geographically can
then facilitate the delivery of targeted interventions to those at the greatest risk of adverse effects.
2.4.3 Geographic Information System Application to Surveillance
Given the spatial relationship between heat and health, it has been suggested that
geographic information systems (GIS) can enhance understanding and improve mitigation of
heat-related health impacts in urban areas.107 A GIS is a tool for integrating, analyzing, and
visualizing spatial information. It includes the hardware, software, people, and geographical data
needed to analyzed geographically referenced data. GIS is thought to have great potential for
syndromic surveillance.74 An earlier study used county-level dot mapping techniques to illustrate
heat-related mortality among the elderly.76 Recent preliminary work in New York City is
exploring the use of similar methods to identify vulnerable areas in the city.141
Remote sensing is another approach being implemented to identify geographical areas at
high risk for the effects of heat.109 Remote sensing can be done at ground-level or from airborne
and satellite platforms to create thermal maps of surface temperatures in urban areas. A thermal
mapping project has recently started in Toronto to provide more detailed information about the
location of the urban heat islands (personal communication, David Mate, Scientific
Communications Officer, Natural Resources Canada). It is plausible that once the spatial burden
of HRI is described, one could overlay maps with this additional information (e.g. location of
urban heat islands) to provide a more integrated perspective on factors that affect HRI burden.

29
Incorporating geospatial information into a syndromic surveillance system will assist public
health practitioners in making decisions of where to target interventions, and therefore put
limited resources to most effective use.
2.5 Chapter Summary
There is an extensive body of literature that demonstrates the adverse effects of heat on
human health. Overall, most of these studies consider mortality as the outcome of interest,
despite the broad spectrum of morbidity outcomes that fall under the umbrella of “heat-related
illness”. Of the limited work that has been done considering morbidity, it is clear that there is a
contrast between morbidity and mortality data, with hospital admissions representing smaller
increases in magnitude than measures of excess mortality during extreme heat. These findings
have serious implications as they suggest that people who die during heat waves are not reaching
the attention of medical services. Given this, there is a need for surveillance to detect HRI, both
in time and in space, to identify those most vulnerable to effects and deliver public health
interventions. Research in syndromic surveillance suggests that 911 medical dispatch
information is a promising data source for monitoring HRI. The application of temporal and
geospatial techniques using 911 data has the potential to provide new information about the
burden of HRI in Toronto.

30
Chapter 3
Methods and Approach 3.1 Study Design
This study was primarily a time series analysis to assess the relationship between
temperature and 911 calls for HRI. The utility of two different indicators of heat exposure was
evaluated, and the role of lag effects, day effects, and influences of other meteorological
variables (e.g. relative humidity, ozone) was explored. This research was supplemented with
measurement development of a case definition for HRI using clinical and empirical methods. A
validity and comparison analysis across multiples systems to detect HRI episodes (e.g.
emergency department, heat health warning system) was conducted. Finally, geospatial analyses
were used to explore the spatial distribution of HRI.
3.2 Data Sources
Several data sources were used in the current study. Health outcome data included 911
medical dispatch information from Toronto Emergency Medical Services (EMS) and emergency
department (ED) visits from the National Ambulatory Care Reporting System (NACRS). The
former was the primary morbidity data source under investigation and used in all analyses. ED
information provided a measure to assess the validity of the 911 call data as an indicator of
community burden of HRI. Meteorological data from local monitoring stations were provided by
Environment Canada and provided indicators of heat exposure. Finally, Toronto Public Health

31
provided information about all past heat alerts declared through the currently used heat health
warning system. These data were used in the comparative assessment of the timing of the spikes
in ED and 911 data. The layers of base geospatial data were provided by Statistics Canada
through Toronto Public Health including neighbourhood shape files and socioeconomic profile
data.
3.2.1 Toronto EMS Dispatch System
The main data source used was the Toronto Emergency Medical Services (TEMS)
medical dispatch database. All emergency medical services in Toronto are provided by a single
municipal government agency, Toronto EMS. The Toronto EMS Communications Centre is
responsible for coordinating and dispatching medical emergency calls and processes
approximately 425,700 calls each year; approximately half of these are for emergencies and the
other half for scheduled inter-facility patient transfer.142 The Toronto EMS Communications
Centre is staffed by call receivers and dispatchers who have received formal training in call
taking, medical terminology, and pre-hospital medical care.
Initially, a caller contacts a 911 operator who connects them to one of three emergency
service operators: police, ambulance (EMS), or fire service, depending on the nature of the
emergency. When the call is directed to the Toronto EMS Communications Centre for possible
ambulance dispatch, the pick up location is first confirmed and then further information sought
from the caller regarding the nature of the problem by the call receiver. EMS call receivers
classify and prioritize calls for service with the Medical Priority Dispatch System (MPDS,
Priority Dispatch Corporation, Version 1.1, Salt Lake City, Utah). This widely used

32
computerized triage algorithm scripts the dispatcher’s interview with the 911 caller to identify
the nature of the incident and the probable acuity of the patient to determine the appropriate level
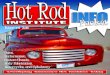
of EMS response in the pre-hospital setting. Based on the caller’s answers, MPDS’s software
assigns the call to one of more than 500 “determinants” and recommends a dispatch priority. An
example of the questioning and code-assignment process is provided in Figure 3.1.
Figure 3.1: MPDS code categorization process
Entry Questions
Key Questions:1. Is s/he completely awake?2. Is s/he breathing normally?
3. Is s/he changing colour?4. What is her/his skin temperature?
Dispatch Codes:20-D-1 Heat/Cold Exposure, not alert
20-C-1 Heat/Cold Exposure, cardiac history20-B-1 Heat/Cold Exposure, change in skin colour
20-A-1 Heat/Cold Exposure, alert
Medical Priority Dispatch System, Priority Dispatch Corp., Salt Lake City, Utah
The call information is electronically forwarded by the call receiver to an emergency
medical dispatcher who will locate the call, select the closest ambulance unit, and assign the unit
to that call. This system is fully integrated into the EMS Computer-Aided Dispatch (CAD)
system, a computerized system linked to an electronic database. Each call has its own individual
record, which includes all data from the MPDS interview, and this information is stored in a
database housed at TEMS. It has been suggested that this automated, protocol-based call taking
approach is more accurate and consistent than subjective or experience-based determinants made
by individual dispatchers.143 It has also been reported that the introduction of these protocols has

33
resulted in more accurate identification of patients experiencing adverse health outcomes,
particularly for acute effects.144
The MPDS system is used in over 3,000 jurisdictions worldwide, as well as 130 in
Canada including all of Nova Scotia and British Columbia, as well as Calgary, Winnipeg,
Montreal, Niagara, and others (personal communication, Jon Stones, Client Services
Representative, Priority Dispatch Corporation). Between December 2000 and November 2005,
and therefore during the study period, version 11.1 was used with no major changes or updates
made during this time (personal communication, Mark Toman, Systems Control Supervisor,
TEMS). Slight modifications have since been made and an updated version, 11.2, was
implemented at Toronto EMS in November 2005.
The accuracy and reliability of the MPDS determinant-assignment process has been
evaluated. In Toronto, a 5% sample of calls is monitored each day and assessed for compliance
with the National Academy of Emergency Dispatch quality assurance guidelines. Values of
recent assessments of Toronto EMS call receiver compliance with MPDS protocols between
May and October 2007 documented a 96 to 98% compliance score (personal communication,
Mark Toman, Systems Control Supervisor, TEMS).
In addition to call receiver compliance, the sensitivity and specificity of MPDS codes
have also been investigated. A performance analysis of the ability of the MPDS system to detect
high acuity of illness or injury reported an overall sensitivity of approximately 70%.145 Adequate
sensitivity has also been reported in other studies for detecting high acuity calls; MPDS coding

34
for all emergency calls had high sensitivity for the prediction of calls that required advanced life
support intervention including “Chest pain” and “Unconscious/fainting”. However, these codes
were also associated with lower specificity.146 Recent studies indicate that the lower acuity
determinants are also reliably assigned. For low-acuity illness or injury, the use of MPDS
standard protocols has been found to reliably identify patients as low acuity 99% of the time.147
Aside from these evaluations of the ability of MPDS to distinguish between high and
low-acuity calls, there has not been research to more formally assess sensitivity and specificity of
individual determinants. However, there are current discussions to plan this kind of evaluation in
Toronto by linking the original call-assigned MPDS determinants to subsequent paramedic
assessment and hospital discharge diagnosis records. This is pending the implementation of an
electronic data tablet, upon which the paramedic will complete their onsite assessment (personal
communication, Alan Craig, Deputy Chief, Toronto EMS).
Toronto EMS provided 911 medical dispatch data for the four-year period of 2002-2005
in Microsoft Access database format. All of the emergency ambulance response calls that were
made during the study period were transferred electronically in a secure, password-protected
shared server to the study researcher. A list of the key data fields included can be found in Table
3.1. The dataset contains three days in 2005 (January 20, January 28, March 26) with unusually
low volumes of calls due to a CAD failure (personal communication, Adrian Mateescu, Senior
Planning Officer, & David Lyons, Manager CACC Redesign Project, TEMS). However, these
dates fall outside of the study period, thus daily information was complete for this research.

35
Table 3.1: Data variables from the 911 EMS database
Data Variable Description Example RMI_ID Master incident number; unique identifier for
each call 853266
RMI_Location_Type Kind of location of the call Park/Playground RMI_Call_City Municipality in which call pick-up is located Toronto RMI_Call_Latitude Latitude of the call location 43.796996 RMI_Call_Longitude Longitude of the call location -79.27836 UTM Square 1 km UTM square 09663E1 RMI_ResponseDate Time of the call 1/4/2002 12:38:39 PM RMI_MPDSDeterminant Full MPDS (Medical Priority Dispatch
System) determinant code 06C02
RT_CTAS CTAS (Canadian Triage Acuity Scale) of this patient
2 CTAS
RT_Location_Name Name of receiving hospital HO MTS RT_Hosp_Latitude Latitude of the receiving hospital 43.769445 RT_Hosp_Longitude Longitude of the receiving hospital -79.364471 Comment Additional text information about the call M 81 SOB PALE
CLAMMY
To gain a better understanding of the call coding and ambulance dispatch process, the
researcher spent two days at TEMS Communications Centre. One day was spent sitting with a
call receiver, listening to 911 calls on headphones, and learning how the calls are received,
categorized and information entered into the CAD system. The second day was spent sitting with
an emergency medical dispatcher to gain an understanding of how this information is then used
to dispatch an ambulance and the appropriate level of medical assistance. Ongoing consultation
was provided by colleagues at TEMS throughout the research process. This was supplemented
with educational materials regarding the emergency medical dispatch process including texts,148
presentations, MPDS guides,149 and internal training documents.

36
3.2.2 Emergency Department Visits, National Ambulatory Care Reporting System
(NACRS)
All emergency departments (EDs) in the province of Ontario submit data on ED visits to
the National Ambulatory Care Reporting System (NACRS), developed by the Canadian Institute
of Health Information (CIHI). Demographic information, reason for visit (coded according to the
Canadian Enhancement to the International Statistical Classification of Diseases and Related
Health Problems, Tenth Revision [ICD-10-CA] introduced in 2001), and other diagnostic
information is collected.150 Regular data quality reviews are performed on the NACRS data by
CIHI. It is deemed to be thoroughly comprehensive as Ontario EDs are mandated to report.151
However, a commonly cited data quality caveat with the NACRS data is the lack of
completeness of data, particularly in 2001 and 2002 due to some EDs not reporting data or only
partially reporting data. However, these geographical areas were outside of the Toronto area and
thus not relevant to the data set for this study.
Toronto Public Health has access to NACRS data through the Ministry of Health and
Long-Term Care Data Warehouse, the Provincial Health Planning Database (personal
communication, Catalina Yokingco, Senior Health Information Analyst, Toronto Public Health).
Note that unlike 911 data, NACRS data were available for Toronto residents only. The
researcher met with a Data Manager at Toronto Public Health to review the data variables
available in the NACRS database and plan the data request.
The “registration date” field was used to select day of visit. Registration date is one of the
most precise variables in the NACRS dataset. It represents the date the patient’s ED visit was

37
registered on the hospital system, which is at the beginning of the ED visit. Any possible delay
between actual arrival at the ED and registration is typically no longer than 30 minutes (personal
communication, Michael Schull, Scientist, Institute for Clinical Evaluative Sciences).
Visits specifically related to heat were selected based on the “reason for visit” field in the
NACRS dataset. This is coded by ICD-10-CA codes, which are routinely used as health
indicators in syndromic surveillance systems, particularly for influenza-like-illness.123, 134, 152-156
In addition to meeting with an ICD-10-CA coder at St. Michael’s Hospital to review likely
codes, a literature review was conducted to determine the appropriate ICD-10 codes to be used in
this study. These codes were subsequently noted to be identical to ones selected in another
Canadian study using these data157 and a study of ED visits for heat during the 1995 Chicago
heat wave.158 The selected codes are presented in Table 3.2.
Table 3.2: ICD-10-CA codes used in construction of the case definition of HRI for ED visits
T67 Effects of heat and light T67.0 Heatstroke and sunstroke T67.1 Heat syncope T67.2 Heat cramp T67.3 Heat exhaustion, anhydrotic T67.4 Heat exhaustion, due to salt depletion T67.5 Heat exhaustion, unspecified T67.6 Heat fatigue, transient T67.7 Heat oedema T67.8 Other effects of heat and light T67.9 Effect of heat and light, unspecified (International Statistical Classification of Disease and Related Health Problems, Tenth Revision [ICD-10-CA])
A data request was created and submitted to Toronto Public Health requesting aggregate
counts of daily ED visits for the 17 EDs in Toronto for each study summer. Additionally, all

38
visits categorized with any of the heat-related ICD-10-CA codes were requested for each day.
This information was sent to the researcher in an Excel file.
3.2.3 Meteorological Data
Daily meteorological data, including the average value of mean and maximum
temperature (ºC), and daily minimum and maximum relative humidity (%), were obtained for
Toronto (measured at Pearson International Airport, 27 km northwest of downtown) from
Environment Canada’s Digital Archive of Canadian Climatological Data. This archive contains
hourly, daily, and monthly climatological records for monitoring stations across Canada. Given
the uncertainty in the literature regarding the most appropriate indicator of heat exposure for
studies of health outcomes, both maximum and mean temperature were examined to determine
their relationship with medical dispatch calls. The daily mean relative humidity (%) was
calculated by averaging the daily minimum and maximum values, as advised by colleagues at
Environment Canada (personal communication, Chad Cheng, Research Climatologist,
Environment Canada). Daily ozone data were also obtained for Toronto (measured at Bay and
Wellesley Streets), though this was only available for the years 2002-2004. Ozone data were
from Environment Canada’s National Air Pollution Surveillance Network (NAPS) which uses a
network of air monitoring stations strategically located across Canadian cities to capture ambient
air pollution concentrations.
3.2.4 Toronto Heat Health Warning System (HHWS)
All of the dates of heat alerts and extreme heat alerts were provided by Toronto Public
Health for the study period (a complete list is provided in Appendix C). For the purpose of the

39
analysis, days were considered as either being a heat alert day or not (1 or 0), rather than making
a distinction between a regular and extreme heat alert. The aim of this component of the research
was to make comparisons with the timing of Toronto Public Health initiating a response, rather
than on the details of the type of alert generated.
3.3 Data Acquisition
3.3.1 Partner Agencies
Three organizations collaborated in the current research. The first is the Department of
Public Health Sciences at the University of Toronto, where the researcher is a PhD candidate.
During the study, the researcher was provided with work-space resources at Toronto Public
Health (TPH) where much of the analysis was completed. Toronto EMS is the third partner
agency who provided the primary data for the research. TPH and Toronto EMS had a previous
collaborative relationship for earlier syndromic surveillance work during World Youth Day in
2002. Communication between organizations was maintained through the establishment of a
study steering committee. This was comprised of members from all three organizations, and
meetings were regularly convened to guide the research process.
3.3.2 Institutional Reviews & Privacy Issues
Given the collaborative nature of this project, several institutional reviews were obtained
prior to the start of the research. The study received expedited ethics approval from the
University of Toronto in February 2005, with subsequent annual renewals in 2006 and 2007. It
also received ethics approval through the internal review process at Toronto Public Health,

40
where much of the research was conducted, in February 2006. Finally, a Memorandum of
Understanding was created between TPH and TEMS outlining the agreement regarding data
sharing and use in March 2006.
This study used non-nominal data and therefore callers were not identified. The data
collected and generated through this study were protected from unauthorized access; only
members of the research team had access to the data. Laws regarding privacy and access to
information were applied, as appropriate, to all access to and applications of the data, with
particular regard to the protection of the confidential nature of the individual caller’s data. All
electronic data was securely stored and protected by access passwords. Hard copy information is
stored in locked files at TPH. Upon completion of the research these documents will be
destroyed appropriately using secure methods.
3.4 Software
Several software packages were used for the data preparation, extraction, and analysis.
The 911 medical dispatch information was stored in a Microsoft Access 2002 database.
However, all statistical analyses (descriptive and time series) were executed using SAS 9.1 (SAS
Institute, Cary, North Carolina) and S-PLUS 7.0 (Insightful Inc., Seattle, Washington). Microsoft
Office Excel 2003 was used for creating some of the descriptive graphs. Geospatial analyses
were achieved using MapInfo (MapInfo Professional v8), the geographical information system
software currently licensed for use at TPH, and GeoDA 0.9 5-i5 (Luc Anselin and The Regents
of the University of Illinois). Aberration detection was accomplished using the Early Aberration

41
Reporting System (EARS) (Centers for Disease Control and Prevention, Atlanta, Georgia), an
Excel-based, freely available software commonly used in syndromic surveillance.
3.5 Data Preparation and Extraction
Given that the 911 medical dispatch database is not routinely used for analysis,
particularly by researchers outside of Toronto EMS, there was substantial work required to
prepare and extract the data for its use in the current study. The other data sources were more
readily available for analysis without extensive preparation.
The information for the 911 medical dispatch data between 2002-2005 was posted on a
secure, password protected, shared server between Toronto EMS and Toronto Public Health.
Given the large size of the files, the database was sent in smaller sections, and then reconstructed
by the researcher at Toronto Public Health in an Access database format. Prior to the data
cleaning and extraction phase, the researcher received training in the terminology used in the
database by a number of colleagues at Toronto EMS including the Communications Manager,
Research Analyst, Research Coordinator, and an Emergency Medical Dispatcher Instructor.
A series of Access queries and SAS programs were developed to combine the various
database sections and then clean the 911 database so it was suitable for use for the research
purposes. Data were provided for the entire time period of 2002-2005, however, only the calls
for the study period, June 1st-August 31st of each year, were extracted in order to focus on HRI
rather than cold-related illness. As will be later explained, the determinants used to capture HRI
also capture cold-related illness. Only emergency calls to which an ambulance actually

42
responded were used in this study; calls cancelled before dispatch (such as when a 911 caller
person calls back indicating an ambulance is no longer required), duplicate calls, and scheduled
inter-facility transfers were removed from the dataset. Duplicate calls have the same RMI_ID
number so these were checked and the duplicate removed to avoid double-counting. Emergency
calls were selected based on their assigned call priority; “Alpha”, “Bravo”, “Charlie”, “Delta”,
“Echo”, “Alpha1”, “Alpha2”, “Alpha3”, are call priority categories and considered emergency
calls (personal communication, Adrian Mateescu, Senior Planning Officer, TEMS).
The database was reconstructed on the TPH secure server and two key sections
organized. One, suitable for the majority of the analysis, included aggregate daily values for all
emergency calls and for calls meeting the various syndrome definitions (see case definition
section following). However, for the geospatial methods non-aggregate individual call records
were required so a second section of the database was created with this information.
3.6 Data Interpretation and Analysis
A variety of analytical methods were used in the current study. Following initial
exploratory and descriptive analysis, the first step was to create a case definition of HRI. This
was a necessary initial step as all subsequent analyses used this case definition. Following this, a
time series analysis was conducted to assess the relationship of 911 calls with meteorological
variables. Geospatial techniques were then applied to identify vulnerable areas in Toronto. A
validation study of the 911 medical dispatch data was performed using another source of
morbidity data, ED visits. The use of these data in the public health setting was then investigated
through the application to a commonly used aberration detection technique and comparisons
made with the current Toronto HHWS.

43
3.6.1 Descriptive Analysis
Univariate analysis was conducted to determine the frequency, means, and standard
deviations of all study variables in SAS 9.1 using the “proc univariate” procedure. Descriptive
graphs were created in both SAS 9.1 and Microsoft Excel.
3.6.2 Development of a Case Definition
To identify potential HRI-relevant MPDS determinants, a staged combination of
clinically informed “expert” opinion and empirical testing was used. This is in keeping with
others’ approaches to syndrome definition and validation.159
3.6.2.1 Clinical Assessment
A clinician group comprised of partners from collaborating organizations reviewed all
MPDS determinants and selected a set which they felt were most likely to include patients
suffering from HRI (Appendix D). This selected list was then reviewed in two focus groups. The
first included colleagues at Toronto EMS – paramedics, call receivers, dispatch operators, and
emergency room physicians who ranked the categories according to their judgements in
identifying HRI cases. The group was provided with a list of all of the codes under consideration
and asked to first identify whether each of the codes may represent HRI, and then rank from
most to least specific. This was accomplished through an open discussion facilitated by the
researcher. Areas of disagreement were resolved through extensive discussion between the
group. The second focus group comprised public health physicians, epidemiologists, public
health managers, and medical residents, who reviewed the ranked and selected list to ensure that
all determinants of public health relevance were captured.

44
3.6.2.2 Statistical Analysis
Mean daily temperature (smoothed using spline160) and the percent of the total EMS call
volume for all determinant groupings, as well as those selected by the expert groups, for which
sufficient call volume existed (determinant groupings with median calls volumes of 0 were
excluded) were jointly plotted using SAS 9.1. Given the lack of appropriate denominator data,
the percentage of all emergency calls for HRI was used in most of the analyses. Use of
percentages rather than counts was meant to partially control for transient population at risk
differences associated with day effects (e.g. commuters working downtown during the week and
visitors to major recreation centres on weekends). In these cases, using census information as the
denominator would be inappropriate and misleading given it would not accurately represent the
population at risk.
For those plots in which some co-variation could be visually observed, Spearman’s
correlations were computed using SAS 9.1. Conducting Spearman’s correlations was appropriate
given the non-normal distribution of the data. The Spearman’s correlation coefficients range in
value from -1 to 1. Values close to the extremes indicate a high degree of correlation between the
variables; values near 0 imply a lack of linear association.161 It was hypothesized that there
would be stronger positive correlations for determinants which represented: greater recognition,
labeling or occurrence of HRI per se, aggravation of pre-existing conditions, and de-
compensation of already vulnerable individuals.

45
3.6.3 Assessing the Relationship between Temperature and HRI
Fisher’s exact test was used to detect differences in the proportion of heat-related calls on
days with mean and maximum daily temperatures above and below predetermined thresholds.
Thresholds of 28°C for maximum temperature and 24ºC for mean temperature were selected for
this part of the analysis. These threshold values were selected because they represent the
approximate daily summertime averages during the most recent study summer of 2005 and the
aim of the analysis was in detecting the effects of above average temperatures on health. Fisher’s
was selected as the preferred inferential test for count data, because some cells may have less
than five observations.162 The Fisher’s exact test can be used to detect group differences when
values fall into one of two mutually exclusive categories and is suited to highly imbalanced 2 x 2
tables. The Fisher’s exact test computes an exact probability of observing the given result.
In environmental epidemiology, data often come in a time series of discrete and non-
normal response variables, often count data. These data are likely to exhibit seasonal variation
and time trends that may be related to meteorological factors, so the latter must be taken into
consideration in the selection of the appropriate statistical methods. In this study, Zero inflated
Poisson regression (ZIP) and time series analyses using the Generalized Additive Model (GAM)
were each performed to determine the association between calls for HRI and daily maximum and
mean temperature. Both are widely used in the environmental epidemiology literature,
particularly in studies of the health effects of air pollution.48, 50, 71, 90, 163-168 However, it has been
suggested that GAM models may produce biased estimates in situations where regression
coefficients are small.169, 170 The medical dispatch call dataset has a high number of days with

46
zero calls for HRI. As a result, the Poisson regression model would underestimate the probability
of zeros. Hence, both approaches were used.
ZIP is an extension of Poisson regression that is designed to apply to non-negative count
data with an overabundance of zero outcomes and thus was deemed appropriate for this
analysis.171 Other analyses of datasets with a high proportion of zeros have found ZIP to be a
better model fit than pure Poisson models.172-174 In particular, it has also been used in testing of
air pollution – daily asthma admission relationships.175 As a result, ZIP was used with the
“nlmixed” procedure of SAS 9.1 software.
The Poisson part of the ZIP model takes the following form:
log[E(Y)] = ß0 + ß1 temperature + ß2 time + ß3 time2 + ß4 relative humidity + ß5day+
ß6ozone+offset
where Y is the number of ambulance response calls for HRI, ß0 is the intercept, and day is the
dummy variable, coded as 0 for weekdays and 1 for weekends and holidays.
Generalized Additive Model (GAM)176 is an extension of the generalized linear model.
The advantage of the GAM is that it is more flexible than other regression methods for non-
normally distributed variables and is more suitable for time series data. Non-normal outcome
distribution often occurs when looking at the rate of some health outcomes over time, especially
those with a lower range of distribution, like 911 calls for HRI which could range daily from
only 0-1% of total calls. Furthermore, GAM adjusts for possible serial correlation of the calls

47
and includes nonparametric smoothing functions to control for non-linear effects of the
covariates. A Poisson GAM with a log-link function was used to investigate the relationship
between the number of HRI calls divided by the number of all 911 calls and maximum/mean
temperature. The rate of HRI calls to all ambulance response calls was modeled using smoothing
splines adjusted for relative humidity, ozone, and time. Potential over-dispersion, where the
observed variance is higher than the mean of the distribution of the selected model, was
controlled for in the models. The basic GAM model used took the following form:
GAM model:
log[E(Y)] = ß0 + ß1 temperature + ß2 day + s(time) +s(relative humidity) + s(ozone)+offset
where “s” is the smooth function (smoothing spline). The degree of smoothing was selected
based on the Akaike information criterion (AIC), a statistic that accounts for the number of
degrees of freedom used by the smoothers. This was accomplished by testing for different spans
and types of smoothers. The model with the lowest AIC was selected for subsequent analyses.
The loess smoother was also explored and there were no major differences found in resulting
parameter estimates (Appendix E).
Smoothed functions of the same day and of lags up to one day of daily mean and
maximum temperature were investigated, given the literature that suggests that temperature can
affect health not only on the same day, but on consequent days. S-PLUS 7.0 (Insightful Inc.,
Seattle, Washington) was used for the GAM time series analysis.

48
In both sets of models, the regression coefficients are ß’s, so relative risks (RR) were calculated
as follows:
RR= exp(ß)
Here, the RR associated with ß1 indicates the change in expected morbidity due to a 1°C increase
in mean or maximum temperature.
3.6.4 Validation and Timing Assessment
To test the validity of the 911 data source, comparisons were made with another source of
morbidity data, ED visits. Initially, the same ZIP model that was used in the earlier 911 call
analysis was used, replacing the proportion of 911 calls for HRI with the proportion of ED visits
for HRI in order to evaluate the relationship between the proportion of ED visits for HRI and
mean and maximum temperature. This analysis was performed in SAS 9.1.
The volume of absolute numbers of 911 HRI calls and ED HRI visits were also
graphically assessed using Microsoft Excel to get a sense of any difference in capturing the
burden of illness. Days of Toronto heat alerts were also added to these graphs to get a sense of
the timing of morbidity increases in relation to the current mortality-based heat health warning
system. A similar approach has been used in another recent study.177
One of the challenges in developing syndromic surveillance systems is that of defining
what constitutes a spike in calls/visits. In this study, spike thresholds were selected for each of
911 calls and ED visits for HRI using the daily mean values for each, with other possible
thresholds based on the closest integer of the standard deviation above and below the mean.

49
These various thresholds were examined using a Receiver Operating Characteristic (ROC)178
plot, a useful tool for selecting decision thresholds by examining tradeoffs in sensitivity and
specificity at various cut-offs. The sensitivity and specificity of both 911 and NACRS were
calculated, using heat alerts as the gold standard. The sensitivity, or true positive fraction (TPF)
was then plotted against the false positive fraction (FPF) (1-specificity) for both, and the
coordinates closest to coordinate (0,1) selected as the optimum threshold. This method of
selection is often used because the (0,1) coordinate represents 100% sensitivity and 100%
specificity. These threshold spikes of each data source were then compared with each other and
with the mortality based algorithm informed heat alerts to obtain a better understanding of the
relevant timing and sensitivity of each. A McNemar’s test for paired data was applied to
determine the statistical significance of associations between these spike thresholds in SAS 9.1.
The timing of spikes of ED HRI visits and 911 HRI calls was further explored using an
aberration detection software, the Early Aberration Reporting System (EARS). This free
software is available from the USA Centers for Disease Control and is most commonly used for
the surveillance of syndromes. EARS uses three baseline aberration detection methods, C1-
MILD (C1), C2-MEDIUM (C2), and C3-ULTRA (C3) using simulated data. The terms mild,
medium, and ultra refer to the level of sensitivity of these methods where C1-MILD is
considered to have the lowest sensitivity and C3 the most sensitive.179, 180 The thresholds for
these statistical methods are based on a cumulative sum (CUSUM) calculation, designed to
detect sudden changes in the mean value of a quantity of interest. EARS maintains a running
total of the deviations between the observed and expected values; if the total exceeds a
predetermined threshold then an alarm is generated. For C1 and C2, the CUSUM thresholds are

50
the mean plus 3 standard deviations. A moving window of the past 7 days is used for the former,
and the past 3 to 10 days for the latter. For C3, the CUSUM flag is based on two standard
deviations with a moving window width of the previous two days and the current day.179
Finally, the timing association between spikes in 911 calls and ED visits was further
assessed by calculating cross-correlations using the “proc arima” procedure in SAS 9.1. Given
the autocorrelation of the data, it was necessary to first fit an ARIMA model181 sufficient to
reduce the residuals to white noise and then filter the data series with this model to get the white
noise residual series. The “proc arima” procedure performs this process called, “pre-whitening”.
The filtered data series are then cross-correlated. This was done both for all summers combined
and each individual study summer.
3.6.5 Geospatial Approach
Geospatial methods have been deemed to be extremely useful in conducting research into
health services and disparities.182 Increasingly, they are being used to understand the relationship
between heat and human health and other environmental exposures.10, 76, 141, 183
The maps created in this research were constructed using layers of spatial data. A base
layer of Toronto, divided according to its 140 neighbourhoods was used as the foundation of the
descriptive maps. Neighbourhood level was selected as the scale of interest given that this is how
many public health interventions are planned, and thus it is the typical scale used in public health
mapping in Toronto (personal communication, Eleni Kefalas, Health Analyst, Toronto Public
Health). This layer of spatial data was provided by Statistics Canada (2001 Census Cartographic

51
Boundary Files). A thematic layer of 911 calls for HRI was then placed on top of this base layer.
To accomplish this, a choropleth, or shaded map, was created. The intensity of the shades
indicates the magnitude of values for a variable, facilitating comparisons between geographical
areas.182,184 In this research, choropleth maps were used to illustrate the range of percentages of
911 calls for HRI by neighbourhood, with a different shade used for each level depicted. Data
values were divided into classes using natural breaks in the data distribution. The use of a shaded
map, rather than dot density, also eliminated the problem of depicting small cell counts, which
would conflict with ethical/privacy guidelines.
The percentage of HRI calls was calculated per summer for each of Toronto’s 140
neighbourhoods using the latitude and longitude values available for each call. The mean annual
proportion of HRI calls to all emergency calls was then calculated across study years. These
proportions were mapped using the software, MapInfo (MapInfo Professional v8). Data for three
periods of unusually high calls that occurred during a major outdoor event in 2002 (July 27 &
28), the 2003 Northeast Blackout (August 14) and an outdoor concert in 2003 (July 30), were
removed to avoid capturing event-specific geospatial burden.
The same approach was used to map a socioeconomic profile, using the number of
families under the Low Income Cut-Off (LICO) as a percentage of all economic families, based
on 2001 Census data. LICO is a commonly used poverty index. It considers households that
spend disproportionate amounts of their income on food, clothing, and shelter (i.e. 20% above
the average family) as low-income. A choropleth map was created using different colour shades
for groups of percentages, again using natural breaks in the data distribution.

52
In addition to this descriptive geospatial work, analyses were conducted to determine the
spatial autocorrelation between neighbourhoods and therefore identify “hot spots” in Toronto
with a relatively high burden of HRI. Spatial autocorrelation is used to describe and analyze the
influence of neighbouring regions on each other and assess the degree of autocorrelation. To test
for spatial autocorrelation, Moran’s I was calculated using GeoDA 0.9 5-i5 (Luc Anselin and
The Regents of the University of Illinois). Moran’s I is a weighted correlation coefficient used to
detect departures from spatial randomness.185,186 A departure from randomness indicates a spatial
pattern, like a cluster, for example. Values fall between -1 and +1, with values close to zero
indicating no spatial trends, those close to +1 indicating spatial clustering, and those close to -1
indicating negative spatial autocorrelation. In this analysis, Local Moran’s I was calculated to
determine the presence or absence of significant spatial clusters for each location.

53
Chapter 4
Results 4.1 Descriptive Statistics
The daily number of all emergency calls to Toronto EMS was relatively consistent
throughout the study period, with approximately 500 – 600 calls per day. Three dates were an
exception to this pattern. There was an increase in all calls during World Youth Day in 2002
during the outdoor vigil and papal mass (A), in 2003 during an outdoor Rolling Stones concert
(B), and in 2003 during the largest electricity blackout in North America’s history (C). These
patterns are illustrated in Figure 4.1.
The four study summers had different weather patterns. As illustrated in Table 4.1, the
summers of 2002 and 2005 were characterized by high mean and maximum temperatures. These
hotter summers also had higher minimum temperatures than 2003 and 2004, indicating that there
was not substantial overnight temperature relief. The high temperatures are also reflected in the
large numbers of heat and extreme heat alerts that were declared in 2002 and 2005 as compared
with the relatively cooler summers of 2003 and 2004. Conversely, the cooler summers of 2003
and 2004 had higher mean values for relative humidity. Ozone levels varied throughout the three
study summers for which data was available, with the highest mean levels in 2003.

54
Figure 4.1: All daily 911 emergency calls, Toronto 2002-2005 (June 1- August 31) (letters represent special events, as indicated) Figure 4.1a: 2002 Figure 4.1b: 2003
400
500
600
700
800
900
1000
6/1 6/8 6/15
6/22
6/29 7/6 7/13
7/20
7/27 8/3 8/10
8/17
8/24
8/31
Date
Num
ber o
f Cal
ls
400
500
600
700
800
900
1000
6/1 6/8 6/15
6/22
6/29 7/6 7/13
7/20
7/27 8/3 8/10
8/17
8/24
8/31
Date
Num
ber o
f Cal
ls
A: World Youth Day B: Rolling Stones Concert; C: North American Blackout
Figure 4.1c: 2004 Figure 4.1d: 2005
400
500
600
700
800
900
1000
6/1 6/8 6/15
6/22
6/29 7/6 7/13
7/20
7/27 8/3 8/10
8/17
8/24
8/31
Date
Num
ber o
f Cal
ls
400
500
600
700
800
900
10006/1 6/8 6/1
5
6/22
6/29 7/6 7/13
7/20
7/27 8/3 8/10
8/17
8/24
8/31
Date
Num
ber o
f Cal
ls
AB
C

55
Table 4.1: Descriptive meteorological statistics by summer, Toronto 2002-2005 (June 1-August 31)
Variable 2002 2003 2004 2005
Weather variables* Daily mean (st. dev.) Daily mean (st. dev.) Daily mean (st. dev.) Daily mean (st. dev.)
Mean temperature (°C) 22.0 (4.1) 20.8 (3.5) 19.3 (3.0) 23.1 (3.4) Maximum temperature (°C) 27.7 (4.9) 26.0 (4.1) 24.2 (3.4) 28.5 (4.0) Minimum temperature (°C) 16.3 (3.7) 15.5 (3.4) 14.3 (3.2) 17.6 (3.4)
Relative humidity (%) 65.3 (10.0) 69.3 (11.2) 71.3 (8.6) 66.1 (9.2)
Ozone (ppb) 32.6 (11.0) 34.6 (12.0) 28.6 (10.0) n/a
HHWS Alerts† Number of days Number of days Number of days Number of days
Heat alerts 15 3 2 8
Extreme heat alerts 2 3 0 18 * Provided by Environment Canada † Provided by Toronto Public Health n/a Not available

56
4.2 Study Objective 1a: Developing a Case Definition for HRI
The clinical assessment process of case definition development through a series of focus
groups led to a list of 12 EMS call determinant groupings deemed to be potentially relevant for a
case definition of HRI (Figure 4.2). These groupings ranged in degree of specificity and
sensitivity. For example, the “Heat/cold exposure” category was expected to capture many heat-
related calls, but likely to miss others that may be coded as “Unconscious/fainting” or “Breathing
problems”. Conversely, while the “Unknown problem (man down)” category is more sensitive
and more likely to capture all calls that might be related to heat, this call category also captures a
range of other calls that are not heat-related and therefore is the least specific determinant
grouping. Hence, there is a trade-off in sensitivity and specificity when selecting call codes for a
case definition of HRI.
Figure 4.2: 911 call “determinant” selection summary – focus groups
Card 20: Heat/cold exposure Card 31: Unconscious/fainting Card 09: Cardiac or respiratory arrest/death Card 18: Headache Card 26: Sick person Card 28: Stroke/CVA Card 06: Breathing problems Card 01: Abdominal pain Card 25: Psychiatric problems Card 10: Chest pain Card 13: Diabetic problems Card 32: Unknown problem (man down)
The temporal trend of calls for each of the 12 call groupings was plotted with daily mean
temperature for the same time period and visually inspected (Figure 4.3 and Appendix F). Four
of these appeared to co-vary most consistently with temperature (Figure 4.3), including
Most specific
Most sensitive

57
“Heat/cold exposure”, “Breathing problems”, “Unconscious/fainting”, and “Unknown problem
(man down)”.

58
Figure 4.3: Percentage of heat-related calls and mean daily temperature by determinant, 2002-2005 (June 1-August 31) Figure 4.3a: 2002
Figure 4.3b: 2003
---------- mean temperature ______ percent of calls

59
Figure 4.3c: 2004
Figure 4.3d: 2005
---------- mean temperature ______ percent of calls

60
Correlation analyses supported this observation for both mean and maximum temperature
(Table 4.2). “Heat/cold exposure”, the most specific, demonstrated the strongest positive
correlations in all study summers with both mean and maximum temperature (Spearman’s
correlation coefficient (SCC) ranged between 0.34 and 0.73, p<.0001) i.e. as daily mean and
maximum temperature increased, so did the percentage of total daily emergency call volume
assigned to this MPDS determinant grouping. These relationships were all strongly statistically
significant. The correlations were greatest in the hottest study summers of 2002 and 2005.
However, this was the only determinant grouping that had consistent results for every summer,
for both mean and maximum temperature. Findings for other determinant groupings were less
consistent.
Those determinants more related to pre-existing conditions were either not significant
e.g. “Breathing problems” (in 2005 mean temperature, SCC=0.12, p=0.24) or negatively
correlated e.g. “Stroke/CVA” (in 2005 mean and maximum temperature, SCC=-0.26, p=0.01).
Inconsistent relationships were seen for other determinant groupings that have been reported as
associated with temperature in other literature, e.g. “Psychiatric problems” (in 2002 mean
temperature, SCC=-0.22, p=0.03, but insignificant in other years) and “Diabetic problems” (in
2004, SCC=0.24, p=0.02, but statistically insignificant in other years and for maximum
temperature). Finally, less specific but perhaps most relevant to vulnerable populations were that
for “Unknown problem (man down)” (in 2005 mean temperature, SCC=0.21, p=0.04 and 2002
maximum temperature, SCC=0.21, p=0.05) and that for “Unconscious/fainting” (in 2005 mean
temperature, SCC=0.18, p=0.09).

61
Table 4.2: Correlations between daily % 911 calls for HRI and mean temperature for selected determinant groupings Table 4.2a: Mean temperature
Call Determinant Groupings 2002 2003 2004 2005 SCC p-value* SCC p-value* SCC p-value* SCC p-value* Heat/cold exposure 0.5632 <.0001 0.4496 <.0001 0.3371 0.0010 0.7150 <.0001 Unconscious/fainting 0.1031 0.3282 -0.0024 0.9822 0.0526 0.6188 0.1778 0.0900 Cardiac or respiratory arrest/death 0.0196 0.8532 0.0633 0.5486 0.0002 0.9984 -0.0039 0.9706 Headache 0.0421 0.6906 -0.2717 0.0088 -0.0366 0.7293 -0.1106 0.2939 Sick person -0.1263 0.2303 0.1660 0.1137 0.0777 0.4619 0.1390 0.1862 Stroke/CVA -0.2163 0.0383 -0.1373 0.1918 -0.0050 0.9621 -0.2563 0.0137 Breathing problems 0.0796 0.4506 -0.0296 0.7792 -0.0275 0.7944 0.1234 0.2411 Abdominal pain 0.1187 0.2599 0.0005 0.9961 -0.0518 0.6240 0.0510 0.6295 Psychiatric problems -0.2249 0.0311 0.1221 0.2462 0.0587 0.5786 0.0062 0.9530 Chest pain -0.2137 0.0408 -0.1433 0.1728 0.0989 0.3484 -0.0923 0.3813 Diabetic problems 0.0523 0.6205 -0.0673 0.5237 0.2412 0.0206 -0.0047 0.9643 Unknown problem (man down) 0.1444 0.1697 0.2171 0.0376 0.1586 0.1310 0.2137 0.0408 * p < 0.05 bolded ; SCC - Spearman’s correlation coefficient CVA – cerebrovascular incident

62
Table 4.2b: Maximum temperature
Call Determinant Groupings 2002 2003 2004 2005 SCC p-value* SCC p-value* SCC p-value* SCC p-value* Heat/cold exposure 0.5541 <.0001 0.4687 <.0001 0.4383 <.0001 0.7268 <.0001 Unconscious/fainting 0.1932 0.0651 0.0380 0.7193 0.1483 0.1584 0.1422 0.1763 Cardiac or respiratory arrest/death 0.0280 0.7910 -0.0015 0.9886 -0.0518 0.6238 -0.0415 0.6948 Headache 0.0505 0.6325 -0.2840 0.0061 -0.0352 0.7394 -0.1394 0.1851 Sick person -0.1133 0.2823 0.1924 0.0662 0.0169 0.8729 0.1300 0.2166 Stroke/CVA -0.1762 0.0929 -0.1038 0.3250 0.0504 0.6332 -0.2550 0.0142 Breathing problems 0.1135 0.2816 -0.0732 0.4882 -0.0390 0.7123 0.0647 0.5401 Abdominal pain 0.1230 0.2429 -0.0497 0.6378 -0.0493 0.6407 0.0453 0.6678 Psychiatric problems -0.2910 0.0049 0.0586 0.5791 0.0053 0.9602 -0.0526 0.6186 Chest pain -0.2491 0.0166 -0.2005 0.0554 0.1135 0.2813 -0.0398 0.7064 Diabetic problems 0.0565 0.5929 0.0076 0.9425 0.1679 0.1096 -0.0027 0.9798 Unknown problem (man down) 0.2052 0.0497 0.1141 0.2790 0.1862 0.0756 0.1859 0.0761 * p < 0.05 bolded ; SCC - Spearman’s correlation coefficient CVA – cerebrovascular incident

63
Further examination of individual MPDS determinants related to “Heat/cold exposure”
indicated that although all sub-determinants were associated with temperature to various degrees,
the most consistent correlation across summers were in determinants describing patients as
“Alert”, to have “Change in skin colour”, or to be of “Unknown status (3rd party caller)” (Table
4.3). The “Alert” sub-determinant grouping was strongly statistically significant for all years for
both mean and maximum temperature, with the exception of 2004. “Unknown status (3rd party
caller)” was relatively consistent in all years and strongly statistically significant, with the
exception of 2004 for mean temperature. Similarly, “Change in skin colour” was strongly
significant in all summers, for both mean and maximum temperature.
Associations for calls with determinants related to ”Unknown problem (man down)”
were less consistent. Callers described as “Standing, sitting, moving or talking” or of
“Unknown status (3rd party caller)” were positively correlated with daily mean and maximum
temperature (Table 4.3). This relationship was most apparent in 2005 (mean temperature,
SCC=0.26, p=0.01 for the former and SCC=0.22, p=0.03 for the latter). There were not any
statistically significant findings for the “Unknown problem (man down)” sub-determinants in
2002.

64
Table 4.3: Correlation between daily % 911 calls for HRI and mean and maximum temperatures for selected individual determinants Table 4.3a: Mean temperature
Call Determinant Groupings 2002 2003 2004 2005 SCC p-value* SCC p-value* SCC p-value* SCC p-value* Heat/cold exposure Alert 0.4357 <.0001 0.2429 0.0197 0.0787 0.4560 0.4521 <.0001 Change in skin colour 0.2981 0.0039 0.3725 0.0003 0.2220 0.0334 0.4838 <.0001 Unknown status (3rd party caller) 0.4721 <.0001 0.4393 <.0001 0.1533 0.1446 0.3377 0.0010 Cardiac history 0.3673 0.0003 0.1584 0.1316 0.2220 0.0334 -0.1548 0.1408 Not alert 0.4035 <.0001 0.2053 0.0496 0.3415 0.0009 0.0617 0.5592 Unknown problem (man down) Standing, sitting, moving, or talking
0.1305 0.2150 0.1087 0.3023 0.0410 0.6982 0.2564 0.0136
Medical alert notifications -0.1859 0.0760 -0.0965 0.3600 -0.0687 0.5152 -0.2837 0.0061 Unknown status (3rd party caller) 0.1332 0.2055 0.2178 0.0370 0.2119 0.0426 0.2224 0.0331 Life status questionable -0.0159 0.8806 0.1356 0.1975 0.1957 0.0615 -0.0337 0.7499 * p < 0.05 bolded ; SCC - Spearman’s correlation coefficient

65
Table 4.3b: Maximum temperature
Call Determinant Groupings 2002 2003 2004 2005 SCC p-value* SCC p-value* SCC p-value* SCC p-value* Heat/cold exposure Alert 0.4293 <.0001 0.2689 0.0096 0.0847 0.4224 0.4426 <.0001 Change in skin colour 0.2989 0.0038 0.4016 <.0001 0.2913 0.0048 0.4857 <.0001 Unknown status (3rd party caller) 0.4646 <.0001 0.4200 <.0001 0.2098 0.0448 0.3591 0.0004 Cardiac history 0.3657 0.0003 0.2060 0.0488 0.2054 0.0495 -0.1411 0.1797 Not alert 0.3721 0.0003 0.2089 0.0457 0.3890 0.0001 0.0931 0.3776 Unknown problem (man down) Standing, sitting, moving, or talking
0.1614 0.1244 0.0478 0.6510 0.1019 0.3336 0.2091 0.0455
Medical alert notifications -0.1194 0.2570 -0.0412 0.6963 -0.1000 0.3427 -0.2242 0.0317 Unknown status (3rd party caller) 0.1751 0.0950 0.1132 0.2827 0.1782 0.0893 0.1970 0.0598 Life status questionable -0.0229 0.8281 0.0340 0.7477 0.2154 0.0392 -0.0125 0.9062 * p < 0.05 bolded ; SCC - Spearman’s correlation coefficient

66
Given these findings, and that the only consistent overall correlation with temperature
was found for the “Heat/cold exposure” category the case definition for HRI used in subsequent
analyses included the codes outlines in Table 4.4. All sub-determinant groupings were used
given that the overall pattern was positively correlated and that sufficiently high numbers were
needed in further analyses. In addition, a more specific case definition was of interest for this
research as an indicator of more classically defined HRI and the direct impacts of heat. This was
deemed a good starting point upon which to build further work incorporating more broadly
defined, and thus more sensitive, case definitions.
Table 4.4: 911 determinants used in construction of the case definition of HRI
Heat/cold exposure Alert Change in skin colour Unknown status (3rd party caller) Cardiac history Not alert
4.3 Study Objective 1b: Time Series of the Relationship of 911 HRI Calls
and Temperature
Using the HRI case definition that was created during the first part of Study Objective 1,
descriptive statistics of 911 calls for both all emergencies and those meeting the case definition
of HRI are presented in Table 4.5.

67
Table 4.5: Descriptive 911 call statistics by summer, Toronto 2002-2005 (June 1-August 31)
Variable 2002 2003 2004 2005 Ambulance dispatch
variables Daily mean
(st. dev.) Daily mean
(st. dev.) Daily mean
(st. dev.) Daily mean
(st. dev.) All emergency calls 554 (72) 546 (59) 532 (35) 536 (39) Heat-related calls* 2 (4) 1 (2) 1 (1) 2 (3)
Number of calls Number of calls Number of calls Number of calls
All emergency calls 50969 50249 48959 49291 Heat-related calls* 191 91 58 201
* As defined in Table 4.4
Figure 4.4 illustrates the daily pattern of the percentage of all emergency calls for HRI
with mean and maximum temperature for each summer. These figures suggest that the majority
of calls for HRI occurred at maximum temperatures above 28°C in most years. In the hotter
summers of 2002 and 2005, the majority of calls seem to occur at even higher maximum
temperatures (e.g. above a maximum of 30°C). For mean temperature, in 2002 and 2005 it
appears that most calls for HRI occur above 24°C, but this was not the case in 2003 and 2004.

68
Figure 4.4: Proportion of heat-related calls among total calls (expressed as percent) graphed co-temporaneously with maximum daily temperature, 2002-2005 (June 1-August 31) Figure 4.4a: 2002
0
0.5
1
1.5
2
2.5
3
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Date
Heat
-Rel
ated
Cal
ls (%
)
0
5
10
15
20
25
30
35
40
Tem
pera
ture
(C)
Proportion Mean temp Max temp

69
Figure 4.4b: 2003
0
0.5
1
1.5
2
2.5
3
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Date
Heat
-Rel
ated
Cal
ls (%
)
0
5
10
15
20
25
30
35
40
Tem
pera
ture
(C)
Proportion Mean temp Max temp
Figure 4.4c: 2004
0
0.5
1
1.5
2
2.5
3
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Date
Heat
-Rel
ated
Cal
ls (%
)
0
5
10
15
20
25
30
35
40
Tem
pera
ture
(C)
Proportion Mean temp Max temp

70
Figure 4.4d: 2005
0
0.5
1
1.5
2
2.5
3
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Date
Heat
-Rel
ated
Cal
ls (%
)
0
5
10
15
20
25
30
35
40
Tem
pera
ture
(C)
Proportion Mean temp Max temp
The findings from visual inspection of the graphs are supported by analysis using the
Fisher’s exact test for both mean and maximum temperatures (Table 4.6). In 2005, 185 of the
HRI calls occurred on days with a maximum temperature above 28°C and only 16 at
temperatures below this threshold (p <.0001, Fisher’s). A similar relationship is seen with mean
temperature, with 171 of the total 201 calls occurring over 24°C (Table 4.7). Similar patterns are
seen in the other very hot summer of 2002. However, these trends are not as consistent in 2003
and 2004. In both of these summers the majority of calls for HRI actually occurred at
temperatures below a mean of 24°C (e.g. 54 of 91 calls in 2003 and 39 of 58 calls in 2004). For
the maximum temperature threshold there is an even split between the number of HRI calls
above and below 28°C in 2004, and a higher number of calls above this maximum temperature
threshold in 2003 (e.g. 70 of 91 calls).

71
Table 4.6: Number of total calls for heat-related illness occurring on days with a maximum temperature above or below 28°C 2002* 2003* 2004* 2005* Call for HRI Call for HRI Call for HRI Call for HRI Maximum Temperature
Yes No Yes No Yes No Yes No
Above 28°C 163 26321 70 17219 29 6671 185 29278 Below 28°C 28 24457 21 32939 29 42230 16 19812 Total 191 50778 91 50158 58 48901 201 49090 * p-value (Fischer’s) <.0001 per year. Note 2004 departs from general pattern. Table 4.7: Number of total calls for heat-related illness occurring on days with a mean temperature above or below 24°C 2002* 2003* 2004* 2005* Call for HRI Call for HRI Call for HRI Call for HRI Mean Temperature
Yes No Yes No Yes No Yes No
Above 24°C 128 17708 37 8172 19 3882 171 22022 Below 24°C 63 33070 54 41986 39 45019 30 27068 Total 191 50778 91 50158 58 48901 201 49090 * p-value (Fischer’s) <.0001 per year. Note 2003 & 2004 have opposite pattern to 2002 & 2005.
Two analyses, ZIP and GAM, were conducted for each year for both mean and maximum
temperature (Table 4.8). Overall, the estimates between the ZIP and GAM models were
generally similar. In all years, for every one degree increase in mean or maximum temperature
there was a corresponding increase in 911 calls for HRI. These values ranged from
approximately 11% to 36% for every one degree increase in temperature, with nearly all of the
estimates strongly statistically significant (p<.0001). The two most recent summers of 2004 and
2005 demonstrated the highest magnitude of association with an increase in calls of
approximately 30% for both mean and maximum temperature (p<.0001). These values were
slightly lower in the earlier summers of 2002 and 2003, at approximately 20% per one degree
increase in temperature.

72
Effect of day (e.g. weekend versus weekday) was also consistent between years, but only
statistically significant in models of the two hottest summers, 2002 and 2005. The increase in
calls was more pronounced on weekends as compared with weekdays. In the models with a
statistically significant value for the effect of day, this increase on weekends averaged
approximately 50% as compared with weekdays (e.g. 2002 maximum temperature, ZIP
RR=1.47, p=0.04; 2002 mean temperature, ZIP RR=1.66, p=0.01; 2005 maximum temperature
ZIP RR=1.53, p=0.01; 2005 mean temperature, ZIP RR=1.60, p=0.004).
The effect of two other meteorological variables, ozone and relative humidity, was also
examined. Although there was a slight increase in calls associated with ozone levels, it was
statistically insignificant in all models. The findings for relative humidity (RH) were inconsistent
across years. In some models RH had a slight positive effect (e.g. 2002 maximum temperature
ZIP model RR=1.02, p=0.03). In a few cases RH actually had a slight negative effect (e.g. 2005
mean temperature ZIP model RR=0.97, p=0.001; 2004 mean temperature ZIP model RR=0.96,
p=0.05).

73
Table 4.8: Regression analyses associating daily meteorological variables and the proportion of HRI among all ambulance emergency calls Table 4.8a: 2002 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day †
Relative humidity‡ Ozone§
0.1526 0.3842 0.0167 0.0099
1.16 1.47 1.02 1.01
0.0382 0.1875 0.0077 0.0114
<.0001 0.0434 0.0319 0.3857
0.1527 0.2413 0.0129 0.0178
1.16 1.27 1.01 1.01
0.0400 0.2157 0.0092 0.0125
0.0003 0.2668 0.1657 0.1586
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase; Table 4.8b: 2002 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day † Relative humidity‡ Ozone§
0.1871 0.5084 0.0120 0.0113
1.21 1.66 1.01 1.01
0.0384 0.1805 0.0074 0.0103
<.0001 0.0059 0.1085 0.2742
0.1884 0.3506 0.0032 0.0167
1.21 1.42 1.00 1.02
0.0421 0.2260 0.0091 0.0119
<.0001 0.1249 0.7312 0.1636
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.8c: 2003 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day †
Relative humidity‡ Ozone§
0.1017 0.0509 -0.0594 0.0228
1.11 1.05 0.95 1.02
0.0640 0.2678 0.0173 0.0148
0.1153 0.8496 0.0009 0.1254
0.1836 0.0811 -0.0408 0.0169
1.20 1.08 0.96 1.02
0.0647 0.2744 0.0167 0.0154
0.0058 0.7683 0.0167 0.2750
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.8d: 2003 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day † Relative humidity‡ Ozone§
0.1320 -0.1034 -0.0688 0.0189
1.14 0.90 0.93 1.02
0.0696 0.2622 0.0156 0.0152
0.0609 0.6943 <.0001 0.2171
0.2339 0.0657 -0.0546 0.0114
1.26 1.07 0.95 1.01
0.0701 0.2747 0.0153 0.0157
0.0013 0.8115 0.0006 0.4711
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase

74
Table 4.8e: 2004 – Maximum temperature Variable ZIP model GAM Poisson model
estimate RR standard error
p-value estimate RR standard error
p-value
Max. daily temperature* Day †
Relative humidity‡ Ozone§
0.2757 0.3428 -0.0082 -0.0025
1.32 1.41 0.99 1.00
0.0614 0.3100 0.0180 0.0180
<.0001 0.2709 0.6501 0.8862
0.2692 0.2867 -0.0152 -0.0056
1.31 1.33 0.98 0.99
0.0610 0.3044 0.0191 0.0181
<.0001 0.3492 0.4288 0.7577
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.8f: 2004 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day †
Relative humidity‡ Ozone§
0.3090 0.3551 -0.0368 0.0019
1.36 1.43 0.96 1.00
0.0699 0.3116 0.0184 0.0170
<.0001 0.2573 0.0490 0.9125
0.3004 0.2975 -0.0417 -0.0003
1.35 1.35 0.96 1.00
0.0698 0.3075 0.0199 0.0176
<.0001 0.3362 0.0391 0.9844
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.8g: 2005 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day †
Relative humidity‡
0.2575 0.4227 0.0005
1.29 1.53 1.00
0.0313 0.1563 0.0090
<.0001 0.0081 0.9525
0.2713 0.2937 -0.0004
1.31 1.34 1.00
0.0305 0.1593 0.0084
<.0001 0.1396 0.9723
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase Table 4.8h: 2005 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day †
Relative humidity‡
0.2746 0.4685 -0.0274
1.32 1.60 0.97
0.0337 0.1598 0.0081
<.0001 0.0042 0.0011
0.2867 0.3759 -0.0274
1.33 1.46 0.97
0.0303 0.1584 0.0073
<.0001 0.0435 0.0016
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase

75
To further investigate the role of relative humidity subsequent models that included an
interaction term of temperature and relative humidity were analyzed using a ZIP model (Table
4.9). The relative risk for the interaction term of relative humidity and both mean and maximum
temperature was 1.00 or 1.01 and statistically insignificant in all models. Further, a comparison
was made between the Akaike’s information criterion (AIC) and Bayesian information criterion
(BIC) values between the models with and without the interaction term. These are two
commonly used measures to estimate model fit. Both values were consistently lower in the
models without the interaction term, indicating a better fit model than the ones with the
interaction term (Table 4.10).
Table 4.9: Regression analyses associating the interaction between temperature and relative humidity with the proportion of HRI among all ambulance emergency calls Table 4.9a: 2002 – Maximum temperature
Variable ZIP model estimate RR standard error p-value Interaction Maximum daily temperature* Day † Relative humidity‡ Ozone§
-0.0028 0.3468 0.4346 0.1011 0.0071
1.00 1.41 1.54 1.11 1.01
0.0023 0.1678 0.1924 0.0709 0.0115
0.2348 0.0415 0.0263 0.1571 0.5397
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.9b: 2002 – Mean temperature
Variable ZIP model estimate RR standard error p-value Interaction Mean daily temperature* Day † Relative humidity‡ Ozone§
-0.0025 0.3535 0.5325 0.0734 0.0107
1.00 1.42 1.70 1.08 1.01
0.0027 0.1806 0.1836 0.0651 0.0103
0.3455 0.0533 0.0047 0.2623 0.3047
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase

76
Table 4.9c: 2003 – Maximum temperature Variable ZIP model
estimate RR standard error p-value Interaction Maximum daily temperature* Day † Relative humidity‡ Ozone§
0.0018 -0.0129 -0.0637 -0.1088 0.0233
1.00 0.99 0.94 0.90 1.02
0.0045 0.2957 0.2699 0.1266 0.0148
0.6934 0.9654 0.8139 0.3922 0.1187
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.9d: 2003 – Mean temperature
Variable ZIP model estimate RR standard error p-value Interaction Mean daily temperature* Day † Relative humidity‡ Ozone§
-0.0006 0.1724 -0.0987 -0.0546 0.0187
1.00 1.19 0.91 0.95 1.02
0.0059 0.3769 0.2658 0.1312 0.0152
0.9134 0.6485 0.7113 0.6784 0.2216
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.9e: 2004 –Maximum temperature
Variable ZIP model estimate RR standard error p-value Interaction Maximum daily temperature* Day† Relative humidity‡ Ozone§
0.0070 -0.2009 0.3575 -0.1911 -0.0046
1.01 0.82 1.43 0.83 1.00
0.0059 0.4008 0.3093 0.1547 0.0178
0.2370 0.6174 0.2508 0.2200 0.7965
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.9f: 2004 – Mean temperature
Variable ZIP model estimate RR standard error p-value Interaction Mean daily temperature* Day † Relative humidity‡ Ozone§
0.0063 -0.1154 0.3676 -0.1690 0.0001
1.01 0.89 1.44 0.84 1.00
0.0059 0.3978 0.3131 0.1249 0.0171
0.2859 0.7725 0.2434 0.1792 0.9990
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase

77
Table 4.9g: 2005 – Maximum temperature Variable ZIP model
estimate RR standard error p-value Interaction Maximum daily temperature* Day † Relative humidity‡
-0.0023 0.4006 0.4070 0.0707
1.00 1.49 1.50 1.07
0.0030 0.1956 0.1578 0.0946
0.4580 0.0435 0.0115 0.4567
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase Table 4.9h: 2005 – Mean temperature
Variable ZIP model estimate RR standard error p-value Interaction Mean daily temperature* Day † Relative humidity‡
0.0031 0.0866 0.4380 -0.1053
1.00 1.09 1.55 0.90
0.0040 0.2491 0.1585 0.1021
0.4402 0.7288 0.0069 0.3049
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase Table 4.10: Comparison of BIC and AIC values between models with and without the interaction term (relative humidity and mean or maximum temperature)
Akaike’s information criterion (AIC) Model With Interaction Term Without Interaction Term 2002 max temp 299.2 298.6 2003 max temp 218.8 217 2004 max temp 176.5 175.9 2005 max temp 303.9 302.4 2002 mean temp 306.2 305.1 2003 mean temp 218 216 2004 mean temp 178.5 177.6 2005 mean temp 293.6 292.1
Bayesian information criterion (BIC) Model With Interaction Term Without Interaction Term 2002 max temp 321.8 318.7 2003 max temp 241.4 237 2004 max temp 199.2 196.1 2005 max temp 324.1 320.1 2002 mean temp 328.9 325.3 2003 mean temp 240.6 236.1 2004 mean temp 201.1 197.7 2005 mean temp 313.8 309.7

78
Given the literature suggesting a lag effect of temperature on health outcomes, a lag of
one day was examined for both mean and maximum temperature using a ZIP model and a GAM
Poisson model (Table 4.11). Although not as strong as the same day effect, a lag effect of one
day is evident, ranging from a 7 to18% increase in ambulance response calls for HRI for a lag of
one day for maximum temperature (p<.0001). For the lag effect of mean temperature the range
was slightly higher, between 9 to 26% increase in HRI calls. The strongest effects were seen in
the most recent summers of 2004 and 2005.
Table 4.11 Regression analyses associating daily meteorological variables and the proportion of HRI among all ambulance emergency calls with a 1 day lag i.e. temperature on day before rather than same day Table 4.11a: 2002 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. prior day temp.* Day † Relative humidity‡ Ozone§
0.1080 0.4248 0.0162 0.0347
1.11 1.53 1.02 1.04
0.0277 0.1947 0.0077 0.0076
0.0002 0.0317 0.0391 <.0001
0.1209 0.3693 0.0076 0.0397
1.13 1.45 1.01 1.04
0.0327 0.2359 0.0092 0.0093
0.0004 0.1215 0.4122 0.0001
p < 0.05 bolded ; * 1°C increase, day before; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.11b: 2002 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean prior day temp.* Day † Relative humidity‡ Ozone§
0.1327 0.4137 0.0123 0.0370
1.14 1.51 1.01 1.04
0.0305 0.1921 0.0078 0.0074
<.0001 0.0339 0.1195 <.0001
0.1569 0.4191 0.0023 0.0406
1.17 1.52 1.00 1.04
0.0352 0.2270 0.0089 0.0088
<.0001 0.0688 0.7999 <.0001
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase

79
Table 4.11c: 2003 – Maximum temperature Variable ZIP model GAM Poisson model
estimate RR standard error
p-value estimate RR standard error
p-value
Max. prior day temp.* Day † Relative humidity‡ Ozone§
0.0713 -0.0861 -0.0753 0.0257
1.07 0.92 0.93 1.03
0.0451 0.2645 0.0163 0.0136
0.1171 0.7456 <.0001 0.0611
0.0666 0.1080 -0.0633 0.0396
1.07 1.11 0.94 1.04
0.0504 0.2903 0.0155 0.0136
0.1907 0.7109 0.0001 0.0046
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.11d: 2003 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean prior day temp.* Day † Relative humidity‡ Ozone§
0.0810 -0.1598 -0.0798 0.0273
1.08 0.85 0.92 1.03
0.0539 0.2647 0.0172 0.0131
0.1362 0.5475 <.0001 0.0400
0.0838 0.0613 -0.0666 0.0404
1.09 1.06 0.94 1.04
0.0559 0.2826 0.0156 0.0127
0.1382 0.8288 0.0001 0.0022
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.11e: 2004 –Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. prior day temp.* Day† Relative humidity‡ Ozone§
0.1679 0.4039 -0.0261 0.0409
1.18 1.50 0.97 1.04
0.0460 0.3064 0.0181 0.0129
0.0004 0.1906 0.1524 0.0021
0.1628 0.3057 -0.0407 -0.0079
1.18 1.36 0.96 0.99
0.0498 0.3289 0.0207 0.0149
0.0016 0.3555 0.0532 0.0041
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.11f: 2004 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean prior day temp.* Day † Relative humidity‡ Ozone§
0.2280 0.4148 -0.0364 0.0424
1.26 1.51 0.96 1.04
0.0534 0.3052 0.0192 0.0125
<.0001 0.1774 0.0605 0.0010
0.2320 0.3432 -0.0510 0.0472
1.26 1.41 0.95 1.05
0.0559 0.3122 0.0207 0.0138
0.0001 0.2751 0.0159 0.0010
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase

80
Table 4.11g: 2005 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. prior day temp.* Day † Relative humidity‡
0.1669 0.2730 -0.0161
1.18 1.31 0.98
0.0260 0.1576 0.0080
<.0001 0.0866 0.0473
0.1653 0.2900 -0.0175
1.18 1.34 0.98
0.0349 0.2235 0.0111
<.0001 0.1981 0.1189
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase Table 4.11h: 2005 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean prior day temp.* Day † Relative humidity‡
0.2280 0.4148 -0.0364
1.26 1.51 0.96
0.0534 0.3052 0.0192
<.0001 0.1774 0.0605
0.1755 0.3066 -0.0301
1.19 1.36 0.97
0.0363 0.2228 0.0104
<.0001 0.1725 0.0049
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase
4.4 Study Objective 2a: Validity Assessment
The number of emergency department visits (i.e. NACRS data) for HRI and 911 calls for
HRI displays a similar pattern, with the highest number of visits/calls occurring during the
summers of 2002 and 2005, and much lower numbers in 2003 and 2004. With the exception of
slightly lower ED visits for all-causes in 2003, the total number of all visits for ED is relatively
consistent throughout the four summers. These patterns are illustrated in the descriptive
summary in Table 4.12.

81
Table 4.12: Descriptive emergency department visit (NACRS dataset) statistics by summer, Toronto 2002-2005 (June 1-August 31)
Variable 2002 2003 2004 2005 NACRS Daily mean
(st. dev.) Daily mean
(st. dev.) Daily mean
(st. dev.) Daily mean (st. dev.)
All visits 2018 (97.4) 1582 (148.9) 1867 (95.6) 1933 (88.0) Heat-related visits* 1 (1.8) 0.5 (0.95) 0.3 (0.63) 0.8 (1.3) Number of visits Number of visits Number of visits Number of visits
All visits 185622 145537 171719 177880 Heat-related visits* 93 41 26 70
* As defined by the ICD-10-CA codes in Table 3.2
Analyses using ZIP and GAM models were also conducted for the NACRS data for each
year for both mean and maximum temperature (Table 4.13). In all years, for every one degree
increase in mean or maximum temperature there was a corresponding increase in emergency
department visits for HRI. These values ranged from approximately 11% to 33% for every one
degree increase in temperature, with nearly all of the estimates strongly statistically significant
(p<.0001) (exception of 2003 with insignificant values for temperature). The most recent study
summer of 2005 demonstrated the highest magnitude of association with an increase in calls of
above 30% per degree increase for both mean and maximum temperature (p<.0001). These
ranges and patterns are very similar to those reported in the HRI 911 call time series analysis.
Estimating the effects of other variables in the models including day (e.g. weekend versus
weekday), ozone, and relative humidity is difficult as none of the models had statistically
significant results for these variables, perhaps because of decreased power associated with lower
absolute number of cases. As the primary aim of this analysis was to compare the relationship
between temperature and ED visits for HRI with 911 calls for HRI, investigation of the role of
these other covariates or lags for ED visits was not pursued.

82
Table 4.13: Regression analyses associating daily meteorological variables and the proportion of HRI among all emergency room visits Table 4.13a: 2002 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day † Relative humidity‡ Ozone§
0.2622 0.1176 0.0074 -0.0106
1.30 1.12 1.01 0.99
0.0574 0.2997 0.0124 0.0162
<.0001 0.6955 0.5524 0.5144
0.2469 -0.0120 0.0167 -0.0064
1.28 0.99 1.02 0.99
0.0450 0.2692 0.0134 0.0126
<.0001 0.9645 0.2142 0.6152
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.13b: 2002 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day † Relative humidity‡ Ozone§
0.2539 0.1861 -0.0051 -0.0028
1.29 1.20 0.99 1.00
0.0587 0.3156 0.0127 0.0155
<.0001 0.5569 0.6892 0.8572
0.2454 0.0335 0.0022 0.0011
1.28 1.03 1.00 1.00
0.0487 0.2907 0.0140 0.0126
<.0001 0.9086 0.8767 0.9337
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.13c: 2003 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day † Relative humidity‡ Ozone
0.0999 -0.0188 -0.0294 0.0416
1.11 0.98 0.97 1.04
0.0960 0.4611 0.0232 0.0228
0.2989 0.9677 0.2084 0.0708
0.1087 -0.1774 -0.0317 0.0438
1.11 0.84 0.97 1.04
0.0871 0.3996 0.0218 0.0211
0.2158 0.6584 0.1496 0.0414
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase

83
Table 4.13d: 2003 – Mean temperature Variable ZIP model GAM Poisson model
estimate RR standard error
p-value estimate RR standard error
p-value
Mean daily temperature* Day † Relative humidity‡ Ozone§
0.1369 -0.0212 -0.0355 0.0373
1.15 0.98 0.97 1.04
0.1098 0.4684 0.2056 0.0238
0.2158 0.9640 0.0875 0.1205
0.1537 -0.1964 -0.0378 0.0382
1.17 0.82 0.96 1.04
0.0962 0.4083 0.0203 0.0217
0.1141 0.6318 0.0667 0.0820
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.13e: 2004 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day † Relative humidity‡ Ozone§
0.1949 0.6969 -0.0004 0.0052
1.22 2.01 1.00 1.01
0.0895 0.4532 0.0251 0.0287
0.0320 0.1276 0.9882 0.8565
0.2037 0.3322 -0.0151 0.0186
1.23 1.39 0.99 1.02
0.0797 0.4134 0.0210 0.0267
0.0126 0.4241 0.4749 0.4879
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.13f: 2004 – Mean temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day † Relative humidity‡ Ozone§
0.2327 0.7031 -0.0213 0.0070
1.26 2.02 0.98 1.01
0.1039 0.4568 0.0253 0.0277
0.0275 0.1272 0.4017 0.8004
0.2428 0.3550 -0.0362 0.0195
1.27 1.43 0.96 1.02
0.0937 0.4239 0.0217 0.0264
0.0114 0.4049 0.0990 0.4617
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase Table 4.13g: 2005 – Maximum temperature
Variable ZIP model GAM Poisson model estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day † Relative humidity‡
0.2701 -0.0226 0.0225
1.31 0.98 1.02
0.0565 0.3032 0.0163
<.0001 0.9406 0.1698
0.2559 0.2122 0.0178
1.29 1.24 1.02
0.0556 0.3156 0.0192
<.0001 0.5032 0.3552
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase

84
Table 4.13h: 2005 – Mean temperature Variable ZIP model GAM Poisson model
estimate RR standard error
p-value estimate RR standard error
p-value
Mean daily temperature* Day † Relative humidity‡
0.2885 0.0066 -0.0071
1.33 1.01 0.99
0.0561 0.2992 0.0149
<.0001 0.9824 0.6370
0.2764 0.3234 -0.0116
1.32 1.38 0.99
0.0539 0.3174 0.0171
<.0001 0.3114 0.4996
* 1°C increase; † weekday vs. weekend; ‡ 1% increase; § 1 ppb increase
Figure 4.5 compares the volume of HRI 911 calls with the volume of HRI ED visits over
each of the four study summers. The temporal trends are very similar, though the volume of ED
visits is less. It is interesting to note that the 911 calls seem more sensitive to the impact of heat
during outdoor events, as is illustrated by the larger spikes during World Youth Day in 2002
(July 27 & 28) and an outdoor concert in 2003 (July 30).
Figure 4.5: HRI 911 calls, emergency room visits, and heat alert days, by summer, Toronto 2002-2005 Figure 4.5a: 2002
0
2
4
6
8
10
12
14
16
18
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Num
ber
of H
eat C
alls
or
Vis
its
Heat Alert Day 911 Calls NACRS

85
Figure 4.5b: 2003
0
2
4
6
8
10
12
14
16
18
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Num
ber
of H
eat C
alls
or
Vis
its
Heat Alert Day 911 Calls NACRS
Figure 4.5c: 2004
0
2
4
6
8
10
12
14
16
18
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Num
ber
of H
eat C
alls
or
Visi
ts
Heat Alert Day 911 Calls NACRS

86
Figure 4.5d: 2005
0
2
4
6
8
10
12
14
16
18
6/1 6/6 6/11 6/16 6/21 6/26 7/1 7/6 7/11 7/16 7/21 7/26 7/31 8/5 8/10 8/15 8/20 8/25 8/30
Num
ber
of H
eat C
alls
or V
isits
Heat Alert Day 911 Calls NACRS
In order to decide the appropriate spike thresholds of 911 calls and ED visits to use in
further comparisons of the two data sources, a Receiver Operating Curve (ROC) was created.
The ROC plot illustrates the tradeoff in sensitivity and specificity using various cut-offs for
spikes in 911 calls and NACRS visits (Figure 4.6). Selecting the values closest to the (0,1)
coordinate results in a spike threshold of days with three or more 911 calls for heat and two or
more ED visits for heat.

87
Figure 4.6: Receiver Operating Curve (ROC) plot of 911 and NACRS thresholds vs. heat alerts
00.10.20.30.40.50.60.70.80.9
1
0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9 1
FPF (1-specificity)
TPF
(sen
sitiv
ity)
911 NACRS
Comparing these two data sources to each other, based on the spike thresholds considered
most appropriate, 911 call spike days were more common than ED visit spike days (Table 4.14).
Using both data sources, spike days were more frequent than heat alert days (McNemar’s p=0.01
(911) and p<.0001 (NACRS)). However, under some spike thresholds, these comparative
relationships changed, demonstrating sensitivity to threshold definition (see Appendix G).
Table 4.14: Comparisons of classifications of days with excess HRI by different systems, across all four summers Table 4.14a: Heat Alerts Compared with 911 Call Spikes (all summers combined) Heat Alert or Extreme Heat Alert Day 911 Call Spike* Yes No Total Yes 35 32 67 No 15 286 301 Total 50 318 368 p-value (McNemar’s) for table = 0.0131 * spike is defined as a day where there are 3 or more heat-related calls

88
Table 4.14b: Heat Alerts Compared with ED Visit Spikes (all summers combined) Heat Alert or Extreme Heat Alert Day NACRS Visit Spike* Yes No Total Yes 28 29 57 No 22 289 311 Total 50 318 368 p-value (McNemar’s) for table <0.0001 * spike is defined as a day where there are 2 or more heat-related visits Table 4.14c: ED Visit Spikes compared with 911 Call Spikes (all summers combined) 911 Call Spike* NACRS Visit Spike** Yes No Total Yes 33 24 57 No 34 277 311 Total 67 301 368 p-value (McNemar’s) for table <0.0001 * 911 call spike is defined as a day where there are 3 or more heat-related calls ** NACRS visit spike is defined as a day where there are 2 or more heat-related visits 4.5 Study Objective 2b: Timing Assessment
A timing assessment was executed to determine whether there were major differences in
the temporal trend of spikes of 911 HRI calls versus ED HRI visits using a commonly used
aberration detection software, EARS. Figure 4.7 illustrates the findings from these analyses.
From these graphs it appears that there was not a consistent lead time by one of the two
morbidity data sources. In some cases it appears that ED visits spike before 911 calls and vice
versa. Specifically, in 2005 it seems that 911 calls may have peaked earlier than ED visits. The
type of CUSUM flag generated is similar throughout years, with all CUSUM alerts, or the two
most sensitive (C2 and C3), generated in most cases.

89
Figure 4.7: Output from EARS analysis of aberrations for 911 and ED HRI visits Figure 4.7a: 911 calls for HRI - 2002
0
2
4
6
8
10
12
14
16
6/1/
02
6/3/
02
6/5/
02
6/7/
02
6/9/
02
6/11
/02
6/13
/02
6/15
/02
6/17
/02
6/19
/02
6/21
/02
6/23
/02
6/25
/02
6/27
/02
6/29
/02
7/1/
02
7/3/
02
7/5/
02
7/7/
02
7/9/
02
7/11
/02
7/13
/02
7/15
/02
7/17
/02
7/19
/02
7/21
/02
7/23
/02
7/25
/02
7/27
/02
7/29
/02
7/31
/02
8/2/
02
8/4/
02
8/6/
02
8/8/
02
8/10
/02
8/12
/02
8/14
/02
8/16
/02
8/18
/02
8/20
/02
8/22
/02
8/24
/02
8/26
/02
8/28
/02
8/30
/02
Figure 4.7b: ED visits for HRI - 2002
0
1
2
3
4
5
6
7
8
9
10
6/1/
02
6/3/
02
6/5/
02
6/7/
02
6/9/
02
6/11
/02
6/13
/02
6/15
/02
6/17
/02
6/19
/02
6/21
/02
6/23
/02
6/25
/02
6/27
/02
6/29
/02
7/1/
02
7/3/
02
7/5/
02
7/7/
02
7/9/
02
7/11
/02
7/13
/02
7/15
/02
7/17
/02
7/19
/02
7/21
/02
7/23
/02
7/25
/02
7/27
/02
7/29
/02
7/31
/02
8/2/
02
8/4/
02
8/6/
02
8/8/
02
8/10
/02
8/12
/02
8/14
/02
8/16
/02
8/18
/02
8/20
/02
8/22
/02
8/24
/02
8/26
/02
8/28
/02
8/30
/02

90
Figure 4.7c: 911 calls for HRI - 2003
0
2
4
6
8
10
12
14
16
186/
1/03
6/3/
03
6/5/
03
6/7/
03
6/9/
03
6/11
/03
6/13
/03
6/15
/03
6/17
/03
6/19
/03
6/21
/03
6/23
/03
6/25
/03
6/27
/03
6/29
/03
7/1/
03
7/3/
03
7/5/
03
7/7/
03
7/9/
03
7/11
/03
7/13
/03
7/15
/03
7/17
/03
7/19
/03
7/21
/03
7/23
/03
7/25
/03
7/27
/03
7/29
/03
7/31
/03
8/2/
03
8/4/
03
8/6/
03
8/8/
03
8/10
/03
8/12
/03
8/14
/03
8/16
/03
8/18
/03
8/20
/03
8/22
/03
8/24
/03
8/26
/03
8/28
/03
8/30
/03
Figure 4.7d: ED visits for HRI - 2003
0
1
2
3
4
5
6
7
6/1/
03
6/3/
03
6/5/
03
6/7/
03
6/9/
03
6/11
/03
6/13
/03
6/15
/03
6/17
/03
6/19
/03
6/21
/03
6/23
/03
6/25
/03
6/27
/03
6/29
/03
7/1/
03
7/3/
03
7/5/
03
7/7/
03
7/9/
03
7/11
/03
7/13
/03
7/15
/03
7/17
/03
7/19
/03
7/21
/03
7/23
/03
7/25
/03
7/27
/03
7/29
/03
7/31
/03
8/2/
03
8/4/
03
8/6/
03
8/8/
03
8/10
/03
8/12
/03
8/14
/03
8/16
/03
8/18
/03
8/20
/03
8/22
/03
8/24
/03
8/26
/03
8/28
/03
8/30
/03

91
Figure 4.7e: 911 calls for HRI - 2004
0
1
2
3
4
5
6
6/1/
04
6/3/
04
6/5/
04
6/7/
04
6/9/
04
6/11
/04
6/13
/04
6/15
/04
6/17
/04
6/19
/04
6/21
/04
6/23
/04
6/25
/04
6/27
/04
6/29
/04
7/1/
04
7/3/
04
7/5/
04
7/7/
04
7/9/
04
7/11
/04
7/13
/04
7/15
/04
7/17
/04
7/19
/04
7/21
/04
7/23
/04
7/25
/04
7/27
/04
7/29
/04
7/31
/04
8/2/
04
8/4/
04
8/6/
04
8/8/
04
8/10
/04
8/12
/04
8/14
/04
8/16
/04
8/18
/04
8/20
/04
8/22
/04
8/24
/04
8/26
/04
8/28
/04
8/30
/04
Figure 4.7f: ED visits for HRI - 2004
0
1
2
3
4
5
6/1/
04
6/3/
04
6/5/
04
6/7/
04
6/9/
04
6/11
/04
6/13
/04
6/15
/04
6/17
/04
6/19
/04
6/21
/04
6/23
/04
6/25
/04
6/27
/04
6/29
/04
7/1/
04
7/3/
04
7/5/
04
7/7/
04
7/9/
04
7/11
/04
7/13
/04
7/15
/04
7/17
/04
7/19
/04
7/21
/04
7/23
/04
7/25
/04
7/27
/04
7/29
/04
7/31
/04
8/2/
04
8/4/
04
8/6/
04
8/8/
04
8/10
/04
8/12
/04
8/14
/04
8/16
/04
8/18
/04
8/20
/04
8/22
/04
8/24
/04
8/26
/04
8/28
/04
8/30
/04

92
Figure 4.7g: 911 calls for HRI - 2005
0
2
4
6
8
10
12
14
16
186/
1/05
6/3/
05
6/5/
05
6/7/
05
6/9/
05
6/11
/05
6/13
/05
6/15
/05
6/17
/05
6/19
/05
6/21
/05
6/23
/05
6/25
/05
6/27
/05
6/29
/05
7/1/
05
7/3/
05
7/5/
05
7/7/
05
7/9/
05
7/11
/05
7/13
/05
7/15
/05
7/17
/05
7/19
/05
7/21
/05
7/23
/05
7/25
/05
7/27
/05
7/29
/05
7/31
/05
8/2/
05
8/4/
05
8/6/
05
8/8/
05
8/10
/05
8/12
/05
8/14
/05
8/16
/05
8/18
/05
8/20
/05
8/22
/05
8/24
/05
8/26
/05
8/28
/05
8/30
/05
Figure 4.7h: ED visits for HRI - 2005
0
1
2
3
4
5
6
7
8
6/1/
05
6/3/
05
6/5/
05
6/7/
05
6/9/
05
6/11
/05
6/13
/05
6/15
/05
6/17
/05
6/19
/05
6/21
/05
6/23
/05
6/25
/05
6/27
/05
6/29
/05
7/1/
05
7/3/
05
7/5/
05
7/7/
05
7/9/
05
7/11
/05
7/13
/05
7/15
/05
7/17
/05
7/19
/05
7/21
/05
7/23
/05
7/25
/05
7/27
/05
7/29
/05
7/31
/05
8/2/
05
8/4/
05
8/6/
05
8/8/
05
8/10
/05
8/12
/05
8/14
/05
8/16
/05
8/18
/05
8/20
/05
8/22
/05
8/24
/05
8/26
/05
8/28
/05
8/30
/05

93
The timing association was further examined by calculating cross-correlations for the
study period. Figure 4.8 confirms the EARS findings that the correlation between the two
variables was greatest at lag 0 (correlation = 0.5472) over all four summers, indicating there was
no delay effect. This same relationship is seen for the summers 2002-2004 (Figures 4.9).
However, the summer of 2005 presents a different relationship, with the cross-correlation
greatest at lag -2 (correlation = 0.6262), indicating that 911 spiked approximately 2 days earlier
than the ED visits (Figure 4.9d), as suggested in the previous EARS graphs.
Figure 4.8: Cross-correlation between 911 and NACRS data – All summers
Lag Covariance Correlation -1 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 1 -10 0.00033797 0.01186 | . | . | -9 0.0011894 0.04175 | . |*. | -8 0.0012662 0.04445 | . |*. | -7 0.0014645 0.05141 | . |*. | -6 0.0017060 0.05989 | . |*. | -5 0.0041266 0.14487 | . |*** | -4 0.0061733 0.21672 | . |**** | -3 0.0089020 0.31251 | . |****** | -2 0.011962 0.41995 | . |******** | -1 0.014567 0.51138 | . |********** | 0 0.015588 0.54724 | . |*********** | 1 0.012401 0.43534 | . |********* | 2 0.0086641 0.30416 | . |****** | 3 0.0045753 0.16062 | . |*** | 4 0.0028832 0.10122 | . |** | 5 0.0025543 0.08967 | . |** | 6 0.0028637 0.10053 | . |** | 7 0.0011119 0.03904 | . |*. | 8 0.0013468 0.04728 | . |*. | 9 0.0020185 0.07086 | . |*. | 10 0.0015627 0.05486 | . |*. |

94
Figure 4.9a: Cross-correlation between 911 and NACRS data – 2002
Figure 4.9b: Cross-correlation between 911 and NACRS data – 2003
Lag Covariance Correlation -1 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 1 -10 -0.0007368 -.01660 | . | . | -9 -0.0013578 -.03058 | . *| . | -8 -0.0020687 -.04660 | . *| . | -7 -0.0014142 -.03186 | . *| . | -6 0.0033486 0.07543 | . |** . | -5 0.0072455 0.16321 | . |***. | -4 0.0069556 0.15668 | . |***. | -3 0.010298 0.23195 | . |***** | -2 0.016310 0.36740 | . |******* | -1 0.027489 0.61919 | . |************ | 0 0.027825 0.62676 | . |************* | 1 0.020114 0.45307 | . |********* | 2 0.012191 0.27462 | . |***** | 3 0.0033113 0.07459 | . |* . | 4 -0.0001159 -.00261 | . | . | 5 0.0032793 0.07387 | . |* . | 6 0.0052438 0.11812 | . |** . | 7 0.0015951 0.03593 | . |* . | 8 -0.0015654 -.03526 | . *| . | 9 0.00012337 0.00278 | . | . | 10 0.0019374 0.04364 | . |* . |
Lag Covariance Correlation -1 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 1 -10 -0.0019277 -.10386 | . **| . | -9 0.00045047 0.02427 | . | . | -8 0.0017353 0.09349 | . |** . | -7 -0.0001465 -.00789 | . | . | -6 -0.0009160 -.04935 | . *| . | -5 -0.0011578 -.06238 | . *| . -4 -0.0012461 -.06713 | . *| . | -3 0.0013292 0.07161 | . |* . | -2 0.0022400 0.12068 | . |** . | -1 0.0047549 0.25617 | . |***** | 0 0.0091106 0.49083 | . |********** | 1 0.0090057 0.48518 | . |********** | 2 0.0038970 0.20995 | . |**** | 3 0.0024977 0.13456 | . |***. | 4 0.00010009 0.00539 | . | . | 5 0.00021729 0.01171 | . | . | 6 -0.0007139 -.03846 | . *| . | 7 -0.0003551 -.01913 | . | . | 8 0.0032374 0.17441 | . |***. | 9 0.0029316 0.15794 | . |***. | 10 0.0015640 0.08426 | . |** . |

95
Figure 4.9c: Cross-correlation between 911 and NACRS data – 2004
Figure 4.9d: Cross-correlation between 911 and NACRS data – 2005
Lag Covariance Correlation -1 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 1 -10 0.00031645 0.05131 | . |* . | -9 0.00001050 0.00170 | . | . | -8 -0.0008078 -.13099 | .***| . | -7 -0.0006823 -.11064 | . **| . | -6 0.00034631 0.05616 | . |* . | -5 -0.0004464 -.07239 | . *| . | -4 -0.0005354 -.08681 | . **| . | -3 -0.0003301 -.05354 | . *| . | -2 0.00042176 0.06839 | . |* . | -1 0.0012529 0.20317 | . |**** | 0 0.0023615 0.38293 | . |******** | 1 0.00039259 0.06366 | . |* . | 2 0.00026366 0.04275 | . |* . | 3 0.00010914 0.01770 | . | . | 4 -0.0003370 -.05465 | . *| . | 5 0.0011753 0.19058 | . |**** | 6 -0.0000343 -.00556 | . | . | 7 0.00011774 0.01909 | . | . | 8 0.00005725 0.00928 | . | . | 9 0.00096997 0.15729 | . |***. | 10 0.00040986 0.06646 | . |* . |
Lag Covariance Correlation -1 9 8 7 6 5 4 3 2 1 0 1 2 3 4 5 6 7 8 9 1 -10 -0.0036682 -.09958 | . **| . | -9 -0.0014776 -.04011 | . *| . | -8 -0.0009440 -.02562 | . *| . | -7 0.0010417 0.02828 | . |* . | -6 -0.0029077 -.07893 | . **| . | -5 0.0041595 0.11291 | . |** . | -4 0.013085 0.35520 | . |******* | -3 0.018204 0.49415 | . |********** | -2 0.023070 0.62624 | . |************* | -1 0.019289 0.52362 | . |********** | 0 0.017901 0.48593 | . |********** | 1 0.014668 0.39818 | . |******** | 2 0.012556 0.34083 | . |******* | 3 0.0065573 0.17800 | . |**** | 4 0.0057333 0.15563 | . |***. | 5 -0.0011434 -.03104 | . *| . | 6 0.00037587 0.01020 | . | . | 7 -0.0033573 -.09114 | . **| . | 8 -0.0033615 -.09125 | . **| . | 9 -0.0030238 -.08208 | . **| . | 10 -0.0042542 -.11548 | . **| . |

96
4.6 Study Objective 3: Geospatial Distribution of HRI in Toronto
The map of the proportion of HRI calls by neighbourhood illustrates clear geospatial
heterogeneity in the burden of HRI in Toronto (Figure 4.10). This is apparent in both the
individual maps of each summer, and the map that combines the mean values per neighbourhood
for all study summers (Figure 4.11). Areas with high rates of HRI include those located along the
waterfront, particularly areas centered around summer outdoor recreational activities. The area
around Toronto Islands consistently shows a relatively high proportion of HRI calls as compared
with other neighbourhoods. Areas around Little Italy, Lansing-Westgate, York University,
recreational locations along the waterfront, and parts of northeast Toronto also exhibit a higher
proportion of HRI calls. Cluster detection analyses of Local Moran maps based on Local
Indicators of Spatial Autocorrelation (LISA) support these findings (Figure 4.12). The Moran’s I
statistic is equal to 0.1257 (p=0.001) indicating some positive spatial autocorrelation. Figure
4.12a illustrates the cluster map of neighbourhoods with a high burden of HRI next to similar
neighbourhoods (high-high), and therefore positive spatial autocorrelation, as well as
neighbourhoods with a low burden of HRI next to similar neighbourhoods (low-low). The
significance of these clusters is provided in the statistical significance map in Figure 4.12b.
In an effort to better understand if HRI burden may be related to socioeconomic status
(SES), a map of SES was created based on 2001 census data of the percentage of low-income
families (number of families under Low Income Cut-Off (LICO). This map illustrates the classic
“u-shaped” or “doughnut” pattern where the inner core of the city is characterized by higher SES
neighbourhoods and the outer suburbs are characterized by lower-income neighbourhoods.182
When comparing these patterns to a map of socioeconomic status, it is clear that there are

97
similarities (Figure 4.13). In particular, areas that consistently have an absence of 911 HRI calls
are also those areas with a higher socioeconomic status (e.g. areas around the Bridle Path). One
of the differences is that there are core areas of the city that have a high burden of 911 HRI calls,
although they are not necessarily low SES neighbourhoods. As will be suggested in the
discussion, this may partly be explained by a greater proportion of green space (e.g. parks) in
these neighbourhoods and therefore more outdoor activity as compared with low SES
neighbourhoods.

98
Figure 4.10: Percentage of 911 calls for HRI by neighbourhood Figure 4.10a: Summer 2002

99
Figure 4.10b: Summer 2003

100
Figure 4.10c: Summer 2004

101
Figure 4.10d: Summer 2005

102
Figure 4.11: Mean percentage of 911 HRI calls for Toronto summers, 2002-2005

103
Figure 4.12a: Spatial autocorrelation, Local Moran’s I

104
Figure 4.12b: Spatial autocorrelation, significance map

105
Figure 4.13: Low-income families (number of families under Low Income Cut-Off (LICO) as a percentage of all economic families (2001)

106
Chapter 5
Discussion 5.1 Study Objective 1a: Developing a Case Definition for HRI
Through a combination of clinically-informed expertise and empirical methods, plausible
HRI indicators were developed using medical dispatch call determinant codes. The most specific
“Heat/cold exposure” category was clearly associated with both mean and maximum
temperature. This relationship was consistent for all study years and supported by both the
clinical and empirical findings. One would expect that these calls would rise with increasing
temperature, reflecting morbidity in the community. However, prior to this work such a
relationship had not been confirmed, and the magnitude of association was previously unknown.
Such attribution may in part reflect changes in 911 caller behaviour during periods of heat alerts
or sustained high temperature, partly prompted by media messages themselves that are broadcast
as part of the Hot Weather Response Plan. It could be that 911 callers are more aware of
dangerously high temperatures on these days and are more likely to self-identify as having HRI.
Similarly, the 911 call receivers themselves may be more aware of the possibility for HRI on
these days.
The increase in “Unconscious/fainting” determinant calls, though not significant, is
consistent with real increases in morbidity. This determinant grouping is relatively broad and it
could be that studying specific sub-groupings with this determinant would demonstrate a

107
stronger relationship with temperature. However, this vast determinant grouping will likely
capture fainting related to a number of other reasons as well as exposure to heat.
Findings regarding indicators of aggravation of pre-existing conditions such as
cardiovascular and respiratory typically demonstrated no effect, or in some cases, a negative
relationship. Correlations were minimal for cardio-respiratory arrest/deaths and positive but
modest for breathing problems. Given the pathophysiological processes in these illnesses, it may
seem that the significant negative correlations are anomalous. However, these findings are quite
consistent with the literature of morbidity of HRI that suggests a contrast between evidence
reported in mortality and morbidity studies. Mortality studies routinely report an increase in
deaths due to cardiovascular and respiratory causes during periods of extreme heat.45,51,86
However, this pattern has not been supported by morbidity studies where hospital admissions are
smaller in magnitude for excess mortality and generally do not increase for cardiovascular and
respiratory causes,90-92 as in this study.
This pattern suggests that people who die during extreme heat are not reaching the
attention of medical services. One possible explanation for this is that the impacts of heat are
relatively immediate, causing people to die quickly. This is supported by the literature that
demonstrates that extreme temperatures typically have an impact on health the same day, i.e.
with minimal lag. Another plausible reason for the contrast in mortality and morbidity is that the
people who die from HRI are socially isolated in some way, posing a barrier to seeking out
medical attention (e.g. live alone). This was the case for many of the deaths during the Chicago
heat wave in 1995.104, 187 It was also evident during the 2003 heat waves in Paris, where the

108
number of deaths registered at home was high, with most of the frailest patients dying before
hospital referral.188 The homeless and marginally housed, who are at increased risk of the effects
of heat, also experience barriers to medical care which may contribute to the contrast between
morbidity and mortality estimates.
The positive correlation between temperature and sub-categories of the “Unknown
problem (man down)” call group are consistent with impacts of heat upon the most socially
vulnerable, as these determinants largely refer to patients, such as the homeless, observed in
public places. Given the increases in mortality observed during heat waves among the socially
vulnerable, this correlation is likely to represent real increases in morbidity.39, 96, 104 Although
there have not been any studies to date that specifically consider the homeless population with
regards to heat there have been several studies that consider factors related to social isolation.
Individuals without a social network, who live alone, are more likely to suffer impacts of
extreme heat.39, 103 Furthermore, there is an association between low socioeconomic status and
increased health impacts from heat. It has been suggested that this is due to a combination of
factors that may include poor-quality housing, no access to air conditioning, and living in the
downtown environment with surrounding urban heat islands. A large proportion of the homeless
population may have pre-existing illness that predisposes them to the effects of heat, particularly
mental health patients taking psychotropic medications.33, 34, 103 An analysis of autopsy reports in
Australia from 1991-1998 found excessive clothing, acute alcohol intoxication, alcoholic liver
disease, and prolonged sun exposure were all predisposing factors for heat-related mortality;189
all these factors are found more commonly in homeless populations.

109
In addition to these predisposing characteristics, there is evidence to suggest that public
health interventions for heat do not adequately reach the homeless population, thus exacerbating
impacts among these groups. Recent work in Toronto that conducted interviews with community
stakeholders in the Hot Weather Response Plan suggests that some of the interventions are not
actually reaching the vulnerable.29 For example, cooling centres are established to protect the
homeless and marginally housed by providing an air-conditioned environment. However, these
centres are limited primarily due to the fact that there are only four in the city, and they require
transportation to get there and back, a clear limitation for the socially isolated. Consequently, the
majority of users of cooling centres in Toronto are individuals who happen to pass by and then
stay for an average of 15 minutes,190 rather than the homeless or socially isolated. Furthermore,
cooling centres are only opened during extreme heat alerts. Although many members of the
population can seek respite in a shopping centre, library, or movie theatre, these options are not
as readily available to the homeless population. Therefore, several plausible sets of factors
contribute to the vulnerability of the homeless and marginally housed population: social
isolation, limited or no resources, pathophysiology, and inadequate access to public health
interventions.
The increased proportions of calls ascribed to the determinants noted above may partly be
due to heightened public awareness and concern about the risks of unprotected heat exposure on
hot days. Consequently, it may be more likely that a bystander will call 911 out of concern on a
hot day than a cooler one. If they are calling for a third party, particularly someone they have not
approached but are passing by, it is likely that they will not have substantial information about
the person’s clinical condition to provide to the 911 call receiver. Without this clinical

110
information the caller is more likely to be coded in a less specific category like, “Unknown
problem (man down)” than a more specific determinant such as “Heat/cold exposure”. This is
further supported by the findings that of the “Unknown problem (man down)” sub-groupings, the
most consistently positively correlated with temperature were “Standing, sitting, moving or
talking” or of “Unknown status (3rd party caller)”, implying a situation of 3rd party callers
observing someone potentially in distress, but having limited information to provide further
diagnostic details.
Interestingly, the findings from the clinical approach and statistical analyses were not in
consistent agreement. The clinical group correctly predicted a relationship of the “Heat/cold
exposure” determinant with temperature. However, it was anticipated that because the
“Unknown problem (man down)” determinant is so broad, and captures so many events that are
not related to heat, any relationship with those calls to temperature would be diluted and thus not
significant in the analysis. The positive correlations found in this research indicate a stronger
influence of temperature on the magnitude of the calls in the “Unknown problem (man down)”
determinant grouping than previously thought. It also suggests that the 911 call data source may
be particularly sensitive to heat-related health outcomes in the vulnerable homeless population,
an important finding given the limited heat-related morbidity information on this susceptible
group.
Inherent trade-offs exist between sensitivity and specificity when developing a case
definition or selecting indicators for any syndrome.123, 191 For HRI, determinants like “Breathing
problems” may include calls for many medical reasons including heat-related aggravation of

111
existing cardio-respiratory disorders. In contrast, limiting calls to only those in the “Heat/cold
exposure” category would not capture calls that may truly be related to temperature increases e.g.
“Unknown problem (man down)”. Corresponding over- and under-estimates of the heat-related
burden of illness would occur, misguiding both our understanding of heat impacts and
prioritization of activities by public health authorities.
For public health surveillance purposes, focusing on a broader set of MPDS determinants
would increase sensitivity and potentially generate more “false alarms” but focusing on the latter
more specific ones will result in more “false negatives”, missing many cases of HRI that might
benefit from interventions. Unfortunately, not having a “gold standard” for an environmental
exposure related syndrome, as understood by the most ample understanding of HRI, means that
formal testing of sensitivity and specificity is not possible. Rather, use of different sets of
determinant codes will result in identification of different amounts and types of heat-relevant
morbidity. For the purpose of this research a more specific case definition was used. While this
may underestimate the burden of it is more likely to accurately capture true cases of HRI than
broader MPDS determinants. This was deemed a reasonable starting point with the potential to
expand the case definition in future research and thus gain a broader picture of both the direct
and indirect health impacts of heat.

112
5.2 Study Objective 1b: Time Series of the Relationship of 911 HRI Calls
and Temperature
This is the first study to demonstrate an association between daily 911 medical dispatch
calls specifically for HRI and maximum and mean temperature. Other than some work on EMS
dispatches and health information lines, there is very limited morbidity data available for HRI.
Of the few studies that have considered morbidity indicators specifically for heat-related reasons,
two investigated ED visits177,188 and another assessed calls to a nurse-led helpline in the UK,
NHS Direct;112 all found increases associated with temperature. The remainder of the research
that has been done, has focused solely on all visits or all calls rather than those specifically for
HRI.9, 10, 192 A Swiss study reported an increase in all ambulance calls over what was expected by
36% for the 65+ age group and 33% for the 75+ age group during the European heat waves of
2003.9 A Toronto study found an increase in all 911 calls 10% above normal levels during
oppressive days (heat alert and extreme heat alerts) between 1999-2002.10
In this study, 911 calls for HRI increased on average up to a maximum of 36% for each
1°C increase in temperature. The increases in 911 calls were higher than what has previously
been reported in mortality studies. An increase in mortality between 1-4% for every 1°C increase
in temperature above 24°C was reported in Valencia, Spain.80 A Brazilian study in Sao Paulo,
reported a 2.6% increase in all-cause mortality per 1°C increase in temperature above 20°C
among people aged 65+.48 The greater magnitude of 911 calls is consistent with the stylized
pyramid of heat health effects and the broader base of morbidity than mortality impacts (see
Figure 2.1). Higher mortality increases were reported in an Arizona study, a 35% increase in
heat-related mortality for every 1° increase in temperature,83 but nearly all of the heat-fatalities

113
were among illegal immigrants attempting to cross the border in a desert region and therefore at
particular risk due to the length and type of heat exposure.193
Other plausible reasons exist as to why the relative increase in 911 calls was greater in
the current study than the values reported in the literature. One possibility is that the other studies
report increases in all-cause mortality, rather than morbidity specifically related to heat. One
would expect a stronger effect in outcomes specifically related to heat rather than among all
causes. This might explain the similarities in values between the current study and the Arizona
work that looked specifically at mortality due to heat rather than excess mortality. Another
plausible reason is that the majority of these studies consider effects in hotter climates, where the
population is likely more acclimatized to high temperatures and therefore are not as affected as
the Toronto population. Previous literature has demonstrated that acclimatized populations are
less susceptible to the adverse effects of heat.47, 166
Interestingly, the magnitude of this increase in calls per degree increase in mean and
maximum temperature was greater in the summers of 2004 and 2005 than in 2002 and 2003.
There were no major changes in MPDS coding or operator training during this time (personal
communication, Alan Craig, Deputy Chief, Toronto EMS). It is plausible that with the greater
awareness of climate change health issues in recent years there may be a labeling effect where
calls are more likely to be coded as heat-related when compared with earlier years when perhaps
less awareness of the potential health impacts of climate change existed.

114
There was also a positive and statistically significant lag effect of one day for both the
effect of mean and maximum temperature on 911 calls for HRI. This was weak in comparison to
the same-day effect. Previous studies have also found a weak lag effect, suggesting that the
impact of heat on health is primarily immediate.80, 165 This has important implications for the
development of interventions for HRI, stressing the importance of timely public health
interventions to mitigate the immediate effects.
A day effect was also evident in this research, with a larger increase in 911 calls for HRI
occurring on the weekends and holidays as compared with weekdays. This is supported by
previous research that reported an increase in all ambulance calls by about 8% greater than
normal on weekdays and 14% higher on weekends in Toronto during heat alert periods.10 This is
likely the result of a combination of factors. One is the higher number of outdoor and
recreational activities that people participate in on the weekends as opposed to weekdays that
may result in greater proportions of the population exposed to high outdoor temperatures.
Another contributing factor is that on the weekends people are more likely to be at home than at
their workplace. For people who do not have access to air-conditioning at home, they may be
more at risk as compared with their being in an air-conditioned environment at work during the
week.
There was a slight increase in HRI calls associated with ozone levels but it is difficult to
draw conclusive findings from these statistically insignificant results. The impact of pollutants,
such as ozone, do have an independent effect on health outcomes, however, the influence they
have on the temperature-health relationship is still uncertain. It could be that their impact is

115
through exacerbation of pre-existing cardiovascular and respiratory conditions, rather than
having a direct influence on heat-related illness.
The findings of the impact of relative humidity were inconsistent. In some models there
was a positive effect, and in others a negative effect. This reflects the uncertainty in the
literature. Based on our understanding of pathophysiology, one might expect high humidity to
have a positive association with increases in 911 calls for HRI. High humidity reduces
evaporation of sweat and thus impairs body cooling mechanisms. However, some studies have
actually reported no effect of humidity on the temperature-mortality relationship.59, 65
Furthermore, other studies have reported the inverse effect that mortality rates are actually lower
when relative humidity is higher on hot days.66, 194, 195 One plausible explanation for this is that
the role of sweating in thermoregulation is not as effective as originally thought or that the
threshold temperatures for sweating onset are not reached often in the Toronto climate. It has
been suggested that sweating typically begins when ambient air temperatures exceed
approximately 30°C.66 In the Toronto climate, this threshold is substantially surpassed on only a
few days. It may be that humidity modifies the effects of temperature on health in only the
hottest regions. Finally, it is possible that given the dependence of relative humidity on
temperature, there is correlation between these variables, making it difficult to assess the
interaction term between the two. Further work is needed to gain a better understanding of the
role of relative humidity in the temperature-mortality/morbidity relationship in different
geographic contexts.

116
A Fisher’s exact test was used to further explore the relationship between 911 HRI calls
and temperature, particularly in terms of assessing thresholds for effect. The results suggest a
significant increase in calls above a maximum temperature of 28°C. This value is slightly lower
than other studies that have examined the relationship between temperature and health outcomes
and have reported thresholds in the lower 30’s.83 It may be that because ambulance response
calls capture morbidity, rather than mortality, they can detect the adverse effects of temperature
in the population at lower temperatures than those associated with mortality. Alternatively, it
could be that the Toronto population is not as acclimatized to hot, humid conditions as
populations in other studies and therefore health impacts are experienced at lower temperatures.
It is not clear whether maximum or mean temperature is a more appropriate measure for
heat-related health outcomes. In this study there was a clear relationship with both, and the
magnitudes were relatively similar suggesting that either mean or maximum temperature could
have been used. It is likely that the best measure will depend on local climate and population and
is not something that can be standardized across areas.
5.3 Study Objective 2a: Validity Assessment
Of the studies of ED visits and heat waves, most have considered excess visits for all-
causes and typically reported increases with increasing temperature. An exception are two
studies that examined ED visits specific for heat-related disorders during the 2003 heat wave in
Paris, and then again in 2006, and found an increase in ED visits.176,188 This finding is supported
by the current study that found significant increases in ED visits for HRI associated with
increases in temperature in Toronto EDs. The 911 calls for HRI followed a similar temporal

117
trend to the ED visits. This validation work provides an indication that 911 calls do reflect an
HRI burden of illness in the community. However, the volume of ED visits for heat was
generally less than the volume of 911 calls. This may suggest that 911 calls are capturing a
greater proportion of the burden of illness than EDs. It may also be that the 911 calls are
capturing a different group of the population, including those individuals that do not have their
own means to get to the hospital, as has been suggested in other literature.7, 196 Finally, another
possibility is that because the ED data used in this study only captured Toronto residents it is
underestimating ED visits for HRI. For example, ED visits from people living outside of Toronto
but visiting for the day for special events and concerts would have been missed in this data
source. This may explain the greater sensitivity of the 911 data to special outdoor events that was
demonstrated in this study and earlier work.
With the spike criteria that were used, both the 911 and ED systems had spikes more
frequently than heat alert days were called. This is in keeping with the greater sensitivity to
morbidity effects than the mortality based system. Furthermore, given that mortality is a
relatively rare health outcome resulting from heat exposure as compared with the many
morbidity effects, one would expect a larger number of spikes in the morbidity indicators than
those based on expected excess mortality.
5.4 Study Objective 2b: Timing Assessment
When compared with heat alert days, the temporal trend of 911 calls was similar, and in a
few cases peaked earlier, than the current heat health warning system. Given that the Toronto
HHWS is based on probabilities of excess mortality, an outcome that occurs later in the severe

118
HRI pathway, one might expect that HRI could be reported in advance of a heat alert being
called, as individuals begin to experience mild to moderate symptoms. A similar pattern was
found in a study in France in 2006 that compared emergency department HRI visits with heat
alerts declared by the French Ministry of Health.176
There was not a substantial difference in the timing between spikes in ED visits versus
911 calls for HRI, with the exception of the summer of 2005 where 911 calls increased on
average about 2 days earlier than ED visits. Given that these sources both capture morbidity, one
would not necessarily expect a difference in the timing between spikes in these indicators.
Rather, they may differ more in terms of the demographics and severity of illness of the people
captured. The case of the 2005 summer is interesting as 911 and NACRS appear to be interacting
differently in this instance. An important consideration is that the data sources differ in their
timeliness of availability; there is a significant lag in obtaining ED data through NACRS (up to
several months). However, the 911 medical dispatch data can be provided on a daily, or more
frequent basis. This timeliness places the 911 data at a clear advantage as the more appropriate
source for a syndromic surveillance system, based on near real-time information.
5.5 Study Objective 3: Geospatial Distribution of HRI in Toronto
There was substantial heterogeneity in the spatial distribution of HRI consistent with both
recreational patterns and the growing literature on variability of neighbourhood microclimates
and vulnerability to heat stress. An analysis of the rates of heat-related deaths in Chicago in 1995
found differential rates according to neighbourhood. Degraded neighbourhood physical
environments that were characterized by low-income, high elderly populations, and more
violence, that tended to isolate residents from networks of social support, were found to have the

119
highest death rates.187 A simulation model that estimated outdoor human thermal comfort in
eight diverse urban neighbourhoods during the summer of 2003 in Phoenix, USA also found
significant variations.106 Higher-income, predominantly white neighbourhoods were at lower risk
of uncomfortable indices than lower-income, predominantly Hispanic neighbourhoods. This
vulnerability was exacerbated by the residents’ lack of adequate social and material resources to
cope with extreme heat (e.g. community pools, housing type, access to air conditioning). Similar
findings were reported in a study of neighbourhoods in St. Louis Missouri; heat-related mortality
rates during severe heat waves were higher in the more disadvantaged areas of the city and lower
in more affluent parts of the city.38, 197
In Toronto, areas along the waterfront had a particularly high rate of HRI as compared
with other neighbourhoods. The most consistent area was Toronto Island and areas along the
waterfront including Ashbridges Bay Park where increases appear on all maps. Although the
mean number of all 911 calls emergency calls is low on Toronto Island, the percentage of calls
for HRI disproportionately increases on hot days. In 2001, the population of Toronto Island was
658, however, more than 1,225,000 people visit it annually, primarily in the summer.10 The
majority of human activity on the island during this time is recreational and outdoors. It is most
likely that the increase in 911 calls for HRI is attributable to the increases in morbidity due to the
high rate of outdoor activities and large transient population exposed to hot weather. Another
possible reason for the higher proportion of calls on Toronto Island is that it has a relatively high
proportion of people aged 65 and older, and older housing (i.e. constructed prior to 1946), two
key risk factors for HRI.198 This is consistent with previous work that considered increases in all
911 medical dispatch calls in Toronto on heat alert days and found higher numbers of calls along

120
the waterfront.10 Interestingly, similar findings were recently presented from work in New York
City.141 Areas of the city with persistent increases in HRI, as monitored through 911 medical
dispatch data, occurred primarily around tourist sites.
Although less consistent, other areas within the downtown core experience high rates of
HRI ambulance dispatch calls. The Palmerston-Little Italy area consistently has higher rates of
HRI calls. The Lansing-Westgate neighbourhood also has consistently higher rates of calls. This
latter neighbourhood is bisected by the greenbelt, has a large golf course, and a higher proportion
of seniors as compared with other Toronto neighbourhoods. Areas around York University are
another “hot spot”. An area in northeast Toronto close to the CPR Railway yard area also has a
higher proportion of calls; this is a highly industrialized areas surrounded by several small parks
and schools with a high immigrant, minority, and elderly population.10 While the reasons for
proportionately higher rates are unclear, possible explanations may include spatial risk factors
like poorer housing type, lack of air conditioning, and particular local heat islands. It could also
be that these areas have a higher proportion of high risk groups like the elderly, homeless,
infants, young children, and people with pre-existing illness.
This geospatial heterogeneity in the burden of HRI across Toronto neighbourhoods has
clear implications for the Hot Weather Response Plan. By identifying areas of the city with a
disproportionately high burden of HRI, interventions can be targeted. For example, there are
currently no heat/health interventions implemented on Toronto Island on hot days. Given the
high number of 911 calls for HRI on Toronto Island each summer it may be advisable to initiate
interventions specifically aimed at the recreational groups there, such as installing more water

121
fountains and providing precautionary educational information on the ferries by which all
visitors arrive. By targeting interventions to known areas of risk, resources could be more
efficiently used and the health impacts mitigated.
5.6 Study Limitations
There are some limitations to this study’s methods. The 911 medical dispatch system is
designed for triage, and rapid assessments to determine the resources that should be dispatched,
rather than to assign an accurate clinical diagnosis. The precision of 911 medical dispatch data is
further limited as 911 callers are usually not clinically trained and often are reporting patients or
events to which they have no direct connection but have only observed. As a result, it is possible
that calls originally coded as HRI turn out to be a different diagnosis and vice versa. This should
be less problematic in the case of ED visits, where clinician diagnoses occurred, though heat
exposure may potentially go under-recognized. One of the key aims of this study was to tap into
a pre-existing and more real-time data source, and assess potential added value without making
any major modifications. Comparisons among sources, including the HHWS, which is not
necessarily a gold standard measurement since it is also algorithm-based, did provide some
assessment of concurrent validity.
In interpreting the data, a labeling phenomenon cannot be ruled out as a possible
explanation for the relationship between temperature and calls for HRI. It is plausible that callers
may be more likely to self-identify as having HRI rather than more general symptoms when
calling emergency services on an oppressively hot day. Dispatch coders may also be more aware
of heat relationships on hot days. However, it may be that during higher temperatures, callers are

122
able to more correctly diagnose themselves with HRI, rather than describe non-specific
symptoms (e.g. headache, malaise), and therefore HRI calls are more accurately collected on
these days. From a public health perspective, this may serve as an advantage in improving the
ability to detect cases of a syndrome that is often challenging to identify and for which limited
information is currently available. It is also possible that the labeling effect may actually result in
an underestimation of burden; on a heat alert day, members of the public may start implementing
interventions (e.g. staying in cool places, hydrating, etc.) and mitigating the effects of heat
themselves. Consequently, they are less likely to seek further medical assistance. Such cases
would not be captured in a surveillance system.
It has been suggested that there are potential biases associated with medical dispatch data.
A study of the ambulance-based surveillance system in New York City assessed potential bias in
patients presenting with influenza-like illness via ambulance as compared with those arriving at
the ED by other means.7 They reported that ambulance-based surveillance is more sensitive for
severe illness affecting older individuals. Another study suggests that several socioeconomic
factors influence a person’s decision to call an ambulance in non-emergency situations; the
elderly, people with a low household income, people who do not possess a car.196 However,
given that these represent the groups at greatest risk for HRI this may actually be a useful feature
in capturing a proportion of the population that more traditional data sources do not and is thus a
challenge to monitor from a public health perspective.
Another limitation particular to the data is the relatively low number of HRI calls. Given
there are 140 neighbourhoods in Toronto, with 90 days of data per neighbourhood (for each

123
summer), the rate of HRI calls per neighbourhood is extremely low (about 1 per 500 calls in
some neighbourhoods for an entire summer). This makes the data quite sparse and limits the
power needed to conduct further possible analysis such as fitting a spatio-temporal model. This
was partly a consequence of creating a specific case definition, thus broadening this definition
for future research would allow further exploration of such models.
Given the particular vulnerability of the elderly to the effects of heat, it would have been
very interesting to consider the effect of age in these analyses. Unfortunately, age is not routinely
captured in the 911 medical dispatch data. On some occasions it will be provided voluntarily by
the caller and added to the “comments” field, however, this is not routine and in the case of a
third party caller, often inaccurate. However, age is provided for the emergency department data
in the NACRS dataset and therefore this is a possibility for future studies, in addition to the
consideration of other demographic factors like gender.
Finally, the meteorological variables are measured at a monitoring station that likely do
not reflect the full range of temperatures in different areas of the city like urban heat islands, or
people’s homes, where they are experiencing HRI. However, until the methods of taking these
measurements is refined to accommodate such factors, information from monitoring stations is
the best available.
5.7 Future Research
Further validation of the applied 911 determinant groupings is warranted. Validating the
determinants with sign and symptom data recorded once a patient is picked up and assessed by

124
paramedics has the potential to improve clinical validity. Hand-held devices that may record this
information should be able to provide additional near real-time data in future studies. This
information could then be compared with the initial 911 determinant grouping, and then the
subsequent discharge diagnosis.
Future important work should include more detailed examination of the spatial
information provided in the medical dispatch dataset to identify vulnerable populations in the
city of Toronto by adding demographic information to the maps such as housing age and type.
Natural Resources Canada is in the early stages of a pilot study to measure the urban heat island
effect in Toronto. One of the planned deliverables of this work is a map identifying the spatial
distribution of the urban heat island. The consideration of this risk factor information will
provide important new information regarding the reasons why some neighbourhoods experience
a higher burden of HRI than others.
Examination of other important meteorological indices is warranted in future research.
For example, given the possible dependence of relative humidity on temperature and the
inconclusive results for humidity in the current work, it would be interesting to look at another
variable, such as Humidex. Humidex combines both temperature and humidity and thus would
be an ideal candidate for future assessment. Furthermore, given that Humidex is the primary
Canadian method for evaluating heat stress, such findings would be useful from an applied
public health perspective. While examination of the role of other air pollutants would also be
interesting, consideration must be given to the high correlation between these variables.

125
The impacts of heat on the homeless population have not been as well-studied as other
vulnerable groups such as the elderly and children. This is partly due to challenges in studying
this population. However, given the characteristics of this population that place them at such
high-risk of the effects of heat, future research is necessary. These studies should focus on
gaining a better understanding of whether public health interventions for HRI actually reach this
vulnerable group, and ways to best mitigate the harmful health effects in this population.
Furthermore, there is a need to better understand the community distribution of heat-related
health outcomes in other “at-risk” groups such as otherwise healthy individuals in high risk
situations such as recreational or occupational with high and/or prolonged heat exposure.
Particularly important for public health practitioners will be the use of 911 in prospective
surveillance for HRI, feeding the results to public health decision makers who currently rely on
algorithms based on total mortality and/or meteorological indicators. Only then can the potential
impacts of such an approach to HRI surveillance be evaluated in its ability to direct timely public
health interventions.
A multi-jurisdictional study would build on the findings of the current research. Including
additional cities would not only increase the methodological power of the study but would also
provide new information about the features of cities that contribute to the heat/health relationship
(e.g. rural versus urban, demographic breakdown, etc.). Furthermore, including cities that do not
currently have a HHWS in operation could potentially improve estimation of community burden,
as significant concerns around interventions already being implemented as a result of heat
warnings would not be present, at least locally (national warning might still be operative).

126
Finally, further evaluation of the use of 911 medical dispatch electronic data sets for
surveillance appears appropriate not only for HRI but for other syndromes. The methods
developed in the current study could be applied to other important conditions like influenza and
gastrointestinal illness in future studies. They could also be applied for broader definitions of
HRI, including other MPDS determinants such as “Breathing problems” and/or
“Unconscious/fainting”. This research would also enable the exploration of spatio-temporal
models, for example, that were not possible with the current data.
5.8 Contributions of This Research
There are several important research contributions of this study:
1) It is the first to develop a case definition of HRI using 911 medical dispatch data. In cities
using a similar 911 coding system, this case definition could be used in future studies. Further,
the methodology used for this process could be applied to the development of case definitions for
other syndromes (e.g. influenza, gastrointestinal illness) using 911 data.
2) This study is one of very few to consider the morbidity effects of heat, specifically related to
HRI and demonstrate the magnitude of this association. Given the implications for surveillance
development, this is a key contribution in understanding the burden of illness related to heat.
3) This study is unique in that it included a validation of 911 data with emergency department
information. This validation exercise has not been previously conducted for HRI and is important
as it indicates 911 as a valid source of morbidity information.

127
5.9 Conclusions
Establishing who is most at risk for HRI and how to reduce their exposure is a complex
public health challenge. Given that heat has an immediate effect on health, timely interventions
are needed, based on near real-time data. There is clear utility in monitoring 911 medical
dispatch data for HRI to assist public health units in both temporal and geospatial surveillance.
This research has demonstrated the strong association between 911 medical dispatch data and
temperature and the validity of these data as a source of HRI morbidity information. It has also
demonstrated the ability to apply the 911 information to a GIS in order to describe the geospatial
distribution of HRI in a major urban centre. The unique geospatial information provided by the
911 data is perhaps one of the most valuable features of this data source. By identifying “hot
spots” that experience the highest burden of HRI, which may or may not represent residential
address, it is possible to advise public health stakeholders as to where to best target interventions
such as distributing water bottles, guiding community agencies and opening cooling stations to
care for at risk populations.
This previously untapped data source should be further explored for its applications in
understanding the relationship between heat and human health and more appropriately targeting
public health interventions. The impacts of heat are not experienced uniformly by populations.
This study has used 911 data to illustrate this phenomenon both in terms of heterogeneity of
burden in time and in space. Therefore, it is a potentially valuable tool to understand disparities
in burden of illness and develop strategies to reduce these inequities between sub-populations.
Given that HRI is both predictable and preventable, developing a surveillance system to mitigate

128
the harmful effects of heat both for the general population, but particularly for the most
vulnerable, is a clear public health priority.

129
References
1. Whitman S, Good G, Donoghue ER, Benbow N, Shou W, Mou S. Mortality in Chicago
attributed to the July 1995 heat wave. Am J Public Health. 1997 Sep;87(9):1515-8.
2. Robine JM. In: The excess mortality in summer 2003: Results of the Canicule project. World
Health Organization meeting: Regional office for Europe: Public health responses to extreme
weather events - euroHEAT; March 22-23, 2007; Bonn, Germany.
3. Canfalonieri U, Menne B, Akhtar R, Ebi KL, Hauengue M, Kovats RS, et al. Human health.
In: Parry ML, Canziani OF, Palutikof JP, van der Linden PJ, Hanson CE, editors. Climate
Change 2007: Impacts, Adaptation and Vulnerability. Contribution of Working Group II to the
Fourth Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, UK:
Cambridge University Press; 2007. p. 391-431.
4. Field CB, Mortsch LD, Brklacich M, Forbes DL, Kovacs P, Patz JA, et al. North America. In:
Parry ML, Canziani OF, Palutikof JP, van der Linden PJ, Hanson CE, editors. Climate Change
2007: Impacts, Adaptation and Vulnerability. Contribution of Working Group II to the Fourth
Assessment Report of the Intergovernmental Panel on Climate Change. Cambridge, UK:
Cambridge University Press; 2007. p. 617-52.
5. Rea E. World Youth Day, Toronto, Canada. 2004. Report for Toronto Public Health.
6. Bork KH, Klein BM, Molbak K, Trautner S, Pedersen UB, Heegaard E. Surveillance of
ambulance dispatch data as a tool for early warning. Euro Surveill. 2006;11(12):229-33.

130
7. Greenko J, Mostashari F, Fine A, Layton M. Clinical evaluation of the emergency medical
services (EMS) ambulance dispatch-based syndromic surveillance system, New York City. J
Urban Health. 2003 Jun;80(2 Suppl 1):i50-6.
8. Mostashari F, Fine A, Das D, Adams J, Layton M. Use of ambulance dispatch data as an early
warning system for communitywide influenza-like illness, New York City. J Urban Health. 2003
Jun;80(2 Suppl 1):i43-9.
9. Cerutti B, Tereanu C, Domenighetti G, Cantoni E, Gaia M, Bolgiani I, et al. Temperature
related mortality and ambulance service interventions during the heat waves of 2003 in Ticino
(Switzerland). Soz Praventivmed. 2006;51(4):185-93.
10. Dolney TJ, Sheridan SC. The relationship between extreme heat and ambulance response
calls for the city of Toronto, Ontario, Canada. Environ Res. 2006;101(1): 94-103.
11. Palecki MA, Changnon SA, Kunkel KE. The nature and impacts of the July 1999 heat wave
in the midwestern United States: Learning from the lessons of 1995. BAMS. 2001
July;82(7):1353-67.
12. Pengelly LD, Campbell ME, Cheng CS, Fu C, Gingrich SE, Macfarlane R. Anatomy of heat
waves and mortality in Toronto: Lessons for public health protection. Can J Public Health. 2007
Sep-Oct;98(5):364-8.
13. Haines A, Kovats RS, Campbell-Lendrum D, Corvalan C. Climate change and human health:
Impacts, vulnerability and public health. Public Health. 2006 Jul;120(7):585-96.

131
14. Knowlton K, Lynn B, Goldberg RA, Rosenzweig C, Hogrefe C, Rosenthal JK, et al.
Projecting heat-related mortality impacts under a changing climate in the New York City region.
Am J Public Health. 2007 Nov;97(11):2028-34.
15. Patz JA, Campbell-Lendrum D, Holloway T, Foley JA. Impact of regional climate change on
human health. Nature. 2005 Nov 17;438(7066):310-7.
16. Toronto Public Health. Combined impact of extreme heat and air pollution on mortality.
Toronto, ON: 2005. 9 pp. Accessed at:
http://www.toronto.ca/health/hphe/pdf/boh_combined_impact_smog_and_heat.pdf
17. Bouchama A, Knochel JP. Heat stroke. N Engl J Med. 2002 Jun 20;346(25):1978-88.
18. Havenith G. Temperature regulation, heat balance and climatic stress. In: Kirch W, Menn B,
Bertollini R, editors. Extreme Weather Events. European Union: World Health Organization;
2005. p. 69-80.
19. Simon HB. Hyperthermia. N Engl J Med. 1993 Aug 12;329(7):483-7.
20. Barrow MW, Clark KA. Heat-related illnesses. Am Fam Physician. 1998 Sep 1;58(3):749,56,
759.
21. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat:
Strategies for maintaining health and performance. Sports Med. 2007;37(8):669-82.
22. World Health Organization. Heat-waves: Risks and responses. Copenhagen: 2004. Report
No.: Health and Global Environmental Change Series, No. 2.

132
23. Nixdorf-Miller A, Hunsaker DM, Hunsaker JC,3rd. Hypothermia and hyperthermia medico-
legal investigation of morbidity and mortality from exposure to environmental temperature
extremes. Arch Pathol Lab Med. 2006 Sep;130(9):1297-304.
24. US Centre for Disease Control (CDC). Heat-related deaths LA County California, 1999-2000
and United States, 1979-1989. MMWR. 2001;50(29):623-6.
25. Dematte JE, O'Mara K, Buescher J, Whitney CG, Forsythe S, McNamee T, et al. Near-fatal
heat stroke during the 1995 heat wave in Chicago. Ann Intern Med. 1998 Aug 1;129(3):173-81.
26. Semenza JC. Acute renal failure during heat waves. Am J Prev Med. 1999 Jul;17(1):97.
27. Argaud L, Ferry T, Le QH, Marfisi A, Ciorba D, Achache P, et al. Short- and long-term
outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007
Aug 13.
28. LoVecchio F, Pizon AF, Berrett C, Balls A. Outcomes after environmental hyperthermia.
Am J Emerg Med. 2007 May;25(4):442-4.
29. Angus J. An evaluation of Toronto's heat watch warning system. MSc thesis in the
Department of Geography. Toronto, ON, Canada: University of Toronto, 2006. 145 pp.
30. Health Canada. 2006. Pyramid of Health Effects. Health Effects from Air Pollution.
Available online at: http://www.hc-sc.gc.ca/ewh-semt/air/out-ext/effe/health_effects-
effets_sante_e.html (Accessed October 18, 2007).
31. Anderson CA. Heat and violence. Curr Dir Psychol Sci. 2001 February;10(1):33-8.

133
32. Page LA, Hajat S, Kovats RS. Relationship between daily suicide counts and temperature in
England and Wales. Br J Psychiatry. 2007 Aug;191:106-12.
33. Bark N. Deaths of psychiatric patients during heat waves. Psychiatr Serv. 1998
Aug;49(8):1088-90.
34. Bulbena A, Sperry L, Cunillera J. Psychiatric effects of heat waves. Psychiatr Serv. 2006
Oct;57(10):1519.
35. Stafoggia M, Forastiere F, Agostini D, Biggeri A, Bisanti L, Cadum E, et al. Vulnerability to
heat-related mortality: A multicity, population-based, case-crossover analysis. Epidemiology.
2006 May;17(3):315-23.
36. Medina-Ramon M, Zanobetti A, Cavanagh DP, Schwartz J. Extreme temperatures and
mortality: Assessing effect modification by personal characteristics and specific cause of death in
a multi-city case-only analysis. Environ Health Perspect. 2006 Sep;114(9):1331-6.
37. Michenot F, Sommet A, Bagheri H, Lapeyre-Mestre M, Montastruc JL, French Network of
PharmacoVigilance Centres. Adverse drug reactions in patients older than 70 years during the
heat wave occurred in France in summer 2003: A study from the French PharmacoVigilance
database. Pharmacoepidemiol Drug Saf. 2006 Oct;15(10):735-40.
38. Smoyer KE. A comparative analysis of heat waves and associated mortality in St. Louis,
Missouri-1980 and 1995. Int J Biometeorol. 1998 Aug;42(1):44-50.

134
39. Semenza JC, Rubin CH, Falter KH, Selanikio JD, Flanders WD, Howe HL, et al. Heat-
related deaths during the July 1995 heat wave in Chicago. N Engl J Med. 1996 Jul 11;335(2):84-
90.
40. Cadot E, Rodwin VG, Spira A. In the heat of the summer: Lessons from the heat waves in
Paris. J Urban Health. 2007 Jul;84(4):466-8.
41. Conti S, Masocco M, Meli P, Minelli G, Palummeri E, Solimini R, et al. General and specific
mortality among the elderly during the 2003 heat wave in Genoa (Italy). Environ Res. 2007
Feb;103(2):267-74.
42. Filleul L, Cassadou S, Medina S, Fabres P, Lefranc A, Eilstein D, et al. The relation between
temperature, ozone, and mortality in nine French cities during the heat wave of 2003. Environ
Health Perspect. 2006 Sep;114(9):1344-7.
43. Johnson H, Kovats RS, McGregor G, Stedman J, Gibbs M, Walton H. The impact of the
2003 heat wave on daily mortality in England and Wales and the use of rapid weekly mortality
estimates. Eurosurveillance Monthly Release. 2005 July/August 2005;10(7-8).
44. Nogueira PJ, Falcao JM, Contreiras MT, Paixao E, Brandao J, Batista I. Mortality in Portugal
associated with the heat wave of August 2003: Early estimation of effect, using a rapid method.
Eurosurveillance Monthly Release. 2005 July/August 2005;10(7-8).
45. Paldy A, Bobvos J, Vamos A, Kovats RS, Hajat S. The effects of temperature and heat waves
on daily mortality in Budapest, Hungary, 1970-2000. In: Kirch W, Menn B, Bertollini R,
editors. Extreme Weather Events. European Union: Springer Verlag on behalf of the World
Health Organization; 2005. p. 99-108.

135
46. Rooney C, McMichael AJ, Kovats RS, Coleman MP. Excess mortality in England and
Wales, and in greater London, during the 1995 heatwave. J Epidemiol Community Health. 1998
Aug;52(8):482-6.
47. Basu R, Samet JM. Relation between elevated ambient temperature and mortality: A review
of the epidemiologic evidence. Epidemiol Rev. 2002;24(2):190-202.
48. Gouveia N, Hajat S, Armstrong B. Socioeconomic differentials in the temperature-mortality
relationship in Sao Paulo, Brazil. Int J Epidemiol. 2003 Jun;32(3):390-7.
49. Hajat S, Kovats RS, Atkinson RW, Haines A. Impact of hot temperatures on death in
London: A time series approach. J Epidemiol Community Health. 2002 May;56(5):367-72.
50. Hajat S, Armstrong B, Baccini M, Biggeri A, Bisanti L, Russo A, et al. Impact of high
temperatures on mortality: Is there an added heat wave effect? Epidemiology. 2006
Nov;17(6):632-8.
51. Diaz J, Linares C, Tobias A. Impact of extreme temperatures on daily mortality in Madrid
(Spain) among the 45-64 age-group. Int J Biometeorol. 2006 Jul;50(6):342-8.
52. Mastrangelo G, Fedeli U, Visentin C, Milan G, Fadda E, Spolaore P. Pattern and
determinants of hospitalization during heat waves: An ecologic study. BMC Public Health. 2007
Aug 9;7:200.
53. Michelozzi P, de'Donato F, Bisanti L, Russo A, Cadum E, DeMaria M, et al. The impact of
the summer 2003 heat waves on mortality in four Italian cities. Eurosurveillance Monthly
Release. 2005 July/August 2005;10(7-8).

136
54. Tan J, Zheng Y, Song G, Kalkstein LS, Kalkstein AJ, Tang X. Heat wave impacts on
mortality in Shanghai, 1998 and 2003. Int J Biometeorol. 2007 Jan;51(3):193-200.
55. Fischer P, Brunekreef B, Lebret E. Air pollution related deaths during the 2003 heat wave in
the Netherlands. Atmos Environ. 2004;38(8):1083-5.
56. Katsouyanni K, Pantazopoulou A, Touloumi G, Tselepidaki I, Moustris K, Asimakopoulos
D, et al. Evidence for interaction between air pollution and high temperature in the causation of
excess mortality. Arch Environ Health. 1993 Jul-Aug;48(4):235-42.
57. Ren C, Tong S. Temperature modifies the health effects of particulate matter in Brisbane,
Australia. Int J Biometeorol. 2006 Nov;51(2):87-96.
58. Ren C, Williams GM, Tong S. Does particulate matter modify the association between
temperature and cardiorespiratory diseases? Environ Health Perspect. 2006 Nov;114(11):1690-6.
59. Shumway RH, Azari AS, Pawitan Y. Modeling mortality fluctuations in Los Angeles as
functions of pollution and weather effects. Environ Res. 1988 Apr;45(2):224-41.
60. Kalkstein LS. A new approach to evaluate the impact of climate on human mortality. Environ
Health Perspect. 1991 Dec;96:145-50.
61. Samet J, Zeger S, Kelsall J, Xu J, Kalkstein L. Does weather confound or modify the
association of particulate air pollution with mortality? An analysis of the Philadelphia data,
1973-1980. Environ Res. 1998 Apr;77(1):9-19.

137
62. Diaz J, Garcia R, Velazquez de Castro F, Hernandez E, Lopez C, Otero A. Effects of
extremely hot days on people older than 65 years in Seville (Spain) from 1986 to 1997. Int J
Biometeorol. 2002 Aug;46(3):145-9.
63. Braga AL, Zanobetti A, Schwartz J. The effect of weather on respiratory and cardiovascular
deaths in 12 U.S. cities. Environ Health Perspect. 2002 Sep;110(9):859-63.
64. Braga AL, Zanobetti A, Schwartz J. The time course of weather-related deaths.
Epidemiology. 2001 Nov;12(6):662-7.
65. Honda Y, Ono M, Uchiyama I. Humidity does not confound temperature-mortality
relationship in Japan. Jpn J Biometeor. 2000;37(4):117-22.
66. Kunst AE, Looman CW, Mackenbach JP. Outdoor air temperature and mortality in the
Netherlands: A time-series analysis. Am J Epidemiol. 1993 Feb 1;137(3):331-41.
67. Shen T, Howe HL, Alo C, Moolenaar RL. Toward a broader definition of heat-related death:
Comparison of mortality estimates from medical examiners' classification with those from total
death differentials during the July 1995 heat wave in Chicago, Illinois. Am J Forensic Med
Pathol. 1998 Jun;19(2):113-8.
68. Luber GE. Heat-related deaths - United States, 1999-2003. MMWR. 2006;55(29):796-8.
69. Kovats RS, Jendritzky G. Heat-waves and human health. In: Menne B, Ebi KL, editors.
Climate Change and Adaptation Strategies for Human Health. Germany: World Health
Organization; 2006. p. 63-97.

138
70. Kovats RS, Koppe C. Heat waves: Past and future impacts on health. In: Ebi KL, Smith JB,
Burton I, editors. Integration of Public Health with Adaptation to Climate Change. London, UK:
Taylor & Francis Group; 2005. p. 136-60.
71. Hajat S, Armstrong BG, Gouveia N, Wilkinson P. Mortality displacement of heat-related
deaths: A comparison of Delhi, Sao Paulo, and London. Epidemiology. 2005 Sep;16(5):613-20.
72. Kilbourne E. Heat waves and hot environments. In: Noji E, editor. The Public Health
Consequences of Disasters. Oxford University Press; 1997. p. 245-69.
73. Smoyer-Tomic KE, Rainham DG. Beating the heat: Development and evaluation of a
Canadian hot weather health-response plan. Environ Health Perspect. 2001 Dec;109(12):1241-8.
74. Lawson AB, Kleinman K. Spatial and syndromic surveillance for public health. West Sussex,
England: John Wiley & Sons, Ltd; 2005.
75. Lawson AB. Disease cluster detection: A critique and a Bayesian proposal. Stat Med. 2006
Mar 15;25(5):897-916.
76. Martinez BF, Annest JL, Kilbourne EM, Kirk ML, Lui KJ, Smith SM. Geographic
distribution of heat-related deaths among elderly persons. Use of county-level dot maps for
injury surveillance and epidemiologic research. JAMA. 1989 Oct 27;262(16):2246-50.
77. Maheswaran R, Craglia M. GIS in public health practice. United States of America: CRC
Press LLC; 2004.

139
78. Olson KL, Bonetti M, Pagano M, Mandl KD. Real time spatial cluster detection using
interpoint distances among precise patient locations. BMC Med Inform Decis Mak. 2005 Jun
21;5:19.
79. Kulldorff M, Mostashari F, Duczmal L, Katherine Yih W, Kleinman K, Platt R. Multivariate
scan statistics for disease surveillance. Stat Med. 2007 Apr 15;26(8):1824-33.
80. Ballester F, Corella D, Perez-Hoyos S, Saez M, Hervas A. Mortality as a function of
temperature. A study in Valencia, Spain, 1991-1993. Int J Epidemiol. 1997 Jun;26(3):551-61.
81. Hajat S, Kovats RS, Lachowycz K. Heat-related and cold-related deaths in England and
Wales: Who is at risk? Occup Environ Med. 2007 Feb;64(2):93-100.
82. Huynen MM, Martens P, Schram D, Weijenberg MP, Kunst AE. The impact of heat waves
and cold spells on mortality rates in the Dutch population. Environ Health Perspect. 2001
May;109(5):463-70.
83. Keim SM, Mays MZ, Parks B, Pytlak E, Harris RM, Kent MA. Heat fatalities in Pima
County, Arizona. Health and Place. 2007 Mar;13(1):288-92.
84. Kim H, Ha JS, Park J. High temperature, heat index, and mortality in 6 major cities in South
Korea. Arch Environ Occup Health. 2006 Nov-Dec;61(6):265-70.
85. Kovats RS, Johnson H, Griffith C. Mortality in southern England during the 2003 heat wave
by place of death. Health Stat Q. 2006 Spring;(29):6-8.

140
86. Saez M, Sunyer J, Castellsague J, Murillo C, Anto JM. Relationship between weather
temperature and mortality: A time series analysis approach in Barcelona. Int J Epidemiol. 1995
Jun;24(3):576-82.
87. Simon F, Lopez-Abente G, Ballester E, Martinez F. Mortality in Spain during the heat waves
of summer 2003. Eurosurveillance Monthly Release. 2005 July/August 2005;10(7-8).
88. Semenza JC, McCullough JE, Flanders WD, McGeehin MA, Lumpkin JR. Excess hospital
admissions during the July 1995 heat wave in Chicago. Am J Prev Med. 1999 May;16(4):269-
77.
89. Dhainaut JF, Claessens YE, Ginsburg C, Riou B. Unprecedented heat-related deaths during
the 2003 heat wave in Paris: Consequences on emergency departments. Crit Care. 2004
Feb;8(1):1-2.
90. Kovats RS, Hajat S, Wilkinson P. Contrasting patterns of mortality and hospital admissions
during hot weather and heat waves in greater London, UK. Occup Environ Med. 2004
Nov;61(11):893-8.
91. Semenza JC. Are electronic emergency department data predictive of heat-related mortality?
J Med Syst. 1999 Oct;23(5):419,21, 423-4.
92. Mastrangelo G, Hajat S, Fadda E, Buja A, Fedeli U, Spolaore P. Contrasting patterns of
hospital admissions and mortality during heat waves: Are deaths from circulatory disease a real
excess or an artifact? Med Hypotheses. 2006;66(5):1025-8.

141
93. Kovats RS, Kristie LE. Heatwaves and public health in Europe. Eur J Public Health. 2006
Dec;16(6):592-9.
94. Kovats RS. Heat waves and health protection. BMJ. 2006 Aug 12;333(7563):314-5.
95. Smoyer KE, Rainham DG, Hewko JN. Heat-stress-related mortality in five cities in southern
Ontario: 1980-1996. Int J Biometeorol. 2000 Nov;44(4):190-7.
96. Brukcer G. Vulnerable populations: Lessons learnt from the summer 2003 heat waves in
Europe. Eurosurveillance Monthly Release. 2005;10(7-8).
97. McGeehin MA, Mirabelli M. The potential impacts of climate variability and change on
temperature-related morbidity and mortality in the United States. Environ Health Perspect. 2001
May;109 Suppl 2:185-9.
98. Bernardo LM, Crane PA, Veenema TG. Treatment and prevention of pediatric heat-related
illnesses at mass gatherings and special events. Dimens Crit Care Nurs. 2006 Jul-Aug;25(4):165-
71.
99. Vandentorren S, Bretin P, Zeghnoun A, Mandereau-Bruno L, Croisier A, Cochet C, et al.
August 2003 heat wave in France: Risk factors for death of elderly people living at home. Eur J
Public Health. 2006 Dec;16(6):583-91.
100. Worfolk JB. Heat waves: Their impact on the health of elders. Geriatr Nurs. 2000 Mar-
Apr;21(2):70-7.
101. Davido A, Patzak A, Dart T, Sadier MP, Meraud P, Masmoudi R, et al. Risk factors for heat
related death during the august 2003 heat wave in Paris, France, in patients evaluated at the

142
emergency department of the Hopital Europeen Georges Pompidou. Emerg Med J. 2006
Jul;23(7):515-8.
102. Stephan F, Ghiglione S, Decailliot F, Yakhou L, Duvaldestin P, Legrand P. Effect of
excessive environmental heat on core temperature in critically ill patients: An observational
study during the 2003 European heat wave. Br J Anaesth. 2005 Jan;94(1):39-45.
103. Bouchama A, Dehbi M, Mohamed G, Matthies F, Shoukri M, Menne B. Prognostic factors
in heat wave related deaths: A meta-analysis. Arch Intern Med. 2007 Aug 13.
104. Klinenberg E. Heat wave: A social autopsy of disaster in Chicago. The University of
Chicago Press; 2002.
105. O'Neill MS, Zanobetti A, Schwartz J. Disparities by race in heat-related mortality in four
US cities: The role of air conditioning prevalence. J Urban Health. 2005 Jun;82(2):191-7.
106. Harlan SL, Brazel AJ, Prashad L, Stefanov WL, Larsen L. Neighborhood microclimates and
vulnerability to heat stress. Soc Sci Med. 2006 Dec;63(11):2847-63.
107. Wilhelmi OV, Purvis KL, Harriss RC. Designing a geospatial information infrastructure for
mitigation of heat wave hazards in urban areas. Nat Hazards Rev. 2004 August:147-58.
108. Sheridan SC, Kalkstein LS. Health watch/warning systems in urban areas. World Resource
Review. 1998:375-83.
109. Kim HH. Urban heat island. Int J Remote Sensing. 1992;13(12):2319-36.
110. Aniello C, Morgan K, Busbey A, Newland L. Mapping micro-urban heat islands using
Lansat TM and a GIS. Computer & Geosciences. 1995;21:965-9.

143
111. Lagadec P. Understanding the French 2003 heat wave experience: Beyond the heat, a multi-
layered challenge. J Contingencies & Crisis Man. 2004 December;12(4):160-9.
112. Leonardi GS, Hajat S, Kovats RS, Smith GE, Cooper D, Gerard E. Syndromic surveillance
use to detect the early effects of heat-waves: An analysis of NHS direct data in England. Soz
Praventivmed. 2006;51(4):194-201.
113. Ebi KL, Schmier JK. A stitch in time: Improving public health early warning systems for
extreme weather events. Epidemiol Rev. 2005;27:115-21.
114. Bernard SM, McGeehin MA. Municipal heat wave response plans. Am J Public Health.
2004 Sep;94(9):1520-2.
115. Sheridan SC, Kalkstein LS. Progress in heat watch-warning system technology. American
Meteorological Society. 2004 December 2004:1931.
116. Kosatsky T, Henry B. How Toronto and Montreal (Canada) respond to heat. In: Kirch W,
Menne B, Bertollini R, editors. Extreme weather events and public health responses. European
Union: Springer-Verlag on behalf of the World Health Organization; 2005. p. 167-72.
117. Lober WB, Karras BT, Wagner MM, Overhage JM, Davidson AJ, Fraser H, et al.
Roundtable on bioterrorism detection: Information system-based surveillance. J Am Med Inform
Assoc. 2002 Mar-Apr;9(2):105-15.
118. Buehler JW, Berkelman RL, Hartley DM, Peters CJ. Syndromic surveillance and
bioterrorism-related epidemics. Emerg Infect Dis. 2003 Oct;9(10):1197-204.

144
119. Henning KJ, Centers for Disease Control and Prevention (CDC). What is syndromic
surveillance? MMWR Morb Mortal Wkly Rep. 2004 Sep 24;53 Suppl:5-11.
120. Hurt-Mullen KJ, Coberly J. Syndromic surveillance on the epidemiologist's desktop:
Making sense of much data. MMWR Morb Mortal Wkly Rep. 2005 Aug 26;54 Suppl:141-6.
121. Sosin DM. Syndromic surveillance: The case for skillful investment. Biosecur Bioterror.
2003;1(4):247-53.
122. Estacio PL. Surge capacity for health care systems: Early detection, methodologies, and
process. Acad Emerg Med. 2006 Nov;13(11):1135-7.
123. Beitel AJ, Olson KL, Reis BY, Mandl KD. Use of emergency department chief complaint
and diagnostic codes for identifying respiratory illness in a pediatric population. Pediatr Emerg
Care. 2004 Jun;20(6):355-60.
124. Heffernan R, Mostashari F, Das D, Besculides M, Rodriguez C, Greenko J, et al. New York
City syndromic surveillance systems. MMWR Morb Mortal Wkly Rep. 2004 Sep 24;53
Suppl:23-7.
125. Irvin CB, Nouhan PP, Rice K. Syndromic analysis of computerized emergency department
patients' chief complaints: An opportunity for bioterrorism and influenza surveillance. Ann
Emerg Med. 2003 Apr;41(4):447-52.
126. Moore K. Real-time syndrome surveillance in Ontario, Canada: The potential use of
emergency departments and Telehealth. Eur J Emerg Med. 2004 Feb;11(1):3-11.

145
127. Hogan WR, Tsui FC, Ivanov O, Gesteland PH, Grannis S, Overhage JM, et al. Detection of
pediatric respiratory and diarrheal outbreaks from sales of over-the-counter electrolyte products.
J Am Med Inform Assoc. 2003 Nov-Dec;10(6):555-62.
128. Vergu E, Grais RF, Sarter H, Fagot JP, Lambert B, Valleron AJ, et al. Medication sales and
syndromic surveillance, France. Emerg Infect Dis. 2006 Mar;12(3):416-21.
129. Wagner MM, Robinson JM, Tsui FC, Espino JU, Hogan WR. Design of a national retail
data monitor for public health surveillance. J Am Med Inform Assoc. 2003 Sep-Oct;10(5):409-
18.
130. Edge VL, Pollari F, Lim G, Aramini J, Sockett P, Martin SW, et al. Syndromic surveillance
of gastrointestinal illness using pharmacy over-the-counter sales. A retrospective study of
waterborne outbreaks in Saskatchewan and Ontario. Can J Public Health. 2004 Nov-
Dec;95(6):446-50.
131. Meyer N, McMenamin J, Robertson C, Donaghy M, Allardice G, Cooper D. A multi-data
source surveillance system to detect a bioterrorism attack during the G8 summit in Scotland.
Epidemiol Infect. 2007 Aug 3:1-10.
132. Lazarus R, Kleinman K, Dashevsky I, Adams C, Kludt P, DeMaria A,Jr, et al. Use of
automated ambulatory-care encounter records for detection of acute illness clusters, including
potential bioterrorism events. Emerg Infect Dis. 2002 Aug;8(8):753-60.
133. Miller B, Kassenborg H, Dunsmuir W, Griffith J, Hadidi M, Nordin JD, et al. Syndromic
surveillance for influenza-like illness in an ambulatory care network. Emerg Infect Dis. 2004
Oct;10(10):1806-11.

146
134. Sloane PD, MacFarquhar JK, Sickbert-Bennett E, Mitchell CM, Akers R, Weber DJ, et al.
Syndromic surveillance for emerging infections in office practice using billing data. Ann Fam
Med. 2006 Jul-Aug;4(4):351-8.
135. Rolland E, Moore KM, Robinson VA, McGuinness D. Using Ontario's "Telehealth" health
telephone helpline as an early-warning system: A study protocol. BMC Health Serv Res. 2006
Feb 15;6(1):10.
136. Baker M, Smith GE, Cooper D, Verlander NQ, Chinemana F, Cotterill S, et al. Early
warning and NHS direct: A role in community surveillance? J Public Health Med. 2003
Dec;25(4):362-8.
137. Cooper DL, Verlander NQ, Smith GE, Charlett A, Gerard E, Willcocks L, et al. Can
syndromic surveillance data detect local outbreaks of communicable disease? A model using a
historical cryptosporidiosis outbreak. Epidemiol Infect. 2006(134):13.
138. Doroshenko A, Cooper D, Smith G, Gerard E, Chinemana F, Verlander N, et al. Evaluation
of syndromic surveillance based on National Health Service Direct derived data--England and
Wales. MMWR Morb Mortal Wkly Rep. 2005 Aug 26;54 Suppl:117-22.
139. Harcourt SE, Smith GE, Hollyoak V, Joseph CA, Chaloner R, Rehman Y, et al. Can calls to
NHS direct be used for syndromic surveillance? Commun Dis Public Health. 2001 Sep;4(3):178-
82.
140. Smith GE, Cooper DL, Loveridge P, Chinemana F, Gerard E, Verlander N. A national
syndromic surveillance system for England and Wales using calls to a telephone helpline. Euro
Surveill. 2006;11(12):220-4.

147
141. Lu J, Metzger K, Cajigal A, Konty K, Matte T. Identifying and modeling spatial patterns of
heat-related illness in New York City. International Society of Disease Surveillance; October;
Indianapolis, IN.; 2007 (poster presentation).
142. Toronto EMS Statistics. Accessed at: http://www.toronto.ca/ems/overview/statistics.htm
143. Clawson J, Olola CH, Heward A, Scott G, Patterson B. Accuracy of emergency medical
dispatchers' subjective ability to identify when higher dispatch levels are warranted over a
medical priority dispatch system automated protocol's recommended coding based on paramedic
outcome data. Emerg Med J. 2007 Aug;24(8):560-3.
144. Heward A, Damiani M, Hartley-Sharpe C. Does the use of the advanced Medical Priority
Dispatch System affect cardiac arrest detection? Emerg Med J. 2004 Jan;21(1):115-8.
145. Feldman MJ, Verbeek PR, Lyons DG, Chad SJ, Craig AM, Schwartz B. Comparison of the
medical priority dispatch system to an out-of-hospital patient acuity score. Acad Emerg Med.
2006 Sep;13(9):954-60.
146. Sporer KA, Youngblood GM, Rodriguez RM. The ability of emergency medical dispatch
codes of medical complaints to predict ALS prehospital interventions. Prehosp Emerg Care.
2007 Apr-Jun;11(2):192-8.
147. Hinchey P, Myers B, Zalkin J, Lewis R, Garner D. Low acuity EMS dispatch criteria can
reliably identify patients without high-acuity illness or injury. Prehosp Emerg Care. 2007 Jan-
Mar;11(1):42-8.

148
148. Clawson JJ, Dernocoeur KB. Principles of emergency medical dispatch. Third ed. Cottle
GW, Hayes N, Horewitz G, et al, editors. USA: Priority Press; 2000.
149. Medical Priority Consultants. The National Academy QA v11 guide: Medical Priority
Dispatch System. In: Medical Priority, editor. ; 2000.
150. Canadian Institute for Health Information (CIHI). Executive summary: Database
background and general data limitations document - National Ambulatory Care Reporting
System (NACRS). Ottawa, Ontario: 2007 October.
151. Institute for Clinical Evaluative Sciences (ICES). Improving health care data in Ontario.
ICES investigative report. Toronto: Institute for Clinical Evaluative Sciences: 2005.
152. Chapman WW, Dowling JN, Wagner MM. Generating a reliable reference standard set for
syndromic case classification. J Am Med Inform Assoc. 2005 Nov-Dec;12(6):618-29.
153. Duchin JS. Epidemiological response to syndromic surveillance signals. J Urban Health.
2003 Jun;80(2 Suppl 1):i115-6.
154. Espino JU, Wagner MM. Accuracy of ICD-9-coded chief complaints and diagnoses for the
detection of acute respiratory illness. Proc AMIA Symp. 2001:164-8.
155. Lazarus R, Kleinman KP, Dashevsky I, DeMaria A, Platt R. Using automated medical
records for rapid identification of illness syndromes (syndromic surveillance): The example of
lower respiratory infection. BMC Public Health. 2001;1:9.

149
156. Lewis MD, Pavlin JA, Mansfield JL, O'Brien S, Boomsma LG, Elbert Y, et al. Disease
outbreak detection system using syndromic data in the greater Washington DC area. Am J Prev
Med. 2002 Oct;23(3):180-6.
157. Koutsavlis AT, Kosatsky T. Environmental-temperature injury in a Canadian metropolis. J
Environ Health. 2003 Dec;66(5):40-5.
158. Rydman RJ, Rumoro DP, Silva JC, Hogan TM, Kampe LM. The rate and risk of heat-
related illness in hospital emergency departments during the 1995 Chicago heat disaster. J Med
Syst. 1999 Feb;23(1):41-56.
159. Beaton DE, Bombardier C, Cole DC, Hogg-Johnson S, Van Eerd D. A pattern recognition
approach to the development of a classification system for upper-limb musculoskeletal disorders
of workers. Scand J Work Environ Health. 2007 Apr;33(2):131-9.
160. Silverman BW. Some aspects of the spline smoothing approach to nonparametric regression
curve fitting. JRSS Series B. 1985 ;47 :1-52.
161. Pagano M, Gauvreau K. Correlation. In: Principles of Biostatistics. Belmont, California:
Duxbury Press; 2004. p. 363-78.
162. Cody RP, Smith JK. Applied statistics and the SAS programming language. Toronto, ON:
Prentice-Hall; 1997.
163. Diaz J, Garcia R, Lopez C, Linares C, Tobias A, Prieto L. Mortality impact of extreme
winter temperatures. Int J Biometeorol. 2005 Jan;49(3):179-83.

150
164. Kassomenos PA, Gryparis A, Katsouyanni K. On the association between daily mortality
and air mass types in Athens, Greece during winter and summer. Int J Biometeorol. 2007
Mar;51(4):315-22.
165. Piver WT, Ando M, Ye F, Portier CJ. Temperature and air pollution as risk factors for heat
stroke in Tokyo, July and August 1980-1995. Environ Health Perspect. 1999 Nov;107(11):911-6.
166. Kim Y, Joh S. A vulnerability study of the low-income elderly in the context of high
temperature and mortality in Seoul, Korea. Sci Total Environ. 2006 Dec 1;371(1-3):82-8.
167. Michelozzi P, De Sario M, Accetta G, de'Donato F, Kirchmayer U, D'Ovidio M, et al.
Temperature and summer mortality: Geographical and temporal variations in four Italian cities. J
Epidemiol Community Health. 2006 May;60(5):417-23.
168. Zhang Y, Huang W, London SJ, Song G, Chen G, Jiang L, et al. Ozone and daily mortality
in Shanghai, China. Environ Health Perspect. 2006 Aug;114(8):1227-32.
169. Dominici F, McDermott A, Zeger SL, Samet JM. On the use of generalized additive models
in time-series studies of air pollution and health. Am J Epidemiol. 2002 Aug 1;156(3):193-203.
170. He S. Generalized additive models for data with concurvity: Statistical issues and a novel
model fitting approach. PhD thesis in the Graduate School of Public Health. Pittsburgh, PA,
USA: University of Pittsburgh, 2004. 45 pp.
171. Lambert D. Zero-inflated Poisson regression, with an application to defects in
manufacturing. Technometrics. 1992;34(1):1-14.

151
172. Afifi AA, Kotlerman JB, Ettner SL, Cowan M. Methods for improving regression analysis
for skewed continuous or counted responses. Annu Rev Public Health. 2007;28:95-111.
173. Dominguez A, Munoz P, Cardenosa N, Martinez A, Cayla J, Meningococcal Disease Study
Group. Time-series analysis of meningococcal disease in Catalonia. Ann Epidemiol. 2007
Sep;17(9):654-62.
174. Khoshgoftaar TM, Gao K, Szabo RM. Comparing software fault predictions of pure and
zero-inflated poisson regression models. Int J Systems Sci. 2005 15 September;36(11):705-15.
175. Galan I, Tobias A, Banegas JR, Aranguez E. Short-term effects of air pollution on daily
asthma emergency room admissions. Eur Respir J. 2003 Nov;22(5):802-8.
176. Hastie TJ, Tibshirani RJ. Generalized additive models. London, UK: Chapman & Hall;
1990.
177. Josseran L, Nicolau J, Caillere N, Astagneau P, Brucker G. Syndromic surveillance based
on emergency department activity and crude mortality: Two examples. Euro Surveill.
2006;11(12):225-9.
178. Green DM, Swets JM. Signal detection theory and psychophysics. New York, USA: John
Wiley and Sons Inc.; 1966.
179. Hutwagner LC, Thompson WW, Seeman GM, Treadwell T. A simulation model for
assessing aberration detection methods used in public health surveillance for systems with
limited baselines. Stat Med. 2005 Feb 28;24(4):543-50.

152
180. Hutwagner L, Browne T, Seeman GM, Fleischauer AT. Comparing aberration detection
methods with simulated data. Emerg Infect Dis. 2005 Feb;11(2):314-6.
181. Box GEP, Jenkins GM. Time series analysis: Forecasting and control. Oakland, USA:
Holden-Day; 1976.
182. Glazier RH, Creatore MI, Gozdyra P, Matheson FI, Steele LS, Boyle E, et al. Geographic
methods for understanding and responding to disparities in mammography use in Toronto,
Canada. J Gen Intern Med. 2004 Sep;19(9):952-61.
183. Pine JC, Diaz JH. Environmental health screening with GIS: Creating a community
environmental health profile. Environ Health. 2000 April:9-22.
184. Lo CP, Yeung AKW. Concepts and techniques of geographic information systems. Clarke
KC, editor. Upper Saddle River, New Jersey: Prentice-Hall, Inc.; 2002.
185. Anselin L. Local indicators of spatial association – LISA. Geo Analysis. 1995
April;27(2):93-115.
186. Moran PAP. Notes on continuous stochastic phenomena. Biometrika. 1950;37:17-33.
187. Klinenberg E. Denaturalizing disaster: A social autopsy of the 1995 Chicago heat wave.
Theory Soc. 1999 April;28(2):239-95.
188. Claessens YE, Taupin P, Kierzek G, Pourriat JL, Baud M, Ginsburg C, et al. How
emergency departments might alert for pre-hospital heat-related excess mortality? Crit Care.
2006 Nov;10(6):R156.

153
189. Green H, Gilbert J, James R, Byard RW. An analysis of factors contributing to a series of
deaths caused by exposure to high environmental temperatures. Am J Forensic Med Pathol. 2001
Jun;22(2):196-9.
190. Toronto Public Health. Hot weather response plan update: Staff report. 2007 November.
191. Berger M, Shiau R, Weintraub JM. Review of syndromic surveillance: Implications for
waterborne disease detection. J Epidemiol Community Health. 2006 Jun;60(6):543-50.
192. Weisskopf MG, Anderson HA, Foldy S, Hanrahan LP, Blair K, Torok TJ, et al. Heat wave
morbidity and mortality, Milwaukee, Wis, 1999 vs 1995: An improved response? Am J Public
Health. 2002 May;92(5):830-3.
193. Keim SM, Mays MZ, Parks B, Pytlak E, Harris RM, Kent MA. Estimating the incidence of
heat-related deaths among immigrants in Pima County, Arizona. J Immigr Minor Health. 2006
Apr;8(2):185-91.
194. Alberdi JC, Diaz J, Montero JC, Miron I. Daily mortality in Madrid community 1986-1992:
Relationship with meteorological variables. Eur J Epidemiol. 1998 Sep;14(6):571-8.
195. Kalkstein LS. Health and climate change. Direct impacts in cities. Lancet. 1993 Dec
4;342(8884):1397-9.
196. Kawakami C, Ohshige K, Kubota K, Tochikubo O. Influence of socioeconomic factors on
medically unnecessary ambulance calls. BMC Health Serv Res. 2007 Jul 27;7:120.
197. Smoyer KE. Putting risk in its place: Methodological considerations for investigating
extreme event health risk. Soc Sci Med. 1998 Dec;47(11):1809-24.

154
198. Dolney TJ. The relationship between extreme heat and ambulance response calls for the city
of Toronto, Ontario, Canada. MA thesis in the Department of Geography. Kent, OH, USA: Kent
State University, 2003:111 pp.

155
Appendices
Appendix A: Summary of epidemiological studies of the relationship between heat and mortality (ordered chronologically by date of
publication from earliest to most recent)
Study population (reference number)
Exposure Outcome Results
All age groups in Barcelona, Spain between 1985-198986
Minimum and maximum temperature
Daily mortality (all-cause) and cardiovascular and respiratory mortality
Periods of at least 3 consecutive days of increased temperature were associated with increased total daily mortality by 2%, cardiovascular mortality by 4.6%, and respiratory mortality by 21.6%.
All age groups in Valencia, Spain, 1991-199380
Mean daily temperature
Daily mortality Increased in mortality between 1-4% for each 1°C increase in temperature for the overall population; greatest effect in those ages >70 years.
People aged > 65 years in the Netherlands between 1979-199782
Daily mean temperature
Daily mortality Average total excess mortality during heat waves was 12%.
All age groups in London, England between 1976-199649
Daily maximum, minimum, and mean temperature.
Daily mortality Increase in deaths of 3% for every one degree increase in mean temperature above 21.5°C.
All age groups in Sao Paulo, Brazil from 1991-199448
Daily mean, maximum, and minimum temperature
Daily mortality (all-cause and type-specific)
2.65 increase in all-cause mortality in the elderly per degree increase in temperature above 20°C
All age groups in England and Wales between August 4-13, 200343
Daily maximum and minimum temperature.
Excess all-cause mortality
There were 16% excess deaths; in London, deaths in those over the age of 75 increased by 59%.
All age groups in Spain between June 1 and August 31, 200387
Heat wave period between June 1 and August 31, 2003
Excess mortality Excess death was 8%.

156
All age groups in Portugal between July 30 and August 12, 200344
Heat wave period between July 30 and August 12, 2003
Excess mortality rate There was a 37% higher mortality rate than the value expected under normal temperature conditions.
All age groups in Budapest, Hungary between 1970-200045
Daily mean temperature
Daily mortality A 5°C increase in daily mean temperature above 18°C increases the risk of total mortality by 10.6% (and an even greater effect is seen on cardiovascular mortality).
People aged 45-64 years in Madrid, Spain between 1986-199751
Daily maximum and minimum temperature
Daily mortality (type-specific)
Attributable risk of 12.0% for circulatory diseases.
Residents of 4 Italian cities aged 35 or older who died during 1997-200335
Mean apparent temperature
All-cause mortality There was an overall increase d risk of mortality by 34% on days with mean apparent temperature of 30°C versus days with 20°C
All age groups in Seoul, Korea between 2000-200284
Daily mean, minimum, and maximum temperature
Daily mortality (all-cause)
There was a 1-3% increase in mortality for every 1°C increase in temperature.
All age groups in southern England between August 4-13 200385
Heat wave period between August 4-13, 2003
Excess mortality There was an overall increase in deaths of 33%; the excess was greatest in nursing homes where deaths increased by 42%.
People > 74 years during the heat wave in Genoa, Italy over 6 weeks in 200341
Daily maximum temperature and humidex
Excess all-cause mortality
Excess mortality was 1.5 times greater than expected.
All age groups in England and Wales between 1993-200381
Daily maximum, minimum, and mean temperature
Daily mortality A mean RR of 1.03 (1.02,1.03) was estimated per degree increase above the heat threshold of the 95th percentile of the temperature distribution in each region.
All heat fatalities reported in Pima county, Arizona in 2002 and 200383
Daily ambient high temperature and heat index.
Heat-related deaths. There was a 35% increase the odds of a heat-related death for each degree of increase in temperature above 32°C.

157
Appendix B: Influencing factors and underlying assumptions in 911 call process for HRI
Individual feels unwell Self-care Individual worsens Call to Toronto EMS
Ambient Temp
Influenced by underlying risk factors
AgePre-existing illness
SESBehavioural
Environmental
Assumptions:i) broad spectrum of morbidity that precedes mortality
ii) this spectrum is variable depending on both individualand environmental factors
Fluids, air conditioning…
Telehealth
Hospital (non-ambulance)
Visit GP, clinic
Does not seek help
Recovery
Assumption:i) individuals who call 911 may not represent the general population
ii) characteristics of residence vs. outdoor events callers will differ
Spectrum of heat-related illnessMild Severe
More severe illnessElderly
No other means of transportationIndividual calls Toronto EMS directly
Assumption: i) labelling phenomenon may influence the decision to seek medical help
DeathDirect effect
Indirect effect(i.e. harvesting)

158
Appendix C: Heat alerts and extreme heat alerts, Toronto, 2002-2005
Day Event 1 July 2002 Heat Alert 2 July 2002 Heat Alert 3 July 2002 Heat Alert 8 July 2002 Heat Alert 15 July 2002 Heat Alert 16 July 2002 Extreme Heat Alert 17 July 2002 Extreme Heat Alert 21 July 2002 Heat Alert 22 July 2002 Heat Alert 28 July 2002 Heat Alert 29 July 2002 Heat Alert 1 August 2002 Heat Alert 11 August 2002 Heat Alert 12 August 2002 Heat Alert 13 August 2002 Heat Alert 14 August 2002 Heat Alert TOTAL: 15 Heat Alerts, 2 Extreme Heat Alerts 23 June 2003 Heat Alert 24 June 2003 Extreme Heat Alert 25 June 2003 Extreme Heat Alert 26 June 2003 Extreme Heat Alert 3 July 2003 Heat Alert 4 July 2003 Heat Alert TOTAL: 3 Heat Alerts, 3 Extreme Heat Alerts 8 June 2004 Heat Alert 9 June 2004 Heat Alert TOTAL: 2 Heat Alerts 6 June 2005 Heat Alert 7 June 2005 Heat Alert 9 June 2005 Heat Alert 10 June 2005 Extreme Heat Alert 11 June 2005 Extreme Heat Alert 12 June 2005 Extreme Heat Alert 13 June 2005 Extreme Heat Alert 14 June 2005 Extreme Heat Alert 25 June 2005 Heat Alert 27 June 2005 Heat Alert 28 June 2005 Extreme Heat Alert 29 June 2005 Extreme Heat Alert 30 June 2005 Extreme Heat Alert 10 July 2005 Heat Alert 11 July 2005 Extreme Heat Alert 12 July 2005 Extreme Heat Alert 13 July 2005 Extreme Heat Alert

159
14 July 2005 Extreme Heat Alert 15 July 2005 Extreme Heat Alert 16 July 2005 Extreme Heat Alert 17 July 2005 Extreme Heat Alert 18 July 2005 Extreme Heat Alert 2 August 2005 Heat Alert 3 August 2005 Extreme Heat Alert 4 August 2005 Extreme Heat Alert 8 August 2005 Heat Alert TOTAL: 8 Heat Alerts, 18 Extreme Heat Alerts

160
Appendix D: 911 MPDS determinants potentially representing HRI
Rank Code Number
Code Description
01D01 Abdominal pain/problems – Not alert 01C04 Abdominal pain/problems – Fainting or near fainting ≥50 01C03 Abdominal pain/problems – Females with fainting or near fainting 12-50 01C02 Abdominal pain/problems – Males with pain above navel ≥35 01C01 Abdominal pain/problems – Females with pain above the navel ≥45 01A01 Abdominal pain/problems – abdominal pain 06E01 Breathing problems – Ineffective breathing 06D01 Breathing problems – Severe respiratory distress 06D02 Breathing problems – Not alert 06D03 Breathing problems – Clammy 06C01 Breathing problems – Abnormal breathing 06C02 Breathing problems – Cardiac history 07A03 Burns/explosion – Sunburn or minor burns (<hand size) 09E01 Cardiac or respiratory arrest/death – Not breathing at all 09E02 Cardiac or respiratory arrest/death – Breathing uncertain (agonal) 09D01 Cardiac or respiratory arrest/death – Ineffective breathing 09B01 Cardiac or respiratory arrest/death – Obvious death (unquestionable) 09O01 Cardiac or respiratory arrest/death – Expected death (unquestionable) 10D01 Chest pain – Severe respiratory distress 10D02 Chest pain – Not alert 10D03 Chest pain – Clammy 10C01 Chest pain – Abnormal breathing 10C02 Chest pain – Cardiac history 10C04 Chest pain – Breathing normally ≥35

161
10A01 Chest pain – Breathing normally <35 13D01 Diabetic problems – Unconscious 13C01 Diabetic problems – Not alert 13C02 Diabetic problems – Abnormal behaviour 13C03 Diabetic problems – Abnormal breathing 13A01 Diabetic problems – Alert 18C01 Headache – Not alert 18C02 Headache – Abnormal breathing 18C03 Headache- Speech problems 18C06 Headache – Change in behaviour (≤3 hours) 18B01 Headache – Unknown status (3rd party caller) 18A01 Headache- Breathing normally 19D01 Heart problem/A.I.C.D – Severe respiratory distress 19D02 Heart problem/A.I.C.D – Not alert 19D03 Heart problem/A.I.C.D – Clammy 19C02 Heart problem/A.I.C.D – Abnormal breathing 20D01 Heat/Cold exposure- Not alert 20C01 Heat/Cold exposure – Cardiac history 20B01 Heat/Cold exposure – Change in skin colour 20B02 Heat/Cold exposure – Unknown status (3rd party caller) 20A01 Heat/Cold exposure - Alert 25D01 Psychiatric/abnormal behaviour/suicide attempt – Not alert 25B01 Psychiatric/abnormal behaviour/suicide attempt – Violent (police must secure scene) 26D01 Sick person (specific diagnosis) – Not alert 26C01 Sick person (specific diagnosis) – Cardiac history (complaint conditions 2-28 not identified) 26B01 Sick person (specific diagnosis) – Unknown status (3rd party caller)

162
26A01 Sick person (specific diagnosis) – No priority symptoms (conditions 2-28 not identified) 26A02-
28 Sick person (specific diagnosis) – Non-priority complaints
28C01 Stroke/CVA – Not alert 28C02 Stroke/CVA – Abnormal breathing 28C03 Stroke/CVA – Speech or movement problems 28C05 Stroke/CVA – Stroke history 28C06 Stroke/CVA – Breathing normally ≥35 28B01 Stroke/CVA – Unknown status (3rd party caller) 28A01 Stroke/CVA – Breathing normally <35 31E01 Unconscious/fainting – Ineffective breathing 31D01 Unconscious/fainting – Unconscious (at end of interrogation) 31D02 Unconscious/fainting – Severe respiratory distress 31D03 Unconscious/fainting – Not alert 31C01 Unconscious/fainting – Alert with abnormal breathing 31C02 Unconscious/fainting – Cardiac history 31C03 Unconscious/fainting – Multiple fainting episodes 31C04 Unconscious/fainting – Single or near fainting episode and alert ≥35 31C05 Unconscious/fainting – Females 12-50 with abdominal pain 31A01 Unconscious/fainting – Single or near fainting episode and alert <35 32D01 Unknown trouble (man down) – Life status questionable 32B01 Unknown trouble (man down) – Standing, sitting, moving or talking 32B02 Unknown trouble (man down) – Medical alert notifications 32B03 Unknown trouble (man down) – Unknown status (3rd party caller)

163
Appendix E: Comparison of different smoothers for GAM models – loess (lo) and spline (s) Table 4.8a: 2002 – Maximum temperature
Variable GAM Poisson model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day †
0.1448 0.2330
1.16 1.26
0.0411 0.2200
0.0007 0.2927
0.1527 0.2413
1.16 1.27
0.0400 0.2157
0.0003 0.2668
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § ppb; Table 4.8b: 2002 – Mean temperature
Variable GAM model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day †
0.1786 0.3395
1.20 1.40
0.0431 0.2300
0.0001 0.1440
0.1884 0.3506
1.21 1.42
0.0421 0.2260
<.0001 0.1249
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § ppb Table 4.8c: 2003 – Maximum temperature
Variable GAM model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day †
0.1928 0.1822
1.21 1.20
0.0620 0.2646
0.0026 0.4931
0.1836 0.0811
1.20 1.08
0.0647 0.2744
0.0058 0.7683
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § ppb Table 4.8d: 2003 – Mean temperature
Variable GAM model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day †
0.2418 0.1632
1.27 1.18
0.0661 0.2660
0.0005 0.5415
0.2339 0.0657
1.26 1.07
0.0701 0.2747
0.0013 0.8115
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § ppb Table 4.8e: 2004 – Maximum temperature
Variable GAM model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day †
0.2789 0.3069
1.32 1.36
0.0610 0.3010
<.0001 0.3110
0.2692 0.2867
1.31 1.33
0.0610 0.3044
<.0001 0.3492
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § ppb

164
Table 4.8f: 2004 – Mean temperature
Variable GAM model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day †
0.3062 0.3108
1.36 1.36
0.0695 0.3045
<.0001 0.3106
0.3004 0.2975
1.35 1.35
0.0698 0.3075
<.0001 0.3362
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase; § ppb Table 4.8g: 2005 – Maximum temperature
Variable GAM model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Max. daily temperature* Day †
0.2783 0.2958
1.32 1.34
0.0383 0.1988
<.0001 0.1407
0.2713 0.2937
1.31 1.34
0.0305 0.1593
<.0001 0.1396
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase Table 4.8h: 2005 – Mean temperature
Variable GAM model (lo) GAM Poisson model (s) estimate RR standard
error p-value estimate RR standard
error p-value
Mean daily temperature* Day †
0.2914 0.3922
1.34 1.48
0.0356 0.1854
<.0001 0.0375
0.2867 0.3759
1.33 1.46
0.0303 0.1584
<.0001 0.0435
p < 0.05 bolded ; * 1°C increase; † weekday vs. weekend; ‡ 1% increase

165
Appendix F: Percentage of heat-related calls and mean daily temperature by determinant grouping, 2002-2005 (June 1-August 31) 2002
------- mean temperature _____ percent of calls

166
2003
------- mean temperature _____ percent of calls

167
2004
------- mean temperature _____ percent of calls

168
2005
------- mean temperature _____ percent of calls

169
Appendix G: Investigation of associations between different spike thresholds for 911 calls and emergency department (ED) visits and public health heat alert notifications (based on synoptic weather system mortality projections) Heat Alert or Extreme Heat Alert Day 911 Call Spike* (>=2) Yes No Total Yes 40 53 93 No 10 265 275 Total 50 318 368 p-value (McNemar’s) for table <0.0001 * spike is defined as a day where there are 2 or more heat-related calls Heat Alert or Extreme Heat Alert Day 911 Call Spike* (>=4) Yes No Total Yes 28 20 48 No 22 298 320 Total 50 318 368 p-value (McNemar’s) for table = 0.7576 * spike is defined as a day where there are 4 or more heat-related calls Heat Alert or Extreme Heat Alert Day ED Visit Spike* (>=1) Yes No Total Yes 40 73 113 No 10 245 255 Total 50 318 368 p-value (McNemar’s) for table <0.0001 * spike is defined as a day where there are 1 or more heat-related visits Heat Alert or Extreme Heat Alert Day ED Visit Spike* (>=3) Yes No Total Yes 17 11 28 No 33 307 340 Total 50 318 368 p-value (McNemar’s) for table <0.0001 * spike is defined as a day where there are 3 or more heat-related visits